
Submitted:
20 August 2024
Posted:
21 August 2024
You are already at the latest version
Abstract
Background: We investigated the significance of the para-aortic node (PALN) and other regional node metastases (RLN), reflecting malignant histological findings or poor patient prognosis, in patients with biliary duct cancers (BDC) and pancreatic carcinomas (PC) who underwent radical resections at two institutes. Methods: Conventional clinicopathological factors, including metastasis to the PALN and RLN, and surgical outcomes or long-term prognosis in 181 PC and 116 BDC patients between 1994 and 2022 were examined. Results: In patients with PC, cancer metastasis was observed in the RLN and PALN in 54% and 9% of patients, respectively. In patients with BDC, cancer metastasis was observed in the RLN and PALN in 39% and 9% of patients, respectively. Disease-free survival (DFS) and overall survival (OS) in patients with BDC and PALN metastasis were significantly lower than those without PALN metastasis; however, several patients survived over three years. Multivariate analysis revealed that, in patients with BDC, PALN metastasis was an independently related factor of OS, and RLN was an independently related factor for DFS, respectively (p
Keywords:
biliary duct carcinoma
; pancreatic carcinoma
; para-aortic lymph node
; intraoperative diagnosis
; postoperative prognosis
1. Introduction
In pancreatic and bile duct cancers, radical surgical resections, such as pancreaticoduodenectomy, distal pancreatectomy, and hepatectomy, are the only curative options, even when regional lymph node (RLN) metastasis is diagnosed [1,2,3,4]. However, in cases where node metastasis around the para-aortic area is observed, radical resection should be avoided because of distant metastasis [5]. If occult para-aortic lymph node (PALN) metastasis, which is not detected on preoperative imaging, is diagnosed through intraoperative histological findings using a solitary sampling node, it becomes challenging to determine whether to continue the scheduled operation. If multiple nodes or related findings of advanced local extension of the primary cancer are found, it is generally reasonable to decide on a probe laparotomy [6,7,8,9,10,11,12,13,14,15]. Usually, the diagnostic accuracy of regional or distant node metastasis using preoperative multimodal image diagnosis with conventional ultrasonography, computed tomography, magnetic resonance, and positron emission tomography is approximately 4-21% in the field of pancreaticobiliary cancers (PBC) [8,9,10,16,17]. Therefore, an intraoperative histological diagnosis using frozen node tissue was performed. However, the clinical significance of this modality in influencing postoperative survival remains unclear. We hypothesize that radical surgery is worthwhile when occult solitary PALN metastasis is first diagnosed using intraoperative PALN node sampling.
To clarify our hypothesis and to determine the institutional strategy for radical surgical resection during surgery in cases where a solitary cancer-positive node is observed, we retrospectively examined the postoperative survival of patients with pancreatic and bile duct cancer with or without PALN metastasis who underwent radical resections at two institutes, which the principal author experienced, between 1994 and 2021. Additionally, clinicopathological factors associated with PALN were analyzed.
2. Materials and Methods
2.1. Patients, Ethics and Data Retrieval
This study retrospectively collected data of 144 consecutive patients with PBC (pancreatic carcinoma [PC], n=82 and bile duct carcinoma [BDC], n=62) at the Division of Surgical Oncology, Department of Translational Medical Sciences, Nagasaki University Graduate School of Biomedical Sciences (NUGSBS), who were treated by the first author between April 1994 and March 2015. Other data were obtained from 153 consecutive patients with PBC (PC, n=99 and BDC, n=54) at the Division of Hepatobiliary Pancreatic Surgery, Department of Surgery, University of Miyazaki Faculty of Medicine (UoM) between April 2015 and December 2021, who have been treated by the first author to date. The in-hospital data of all patients were retrospectively and consecutively collected from the patient charts at the two institutions. The study design was approved by the Ethics Review Board of NUGSBS and UoM (approval numbers: #24031804, March 19, 2024, and #O-1503, January 24, 2024, respectively), and informed consent was obtained via an opt-out procedure at an outpatient clinic and via our website for one month. No financial support was received for this study, and the authors declare no conflicts of interest. This study adhered to the Declaration of Helsinki’s statement on the ethical principles for medical research involving human participants, including research on identifiable human materials and data.
Data were retrieved from the anesthetic and patient electronic charts and the NUGSBS and UoM databases for the duration of initial hospitalization following hepatectomy. Serum levels of carcinoembryonic antigen (CEA) and carbohydrate antigen (CA)19-9 were measured as tumor markers for PC and BDC before and after the primary treatment for every three months, and enhanced computed tomography of the liver was performed every six months after hepatectomy to monitor tumor recurrence. The minimum follow-up period after hepatic resection in patients with BDC who survived was 26 months (range, 12–128 months).
2.2. Comparative Measurement of Tumor Markers and Histological Findings before Surgery
Patient clinicopathological data were retrieved from our institute's archives. Peripheral blood samples were collected from each patient early in the morning before surgery when the patient was stable. In our hospital, the normal levels of CEA, CA19-9, and Duke Pancreas II monoclonal antibody (DUPAN-II) [18] in patients were <5 ng/mL, <37 U/mL, and 150 U/mL, respectively, and these elevated levels were defined as levels that exceeded normal levels. Tumor-related factors were compared with the histopathological findings of the resected specimen. For the clinicopathological assessment of PC and BDC, we used the 7th edition of General Rules for the Study of Pancreatic Cancer by Japan Pancreas Society [19] and the 7th edition of General Rules for Clinical and Pathological Studies on Cancer of the Biliary Tract by Japanese Society of Hepato-Biliary-Pancreatic Surgery [20].
2.3. Statistical Analysis
Differences in categorical data between the groups and prevalence were assessed using the chi-square test, Fisher’s exact test, or Dunnett’s multiple comparison test. Differences in continuous data between groups were evaluated using the Student’s t-test or the Mann–Whitney test. Disease-free intervals and overall survival were calculated using the Kaplan–Meier method, and differences between groups were tested for significance using the log-rank test. Multivariate analysis for survival was performed using the Cox proportional hazards regression model. A log-rank regression analysis test was performed to determine independent risk factors. A two-tailed P value of <0.05 was considered significant. Statistical analyses were performed using the SPSS software version 23 (Statistical Package for the Social Science, Inc., Chicago, IL, USA).
3. Results
3.1. Perioperative Parameters
The primary patient data of 181 PC patients were indicated as follows: the cohort included 100 males and 81 females with a mean age of 68.1 ± 9.4 years at the time of surgery. The mean CEA, CA19-9, and DUPAN-II levels were 10.8 ± 60.5 ng/mL (median 2.6), 509 ± 1,732 U/mL (median 62), and 591 ± 1,605 U/mL (median 92), respectively. The mean tumor size was 3.2 ± 1.7 cm. Neoadjuvant chemotherapy (NAC) was administered to only nine patients (5%) in this cohort. Pancreaticoduodenectomy was performed in 117 patients (65%), distal pancreatectomy in 60, and total pancreatectomy in 4. All patients underwent complete macroscopic radical resection without remnant cancer. Macroscopically resected specimens exhibited the nodular type in 46, invasive type in 105, cystic type in 28, and dilated main duct type in 2 patients. Histological differentiation was papillary in 3, well in 37, moderate in 85, poor in 17, mucinous in 2, acinar in 4, adenosquamous in 2, anaplastic in 2, and unknown in 29 patients (16%). RLN and PALN metastasis were observed in 98 (54%) and 17 patients (9%), respectively. Lymphatic duct, venous, and peri-neural infiltrations were observed in 101 (56%), 131 (72%), and 129 (71%) patients, respectively. Regarding peri-pancreatic cancer involvement, retro-pancreatic, bile duct, and duodenal infiltrations were observed in 101 (58 %), 60 (66 %), and 54 (31%) patients, respectively. With respect to the histologically resected surgical margin, a cancer-positive pancreatic margin was observed in none of the patients; however, a positive dissected exposed margin was observed in 14 patients (8%). Portal vein involvement was observed in 43 patients (24%) and artery in 5 (3%). The mean blood loss was 1560 ± 1018 mL (median 1120 mL). Surgical curability was classified as R0 in 171 (95%) patients, R1 in 8 (4%), and R2 in 2 (1%). Adjuvant chemotherapy after surgery was administered to 74 patients (41%); however, cancer recurred in 117 patients (65%) after surgery. The recurrence was observed in the liver in 61, lymph nodes in 19, lungs in 24, local in 13, peritoneum in 16, bone in 4, and remnant pancreas in 6 patients. All patients except those who experienced recurrence in the remnant pancreas underwent chemotherapy; three of the six patients with recurrence in the remnant pancreas underwent total pancreatectomy. Of the 181 patients, 50 survived without cancer recurrence (28%), 22 with cancer recurrence (12%), 94 died of cancer (52%), and 15 died of other diseases without cancer recurrence (8%); thus, 87 patients (48%) were censored.
The basic patient data of the BDC cohort (116 patients) were indicated as follows: the cohort included 85 males and 31 females with a mean age of 68.5 ± 11.4 years at the time of surgery. Distal BDCs were observed in 68 patients (59%), and proximal BDCs in 48 patients. Obstructive jaundice and a history of biliary disease were observed in 85 (75%) and 15 (13%) patients, respectively. A history of diabetes and smoking was observed in 38 (33%) and 47 (41%), respectively. The mean CEA and CA19-9 levels were 5.1 ± 18.9 ng/mL (median 2.4) and 2815 ± 25639 U/mL (median 37), respectively. The mean tumor size was 1.9 ± 1.7 cm (median 1.6 cm). The mean preoperative total bilirubin level was 1.48 ± 1.05 mg/dL, and the alkaline phosphatase level was 537 ± 484 U/L. Pancreaticoduodenectomy was performed in 78 patients (68%), hepatectomy in 45 (39%), and hepatopancreaticoduodenectomy in 7 patients. The mean blood loss was 1324 ± 888 mL (median 1075 mL). All patients underwent complete macroscopic radical resection without remnant cancer. The resected specimens were macroscopically of papillary, nodular, or flat type without invasiveness in 19 patients and with invasiveness in 97 patients (84%). Histological differentiation was papillary in 14, well in 49, moderate in 38, poor in 14, and unknown in 1 patient. RLN and PLAN metastases were observed in 45 (39%) and 10 patients (9%), respectively. Infiltration type α was observed in 5 (5%) and others in 111 (95%) patients. Lymphatic duct, venous, and perineural infiltrations were observed in 73 (64%), 77 (67%), and 78 (69%) patients, respectively. The depth of tumor infiltration was mucosal in 17 patients, subserosal in 60, serosal in 23, and extraserosal in 16. With respect to peripancreatic cancer involvement, hepatic, gallbladder, pancreatic parenchymal, and duodenal infiltrations were observed in 21 (18%), 6 (5%), 47 (41%), and 18 (16%) patients, respectively. Portal vein and artery involvement was observed in nine patients (8%) and two patients (2%), respectively. Superficial cancer extension > 20 mm was observed in 33 patients (31%). Proximal cholangitis of the resected specimen and pancreaticobiliary malfunction were observed in 29 patients (25%) and 4 patients (4%), respectively. With respect to the histologically resected surgical margins, involvement of cancer at the hepatic bile duct stump was observed in 23 patients (20%), and cancer at the dissected exposed margin was observed in 10 patients (9%). Curability by surgery was classified as R0 in 98 patients (85%), R1 in 18 (15%), and R2 in none. Postoperative complications of Clavien–Dindo classification 2 were observed in 65 patients (56%). Adjuvant chemotherapy over six months after surgery as S-1 alone or gemcitabine-cisplatin combination was administered in 33 patients (28%). Cancer recurrence was observed in 48 patients (41%) after surgery; recurrence was observed in the liver in 23, lymph node in 8, lung in 5, local in 12, peritoneum in 12, and bone in 1 patient. Twenty-seven of the 48 patients (56%) underwent chemotherapy. Out of the 116 patients, 50 patients survived without cancer recurrence (43%), 13 survived with cancer recurrence (11%), 43 died of cancer (37%), and 10 died of other diseases without cancer recurrence (9%); therefore, 73 patients (63%) were censored.
3.2. Relationship between Clinicopathological Parameters and Disease-Free and Overall Survival after Surgery
Figure 1 illustrates that the DFS and OS of patients with PC and PALN metastasis were significantly lower than those without PALN; however, three patients survived for > 3 years. Figure 2 demonstrates that the DFS and OS of patients with BDC and PALN metastasis were significantly lower than those without PALN; however, five patients survived for > 3 years. To clarify the influence of other clinicopathological factors on survival in patients with BDC compared with those with PC”, we performed comprehensive survival analyses as follows: with respect to OS in patients with PC (Table 1a), univariate analysis showed that 17 parameters, including RLN and PALN metastases, were significantly associated with OS. Furthermore, multivariate analysis showed that NAC, poorer histological differentiation, and histological evidence of lymphatic and perineural infiltration of cancer, were independently related factors of OS, whereas RLN and PALN were not (p<0.05). With respect to DFS in patients with PC (Table 1b), univariate analysis showed that 17 parameters, including RLN and PALN metastases, were significantly associated with DFS. Furthermore, multivariate analysis revealed that poorer histological differentiation and histological evidence of perineural infiltration of cancer were independently related factors, whereas RLN and PALN were not (p<0.05).
With respect to OS in patients with BDC (Table 2a), univariate analysis showed that 17 parameters, including RLN and PALN metastases, were significantly associated with OS. Furthermore, multivariate analysis revealed that the serum CA19-9 levels; histological evidence of lymphatic, venous, and perineural infiltration of cancer; PALN; positive margin at the exposed surgical margin; and chemotherapy for recurrence were independent related factors of OS (p<0.05). With respect to DFS of patients with BDC (Table 2b), univariate analysis showed that 14 parameters, including RLN and PALN metastases, were significantly associated with DFS. Furthermore, multivariate analysis revealed that histological lymphatic infiltration of cancer, RLN, histologically non-curative resection, and chemotherapy for cancer recurrence were independent related factors, whereas PALN was not (p<0.05).
3.3. Relationship between Para-Aortic Lymph Node Metastasis and Other Clinicopathological Factors
Table 3 lists the correlations between RLN and PALN metastases and other clinicopathological factors in patients with PC. Univariate analysis revealed that 16 parameters were significantly associated with the existence of RLN metastasis, and nine parameters were significantly associated with the presence of PALN metastasis (p<0.05) (Table 3a). Multivariate regression analysis showed that no factors were associated with RLN, and a higher serum DUPAN-II level before surgery alone was significantly associated with the presence of PALN metastasis (p<0.05) (Table 3b). Table 4 details the correlations between RLN and PALN metastases and other clinicopathological factors in patients with BDC. Univariate analysis showed that 13 parameters were significantly associated with RLN metastasis, and ten parameters were significantly associated with PALN metastasis (p<0.05) (Table 4a). Multivariate regression analysis (Table 4b) revealed that histological lymphatic or perineural infiltration and hepatic or pancreatic involvement were significantly independently associated with RLN metastasis (p<0.05); no other factors were related to the presence of PALN metastasis.
4. Discussion
Specific pancreaticobiliary carcinoma (PBC) markers such as CEA or CA19-9 levels are commonly used in Japan to diagnose or evaluate malignant tumor aggressiveness (8-10, 21). The existence of paraaortic lymph node swelling or positivity on positron emission computed tomography before surgery is a worrisome indication of distant node metastasis, which has been considered a non-curative factor for surgery on digestive organs, including surgery for PBC [22,23]. However, in the era of systemic solid chemotherapy or immunotherapy, some investigators have shown better survival with scheduled surgery, even with positive PALN cancer [7,10,24,25,26]. Furthermore, the concept of oligometastasis in organs distant from the PBC has been proposed, but the significance of radical surgery remains controversial [9]. Thus far, it has been reported that PALN metastasis demonstrated the worst patient survival, and the pre- or intra-operative diagnosis of PALN metastasis resulted in unresectability [5,12,27]. In contrast, Hempel et al. and other investigators reported that PALN metastasis, a predictive factor, can be confirmed during postoperative pathological diagnosis [8,14,28]. The survival of patients with PALN metastasis who underwent radical surgery was poorer than those without PALN metastasis; however, the survival of patients with PALN metastasis who underwent surgery was better than that of patients who did not undergo surgery [29,30]. This issue regarding the significance of radical surgery in cases of PALN metastasis remains unclear, and this might be influenced by neoadjuvant or adjuvant chemotherapy with novel effective anti-cancer drugs (29, 30). Due to the oligometastasis, the significance of metastasectomy has been elucidated in patients with PC undergoing adjuvant chemotherapy [31]. The number of intraoperative PALN metastases is a notable issue [10,12,32] that we recently experienced. In case a solitary PALN node is unexpectedly found during intraoperative sampling, we were challenged to choose an appropriate strategy, borderline resectable or unresectable. Fortunately, other oncological difficulties are not observed in PBC surgery. Thus, the present study attempted to clarify our hypothesis and establish an institutional strategy for cases of solitary PALN metastasis in PBC conducted before the era of aggressive chemotherapy. The study was conducted at two institutes where the principal author performed the same quality radical operations with PALN dissection or sampling for 27 years.
First, patient survival in cases of PALN metastasis in patients with PBC was examined. The results demonstrated that patients with PBC and PALN metastasis had poorer survival than those without PALN metastasis. However, the 5-year OS of patients with PALN metastasis remained stable in both PC and BDC groups, and a two-year median survival period was observed. In this study with PALN metastasis, cases of unexpected solitary PALN metastasis with curative surgery based on preoperative imaging diagnosis were included, whereas cases of multiple PALN metastases were not. Certainly, DFS was significantly poor; however, this can be improved in the future using adjuvant chemotherapy or chemotherapy in recurrent cases (29-31). Furthermore, in the second step, the statistical weights of PALN for patient survival and other regional node metastases (PLN) were examined along with various clinicopathological factors using multivariable analyses. In a recent nationwide Japanese study, neoadjuvant chemotherapy, gemcitabine, and S-1 combination therapy were significantly and strongly beneficial for the survival of patients with PC. CA19-9 level, a valuable marker of PC aggressiveness, showed high significance in the univariate analysis in this study; however, this may have been influenced by obstructive jaundice or NAC. Thus, this was not observed in multivariate analysis. Histological features of cancer, such as lower differentiation and vascular infiltration, were consistent markers of poor DFS and OS in this series, as well as in a previous study [7,10,12,13,14,33,34,35]. Recently, preoperative endoscopic ultrasonography-guided fine needle aspiration or biopsy (EUS-FNA or FNB) has performed better than pancreatic duct aspiration in most patients with PC [36]. However, most samples could not be used to evaluate all PC patients' survival predictions. In contrast, in BDC, CA19-9 was a significant marker for poor survival and histological vascular infiltration in this study, as well as in a previous study [37]. No NAC was administered in this study. CA19-9 remains the most reliable surrogate marker at this stage.
In both PC and BDC, the statistical weight of PALN and PLN metastasis for survival differed. In PC, these tended to be associated with poor survival; however, multivariate analysis did not observe the association. Additionally, other histological markers might exhibit malignant behavior. In BDC, both PALN and PLN were significantly associated with poor survival. In addition to PC, other histological factors may contribute to aggressiveness. A previous study demonstrated that the histological factors related to tumor vascular infiltration showed a higher significance relating to poor survival as described above [7,10,12,13,14,33,34,35]. Furthermore, as a surgical factor, cancer-positive margins, such as exposed margins or R1 resection, were significantly associated with poor prognosis in this study as well as in previous reports [7,9,13,14,38,39]. Although both PALN and PLN were prognostic factors, solitary PALN metastasis was not a definitive prognostic factor determining the decision for radical surgery in our study.
Next, the clinicopathological factors associated with PLN and PALN were examined. On univariate PC analysis, many clinicopathological factors were significantly associated with PLN compared with those with PALN. None of the factors were related to PLN metastasis, whereas only DUPAN-II was significantly associated with PALN metastasis. DUPAN-II is associated with tumor aggressiveness in PC. In BDC, in this study, histological infiltration of cancer and organ involvement was significantly associated with PLN metastasis, whereas no association with PALN metastasis was observed as a previous report [14]. Some PALN metastases may skip metastases but do not follow the course of lymph vessels, unlike other PLN metastases in BDC. In gallbladder cancer, such a direct metastatic route has been identified in a previous report [40]. Based on our hypothesis, if such a case exists without other prognostic factors, it is possible to perform radical surgery when a solitary PALN metastasis is observed. To elucidate the clinical significance of regional node metastasis, including PALN, the efficacy index calculated by the survival rate or period would be required [15].
Eventually, we aimed to determine the performance of radical surgery in this study. A strategy can be determined based on our findings as follows: 1) If solitary PAL was observed during preoperative or intraoperative examination in PC, and if NAC was mostly successful, DUPAN-II levels were > 800 U/ml, and there was no retropancreatic involvement, radical surgery is considered. In addition, histological differentiation or vascular infiltration was investigated using preoperative biopsy specimens and discussed with the pathologists. If DUPAN-II levels increase to > 800 U/ml and retro-pancreatic infiltration is positive, node dissection of the PALN is attempted. This indicates better survival, and R1 resection is prospectively permissible. 2) When a solitary PAL is observed during preoperative or intraoperative examination in BDC, PAL metastasis alone is a significantly poor prognostic factor, and radical surgery must be limited to younger patients (<70 years). If CA19-9 is very high, i.e., > 100 U/ml, R0 or non-exposed surgery cannot be achieved, and histological findings associated with poor prognostic factors were not observed in the preoperative specimens, radical surgery should be performed in the prospective setting.
Limitations
The limitations of the present study are as follows: 1) retrospective two-institutional cohort for a long period but not prospective; 2) the number of patients with PALN metastasis was not high in the recent 6 years due to institutional bias; 3) DUPAN-II levels were not routinely examined, and this must be examined prospectively; 4) surgical indications at the two institutions were due to operator decision bias. These limitations must be verified via interim survival analysis using the proposed operative indication conducted over the next five years, as outlined in the prospective institutional criteria for PBC. However, these unexpected and contradictory results must be confirmed in a larger number of participants at a single institute.
5. Conclusions
We conducted a retrospective and consecutive analysis of the outcomes of 297 patients with PBC, consisting of 181 patients with PC and 116 patients with BDC, who underwent curative surgical resections focusing on solitary PALN metastasis. We analyzed the relationship between PLN and PALN metastasis, conventional clinicopathological parameters, and patient long-term survival. Although histological findings of cancer infiltration, differentiation, and organ involvement were significantly poor prognostic factors, independent prognostic factors before surgery were limited and different between PC and BDC in the multivariable analysis. To clarify the institutional operative indication when a solitary PALN metastasis is diagnosed by sampling during surgery, a prospective trial based on the present results is necessary unless a definite proposal or recommendation has been made by the nationwide guidelines. Future novel adjuvant chemotherapy or treatment for recurrence is expected to control PALN metastasis or other oligometastases in distant regions of PBC.
Author Contributions
AN contributed to the conception and design of this study and wrote this article. JA managed and collected data from Nagasaki University. MH, NI, TH, YT, IS, and TO contributed to collecting patient data from the University of Miyazaki. HK contributed to supervising the preoperative diagnosis, and YS contributed to supervising the histological findings. All authors contributed to the article and approved it.
Funding
This study received no funding or financial support.
Institutional Review Board Statement
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. The study was conducted in accordance with the Declaration of Helsinki in 2013. This study protocol was approved by the two institutions, and the study design was approved by the Ethics Review Board of NUGSBS and UoM (approval numbers: #24031804, March 19, 2024, and #O-1503, January 24, 2024, respectively).
Informed Consent Statement
Informed consent for this retrospective analysis was obtained from the patient using the opt-out procedures on the institutional website of each ethics committee for one month, but there was no disclaimer.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Acknowledgments
The entire text was edited by Elsevier, the English editing company for science and medicine (reference number ASLESTD1045174), on February 20th, 2024.
Conflicts of Interest
Not applicable to any conflict of interest in all authors for this study.
References
- Buanes, T.A. Role of surgery in pancreatic cancer. World J Gastroenterol. 2017, 23, 3765–3770. [Google Scholar] [CrossRef]
- Uenishi, T,; Ariizumi, S,; Aoki, T; , Ebata, T,; Ohtsuka, M,; Tanaka, E,; Yoshida, H,; Imura, S,; Ueno, M,; Kokudo, N,; Nagino, M,; Hirano, S,; Kubo, S,; Unno, M,; Shimada, M,; Yamaue, H,; Yamamoto, M,; Miyazaki, M,; Takada, T. Proposal of a new staging system for mass-forming intrahepatic cholangiocarcinoma: a multicenter analysis by the Study Group for Hepatic Surgery of the Japanese Society of Hepato-Biliary-Pancreatic Surgery. J Hepatobiliary Pancreat Sci. 2014, 21, 499–508. [Google Scholar] [CrossRef] [PubMed]
- Im, J,H,; Choi, G,H,; Lee, W,J,; Han, D,H,; Park, S,W,; Bang, S,; Choi, H,J,; Seong, J. Adjuvant radiotherapy and chemotherapy offer a recurrence and survival benefit in patients with resected perihilar cholangiocarcinoma. J Cancer Res Clin Oncol. 2021, 147, 2435–2445. [Google Scholar] [CrossRef] [PubMed]
- Maeta, T,; Ebata, T,; Hayashi, E,; Kawahara, T,; Mizuno, S,; Matsumoto, N,; Ohta, S,; Nagino, M,; Nagoya Surgical Oncology Group. Pancreatoduodenectomy with portal vein resection for distal cholangiocarcinoma. Br J Surg. 2017, 104, 1549–1557. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, L,; Lupinacci, R,M,; Svrcek, M,; Lesurtel, M,; Bubenheim, M,; Vuarnesson, H,; Balladur, P,; Paye, F. Para-aortic lymph node sampling in pancreatic head adenocarcinoma. Br J Surg. 2014, 101, 530–538. [Google Scholar] [CrossRef]
- Paiella, S,; Sandini, M,; Gianotti, L,; Butturini, G,; Salvia, R,; Bassi, C. The prognostic impact of para-aortic lymph node metastasis in pancreatic cancer: A systematic review and meta-analysis. Eur J Surg Oncol. 2016, 42, 616–624. [Google Scholar] [CrossRef]
- Petrova, E,; Mazzella, E,; Trojan, J,; Koch, C,; Schulze, F,; Bechstein, W,O,; Schnitzbauer, A,A. Prognostic value of paraaortic lymph node metastases in patients with ductal adenocarcinoma of the pancreatic head. Eur J Surg Oncol. 2023, 49, 996–1000. [Google Scholar] [CrossRef]
- Hempel, S,; Oehme, F,; Müssle, B,; Aust, D,E,; Distler, M,; Saeger, H,D,; Weitz, J,; Welsch, T. Prognostic impact of para-aortic lymph node metastases in non-pancreatic periampullary cancer. World J Surg Oncol. 2020, 18, 16. [Google Scholar] [CrossRef]
- Okada, K,; Uemura, K,; Kondo, N,; Sumiyoshi, T,; Seo, S,; Otsuka, H,; Serikawa, M,; Ishii, Y,; Tsuboi, T,; Murakami, Y,; Takahashi, S. Preoperative risk factors for para-aortic lymph node positivity in pancreatic cancer. Pancreatology. 2021, 21, 606–612. [Google Scholar] [CrossRef]
- Sho, M,; Murakami, Y,; Motoi, F,; Satoi, S,; Matsumoto, I,; Kawai, M,; Honda, G,; Uemura, K,; Yanagimoto, H,; Kurata, M,; Fukumoto, T,; Akahori, T,; Kinoshita, S,; Nagai, M,; Nishiwada, S,; Unno, M,; Yamaue, H,; Nakajima, Y. Postoperative prognosis of pancreatic cancer with para-aortic lymph node metastasis: a multicenter study on 822 patients. J Gastroenterol. 2015, 50, 694–702. [Google Scholar] [CrossRef]
- Doussot, A,; Bouvier, A,; Santucci, N,; Lequeu, J,B,; Cheynel, N,; Ortega-Deballon, P,; Rat, P,; Facy, O. Pancreatic ductal adenocarcinoma and paraaortic lymph nodes metastases: The accuracy of intraoperative frozen section. Pancreatology. 2019, 19, 710–715. [Google Scholar] [CrossRef]
- Paiella, S,; Malleo, G,; Maggino, L,; Bassi, C,; Salvia, R,; Butturini, G. Pancreatectomy with Para-Aortic Lymph Node Dissection for Pancreatic Head Adenocarcinoma: Pattern of Nodal Metastasis Spread and Analysis of Prognostic Factors. J Gastrointest Surg. 2015, 19, 1610–1613. [Google Scholar] [CrossRef] [PubMed]
- Murakami, Y,; Uemura, K,; Sudo, T,; Hashimoto, Y,; Nakashima, A,; Kondo, N,; Sakabe, R,; Kobayashi, H,; Sueda, T. Is para-aortic lymph node metastasis a contraindication for radical resection in biliary carcinoma? World J Surg. 2011, 35, 1085–1093. [Google Scholar] [CrossRef] [PubMed]
- Nitta, N,; Ohgi, K,; Sugiura, T,; Okamura, Y,; Ito, T,; Yamamoto, Y,; Ashida, R,; Otsuka, S,; Sasaki, K,; Uesaka, K. Prognostic Impact of Paraaortic Lymph Node Metastasis in Extrahepatic Cholangiocarcinoma. World J Surg. 2021, 45, 581–589. [Google Scholar] [CrossRef] [PubMed]
- Takagi, K,; Nagai, Y,; Umeda, Y,; Yoshida, R,; Yoshida, K,; Fuji, T,; Kumano, K,; Yasui, K,; Yagi, T,; Fujiwara, T. Prognostic Value of the Regional Lymph Node Station in Pancreatoduodenectomy for Ampullary Carcinoma. In Vivo. 2022, 36, 973–978. [Google Scholar] [CrossRef] [PubMed]
- Asaoka, T,; Miyamoto, A,; Maeda, S,; Hama, N,; Tsujie, M,; Ikeda, M,; Sekimoto, M,; Nakamori, S. CA19-9 level determines therapeutic modality in pancreatic cancer patients with para-aortic lymph node metastasis. Hepatobiliary Pancreat Dis Int. 2018, 17, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Safi, S,A,; Rehders, A,; Haeberle, L,; Fung, S,; Lehwald, N,; Esposito, I,; Ziayee, F,; Krieg, A,; Knoefel, W,T,; Fluegen, G. Para-aortic lymph nodes and ductal adenocarcinoma of the pancreas: Distant neighbors? Surgery. 2021, 170, 1807–1814. [Google Scholar] [CrossRef]
- Kato, M,; Shimada, Y,; Tanaka, H,; Hosotani, R,; Ohshio, G,; Ishizaki, K,; Imamura, M. Characterization of six cell lines established from human pancreatic adenocarcinomas. Cancer. 1999, 85, 832–40. [Google Scholar] [CrossRef]
- Japan Pancreas Society. General rules for the study of pancreatic cancer, 7th edn, Revised and Enlarged version. In: Unno, M (eds.) Tokyo: Kanehara Co.; 2020: pp9-81 (in Japanese).
- Japanese Society of Hepato-Biliary-Pancreatic Surgery. General rules for clinical and pathological studies on cancer of the biliary tract, 7th edn. In: Sano, K (eds.) Tokyo: Kanehara Co.; 2021:pp15-74 (in Japanese).
- Ni, X,G,; Bai, X,F,; Mao, Y,L,; Shao, Y,F,; Wu, J,X,; Shan, Y,; Wang, C,F,; Wang, J,; Tian, Y,T,; Liu, Q,; Xu, D,K,; Zhao, P. The clinical value of serum CEA, CA19-9, and CA242 in the diagnosis and prognosis of pancreatic cancer. Eur J Surg Oncol. 2005, 31, 164–169. [Google Scholar] [CrossRef]
- Kurita, A,; Kodama, Y,; Nakamoto, Y,; Isoda, H,; Minamiguchi, S,; Yoshimura, K,; Kuriyama, K,; Sawai, Y,; Uza, N,; Hatano, E,; Uemoto, S,; Togashi, K,; Haga, H,; Chiba, T. Impact of EUS-FNA for preoperative para-aortic lymph node staging in patients with pancreatobiliary cancer. Gastrointest Endosc 2016, 84, 467–475. [Google Scholar] [CrossRef]
- De Gaetano, A,M,; Rufini, V,; Castaldi, P,; Gatto, A,M,; Filograna, L,; Giordano, A,; Bonomo, L. Clinical applications of (18)F-FDG PET in the management of hepatobiliary and pancreatic tumors. Abdom Imaging. 2012, 37, 983–1003. [Google Scholar] [CrossRef]
- Kim, J,S,; Hwang, H,K,; Lee, W,J,; Kang, CM. Unexpected Para-aortic Lymph Node Metastasis in Pancreatic Ductal Adenocarcinoma: a Contraindication to Resection? J Gastrointest Surg. 2020, 24, 2789–2799. [Google Scholar] [CrossRef] [PubMed]
- Kazami, Y,; Oba, A,; Ono, Y,; Sato, T,; Inoue, Y,; Saiura, A,; Takahashi, Y,; Ito, H. Intraoperative paraaortic lymph node sampling during resection for pancreatic cancer: evolving role in the modern chemotherapy era. HPB (Oxford). 2023, 25, 1169–1178. [Google Scholar] [CrossRef] [PubMed]
- Lin, J,Y,; Zhang, X,M,; Kou, J,T,; Fa, H,; Zhang, X,X,; Dai, Y,; He, Q. Analysis of prognostic factors for pancreatic head cancer according to para-aortic lymph node. Cancer Med. 2016, 5, 2701–2707. [Google Scholar] [CrossRef]
- van Rijssen, L,B,; Narwade, P,; van Huijgevoort, N,C,; Tseng, D,S,; van Santvoort, H,C,; Molenaar, I,Q,; van Laarhoven, H,W,; van Eijck, C,H,; Busch, O,R,; Besselink, M,G; Dutch Pancreatic Cancer Group. Prognostic value of lymph node metastases detected during surgical exploration for pancreatic or periampullary cancer: a systematic review and meta-analysis. HPB (Oxford). 2016, 18, 559–566. [Google Scholar] [CrossRef]
- Hempel, S,; Plodeck, V,; Mierke, F,; Distler, M,; Aust, D,E,; Saeger, H,D,; Weitz, J,; Welsch, T. Para-aortic lymph node metastases in pancreatic cancer should not be considered a watershed for curative resection. Sci Rep. 2017, 7, 7688. [Google Scholar] [CrossRef] [PubMed]
- Geerinckx, B,; Teuwen, L,A,; Foo, T,; Vandamme, T,; Smith, A,; Peeters, M,; Price, T. Novel therapeutic strategies in pancreatic cancer: moving beyond cytotoxic chemotherapy. Expert Rev Anticancer Ther. 2023, 23, 1237–1249. [Google Scholar] [CrossRef]
- Hadfield, M,J,; DeCarli, K,; Bash, K,; Sun, G,; Almhanna, K. Current and Emerging Therapeutic Targets for the Treatment of Cholangiocarcinoma: An Updated Review. Int J Mol Sci. 2023, 25, 543. [Google Scholar] [CrossRef]
- Wahler, I,L,; Damanakis, A,; Große, Hokamp, N,; Bruns, C,; Schmidt, T. Therapy of Locally Advanced and Oligometastatic Pancreatic Adenocarcinoma. Cancers (Basel). 2023, 15, 5881. [Google Scholar] [CrossRef]
- Sperti, C,; Gruppo, M,; Blandamura, S,; Valmasoni, M,; Pozza, G,; Passuello, N,; Beltrame, V,; Moletta, L. Para-aortic node involvement is not an independent predictor of survival after resection for pancreatic cancer. World J Gastroenterol. 2017, 23, 4399–4406. [Google Scholar] [CrossRef]
- Hong, S,M,; Goggins, M,; Wolfgang, C,L,; Schulick, R,D,; Edil, B,H,; Cameron, J,L,; Handra-Luca, A,; Herman, J,M,; Hruban, R,H. Vascular invasion in infiltrating ductal adenocarcinoma of the pancreas can mimic pancreatic intraepithelial neoplasia: a histopathologic study of 209 cases. Am J Surg Pathol. 2012, 36, 235–241. [Google Scholar] [CrossRef]
- Chen, J,W,; Bhandari, M,; Astill, D,S,; Wilson, T,G,; Kow, L,; Brooke-Smith, M,; Toouli, J,; Padbury, R,T. Predicting patient survival after pancreaticoduodenectomy for malignancy: histopathological criteria based on perineural infiltration and lymphovascular invasion. HPB (Oxford). 2010, 12, 101–108. [Google Scholar] [CrossRef]
- Chatelain, D,; Farges, O,; Fuks, D,; Trouillet, N,; Pruvot, F,R,; Regimbeau, J,M. Assessment of pathology reports on hilar cholangiocarcinoma: the results of a nationwide, multicenter survey performed by the AFC-HC-2009 study group. J Hepatol. 2012, 56, 1121–1128. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y,; Li, L,; Qu, C,; Liang, S,; Zeng, B,; Luo, Z. Endoscopic ultrasound-guided fine needle core biopsy for the diagnosis of pancreatic malignant lesions: a systematic review and Meta-Analysis. Sci Rep. 2016, 6, 22978. [Google Scholar] [CrossRef] [PubMed]
- Larghi, A,; Correale, L,; Ricci, R,; Abdulkader, I,; Monges, G,; Iglesias-Garcia, J,; Giovannini, M,; Attili, F,; Vitale, G,; Hassan, C,; Costamagna, G,; Rindi, G. Interobserver agreement and accuracy of preoperative endoscopic ultrasound-guided biopsy for histological grading of pancreatic cancer. Endoscopy. 2015, 47, 308–314. [Google Scholar]
- Asakura, Y,; Toyama, H,; Ishida, J,; Asari, S,; Terai, S,; Shirakawa, S,; Yamashita, H,; Shimizu, T,; Ogura, Y,; Matsumoto, I,; Gon, H,; Tsugawa, D,; Komatsu, S,; Kuramitsu, K,; Yanagimoto, H,; Kido, M,; Ajiki, T,; Fukumoto, T. Clinicopathological variables and risk factors for lung recurrence after resection of pancreatic ductal adenocarcinoma. Asian J Surg. 2023, 46, 207–212. [Google Scholar] [CrossRef]
- Agalianos, C,; Gouvas, N,; Papaparaskeva, K,; Dervenis, C. Positive para-aortic lymph nodes following pancreatectomy for pancreatic cancer. Systematic review and meta-analysis of impact on short term survival and association with clinicopathologic features. HPB (Oxford). 2016, 18, 633–641. [Google Scholar] [CrossRef]
- Birnbaum, D,J,; Viganò, L,; Russolillo, N,; Langella, S,; Ferrero, A,; Capussotti, L. Lymph node metastases in patients undergoing, surgery for a gallbladder cancer. Extension of the lymph node dissection and prognostic value of the lymph node ratio. Ann Surg Oncol. 2015, 22, 811–8. [Google Scholar] [CrossRef]
Figure 1.
Overall (OS) and disease-free survival (DFS) in patients with pancreatic cancer (PC) with or without paraaortic lymph node (PALN) metastasis. The Kaplan–Meier survival curves and log-rank test. Survival rates in each year, number of cancer deaths, and mean survival periods (months) were compared between patients with and without PALN metastasis.
Figure 1.
Overall (OS) and disease-free survival (DFS) in patients with pancreatic cancer (PC) with or without paraaortic lymph node (PALN) metastasis. The Kaplan–Meier survival curves and log-rank test. Survival rates in each year, number of cancer deaths, and mean survival periods (months) were compared between patients with and without PALN metastasis.
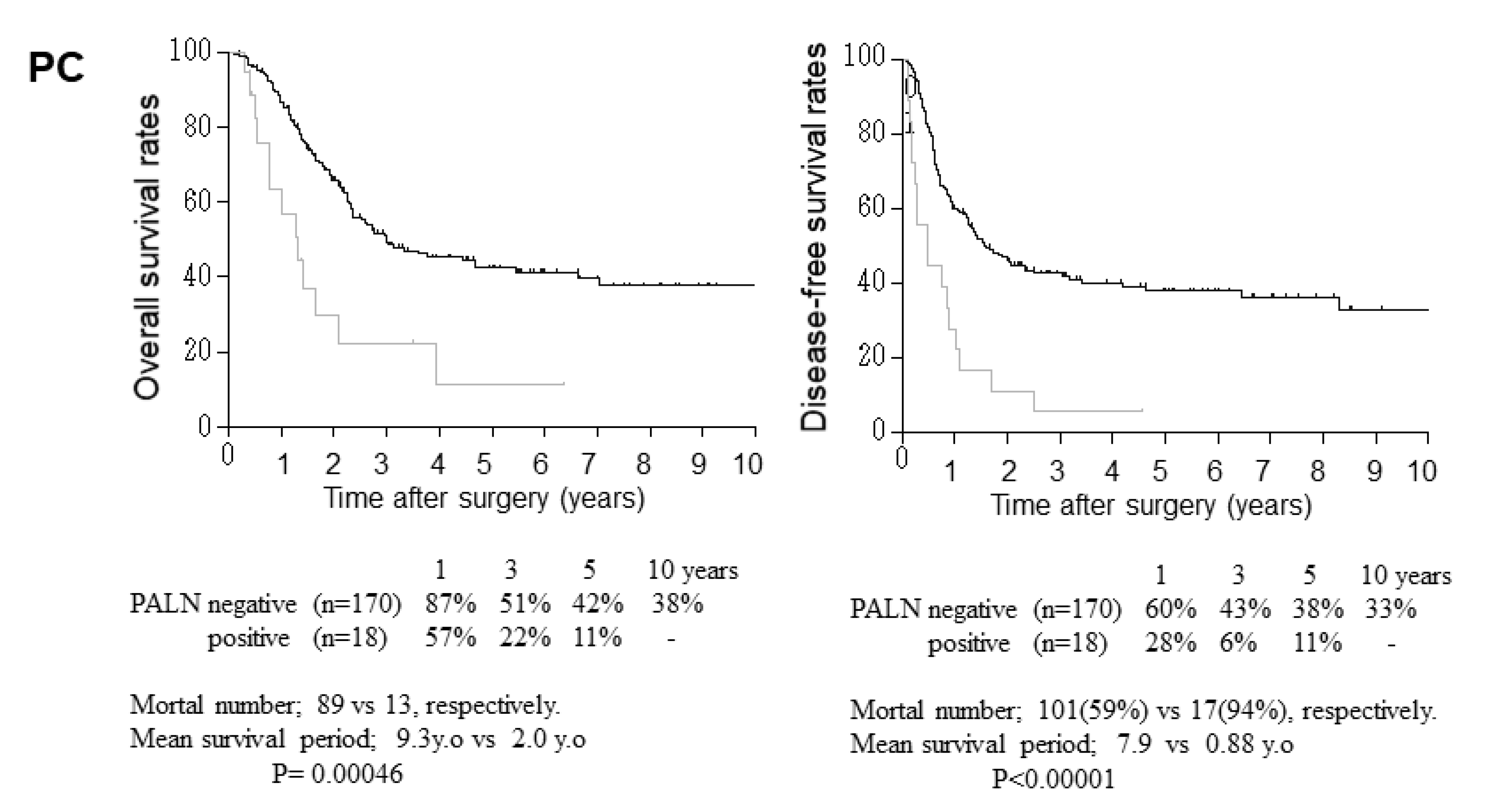
Figure 2.
Overall (OS) and disease-free survival (DFS) in patients with bile duct cancer (BDC) with or without paraaortic lymph node (PALN) metastasis. The Kaplan–Meier survival curves and log-rank test. Survival rates in each year, number of cancer deaths, and mean survival periods (months) were compared between patients with and without PALN metastasis.
Figure 2.
Overall (OS) and disease-free survival (DFS) in patients with bile duct cancer (BDC) with or without paraaortic lymph node (PALN) metastasis. The Kaplan–Meier survival curves and log-rank test. Survival rates in each year, number of cancer deaths, and mean survival periods (months) were compared between patients with and without PALN metastasis.
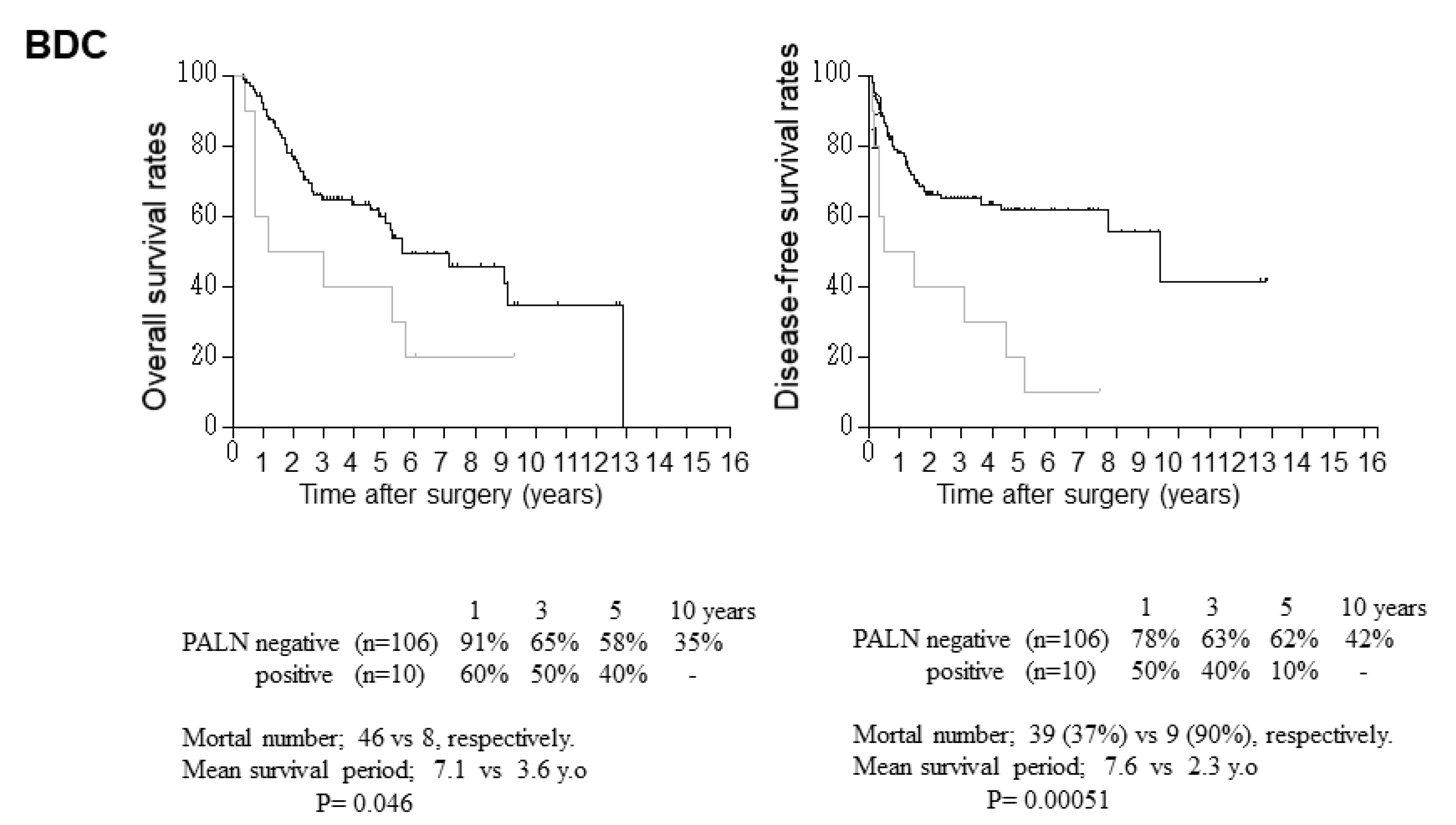

Table 1.
Cox’s proportional hazard analysis for patient prognosis in PC undergoing surgical resection.
Table 1.
Cox’s proportional hazard analysis for patient prognosis in PC undergoing surgical resection.
| a) Overall survival. | ||||||
|---|---|---|---|---|---|---|
| Univariate analysis | Multivariable analysis | |||||
| Probability (p-value) |
Risk ratio | 95% CI Lower - Upper |
Probability (p-value) |
Risk ratio | 95% CI Lower - Upper |
|
| Age, >70 years Sex, female CEA, >5 ng/ml CA199, >37 U/ml DUPAN-II, >150U/ml NAC, yes PD, yes Morphology, invasive Tumor size, >2cm Differentiation, moderately or poorly Histologic infiltration, yes lymphatic venous perineural Tumor involvement, yes retroperitoneal choledochal duodenal portal vein Node metastasis, yes Regional (RLN) para-aortic (PALN) Cancer positive at surgical margin, proximal bile duct exposed area Curability, R1 Adjuvant chemotherapy, yes Chemotherapy for cancer recurrence, yes |
.983 .428 .706 .004 .143 .021 .015 .004 .101 .000 .000 .000 .000 .000 .004 .000 .005 .000 .004 .022 .000 .011 .686 .770 |
.995 1.172 1.099 1.800 1.504 .459 1.711 1.489 1.485 2.837 3.289 4.582 4.036 2.145 1.653 1.781 1.879 3.325 2.447 3.874 4.966 2.208 1.085 1.063 |
.651 - 1.521 .792 - 1.735 .672 - 1.797 1.212 - 2.674 .871 - 2.597 .237 - .887 1.111 - 2.637 1.138 - 1.949 .925 - 2.383 1.768 - 4.555 2.094 - 5.166 2.365 - 8.876 2.339 - 6.964 1.400 - 3.287 1.178 - 2.321 1.363 - 2.326 1.208 - 2.922 2.162 - 5.113 1.332 - 4.493 1.212 - 12.385 2.572 - 9.591 1.197 - 4.072 .731 - 1.609 .706 - 1.599 |
.419 .003 .076 .075 .004 .028 .824 .005 .662 .259 .105 .199 .167 .234 .069 .041 .632 |
1.211 .269 1.760 .693 2.442 1.967 .824 2.841 .878 .736 1.395 1.461 1.481 1.597 3.268 2.483 1.195 |
.761 - 1.926 .114 - .641 .942 - 3.288 .462 - 1.038 1.326 - 4.499 1.077 - 3.594 .320 - 2.122 1.376 - 5.865 .489 - 1.574 .432 - 1.253 .932 - 2.088 .820 - 2.604 .849 - 2.582 .739 - 3.449 .912 - 11.704 1.036 - 5.948 .576 - 2.480 |
| b) Cancer-free survival. | ||||||
| Univariate analysis | Multivariable analysis | |||||
|
Probability (p-value) |
Risk ratio |
95% CI Lower - Upper |
Probability (p-value) |
Risk ratio |
95% CI Lower - Upper |
|
| Age, >70 years Sex, female CEA, >5 ng/ml CA199, >37 U/ml DUPAN-II, >150U/ml NAC, yes PD, yes Blood loss, >1500ml Morphology, invasive Tumor size, >2cm Differentiation, moderately or poorly Infiltration, yes lymph duct venous perineural Tumor involvement, yes retroperitoneal choledochal duodenal portal vein Node metastasis, yes Regional (RLN) para-aortic (PALN) Cancer positive at surgical margin, proximal bile duct exposed area Curability, R1 Adjuvant chemotherapy, yes Chemotherapy for cancer recurrence, yes |
.936 .279 .440 .001 .119 .051 .461 .098 .000 .540 .000 .000 .000 .000 .000 .033 .000 .007 .000 .004 .041 .000 .010 .360 .001 |
1.016 1.222 1.188 1.911 1.501 0.232 1.155 1.788 1.609 1.139 2.860 3.726 4.358 3.654 2.853 1.404 2.018 1.762 3.705 2.779 3.337 4.838 2.146 .840 1.862 |
.690 - 1.496 .850 - 1.757 .767 - 1.842 1.324 - 2.759 .901 - 2.501 0.061 - 1.020 .788 - 1.693 .897 - 2.033 1.243 - 2.082 .752 - 1.752 1.858 - 4.403 2.417 - 5.746 2.425 - 7.835 2.286 - 5.841 1.885 - 4.320 1.029 - 1.917 1.520 - 2.679 1.168 - 2.658 2.460 - 5.580 1.632 - 4.731 1.052 - 10.588 2.684 - 8.721 1.199 - 3.842 .579 - 1.219 1.283 - 2.702 |
.258 .801 .389 .005 .062 .870 .013 .970 .131 .051 .570 .110 .198 .217 .101 .749 .099 .077 |
1.279 1.078 .839 2.195 1.727 1.068 2.206 1.011 .674 1.522 1.173 1.536 1.578 2.209 2.049 1.133 .670 1.539 |
.835 - 1.960 .600 - 1.937 .562 - 1.251 1.271 - 3.789 .973 - 3.065 .486 - 2.349 1.180 - 4.121 .578 - 1.768 .404 - 1.125 .997 - 2.322 .676 - 2.036 .908 - 2.600 .788 -3.158 .627 - 7.785 .870 - 4.823 .527 - 2.440 .416 - 1.078 .954 - 2.485 |
CI: Confidence interval, CEA; carcinoembryonic antigen, CA19-9: cancer antigen 19-9, DUPAN-II: Duke pancreatic mono-clonal antigen type 2, NAC: neoadjuvant chemotherapy by gemcitabine+S-1, PD: pancreaticoduodenectomy, R1: histologically cancer positive at the cutting edge of specimens.
Table 2.
Cox’s proportional hazard analysis for patient prognosis in BDC undergoing surgical.resection.
Table 2.
Cox’s proportional hazard analysis for patient prognosis in BDC undergoing surgical.resection.
| a) Overall survival. | ||||||
|---|---|---|---|---|---|---|
| Univariate analysis | Multivariable analysis | |||||
| Probability (p-value) |
Risk ratio |
95% CI Lower - Upper |
Probability (p-value) |
Risk ratio | 95% CI Lower - Upper |
|
| Age, >70 years Sex, female jaundice, yes Total bilirubin, >2mg/dL ALP, >400U/ml CEA, >5 ng/ml CA19-9, >37 U/ml Blood loss, >1500mL Morphology, invasive Tumor size, >2cm Differentiation, moderately or poorly Infiltration, yes lymph duct venous perineural Depth, beyond subserosa Tumor invasion liver gallbladder pancreas duodenum portal vein hepatic artery Cholangitis of bile duct, yes Node metastasis, yes Regional (RLN) para-aortic (PALN) Cancer positive at surgical margin proximal bile duct exposed area distal bile duct Curability, R1 PBMJ, yes Adjuvant chemotherapy, yes Chemotherapy for cancer recurrence, yes |
.052 .984 .115 .210 .087 .040 .005 .008 .150 .229 .056 .008 .001 .000 .000 .710 .257 .026 .416 .002 .046 .026 .003 .049 .080 .000 .348 .005 .002 .078 .000 |
.564 1.003 1.740 1.460 1.649 2.128 2.222 2.163 1.974 1.438 1.712 2.390 3.640 5.376 2.283 1.096 1.276 1.696 1.350 2.215 2.532 2.042 2.254 2.215 1.643 7.039 1.611 2.156 5.256 1.632 3.158 |
.316 - 1.006 .739 - 1.362 .874 - 3.466 .807 - 2.461 .929 - 2.927 1.034 - 4.379 1.272 - 3.883 1.220 - 3.836 .781 - 4.989 .795 - 2.603 .986 - 2.975 1.252 - 4.561 1.711 - 7.744 2.290 - 12.619 1.452 - 3.590 .676 - 1.776 .837 - 1.946 1.066 - 2.699 .655 - 2.780 1.340 - 3.660 1.017 - 6.301 1.087 - 3.835 1.310 - 3.877 1.010 - 4.614 .943 - 2.862 3.205 - 15.458 .595 - 4.361 1.259 - 3.691 1.834 - 15.068 .947 - 2.811 1.821 - 5.477 |
.660 .003 .051 .025 .025 .004 .654 .169 .864 .922 .495 .255 .049 .006 .672 .140 .000 |
1.280 3.325 2.817 4.042 5.290 7.529 1.195 2.012 1.188 1.152 1.398 1.625 6.896 18.114 .776 2.851 5.438 |
.427 - 3.839 1.103 - 10.019 .996 - 7.968 1.191 - 13.718 1.240 - 22.71 1.930 - 29.374 .548 - 2.604 .743 - 5.449 .166 - 8.506 .068 - 19.435 .535 - 3.652 .705 - 3.745 1.008 - 61.629 2.339 - 140.733 .239 - 2.517 .708 - 11.473 2.400 - 12.320 |
| b) Cancer-free survival. | ||||||
| Univariate analysis | Multivariable analysis | |||||
|
Probability (p-value) |
Risk ratio |
95% CI Lower - Upper |
Probability (p-value) |
Risk ratio |
95% CI Lower - Upper |
|
| Age, >70 years. Sex, female jaundice, yes Total bilirubin, >2mg/dL ALP, >400U/ml CEA, >5 ng/ml CA199, >37 U/ml Blood loss, >1500mL Morphology, invasive Tumor size, >2cm Differentiation, moderately or poorly Histologic infiltration, yes lymphatic venous perineural Depth, beyond subserosa Tumor invasion liver gallbladder pancreas duodenum portal vein hepatic artery Cholangitis of the proximal bile duct, yes Node metastasis, yes Regional (PLN) para-aortic (PALN) Cancer positive at surgical margin proximal bile duct exposed area distal bile duct Curability, R1 PBMJ, yes Adjuvant chemotherapy, yes Chemotherapy for cancer recurrence, yes |
.048 .563 .126 .434 .945 .105 .145 .056 .100 .118 .019 .009 .071 .001 .000 .863 .169 .007 .210 .001 .002 .008 .000 .001 .221 .000 .596 .048 .059 .249 .000 |
.544 .905 1.765 1.295 .978 1.854 1.561 1.455 2.436 1.642 1.996 2.485 2.760 4.165 2.646 .952 1.368 2.022 1.597 2.916 4.998 2.368 3.166 3.373 1.477 4.789 1.300 1.921 3.109 1.632 5.735 |
.298 - .994 .645 - 1.270 .853 - 3.652 .677 - 2.477 .524 - 1.826 .979 - 3.909 .858 - 2.838 .878 - 2.456 .844 - 7.034 .882 - 3.054 1.118 - 3.565 1.255 - 4.922 1.323 - 5.759 1.845 - 9.403 1.618 - 4.326 .545 - 1.665 .875 - 2.138 1.214 - 3.368 .769 - 3.317 1.536 - 5.535 1.813 - 13.781 1.248 - 4.491 1.769 - 5.667 1.626 - 6.999 .791 - 2.757 2.181 - 10.516 .493 - 3.425 1.003 - 3.024 .956 - 10.115 .786 - 2.530 3.147 - 10.450 |
.010 .110 .028 .350 .879 .097 .836 .321 .481 .013 .447 .242 .049 .000 |
3.662 2.027 3.352 1.704 .939 2.585 1.218 3.971 1.427 2.917 .577 2.551 2.763 12.944 |
1.370 - .3.661 1.143 - 9.831 1.560 - 8.792 .557 - 5.216 .418 - 2.109 .842 - 7.934 .190 - 7.823 .261 - 60.475 .531 - 3.836 1.258 - 6.765 .140 - 2.383 .530 - 12.260 1.005 - 7.597 4.640 - 36.104 |
ALP; alkaline phosphatase. See other abbreviations in Table 1.
Table 3.
Relationship between clinicopathological factors and regional or para-aortic lymph node metastasis in PC.
Table 3.
Relationship between clinicopathological factors and regional or para-aortic lymph node metastasis in PC.
| a) Univariate analysis. | ||||||||
|---|---|---|---|---|---|---|---|---|
| RLN metastasis | probability (p-value) |
PALN metastasis | probability (p-value) |
|||||
| negative (n=83) |
positive (n=98) |
negative (n=164) |
positive (n=17) |
|||||
| Age (years) | 69.3±8.8 | 67.0±9.9 | .190 | 68.5±9.4 | 64.0±9.2 | .103 | ||
| Gender, male/female | 47/36 | 44/54 | .846 | 91/73 | 9/8 | 1.0 | ||
| Operation., DP/ PD/ TP | 36/44/3 | 24/73/1 | .009 | 56/106/2 | 4/13/0 | .588 | ||
| CEA (ng/ml) | 14.6±86.5 | 7.7±24.1 | .884 | 6.8±20.5 | 50.6±189.8 | .886 | ||
| CA199 (U/ml) | 449±2280 | 557±1130 | <.001 | 406±982 | 1473±4710 | .115 | ||
| DUPAN-II (U/ml) | 543±2018 | 630±1188 | .004 | 569±1685 | 778±620 | .0012 | ||
| Neoadjuvant chemotherapy, no/yes | 78/5 | 93/4 | .810 | 92/72 | 13/4 | .056 | ||
| Morphology, Nodular/mixed/invasive/cystic/MPD |
14/1/40/26/2 | 27/1/68/2/0 | <.001 | 36/1/97/28/2 | 5/1/10/0/0 | .106 | ||
| Histological differentiation, papillary/well/moderately/poorly/other |
1/19/52/5/6 | 1/23/58/12/4 | .379 | 2/39/90/23/10 | 1/5/9/2/0 | .887 | ||
| Tumor size (cm) | 3.16±2.20 | 3.26±1.23 | .024 | 3.17±1.78 | 3.74±1.21 | .067 | ||
| Tumor infiltration, no/yes Lymphatic duct Venous Perineural |
55/28 37/46 36/47 |
19/79 8/90 10/88 |
<.001 <.001 <.001 |
73/91 45/119 43/121 |
1/16 1/16 2/15 |
.125 .126 .0047 |
||
| Extra-pancreatic involvement, no/yes Retro-pancreatic choledochal duodenal portal vein |
55/28 69/14 73/10 70/13 |
21/77 51/47 54/44 67/31 |
<.001 <.001 <.001 .022 |
75/89 113/51 116/48 126/38 |
0/17 6/11 10/7 10/7 |
<.001 .038 .436 .332 |
||
| PALN metastasis, no/yes | 81/2 | 83/15 | .0037 | - | - | - | ||
| R, 0/ 1 | 82/1 | 91/7 | .062 | 156/8 | 17/0 | <.001 | ||
| Adjuvant chemotherapy, no/yes | 48/35 | 59/39 | .864 | 92/72 | 15/2 | .021 | ||
| Cancer recurrence, no/yes | 49/34 | 15/83 | <.001 | 63/101 | 1/16 | .016 | ||
| Recurrence-free Survival (days) | 1385±472 | 472±553 | <.001 | 948±1129 | 333±416 | <.002 | ||
| Overall survival (days) | 1599±1275 | 815±802 | <.001 | 1235±1139 | 595±582 | .0028 | ||
| b) Multivariate logistic regression analysis. | ||||||||
| PLN | PALN | |||||||
|
Probability p-value |
Odds ratio | 95%CI lower | 95%CI upper |
Probability p-value |
Odds ratio | 95%CI lower | 95%CI upper | |
| Op., PD | .363 | .260 | .014 | 4.719 | ||||
| CA199, >37U/mL | .957 | 1.028 | .377 | 2.801 | ||||
| Dupan-II, >150u/mL | .598 | 1 | 1 | 1 | .023 | 4.921 | 1.243 | 19.475 |
| Morphology, invasive | .261 | 1.614 | .701 | 3.719 | ||||
| Size, >20mm | .406 | 1.637 | .511 | 5.244 | ||||
| Lymphatic invasion | .089 | 2.483 | .872 | 7.07 | ||||
| Venous invasion | .884 | .887 | .176 | 4.458 | ||||
| Perineural invasion | .104 | 3.222 | .786 | 13.217 | .141 | .2807 | .025 | 1.689 |
| Extra-pancreatic involvement Retro-pancreatic |
.080 |
2.681 |
.888 |
8.091 |
.997 |
5.760 |
.001 |
16.355 |
| Choledochal | .383 | 1.654 | .535 | 5.114 | .226 | 2.38 | .585 | 9.673 |
| Duodenal | .189 | 2.376 | .654 | 8.627 | ||||
| PALN metastasis, yes | .502 | 1.889 | .295 | 12.106 | ||||
Table 4.
Relationship between clinicopathological factors and regional or para-aortic lymph node metastasis in BDC.
Table 4.
Relationship between clinicopathological factors and regional or para-aortic lymph node metastasis in BDC.
| a) Univariate analysis. | ||||||||
|---|---|---|---|---|---|---|---|---|
| RLN metastasis | probability (p-value) |
PALN metastasis | probability (p-value) |
|||||
| negative (n=71) |
positive (n=45) |
negative (n=106) |
positive (n=10) |
|||||
| Age (years) | 69.8±10.6 | 66.4±12.3 | .092 | 69.5±10.2 | 58.2±17.3 | .027 | ||
| Gender, male/female | 55/16 | 30/15 | .286 | 79/27 | 6/4 | .454 | ||
| Operation, PD/HPD/Hepatectomy | 1944/4/23 | 2026/7/12 | .238 | 66/7/33 | 2004/4/2 | .0092 | ||
| Total bilirubin (mg/dl) | 1.49±2.40 | 1.45±1.39 | .120 | 1.51±2.14 | 1.10±0.40 | .593 | ||
| Alkaline phosphatase (U/ml) | 475±438 | 634±540 | .037 | 521±477 | 702±562 | .196 | ||
| CEA (ng/ml) | 6.0±24.3 | 3.8±3.6 | .089 | 5.3±19.8 | 3.0±2.2 | .928 | ||
| CA199 (U/ml) | 4394±33262 | 502±995 | .0019 | 3075±26940 | 324±729 | .310 | ||
| Jaundice, no/yes | 20/51 | 10/35 | .677 | 28/78 | 3/7 | .713 | ||
| PBMJ, no/yes | 69/2 | 43/2 | 1 | 103/3 | 9/1 | .809 | ||
| Morphology, Papillary/nodular/invasive/IPNB | 15/31/24/1 | 3/6/36/0 | .300 | 17/7/81/1 | 0/0/10/0/0 | .362 | ||
| Cholangitis of the proximal bile duct, no/yes | 52/19 | 31/14 | .484 | 81/25 | 6/4 | .078 | ||
| Histological differentiation, papillary/well/moderately/poorly/other |
12/31/19/9 | 2/19/19/5 | .134 | 13/43/36/14 | 1/5/3/1/0 | .535 | ||
| Tumor size (cm) | 1.56±1.55 | 2.34±1.69 | .036 | 1.72±1.57 | 3.54±1.62 | .0006 | ||
| Depth of invasion, m, fm/ss/se/si | 16/35/12/8 | 1/23/13/8 | .056 | 15/49/21/13 | 0/5/2/3 | .252 | ||
| Tumor infiltration, no/yes Lymphatic duct Venous Perineural |
37/34 31/40 30/41 |
5/40 6/39 6/39 |
<.001 .001 .002 |
41/65 37/69 35/71 |
0/10 0/10 1/9 |
.033 .052 .238 |
||
| Extra-pancreatic involvement, no/yes liver gallbladder pancreas duodenum portal vein hepatic artery |
63/8 68/3 52/19 63/8 68/3 70/1 |
38/7 43/2 19/26 3510 39/6 44/1 |
.017 .055 .0005 .196 .163 .333 |
87/19 104/2 67/39 88/18 100/6 104/2 |
6/4 6/4 3/7 10/0 7/3 10/0 |
.201 <.001 .029 .358 .011 .907 |
||
| Number of node metastasis | 0.82±4.09 | 1.94±1.56 | <.001 | 1.17±3.59 | 1.96±2.22 | .226 | ||
| PALN metastasis, no/yes | 69/2 | 37/8 | .0139 | - | - | - | ||
| Cancer positive at cutting edge, no/yes bile duct exposed area |
58/13 68/3 |
35/10 38/7 |
.578 .079 |
87/19 100/6 |
6/4 6/4 |
.202 .002 |
||
| R, 0/ 1 | 57/14 | 30/15 | .212 | 82/24 | 4/6 | .029 | ||
| Cancer recurrence, no/yes | 49/34 | 15/83 | <.001 | 67/39 | 1/9 | .00034 | ||
| Recurrence-free Survival (days) | 14195±1105 | 787±942 | <.001 | 1203±1096 | 836±941 | .171 | ||
| Overall survival (days) | 1605±1083 | 1059±943 | .0014 | 1411±1058 | 1206±1132 | .4 | ||
| b) Multivariate logistic regression analysis. | ||||||||
| RLN metastasis | PALN metastasis | |||||||
|
Probability p-value |
Odds ratio | 95%CI lower | 95%CI upper |
Probability p-value |
Odds ratio | 95%CI lower | 95%CI upper | |
| Age, >70 | .161 | .182 | .017 | 1.969 | ||||
| ALP, >400U/ml | .694 | .777 | .221 | 2.731 | ||||
| CA199, >37U/mL | .177 | 2.345 | .68 | 8.084 | ||||
| Op., PD | .286 | 4.345 | .292 | 64.649 | ||||
| Size, >20mm | .876 | 1.113 | .292 | 4.241 | .156 | 4.38 | .569 | 33.702 |
| Lymphatic invasion | .016 | 5.561 | 1.376 | 22.468 | .997 | 2.512 | .001 | 100.678 |
| Venous invasion | .361 | .487 | .104 | 2.282 | ||||
| Perineural invasion | .032 | 5.094 | 1.152 | 22.523 | ||||
| Organ involvement Liver Gallbladder Pancreas Portal vein |
.026 .002 |
4.582 7.204 |
2. 123 3.455 |
24.448 42.159 |
.290 .143 .204 |
3.325 7.843 2.788 |
.359 .497 .573 |
30.797 123.835 13.560 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



