Submitted:
10 October 2024
Posted:
11 October 2024
You are already at the latest version
Abstract
Background: Rabies, a zoonotic disease caused by the Lyssavirus genus, is widely distributed and a significant cause of human death in Africa and Asia. This study aimed to investigate human rabies exposure and associated risk factors in Northwest Ethiopia. Methods: The study encompassed four zones, seven districts, and four kebeles from each district. The research team developed a questionnaire for data collection. Results: A total of 642 households were interviewed. The present study highlighted an exposure to rabies of 10.47%.”. Over 98% of residents displayed a strong understanding of rabies, with 99.69% correctly identifying rabies as a zoonotic disease. However, 80.22% of the interviewees believed that traditional medicine can treat the disease. Only 21.93% of victims were subjected to post-exposure prophylaxis. More than 87% of exposed residents were affected by the dogs. Of that, 48.70% were bitten by their own dogs. Metema district had the highest risk of exposure (p < 0.001) compared to the other six that were investigated. Dog ownership (p<0.05) and a higher number of households (p<0.01) were also identified as risk factors for rabies exposure. Conclusion: Residence, low education levels, high household density, free-roaming dogs, and dog ownership are key risk factors for rabies exposure. Public health awareness campaigns are crucial to emphasize the risks associated with animal bites.
Keywords:
Dog-bite
; Epidemiology
; Ethiopia
; exposure
; human rabies
; Risk factor
INTRODUCTION
Rabies is caused by rabies virus of the genus Lyssavirus, family Rhabdoviridae and order Mononegavirales that can cause fatal infection in all warm-blooded mammals. Primarily, it attacks the nervous system and salivary glands, and it is shed in saliva [1, 2]. The virus is 100% fatal once clinical signs appear. Rabies is a widespread zoonotic disease causing a significant social and economic burden in many countries [3].
Rabies virus is transmitted mainly by the bite of rabid dogs. This virus can also be transmitted through direct contact of fresh wounds or intact mucosal surfaces (eyes, nose) with infectious saliva or by licks of rabid animals, and transdermal scratches contaminated with infectious material [4,5].
After virus replication inside the bitten muscle tissue and travels from a point of bite to the brain via the nerve cells [6]. Once the virus reaches the nervous system, it can manifest either of two forms: “dumb rabies” which results in paralysis of the affected one or the more common “furious rabies” which shows the clinical manifestation of excessive saliva production and in most cases, hydrophobia [7]. The entrance of the virus inside tissues of the brain leads to death by causing respiratory dysfunction and secondary metabolic and circulatory defects [8].
Rabies disproportionally affects the poorest and under-resourced populations living in low- and middle-income countries, and its incidence is increasing in several countries. In addition to its negative impact on mortality, rabies also causes a negative economic impact in already impoverished populations The possible risk factors associated with the developing of rabies in humans are many; however, lower age is considered as a main risk factor in developing rabies, however, lower age is considered as a main risk factor in developing rabies ([9, 10]. Occupational differences and level of education are additional known risk factors for rabies. Poor management of wounds and poor adherence to post-exposure prophylaxis are also associated with a higher risk of developing human rabies [10].
Epidemiologically, rabies is widely distributed and causes numerous human deaths in the world especially, in Africa and Asia. It is a public health threat to these regions [11,12]. More than 95% of all deaths associated with rabies happen in these continents. The disease kills the lives of 24,000 people in Africa annually [13]. Rural communities are especially impacted by rabies outbreaks, through the combination of limited access to health care and the threat to their livelihoods through rabies attacks on livestock [3,14].
Ethiopia has had a high rabies burden among African countries concerning human rabies virus exposure since the early 17th century [15, 16]. The Ethiopian Health and Nutrition Research Institute, the current Ethiopian Public Health Institute, indicated that human rabies was reported in Ethiopia in 1903 for the first time [17]. A national surveillance data conducted from 2007 until 2012 showed 15,178 exposure cases and 272 fatal cases with more than 88% of the exposure cases being dog bites [15]. Most of the exposed individuals (59.2%) were males. The majority of the exposure cases (98.9%) were from Addis Ababa, Oromia, Amhara, Southern Nations, Nationalities, and Peoples' Region (SNNPR), and Tigray regions. Nowadays, in Ethiopia, approximately 97,000 people are exposed to rabies annually with approximately 3,000 deaths [18]. Despite this information, accurate data regarding the annual number of rabies cases is not available. One of the biggest obstacles to developing effective rabies control policies and strategies is the absence of trustworthy data on the frequency of dog bites and the risk factors associated with human exposure to rabies. Therefore, this study aims to estimate the incidence of rabies exposure and identify associated risk factors and access to post-exposure prophylaxis in humans in North West Ethiopia.
2. Materials and Methods
2.1. Description of the study area
Amhara region is located between 8°45'N and 13°45' N latitude and 35° 46' and 40° 25' E longitude with about 170,000 square kilo-meters of land area in the northwestern part of Ethiopia [19]. The region is known for its diversified topography, climatic conditions, agro ecology and animal population. Regarding the climatic condition of the Amhara region, 31% of the region with an altitude of 1500 m.a.s.l. is categorized as Kola (hot zone) 44% of the region with an altitude of 1500-2500 m.a.s.l is classified as Woyina Dega (warm zone) and 25% with an elevation of 2500-4620 m.a.s.l is classified as Dega (cold zone) [20].
The mean annual temperature of the region is between 15 °C and 21 °C, while in the valleys and marginal areas the temperature exceeds 27 °C. Relatively high temperatures are observed in some valleys and the marginal regions exhibiting arid climates. There are two distinct seasons, a short rainy season lasting three to four months and a long dry season of eight to nine months [21].
The total human population of the region is estimated at around 22,877,365 of which about 88% are rural, and the rest 12% are urban dwellers.[19]. From which the study area has a total population of 5,464,079 humans, 5,474,545 cattle; 2,484,400 sheep; 2,461,942 goats; 44,860 horses, 847,780 donkeys and 6,609 dogs respectively [22, ]. The current study was conducted in four zones of Gondar. From these zones, we selected seven districts (East Dembia and Tach Armachiho from Central Gondar, Genda wuha and Metema from West Gondar, Fogera and Debre Tabor from South Gondar and Debark from North Gondar zones) of Amhara region, northwest Ethiopia (Figure 1).
2.2. Study population
The study populations were total human populations in the Central, West, North, and South Gondar zones of the Amhara region, northwest Ethiopia.
2.3. Sampling methods
Three-stage cluster sampling technique was used to select sampling units. First, the four zones of Gondar were selected purposively because rabies is common in these zones. Then districts or towns that we think are representative of the zones were selected: East Dembia and Tach Armachiho from Central, Debark from North, Metema and Genda-wuha from West and Debre Tabor and Fogera from South Gondar zones. Finally, four kebeles were randomly selected from each district making a total of 28 kebeles [23, 24].
2.4. Design of the questionnaire and data collection
A survey questionnaire was developed using the literature and our own experience. The questionnaire aimed to collect data on the occurrence and/or exposure of rabies, associated risk factors for exposure, and post-exposure treatment in the human population. The checklist in the questionnaire had three categories. 1) about the demography of participants: such as “age, gender, religion, educational level, and family size”; 2) about knowledge and management of dogs related to rabies such as “knowledge of rabies infection, rabies vaccination history, awareness of post-exposure vaccination, and understanding of the rabies virus (disease awareness, transmission to humans, and dog symptoms)” and 3) “about previous dog bite exposure”.
The original questionnaire was prepared in English and then it was later translated into the local language (Amharic). The translated questionnaires were then back-translated into English to check consistency. The English version of the questionnaire is attached as a supplementary file (Supplementary File 1). Face-to-face interviews were administered in the final questionnaire. Data was collected by asking respondents whether they had rabies exposure in one or more of their family members in the last two years.
2.5. Sample size determination
Multistage cluster sampling was used to select study participants. The sample size was determined using the sample size estimation formula for random sampling in an infinite population from Thrusfield [25].
Where:
n= number of the household
P =proportion of the population taken as 50% since it is unknown in the study area
d2= desired level of precision (margin of error) taken as 5%
D= design effect
Based on these assumptions, a sample of 385 households was required. However, the actual sampling method used was multistage cluster sampling. Therefore, the sample size was adjusted using the following formula .
Where:
b= the number of household responses at least one from the cluster
ICC= intra correlation coefficient
D =design effect
Design effect (D) accounts for the loss of precision in cluster surveys. It's calculated using the predetermined cluster size (28 kebeles) and the number of households selected per cluster; i. e. 23. In multistage cluster surveys, ICC reflects variability across all sampling stages. We used an ICC value of around 0.03 [26]. Considering these factors, the design effect for this sample size determination was calculated to be 1.67. This resulted in a final estimated sample size of 642 households.
2.6. Data analysis
The data were entered into Microsoft Excel. Completeness of the data was checked, followed by calculations of descriptive statistics such as percentages and rates. Risk factor analysis was conducted using binary logistic regression models. Univariable analysis was performed first, followed by pairwise correlation for variables significantly associated with the univariable analysis. Multivariable logistic regression models were then performed to identify factors associated with rabies exposure. Model building considered statistically significant variables (p < 0.05) in the univariable analysis. Any variables with a p-value ≤ 0.05 were considered significant in the final model. The Hosmer-Lemeshow test was used to assess the model's goodness of fit. This test evaluated the overall fit of the final logistic regression model. The presence of confounding was checked by adding one variable at a time in the model-building process. The presence of interactions was checked for variables that remained in the final model. Findings were presented with odds ratios (ORs), 95% confidence intervals (CIs), and p-values. Stata release 17 (Stata Corp LP, USA) was used for the statistical analysis
3. Results
3.1. Respondents’ awareness and management of rabies
A total of 642 respondents were interviewed in the survey. Majorities (94% to 99%) of respondents are aware rabies exists, is a zoonotic disease, and has one or more transmission methods of rabies. However, only a small proportion of them implement control measures such as vaccinating their dogs (41%) and taking post-exposure prophylaxis (23%). Table 2 summarizes the demography of respondents and their awareness and management of rabies.
3.2. Prevalence of rabies exposure and associated risk factors
The incidence of rabies exposure was 10.47%. Rabies exposure had shown large variability between districts, zones, respondents’ level of education and family size, and between respondents who owned and didn’t own dogs. The level of rabies exposure is illustrated in Table 3.
3.3. Sources of rabies exposure
The result showed that 87.73% of the victims were bitten by dog and 11.52% were bitten by equines (donkeys). In the case of ownership of the source animals, 48.70% were exposed by their animals (dogs and donkeys), while 26.39% were exposed by stray dogs, and the rest 24.91% were exposed by neighbors’ animals. Measures taken by respondents after rabies exposure 42.37 % of 269 victims washed the wound using plain water, 36.02% washed using water and soap, 12.29% applied other materials (antiseptics, benzene, kerosene, etc.) and 9.32% applied holy water (Table 4).
3.4. Risk factors associated with rabies exposure.
Twelve variables were tested for statistical association with rabies exposure. Nine of them were statistically significantly associated (P<0.05) with rabies exposure. Variables; like high educational background, being female and vaccinating their dogs reduce rabies exposure while high family size, presence of free contact of the dog, presence of a dog in the house and low level of education increased rabies exposure. The details of univariable associations of rabies exposure and risk factors are summarized in Table 5.
3.5. Multivariate logistic regression model for risk association of rabies exposure
The stepwise multivariate logistic regression model of rabies exposure removes the variables which were not statistically significant (p > 0.05). The multivariable regression analysis demonstrated that the variables ‘district difference, ‘family size’ and ‘dog ownership’ were strongly associated with rabies exposure in humans. In the final logistic regression model analysis only three were significant (P<0.05) from twelve variable i.e., residence(districts) family size, and dog ownership were all significantly associated with exposure of rabies in human. The logistic regression model exhibited a good overall fit (Hosmer and Lemeshow Chi-square value 43.76, P=0.064) (Table 6).
Discussion
In this study, a number of factors associated with dog bites and risky behaviour were investigated in conjunction with assessing the interviewee's knowledge about safe dog interaction. Regarding the interviewees, more than 98% of the respondents very well knew the rabies disease, 99.69% answered that rabies is a zoonotic disease and 94% knew the transmission method of rabies. The result was supported by the previous study of Ntampaka et al. [27] They stated that 85% of the respondents very well knew rabies and how rabies can be transmitted between dogs and other animals (bites, licking wounds and skin scratches). Bahiru et al [28] stated that 98.4% of the respondents had a good understanding of the transmission of rabies. In this study, more than 93% of the respondents answered that the presence of a dog in the house is one of the factors contributing to rabies infection. Similar results were reported in Tanzania [29]. They were reported, that most suspected rabies exposures were due to domestic animals (89%), particularly dogs. Eighty-point twenty-two percent of the respondents believed traditional medicaments could treat rabies, whereas the rest, 19.88%, did not believe traditional drugs could treat rabies or didn't know about traditional medicine. Regarding the vaccination history, 41.28% of the households answered that they had vaccinated their dogs, while 58.72% of the respondents had no idea about the vaccine or were not vaccinated due to a lack of vaccine near their area. In this study, 21.93% of exposed people took PEP after exposure, while 78.07% were either treated by a traditional healer or left as it is. This result is also similar to previous reports from different parts of Ethiopia [30, 16]. Underreporting of rabies exposure in Ethiopia primarily occurs due to the deep relationship of the traditional practice of treating rabies by healers, which as such interferes with assessing the real magnitude of the disease [30]. The other authors also found that about half of the bite victims they contacted in rural areas did not report to health centres but visited traditional or spiritual healers [6]. This showed that lack of awareness or limited knowledge about PEP and low accessibility of the PEP may be one of the factors contributing to the low number of people using PEP. In addition to low awareness, economic background was also one of the bottleneck factors, especially for rural victims [31; 3].
More than 58% of dog owners were releasing their dogs freely during the day and night time while the rest were kept indoors or released at night time. This was had a chance to contact with any dog, as well as wild carnivores. This showed that more susceptible dogs were freely contacted by infected stray dogs. Therefore, roaming dogs are ideal for transmission of the rabies virus between dogs and to other species [32, 33]. In the current study, 3.12% of dog owners answered that they castrated or spayed their dogs. The result showed that one of the failures of WHO strategies [33] was that birth controls were adopted as one of the strategies for reducing and controlling rabies. Therefore, movement control and birth control are the main strategies to reduce rabies [34,31].
Regarding dog ownership, 77.41% of the interviewees had one or more dogs in their house. The results indicated that the relationship dog-human connection is stronger in the area. Out of this number, 71.91% of them had one or more rabies exposures. Due to this, the author stated that if there is a stronger attachment, the chance of getting bitten by rabid animals (bitten by dogs) might be higher when compared to non-dog owners. This is why the results revealed that 48.70% of the exposures were caused by their own dogs. The likelihood of being bitten by a family dog among dog - owners was higher than among children who reported not having no dogs in their household. Naturally, children with dogs in their household are more exposed to dogs, so the chances of getting bitten dramatically increase [35].
In this study, the prevalence of rabies exposure was 10.47%. The results were recorded as rabies exposure (either the household owner or his or her family were exposed) to rabid animals for the past two years. This result is almost similar to the previous results of [18] (10.1%) and Jemberu et al. [37] (12.1%) in different parts of Ethiopia [38]. In terms of zonal distribution, the west Gondar zone was the first exposed (50.19%) area in the current study, and the result showed a statistically highly significant (P<0.001) difference among the zones. This might be due to the way of living together, the clustered settlement of villagers, and the attachment of the farmer with a dog to have close connections, resulting in the rapid spread and persistence of infection in the area. Regarding the district distribution of victims, the highest records were found to be at Metema (58.49%), Genda wuha (58.33%), and Tach Armachiho (49.07%), respectively, whereas the lowest was recorded in Debre Tabor town (15.07%). This result showed that more exposure was found in districts or towns that were away from the center. This may be due to a lack of enough amount of vaccine or because it is unavailable because of its distance from the vaccine centre. Even though dog-human attachments are close to this area, dogs are important when farmers go to the farming area for ploughing and seeking pasture for their animals to use as guards from wild predators [38]. But, during data collection, we observed free-roaming dogs in the area because most of the respondents could not feed their dogs; so, dogs moved freely to find their feed. So, free-roaming dogs may be provided with opportunities for infected dogs to transmit the virus to susceptible dogs and then to humans. Previously, the authors stated that the movement of free-roaming dogs may have been responsible for the spread of the disease and spillover infection to the community [39,31].
In terms of sex, males were exposed more than females' respondents. Similar results were stated for males (54%) and females (46%) [40]. Regarding family size (i.e., more household members), they were affected or exposed more. However, respondents who have fewer family members were recorded as having fewer victims than those with more family members. The result shows a statistically significant difference (p<0.05) among family size groups. These results showed that if more family is found in the house, it is true that more children may be found. Salomão et al. [10] stated that if more children were found in the house, there might have been a high risk for bites [41] and the presence of children in a household increased the probability of a dog bite incident [42]. In the case of educational background, non-educated interviewees were more victims (50.70%), either themselves or their families, than educated ones. The results were statistically highly significant (p< 0.001) among the educational background groups. This result showed that there may be an awareness difference between the groups because most educated people are taking care of their free-roaming dogs, or they may be vaccinating their dogs regularly. Non-educated people lived in rural areas, which might indicate the presence of a possible intimate relationship between farmers and their dogs. In addition to living behavior, there was also an awareness difference between educated and non-educated persons about rabies risk (3, 43]. This finding was also similar to other scholarly reports that stated that rural and urban communities have different awareness about rabies. Rural areas far from the treatment centres could potentially have a higher incidence of rabies-associated death, which may increase their level of awareness and is additionally worthy of consideration. Voupawoe et al. [44] stated that the majority occur in rural communities in Asia (60%) and Africa (36%).
Similarly, in relation to dog ownership, 71.75% of the victims were dog owners, while 28.25% were non-dog owners. The results showed a statistically significant (p< 0.01) difference between dog owners and non-dog owners. Evangelio et al. [40] who stated the biting incidence involved with owned dogs was 98.1%, and the remaining 1.9% involved stray dogs. Seligsohn et al. [34] also stated that a majority of the children (55.9%) had been bitten by a family dog, 42.7% had been bitten by a stray dog, and the remaining 1.5% reported they had been bitten by both a family dog and a stray dog [44].
In terms of the source of the infection, 87.73% of the victims were bitten by dogs and 11.52% by equines (donkeys). The result was similar to that of Shwiff et al. [45], who reported that canine rabies is the biggest source of both human and livestock infections in the developing countries of Asia, Latin America and Africa [46]. It was also agreed with the past report in Asia and Africa, where dogs are responsible for 85%–95% of bites [47,48, 49] In the case of ownership of the source animals, 48.70% were bitten by their own animals, while 26.39% were stray dogs, and the rest, 24.91%, by the neighbors’ dogs. This result is supported by Seligsohn [35] in Tamil Nadu, India. The likelihood of being bitten by a family dog among dog owners was higher than among those who have no dogs in their household. Regarding the immediate action to be taken after a bite if they suspected it to be rabid, respondents had different practices, of 42.37% of victims used plain water to wash the wound, 36.02% washed using water and soap, 12.29% used to pour other materials (antiseptics, benzene, kerosene, etc.), and 9.32% poured holly water. This type of practice was also performed in Namibia, Omusati region [49], where they stated that 41% of the respondents carried out good practices such as washing the wound with soap and water before seeking medical attention after the bite.
In this study, 98.19% of dog owners used dogs as a guard. The result supported by Kanutus et al., [49] is that 95% of the respondents keep dogs as guards. Regarding the feeding and keeping system of the dog, 52.53% of dog owners did not tie their dogs totally, whereas 47.47% tied their dogs either at night or daytime only. Regarding the feeding system, 59.76% of dog owners were given a feed, and 38.63% of dogs were getting feed from both roaming and hand feeding systems. These might aid in acquiring infections such as rabies when they roam around to search for feed and facilitate disease transmission. Tintinalli and Stapczynski, [50] stated that stray dogs account for about 99% of dog-transmitted rabies in countries where dogs are the main mode of rabies transmission [51].
The univariable logistic regression showed that people who lived in Matema district were more likely to get sick (OR = 7.94, 95% CI= 3.89-16.23) (Table 5). According to this result, residence distance from the center was one of the risk factors for getting more victims than nearby districts. It may have been that the relationship between dogs and humans and the number of dog populations in the area were the main factors. This indicated that increased incidences due to dog population densities and the absence of a sustained vaccination program resulted in the maintenance of rabies endemicity in the area, as we observed [52]. Based on sex differences, females had a relatively lower risk than males. But the odd ratio was not significant (OR = 0.96, 95% CI= 0.673-1.363 at p > 0.05). As for educational status, there was a statistically significant difference among educational groups. The tertiary level showed (62%) less risk than the Secondary level (p< 0.01, 95% CI= 0.21-0.70), whereas the secondary had (60%) less risk than the basic and non-educated one at (p<0.001, 95% CI= 0.23-0.68). This might be due to having better awareness of the educated person (as the level of education increases, levels of awareness also increase) than the non-educated. The results were in line with Yalemebrat et al. [53] who stated that 51.1% of the illiterates, 69.0% of secondary school preparatory students, and 91.3% of the Diploma and above education level students had good knowledge in a study conducted in Debark district of North Gondar, Ethiopia. Hence, if the level of education is increased, the risk of being affected by rabies may decrease. Since knowledgeable individuals would have easier access to information, be able to comprehend the illness and be able to defend themselves against stray dogs and needless interactions with dogs which are not vaccinated [54,53].
Concerning dog ownership, the presence of dogs in the house was 58% more risky than a household living without dogs. The possible explanation could be that dog owners have more attachment to their dogs, children with greater possibility. In the current study about the number of households, if they had more family members. Households having more than 7 members were found to be at greater risk than households having 4-6 family members than households that had less than 3 family members (Table 4). This may be due to the presence of more children in the house. Increased dog bite incidents in children are considered a behavioural risk because of their extreme curiosity, lack of inhibition, limited knowledge and experience about dog behavior, and inability to protect themselves from an attack [55, 56, 31].
In multivariate logistic regression of rabies exposure, the variables were not statistically significant (p >0.05). The multivariable regression analysis demonstrated that the variables ‘district', ‘family size’, ‘educational status’, ‘dog ownership,' and ‘free contact with the dog’ were strongly associated with rabies exposure in humans. The final logistic regression analysis showed that residence (districts) (OR = 7.676, p <0.001), family size (OR=2.225, p <0.001), and dog ownership (OR = 0.591, p <0.05) were associated with exposure to rabies in humans. (Table 6). The model showed that the presence of more family in the house and the presence of a dog in the house had a strong association with rabies exposure. These show that the presence of more families in the house means the presence of more children in the house. This indicates an increase in rabies exposure in humans because children (especially those less than 15 years old) are more exposed to rabies than adults and old [57]. Evangelio et al. [40] Stated that they observed in the data that the percentage of severe rabies exposure is highest in the age group 5–15 years. In the case of dog ownership, most exposed people were bitten by their dogs because of their close attachments to their dogs. In multivariate logistic regression, people living away from the centre districts had a strong association with rabies exposure. For people living away from the centre access to healthcare services may be limited. This can result in delays in receiving post-exposure prophylaxis (PEP) after a potential rabies exposure, increasing the risk of developing the disease. Remote regions may have less effective animal control measures, leading to higher populations of stray or unvaccinated domestic animals. These animals can also transmit rabies to humans.
Conclusions and Recommendations
In conclusion, the current study indicates rabies is still the basic human killer disease in the area. The residence difference, low level of educational background, presence of a high number of households, free movement of dogs and being dog owners were the main risk factors for rabies exposure. The data of surveillance showed that communities who live in the study area are still tilted to traditional medicaments rather than post-exposure prophylaxis. Overall, while rabies is a global concern, its impact can be more pronounced in remote areas due to the interplay of wildlife interactions, healthcare accessibility, and community practices. Public health efforts in these regions often focus on vaccination programs for pets, education about rabies prevention, and improving access to medical care.
- ➢
- Regarding, the above conclusion, we recommended the following suggestion for further study as well as prevention of rabies.
- ➢
- Public educational programs on dog behavior, dog-child interaction, and the importance of responsible dog ownership, especially reduction of free contact of the dogs.
- ➢
- Teaching the communities about the importance of the vaccine raising awareness about dog vaccination and improving access and affordability of the vaccine
- ➢
- Both the local government and the federal government take action for the availability of the dog vaccine for the especially inaccessible districts.
- ➢
- The disease is a continuing high community hazard in the study area; therefore, rabies needs continuous surveillance of dog bites to detect trends and evaluate the effect of prevention efforts.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas, took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
There is no external funding to report.
Ethical Approval and Consent to Participate
The study protocol and consent procedure were approved by the Institutional Ethical Review Board (IERB) of the University of Gondar. The research project entitled “Epidemiology, Public Health and economic burden of Rabies in North-West Ethiopia” has been reviewed by the IERB of the University of Gondar for its Ethical soundness, and it is found to be ethically acceptable. Thus, the Research and Technology Transfer Vic President Office has awarded this Ethical Clearance for the above-mentioned study to be reported by Mr. Workneh Wondimagegn as the Principal Investigator and Dr. Sefinew Alemu, Professor Wudu Temesgen as a co-investigator, as of July 8, 2022 (Ref. No VP/RTT/05/1037/2022, July 27, 2022).
Informed Consent
Informed verbal consent was obtained from the respondents before the start of the interview. All the respondents were approached verbally and agreed to participate in the interview without any payment. Data were analyzed and reported anonymously (agreement written in the beginning of the questionnaire. We proceeded after the participant gave permission).
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Acknowledgments
The authors thank the University of Gondar for providing logistical and administrative support during the field visits and incidence follow-up. We also thank the entire district livestock office heads and vet professionals for their support and helpfulness during data collection and fieldwork.
Conflict Interest
The authors report no conflicts of interest in this work.
References
- 1. Hayman DT, Johnson N, Horton DL, Hedge J, Wakeley PR, Banyard AC, Zhang S, Alhassan A, Fooks AR. Evolutionary history of rabies in Ghana. PLoS Negl Trop Dis. 2011 Apr 5;5(4): e1001. [CrossRef]
- Coetzer A, Gwenhure L, Makaya P, Markotter W, Nel L. Epidemiological aspects of the persistent transmission of rabies during an outbreak (2010 - 2017) in Harare, Zimbabwe. PLoS One. 2019 Jan 10;14(1):e0210018. [CrossRef]
- Hampson K, Coudeville L, Lembo T, Sambo M, Kieffer A, Attlan M, Barrat J, Blanton JD, Briggs DJ, Cleaveland S, Costa P, Freuling CM, Hiby E, Knopf L, Leanes F, Meslin FX, Metlin A, Miranda ME, Müller T, Nel LH, Recuenco S, Rupprecht CE, Schumacher C, Taylor L, Vigilato MA, Zinsstag J, Dushoff J; Global Alliance for Rabies Control Partners for Rabies Prevention. Estimating the global burden of endemic canine rabies. PLoS Negl Trop Dis. 2015 Apr 16;9(4): e0003709. doi: 10.1371/journal.pntd.0003709. Erratum in: PLoS Negl Trop Dis. 2015 May 11;9(5):e0003786. doi: 10.1371/journal.pntd.0003786. PMID: 25881058; PMCID: PMC4400070.
- Al-Mustapha AI, Tijani AA, Bamidele FO, Muftau O, Ibrahim A, Abdulrahim I, Osu MS, Kia G, Patrick N, Endie WN. Awareness and knowledge of canine rabies: A state-wide cross-sectional study in Nigeria. PLoS One. 2021 Mar 3;16(3):e0247523. [CrossRef]
- Jackson, A.C. Human disease and pathogenesis. In: Jackson AC, Wunner WH, (eds). Rabies. Second edition. Academic Press, London, UK. 2007, pp. 309–333 and 341-381.
- Ugolini G. Use of rabies virus as a transneuronal tracer of neuronal connections: implications for the understanding of rabies pathogenesis. Dev Biol (Basel). 2008; 131:493-506.
- Mitrabhakdi E, Shuangshoti S, Wannakrairot P, Lewis RA, Susuki K, Laothamatas J, Hemachudha T. Difference in neuropathogenetic mechanisms in human furious and paralytic rabies. J Neurol Sci. 2005 Nov 15;238(1-2):3-10.
- Suite A, Guadu T, Admassu B. Challenges of rabies. International Journal of Basic and Applied Virology. 2015;4(2):41-52.
- Ichhpujani RL, Mala C, Veena M, Singh J, Bhardwaj M, Bhattacharya D, Pattanaik SK, Balakrishnan N, Reddy AK, Samnpath G, Gandhi N. Epidemiology of animal bites and rabies cases in India. A multicentric study. The Journal of communicable diseases. 2008 Mar 1;40(1):27-36.
- Salomao C, Nacima A, Cuamba L, Gujral L, Amiel O, Baltazar C, Cliff J, Gudo ES. Epidemiology, clinical features and risk factors for human rabies and animal bites during an outbreak of rabies in Maputo and Matola cities, Mozambique, 2014: Implications for public health interventions for rabies control. PLOS Neglected Tropical Diseases. 2017 Jul 24;11(7):e0005787.
- Lembo T, Hampson K, Kaare MT, Ernest E, Knobel D, Kazwala RR, Haydon DT, Cleaveland S. The feasibility of canine rabies elimination in Africa: dispelling doubts with data. PLoS Negl Trop Dis. 2010 Feb 23;4(2):e626. [CrossRef]
- Wilde H, Khawplod P, Khamoltham T, Hemachudha T, Tepsumethanon V, Lumlerdacha B, Mitmoonpitak C, Sitprija V. Rabies control in South and Southeast Asia. Vaccine. 2005 Mar 18;23(17-18):2284-9.
- Yousaf, M.Z., Qasim, M., Zia, S. Rehman Khan, MU. Ashfaq, UA. and Khan, S, Rabies molecular virology, diagnosis, prevention and treatment. Virol J 2012 : 9(50). [CrossRef]
- Jibat T, Mourits MC, Hogeveen H. Incidence and economic impact of rabies in the cattle population of Ethiopia. Prev Vet Med. 2016 Aug 1; 130:67-76.
- Yibrah M, Damtie D. Incidence of human rabies exposure and associated factors at the Gondar Health Center, Ethiopia: a three-year retrospective study. Infect Dis Poverty. 2015 Feb 2;4(1):3. [CrossRef]
- Beyene TJ, Mourits MCM, Kidane AH, Hogeveen H. Estimating the burden of rabies in Ethiopia by tracing dog bite victims. PLoS One. 2018 Feb 21;13(2): e0192313. [CrossRef]
- Pankhurst R. The history and traditional treatment of rabies in Ethiopia. Med Hist. 1970 Oct;14(4):378-89. [CrossRef]
- Nomoto H, Yamamoto K, Kutsuna S, Asai Y, Kasamatsu Y, Shirano M, Sahara T, Nakamura F, Katsuragi Y, Yamato M, Shinohara K, Sakamoto N, Hase R, Ogawa T, Nagasaka A, Miyata N, Ohmagari N. Evaluation of potential rabies exposure among Japanese international travellers: A retrospective descriptive study. PLoS One. 2023 Aug 18;18(8):e0287838. [CrossRef]
- Central Statistics Agency (CSA). National Population Statistics. Federal Democratic Republic of Ethiopia, Central Statistical Authority, 2007 Addis Ababa, Ethiopia.
- Waktola A. Exploratory Study of two regions in Ethiopia to Identify target areas and partners for intervention. DCG; 1999 Oct.
- Yalew S, Teferi E, Van Griensven A, Uhlenbrook S, Mul M, Van Der Kwast J, Van der Zaag P. Land use change and suitability assessment in the Upper Blue Nile basin under water resources and socio-economic constraints: a drive towards a decision support system.
- Central Statistics Agency (CSA). Living Standard Measurement Study-Integrated Surveys on Agriculture((LSMS-ISA), Ethiopia Socioeconomic Survey (ESS) 2015/16, situation analysis of children and women: Amhara Region: CSA, 2017 p. 8.
- Krishna AK, Satyanarayanan M, Govil PK. Assessment of heavy metal pollution in water using multivariate statistical techniques in an industrial area: a case study from Patancheru, Medak District, Andhra Pradesh, India. Journal of hazardous materials. 2009 Aug 15;167(1-3):366-73.
- Yizengaw, L., Jemberu, W.T., Bahiru, A. Molla, W.Mekonnen, S.A. Dog Ecology and Demography with Reference to Rabies in Amhara Region, Ethiopia, University of Gondar,Ethiopia, 2021. Master’s Thesis.
- Thrusfield M. Veterinary epidemiology. John Wiley & Sons; 2018 Apr 30.
- Bennett MD, Smith JB. Nuclear DNA amounts in angiosperms. Philosophical Transactions: Biological Sciences. 1991 Dec 30:309-45.
- Ntampaka P, Nyaga PN, Niragire F, Gathumbi JK, Tukei M. Knowledge, attitudes and practices regarding rabies and its control among dog owners in Kigali city, Rwanda. PLoS One. 2019 Aug 20;14(8): e0210044. [CrossRef]
- Bahiru A, Molla W, Yizengaw L, Mekonnen SA, Jemberu WT. Knowledge, attitude and practice related to rabies among residents of Amhara region, Ethiopia. Heliyon. 2022 Nov 3;8(11): e11366. [CrossRef]
- Hampson K, Dobson A, Kaare M, Dushoff J, Magoto M, Sindoya E, Cleaveland S. Rabies exposures, post-exposure prophylaxis and deaths in a region of endemic canine rabies. PLoS Negl Trop Dis. 2008;2(11): e339. [CrossRef]
- Deressa A, Ali A, Bayene M, Selassie BN, Yimer E, Hussen K. The status of rabies in Ethiopia: A retrospective record review. Ethiopian Journal of Health Development. 2010;24(2).
- Tenzin, Wangdi K, Ward MP. Human and animal rabies prevention and control cost in Bhutan, 2001-2008: the cost-benefit of dog rabies elimination. Vaccine. 2012 Dec 17;31(1):260-70. [CrossRef]
- Acosta-Jamett G, Cleaveland S, Cunningham AA, Bronsvoort BM. Demography of domestic dogs in rural and urban areas of the Coquimbo region of Chile and implications for disease transmission. Prev Vet Med. 2010 May 1;94(3-4):272-81. [CrossRef]
- Mustiana A. Assessment of the risk for rabies introduction and establishment in Lombok, Indonesia 2013, (Master's thesis, University of Sydney).
- World Health Organization: Guidelines for dog rabies control. WHO document VPH/83.43: Rev.1. World Health Organization, Geneva, Switzerland; 1987.
- Seligsohn, D. Dog bite incidence and associated risk factors—a cross-sectional study on school children in Tamil Nadu. Degree Project, Faculty of Veterinary Medicine and Animal Science, Department of Biomedical Sciences and Veterinary Public Health, Swedish University of Agricultural Sciences 2014, http://stud. epsilon. slu. se/6622.
- Seligsohn, D. Dog bite incidence and associated risk factors—a cross-sectional study on school children in Tamil Nadu. Degree Project, Faculty of Veterinary Medicine and Animal Science, Department of Biomedical Sciences and Veterinary Public Health, Swedish University of Agricultural Sciences 2014, http://stud. epsilon. slu. se/6622.
- Seligsohn, D., (2014). Dog bite incidence and associated risk factors—a cross-sectional study on school children in Tamil Nadu. Degree Project, Faculty of Veterinary Medicine and Animal Science, Department of Biomedical Sciences and Veterinary Public Health, Swedish University of Agricultural Sciences, http://stud. epsilon. slu. se/6622.
- Mediouni S, Brisson M, Ravel A. Epidemiology of human exposure to rabies in Nunavik: incidence, the role of dog bites and their context, and victim profiles. BMC Public Health. 2020 Apr 29;20(1):584. [CrossRef]
- Tenzin, Dhand NK, Dorjee J, Ward MP. Re-emergence of rabies in dogs and other domestic animals in eastern Bhutan, 2005-2007. Epidemiol Infect. 2011 Feb;139(2):220-5. [CrossRef]
- Evangelio SA, Satur DA, Lachica ZP, Mata MA, Alviola PA. Risk Factor Analysis for Dog Bite Victims in Davao City, Southern Philippines. Philippine Journal of Science. 2020 Jun 1;149(2).
- Arias Caicedo MR, Xavier DA, Arias Caicedo CA, Andrade E, Abel I. Epidemiological scenarios for human rabies exposure notified in Colombia during ten years: A challenge to implement surveillance actions with a differential approach on vulnerable populations. PLoS One. 2019 Dec 27;14(12): e0213120. [CrossRef]
- World Health Organization (WHO). Expert consultation on rabies. First report; technical report series 918. Switzerland: Geneva;2018 p. 1–130.
- Voupawoe G, Varkpeh R, Kamara V, Sieh S, Traoré A, De Battisti C, Angot A, de J Loureiro LF, Soumaré B, Dauphin G, Abebe W. Rabies control in Liberia: Joint efforts towards zero by 30. Acta Tropica. 2021 Apr 1; 216:105787.
- Shwiff SA, Sweeney SJ, Elser JL, Miller RS, Farnsworth ML, Nol P, Shwiff SS, Anderson AM. A benefit-cost analysis decision framework for mitigation of disease transmission at the wildlife–livestock interface. Human-Wildlife Interactions. 2016 Apr 1;10(1):91-102.
- Ditsele, B. “The epidemiology of Rabies in domestic ruminants in Botswana.” (2016). https://api.semanticscholar.org/CorpusID:133353622.
- Tang X, Luo M, Zhang S, Fooks AR, Hu R, Tu C. Pivotal role of dogs in rabies transmission, China. Emerg Infect Dis. 2005 Dec;11(12):1970-2. [CrossRef]
- Fitzpatrick MC, Hampson K, Cleaveland S, Meyers LA, Townsend JP, Galvani AP. Potential for rabies control through dog vaccination in wildlife-abundant communities of Tanzania. PLoS Negl Trop Dis. 2012;6(8): e1796.
- Singh R, Singh KP, Cherian S, Saminathan M, Kapoor S, Manjunatha Reddy GB, Panda S, Dhama K. Rabies - epidemiology, pathogenesis, public health concerns and advances in diagnosis and control: a comprehensive review. Vet Q. 2017 Dec;37(1):212-251. [CrossRef]
- Kanutus, Benediktus Shiikufeni. "A household survey to assess knowledge, attitudes and practices regarding Rabies among dog owners in Omusati region." PhD diss., University of Namibia, 2020.
- Tintinalli, J. E. & Stapczynski, J. S. Tintinalli’s emergency medicine: a comprehensive study guide, 2011 McGraw-Hill New York.
- Mulipukwa, C.P., 2016. Socio-Demographic Factors Associated with Vaccination of Dogs against Rabies and Dog Bite Management in Nyimba District 2016 Doctoral dissertation, The University of Zambia. http://thesisbank.jhia.ac.ke/id/eprint/8868.
- Zinsstag J, Dürr S, Penny MA, Mindekem R, Roth F, Menendez Gonzalez S, Naissengar S, Hattendorf J. Transmission dynamics and economics of rabies control in dogs and humans in an African city. Proc Natl Acad Sci U S A. 2009 Sep 1;106(35):14996-5001. [CrossRef]
- Yalemebrat, N, Bekele T, Melaku M. Assessment of public knowledge, attitude and practices towards rabies in Debark Woreda, North Gondar, Ethiopia. Journal of Veterinary Medicine and Animal Health. 2016 Nov 30;8(11):183-92.
- McCollum AM, Blanton JD, Holman RC, Callinan LS, Baty S, Phillips R, Callahan M, Levy C, Komatsu K, Sunenshine R, Bergman DL. Community survey after rabies outbreaks, Flagstaff, Arizona, USA. Emerging infectious diseases. 2012 Jun;18(6):932.
- Overall KL, Love M. Dog bites to humans—demography, epidemiology, injury, and risk. Journal of the American Veterinary Medical Association. 2001 Jun 15;218(12):1923-34.
- Daniels DM, Ritzi RB, O'Neil J, Scherer LR. Analysis of nonfatal dog bites in children. J Trauma. 2009 Mar;66(3 Suppl): S17-22. [CrossRef]
- Auplish A, Clarke AS, Van Zanten T, Abel K, Tham C, Bhutia TN, Wilks CR, Stevenson MA, Firestone SM. Estimating the intra-cluster correlation coefficient for evaluating an educational intervention program to improve rabies awareness and dog bite prevention among children in Sikkim, India: A pilot study. Acta Trop. 2017 May; 169:62-68. [CrossRef]
Figure 1.
Map of the study area.
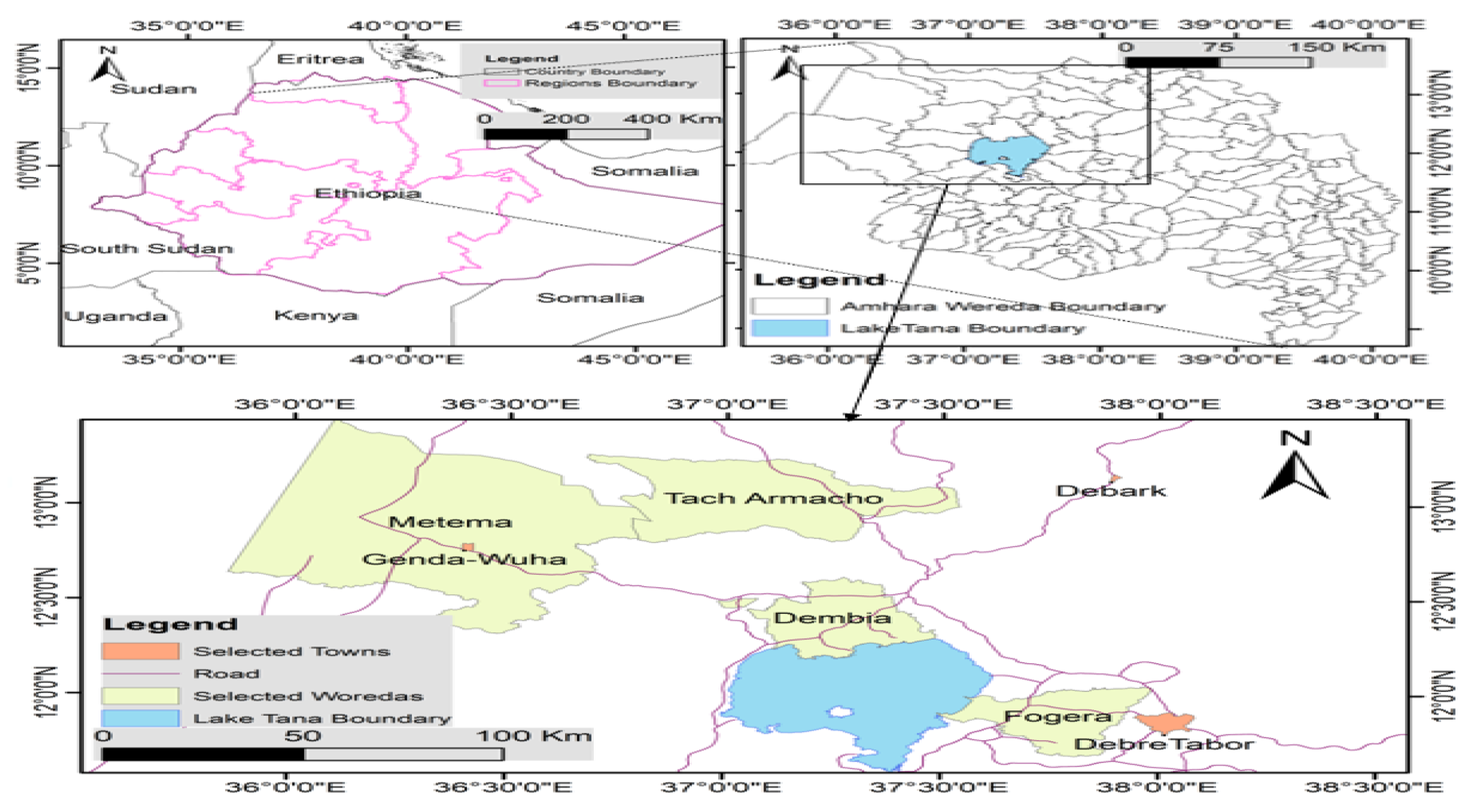

Table 1.
Variables potentially associated with rabies exposure in North-wet Ethiopia.
| Variable | Levels |
|---|---|
| Do you know rabies exists? | No/Yes |
| Do you know rabies affects humans? | No/Yes |
| Do you know the way of transmission of rabies? | No/Yes |
| Do you have a dog(s)? | No/Yes |
| Do you know dogs as a predisposing risk factor of rabies? | No/Yes |
| Do you believe traditional medicine can treat rabies? | No/Yes |
| Do you vaccinate your dog against rabies? | No/Yes |
| Do you perceive rabies as severe/fatal? | No/Yes |
| Have you or a member of your family ever been bitten by a rabid animal | No/Yes |
| What was the species of the animal that bit you or your family? | Dog/cat/Equines/wild carnivore. |
| Do you wash the bite wound? | No/Yes |
| Do you know the presence of post-exposure prophylaxis (PEP)? | No/Yes |
| Do you or your family ever take PEP | No/Yes |
| Do your dog contact with other dogs frequently | No/Yes |
| Do you castrate your dog (s) | No/Yes |
| Is there any wild carnivore near your area? | No/Yes |
Table 2.
Demography of respondents and their awareness and management of rabies in North-Western Ethiopia.
Table 2.
Demography of respondents and their awareness and management of rabies in North-Western Ethiopia.
| Variables | Number of respondents | Proportion in % | |
| Zone | West Gondar | 231 | 35.98 |
| Central Gondar | 191 | 29.75 | |
| South Gondar | 166 | 25.86 | |
| North Gondar | 54 | 8.41 | |
| District | Metema | 159 | 24.76 |
| Debre tabor | 73 | 11.37 | |
| East Dembia | 138 | 21.50 | |
| Fogera | 93 | 15.42 | |
| Genda wuha | 72 | 81.94 | |
| Debark | 54 | 8.41 | |
| Tach Armachiho | 53 | 8.26 | |
| Sex of respondents | Male | 467 | 72.74 |
| Female | 175 | 27.26 | |
| Family size | 1-3 family | 107 | 16.67 |
| 6 persons | 293 | 45.63 | |
| 7 persons | 242 | 37.69 | |
| Level of education | Non educated | 280 | 43.61 |
| Basic | 215 | 33.49 | |
| Secondary | 83 | 12.93 | |
| Tertiary | 64 | 9.97 | |
| Dog ownership | Owner | 497 | 77.41 |
| Non dog owner | 145 | 22.39 | |
| Knowledge rabies exists | Yes | 635 | 98.44 |
| No | 7 | 1.56 | |
| Knowledge rabies is zoonotic | Yes | 640 | 99.69 |
| No | 2 | 0.31 | |
| Know the transmission of rabies | Yes | 603 | 93.93 |
| No | 39 | 6.07 | |
| The presence of a dog in the house is a factor in rabies exposure | Yes | 598 | 93.15 |
| No | 44 | 6.85 | |
| Knowledge of ways of rabies transmission | Bite and saliva | 574 | 89.41 |
| Salva only | 47 | 7.32 | |
| Other methods | 21 | 3.27 | |
| Treatment by a traditional healer | Treated | 515 | 80.22 |
| Not treated | 127 | 19.78 | |
| Vaccinating dogs in the last two years | Vaccinate | 265 | 41.28 |
| No vaccinate | 377 | 58.72 | |
| Rabies killer disease | Yes | 634 | 98.75 |
| No | 8 | 1.25 | |
| Washing bite wounds | Yes | 236 | 87.73 |
| No | 33 | 12.27 | |
| Knowledge of PEP | Yes | 338 | 52.65 |
| No | 304 | 47.35 | |
| Experience of taking PEP | Yes | 59 | 21.93 |
| No | 210 | 78.07 | |
| Own dog contact with other dogs | Yes | 292 | 58.75 |
| No | 205 | 41.15 | |
| Castrating/spaying dog(s) | yes | 622 | 96.88 |
| No | 20 | 3.12 | |
| Presence of wild carnivores nearby | yes | 394 | 61.37 |
| No | 248 | 38.63 | |
Table 3.
Number of rabies exposure among the study districts, zones and group of respondents in North-Western Ethiopia.
Table 3.
Number of rabies exposure among the study districts, zones and group of respondents in North-Western Ethiopia.
| Variables Levels | Number of respondents HHs | No of rabies exposed individuals | Percentage of rabies exposure | P -value | |
| Zone | West Gondar | 231 | 135 | 50.19 | 0.001 |
| Central Gondar | 191 | 66 | 24.53 | ||
| South Gondar | 166 | 44 | 16.36 | ||
| North Gondar | 54 | 24 | 8.92 | ||
| District | Metema | 159 | 93 | 58.49 | 0.001 |
| Genda wuha | 72 | 42 | 58.33 | ||
| Tach Armachiho | 53 | 26 | 49.06 | ||
| Debark | 54 | 24 | 44.44 | ||
| Fogera | 93 | 33 | 35.48 | ||
| East Dembia | 138 | 40 | 28.99 | ||
| Debre tabor | 73 | 11 | 15.07 | ||
| Sex | Male | 467 | 197 | 42.18 | 0.812 |
| Female | 175 | 72 | 41.14 | ||
| Family Size | >6 | 242 | 117 | 48.35 | 0.036 |
| 4-6 | 293 | 120 | 40.96 | ||
| 0-3 | 107 | 32 | 29.91 | ||
| Level of Education | No education | 215 | 109 | 50.70 | 0.001 |
| Basic | 280 | 118 | 42.14 | ||
| Secondary | 83 | 24 | 28.92 | ||
| Tertiary | 64 | 18 | 28.13 | ||
| Dog ownership | owner | 497 | 193 | 71.75 | 0.004 |
| Non dog owner | 145 | 76 | 28.25 | ||
| Vaccination history | Yes | 377 | 96 | 35.69 | 0.015 |
| No | 265 | 173 | 64.31 | ||
| Distance from Hospital/ Health centre | <1 day | 553 | 217 | 39.24 | 0.000 |
| 1-2days | 55 | 37 | 62.27 | ||
| >2days | 34 | 15 | 44.12 | ||
| Dogs have free contact with others | yes | 292 | 133 | 68.91 | 0.000 |
| No | 205 | 60 | 31.09 | ||
| Presence of wildlife near his/her area | yes | 248 | 93 | 34.57 | 0.073 |
| No | 394 | 176 | 65.43 | ||
| The presence of a Forest near the residence | yes | 209 | 80 | 29.74 | 0.196 |
| No | 433 | 189 | 70.26 | ||
| Presence of high-road access | Yes | 502 | 214 | 79.55 | 0.478 |
| No | 140 | 55 | 20.45 | ||
HHs = Households.
Table 4.
Source of exposure and measure of the respondents after bite(exposure).
| Variables | Frequency | Percentage | |
| Species of bitten animals | Dog | 236 | 87.73 |
| Equine | 31 | 11.52 | |
| Cat | 1 | 0.37 | |
| Ownership of bite animals | Own | 131 | 48.70 |
| Stray | 71 | 26.39 | |
| Neighbours | 67 | 24.91 | |
| Wound Washing materials | Water only | 100 | 42.37 |
| Water and Soap | 85 | 36.02 | |
| Other material | 29 | 12.29 | |
| Holy water | 22 | 9.32 | |
Table 5.
Univariable logistic regression analyses summarizing associations (P<0.05) between potential risk factors and rabies exposure.
Table 5.
Univariable logistic regression analyses summarizing associations (P<0.05) between potential risk factors and rabies exposure.
| Variables Labels | OR | P- value | 95% CI | |
| District | Debre Tabor Ref. | |||
| Metema | 7.94 | 0.0001 | 3.89-16.23 | |
| Genda Wuha | 7.89 | 0.0001 | 3.57-17.46 | |
| Tach Armachiho | 5.43 | 0.0001 | 2.35-12.54 | |
| Debark | 4.50 | 0.0001 | 1.95-10.41 | |
| Fogera | 3.1 | 0.004 | 1.44-6.69 | |
| East Dembia | 2.30 | 0.027 | 1.10-4.82 | |
| Sex | Male Ref. | |||
| Female | 0.96 | 0.812 | 0.67-1.36 | |
| Family size | 1-3 family Ref. | |||
| 7 and above | 1.93 | 0.009 | 1.18-3.16 | |
| 4-6 Family | 1.36 | 0.210 | 0.84-2.20 | |
| Education level | Non educated Ref | |||
| Basic | 0.71 | 0.059 | 0.50-1.01 | |
| Secondary | 0.40 | 0.001 | 0.23-0.68 | |
| Tertiary | 0..38 | 0.002 | 0.21-0.69 | |
| Dog ownership | Dog owner Ref. | |||
| Non-dog owner | 0.58 | 0.004 | 0.397-0.84 | |
| The presence of wildlife nearby | yes Ref | |||
| No | 0.714 | 0.041 | 0.51-0.99 | |
| Presence of freecontactwith dogs | Yes Ref | |||
| No | 2.07 | 0.0001 | 1.42- 3.03 | |
| Forest Availability | Yes | Ref. | ||
| No | 0.80 | 0.197 | 0.57-1.12 | |
| Vaccination history | yes | Ref. | ||
| No | 0.67 | 0.015 | 0.49-0.92 | |
| Distance from Hospital/health centre | < one day | Ref. | ||
| 1-2day | 3.18 | 0.000 | 1.77-5.73 | |
| >2days | 1.22 | 0.573 | 0.61-2.46 | |
| Have you ever castrated your dog/s | No | Ref. | ||
| Yes | 0.24 | 0.022 | 0.07-0.81 | |
| Presence of high-road access | Yes Ref | |||
| No | 1.15 | 0.478 | 0.78-1.68 | |
OR= odd ratio, CI= confidence interval.
Table 6.
Multivariate logistic regression model for risk association of rabies exposure and variables.
Table 6.
Multivariate logistic regression model for risk association of rabies exposure and variables.
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



