
Submitted:
19 August 2024
Posted:
20 August 2024
You are already at the latest version
Abstract
The purpose of this scoping review was to identify gaps in the literature and summarize findings from studies examining the use of silicon-, silica-, and silicate-based toothpastes for the remineralization and repair of mineralized tooth tissues. A 10-year literature search was conducted using PubMed and Scopus, adhering to PRISMA 2020 guidelines. A total of 331 studies were initially identified, with 56 full-text review articles. After selecting the manuscripts, 27 studies were qualitatively analyzed by four reviewers, focusing on the results of both in vivo and in vitro methods. The findings suggest that toothpastes containing silicon, silica, and silicate demonstrate promising results for remineralization and enamel repair, with evidence of mineral layer formation and/or deep enamel surface remineralization under various conditions. Additionally, the use of these toothpastes can lead to the obliteration of dentinal tubules within a few days. The results collectively support the efficacy of these toothpastes in enamel repair. Most of the clinical studies focused on dentine hypersensitivity, followed by white spot lesions. In conclusion, silicon-, silica-, and silicate-based toothpastes (bioactive-Si-toothpastes) can be considered effective based mostly on laboratory studies. There remains a need for more in vivo research studies on enamel and dentin mineral repair. Existing studies provide strong evidence that these technologies can reduce dentin hypersensitivity and promote enamel-dentin repair.
Keywords:
Silicon
; silica
; silicate
; bioactive
; toothpastes
; dental caries
; dentin hypersensitivity
1. Introduction
The mechanisms underlying the remineralization of dental hard tissues are now increasingly well-understood. It is also noteworthy recognized the importance of fluoride in this process particularly when fluoride in its ionic form is available in toothpastes and other dental products [1,2]. Fluoride-containing toothpastes have been regarded as one of the most important strategies for dental caries prevention and for the caries decline in many countries. Therefore, fluoride-based strategies remain the standard for caries prevention [2].
However, dental caries persists as a major public health problem in many parts of the world, and new approaches for remineralization of dental hard tissues have been proposed in the last decade [3,4,5,6,7,8]. These technologies can be divided into two major groups: a) the non-fluoride remineralization technologies (biomimetic enamel regenerative formulations) that claim to achieve deeper remineralization of lesions; and b) the group of products that enhance fluoride efficacy known as F-boosters [9].
A straightforward simply strategy to enhance fluoride efficacy and its bioavailability in the oral cavity would be to just add more fluoride into oral care products. However, this approach can raise concerns about the potential risk for dental fluorosis as some children are exposed to multiple sources of fluoride. Moreover, a higher amount of fluoride in the oral mouth might not be efficacious for controlling erosive tooth wear and other oral complex conditions such as MIH (molar incisors hypomineralization) associated with hypersensitivity [10,11,12]. In this manner, non-fluoride remineralization technologies and F-boosters can be interesting approaches for consumers that avoid F- toothpastes and for those who prefer low F- in oral care products [2,9].
The incorporation of ions into the hydroxyapatite (HA) structure directly influences its physical, chemical, and physiological properties and, consequently the tissue mineralization process. In general terms, demineralization is the removal of mineral ions from hydroxyapatite crystals of hard tissues (e.g.,: enamel, dentin, cementum, and bone). Remineralization is the opposite process and can be enhanced by substituting ionic species in the sites of the hydroxyapatite molecule [13]. The presence of substitute ions, either incorporated within the apatite lattice or only adsorbed on the surface, can modify the solubility of a dentin/enamel structure. These substitute ions could be anions such as fluoride and silicon.
Remineralization process can occur within the demineralized tooth structure as a natural repair event. Basically, remineralization is a net mineral gain since calcium (Ca2+) and phosphate (PO43–) ions are deposited into the crystal voids of the demineralized tooth structure [1,9]. The incorporation of Ca2+ and PO43– ions into the crystal lattice can be enhanced by the presence of free fluoride (F–) ions in the oral environment. This process can result in an apatite that is significantly more resistant to a subsequent acid challenge [14].
While studies on remineralization modulated by fluoride ions are already well studied, there are still gaps regarding the mechanisms of remineralization orchestrated by silicon. Each ionic grouping of apatite, namely calcium, phosphate, and hydroxyl, can be replaced by another ionic grouping of the same or different valence. In bones, the sites of hydroxyl (OH) and phosphate (PO4) of hydroxyapatite (HA) are noted as A and B, respectively. Hence, fluoride ions (F-) can substitute hydroxyls in site A to form Ca10(PO4)6(OH)2-2xF2x, whereas (SiO4)4− operates in site B. This substitution in site B will produce Ca10(PO4)6-x(SiO4)x(OH)2-x chemical structures [15,16].
Contrary to fluorine, silicon is a relatively inactive chemical element. However, both cannot be found in their isolated pure form in nature and both of them can form bioactive molecules. Silicon is a half-metallic element that reacts with oxygen to form silicon dioxide at high temperatures (SiO2). In this form, the (SiO4)4− anions are versatile tetrahedral molecules that can be connected in different ways and may become bioactive. This natural form of silicon dioxide is also known as “silica” and can be found in different crystalline or amorphous forms. Silicates occur when silicon dioxide is bound to other elements (e.g.,: calcium, aluminum, iron, and magnesium) and can be defined as salts [17]. All forms (silicon ion, silica, and silicate) can be of great importance in dental products.
Toothpastes are regarded as one of the most complex healthcare products to produce [18]. It is a mixture of abrasives suspended in an aqueous humectant phase to form a hydrocolloid material that active ingredients will be incorporated. Furthermore, this material will form a slurry in the oral cavity, a mixture of saliva and denser solids from toothpastes. On one hand, saliva will facilitate the dispersion of ingredients in the oral cavity. On the other hand, saliva will dilute all toothpaste ingredients including the bioactive ones. Finally, the bioactive ingredients must be stable in different pH environments.
The aims of this scoping revision were to identify gaps in the literature and summarize findings from several studies related to silicon-, silica- and silicate- toothpastes that can be used for tooth remineralization and repair of mineralized tissues such as dental caries, molar incisor hypomineralization (MIH), and erosive tooth wear. It is also relevant to update information on this topic because there are many technologies claiming enamel-dentin repair. However, it appears that few clinical trials were carried out to provide robust evidence about the magnitude of the efficacy of these bioactive ingredients.
1.1. Enamel Regeneration or Repair: Background and Definitions
The term “regenerative dentistry” has several definitions that can overlap concepts and goals and raise some confusion. Regenerative dentistry and tissue engineering have been exploring at least three domains that aim to act as scaffolds to promote cell growth and differentiation for tissue regeneration/healing: stem cells, bioactive molecules, and biomaterials [19]. However, a direct approach to hard tissues brings into question whether this concept is suitable. Certainly, it is appropriate for bones and dentin, but for dental enamel, some additional thoughts are worth the effort.
Dental enamel is the only cell-free tissue in the human body, organized in a complex multilevel structure [20]. As a result, dental enamel cannot be biologically repaired or regenerated, and simply recovering the lost minerals may not be sufficient. The challenge lies in recreating the hierarchical structure on the surface of the damaged enamel, mimicking its original structure [21]. As for dentin, the concept of “healing” of the damaged tissue must include the organic portion. This challenging scenario is an open opportunity for a biomimetic approach within a broad perspective of the regenerative dentistry field.
Biomimetics in Dentistry was first proposed by Professor Stephen Mann in 1997: “…biomimetics concepts can be useful for the fabrication of biomaterial implants with controlled porosity and microstructure” [22]. The original idea was related to dental materials and was later expanded to other oral care products. Nevertheless, for both dental materials and toothpastes, the challenges continue: mature enamel, conversely, to dentin and bone, is acellular and does not resorb or remodel. Therefore, a true enamel regeneration cannot occur in vivo [23]; and considering many toothpastes that claim a full regeneration of enamel, the appropriate terminology for their beneficial effect is probably “enamel repair”. To justify the choice of the term “repair” instead of “regeneration”, one must bear in mind that these concepts are commonly used in soft tissues healing processes. A healing repair event takes place when, eventually the outcome of a previous damaged skin/mucosa is a restored tissue with some failures or even scars. Whereas a regenerative healing process brings the idea of a complete restoration of the whole tissue architecture, function, and esthetics [24]. Transposing these definitions to hard tissue is of utmost importance to avoid some conflicting concepts.
It is relevant to point out that the concept of enamel regeneration is preserved when cell-based strategies, tissue engineering laboratory techniques, and similar methods are proposed. However, the focus of this review is the ion-based remineralization and repair of the enamel and dentin by the regular use of toothpastes.
There are more definitions that can raise confusion and need to be clarified, particularly for remineralization (e.g.,: functional remineralization, biomineralization, and biomimetic remineralization).
Functional remineralization (FR) stands for remineralization that leads to improved tissue mechanics and functionality [25]. This is a close concept to enamel repair.
Biomineralization of hard tissues (enamel, dentin, and bone) involves the deposition of apatite mineral crystals within an organic matrix. Bone and teeth are regarded as biomaterials with unique biomechanical properties that are crucial to their function [26]. Hence, biomineralization is a complex series of events regulated by cells expressing matrix proteins that act as crystallization promoters or inhibitors [27,28]. As a result, the use of a bioactive agent for dental remineralization is not necessarily a biomineralization process.
Biomimetic mineralization (BIMIN) is another technique developed to stimulate the guided formation of a layer of fluorapatite that resembles enamel. This is done on a mineral substrate and has the potential to enhance the remineralization of superficial enamel and exposed demineralized dentin [29].
Bioactive remineralization: it is a general term related to the net mineral gain of a demineralized dentin surface and the following clinical benefits promoted by bioactive agents: acid resistance (carious and erosive challenges), abrasion resistance (mechanical/masticatory wear), and surface impermeability (microleakage and hypersensitivity) [30].
1.2. Silicon, Silica, and Silicate Toothpastes
In Dentistry, silicon and silica are best known as hydrated silica SiO2·nH2O (silicon dioxide with a variable amount of water) which is used as abrasive component of many brands of toothpastes. It is the abrasive of choice in clear gel formulations [18]. However, silicon, silica and silicate can push forward and act as bioactive agents or compose a bioactive material for enamel/dentin remineralization or repair. Since the 1980s a bioactive material has been explained as one that “elicits a specific biological response at the interface of the material that results in the formation of a bond between tissues and the material” [30,31,32].
Bioactive glasses (BGs or BAG), also known as bioglasses are a quaternary oxide system of SiO2–CaO–Na2O–P2O5. It is regarded as the first inorganic material with the ability to bond with living bone tissue and form a stable and tightly bound interface. In addition to bone regeneration, this material is highly versatile. It can deliver pharmaceutical compounds and be useful in many hard tissues engineering challenging conditions. Bioactive glass can mineralize dentine tubules to relieve tooth sensitivity. [32,33].
In the oral cavity, once interacting with saliva, bioglass particles trigger a complex phenomenon termed bioactivity. As a result, this ionic-rich bioglass environment fosters the creation of hydroxyapatite layers and calcium phosphate compounds (Ca3(PO4)2) within the tooth structure [34]. The formation of a crystalline hydroxyl carbonate apatite (HCA) layer is regarded as strong evidence of bioactivity in bones and other hard tissues [35]. Basically, a proposed mechanism of action of bioglass for remineralizing dental enamel relies on the following steps, as described by Dai and co-workers [36]: a) the aqueous oral environment stimulates sodium bioglass ions exchange with hydrogen ions (H+); b) calcium ions (Ca2+) in the particles as well as phosphate ions (PO43−) are released from the biomaterial; c) a localized pH rise will allow the precipitates of calcium and phosphate ions, together with the ions from saliva, to form a calcium phosphate (Ca–P) layer on the hard tissue (lesion surface); d) The silica network from bioactive glass can react with hydroxyl ions (OH−) from aqueous solution and form soluble silanol compounds; e) experimental observations indicate that the increase in Ca and P content would induce a decrease in silicon content. Finally, the newly formed layer displays good resistance to abrasion and transforms to a hydroxyapatite layer, which is structurally like those of original enamel and dentine [36,37,38,39]. It is important to keep in mind that this cycle has a continuum. Hence, it further increases calcium and phosphate ion concentrations and leads to the precipitation of calcium phosphate on the silica-rich layer [38].
Bioglass® 45S5 was the first commercial bioglass. Later, other formulations were developed: Class A and Class B, with and without sodium. Novamin® is a calcium–sodium–phosphatesilicate glass also described as amorphous sodium calcium phosphosilicate (SCPS) that has the ability of a consistently release calcium ions. To increase remineralization performance, a bioglass combined with fluoride and high phosphate content was developed: BiominF® [39]. This product seems to form a more stable and resistant layer. Fluoride is particularly relevant in improving the bioactivity for enamel protection by the formation of the more acid-resistant fluorapatite, rather than hydroxyapatite [39]. In addition, fluoride-bioglass may enhance the remineralization of dentin and decrease the risk of dentin-matrix degradation. A further beneficial effect of bioglass is the antimicrobial activity of this material.
Conversely to other technologies that operate in an alkaline milieu, REFIX dental regeneration technology is an acidified bioactive complex produced mainly from compounds containing silica and phosphates [7,12]. Upon contact with the oral environment, they ionize, and these particles bind to the tooth structure, capturing calcium particles available in the oral environment. The interaction of these elements forms layers of hydroxyapatite enriched with silicon. REFIX technology has proven to be effective in tooth remineralization/regeneration, depositing minerals in areas deficient in mineral structures. This action reduces tooth sensitivity, prevents dental caries and erosive tooth wear [40].
The evidence supporting the efficacy of these technologies for enamel repair and reducing dentin hypersensitivity is increasing. For instance, a recent clinical study comparing NOVAMIN (Sensodyne Repair & Protect GlaxoSmithKline, Philadelphia, PA, USA) and REFIX Technology (Regenerador Sentitive, DentalClean, Londrina, PR, Brazil) showed that both products reduced the tooth hypersensitivity reported by the volunteers [41]. Similar results were also observed in pilot study performed with participants that report dentin hypersensitivity (DH) caused by root surface exposure or periodontal treatment [42].
NR5™ technology is known for its combination of two compounds – sodium phosphate and calcium silicate. When they encounter the tooth surface during brushing, the combination of these compounds fosters the formation of a new mineral layer of hydroxyapatite, depositing minerals in areas lacking mineral structures. This action reduces tooth sensitivity and prevents tooth decay and erosion [43]. The producers of the NR5™ technology claim that, when the REGENERATE Advanced Toothpaste is used in combination with the serum, it boosts the toothpaste’s effectiveness, enhancing the power of enamel regeneration [4,44].
1.3. Rationale for the Review – Guiding Question
Silica is an impressive, versatile compound that can be modified for many purposes in toothpastes. Recently, a modified silica surface produced a promising mucoadhesive compound that may increase the retention of toothpaste particles in the oral cavity [4].
Until now, there have been few publications concerning the effect of bioactive silicon on tooth enamel. Silicon and silica, along with calcium, phosphates, and fluoride induce the remineralization of demineralized tooth enamel and dentine in vitro [4,39,40,41,42,43].
Therefore, this issue needs updated information regarding the positive points and potential limitations regarding the silicon-, silica-, and silicate-toothpastes aiming for dental remineralization and other therapeutic uses. Thus, the guiding question of the review can be summarized as: “Is there supporting evidence about silicon-, silica-, and silicate-toothpastes efficacy for remineralization and/or enamel repair of teeth?”
2. Material and Methods
This scoping review was performed following the 2020 PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines for the Scoping Reviews Checklist [48]. This review was registered with the OSF Registries (registration DOI: https://doi.org/10.17605/OSF.IO/U2B8D, accessed on August 12th,2024).
A literature research of papers published in the last 10 years was carried out on PubMed and Scopus (July 21st,2024), using the following search strategy:
“silicon” OR “silica” OR “silicate”
AND
“toothpaste” OR “dental gel”
AND
“bioactive” OR “biomimetics”
AND
“teeth”.
It is important to point out that only articles shedding light on bioactive toothpastes/dentifrices/gels were included. Articles presenting results about hydroxyapatites in these products were excluded unless a combination with silicon, silica, and/or silicate was present. The primary target was enamel-dentin repair. Additionally, relevant literature was hand-searched and included if the criteria for testing these silicon/silica/silicate technologies for enamel/dentin repair were tested for: “dental caries”; “molar incisor hypomineralization”; “dentine hypersensitivity”; “dental erosion”.
All types of studies were included (reviews, systematic reviews and meta-analyses). However, the final reading focused on the therapeutic potential of these technologies in two major categories: A: “in vitro” or “laboratory studies” and B: “in vivo” studies, or general clinical studies, or clinical trials.
A total of 331 studies were imported from screening (148 from PubMed and 183 from Scopus). After the removal of articles related to dental materials and implants or other issues (169) and duplicates (106 studies). F.C.S. and F.V. screened 56 articles (title and abstract). The final number of studies retrieved from the query was 27 (Figure 1). Twelve articles had their full text read by N.L.S.F. and A.F.B.O. in group A (in vitro studies). A.C.C.G. and G.B.M read 15 full-text articles in group B (in vivo, clinical trials).
3. Results
Qualitative and quantitative analyses were carried out considering the therapeutic potential of silicon, silica and silicates in toothpastes. Technical and methodological strengths and weaknesses were also explored. However, there are significant methodological differences that need to be considered. From 12 in vitro experiments half of them used human enamel or dentin specimens, the other half used bovine blocks for pH cycling and subsequently characterization by different techniques (e.g.,: Scanning Electron Microscopy-SEM imaging, EDX elemental analysis, surface microhardness and roughness). The technologies investigated included also non silicon-, silica-toothpastes, such as: arginine sodium monofluorophosphate and casein phosphopeptide-amorphous calcium phosphate (CCP-ACP).
Among the in vivo clinical studies (n=15), 11 were randomized clinical trial (RCT). Only two of these RCTs were testing the effect on white spot lesions whereas the others aimed the reduction of pain due to dentin hypersensitivity.
4. Discussion
The lack of consensus on terminologies related to these Si-based technologies for remineralizing dental hard tissues was a survey problem since hydrated silica is a common component of many toothpastes. As a result, the search query used for this scoping review eventually selected studies testing abrasives. In addition, remineralization is frequent surveyed issue of research related to bioactive materials for repairing or regenerating bones and teeth.
A similar commercial and academic terminology may be useful to encompass technologies using silicon (Si), silica (SiO2) and silicate (Si2O5)2n-n in toothpastes. This could facilitate communication and differentiate these products from regular hydrated silica. This approach is very important since the borderline between biomimetic products and F-boosters is increasingly blurred [9]. Accordingly, a parallel outcome of this scoping review is the proposal for using the term “bioactive Si-toothpaste” for biomimetic or F-boosters technologies for enamel repair that use silicon (Si), silica (SiO2) and silicate (Si2O5)2n-n in toothpastes.
The major technologies investigated in the 27 articles selected for this review were: Novamin®, BiominF®, REFIX Technology and NR5™technology (with and without serum booster).
In vitro study articles evaluating NOVAMIN and REFIX technologies followed similar methodologies, involving the preparation of bovine enamel blocks, demineralization to create caries-like lesions, pH cycling with treatment based on different toothpastes, and subsequent analysis with surface microhardness, scanning electron microscopy, and EDS [4].
However, if we take a closer look at the methodological aspects, some differences are worth highlighting. While some researchers [45,46] used human teeth, others [4,12,40,47] used bovine teeth. This may influence the comparability of the results due to differences in the composition and structure of human and bovine teeth. However, the polishing and sample preparation procedures are similar between the articles using bovine teeth, ensuring a uniform surface for the tests.
Most of the articles used demineralization methods with acetate solutions to simulate caries lesions and pH cycling, ensuring controlled conditions for evaluating the effects of the dentifrices tested. However, some studies used brushing methods associated with pH cycling, which varied between manual brushing [45] and electric brushing [12,40], which may impact the effectiveness of the remineralization and protection effects observed.
For sample analysis and characterization, scanning electron microscopy (SEM) and EDS are the most common methods, allowing a detailed comparison of the morphology and chemical composition of the samples after treatment. However, quantitative methods such as surface microhardness and enamel surface roughness [4,46] are important and deserve to be highlighted, as they provide more robust evidence on the clinical applicability of these composites.
Methodological differences are crucial for interpreting the results of each study, as they directly influence conclusions about the effectiveness of the technologies evaluated and the comparison of data [46]. When it comes to methodological rigor, we must consider certain aspects, such as clarity and detail of the methodology, control of variables, reproducibility, data analysis and interpretation, validity, and reliability of the methods used. Thus, the studies [4,12,40,47], demonstrate greater methodological rigor due to the following points: preparation and polishing of detailed samples, which ensures uniformity of the specimens; standardized procedures for demineralization and pH cycling, ensuring controlled conditions for the creation of caries lesions; use of electric brushing [12,40], as it reduces variability and improves the reproducibility of results; SEM and EDS analyses, offering a detailed characterization of the morphology and chemical composition of dental tissues after treatments [47].
The main differences found in the results of the studies evaluated are related to the effectiveness of the different toothpastes in remineralizing enamel and forming new “layers” of minerals. Each study observed variations, depending on the compounds tested, in the presence of elements such as silicon and fluoride, as well as in the hardness and roughness properties of the enamel and dentin surfaces after treatment.
REFIX technology induces the formation of a mineralized layer on both enamel and dentin. On enamel, this layer is approximately 6 µm thick and forms on the surface after pH cycling. In dentin, after brushing with the same toothpaste, a mineralized layer is formed, only less thick, up to 3 µm. After 7 days of treatment, partial obliteration of the dentinal tubules is observed [40].
In terms of erosion prevention, enamel samples treated with REFIX exhibit a smoother surface and resistance to subsequent erosive challenges. Elemental mapping analyses with EDS indicate that there are no significant changes in the chemical elements present on the surface after the erosive challenge, confirming the robustness of the layer formed [47].
NOVAMIN technology, in turn, induces the formation of a mineralized layer both on the dentin surface and inside the dentin tubules. The mechanism of action suggested for this dentifrice is through the release of calcium and phosphate when in contact with saliva, promoting remineralization and obliteration of the dentinal tubules [45].
However, the results presented in the studies show that NOVAMIN technology was less effective in forming a new mineral layer on the surface enamel compared to REFIX. In addition, there was a significant reduction in the percentage weight of calcium in NOVAMIN-treated samples after erosive challenges, indicating a lower resistance and stability of the mineral content.
In short, depending on what the study sets out to analyze, REFIX stands out in terms of enamel surface remineralization and erosion prevention. However, when applied to dentin, both technologies promote obliteration of the dentinal tubules, which can help control tooth sensitivity. However, the mineral deposition provided by REFIX forms a thicker and more resistant layer over time.
All in vitro studies support that a net mineral gain is achieved and an enamel repair is also observed depending on the technique used. These in vitro investigations support the beneficial effect of these bioactive-Si-toothpastes is related to the potential control of dental caries lesions, erosive tooth wear [4,7,12,40,43,45,46,47,48,49,50].
The clinical efficacy of various bioactive Si-toothpastes toothpastes has been extensively studied, with a particular emphasis on formulations containing sodium calcium phosphosilicate (SCPS) and related technologies. Clinical studies have consistently demonstrated the ability of SCPS to occlude dentinal tubules, thereby alleviating pain associated with dentin hypersensitivity (DH). For instance, Chałas et al. (2015) [51] and Zang et al. (2016)[52] observed significant pain reduction with smaller SCPS particles, which exhibited greater efficiency in tubule occlusion. Similarly, Sufi et al. (2016) [53] reported a marked reduction in DH with the use of toothpastes containing 5% SCPS. Hall et al. (2017) [54] further confirmed the superiority of SCPS over arginine/calcium carbonate in long-term treatments, although a work performed later found no significant differences when comparing smaller SCPS particles (2.5%) to arginine/carbonate formulations [55].
Studies by Patel et al. (2019) [16] and Bhowmik et al. (2021) [56] have also highlighted the efficacy of bioglass-containing toothpastes in reducing DH, particularly the remineralizing effect of BioMin-F compared to popular brands like Colgate Sensitive Pro-Relief and Sensodyne Rapid Action [57]. In a clinical comparison of four different interventions for DH reduction, Majji & Murthy (2016) [58] concluded that SCPS-based pastes were the most effective, a finding consistent with other investigation that demonstrated significant DH reduction using a toothpaste containing REFIX technology [12].
Additionally, Seong et al. (2020) [10] conducted a randomized controlled trial evaluating a toothpaste with calcium silicate and sodium phosphate, finding a significant pain reduction compared to a control group using only fluoridated toothpaste. Gallob et al. (2017) [59] also supported the efficacy of experimental toothpastes containing silica, silicate, and silicon in reducing DH.
In the treatment of white spot lesions, few clinical studies explored bioglass-based technologies, showing that these formulations not only alleviate DH but also promote the remineralization of enamel, particularly in orthodontic patients [60,61]. A further study demonstrated that combining NovaMin® with a fluoridated toothpaste significantly improved the remineralization of white lesions, highlighting the potential of sodium monofluorophosphate (SMFP) to enhance fluoride therapy’s efficacy [62].
Surprisingly, this review retrieved no clinical studies about these bioactive Si-toothpastes for DH associated with molar incisor hypomineralization (MIH). MIH is a developmental enamel defect primarily diagnosed in childhood and adolescence, which can lead to compromised function of the affected teeth [63]. Characterized by increased porosity and dentin tubule exposure [64], this defect can result in post-eruptive fractures, dentin hypersensitivity, and pain. These conditions can significantly impact patients’ oral health-related quality of life (OHRQoL) [65,66], including difficulties with mastication, particularly when consuming hot or cold foods and beverages [67]. Moreover, MIH can lead to psychosocial challenges such as decreased self-esteem, embarrassment when smiling, and difficulties with socialization [68].
Given these challenges, silica-, silicate-, and silicon-based technologies have shown promise in dental remineralization and the reduction of dentin hypersensitivity through dentin tubule obliteration. Therefore, these materials can alleviate pain, reduce dentin hypersensitivity, and, in turn, a negative impact on OHRQoL.
In vitro and in vivo studies are currently underway to evaluate the efficacy of these remineralizing agents in teeth with MIH, particularly in children. These studies aim to assess the potential of toothpastes containing these technologies as adjuncts in the treatment and management of dentin hypersensitivity and their impact on the oral health-related quality of life of these patients.
5. Conclusions
In conclusion, clinical studies support the effectiveness of SCPS, bioglass, and innovative technologies like REFIX in occluding dentinal tubules and remineralizing enamel, offering long-lasting relief from DH. The choice of treatment should be tailored to the patient’s specific needs and the properties of the desensitizing agent used. Finally, it can be also concluded that there is a consistent support of evidence confirming the beneficial effects of using silicon-, silica-, and silicate-toothpastes for enamel repair and remineralization. The mechanisms of action may differ between the available technologies using silicon-, silica-, and silicate-bioactive materials (bioactive-Si-materials). However, there is also a lack of long-lasting clinical studies exploring this issue. Most of the clinical studies confirm the effectiveness of these products for dentin hypersensitivity (DH). Other oral health conditions can also benefit from these technologies. The combination of silicon and derivates with other strategies will probably be the next frontier for new bioactive-Si-toothpastes on the market.
Acknowledgments
We acknowledge the support of the Post graduation Program in Dentistry at the Federal University of Paraíba (UFPB) and the FORP/USP Graduate Program in Pediatric Dentistry for the academic support for N.L.S.F. (UFPB) and S.C. C.G. and G.B. M. (USP).
Author Contributions
Conceptualization, F.V.V. and F.C.S.; methodology, F.V.V., F.C.S., A.F.O, N.L.S.F., A.C. and G.; data curation, A.F.O., A.F.O, N.L.S.F., A.C. and G.; writing-original draft, F.V.V., F.C.S., A.F.O, N.L.S.F., A.C. and G.; review & editing, M.B. , M.P. and P.H.P.D.; supervision, F.V.V. and F.C.S. All authors have read and agreed to the published version of the manuscript.
Conflicts of Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
- Pitts, N.B.; Zero, D.T.; Marsh, P.D.; Ekstrand, K.; Weintraub, J.A.; Ramos-Gomez, F.; Tagami, J.; Twetman, S.; Tsakos, G.; Ismail, A. Dental caries. Nature reviews. Disease primers 2017, 3, 17030. [Google Scholar] [CrossRef] [PubMed]
- Fontana, M. Enhancing fluoride: clinical human studies of alternatives or boosters for caries management. Caries Res 2016, 50 Suppl 1, 22–37. [Google Scholar] [CrossRef]
- Sampaio, F.C.; Bonecker, M.; Paiva, S.M.; Martignon, S.; Ricomini Filho, A.P.; Pozos-Guillen, A.; Oliveira, B.H.; Bullen, M.; Naidu, R.; Guarnizo-Herreno, C.; et al. Dental caries prevalence, prospects, and challenges for Latin America and Caribbean countries: a summary and final recommendations from a Regional Consensus. Braz Oral Res 2021, 35, e056. [Google Scholar] [CrossRef]
- Fernandes, N.L.S.; Silva, J.; de Sousa, E.B.G.; D’Alpino, P.H.P.; de Oliveira, A.F.B.; de Jong, E.J.; Sampaio, F.C. Effectiveness of fluoride-containing toothpastes associated with different technologies to remineralize enamel after pH cycling: an in vitro study. BMC oral health 2022, 22, 489. [Google Scholar] [CrossRef]
- Parker, A.S.; Patel, A.N.; Al Botros, R.; Snowden, M.E.; McKelvey, K.; Unwin, P.R.; Ashcroft, A.T.; Carvell, M.; Joiner, A.; Peruffo, M. Measurement of the efficacy of calcium silicate for the protection and repair of dental enamel. J Dent 2014, 42 Suppl 1, S21–29. [Google Scholar] [CrossRef]
- Joiner, A.; Schäfer, F.; Naeeni, M.M.; Gupta, A.K.; Zero, D.T. Remineralisation effect of a dual-phase calcium silicate/phosphate gel combined with calcium silicate/phosphate toothpaste on acid-challenged enamel in situ. J Dent 2014, 42, S53–S59. [Google Scholar] [CrossRef] [PubMed]
- Vilhena, F.V.; Grecco, S.D.S.; Gonzalez, A.H.M.; D’Alpino, P.H.P. Regenerative and protective effects on dental tissues of a fluoride-silicon-rich toothpaste associated with a calcium booster: an in vitro study. Dent J (Basel) 2023, 11. [Google Scholar] [CrossRef]
- Pandya, M.; Diekwisch, T.G.H. Enamel biomimetics-fiction or future of dentistry. Int J Oral Sci 2019, 11, 8. [Google Scholar] [CrossRef] [PubMed]
- Philip, N. State of the art enamel remineralization systems: the next frontier in caries management. Caries Res 2019, 53, 284–295. [Google Scholar] [CrossRef]
- Seong, J.; Newcombe, R.G.; Matheson, J.R.; Weddell, L.; Edwards, M.; West, N.X. A randomised controlled trial investigating efficacy of a novel toothpaste containing calcium silicate and sodium phosphate in dentine hypersensitivity pain reduction compared to a fluoride control toothpaste. J Dent 2020, 98, 103320. [Google Scholar] [CrossRef]
- Meyer, F.; Amaechi, B.T.; Fabritius, H.O.; Enax, J. Overview of calcium phosphates used in biomimetic oral care. Open Dent J, 2018, 12, 406–423. [Google Scholar] [CrossRef] [PubMed]
- Vilhena, F.V.; de Oliveira, S.M.L.; Matochek, M.H.M.; Tomaz, P.L.S.; Oliveira, T.S.; D’Alpino, P.H.P. Biomimetic Mechanism of Action of Fluoridated Toothpaste Containing Proprietary REFIX Technology on the Remineralization and Repair of Demineralized Dental Tissues: An In Vitro Study. Eur J Dent 2021, 15, 236–241. [Google Scholar] [CrossRef] [PubMed]
- Vallet-Regí, M.; Arcos, D. Silicon substituted hydroxyapatites. A method to upgrade calcium phosphate based implants. J Mater Chem 2005, 15, 1509–1516. [Google Scholar] [CrossRef]
- Ten Cate, J.M.; Buzalaf, M.A.R. Fluoride Mode of Action: Once There Was an Observant Dentist. J Dent Res 2019, 98, 725–730. [Google Scholar] [CrossRef] [PubMed]
- Gibson, I.R.; Huang, J.; Best, S.M.; Bonfield, W. Enhanced in vitro cell activity and surface apatite layer formation on novel silicon-substituted hydroxyapatites. In Proceedings of the 12th International Symposium on Ceramics in Medicine, Nam, Japan; 1999. [Google Scholar]
- Patel, N.; Best, S.M.; Bonfield, W.; Gibson, I.R.; Hing, K.A.; Damien, E.; Revell, P.A. A comparative study on the in vivo behavior of hydroxyapatite and silicon substituted hydroxyapatite granules. Journal of materials science. Materials in medicine 2002, 13, 1199–1206. [Google Scholar] [CrossRef]
- Luhrs, A.K.; Geurtsen, W. The application of silicon and silicates in dentistry: a review. Progress in molecular and subcellular biology 2009, 47, 359–380. [Google Scholar] [CrossRef] [PubMed]
- Lippert, F. An introduction to toothpaste - its purpose, history and ingredients. Monogr Oral Sci 2013, 23, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Thalakiriyawa, D.S.; Dissanayaka, W.L. Advances in Regenerative Dentistry Approaches: An Update. Int Dent J 2024, 74, 25–34. [Google Scholar] [CrossRef]
- Luo, X.; Niu, J.; Su, G.; Zhou, L.; Zhang, X.; Liu, Y.; Wang, Q.; Sun, N. Research progress of biomimetic materials in oral medicine. Journal of biological engineering 2023, 17, 72. [Google Scholar] [CrossRef]
- Volponi, A.A.; Zaugg, L.K.; Neves, V.; Liu, Y.; Sharpe, P.T. Tooth repair and regeneration. Curr Oral Health Rep 2018, 5, 295–303. [Google Scholar] [CrossRef]
- Mann, S. The biomimetics of enamel: a paradigm for organized biomaterials synthesis. Ciba Foundation symposium 1997, 205, 261–269, discussion 269-274. [Google Scholar]
- Palmer, L.C.; Newcomb, C.J.; Kaltz, S.R.; Spoerke, E.D.; Stupp, S.I. Biomimetic systems for hydroxyapatite mineralization inspired by bone and enamel. Chem Rev 2008, 108, 4754–4783. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.; Yoon, M.; Choi, K.Y. Approaches for Regenerative Healing of Cutaneous Wound with an Emphasis on Strategies Activating the Wnt/beta-Catenin Pathway. Adv Wound Care (New Rochelle) 2022, 11, 70–86. [Google Scholar] [CrossRef]
- Braga, R.R.; Habelitz, S. Current developments on enamel and dentin remineralization. Curr Oral Health Rep 2019, 6, 257–263. [Google Scholar]
- Moradian-Oldak, J.; George, A. Biomineralization of Enamel and Dentin Mediated by Matrix Proteins. J Dent Res 2021, 100, 1020–1029. [Google Scholar] [CrossRef]
- George, A.; Veis, A. Phosphorylated proteins and control over apatite nucleation, crystal growth, and inhibition. Chem Rev 2008, 108, 4670–4693. [Google Scholar] [CrossRef] [PubMed]
- Moradian-Oldak, J. Protein-mediated enamel mineralization. Frontiers in bioscience 2012, 17, 1996–2023. [Google Scholar] [CrossRef]
- Singer, L.; Fouda, A.; Bourauel, C. Biomimetic approaches and materials in restorative and regenerative dentistry: review article. BMC oral health 2023, 23, 105. [Google Scholar] [CrossRef]
- Devadiga, D.; Shetty, P.; Hegde, M.N.; Reddy, U. Bioactive remineralization of dentin surface with calcium phosphate-based agents: An in vitro analysis. Journal of conservative dentistry : JCD 2022, 25, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Darvell, B.W.; Smith, A.J. Inert to bioactive - A multidimensional spectrum. Dent Mater 2022, 38, 2–6. [Google Scholar] [CrossRef]
- Hulbert, S.F.; Hench, L.L.; Forbers, D.; Bowman, L.S. History of bioceramics. Ceramics International 1982, 8, 131–140. [Google Scholar] [CrossRef]
- Al-Harbi, N.; Mohammed, H.; Al-Hadeethi, Y.; Bakry, A.S.; Umar, A.; Hussein, M.A.; Abbassy, M.A.; Vaidya, K.G.; Al Berakdar, G.; Mkawi, E.M.; et al. Silica-Based Bioactive Glasses and Their Applications in Hard Tissue Regeneration: A Review. Pharmaceuticals 2021, 14, 75. [Google Scholar] [CrossRef]
- Prasad, P.S.; Pasha, M.B.; Rao, R.N.; Rao, P.V.; Madaboosi, N.; Ozcan, M. A Review on Enhancing the Life of Teeth by Toothpaste Containing Bioactive Glass Particles. Curr Oral Health Rep 2024, 11, 87–94. [Google Scholar] [CrossRef]
- Greenspan, D. Bioglass at 50 – A look at Larry Hench’s legacy and bioactive materials. Biomedical Glasses 2019, 5, 178–184. [Google Scholar] [CrossRef]
- Dai, L.L.; Mei, M.L.; Chu, C.H.; Lo, E.C.M. Mechanisms of Bioactive Glass on Caries Management: A Review. Materials (Basel) 2019, 12. [Google Scholar] [CrossRef]
- El-Wassefy, N.A. Remineralizing effect of cold plasma and/or bioglass on demineralized enamel. Dent Mater J 2017, 36, 157–167. [Google Scholar] [CrossRef] [PubMed]
- Ramadoss, R.; Padmanaban, R.; Subramanian, B. Role of bioglass in enamel remineralization: Existing strategies and future prospects-A narrative review. Journal of biomedical materials research. Part B, Applied biomaterials 2022, 110, 45–66. [Google Scholar] [CrossRef]
- Skallevold, H.E.; Rokaya, D.; Khurshid, Z.; Zafar, M.S. Bioactive Glass Applications in Dentistry. Int J Mol Sci 2019, 20. [Google Scholar] [CrossRef]
- Vilhena, F.V.; Lonni, A.A.S.G.; D’Alpino, P.H.P. Silicon-enriched hydroxyapatite formed induced by REFIX-based toothpaste on the enamel surface. Braz Dent Sci 2021, 24, 1–7. [Google Scholar] [CrossRef]
- Alonso, R.C.B.; Oliveira, L.d.; Silva, J.A.B.; Santos, W.B.B.d.; Ferreira, L.R.d.S.L.; Guiraldo, R.D.; Vilhena, F.V.; D’Alpino, P.H.P. Effectiveness of Bioactive Toothpastes against Dentin Hypersensitivity Using Evaporative and Tactile Analyses: A Randomized Clinical Trial. Oral 2024, 4, 36–49. [Google Scholar] [CrossRef]
- Zangrando, M.S.R.; Silva, G.F.F.; Bigotto, M.L.B.; Cintra, F.M.R.N.; Damante, C.A.; Sant’Ana, A.C.P.; Vilhena, F.V. Blocking tubules technologies for dentin hypersensitivity in periodontal patients – pilot study. Res Soc Dev 2021, 10, e35101320398. [Google Scholar] [CrossRef]
- Moras, C.G.; Acharya, S.R.; Adarsh, U.K.; Unnikrishnan, V.K. Regenerative biomineralization potential of commercially available remineralizing agents as a preventive treatment approach for tooth erosion - An in vitro laser-induced breakdown spectroscopy analysis. Journal of conservative dentistry : JCD 2023, 26, 165–169. [Google Scholar] [CrossRef]
- Rahman, B.; El-Damanhoury, H.M.; Sheela, S.; Ngo, H.C. Effect Of Calcium Silicate, Sodium Phosphate, and Fluoride on Dentinal Tubule Occlusion and Permeability in Comparison to Desensitizing Toothpaste: An In Vitro Study. Operative dentistry 2021, 46, 641–649. [Google Scholar] [CrossRef]
- Athanasiadou, D.; Eymael, D.; Hajhamid, B.; Carneiro, K.M.M.; Prakki, A. Chemical and Ultrastructural Characterization of Dentin Treated with Remineralizing Dentifrices. Journal of functional biomaterials 2024, 15. [Google Scholar] [CrossRef]
- Tomaz, P.L.S.; Sousa, L.A.; Aguiar, K.F.; Oliveira, T.S.; Matochek, M.H.M.; Polassi, M.R.; D’Alpino, P.H.P. Effects of 1450-ppm fluoride-containing toothpastes associated with boosters on the enamel remineralization and surface roughness after cariogenic challenge. Eur J Dent 2020, 14, 161–170. [Google Scholar] [CrossRef]
- Fernandes, N.L.S.; Juliellen, L.D.C.; Andressa, F.B.O.; D’Alpino, H.P.P.; Sampaio, C.F. Resistance against erosive challenge of dental enamel treated with 1,450-PPM fluoride toothpastes containing different biomimetic compounds. Eur J Dent 2021, 15, 433–439. [Google Scholar] [CrossRef]
- Poggio, C.; Gulino, C.; Mirando, M.; Colombo, M.; Pietrocola, G. Preventive effects of different protective agents on dentin erosion: An in vitro investigation. J Clin Exp Dent 2017, 9, e7–e12. [Google Scholar] [CrossRef] [PubMed]
- Altan, H.; Goztas, Z.; Kahraman, K.; Kus, M.; Tosun, G. Inhibition Effects of Different Toothpastes on Demineralisation of Incipient Enamel Lesions. Oral Health Prev Dent 2019, 17, 179–185. [Google Scholar] [CrossRef]
- El-Damanhoury, H.M.; Elsahn, N.A.; Sheela, S.; Bastaty, T. In Vitro Enamel Remineralization Efficacy of Calcium Silicate-Sodium Phosphate-Fluoride Salts versus NovaMin Bioactive Glass, Following Tooth Whitening. Eur J Dent 2021, 15, 515–522. [Google Scholar] [CrossRef] [PubMed]
- Chalas, R.; Wojcik-Checinska, I.; Zamoscinska, J.; Bachanek, T. Assessment of Pain Intensity in Patients with Dentin Hypersensitivity After Application of Prophylaxis Paste Based on Calcium Sodium Phosphosilicate Formula. Medical science monitor : international medical journal of experimental and clinical research 2015, 21, 2950–2955. [Google Scholar] [CrossRef] [PubMed]
- Zang, P.; Parkinson, C.; Hall, C.; Wang, N.; Jiang, H.; Zhang, J.; Du, M. A Randomized Clinical Trial Investigating the Effect of Particle Size of Calcium Sodium Phosphosilicate (CSPS) on the Efficacy of CSPS-containing Dentifrices for the Relief of Dentin Hypersensitivity. J Clin Dent 2016, 27, 54–60. [Google Scholar]
- Sufi, F.; Hall, C.; Mason, S.; Shaw, D.; Milleman, J.; Milleman, K. Efficacy of an experimental toothpaste containing 5% calcium sodium phosphosilicate in the relief of dentin hypersensitivity: An 8-week randomized study (Study 2). Am J Dent 2016, 29, 101–109. [Google Scholar] [PubMed]
- Hall, C.; Mason, S.; Cooke, J. Exploratory randomised controlled clinical study to evaluate the comparative efficacy of two occluding toothpastes - a 5% calcium sodium phosphosilicate toothpaste and an 8% arginine/calcium carbonate toothpaste - for the longer-term relief of dentine hypersensitivity. J Dent 2017, 60, 36–43. [Google Scholar] [CrossRef]
- Fu, Y.; Sufi, F.; Wang, N.; Young, S.; Feng, X. An Exploratory Randomised Study to Evaluate the Efficacy of an Experimental Occlusion-based Dentifrice in the Relief of Dentin Hypersensitivity. Oral Health Prev Dent 2019, 17, 107–115. [Google Scholar] [CrossRef]
- Bhowmik, E.; Pawar Chandrashekhar, D.; Sharma Hareesha, M. Comparative evaluation of fluorinol and calcium sodium phosphosilicate-containing toothpastes in the treatment of dentin hypersensitivity. Int J Dent Hyg 2021, 19, 421–428. [Google Scholar] [CrossRef] [PubMed]
- Arshad, S.; Zaidi, S.J.A.; Farooqui, W.A. Comparative efficacy of BioMin-F, Colgate Sensitive Pro-relief and Sensodyne Rapid Action in relieving dentin hypersensitivity: a randomized controlled trial. BMC oral health 2021, 21, 498. [Google Scholar] [CrossRef]
- Majji, P.; Murthy, K.R. Clinical efficacy of four interventions in the reduction of dentinal hypersensitivity: A 2-month study. Indian journal of dental research : official publication of Indian Society for Dental Research 2016, 27, 477–482. [Google Scholar] [CrossRef]
- Gallob, J.; Sufi, F.; Amini, P.; Siddiqi, M.; Mason, S. A randomised exploratory clinical evaluation of dentifrices used as controls in dentinal hypersensitivity studies. J Dent 2017, 64, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Salah, R.; Afifi, R.R.; Kehela, H.A.; Aly, N.M.; Rashwan, M.; Hill, R.G. Efficacy of novel bioactive glass in the treatment of enamel white spot lesions: a randomized controlled trial. J Evid Based Dent Pract 2022, 22, 101725. [Google Scholar] [CrossRef]
- Hamdi, K.; Hamama, H.H.; Motawea, A.; Fawzy, A.; Mahmoud, S.H. Long-term evaluation of early-enamel lesions treated with novel experimental tricalcium silicate paste: A 2-year randomized clinical trial. Journal of esthetic and restorative dentistry : official publication of the American Academy of Esthetic Dentistry... [et al.] 2022, 34, 1113–1121. [Google Scholar] [CrossRef]
- Mollabashi, V.; Heydarpour, M.; Farhadifard, H.; Alafchi, B. DIAGNOdent pen quantification of the synergy of NovaMin(R) in fluoride toothpaste to remineralize white spot lesions in patients with fixed orthodontic appliances: A double-blind, randomized, controlled clinical trial. International orthodontics 2022, 20, 100632. [Google Scholar] [CrossRef] [PubMed]
- Michaelis, L.; Ebel, M.; Bekes, K.; Klode, C.; Hirsch, C. Influence of caries and molar incisor hypomineralization on oral health-related quality of life in children. Clin Oral Investig 2021, 25, 5205–5216. [Google Scholar] [CrossRef] [PubMed]
- Weerheijm, K.L. Molar incisor hypomineralisation (MIH). European journal of paediatric dentistry 2003, 4, 114–120. [Google Scholar] [PubMed]
- Jalevik, B.; Klingberg, G. Treatment outcomes and dental anxiety in 18-year-olds with MIH, comparisons with healthy controls - a longitudinal study. Int J Paediatr Dent 2012, 22, 85–91. [Google Scholar] [CrossRef]
- Jälevik, B.; Sabel, N.; Robertson, A. Can molar incisor hypomineralization cause dental fear and anxiety or influence the oral health-related quality of life in children and adolescents?—a systematic review. Eur Arch Paediatr Dent 2022, 23, 65–78. [Google Scholar] [CrossRef]
- Raposo, F.; de Carvalho Rodrigues, Ana C.; Lia, Érica N.; Leal, Soraya C. Prevalence of Hypersensitivity in Teeth Affected by Molar-Incisor Hypomineralization (MIH). Caries Res 2019, 53, 424–430. [CrossRef]
- Rodd, H.D.; Graham, A.; Tajmehr, N.; Timms, L.; Hasmun, N. Molar Incisor Hypomineralisation: Current Knowledge and Practice. Int Dent J 2021, 71, 285–291. [Google Scholar] [CrossRef]
Figure 1.
PRISMA 2020 flow diagram.
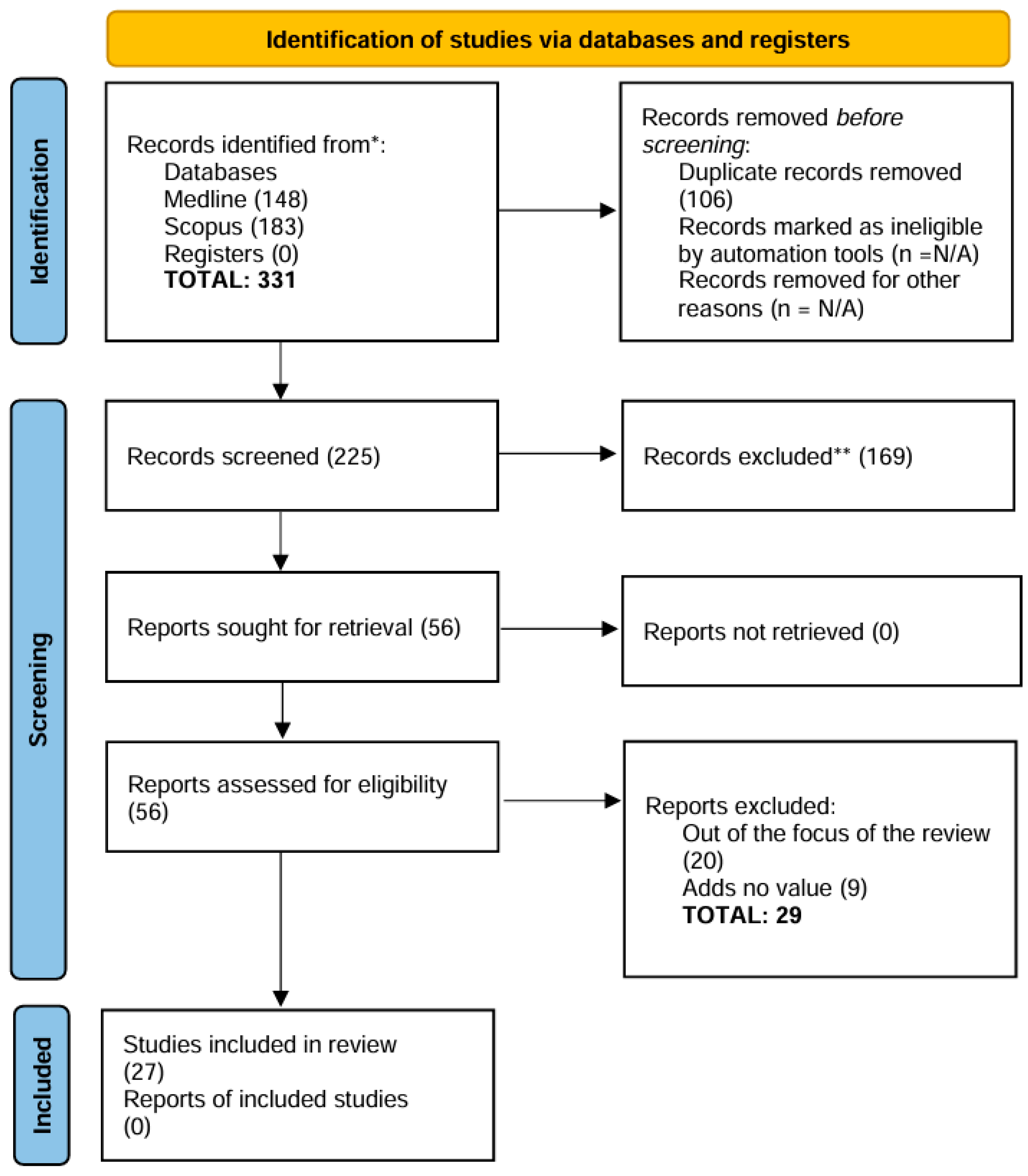

Table 1.
Characteristics of the included articles (in vitro studies).
| Author (Year) | Title | Study aim | Outcome Measurement | Sample Size (SS), Follow-Up (FU) | Material(s) or Technology (ies) Used |
Active agent(s) | Primary results |
|---|---|---|---|---|---|---|---|
| Poggio et al. (2017) | Preventive effects of different protective agents on dentin erosion: An in vitro investigation | To evaluate the preventive effects of different protective agents on dentin erosion caused by soft drinks | Percent weight loss, SEM imaging | SS: 70 human dentin specimens; FU: 32 minutes total immersion in Coca-Cola | Remin Pro, MI Paste Plus, Tooth Mousse, Biorepair, Biorepair Plus, Regenerate | Hydroxyapatite, CPP-ACP, CPP-ACPF, zinc hydroxyapatite, calcium silicate, sodium phosphate, sodium monofluorophosphate (1450 ppm fluoride) | Biorepair and Regenerate significantly reduced dentin weight loss, showing greater resistance to acid erosion compared to other agents. Remin Pro and MI Paste Plus showed results similar to the control group, while Tooth Mousse and Biorepair Plus increased dentin demineralization |
| Altan et al. (2019) | Inhibition effects of different toothpastes on demineralisation of incipient enamel lesions | To Evaluate the inhibitory effects of different toothpastes on demineralisation of incipient enamel lesions using a toothbrush simulator | Scanning Electron Microscopy (SEM) and Energy Dispersive Spectroscopy (EDX) with weight percentage of mineral changes (Ca, P, Na, Si) | 50 Human enamel blocks (n=10 per group) 5 days pH cycling |
Toothpaste with Arginine, Fluoride, CPP-ACP, and Bioactive Glass (NovaMin) | Arginine, Sodium Monofluorophosphate (Fluoride), CPP-ACP, Bioactive Glass (NovaMin) | All toothpaste groups showed a statistically significant increase in Ca and P compared to the control group (p < 0.05). CPP-ACP showed the highest increase in Ca and P. NovaMin increased Na and Si significantly |
| Vilhena et al. (2020) |
Biomimetic Mechanism of Action of Fluoridated Toothpaste Containing Proprietary REFIX Technology on the Remineralization and Repair of Demineralized Dental Tissues: An in vitro Study |
Characterize the mineral content and surface and cross-sectional morphology of enamel and dentin tissues treated with a 1450 ppm fluoride-containing toothpaste with REFIX technology. |
The surface and cross-sectional micromorphology were assessed using scanning electron microscopy (SEM). The ele- mental analyses (weight%) were determined with an energy-dispersive X-ray spectros- copy (EDS). |
Bovine enamel blocks (n=5) 7 days of pH cycling |
REFIX technology | Fluoride sodium, tetrasodium pyrophosphate |
REFIX technology remineralized and repaired the surface enamel effectively. Enamel with the toothpaste formed a silicon-enriched mineral layer on the enamel surface. The results were also consistent in the dentin, where the dentinal tubules were progressively occluded until there was complete occlusion after 7 days. |
| Tomaz et al. (2020) |
Effects of 1450-ppm Fluoride-containing Toothpastes Associated with Boosters on the Enamel Remineralization and Surface Roughness after Cariogenic Challenge |
Investigated the remineralization potential of 1450 ppm, fluoride-containing toothpastes containing different active remineralization agents after cariogenic challenge with pH cycling. |
Mean and percentage of surface hardness recovery (% SHR) were calculated. Surface enamel roughness (Ra) was also evaluated. The pH, %weight of particles, zeta potential, and polydispersity index of toothpaste slurries were also evaluated. |
Bovine enamel blocks (n=8/ per group) 7 days of pH cycling |
REFIX, NR-5, Candida Professional, Colgate Total 12 Daily Repair, Bianco Pro Clinical, Elmex Sensitive |
Sodium fluoride, Tricalcium phosphate (β-TCP), Sodium Monofuoro-phosphate, Oligopeptide-104, Calcium glycerophosphate, Triclosan, Arginine, Tetrasodium pyrophosphate, Calcium silicate and sodium phosphate |
The enamel subsurface was more effectively remineralized when treated with Bianco Pro Clinical, Elmex Sensitive, and Refix. The surface roughness was higher when the demineralized third was treated with Refix, and NR-5 and after the cariogenic challenge. |
| El-Damanhouryet al. (2021) | In Vitro Enamel Remineralization Efficacy of Calcium Silicate-Sodium Phosphate-Fluoride Salts versus NovaMin Bioactive Glass, Following Tooth Whitening | To evaluate the effect of in-office bleaching on enamel surface and compare the efficacy of Calcium Silicate-Sodium Phosphate-Fluoride (CS) and NovaMin bioactive glass (NM) in remineralizing bleached enamel | Surface Microhardness (Knoop Hardness Number (KHN), Surface Roughness, SEM/EDX Elemental Analysis | 40 human premolars (n=10) 7 days pH cycling |
Toothpaste with Novamin Bioactive Glass (NM), NR-5 (CS) and additional treatment with NR-5 boosting serum (CS+NR-5), |
silica, calcium sodium phosphosilicate (Novamin), sodium monofluorophosphate Calcium Silicate-Sodium Phosphate with Sodium Monofluorophosphate, hydrated silica (NR-5) |
CS and CS+NR-5 showed superior remineralization compared to NM. All remineralization agents increased hardness and decreased surface roughness after bleaching, but NM had a significantly higher surface roughness. CS and CS+NR-5 were more effective in restoring hardness and smoothness. |
| Fernandes et al. (2021) |
Resistance against Erosive Challenge of Dental Enamel Treated with 1,450-PPM Fluoride Toothpastes Containing Different Biomimetic Compounds |
This in vitro study aimed to characterize the superficial and subsurface morphology of dental enamel treated with fluoridated gels containing different bio- mimetic compounds after erosive challenge. |
The surface and cross-sectional micromorphology were assessed using scanning electron microscope (SEM). The elemental analyses (weight percent- age) were determined with an energy-dispersive X-ray spectroscopy (EDS). |
Bovine enamel blocks (n=5/ per group) 6 days of pH cycling |
NR-5, REFIX, Novamin. |
Fluoride sodium, triclosan, arginine, tetrasodium pyrophosphate Sodium monofuorophosphate, calcium silicate and sodium phosphate Calcium sodium phosphosilicate 5% |
Enamel treated with the product containing REFIX technology presented a smoother surface morphology compared to the other treatments. The higher resis- tance to the erosive challenge can be attributed to a silicon-enriched mineral layer formed on the enamel induced by the REFIX-based toothpaste. |
| Rahman et al. (2021) | Effect of Calcium Silicate, Sodium Phosphate, and Fluoride on Dentinal Tubule Occlusion and Permeability in Comparison to Desensitizing Toothpaste: An In Vitro Study | To compare the efficacy of a calcium silicate-, sodium phosphate-, and fluoride-based (CSSPF)toothpaste in promoting dentinal tubule occlusion and reducing dentin permeability against other commercial desensitizing toothpastes | Dye Percolation (DP%) test, SEM microphotographs, EDS elemental analysis | SS: 78 human dentin discs; FU: 7 days | Calcium silicate, sodium phosphate, fluoride (Regenerate Advanced); Bioactive Glass (NovaMin - Sensodyne Repair and Protect); Potassium Nitrate (Signal Sensitive Expert) | Sodium monofluorophosphate (1450 ppm fluoride), calcium silicate, trisodium phosphate, hydrated silica (Regenerate); Sodium monofluorophosphate (Sensodyne); Potassium nitrate, Sodium fluoride (Signal) | The Regenerate demonstrated the highest dentinal tubule occlusion and calcium deposition, significantly reducing dentin permeability. Novamin also showed effective tubule occlusion but with less calcium deposition compared to Regenerate. Signal Sensitive Expert, using potassium nitrate, showed effective tubule occlusion and permeability reduction, but was less effective overall compared to both Regenerate and Sensodyne in terms of calcium deposition and tubule occlusion. |
| Vilhena et al. (2021) |
Silicon-enriched hydroxyapatite formed induced by REFIX-based toothpaste on the enamel surface |
At characterizing the mineral content and filler particle morphology of a fluoridated toothpaste containing REFIX technology and the mineral content and the morphology of the enamel surface treated with this product. |
The surface morphology was assessed using scanning electron microscopy (SEM). The elemental analyses were performed using an energy-dispersive X-ray spectrometer (EDS). |
Bovine enamel blocks (n=5) 7 days of pH cycling |
REFIX technology | Fluoride sodium, tetrasodium pyrophosphate |
Elemental analysis of the toothpaste’s formulation demonstrated the presence of Si (silicon), Na (sodium), P (phosphorus), and F (fluorine), among others. We also detected a mineral layer that had formed on the treated enamel surface; the layer had a consistent uniform thickness of ~14 μm. |
| Fernandes et al. (2022) |
Efectiveness of fuoride-containing toothpastes associated with diferent technologies to remineralize enamel after pH cycling: an in vitro study |
To evaluate the efcacy of fuoride-containing toothpastes with diferent technologies to remineralize artifcial caries lesions in enamel. |
Surface microhardness recovery (%SMHR) and the fuorescence recovery (ΔFRE) with quantitative light-induced fuores- cence. The cross-sectional micromorphology of the enamel surface was also assessed using scanning electron micros- copy. Elemental analyses (weight%) were determined with an energy-dispersive X-ray spectrometer (EDS). |
Bovine enamel blocks (n=12/ per group) 6 days of pH cycling |
REFIX, NR-5, and NOVAMIN. |
Fluoride sodium, triclosan, arginine, tetrasodium pyrophosphate Sodium monofuorophosphate, calcium silicate and sodium phosphate Calcium sodium phosphosilicate 5% |
The Refix to recover the surface microhardness with a signifcantly lower mean of ΔFRE. Only Refix was able to promote the formation of a mineralized layer on the surface of enamel enriched with silicon on the surface. |
| Moras et al. (2023) | Regenerative Biomineralization Potential of Commercially Available Remineralizing Agents as a Preventive Treatment Approach for Tooth Erosion – An In Vitro Laser-Induced Breakdown Spectroscopy Analysis | To evaluate and compare the surface remineralization potential of SAP P11-4 (self-assembling peptide) and CSSP (calcium silicate plus sodium phosphate) on intact and demineralized enamel | Laser-induced breakdown spectroscopy (LIBS) to measure changes in Ca and P levels | SS:32 human enamel samples (16 intact, 16 demineralized) 30 days pH cycling |
SAP P11-4 (CURODONT™ PROTECT), CSSP (REGENERATE™ Enamel Science™ Advanced Toothpaste and Serum) | SAP P11-4, calcium silicate, sodium phosphate, fluoride | Both SAP P11-4 and CSSP significantly increased Ca and P levels in demineralized enamel. No significant difference in remineralization potential was observed between the two agents on intact and demineralized enamel. |
| Vilhena et al. (2023) | Regenerative and Protective Effects on Dental Tissues of a Fluoride–Silicon-Rich Toothpaste Associated with a Calcium Booster: An In Vitro Study | To characterize the regenerative and protective effects of a fluoride-silicon-rich toothpaste combined with a calcium booster on dental tissues | SEM imaging, Energy-Dispersive X-ray Spectroscopy (EDS), Elemental analysis (weight %) | SS: 5 bovine enamel and 5 bovine dentin blocks; FU: Immediate and after 5 days |
Fluoride-silicon-rich toothpaste with calcium booster - REFIX technology | Sodium Fluoride (1450 ppm), Silicon-rich compounds, Calcium Carbonate, Tricalcium Phosphate | The treatment formed a mineralized layer on enamel and dentin surfaces. After 5 days, the enamel had a 4-5 µm layer and dentin had a 7 µm layer. The calcium and silicon signals increased after immediate treatment, showing significant remineralization and occlusion of dentin tubules. |
| Athanasiadou et al. (2024) |
Chemical and Ultrastructural Characterization of Dentin Treated with Remineralizing Dentifrices |
Investigate dentin chemical and ultrastructural changes upon exposure to remineralizing dentifrices. | Atomic force microscopy (AFM), scanning electron microscopy (SEM) and energy-dispersive X-ray spectroscopy (EDX), transmission electron microscopy (TEM) and selected area electron diffraction (SAED). |
12 human dentin blocks (n= 3 per group) 14 days of toothbrushing |
REFIX, REFIX + Booster and Novamin | Fluoride sodium, tetrasodium pyrophosphate Calcium |
All evaluated dentifrices led to successful formation of hydroxyapatite and increased dentin stiffness. |
Table 2.
Characteristics of included articles (in vivo studies).
| Author (Year) | Title | Study design | Study aim | Outcome Measurement | Sample Size (SS), Follow-Up (FU) | Material(s) or Technology(ies) Used | Active agent(s) | Primary results |
|---|---|---|---|---|---|---|---|---|
| Chalas (2015) | Assessment of Pain Intensity in Patients with Dentin Hypersensitivity After Application of Prophylaxis Paste Based on Calcium Sodium Phosphosilicate Formula |
Longitudinal study | The clinical evaluation of the effectiveness in eliminating dentin hypersensitivity after a single application | The pain reaction of exposed dentine was induced by tactile and dehydrating stimuli, asking patients to assess the severity of pain on the VAS scale |
SS: 92 teeth with hypersensitivity FU: baseline and after 1 week |
NUPRO® Sensodyne® Prophylaxis Paste, Dentsply (NovaMin Formula) |
Calcium Sodium Phosphosilicate (CSPS) | In-office use of professional prophylactic paste with NovaMin formula noticeably reduces dentin hypersensitivity 1 week after application |
| Zang (2016) | A Randomized Clinical Trial Investigating the Effect of Particle Size of Calcium Sodium Phosphosilicate (CSPS) on the Efficacy of CSPS-containing Dentifrices for the Relief of Dentin Hypersensitivity |
Randomized clinical trial | To compare the efficacy in dentin hypersensitivity relief | The hypersensitivity was measured by tactile stimulus (Yeaple probe) and evaporative (air) stimulus (Schiff Sensitivity Scale, visual analogue scale) | SS: 133 subjects FU: baseline and after 1, 2, 4 and 8 weeks |
Vitryxx® (NaF and < 5% CSPS) NovaMin® (NaF or SMFP and 5% CSPS) Regular fluoride toothpaste |
Sodium fluoride and Calcium Sodium Phosphosilicate (CSPS) Sodium mono fluorophosphate (SMFP) and CSPS Fluoride |
The apparent absence of a positive treatment effect for the CSPS-containing dentifrices compared to the regular fluoride dentifrice is inconsistent with other previously reported efficacy studies for CSPS dentifrices |
| Majji (2016) | Clinical efficacy of four interventions in the reduction of dentinal hypersensitivity: A 2-month study | Randomized clinical trial | To compare the efficacy in reduction of dentinal hypersensitivity |
The patients’ dentin hypersensitivity scores for tactile, thermal, and evaporative stimuli were recorded on a visual analog scale | SS: 160 subjects FU: baseline, after 2 weeks and after 1 and 2 months |
Toothpaste with 5% potassium nitrate NovaMin toothpaste (calcium sodium phosphosilicate) Toothpaste with |
Potassium Nitrate Calcium Sodium Phosphosilicate (CSPS) Strontium chloride |
The four desensitizing kinds of toothpaste containing different active agents were effective in relieving dentinal hypersensitivity. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



