Submitted:
19 August 2024
Posted:
21 August 2024
You are already at the latest version
Abstract
It is documented that maternal diseases or treatments influence a newborn’s clinical status at birth; autoimmune diseases with circulating antibodies are often clinically expressed transiently in newborns due to the crossover of the specific IgG through the placenta during pregnancy. The offspring can inherit maternal genetic anomalies, but clinical expression usually becomes patent later in life. If prenatal medical history is not available or if signs or symptoms of a mother’s disease are revealed for the first time during pregnancy or postpartum, their effects on the newborn may be misattributed.
In this article, we present three cases of pregnant women, without any known pathology before or during pregnancy, who gave birth to very sick preterm newborns that required admission to the Neonatal Intensive Care Unit (NICU). The neonates’ complications were considered initially as consequences of prematurity or infection, but later investigations revealed transient autoimmune disease in two of the cases (myasthenia gravis and hyperthyroidism) and a severe form of thrombophilia in the third case. In all cases, mothers were asymptomatic and unaware of their subclinical disease.
Preemies’ diagnosis has contributed to the identification of their mothers’ pathology and adequate treatment was prescribed with favourable short- and long-term outcomes. In one of the cases (myasthenia gravis) both mother and child had associated infectious diseases in the perinatal period that complicated the clinical picture and created problems of diagnosis.
This article intends to emphasize the paramount importance of prenatal care, for both mother and newborn. Repeated medical visits and investigations throughout the pregnancy are a good opportunity to detect subclinical diseases or predispositions. As newborns usually develop non-specific signs, one should have experience and pay attention to differentiate among etiologies. Our paper takes a reversed approach to the usual medical diagnosis pathway: from infant to mother instead of mother towards the infant, proving that inter-speciality collaboration can work bi-directionally.
Keywords:
postpartum diagnosis
; maternal-infant disease
; asymptomatic diseases in pregnancy
; neonatal effect of maternal antibodies
; genetic diseases during pregnancy
1. Introduction
Prenatal information comprising maternal medical history, family history, pregnancy events and paraclinical investigations are of paramount importance for neonatologists. Neonatal clinical exam is known to offer poor or non-specific signs: respiratory distress, for example, is a common manifestation for both pulmonary and non-pulmonary conditions. Severe septic shock may often be signalled initially only by mottling of the skin. Extreme premature babies develop complications generated by the immaturity of their organs and systems and is difficult to distinguish between these and other associated co-morbidities. Worldwide medical guidelines for neonatology promote caution with interventions in extremely premature newborns, both for diagnosis and treatment, as these may be aggressive, stressful and imbalance their fragile organism. The concept of neurodevelopmental care describes the influence of early care interventions on preemies on their development. It has been demonstrated that from 24 to 40 weeks of gestation, the brain experiences a critical period of growth [1]. Studies have shown that exogenous and endogenous experiences of preterm infants in Neonatal Intensive Care Unit (NICU) can lead to developmental disorders [2,3] because patients face excessive sensory stimulation, rapid and inappropriate handling, recurrent aggressive and painful procedures, inappropriate sleep patterns, separation from parents; all these impair the development of the immature brain [4].
Thus, for the smallest babies, it is important simply to support their vital functions and provide a safe environment until laboratory tests and paraclinical investigations reveal a certain aetiology. Overtreatment of these babies may happen in the first days of life due to the lack of strict medical protocols. On the other hand, access to advanced investigations, such as genetic, immunologic or molecular tests is limited, therefore diagnosis of rare diseases may be missed or delayed [5].
A significant help to neonatologists` medical judgement is given by informational input from the obstetricians, as there are strong evidenced-based correlations between maternal illnesses and fetal/neonatal outcomes. Like anamnesis in adult medicine, prenatal interrogation is a compulsory and useful diagnostic tool in neonatal pathologies. Unfortunately, in our practice, we also encounter cases of affected babies from asymptomatic mothers or with no or insufficient prenatal care, therefore without any clues for a quick and accurate diagnosis.
For example, Group B Streptococcus (GBS) is a common commensal in the human gut and low genital tract of women, completely harmless in adults, but its presence during pregnancy can lead to important consequences for the offspring: sepsis or long-term sequelae meningitis are reported [6]. Fortunately, there is a universal screening and treatment protocol for SGB in pregnancy that avoids perinatal infection; unfortunately, there are other diseases affecting young child-bearing women that can be misdiagnosed and can exert potential effects on the fetus or newborn, for example, genetic or autoimmune diseases.
Thrombophilia is defined as a predisposition for thrombosis, mostly due to genetic anomalies, but also postnatal acquired. Pregnancy is one of the conditions that induce a hypercoagulable state by itself (decreased anticoagulant factors level); in association with hereditary thrombophilia, pregnancy represents a higher risk for localized thrombosis and venous or arterial thromboembolism. Screening for thrombophilia before or during pregnancy is not a standard of care but is recommended for women with personal or family history of thromboembolism, an eventful pregnancy or after repeated miscarriages. The incidence of venous thromboembolism (VTE) in pregnancy increases up to five times, with a rate of 0.76-1.72 out of 1000 pregnancies, but most thrombotic events occur mostly in the puerperal period [7,8]. Inherited thrombophilia is assumed to cause up to 50% of venous thrombotic events that occur during gestation and puerperium and may have severe consequences for both the mother and the foetus [8,9,10].
Even if the maternal genetic anomaly is inherited by the fetus, thromboembolic disease is rare in childhood [11,12]. The annual incidence in children is estimated at 0.7 cases of venous thrombosis per 100,000 population, 1.0 of stroke and 0.1 of myocardial infarction. For critically ill neonates prevalence of VTE is much higher (about 10% of VTE occurs in the first four weeks of life). Other conditions that increase the general risk are lower concentrations of natural inhibitors and impaired fibrinolytic activity, elevated levels of factor von Willebrand, [13,14] high viscosity of blood due to the high haematocrit and the small vascular diameter of newborns, dehydration or hypercoagulable state because of infection or prematurity. The use of venous or arterial central catheters is a widespread practice in the NICUs and represents a risk factor for thrombosis [15].
Although encountered more frequently in newborns compared to older children, ischemic stroke is a rare diagnosis in the neonatal period in the absence of general imagistic screening; it is considered that the thromboembolic events are underdiagnosed, being discovered later in life as motor impairments. Still, there is no consensus regarding the administration of preventive low doses of aspirin or anticoagulation with low molecular weight heparin to pregnant women with thrombophilia; coagulation or molecular tests are expensive and not easily available; therefore they are not routinely recommended for all pregnant women or newborns from thrombophilic mothers [16].
In women of childbearing age, there is also a high prevalence of systemic autoimmune disorders, with possible consequences on the fetus and newborn infant, caused by the disease itself, or due to corticoid or immunosuppressive treatment [17]. Gestational complications of autoimmune disorders are miscarriage, stillbirth, preeclampsia, blood cloth, preterm delivery, intrauterine growth retardation, and if maternal disease is characterized by the presence of IgG isotype auto-antibodies, these can cross the placenta with possible antibody-mediated damage to the fetus. In neonatal lupus erythematosus, neonatal congenital heart block is encountered, and neurodevelopmental dysfunctions (learning disabilities or attention deficit) were also described in children born to mothers with systemic lupus erythematosus [18,19].
Maternal glucocorticoid (GC) use or non-use does not affect the incidence or level of autoantibodies and infant symptoms, but the probabilities of preterm delivery and LBW infants were higher and more remarkable in gravidas treated with GC [20,21].
Other neonatal autoimmune diseases involving interaction between maternal antibodies and fetal/neonatal antigens include neonatal anti-phospholipid syndrome, Behcet's disease, neonatal autoimmune thyroid disease, neonatal polymyositis and dermatomyositis, neonatal scleroderma and neonatal type I diabetes mellitus, neonatal myasthenia gravis, and Kawasaki disease. While autoantibodies have been detected in patients with neonatal autoimmune disease, other mechanisms may play a role in developing neonatal autoimmunity, such as fetal/maternal microchimerism and aberrant apoptosis of fetal cells. In some of these conditions, the target antigen may remain unknown [22].
The prevalence of autoimmune diseases among pregnant women is difficult to estimate and there are different mechanisms by which they can affect the fetus or newborn; the neonatal clinical picture has different degrees of expression, not necessarily depending on the maternal severity of the disease, level of maternal antibodies, or types of treatment administered. The discrepancy between maternal and neonatal severity can be partially explained by the protective effect of α-fetoprotein, which inhibits the binding of specific antibodies to its receptors [23].
Usually, the diagnosis of the maternal disease precedes the diagnosis of the fetal or neonatal complications. It is not necessary to test the presence or the level of neonatal antibodies if the mother has a clear previous diagnosis and the child`s signs are suggestive of the mother’s disease. If the mother is not diagnosed it is much more difficult to rely only on the baby's clinical exam, except for some evidence-based associations, like complete atrioventricular block, that strongly suggests lupus erythematosus. Differential diagnosis, especially if the patient is born prematurely and has alterations of vital functions attributed to immaturity or there is an overlapping infectious disease, can be difficult and specific treatment may be delayed.
Therefore, it is important to diagnose pathologies previously existing or related to pregnancy to anticipate and adequately treat any potential complications of the newborn.
2. Materials and Methods
We present three cases of pregnant women without any diagnosed pathology associated with pregnancy who gave birth to 4 premature newborns (one twin pregnancy) that developed postnatally severe symptoms: seizures (#1), respiratory distress and hypotonia (#2), arrhythmia (#3,4), that required admittance in NICU; the onset of the symptoms was immediate after birth for baby #2, and after a certain period in the other cases, raising problems of differential diagnosis and management. All cases were disproportionately affected compared with prenatal history or gestational age and required specific treatment to control the symptoms. The baseline characteristics of the newborns and mothers are summarised in Table 1.
Newborn #1 was born at 36-37 weeks of gestation, 3000g/50cm, female, first child of a healthy mother, from an uneventful pregnancy, extracted by caesarean section for premature rupture of membranes, Apgar score 9, smooth transition to the extrauterine environment, normal clinical examination after birth; baby develops at 36 hours of life tonic-clonic seizures of the left hemibody associated with cyanosis, apnea and bradycardia and was admitted into the NICU, was tested for metabolic causes of the seizures, lumbar puncture and inflammatory panel and bacteriologic tests were performed and Phenobarbital was started. Because of recurrent apneic spells respiratory support was initiated and imagistic investigations were ordered. Head ultrasonography raised suspicion of a large right frontal-parietal infarction confirmed later through Magnetic Resonance Imaging (MRI). Echocardiography revealed no abnormalities. Laboratory tests were all within normal limits except a mild thrombocytopenia (105000/mmc).
Figure 1.
CT examination for newborn #1.
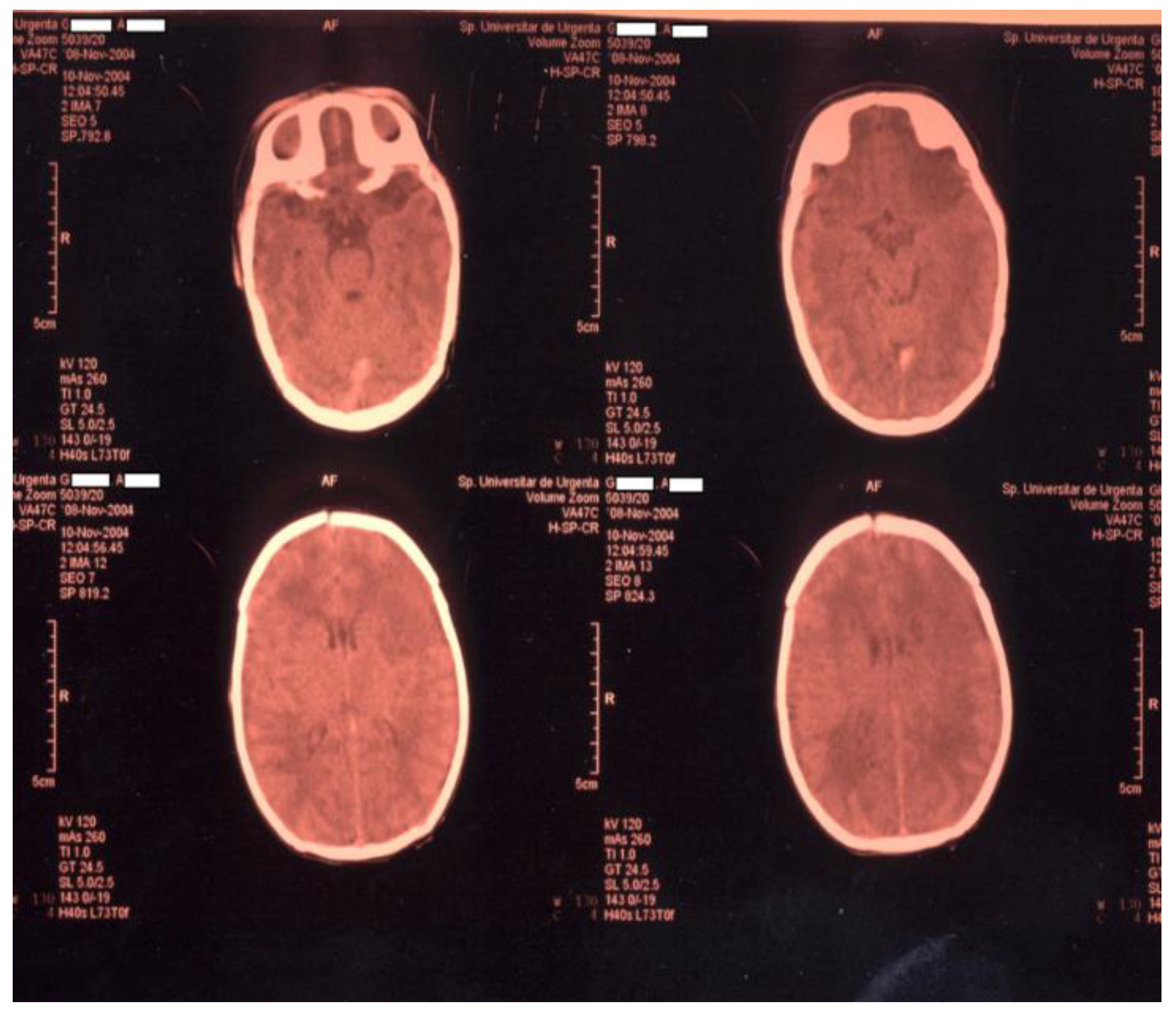
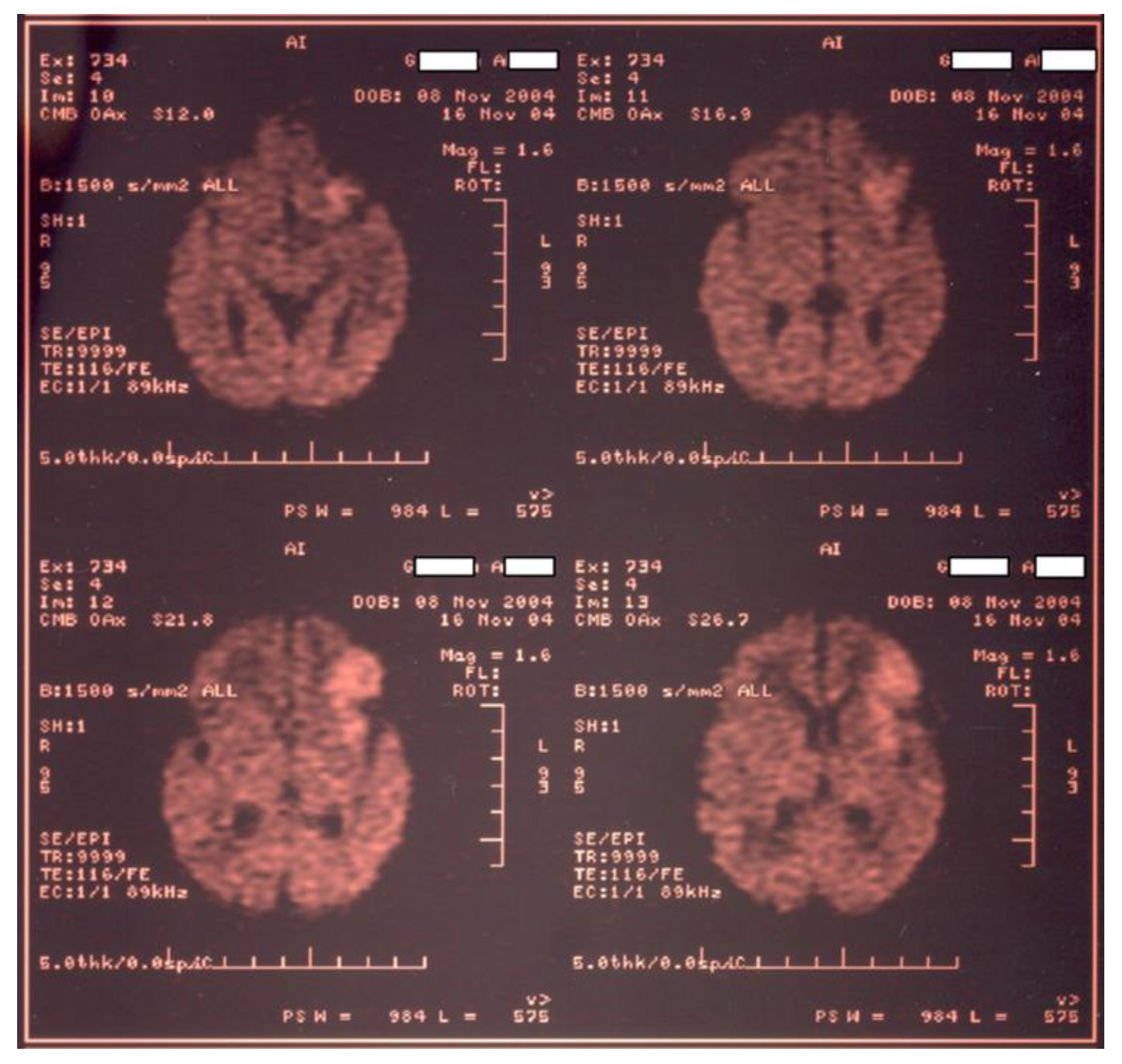
Figure 2.
MRI examination for newborn #1 confirms large right frontal-parietal infarction.
Within differential diagnosis, we considered: maternal chorioamnionitis, hypoxic ischemic encephalopathy, vascular malformations, cardiac lesions, trauma and a hereditary coagulopathy. We performed molecular tests for both mother and infant that revealed heterozygote G1691A mutation on the gene responsible for synthesising factor V Leiden. A less frequent condition related to ischemic stroke in children and adults is sickle cell disease, although not documented in newborns, was also excluded [24,25].
Despite the highest incidence of thrombosis in the neonatal period compared to later childhood, most of the guidelines for neonatal thrombosis do not recommend systematic thrombolysis or anticoagulants [26], therefore our therapeutic approach was conservative.
The newborn was weaned from the ventilator after 72 hours and continued with phenobarbital (maintaining dose) for up to 3 months, according to the neurologist's recommendation, no thrombolytic agents or heparin was given, required long-term physical therapy for motor deficits and spasticity of the left hemibody, with favourable outcome at 5 years of age, recovery ad integrum, but the child is left-handed!
Mother had a second pregnancy after two years, received low-weight heparin during pregnancy and delivered a second female baby at term, 3500g / 50cm, Apgar score of 10 and no pathology, although genetic tests performed for her showed the same mutation as her sibling.
Newborn #2 provided a challenging situation: a premature female baby (30 weeks of gestation), with intrauterine growth restriction (1600g/43cm) born to an un-investigated mother, with a negative familial or personal medical history, with oligoamnios, opalescent amniotic fluid; baby had Apgar score 2 at 1 minute and 5 at 5 minutes (general tone and respiratory effort were significantly decreased), requiring resuscitation but responded poor to interventions. Admitted to the NICU, the baby was mechanically ventilated with low FiO2 and pressures for apnea resistant to continuous positive airway pressure (CPAP) and administration of high doses of caffeine. Clinical picture included hypotonia, hypo reactivity, lack of archaic reflexes and signs of apparent dehydration (low skin turgor, depressed fontanelle), feeding intolerance and a discreet facial dysmorphism. Laboratory tests indicated positive inflammatory syndrome, mild hyponatremia (130mEq/ml), and positive bacteriological tests (Escherichia Coli). Head ultrasound identified a grade II intraventricular haemorrhage, pulmonary X-ray excluded a pulmonary condition and echocardiography showed persistent ductus arteriosus (PDA); aEEG recorded normal cerebral activity. Differential diagnoses included asphyxia, respiratory depression due to prematurity, intracranial haemorrhage, early neonatal sepsis, suprarenal insufficiency, and genetic syndrome (Prader Willi was suspected). Another considered cause for hypotonia was myasthenia gravis, but clinical examination of the mother was perfectly normal and none of the usual investigations done pre- and post-caesarean section did not reveal any abnormalities; she was discharged home at 4 days after birth. The newborn was treated with broad-spectrum antibiotics, caffeine, prolonged total parenteral nutrition (TPN), with correction of biochemical deficits, fresh frozen plasma (for intracranial haemorrhage), hydrocortisone hemisuccinate (for suspicion of SR insufficiency) and intravenous nonspecific human immunoglobulin (i.v. Ig) as adjuvant therapy for sepsis. After more than two weeks of intensive treatment, inflammatory tests and cultures were negative, biochemical tests were normalized, negative lumbar puncture and stable head US, the clinical picture was not improving, except for a slight alleviation after the cure with i.v. Ig (3 x 0,5g/kg/day).
At that time mother had been re-admitted to the hospital with severe bronchopneumonia and respiratory failure (she was mechanically ventilated) and neurological alterations (dysphonia, dysphagia, difficulties in swallowing, speaking, tetraparesys). She tested positive for SARS-COV-2 infection. Her condition was initially considered to be caused by the coronavirus and all therapeutic efforts were conducted in this direction. She received Remdesivir, broad-spectrum antibiotics, corticotherapy and plasmapheresis for cytokine removal (a therapeutic approach used in the second phase of coronavirus infection at that time). After the second session of plasmapheresis, the patient recovered from a respiratory point of view, but she remained with major fatigue and motor deficit with circadian variations that raised suspicion of myasthenia gravis; Miostin was added in treatment and rapidly alleviated the patient’s condition. Serologic tests came positive for anti-acetylcholine receptor antibodies after the disease had been controlled. The baby showed slow progressive improvement in clinical state, before any specific treatment to be used, probably due to a natural decrease in the level of antibodies (already almost 4 weeks of age). Spontaneous respiratory effort allowed extubation at one month of age, feeding was improved by efficient sucking and swallowing reflex and tone and reactivity significantly increased. Long-term follow-up of the case showed normal growth and development and despite long-term mechanical ventilation, associated sepsis and complications, the child presents no neurologic dysfunctions. Although rare, there are documented unfavourable outcomes for babies born to mothers with Myasthenia Gravis, like arthrogryposis multiplex congenital (AMC) or foetal acetylcholine receptor antibody-associated disorders (FARAD), or even neonatal demise [27,28].
Newborn #3 and #4 were two female premature twins (28 weeks of gestation, 900g and 890 g), referred to our hospital from another clinic, a result of a not investigated pregnancy, home-delivered, that developed respiratory distress syndrome requiring mechanical ventilation and surfactant administration, with difficult recovery due to an associated early neonatal sepsis with Corynebacterium pseudotuberculosis; despite treatment with antibiotics and symptomatic, oral feeding and parenteral nutrition, our patients had poor growth and intermittent fever spells associated with tachycardia. Initially, these signs were attributed to infection, but persistence beyond the first week of life and treatment, with negative bacteriological tests, led to suspicion of neonatal hyperthyroidism, although the mother did not have any documented related condition. Values for TSH were extremely low and thyroxine and tri-iodothyronine levels were above normal limits. No somatic clinical sign of hyperthyroidism was present (exophthalmia, goitre). Patients were treated with Tyrosol and Propranolol in doses adjusted in time for their age and weight and followed up by the endocrinologist; after 7 days of treatment, clinical symptoms disappeared and babies began to gain weight, hormonal tests came back to normal (treatment was discontinued at 3 months of age).
During the children's hospitalization (day 5 after birth) mother presented a symptomatic tachyarrhythmia (dyspnoea, oedema, chest pain) and was admitted to the cardiology department of our hospital with a diagnosis of cardiac failure class IV NYHA (ejection fraction 35%), intracardiac thrombosis with possible cardioembolism, later attributed to thyrotoxicosis. TSH level was 0,001 UI/ml, she was given Tyrosol and Lugol solution in decreased doses along with cardiologic treatment (anticoagulants, BB, IEC, diuretics). Correlation between maternal and fetal hyperthyroidism raised suspicion of Basedow Graves’ disease, confirmed later by the results of serological testing. Both the mother and her babies had a favourable outcome.
4. Discussion
We chose to present these three different complexes and surprising cases, because all of them had an unusual but common sequence: no prenatal information or negative history, prematurity-related complications, poor response to standard care; babies were diagnosed before their mothers, information from neonatologists served to diagnose the mothers. Because these three medical conditions have different pathogenesis and clinical picture, we will discuss them separately to emphasize their particularities.
Regarding thrombophilia during pregnancy medical literature reports a low incidence of fetal or neonatal events, the most cited association being between miscarriages and genetic coagulopathies [8].
Most perinatal strokes are ischemic and affect the left cerebral hemisphere, in the territory of the middle cerebral artery [26]. In our case, the infarct was in the frontal-parietal right cortical region. We could not identify in this case any of the supplementary risk factors for thrombosis.
In 2015 we performed in our clinic a retrospective study for 5 years (2010-2014) regarding the postnatal effect of maternal thrombophilia; we analysed all medical records of our patients (mothers and children) to discover associations between maternal genetic anomalies and neonatal outcomes. Results showed no statistically significant correlation between maternal thrombophilia and specific neonatal pathology. From 19.910 births that took place in University Hospital in the study period we identified 2548 pregnant women with genetic thrombophilia (12,8%). The number of preterm labourers was not statistically significantly higher among mothers with thrombophilia, although there were more babies born before 37 weeks of gestation in the group of women with thrombophilia. Weight at gestation was similar for babies born from mothers with and without thrombophilia. There was no higher prevalence of neonatal complications in the group of children from mothers with thrombophilia. None of the cases from that period was diagnosed with thrombotic complications (nor the mother, nor the babies). Women included in the study were either not treated at all (if they were asymptomatic and with a negative family history) or received aspirin or low molecular weight heparin (if they had been diagnosed with intrauterine growth restriction - IUGR or other signs of fetal distress). There was no statistical difference regarding neonatal outcomes between treated or not treated mothers. In this context, we consider the presented case very interesting and unexpected: ischemic stroke in a term baby without associated maternal pathology during pregnancy or perinatal is a rare condition. In some cases, events like this may be asymptomatic, discovered by a routine imaging investigation, or can be expressed later in life when motor development progresses asymmetrically. Prognosis in most of the cases is poor, with motor deficits, depending on size, localization and time of diagnosis and initiation of kinetotherapy. Despite the severe clinical picture, our case had a favourable outcome due to rapid interventions. Moreover, during a second pregnancy of the same woman, preventive anticoagulation was administered and despite inheriting the same genetic mutation, the sibling had no anomalies in coagulation status.
In case #2 the most important clinical sign was severe neurologic depression disproportioned with the grade of prematurity or intraventricular haemorrhage; sepsis or meningitis could have been also responsible for symptomatology, but lumbar puncture was negative, and antibiotics did not influence clinical course in that matter. Associated hyponatremia, signs of dehydration and slightly dysmorphic features led us to metabolic or genetic rare diseases, which were excluded by normal results of specific tests. Myasthenia gravis was initially excluded from differentials as there was no positive maternal or family history and congenital myasthenia gravis (neonatal genetic condition - autosomal recessive inherited) is an extremely rare and lifelong condition. There is also a juvenile myasthenia gravis which resembles the adult form, but it is not expressed in the neonatal period [29]. Even if the mother is diagnosed with myasthenia gravis only 10-20% of infants develop postnatal symptoms [30].
Use of i.v. immunoglobulin in our case as adjuvant therapy for sepsis and/or meningitis might have been beneficial for the baby, as it could bind some of the circulating specific antibodies [29]. Prolonged cardiorespiratory support and parenteral nutrition were essential to ensure babies' well-being until diagnostic and natural clearance of the antibodies.
An interesting fact is that the mother’s disease became clinically patent only postpartum, in the context of a respiratory infection with SARS-COV-2 and her respiratory failure (requiring mechanical invasive ventilation) was severe and prolonged due to the overlapping of the two ethiologies. Although not consistent, studies demonstrate that pregnancy or peripartum period can exacerbate myasthenia gravis symptoms [27,31,32].
Serological testing in our case was positive for anti-acetylcholine antibodies (55,5nmoli/l compared to normal limit ˂ 0,25 nmoli/l) and negative for anti-MUSK antibodies. The case is because the onset of neonatal symptomatology was immediately after birth (usually symptoms appear after 2-3 days of life) and the disease had such severe clinical expression in the newborn, affecting respiratory muscles, while the mother was asymptomatic; the level of antibodies (more than 20 times to normal) may have influenced the severity of the disease. Facial dysmorphism which has been interpreted as syndromic was a sign of diplegia [29].
Our previous recent experience with transient myasthenia gravis consists of asymptomatic or mildly symptomatic cases, with no vital risk, self-limited. The most severe clinical expression among our patients was represented by difficulties in sucking and swallowing requiring short-term specific treatment (Miostin). Mothers were diagnosed antepartum, with or without chronic treatment. All of this demonstrates great variability of the clinical course and picture of this disease; due to the physiologic effects of acetylcholine in the human body and the presence of the receptors in many anatomic structures of the body, symptomatology can be mild or life-threatening, usually self-limited in weeks or months [33].
The third case presents two premature female twins (28 weeks of gestation) born to a mother with no prenatal care and with risk factors for early onset sepsis, with poor response to standard postnatal care. Persistence of fever, episodes of tachycardia, and unsatisfactory weight gain despite enteral and parenteral nutrition raised suspicion of hyperthyroidism, although clinical exam showed no exophthalmia or goitre and no maternal symptomatology or history seemed to support a thyroid disorder. Hormonal testing in both babies confirmed hyperthyroidism (low TSH, elevated T3, T4), although usually, premature babies have transient hypothyroidism in the first weeks of life [34]. It may be that the mother’s disease was only recently decompensated, or the decreased thyroid function due to prematurity may have counterbalanced the effect of maternal stimulating antibodies on the newborns and the symptomatology was not obvious from the beginning.
The infants were transferred to our hospital for treatment of complications of prematurity not accompanied by their mother, so we could not observe her facial features - a certain degree of exophthalmia, which was noticed after she was admitted to our hospital for a severe cardiac condition, proven to be caused by to thyrotoxicosis; such an abrupt onset and severe clinical course it is unusual for Basedow Graves’ disease. The concordance of hormonal abnormalities in both mothers and infants raised suspicion of a maternal autoimmune disease before serological tests (specific antibodies) to confirm it.
To our knowledge, we had a previous case of a newborn, whose mother had been diagnosed and treated for Basedow Graves’ disease before pregnancy, having an elevated level of TRAB antibodies; the baby was born at 35 weeks of gestation, with typical signs of hyperthyroidism: exophthalmia, goitre, hypertonia agitation, myoclonus, feeding difficulties and slow weight gain; fever and sinus tachycardia were also noted. Being a documented and treated pathology of pregnancy, the baby was approached immediately after birth with specific investigations and treatment with rapid good clinical outcomes.
This case is atypic since the onset of symptoms was later than usual and had a poor clinical picture: tachycardia and failure to thrive. Infants born to a mother with active Graves’ disease, untreated, become usually clinically manifest in the first 1-2 days of life, unlike infants born to a mother who received antithyroid treatment, which can be euthyroid or even hypothyroid at birth, and clinical manifestation of Graves neonatal disease appear up to two weeks after birth.
Neonatal manifestations are more likely to appear in cases with higher maternal stimulatory Trab concentration in the third trimester and in the absence of diagnosis and treatment, neonatal thyrotoxicosis can increase the mortality rate up to 15%, especially through cardiovascular complications. Our patients were diagnosed in the second week of life, but prompt intervention led to a favourable outcome, despite supplemental risk factors (prematurity, sepsis).
4. Conclusions
Genetic and autoimmune diseases associated with pregnancy are rather rare conditions, there are not enough evidence-based data to conduct standard postnatal care and, therefore, they represent a concern for the neonatologist; the impact on the newborn is difficult to anticipate as the clinical picture in the first days of life may not be relevant, and still, they can influence short- or longer-term outcomes. Fortunately, most of the autoimmune pathologies at neonatal age are transient and self-limited but is difficult to estimate the intensity and the duration of the symptoms. Genetic diseases such as thrombophilia do not require routine extended investigations or treatment but should be considered as risk factors for serious complications. When the maternal disease is not documented or there is an asymptomatic pregnancy, management of neonatal patients becomes more difficult, and it takes longer time for appropriate intervention. We emphasize the importance of thorough prenatal care and a close interdisciplinary approach, as more information gathered from different sources can provide a relevant diagnostic argument that can sometimes substitute expensive and unavailable medical investigations.
Author Contributions
Conceptualization, A.M.D. and D.I.V.; methodology, M.C.; software, S.V.; validation, M.C., V.D.; formal analysis, A.M.D.; investigation, D.I.V.; resources, A.M.D, S.V., V.D.; data curation, A.M.D.; writing—original draft preparation, A.M.D.; writing—review and editing, V.D.; visualization, M.C..; supervision, M.C.; project administration, A.M.D.
Funding
This research received no external funding
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Local Ethics Committee of the Emergency University Hospital Bucharest 29930/2 Approval Date: 24.07.2023.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
In this section, you can acknowledge any support given which is not covered by the author contribution or funding sections. This may include administrative and technical support, or donations in kind (e.g., materials used for experiments).
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Lammertink, F.; Vinkers, C.H.; Tataranno, M.L.; Benders, M.J.N.L. Premature Birth and Developmental Programming: Mechanisms of Resilience and Vulnerability. Front. Psychiatry 2021, 11. [Google Scholar] [CrossRef] [PubMed]
- Als, H.; Duffy, F.H.; McAnulty, G.B.; Rivkin, M.J.; Vajapeyam, S.; Mulkern, R.V.; Warfield, S.K.; Huppi, P.S.; Butler, S.C.; Conneman, N.; et al. Early Experience Alters Brain Function and Structure. Pediatrics 2004, 113, 846–857. [Google Scholar] [CrossRef] [PubMed]
- Peters, K.L.; Rosychuk, R.J.; Hendson, L.; Coté, J.J.; McPherson, C.; Tyebkhan, J.M. Improvement of Short- and Long-Term Outcomes for Very Low Birth Weight Infants: Edmonton NIDCAP Trial. Pediatrics 2009, 124, 1009–1020. [Google Scholar] [CrossRef] [PubMed]
- Soleimani, F.; Azari, N.; Ghiasvand, H.; Fatollahierad, S. Effects of Developmental Care on Neurodevelopment of Preterm Infants. Iran J Child Neurol. 2020, 14, 7–15. [Google Scholar]
- Dima, V. Actualities in neonatal endocrine and metabolic screening. Acta Endocrinol (Buchar). 2021, 17, 416–421. [Google Scholar] [PubMed] [PubMed Central]
- Steer, P.J.; Russell, A.B.; Kochhar, S.; Cox, P.; Plumb, J.; Rao, G.G. Group B streptococcal disease in the mother and newborn—A review. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 252, 526–533. [Google Scholar] [CrossRef]
- Samfireag, M.; Potre, C.; Potre, O.; Moleriu, L.-C.; Petre, I.; Borsi, E.; Hoinoiu, T.; Preda, M.; Popoiu, T.-A.; Anghel, A. Assessment of the Particularities of Thrombophilia in the Management of Pregnant Women in the Western Part of Romania. Medicina 2023, 59, 851. [Google Scholar] [CrossRef]
- Samfireag, M.; Potre, C.; Potre, O.; Tudor, R.; Hoinoiu, T.; Anghel, A. Approach to Thrombophilia in Pregnancy—A Narrative Review. Medicina 2022, 58, 692. [Google Scholar] [CrossRef]
- Daughety, M.M. Samuelson Bannow B.T. Hemostasis and Thrombosis in Pregnancy. In Hemostasis and Thrombosis; DeLoughery, T., Ed.; Springer: Cham, Switzerland, 2019. [Google Scholar]
- Greer, I.A. Thrombosis in pregnancy: maternal and fetal issues. Lancet 1999, 353, 1258–1265. [Google Scholar] [CrossRef]
- Khizroeva, J.; Makatsariya, A.; Vorobev, A.; Bitsadze, V.; Elalamy, I.; Lazarchuk, A.; Salnikova, P.; Einullaeva, S.; Solopova, A.; Tretykova, M.; et al. The Hemostatic System in Newborns and the Risk of Neonatal Thrombosis. Int. J. Mol. Sci. 2023, 24, 13864. [Google Scholar] [CrossRef]
- Guzman, R.E.; Hughes, A.; Kiskaddon, A.; Fort, P.; Betensky, M. Thrombosis in the Neonatal Intensive Care Unit. NeoReviews 2023, 24, e356–e369. [Google Scholar] [CrossRef] [PubMed]
- Vasilescu, D.I.; Rosoga, A.M.; Vasilescu, S.; Dragomir, I.; Dima, V.; Dan, A.M.; Cirstoiu, M.M. SARS-CoV-2 Infection during Pregnancy Followed by Thalamic Neonatal Stroke—Case Report. Children 2023, 10, 958. [Google Scholar] [CrossRef]
- Komitopoulou, A.; Platokouki, H.; Kapsimali, Z.; Pergantou, H.; Adamtziki, E.; Aronis, S. Mutations and Polymorphisms in Genes Affecting Hemostasis Proteins and Homocysteine Metabolism in Children with Arterial Ischemic Stroke. Cerebrovasc. Dis. 2006, 22, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Komitopoulou, A. Thrombophilia and Thrombotic Disorders in Newborns. Hematol. Transfus. Int. J. 2016, 2, 1–2. [Google Scholar] [CrossRef]
- Skeith, L. Prevention and management of venous thromboembolism in pregnancy: cutting through the practice variation. Hematol. 2021, 2021, 559–569. [Google Scholar] [CrossRef]
- Bhatt, M.D.; Chan, A.K. Venous thrombosis in neonates. Fac. Rev. 2021, 10. [Google Scholar] [CrossRef] [PubMed]
- Gyawali, S.; Rauniyar, S.P.G.; Gyawali, B.; Bhusal, T.; Basnet, S. Neonatal lupus erythematosus manifested as a complete heart block: A case report. Clin. Case Rep. 2023, 11, e7758. [Google Scholar] [CrossRef]
- Liu, W.; Ma, D.-L. Neonatal lupus erythematosus. Can. Med Assoc. J. 2020, 192, E163–E163. [Google Scholar] [CrossRef]
- He, H.; Yu, Y.; Liew, Z.; Gissler, M.; László, K.D.; Valdimarsdóttir, U.A.; Zhang, J.; Li, F.; Li, J. Association of Maternal Autoimmune Diseases With Risk of Mental Disorders in Offspring in Denmark. JAMA Netw. Open 2022, 5, e227503–e227503. [Google Scholar] [CrossRef]
- Sim, S.Y.; Choi, H.Y.; Jung, M.H.; Lee, S.Y.; Rhim, J.W.; Kang, H.M.; Jeong, D.C. Catch-up growth of infants born to mothers with autoimmune rheumatic disorders. Pediatr. Rheumatol. 2022, 20, 1–7. [Google Scholar] [CrossRef]
- Chang, C. Neonatal autoimmune diseases: A critical review. J. Autoimmun. 2012, 38, J223–J238. [Google Scholar] [CrossRef] [PubMed]
- Singh, M.; Wambua, S.; Lee, S.I.; Okoth, K.; Wang, Z.; Fayaz, F.F.A.; Eastwood, K.-A.; Nelson-Piercy, C.; Reynolds, J.A.; Nirantharakumar, K.; et al. Autoimmune diseases and adverse pregnancy outcomes: an umbrella review. BMC Med. 2024, 22, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Light, J.; Boucher, M.; Baskin-Miller, J.; Winstead, M. Managing the Cerebrovascular Complications of Sickle Cell Disease: Current Perspectives. J. Blood Med. 2023, 14, 279–293. [Google Scholar] [CrossRef] [PubMed]
- Talahma, M.; Strbian, D.; Sundararajan, S. Sickle Cell Disease and Stroke. Stroke 2014, 45, e98–100. [Google Scholar] [CrossRef] [PubMed]
- Ferriero, D.M.; Fullerton, H.J.; Bernard, T.J.; Billinghurst, L.; Daniels, S.R.; DeBaun, M.R.; Deveber, G.; Ichord, R.N.; Jordan, L.C.; Massicotte, P.; et al. Management of Stroke in Neonates and Children: A Scientific Statement From the American Heart Association/American Stroke Association. Stroke 2019, 50, E51–E96. [Google Scholar] [CrossRef]
- Draxler, J.; Meisel, A.; Stascheit, F.; Stein, M.; Gerischer, L.; Mergenthaler, P.; Herdick, M.; Doksani, P.; Lehnerer, S.; Verlohren, S.; et al. Pregnancy in myasthenia gravis: a retrospective analysis of maternal and neonatal outcome from a large tertiary care centre in Germany. Arch. Gynecol. Obstet. 2024, 310, 277–284. [Google Scholar] [CrossRef]
- Hoff, J.M.; et al. Myasthenia gravis consequences for pregnancy, delivery and the newborn. Neurology 2003, 61, 1362. [Google Scholar] [CrossRef]
- Bardhan, M.; Dogra, H.; Samanta, D. Neonatal Myasthenia Gravis. 2023 Jan 9. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar] [PubMed]
- Isaac Buckstein, Fetal Effects of Autoimmune Diseeases, in Fanaroff & Martin s Neonatal-Perinatal Medicine – Diseases of the Fetus and Infant, 10th Edition, Elsevier 2015, p.304-311.
- Batocchi, A.P.; et al. Course and treatment of myastenia gravis during pregnancy. Neurology. 1999;52-447 / Djelmis J, et al. Myasthenia gravis in pregnancy: report on 69 cases. Eur J Obstet GynecolReprod Biol. 2002;104:21 /.
- Banner, H.; Niles, K.M.; Ryu, M.; Sermer, M.; Bril, V.; E Murphy, K. Myasthenia gravis in pregnancy: Systematic review and case series. Obstet. Med. 2022, 15, 108–117. [Google Scholar] [CrossRef]
- Vasilescu, D.I.; Dan, A.M.; Dima, V.; Hospital, B.F.C.; Cirstoiu, M.M. Transient neonatal myasthenia gravis: case report. Romanian Med J. 2022, 69, 166–168. [Google Scholar] [CrossRef]
- Klosinska, M.; Kaczynska, A.; Ben-Skowronek, I. Congenital Hypothyroidism in Preterm Newborns – The Challenges of Diagnostics and Treatment: A Review. Front. Endocrinol. 2022, 13, 860862. [Google Scholar] [CrossRef]

Table 1.
Characteristics of the 4 newborns and associated pathology of their mothers.
| Newborn 1 | Newborn 2 | Newborn 3 | Newborn 4 | |
|---|---|---|---|---|
| Gender | F | F | F | F |
| Gestational age weeks | 36 | 30 | 28 | 28 |
| Birth weight | 3000g | 1600g | 900g | 890g |
| Apgar score | 9/9 | 2/5 | unknown | unknown |
| Delivery | cesarean section | home delivery | home delivery | |
| Newborn’s first symptoms | 36 hours of life | At birth | 72 hours of life | 72 hours of life |
| Investigations during pregnancy | yes | no | no | no |
| Mother’s disease | Thrombophilia | Myasthenia gravis | Basedow Graves | Basedow Graves |
| Time of diagnosis of the maternal disease | 5 days after delivery | 2 weeks after delivery | 5 days after delivery | 5 days after delivery |
| Postpartum clinical expression of maternal disease | none | Neurologic depression | cardiac failure | cardiac failure |
| Method of diagnosis of maternal disease | Genetic tests | Anti-Ach receptors antibodies | TSH, fT4, Trab antibodies | TSH, fT4, Trab antibodies |
| Discharged home with chronic medication | Phenobarbital for 3 months | No | Tyrosol and Propranolol for 3 months | Tyrosol and Propranolol for 3 months |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



