
Submitted:
16 August 2024
Posted:
16 August 2024
You are already at the latest version
Abstract
Background: Obesity remains a widely debated issue, often criticized for the limitations in its identification and classification. This study aims to compare two distinct systems for classifying obesity: Body Mass Index (BMI) and body fat percentage (BFP) as assessed by bioelectrical impedance analysis (BIA). By examining these measures, the study seeks to clarify how different metrics of body composition influence the identification of obesity-related risk factors. Methods: The study enrolled 1255 adults, comprising 471 males and 784 females, with a mean age of 36 ± 11.90 years. Participants exhibited varying degrees of weight status, including optimal weight, overweight, and obesity. Body composition analysis was conducted using the TANITA Body Composition Analyzer BC-418 MA III device (T5896, Tokyo, Japan), evaluating the following parameters: current weight, basal metabolic rate (BMR), adipose tissue (%), muscle mass (%), and hydration status (%). Results: Age and psychological factors like cravings, fatigue, stress, and compulsive eating were significant predictors of obesity in the BMI model but not in the BFP model. Additionally, having a family history of diabetes was protective in the BMI model (OR: 0.33) but increased risk in the BFP model (OR: 1.66). The BMI model demonstrates exceptional predictive ability (AUC=0.998). In contrast, the BFP model, while still performing well, exhibits a lower AUC (0.975), indicating slightly reduced discriminative power compared to the BMI model. Conclusions:BMI classification demonstrates superior predictive accuracy, specificity, and sensitivity. This suggests that BMI remains a more reliable measure for identifying obesity-related risk factors compared to the BFP model.
Keywords:
obesity
; overweight
; bioimpedance
; adipose tissue
; dietary habits
; body mass index
1. Introduction
Currently, the increasing prevalence of chronic metabolic disorders, with overweight, obesity and diabetes as primary factors, has become a significant public health concern in both developed and developing countries [1,2,3]. Obesity, recognized for its complexity and myriad associated complications, is regarded as a major public health issue. Various factors contribute to the early onset of these pathologies, including genetic predispositions, environmental variables such as pollution, and sedentary lifestyles. However, the most prevalent cause is the imbalance between excessive caloric intake and insufficient physical activity [4,5]. According to The Lancet, more than 1 billion people globally are expected to face obesity by the year 2022 [6]. Additionally, there has been a doubling in the number of overweight cases worldwide since 1990 and a fourfold increase in the number of children aged 5 to 19 affected by this condition [6]. In 2019, European countries reported that between 40-65% of their populations were diagnosed with overweight [7].
In addition to the global statistics, it has been observed that ethnic and racial minority groups present an additional risk of overweight and type 2 diabetes, thereby contributing to an increased risk of cardiovascular diseases [8,9,10]. The diagnosis of obesity is more frequent among women, with the highest increases reported among black populations [11]. Although all populations show an increase in the prevalence of obesity, the development of type 2 diabetes as a complication of obesity at a lower BMI (body mass index) value has been observed in Non-Hispanic Blacks (NHB) compared to Non-Hispanic Whites (NHW) [10,11,12,13]. This disparity is mainly attributed to significant differences in diet quality and eating habits [14,15,16].
Lately, there have been significant advances in understanding the pathophysiological mechanisms underlying the development of excess weight. Despite these substantial research efforts, these findings have yet to be widely applied in clinical practice, where obesity continues to be diagnosed and treated in a general manner [17]. The factors leading to obesity are multiple and interconnected, encompassing both genetic and environmental influences, with many being modifiable: food consumption, physical activity, social and individual psychology [18,19,20]. Moreover, it has been observed that urbanization, wide access to high-calorie and refined foods, and a sedentary lifestyle are the main contributors to excess weight [1,20]. From a nutritional standpoint, excess weight has been correlated with various eating patterns, such as meal frequency, meal volume or quantity, types of snacks, the removal of breakfast as the main meal, and overall diet quality [21,22]. Among these factors, the most recognized and significant contributor to the current obesity epidemic is quantity of food intake, which disrupts the energy balance [23]. A diversity of foods and nutrients have been identified and associated with both the risk of obesity and the management of this pathology [24,25,26,27].
The daily and conscious eating habits of an individual, influenced by cultural and social factors, include the amount, type, and frequency of food consumed and are collectively defined as “eating patterns” [28,29,30,31]. Given that unhealthy food choices and, consequently, poor diet quality predominantly contribute to excess weight, identifying and analyzing food patterns is currently the most effective method for evaluating the influence of general eating routines among people with obesity [20]. Additionally, this approach allows for the association of dietary patterns with nutritional status variables, such as anthropometric measurements and cardiometabolic markers [32,33]. Increased portion sizes and the frequency of hypercaloric foods are primary precursors of energy imbalance, and thus, obesity [29]. Accurately quantifying food patterns can be challenging due to differences in perception, including gender differences [34]. Moreover, assessing a person’s dietary pattern provides greater insights compared to evaluating daily individual macronutrient intake [35].
Although the report justifying the value of the most widely used anthropometric indicator, BMI, was proposed approximately 200 years ago, it was only 50 years ago that a concrete definition was implemented for this concept [36,37,38]. This delay resulted from prolonged debates in the field of research to confirm that BMI is a useful and accurate tool for diagnosing overweight and obesity [36,39]. Therefore, to evaluate the nutritional status of an adult, BMI is the most commonly used parameter, as it defines the excess of adipose tissue with generalized distribution [40]. Despite its widespread use, uncertainties persist regarding the relationship between BMI and mortality risk [39]. Nonetheless, studies have identified associations between BMI and both general and cardiovascular mortality risks, with stronger correlations observed among young adults and more significant associations in men compared to women [42,43]. A significant limitation of BMI is its inability to provide detailed information about the distribution and percentage of adipose tissue in the body [43,44,45]. Moreover, this parameter can provide misleading information in various situations, such as during different stages of life like childhood and adolescence, for performance athletes, or during the dynamic monitoring of a weight loss process [46]. Additionally, the percentage of adipose tissue varies by sex and age, regardless of BMI [44]. However, a universal definition of adult obesity based strictly on the percentage of adipose tissue has not been established [47,48]. The fat mass index (FMI) is a more precise indicator for evaluating body fat, but its interpretation is also limited [47,48,49,50]. Specific thresholds for FMI values have not been identified, unlike the percentage of adipose tissue used for diagnosing obesity [51,52]. Conversely, the percentage of adipose tissue determined by electrical bioimpedance techniques can fall within optimal limits based on age, sex, and ethnicity, as indicated by the device-specific reference charts for both adults and children [53,54,55].
Obesity is known to negatively impact quality of life and life expectancy. However, the risk of developing complications varies significantly among individuals, a variation that cannot be fully explained by BMI or the degree of adipose tissue alone [56]. Metabolically healthy obesity (MHO) is a well-recognized condition, with a prevalence between 10-30%, and is influenced by factors such as gender and age [56,57]. While there is no standard definition of MHO, it is characterized by a lower cardiometabolic risk compared to metabolically unhealthy obesity (MHU) [58,59,60]. Despite the significant role of adipose tissue distribution in defining obesity subtypes, MHO remains a transient phenotype. Therefore, nutritional intervention aimed at weight loss is crucial for MHO individuals, as the presence of excess adipose tissue is more critical than its distribution when compared to normal-weight individuals [56].
Adipose tissue, due to its complexity and various functions—such as mechanical protection, lipid storage, thermogenesis, and regulation of systemic energy and nutrient homeostasis—is considered a metabolically active endocrine tissue with a remarkable ability to change size in response to different factors [44,61,62,63]. This dynamic nature of adipose tissue underscores the importance of comprehensive methods for evaluating body composition and health risks beyond BMI alone. This component belongs to the endocrine system, being essential in regulating homeostasis [64,65]. Consequently, its distribution, especially at the abdominal level, is a critical factor for the development of metabolic syndrome, type 2 diabetes and, implicitly, for the increase in cardiovascular risk [66].
With the advent of advanced technology, it is now possible to accurately determine not only the total amount but also the distribution of adipose tissue, both in percentage and in kilograms. Various devices have been developed and validated to assess the percentage of adipose tissue, including plethysmography, dual-energy X-ray absorptiometry (DXA), computed tomography (CT), and magnetic resonance imaging (MRI) [67,68]. However, the most commonly used technique in recent years is BIA [69]. Compared to other methods of quantifying body composition, BIA offers several advantages: it is easy to use, relatively low-cost, non-invasive and can be applied to most individuals regardless of age [70]. These advantages make BIA a practical and accessible tool for widespread use in clinical and research settings.
Therefore, the aim of this study is to identify and analyze the impact of a wide range of eating habits and various medical conditions on body weight, as well as the potential risk factors contributing to overweight. This will be achieved using two different classifications of nutritional status: the BMI value and the percentage of adipose tissue, assessed through electrical bioimpedance. These models were constructed to identify and quantify the impact of various predictors on the probability of obesity. By contrasting the outcomes derived from the BMI-based and BFP-based models, this study seeks to highlight the similarities and differences in obesity risk factors as determined by these two classification systems. This comparative analysis offers a more detailed understanding of how different measures of body composition may influence the identification of obesity-related risk factors.
2. Materials and Methods
The prospective observational study was conducted over approximately four years, from July 2020 to June 2024, in our endocrinology unit. The total cohort comprised 1255 adults, 471 males (34%) and 927 females (66%), with a mean age of 36 ± 11.90, who were willing to assess their eating habits and undergo a comprehensive evaluation of their nutritional status with the aim of lifestyle modification. All participants provided informed consent. The study adhered to the ethical standards of the Helsinki Declaration and was approved by the Scientific Research Ethics Committee (CECS) of the “Victor Babeș” University of Medicine and Pharmacy Timișoara (No. 69/03.10.2022). To allow a complex comparative analysis of the final set of evaluated data, the entire group was divided as follows:
Based on the nutritional status evaluation, the cohort was divided into three subgroups according to BMI values [71,72]:
- The control group (normal weight, BMI 18-24.9 kg/m²), which consisted of individuals with no family or personal medical history of metabolic and cardiovascular diseases.
- The overweight group: BMI 25-29.9 kg/m²
- The obese group: BMI ≥ 30 kg/m².
Based on age and sex, independent of BMI value, according to the severity of excess adipose tissue [53,54], as follows:
- 1.
- Control Group:
- ▪
-
Normal weight women with distribution of adipose tissue according to age:
- 20-39 years (21-32.9% adipose tissue)
- 40-59 years (23-33.9% adipose tissue)
- 60-79 years (24-35.9% adipose tissue)
- ▪
-
Normal weight men with distribution of adipose tissue according to age:
- 20-39 years (8-20% adipose tissue)
- 40-59 years (11-22% adipose tissue)
- 60-79 years (13-25% adipose tissue)
- 2.
- Overweight Group:
- ▪
-
Overweight women with distribution of adipose tissue according to age:
- 20-39 years (33-38.9% adipose tissue)
- 40-59 years (34-39.9% adipose tissue)
- 60-79 years (36-42% adipose tissue)
- ▪
-
Overweight men with distribution of adipose tissue according to age:
- 20-39 years (adipose tissue)
- 40-59 years (adipose tissue)
- 60-79 years (adipose tissue)
- 3.
- Obesity Group (excess adipose tissue):
- ▪
-
Women with excess distribution of adipose tissue according to age:
- 20-39 years (adipose tissue)
- 40-59 years (adipose tissue)
- 60-79 years (adipose tissue)
- ▪
-
Men with excess distribution of adipose tissue according to age:
- 20-39 years (adipose tissue)
- 40-59 years (adipose tissue)
- 60-79 years (adipose tissue)
2.1. Patient Inclusion and Exclusion Criteria
Inclusion Criteria: Participants were required to be adults, both men and women, with overweight or obesity, who have maintained the same residence for at least five years. They must have accurately completed a comprehensive questionnaire regarding eating habits, lifestyle habits, and personal and family history of cardiometabolic diseases. Additionally, a control group of normal-weight individuals without personal or family medical history of metabolic or cardiovascular conditions was included. Only those who consented to a thorough anamnestic and clinical evaluation by signing the informed consent form were included in the final assessment.
Exclusion Criteria: Patients with secondary obesity, regardless of its etiology (e.g., endocrinological conditions such as hypothyroidism or Cushing’s syndrome; genetic disorders like Prader-Willi syndrome; or iatrogenic causes such as glucocorticoid or insulin therapy within tha past 12 weeks) were excluded from the study [73,74,75]. Additionally, subjects who had followed a hypocaloric diet or received anti-obesity treatments (e.g., liraglutide, semaglutide, Orlistat, Bupropion/Naltrexone) within the past 16 weeks were excluded [73]. Individuals with documented psychiatric conditions and children were also not included in the research.
2.2. Patient Complete Evaluation:
Each participant was thoroughly informed about the stages of the study, including anamnesis, clinical and paraclinical evaluation, and provided with informed consent documentation. A detailed anamnesis was conducted for each patient, which encompassed the food survey, personal medical history of documented cardiometabolic pathologies, and family history, with particular attention to the presence of these conditions among first-degree relatives. Body analysis by bioimpedance was employed as the primary non-invasive method to estimate segmental body composition. Consequently, the following parameters were included in the initial evaluation of the participants:
Body Weight Measurement: Body weight was assessed using a mechanical scale with metrological certification, capable of measuring up to 200 kg. Participants were instructed to stand in a vertical posture on the scale while wearing minimal clothing.
Height Measurement: Height was measured using a calibrated wall-mounted stadiometer. Participants were instructed to stand in a vertical posture on the platform without wearing shoes.
Nutritional Status: The nutritional status of each participant in our study was assessed using BMI, a widely utilized, cost-effective parameter. The BMI was calculated using the formula: BMI = weight (in kg) / height² (in m²) [71,72], as previously mentioned.
Family medical history and conditions: A detailed family medical history focusing on cardiometabolic pathologies was obtained from each participant. The pathologies of interest, particularly concerning first-degree relatives, included obesity, overweight, type 2 diabetes, stroke, essential hypertension, and acute myocardial infarction.
Personal medical history and conditions: Similar to those mentioned previously, a pre-announced evaluation through directed questioning of the personal medical history was conducted individually for each participant. The primary pathologies emphasized were within the cardiovascular and metabolic categories, including diagnosed essential hypertension or use of antihypertensive treatment, prediabetes, type 2 diabetes, metabolic syndrome, lipid profile alterations, and asymptomatic hyperuricemia. Additionally, for patients who were undergoing insulin treatment in the past (more than 6 months), potential weight gain following its initiation was assessed. Among women, other parameters of interest included in the anamnesis were weight gain postpartum, diagnosis of polycystic ovary syndrome (regardless of subtype), daily use of oral contraceptives, onset of menopause, preclimax, and increased appetite during the premenstrual period. Regardless of gender and medical history, other significant factors addressed were previous weight loss, food intolerances, and weight gain after smoking cessation.
Demographic and lifestyle factors: In this category, parameters associated with the daily routine were also included due to the complexity of the anamnesis:
- ◦
- Cigarette smoking status: this was defined as smoking at least one cigarette every day for more than a year.
- ◦
- Alcohol consumption: To quantify alcohol consumption, participants reported the number of units of alcohol consumed (equivalent to 10 ml of pure ethanol) via self-reporting. The units were defined as follows: two units equated to a pint or can of beer, one unit to a 25 ml shot of hard liquor, and one unit to a standard 175 ml glass of white or red wine. Participants consuming more than two units of alcohol daily were categorized as “alcoholic,” while those who had never consumed alcohol were classified as “non-alcoholic” [76].
- ◦
- Physical activity level: To be excluded from the sedentary category, it was necessary to confirm a sustained physical effort of at least 30 minutes per day or 150 minutes per week (activity level > active plus basal).
- ◦
- Sleep schedule: The duration of sleep for each subject was assessed, with a nightly duration of less than 7 hours being classified as sleep deprivation or an insufficient sleep schedule [77].
Eating habits and preferences: The dietary habits of participants were meticulously documented from multiple perspectives. Key criteria included: daily breakfast consumption, adherence to the three main meals of the day, and the inclusion of two main courses at lunch. Additionally, the focus was placed on portion sizes relative to individual energy requirements, snacking between meals, the need for additional servings due to reduced satiety, and daily intake of fruits and whole foods. Eating habits were further categorized by quality, such as the consumption of home-cooked meals, dining at restaurants, fast-food intake, and dessert consumption. The study also examined the quantity of non-caloric clear liquids consumed, specifically plain water, as well as coffee and dairy consumption.
Psychological and emotional factors: Finally, psychological and emotional factors were assessed through targeted questions during the anamnesis, similar to the previous sections. The focus was on the presence of overeating or excessive eating triggered by negative and positive emotions, including eating for pleasure, as a reward, and secondary to loneliness, psychological stress, fatigue, or boredom.
2.3. Bioimpedance Body Analyzed Variables
All subjects included in the study underwent an initial examination of their nutritional status using body bioimpedance analysis with the Tanita Body Composition Analyzer BC-418 MA III device (T5896, Tokyo, Japan). This analysis focused particularly on the percentage and distribution of adipose tissue. This involved a detailed analysis of the complete body composition utilizing a constant high-frequency current source (50 kHz, 500 μA) and employing a tetra-polar eight-point tactile electrode system. Participants were instructed to maintain an upright posture and grasp the analyzer’s handles to ensure contact with a total of eight electrodes, two for each foot and hand [78]. During the bioelectrical impedance analysis, a low-level electrical current passed through each participant’s body, and impedance (resistance to the current flow) was measured [79]. The entire procedure lasted approximately three minutes, and the results were thoroughly explained and recorded for each patient. Based on the results, the analyzed parameters were categorized into:
- Current weight or weight at the time of examination (kg)
- Metabolic basal rate (BMR) (kcal)
- Percentage of adipose tissue (%)
- Percentage of lean mass or muscle tissue (%)
- Percentage of total body water or hydration status (%)
The following personal information was collected and entered into the operating system of the instrument model used: identification data, gender, birth date and height (cm). Upon entering the personal data for each patient, the instrument’s operating system automatically generated the BMR values.
2.4. Statistical Analysis
Numerical variables, based on their distribution type, were presented as median and interquartile range, while categorical variables were presented as frequency and proportions. The normality of distributions was assessed using the Shapiro-Wilk test, with a p-value < 0.05 indicating a non-Gaussian distribution. The test indicated non-normality for all numerical variables; hence, non-parametric methods were employed. To investigate differences between numerical variables, the Mann-Whitney U test was used. For exploring statistically significant differences between categorical variables, the Pearson Chi-square test was employed. To identify risk factors for obesity, multivariate logistic regression was used. The Nagelkerke R² was used to assess model quality. The ROC curve parameters, including specificity, sensitivity, accuracy, and AUC, were utilized to compare the two models. The results were presented in both tabular and graphical formats. The statistical analysis was performed using R (R Core Team, 2024), a language and environment for statistical computing provided by the R Foundation for Statistical Computing, Vienna, Austria. A p-value < 0.05 was considered statistically significant, with a 95% confidence interval.
3. Results
The data collected from these patients is comprehensive, encompassing bioimpedance measurements, demographic and lifestyle factors, family medical history, eating habits and preferences, psychological and emotional factors, as well as specific conditions and health issues. The analysis began by classifying the patients into control, overweight, and obese categories using the Body Mass Index system. Subsequently, the classification was repeated using the Body Fat Percentage system. The results from these two classification methods were then compared to understand the differences and similarities in the determinants of weight status identified by each approach.
3.1. Numerical Variables
The analysis of the study population using both the BMI model and the adiposity-based model revealed significant differences in various health and lifestyle parameters between normal weight, overweight, and obese participants, as detailed in Table 1 and Table 2. In the BMI model, the highest average age was observed among the obese group (38 years), while the overweight group had the lowest average age (31 years) (p<0.001). Conversely, the adiposity model indicated a higher average age among both obese (37 years) and overweight (35 years) individuals compared to the control group (34 years) (p<0.001). In both models, the sleep duration was significantly longer in the control group compared to the study group, with statistically significant differences (p<0.001). Regarding water intake, the control group exhibited the highest daily consumption (2500 ml/day), whereas the overweight and obese groups had the lowest (1500 ml/day) (p<0.001). Consequently, hydration status, as evaluated by electrical bioimpedance, demonstrated statistical differences among the three groups (p<0.001). These findings suggest that, regardless of the classification method, individuals with optimal body weight demonstrated healthier body composition and more appropriate lifestyle habits, such as higher consumption of non-caloric clear liquids and longer sleep duration, compared to those who are overweight or obese.
3.2. Demographic and Lifestyle Factors
Using the BMI classification for nutritional status, the demographic and risk factor analysis reveals statistically significant differences between the evaluated groups. Therefore, in terms of gender distribution, the control group is evenly split with 50% males and 50% females, while the overweight group has a higher proportion of females as well as in the case of the obese group with a p-value of < 0.001. Supplementing meals as a result of an insufficient feeling of satiety varies significantly, with no supplement use in the control group, 21% in the overweight group, and 18% in the obese group (p < 0.001). Consumption of more food during holidays shows a slight but significant difference between the three evaluated groups. The consumption of meals while watching TV or using other devices proved to be drastically higher among overweight and obese people versus those of normal weight. Engagement in physical activity for at least 30 minutes per day was significantly higher in the control group, decreasing markedly with increasing overweight. Daily alcohol consumption increased with overweight status, irrespective of classification method, showing significant differences among the groups (p<0.001). Smoking was more frequent among individuals without obesity, confirming the relationship between lower weight, higher metabolic rate, and smoking status. All the comparative results between the two evaluated models can be found in Table 3 and Table 4.
3.3. Family Medical History
In Table 5 and Table 6, the results related to the family medical history of cardiometabolic pathology are detailed, with analysis performed both based on BMI classification and according to the proportion of body adipose tissue. A greater predisposition to obesity was observed among the first-degree relatives of participants in the control group when considering the second classification (24% versus 9%). However, the highest percentages in both classifications were associated with the overweight group (99% and 81%). Regarding the family medical history of type 2 diabetes, significant statistical differences were observed between the evaluated groups, both in terms of BMI and the percentage of adiposity. For cardiovascular pathologies, no cases of stroke were reported among the first-degree relatives in the control group from the BMI classification, with only a small percentage (4%) from the BFP classification. The prevalence of essential arterial hypertension in first-degree relatives increased directly in proportion to both BMI and the percentage of adipose tissue, showing significant statistical differences (p < 0.001). The history of acute myocardial infarction was similar in the overweight and obese groups, regardless of the classification used. These findings highlight significant variations in family medical history among individuals of different body fat percentage categories and BMI values, emphasizing the genetic and familial predisposition to various health conditions in overweight and obese populations.
3.4. Eating Habits and Preferences
Table 7 and Table 8 present the analysis of food preferences and habits based on both BMI values and the percentage of adipose tissue, revealing statistically significant differences among the control, overweight, and obese groups. The prevalence of craving eating increased with higher BMI and adipose tissue percentages, with only 1% and 7% of normal weight subjects reporting this behavior, respectively. Fast eating and large meal portions were less common in the control group (1% for both) when classified by BMI, compared to the BFP classification (13% and 15%, respectively), showing significant differences across all groups in both classifications (p<0.001). Daily fast food consumption was similar in the control groups (4% for BMI vs. 6% for BFP classification) but differed significantly in the overweight group (14% vs. 34%). No normal-weight participants in the BMI classification ate outside the table. Dessert consumption after main meals was significantly higher in the overweight and obese groups compared to the control group (p<0.001). Snacking was not reported by normal-weight individuals, whereas it was common among overweight participants (p<0.001). Eating out at restaurants and on weekends was significantly more frequent in the study group across both classifications, likely because normal-weight individuals reported higher consumption of home-cooked meals and adherence to three main meals per day (p<0.001). Breakfast was regularly consumed by only 3% of obese individuals based on BMI and 8% based on BFP classification, with statistically significant differences between groups (p<0.001). The trend continued for daily fruit and whole product consumption. These findings underscore significant variations in dietary preferences and habits, highlighting the importance of dietary behaviors on weight gain and quality of life, regardless of the classification method used for nutritional status.
3.5. Psychological and Emotional Factors
The analysis of the evaluated emotional and psychological factors reveals statistically significant differences between the groups for both the BMI and BFP models. Notably, no participants in the control group reported stress-related eating in the BMI classification, with only 5% in the BFP model. In contrast, a significantly higher proportion of subjects indicated stress as a stimulus for eating in the BMI model (94%) compared to the BFP model (86%). Similarly, fatigue-related eating behaviors were scarcely present in the control group (1% in the BMI model and 4% in the BFP model). These differences highlight the absence of emotional components in eating behaviors among normal-weight individuals, as opposed to those with obesity or overweight. The findings underscore significant variations in psychological and emotional factors influencing excessive eating behaviors in individuals with obesity, according to both BMI and BFP classifications. This suggests that comprehensive evaluations of overweight patients should include psychological counseling to address and treat the multifaceted nature of obesity. Detailed results are presented in Table 9 and Table 10.
3.6. Specific Conditions and Health Issues
With few exceptions, the statistical analysis of this category’s elements identifies significant differences between the evaluated groups, highlighting the risks to quality of life associated with both increased BMI and a higher percentage of adiposity. Notably, weight gain resulting from the initiation of insulin therapy and weight regain after metabolic surgery, both within the last six months, were not reported in any group. However, other pathologies associated with excess adiposity and elevated BMI were noted among the study participants and are described in detail in Table 11 and Table 12.
3.7. Risk Factors for Obesity
To assess the risk factors for obesity, logistic regression models were employed using both BMI and BFP as classification criteria. These models aimed to identify and quantify the impact of various predictors on the likelihood of obesity. By comparing the results from the BMI-based and BFP-based models, this study seeks to elucidate the similarities and differences in the risk factors for obesity identified by these two classification systems. This comparative approach facilitates a more nuanced understanding of how different measures of body composition may influence the identification of obesity-related risk factors.
The logistic regression model based on BMI highlighted several significant risk factors for obesity. Age, a non-modifiable risk factor, was positively associated with obesity, with each additional year increasing the odds by 8% (OR: 1.08, CI: 1.03 – 1.13, p = 0.004). Emotional and behavioral factors also correlated positively with obesity risk. Notable factors include eating with appetite (OR: 17.08, CI: 4.82 – 68.55, p < 0.001), fatigue (OR: 16.90, CI: 5.20 – 64.03, p < 0.001), and stress (OR: 42.07, CI: 12.70 – 172.12, p < 0.001). Additionally, snoring (OR: 4.37, CI: 1.19 – 17.04, p = 0.029), compulsive eating (OR: 32.93, CI: 10.16 – 128.04, p < 0.001), and fast-food consumption (OR: 10.20, CI: 3.54 – 31.95, p < 0.001) significantly increased obesity risk. Interestingly, some factors were associated with a lower risk of obesity, contrary to expectations. These include eating quickly or consuming large amounts of food (OR: 0.18, CI: 0.04 – 0.76, p = 0.025) and consuming large portions (OR: 0.06, CI: 0.01 – 0.40, p = 0.005), potentially indicating compensatory behaviors. Similarly, eating at restaurants (OR: 0.12, CI: 0.03 – 0.49, p = 0.003), feeling angry or upset (OR: 0.14, CI: 0.03 – 0.53, p = 0.006), experiencing premenstrual syndrome (PMS) (OR: 0.10, CI: 0.03 – 0.38, p = 0.001), and using other devices while eating (OR: 0.15, CI: 0.03 – 0.79, p = 0.024) were all linked to lower obesity risk. Conversely, the presence of snacks after meals and the addition of portions were significant risk factors for developing overweight conditions (OR: 26.98, CI: 8.29 – 106.49, p < 0.001). Table 13 and Figure 1 present all data derived from the logistic regression analysis based on the BMI model.
In the logistic regression model based on BFP, several significant risk factors for obesity were identified, as detailed in Table 14 and Figure 1. A family history of diabetes notably increases the likelihood of developing obesity (OR: 1.66, CI: 1.01 – 2.76, p = 0.046), compared to the previously model. Regarding eating habits, binge eating is a significant risk factor (OR: 1.78, CI: 1.06 – 3.03, p = 0.031). Interestingly, eating quickly or consuming large quantities appears to be protective (OR: 0.39, CI: 0.16 – 0.91, p = 0.032). Additionally, detrimental lifestyle habits, such as smoking (OR: 4.97, CI: 2.09 – 12.36, p < 0.001) and daily alcohol consumption (OR: 1.98, CI: 1.11 – 3.57, p = 0.022), are significant risk factors for excess adipose tissue. Moreover, eating while watching TV was identified as a strong risk factor (OR: 2.28, CI: 1.26 – 4.13, p = 0.006).
Several risk factors appear consistently in both the BMI and BFP models, underscoring their robust association with obesity. Hydration status is protective in both models (BMI: OR: 0.84, CI: 0.75 – 0.92, p < 0.001; BFP: OR: 0.86, CI: 0.77 – 0.95, p = 0.005). Family history of diabetes has contrasting effects, increasing the risk only in the BFP model. Rapid or large-quantity eating behaviors are protective in both models (BMI: OR: 0.18, CI: 0.04 – 0.76, p = 0.025; BFP: OR: 0.39, CI: 0.16 – 0.91, p = 0.032). Experiencing PMS is associated with a lower risk of obesity in both models (BMI: OR: 0.10, CI: 0.03 – 0.38, p = 0.001; BFP: OR: 0.38, CI: 0.17 – 0.83, p = 0.017). These common factors highlight the complex interplay between physiological, behavioral, and emotional determinants of obesity risk. Figure 1 illustrates the differences between the logistic regression models for the two evaluated classifications.
3.8. Comparison between BMI and BFP Models
The comparison of the BMI and BFP models reveals differences in their predictive performance for obesity. The BMI model demonstrates exceptional predictive ability with an AUC of 0.998 (95% CI: 0.996 - 0.999), indicating near-perfect discrimination between obese and non-obese individuals. It also shows high accuracy (0.983), specificity (0.985), and sensitivity (0.982), suggesting that it accurately identifies both true positives and true negatives. On the other hand, the BFP model, while still performing well, has a lower AUC of 0.975 (95% CI: 0.967 - 0.982), indicating slightly less discriminative power compared to the BMI model. The BFP model’s accuracy is 0.922, with a specificity of 0.937 and a sensitivity of 0.904. These metrics suggest that the BFP model, although effective, is less accurate in identifying obese individuals compared to the BMI model. Overall, while both models perform robustly, the BMI model shows superior performance in predicting obesity. The results are presented in Table 15 and Figure 2.
4. Discussion
The diversity of eating habits, lifestyle factors, psychological and emotional influences, and genetic components, all contribute significantly to an individual’s nutritional status, impacting the distribution of adipose and lean tissue masses. Obesity remains a contentious topic, often criticized for the limitations in its identification and classification. The importance of understanding these factors is critical for developing effective obesity management strategies. Although BMI has long been used as a standard measure to classify individuals based on their weight relative to height, it fails to account for the distribution and composition of body fat, which are crucial for understanding the health risks associated with obesity [80]. Contrary to expectations, the present study underscored the importance of BMI determination in clinical practice among overweight and obese individuals. While recognizing BMI’s limitations, our findings highlight its utility in providing a quick, accessible, and general indication of obesity, which can be essential for initial screenings and epidemiological studies. The implications of these findings are particularly relevant for nutrition clinicians, offering valuable insights for enhancing nutritional counseling and long-term monitoring of the nutritional status of overweight individuals. This approach can aid in developing personalized intervention strategies that address both dietary and lifestyle factors contributing to obesity. Furthermore, the study emphasizes the necessity of a comprehensive dietary assessment to identify the underlying factors leading to excess weight. This assessment should be part of a multidisciplinary team approach, allowing for the treatment of potential causes of obesity from various perspectives. Additionally, our research highlights the impact of different obesity classification models on the nutritional status of adults, regardless of their body weight, demonstrating that both BMI and adipose tissue measurements should be considered for a more accurate evaluation and management of obesity.
Furthermore, alongside modifiable risk factors for excess weight, such as dietary habits, several other parameters contribute to weight gain in individuals. Age is a prominent, yet immutable risk factor for overweight, primarily due to the progressive decline in basal metabolic rate with advancing age and the concomitant reduction in physical activity levels [81,82]. Additionally, aging is associated with a redistribution of adipose tissue, favoring visceral fat accumulation over subcutaneous fat [83]. In our study, statistically significant differences were observed between the study and control groups in both the BMI-based and BFP-based models (p<0.001). Notably, in the BFP-based model, an increase in age was directly proportional to the degree of adiposity, contrasting with the BMI-based model, where younger ages were predominantly in the overweight category. However, age emerged as a predictor for obesity onset exclusively in the BMI-based model.
Measurements were conducted under comparable levels of hydration to avoid misinterpretation, as BIA is particularly sensitive to total body water. This method was utilized to estimate total body water, fat mass percentage, muscle mass and total body water [84,85]. In the context of its application in sports and medicine, the raw BIA variable of phase angle, representing the ratio of resistance to reactance, has gained prominence and is provided by certain BIA devices [85]. Numerous studies have demonstrated the reliability of both single-frequency and multi-frequency BIA instruments, concluding that BIA can serve as a substitute for DXA in the analysis of whole-body and segmental body composition in large populations [86,87]. Recently, the association BMR and muscle tissue has been confirmed, both identified through body composition analysis [3,88]. Sarcopenia, the decline in muscle mass, frequently coexists with excess weight, especially among the elderly, representing an age-related abnormality [3,88,89]. The reduction in BMR is linked to excess weight, while variations in hydration status or total body water have been observed in both children and individuals with obesity [90,91,92]. Additionally, eating habits have been shown to negatively impact the percentage of adipose tissue, BMR, and hydration status [93,94]. In the current study, significant differences were observed in the parameters evaluated by BIA among the normal weight, overweight, and obese groups in both the BMI-based and BFP-based models. The highest percentage of adipose tissue was found in the obesity group, while the highest percentage of muscle tissue was attributed to the control group. BMR was comparable between the obese and normal weight groups but significantly lower in the overweight group. However, predictors for the development of obesity were identified only in the BFP-model. Specifically, an increased percentage of muscle tissue was found to be protective, reducing the chances of obesity by 32%. Additionally, a higher percentage of total body water also proved to be protective. BMR showed a small but significant increase in the odds ratio per unit (OR: 1.01, CI: 1.00-1.01, p<0.001).
Various factors, some more extensively researched than others contribute to the development of obesity. Physical activity, defined as “any type of body movement performed by skeletal muscles that results in energy expenditure”, plays a critical role [95]. Insufficient physical activity is linked to the onset of obesity, reduced cardiovascular fitness from childhood, and the development of various chronic cardiometabolic conditions in adulthood [96,97]. Consequently, a sedentary lifestyle is recognized as a significant contributor to obesity [96,98]. Additionally, regular physical activity has been associated with improvements in body composition and reductions in insulin resistance among adults [99,100]. Similar findings were observed in our study. In both evaluated models, the recommended physical activity of at least 30 minutes per day decreased proportionally with increases in BMI and adipose tissue percentage, being lowest in the group with obesity. The differences between the groups were significant (p<0.001). Furthermore, a decrease in physical activity duration to less than 30 minutes per day was identified as a predictive factor for obesity development only in the BFP-based model.
There are discernible differences in dietary patterns and eating behaviors concerning the quality and quantity of food by gender [101]. Gender-specific differences are also evident in the complications associated with obesity. A higher prevalence of obesity is typically observed among women, whereas men are more likely to develop metabolic complications secondary to excess weight [102,103]. Our study aligns with previous observations indicating that the prevalence of obesity is higher among women compared to men, with these gender differences being evident in most regions worldwide [104,105]. The type of adipose tissue expansion also varies by gender [104]. Although the overall obesity rate is 10% higher in women than in men, women tend to have a higher percentage of visceral fat [106,107,108]. In the current study, a significantly higher percentage of women was observed in the overweight (79%) and obesity (68%) groups within the BMI-based model. Similarly, in the adiposity-based model, 76% of the overweight group and 65% of the obese group were women. These findings indicate a higher prevalence of excess weight among females, with statistically significant differences (p<0.001). However, gender was not identified as a risk factor for the development of obesity in the logistic regression analysis.
An association has been observed between excess weight and functional as well as structural changes in the brain’s reward system [109,110]. The consumption of hypercaloric and palatable foods in excess can trigger reward phenomena [104]. Eating behaviors and preferences vary according to gender and age [104,111]. Cross-sectional studies have shown that women consume more fruits compared to men [111,112]. Additionally, women tend to prefer sweet and easily accessible snacks such as candies, whereas men are more likely to opt for fast food items like pizza [113]. It has also been observed that men tend to eat more quickly, while women may eat uncontrollably, even in the absence of hunger [114]. These differences highlight the need for gender-specific approaches in dietary interventions and obesity management. In the current study, various dietary behavioral factors were identified as predictors of weight gain and obesity, with both similarities and differences observed between obesity classification based on BMI and that based on the percentage of adipose tissue. This comparative approach provided a more comprehensive understanding of how different body composition measures can influence the assessment and identification of obesity risk factors. Specifically, daily consumption of fast food, snacking immediately after the main meal, nibbling, and experiencing cravings significantly increased the risk of obesity in the BMI-based model. Conversely, behaviors such as quickly eating, dining in social settings like restaurants, and consuming larger portions were identified as compensatory behaviors and were not associated with an increased risk of obesity in the same model. All these eating behaviors showed statistically significant differences between the evaluated groups (p<0.001). In contrast, the adiposity-based model identified different predictive factors for excess of adipose tissue. For instance, watching TV during meals increased the risk of obesity, while daily fruit consumption was a protective factor. Additionally, eating quickly, on the run, did not predict the development of obesity in either model.
Both diet and psycho-affective factors play crucial roles in maintaining quality of life and preventing chronic diseases. Emotional eating, a problematic eating pattern, often negatively impacts eating decisions and is associated with various degrees of obesity and the emotional factors underlying its etiology [115]. Adult women are most frequently affected by emotional eating [116,117], which is linked to both psychological state and nutritional status [118]. Emotional eating results from an accumulation of emotions and behaviors associated with eating, rather than being considered a separate eating disorder [118,119]. Amplification of negative emotions plays a significant role in the onset and progression of obesity, demonstrating a bidirectional correlation between these entities [120,121]. Through a detailed anamnesis, our study identified psycho-emotional predictive factors for the development of obesity. Significant differences were observed between the normal weight, overweight, and obesity groups in terms of stress, fatigue, compulsive eating, reward, and pleasure. Notably, most of these factors were risk factors for obesity only in the BMI-based model. Eating for pleasure was the only predictive factor within the adiposity-based model, while upset/anger eating was protective in the BMI model but a risk factor for obesity in the adiposity-based model. These findings highlight the complex interactions between different models of body composition and their influence on the risk of developing obesity from distinct perspectives.
The current research also focused on identifying and analyzing parameters specific to females. In the BMI-based model, significant differences were observed among the control, overweight, and obese groups concerning menopause (p<0.001). Conversely, in the BFP-based model, these differences were not significant (p=0.15). Thus, menopause was identified as a risk factor for increased BMI but not for excess adipose tissue. However, literature indicates that menopause is associated with changes in body composition, particularly an increase in the percentage of visceral adipose tissue, which amplifies cardiometabolic risk and deteriorates the quality of life among women [122]. This is primarily due to the absence of estrogen hormones during menopause, which significantly contributes to weight gain [123]. The reduction in circulating estrogens is also associated with a redistribution of adipose tissue, decreasing subcutaneous fat and increasing abdominal fat [124]. Additionally, it has been observed that the rate of developing obesity during menopause is three times higher compared to the pre-menopausal phase [125]. Therefore, in the present study, statistical differences were reported between the evaluated groups concerning pre-menopause diagnosis. Thus, pre-menopause was not noted as a risk factor for increased adiposity or BMI. Further research is necessary to clarify how hormonal fluctuations during menopause influence fat distribution, metabolic rate, and overall weight gain. Additionally, the synergistic effects of aging and menopause on these processes warrant more extensive investigation to inform the development of targeted interventions aimed at mitigating the associated health risks. Excess weight and the use of COCs are independent cardiovascular risk factors. Their concurrent use among women significantly increases the risk of pulmonary thromboembolism, with risk estimates ranging from 12 to 24 times higher [126]. In the current study, the use of COCs was not identified as a risk factor for the development of obesity. However, differences were observed between the groups; the overweight group had the highest percentage of COC use (7%) in both evaluated models.
The duration of sleep plays a crucial role in predicting cardiometabolic risk. Adequate sleep is crucial for maintaining cardiovascular health and metabolic function, as insufficient sleep has been associated with an increased risk of hypertension, obesity, diabetes mellitus, and cardiovascular disease (CVD) [127]. Short sleep duration (less than 7 hours per night) has been linked to an elevated risk of cardiometabolic diseases [128]. In particular, short sleep duration can lead to alterations in glucose metabolism, increased appetite, and reduced insulin sensitivity [129]. In our study, the normal weight group exhibited a significantly longer sleep duration compared to the overweight and obese groups in both evaluated models, with statistically significant differences (p<0.001). However, a sleep duration of less than 7 hours per night was not identified as a predictor for obesity in this analysis.
Both overweight and smoking status are significant factors for cardiovascular risk [130]. Quitting smoking reduces cardiovascular risk, but it is often accompanied by increased appetite and subsequent weight gain [131]. While weight gain is a common consequence of smoking cessation, the health benefits of quitting smoking far outweigh the risks associated with moderate weight gain. Nicotine, the primary addictive substance in cigarettes, increases metabolic rate. When smoking is discontinued, the metabolic rate decreases, leading to fewer calories being burned at rest [132]. Research indicates that quitting smoking results in an average weight gain of 4-5 kilograms within the first year, though this can vary widely among individuals [133]. Interestingly, despite the weight gain following smoking cessation, cardiovascular risk was still reduced compared to those whose weight remained constant [134]. In the present study, smoking was more prevalent among individuals with normal weight, confirming the relationship between lower weight, higher metabolic rate, and smoking status. Additionally, both the BMI-based and BFP-based models showed a significantly reduced percentage of weight gain after quitting smoking. However, smoking status, specifically smoking at least one cigarette daily for more than a year, was identified as a predictive factor for obesity when classified according to the percentage of adipose tissue.
Similar to smoking, alcohol consumption is another harmful factor within the category of lifestyle choices. The impact of alcohol consumption on nutritional status is influenced by several factors, leading to significant inter-individual variations [135]. Cross-sectional studies have found that alcohol consumption is not consistently associated with BMI, regardless of gender [135,136]. However, gender differences have been observed, with a stronger association between alcohol consumption and BMI among men. This disparity is primarily attributed to the quantity and type of alcohol consumed [137]. The current results identified significant differences in alcohol consumption between the control group and the overweight and obese groups (p<0.001), with consumption being higher among obese individuals in both evaluated models. Furthermore, alcohol consumption was identified as a risk factor for excess adipose tissue in the BFP-model.
According to the results, several risk factors were identified in both models—namely, BMI value and percentage of adipose tissue. However, certain predictors were associated only within a single model. This indicates that both models complement each other in the comprehensive assessment of an adult’s nutritional status. Furthermore, the comparative analysis of these models highlighted important differences in their predictive performance regarding various behaviors and eating patterns. The BMI-based model demonstrated an almost perfect discrimination between individuals with and without obesity, with an accuracy of 0.983, a specificity of 0.985, and a sensitivity of 0.982. These findings suggest that while each model has its strengths, their combined use provides a more holistic understanding of obesity-related risk factors.
Despite the promising results, there are several limitations associated with this study. While no other study has approached this subject with such precision, these findings must be interpreted within the context of these limitations. The study does not account for ethnic, cultural, and regional differences in the evaluated parameters, which negatively impacts the generalizability of the findings to populations with different eating habits compared to the evaluated groups. Another limitation is the use of the bioimpedance body analyzer, a device that may not be accessible to all clinicians for evaluating nutritional status and body composition, unlike the more readily available measurement of BMI. Additionally, the study did not aim to correlate the scores obtained from validated food and eating behavior questionnaires but rather to identify possible predictive factors for obesity from the perspective of two different classifications in a significant group of subjects. Furthermore, eating habits and their impact on nutritional status can change over time, an aspect that was not dynamically monitored in this study. Therefore, this research represents a preliminary step toward a more comprehensive approach in the field of nutrition and obesity research.
5. Conclusions
Even though BMI is considered limited in identifying and quantifying adipose tissue among individuals with obesity, it remains a valuable tool for evaluating the nutritional status of adults. Our research emphasizes the importance of employing various evaluation strategies and dynamic assessments in overweight adults to establish a correct and comprehensive management plan. By highlighting the complexity of the predictive factors contributing to overweight, our findings support the development of more effective and cost-efficient approaches, primarily aimed at preventing obesity. The adiposity-based model demonstrated good results with increased sensitivity and specificity; however, the BMI-based model exhibited superior performance in predicting obesity and overweight. Future research should focus on refining these models and exploring their implications across different population groups to establish more precise approaches for the prevention, monitoring, and treatment of obesity. This study underscores the necessity of integrated evaluation strategies that consider multiple dimensions of body composition and behavior, paving the way for improved interventions tailored to individual needs and broader public health strategies.
Author Contributions
Conceptualization, D.P. and D.S.; methodology, D.P and S.M; software, S.M.; validation, D.S., D.P. and A.B.; formal analysis, A.B.; investigation, D.P.; resources, D.S.; data curation, D.P.; writing—original draft preparation, D.P.; writing—review and editing, D.P.; visualization, D.S.; supervision, S.M. All authors have read and agreed to the published version of the manuscript.
Funding
Please add: “We would like to acknowledge VICTOR BABES UNIVERSITY OF MEDICINE AND PHARMACY TIMISOARA for their support in covering the costs of publication for this research paper.”.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by Scientific Research Ethics Committee (CECS) of the “Victor Babeș” University of Medicine and Pharmacy Timișoara (No. 69/03.10.2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
| Abbreviation | Meaning |
| BMI | Body mass index |
| BFP | Body fat percentage |
| BIA | Bioelectrical impedance analysis |
| BMR | Basal metabolic rate |
| OR | Odds ratio per unit |
| AUC | Confidence intervals for the area under the ROC curve |
| NHB | Non-Hispanic Blacks |
| NHW | Non-Hispanic whites |
| MHO | Metabolically healthy obesity |
| MHU | Metabolically unhealthy obesity |
| DXA | Dual-energy X-ray absorptiometry |
| CT | Computed tomography |
| MRI | Magnetic resonance imaging |
| CECS | Scientific Research Ethics Committee |
| m | Meter |
| ml | Millilitre |
| μA | Microampere |
| kHz | kilohertz |
| kg | kilos |
| kcal | kilocalories |
| R2 | Nagelkerke R Square ranges |
| R | R Core Team, 2024, a language and environment for statistical computing provided by the R Foundation for Statistical Computing, Vienna, Austria |
| CI | Confidence interval |
| FMH | Family Medical History |
| MI | Myocardial infarction |
| p-value | Pearson Chi-square test |
| PMS | Premenstrual syndrome |
| COCs | Combined oral contraceptives |
| PCOS | Polycystic ovarian syndrome |
References
- Amerikanou, C.; Kleftaki, S.A.; Valsamidou, E.; Tzavara, C.; Gioxari, A.; Kaliora, A.C. Dietary patterns, cardiometabolic and lifestyle variables in Greeks with obesity and metabolic disorders. Nutrients. 2022, 14, 5064. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cefalu, W.T.; Rodgers, G.P. COVID-19 and metabolic diseases: A heightened awareness of health inequities and a renewed focus for research priorities. Cell Metab. 2021, 33, 473–478. [Google Scholar] [CrossRef] [PubMed]
- Guan, L.; Li, T.; Wang, X.; Yu, K.; Xiao, R.; Xi, Y. Predictive roles of basal metabolic rate and body water distribution in sarcopenia and sarcopenic obesity: The link to carbohydrates. Nutrients. 2022, 14, 3911. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Koenen, M.; Hill, M.A.; Cohen, P.; Sowers, J.R. Obesity, adipose tissue, and vascular dysfunction. Circ Res. 2021, 128, 951–968. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lin, X.; Li, H. Obesity: Epidemiology, pathophysiology, and therapeutics. Front Endocrinol (Lausanne). 2021, 12, 706978. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in underweight and obesity from 1990 to 2022: A pooled analysis of 3663 population-representative studies with 222 million children, adolescents, and adults. Lancet. 2024, 403, 1027–1050. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Stewart, C. Obesity in Europe [Internet]. Statista. Available from: https://www.statista.com/topics/9419/obesity-in-europe/.
- Chang, V.W. Racial residential segregation and weight status among US adults. Soc Sci Med. 2006, 63, 1289–1303. [Google Scholar] [CrossRef] [PubMed]
- Kirby, J.B.; Liang, L.; Chen, H.J.; Wang, Y. Race, place, and obesity: The complex relationships among community racial/ethnic composition, individual race/ethnicity, and obesity in the United States. Am J Public Health. 2012, 102, 1572–1578. [Google Scholar] [CrossRef] [PubMed]
- Joseph, J.J.; Ortiz, R.; Acharya, T.; Golden, S.H.; López, L.; Deedwania, P. Cardiovascular impact of race and ethnicity in patients with diabetes and obesity: JACC focus seminar 2/9. J Am Coll Cardiol. 2021, 78, 2471–2482. [Google Scholar] [CrossRef] [PubMed]
- Beydoun, M.A.; Wang, Y. Gender-ethnic disparity in BMI and waist circumference distribution shifts in US adults. Obesity (Silver Spring). 2009, 17, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Chiu, M.; Austin, P.C.; Manuel, D.G.; Shah, B.R.; Tu, J.V. Deriving ethnic-specific BMI cutoff points for assessing diabetes risk. Diabetes Care. 2011, 34, 1741–1748. [Google Scholar] [CrossRef] [PubMed]
- Hales, C.M.; Carroll, M.D.; Fryar, C.D.; Ogden, C.L. Prevalence of obesity and severe obesity among adults: United States, 2017–2018. NCHS Data Brief, no 360. Hyattsville, MD: National Center for Health Statistics; 2020.
- Faith, J.J.; Guruge, J.L.; Charbonneau, M.; Subramanian, S.; Seedorf, H.; Goodman, A.L.; et al. The long-term stability of the human gut microbiota. Science. 2013, 341, 1237439. [Google Scholar] [CrossRef] [PubMed]
- Fontana, A.; Panebianco, C.; Picchianti-Diamanti, A.; Laganà, B.; Cavalieri, D.; Potenza, A.; et al. Gut microbiota profiles differ among individuals depending on their region of origin: An Italian pilot study. Int J Environ Res Public Health. 2019, 16, 4065. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- He, Y.; Wu, W.; Zheng, H.M.; Li, P.; McDonald, D.; Sheng, H.F.; et al. Regional variation limits applications of healthy gut microbiome reference ranges and disease models. Nat Med. 2018, 24, 1532–1535. [Google Scholar] [CrossRef] [PubMed]
- Yárnoz-Esquiroz, P.; Olazarán, L.; Aguas-Ayesa, M.; Perdomo, C.M.; García-Goni, M.; et al. Obesities’: Position statement on a complex disease entity with multifaceted drivers. Eur J Clin Invest. 2022, 52, e13811. [Google Scholar] [CrossRef] [PubMed]
- Masood, B.; Moorthy, M. Causes of obesity: A review. Clin Med (Lond). 2023, 23, 284–291. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Butland, B.; Jebb, S.; Kopelman, P.; McPherson, K.; Thomas, S.; Mardell, J.; et al. FORESIGHT-Tackling obesities: Future choices. London: Government Office for Science; 2007.
- Sarma, S.; Sockalingam, S.; Dash, S. Obesity as a multisystem disease: Trends in obesity rates and obesity-related complications. Diabetes Obes Metab. 2021, 23(S1), 3–16. [Google Scholar] [CrossRef] [PubMed]
- Agostoni, C.; Braegger, C.; Decsi, T.; Kolacek, S.; Koletzko, B.; Michaelsen, K.F.; et al. Breast-feeding: A commentary by the ESPGHAN Committee on Nutrition. J Pediatr Gastroenterol Nutr. 2009, 49, 112–125. [Google Scholar] [CrossRef] [PubMed]
- Morgan, K.J.; Zabik, M.E.; Stampley, G. The role of breakfast in diet adequacy of the U. S. adult population. J Am Coll Nutr. 1986, 5, 551–563. [Google Scholar] [CrossRef] [PubMed]
- Hruby, A.; Hu, F.B. The epidemiology of obesity: A big picture. Pharmacoeconomics. 2015, 33, 673–689. [Google Scholar] [CrossRef] [PubMed]
- Gardner, C.D.; Kiazand, A.; Alhassan, S.; Kim, S.; Stafford, R.S.; Balise, R.R.; et al. Comparison of the Atkins, Zone, Ornish, and LEARN diets for change in weight and related risk factors among overweight premenopausal women: The A TO Z Weight Loss Study: A randomized trial. JAMA. 2007, 297, 969–977. [Google Scholar] [CrossRef] [PubMed]
- Sacks, F.M.; Bray, G.A.; Carey, V.J.; Smith, S.R.; Ryan, D.H.; Anton, S.D.; et al. Comparison of weight-loss diets with different compositions of fat, protein, and carbohydrates. N Engl J Med. 2009, 360, 859–873. [Google Scholar] [CrossRef] [PubMed]
- Pol, K.; Christensen, R.; Bartels, E.M.; Raben, A.; Tetens, I.; Kristensen, M. Whole grain and body weight changes in apparently healthy adults: A systematic review and meta-analysis of randomized controlled studies. Am J Clin Nutr. 2013, 98, 872–884. [Google Scholar] [CrossRef] [PubMed]
- Flores-Mateo, G.; Rojas-Rueda, D.; Basora, J.; Ros, E.; Salas-Salvadó, J. Nut intake and adiposity: Meta-analysis of clinical trials. Am J Clin Nutr. 2013, 97, 1346–1355. [Google Scholar] [CrossRef] [PubMed]
- Keski-Rahkonen, A.; Kaprio, J.; Rissanen, A.; Virkkunen, M.; Rose, R.J. Breakfast skipping and health compromising behaviors in adolescents and adults. Eur J Clin Nutr. 2003, 57, 842–853. [Google Scholar] [CrossRef] [PubMed]
- Sahoo, K.; Sahoo, B.; Choudhury, A.K.; Sofi, N.Y.; Kumar, R.; Bhadoria, A.S. Childhood obesity: causes and consequences. J Family Med Prim Care. 2015, 4, 187–192. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rivera Medina, C.; Briones Urbano, M.; de Jesús Espinosa, A.; Toledo López, Á. Eating habits associated with nutrition-related knowledge among university students enrolled in academic programs related to nutrition and culinary arts in Puerto Rico. Nutrients. 2020, 12, 1408. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Birch, L.L.; Davison, K.K. Family environmental factors influencing the developing behavioral controls of food intake and childhood overweight. Pediatr Clin North Am. 2001, 48, 893–907. [Google Scholar] [CrossRef] [PubMed]
- Ebrahimi, S.; Leech, R.M.; McNaughton, S.A.; Abdollahi, M.; Houshiarrad, A.; Livingstone, K.M. Associations between diet quality and obesity in a nationally representative sample of Iranian households: A cross-sectional study. Obes Sci Pract. 2021, 8, 12–20. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Latorre-Millán, M.; Rupérez, A.I.; González-Gil, E.M.; Santaliestra-Pasías, A.; Vázquez-Cobela, R.; Gil-Campos, M.; et al. Dietary patterns and their association with body composition and cardiometabolic markers in children and adolescents: Genobox cohort. Nutrients. 2020, 12, 3424. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Davy, S.R.; Benes, B.A.; Driskell, J.A. Sex differences in dieting trends, eating habits, and nutrition beliefs of a group of Midwestern college students. J Am Diet Assoc. 2006, 106, 1673–1677. [Google Scholar] [CrossRef] [PubMed]
- de Toro-Martín, J.; Arsenault, B.J.; Després, J.P.; Vohl, M.C. Precision nutrition: A review of personalized nutritional approaches for the prevention and management of metabolic syndrome. Nutrients. 2017, 9, 913. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Salmón-Gómez, L.; Catalán, V.; Frühbeck, G.; Gómez-Ambrosi, J. Relevance of body composition in phenotyping the obesities. Rev Endocr Metab Disord. 2023, 24, 809–823. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Quetelet, L.A.J. Sur l’homme et le développement de ses facultés, ou essai de physique sociale. Paris: Bachelier; 1835.
- Keys, A.; Fidanza, F.; Karvonen, M.J.; Kimura, N.; Taylor, H.L. Indices of relative weight and obesity. J Chronic Dis. 1972, 25, 329–343. [Google Scholar] [CrossRef] [PubMed]
- Blundell, J.E.; Dulloo, A.G.; Salvador, J.; Frühbeck, G. Beyond BMI: Phenotyping the obesities. Obes Facts. 2014, 7, 322–328. [Google Scholar] [CrossRef] [PubMed]
- Khattak, Z.E.; Zahra, F. Evaluation of patients with obesity. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023.
- Stewart, C. Obesity in Europe [Internet]. Statista. Available from: https://www.statista.com/topics/9419/obesity-in-europe/.
- Di Angelantonio, E.; Bhupathiraju, S.N.; Wormser, D.; Gao, P.; Kaptoge, S.; Berrington de Gonzalez, A.; et al. Body-mass index and all-cause mortality: Individual-participant-data meta-analysis of 239 prospective studies in four continents. Lancet. 2016, 388, 776–786. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bhaskaran, K.; Dos-Santos-Silva, I.; Leon, D.A.; Douglas, I.J.; Smeeth, L. Association of BMI with overall and cause-specific mortality: A population-based cohort study of 3.6 million adults in the UK. Lancet Diabetes Endocrinol. 2018, 6, 944–953. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Atakan, M.M.; Koşar, Ş.N.; Güzel, Y.; Tin, H.T.; Yan, X. The role of exercise, diet, and cytokines in preventing obesity and improving adipose tissue. Nutrients. 2021, 13, 1459. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Neeland, I.J.; de Lemos, J.A. Time to retire the BMI?: Evaluating abdominal adipose tissue imaging as a novel cardiovascular risk biomarker. J Am Coll Cardiol. 2016, 68, 1522–1524. [Google Scholar] [CrossRef] [PubMed]
- Prentice, A.M.; Jebb, S.A. Beyond body mass index. Obes Rev. 2001, 2, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, B.R.; Magalhães, E.I.D.S.; Bragança, M.L.B.M.; Coelho, C.C.N.D.S.; Lima, N.P.; Bettiol, H.; et al. Performance of body fat percentage, fat mass index and body mass index for detecting cardiometabolic outcomes in Brazilian adults. Nutrients. 2023, 15, 2974. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ho-Pham, L.T.; Campbell, L.V.; Nguyen, T.V. More on body fat cutoff points. Mayo Clin Proc. 2011, 86, 584. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- VanItallie, T.B.; Yang, M.U.; Heymsfield, S.B.; Funk, R.C.; Boileau, R.A. Height-normalized mass: Potentially. Am J Clin Nutr. 1990, 52, 953–959. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.; Ma, F.; Lou, H.; Liu, Y. The utility of fat mass index vs. body mass index and percentage of body fat in the screening of metabolic syndrome. BMC Public Health. 2013, 13, 629. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ramírez-Vélez, R.; Correa-Bautista, J.E.; Sanders-Tordecilla, A.; Ojeda-Pardo, M.L.; Cobo-Mejía, E.A.; Castellanos-Vega, R.d.P.; et al. Percentage of body fat and fat mass index as a screening tool for metabolic syndrome prediction in Colombian university students. Nutrients. 2017, 9, 1009. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pasdar, Y.; Hamzeh, B.; Najafi, F.; Darbandi, M. Optimal cutoff values of fat mass index, body fat percentage and visceral fat area for identifying metabolic syndrome in the Kurdish population: Results from an Iranian RaNCD cohort study. Med J Nutr Metab. 2019, 12, 397–409. [Google Scholar] [CrossRef]
- TANITA Europe B.V. Body fat percentage - are you at a healthy weight? Available from: https://tanita.co.uk/understanding-your-measurements/body-fat-percentage. Accessed 20 June 2024.
- Gallagher, D.; Heymsfield, S.B.; Heo, M.; Jebb, S.A.; Murgatroyd, P.R.; Sakamoto, Y. Healthy percentage body fat ranges: an approach for developing guidelines based on body mass index. Am J Clin Nutr. 2000, 72, 694–701. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, H.D.; Cole, T.J.; Fry, T.; Jebb, S.A.; Prentice, A.M. Body fat reference curves for children. Int J Obes (Lond). 2006, 30, 598–602. [Google Scholar] [CrossRef] [PubMed]
- Blüher, M. Metabolically healthy obesity. Endocr Rev. 2020, 41, bnaa004. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Vague, J. The degree of masculine differentiation of obesities: a factor determining predisposition to diabetes, atherosclerosis, gout, and uric calculous disease. Am J Clin Nutr. 1956, 4, 20–34. [Google Scholar] [CrossRef] [PubMed]
- van Vliet-Ostaptchouk, J.V.; Nuotio, M.L.; Slagter, S.N.; et al. The prevalence of metabolic syndrome and metabolically healthy obesity in Europe: a collaborative analysis of ten large cohort studies. BMC Endocr Disord. 2014, 14, 9. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Magkos, F. Metabolically healthy obesity: what’s in a name? Am J Clin Nutr. 2019, 110, 533–539. [Google Scholar] [CrossRef] [PubMed]
- Rey-López, J.P.; de Rezende, L.F.; Pastor-Valero, M.; Tess, B.H. The prevalence of metabolically healthy obesity: a systematic review and critical evaluation of the definitions used. Obes Rev. 2014, 15, 781–790. [Google Scholar] [CrossRef] [PubMed]
- Chouchani, E.T.; Kajimura, S. Metabolic adaptation and maladaptation in adipose tissue. Nat Metab. 2019, 1, 189–200. [Google Scholar] [CrossRef] [PubMed]
- Feng, B.; Zhang, T.; Xu, H. Human adipose dynamics and metabolic health. Ann N Y Acad Sci. [CrossRef] [PubMed]
- Coelho, M.; Oliveira, T.; Fernandes, R. Biochemistry of adipose tissue: an endocrine organ. Arch Med Sci. 2013, 9, 191–200. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Luo, L.; Liu, M. Adipose tissue in control of metabolism. J Endocrinol. 2016, 231, R77–R99. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chait, A.; den Hartigh, L.J. Adipose tissue distribution, inflammation and its metabolic consequences, including diabetes and cardiovascular disease. Front Cardiovasc Med. 2020, 7, 22. [Google Scholar] [CrossRef] [PubMed]
- Klebanova, E.M.; Balabolkin, M.I.; Kreminskaia, V.M. The role of the fat tissue and its hormones in the mechanisms of insulin resistance and the development of type 2 diabetes mellitus. Klin Med (Mosk). 2007, 85, 20–27. [Google Scholar] [PubMed]
- Lohman, T.M. ACSM’s Body Composition Assessment. Champaign, IL: Human Kinetics; 2019.
- Commean, P.K.; Mueller, M.J.; Chen, L.; Wolfsberger, M.A.; Hastings, M.K. Computed Tomography and Magnetic Resonance Correlation and Agreement for Foot Muscle and Adipose Tissue Measurements. J Comput Assist Tomogr. 2022, 46, 212–218. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Jaffrin, M. Body composition determination by bioimpedance: An update. Curr Opin Clin Nutr Metab Care. 2009, 12, 482–486. [Google Scholar] [CrossRef] [PubMed]
- Haroun, D.; Taylor, S.J.C.; Viner, R.M.; Hayward, R.S.; Darch, T.S.; Eaton, S.; et al. Validation of bioelectrical impedance analysis in adolescents across different ethnic groups. PLoS One. 2012, 7, e30925. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kuriyan, R. Body composition techniques. Indian J Med Res. 2018, 148, 648–658. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Weir, C.B.; Jan, A. BMI Classification Percentile and Cut-Off Points. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023. Updated 2022 Jun 27.
- Holt, R.I.; Bushe, C.; Citrome, L. Diabetes and schizophrenia 2005: Are we any closer to understanding the link? J Psychopharmacol. 2005, 19 (Suppl. 6), 56–65. [Google Scholar] [CrossRef] [PubMed]
- Magiakou, M.A.; Mastorakos, G.; Oldfield, E.H.; et al. Cushing’s syndrome in children and adolescents. Presentation, diagnosis and therapy. N Engl J Med. 1994, 331, 629–636. [Google Scholar] [CrossRef] [PubMed]
- Consensus development conference on antipsychotic drugs and obesity and diabetes (Consensus Statement). Diabetes Care. 2004, 27, 596–601. [CrossRef] [PubMed]
- Daviet, R.; Aydogan, G.; Jagannathan, K.; et al. Associations between alcohol consumption and gray and white matter volumes in the UK Biobank. Nat Commun. 2022, 13, 1175. [Google Scholar] [CrossRef]
- Watson, N.F.; Badr, M.S.; Belenky, G.; Bliwise, D.L.; Buxton, O.M.; Buysse, D.; et al. Recommended amount of sleep for a healthy adult: A joint consensus statement of the American Academy of Sleep Medicine and Sleep Research Society. Sleep. 2015, 38, 843–4. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Brunani, A.; Perna, S.; Soranna, D.; Rondanelli, M.; Zambon, A.; Bertoli, S.; et al. Body composition assessment using bioelectrical impedance analysis (BIA) in a wide cohort of patients affected with mild to severe obesity. Clin Nutr. 2021, 40, 3973–3981. [Google Scholar] [CrossRef] [PubMed]
- Heyward, V.H.; Wagner, D.R. Applied Body Composition Assessment. Champaign, IL: Human Kinetics; 2004.
- Nuttall, F.Q. Body mass index: Obesity, BMI, and health: A critical review. Nutr Today. 2015, 50, 117–128. [Google Scholar] [CrossRef] [PubMed]
- Slawik, M.; Vidal-Puig, A.J. Lipotoxicity, overnutrition, and energy metabolism in aging. Ageing Res Rev. 2006, 5, 144–164. [Google Scholar] [CrossRef] [PubMed]
- Jura, M.; Kozak, L.P. Obesity and related consequences to ageing. Age (Dordr). 2016, 38, 23. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kuk, J.L.; Saunders, T.J.; Davidson, L.E.; Ross, R. Age-related changes in total and regional fat distribution. Ageing Res Rev. 2009, 8, 339–348. [Google Scholar] [CrossRef] [PubMed]
- Chapman, C.D.; Nilsson, V.C.; Thune, H.Å.; Cedernaes, J.; Le Grevès, M.; Hogenkamp, P.S.; et al. Watching TV and food intake: the role of content. PLoS One. 2014, 9, e100602. [Google Scholar] [CrossRef] [PubMed]
- Holmes, C.J.; Racette, S.B. The utility of body composition assessment in nutrition and clinical practice: an overview of current methodology. Nutrients. 2021, 13, 2493. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Campa, F.; Toselli, S.; Mazzilli, M.; Gobbo, L.A.; Coratella, G. Assessment of body composition in athletes: a narrative review of available methods with special reference to quantitative and qualitative bioimpedance analysis. Nutrients. 2021, 13, 1620. [Google Scholar] [CrossRef]
- Anderson, L.J.; Erceg, D.N.; Schroeder, E.T. Utility of multifrequency bioelectrical impedance compared with dual-energy X-ray absorptiometry for assessment of total and regional body composition varies between men and women. Nutr Res. 2012, 32, 479–485. [Google Scholar] [CrossRef] [PubMed]
- Batsis, J.A.; Villareal, D.T. Sarcopenic obesity in older adults: Aetiology, epidemiology and treatment strategies. Nat Rev Endocrinol. 2018, 14, 513–537. [Google Scholar] [CrossRef] [PubMed]
- Ji, T.; Li, Y.; Ma, L. Sarcopenic obesity: an emerging public health problem. Aging Dis. 2022, 13, 379–388. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pontzer, H.; Yamada, Y.; Sagayama, H.; Ainslie, P.N.; Andersen, L.F.; Anderson, L.J.; et al. Daily energy expenditure through the human life course. Science. 2021, 373, 808–812. [Google Scholar] [CrossRef] [PubMed]
- Mohammadi, S.; Dolatshahi, M.; Zare-Shahabadi, A.; Rahmani, F. Untangling narcolepsy and diabetes: pathomechanisms with eyes on therapeutic options. Brain Res. 2019, 1718, 212–222. [Google Scholar] [CrossRef] [PubMed]
- Celik, A.; Cebeci, A.N. Evaluation of hydration status of children with obesity—a pilot study. J Pediatr Endocrinol Metab. 2021, 34, 295–300. [Google Scholar] [CrossRef] [PubMed]
- Rashidmayvan, M.; Sharifan, P.; Darroudi, S.; Saffar Soflaei, S.; Salaribaghoonabad, R.; Safari, N.; et al. Association between dietary patterns and body composition in normal-weight subjects with metabolic syndrome. J Diabetes Metab Disord. 2022, 21, 735–741. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bahrampour, N.; Mirzababaei, A.; Shiraseb, F.; Clark, C.C.; Mirzaei, K. The mediatory role of inflammatory markers on the relationship between dietary energy density and body composition among obese and overweight adult women: a cross-sectional study. Int J Clin Pract. 2021, 75, e14579. [Google Scholar] [CrossRef] [PubMed]
- Caspersen, C.J.; Powell, K.E.; Christenson, G.M. Physical activity, exercise, and physical fitness: definitions and distinctions for health-related research. Public Health Rep. 1985, 100, 126–131. [Google Scholar] [PubMed] [PubMed Central]
- Yuksel, H.S.; Şahin, F.N.; Maksimovic, N.; Drid, P.; Bianco, A. School-based intervention programs for preventing obesity and promoting physical activity and fitness: A systematic review. Int J Environ Res Public Health. 2020, 17, 347. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ogden, C.L.; Carroll, M.D.; Curtin, L.R.; McDowell, M.A.; Tabak, C.J.; Flegal, K.M. Prevalence of overweight and obesity in the United States, 1999–2004. JAMA. 2006, 295, 1549–1555. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, C.; Reilly, J.J.; Huang, W.Y. Longitudinal changes in objectively measured sedentary behaviour and their relationship with adiposity in children and adolescents: Systematic review and evidence appraisal. Obes Rev. 2014, 15, 791–803. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Li, X.; Chattopadhyay, K.; Chen, X.; Li, J.; Xu, M.; Chen, X.; et al. Association between physical activity and arterial stiffness in patients with type 2 diabetes in Ningbo, China: A cross-sectional study. Diabetes Metab Syndr Obes. 2023, 16, 4133–4141. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Langleite, T.; Jensen, J.; Norheim, F.; et al. Insulin sensitivity, body composition, and adipose depots following 12 weeks of combined endurance and strength training in dysglycemic and normoglycemic sedentary men. Arch Physiol Biochem. 2016, 122, 167–179. [Google Scholar] [CrossRef] [PubMed]
- Grzymisławska, M.; Puch, E.A.; Zawada, A.; Grzymisławski, M. Do nutritional behaviors depend on biological sex and cultural gender? Adv Clin Exp Med. 2020, 29, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Smith, D.L.; Keating, K.D.; Allison, D.B.; Nagy, T.R. Variations in body weight, food intake, and body composition after long-term high-fat diet feeding in C57BL/6J mice: Variations in diet-induced obese C57BL/6J mice. Obesity (Silver Spring). 2014, 22, 2147–2155. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hwang, L.; Wang, C.; Li, T.; Chang, S.; Lin, L.; Chen, C.; et al. Sex differences in high-fat diet-induced obesity, metabolic alterations and learning, and synaptic plasticity deficits in mice. Obesity (Silver Spring). 2010, 18, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Koceva, A.; Herman, R.; Janez, A.; Rakusa, M.; Jensterle, M. Sex- and gender-related differences in obesity: From pathophysiological mechanisms to clinical implications. Int J Mol Sci. 2024, 25, 7342. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lostein, T.; Jackson-Leach, R.; Powis, J.; Brinsden, H.; Gray, M. World Obesity Federation, World Obesity Atlas 2023. Available online: https://www.worldobesity.org/resources/resource-library/world-obesity-atlas-2023 (accessed on 21 June 2024).
- Karastergiou, K.; Smith, S.R.; Greenberg, A.S.; Fried, S.K. Sex differences in human adipose tissues—The biology of pear shape. Biol Sex Differ. 2012, 3, 13. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Jackson, A.; Stanforth, P.; Gagnon, J.; Rankinen, T.; Leon, A.; Rao, D.; et al. The effect of sex, age, and race on estimating percentage body fat from body mass index: The Heritage Family Study. Int J Obes. 2002, 26, 789–96. [Google Scholar] [CrossRef] [PubMed]
- Christen, T.; Trompet, S.; Noordam, R.; Van Klinken, J.B.; Van Dijk, K.W.; Lamb, H.J.; et al. Sex differences in body fat distribution are related to sex differences in serum leptin and adiponectin. Peptides. 2018, 107, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Kroll, D.S.; Feldman, D.E.; Biesecker, C.L.; McPherson, K.L.; Manza, P.; Joseph, P.V.; et al. Neuroimaging of sex/gender differences in obesity: A review of structure, function, and neurotransmission. Nutrients. 2020, 12, 1942. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Stice, E.; Spoor, S.; Bohon, C.; Small, D.M. Relation between obesity and blunted striatal response to food is moderated by TaqIA A1 allele. Science. 2008, 322, 449–52. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Stea, T.H.; Nordheim, O.; Bere, E.; Stornes, P.; Eikemo, T.A. Fruit and vegetable consumption in Europe according to gender, educational attainment and regional affiliation—a cross-sectional study in 21 European countries. PLoS One. 2020, 15, e0232521. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Emanuel, A.S.; McCully, S.N.; Gallagher, K.M.; Updegraff, J.A. Theory of Planned Behavior explains gender difference in fruit and vegetable consumption. Appetite. 2012, 59, 693–7. [Google Scholar] [CrossRef] [PubMed]
- Wansink, B.; Cheney, M.; Chan, N. Exploring comfort food preferences across age and gender. Physiol Behav. 2003, 79, 739–47. [Google Scholar] [CrossRef] [PubMed]
- Lombardo, M.; Aulisa, G.; Padua, E.; Annino, G.; Iellamo, F.; Pratesi, A.; et al. Gender differences in taste and food habits. Nutr Food Sci. 2019, 50, 229–39. [Google Scholar] [CrossRef]
- Lazarevich, I.; Irigoyen Camacho, M.E.; Velázquez-Alva, M.D.C.; Zepeda Zepeda, M. Relationship among obesity, depression, and emotional eating in young adults. Appetite. 2016, 107, 639–44. [Google Scholar] [CrossRef] [PubMed]
- Van Strien, T.; Herman, C.P.; Verheijden, M.W. Eating style, overeating and overweight in a representative Dutch sample: Does external eating play a role? Appetite. 2009, 52, 380–7. [Google Scholar] [CrossRef] [PubMed]
- Van Strien, T.; Herman, C.P.; Verheijden, M.W. Eating style, overeating and weight gain: A prospective 2-year follow-up study in a representative Dutch sample. Appetite. 2012, 59, 782–9. [Google Scholar] [CrossRef] [PubMed]
- Dakanalis, A.; Mentzelou, M.; Papadopoulou, S.K.; Papandreou, D.; Spanoudaki, M.; Vasios, G.K.; et al. The Association of Emotional Eating with Overweight/Obesity, Depression, Anxiety/Stress, and Dietary Patterns: A Review of the Current Clinical Evidence. Nutrients. 2023, 15, 1173. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Grajek, M.; Krupa-Kotara, K.; Białek-Dratwa, A.; Staśkiewicz, W.; Rozmiarek, M.; Misterska, E.; et al. Prevalence of Emotional Eating in Groups of Students with Varied Diets and Physical Activity in Poland. Nutrients. 2022, 14, 3289. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Czepczor-Bernat, K.; Brytek-Matera, A.; Gramaglia, C.; Zeppegno, P. The moderating effects of mindful eating on the relationship between emotional functioning and eating styles in overweight and obese women. Eat Weight Disord. 2020, 25, 841–849. [Google Scholar] [CrossRef] [PubMed]
- D’Innocenzo, S.; Biagi, C.; Lanari, M. Obesity and the Mediterranean Diet: A Review of Evidence of the Role and Sustainability of the Mediterranean Diet. Nutrients. 2019, 11, 1306. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Palacios, S.; Chedraui, P.; Sánchez-Borrego, R.; Coronado, P.; Nappi, R.E. Obesity and menopause. Gynecol Endocrinol. Epub 2024 Feb 11. 2024, 40, 2312885. [Google Scholar] [CrossRef] [PubMed]
- Lizcano, F.; Guzmán, G. Estrogen Deficiency and the Origin of Obesity during Menopause. Biomed Res Int. 2014, 2014, 757461. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Toth, M.J.; Poehlman, E.T.; Matthews, D.E.; Tchernof, A.; MacCoss, M.J. Effects of estradiol and progesterone on body composition, protein synthesis, and lipoprotein lipase in rats. Am J Physiol Endocrinol Metab. 2001, 280, E496–E501. [Google Scholar] [CrossRef] [PubMed]
- Eshtiaghi, R.; Esteghamati, A.; Nakhjavani, M. Menopause is an independent predictor of metabolic syndrome in Iranian women. Maturitas. 2010, 65, 262–266. [Google Scholar] [CrossRef] [PubMed]
- Rosano, G.M.C.; Rodriguez-Martinez, M.A.; Spoletini, I.; Regidor, P.A. Obesity and contraceptive use: impact on cardiovascular risk. ESC Heart Fail. 2022, 9, 3761–3767. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cappuccio, F.P.; Cooper, D.; D’Elia, L.; Strazzullo, P.; Miller, M.A. Sleep duration predicts cardiovascular outcomes: a systematic review and meta-analysis of prospective studies. Eur Heart J. 2011, 32, 1484–1492. [Google Scholar] [CrossRef] [PubMed]
- Gangwisch, J.E.; Heymsfield, S.B.; Boden-Albala, B.; Buijs, R.M.; Kreier, F.; Pickering, T.G.; et al. Short sleep duration as a risk factor for hypertension: analyses of the first National Health and Nutrition Examination Survey. Hypertension. 2006, 47, 833–839. [Google Scholar] [CrossRef] [PubMed]
- Spiegel, K.; Leproult, R.; Van Cauter, E. Impact of sleep debt on metabolic and endocrine function. Lancet. 1999, 354, 1435–1439. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Qin, L.Q.; Arafa, A.; Eshak, E.S.; Hu, Y.; Dong, J.Y. Smoking Cessation, Weight Gain, Cardiovascular Risk, and All-Cause Mortality: A Meta-analysis. Nicotine Tob Res. 2021, 23, 1987–1994. [Google Scholar] [CrossRef] [PubMed]
- Duncan, M.S.; Freiberg, M.S.; Greevy RAJr Kundu, S.; Vasan, R.S.; Tindle, H.A. Association of smoking cessation with subsequent risk of cardiovascular disease. JAMA. 2019, 322, 642–650. [Google Scholar] [CrossRef]
- Filozof, C.; Fernández Pinilla, M.C.; Fernández-Cruz, A. Smoking cessation and weight gain. Obes Rev. 2004, 5, 95–103. [Google Scholar] [CrossRef]
- Aubin, H.J.; Farley, A.; Lycett, D.; Lahmek, P.; Aveyard, P. Weight gain in smokers after quitting cigarettes: meta-analysis. BMJ. 2012, 345, e4439. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.H.; Kwon, H.M.; Park, S.E.; et al. Protective effect of smoking cessation on subsequent myocardial infarction and ischemic stroke independent of weight gain: a nationwide cohort study. PLoS One. 2020, 15, e0235276. [Google Scholar] [CrossRef] [PubMed]
- Traversy, G.; Chaput, J.P. Alcohol Consumption and Obesity: An Update. Curr Obes Rep. 2015, 4, 122–30. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sayon-Orea, C.; Martinez-Gonzalez, M.A.; Bes-Rastrollo, M. Alcohol consumption and body weight: a systematic review. Nutr Rev. 2011, 69, 419–31. [Google Scholar] [CrossRef]
- French, M.T.; Norton, E.C.; Fang, H.; Maclean, J.C. Alcohol consumption and body weight. Health Econ. 2010, 19, 814–832. [Google Scholar] [CrossRef]
Figure 1.
Significant risk factors for BMI and BFP models. Abbreviations: BMI - Body Mass Index, BMR - Basal Metabolic Rate, PMS - Premenstrual syndrome.
Figure 1.
Significant risk factors for BMI and BFP models. Abbreviations: BMI - Body Mass Index, BMR - Basal Metabolic Rate, PMS - Premenstrual syndrome.
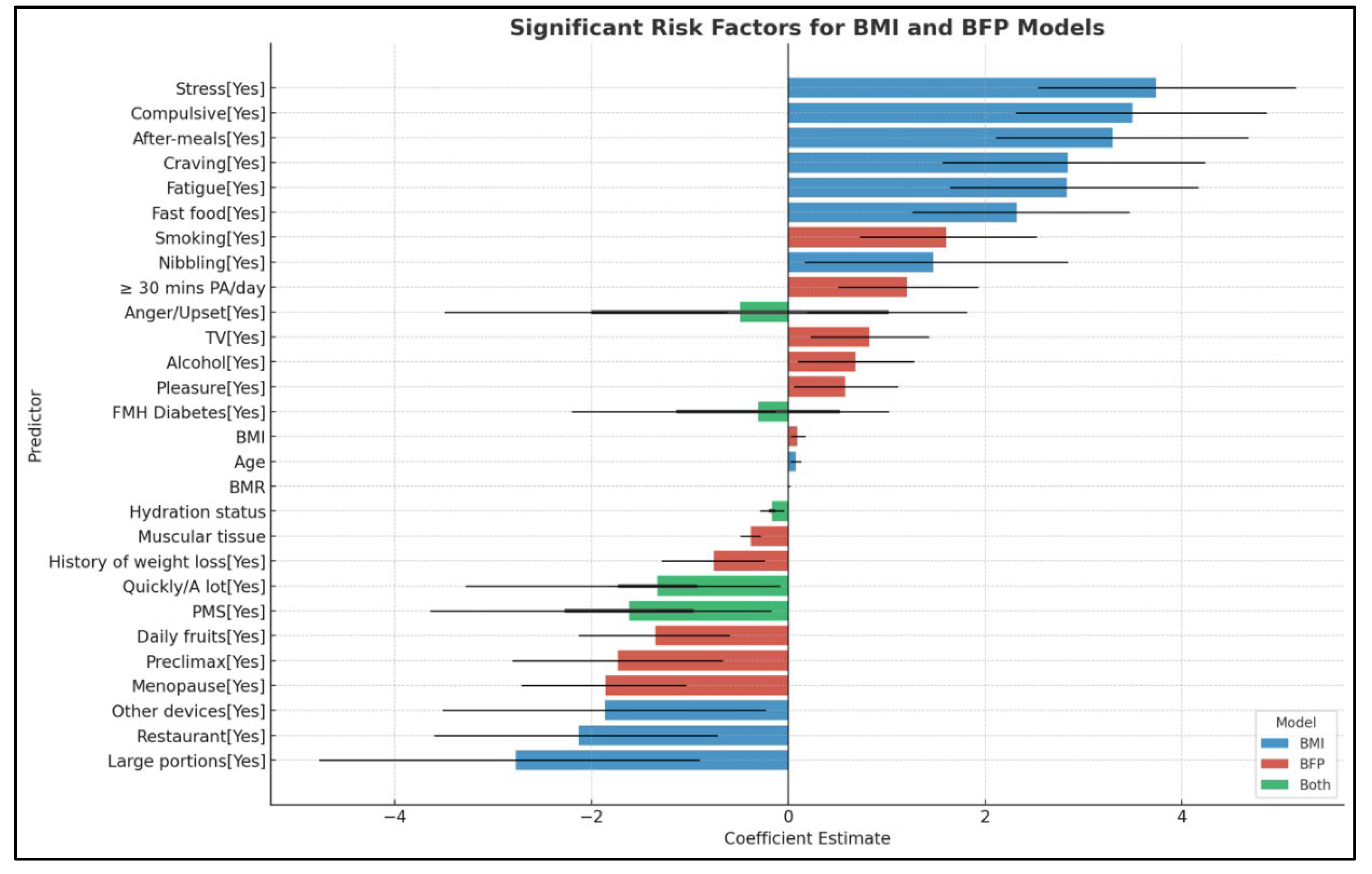
Figure 2.
Comparison of BMI and BFP models.
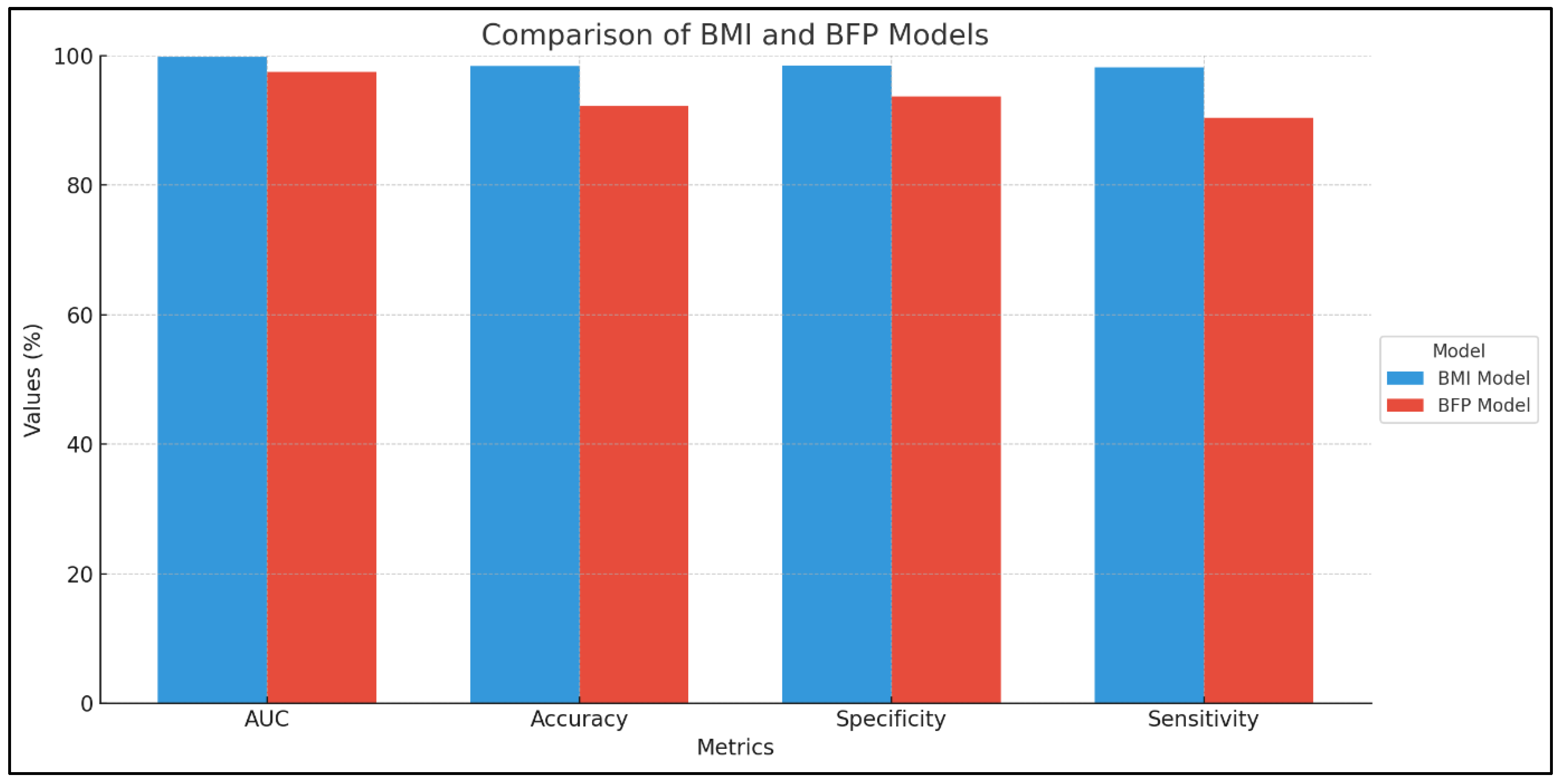

Table 1.
Numerical variables based on BMI classification.
| Variable | Control (n=397) | Overweight (n=261) | Obese (n=597) | p-value |
|---|---|---|---|---|
| Age | 33 | 31 | 38 | < 0.001 |
| Water intake | 2500 | 1500 | 1500 | < 0.001 |
| Coffee | 250 | 0 | 100 | < 0.001 |
| Milk | 0 | 0 | 0 | < 0.001 |
| Sweetened liquids | 0 | 0 | 0 | < 0.001 |
| Hours of sleep | 9 | 7 | 7 | < 0.001 |
| Adipose tissue (%) | 21 | 35 | 42 | < 0.001 |
| Muscular tissue (%) | 76 | 61 | 54 | < 0.001 |
| BMR | 1823 | 1498 | 1805 | <0.001 |
| Hydration status | 61 | 47 | 42 | < 0.001 |
Abbreviations: BMR - Basal Metabolic Rate, p-value - Mann-Whitney U test.
Table 2.
Numerical variables based on BFP classification.
| Variable | Control (n=394) | Overweight (n=225) | Obese (n=542) | p-value |
|---|---|---|---|---|
| Age | 34 | 35 | 37 | < 0.001 |
| Water intake | 2500 | 1500 | 1500 | < 0.001 |
| Coffee | 250 | 0 | 100 | < 0.001 |
| Milk | 0 | 0 | 0 | < 0.001 |
| Sweetened liquids | 0 | 0 | 0 | < 0.001 |
| Hours of sleep | 9 | 7 | 7 | < 0.001 |
| BMI | 22 | 29 | 36 | < 0.001 |
| Muscular tissue (%) | 73 | 60 | 54 | < 0.001 |
| BMR | 1795 | 1545 | 1801 | <0.001 |
| Hydration status | 60 | 46 | 41 | < 0.001 |
Abbreviations: BMR - Basal Metabolic Rate, p-value - Mann-Whitney U test.
Table 3.
Demographic and lifestyle factors based on BMI classification.
| Variable | Class | Control (n=397) | Overweight (n=261) | Obese (n=597) | p-value |
|---|---|---|---|---|---|
| Sex | M | 50% | 21% | 32% | < 0.001 |
| F | 50% | 79% | 68% | ||
| Supplement | Yes | 0% | 21% | 18% | < 0.001 |
| No | 100% | 79% | 82% | ||
| Holiday | Yes | 8% | 14% | 13% | 0.04 |
| No | 92% | 86% | 87% | ||
| TV | Yes | 2% | 5% | 88% | < 0.001 |
| No | 98% | 95% | 12% | ||
| Other devices | Yes | 0% | 7% | 6% | < 0.001 |
| No | 100% | 93% | 94% | ||
| 30 mins PA/day | Yes | 94% | 16% | 10% | < 0.001 |
| No | 6% | 84% | 90% | ||
| Alcohol | Yes | 2% | 26% | 29% | < 0.001 |
| No | 98% | 74% | 71% | ||
| Smoking | Yes | 39% | 4% | 7% | < 0.001 |
| No | 61% | 96% | 93% |
Abbreviations: PA - Physical activity, p-value - Pearson Chi-square test.
Table 4.
Demographic and lifestyle factors based on BFP classification.
| Variable | Class | Control (n=394) | Overweight (n=225) | Obese (n=542) | p-value |
|---|---|---|---|---|---|
| Sex | M | 45% | 24% | 35% | < 0.001 |
| F | 55% | 76% | 65% | ||
| Supplement | Yes | 3% | 17% | 20% | < 0.001 |
| No | 97% | 83% | 80% | ||
| Holiday | Yes | 7% | 13% | 15% | 0.002 |
| No | 93% | 87% | 85% | ||
| TV | Yes | 4% | 32% | 79% | < 0.001 |
| No | 96% | 68% | 21% | ||
| Other devices | Yes | 1% | 3% | 6% | < 0.001 |
| No | 99% | 97% | 94% | ||
| 30 mins PA/day | Yes | 82% | 16% | 13% | < 0.001 |
| No | 18% | 84% | 87% | ||
| Alcohol | Yes | 7% | 20% | 31% | < 0.001 |
| No | 93% | 80% | 69% | ||
| Smoking | Yes | 27% | 10% | 9% | < 0.001 |
| No | 73% | 90% | 91% |
Abbreviations: PA - Physical activity, p-value - Pearson Chi-square test.
Table 5.
Family medical history based on BMI classification.
| Variable | Class | Control (n=397) | Overweight (n=261) | Obese (n=597) | p-value |
|---|---|---|---|---|---|
| FMH Obesity/Overweight | Yes | 9% | 99% | 66% | < 0.001 |
| No | 91% | 1% | 34% | ||
| FMH Diabetes | Yes | 4% | 60% | 37% | < 0.001 |
| No | 96% | 40% | 63% | ||
| FMH Stroke | Yes | 0% | 19% | 23% | < 0.001 |
| No | 100% | 81% | 77% | ||
| FMH Hypertension | Yes | 4% | 49% | 56% | < 0.001 |
| No | 96% | 51% | 44% | ||
| FMH MI | Yes | 5% | 11% | 11% | < 0.001 |
| No | 95% | 89% | 89% |
Abbreviations: FMH - Family medical history, MI - myocardial infarction, p-value - Pearson Chi-square test.
Table 6.
Family medical history based on BFP classification.
| Variable | Class | Control (n=394) | Overweight (n=225) | Obese (n=542) | p-value |
|---|---|---|---|---|---|
| FMH Obesity/Overweight | Yes | 24% | 81% | 69% | < 0.001 |
| No | 76% | 19% | 31% | ||
| FMH Diabetes | Yes | 14% | 43% | 39% | < 0.001 |
| No | 86% | 57% | 61% | ||
| FMH Stroke | Yes | 4% | 16% | 23% | < 0.001 |
| No | 96% | 84% | 77% | ||
| FMH Hypertension | Yes | 10% | 48% | 55% | < 0.001 |
| No | 90% | 52% | 45% | ||
| FMH MI | Yes | 4% | 12% | 12% | < 0.001 |
| No | 96% | 88% | 88% |
Abbreviations: FMH - Family medical history, MI - myocardial infarction, p-value - Pearson Chi-square test.
Table 7.
Eating habits and preferences based on BMI classification.
| Variable | Class | Control (n=397) | Overweight (n=261) | Obese (n=597) | p-value |
|---|---|---|---|---|---|
| Craving | Yes | 1% | 41% | 91% | < 0.001 |
| No | 99% | 59% | 9% | ||
| Quickly/A lot | Yes | 1% | 82% | 91% | < 0.001 |
| No | 99% | 18% | 9% | ||
| Large portions | Yes | 1% | 94% | 94% | < 0.001 |
| No | 99% | 6% | 6% | ||
| Fast Food | Yes | 4% | 14% | 85% | < 0.001 |
| No | 96% | 86% | 15% | ||
| Not on table | Yes | 0% | 20% | 83% | < 0.001 |
| No | 100% | 80% | 17% | ||
| Desert | Yes | 29% | 37% | 87% | < 0.001 |
| No | 71% | 63% | 13% | ||
| After-meals | Yes | 1% | 23% | 95% | < 0.001 |
| No | 99% | 77% | 5% | ||
| Weekends | Yes | 3% | 18% | 18% | < 0.001 |
| No | 97% | 82% | 82% | ||
| Restaurant | Yes | 3% | 8% | 8% | 0.003 |
| No | 97% | 92% | 92% | ||
| Mindless | Yes | 0% | 83% | 96% | < 0.001 |
| No | 100% | 17% | 4% | ||
| Childhood like | Yes | 0% | 43% | 92% | < 0.001 |
| No | 100% | 57% | 8% | ||
| Cooked food | Yes | 74% | 17% | 16% | < 0.001 |
| No | 26% | 83% | 84% | ||
| 3 meals/day | Yes | 87% | 43% | 5% | < 0.001 |
| No | 13% | 57% | 95% | ||
| Breakfast | Yes | 90% | 44% | 3% | < 0.001 |
| No | 10% | 56% | 97% | ||
| 2 courses lunch | Yes | 1% | 57% | 63% | < 0.001 |
| No | 99% | 43% | 37% | ||
| Daily fruits | Yes | 66% | 11% | 7% | < 0.001 |
| No | 34% | 89% | 93% | ||
| Whole foods | Yes | 71% | 12% | 9% | < 0.001 |
| No | 29% | 88% | 91% |
Abbreviations: p-value - Pearson Chi-square.
Table 8.
Eating habits and preferences based on BFP classification.
| Variable | Class | Control (n=394) | Overweight (n=225) | Obese (n=542) | p-value |
|---|---|---|---|---|---|
| Craving | Yes | 7% | 52% | 87% | < 0.001 |
| No | 93% | 48% | 13% | ||
| Quickly/A lot | Yes | 13% | 80% | 90% | < 0.001 |
| No | 87% | 20% | 10% | ||
| Large portions | Yes | 15% | 87% | 93% | < 0.001 |
| No | 85% | 13% | 7% | ||
| Fast Food | Yes | 6% | 34% | 79% | < 0.001 |
| No | 94% | 66% | 21% | ||
| Not on table | Yes | 5% | 34% | 79% | < 0.001 |
| No | 95% | 66% | 21% | ||
| Desert | Yes | 33% | 47% | 82% | < 0.001 |
| No | 67% | 53% | 18% | ||
| After-meals | Yes | 6% | 46% | 87% | < 0.001 |
| No | 94% | 54% | 13% | ||
| Weekends | Yes | 5% | 16% | 18% | < 0.001 |
| No | 95% | 84% | 82% | ||
| Restaurant | Yes | 4% | 7% | 8% | 0.02 |
| No | 96% | 93% | 92% | ||
| Mindless | Yes | 14% | 81% | 94% | < 0.001 |
| No | 86% | 19% | 6% | ||
| Childhood like | Yes | 8% | 56% | 85% | < 0.001 |
| No | 92% | 44% | 15% | ||
| Cooked food | Yes | 64% | 22% | 19% | < 0.001 |
| No | 26% | 78% | 81% | ||
| 3 meals/day | Yes | 76% | 34% | 11% | < 0.001 |
| No | 24% | 66% | 89% | ||
| Breakfast | Yes | 80% | 34% | 8% | < 0.001 |
| No | 20% | 66% | 92% | ||
| 2 courses lunch | Yes | 11% | 55% | 61% | < 0.001 |
| No | 89% | 45% | 39% | ||
| Daily fruits | Yes | 57% | 13% | 7% | < 0.001 |
| No | 43% | 87% | 93% | ||
| Whole foods | Yes | 61% | 14% | 11% | < 0.001 |
| No | 39% | 86% | 89% |
Abbreviations: p-value - Pearson Chi-square.
Table 9.
Psychological and emotional factors based on BMI classification.
| Variable | Class | Control (n=397) | Overweight (n=261) | Obese (n=597) | p-value |
|---|---|---|---|---|---|
| Stress | Yes | 0% | 20% | 94% | < 0.001 |
| No | 100% | 80% | 6% | ||
| Fatigue | Yes | 1% | 8% | 64% | < 0.001 |
| No | 99% | 92% | 36% | ||
| Nibbling | Yes | 1% | 54% | 91% | < 0.001 |
| No | 99% | 46% | 9% | ||
| Boredom | Yes | 1% | 17% | 44% | < 0.001 |
| No | 99% | 83% | 56% | ||
| Compulsive | Yes | 0% | 30% | 92% | < 0.001 |
| No | 100% | 70% | 8% | ||
| Reward | Yes | 0% | 36% | 79% | < 0.001 |
| No | 100% | 64% | 21% | ||
| Pleasure | Yes | 0% | 58% | 44% | < 0.001 |
| No | 100% | 42% | 56% | ||
| Loneliness | Yes | 0% | 3% | 58% | < 0.001 |
| No | 100% | 97% | 42% | ||
| Socially | Yes | 1% | 13% | 12% | < 0.001 |
| No | 99% | 87% | 88% | ||
| Anger/upset | Yes | 0% | 85% | 90% | < 0.001 |
| No | 100% | 15% | 10% | ||
| Major issues | Yes | 0% | 4% | 87% | < 0.001 |
| No | 100% | 96% | 13% |
Abbreviations: p-value - Pearson Chi-square.
Table 10.
Psychological and emotional factors based on BFP classification.
| Variable | Class | Control (n=394) | Overweight (n=225) | Obese (n=542) | p-value |
|---|---|---|---|---|---|
| Stress | Yes | 5% | 44% | 86% | < 0.001 |
| No | 95% | 56% | 14% | ||
| Fatigue | Yes | 4% | 31% | 56% | < 0.001 |
| No | 96% | 69% | 44% | ||
| Nibbling | Yes | 10% | 62% | 86% | < 0.001 |
| No | 90% | 38% | 14% | ||
| Boredom | Yes | 3% | 16% | 44% | < 0.001 |
| No | 97% | 84% | 56% | ||
| Compulsive | Yes | 6% | 47% | 86% | < 0.001 |
| No | 94% | 53% | 14% | ||
| Reward | Yes | 7% | 42% | 76% | < 0.001 |
| No | 93% | 58% | 24% | ||
| Pleasure | Yes | 10% | 41% | 47% | < 0.001 |
| No | 90% | 59% | 53% | ||
| Loneliness | Yes | 2% | 24% | 50% | < 0.001 |
| No | 98% | 76% | 50% | ||
| Socially | Yes | 2% | 12% | 12% | < 0.001 |
| No | 98% | 88% | 88% | ||
| Anger/upset | Yes | 14% | 79% | 89% | < 0.001 |
| No | 86% | 21% | 11% | ||
| Major issues | Yes | 3% | 29% | 78% | < 0.001 |
| No | 97% | 71% | 22% |
Abbreviations: p-value - Pearson Chi-square.
Table 11.
Specific conditions and health issues based on BMI classification.
| Variable | Class | Control (n=397) | Overweight (n=261) | Obese (n=597) | p-value |
|---|---|---|---|---|---|
| Food intolerance | Yes | 5% | 2% | 3% | 0.02 |
| No | 95% | 98% | 97% | ||
| PMS | Yes | 0% | 14% | 11% | < 0.001 |
| No | 100% | 86% | 89% | ||
| Weight gain after quit smoking | Yes | 0% | 3% | 3% | 0.005 |
| No | 100% | 97% | 97% | ||
| Oral contraceptives | Yes | 2% | 7% | 4% | 0.004 |
| No | 98% | 93% | 96% | ||
| Menopause | Yes | 8% | 3% | 13% | < 0.001 |
| No | 92% | 97% | 87% | ||
| Preclimax | Yes | 1% | 5% | 7% | < 0.001 |
| No | 99% | 95% | 93% | ||
| PCOS | Yes | 0% | 3% | 3% | 0.005 |
| No | 100% | 97% | 97% | ||
| Prediabetes | Yes | 0% | 1% | 8% | < 0.001 |
| No | 100% | 99% | 92% | ||
| Dyslipidemia | Yes | 0% | 5% | 77% | < 0.001 |
| No | 100% | 95% | 23% | ||
| Arterial hypertension | Yes | 1% | 5% | 18% | < 0.001 |
| No | 99% | 95% | 82% | ||
| History of weight loss | Yes | 2% | 36% | 40% | < 0.001 |
| No | 98% | 64% | 60% | ||
| Gout | Yes | 0% | 0% | 4% | < 0.001 |
| No | 100% | 100% | 96% | ||
| Metabolic syndrome | Yes | 0% | 3% | 88% | < 0.001 |
| No | 100% | 97% | 12% | ||
| Post-insulin therapy weight gain | Yes | 0% | 0% | 1% | 0.19 |
| No | 100% | 100% | 99% | ||
| Postpartum | Yes | 0% | 5% | 5% | < 0.001 |
| No | 100% | 95% | 95% | ||
| Post-metabolic surgery | Yes | 0% | 0% | 0% | 0.15 |
| No | 100% | 100% | 100% |
Abbreviations: PMS - Premenstrual syndrome, PCOS - polycystic ovarian syndrome, p-value - Pearson Chi-square.
Table 12.
Specific conditions and health issues based on BFP classification.
| Variable | Class | Control (n=394) | Overweight (n=225) | Obese (n=542) | p-value |
|---|---|---|---|---|---|
| Food intolerance | Yes | 3% | 2% | 4% | 0.33 |
| No | 97% | 98% | 96% | ||
| PMS | Yes | 3% | 12% | 11% | < 0.001 |
| No | 97% | 88% | 89% | ||
| Weight gain after quit smoking | Yes | 0% | 3% | 3% | 0.004 |
| No | 100% | 97% | 97% | ||
| Oral contraceptives | Yes | 2% | 7% | 4% | 0.004 |
| No | 98% | 93% | 96% | ||
| Menopause | Yes | 8% | 9% | 12% | 0.15 |
| No | 92% | 91% | 88% | ||
| Preclimax | Yes | 1% | 8% | 6% | < 0.001 |
| No | 99% | 92% | 94% | ||
| PCOS | Yes | 1% | 4% | 3% | 0.04 |
| No | 99% | 96% | 97% | ||
| Prediabetes | Yes | 0% | 2% | 8% | < 0.001 |
| No | 100% | 98% | 92% | ||
| Dyslipidemia | Yes | 2% | 34% | 67% | < 0.001 |
| No | 98% | 66% | 33% | ||
| Arterial hypertension | Yes | 2% | 9% | 18% | < 0.001 |
| No | 98% | 91% | 82% | ||
| History of weight loss | Yes | 8% | 40% | 37% | < 0.001 |
| No | 92% | 60% | 63% | ||
| Gout | Yes | 0% | 2% | 3% | 0.006 |
| No | 100% | 98% | 97% | ||
| Metabolic syndrome | Yes | 2% | 32% | 79% | < 0.001 |
| No | 98% | 68% | 21% | ||
| Post-insulin therapy weight gain | Yes | 0% | 0% | 1% | 0.18 |
| No | 100% | 100% | 99% | ||
| Postpartum | Yes | 1% | 6% | 4% | 0.002 |
| No | 99% | 94% | 96% | ||
| Post-metabolic surgery | Yes | 0% | 0% | 0% | 0.38 |
| No | 100% | 100% | 100% |
Abbreviations: PMS - Premenstrual syndrome, PCOS - polycystic ovarian syndrome, p-value - Pearson Chi-square.
Table 13.
Obesity risk factors based on BMI model.
| Risk Factors | Odds Ratio | 95% CI | p-value |
|---|---|---|---|
| Age | 1.08 | 1.03 – 1.13 | 0.004 |
| Hydration status | 0.84 | 0.75 – 0.92 | <0.001 |
| FMH Diabetes [Yes] | 0.33 | 0.11 – 0.87 | 0.032 |
| Craving [Yes] | 17.08 | 4.82 – 68.55 | <0.001 |
| Fatigue [Yes] | 16.90 | 5.20 – 64.03 | <0.001 |
| Stress [Yes] | 42.07 | 12.70 – 172.12 | <0.001 |
| Nibbling [Yes] | 4.37 | 1.19 – 17.04 | 0.029 |
| Compulsive [Yes] | 32.93 | 10.16 – 128.04 | <0.001 |
| Quickly/A lot [Yes] | 0.18 | 0.04 – 0.76 | 0.025 |
| Large portions [Yes] | 0.06 | 0.01 – 0.40 | 0.005 |
| Fast food [Yes] | 10.20 | 3.54 – 31.95 | <0.001 |
| After meals [Yes] | 26.98 | 8.29 – 106.49 | <0.001 |
| Restaurant [Yes] | 0.12 | 0.03 – 0.49 | 0.003 |
| Anger/Upset [Yes] | 0.14 | 0.03 – 0.53 | 0.006 |
| PMS [Yes] | 0.10 | 0.03 – 0.38 | 0.001 |
| Other devices [Yes] | 0.15 | 0.03 – 0.79 | 0.024 |
| R2 Nagelkerke = 0.959 | |||
Abbreviations: PMS - premenstrual syndrome, CI - confidence interval, p-value - Wald test.
Table 14.
Obesity risk factors based on BFP model.
| Risk Factors | Odds Ratio | CI | p-value |
|---|---|---|---|
| BMI | 1.09 | 1.03 – 1.18 | 0.007 |
| Muscular tissue | 0.68 | 0.62 – 0.75 | <0.001 |
| BMR | 1.01 | 1.00 – 1.01 | <0.001 |
| Hydration status | 0.86 | 0.77 – 0.95 | 0.005 |
| FMH Diabetes [Yes] | 1.66 | 1.01 – 2.76 | 0.046 |
| Pleasure [Yes] | 1.78 | 1.06 – 3.03 | 0.031 |
| Quickly/A lot [Yes] | 0.39 | 0.16 – 0.91 | 0.032 |
| Anger/Upset [Yes] | 2.72 | 1.22 – 6.10 | 0.015 |
| PMS [Yes] | 0.38 | 0.17 – 0.83 | 0.017 |
| TV [Yes] | 2.28 | 1.26 – 4.13 | 0.006 |
| Daily fruits [Yes] | 0.26 | 0.12 – 0.55 | <0.001 |
| Alcohol [Yes] | 1.98 | 1.11 – 3.57 | 0.022 |
| Smoking [Yes] | 4.97 | 2.09 – 12.36 | <0.001 |
| Menopause [Yes] | 0.16 | 0.07 – 0.35 | <0.001 |
| Preclimax [Yes] | 0.18 | 0.06 – 0.51 | 0.001 |
| History of weight loss [Yes] | 0.47 | 0.28 – 0.78 | 0.004 |
| 30 mins PA/day | 3.33 | 1.67 – 6.84 | 0.001 |
| R2 Nagelkerke = 0.831 | |||
Abbreviations: PMS - premenstrual syndrome, BMI - Body Mass Index, BMR - Basal Metabolic Rate, PA - Physical activity, CI - confidence interval, p-value - Wald test.
Table 15.
Comparison between BMI and BFP models.
| Model | AUC | 95% CI | Accuracy | Specificity | Sensitivity |
|---|---|---|---|---|---|
| BMI | 0.998 | 0.996 - 0.999 | 0.983 | 0.985 | 0.982 |
| BFP | 0.975 | 0.967 - 0.982 | 0.922 | 0.937 | 0.904 |
Abbreviations: BMI - Body Mass Index, BFP - Body Fat Percentage, AUC - Area under Roc curve, CI - confidence interval.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



