
Submitted:
22 August 2024
Posted:
27 August 2024
You are already at the latest version
Abstract
This cross-sectional survey assessed the resilient coping levels and their relationship with the socio-demographic characteristics of nursing professionals in Saudi Arabia. Adult (≥18 years) registered nurses and practicing for ≥1 year were included. Resilient coping levels (as assessed via a 4-item Brief Resilience Coping Scale; BRCS) and socio-demographic and other characteristics data were collected. Descriptive analysis and ordinal logistic regressions were used to analyze the data. Further, the psychometric properties of the BRCS were reported. A total of 216 nursing professionals were included. The mean BRCS score was 14.6 (standard deviation=3.6), with most nursing professionals (62.5%) reporting medium to high resilience coping levels. The ordinal logistic regression model demonstrated that increasing age (p=0.002), best overall health (p=0.001), and nurses posted in the outpatient department (p=0.049) and intensive care unit (p=0.032) had significantly high resilient coping levels. The internal consistency of the BRCS was good (Cronbach’s alpha=0.80). In summary, nursing professionals in Saudi Arabia showed medium resilient coping levels. Moreover, this study suggests that BRCS is a psychometrically reliable and adequate tool for assessing resilience coping levels and provides valuable insights into the relationship between resilient coping levels and socio-demographic characteristics of the nursing professionals in Saudi Arabia.
Keywords:
brief resilient coping scale
; nursing professionals
; resilient coping
; Saudi Arabia
1. Introduction
Nursing professionals play a key role in the healthcare systems across the world [1]. Despite their invaluable contributions, nurses often experience tremendous stress caused due to several physical (exposure to illness, burnout), psychological (lack of support and acknowledgment, exploitation), and environmental factors (safety at the workplace) [1,2,3]. Furthermore, lack of appreciation, social status and support, high workload, staffing shortages, under-compensation, etc further increase their stress levels affecting their professional and personal lives [4].
Resilience is an individual’s cognitive and behavioral ability to effectively counter the adverse effects of stress and successfully thrive in the face of adversity or traumatic experiences [5]. Several studies have reported high resilience levels improve a person’s physical and mental well-being and quality of life [6,7,8,9]. In a recent study that investigated the impact of psychological resilience in the context of adverse effects, resilience exerted a protective effect on the well-being of individuals [9]. Similarly, in a survey-based study of 2063 individuals, high resilience levels were reported to exert beneficial effects (i.e., on the perception of stress, psychological responses to stress, and job-related stress) among workers in challenging work environments [8].
Given the highly stressful profession of nursing professionals, resilience could be an important mechanism to protect them against adverse effects of personal and occupational stress [10]. Several studies have reported a positive impact of resilient coping on the personal and professional aspects of nursing professionals [11,12,13,14]. In a Japanese study of nurses working in a psychiatric hospital (n=313), nurses who had high resilience levels experienced lower levels of depression and exhaustion [11]. A US-based study reported work satisfaction and resilience positively affected the organizational commitment of the nurses [12]. Moreover, resilient nurses exhibit better adaptive strategies, and coping skills, and thrive through adversities while delivering quality care to the patients [13,14]. However, little is known about the resilience capacity of the nursing professionals in Saudi Arabia. To address this knowledge gap, the present study explored the resilient coping levels and their relationship with the socio-demographic characteristics of nursing professionals in Saudi Arabia. Additionally, the psychometric properties of the Brief Resilient Coping Scale (BRCS; a tool used to assess resilient coping) in this population were reported.
1. Methods
1.1. Study Design
This cross-sectional survey was conducted between January and May 2023. Adult (18 years or older) registered nursing professionals, working for at least a year, and provided informed consent were eligible for participation in this study. The data collection was done in a tertiary care hospital in Riyadh, Saudi Arabia. The protocol and questionnaire used for the survey were reviewed by the Institutional Review Board (IRB) and was exempted from IRB approval (IRB number: 21-522E).
All study participants were informed about the purpose of the survey and assured that the collected information would be kept confidential and used solely for the study. Following their approval, the data was collected, analyzed, and reported as per the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines (https://www.strobe-statement.org/) [15].
1.1. Socio-Demographic and Other Characteristics
The socio-demographic characteristics viz., age, sex, marital status, education, and nationality, were collected. In addition, information on the years of clinical experience, work shift, posting ward in the hospital, overall health, and the presence of chronic conditions were recorded.
1.1. Resilience Coping Levels
The resilience coping levels of the participants were measured using a 4-item BRCS designed to capture tendencies to cope with stress adaptively. The scale focuses on the tendency to effectively employ coping strategies in flexible, committed ways to actively solve problems despite stressful circumstances. Each item in the scale is scored on a 5-point Likert scale from 1 to 5. The total score is summed from the individual item scores and ranges from 4 to 20 (4–13 indicating low resilient coping; 14–16 indicating medium resilient coping; 17–20 indicating high resilient coping) [16].
1.1. Statistical Analysis
Socio-demographic characteristics (age, sex, marital status, education level, nationality) and other characteristics (clinical experience, work shift, posting ward in the hospital, overall health, and the presence of chronic conditions) were analyzed descriptively. Categorical variables were summarized as absolute values and percentages, while continuous variables were presented as means and standard deviations (SDs). The categorical variables were analyzed using the Chi-square test. For continuous measures, one-way Analysis of Variance (ANOVA) followed by Tukey’s post hoc honestly significant difference test was used to detect the difference across the groups. For the multivariate analysis, ordinal logistic regression was used to examine the relationship between resilient coping levels and socio-demographic factors with a 95% confidence interval (CI). The threshold for significance was set at p<0.05.
The psychometric properties of the BRCS were based on several analyses. As a measure of internal consistency, Cronbach’s alpha was calculated for the BRCS scale and its four items. Pearson correlation (r) was used to measure item correlations. The construct validity of BRCS was evaluated using exploratory factor analysis (EFA) using principal component analysis and varimax rotation. Bartlett’s test of sphericity (expressed as χ2) and the Kaiser-Meyer-Olkin (KMO) were performed. The threshold for Bartlett’s test of sphericity was set to p<0.05 and KMO values close to 1.0, indicating the usefulness of factor analysis in this study population. The minimum factor loading criteria was set to 0.50. The commonality of the BRCS (which indicates the amount of variance in each dimension) was also assessed to ensure acceptable levels of explanation. Data analyses were performed using Statistical Package for the Social Sciences (SPSS, version 26.0. IBM, NY, USA) and the software R version 4.4.1 (R Foundation for Statistical Computing, Vienna, Austria).
1. Results
1.1. Sample Characteristics
Overall, 216 nurses (132 via offline mode, and 84 via online mode) participated in this study. The mean age of the study participants was 32.0 (SD=5.3) years, men (52.8%), and married (58.8%). Participants were predominantly from Saudi Arabia (80.1%), had a bachelor’s in nursing (80.6%), and 6 to 15 years of clinical experience (56.5%). Most nurses worked in the morning shift (60.6%) and were posted in an emergency ward (29.2%) followed by surgical and medical wards (Table 1). The overall health of most participants (68.5%) was high (i.e., scored 8–10 on a 10-point rating scale; a lower scale indicates poor health, and a higher score indicates best health), and only 18.5% of the participants reported the presence of a chronic condition (Table 1).
1.1. Resilience Coping Levels
The mean total score of BRCS among all participants was 14.6 (SD=3.6), indicating medium coping levels. Most participants reported medium to high coping levels (Figure 1).
1.1. Relationship between Resilience Coping Levels and Socio-demographic and Other Variables
When different levels of resilience coping were analyzed in relation to the socio-demographic characteristics, a significant association was found with the age of the nursing professionals i.e., levels of resilience coping increased with the age of the nursing professionals (F=12.07; p=0.000). Tukey’s post hoc analyses confirmed the differences between the groups i.e., the mean age of the nursing professionals with medium and high resilient coping levels was significantly higher than those with low resilient coping (Table 2). Furthermore, a significant association was also found between resilient coping levels and overall health (χ2=49.34; p=0.000), and the presence/absence of a chronic condition (χ2=82.22; p=0.000) (Table 2).
Low vs. medium resilient coping levels (Q=5.65; p=0.000)
Low vs. high resilient coping levels (Q=6.00; p=0.001)
Medium vs. high resilient coping levels (Q=0.34; p=0.967)
As shown in Table 3, the ordinal logistic regression model demonstrated significant relationships between resilience coping levels and a few characteristics of nursing professionals. Resilience coping levels showed a positive association with age, indicating the older the age, the higher the resilience coping levels among the nurses (p=0.002). Similarly, nurses posted in an outpatient department (p=0.049), intensive care unit (p=0.032), and laboratory (p=0.052) were found to be significantly more resilient than those posted in other wards. Additionally, coping levels were associated with one’s perception of their overall health i.e., nursing professionals who rated their overall health as “best” demonstrated significantly higher coping levels compared to those who were in poor (p=0.000) or moderate overall health (p=0.001) (Table 3).
1.1. Psychometric Properties of BRCS
The parameter of internal consistency (i.e., Cronbach alpha) for the BRCS was 0.80, indicating a good internal consistency. In our scale analysis to obtain Cronbach’s alpha, the item-total correlations ranged from 0.56 to 0.73. If any of the four items were deleted, it would cause a decrease in the α-value, highlighting the importance of each of the four BRCS items for the scale’s reliability (Table 4). The EFA performed with the total sample (N=216) showed that the results were significant (i.e., χ2=279.78; df=6; p<0.001) indicating its suitability for factor analysis. The coefficient of the KMO test was 0.74, indicating that the sampling is adequate. Furthermore, the analysis revealed the existence of one factor including all items, which explained 62.33% of the total variance (factor loadings were 0.75 for both BRCS1&2, 0.78 for BRCS3, and 0.88 for BRCS4 items).
1. Discussion
To our knowledge, this is the first study to report the resilience coping levels among nursing professionals in Saudi Arabia. Overall, nursing professionals in this study had an intermediate BRCS score, indicating medium resilient coping levels. Most nursing professionals (62.5%) surveyed demonstrated medium to high coping levels. Furthermore, socio-demographic correlates of nursing professionals viz., age, overall health, and posting in certain wards were significantly associated with the resilience coping levels in this population. Finally, BRCS was a psychologically reliable and adequate tool for assessing resilience coping levels in this population.
There has been an upsurge of interest in understanding resilience capacity and the factors affecting the coping levels of nursing professionals [17,18,19]. The present study was conducted among nursing professionals given their susceptibility to several professional and personal stress factors that adversely affect their health and abilities to manage their job. Our study revealed that most nursing professionals in Saudi Arabia had moderate to high resilience coping capabilities, consistent with the levels reported among Brazilian nurses [18]. Analysis of the factors influencing coping levels demonstrated age to be positively associated with the levels of resilience (i.e., the older the participants, the greater their resilience coping levels), in alignment with the previous studies [18,19]. In a cross-sectional study that included nursing workers in Brazil (n=375), age and working time were reported as a determinant of resilience [18]. Similarly, a UK-based study that assessed the experiences of nurses working in a respiratory environment during the COVID-19 pandemic reported younger nurses with less experience had higher levels of anxiety and depression and lower resilience [19]. Importantly, the relationship between resilience and age observed in our study contrasts with those reported by some studies [23,24]. A possible explanation of this discrepancy could be attributed to the population, study period, and the setting considered in the present study versus the previously published studies [19,23,24]. The overall health of the nursing professionals was another socio-demographic variable that significantly influenced the resilience levels, i.e., nursing professionals with best overall health demonstrated significantly higher coping levels compared to those with poor or moderate overall health. This finding is similar to a previous study in which students with good perceptions of their health more often showed high resilience than those with regular or poor perceptions [24]. This is quite expected as individuals in the best health state (i.e., physical, and psychological) are more engaged and productive, and tend to be overcome stress more effectively versus those with poor health states [25,26]. With regards to the other variables, nursing professionals posted in an outpatient department, intensive care unit, and laboratory demonstrated significantly higher resilience coping levels than those posted in other wards. The effect of posting in various hospital wards and resilience levels has not been reported in previous studies, therefore, this association needs to be investigated in future studies.
Furthermore, the present study investigated the psychometric properties of BRCS in the nursing population in Saudi Arabia. The internal consistency of the BRCS was good (i.e., Cronbach’s alpha was 0.80), which is consistent with the previous studies that reported Cronbach’s alpha between 0.59 to 0.86 [16,27,28,29,30,31,32]. The scale also presented an adequate inter-total correlation (ranging from 0.56 to 0.73), thus, adding to the empirical evidence of the internal consistency of the BRCS in Saudi nursing professionals. Furthermore, the results of EFA substantiate that the one-factor solution was the most acceptable for all the BRCS items, consistent with the findings of previous studies [30,32,33].
A few caveats of this study merit consideration. The cross-sectional design ruled out a causal and longitudinal relationship between resilient coping levels and related indicators. The small sample size from a single center and convenience sampling add to the bias. Participation in this study was voluntary; therefore, underlying selection bias cannot be ruled out. Moreover, the self-reported nature of the survey may further introduce other potential biases (i.e., false reporting and inaccurate recall). Finally, this study reflects the opinions and experiences of nursing professionals in Saudi Arabia; therefore, findings of this study cannot be generalized to participants from other professions across Saudi Arabia.
Despite the limitations, the current study adds to our understanding of the association between resilient coping levels and socio-demographic characteristics of nursing professionals in Saudi Arabia. Furthermore, this study used a psychometrically validated and reliable BRCS to assess the resilient coping levels, which has been extensively used across several studies.
1. Conclusions
In summary, nursing professionals surveyed in this study demonstrated medium resilient coping levels and calls for devising effective strategies that could enhance their coping levels. Moreover, this study suggests that BRCS is a psychometrically reliable and adequate tool for assessing resilience coping levels and sheds light on the relationship between resilience coping levels and socio-demographic characteristics of the nursing professionals in Saudi Arabia. Further, future studies are warranted to explore the specific concerns and devise adequate strategies to improve the resilience coping levels of the nursing professionals in Saudi Arabia.
Author Contributions
Abdulrhman Albougami was involved in the conceptualization, methodology, formal analysis, investigation, data curation, writing (original draft preparation, review and editing) of the study. The author has read and agreed to the published version of the manuscript.
Funding
This study received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. The study protocol, questionnaire used for the survey were reviewed by the Institutional Review Board (IRB) and was exempted from IRB approval (IRB number: 21-522E).
Informed Consent Statement
Informed consent was obtained from all the participants involved in the study.
Data Availability Statement
The data presented in this manuscript are available on request from the corresponding author. The data are not publicly available due to privacy reasons.
Acknowledgments
None.
Conflicts of Interest
The author declares no conflict of interest.
References
- Dos Santos, L.M. Stress, burnout, and low self-efficacy of nursing professionals: A qualitative inquiry. Healthcare (Basel). 2020, 8, 424. [Google Scholar] [CrossRef] [PubMed]
- Babapour, A.R.; Gahassab-Mozaffari, N.; Fathnezhad-Kazemi, A. Nurses' job stress and its impact on quality of life and caring behaviors: A cross-sectional study. BMC Nurs. 2022, 21, 75. [Google Scholar] [CrossRef]
- Jacobs, A.C.; Lourens, M. Emotional challenges faced by nurses when taking care of children in a private hospital in South Africa. Africa J. Nurs. Midwifery. 2016, 18, 196–210. [Google Scholar] [CrossRef]
- Mróz, J. Predictive roles of coping and resilience for the perceived stress in nurses. Prog. Health. Sci. 2015, 5, 77–83. [Google Scholar]
- Babić, R.; Babić, M.; Rastović, P.; Ćurlin, M.; Šimić, J.; Mandić, K.; Pavlović, K. Resilience in health and illness. Psychiatr. Danub. 2020, 32, 226–232. [Google Scholar] [PubMed]
- Windle, G. The contribution of resilience to healthy ageing. Perspect. Public Heal. 2012, 132, 159–160. [Google Scholar]
- Friedly, L. Mental health, resilience, and inequalities. World Health Organization. 2009 (Available: https://www.womenindisplacement.org/sites/g/files/tmzbdl1471/files/2020-10/Mental%20health%2C%20resilience%20and%20inequalities.pdf) (Accessed June 2024).
- Shatté, A.; Perlman, A.; Smith, B.; Lynch, W. The positive effect of resilience on stress and business outcomes in difficult work environments. J. Occup. Environ. Med. 2017, 59, 135–140. [Google Scholar] [CrossRef]
- Hsieh, S.; Chang, Y.H.; Yao, Z.F.; Yang, M.H.; Yang, C.T. The effect of age and resilience on the dose-response function between the number of adversity factors and subjective well-being. Front. Psychol. 2024, 15, 1332124. [Google Scholar] [CrossRef]
- Yu, F.; Chu, G.; Yeh, T.; Fernandez, R. Effects of interventions to promote resilience in nurses: A systematic review. Int. J. Nurs. Stud. 2024. [CrossRef]
- Gito, M.; Ihara, H.; Ogata, H. The relationship of resilience, hardiness, depression and burnout among Japanese psychiatric hospital nurses. J. Nurs. Educ. Pract. 2013, 3, 11. [Google Scholar] [CrossRef]
- Seo, S.K.; Kim, M.; Park, J. Effects of resilience and job satisfaction on organizational commitment in Korean-American registered nurses. J. Korean Acad. Nurs. Adm. 2014, 20, 48–58. [Google Scholar] [CrossRef]
- Mealer, M.; Jones, J.; Newman, J.; McFann, K.K.; Rothbaum, B.; Moss, M. The presence of resilience is associated with a healthier psychological profile in intensive care unit (ICU) nurses: Results of a national survey. Int. J. Nurs. Stud. 2012, 49, 292–299. [Google Scholar] [CrossRef] [PubMed]
- McDonald, G.; Jackson, D.; Vickers, M.H.; Wilkes, L. Surviving workplace adversity: A qualitative study of nurses and midwives and their strategies to increase personal resilience. J. Nurs. Manag. 2016, 24, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. Int. J. Surg. 2014, 12, 1500–1524. [Google Scholar] [CrossRef] [PubMed]
- Sinclair, V.G.; Wallston, K.A. The development and psychometric evaluation of the Brief Resilient Coping Scale. Assessment. 2004, 11, 94–101. [Google Scholar] [CrossRef]
- Hart, P.L.; Brannan, J.D.; De Chesnay, M. Resilience in nurses: an integrative review. J. Nurs. Manag. 2014, 22, 720–734. [Google Scholar] [CrossRef] [PubMed]
- Silva, S.M.D.; Baptista, P.C.P.; Silva, F.J.D.; Almeida, M.C.D.S.; Soares, R.A.Q. Resilience factors in nursing workers in the hospital context. Rev. Esc. Enferm. USP. 2020, 54, e03550. [Google Scholar] [CrossRef] [PubMed]
- Roberts, N.J.; McAloney-Kocaman, K.; Lippiett, K.; Ray, E.; Welch, L.; Kelly, C. Levels of resilience, anxiety and depression in nurses working in respiratory clinical areas during the COVID pandemic. Respir. Med. 2021, 176, 106219. [Google Scholar] [CrossRef]
- Khamisa, N.; Oldenburg, B.; Peltzer, K.; Ilic, D. Work related stress, burnout, job satisfaction and general health of nurses. Int. J. Environ. Res. Public Health. 2015, 12, 652–666. [Google Scholar] [CrossRef]
- Maharaj, S.; Lees, T.; Lal, S. Negative mental states and their association to the cognitive function of nurses. J. Psychophysiol. 2019, 33, 207–218. [Google Scholar] [CrossRef]
- Barnawi, N.; Barnawi, B. The relationship between nurses’ self-efficacy and occupational stress in the critical care unit at King Abdul-Aziz Hospital in Jeddah, Saudi Arabia. Nurs. Commun. 2023, 7, e2023028. [Google Scholar] [CrossRef]
- Aryuwat, P.; Holmgren, J.; Asp, M.; Lövenmark, A.; Radabutr, M.; Sandborgh, M. Factors associated with resilience among Thai nursing students in the context of clinical education: A cross-sectional study. Educ. Sci. 2024, 14, 78. [Google Scholar] [CrossRef]
- Oliveira, A.C.P.; Machado, A.P.G., Aranha, R.N. Identification of factors associated with resilience in medical students through a cross-sectional census. BMJ Open. 2017, 7, e017189. [CrossRef]
- Neumann, R.J.; Ahrens, K.F.; Kollmann, B.; Goldbach, N.; Chmitorz, A.; Weichert, D.; Fiebach, C.J.; Wessa, M.; Kalisch, R.; Lieb, K.; Tüscher, O.; Plichta, M.M.; Reif, A.; Matura, S. The impact of physical fitness on resilience to modern life stress and the mediating role of general self-efficacy. Eur. Arch. Psychiatry Clin. Neurosci. 2022, 272, 679–692. [Google Scholar] [CrossRef] [PubMed]
- Weitzel, E.C.; Löbner, M.; Glaesmer, H.; Hinz, A.; Zeynalova, S.; Henger, S.; Engel, C.; Reyes, N.; Wirkner, K.; Löffler, M.; Riedel-Heller, S.G. The association of resilience with mental health in a large population-based sample (LIFE-Adult-Study). Int. J. Environ. Res. Public Health. 2022, 19, 15944. [Google Scholar] [CrossRef]
- Tomás, J.M.; Meléndez, J.C.; Sancho, P.; Mayordomo, T. Adaptation and initial validation of the BRCS in an elderly Spanish sample. Eur. J. Psychol. Assess. 2012, 28, 283–289. [Google Scholar] [CrossRef]
- Limonero, J.T.; Tomás-Sábado, J.; Gómez-Romero, M.J.; Maté-Méndez, J.; Sinclair, V.G.; Wallston, K.A.; Gómez-Benito, J. Evidence for validity of the brief resilient coping scale in a young Spanish sample. Span. J. Psychol. 2014, 17, E34. [Google Scholar] [CrossRef]
- Moret-Tatay, C.; Muñoz, J.J.F.; Mollá, C.C.; Navarro-Pardo, E.; Alcover de la Hera, C.M. Psychometric properties and factor structure of the BRCS in an elderly Spanish sample. Anales De Psicología. 2015, 31, 1030–1034. [Google Scholar] [CrossRef]
- Kocalevent, R.D.; Zenger, M.; Hinz, A.; Klapp, B.; Brähler, E. Resilient coping in the general population: standardization of the Brief Resilient Coping Scale (BRCS). Health Qual. Life Outcomes. 2017, 15, 251. [Google Scholar] [CrossRef]
- Fung, SF. Validity of the Brief Resilience Scale and Brief Resilient Coping Scale in a Chinese sample. Int. J. Environ. Res. Public Health. 2020, 17, 1265. [Google Scholar] [CrossRef]
- Sirkiä, C.; Koivumaa-Honkanen, H.; Parkkola, K.; Hurtig, T. Resilient coping and the psychometric properties of the Brief Resilient Coping Scale (BRCS) among healthy young men at military call-up. Mil. Behav Health. 2024. [Google Scholar] [CrossRef]
- Poejo, J.; Gomes, AI.; Granjo, P.; Dos Reis Ferreira, V. Resilience in patients and family caregivers living with congenital disorders of glycosylation (CDG): A quantitative study using the Brief Resilience Coping Scale (BRCS). Orphanet J. Rare Dis. 2024, 19, 98. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Distribution of study participants based on resilience coping score* (N=216). Notes: *Measured using the Brief Resilience Coping Scale (4–13 indicates low resilient coping; 14–16 indicates medium resilient coping; 17–20 indicates high resilient coping).
Figure 1.
Distribution of study participants based on resilience coping score* (N=216). Notes: *Measured using the Brief Resilience Coping Scale (4–13 indicates low resilient coping; 14–16 indicates medium resilient coping; 17–20 indicates high resilient coping).
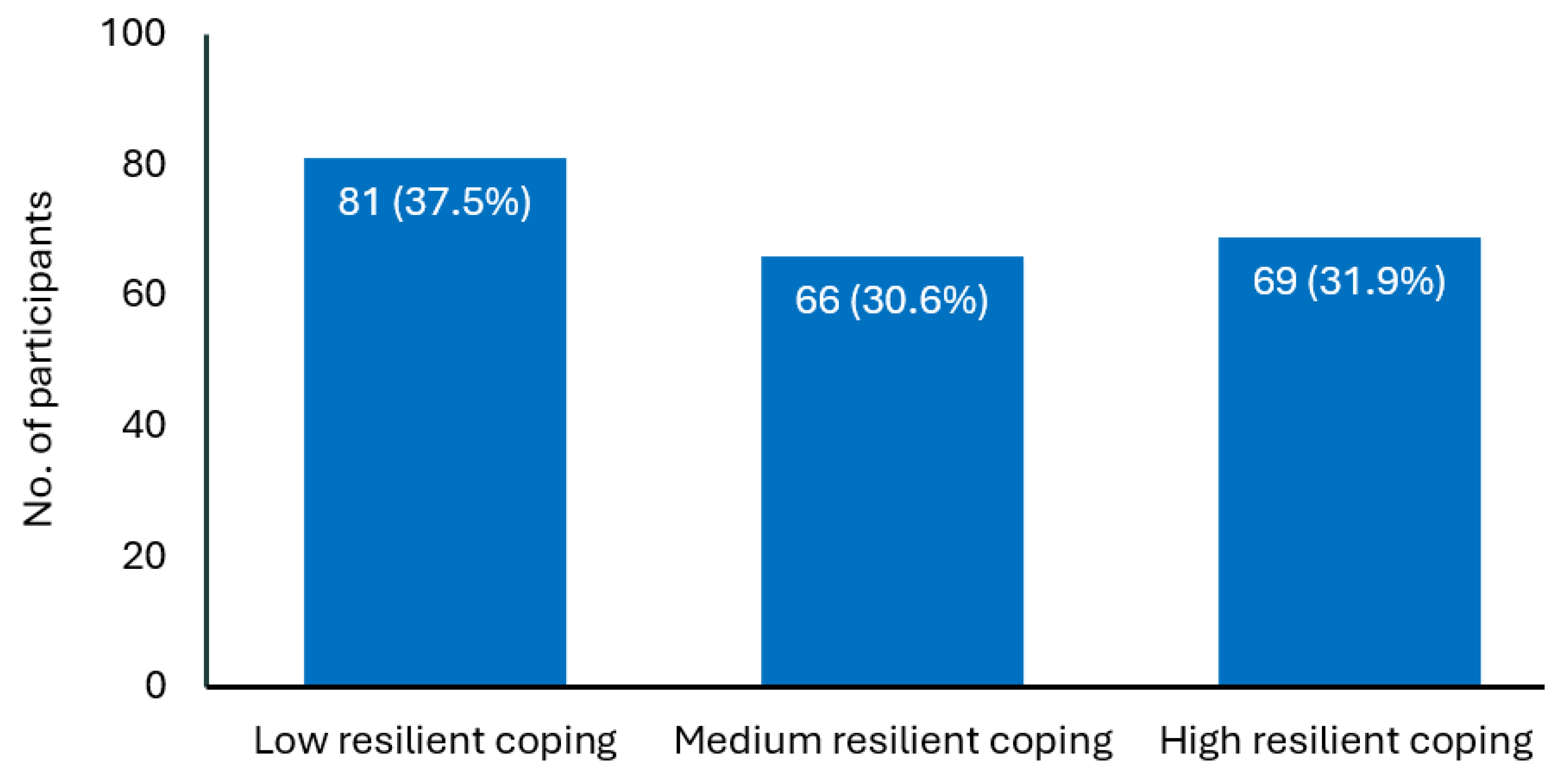

Table 1.
Socio-demographic and other characteristics.
| Overall participants (N=216) | |
|---|---|
| Mean (SD) age, in years | 32.0 (5.3) |
| Age group, n (%) | |
| ≤25 years | 12 (5.6%) |
| 26–39 years | 189 (87.5%) |
| Over 40 years | 15 (6.9%) |
| Sex, n (%) | |
| Male | 114 (52.8%) |
| Female | 96 (44.4%) |
| Prefer not to disclose | 6 (2.8%) |
| Marital status, n (%) | |
| Single | 66 (30.6%) |
| Married | 127 (58.8%) |
| Divorced | 19 (8.8%) |
| Widow | 4 (1.9%) |
| Education, n (%) | |
| Diploma in nursing | 29 (13.4%) |
| Graduate in nursing | 174 (80.6%) |
| Postgraduation in nursing | 13 (6.0%) |
| Nationality, n (%) | |
| Saudi | 173 (80.1%) |
| Filipino | 22 (10.2%) |
| Indian | 11 (5.1%) |
| Other | 10 (4.6%) |
| Clinical experience, n (%) | |
| ≤5 years | 68 (31.5%) |
| 6−14 years | 109 (50.5%) |
| ≥15 years | 39 (18.1%) |
| Work shift, n (%) | |
| Morning | 131 (60.6%) |
| Afternoon | 33 (15.3%) |
| Evening | 24 (11.1%) |
| Rotating | 28 (13.0%) |
| Posting ward, n (%) | |
| Emergency | 63 (29.2%) |
| Surgical | 49 (22.7%) |
| Medical | 41 (19.0%) |
| OPD | 22 (10.2%) |
| ICU | 18 (8.3%) |
| PHC | 8 (3.7%) |
| Others | 5 (2.3%) |
| Pediatric | 4 (1.9%) |
| Obstetrics/Gynecology | 3 (1.4%) |
| Laboratory | 3 (1.4%) |
| Overall health*, n (%) | |
| ≤4 | 25 (11.6%) |
| 5−7 | 43 (19.9%) |
| 8−10 | 148 (68.5%) |
| Presence of a chronic condition**, n (%) | |
| Yes | 40 (18.5%) |
| No | 176 (81.5%) |
Abbreviations: ICU, intensive care unit; OPD, outpatient department; PHC, primary healthcare. Notes: *Measured on a 0-10 rating scale (score of ≤4 indicates poor health; score between 5–7 indicates moderate health; score 8–10 indicates best health). **Conditions such as hypertension, diabetes, neurological, cardiovascular, and any other disease.
Table 2.
Relationship between resilience coping levels and socio-demographic and other variables.
| Variable | Resilience coping levels | Point estimates | p value | ||
|---|---|---|---|---|---|
| Low | Moderate | High | |||
| Age | F=12.07 | 0.000† | |||
| Mean (SD) | 29.9 (5.1) | 33.2 (5.0) | 33.4 (5.0) | ||
| 95% CI | 28.79–31.01 | 31.99–34.41 | 32.22–35.58 | ||
| Sex, n (%) | χ2=2.59 | 0.628 | |||
| Male | 40 (35.1%) | 37 (32.5%) | 37 (32.5%) | ||
| Female | 37 (38.5%) | 28 (29.2%) | 31 (32.3%) | ||
| Prefer not to disclose | 4 (66.7%) | 1 (16.7%) | 1 (16.7%) | ||
| Marital status, n (%) | χ2=6.22 | 0.399 | |||
| Single | 28 (42.4%) | 18 (27.3%) | 20 (30.3%) | ||
| Married | 41 (32.3%) | 44 (34.6%) | 42 (33.1%) | ||
| Divorced | 9 (47.4%) | 4 (21.1%) | 6 (31.6%) | ||
| Widow | 3 (75.0%) | 0 (0.0%) | 1 (25.0%) | ||
| Education, n (%) | χ2=2.21 | 0.697 | |||
| Diploma in nursing | 14 (48.3%) | 8 (27.6%) | 7 (24.1%) | ||
| Graduate in nursing | 62 (35.6%) | 55 (31.6%) | 57 (32.8%) | ||
| Postgraduation in nursing | 5 (38.5%) | 3 (23.1%) | 5 (38.5%) | ||
| Nationality, n (%) | χ2=7.00 | 0.320 | |||
| Saudi | 7 (63.6%) | 1 (9.1%) | 3 (27.3%) | ||
| Filipino | 5 (22.7%) | 10 (45.5%) | 7 (31.8%) | ||
| Indian | 66 (38.2%) | 52 (30.1%) | 55 (31.8%) | ||
| Other | 3 (30.0%) | 3 (30.0%) | 4 (40.0%) | ||
| Clinical experience, n (%) | χ2=7.00 | 0.320 | |||
| ≤5 years | 33 (47.1%) | 17 (24.3%) | 20 (28.6%) | ||
| 6−14 years | 42 (34.4%) | 40 (32.8%) | 40 (32.8%) | ||
| ≥15 years | 6 (25.0%) | 9 (37.5%) | 9 (37.5%) | ||
| Work shift, n (%) | χ2=4.31 | 0.635 | |||
| Morning | 49 (37.4%) | 43 (32.8%) | 39 (29.8%) | ||
| Afternoon | 16 (48.5%) | 7 (21.2%) | 10 (30.3%) | ||
| Evening | 8 (33.3%) | 8 (33.3%) | 8 (33.3%) | ||
| Rotating | 8 (28.6%) | 8 (28.6%) | 12 (42.9%) | ||
| Posting ward, n (%) | χ2=24.75 | 0.132 | |||
| Emergency | 19 (46.3%) | 12 (29.3%) | 10 (24.4%) | ||
| Surgical | 26 (53.1%) | 14 (28.6%) | 9 (18.4%) | ||
| Medical | 14 (22.2%) | 23 (36.5%) | 26 (41.3%) | ||
| OPD | 6 (27.3%) | 8 (36.4%) | 8 (36.4%) | ||
| ICU | 4 (22.2%) | 6 (33.3%) | 8 (44.4%) | ||
| PHC | 1 (33.3%) | 0 (0.0%) | 2 (66.7%) | ||
| Others | 2 (66.7%) | 0 (0.0%) | 1 (33.3%) | ||
| Pediatric | 3 (75.0%) | 0 (0.0%) | 1 (25.0%) | ||
| Obstetrics/Gynecology | 3 (37.5%) | 2 (25.0%) | 3 (37.5%) | ||
| Laboratory | 3 (60.0%) | 1 (20.0%) | 1 (20.0%) | ||
| Overall health*, n (%) | χ2=49.34 | 0.000 | |||
| ≤4 | 20 (80.0%) | 4 (16.0%) | 1 (4.0%) | ||
| 5−7 | 28 (65.1%) | 9 (20.9%) | 6 (14.0%) | ||
| 8−10 | 33 (22.3%) | 53 (35.8%) | 62 (41.9%) | ||
| Presence of a chronic condition**, n (%) | χ2=82.22 | 0.000 | |||
| Yes | 21 (25.0%) | 55 (65.5%) | 8 (9.5%) | ||
| No | 60 (45.5%) | 11 (8.3%) | 61 (46.2%) | ||
Abbreviations: CI, confidence interval; ICU, intensive care unit; OPD, outpatient department; PHC, primary healthcare. Notes: *Measured on a 0-10 rating scale (score of ≤4 indicates poor health; score between 5–7 indicates moderate health; score 8–10 indicates best health). **Conditions such as hypertension, diabetes, neurological, cardiovascular, and any other disease. † One-Way Analysis of Variance followed by post hoc Tukey honestly significant difference.
Table 3.
Ordinal logistic regression model for the association between the levels of resilience coping and socio-demographic and other characteristics.
Table 3.
Ordinal logistic regression model for the association between the levels of resilience coping and socio-demographic and other characteristics.
| Characteristics | Estimate | SE | Walds χ2 | p-value | 95% CI |
|---|---|---|---|---|---|
| Resilience coping level | |||||
| Low | 5.896 | 2.720 | 4.699 | 0.030 | 0.565 to 11.228 |
| Medium | 7.609 | 2.739 | 7.719 | 0.005 | 2.241 to 12.976 |
| High | 0a | – | – | – | – |
| Data mode | |||||
| Offline | 0.422 | 0.448 | 0.885 | 0.347 | -0.457 to 1.300 |
| Online | 0a | – | – | – | – |
| Age | 0.166 | 0.055 | 9.152 | 0.002 | 0.058 to 0.273 |
| Sex | |||||
| Male | -0.361 | 1.148 | 0.076 | 0.783 | -2.567 to 1.934 |
| Female | 0.062 | 1.126 | 0.003 | 0.956 | -2.145 to 2.268 |
| Prefer not to disclose | 0a | – | – | – | – |
| Marital status | |||||
| Single | 2.169 | 1.608 | 1.819 | 0.177 | -0.983 to 5.320 |
| Married | 1.891 | 1.558 | 1.474 | 0.225 | -1.161 to 4.994 |
| Divorced | 2.122 | 1.653 | 1.649 | 0.199 | -1.117 to 5.361 |
| Widow | 0a | – | – | – | – |
| Education | |||||
| Diploma in nursing | -1.425 | 0.826 | 2.972 | 0.085 | -3.044 to 0.195 |
| Graduate in nursing | -0.793 | 0.706 | 1.259 | 0.262 | -2.177 to 0.592 |
| Postgraduation in nursing | 0a | – | – | – | – |
| Nationality | |||||
| Saudi | -0.826 | 1.074 | 0.592 | 0.442 | -2.932 to 1.279 |
| Filipino | -0.692 | 0.934 | 0.549 | 0.459 | -2.522 to 1.138 |
| Indian | -0.460 | 0.817 | 0.317 | 0.574 | -2.061 to 1.141 |
| Other | 0a | – | – | – | – |
| Clinical experience | -0.072 | 0.055 | 2.495 | 0.114 | -0.162 to 0.017 |
| Work shift | |||||
| Morning | -0.749 | 0.466 | 2.586 | 0.108 | -1.661 to 0.164 |
| Afternoon | -0.840 | 0.612 | 1.884 | 0.170 | -2.039 to 0.359 |
| Evening | -0.707 | 0.646 | 1.197 | 0.274 | -1.973 to 0.559 |
| Rotating | 0a | – | – | – | – |
| Posting ward | |||||
| Medical | 2.159 | 1.423 | 2.300 | 0.129 | -0.631 to 4.949 |
| Surgical | 2.115 | 1.384 | 2.335 | 0.127 | -0.598 to 4.827 |
| Emergency | 2.477 | 1.334 | 3.449 | 0.063 | -0.137 to 5.091 |
| OPD | 2.755 | 1.398 | 3.885 | 0.049 | 0.016 to 5.494 |
| ICU | 2.980 | 1.394 | 4.573 | 0.032 | 0.249 to 5.712 |
| Laboratory | 3.486 | 1.798 | 3.761 | 0.052 | 0.037 to 7.010 |
| Obstetrics/Gynecology | 2.049 | 1.856 | 1.219 | 0.270 | -1.589 to 5.687 |
| Pediatric | 1.626 | 1.780 | 0.834 | 0.361 | -1.863 to 5.116 |
| PHC | 1.711 | 1.420 | 1.451 | 0.228 | -1.863 to 5.116 |
| Others | 0a | – | – | – | – |
| Overall health* | |||||
| ≤4 | -2.548 | 0.613 | 17.270 | 0.000 | -3.750 to -1.346 |
| 5−7 | -1.394 | .410 | 11.582 | 0.001 | -2.197 to -0.591 |
| 8−10 | 0a | – | – | – | – |
| Presence of a chronic condition** | |||||
| Yes | -0.099 | 0.415 | 0.057 | 0.811 | -0.914 to 0.715 |
| No | 0a | – | – | – | – |
Abbreviations: CI, confidence interval; ICU, intensive care unit; OPD, outpatient department; PHC, primary healthcare; SE, standard error. Notes: aThis parameter is set to zero because it is redundant. Nagelkerke R2=0.357; parallel-lines assumption verified (p=0.999). *Measured on a 0-10 rating scale (score of ≤4 indicates poor health; score between 5–7 indicates moderate health; score 8–10 indicates best health). **Conditions such as hypertension, diabetes, neurological, cardiovascular, and any other disease.
Table 4.
Psychometric properties of Brief Resilient Coping Scale items.
| S. No. | BRCS item | Mean (SD) | Item-Total Correlations | Cronbach’s alpha if item deleted |
|---|---|---|---|---|
| 1 | I look for creative ways to alter difficult situations | 3.64 (1.06) | 0.56 | 0.77 |
| 2 | Regardless of what happens to me, I believe I can control my reaction to it | 3.65 (1.16) | 0.59 | 0.76 |
| 3 | I believe I can grow in positive ways by dealing with difficult situations | 3.67 (1.17) | 0.56 | 0.77 |
| 4 | I actively look for ways to replace the losses I encounter in life | 3.62 (1.21) | 0.73 | 0.68 |
Abbreviations: BRCS, Brief Resilient Coping Scale; SD, standard deviation.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



