
Submitted:
21 August 2024
Posted:
22 August 2024
You are already at the latest version
Abstract
Background: The Fat-Augmented Latissimus Dorsi (FALD) flap is an autologous flap that combines Latissimus Dorsi (LD) flap with immediate autologous fat transfer (AFT) in order to improve breast reconstruction (BR) volume. In recent years, our team has described the ergonomic FALD flap, an evolution of this technique which helps to achieve a complete BR in a single surgical step. In this long-term study, we analyze morphological variations of the breast after ergonomic FALD flap reconstruction compared to the traditional transverse FALD flap technique. Methods: Between December 2020 and September 2022 we prospectively enroll patients undergoing BR using FALD flap into 2 groups: Group A included ergonomic FALD flap, while Group B included traditional FALD flap. The primary endpoint of the study was to compare the two groups in terms of breast projection (BP), breast width (BW) and breast height (BH), while the second endpoint concerned the analysis of the aesthetic outcomes. Results: 32 FALD flaps (23 patients) were performed for the Group-A and 31 FALD flaps (25 patients) for Group-B. There were no significant differences regarding demographic variables. After propensity score weighting analysis, Group-A showed a statistically significant better breast projection (p<0.0001) compared to Group-B. (6.05 vs 5.60). Final aesthetic analyses showed to be superior in Group-A concerning breast shape (p=0.001) and global score evaluation (p=0.004). Conclusion: The ergonomic FALD flap offers better long-term aesthetic outcomes for autologous BR with higher breast projection compared to the traditional transverse FALD flap.
Keywords:
breast reconstruction
; autologous breast reconstruction
; ergonomic flap
; latissimus dorsi flap
; FALD flap
; fat grafting
; autologous fat transfer
; aesthetic outcomes
; pedicled flap
Introduction
The Fat-Augmented Latissimus Dorsi (FALD) flap is a totally autologous flap recently described for breast reconstruction (BR) [1,2]. It combines Latissimus Dorsi (LD) flap reconstruction with immediate intraoperative autologous fat transfer (AFT) in order to improve its volume [3]. Intraoperative AFT is usually performed into the flap at the level of the subcutaneous adipose tissue of the skin paddle and below the LD muscle fascia cranially and caudally to the skin paddle [4]. At the recipient site, the AFT can be performed in mastectomy flaps in cases of delayed BR while it can be performed in the loose areolar space just below the major pectoralis muscle in case of immediate BR [5]. In recent years, our team has described an evolution of the FALD flap, i.e. the ergonomic FALD flap, characterized by a remodeling of the skin paddle and its vertical positioning at recipient breast site, which helps to achieve a complete BR in a single surgical step reducing the need for additional AFT sessions [6,7]. Specifically, the ergonomic position of the flap allows improving the shape of the new breast, filling both lower and upper poles appropriately and increasing the new breast projection [8,9].
In this long-term study, we analyze the morphological variations of the breast after the ergonomic FALD flap reconstruction compared to the traditional transverse FALD flap technique.
Patients and Methods
This is a prospective clinical study of a cohort of patients enrolled between December 2020 and September 2022 at our institute, the Policlinico Tor Vergata University Hospital, in accordance with the Declaration of Helsinki statement.
Inclusion criteria were patients scheduled for breast reconstruction using FALD flap, while exclusion criteria were patients with paraplegia problems or who practiced climbing or windsurfing. Breast candidates for Modified Radical Mastectomy (MRM) were also excluded from the study. Patients were randomly enrolled into 2 groups: Group A included BR using ergonomic FALD flap, while Group B included BR using traditional transverse FALD flap.
During the preoperative drawing of the LD skin paddle [Figure 1], we measured the breast projection (BP), breast width (BW) and breast height (BH) using a millimeter caliper in all patients.
Data regarding age, BMI, smoke, laterality, mastectomy type, timing of reconstruction, preoperative weight of the breast, intraoperative fat grafting volume, additional fat grafting sessions, duration of surgery and complications were collected, and breast pictures were taken. Preoperative volume assessments of the breast were performed using BREAST-V formula, available on the WebApp 3.0 www.braflap.com [10]. Exactly 12 months after breast reconstruction, all patients underwent accurate measurement of the post-operative breast projection (BP), breast width (BW) and breast height (BH) using a millimeter caliper [Figure 2].
Study Endpoints
The primary endpoint of our study was to evaluate the two groups in terms of breast projection (BP), breast width (BW) and breast height (BH), assessing whether these differences were statistically significant. The second endpoint was about the assessment of aesthetic outcomes in the groups. We used a modification of the rating scale described by Garbay et al. firstly and adapted by Carlson et al. [11,12] for the aesthetic analysis, comparing the treated breast to the preoperative situation or the contralateral by two independent blinded reconstructive surgeons, 12 months after reconstruction. Standardized photographs were used from 5 specific views: frontal view, oblique view from each lateral side and complete lateral view at each side. Volume, shape, breast mound placement, inframammary fold, texture of the skin and scar location were evaluated ranging from 0 to 2 and analyzed for statistical assessment (Table 1). The total score represents the sum of each subscale averages. We also assessed a global aesthetic score by categorizing each breast into one of 4 groups: excellent (treated breast nearly identical to opposite breast), good (treated breast only slightly different from opposite breast), fair (treated breast clearly different from opposite breast but not seriously distorted ) and poor (treated breast severely distorted), as described by Harris et al. [13] (Table 2).
Statistical Analysis
All patient data regarding demographics, surgical report and complications were collected in a database (Microsoft Excel Office 365, Redmond, WA, USA). Statistical analyses were performed using R version 4.4.1 (R Development Core Team, Vienna, Austria). Inter-rater reliability was calculated for all of the picture grading subscales and the total amount of the subscales using the Cohen’s Kappa [14]. The strength of agreement was classified considering the j score as follows: less than 0.00, poor; 0.00–0.20, slight; 0.21–0.40, fair; 0.41–0.60, moderate; 0.61–0.80, substantial; and 0.81–1.00, almost perfect agreement [15]. Continuous endpoints were compared between the two groups with a linear mixed regression model with a categorical predictor and random subject-specific intercepts, to take into account dependence arising from clustered data (i.e., two breasts from the same patient). Ordinal endpoints were compared with respect to their median with a similar mixed model devised for quantile regression [16,17]. Since patients are not randomized, we also compute a propensity score to balance for age, BMI, smoking status, timing, preoperative breast projection, preoperative breast width and height. The comparison of the two groups is then repeated with the same approach, after weighting for the propensity score of the assigned group. A p-value lower than 0.05 was considered as significant.
Results
We included in the study 32 ergonomic FALD flaps (23 patients) who belonged to group A and 31 traditional FALD flaps (25 patients) who belonged to group B. Statistical analysis did not show significant differences (p>0.05) between the groups concerning age, BMI, smoking habits, laterality, timing of BR, mastectomy type and preoperative breast volume. All results regarding patient data are summarized in Table 3.
We did not observe statistically significant differences regarding the preoperative breast projection (BP), breast width (BW) and breast height (BH) among the two groups (respectively p=0.408, p=0.247 and p=0.147). After 18 months from reconstruction, the average post-operative BP was 6.05 cm (SD 0.56, range 5.5 – 7.5) for group A, while 5.60 cm (SD 0.65, range 9.5 - 12) for group B, presenting a statistically significant difference (p<0.0001). Conversely, post-operative BW and BH had no statistically significant differences between the two groups, respectively p=0.477 and p=0.390. Mean post-operative BW was 11.00 cm for group A and 11.03 cm for group B, while BH was 10.63 cm for group A and 10.47 cm for group B [Table 4].
Mean intraoperative AFT volume was 173.9 cc (SD 34.0) for ergonomic flap group and 177.7 cc (SD 43.9) for control group, with no significant differences (p=0.351). Contrariwise, we observed a statistically significant difference between the groups regarding additional AFT (p<0.00001). Particularly, patients underwent ergonomic FALD reconstruction required 0.26 (SD 0.45) mean additional AFT sessions, while patients from the traditional FALD group 1.52 (SD 0.71).
The amount of surgical complications was similar between the active and control groups, with no statistically significant differences (p=0.973).
Aesthetic Outcome
The analysis of the surgeons’ assessment 12 months after breast reconstruction was performed using an adapted rating scale firstly described by Garbay et al. and modified by Carlson.
Only the comparison of breast shape was statistically superior in group A (p=0.001), while as regards the other variables taken into consideration, no significant difference was found [Table 5]. Furthermore, a statistically significant difference was observed regarding the global aesthetic score (3.44 vs 3.06; p=0.004), with superior aesthetic outcome in group A using a classification described by Harris et al.
Discussion
The FALD flap was a revolution in the field of breast reconstructive surgery as it allowed for a totally autologous BR, avoiding the use of breast implants and their possible short- and long-term complications [18,19,20,21]. Furthermore, this procedure does not require any microsurgical expertise [22,23,24].
A significant drawback of this technique initially described with a transverse skin paddle orientation at the breast recipient site, was the poor projection of the reconstructed breast and the emptying of the upper pole which required the need for several additional fat grafting sessions [25,26]. The additional AFT sessions were specifically aimed at filling the upper pole and giving better projection to the reconstructed breast. These defects have been overcome by an evolution of this flap, that is the ergonomic FALD flap, recently described by our team [6]. This modification allowed us to significantly reduce the additional AFT sessions and obtain a finalized result after the first reconstructive procedure. The key point is the folding of the de-epithelialized skin paddle, since the lower part of the skin paddle was folded back, suturing its inferior apex to the posterior surface of the LD muscle. In this way we try to replicate the shape of an anatomical implant [27,28]. [Video 1, https://drive.google.com/file/d/1gFaU4OlixutzGaxp0BpmV6RaK_POuOIC/view?usp=drive_link]
In 2018, Demiri et al. conducted an interesting study compared a series of delayed breast reconstructions using the FALD flap with implant-based reconstructions in irradiated patients, observing a significantly lower range of complications in FALD flaps [29]. Economides et al. in 2017 described a case series of patients undergoing FALD flap, demonstrating that the immediate infiltration of adipose tissue into the flap allows avoiding the use of breast implant [30].
In our prospective study we focused on evaluating the morphological variations of the reconstructed breast after the ergonomic FALD flap, comparing them with the traditional FALD flap. The statistical analysis highlighted a significant difference regarding the post-operative breast projection in favor of patients undergoing ergonomic FALD flap reconstruction (p<0.0001). The increase in breast projection is due to the vertical positioning of the skin paddle and its folding in the lower portion, ensuring good volume at the lower pole and at the same time fullness at the upper pole.
The management of the thoracodorsal nerve during the LD flap harvest is controversial in literature [31,32,33]. We do not denervate the LD muscle when performing a FALD flap, while we use to denervate the thoracodorsal nerve in cases of BR with LD flap and implant, in order to reduce muscle animation and possible implant migration [34,35]. In our opinion, leaving the thoracodorsal nerve intact could contribute to maintaining muscle trophism and therefore maintaining good projection and volume over time [36]. Furthermore, in our technique long-term maintenance of volume is due to the use of multiple recipient site for AFT located at the breast region, i.e. the retro-pectoral space between the pectoralis major and minor muscles, the subcutaneous adipose tissue of the mastectomy skin flaps, the subcutaneous tissue of LD skin paddle and the space under LD muscle fascia [3].
Regarding aesthetic assessment, the surgeons’ evaluation confirmed a better long-term aesthetic outcome of the ergonomic FALD flap compared to the traditional transverse FALD, especially in terms of breast shape.
Conclusion
The ergonomic FALD flap represents a valid alternative for autologous breast reconstruction with a good long-term aesthetic outcome. This technique allows to obtain a significantly higher breast projection and superior aesthetic results compared to the traditional FALD flap, maintaining an equal range of complications.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the tenets of the Declaration of Helsinki.
Informed Consent Statement
The study was conducted in accordance with the tenets of the Declaration of Helsinki. All patients were duly informed and signed a specific informed consent on the procedure before the surgery.
Conflicts of Interest disclosure statement
We, hereby certify, that to the best of our knowledge no financial support or benefits have been received by author or any co-author, by any member of our immediate family or any individual or entity with whom or with which we have a significant relationship from any commercial source which is related directly or indirectly to the scientific work which is reported on in the article. None of the authors has a financial interest in any of the products, devices, or drugs mentioned in this manuscript.
References
- Demiri EC, Tsimponis A, Pagkalos A, et al. Fat-Augmented Latissimus Dorsi versus Deep Inferior Epigastric Perforator Flap: Comparative Study in Delayed Autologous Breast Reconstruction. J Reconstr Microsurg. 2021;37(3):208-215. [CrossRef]
- Longo, B., D’orsi, G., Orlando, G., Giacalone, M. and Cervelli, V. 2022. Recurrent dermatofibrosarcoma protuberans of the clavicular region: radical excision and reconstruction with Latissimus Dorsi myocutaneous flap. Plastic Reconstructive and Regenerative Surgery. 1, 1 (Jul. 2022), 14–19. [CrossRef]
- Longo B, D’Orsi G, Vanni G, Gagliano E, Buonomo CO, Cervelli V. Fat-Augmented Latissimus Dorsi Flap for Secondary Breast Reconstruction in Small to Medium-Sized Irradiated Breasts. Plast Reconstr Surg. 2023;152(6):1165-1173. [CrossRef]
- Herbst, I. and Saltvig, I. 2022. Cannula tip breakage inside adipose tissue during liposuction – a rare case report. Plastic Reconstructive and Regenerative Surgery. 1, 2 (Nov. 2022), 76–78. [CrossRef]
- Longo B, D’Orsi G, Farcomeni A, et al. The FALD-V: A predictive formula for preoperative volume assessment of adipose tissue transplantation in FALD flap. J Plast Reconstr Aesthet Surg. 2024;90:25-34. [CrossRef]
- Longo B, D’Orsi G, Giacalone M, et al. The Ergonomic FALD Flap for One-stage Total Breast Reconstruction. Plast Reconstr Surg Glob Open. 2023;11(9):e5262. Published 2023 Sep 18. [CrossRef]
- Longo B, D’Orsi G, Farcomeni A, et al. The LD-V: An innovative formula for latissimus dorsi flap volume assessment. J Plast Reconstr Aesthet Surg. Published online July 14, 2024. [CrossRef]
- Longo B, Timmermans FW, Farcomeni A, et al. Septum-Based Mammaplasties: Surgical Techniques and Evaluation of Nipple-Areola Sensibility. Aesthetic Plast Surg. 2020;44(3):689-697. [CrossRef]
- Mazzocchi, M., Sigorini, G., Cerciello, E. and Barberini, F. 2022. The use of Exashape (TM) Bioshield Pocket in prepectoral breast reconstruction: a preliminary experience. Plastic Reconstructive and Regenerative Surgery. 1, 2 (Nov. 2022), 51–57. [CrossRef]
- Longo B, Farcomeni A, Ferri G, Campanale A, Sorotos M, Santanelli F. The BREAST-V: a unifying predictive formula for volume assessment in small, medium, and large breasts. Plast Reconstr Surg. 2013;132(1):1e-7e. [CrossRef]
- Garbay JR, Rietjens M, Petit JY. Résultats esthétiques de la reconstruction mammaire après amputation pour cancer. A propos de 323 cas [Esthetic results of breast reconstruction after amputation for cancer. 323 cases]. J Gynecol Obstet Biol Reprod (Paris). 1992;21(4):405-412. [PubMed]
- Carlson GW, Page AL, Peters K, Ashinoff R, Schaefer T, Losken A. Effects of radiation therapy on pedicled transverse rectus abdominis myocutaneous flap breast reconstruction. Ann Plast Surg. 2008;60(5):568-572. [CrossRef]
- Harris JR, Levene MB, Svensson G, Hellman S. Analysis of cosmetic results following primary radiation therapy for stages I and II carcinoma of the breast. Int J Radiat Oncol Biol Phys. 1979;5(2):257-261. [CrossRef]
- Cohen, J. A Coefficient of Agreement for Nominal Scales. Educational and Psychological Measurement. 1960;20(1):37-46. [CrossRef]
- Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159-174. [PubMed]
- Geraci M, Farcomeni A. Mid-quantile regression for discrete responses. Stat Methods Med Res. 2022;31(5):821-838. [CrossRef]
- Russo, A., Farcomeni, A., & Geraci, M. (2024). Mid-quantile regression for discrete panel data. Journal of Statistical Computation and Simulation, 1–18. [CrossRef]
- D’Orsi G, Giacalone M, Calicchia A, et al. BIA-ALCL and BIA-SCC: Updates on Clinical Features and Genetic Mutations for Latest Recommendations. Medicina (Kaunas). 2024;60(5):793. Published 2024 May 10. [CrossRef]
- Bottosso S, Sidoti GB, Vita L, et al. A Multi-Center Retrospective Observational Analysis of Three-Year Experience of Our Protocol for Prevention and Monitoring of Surgical Site Infections in Implant-Based Breast Reconstruction. Cancers (Basel). 2024;16(13):2439. Published 2024 Jul 2. [CrossRef]
- Liu L, Kim L, Teotia SS, Haddock NT. Long-term Implications of Cosmetic Breast Surgeries on Subsequent Breast Reconstruction. Aesthet Surg J. Published online June 24, 2024. [CrossRef]
- Longo B, Di Napoli A, Curigliano G, et al. Clinical recommendations for diagnosis and treatment according to current updated knowledge on BIA-ALCL. Breast. 2022;66:332-341. [CrossRef]
- Meier EL, Ulrich DJO, Hummelink S. Projected augmented reality in DIEP flap breast reconstruction: Projecting perforators on the skin using dynamic infrared thermography. J Plast Reconstr Aesthet Surg. 2024;94:83-90. [CrossRef]
- Longo B, Alberti FB, Pomahac B, et al. International consensus recommendations on face transplantation: A 2-step Delphi study. Am J Transplant. 2024;24(1):104-114. [CrossRef]
- Longo, B., Pistoia, A., D’Orsi, G., Gagliano, E., Vannucchi, L. and Cervelli, V. 2023. Lympho-diep flap transfer perfused by reverse-flow thoracodorsal artery: a case report. Plastic Reconstructive and Regenerative Surgery. 2, 1-2 (Oct. 2023), 20–24. [CrossRef]
- Longo B, D’Orsi G, La Padula S, et al. Narrow inferior-central septum-based pedicle: A safe technique to improve aesthetic outcomes in breast reduction. J Plast Reconstr Aesthet Surg. 2023;85:226-234. [CrossRef]
- Schonauer, F., Cavaliere, A., Pezone, G., D’Andrea, F., Longo, B., D’Orsi, G. and Cervelli, V. 2022. Thoraco-acromial artery perforator (TAAP) flap for reconstruction of a recurrent dermatofibrosarcoma protuberans of the clavicular region. Plastic Reconstructive and Regenerative Surgery. 1, 2 (Nov. 2022), 79–81. [CrossRef]
- D’Andrea, F., Errico, C., D’Andrea, L. and Zaffiro, A. 2023. The treatment of capsular contracture after breast surgery with implants using Capsulase®. Plastic Reconstructive and Regenerative Surgery. 2, 1-2 (Jul. 2023), 49–54. [CrossRef]
- Longo, B., Giacalone, M., Iundusi, R., D’Orsi, G., Gagliano, E., Vannucchi, L., Gargari, T., Tarantino, U. and Cervelli, V. 2023. Calcaneal hybrid reconstruction with femur head allograft enriched with bone marrow and ALT flap. Plastic Reconstructive and Regenerative Surgery. 2, 3 (Dec. 2023), 98–103. [CrossRef]
- Demiri EC, Dionyssiou DD, Tsimponis A, Goula CO, Pavlidis LC, Spyropoulou GA. Outcomes of Fat-Augmented Latissimus Dorsi (FALD) Flap Versus Implant-Based Latissimus Dorsi Flap for Delayed Post-radiation Breast Reconstruction. Aesthetic Plast Surg. 2018;42(3):692-701. [CrossRef]
- Economides JM, Song DH. Latissimus Dorsi and Immediate Fat Transfer (LIFT) for Complete Autologous Breast Reconstruction. Plast Reconstr Surg Glob Open. 2018;6(1):e1656. Published 2018 Jan 23. [CrossRef]
- Longo, B., Vannucchi, L., D’Orsi, G., Pistoia, A., Giacalone, M., Gagliano, E., Ventimiglia, M., Piscitelli, L., Di Giacomo, G., Vanni, G., Buonomo, O.C. and Cervelli, V. 2024. Shoulder function assessment after FALD flap breast reconstruction: comparing ultrasound results and patients’ self perception. Plastic Reconstructive and Regenerative Surgery. 3, 1 (May 2024), 9–16. [CrossRef]
- Otani N, Tomita K, Kuroda K, Taminato M, Kubo T. Effects of Temporary and Permanent Muscle Denervation on Fat Graft Retention in the Latissimus Dorsi Muscle: An Experimental Study in Rats. Aesthetic Plast Surg. 2022;46(4):1942-1949. [CrossRef]
- Escandón JM, Manrique OJ, Christiano JG, et al. Breast reconstruction with latissimus dorsi flap: a comprehensive review and case series. Ann Transl Med. 2023;11(10):355. [CrossRef]
- Taminato M, Tomita K, Nomori M, et al. Fat-augmented latissimus dorsi myocutaneous flap for total breast reconstruction: A report of 54 consecutive Asian cases. J Plast Reconstr Aesthet Surg. 2021;74(6):1213-1222. [CrossRef]
- Felici, N., Delle Femmine, P.F., Tosi, D., Ornelli, M., Mori, F.L.R., Turriziani, G. and Amadei, F. 2022. Common peroneal nerve injuries at the knee: outcomes of nerve repair. Plastic Reconstructive and Regenerative Surgery. 1, 1 (Jul. 2022), 6–13. [CrossRef]
- Messana, F., Lucchetta, G. , Bassetto, F. and Tiengo, C. 2024. Comparative evaluation of neurotubules and autologous nerve grafts for peripheral nerve repair: a retrospective case series. Plastic Reconstructive and Regenerative Surgery. 3, 1 (May 2024), 32–38. [CrossRef]
Figure 1.
Preoperative markings on the back of bilateral FALD flap.
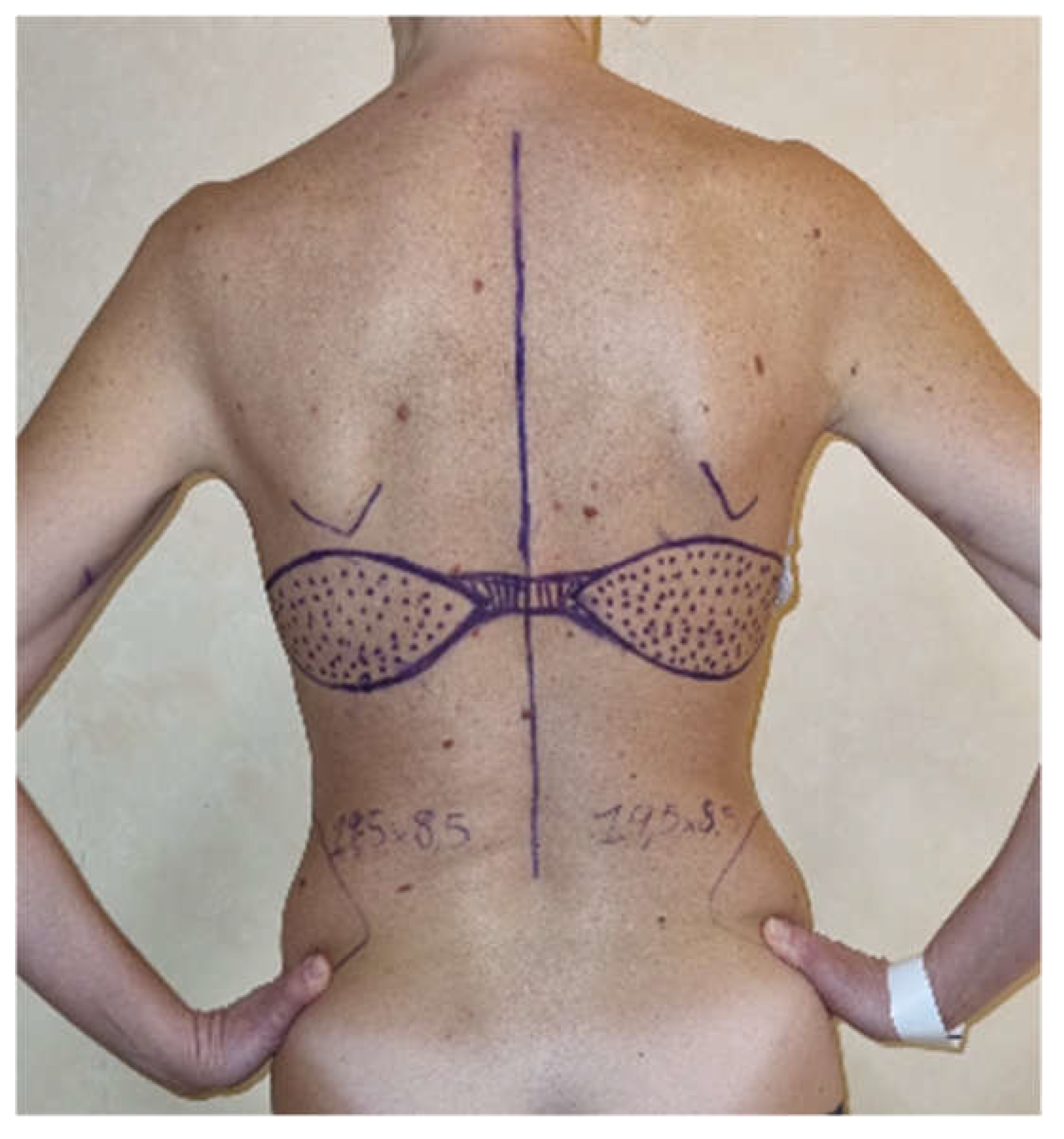
Figure 2.
Measurement of the post-operative breast projection (BP) using a millimeter caliper.
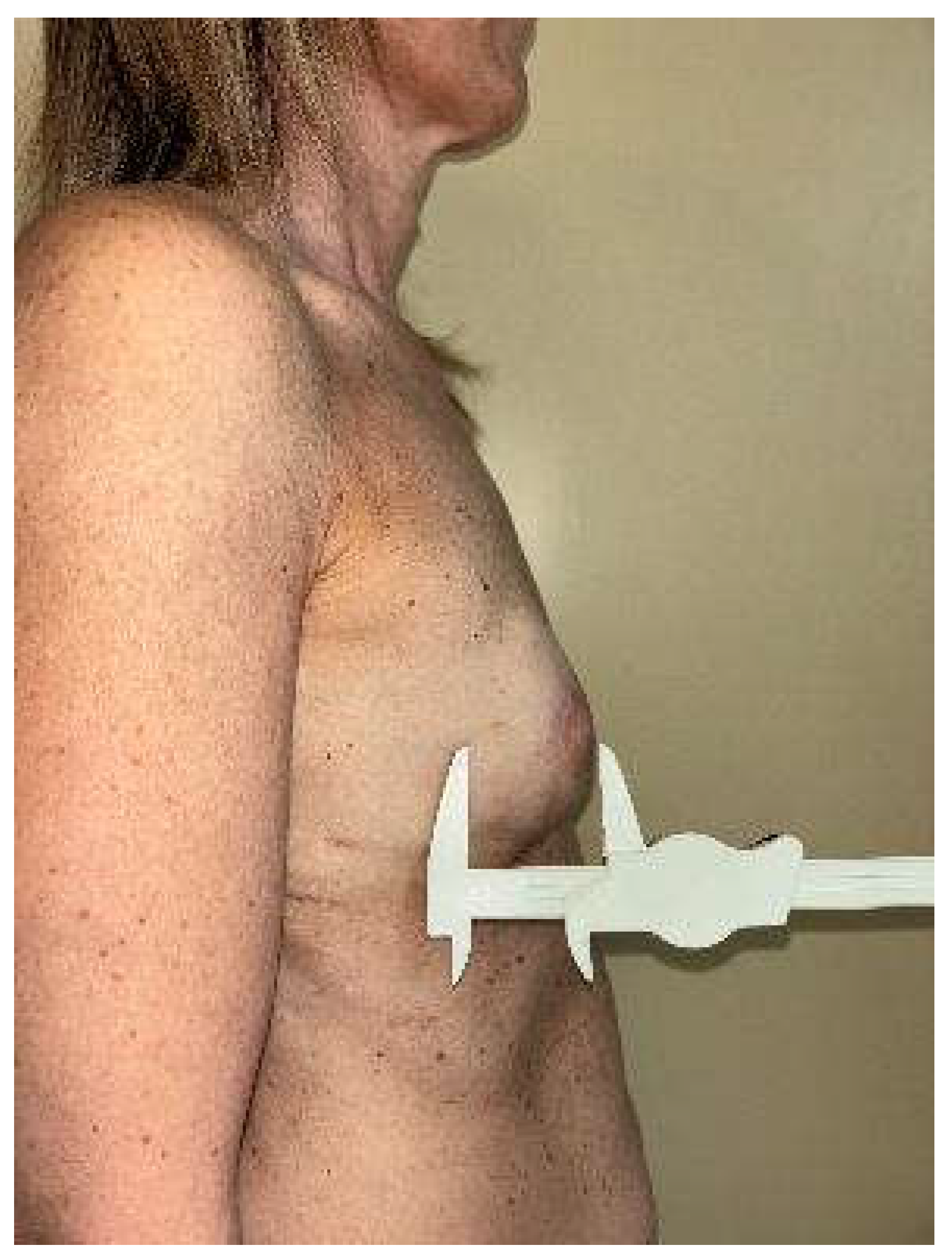
Figure 3.
Pre-operative picture (frontal view) of a patient scheduled for bilateral NSM and immediate breast reconstruction with bilateral ergonomic FALD flap.
Figure 3.
Pre-operative picture (frontal view) of a patient scheduled for bilateral NSM and immediate breast reconstruction with bilateral ergonomic FALD flap.
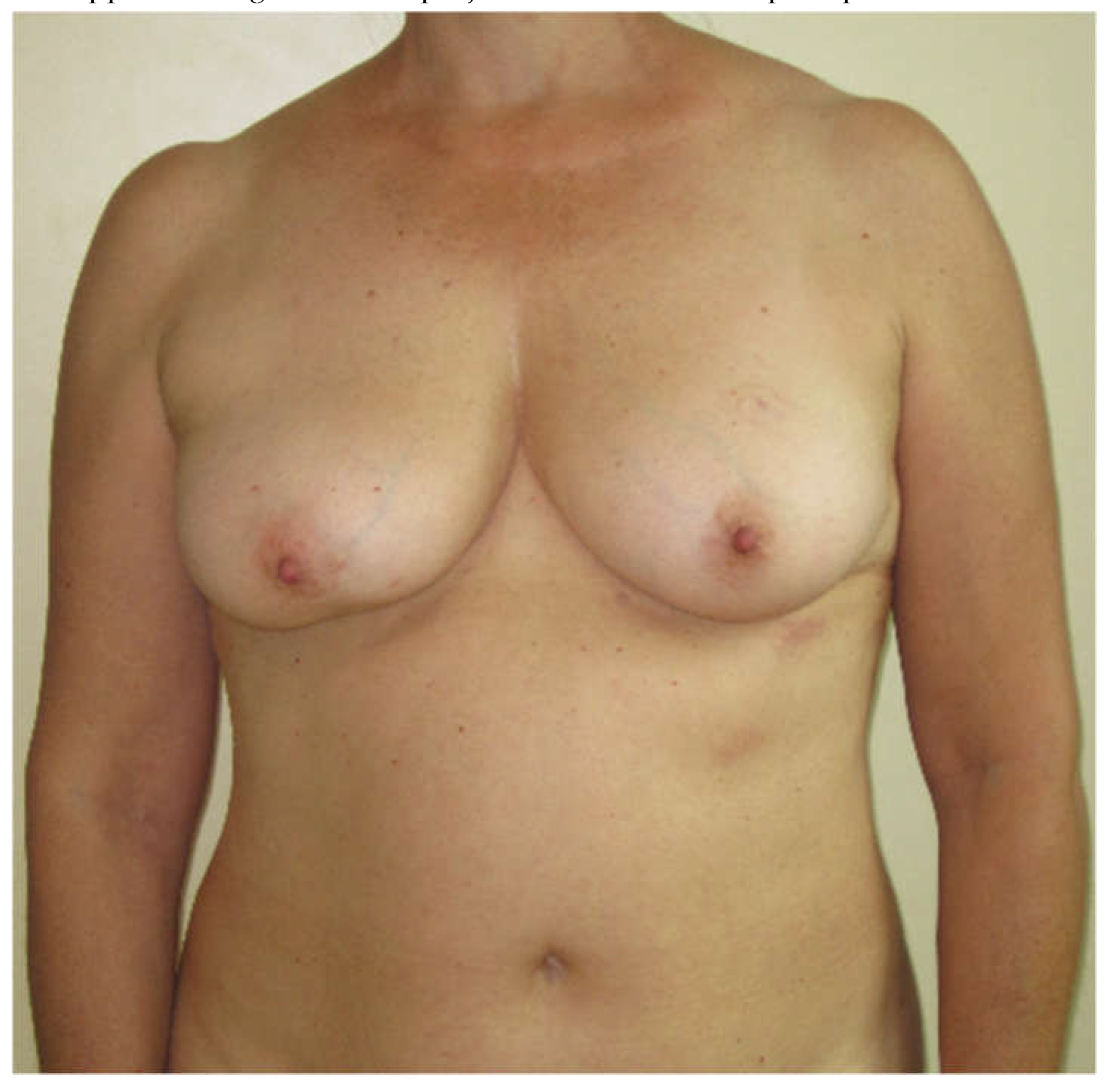
Figure 4.
Post-operative picture 6 months after bilateral NSM and immediate autologous breast reconstruction using FALD flap. The LD flap volume calculated using LD-V formula was 214.40 cc for each flap.
Figure 4.
Post-operative picture 6 months after bilateral NSM and immediate autologous breast reconstruction using FALD flap. The LD flap volume calculated using LD-V formula was 214.40 cc for each flap.
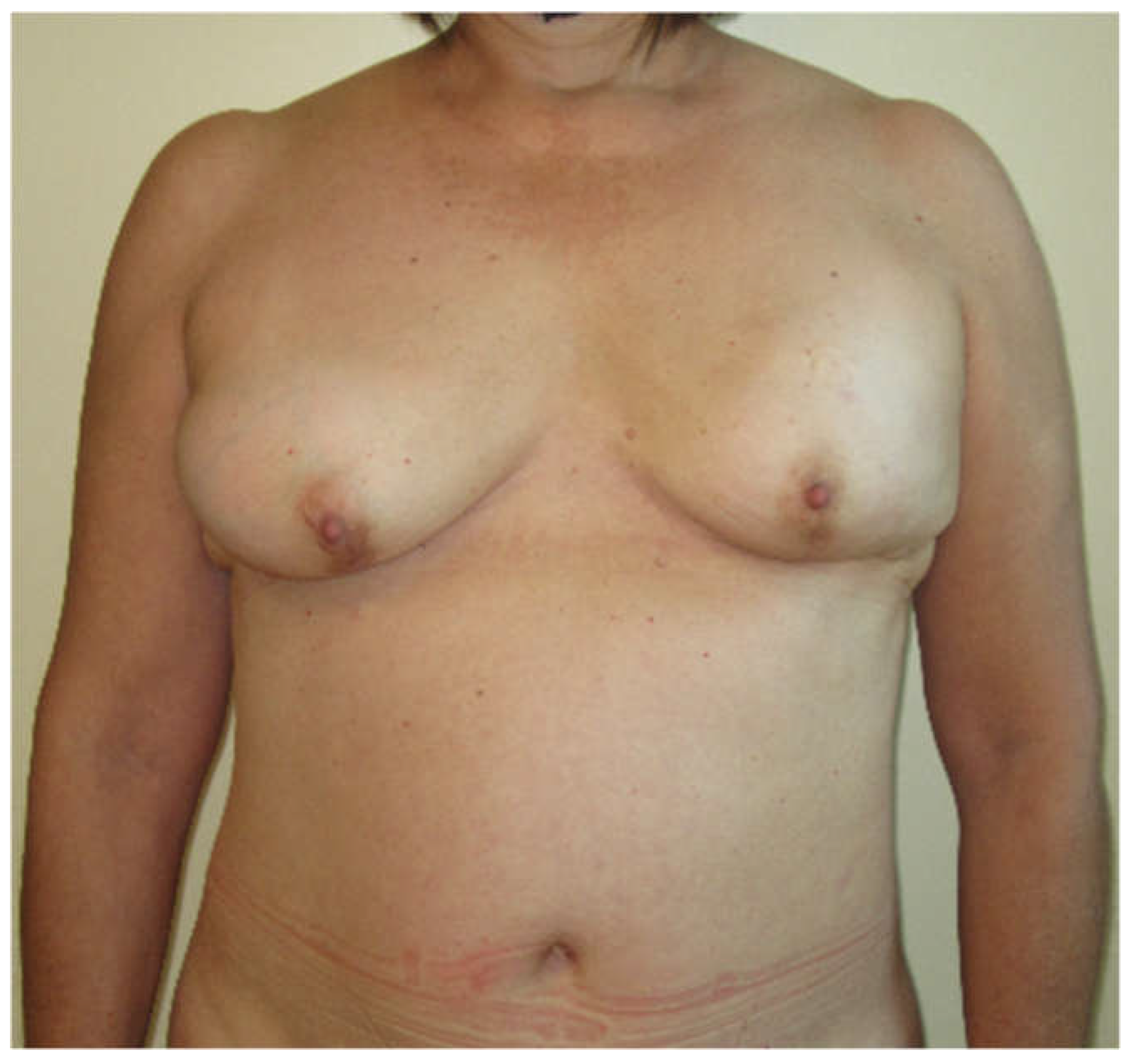
Figure 5.
Pre-operative picture (frontal view) of a patient scheduled for right NSM and immediate breast reconstruction using FALD flap.
Figure 5.
Pre-operative picture (frontal view) of a patient scheduled for right NSM and immediate breast reconstruction using FALD flap.

Figure 6.
Post-operative picture 4 months after right NSM and immediate autologous breast reconstruction with FALD flap. The estimated right LD flap volume using LD-V formula was 221.18 cc.
Figure 6.
Post-operative picture 4 months after right NSM and immediate autologous breast reconstruction with FALD flap. The estimated right LD flap volume using LD-V formula was 221.18 cc.


Table 1.
Subscale analysis of breast reconstruction.
| Subscale | Category 0 | Category 1 | Category 2 |
| Volume of breast mound | Marked discrepancy relative to contralateral side | Mild discrepancy relative to contralateral side | Symmetrical volume |
| Shape of breast mound | Marked shape deformity | Mild shape deformity | Natural or symmetrical shape |
| Placement of breast mound | Marked displacement | Mild displacement | Symmetrical and aesthetic placement |
| IMF | Poorly defined/not identified | Defined but with asymmetry or lack of medial definition | Defined and symmetrical |
| Skin texture | Marked discrepancy relative to contralateral side | Mild discrepancy relative to contralateral side | Natural texture |
| Scar location | More noticeable | Less noticeable | Well hidden |
Table 2.
Global Aesthetic Score described by Harris et al.
| Category 4 | Category 3 | Category 2 | Category 1 |
|---|---|---|---|
| Excellent: treated breast nearly identical to opposite breast | Good: treated breast only slightly different from opposite breast | Fair: treated breast clearly different from opposite breast but not seriously distorted | Poor: treated breast severely distorted |
Table 3.
Patients characteristics among the two groups.
| Group A | Group B | P value | |
|---|---|---|---|
| Flaps number | 32 | 31 | |
| Patients number | 23 | 25 | |
| Mean Age [y] | 50.5 (SD 9.51, range 33-70) | 50.42 (SD 9.66, range 40-80) | 0.796 |
| Mean BMI [kg/m2] | 23.93 (SD 3.58, range 18.9-35.8) | 23.08 (SD 2.69, range 18.6-30.4) | 0.495 |
| Smoking history | 6 (26.1 %) | 7 (28.0 %) | 0.882 |
| Laterality | Unilateral: 14 (60.9 %) Bilateral: 9 (39.1 %) |
Unilateral: 19 (76.0 %) Bilateral: 6 (24.0 %) |
0.259 |
| Timing of reconstruction | Immediate: 18 (56.2%) Delayed: 14 (43.8%) |
Immediate: 14 (45.2%) Delayed: 17 (54.8%) |
0.378 |
| Mastectomy type | SSM: 9 (28.1 %) NSM: 13 (40.6 %) Secondary: 10 (31.3 %) |
SSM: 4 (12.9 %) NSM: 11 (35.5 %) Secondary: 16 (51.6 %) |
0.177 |
| Preoperative breast volume [cc] | 298.74 (SD 99.69, range 120-520) | 288.75 (SD 78.81, range 130-430) | 0.549 |
| Preoperative Breast Projection [cm] | 6.38 (SD 0.74; range 5 - 8) | 6.42 (SD 0.77; range 5 - 8.5) | 0.408 |
| Preoperative Breast Width [cm] | 11.36 (SD 0.77; range 10 – 13) | 11.21 (SD 0.95; range 9.5 – 13) | 0.247 |
| Preoperative Breast Height [cm] | 11.13 (SD 1.16; range 9 – 13) | 11.37 (SD 1.01; range 9.5 – 13) | 0.147 |
Table 4.
Post-operative breast morphological analysis after weighting for the propensity score of the assigned group.
Table 4.
Post-operative breast morphological analysis after weighting for the propensity score of the assigned group.
| Group A | Group B | BminusA | CIlow | CIup | P value | |
|---|---|---|---|---|---|---|
| Flaps number | 32 | 31 | ||||
| Patients number | 23 | 25 | ||||
| Post-operative Breast Projection [cm] | 6.05 (SD 0.56; range 5.5 – 7.5) | 5.60 (SD 0.65; range 4.5 – 7) | -0.795 | -1.102 | -0.488 | < 0.0001 |
| Post-operative Breast Width [cm] | 11. 00 (SD 0.84; range 9.5 – 12.5) | 11.03 (SD 0.74; range 9.5 – 12) | 0.165 | -0.287 | 0.617 | 0.477 |
| Post-operative Breast Height [cm] | 10.63 (SD 1.22; range 8.5 – 13) | 10.47 (SD 0.96; range 9 – 13) | -0.281 | -0.916 | 0.355 | 0.390 |
Table 5.
Aesthetic propensity scores weighted analysis using surgeons’ evaluations. Propensity scores were estimated by means of a logistic regression model in which treatment was the outcome and predictors were age, BMI, operative time, mastectomy weight, and smoking habit. A value of p <0.05 was considered as significant.
Table 5.
Aesthetic propensity scores weighted analysis using surgeons’ evaluations. Propensity scores were estimated by means of a logistic regression model in which treatment was the outcome and predictors were age, BMI, operative time, mastectomy weight, and smoking habit. A value of p <0.05 was considered as significant.
| Group A | Group B | BminusA | CIlow | CIup | p-value | |
|---|---|---|---|---|---|---|
| Volume | 1.75 | 1.71 | -0.104 | -0.316 | 0.108 | 0.335 |
| Shape | 1.75 | 1.39 | -0.454 | -0.711 | -0.198 | 0.001 |
| Placement of breast mound | 1.72 | 1.52 | -0.232 | -0.476 | 0.011 | 0.061 |
| IMF | 1.69 | 1.61 | -0.107 | -0.341 | 0.128 | 0.374 |
| Skin texture | 1.69 | 1.58 | -0.093 | -0.333 | 0.146 | 0.445 |
| Scar | 1.66 | 1.51 | -0.171 | -0.417 | 0.075 | 0.174 |
| Total score | 10.25 | 9.32 | -0.500 | -3.853 | 2.353 | 0.752 |
| Global score | 3.44 | 3.06 | -0.509 | -0.858 | -0.160 | 0.004 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



