
Submitted:
21 August 2024
Posted:
22 August 2024
You are already at the latest version
Abstract
Nasal polyposis is defined by a Th2-driven chronic inflammation of the nose and sinus with polyps visible in the nasal fossae. It is a prevalent disease with a significant impact on the HRQL. Allergy, allergic rhinitis, asthma, and aspirin intolerance are frequently associated. The management is individual. The first line of treatment is a long-term treatment with intranasal corticosteroids. Oral corticosteroids should be used with caution. When the medical treatment fails the patient is eligible for sinus surgery. In case of symptomatic recurrence after both medical treatment and ethmoidectomy, biologics are nowadays a very promising treatment effective on all the respiratory tract. Dupilumab seems in the literature the molecule of choice. However, besides the international guidelines published by EPOS and Euforea, the molecule prescribed depends also on the availability of it in each country and the criteria edited by the health authorities to get reimbursement. Long treatment is mandatory. Traditional medical treatment is necessary as a complement to biologics.
Keywords:
Nasal Polyposis
Introduction
Sinonasal polyposis is a distinct form of chronic rhinosinusitis characterized by various phenotypes and endotypes [1,2].
Chronic rhinosinusitis (CRS) in adults is defined as a chronic inflammation of the nose and paranasal sinuses, characterized by two or more symptoms, one of which should be a nasal blockage or nasal discharge and/or facial pain or pressure and/or reduction or loss of smell. The diagnosis is confirmed by endoscopic signs (such as nasal polyps/mucopurulent discharge/edema of the middle meatus) or radiologic signs such as (mucosal changes in the sinuses/ostiomeatal complex on CT). In order to comply with the diagnosis of chronic rhinosinusitis the clinical manifestations should last without resolution longer than 12 weeks
CRS is classified in chronic rhinosinusitis with nasal polyps (CRSwNP) and chronic rhinosinusitis without nasal polyps (CRSsNP) [2]. Patients with nasal polyps account for 10 to 40% of all CRS patients [3,4,5].
The EPOS guidelines distinguish between primary nasal polyposis and secondary nasal polyposis, associated with cystic fibrosis, primary ciliary dyskinesia and immunodeficiency [1,2].
We will focus our topic on the primary nasal polyposis.
Epidemiology
CRS affects approximately 10-12% of the general population although there are significant geographical variations all over the world [4,5,6,7,8]. : Europe 10.9% [3,4],USA 12% [7], France 2% [8], Denmark 7.8% [9], China 8%[10], Korea 6.9% [11,12].
The exact prevalence of NP in the general population is also not clearly known as epidemiological studies are missing. However, in the literature we can find some percentages : an overall prevalence of 1% to 4% and also, great differences between countries ranging from 2.1% in France [8], 7% in Sweden [9], 4.3% in Finland, 1–4.2% in the USA [9], 1.1–2.2% in China [10].
Nasal polyposis (NP) is more prevalent in men than in women, except in cases of aspirin intolerance. It predominantly affects adults after the age of 40, and its prevalence increases with age [5,13].
Special attention is needed in the case of polyposis with debut in childhood.
Etiology and Pathophysiology (Phenotypic and Endotypic Variants of Polyposis)
The pathophysiology of CRSwNP is considered multifactorial as there is not a single molecular pathway explaining the modifications of the mucosa leading to the formation of polyps [14]. The present conception is that CRS is a chronic inflammation generated by an imbalance of interactions between the host, the commensal flora, different pathogens, and exogen stresses [15]. In the last period, a superantigen theory has been proposed for the pathophysiology of CRSwNP hypothesizing that the colonization with staphylococcus aureus which secretes superantigenic enterotoxins increases an eosinophilic inflammation leading to the formation of the polyps [16].
The categorization of CRSwNP into phenotypes and endotypes helps in understanding the underlying mechanisms and treat accordingly [1,2].
From the phenotypic perspective, NP can be categorized into two variants: neutrophilic and eosinophilic polyposis.
The polyposis with neutrophils is associated to a TH1 inflammatory profile. It is more common in Asian or Chinese adults or in children with conditions such as cystic fibrosis or primary ciliary dyskinesia.
The NP with eosinophils is mainly found in Caucasian patients, particularly in those with aspirin intolerance, allergic fungal sinusitis, or the Churg Strauss syndrome.
In the past these polyps were considered allergic polyps.
Endotypes are classified based on pathophysiologic mechanisms, and molecular and immunological profiles.
NP in Caucasians is mostly associated to a TH2 driven chronic inflammation. Type 2 immune response involves Th2 cells, eosinophils, ECP, and upregulation of IL4, IL5, and IL13. There is also a high level of total IgE in the serum and the nasal secretion [17,18].
Table 1 reminds the endotypîng of CRS, the different mediators and their localization. This is modified from Van Zele et al 2006.
Type 1 (Th1) endotype is dominated by a type 1 immune response involving Th1 cells, macrophages, and cytokines like TNF α and IFN γ. These patients have persistent polyps with less eosinophilic infiltration and are resistant to corticosteroids.
Recognizing phenotypes and endotypes helps understanding the disease and ultimately improves patient management and outcomes.
Th2-driven inflammation responds well to corticosteroids and biologics.
Nasal polyposis is frequently associated with other diseases or comorbidities such as allergy, allergic rhinitis, asthma, and aspirin intolerance.
Allergic rhinitis is a very prevalent disease in the general population. Its prevalence can be up to 30% in the Belgian population. It is therefore logical to suspect a causal etiologic link between allergic rhinitis and CRS with or without polyps [20].
A paper written by Wilson and published in 2014 tried to answer the question [21]. He searched the literature of articles examining the link between AR and CRS with NP. He found 18 articles. 10 of them found an association, 7 articles showed no association, and 1 article established a possible association. No articles examined the outcomes of CRSsNP or CRSwNP following allergy treatment. The conclusion was that the role of allergy in CRSwNP and CRSsNP continues to be controversial. Therefore and because of the high prevalence of allergic rhinitis in the general population, allergy testing and treatment remain a must in the diagnostic workup of CRSwNP.
In the past eosinophilic polyps were considered as allergic polyps, however studies did not demonstrate a higher incidence of allergic patients in the population of NP. Nasal polyposis is therefore no longer regarded as an allergic process but an inflammatory process that can involve the entire respiratory tract [22,23,24].
An interesting direction to be studied in the future would be the link between food allergy and nasal polyps signaled by some authors [25,26].
CRSwNP is frequently associated with asthma [27]. Nasal polyposis is associated with asthma in 40% of cases, thus indicating the fact that it is an inflammatory disease affecting the whole respiratory tract. A lung function testing must be done for a complete assessment of nasal polyposis to rule out asthma or bronchial hyperreactivity.
As a clinical presentation, NP can present as an isolated condition or can be associated with asthma with/or without aspirin intolerance. Aspirin intolerance is a condition that is associated with CRSwNP in 36-93%of cases [1,2]. The association between nasal polyps, aspirin intolerance, and asthma was known historically as Widal syndrome or Samter’s triad is called nowadays aspirin-exacerbated respiratory disease (AERD) or NSAID exacerbated respiratory disease (N-ERD) [7]. Compared to the case of patients tolerant to aspirin, nasal polyps and asthma have generally a severe evolution in patients with aspirin sensitivity [28,29].
Clinical Manifestations and Diagnostic Methods
Subjective evaluation of CRSwNP is based on its symptoms: nasal obstruction, nasal discharge or postnasal drip, facial pain or pressure, and reduction/loss of smell.
Table 2 shows the severity of the symptoms, the radiologic signs, and the Polyp nasal score in the case of CRSsNP, CRS wNP, and cystic fibrosis.
Obviously, nasal obstruction is a typical symptom more severe in the case of NP while cephalalgia is less frequent in CRSwNP compared to CRSsNP, except for patients with a surgical history. Nasal obstruction can be evaluated using rhinomanometry, acoustic rhinometry, a simple PNIF test, or a visual analogic scale (VAS).
The smell disorders encountered in CRSwNP are more common than in CRSsNP. Olfactory dysfunction is frequent in patients with CRSwNP (90%) and does not depend on the degree of nasal obstruction. The smell dysfunctions can vary significantly among patients with nasal polyps. Assessing the smell with olfactometry is important because the patient has difficulty evaluating his smell; Nowadays, olfactometry can be easily conducted using either a sniffing test [30] or a UPSIT test [31].
Sleep apnea syndrome can be associated with nasal polyposis and is quite frequent [32]. Patients with CRSwNP with important polyposis should be assessed in order to detect sleep disturbances [32,33,34].
Anterior rhinoscopy is used to assess the patient with polyposis but the fiberoptic endoscopy is preferable because it allows a better visualization of the interior of the nasal fossae for the diagnoses of polyposis in the nasal meatus [35] . Figure 1 shows a grade IV at the anterior rhinoscopy
Figure 2 presents images of a nasal endoscopy showing nasal polyps in the middle and superior meatus on both sides.
It also enables scoring the size of the nasal polyps. Many scoring systems have been used over the years to quantify the dimensions of nasal polyps [35,36]. One of the most used scoring systems for grading nasal polyps is the Meltzer clinical scoring system [37]. This scoring categorizes polyps into four grades:
| 0= no polyps |
| 1= polyps confined to the middle meatus |
| 2=multiple polyps occupying the middle meatus |
| 3=polyps extending beyond the middle meatus |
| 4=polyps completely obstructing the nasal cavity |
In 2023, Gevaert et al [38] proposed a new scoring system for the nasal polyps that also involves 4 grades as follows:
| 0=no polyps |
| 1=small polyps in the middle meatus not reaching the inferior border of the middle meatus |
| 2=nasal polyps reaching bellow the lower border of the middle meatus |
| 3=large polyps reaching the lower border of the inferior turbinate or polyps medial to the middle turbinate |
| 4=large nasal polyps causing complete obstruction of the inferior nasal cavity |
CT scans are the radiological investigation of choice for the diagnosis of CRSwNP [39]. The CT scans are useful in confirming the type of polyposis, either a diffuse type involving the ethmoidal sinuses allergic and the other paranasal cavities bilaterally or a central localization, called CCDA (central compartment atopic disease) [40]. The central compartment type is frequently associated with allergies.
As the concern for radiation exposure is increased worldwide, cone-beam technology might be an alternative to classic CT scans [41].
The classic radiologic staging used in rhinosinusal polyposis is the one proposed by Lund-Makay in 1993 [42]. When reading a CT scan of the paranasal sinuses, the reader assigns each sinus a score
- No abnormality = 0 points
- Partial opacification = 1 point
- Complete opacification = 2 points
- For the ostiomeatal complex, the score is different:
- No opacification = 0 points
- Opacification = 2 points
The sinuses are grouped into frontal sinus, anterior ethmoidal sinus, posterior ethmoidal sinus, maxillary sinus, sphenoid sinus, and ostiomeatal complex. Each side is scored separately. A maximum of 24 points is possible. Despite its simplicity, it correlates well with the severity of the disease, the extent of surgery, treatment response, and complication rates [32,43].
Isolated areas of the scanner do not allow the differentiation between meatal polyposis and chronic sinusitis without polyps. The endoscopy remains the complementary examination of choice.
The MRI is not typically part of the assessment except for the patients in previously operated patients with the suspicion of mucocele, or neoplasia. MRI has a better capacity to describe soft tissue and does not have a radiation risk. By better defining soft tissue it can differentiate different masses of retained secretions.
The analysis of the nasal secretions proposed by ST Vlaminck can be a valuable diagnostic tool in the diagnosis and monitoring of eosinophilic polyposis. The secretions can be collected by simple blowing or preferably by aspiration under endoscopic control. The collected material is then examined for eosinophils, Charcot Leyden chrystals, allergic mucin, and fungal hyphae [44,45,46].
Impact on the Quality of Life
CRS has a remarkable impact on health-related quality of life [47,48] and is associated with important healthcare costs [49,50,51]. The quality of life of the patient with nasal polyposis can be severely impaired and it should be assessed by questionnaires meant to analyze the impact of the pathology on daily life. SNOT 22 test is an effective tool for this purpose [52,53,54,55]. See Figure 3.
Sino-nasal Outcome Test (SNOT-22) has 22 questions with scores from 0-5 for each question. Studies have described the following stratifications: Mild: 8-20, Moderate: >20-50, Severe: >50.
The visual analogue scale is also another method to quantify the severity of the symptoms .
Management and Treatment Approaches
The management of nasal polyposis remains individual [56]. The classic treatment of rhinosinusitis with polyps is based on nasal lavages associated to long-term intranasal corticosteroids [57,58]. These corticosteroids reduce rhinitis symptoms, improve nasal breathing, reduce the size of polyps, and prevent, in part, their recurrence, but this treatment has minimal effect on the sense of smell [57]. The effect of corticosteroids is based on their ability to diminish eosinophilic infiltration by reducing their viability and activation. Intranasal corticosteroids can be administered via spray or in lavages and the literature regarding their use is quite rich and favoring nasal steroids. Topical corticosteroids usually used are fluticasone propionate, mometasone furoat, betamethasone, beclomethasone dipropionate. Budesonide in nasal rinses is commonly used, though it is off-label [59,60,61]. Side effects of nasal steroids are epistaxis, dry nose, local irritation but usually they are well tolerated.
Oral corticosteroids (OC) should be reserved for obvious polyps associated to severe symptoms. Despite their effectiveness, OC should be used for short term (less than 7 days and a maximum of 3 courses per year), given the important side-effects (osteoporosis, diabetes melitus, necrosis of the head of the hip, glaucoma). The anti-inflammatory effect cannot be separated from the metabolic effect. There is a need for special attention for patients with diabetes mellitus or severe glaucoma.
The mean annual cumulative dose of oral corticosteroids over the year should be monitored and should not exceed 1ooo mg of prednisolone [32].
Short term or long-term antibiotic treatments with macrolides or doxycycline are reported by some studies to have a moderately positive effect on the size of polyps, and patient symptoms [62,63]. Nevertheless, the danger of antimicrobial resistance should be considered.
Patients not responding after a trial of a maximum medical treatment (intranasal steroids for at least 8 weeks, at least 2 courses of OC over the year, and symptomatic recurrence) are eligible for surgery [2,32,64].
Surgical options include a primary surgery, a simple polypectomy, a polypectomy associated with a skeletonization of the different meatuses or a functional ethmoidectomy. In fact, there is no definitive consensus. Simple polypectomy improves the nasal blockage but is associated with early and high recurrence rate [65].
Therefore, most rhinologists recommend performing a complete ethmoidectomy with sparing of the sinus mucosa [66,67].
In the case of revision surgery for massive symptomatic recurrence of the polyposis the surgery is usually more extended, more aggressive and the attitude towards the mucosa is less conservative.
The surgical options are therefore a nasalization, a Draf procedure, or a reboot procedure with complete resection of the mucosa of all the paranasal sinus cavities [68,69] .
Surgery has its advantages but also its inconveniences and obvious risks. There are anesthetic risks, neurological, vascular, and orbital complications. There are also risks of late complications such as synechiae, mucoceles, and colonization with staphylococcus aureus. In Table 3 we compared the benefits and weaknesses of the surgical treatment versus the medical in the case of the CRSwNP.
One important issue after surgery is recurrence of the nasal polyps. The percentage is highly variable. In EPOS they reported a percent of at least 40% of recurrence of nasal polyps at 3-5 years after FESS before the arrival of biologics [70,71].
Vlaminck S. found 40% recurrence rates 3 years after FESS and 62% recurrence rate after 10 years of follow up [44,46].
Calus et al found a 78.9% recurrence rate with a follow-up of 12 years. Among them, there was a 36.8% need for a revision surgery [72].
Biological Treatment and Ongoing Care
Based on these data it seems necessary to find new molecules as add-on treatments to intranasal steroids and surgery [73].
In recent years, biological therapies have been developed as an endotype-driven therapy. Indeed, they are monoclonal antibodies acting as antagonists to some specific mediators of the Th2 inflammatory cascade. Historically biologics have first demonstrated their efficacy for the treatment of moderate or severe asthma unresponsive to traditional therapies. Afterward, they have been used to treat uncontrolled nasal polyposis. Therefore, ENT specialists benefit from the experience of pulmonologists.
Specific criteria have been edited by EPoS and EUFOREA guidelines for the prescription of biologics by an ENT (1,2, 73-,75).
Biological treatment is indicated in the event of symptomatic recurrence of nasal polyposis after a well-conducted medical treatment, an complete ethmoidectomy, or in case of a contraindication for anesthesia.
According to EPOS, the indication of biological treatment in CRSwNP is
- Symptomatic uncontrolled nasal polyposis unresponsive to traditional medical treatment (medical therapy +/- surgery) with these additional criteria:
- Evidence of type 2 inflammation (tissue eos>10/hpf, or blood eos>250, or total IgE>100)
- Need for systemic corticosteroids or contraindication for systemic corticosteroids (>2 courses per year, or long term . 3 months low dose steroids)
- Significantly impaired quality of life (SNOT22>40)
- Significant loss of smell (anosmic on smell test)
- Diagnosis of comorbid asthma (asthma needing regular inhaled corticosteroids)
In the absence of surgical history, four criteria are required. In case of a surgical history, three criteria are sufficient.
In 2023 they changed a little bit the criteria. The blood eosinophilia should be \150 instead of 250 in the initial report [76].
3 molecules are currently prescribed by the ENT and available in Belgium: omalizumab, mepolizumab and dupilumab.
Omalizumab is an anti-IgE monoclonal antibody. It reduces the levels of the total IgE in a dose-dependent way. Very early after its administration a quick drop of the level of the serum IgE of 89 to 90% is observed.
Gevaert published 5 studies in 2013 (first study), 2021 (comparison of 2 cohorts of patients : polyp 1 and polyp 2), 2023, 2024 (long-term results) [77,78,79,80,81]. He demonstrated that compared to the placebo group, omlizumab reduced significantly the polyp nasal score, the symptomatology, the sense of smell and the opacity (Lund McKay score) on CT. The efficacy was similar in allergic and non-allergic patients. In patients with concomitant asthma lung function was also improved.
Mepolizumab is an anti-IL5 monoclonal antibody validated by the FDA. IL 5 is an interleukin that plays a major role in the multiplication, maturation and survival of the eosinophils, key cells in the TH2 inflammatory cascade [81,82].
JK Han published in 2021 a well known study called Synapse conducted during 52 weeks [84]. This is a phase 3 RCT double-blind study demonstrating the efficacy and safety of Mepolizumab for the management of severe bilateral refractory nasal polyposis refractory to conventional treatment and requiring multiple sinus surgeries. The study demonstrated a significant reduction of the level of blood eosinophilia, an improvement of the nasal polyp score, an Improvement of the SNOT 22 after 8 weeks, a reduction of the VAS for nasal blockage, a reduction of the rescue medication by oral steroids, a reduction and delayed for revision surgeries for 52%, which was significant compared to the placebo group [85]. The Safety profile was similar to that observed with the placebo. A significantly greater proportion of patients (30%) in the mepolizumab group compared with the placebo group (10%), no longer required surgery at Week 25.
Dupilumab is an anti-IL4 and IL13 monoclonal antibody also validated by the FDA.
A study called Liberty NP sinus 24 & Liberty NP sinus 52 was published by Bachert et al in 2019 in the Lancet [86]. This was a multicentric RCT double blind control study with 2 different timing: the first conducted during 24 weeks and the other during 52 weeks. During these periods, they observed a significant reduction of the nasal polyp score, and nasal congestion, statistically significant after 8 weeks of treatment, compared to placebo. The period of time before using OC or performing a revision surgery was longer in the group with dupilumab. The symptoms recurred if the medication was stopped after 24 weeks. However, it is still as effective in the group of treatment for 52 weeks.
The question to be answered for the clinicians : which is the best biologic to prescribe to treat severe uncontrolled nasal polyposis.
Based on some metaanalysis and recent real life studies, dupilumab seems to be the most effective biologic compared to mepolizumab or omalizumab [87,88,89,90] with a good safety profile.
However, dupilumab can be associated with a transitory hypereosinophilia whose meaning is unclear [90].
However, the prescription of one drug instead of another depends also on the availability, the costs, and the criteria elaborated in the specific country to obtain reimbursement.
These molecules must be used for a long period of time. In any case, the clinician should wait for a minimum 2 months of treatment to observe significant effect and there are rapid responders and slow responders. This was perfectly well demonstrated in the Synapse Study. Patients stopping their treatment after 24 week shave a recurrence of their symptoms and polyps; patients treated for 52 weeks without interruption remain improved during all the duration of the study [86].
An important factor for the future is the cost and the criteria edited by the authorities to give the reimbursement compared to the cost of the most classical management. The response is evaluated based on the history, the presence of polyps at the nasal endoscopy, or the scanner.
According to EPOS and EUFOREA a minimum of 6 months of treatment is required to evaluate the efficacy. The two international forums recommend the evaluation of the response to biological treatment in CRSwNP based on 5 criteria:
- Reduced nasal polyp size
- Reduced need for systemic oral corticosteroids
- Improved quality of life
- Improved sense of smell
- Reduced impact of comorbidities
The response is evaluated at 6 months and 1 year.
If the treatment is effective, it should be continued for several years with regular checks every 6 months. In any case, the patient should not discontinue the intranasal corticoids or the bronchodilator. If there is no response to any of the criteria the treatment should be discontinued or a switch to another drug can be done. Now there is no deadline to stop the treatment. Real-life studies with long-term follow-up (5 or 10 years) are necessary to confirm all our expectations.
Conclusion
Nasal polyposis is defined by a Th2-driven chronic inflammation of the nose and sinus with polyps visible in the nasal fossae
It is a prevalent disease with a significant impact on the HRQL.
Allergy, allergic rhinitis, asthma, and aspirin intolerance are frequently associated.
The management is individual.
The first line of treatment is a long-term treatment with intranasal corticosteroids. Oral corticosteroids should be used with caution.
When the medical treatment fails the patient is eligible for sinus surgery.
In case of symptomatic recurrence after both medical treatment and ethmoidectomy, biologics are nowadays a very promising treatment effective on all the respiratory tract. Dupilumab seems in the literature the molecule of choice.
However, besides the international guidelines published by EPOS and Euforea, the molecule prescribed depends also on the availability of it in each country and the criteria edited by the health authorities to get reimbursement.
Long treatment is mandatory. Traditional medical treatment is necessary as a complement to biologics.
References
- W. J. Fokkens et al., “EPOS 2012: European position paper on rhinosinusitis and nasal polyps 2012. A summary for otorhinolaryngologists,” Rhinology journal, vol. 50, no. 1, pp. 1–12, Mar. 2012. [CrossRef]
- W. J. Fokkens et al., “European Position Paper on Rhinosinusitis and Nasal Polyps 2020,” Rhinology journal, vol. 0, no. 0, pp. 1–464, Feb. 2020. [CrossRef]
- D. Hastan et al., “Chronic rhinosinusitis in Europe - an underestimated disease. A GA2LEN study,” Allergy, vol. 66, no. 9, pp. 1216–1223, Sep. 2011. [CrossRef]
- Khan A, Vandeplas G, Huynh TMT, Joish VN, Mannent L, Tomassen P, Van Zele T, Cardell LO, Arebro J, Olze H, Foerster-Ruhrmann U, Kowalski ML, Olszewska-Ziaber A, Holtappels G, De Ruyck N, van Drunen C, Mullol J, Hellings PW, Hox V, Toskala E, Scadding G, Lund VJ, Fokkens WJ, Bachert C. The Global Allergy and Asthma European Network (GALEN rhinosinusitis cohort: a large European cross-sectional study of chronic rhinosinusitis patients with and without nasal polyps. Rhinology. 2019 Feb 1;57(1):32-421;57(1):32-42. [CrossRef] [PubMed]
- Chen, S., Zhou, A., Emmanuel, B., Thomas, K., & Guiang, H. (2020). Systematic literature review of the epidemiology and clinical burden of chronic rhinosinusitis with nasal polyposis. Current Medical Research and Opinion, 36(11), 1897–1911. [CrossRef]
- E. Esen, A. Selçuk, and D. Passali, “Epidemiology of Nasal Polyposis,” in All Around the Nose, Cham: Springer International Publishing, 2020, pp. 367–371. [CrossRef]
- A. G. Hirsch et al., “Nasal and sinus symptoms and chronic rhinosinusitis in a population-based sample,” Allergy, vol. 72, no. 2, pp. 274–281, Feb. 2017. [CrossRef]
- Palmer JN, Messina JC, Biletch R, et al. A cross-sectional, population-based survey of U.S. adults with symptoms of chronic rhinosinusitis. Allergy Asthma Proc 2019; 40: 48-56. [CrossRef]
- Klossek JM, Neukirch F, Pribil C, Jankowski R, Serrano E, Chanal I, El Hasnaoui A. Prevalence of nasal polyposis in France: a cross-sectional, case-control study. Allergy. 2005;60:233–7. [CrossRef]
- Johansson L, Akerlund A, Holmberg K, et al. Prevalence of nasal polyps in adults: the Skovde population-based study. Ann Otol Rhinol Laryngol 2003; 112: 625-9. [CrossRef]
- Shi JB, Fu QL, Zhang H, et al. Epidemiology of chronic rhi- nosinusitis: results from a cross-sectional survey in seven Chinese cities. Allergy 2015; 70: 533-9. [CrossRef]
- J. H. Kim, C. Cho, E. J. Lee, Y. S. Suh, B. I. Choi, and K. S. Kim, “Prevalence and risk factors of chronic rhinosinusitis in South Korea according to diagnostic criteria,” Rhinology journal, vol. 54, no. 4, pp. 329–335, Dec. 2016. [CrossRef]
- Min YG, Jung HW, Kim HS, Park SK, Yoo KY. Prevalence and risk factors of chronic sinusitis in Korea: results of a nationwide survey. Eur Arch Otorhinolaryngol. 1996;253:435–9. [CrossRef]
- Raciborski, Filip, Magdalena Arcimowicz, Bolesław Krzysztof Samoliński, Wojciech Pinkas, Piotr Samel-Kowalik and Andrzej Śliwczyński. “Recorded prevalence of nasal polyps increases with age.” Advances in Dermatology and Allergology/Postȩpy Dermatologii i Alergologii 38 (2020): 682 - 688. [CrossRef]
- M. A. DeMarcantonio and J. K. Han, “Nasal Polyps: Pathogenesis and Treatment Implications,” Otolaryngol Clin North Am, vol. 44, no. 3, pp. 685–695, Jun. 2011. [CrossRef]
- D. R. Littman and E. G. Pamer, “Role of the Commensal Microbiota in Normal and Pathogenic Host Immune Responses,” Cell Host Microbe, vol. 10, no. 4, pp. 311–323, Oct. 2011. [CrossRef]
- Staphylococcus aureus enterotoxins: a key in airway disease?C. Bachert, P. Gevaert, P. Van CauwenbergeAllergy1..2002VOL57, Issue 6: 480-487 7 May 2002. [CrossRef]
- van der Lans R, Otten JJ, Adriaensen GFJPM, Benoist LBL, Cornet ME, Hoven DR, Rinia AB, Fokkens WJ, Reitsma S. Eosinophils are the dominant type2 marker for the current indication of biological treatment in severe uncontrolled chronic rhinosinusitis with nasal polyps. Rhinology. 2024 Jun 1;62(3):383-384. [CrossRef] [PubMed]
- EUFOREA/EPOS2020 statement on the clinical considerations for chronic rhinosinusitis with nasal polyps care.Hellings PW, Alobid I, Anselmo-Lima WT, Bernal-Sprekelsen M, Bjermer L, Caulley L, Chaker A, Constantinidis J, Conti DM, De Corso E, Desrosiers M, Diamant Z, Gevaert P, Han JK, Heffler E, Hopkins C, Landis BN, Lourenco O, Lund V, Luong AU, Mullol J, Peters A, Philpott C, Reitsma S, Ryan D, Scadding G, Senior B, Tomazic PV, Toskala E, Van Zele T, Viskens AS, Wagenmann M, Fokkens WJ.Allergy. 2024 May;79(5):1123-1133. [CrossRef] [PubMed]
- T. Van Zele et al., “Differentiation of chronic sinus diseases by measurement of inflammatory mediators,” Allergy, vol. 61, no. 11, pp. 1280–1289, Nov. 2006. [CrossRef]
- Benninger MS, “Rhinitis, sinusitis and their relationships to allergies,” American Journal of 7hinology , vol. 6, pp. 37–43, 1992. [CrossRef]
- Wilson KF, McMains KC, Orlandi RR. The association between allergy and chronic rhinosinusitis with and without nasal polyps: an evidence-based review with recommendations. Int Forum Allergy Rhinol. 2014 Feb;4(2):93-103. [CrossRef] [PubMed]
- Caplin I, Haynes GT, and Sphan J, “Are nasal polyps an allergic phenomenon?,” Ann Alergy, vol. 29 dec, no. 12, pp. 631–634, 1971.
- M. Gelardi, L. Iannuzzi, S. Tafuri, G. Passalacqua, and N. Quaranta, “Allergic and non-allergic rhinitis: relationship with nasal polyposis, asthma and family history.,” Acta Otorhinolaryngol Ital, vol. 34, no. 1, pp. 36–41, Feb. 2014.
- S. Marcus, L. T. Roland, J. M. DelGaudio, and S. K. Wise, “The relationship between allergy and chronic rhinosinusitis,” Laryngoscope Investig Otolaryngol, vol. 4, no. 1, pp. 13–17, Feb. 2019. [CrossRef]
- Y. Pang, O. Eskici, and J. A. Wilson, “Nasal polyposis: Role of subclinical delayed food hypersensitivity,” Otolaryngology–Head and Neck Surgery, vol. 122, no. 2, pp. 298–301, Feb. 2000. [CrossRef]
- M. M. Collins, S. Loughran, P. Davidson, and J. A. Wilson, “Nasal polyposis: Prevalence of positive food and inhalant skin tests,” Otolaryngology–Head and Neck Surgery, vol. 135, no. 5, pp. 680–683, Nov. 2006. [CrossRef]
- J. Bousquet et al., “Allergic Rhinitis and its Impact on Asthma (ARIA): Achievements in 10 years and future needs,” Journal of Allergy and Clinical Immunology, vol. 130, no. 5, pp. 1049–1062, Nov. 2012. [CrossRef]
- M. P. Berges-Gimeno, R. A. Simon, and D. D. Stevenson, “The natural history and clinical characteristics of aspirin-exacerbated respiratory disease,” Annals of Allergy, Asthma & Immunology, vol. 89, no. 5, pp. 474–478, Nov. 2002. [CrossRef]
- J. E. Chang, W. Chin, and R. Simon, “Aspirin-Sensitive Asthma and Upper Airway Diseases,” Am J Rhinol Allergy, vol. 26, no. 1, pp. 27–30, Jan. 2012. [CrossRef]
- C. Rumeau, D. T. Nguyen, and R. Jankowski, “How to assess olfactory performance with the Sniffin’ Sticks test ®,” Eur Ann Otorhinolaryngol Head Neck Dis, vol. 133, no. 3, pp. 203–206, Jun. 2016. [CrossRef]
- R. L. Doty, R. E. Frye, and U. Agrawal, “Internal consistency reliability of the fractionated and whole University of Pennsylvania Smell Identification Test,” Percept Psychophys, vol. 45, no. 5, pp. 381–384, Sep. 1989. [CrossRef]
- Ref Recommandation de pratique Clinique pour la polypose nasosinusienne. Reco-PNS-FINAL-290923-.pdf (sforl.org).
- D. P. Migueis et al., “Obstructive sleep apnea in patients with chronic rhinosinusitis with nasal polyps: a cross-sectional study,” Sleep Med, vol. 64, pp. 43–47, Dec. 2019. [CrossRef]
- Serrano E, Neukirch F, Pribil C, Jankowski R, Klossek JM, Chanal I, El Hasnaoui A. Nasal polyposis in France: impact on sleep and quality of life. J Laryngol Otol. 2005 Jul;119(7):543-9. [CrossRef] [PubMed]
- N. Bhattacharyya and L. N. Lee, “Evaluating the diagnosis of chronic rhinosinusitis based on clinical guidelines and endoscopy,” Otolaryngology–Head and Neck Surgery, vol. 143, no. 1, pp. 147–151, Jul. 2010. [CrossRef]
- Djupesland PG, Reitsma S, Hopkins C, Sedaghat AR, Peters A, Fokkens WJ. Endoscopic grading systems for nasal polyps: are we comparing apples to oranges? Rhinology. 2022 Jun 1;60(3):169-176. [CrossRef] [PubMed]
- E. O. Meltzer et al., “Rhinosinusitis: Developing guidance for clinical trials,” Journal of Allergy and Clinical Immunology, vol. 118, no. 5, pp. S17–S61, Nov. 2006. [CrossRef]
- P. Gevaert et al., “European Academy of Allergy and Clinical Immunology position paper on endoscopic scoring of nasal polyposis,” Allergy, vol. 78, no. 4, pp. 912–922, Apr. 2023. [CrossRef]
- H. Varshney, J. Varshney, S. Biswas, and S. K. Ghosh, “Importance of CT Scan of Paranasal Sinuses in the Evaluation of the Anatomical Findings in Patients Suffering from Sinonasal Polyposis,” Indian Journal of Otolaryngology and Head & Neck Surgery, vol. 68, no. 2, pp. 167–172, Jun. 2016. [CrossRef]
- C. Davies, F. Wu, E. Y. Huang, M. Takashima, N. R. Rowan, and O. G. Ahmed, “Central Compartment Atopic Disease as a Pathophysiologically Distinct Subtype of Chronic Rhinosinusitis: A Scoping Review,” Sinusitis, vol. 7, no. 2, pp. 12–26, Sep. 2023. [CrossRef]
- K. Bacher, K. Mermuys, J. Casselman, and H. Thierens, “Evaluation of Effective Patient Dose in Paranasal Sinus Imaging: Comparison of Cone Beam CT, Digital Tomosynthesis and Multi Slice CT,” 2009, pp. 458–460. [CrossRef]
- Lund VJ and Mackay IS, “Staging in rhinosinusitis,” Rhinology, vol. 31, no. 4, pp. 183–184, 1993.
- S. G. Brooks et al., “Preoperative Lund-Mackay computed tomography score is associated with preoperative symptom severity and predicts quality-of-life outcome trajectories after sinus surgery,” Int Forum Allergy Rhinol, vol. 8, no. 6, pp. 668–675, Jun. 2018. [CrossRef]
- Vlaminck S, Vauterin T, Hellings PW, et al. The importance of local eosinophilia in the surgical outcome of chronic rhinosinusitis. Am J Rhinol Allergy. 2014; 28:260–264.
- Vlaminck S, Casselman J, De Groef K, Van den berghe I, Kuhweide R, Joniau S. Eosinophilic fungal rhinosinusitis (EFRS): a distinct CT/MRI-entity? A European experience. BENT 2005; 1(2):73-82.
- Vlaminck S.; Prokopakis, E.; Kawauchi, H.; Haspeslagh, M.; Van Huysse, J.; Simões, J.; Acke, F.; Gevaert, P. Proposal for Structured Histopathology of Nasal Secretions for Endotyping Chronic Rhinosinusitis: An Exploratory Study. Allergies 2022, 2, 128–137. [CrossRef]
- S. Erskine et al., “A cross sectional analysis of a case-control study about quality of life in CRS in the UK; a comparison between CRS subtypes,” Rhinology journal, vol. 54, no. 4, pp. 311–315, Dec. 2016. [CrossRef]
- L. P. Hoehle, K. M. Phillips, R. W. Bergmark, D. S. Caradonna, S. T. Gray, and A. R. Sedaghat, “Symptoms of chronic rhinosinusitis differentially impact general health-related quality of life,” Rhinology journal, vol. 54, no. 4, pp. 316–322, Dec. 2016. [CrossRef]
- N. Bhattacharyya, “Incremental Health Care Utilization and Expenditures for Chronic Rhinosinusitis in the United States,” Annals of Otology, Rhinology & Laryngology, vol. 120, no. 7, pp. 423–427, Jul. 2011. [CrossRef]
- K. A. Smith, R. R. Orlandi, and L. Rudmik, “Cost of adult chronic rhinosinusitis: A systematic review,” Laryngoscope, vol. 125, no. 7, pp. 1547–1556, Jul. 2015. [CrossRef]
- L. Rudmik, “Economics of Chronic Rhinosinusitis,” Curr Allergy Asthma Rep, vol. 17, no. 4, p. 20, Apr. 2017. [CrossRef]
- Kennedy JL, Hubbard MA, Huyett P, Patrie JT, Borish L, Payne SC. Sino-nasal outcome test (SNOT-22): a predictor of postsurgical improvement in patients with chronic sinusitis. Ann Allergy Asthma Immunol. 2013;111(4):246-251.e2. [CrossRef]
- Khan AH, Reaney M, Guillemin I, Nelson L, Qin S, Kamat S, Mannent L, Amin N, Whalley D, Hopkins C. Development of Sinonasal Outcome Test (SNOT-22) Domains in Chronic Rhinosinusitis With Nasal Polyps. Laryngoscope. 2022 May;132(5):933-941. [CrossRef] [PubMed]
- Toma S, Hopkins C. Stratification of SNOT-22 scores into mild, moderate or severe and relationship with other subjective instruments. Rhinology. 2016;54(2):129-33.
- De Dorlodot C, et al. French adaptation and validation of the sino-nasal outcome test-22: a prospective cohort study on quality of life among 422 subjects. Clin Otolaryngol. 2015; 40(1): 29-35. [CrossRef]
- D. Passali, L. M. Bellussi, V. Damiani, M. A. Tosca, G. Motta, and G. Ciprandi, “Chronic rhinosinusitis with nasal polyposis: the role of personalized and integrated medicine.,” Acta Biomed, vol. 91, no. 1-S, pp. 11–18, Feb. 2020. [CrossRef]
- N. Mygind and V. Lund, “Intranasal Corticosteroids for Nasal Polyposis,” Treat Respir Med, vol. 5, no. 2, pp. 93–102, 2006. [CrossRef]
- S. Tait, D. Kallogjeri, J. Suko, S. Kukuljan, J. Schneider, and J. F. Piccirillo, “Effect of Budesonide Added to Large-Volume, Low-pressure Saline Sinus Irrigation for Chronic Rhinosinusitis,” JAMA Otolaryngology–Head & Neck Surgery, vol. 144, no. 7, p. 605, Jul. 2018. [CrossRef]
- S. M. Jung, J. H. Kwak, M. K. Kim, K. Tae, S. H. Cho, and J. H. Jeong, “The Long-Term Effects of Budesonide Nasal Irrigation in Chronic Rhinosinusitis with Asthma,” J Clin Med, vol. 11, no. 10, p. 2690, May 2022. [CrossRef]
- D.-Y. Park et al., “Clinical Practice Guideline: Nasal Irrigation for Chronic Rhinosinusitis in Adults,” Clin Exp Otorhinolaryngol, vol. 15, no. 1, pp. 5–23, Feb. 2022. [CrossRef]
- S. Ahamed, D. Samson, R. Sundaresan, B. Balasubramanya, and R. Thomas, “Double Blinded Randomized Controlled Trial Comparing Budesonide and Saline Nasal Rinses in the Post-operative Management of Chronic Rhinosinusitis,” Indian Journal of Otolaryngology and Head & Neck Surgery, vol. 76, no. 1, pp. 408–413, Feb. 2024. [CrossRef]
- T. Yamada, S. Fujieda, S. Mori, H. Yamamoto, and H. Saito, “Macrolide Treatment Decreased the Size of Nasal Polyps and IL-8 Levels in Nasal Lavage,” Am J Rhinol, vol. 14, no. 3, pp. 143–148, May 2000. [CrossRef]
- T. Van Zele et al., “Oral steroids and doxycycline: Two different approaches to treat nasal polyps,” Journal of Allergy and Clinical Immunology, vol. 125, no. 5, pp. 1069-1076.e4, May 2010. [CrossRef]
- D. M. Poetker, S. Mendolia-Loffredo, and T. L. Smith, “Outcomes of Endoscopic Sinus Surgery for Chronic Rhinosinusitis associated with Sinonasal Polyposis,” Am J Rhinol, vol. 21, no. 1, pp. 84–88, Jan. 2007. [CrossRef]
- R. Wynn and G. Har-El, “Recurrence Rates after Endoscopic Sinus Surgery for Massive Sinus Polyposis,” Laryngoscope, vol. 114, no. 5, pp. 811–813, May 2004. [CrossRef]
- Laure-Marine Piquet. Prise en charge chirurgicale de la polypose naso-sinusienne : indications et résultats. Médecine humaine et pathologie. 2019. ffdumas-02297746.
- C. Bachert, L. Zhang, and P. Gevaert, “Current and future treatment options for adult chronic rhinosinusitis: Focus on nasal polyposis,” Journal of Allergy and Clinical Immunology, vol. 136, no. 6, pp. 1431–1440, Dec. 2015. [CrossRef]
- Alsharif S, Jonstam K, van Zele T, Gevaert P, Holtappels G, Bachert C. Endoscopic Sinus Surgery for Type-2 CRS wNP: An Endotype-Based Retrospective Study. Laryngoscope. 2019 Jun;129(6):1286-1292. [CrossRef] [PubMed]
- Gomes SC, Cavaliere C, Masieri S, Van Zele T, Gevaert P, Holtappels G, Zhang N, Ramasamy P, Voegels RL, Bachert C. Reboot surgery for chronic rhinosinusitis with nasal polyposis: recurrence and smell kinetics. Eur Arch Otorhinolaryngol. 2022 Dec;279(12):5691-5699. [CrossRef] [PubMed]
- EUFOREA expert board meeting on uncontrolled severe chronic rhinosinusitis with nasal polyps (CRSwNP) and biologics: Definitions and management Journal of Allergy and Clinical Immunology, Volume 147, Issue 5, May 2021, Pages 1981-1982. [CrossRef]
- Fokkens WJ, Lund V, Bachert C, et al.EUFOREA consensus on biologics for CRSwNP with or withoutasthma. Allergy 2019;74:2312-2319. [CrossRef]
- Calus L, Van Bruaene N, Bosteels C, Dejonckheere S, Van Zele T, Holtappels G, Bachert C, Gevaert P. Twelve-year follow-up study after endoscopic sinus surgery in patients with chronic rhinosinusitis with nasal polyposis. Clin Transl Allergy. 2019 Jun 14;9:30. [CrossRef] [PubMed]
- EUFOREA consensus on biologics for CRSwNP with or without asthma. Fokkens WJ, Lund V, Bachert C, Mullol J, Bjermer L, Bousquet J, Canonica GW, Deneyer L, Desrosiers M, Diamant Z, Han J, Heffler E, Hopkins C, Jankowski R, Joos G, Knill A, Lee J, Lee SE, Mariën G, Pugin B, Senior B, Seys SF, Hellings PW.Allergy. 2019 Dec;74(12):2312-2319. [CrossRef] [PubMed]
- EUFOREA expert board meeting on uncontrolled severe chronic rhinosinusitis with nasal polyps (CRSwNP) and biologics: Definitions and management.Bachert C, Han JK, Wagenmann M, Hosemann W, Lee SE, Backer V, Mullol J, Gevaert P, Klimek L, Prokopakis E, Knill A, Cavaliere C, Hopkins C, Hellings P.J Allergy Clin Immunol. 2021 Jan;147(1):29-36. [CrossRef] [PubMed]
- Fokkens WJ, Viskens AS, Backer V, Conti D, De Corso E, Gevaert P, Scadding GK, Wagemann M, Bernal-Sprekelsen M, Chaker A, Heffler E, Han JK, Van Staeyen E, Hopkins C, Mullol J, Peters A, Reitsma S, Senior BA, Hellings PW. EPOS/EUFOREA update on indication and evaluation of Biologics in Chronic Rhinosinusitis with Nasal Polyps 2023. Rhinology. 2023 Jun 1;61(3):194-202. [CrossRef] [PubMed]
- Fokkens WJ, Viskens AS, Backer V, Conti D, De Corso E, Gevaert P, Scadding GK, Wagemann M, Bernal-Sprekelsen M, Chaker A, Heffler E, Han JK, Van Staeyen E, Hopkins C, Mullol J, Peters A, Reitsma S, Senior BA, Hellings PW. EPOS/EUFOREA update on indication and evaluation of Biologics in Chronic Rhinosinusitis with Nasal Polyps 2023. Rhinology. 2023 Jun 1;61(3):194-202. [CrossRef] [PubMed]
- Gevaert P, Calus L, Van Zele T, Blomme K, De Ruyck N, Bauters W, Hellings P, Brusselle G, De Bacquer D, van Cauwenberge P, Bachert C. Omalizumab is effective in allergic and nonallergic patients with nasal polyps and asthma. J Allergy Clin Immunol. 2013 Jan;131(1):110-6.e1. [CrossRef] [PubMed]
- Gevaert P, Omachi TA, Corren J, Mullol J, Han J, Lee SE, Kaufman D, Ligueros-Saylan M, Howard M, Zhu R, Owen R, Wong K, Islam L, Bachert C. Efficacy and safety of omalizumab in nasal polyposis: 2 randomized phase 3 trials. J Allergy Clin Immunol. 2020 Sep;146(3):595-605. Erratum in: J Allergy Clin Immunol. 2021 Jan;147(1):416. [CrossRef] [PubMed]
- Gevaert P, Saenz R, Corren J, Han JK, Mullol J, Lee SE, Ow RA, Zhao R, Howard M, Wong K, Islam L, Ligueros-Saylan M, Omachi TA, Bachert C. Long-term efficacy and safety of omalizumab for nasal polyposis in an open-label extension study. J Allergy Clin Immunol. 2022 Mar;149(3):957-965.e3. [CrossRef] [PubMed]
- Gevaert P, Mullol J, Saenz R, Ko J, Steinke JW, Millette LA, Meltzer EO. Omalizumab improves sinonasal outcomes in patients with chronic rhinosinusitis with nasal polyps regardless of allergic status. Ann Allergy Asthma Immunol. 2024 Mar;132(3):355-362.e1. [CrossRef] [PubMed]
- Gevaert P, Han JK, Smith SG, Sousa AR, Howarth PH, Yancey SW, Chan R, Bachert C. The roles of eosinophils and interleukin-5 in the pathophysiology of chronic rhinosinusitis with nasal polyps. Int Forum Allergy Rhinol. 2022 Nov;12(11):1413-1423. [CrossRef] [PubMed]
- Gevaert P, Van Bruaene N, Cattaert T, Van Steen K, Van Zele T, Acke F, De Ruyck N, Blomme K, Sousa AR, Marshall RP, Bachert C. Mepolizumab, a humanized anti-IL-5 mAb, as a treatment option for severe nasal polyposis. J Allergy Clin Immunol. 2011 Nov;128(5):989-95.e1-8. [CrossRef] [PubMed]
- Han JK, Bachert C, Fokkens W, Desrosiers M, Wagenmann M, Lee SE, Smith SG, Martin N, Mayer B, Yancey SW, Sousa AR, Chan R, Hopkins C; SYNAPSE study investigators. Mepolizumab for chronic rhinosinusitis with nasal polyps (SYNAPSE): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Respir Med. 2021 Oct;9(10):1141-1153. [CrossRef] [PubMed]
- Bachert C, Sousa AR, Lund VJ, Scadding GK, Gevaert P, Nasser S, Durham SR, Cornet ME, Kariyawasam HH, Gilbert J, Austin D, Maxwell AC, Marshall RP, Fokkens WJ. Reduced need for surgery in severe nasal polyposis with mepolizumab: Randomized trial. J Allergy Clin Immunol. 2017 Oct;140(4):1024-1031.e14. [CrossRef] [PubMed]
- Bachert C, Han JK, Desrosiers M, Hellings PW, Amin N, Lee SE, Mullol J, Greos LS, Bosso JV, Laidlaw TM, Cervin AU, Maspero JF, Hopkins C, Olze H, Canonica GW, Paggiaro P, Cho SH, Fokkens WJ, Fujieda S, Zhang M, Lu X, Fan C, Draikiwicz S, Kamat SA, Khan A, Pirozzi G, Patel N, Graham NMH, Ruddy M, Staudinger H, Weinreich D, Stahl N, Yancopoulos GD, Mannent LP. Efficacy and safety of dupilumab in patients with severe chronic rhinosinusitis with nasal polyps (LIBERTY NP SINUS-24 and LIBERTY NP SINUS-52): results from two multicentre, randomised, double-blind, placebo-controlled, parallel-group phase 3 trials. Lancet. 2019 Nov 2;394(10209):1638-1650. Erratum in: Lancet. 2019 Nov 2;394(10209):1618. [CrossRef] [PubMed]
- Comparative efficacy and safety of monoclonal antibodies and aspirin desensitization for chronic rhinosinusitis with nasal polyposis: A systematic review and networkmeta-analysis. Paul Oykhman, MD, MSc,a Fernando Aleman Paramo, MD,a Jean Bousquet, MD,d,e,f David W. Kennedy, MD,g Romina Brignardello-Petersen, PhD,b and Derek K. Chu, MD, PhDa,b,cJ ALLERGY CLIN IMMUNOLAPRIL 2022.
- Haxel BR, Hummel T, Fruth K, Lorenz K, Gunder N, Nahrath P, Cuevas M. Real-world-effectiveness of biological treatment for severe chronic rhinosinusitis with nasal polyps. Rhinology. 2022 Dec 1;60(6):435-443. [CrossRef] [PubMed]
- Wu Q, Zhang Y, Kong W, Wang X, Yuan L, Zheng R, Qiu H, Huang X, Yang Q. Which Is the Best Biologic for Nasal Polyps: Dupilumab, Omalizumab, or Mepolizumab? A Network Meta-Analysis. Int Arch Allergy Immunol. 2022;183(3):279-288. [CrossRef] [PubMed]
- Severe hypereosinophilia in a patient treated with dupilumab and shift to mepolizumab: the importance of multidisciplinary management. A case report and literature review.Munari S, Ciotti G, Cestaro W, Corsi L, Tonin S, Ballarin A, Floriani A, Dartora C, Bosi A, Tacconi M, Gialdini F, Gottardi M, Menzella F.Drugs Context. 2024 May 22;13:2024-3-5. [CrossRef] [PubMed]
Figure 1.
Nasal polyps, anterior rhinoscopy.
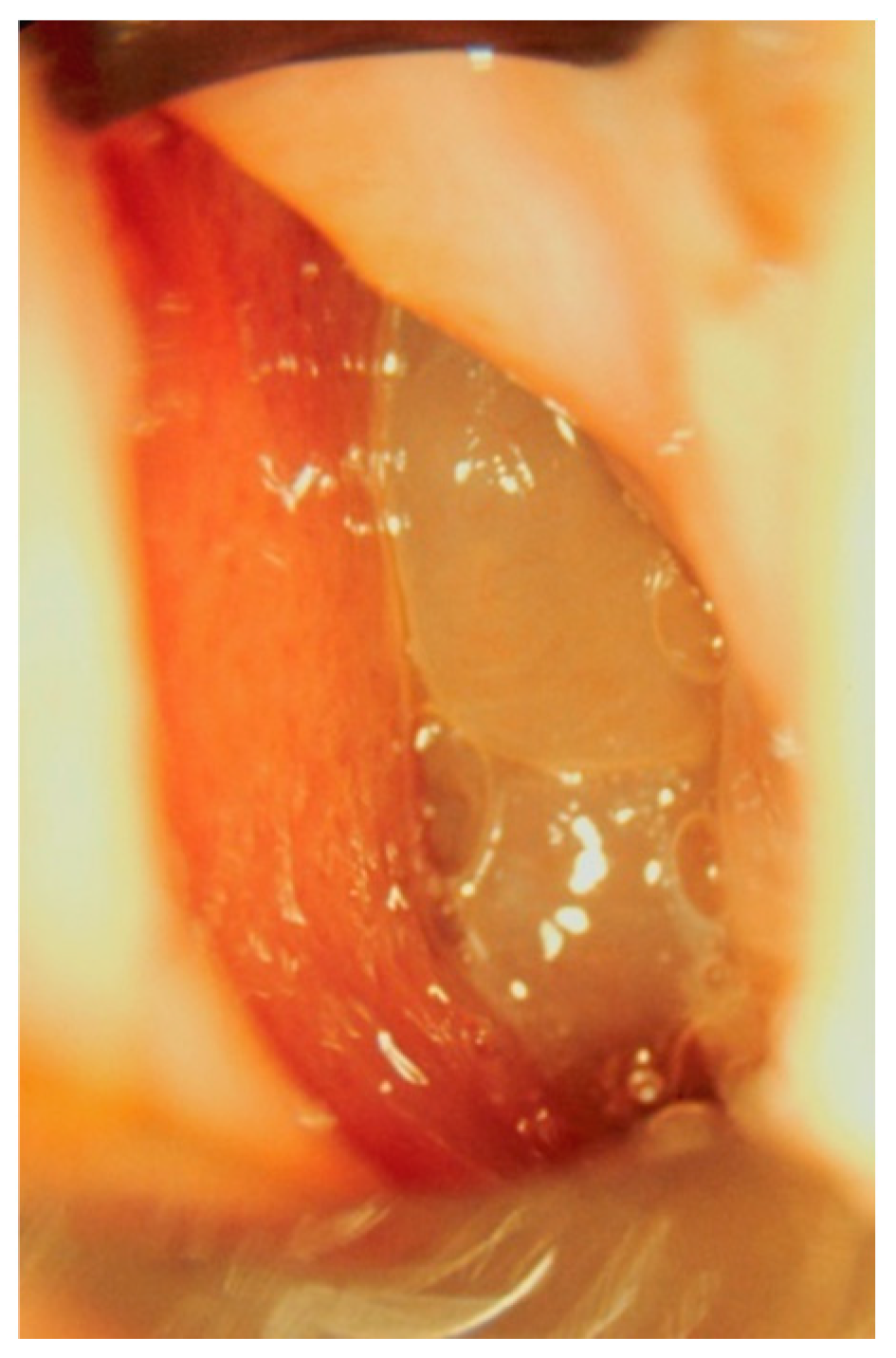
Figure 2.
Nasal polyps, endoscopic view.
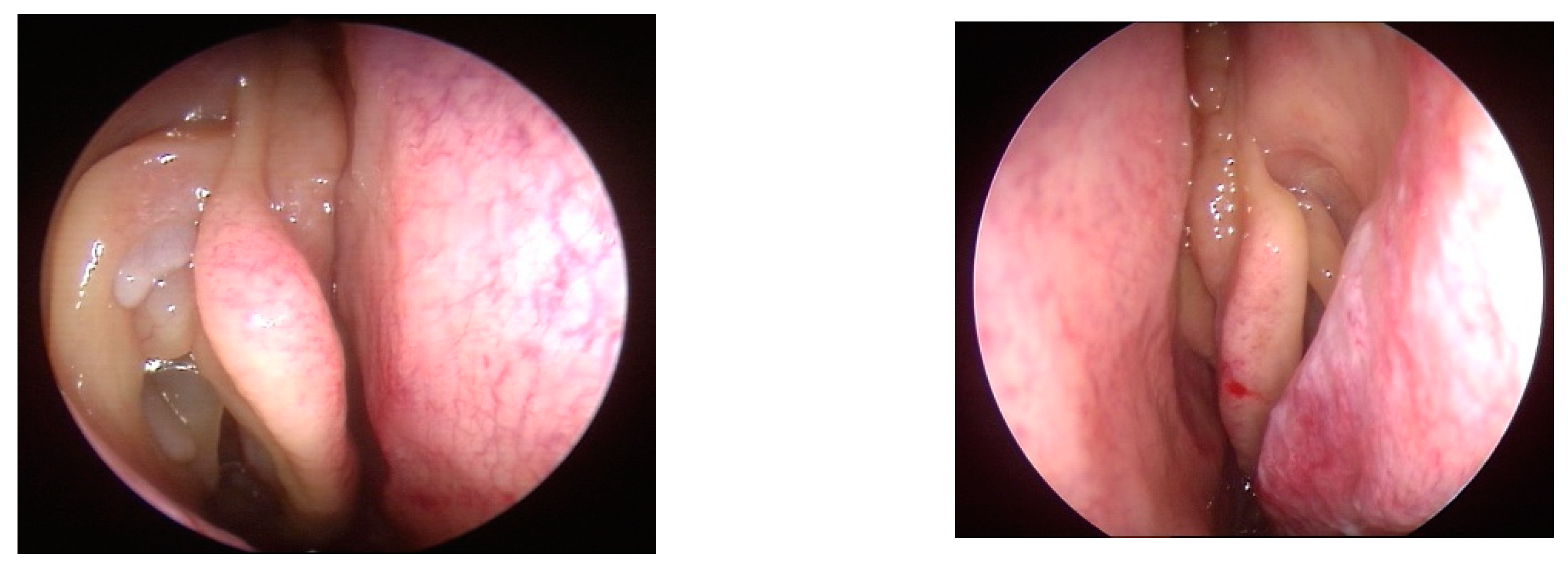
Figure 3.
SNOT test questionnaire.
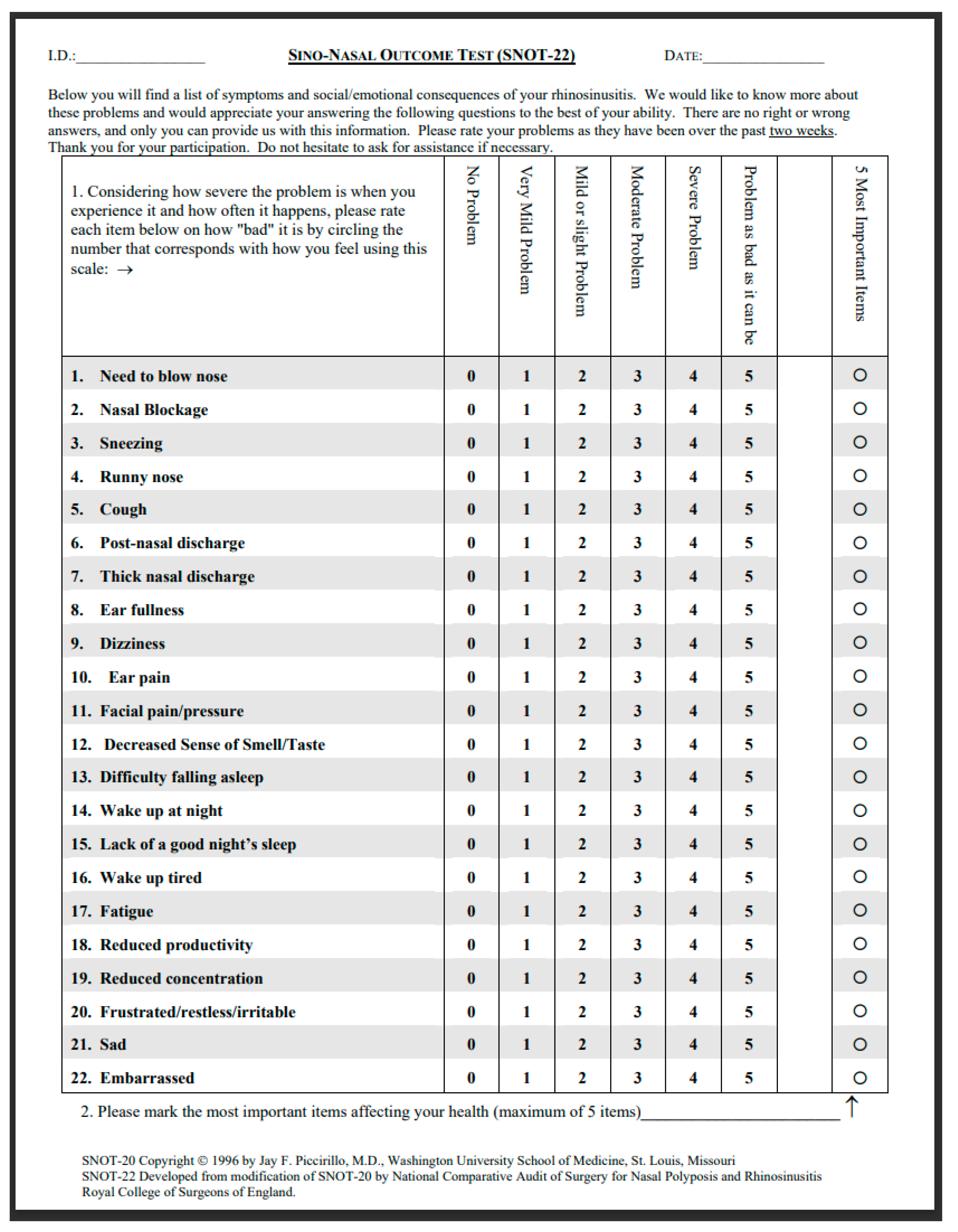

Table 1.
T. Van Zele et al., “Differentiation of chronic sinus diseases by measurement of inflammatory mediators,” Allergy, vol. 61, no. 11, pp. 1280–1289, Nov. 2006, doi: 10.1111/j.1398-9995.2006.01225.x. (19).
Table 1.
T. Van Zele et al., “Differentiation of chronic sinus diseases by measurement of inflammatory mediators,” Allergy, vol. 61, no. 11, pp. 1280–1289, Nov. 2006, doi: 10.1111/j.1398-9995.2006.01225.x. (19).
| Cells : eosino/neutron | IgE (tot or specific |
Pathogens Staphylo or other |
Cytokines | Other mediators | |
|---|---|---|---|---|---|
| Blood | + | + | (+) | (+) | |
| Culture Swab | + | ||||
| Nasal secretion | + | + | + | + | |
| Nasal cytology | + | ||||
| Tissue | + | + | + | + | |
| Nasal NO | (+) |
Table 2.
Ref. T. Van Zele et al., “Differentiation of chronic sinus diseases by measurement of inflammatory mediators,” Allergy, vol. 61, no. 11, pp. 1280–1289, Nov. 2006, doi: 10.1111/j.1398-9995.2006.01225. x. [19].
Table 2.
Ref. T. Van Zele et al., “Differentiation of chronic sinus diseases by measurement of inflammatory mediators,” Allergy, vol. 61, no. 11, pp. 1280–1289, Nov. 2006, doi: 10.1111/j.1398-9995.2006.01225. x. [19].
| Controls | Chronic sinusitis | Nasal polyps | Cystic fibrosis: nasal polyps | One-way Anova Fisher test |
|
|---|---|---|---|---|---|
| N | 10 | 10 | 14 | 14 | 14 |
| Ct score/ Lund & Mackay | 0.75 (0-2) | 6 (2-11) | 16.3 (7-24) | 14.5 (5-20) | <0.0001 |
| Polyp score (Davos) | 0 | 0 | 4.8 (2-6) | 2.9 (0-6) | <0.0001 |
| Total symptom score | 4(3-5) | 6.6 (4-10) | 9.6 (3-14) | 4.3 (0-9) | <0.0001 |
| Nasal congestion | 1.1 (0-3) | 1.0 (0-3) | 2.6 (0-3) | 2.8 (2-3) | 0.001 |
| Sneezing | 0 | 0.1 (0-1) | 0.2 (0-2) | 0.6 (0-2) | 0.761 |
| Rhinorea | 0.3 (0-2) | 1.6 (0-3) | 1.6 (0-3) | 1.0 (0-3) | 0.19 |
| Loss of smell | 0 | 0 | 2.3 (0-3) | 1.0 (0-3) | <0.0001 |
| Postnasal drip | 0 | 1.4 (0-2) | 1.3 (0-3) | 0.6 (0-2) | 0.001 |
| Headache | 0.9 (0-2) | 2.5 (1-3) | 1.6 (0-3) | 1.2 (0-3) | 0.003 |
Table 3.
Comparison of the benefits and weaknesses of oral corticosteroids versus sinus surgery.
| Benefits | Weakness | |
|---|---|---|
| Oral corticosteroids | Big improvement of the major symptoms Improvement of the HRQL: Improvement of the sleep quality, sense of smell, reduction of the facial pain, reduction of nasal blockage |
Frequent and early recurrence of the symptoms Rebound effect Advers events: gain of weight, anxiety, nervosity, irritability Osteoporosis, diabetes melittus, necrosis of the head of the hip |
| Sinus surgery | Improvement of the HRQL Good outcome after a short and middle term |
Frequent recurrence of the disease Iatrogenicity Need for a general anesthesia Possibility of minor and major intraoperative and postoperativecomplications |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



