
Submitted:
23 August 2024
Posted:
26 August 2024
You are already at the latest version
Abstract
Both aging and chronic obstructive pulmonary disease (COPD) are strongly associated with changes in the metabolome; however, it is unknown whether there are common aging/COPD metabolomic signatures and if accelerated aging is associated with COPD. Plasma from 5,704 subjects from COPDGene and 2,449 subjects from SPIROMICS were profiled using the Metabolon global metabolomics platform (1,013 annotated metabolites). Post-bronchodilator spirometry measures of airflow obstruction (forced expiratory volume at one second (FEV1)/forced vital capacity (FVC) < 0.7) were used to define COPD. Elastic net regression was trained on never and former smokers with normal spirometry and no emphysema to create a metabolomic age score which was validated in SPIROMICS subjects. Our metabolic age score was strongly associated with chronic age in the validation cohort (correlation coefficient 0.8). COPD subjects with accelerated aging (> 7 years difference between metabolic and actual age) had more severe disease compared with those who had decelerated aging (< -7 years difference between metabolic and actual age). COPD and aging metabolites were shared more than expected (P < 0.001) with overrepresented included amino acid and glutathione metabolism pathways. These findings suggesting a common mechanism between aging and COPD and that COPD is associated with accelerated metabolic aging.
Keywords:
aging
; COPD
; metabolic age
1. Introduction
Persistent respiratory symptoms and airflow limitation due to chronic obstructive pulmonary disease (COPD) makes the disease a strong negative impactor of quality of life, as well as a leading cause of death and hospitalizations both worldwide and in the United States [1,2]. These symptoms are usually caused by repeated exposure to noxious particles or gases, including cigarette smoke, that damage the airways and lungs, ultimately resulting in airway and/or alveolar abnormalities [3]. COPD is also characterized by many comorbidities including muscle wasting, cardiovascular disease, osteoporosis, and depression [4]. This suggests that COPD is a generalized systemic disease not just limited to the lungs, and that there are subsequent downstream changes to molecular pathways, including disturbances to the metabolome. Many of these comorbidities are also associated with age; however, COPD patients often present with these comorbidities earlier than those at a similar age without COPD, indicating that COPD might be a disease of early aging [5]. In this study we examine the metabolomic signatures of COPD and aging to identify the shared and distinct pathologic signatures of each disease.
The aging metabolome is now well established and includes changes in energy metabolism (e.g., decreasing nicotinamide adenine dinucleotide (NAD+)), lipids (e.g., those carried by low-density lipoprotein (LDL) particles) such as ceramides and sphingomyelins), and amino acids [6]. For instance, in a large NMR study of 135 metabolites from 26,065 individuals of Northern European ancestry (Finns and Estonians), age-specific and sex-specific metabolic fingerprints were identified from the serum (Finns) or plasma (Estonians) with significant differences observed with age in males and females for lipoproteins, cholesterol, and triglyceride levels, whereas atherogenic metabolites and certain amino acids were only found to be increased in females during the time of menopausal transition [7]. In a different small untargeted LC-MS study of 126 plasma metabolites from 15 young and 15 elderly individuals there were 14 compounds associated with age [8]. The metabolites that declined with age included antioxidants and compounds associated with high physical activity (e.g., carnosine, UDP-acetyl-glucosamine, NAD+, and leucine), whereas metabolites that increased with age included those that were associated with a decline in renal and liver functions. In another more comprehensive LC-MS/MS study of 2,578 plasma metabolites from 150 healthy humans from age 30 to 100 years, there were age-related metabolites that were gender and non-gender specific including multiple lipid species that decreased with aging [9]. These studies illustrate some of the systemic age-related metabolic changes that are common across multiple different metabolomics platforms.
The relationship between individual metabolites and COPD has also been explored, particularly for spirometry tests of lung function. Specifically, three metrics obtained from these tests are typically used: forced expiratory volume in 1 second (FEV1), FEV1 percentage of predicted (FEV1%), and the FEV1/Forced Vital Capacity (FVC) ratio (FEV1 /FVC) (see review [10]). Multivariate models using more than one metabolite have also been used to predict COPD. Pinto-Plata et al. used machine learning methods to identify distinct plasma metabolomic profiles between survivors and non-survivors of COPD two years prior to their death [11]. These profiles were also characterized by differences in energy metabolism pathways. In Godbole et al 2022 [12], metabolomic scores with 132 and 129 metabolites were used to predict FEV1 and emphysema respectively. These models performed better than models with clinical covariates alone. COPD metabolites were enriched in arginine biosynthesis; aminoacyl-tRNA biosynthesis; and glycine, serine, and threonine metabolism. Others have created metabolomic scores to predict COPD acute exacerbations [13], as well as a number of other diseases including coronary heart disease [14,15], type 2 diabetes [16], incident heart failure [17], and pulmonary arterial hypertension [18]. Many of these scores were derived with regularized regression models, a family of statistical methods which avoid overfitting from datasets with many features by penalizing and constraining the coefficient estimates. Others used machine learning methods, such as Random Forest, which may be powerful but have the disadvantage of less interpretability. When creating scores to predict pulmonary arterial hypertension, Alotaibi et al found relatively similar metabolites identified across 6 methods including elastic net and several machine learning methods. Furthermore, they found that elastic net selected more metabolites that were not as highly inter-correlated compared to those that conventional linear regression or random forest identified, suggesting that elastic net may perform better in capturing metabolites from a variety of different pathways, while also being more efficient and interpretable [18].
Elastic net has also been used by others to create -omic age scores. This began with Horvath [19] and Hannum et al. [20] who both trained Elastic Net models on transcriptomic data to predict age, arriving at transcriptomic age scores. Horvath found accelerated age, or when the transcriptomic age score was greater than the chronological age, in cancer tissues. Hannum et al found that the rate of transcriptomic age was impacted by gender and genetic variants. Since then, many have created age scores using a variety of -omic markers and the concept has been named “biological” age. Many have also found that accelerated biological age is associated with a number of health outcomes. These studies have been reviewed in Rutledge et al. [21] and Li et al. [22]. Although elastic net has been used to create age and COPD metabolite scores, there have been no investigations into the overlap between the two.
This study investigates the overlap between the aging and COPD metabolome and address some of the limitations of previous studies by using two independent, well-phenotyped case-control populations with 8,153 subjects who have comprehensive plasma metabolomics profiling > 1,000 annotated metabolites. The study is the largest COPD metabolomics study to date. It also creates a normal lung function aging score as well as a COPD metabolome score and then contrasts the metabolites that make up aging scores with COPD scores to identify common and distinct aging and COPD metabolic features as well as identify COPD subjects who have accelerated aging.
2. Materials and Methods
Cohorts
The Genetic Epidemiology of COPD (COPDGene) (ClinicalTrials.gov Identifier: NCT00608764), is a NIH-sponsored multicenter cohort of never, former, and current smokers 45-80 years old. Written Informed consent was obtained from all subjects involved in the study. Details of the COPDGene study are provided elsewhere [23]. In brief, this study enrolled 10,198 non-Hispanic white and African American participants with at least 10 pack-years of smoking, and 465 individuals with no smoking history. Metabolomic profiling was performed on 5,704 participants from the second visit of the study.
The Subpopulations and Intermediate Outcome Measures in COPD Study (SPIROMICS) (ClinicalTrials.gov Identifier: NCT01969344) is a NIH-sponsored multicenter cohort of never, former, and current smokers 40-80 years old. Written Informed consent was obtained from all subjects involved in the study. Details of the cohort are provided elsewhere [24]. In brief, this study recruited 2,771 participants with at least 20 pack-years of smoking and 202 participants who were never smokers. 73% of participants self-identified as non-Hispanic white. 2,449 had plasma available for metabolomic profiling of baseline fasting blood samples. Metabolomic profiling as performed on the baseline blood draw of the study.
Clinical Data and Definitions
COPD was defined using post-bronchodilator FEV1/FVC with a case defined as FEV1/FVC < 0.7. Emphysema was quantitated by CT scan at total lung capacity using low attenuation area (LAA) voxels < -950 Hounsfield units. GOLD 0 grade (FEV1>= 80% & FEV1/FVC >= 0.7), no emphysema by LAA < 5%, and never smoking or former smokers who stopped smoking at least 5 years ago were used to define control subjects. A never smoker was defined as someone who smoked < 100 lifetime cigarettes. A former smoker was defined as someone who had quit smoking and not smoked a cigarette in the past 30 days.
Metabolomic Profiling and Processing
Plasma samples from both cohorts were profiled using Metabolon (Durham, NC, USA) Global Metabolomics Platform, as described previously, although profiling for each cohort occurred approximately 6 months apart [12]. Metabolite values were batch normalized, within each study, by dividing by the median metabolite value for each metabolite within a batch. After batch normalization, metabolite principal components showed a significant reduction in association with batch, so no further normalization was needed[25]. For this analysis, metabolites were excluded if missing in >20% of subjects and we only examined metabolites that had the same missing pattern in both studies (e.g., mediations and nicotine metabolites). This resulted in 831 metabolites of the 1,314 metabolites identified in both studies. The missing values of these 831 metabolites were then imputed with k- nearest neighbor imputation (kNN; k = 10) using the R package ‘impute’, and then log2-transformed for all analyses. The other metabolites that were excluded from analysis had discrepant missing patterns: 122 metabolites had <20% missing samples in one study and 20–80% missing in the other, and 361 metabolites had at least one cohort with ≥80% missing samples.
Software, Statistical and Bioinformatics Analysis
The statistical software R Version 4.0.2 was used for all analyses. The R package glmnet was used for ElasticNet, stats for over-representation analysis and univariate linear models, and table1 for creating characteristic tables. The coefficients from ElasticNet are used as weights to develop a final score and are interpretable in terms of the linear relationship between the metabolite and the outcome. For the aging score, the elastic net model was trained on COPDGene never and former smokers (subjects who quit at least 5 years ago, had less than 5% emphysema, and normal spirometry). We then tested the score on SPIROMICS subjects meeting the same criteria. The final score was then applied to other independent former and current smokers in each of the cohorts, looking separately at those without obstruction (GOLD 0) and with less than 5% emphysema compared (described as current/former smokers without COPD and emphysema) to those who do not meet those criteria (described as current/former smokers with COPD or emphysema). For the lung obstruction score, all COPDGene metabolite data were used to train an elastic net model predicting continuous FEV1/FVC. It was then tested on all SPIROMICS data. For both scores, 10-fold cross validation was performed in the training data set to obtain the penalty parameter (λ), which corresponded to the largest lambda that minimizes MSE plus one standard error. This was iterated across alpha values of 0 to 1 at a 0.05 interval to identify the alpha that produced the best performing model. The metabolite score models did not include clinical covariates. Predictions were created with the metabolite coefficients and the set of metabolites selected by the ElasticNet procedure.
To assess the difference between metabolomic age and actual age, a spline was fitted between ageactual and agemetabolomic using the smooth.spline function from the stats R package. The age difference is then calculated by agemetabolomic – agespline. To compare the subjects on the tail ends of age difference while maintaining sufficient sample size, we used a cutoff of 7 years in former and current smokers with COPD or emphysema to select about 10% of the subjects who were most accelerated or decelerated metabolic age. Specifically, subjects with accelerated age were defined as agemetabolomic – agespline > 7 years and those having decelerated age as agemetabolomic – agespline < -7 years. We examined differences in the demographic and clinical characteristics between these two groups, using a t-test for continuous variables and a Chi-squared test for categorical/binary variables. This was repeated separately in current smokers without COPD and emphysema. A chi-squared test was used to test the probability that the overlap in metabolites happened by chance.
Pathway Analysis
Pathway analysis was conducted by a Fisher’s test to determine over-representation of sub- and super-pathways based on metabolites of interest. The sub- and super-pathways used were annotated and provided by Metabolon (Durham, NC, USA). 129 of the 831 metabolites used In our analysis have not been annotated yet. The Fisher’s test p-values were also adjusted using the Benjamini-Hochberg procedure to account for multiple-testing [26].
Univariate Associations
To identify metabolites associated with age and FEV1/FVC, simple univariate linear models without any other covariates were conducted with each phenotype. For association with FEV1/FVC, all subjects were used for analysis. The analysis with age was repeated separately in never/former smokers without emphysema or COPD and in current/former smokers with COPD or emphysema.
3. Results
Demographic Characteristics
Demographics and clinical characteristics for the COPDGene never/former smoker without COPD or emphysema training, SPIROMICS never/former smoker without COPD or emphysema testing, and COPDGene and SPIROMICS other former and current smoker application groups are presented in Table 1. In general, the current smokers without COPD or emphysema were slightly younger, more likely to be women and African American, and less likely to have coronary artery disease (p < 0.001).

Table 1.
Characteristics of COPDGene and SPIROMICS subjects.
| never/former smokers without COPD or emphysema | current smokers without COPD or emphysema | former/current smokers with COPD or emphysema | ||||||
| COPDGene (N=1,346) |
SPIROMICS (N=413) |
COPDGene (N=818) |
SPIROMICS (N=323) |
COPDGene (N=3,540) |
SPIROMICS (N=1,681) | P-value | ||
| Age (years), mean (SD) | 65.4 (9.25) | 62.9 (9.51) | 59.1 (6.33) | 55.2 (8.82) | 66.2 (8.56) | 65.0 (8.05) | < 0.001 | |
| Race White/Black/Other % | 87.4/12.6/0 | 81.8/12.3/5.9 | 42.7/57.3/0 | 55.7/38.7/5.6 | 71.3/28.7/0 | 80.5/15.2/4.3 | < 0.001 | |
| Gender, Male, n (%) | 582 (43.2%) | 181 (43.8%) | 387 (47.3%) | 154 (47.7%) | 1888 (53.3%) | 945 (56.2%) | < 0.001 | |
| Smoking Status Never/Former/Current % | 29.3/70.7/0 | 40/60/0 | 0/0/100 | 0/0/100 | 0/65.2/34.8 | 0/67.3/32.7 | NA | |
| Num. recent exacerbations | 0 (0, 1.00) | 0 (0, 1.00) | 0 (0, 1.00) | 0 (0, 2.00) | 0 (0, 2.00) | 0 (0, 2.00) | < 0.001 | |
| GOLD stage, n (%) | NA | |||||||
| GOLD 0 | 951 (70.7%) | 248 (60.0%) | 818 (100%) | 323 (100%) | 514 (14.5%) | 130 (7.7%) | ||
| GOLD 1 | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 507 (14.3%) | 334 (19.9%) | ||
| GOLD 2 | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 1063 (30.0%) | 667 (39.7%) | ||
| GOLD 3 | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 565 (16.0%) | 347 (20.6%) | ||
| GOLD 4 | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 235 (6.6%) | 142 (8.4%) | ||
| PRISm | 12 (0.9%) | 0 (0%) | 0 (0%) | 0 (0%) | 656 (18.5%) | 61 (3.6%) | ||
| Never smoker | 383 (28.5%) | 165 (40.0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | ||
| FEV1 (Liters) | 2.71 (0.700) | 2.85 (0.697) | 2.69 (0.671) | 2.89 (0.704) | 1.86 (0.792) | 1.86 (0.823) | NA | |
| Emphysema% | 1.59 (1.85) | 1.64 (1.39) | 0.883 (1.06) | 0.997 (0.903) | 8.01 (10.6) | 10.4 (11.2) | NA | |
| FVC (Liters) | 3.45 (0.876) | 3.62 (0.882) | 3.45 (0.884) | 3.71 (0.908) | 2.98 (0.967) | 3.38 (1.06) | NA | |
| FEV1/FVC | 0.787 (0.0493) | 0.788 (0.0505) | 0.784 (0.0487) | 0.782 (0.0487) | 0.616 (0.151) | 0.542 (0.147) | NA | |
| History of diabetes, n (%) | 169 (12.6%) | 54 (13.1%) | 125 (15.3%) | 25 (7.7%) | 670 (18.9%) | 231 (13.7%) | < 0.001 | |
| History of stroke, n (%) | 20 (1.5%) | 14 (3.4%) | 28 (3.4%) | 10 (3.1%) | 130 (3.7%) | 66 (3.9%) | 0.00323 | |
| History of heart attack, n (%) | 56 (4.2%) | 17 (4.1%) | 32 (3.9%) | 5 (1.5%) | 244 (6.9%) | 123 (7.3%) | < 0.001 | |
| History of coronary artery disease, n (%) | 86 (6.4%) | 24 (5.8%) | 32 (3.9%) | 7 (2.2%) | 346 (9.8%) | 172 (10.2%) | < 0.001 | |
| Chronic Bronchitis, n (%) | 46 (3.4%) | 30 (7.3%) | 116 (14.2%) | 74 (22.9%) | 643 (18.2%) | 367 (21.8%) | < 0.001 | |
| Exacerbations included those treated with antibiotics and/or corticosteroids in the 12 months prior to the visit; shown are n (percentage), mean (standard deviation), or median (5th, 95th percentiles); spirometry volumes are in post-bronchodilator therapy and in liters; GOLD 0 (FEV1 >= 80% & FEV1/FVC >= 0.7) | GOLD 1 (FEV1 >= 80% & FEV1 /FVC < 0.7) | GOLD 2 (50% <= FEV1 < 80% & FEV1 /FVC < 0.7) | GOLD 3 (30% <= FEV1 < 50% & FEV1/FVC < 0.7) | GOLD 4 (FEV1 < 30% & FEV1 /FVC < 0.7) | PRISm (Preserved Ratio, Impaired Spirometry) (FEV1/FVC >= 0.7 but FEV1 < 80%); history of diabetes, stroke, heart attack, and coronary artery disease based on subject self-report; chronic Bronchitis defined by answers to questions about both cough and phlegm. | ||||||||
Metabolomic Age Score
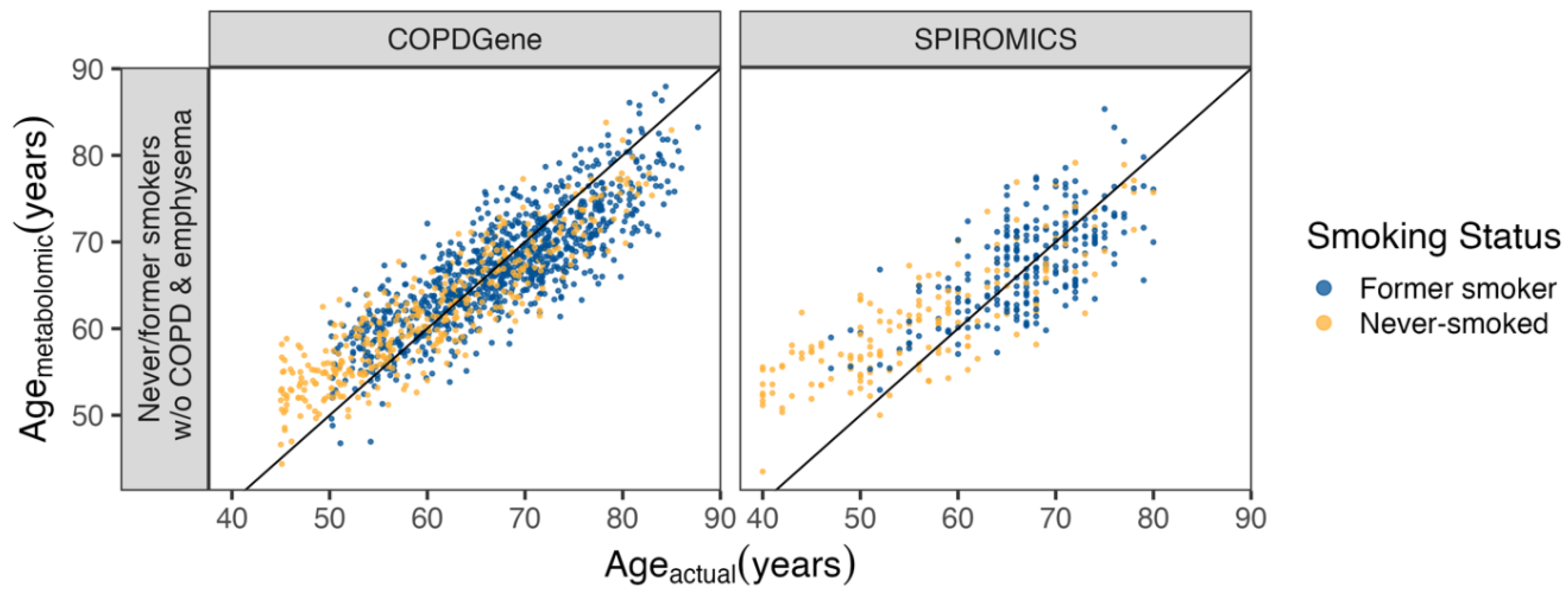
Elastic net (alpha 0.05) selected 378 metabolites for the age model. When testing this model using independent never and former smoker control subjects without COPD or emphysema, the predicted-actual age correlations were 0.875 in COPDGene and 0.806 in SPIROMICS (Figure 1). Leucine, Isoleucine and Valine Metabolism was the most overrepresented sub-pathway and Amino acids were the most overrepresented super-pathway (Supplemental table 1B&C).
Figure 1.
Metabolite age score. The age model was trained on COPDGene never (yellow) and former (blue) smokers without COPD and emphysema (left panel) and tested on SPIROMICS never and former smokers without COPD and emphysema (right panel). The subjects’ actual ages are on the x-axis and predicted metabolomic age on the y-axis.
Figure 1.
Metabolite age score. The age model was trained on COPDGene never (yellow) and former (blue) smokers without COPD and emphysema (left panel) and tested on SPIROMICS never and former smokers without COPD and emphysema (right panel). The subjects’ actual ages are on the x-axis and predicted metabolomic age on the y-axis.
Differences between COPD Subjects with Accelerated and Decelerated Metabolomic Age
To evaluate whether metabolic age difference was associated with COPD, a spline was fit between actual and metabolomic age (Figure 2). Current and former smokers with COPD or emphysema with accelerated age (agemetabolomic – agespline > 7) were compared to those with decelerated age (agemetabolomic – agespline < -7) (Table 2). Using a spline allowed us to compare subjects on each tail end of the age difference within the same age group more equivalently, particularly in younger subjects where the sample size was smaller. Agespline did not differ greatly from Ageactual, with a mean difference of 0.5462 years and 25th and 75th percentiles of -1.6768 and 2.6501 years respectively. Those with accelerated metabolic age were more likely to be white (p < 0.001), female (p < 0.001), former smokers (p < 0.001), have more severe COPD by GOLD grade (p < 0.001), worse spirometry and more emphysema (p < 0.001), and to have higher rates of diabetes and cardiological comorbidities. The same comparison in current smokers without COPD or emphysema (Supplement table 2 and Supplement figure 1) showed that subjects without COPD or emphysema with accelerated metabolic age were also more likely to be white and female. They also were more likely to have had a stroke and chronic bronchitis, as well as greater rates of other comorbidities that did not reach statistical significance.
Figure 2.
Age acceleration in former (triangle) and current (circle) smokers with COPD or emphysema. A spline was fitted between ageactual and agemetabolomic (black line). Age difference is calculated by agemetabolomic – agespline, with subjects having accelerated metabolomic age (red) having a difference greater than 7 years and those having decelerated age (blue) having a difference less than -7 years.
Figure 2.
Age acceleration in former (triangle) and current (circle) smokers with COPD or emphysema. A spline was fitted between ageactual and agemetabolomic (black line). Age difference is calculated by agemetabolomic – agespline, with subjects having accelerated metabolomic age (red) having a difference greater than 7 years and those having decelerated age (blue) having a difference less than -7 years.
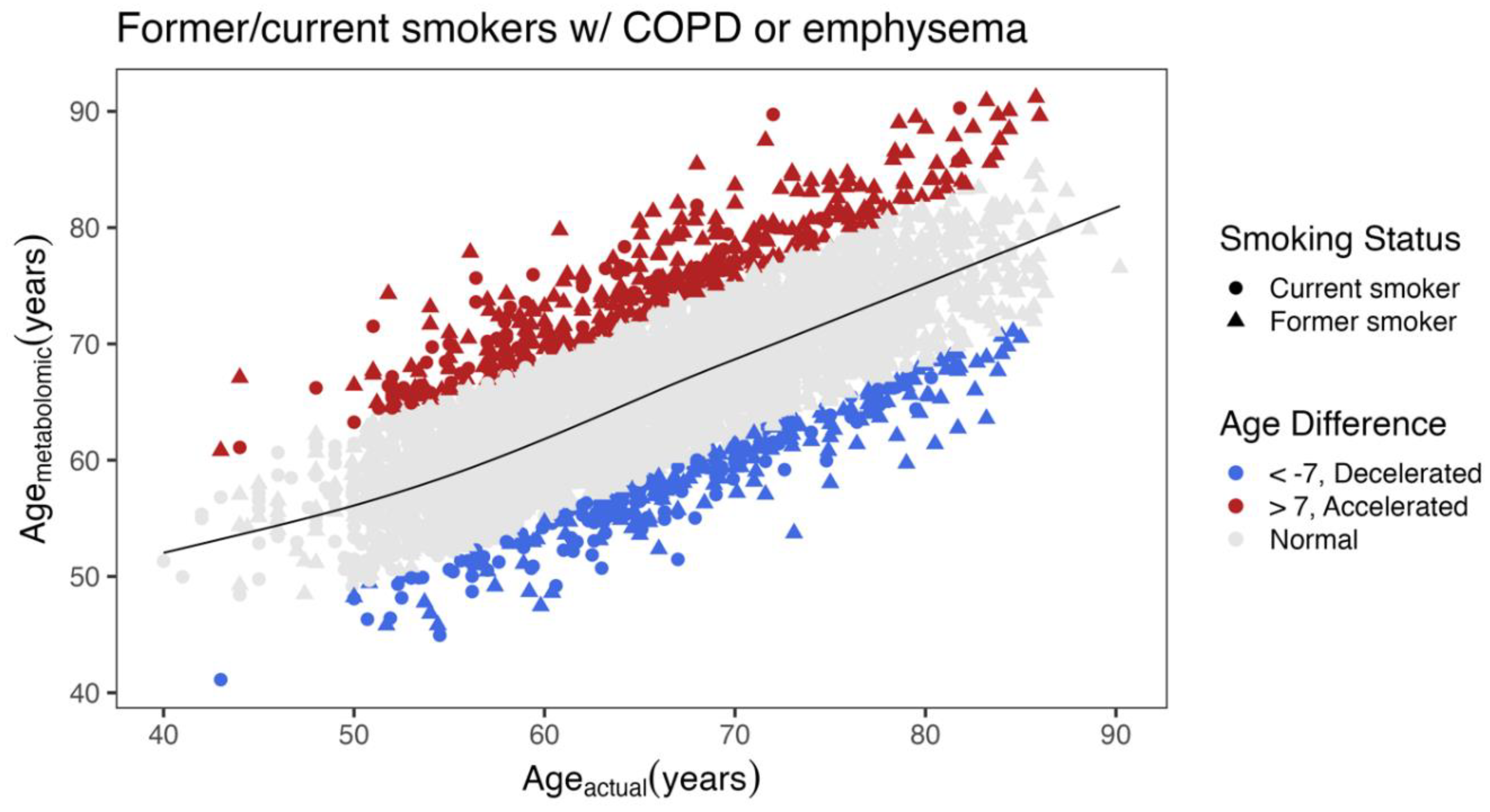
Table 2.
Accelerated age (agemetabolomic – agespline > 7) vs. decelerated age (agemetabolomic – agespline < -7) in current and former smokers with COPD or emphysema.
Table 2.
Accelerated age (agemetabolomic – agespline > 7) vs. decelerated age (agemetabolomic – agespline < -7) in current and former smokers with COPD or emphysema.
| Decelerated (N=277) |
Accelerated (N=400) |
P-value | |||
| Age (years), mean (SD) | 67.9 (8.32) | 65.3 (8.56) | < 0.001 | ||
| Metabolomic age (years) | 58.3 (5.79) | 75.2 (6.18) | NA | ||
| Race White/Black/Other % | 45.1/53.4/1.5 | 88.3/10.5/1.4 | < 0.001 | ||
| Gender, Male, n (%) | 197 (71.1%) | 172 (43.0%) | < 0.001 | ||
| Smoking Status Former/Current % | 57.8/42.2 | 75.0/25.0 | < 0.001 | ||
| Exacerbations | 0 (0, 2.00) | 0 (0, 2.00) | 0.0178 | ||
| GOLD stage, n (%) | |||||
| GOLD 0 | 38 (13.7%) | 27 (6.8%) | < 0.001 | ||
| GOLD 1 | 65 (23.5%) | 45 (11.3%) | |||
| GOLD 2 | 90 (32.5%) | 131 (32.8%) | |||
| GOLD 3 | 41 (14.8%) | 93 (23.3%) | |||
| GOLD 4 | 10 (3.6%) | 50 (12.5%) | |||
| PRISm | 33 (11.9%) | 54 (13.5%) | |||
| FEV1 (liters) | 2.00 (0.801) | 1.60 (0.724) | < 0.001 | ||
| Emphysema% | 7.16 (9.45) | 10.8 (12.4) | < 0.001 | ||
| FVC | 3.21 (0.967) | 2.87 (0.938) | < 0.001 | ||
| FEV1/FVC | 0.613 (0.136) | 0.554 (0.160) | < 0.001 | ||
| History of diabetes, n (%) | 43 (15.5%) | 96 (24.0%) | 0.00879 | ||
| History of stroke, n (%) | 12 (4.3%) | 29 (7.3%) | 0.157 | ||
| History of heart attack, n (%) | 7 (2.5%) | 59 (14.8%) | < 0.001 | ||
| History of coronary artery disease, n (%) | 11 (4.0%) | 79 (19.8%) | < 0.001 | ||
| Chronic Bronchitis, n (%) | 52 (18.8%) | 87 (21.8%) | 0.396 | ||
| Exacerbations included those treated with antibiotics and/or corticosteroids in the 12 months prior to the visit; shown are n (percentage), mean (standard deviation), or median (5th, 95th percentiles); spirometry volumes are in post-bronchodilator therapy and in liters; GOLD 0 (FEV1 >= 80% & FEV1/FVC >= 0.7) | GOLD 1 (FEV1 >= 80% & FEV1 /FVC < 0.7) | GOLD 2 (50% <= FEV1 < 80% & FEV1 /FVC < 0.7) | GOLD 3 (30% <= FEV1 < 50% & FEV1/FVC < 0.7) | GOLD 4 (FEV1 < 30% & FEV1 /FVC < 0.7) | PRISm (Preserved Ratio, Impaired Spirometry) (FEV1/FVC >= 0.7 but FEV1 < 80%); history of diabetes, stroke, heart attack, and coronary artery disease based on subject self-report; chronic Bronchitis defined by answers to questions about both cough and phlegm. | |||||
A metabolomic Lung Obstruction Score
We next evaluated metabolites associated with obstruction on spirometry. 461 metabolites were selected by elastic net with an alpha of 0.1 for the lung obstruction metabolomic score model. Correlations between actual and metabolome predicted FEV1/FVC were 0.705 in COPDGene training and 0.651 in SPIROMICS testing (Figure 3).
Overlap between the Age and COPD Metabolome Scores
Between the elastic net models of age and lung obstruction, there was a higher than expected by chance overlap in the metabolites selected (Figure 4; P < 0.001). Amino acids were overrepresented in both the lung obstruction and age models although from different sets of amino acids (Supplement table 1C&E). For example, metabolites in the FEV1/FVC model, but not in an aging model included dimethylarginine, and specific sphingolipids and ceramides. Metabolites in both models included creatinine, urea, cortisol.
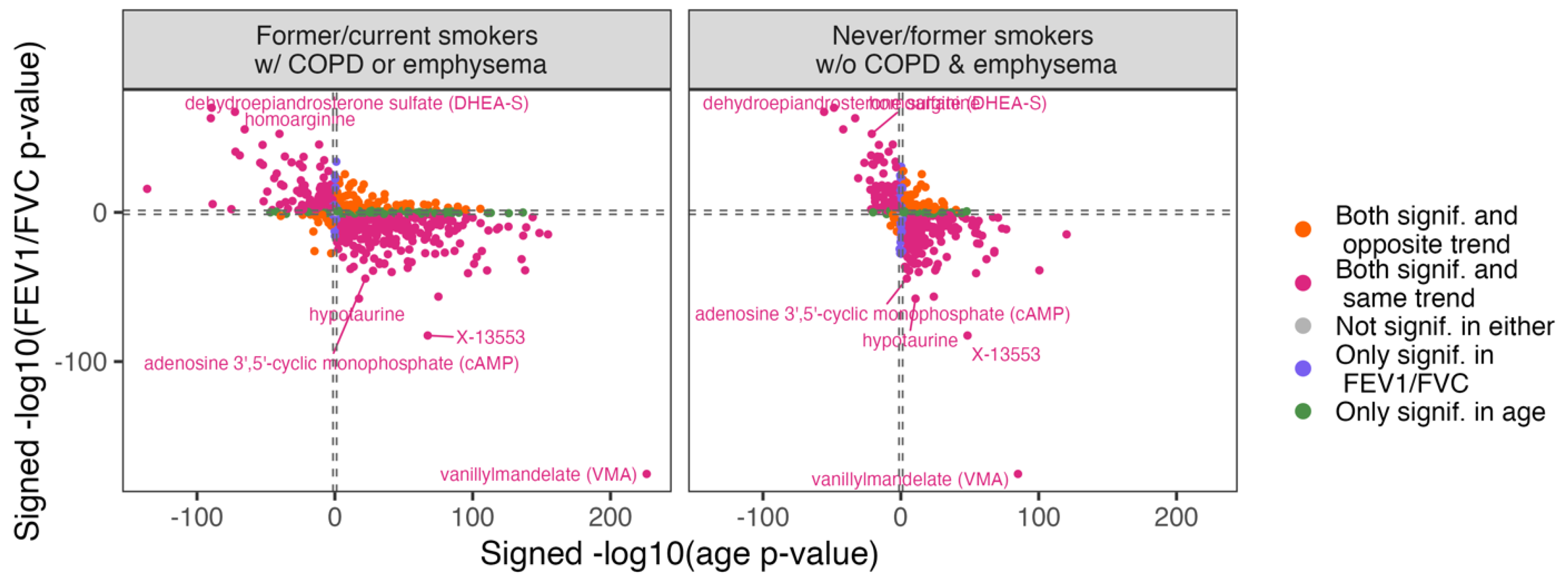
Overlap between Metabolite Univariate Associations with Age and COPD
In general, most metabolites univariately associated with age were also associated with lung obstruction with similar trend and p-value (Figure 5, Supplemental Table 1F). Examples of the metabolites that were higher with age and obstruction are vanillylmandelate, hydroxyasparagine, and arabonate/xylonate. Others such as androstenodiol and homoarginine were lower with age and amount of obstruction. These metabolites that were significant and concordant in both age and COPD were highly enriched in the Androgenic Steroids sub-pathway and in the nucleotide super-pathway (Supplemental Table 1G&H). Only a few significant metabolites were significant for only age or COPD or were discordant with age and obstruction severity. Those significant for only age include 3-methylglutaconate, N,N-dimethyl-pro-pro, dimethylarginine, and urea. Those only significantly associated with FEV1/FVC include valine and methyl-4-hydroxybenzoate sulfate. The metabolites 2-O-methylascorbic acid, myo-inositol, choline, tetrahydrocortisol glucuronide were among those that were significantly associated with both age and FEV1/FVC but with trends in discordant directions. These discordant metabolites were enriched in several sub-pathways including the Urea cycle; Arginine and Proline Metabolism (p-value = 0.002) and corticosteroids (p-value = 0.014), although these were no longer significant following multiple-testing corrections (Supplemental Table 1I).
4. Discussion
COPD is a disease that occurs primarily in older persons. While COPD has been postulated to be a disease of accelerate lung aging for some time (PMID: 19136405), this is the first study to show that many of the metabolic signatures of COPD and age overlap and that accelerated aging is associated with worse COPD. Although aging is a complex multisystem process, López-Otín et al. described aging in reference to multiple hallmarks of aging. These hallmarks include: genomic instability, telomere attrition, epigenetic alterations, loss of proteostasis, deregulated nutrient sensing, mitochondrial dysfunction, cellular senescence, stem cell exhaustion, and altered intercellular communication [27,28]. Some of these features have been described in COPD. For instance, other biomarkers of aging such as teleomere shortening {[29] and oxidative damage to DNA [30,31], and mTOR pathway [32,33] are associated with both aging and COPD or emphysema. In this study we also find evidence for shared pathology with deregulated nutrient signaling with many amino acids and carnitines associated with both age and COPD. We also find evidence for altered intercellular signaling as with androstenodiol and sphingolipids. The strongest positive association between age and COPD was VMA, which is a metabolite of catecholamines and may reflect elevated physiologic or psychologic stress [34].
Dimethylarginine (DMA) was one of 231 metabolites selected in the lung obstruction score but not in the age score. DMA is a product of methylated arginine residue protein degradation and may play a role in inflammation through inhibition of nitric oxide synthases [35]. We have previously reported an association with DMA and COPD in Godbole et al. 2022, as well as with the arginine pathway. As we noted in Godbole et al. 2022, several small studies and mouse models have also identified this relationship [35,36,37,38,39]. Other strong markers for both age and COPD were anabolic steroids such as androstenodiol, albeit in an opposite direction where lower levels were associated with more severe COPD and older age. Lower levels of these hormones may explain with both older age and COPD are associated with lower muscle mass.
We identified several metabolites that had significant univariate associations only with COPD, or metabolites that were significantly associated with both age and COPD but in discordant directions. These findings point to some biological processes unique to COPD separate from healthy aging. Those only significantly associated with FEV1/FVC include valine and methyl-4-hydroxybenzoate sulfate. Valine, involved in BCAA degradation, has previously been found to distinguish between patients with advanced COPD (GOLD grade 4) from healthy controls and is associated with increased systemic inflammation [40]. The discordant metabolites included 2-O-methylascorbic acid, myo-inositol, choline, tetrahydrocortisol glucuronide and represented the urea cycle; Arginine and Proline Metabolism and corticosteroids sub-pathways.
A major limitation of this study is that it is observational, and thus is not clear whether any of these pathways can be modified to prevent COPD progression. For instance, there have been mixed results with androgenic steroids to treat COPD and mTOR targeted interventions have not been successful for COPD. While diminished energy metabolism as evidence by amino acids and carnitine pathways, this may be secondary to the general inactivity of COPD patients, possibly from ventilatory limitation which prevents normal energy use. It would be useful to see if these biomarkers improve after COPD patients undergo a combine physical and nutritional rehabilitation. We did not use any clinical or demographic covariates in our analyses, which could potentially change the performance of the age and obstruction scores and change the results of the univariate associations. However, our univariate associations can provide a sense of metabolomic correlations with lung obstruction and age without the effect of covariates. We also did not adjust for lifestyle factors including diet, exercise, or medications, which also could have strong effects on the metabolome. Both our age and lung obstruction scores had poorer performance at the lower range of each outcome. This is likely due to smaller sample sizes of younger subjects and subjects with strong lung obstruction and would likely improve with greater sample sizes.
5. Conclusions
This study provides strong molecular evidence for shared pathophysiology of aging in COPD including diminished nutritional functioning (amino acids, carnitine), impaired androgenic signaling, and increased stress and inflammation (VMA, sphingolipids, DMA). People who have accelerated metabolic aging also have more severe COPD, thus any interventions that reduce aging, might also diminish COPD progression.
Funding
The Joe W. and Dorothy Dorsett Brown Foundation NIH X01 HL153656 DLD: NIH P01 HL 114501, R01 HG011393, K24HL171900 SPIROMICS: The authors thank the SPIROMICS participants and participating physicians, investigators, study coordinators, and staff for making this research possible. More information about the study and how to access SPIROMICS data is available at www.spiromics.org. The authors would like to acknowledge the University of North Carolina at Chapel Hill BioSpecimen Processing Facility (http://bsp.web.unc.edu/) and Alexis Lab (https://www.med.unc.edu/cemalb/facultyresearch/alexislab/) for sample processing, storage, and sample disbursements.We would like to acknowledge the following current and former investigators of the SPIROMICS sites and reading centers: Neil E Alexis, MD; Wayne H Anderson, PhD; Mehrdad Arjomandi, MD; Igor Barjaktarevic, MD, PhD; R Graham Barr, MD, DrPH; Patricia Basta, PhD; Lori A Bateman, MS; Christina Bellinger, MD; Surya P Bhatt, MD; Eugene R Bleecker, MD; Richard C Boucher, MD; Russell P Bowler, MD, PhD; Russell G Buhr, MD, PhD; Stephanie A Christenson, MD; Alejandro P Comellas, MD; Christopher B Cooper, MD, PhD; David J Couper, PhD; Gerard J Criner, MD; Ronald G Crystal, MD; Jeffrey L Curtis, MD; Claire M Doerschuk, MD; Mark T Dransfield, MD; M Bradley Drummond, MD; Christine M Freeman, PhD; Craig Galban, PhD; Katherine Gershner, DO; MeiLan K Han, MD, MS; Nadia N Hansel, MD, MPH; Annette T Hastie, PhD; Eric A Hoffman, PhD; Yvonne J Huang, MD; Robert J Kaner, MD; Richard E Kanner, MD; Mehmet Kesimer, PhD; Eric C Kleerup, MD; Jerry A Krishnan, MD, PhD; Wassim W Labaki, MD; Lisa M LaVange, PhD; Stephen C Lazarus, MD; Fernando J Martinez, MD, MS; Merry-Lynn McDonald, PhD; Deborah A Meyers, PhD; Wendy C Moore, MD; John D Newell Jr, MD; Elizabeth C Oelsner, MD, MPH; Jill Ohar, MD; Wanda K O’Neal, PhD; Victor E Ortega, MD, PhD; Robert Paine, III, MD; Laura Paulin, MD, MHS; Stephen P Peters, MD, PhD; Cheryl Pirozzi, MD; Nirupama Putcha, MD, MHS; Sanjeev Raman, MBBS, MD; Stephen I Rennard, MD; Donald P Tashkin, MD; J Michael Wells, MD; Robert A Wise, MD; and Prescott G Woodruff, MD, MPH. The project officers from the Lung Division of the National Heart, Lung, and Blood Institute were Lisa Postow, PhD, and Lisa Viviano, BSN; SPIROMICS was supported by contracts from the NIH/NHLBI (HHSN268200900013C, HHSN268200900014C, HHSN268200900015C, HHSN268200900016C, HHSN268200900017C, HHSN268200900018C, HHSN268200900019C, HHSN268200900020C), grants from the NIH/NHLBI (U01 HL137880, U24 HL141762, R01 HL182622, and R01 HL144718), and supplemented by contributions made through the Foundation for the NIH and the COPD Foundation from Amgen; AstraZeneca/MedImmune; Bayer; Bellerophon Therapeutics; Boehringer-Ingelheim Pharmaceuticals, Inc.; Chiesi Farmaceutici S.p.A.; Forest Research Institute, Inc.; Genentech; GlaxoSmithKline; Grifols Therapeutics, Inc.; Ikaria, Inc.; MGC Diagnostics; Novartis Pharmaceuticals Corporation; Nycomed GmbH; Polarean; ProterixBio; Regeneron Pharmaceuticals, Inc.; Sanofi; Sunovion; Takeda Pharmaceutical Company; and Theravance Biopharma and Mylan/Viatris. COPDGene: This work was supported by NHLBI grants U01 HL089897 and U01 HL089856 and by NIH contract 75N92023D00011. The COPDGene study (NCT00608764) has also been supported by the COPD Foundation through contributions made to an Industry Advisory Committee that has included AstraZeneca, Bayer Pharmaceuticals, Boehringer-Ingelheim, Genentech, GlaxoSmithKline, Novartis, Pfizer, and Sunovion.
Institutional Review Board Statement
This study was reviewed by the Institutional Review Board Statement at National Jewish Health (HS-1883a). The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Clinical and metabolomic data are available through dgGaP (TOPMed) for both COPDGene (phs000179) and SPIROMICS (phs001119)
Acknowledgments
We thank Amy Petriella for assistance in preparing the manuscript for submission.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Zamzam, M.A.; Azab, N.Y.; El Wahsh, R.A.; Ragab, A.Z.; Allam, E.M. Quality of life in COPD patients. Egyptian Journal of Chest Diseases and Tuberculosis. 2012, 61, 281–289. [Google Scholar] [CrossRef]
- Syamlal, G.; Kurth, L.M.; Dodd, K.E.; Blackley, D.J.; Hall, N.B.; Mazurek, J.M. Chronic Obstructive Pulmonary Disease Mortality by Industry and Occupation - United States, 2020. MMWR Morb Mortal Wkly Rep. 2022, 71, 1550–1554. [Google Scholar] [CrossRef]
- Agusti, A.; Celli, B.R.; Criner, G.J.; et al. Global Initiative for Chronic Obstructive Lung Disease 2023 Report: GOLD Executive Summary. Am J Respir Crit Care Med. 2023, 207, 819–837. [Google Scholar] [CrossRef] [PubMed]
- Agusti, A.; Soriano, J.B. COPD as a systemic disease. COPD. 2008, 5, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Divo, M.J.; Celli, B.R.; Poblador-Plou, B.; et al. Chronic Obstructive Pulmonary Disease (COPD) as a disease of early aging: Evidence from the EpiChron Cohort. PLoS One. 2018, 13, e0193143. [Google Scholar] [CrossRef] [PubMed]
- Adav, S.S.; Wang, Y. Metabolomics Signatures of Aging: Recent Advances. Aging Dis. 2021, 12, 646–661. [Google Scholar] [CrossRef] [PubMed]
- Auro, K.; Joensuu, A.; Fischer, K.; et al. A metabolic view on menopause and ageing. Nat Commun. 2014, 5, 4708. [Google Scholar] [CrossRef]
- Chaleckis, R.; Murakami, I.; Takada, J.; Kondoh, H.; Yanagida, M. Individual variability in human blood metabolites identifies age-related differences. Proc Natl Acad Sci U S A. 2016, 113, 4252–4259. [Google Scholar] [CrossRef]
- Jove, M.; Mate, I.; Naudi, A.; et al. Human Aging Is a Metabolome-related Matter of Gender. J Gerontol A Biol Sci Med Sci. 2016, 71, 578–585. [Google Scholar] [CrossRef]
- Godbole, S.; Bowler, R.P. Metabolome Features of COPD: A Scoping Review. Metabolites. 2022, 12. [Google Scholar] [CrossRef]
- Pinto-Plata, V.; Casanova, C.; Divo, M.; et al. Plasma metabolomics and clinical predictors of survival differences in COPD patients. Respir Res. 2019, 20, 219. [Google Scholar] [CrossRef] [PubMed]
- Godbole, S.; Labaki, W.W.; Pratte, K.A.; et al. A Metabolomic Severity Score for Airflow Obstruction and Emphysema. Metabolites. 2022, 12. [Google Scholar] [CrossRef] [PubMed]
- Peng, L.; You, H.; Xu, M.Y.; et al. A Novel Metabolic Score for Predicting the Acute Exacerbation in Patients with Chronic Obstructive Pulmonary Disease. Int J Chron Obstruct Pulmon Dis. 2023, 18, 785–795. [Google Scholar] [CrossRef] [PubMed]
- Vaarhorst, A.A.; Verhoeven, A.; Weller, C.M.; et al. A metabolomic profile is associated with the risk of incident coronary heart disease. Am Heart J. 2014, 168, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Zhu, C.; Nambi, V.; et al. Metabolomic Pattern Predicts Incident Coronary Heart Disease. Arterioscler Thromb Vasc Biol. 2019, 39, 1475–1482. [Google Scholar] [CrossRef]
- Floegel, A.; Stefan, N.; Yu, Z.; et al. Identification of serum metabolites associated with risk of type 2 diabetes using a targeted metabolomic approach. Diabetes. 2013, 62, 639–648. [Google Scholar] [CrossRef]
- Oexner, R.R.; Ahn, H.; Theofilatos, K.; et al. Serum metabolomics improves risk stratification for incident heart failure. Eur J Heart Fail. 2024, 26, 829–840. [Google Scholar] [CrossRef]
- Alotaibi, M.; Liu, Y.; Magalang, G.A.; et al. Deriving Convergent and Divergent Metabolomic Correlates of Pulmonary Arterial Hypertension. Metabolites. 2023, 13. [Google Scholar] [CrossRef]
- Horvath, S. DNA methylation age of human tissues and cell types. Genome Biol. 2013, 14, R115. [Google Scholar] [CrossRef]
- Hannum, G.; Guinney, J.; Zhao, L.; et al. Genome-wide methylation profiles reveal quantitative views of human aging rates. Mol Cell. 2013, 49, 359–367. [Google Scholar] [CrossRef]
- Rutledge, J.; Oh, H.; Wyss-Coray, T. Measuring biological age using omics data. Nat Rev Genet. 2022, 23, 715–727. [Google Scholar] [CrossRef]
- Li, Z.; Zhang, W.; Duan, Y.; et al. Progress in biological age research. Front Public Health. 2023, 11, 1074274. [Google Scholar] [CrossRef] [PubMed]
- Regan, E.A.; Hokanson, J.E.; Murphy, J.R.; et al. Genetic epidemiology of COPD (COPDGene) study design. COPD. 2010, 7, 32–43. [Google Scholar] [CrossRef] [PubMed]
- Couper, D.; LaVange, L.M.; Han, M.; et al. Design of the Subpopulations and Intermediate Outcomes in COPD Study (SPIROMICS). Thorax. 2014, 69, 491–494. [Google Scholar] [CrossRef] [PubMed]
- Gillenwater, L.A.; Pratte, K.A.; Hobbs, B.D.; et al. Plasma Metabolomic Signatures of Chronic Obstructive Pulmonary Disease and the Impact of Genetic Variants on Phenotype-Driven Modules. Netw Syst Med. 2020, 3, 159–181. [Google Scholar] [CrossRef] [PubMed]
- Hochberg, Y.; Benjamini, Y. More powerful procedures for multiple significance testing. Stat Med. 1990, 9, 811–818. [Google Scholar] [CrossRef]
- Li, S.; Kim, H.E. Implications of Sphingolipids on Aging and Age-Related Diseases. Front Aging. 2021, 2, 797320. [Google Scholar] [CrossRef]
- Lopez-Otin, C.; Blasco, M.A.; Partridge, L.; Serrano, M.; Kroemer, G. The hallmarks of aging. Cell. 2013, 153, 1194–1217. [Google Scholar] [CrossRef]
- Houben, J.M.; Mercken, E.M.; Ketelslegers, H.B.; et al. Telomere shortening in chronic obstructive pulmonary disease. Respir Med. 2009, 103, 230–236. [Google Scholar] [CrossRef]
- Aoshiba, K.; Zhou, F.; Tsuji, T.; Nagai, A. DNA damage as a molecular link in the pathogenesis of COPD in smokers. European Respiratory Journal. 2012, 39, 1368–1376. [Google Scholar] [CrossRef]
- Caramori, G.; Adcock, I.M.; Casolari, P.; et al. Unbalanced oxidant-induced DNA damage and repair in COPD: a link towards lung cancer. Thorax. 2011, 66, 521–527. [Google Scholar] [CrossRef] [PubMed]
- Johnson, S.C.; Rabinovitch, P.S.; Kaeberlein, M. mTOR is a key modulator of ageing and age-related disease. Nature. 2013, 493, 338–345. [Google Scholar] [CrossRef] [PubMed]
- Yao, Y.; Gu, Y.; Yang, M.; Cao, D.; Wu, F. The Gene Expression Biomarkers for Chronic Obstructive Pulmonary Disease and Interstitial Lung Disease. Front Genet. 2019, 10, 1154. [Google Scholar] [CrossRef]
- Fukuda, M.; Hata, A.; Niwa, S.; et al. Plasma vanillylmandelic acid level as an index of psychological stress response in normal subjects. Psychiatry Res. 1996, 63, 7–16. [Google Scholar] [CrossRef]
- Aydin, M.; Altintas, N.; Cem Mutlu, L.; et al. Asymmetric dimethylarginine contributes to airway nitric oxide deficiency in patients with COPD. Clin Respir J. 2017, 11, 318–327. [Google Scholar] [CrossRef] [PubMed]
- Scott, J.A.; Duongh, M.; Young, A.W.; Subbarao, P.; Gauvreau, G.M.; Grasemann, H. Asymmetric dimethylarginine in chronic obstructive pulmonary disease (ADMA in COPD). Int J Mol Sci. 2014, 15, 6062–6071. [Google Scholar] [CrossRef]
- Ruzsics, I.; Nagy, L.; Keki, S.; et al. L-Arginine Pathway in COPD Patients with Acute Exacerbation: A New Potential Biomarker. COPD. 2016, 13, 139–145. [Google Scholar] [CrossRef]
- Jonker, R.; Deutz, N.E.; Erbland, M.L.; Anderson, P.J.; Engelen, M.P. Alterations in whole-body arginine metabolism in chronic obstructive pulmonary disease. Am J Clin Nutr. 2016, 103, 1458–1464. [Google Scholar] [CrossRef]
- Valenca, S.S.; Rueff-Barroso, C.R.; Pimenta, W.A.; et al. L-NAME and L-arginine differentially ameliorate cigarette smoke-induced emphysema in mice. Pulm Pharmacol Ther. 2011, 24, 587–594. [Google Scholar] [CrossRef]
- Ubhi, B.K.; Riley, J.H.; Shaw, P.A.; et al. Metabolic profiling detects biomarkers of protein degradation in COPD patients. Eur Respir J. 2012, 40, 345–355. [Google Scholar] [CrossRef]
Figure 3.
Metabolite based lung obstruction score. Shown on the x- and y-axis is observed and predicted FEV1/FVC respectively. COPDGene (left) was used as the training dataset (cor = 0.705) and SPIROMICS (right) as the testing dataset (cor = 0.651), with an alpha of 0.1.
Figure 3.
Metabolite based lung obstruction score. Shown on the x- and y-axis is observed and predicted FEV1/FVC respectively. COPDGene (left) was used as the training dataset (cor = 0.705) and SPIROMICS (right) as the testing dataset (cor = 0.651), with an alpha of 0.1.
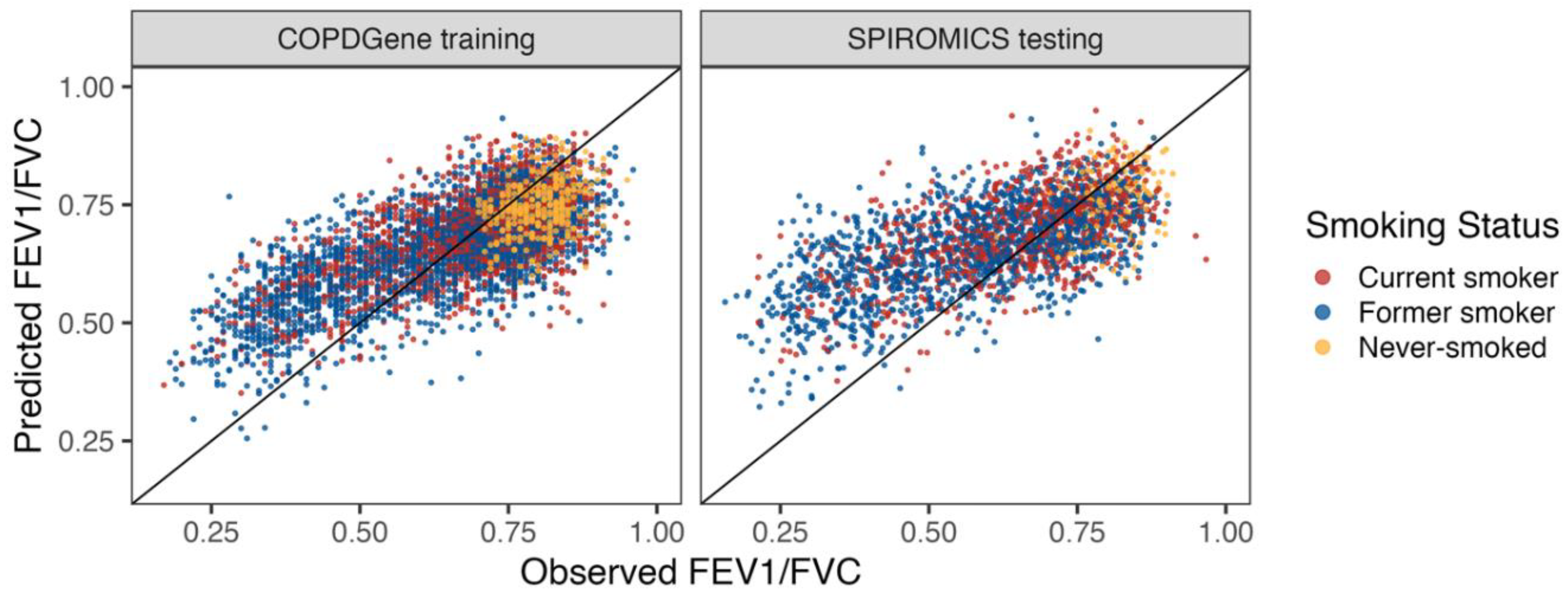
Figure 4.
Overlap between metabolites in the COPD and age metabolite score models. There were 230/831 common to both models, 231/831 included only in the COPD model and 148/831 only in the age model. The 10 largest beta coefficient metabolites for age (overlap and age only) or obstruction (FEV1/FVC score).
Figure 4.
Overlap between metabolites in the COPD and age metabolite score models. There were 230/831 common to both models, 231/831 included only in the COPD model and 148/831 only in the age model. The 10 largest beta coefficient metabolites for age (overlap and age only) or obstruction (FEV1/FVC score).
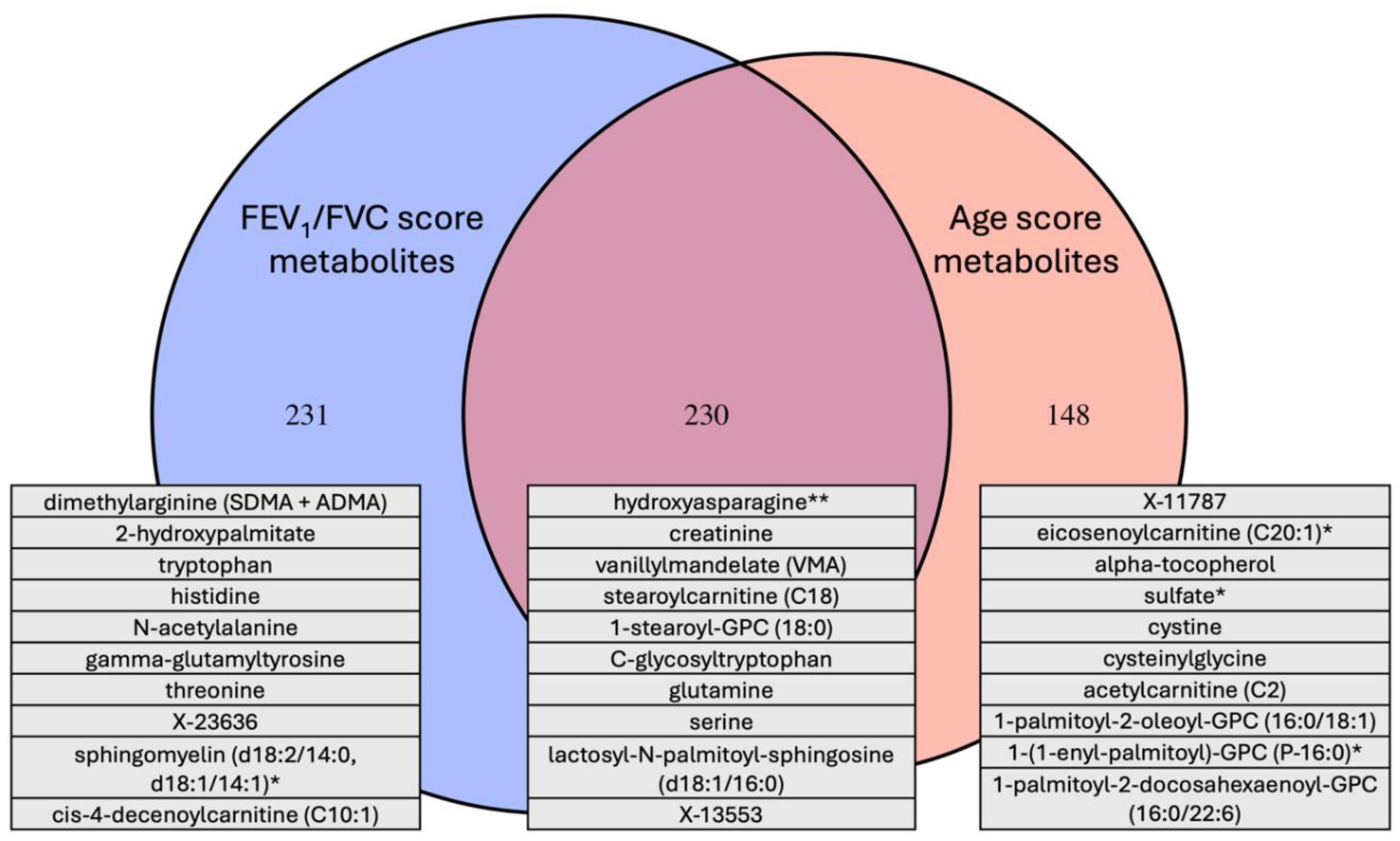
Figure 5.
Overlap of metabolite associations with age and lung obstruction in never and former smokers without COPD or emphysema (left panel) and in former and current smokers with COPD or emphysema (right panel). The sign of the coefficient estimate is multiplied by the -log10(p-value), with the x-axis showing results from univariate metabolite association with age and the y-axis showing results from univariate metabolite association with FEV1/FVC. Dashed lines at log10(0.05) and -log10(0.05) on both axes distinguish proteins that were statistically significant.
Figure 5.
Overlap of metabolite associations with age and lung obstruction in never and former smokers without COPD or emphysema (left panel) and in former and current smokers with COPD or emphysema (right panel). The sign of the coefficient estimate is multiplied by the -log10(p-value), with the x-axis showing results from univariate metabolite association with age and the y-axis showing results from univariate metabolite association with FEV1/FVC. Dashed lines at log10(0.05) and -log10(0.05) on both axes distinguish proteins that were statistically significant.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



