
Submitted:
15 August 2024
Posted:
20 August 2024
You are already at the latest version
Abstract
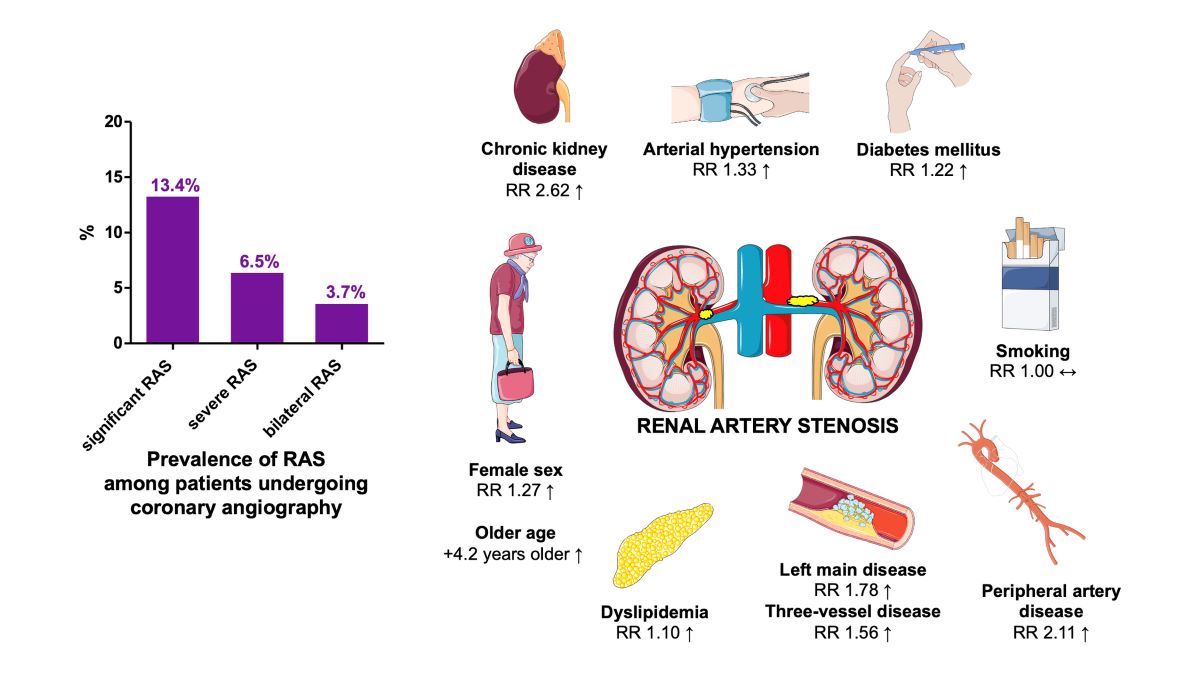
Background/Objectives: RAS is associated with coronary artery disease (CAD), exacerbation of arterial hypertension and progression to heart failure, but remains frequently unrecognised in clinical practice. Methods: We conducted a systematic review and meta-analysis of studies by pooling data of patients undergoing CAG due to suspected or stable CAD that received a bilateral renal artery angiography; Results: A total of 31 studies with 31,689 patients were included (mean age 63.2±8.7 years, 20.9% were female). Overall, 13.4% (95%CI 10.5-16.7%) of patients undergoing coronary angiography had significant RAS, with 6.5% (95% CI 4.5-8.9%) and 3.7% (95%CI 2.5-5.2%) having severe and bilateral RAS. The mean weighted proportion of patients with 3-vessel coronary disease (3VD) was 25.1 (95%CI 19.6-30.9%) while 4.2% (95%CI 2.6-6.2%) had leftmain (LM) coronary disease. Patients with RAS compared to those without RAS were significantly older (mean difference - MD 4.2 years, (95%CI 3.8-4.6). The relative risk of RAS was greater for the female sex (risk ratio, 95%CI; RR 1.3, 1.03-1.57), presence of diabetes (RR 1.2, 1.10-1.36), arterial hypertension (RR 1.3, 1.21-1.46), dyslipidemia (RR 1.1, 1.06-1.14), peripheral artery disease-PAD (RR 2.1, 1.40-3.16), chronic kidney disease-CKD (RR 2.6, 2.04-3.37), 3VD (RR 1.6, 1.30-1.87), and LM disease (RR 1.8, 1.28-2.47). Smoking had a neutral effect on the risk of RAS occurrence (RR 1.0, 0.94-1.06); Conclusions: RAS is common in patients undergoing coronary angiography. CKD, PAD, older age, and severe CAD were among the strongest predictors for the presence of significant RAS.
Keywords:
coronary artery disease
; coronary angiography
; prevalence
; renal artery stenosis
; risk factors
1. Introduction
Renal artery stenosis (RAS) is an important, but frequently unrecognised clinical condition. It shares common etiopatogenesis with other atherosclerotic diseases such as coronary artery disease (CAD), cerebrovascular disease (CVD) or peripheral artery disease (PAD).[1] The detection of significant RAS is clinically relevant as the condition can perpetuate the progression of associated cardiovascular disease due to renovascular hypertension and lead to heart failure due to cardiorenal syndrome with renin-angiotensin-aldosterone (RAAS) system activation.[2] Among patients with suspected CAD undergoing diagnostic coronary angiography, presence of RAS carries important prognostic implications. It was independently associated with a 2-fold increased risk of all-cause mortality, regardless of many confounders and type of revascularization received.[3] Four-year survival among patients undergoing catheterization was 21% lower among patients with established RAS compared to those without RAS.[4] In patients with renal insufficiency or PAD, RAS was common and its presence was strongly associated with increased mortality.[5,6] Even in asymptomatic individuals without known CVD, presence of renal artery calcification on CT was associated with increased all-cause mortality.[7]
To our best knowledge, this study is the first systematic review and meta-analysis examining the prevalence and clinical factors associated with renal artery stenosis among patients with suspected or established CAD. We conducted an up-to-date analysis of the most relevant literature in past two decades reporting on the prevalence and characteristics of RAS in patients who underwent simultaneous coronary and renal angiography.
2. Materials and Methods
The search strategy was devised by one of the investigators (JAB) while the search of electronic databases was independently carried out by JAB and ISB. Electronic databases included in the search were the National Library of Medicine (NLM) – PubMed, Ovid MEDLINE, Ovid Journals (full text), EMBASE, and SCOPUS. Search was conducted by using search terms: ”renal artery stenosis“ AND ”coronary artery disease” AND ”diagnostic angiography” AND/OR ”cardiac catheterization”. These databases were manually searched to obtain full records of original articles (observational cohort studies) that were specifically designed to investigate and to report on occurence of renal artery stenosis in the setting of cardiac catheterization for stable CAD or suspected CAD. The search was limited to records published in relevant peer-reviewed journals in the English language in the last 20 years (from 2002 until 2022). Similarly, only observational cohort studies involving adult human subjects were considered. The date of the last database search was performed on July 1st, 2022. All searches were independently manually performed by two reviewers (JAB, ISB) and potential studies were independently screened. Each investigator performed independent deletion of duplicate records, screening of available titles and abstracts, and provided final classification of studies as ”excluded“ or requiring further assessment or additional clarification. Such studies were labeled as “potential for inclusion“. If there was a discrepancy between the two investigators concerning the search strategy, this was resolved by the joint discussion involving the opinion of the third investigator. The meta-analysis was conducted in accordance to the PRISMA reporting recommendations (Preferred Reporting Items for Systematic Review and Meta-Analyses).[8]
Study inclusion criteria were: a) adult patients 18 years of age or older; b) patients with established stable CAD (chronic coronary syndrome) or suspected CAD undergoing diagnostic coronary angiography accompanied with additional angiography of renal arteries; c) non-randomized/retrospective/observational study design; d) studies explicitly reporting on the main outcome for this study which was the prevalence of renal artery stenosis in previously described cohorts. Exclusion criteria were: a) studies involving non-adult patients; b) studies that examined renal artery stenosis in the setting of acute coronary syndromes; c) studies designed as randomized controlled trials; d) studies that were conducted among patients with established or suspected CAD undergoing diagnostic coronary angiography but did not perform concomitant angiography of renal arteries; e) studies that did not report on the principal outcome of the interest such as the prevalence of renal artery stenosis (being significant and/or severe and/or bilateral); f) studies that did not provide basic data on study length, setting, and provided no description about relevant baseline patients characteristics such as age, sex, comorbidities, and other clinical factors; g) studies that were duplicate reports without additional or updated outcome data.
Data were manually extracted by three investigators (JAB, ISB, and KS) and were inserted in predefined and customized tables in MS Word format. Baseline data on age, sex distribution, diabetes mellitus, arterial hypertension, dyslipidemia, smoking, renal failure, peripheral vascular disease, carotid artery stenosis, and previous myocardial infarction were captured in these tables. Furthermore, study data including the total number of enrolled patients, study period and location, type of study (multicentric or single-center), and study design were recorded. For each study, following angiographic variables and their prevalences were recorded in the predefined tables: significant RAS (in most studies defined as 50% or more luminal stenosis of at least one renal artery), severe RAS (in most studies defined as 70% or more luminal stenosis of at least one renal artery), bilateral RAS (significant RAS affecting both renal arteries), one vessel CAD, two vessel CAD, three vessel CAD, and left main CAD. Study quality assessment was performed by using the Ottawa-Newcastle Scale for the assessment of quality of non-randomized studies.[9] All studies were independently scored by investigators KS and WM and the maximum of 9 stars could be assigned to an individual study (shown in Supplemental Table S1).
For the estimation of prevalence of significant RAS, severe RAS, bilateral RAS, three vessel CAD, and left main CAD we used weighted-proportion analysis and for these endpoints a sample size-weighted pooled proportions were reported at all instances. Risk ratio (RR) with 95% confidence intervals (95% CI) was used as the main summary measure for effect estimates on predefined dichotomous outcomes. Mean difference analysis was performed to determine possible absolute numerical differences in prespecified continuous outcomes such as age in patiens with vs. without RAS. Random-effects model with Mantel-Haenszel statistics was applied for the principal meta-analysis. Meta-analysis was performed by using Review Manager software (RevMan, version 5.4, The Cochrane Collaboration, 2020) and MedCalc Statistical software (version 20.112, Medcalc Software Ltd, Ostend, Belgium).
Chi-square (χ2) test of heterogeneity and Higgins I2 statistic of non-consistency were used to assess heterogeneity across included studies. Studies with an I2 statistic of 15% to <35% were considered to have low heterogeneity; >35% to 75% - moderate heterogeneity, and those with I2 statistic >75% were considered to have a high heterogeneity.
Publication bias was assessed by visual inspection of obtained funnel plots and with formal Egger’s test calculation. In this regard, p-values <0.05 indicated significant publication bias across included studies. All p-values reported in the manuscript were two-tailed and results were considered statistically significant if p<0.05 unless explicitly stated otherwise.
3. Results
Thirty-one international study with total of 31,689 patients enrolled were included in the final analysis, as shown in the PRISMA flowchart depicted in Figure 1.[10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40]
Most studies were single-center, prospective or observational cohort studies. Only two were multicentre cross-sectional studies.[16,41] Three studies were from North America, six from Europe, seven from Central or East Asia, thirteen from Middle East or North Africa, and two form South America as shown in Table 1.
The weighted mean age of the entire studied population was 63.2±8.7 years. Across whole patient sample, women were represented with a weighted average of 36.4%. The weighted mean proportion of standard modifiable cardiovascular risk factors such as diabetes mellitus, arterial hypertension, dyslipidemia, smoking, peripheral vascular disease, carotid artery stenosis, and history of MI are shown in Table 2 while detailed baseline patient characteristics across individual studies are provided in the Supplemental Table S1.
The pooled proportion of significant RAS (≥50% stenosis) in 22,757 patients undergoing coronary angiography was 13.4% (95% CI 10.5-16.7%) as shown in Figure 2A. Furthermore, the pooled proportion of severe RAS (≥70% stenosis) in 11,903 patients undergoing coronary angiography was 6.5% (95% CI 4.5-8.9%) as shown in Figure 2B. Finally, the pooled proportion of bilateral RAS in 17,167 patients undergoing coronary angiography was 3.7% (95% CI 2.5-5.2%) as depicted in Figure 2C.
In terms of angiographic coronary artery disease (CAD) burden, the pooled weight-adjusted proportion of three-vessel coronary artery disease (3VD) was 25.1 (95% CI 19.6-30.9%) and this finding was based on data from 14,771 patients pooled from 23 studies (Figure 3A). Significant left main (LM) coronary disease was detected in 4.2% of cases (95% CI 2.6-6.2%) and this was based on data from 10,670 patients from 13 studies (Figure 3B). Detailed angiographic characteristics for each particular study (where available) are also provided in Supplemental Table 2. Detailed characteristics of each particular study included in this systematic review and meta-analysis are shown in Supplemental Table 3.
The impact of anthropometric factors such as age and female sex, and cardiovascular/clinical factors including diabetes mellitus (DM), arterial hypertension, dyslipidemia, smoking, chronic kidney disease (CKD), three-vessel coronary disease (3VD), left-main (LM) disease and peripheral artery disease (PAD) were evaluated for the potential association with RAS occurence in the meta-analysis. As shown in Table 3, and in the order of decreasing magnitude, CKD was found to be the most robust predictor of RAS as it was associated with more than 2.5-fold increase in the relative risk of RAS compared to patients without CKD. This was followed by PAD and LM disease that were associated with a 2-fold and 1.8-fold increases in the relative risk of RAS occurence. Likewise, 3VD was associated with a 56% relative risk increase of RAS.
Female sex and arterial hypertension were both associated with an increase of a relative risk of RAS (RR 1.3, and RR 1.33,) while smoking was not identified as a significant variable impacting on RAS occurence (RR 1.0). Similarly, diabetes mellitus and dyslipidemia were associated with a 22% and 10% increases in the relative risk of RAS occurence (RR 1.2 and RR 1.10). In terms of age, meta-analysis showed that patients with RAS were significantly older than patients without RAS. In fact, there was a mean age difference of 4.16 years (95% CI 3.75-4.58 years,) between patients with RAS versus those without RAS. The Figure 4 (Graphical Abstract) summarizes clinical factors associated with RAS and shows prevalence of significant, severe, and bilateral RAS among patients undergoing simultaneous coronary and renal angiography.
Detailed analyses with generated funnel plots (publication bias) and forest plots of individual clinical risk factors and consequent risk ratios comparing patients with RAS vs. non-RAS are provided in Supplemental Appendix (Supplemental Figures 1-15).
4. Discussion
We present the largest published data set on patients undergoing simultaneous coronary artery and renal artery catheterization. The key finding of our systematic review and meta-analysis is that among patients undergoing coronary angiography, around 13% have a significant RAS. About 6% of patients will have severe RAS and in almost 4% RAS is bilateral. Most included studies reported similar prevalence, however, two papers reported a markedly higher prevalence of significant RAS (38 to 39%).[30,40] Part of the reasons why in these two studies the proportions of RAS were higher could be due to the pooling and reporting of significant and severe RAS together. Another reason is possibly a high proportion of patients with previous MI (36%) in the study by Rokni et al. which is in contrast to other studies (range 15-30%) and hence possibly indicating a population with higher end-organ damage. Both studies originate from Iran and therefore racial or regional factors may play an additional role.
The prevalence of significant RAS in patients undergoing coronary angiography appears high compared to previously reported 2.7% found among patients with moderate-to-severe arterial hypertension.[42] In a population with established end-organ disease, such as peripheral artery disease (PAD), the prevalence of significant RAS was with 9.6% similar to our findings.[43] In very high-risk cohorts, RAS was previously even more frequently reported. Kuroda et al. described in a small study of patients who suffered fatal stroke on autopsy severe RAS (≥75% luminal area narrowing) in 10.4% patients, and the proportion of severe RAS was even higher in a subgroup of stroke patients who died and were known to have renal insufficiency with 28.6%.[44] These data reflect intricate pathophysiological relationships since significant or severe renal artery stenosis is an important driver of renal failure and CKD while CKD is an independent risk factor for CAD development.
Another key finding of our study was the determination of clinical factors associated with RAS occurence. Factors showing strongest association were older age, known CKD, and PAD. Patients with RAS were more than 4 years older compared to patients without RAS. Pre-existing CKD increased the relative risk of having RAS by almost three-fold, while patients with PAD were almost 2.5 times more at risk of having a significant RAS. Other clinical factors increasing the relative risk of RAS by 20 to 90% were female sex, arterial hypertension, diabetes, 3VD and LM disease. Interestingly, smoking did not pose any additional risk. However, it should be noted that smoking was not equally defined in all studies as it is unclear if some studies considered previous smoking as smoking or if only active smoking at the time of enrollment was captured. Other authors reported similar findings. For example, Ozkan et al. showed that in PAD patients, advanced age and hypertension were closely associated with the presence of significant RAS.[43] Sani et al. reported in 260 hypertensive and/or diabetic consecutive patients who underwent simultaneous coronary and renal artery catheterization that female sex, multivessel coronary disease and reduced glomerular filtration rate were independent predictors of significant RAS .[41] In a smaller study (n=165), Zandparsa et al. again identified arterial hypertension and increased serum creatinine levels as independent predictors of RAS. However, in this study, the severity of CAD as assessed by the Gensini score was not predictive of RAS.[45] This is possibly due to the rather smaller sample size.
The important question remaining is the clinical implication of RAS finding during coronary angiography and if such investigation should be pursued. In other words, if the RAS is detected, whether a simultaneous percutaneous coronary intervention (PCI) and intervention on renal arteries is feasible and what would be the clinical impact and net potential benefit for the patient. Unfortunately, there is a great paucity of data on this topic. Dong et al. published an article describing a retrospective cohort of 149 patients with simultaneous PCI and PTRAS (percutaneous transluminal renal artery stenting) and reported on the feasibility and safety of such an approach. This intervention led to improved arterial blood pressure control and reduced left ventricular mass (LVM) index, however it did not impact on changes in renal function.[46] Reznik et al. reported similar finding of LVM reduction in patients undergoing RAS stenting, however in their study this effect was independent from blood pressure reduction.[47] Following RAS stenting, reduction in LV filling pressures was observed in heart failure (HF) patients.[48] However, no randomized studies have thus far addressed the approach of PCI + PTRAS vs. PCI alone in patients with both established CAD and RAS and if such an approach would improve clinicial and patient-oriented outcomes. The retrospective study of Dong and colleagues combining PCI and PTRAS suggested a net clinical benefit in population of patients with HF and preserved ejection fraction, however, these findings should be first replicated in randomized studies.
Taken together, such a dual revascularization approach might be feasible for selected patient populations exhibiting both high-risk coronary and renal anatomy thus reflecting severe atherosclerotic burden. The risk of contrast-induced nephropathy (CIN) should be weighted against the potential benefits of dual revascularization and even vascular access approach and other factors might play an important role in this - e.g., femoral vs. radial approach (femoral naturally being more convenient for performing bilateral renal angiography), the experience of the operator (more experienced operators will likely use fewer contrast injections and will establish faster access to designated vascular territories).
There are several limitations to our study. First, the exact technique of RAS severity assessment is not described in detail in many of the studies involved in this analysis. Secondly, many of the studies do not describe clearly which cases of bilateral RAS had significant or severe stenoses. Third, the lack of individual data does not allow a direct comparison between patients who had normal coronary angiograms vs. patients who had significant coronary artery disease. However, pooled risk ratios from individual analyses confirm a significantly higher proportion of RAS occurrence in patients with significant coronary disease burden. Furthermore, due to the observational design of studies included in the analysis and the lack of consecutive enrollment of patients in most of the studies, a potential selection bias should be acknowledged. In that sense, it remains unclear how and which patients were selected to receive renal artery angiography on top of standard coronary angiography. Finally, an issue of high heterogeneity for some of the outcomes should be mentioned which can be reasonably explained by the large variability of studies in terms of their country of origin, patient population, and differences in definition/reporting of the RAS. On the other hand, the generalizability and representativeness of the presented findings in this study should be high due to the inclusion of a robust number of studies conducted in centers worldwide.
5. Conclusions
Renal artery stenosis is common in patients undergoing coronary artery catheterization. Our results show that between 1:7 to 1:10 patients undergoing diagnostic coronary angiography is likely to have significant RAS. Clinical factors such as chronic kidney disease, peripheral artery disease, older age, and severe coronary artery disease are the strongest associated factors with risk of having a significant RAS. Factors showing weaker, however, significant association with significant RAS were female gender, arterial hypertension, dyslipidemia, and diabetes mellitus. Smoking does not appear to be associated with RAS.
Supplementary Materials
The following supporting information can be downloaded at: preprints.org, Supplemental Figures: publication bias blots and calculations for the pooled proportions; Supplemental Tables: title; Video S1: title.
Author Contributions
Conceptualization, K.S. and J.A.B.; methodology, K.S., J.B., M.W., and C.S.K.; formal analysis, K.S., J.M., M.K., I.S.B. and J.A.B.; writing—original draft preparation, K.S., M.W, I.S.B., C.S.K., J.M. and M.K.; writing—review and editing, J.B. and J.A.B.; visualization, K.S. and I.S.B.; project administration, J.A.B; funding acquisition, J.A.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available upon reasonable request from the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- McLaughlin K, Jardine AG, Moss JG. Renal artery stenosis. BMJ. 2000;320(7242):1124-7.
- Gupta R, Syed M, Ashcherkin N, Chen K, Vaidya PP, Cooper CJ. Renal Artery Stenosis and Congestive Heart Failure: What Do We Really Know? Curr Cardiol Rep. 2019;21(8):74.
- Conlon PJ, Little MA, Pieper K, Mark DB. Severity of renal vascular disease predicts mortality in patients undergoing coronary angiography. Kidney Int. 2001;60(4):1490-7. [CrossRef]
- Conlon PJ, Athirakul K, Kovalik E, et al. Survival in renal vascular disease. Journal of the American Society of Nephrology. 1998;9(2):252-6. [CrossRef]
- Uzu T, Takeji M, Yamada N, et al. <B>Prevalence and Outcome of Renal Artery Stenosis in Atherosclerotic Patients with Renal Dysfunction</B>. Hypertension Research. 2002;25(4):537-42. [CrossRef]
- Mui K-W, Zeebregts CJ, van den Hout H, van Baal JG, Navis G, Jan-Woittiez A. Impact of incidental renal artery stenosis on long-term mortality in patients with peripheral arterial disease undergoing vascular procedure. J Vasc Surg. 2011;54(3):785-90. [CrossRef]
- Rifkin DE, Ix JH, Wassel CL, Criqui MH, Allison MA. Renal artery calcification and mortality among clinically asymptomatic adults. J Am Coll Cardiol. 2012;60(12):1079-85. [CrossRef]
- Moher D, Liberati A, Tetzlaff J, Altman DG, The PG. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLOS Medicine. 2009;6(7):e1000097. [CrossRef]
- Wells GA, Wells G, Shea B, et al., editors. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses2014.
- Aqel RA, Zoghbi GJ, Baldwin SA, et al. Prevalence of renal artery stenosis in high-risk veterans referred to cardiac catheterization. J Hypertens. 2003;21(6):1157-62. [CrossRef]
- Bageacu S, Cerisier A, Isaaz K, Nourissat A, Barral X, Favre JP. Incidental Visceral and Renal Artery Stenosis in Patients Undergoing Coronary Angiography. European Journal of Vascular and Endovascular Surgery. 2011;41(3):385-90. [CrossRef]
- Buller CE, Nogareda JG, Ramanathan K, et al. The profile of cardiac patients with renal artery stenosis. J Am Coll Cardiol. 2004;43(9):1606-13. [CrossRef]
- Cohen MG, Pascua JA, Garcia-Ben M, et al. A simple prediction rule for significant renal artery stenosis in patients undergoing cardiac catheterization. Am Heart J. 2005;150(6):1204-11. [CrossRef]
- Dzielińska Z, Januszewicz A, Demkow M, et al. Cardiovascular risk factors in hypertensive patients with coronary artery disease and coexisting renal artery stenosis. J Hypertens. 2007;25(3):663-70. [CrossRef]
- El-Mawardy RH, Ghareeb MA, Mahdy MM, Sabet SS, Nammas WM. Prevalence and predictors of renal artery stenosis in hypertensive patients undergoing elective coronary procedures. 2008;10(11):844-9. [CrossRef]
- Ghaffari S, Sohrabi B, Siahdasht RB, Pourafkari L. Prevalence and predictors of renal artery stenosis in hypertensive patients undergoing coronary angiography. Hypertens Res. 2009;32(11):1009-14. [CrossRef]
- Imori Y, Akasaka T, Ochiai T, et al. Co-existence of carotid artery disease, renal artery stenosis, and lower extremity peripheral arterial disease in patients with coronary artery disease. Am J Cardiol. 2014;113(1):30-5. [CrossRef]
- Khatami MR, Edalati-Fard M, Sadeghian S, Salari-Far M, Bs MP. Renal artery stenosis in patients with established coronary artery disease: prevalence and predicting factors. Saudi J Kidney Dis Transpl. 2014;25(5):986-91. [CrossRef]
- Kobo O, Hammoud M, Makhoul N, Omary H, Rosenschein U. Screening, diagnosis, and treatment of renal artery stenosis by percutaneous transluminal renal angioplasty with stenting. Isr Med Assoc J. 2010;12(3):140-3.
- Liu B-C, Tang R-N, Feng Y, Wang Y-L, Yin L-F, Ma G-S. A single chinese center investigation of renal artery stenosis in 141 consecutive cases with coronary angiography. Am J Nephrol. 2004;24(6):630-4. [CrossRef]
- Marcantoni C, Rastelli S, Zanoli L, et al. Prevalence of renal artery stenosis in patients undergoing cardiac catheterization. Intern Emerg Med. 2013;8(5):401-8.
- Mirbolouk F, Salari A, Ashouri A, Mahdavi-Roshan M, Gholipour M. Frequency of renal artery stenosis and associated factors in patients undergoing coronary angiography. Journal of Nephropathology. 2019;8(2):14-. [CrossRef]
- Ollivier R, Boulmier D, Veillard D, et al. Frequency and predictors of renal artery stenosis in patients with coronary artery disease. Cardiovasc Revasc Med. 2009;10(1):23-9. [CrossRef]
- Omeish AF, Abbadi HH, Ghanma IM, Botoosh FA, Shwabkeh MK. Frequency of renal artery stenosis among cohort of Jordanians undergoing drive-by renal angiography at time of conventional cardiac catheterization. Saudi Med J. 2009;30(11):1459-64.
- Park S, Jung J-H, Seo H-S, et al. The prevalence and clinical predictors of atherosclerotic renal artery stenosis in patients undergoing coronary angiography. Heart Vessels. 2004;19(6):275-9. [CrossRef]
- Payami B, Jafarizade M, Beladi Mousavi SS, Sattari S-A, Nokhostin F. Prevalence and predictors of atherosclerotic renal artery stenosis in hypertensive patients undergoing simultaneous coronary and renal artery angiography; a cross-sectional study. J Renal Inj Prev. 2016;5(1):34-8. [CrossRef]
- Przewłocki T, Kabłak-Ziembicka A, Tracz W, et al. Renal artery stenosis in patients with coronary artery disease. Kardiol Pol. 2008;66(8):856-62; discussion 63-4. [CrossRef]
- Rihal CS, Textor SC, Breen JF, et al. Incidental renal artery stenosis among a prospective cohort of hypertensive patients undergoing coronary angiography. Mayo Clin Proc. 2002;77(4):309-16. [CrossRef]
- Rimoldi SF, de Marchi SF, Windecker S, Meier B, Allemann Y. Screening renal artery angiography in hypertensive patients undergoing coronary angiography and 6-month follow-up after ad hoc percutaneous revascularization. J Hypertens. 2010;28(4):842-7. [CrossRef]
- Rokni N, Salarifar M, Hakki Kazazi E, Goodarzynejad H. Frequency and predictors of renal artery stenosis in patients undergoing simultaneous coronary and renal catheterization. J Tehran Heart Cent. 2012;7(2):58-64.
- Salehi N, Firouzi A, Gholoobi A, et al. relationship between distribution of coronary artery lesions and renal artery stenosis in patients undergoing simultaneous coronary and renal angiography. Clin Med Insights Cardiol. 2011;5:35-40. [CrossRef]
- Sani SH, Hasanzadeh M Fau - Gholoobi A, Gholoobi A Fau - Alimi H, Alimi H Fau - allah Esmaily H, allah Esmaily H Fau - Gifani M, Gifani M. Relationship between coronary and renal artery disease and associated risk factors in hypertensive and diabetic patients undergoing coronary angiography. (1774-024X (Print)).
- Shukla AN, Madan TH, Jayaram AA, et al. Prevalence and predictors of renal artery stenosis in patients undergoing peripheral and coronary angiography. Int Urol Nephrol. 2013;45(6):1629-35. [CrossRef]
- Tumelero RT, Duda NT, Tognon AP, Thiesen M. Prevalence of renal artery stenosis in 1,656 patients who have undergone cardiac catheterization. Arq Bras Cardiol. 2006;87(3):248-53. [CrossRef]
- Vahedparast H, Pourbehi MR, Amini A, et al. Renal artery stenosis and its predictors in hypertensive patients undergoing coronary artery angiography. Iran J Radiol. 2011;8(4):235-40. [CrossRef]
- Wang Y, Ho DSW, Chen WH, et al. Prevalence and predictors of renal artery stenosis in Chinese patients with coronary artery disease. Intern Med J. 2003;33(7):280-5. [CrossRef]
- Weber-Mzell D. Coronary anatomy predicts presence or absence of renal artery stenosis. A prospective study in patients undergoing cardiac catheterization for suspected coronary artery disease. European Heart Journal. 2002;23(21):1684-91.
- Yamashita T, Ito F, Iwakiri N, Mitsuyama H, Fujii S, Kitabatake A. Prevalence and predictors of renal artery stenosis in patients undergoing cardiac catheterization. Hypertens Res. 2002;25(4):553-7. [CrossRef]
- Yorgun H, Kabakci G, Canpolat U, et al. Frequency and predictors of renal artery stenosis in hypertensive patients undergoing coronary angiography. Angiology. 2013;64(5):385-90. [CrossRef]
- Zandparsa A, Habashizadeh M, Moradi Farsani E, Jabbari M, Rezaei R. Relationship between Renal Artery Stenosis and Severity of Coronary Artery Disease in Patients with Coronary Atherosclerotic Disease. Int Cardiovasc Res J. 2012;6(3):84-7.
- Sani SHD, Hasanzadeh M, Gholoobi A, Alimi H, allah Esmaily H, Gifani M. Relationship between coronary and renal artery disease and associated risk factors in hypertensive and diabetic patients undergoing coronary angiography. EuroIntervention : journal of EuroPCR in collaboration with the Working Group on Interventional Cardiology of the European Society of Cardiology. 2008;4(3):373-7. [CrossRef]
- Andersen UB, Borglykke A, Jørgensen T. Prevalence of renal artery stenosis in subjects with moderate hypertension. A population-based study. Blood Press. 2011;20(3):140-4. [CrossRef]
- Ozkan U, Oguzkurt L, Tercan F, Nursal TZ. The prevalence and clinical predictors of incidental atherosclerotic renal artery stenosis. Eur J Radiol. 2009;69(3):550-4. [CrossRef]
- Kuroda S, Nishida N, Uzu T, et al. Prevalence of renal artery stenosis in autopsy patients with stroke. Stroke. 2000;31(1):61-5. [CrossRef]
- Gensini GG. A more meaningful scoring system for determining the severity of coronary heart disease. Am J Cardiol. 1983;51(3):606. [CrossRef]
- Dong H, Mo Y, Liu Y, Luo J, Zhou Y, Huang W. [Impact of simultaneous renal artery and coronary artery stenting on cardiac and renal function in patients with renal artery stenosis and coronary artery disease]. Zhonghua Xin Xue Guan Bing Za Zhi. 2014;42(1):19-24.
- Rzeznik D, Przewlocki T, Kablak-Ziembicka A, et al. Effect of renal artery revascularization on left ventricular hypertrophy, diastolic function, blood pressure, and the one-year outcome. J Vasc Surg. 2011;53(3):692-7. [CrossRef]
- Kawarada O, Kume T, Zen K, et al. Cardiac function response to stenting in atherosclerotic renal artery disease with and without heart failure: results from the Carmel study. ESC Heart Failure. 2019;6(2):319-27. [CrossRef]
Figure 1.
PRISMA flowchart depicting selection and inclusion process of potential studies.
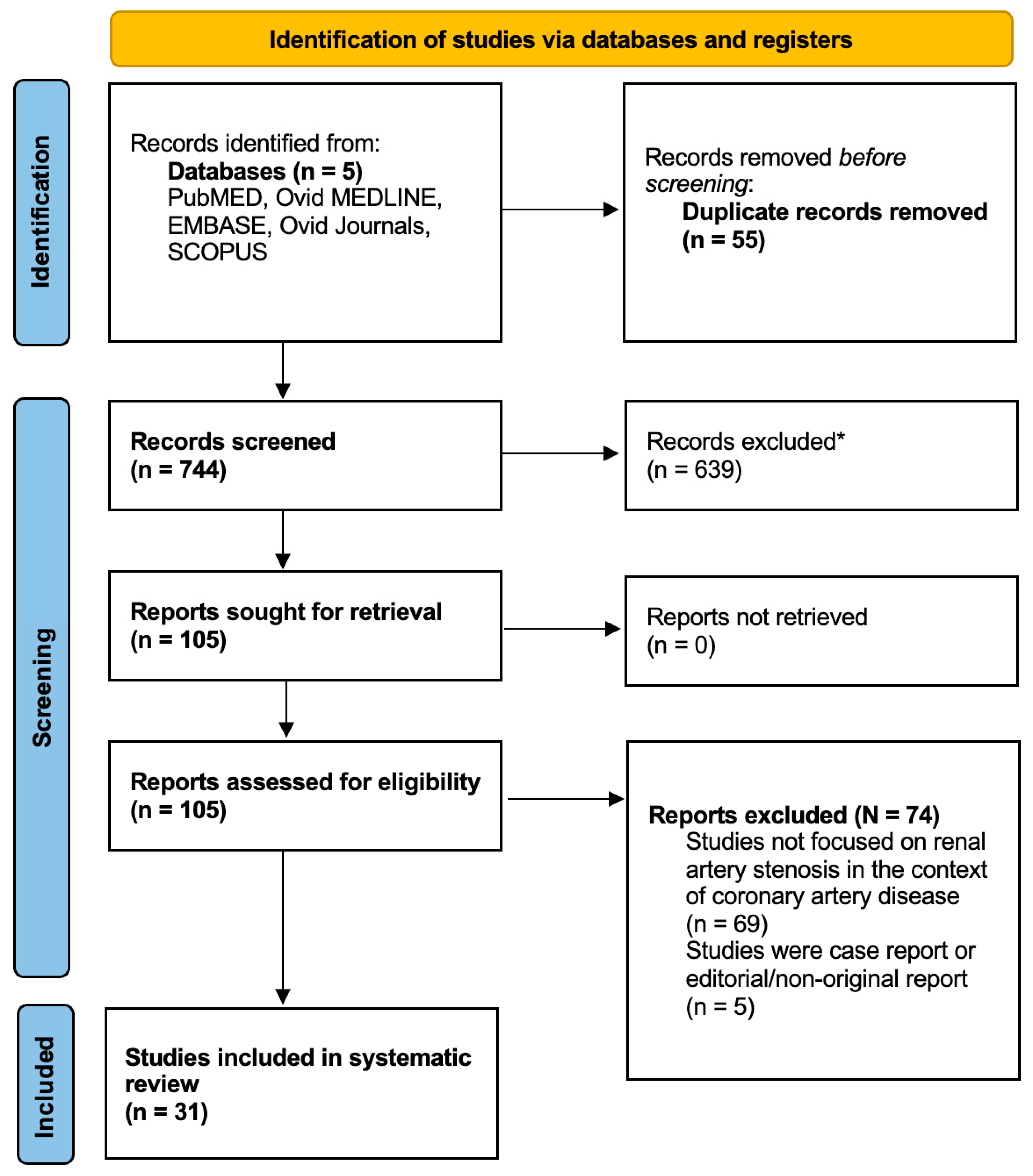
Figure 2.
The pooled weighted-proportions of significant, severe, and bilateral renal artery stenosis (RAS). Panel A) proportion of significant RAS; Panel B) proportion of severe RAS; Panel C) proportion of bilateral RAS in patients undergoing simultaneous coronary artery and renal artery angiography. Abbreviations: RAS - renal artery stenosis.
Figure 2.
The pooled weighted-proportions of significant, severe, and bilateral renal artery stenosis (RAS). Panel A) proportion of significant RAS; Panel B) proportion of severe RAS; Panel C) proportion of bilateral RAS in patients undergoing simultaneous coronary artery and renal artery angiography. Abbreviations: RAS - renal artery stenosis.
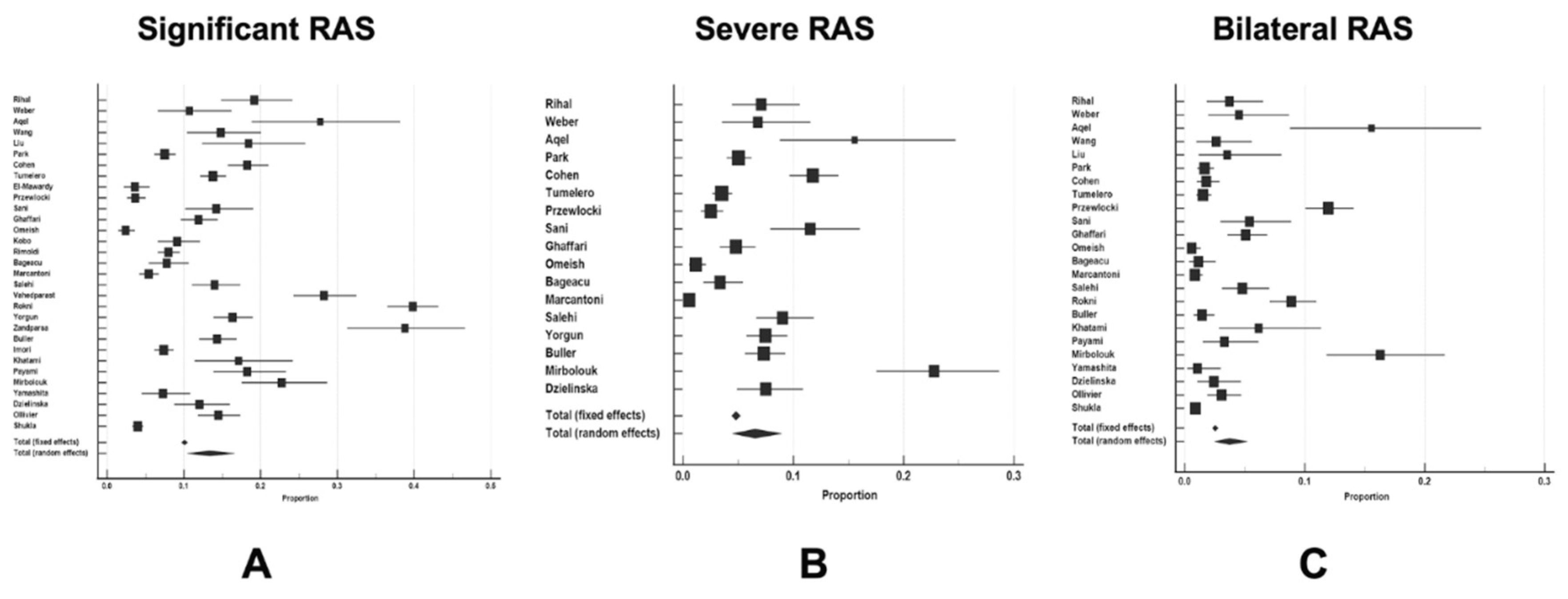
Figure 3.
The pooled weighted-proportions of three vessel disease Panel A, based on available data from 14,771 patients and left main disease - Panel B, based on available data from 10,670 patients with CAD undergoing cardiac catheterization.
Figure 3.
The pooled weighted-proportions of three vessel disease Panel A, based on available data from 14,771 patients and left main disease - Panel B, based on available data from 10,670 patients with CAD undergoing cardiac catheterization.
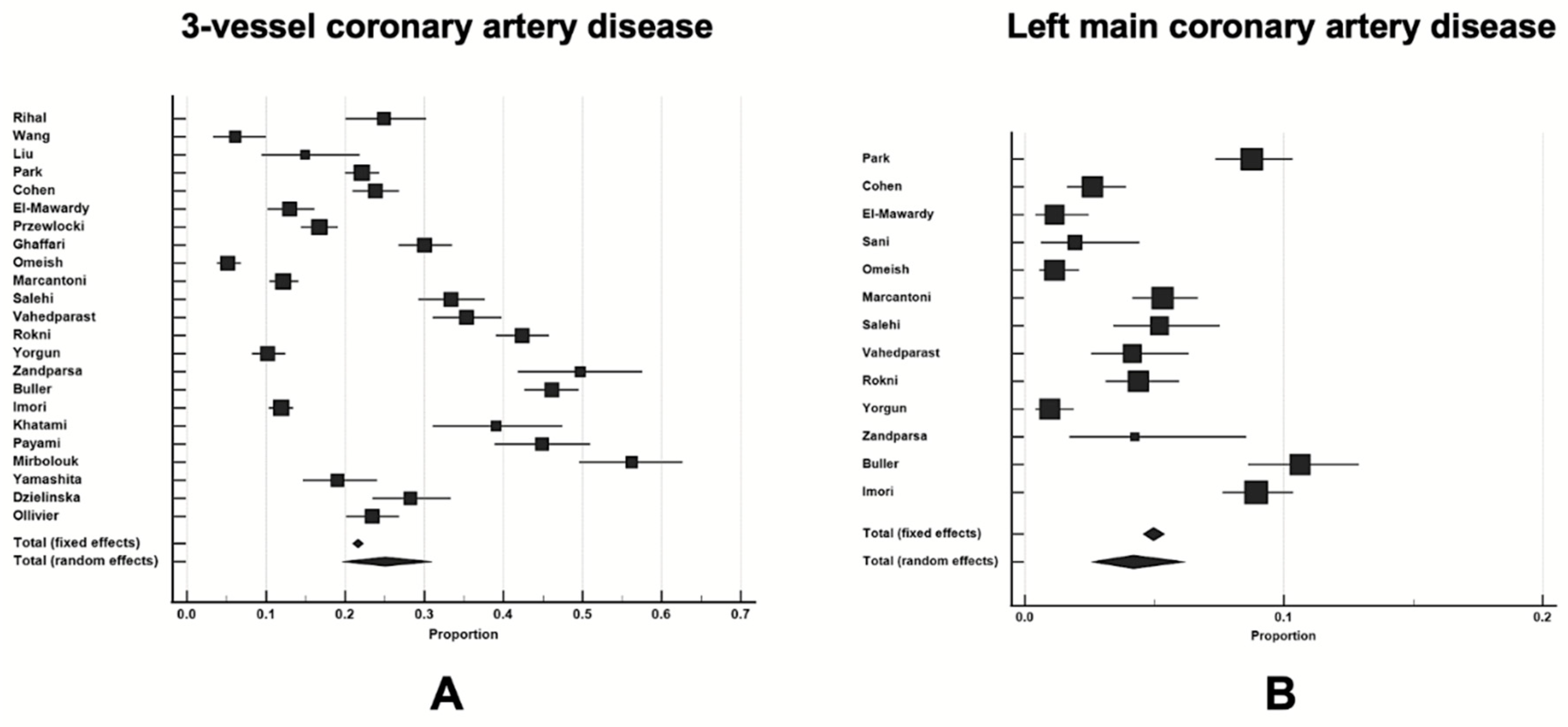
Figure 4.
Graphical Abstract – A summarizing figure depicting renal artery stenosis prevalence in patients undergoing elective coronary angiography and its associated risk factors (created by using Servier Medical Art ©). Abbreviations: RAS-renal artery stenosis.
Figure 4.
Graphical Abstract – A summarizing figure depicting renal artery stenosis prevalence in patients undergoing elective coronary angiography and its associated risk factors (created by using Servier Medical Art ©). Abbreviations: RAS-renal artery stenosis.
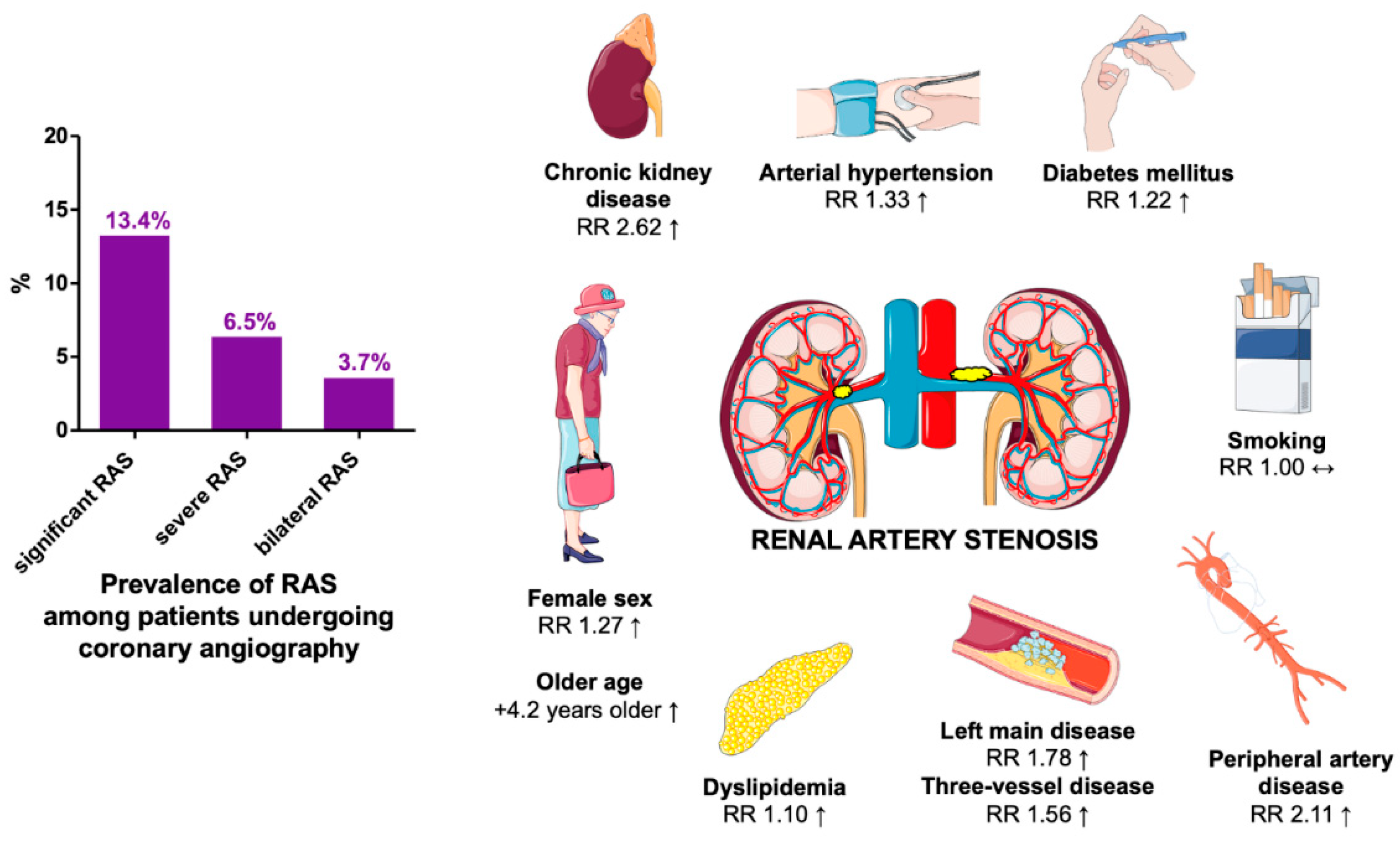

Table 1.
The overview of design and setting of studies included in the analysis.
| Authors of the study and year | Total number of patients | Study period | Study location | Multicentric or single-centre study | Study type |
|---|---|---|---|---|---|
| Rihal et al. 2002 | N=300 | July 1998 to March 1999 | Mayo Clinic, Rochester, USA | Single-center | Prospective cohort analysis |
| Weber et al. 2002 | N=177 | - | University Graz, Austria | Single-center | Cohort study |
| Yamashita et al. 2002 | N=289 | April 2000 to October 2000 | Kitami Red Cross Hospital, Japan | Single-center | Cohort study |
| Aqel et al. 2003 | N=542 | February 2001 to November 2001 | Veterans’ Administration (VA) Medical Center, USA | Single-center | Prospective study |
| Wang et al. 2003 | N=230 | - | Queen Mary Hospital, Hong Kong | Single-center | Prospective study |
| Liu et al. 2004 | N=141 | January 2000 to March 2004 | Zhong Da Hospital, Nanjing, PR China | Single-center | Cohort study |
| Park et al. 2004 | N=1459 | March 1998 to July 1999 | Yonsei University Cardiovascular Center, Seoul, South Korea | Single-center | Retrospective cohort study |
| Cohen et al. 2005 | N=843 | September 2000 to May 2002 | Hospital Italiano de Buenos Aires, Argentina | Single-center | Prospective study |
| Dzielinska et al. 2006 | N=333 | - | Institute of Cardiology in Warsaw, Poland | Single-centre | Prospective cohort study |
| Tumelero et al. 2006 | N=1656 | January 2002 to February 2004 | Hospital Sao Vicente de Paulo, Passo Fondo, Brazil | Single-center | Prospective cross-sectional study |
| Ollivier et al. 2008 | N=650 | May 2004 to May 2006 | CHU de Rennes, France | Single-centre | Prospective cohort study |
| El-Mawardy et al. 2008 | N=525 | November 2000 to June 2002 | Ain Shams University Hospital, Cairo, Egypt | Single-center | Cohort study |
| Przewlocki et al. 2008 | N=1036 | Period of 12 months | University Hospital, Krakow, Poland | Single-center | Cohort study |
| Sani et al. 2008 | N=260 | April 2005 to 2006 | Two educational hospitals in Mashhad (Emam Reza & Qaem), Iran | Multicentric | Cross-sectional study |
| Ghaffari et al. 2009 | N=732 | April 2007 to May 2008 | 3 hospitals in Tabriz, Iran | Multicenter | Cross-sectional study |
| Omeish et al. 2009 | N=870 | Januar 2006 to April 2006 | Queen Alia Heart Institute, Amman, Jordan | Single-center | Prospective cross-sectional study |
| Kobo et al. 2010 | N=7500 | 2001 to 2007 | Bnai-Zion Medical Center, Haifa, Israel | Single-center | Cohort study |
| Rimoldi et al. 2010 | N=1504 | 1st of January 2004 to 31st of August 2007 | Swiss Cardiovascular Center Bern, University Hospital Bern, Bern, Switzerland | Single-center | Retrospective study |
| Bageacu et al. 2011 | N=492 | 4 months period | University Hospital of Saint-Erienne, France | Single-center | Prospective study |
| Marcantoni et al. 2011 | N=1298 | April 2007 to March 2008 | The Division of Cardiology, University of Catania, Italy | Single-center | Prospective study |
| Salehi et al. 2011 | N=500 | Period of 12 months from November 2008 | Shaheed Rajeie Cardiovascular Medical, and Research Center, Iran | Single-center | Prospective cohort study |
| Vahedparast et al. 2011 | N=835 | August 2008 to August 2009 | Bent Al-Hoda Hospital od Bushehr University of Medical Science, Iran | Single-center | Prospective cross-sectional study |
| Rokni et al. 2012 | N=18419 | October 2009 to July 2011 | Tehran Heart Center, Iran | Single-center | Retrospective cross-sectional study |
| Yorgun et al. 2012 | N=832 | - | Hacettepe University, Ankara, Turkey | Single-center | Observational study |
| Zandparsa et al. 2012 | N=165 | September 2010 to May 2011 | Tehran University of Medical Sciences, Tehran, Iran | Single-center | Cohort study |
| Shukla et al. 2013 | N=3500 | January 2012 to June 2012 | Civil Hospital, Ahmedabad, India | Single-centre | Prospective cohort sudy |
| Buller et al. 2014 | N=851 | June 2001 to May 2002 | Vancouver Hospital, Canada | Single-center | Prospective cohort study |
| Imori et al. 2014 | N=2571 | September 2010 to July 2011 | Shonan Kamakura General Hospital, Kanagawa, Japan | Single-center | Cross-sectional analysis |
| Khatami et al. 2014 | N=173 | - | Tehran Unviversity of Medical Sciences, Tehran, Iran | Single-center | Cross-sectional study |
| Payami et al. 2016 | N=312 | March 2009 to October 2010 | Emam Hospital, Ahvaz, Iran | Single-center | Cross-sectional study |
| Mirbolouk et al. 2019 | N=247 | May 2015 to June 2016 | Heshmat Heart Hospital, Rasht, Iran | Single-center | Cross-sectional study |
Table 2.
Pooled weighted proportions (%) and mean of baseline patient characteristics from included studies.
Table 2.
Pooled weighted proportions (%) and mean of baseline patient characteristics from included studies.
| Variable | Mean ± SD or % (95% CI) |
|---|---|
| Age, mean (years) | 63.2 ± 8.7 |
| Female sex, % | 36.4 (32.4-40.5) |
| Diabetes mellitus, % | 28.7 (25.0-32.5) |
| Arterial hypertension, % | 80.3 (70.3-88.6) |
| Dyslipidemia, % | 61.6 (53.5-69.3) |
| Smoking, % | 38.4 (31.7-45.2) |
| Renal failure, % | 10.9 (7.0-15.6) |
| Peripheral vascular disease, % | 14.9 (6.9-25.2) |
| Carotid artery disease, % | 23.4 (2.9-55.4) |
| Previous myocardial infarction, % | 22.9 (18.7-27.4) |
Abbreviations: CI-confidence interval; SD-standard deviation.
Table 3.
Clinical factors associated with the risk of RAS occurence during coronary angiography in CAD patients.
Table 3.
Clinical factors associated with the risk of RAS occurence during coronary angiography in CAD patients.
| Variable | Risk ratio (RR) | 95% confidence interval | P-value | Heterogeneity* |
|---|---|---|---|---|
|
Female sex N=27 studies |
1.27 | 1.03 - 1.57 | 0.030 | High I2=92% |
|
Diabetes mellitus N=28 studies |
1.22 | 1.10 - 1.36 | <0.001 | Moderate I2=57% |
|
Arterial hypertension N=19 studies |
1.33 | 1.21 - 1.46 | <0.001 | High I2=94% |
|
Dyslipidemia N=24 studies |
1.10 | 1.06 - 1.14 | <0.001 | Moderate I2=59% |
|
Current smoking N=24 studies |
1.00 | 0.94 - 1.06 | 0.930 | Low I2=26% |
|
Chronic kidney disease N=13 studies |
2.62 | 2.04 - 3.37 | <0.001 | Moderate I2=66% |
|
Three-vessel disease N=17 studies |
1.56 | 1.30 - 1.87 | <0.001 | High I2=81% |
|
Left main disease N=10 studies |
1.78 | 1.28 - 2.47 | <0.001 | Moderate I2=52% |
|
Peripheral artery disease N=13 studies |
2.11 | 1.40 - 3.16 | <0.001 | High I2=94% |
*Heterogeneity of each meta-analysis was determined by Chi-square (χ2) test of heterogeneity and Higgins I2 statistic and following criteria were applied: studies with an I2 statistic of 15% to <35% were considered to have low heterogeneity; >35% to 75% - moderate heterogeneity, and those with I2 statistic >75% were considered to exhibit a high heterogeneity.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



