
Submitted:
19 August 2024
Posted:
20 August 2024
You are already at the latest version
Abstract
According to current knowledge, although the beneficial effects of regular exercise training are well recognized, there are conflicting data regarding its relation with the occurrence of atrial fibrillation (AF) in competitive athletes. The aim of this literature review was to demonstrate a comprehensive report of incidence, pathophysiology and management of AF in elite athletes. The frequency of AF to be 2 to 10 times greater in high intensity endurance athletes compared to sedentary individuals. A U-shaped relationship between male elite athletes and AF has been observed, while the type and the dose of physical activity seems to play a major role in AF development. Male gender, increasing age, endurance sports, and time of training are associated with AF, thereby confirming a likely association between athleticism and AF. Pathophysiology of AF still remains unclear but, there are suggested theories that include complex mechanisms such as alterations of autonomic tone, left atrial enlargement and fibrosis, electrical remodeling, and increased inflammation. Elite athletes with AF require a comprehensive clinical evaluation and risk factor optimization, similar to that for nonathletes. Although anticoagulation and rate or rhythm control are corner stones for AF management, however, there are still no specific guidelines for elite athletes.
Keywords:
atrial fibrillation
; elite athletes
; pathophysiology
; management
1. Introduction
Regular exercise training has shown excellent results in the battle against traditional cardiovascular risk factors, and have demonstrated improvement in insulin sensitivity, lipidemic profile, and mortality by all causes, with advanced levels of endurance training further improving these outcomes [1,2,3]. Although the benefits of exercise training have been shown repeatedly in many studies, its relation with the occurrence of atrial fibrillation (AF) in competitive athletes still remains controversial.
AF is one of the most frequent cardiac arrhythmias in middle-aged athletes [4]. Recent studies have presented a significant association between regular endurance exercise and increased risk of AF, not only in elite athletes, but also in non-elite athletes who participate in vigorous exercise [5,6,7,8]. Despite exercise’s favorable effect in various traditional risk factors of arrhythmogenesis, increase in physical activity only modestly reduces incident atrial fibrillation and on the other hand, approaching the extreme border of exercise activities, endurance athletes, who participate in intense exercise training programs, demonstrate higher AF risk [9].
“Athlete” is a term that derives from the Greek word “athlos” which means achievement. Athletes are “individuals of young and adult age, either amateur or professional, who are engaged in exercise training on a regular basis and participate in official sports competition”, according with the European Society of Cardiology (ESC) [10,11], while elite athletes are “athletes who participate at the highest level of national or international competitions such as the Olympic Games (>10 h/wk)” [10,11].
In the present review we sought to demonstrate a comprehensive report of incidence, pathophysiology and therapy management of AF in elite athletes.
2. Epidemiology and Predisposal Factors
Many retrospective, observational studies and meta-analyses have estimated a 2 to 10 times higher frequency of AF in high intensity endurance athletes compared to individuals who do not exercise [6,7,8,12,13,14,15,16,17]. A U-shaped relationship between male elite athletes and AF is demonstrated through this finding, while the type (endurance) and the dose (hours of training) of physical activity seems to relate with AF development [14,18,19,20,21]. This U-shaped relationship has not been confirmed in women [14]. Regular exercise of either low or moderate intensity seems to be a preventive strategy for cardiovascular disease and AF, but higher intensity of endurance exercise could lead to AF [6,7,8,12,13,14,15,16,17,18,19,20,21]. Moreover, although the prevalence of AF increases with age, the relative risk for athletes compared with nonathletes seems to be higher in younger athletes [22,23]. A retrospective observational cohort among young elite Spanish athletes (N=6813) with mean age 22 years, assessed AF incidence within a 20-year time period, and found that it was low (0.3%), even in endurance athletes, with only 21 out of 6813 athletes having AF (18 with paroxysmal, 1 with persistent, and 2 with long-standing persistent AF) during the 20-year study [24]. In the same study, there was an association of increased AF risk and years of exercise training, age and left atrial (LA) anteroposterior diameter [24]. The prevalence of AF in competitive athletes ranges from 0.3% to approximately 13%, and differs according to the age and the modality of exercise training [13,25,26,27]. A large meta-analysis of 13 studies including approximately 64,000 athletes showed that athletes were 2.46 times more likely to have prevalent AF (95% CI 1.73 to 3.51), while the odds ratio increased to 3.6 when athletes aged < 55 years [25]. Athletes participating in mixed sports (football, basketball, American football) have increased AF burden compared to endurance sports (Nordic skiing, orienteering, rowing; B=−0.5476, p=0.0204) [25]. AF risk across the spectrum of exercise training is demonstrated in Figure 1.
Data about differences in AF incidence between males and females is limited due to lack of specifically trials. Only retrospective studies with small sample sizes that have been conducted the last 2 decades, comparing men and women, showed that AF incidence may be higher in female endurance athletes compared to males [28,29]. Specifically, Wilhelm et al. enrolled 61 female and 60 male athletes and found that, for a comparable amount of training and performance, male athletes showed a more pronounced atrial remodeling, a concentric type of ventricular remodeling, and an altered diastolic function [30]. Another study by Sanchis et al., presented gender-related differences in the adaptation of atrial performance to training, with women having greater bi-atrial deformation and smaller right atrial size compared to men [31].
An association among type of exercise (endurance sports), age (>55years), gender (males) and time of exercise training, and increased AF risk has been proven through studies [24]. Another significant clue of AF spectrum is the strong association between cardiomyopathies including dilated, hypertrophic, and arrhythmogenic cardiomyopathy and AF in younger athletes (prevalence of AF ranges between 10% and 25% in each subtype), as well as the association between long QT syndrome (LQTS) and Brugada syndrome and AF [32]. Finally, the highest incidence studies of AF are presented in the Caucasian population compared to other racial classifications [33,34].
AF may be the first manifestation of an inherited cardiac condition in young athletes. There is a strong association between AF and genes such as KCNA5, SCN5A and TTN, as well as genes including LMNA and KCNQ1 which present weaker association with AF [35,36,37,38].
Another predisposal factor of AF might be the consumption of sports supplements which are common in individuals who exercise regularly, at competitive and non-competitive level. Non-approved anabolic steroids are being used in competitive level in order to improve performance and have been associated with increased risk of AF in young athletes [39,40]. Other sports supplements that contain high concentration of caffeine and stimulants such as taurine and guarana, may cause cardiac arrhythmias after regular consumption, including AF, possibly by stimulating autonomic system [41,42]. Moreover, high consumption of these supplements may lead in both increase of blood pressure by 10 mmHg and heart rate by 5-7 beats per minute, even in healthy people [43].
3. Pathophysiology
Pathophysiology and underlying mechanisms of AF in elite athletes still remain unclear. There are suggested theories that include complex mechanisms such as alterations of autonomic tone, systemic inflammation, electrical remodeling, and LA enlargement and fibrosis [12,44,45,46,47,48,49,50].
Cardiac remodeling is the first proposed mechanism of AF. Mechanisms including LA structural changes such as dilatation and pulmonary veins stretch, cardiac inflammation, fibrosis, and increased vagal tone which may cause conduction heterogeneity and reduction in refractoriness, are responsible for the AF development in endurance athletes [51]. Athletes present increased arterial blood pressure during exercise and, in combination with atrial wall stretching after long-term strenuous endurance exercise, arrhythmogenic areas might occur due to microtrauma, inflammation, and fibrosis [13]. Furthermore, there is an association between endurance exercise and both bi-atrial and ventricular enlargement [52]. Specifically, LA enlargement both as size and volume which is associated with an increased risk of AF, is approximately present in 20% of young competitive athletes [13,50]. An observational study including 492-marathon runners, reported an association between hours of training and LA enlargement, indicating higher risk of AF in athletes with more hours of exercise training (24% in <1500 hours, 40% 1500-4500 hours and 83% in >4500 hours) [6].
Fibrosis and its potential role in exercise induced-AF is still under investigation. A study including 45 veteran elite athletes showed increased markers of myocardial fibrosis in athletes such as carboxyterminal telopeptide of collagen type I (CITP 5.4 vs. 2.9 microg/l, p<0.001), plasma carboxyterminal propeptide of collagen type I (PICP 259 vs. 166 microg/l, p<0.001), and tissue inhibitor of matrix metalloproteinase type I (350 vs. 253 ng/ml, p=0.01) compared to sedentary controls [53]. Similar findings of myocardial fibrosis were presented a few years later, in another study of 12 veteran male endurance athletes who were assessed by cardiac magnetic resonance imaging (MRI) [54]. Specifically, half of them (6/12 athletes) demonstrated late gadolinium enhancement (LGE) compared to sedentary controls. Number of years spent in training (p<0.001) and participation in number of competitive marathons (p<0.001) predicted prevalence of LGE on cardiac MRI. The proposed theory is that regular exercise can induce chronic systemic inflammation, as shown by increased levels of CRP, and may lead to atrial electrical remodeling and therefore, to development of AF [55]. However, whether AF could be treated with anti-inflammatory drugs remains controversial and more evidence is required. In a retrospective cohort study based on male long-distance cross-country ski race participants and general population men, authors evaluated the risk of AF and atrial flutter (AFl) depending on years of exercise [8]. It was shown that years of regular endurance exercise were significantly associated with increased risk for both arrhythmias; 1.16 (95% confidence interval 1.06 to 1.29) times higher risk for AF and 1.42 (95% confidence interval 1.20 to 1.69) for AFl per 10 years of endurance exercise [8].
AF in athletes is considered to be vagal-mediated [7]. AF is triggered through the macro-reentry pathway by increase in the dispersion of the atrial refractory period via activation of the iKach channel [56]. Moreover, most athletes present a lower baseline resting heart rate which is also shown as a predictor of AF [49,57]. Exercise-related increase in sympathetic tone in endurance athletes could also be a predisposal factor of AF [58,59]. In general, the combination of increased basal vagal activity and adrenergic activation might be a predisposal factor of AF [12].
There is still no clear pathophysiological mechanism regarding differential response in AF between male and female elite athletes. The most dominant hypothesis is that specific criteria in females including smaller atria, shorter P-wave duration, differences in autonomic tone, and lower LV mass and wall thickness, may be the key to these differences [17].
Electrolyte abnormalities may also be a possible trigger of AF in athletes involved in vigorous exercise. Vigorous intensity activities are defined as activities with more than 6 METS oxygen consumption and endurance sports require repeated isotonic contractions of large skeletal muscle group. Such athletic activities include: running (>5 mph), cycling, swimming, shoveling, soccer and cross-country skiing or speed skating among winter sports. These athletes may present dynamic fluid alterations which can lead to dehydration, change in pH and depletion of electrolytes including Na, K and Mg [51]. These biochemical changes could lead to supraventricular arrhythmias such as AF.
Finally, a less possible theory is the acid reflux disease. Specifically, physical activity could induce gastroesophageal reflux, and therefore, lead to AF [60]. The direct correlation between exercise and decrease in intra-esophageal pH, as well as acid reflux disease and increased risk of AF, have been shown in many observational studies in elite athletes [61,62,63,64]. Among 163,627 patients, acid reflux disease was shown to significantly increase AF risk by 39% [64].
The pathophysiological mechanisms involved in AF in competitive athletes are demonstrated in details in Figure 2.
4. Clinical Significance, Screening and Management
Physical activity seems to contribute in the decrease of all cause cardiovascular mortality and ischemic stroke, as shown in the EORP-AF study [65]. This study included 2442 patients diagnosed with AF, separated in groups of mild, moderate or high intensity training, and controls without exercise. The intensity of physical activity was reversely correlated with CHA2DS2-VASc score, indicating that smaller percentage of patients of high intensity required anticoagulation compared to mild intensity where the percentage of patients receiving anticoagulants was higher [65]. Moreover, the high-intensity exercise training group presented reduced mortality and progression rates to permanent AF compared to groups of mild intensity or no exercise [65].
Elite athletes may present higher levels of profibrotic markers which have been associated with incident or recurrent AF in the general population [66,67,68], including galectin-3 [69], suppression of tumorigenicity 2 (ST2) [70], microRNA-21 (miR-21) [71], as well as tissue inhibitor of metalloproteinase 1 (TIMP-1), C-terminal telopeptide of type I collagen (CITP) and procollagen type I carboxy-terminal propeptide (PICP) [53].
Clinical AF subtypes include AF secondary to underlying structural heart diseases i.e heart failure or valve disease, lone AF and AF in athletes. Physical activity seems to limit the presence of AF symptoms and improve cardiac remodelling in people with cardiac structural disease. However, trials often fail to prove the positive effect of exercise training. In the HF-ACTION Study, 193 individuals with AF and heart failure (HF) initially underwent 36 sessions of supervised exercise, and then continued a 2-year home-based rehabilitation program [72]. Investigators did not observe any difference in number of hospitalizations, mortality, events due to AF or other major outcomes between the training and the control group after a median 2.6-year follow-up. In another equally significant study, the RACE 3 trial, 119 individuals with persistent AF and HF performed moderate intensity cardiac rehabilitation while 126 controls with the same background received usual care. The trial showed that sinus rhythm was present in 75% of patients who performed cardiac rehabilitation versus 63% in patients who received usual care after 1 year of follow-up [73]. The triggering of the sympathetic nervous system through the acute exercise results in positive inotropic, chronotropic and lusitropic effects on the myocardium. Regular training improves peak oxygen uptake, increases cardiac output and therefore, improves functional capacity in all patients, regardless of whether they have an initial sinus rhythm or AF [74]. Another beneficial effect of exercise is the improved cardiomyocyte calcium handling which contributes to gradual hypertrophy and increased contractility of the myocardium [75]. It is a general consensus that athletes and non-athletes who present AF should exercise in a regular basis after a comprehensive clinical assessment for underlying pathology and guidelines should be more individualized.
In studies such as the ARREST-AF Cohort Study or the ACTIVE-AF Trial, regular exercise programs exhibited reduction in AF related symptoms, AF incidence and recurrence rates [76,77]. In a meta-analysis, effects of different exercise modalities on quality of life in AF patients were evaluated [78]. In 12 studies, 670 participants underwent aerobic exercise, aerobic interval training (AIT), or other exercise modalities such as yoga, Qigong, and cardiac rehabilitation protocols. All exercise modalities demonstrated statistically significant beneficial effects on general health and vitality of the Short Form 36-item questionnaire. Specifically, cardiac rehabilitation protocols and AIT increased peak VO2, while AIT also significantly reduced AF burden. Moreover, Qigong significantly improved the 6-min walk test in these individuals. [78].
It is a common policy that an athlete with a previous medical history of paroxysmal AF, but with a sinus rhythm in the ECG is able to exercise without limitations. However, elite athletes in more competitive sports who present more than one episode of AF, are recommended to be more cautious as rate control cannot be assured during high intensity training, even under medication [79]. In this case, catheter ablation for AF could be a promising solution for athletes who present AF symptoms. Younger and middle-aged athletes with paroxysmal AF are recommended to reduce the intense and the hours of physical activity as an initial approach to limit exercise-induced AF [8,79]. However, due to shortage of cumulating data, further studies with a longer follow-up of training effects are required for athletes and other clinical subgroups of AF patients, in order to extract information and provide specific recommendations.
Endurance athletes with AF are shown to present more adverse symptoms than sedentary patients without exercise [65]. Athletes with symptoms including fatigue, dizziness and syncope, induced by rapid AV nodal conduction during physical activity, are recommended to terminate physical activity and they should be referred to physicians for better rate control [11]. Although the negative impact of beta-blockers on athletes’physical performance, they are a common option among drug therapies [11]. On the other hand, monotherapy with calcium-channel blockers or digitalis does not have a satisfactory therapeutic effect. The most potent solution in order to prevent athletes from sinus bradycardia at rest or chronotropic incompetence during training would be a combination of individually titrated negatively chronotropic agents [11].
Class I and class III antiarrhythmics are main components of the armamentarium of the rhythm control in AF but, they have some limitations. On the one hand, class III antiarrhythmics such as sotalol and amiodarone may be insufficient for control or relatively contraindicated in young athletes, respectively [11]. On the other hand, athletes receiving class I antiarrhythmics usually have increased risk of developing atrial flutter and, as a result, this medication should not be used in monotherapy despite their ability to prevent recurrences of AF [11]. Prophylactic cavo-tricuspid-isthmus ablation would be a reasonable solution in athletes in this case [11]. Class I antiarrhythmics could be used as a ‘pill-in-the-pocket’ approach in patients with sporadic AF [80].
CHA2DS2-VASc score is a reliable clinical risk profile s cale for prescription of oral anticoagulants (OAC) [81]. Patients receiving OAC should not participate in sports with direct bodily contact or prone to trauma [82]. In case of drug therapy failure, or inability to receive medication, athletes would be recommended to procced with catheter ablation by pulmonary vein isolation (PVI) [83]. Patients should not participate in sports activities for at least 1 month after a successful ablation, and sports activity may be resumed only in case of no recurrences of AF within this time period [11]. It is important to be highlighted that PVI ablation does not ensure recurrence of non-pulmonary vein dependent AF in the future.
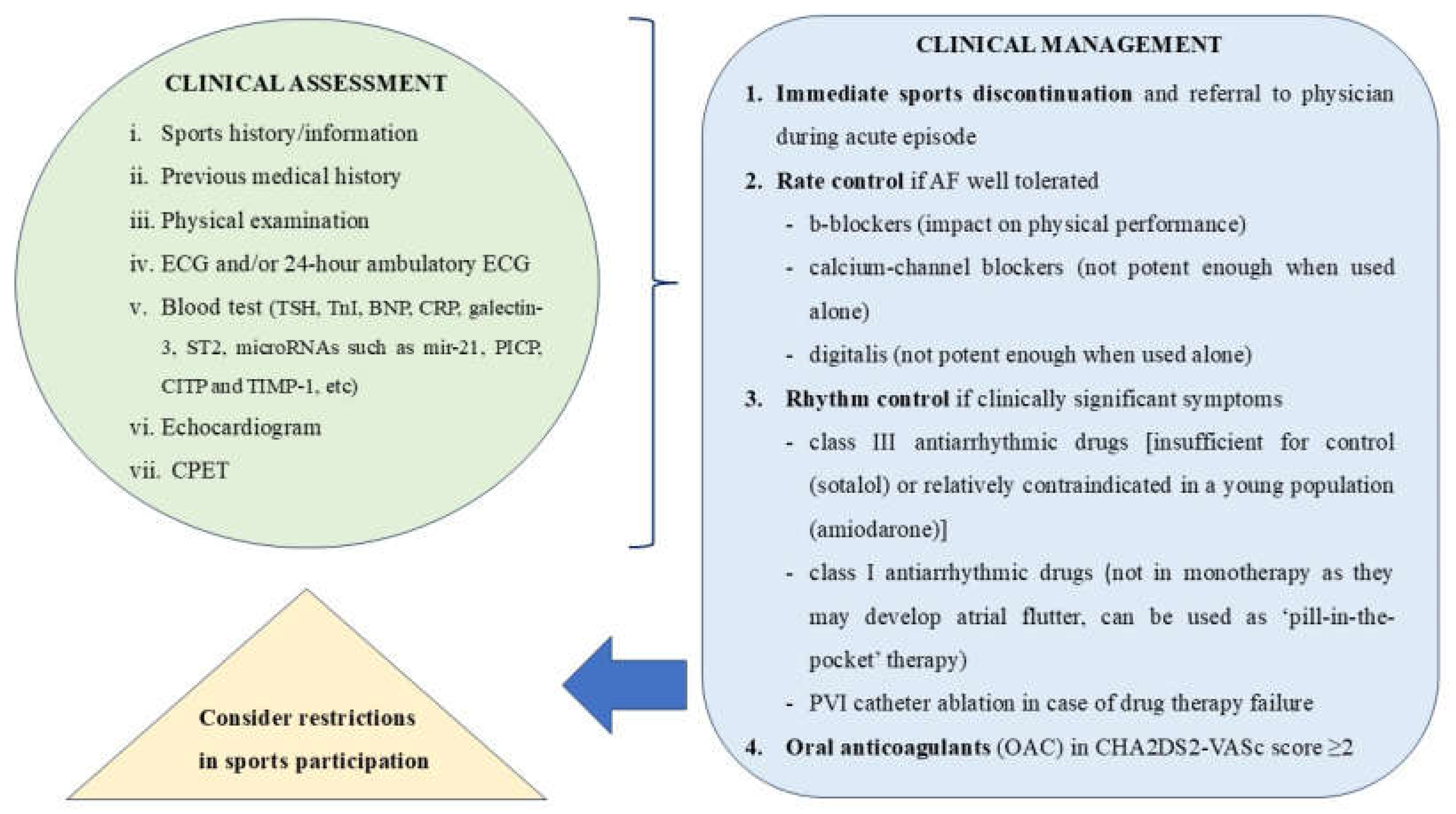
In conclusion, in the latest ESC and US AF guidelines, physical activity and risk factor optimization are corner stones for AF management before anticoagulation and rate or rhythm control. Still, there are no specific guidelines of exercise training for elite and non-elite athletes with AF, but only some consensus and recommendations. Below in Figure 3, we present a comprehensive evaluation and management approach of an elite athlete with AF.
5. Conclusions
AF is a complex syndrome in elite athletes with multiple knowledge gaps, including pathophysiological mechanisms such as alterations of autonomic system, systemic inflammation, and LA enlargement and fibrosis. Elite athletes with AF require a comprehensive clinical evaluation and risk factor optimization, similar to that for nonathletes. Although anticoagulation and rate or rhythm control are corner stones for AF management, however, there are still no specific guidelines for this subgroup. As a result, more studies are necessary for the further comprehension of the pathophysiological mechanisms and the establishment of individualized management algorithms.
Author Contributions
Conceptualization, I.P.; data curation, C.K. and A.B.; writing—original draft preparation, C.K.; writing—review and editing, A.B., E.T. and I.P.; supervision, I.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Acknowledgments
None.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Abed HS, Wittert GA, Leong DP, Shirazi MG, Bahrami B, Middeldorp ME, Lorimer MF, Lau DH, Antic NA, Brooks AG, et al. Effect of weight reduction and cardiometabolic risk factor management on symptom burden and severity in patients with atrial fibrillation: a randomized clinical trial. JAMA. 2013;310(19):2050-60.
- Lee DC, Sui X, Artero EG, Lee IM, Church TS, McAuley PA, Stanford FC, Kohl HW 3rd, Blair SN. Long-term effects of changes in cardiorespiratory fitness and body mass index on all-cause and cardiovascular disease mortality in men: the Aerobics Center Longitudinal Study. Circulation. 2011;124(23):2483-90.
- Lee DC, Pate RR, Lavie CJ, Sui X, Church TS, Blair SN. Leisure-time running reduces all-cause and cardiovascular mortality risk. J Am Coll Cardiol. 2014;64(5):472-81.
- Turagam MK, Velagapudi P, Kocheril AG. Atrial fibrillation in athletes. Am J Cardiol. 2012;109(2):296-302.
- Abdulla J, Nielsen JR. Is the risk of atrial fibrillation higher in athletes than in the general population? A systematic review and meta-analysis. Europace. 2009;11(9):1156-9.
- Wilhelm M, Roten L, Tanner H, Wilhelm I, Schmid JP, Saner H. Atrial remodeling, autonomic tone, and lifetime training hours in nonelite athletes. Am J Cardiol. 2011;108(4):580-5.
- Mont L, Tamborero D, Elosua R, Molina I, Coll-Vinent B, Sitges M, Vidal B, Scalise A, Tejeira A, Berruezo A, et al. Physical activity, height, and left atrial size are independent risk factors for lone atrial fibrillation in middle-aged healthy individuals. Europace. 2008;10(1):15-20.
- Myrstad M, Nystad W, Graff-Iversen S, Thelle DS, Stigum H, Aarønæs M, Ranhoff AH. Effect of years of endurance exercise on risk of atrial fibrillation and atrial flutter. Am J Cardiol. 2014;114(8):1229-33.
- Elliott AD, Mahajan R, Pathak RK, Lau DH, Sanders P. Exercise Training and Atrial Fibrillation: Further Evidence for the Importance of Lifestyle Change. Circulation. 2016;133(5):457-9.
- Pelliccia A, Fagard R, Bjørnstad HH, Anastassakis A, Arbustini E, Assanelli D, Biffi A, Borjesson M, Carrè F, Corrado D, et al. Recommendations for competitive sports participation in athletes with cardiovascular disease: a consensus document from the Study Group of Sports Cardiology of the Working Group of Cardiac Rehabilitation and Exercise Physiology and the Working Group of Myocardial and Pericardial Diseases of the European Society of Cardiology. Eur Heart J. 2005;26(14):1422-45.
- Pelliccia A, Sharma S, Gati S, Bäck M, Börjesson M, Caselli S, Collet JP, Corrado D, Drezner JA, Halle M, et al. 2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease. Eur Heart J. 2021;42(1):17-96.
- Estes NAM 3rd, Madias C. Atrial Fibrillation in Athletes: A Lesson in the Virtue of Moderation. JACC Clin Electrophysiol. 2017;3(9):921-928.
- Sanchis-Gomar F, Perez-Quilis C, Lippi G, Cervellin G, Leischik R, Löllgen H, Serrano-Ostáriz E, Lucia A. Atrial fibrillation in highly trained endurance athletes - Description of a syndrome. Int J Cardiol. 2017;226:11-20.
- Andersen K, Farahmand B, Ahlbom A, Held C, Ljunghall S, Michaëlsson K, Sundström J. Risk of arrhythmias in 52 755 long-distance cross-country skiers: a cohort study. Eur Heart J. 2013;34(47):3624-31.
- Mozaffarian D, Furberg CD, Psaty BM, Siscovick D. Physical activity and incidence of atrial fibrillation in older adults: the cardiovascular health study. Circulation. 2008;118(8):800-7.
- Ofman P, Khawaja O, Rahilly-Tierney CR, Peralta A, Hoffmeister P, Reynolds MR, Gaziano JM, Djousse L. Regular physical activity and risk of atrial fibrillation: a systematic review and meta-analysis. Circ Arrhythm Electrophysiol. 2013;6(2):252-6.
- Mohanty S, Mohanty P, Tamaki M, Natale V, Gianni C, Trivedi C, Gokoglan Y, DI Biase L, Natale A. Differential Association of Exercise Intensity With Risk of Atrial Fibrillation in Men and Women: Evidence from a Meta-Analysis. J Cardiovasc Electrophysiol. 2016;27(9):1021-9.
- Petrungaro M, Fusco L, Cavarretta E, Scarà A, Borrelli A, Romano S, Petroni R, D’Ascenzi F, Sciarra L. Long-Term Sports Practice and Atrial Fibrillation: An Updated Review of a Complex Relationship. J Cardiovasc Dev Dis. 2023;10(5):218.
- Morseth B, Graff-Iversen S, Jacobsen BK, Jørgensen L, Nyrnes A, Thelle DS, Vestergaard P, Løchen ML. Physical activity, resting heart rate, and atrial fibrillation: the Tromsø Study. Eur Heart J. 2016;37(29):2307-13.
- Sciarra L, Cavarretta E, Siciliani S, Sette A, Scarà A, Grieco D, DE Ruvo E, Palamà Z, Nesti M, Romano S, et al. Managing athletes with palpitations of unknown origin with an external loop recorder: a cohort study. J Sports Med Phys Fitness. 2022;62(4):554-559.
- La Gerche A, Schmied CM. Atrial fibrillation in athletes and the interplay between exercise and health. Eur Heart J. 2013;34(47):3599-602.
- Johansen KR, Ranhoff AH, Sørensen E, Nes BM, Heitmann KA, Apelland T, Bucher Sandbakk S, Wilsgaard T, Løchen ML, Thelle DS, et al. Risk of atrial fibrillation and stroke among older men exposed to prolonged endurance sport practice: a 10-year follow-up. The Birkebeiner Ageing Study and the Tromsø Study. Open Heart. 2022;9(2):e002154.
- Svedberg N, Sundström J, James S, Hållmarker U, Hambraeus K, Andersen K. Long-Term Incidence of Atrial Fibrillation and Stroke Among Cross-Country Skiers. Circulation 2019;140(11):910–920.
- Boraita A, Santos-Lozano A, Heras ME, González-Amigo F, López-Ortiz S, Villacastín JP, Lucia A. Incidence of Atrial Fibrillation in Elite Athletes. JAMA Cardiol. 2018;3(12):1200-1205.
- Newman W, Parry-Williams G, Wiles J, Edwards J, Hulbert S, Kipourou K, Papadakis M, Sharma R, O’Driscoll J. Risk of atrial fibrillation in athletes: a systematic review and meta-analysis. Br J Sports Med. 2021;55(21):1233-1238.
- Wernhart S, Halle M. Atrial fibrillation and long-term sports practice: epidemiology and mechanisms. Clin Res Cardiol. 2015;104(5):369-79.
- Calvo N, Ramos P, Montserrat S, Guasch E, Coll-Vinent B, Domenech M, Bisbal F, Hevia S, Vidorreta S, Borras R, et al. Emerging risk factors and the dose-response relationship between physical activity and lone atrial fibrillation: a prospective case-control study. Europace. 2016;18(1):57-63.
- Drca N, Larsson SC, Grannas D, Jensen-Urstad M. Elite female endurance athletes are at increased risk of atrial fibrillation compared to the general population: a matched cohort study. Br J Sports Med. 2023;57(18):1175-1179.
- Myrstad M, Johansen KR, Sørensen E, Løchen ML, Ranhoff AH, Morseth B. Atrial fibrillation in female endurance athletes. Eur J Prev Cardiol. 2024;31(5):e27-e29.
- Wilhelm M, Roten L, Tanner H, Wilhelm I, Schmid JP, Saner H. Gender differences of atrial and ventricular remodeling and autonomic tone in nonelite athletes. Am J Cardiol. 2011;108(10):1489-95.
- Sanchis L, Sanz-de La Garza M, Bijnens B, Giraldeau G, Grazioli G, Marin J, Gabrielli L, Montserrat S, Sitges M. Gender influence on the adaptation of atrial performance to training. Eur J Sport Sci. 2017;17(6):720-726.
- Shoemaker MB, Shah RL, Roden DM, Perez MV. How Will Genetics Inform the Clinical Care of Atrial Fibrillation? Circ Res. 2020;127(1):111-127.
- Norby FL, Benjamin EJ, Alonso A, Chugh SS. Racial and Ethnic Considerations in Patients With Atrial Fibrillation: JACC Focus Seminar 5/9. J Am Coll Cardiol. 2021;78(25):2563-2572.
- Gomez SE, Fazal M, Nunes JC, Shah S, Perino AC, Narayan SM, Tamirisa KP, Han JK, Rodriguez F, Baykaner T. Racial, ethnic, and sex disparities in atrial fibrillation management: rate and rhythm control. J Interv Card Electrophysiol. 2023;66(5):1279-1290.
- Chalazan B, Freeth E, Mohajeri A, Ramanathan K, Bennett M, Walia J, Halperin L, Roston T, Lazarte J, Hegele RA, et al. Genetic testing in monogenic early-onset atrial fibrillation. Eur J Hum Genet. 2023;31(7):769-775.
- Yoneda ZT, Anderson KC, Quintana JA, O’Neill MJ, Sims RA, Glazer AM, Shaffer CM, Crawford DM, Stricker T, Ye F, et al. Early-Onset Atrial Fibrillation and the Prevalence of Rare Variants in Cardiomyopathy and Arrhythmia Genes. JAMA Cardiol. 2021;6(12):1371-1379.
- Hateley S, Lopez-Izquierdo A, Jou CJ, Cho S, Schraiber JG, Song S, Maguire CT, Torres N, Riedel M, Bowles NE, et al. The history and geographic distribution of a KCNQ1 atrial fibrillation risk allele. Nat Commun. 2021;12(1):6442.
- Lampert R, Chung EH, Ackerman MJ, Arroyo AR, Darden D, Deo R, Dolan J, Etheridge SP, Gray BR, Harmon KG, et al. 2024 HRS expert consensus statement on arrhythmias in the athlete: Evaluation, treatment, and return to play. Heart Rhythm. 2024:S1547-5271(24)02560-8.
- https://www.wada-ama.org/sites/default/files/2022-01/2022list_final_en_0.pdf. Accessed on 13th August, 2024.
- Lau DH, Stiles MK, John B, Shashidhar, Young GD, Sanders P. Atrial fibrillation and anabolic steroid abuse. Int J Cardiol. 2007;117(2):e86-7.
- Seifert SM, Schaechter JL, Hershorin ER, Lipshultz SE. Health effects of energy drinks on children, adolescents, and young adults. Pediatrics. 2011;127(3):511-28.
- Di Rocco JR, During A, Morelli PJ, Heyden M, Biancaniello TA. Atrial fibrillation in healthy adolescents after highly caffeinated beverage consumption: two case reports. J Med Case Rep. 2011;5:18.
- Steinke L, Lanfear DE, Dhanapal V, Kalus JS. Effect of “energy drink” consumption on hemodynamic and electrocardiographic parameters in healthy young adults. Ann Pharmacother. 2009;43(4):596-602.
- Elliott AD, Mahajan R, Lau DH, Sanders P. Atrial Fibrillation in Endurance Athletes: From Mechanism to Management. Cardiol Clin. 2016;34(4):567-578.
- Nattel S, Harada M. Atrial remodeling and atrial fibrillation: recent advances and translational perspectives. J Am Coll Cardiol. 2014;63(22):2335-45.
- La Gerche A, Inder WJ, Roberts TJ, Brosnan MJ, Heidbuchel H, Prior DL. Relationship between Inflammatory Cytokines and Indices of Cardiac Dysfunction following Intense Endurance Exercise. PLoS One. 2015;10(6):e0130031.
- Sugama K, Suzuki K, Yoshitani K, Shiraishi K, Miura S, Yoshioka H, Mori Y, Kometani T. Changes of thioredoxin, oxidative stress markers, inflammation and muscle/renal damage following intensive endurance exercise. Exerc Immunol Rev. 2015;21:130-42.
- Aschar-Sobbi R, Izaddoustdar F, Korogyi AS, Wang Q, Farman GP, Yang F, Yang W, Dorian D, Simpson JA, Tuomi JM, et al. Increased atrial arrhythmia susceptibility induced by intense endurance exercise in mice requires TNFα. Nat Commun. 2015;6:6018.
- Baggish, AL. Mechanisms underlying the cardiac benefits of exercise: Still running in the dark. Trends Cardiovasc Med. 2015;25(6):537-9.
- Pelliccia A, Maron BJ, Di Paolo FM, Biffi A, Quattrini FM, Pisicchio C, Roselli A, Caselli S, Culasso F. Prevalence and clinical significance of left atrial remodeling in competitive athletes. J Am Coll Cardiol. 2005;46(4):690-6.
- Turagam MK, Flaker GC, Velagapudi P, Vadali S, Alpert MA. Atrial Fibrillation In Athletes: Pathophysiology, Clinical Presentation, Evaluation and Management. J Atr Fibrillation. 2015;8(4):1309.
- Mont L, Elosua R, Brugada J. Endurance sport practice as a risk factor for atrial fibrillation and atrial flutter. Europace. 2009;11(1):11-7.
- Lindsay MM, Dunn FG. Biochemical evidence of myocardial fibrosis in veteran endurance athletes. Br J Sports Med. 2007;41(7):447-52.
- Wilson M, O’Hanlon R, Prasad S, Deighan A, Macmillan P, Oxborough D, Godfrey R, Smith G, Maceira A, Sharma S, et al. Diverse patterns of myocardial fibrosis in lifelong, veteran endurance athletes. J Appl Physiol (1985). 2011;110(6):1622-6.
- Swanson, DR. Atrial fibrillation in athletes: implicit literature-based connections suggest that overtraining and subsequent inflammation may be a contributory mechanism. Med Hypotheses. 2006;66(6):1085-92.
- Bettoni M, Zimmermann M. Autonomic tone variations before the onset of paroxysmal atrial fibrillation. Circulation. 2002;105(23):2753-9.
- Grimsmo J, Grundvold I, Maehlum S, Arnesen H. High prevalence of atrial fibrillation in long-term endurance cross-country skiers: echocardiographic findings and possible predictors--a 28-30 years follow-up study. Eur J Cardiovasc Prev Rehabil. 2010;17(1):100-5.
- Carpenter A, Frontera A, Bond R, Duncan E, Thomas G. Vagal atrial fibrillation: What is it and should we treat it? Int J Cardiol. 2015;201:415-21.
- Grundvold I, Skretteberg PT, Liestøl K, Erikssen G, Engeseth K, Gjesdal K, Kjeldsen SE, Arnesen H, Erikssen J, Bodegard J. Low heart rates predict incident atrial fibrillation in healthy middle-aged men. Circ Arrhythm Electrophysiol. 2013;6(4):726-31.
- Swanson, DR. Running, esophageal acid reflux, and atrial fibrillation: a chain of events linked by evidence from separate medical literatures. Med Hypotheses. 2008;71(2):178-85.
- Collings KL, Pierce Pratt F, Rodriguez-Stanley S, Bemben M, Miner PB. Esophageal reflux in conditioned runners, cyclists, and weightlifters. Med Sci Sports Exerc. 2003;35(5):730-5.
- Soffer EE, Merchant RK, Duethman G, Launspach J, Gisolfi C, Adrian TE. Effect of graded exercise on esophageal motility and gastroesophageal reflux in trained athletes. Dig Dis Sci. 1993;38(2):220-4.
- Choi SC, Choi SJ, Kim JA, Kim TH, Nah YH, Yazaki E, Evans DF. The role of gastrointestinal endoscopy in long-distance runners with gastrointestinal symptoms. Eur J Gastroenterol Hepatol. 2001;13(9):1089-94.
- Kunz JS, Hemann B, Edwin Atwood J, Jackson J, Wu T, Hamm C. Is there a link between gastroesophageal reflux disease and atrial fibrillation? Clin Cardiol. 2009;32(10):584-7.
- Proietti M, Boriani G, Laroche C, Diemberger I, Popescu MI, Rasmussen LH, Sinagra G, Dan GA, Maggioni AP, Tavazzi L, et al. Self-reported physical activity and major adverse events in patients with atrial fibrillation: a report from the EURObservational Research Programme Pilot Survey on Atrial Fibrillation (EORP-AF) General Registry. Europace. 2017;19(4):535-543.
- Nortamo S, Ukkola O, Lepojärvi S, Kenttä T, Kiviniemi A, Junttila J, Huikuri H, Perkiömäki J. Association of sST2 and hs-CRP levels with new-onset atrial fibrillation in coronary artery disease. Int J Cardiol. 2017;248:173-178.
- Fashanu OE, Norby FL, Aguilar D, Ballantyne CM, Hoogeveen RC, Chen LY, Soliman EZ, Alonso A, Folsom AR. Galectin-3 and incidence of atrial fibrillation: The Atherosclerosis Risk in Communities (ARIC) study. Am Heart J. 2017;192:19-25.
- McManus DD, Tanriverdi K, Lin H, Esa N, Kinno M, Mandapati D, Tam S, Okike ON, Ellinor PT, Keaney JF Jr, et al. Plasma microRNAs are associated with atrial fibrillation and change after catheter ablation (the miRhythm study). Heart Rhythm. 2015;12(1):3-10.
- Hättasch R, Spethmann S, de Boer RA, Ruifrok WP, Schattke S, Wagner M, Schroeckh S, Durmus T, Schimke I, Sanad W, et al. Galectin-3 increase in endurance athletes. Eur J Prev Cardiol. 2014;21(10):1192-9.
- Roca E, Nescolarde L, Lupón J, Barallat J, Januzzi JL, Liu P, Cruz Pastor M, Bayes-Genis A. The Dynamics of Cardiovascular Biomarkers in non-Elite Marathon Runners. J Cardiovasc Transl Res. 2017;10(2):206-208.
- Baggish AL, Hale A, Weiner RB, Lewis GD, Systrom D, Wang F, Wang TJ, Chan SY. Dynamic regulation of circulating microRNA during acute exhaustive exercise and sustained aerobic exercise training. J Physiol. 2011;589(Pt 16):3983-94.
- Luo N, Merrill P, Parikh KS, Whellan DJ, Piña IL, Fiuzat M, Kraus WE, Kitzman DW, Keteyian SJ, O’Connor CM, et al. Exercise Training in Patients With Chronic Heart Failure and Atrial Fibrillation. J Am Coll Cardiol. 2017;69(13):1683-1691.
- Rienstra M, Hobbelt AH, Alings M, Tijssen JGP, Smit MD, Brügemann J, Geelhoed B, Tieleman RG, Hillege HL, Tukkie R, et al. Targeted therapy of underlying conditions improves sinus rhythm maintenance in patients with persistent atrial fibrillation: results of the RACE 3 trial. Eur Heart J. 2018;39(32):2987-2996.
- Malmo V, Nes BM, Amundsen BH, Tjonna AE, Stoylen A, Rossvoll O, Wisloff U, Loennechen JP. Aerobic Interval Training Reduces the Burden of Atrial Fibrillation in the Short Term: A Randomized Trial. Circulation. 2016;133(5):466-73.
- Kemi OJ, Wisløff U. Mechanisms of exercise-induced improvements in the contractile apparatus of the mammalian myocardium. Acta Physiol (Oxf). 2010;199(4):425-39.
- Pathak RK, Middeldorp ME, Lau DH, Mehta AB, Mahajan R, Twomey D, Alasady M, Hanley L, Antic NA, McEvoy RD, et al. Aggressive risk factor reduction study for atrial fibrillation and implications for the outcome of ablation: the ARREST-AF cohort study. J Am Coll Cardiol. 2014;64(21):2222-31.
- Elliott AD, Verdicchio CV, Mahajan R, Middeldorp ME, Gallagher C, Mishima RS, Hendriks JML, Pathak RK, Thomas G, Lau DH, et al. An Exercise and Physical Activity Program in Patients With Atrial Fibrillation: The ACTIVE-AF Randomized Controlled Trial. JACC Clin Electrophysiol. 2023;9(4):455-465.
- AbuElkhair A, Boidin M, Buckley BJR, Lane DA, Williams NH, Thijssen D, Lip GYH, Barraclough DL. Effects of different exercise types on quality of life for patients with atrial fibrillation: a systematic review and meta-analysis. J Cardiovasc Med (Hagerstown). 2023;24(2):87-95.
- Zipes DP, Link MS, Ackerman MJ, Kovacs RJ, Myerburg RJ, Estes NAM 3rd. Eligibility and Disqualification Recommendations for Competitive Athletes With Cardiovascular Abnormalities: Task Force 9: Arrhythmias and Conduction Defects: A Scientific Statement From the American Heart Association and American College of Cardiology. J Am Coll Cardiol. 2015;66(21):2412-2423.
- Alboni P, Botto GL, Baldi N, Luzi M, Russo V, Gianfranchi L, Marchi P, Calzolari M, Solano A, Baroffio R, et al. Outpatient treatment of recent-onset atrial fibrillation with the “pill-in-the-pocket” approach. N Engl J Med. 2004;351(23):2384-91.
- Kirchhof P, Benussi S, Kotecha D, Ahlsson A, Atar D, Casadei B, Castella M, Diener HC, Heidbuchel H, Hendriks J, et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur J Cardiothorac Surg. 2016;50(5):e1-e88.
- Steffel J, Verhamme P, Potpara TS, Albaladejo P, Antz M, Desteghe L, Haeusler KG, Oldgren J, Reinecke H, Roldan-Schilling V, et al. The 2018 European Heart Rhythm Association Practical Guide on the use of non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation. Eur Heart J. 2018;39(16):1330-1393.
- Calkins H, Hindricks G, Cappato R, Kim YH, Saad EB, Aguinaga L, Akar JG, Badhwar V, Brugada J, Camm J, et al. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation. Heart Rhythm. 2017;14(10):e275-e444.
Figure 1.
Atrial fibrillation (AF) risk across the spectrum of exercise training. Approaching the extreme borders of physical activities (minimum physical activity in the one border and endurance sports on the other), there is an increase in AF incidence.
Figure 1.
Atrial fibrillation (AF) risk across the spectrum of exercise training. Approaching the extreme borders of physical activities (minimum physical activity in the one border and endurance sports on the other), there is an increase in AF incidence.
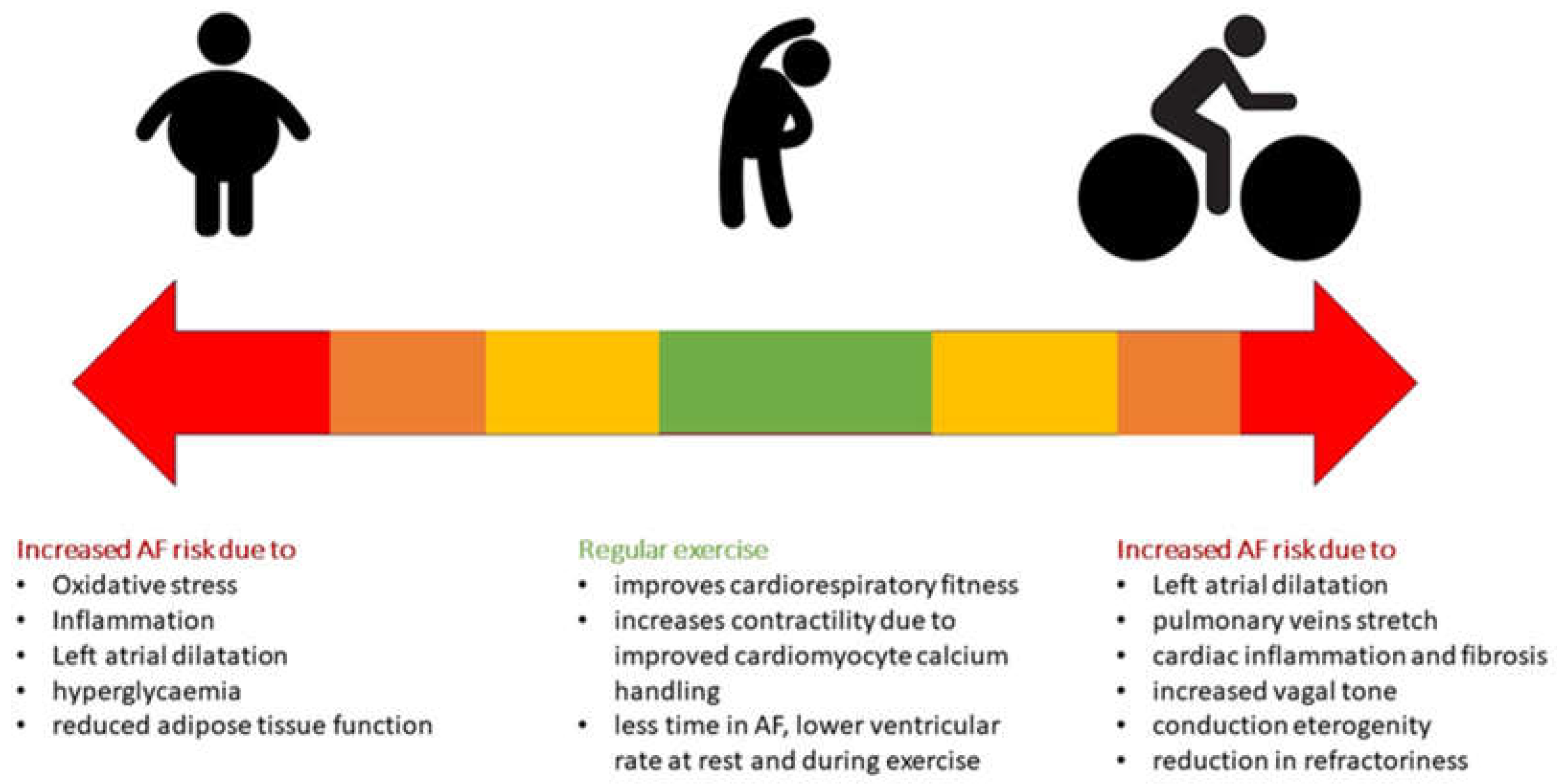
Figure 2.
Presumed Mechanisms of AF in Elite Athletes.
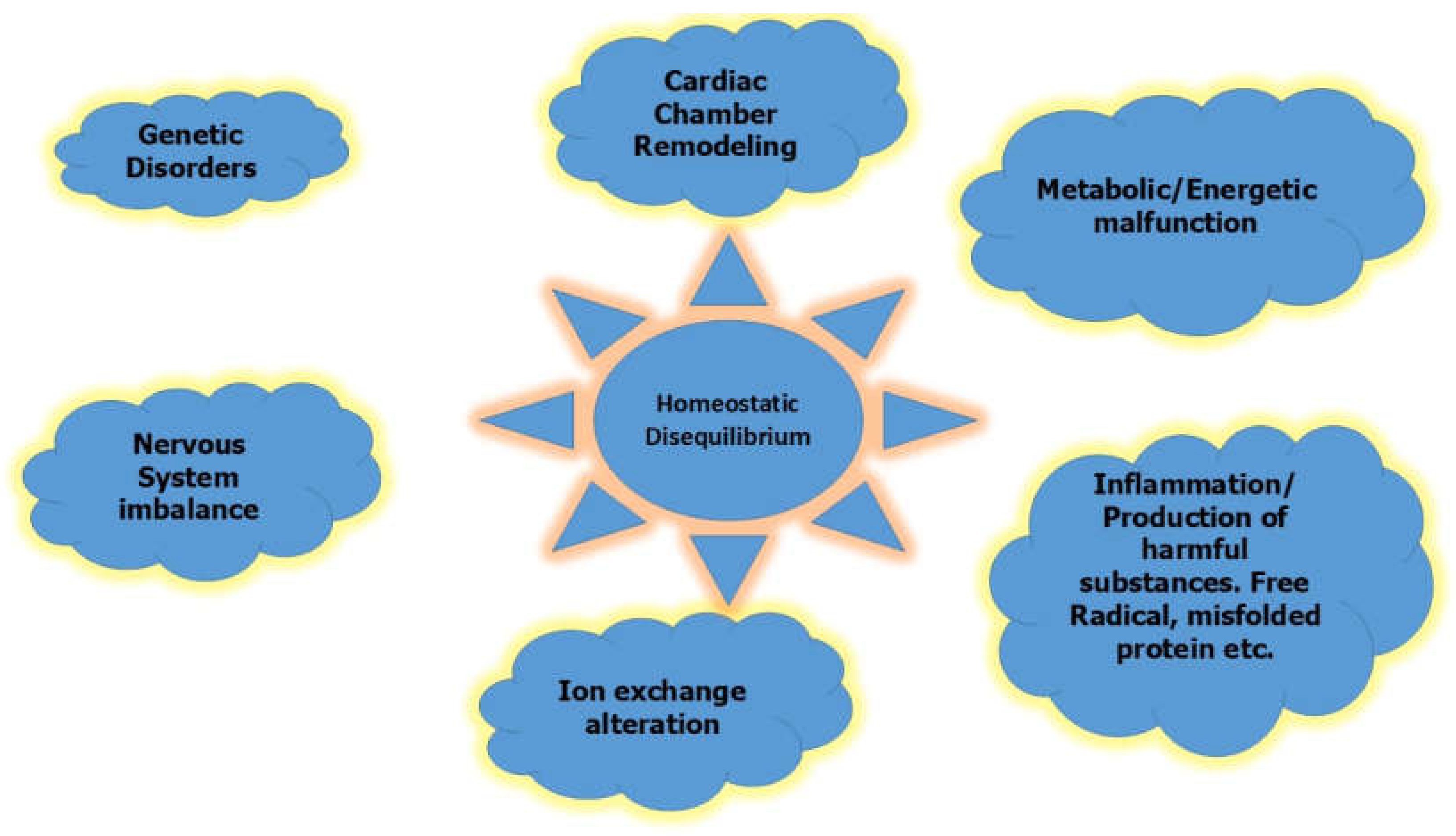
Figure 3.
A proposed algorithm of clinical assessment and therapeutic strategy of an elite athlete with AF.
Figure 3.
A proposed algorithm of clinical assessment and therapeutic strategy of an elite athlete with AF.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



