
Submitted:
24 August 2024
Posted:
26 August 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Severe acute respiratory infection (SARI) is mainly caused by viral pathogens, with a high prevalence in high-risk populations such as infants and older adults. Co-infections by different viruses are frequent and, in some cases, associated with severe disease outcomes. Purpose: The main purpose of this study was to identify respiratory viruses circulating in Barranquilla during the COVID-19 pandemic peaks and estimate the prevalence of viral co-infections in samples from individuals with different degrees of respiratory infection. Methods: Between August and October 2021, 101 samples were collected from individuals with influenza-like illness (ILI) by the District Health Laboratory of Barranquilla and four local health care institutions and analyzed at Universidad Simón Bolívar. Eighteen respiratory viruses, including SARS-CoV-2, were analyzed via qRT-PCR using nasal swabs or nasopharyngeal aspirate samples. Results: Of the 101 study individuals, 56 were male and 45 were female (55.5% and 44.5%, respectively); 25.7% of individuals were infected with at least one of the evaluated viruses. Respiratory syncytial virus (RSV) and human rhinovirus (HRV) were the two most frequently detected viruses (30.7% and 15.4% of total positives, respectively). Co-infections with two or more respiratory viruses accounted for 42% of the total positive cases. Conclusion: Our findings indicate the presence of different respiratory viruses in swab or nasopharyngeal aspirate samples from individuals with ILI, including coinfection. These results reveal the circulation of several respiratory viruses in the city of Barranquilla, confirming their importance as potential causes of SARI in Colombia and the need for their active surveillance.
Keywords:
Influenza-like illness
; acute respiratory infection
; molecular diagnosis
; RT-qPCR
; epidemiological surveillance
; public health
; quantitative polymerase chain reaction
1. Introduction
Acute respiratory infection (ARI) is a major public health concern worldwide and is defined as “an infectious process of the upper and lower respiratory tracts caused by bacteria and viruses, with progression of less than 15 days” [1]. However, it is estimated that in 80% of cases, the etiological agent is viral [1]. The most frequent forms of transmission are direct contact with infected subjects and contact with fomites [2]. ARI mainly affects children under 5 years of age, adults over 60 years of age, individuals with chronic underlying diseases, and immunosuppressed patients [3].
In Colombia, surveillance of this disease is framed within four strategies: sentinel surveillance of influenza-like illness-severe acute respiratory infection (ILI-SARI), intensified surveillance of unusual SARI cases, surveillance of ARI mortality in children under 5 years of age, and surveillance of ARI morbidity in all age groups, encompassing both hospitalized and ambulatory patients [3]. These strategies focus on establishing risk factors and directing promotion, prevention, and control measures.
Local longitudinal active sampling is an alternative to determining the ARI trend [4]. Over the last few years, the ability to detect respiratory viruses has improved owing to polymerase chain reaction (PCR) tests and their quantitative variants (qPCR, RT-qPCR). As a result, the spectrum of respiratory viruses detected through surveillance actions was broadened [5]. Monitoring circulating respiratory viruses can help identify patterns in respiratory infections in Barranquilla, contributing to the development of strategies to prevent outbreaks, epidemics, and eventually, pandemics.
Using the RT-qPCR technique, our study aimed to identify the respiratory viruses causing ARI-SARI to circulate in Barranquilla between August and October of 2021, during the COVID-19 pandemia, and to estimate the prevalence of viral co-infections in samples from individuals with different degrees of respiratory infection.
2. Materials and Methods
2.1. Sample Reception
The samples used to detect respiratory viruses were provided by the District Health Laboratory of Barranquilla and four local health care institutions. The samples were sent to the Molecular Diagnostics Laboratory of Universidad Simón Bolívar in triple packaging and under adequate refrigeration conditions (2°C–8°C). For patients under outpatient and emergency care, nasopharyngeal swab (NPS) samples were submitted, whereas for patients under hospitalized and intensive care, nasopharyngeal aspirates (NPA) were used. The NPS samples were sent in viral transport medium and collected in saline solution in a volume of no less than 2 mL, in accordance with the guidelines of Colombia’s National Institute of Health (INS) [6].
2.2. Selection Criteria
In this study, all patients whose samples were received during epidemiological weeks 33–42 of 2021 were included (Figure 1). For the surveillance process, typical symptomatic ILI cases were selected. Samples for the detection of respiratory viruses were collected from patients with acute episodes of fever, headache, and cough of no more than 7 days of progression, along with symptoms such as adynamia, odynophagia, rhinorrhea, and respiratory distress. Similarly, pre-existing diseases as a predisposing factor and a possible SARS-CoV-2 infection were included in the selection profile. The primary source of information was the data provided in the patient’s discharge report and epidemiologic record (FE 345-346-348, INS) for each case.
2.3. Total RNA/DNA Extraction and RT-qPCR for Respiratory Viruses
RNA/DNA extraction was performed using the commercial Quick-DNA/RNA Viral MagBead kit (Zymo Research, US) following the manufacturer’s instructions. Briefly, 200-µL aliquots of each sample (NPA or NPS) were treated with the lysis buffer provided in the kit. Subsequently, the RNA and DNA molecules released using the previous procedure were adsorbed on magnetic beads and subjected to a series of washes with different buffer solutions and ethanol. Finally, total RNA/DNA was eluted in 50 µL of nuclease-free water.
The detection of respiratory viruses was performed via RT-PCR using the Allplex™ Respiratory Panel 1, Respiratory Panel 2, and Respiratory Panel 3 kits (Seegene, US) (Table 1).
The reactions were prepared according to the manufacturer’s instructions, using a total volume of 25 µL per reaction: 17 µL reaction mix and 8 µL RNA/DNA from each sample. The amplification reactions were performed on the CFX96™ Real-time PCR System thermal cycler (Bio-Rad).
3. Data Analysis
The collected information was tabulated and analyzed using descriptive statistical tools. For this purpose, a database was created in Excel™ format, in which the relevant variables of the patients evaluated were recorded: sex, age, severity criteria, comorbidities (if any), and the symptoms described in the epidemiological records. Contingency tables and independence tests were estimated using the OpenEpi Version 3 platform. Using RT-qPCR tests, the prevalence of respiratory viruses during each epidemiological week was established.
4. Results
Our study reports the circulation of a group of respiratory viruses commonly associated with ARI in the city of Barranquilla. These viruses include respiratory syncytial virus (RSV A and B), parainfluenza virus (PIV 2, 3, and 4), human rhinovirus (HRV), metapneumovirus (MPV), adenovirus (AdV), human enterovirus (HEV), and three coronavirus subtypes (CoV OC43, CoV 229E, and NL63) between epidemiological weeks 33 and 42 of 2021. Using qRT-PCR, a prevalence of 36.9% was observed in patients infected with one or more respiratory viruses other than SARS-CoV-2 and 5.5% for those infected with SARS-CoV-2 (Table 2 and Table 3, respectively). Interweek positivity showed an increasing trend. Of the included patients, 58.4% were hospitalized, 40.7% of whom were under high-complexity care. Additionally, 2% were post-mortem patients
RSV and HRV were the most frequently detected viruses, with eight and four cases (representing 30.7% and 15.4% of the total positives, respectively). Co-infections with two or more respiratory viruses accounted for 42.3% of positive cases (Table 4).
Most study patients were infants aged 0–5 years, and this age group exhibited the greatest diversity of respiratory viruses (Table 5).
Based on the collected data, we studied the possible dependence relationship between SARS-CoV-2 infection and the symptoms caused by other respiratory viruses. Therefore, although there was a dependence between exposure to SARS-CoV-2 and the occurrence of ARI caused by other respiratory viruses (χ2:10.34; p-value: 0.00015), we found that the association was relatively low (OR: 0.102; CI: 0.015–0.407).
Coinfection with PIV-4 and MPV was the most common and observed in 50% of individuals with more than one viral agent detected. The highest number of combinations between respiratory viruses causing ARI-SARI occurred in infants. The frequency of co-infections was predominant among hospitalized adults (28–60 years) and older adults (60–80 years), 80% of whom already had pre-existing diseases (COPD, Chronic obstructive pulmonary disease, active pneumonia, and/or tuberculosis).
Of the patients, 65.3% had no comorbidities. In the remaining patients, the following comorbidities were observed: diabetes (14.8 %), pneumonia (14.8 %), heart disease (7.4 %), severe respiratory disease (COPD, asthma) (22.2 %), autoimmune disease (7.4 %), HIV (3.7 %), tuberculosis (3.7 %), and involvement of other systems (7.4 %). In 25.7% of these cases, one or more respiratory viruses were detected (Table 6).
5. Discussion
Within the context of the SARS-CoV-2/COVID-19 health emergency, the prevalence of respiratory viruses was investigated among patients with ARI-SARI symptoms. Results indicated a significant variety of respiratory viruses in Barranquilla. The prevalence reported in this study aligns with findings from other studies in Colombia and Latin America [7,8]. However, variability in the dynamics of infection caused by viral agents has been linked to the weather characteristics of the tropical zone [9].
According to INS figures, during weeks 33−42 of 2021, the sentinel surveillance for ARI-SARI identified several viruses, including RSV (55.2%), HRV (11.2%), AdV (20.8%), hMPV (5.9%), PIV (3.7%), and CoV (0.7%) [10,11,12]. The values for RSV and HRV infections were similar to those reported in this study. For PIV, the kit allowed for the segregation of different virus serotypes, and analysis was conducted accordingly. Conversely, PIV was frequently found in coinfection with one or more respiratory viruses.
In 2018 and 2019, the INS reported RSV in approximately 50% of ARI cases, followed by influenza A (Flu A) and adenovirus (AdV) as the most prevalent respiratory viruses over the same epidemiological period of interest [13]. This finding is consistent with that of our study. AdV was found in low proportions and only in coinfection with other viruses. Conversely, due to the COVID-19 pandemic, sentinel surveillance of ARI-SARI was suspended during weeks 33–42 of 2020, except for week 40, when cases of RSV and AdV [3] were reported. The incidence of SARS-CoV-2 in Barranquilla was 88.7/100,000 inhabitants (CI: 71.48–105.96) during the study period, compared to 207.58/100,000 inhabitants in the Colombian territory [14].
RSV infection in children under 5 years of age has been previously reported in Colombia [7,8,15,16]. RSV incidence in patients under 1 year of age with lower tract ARI ranged from 30% to 46%, with peaks between March and May, coinciding with the first annual rainy season [8,15]. In Brazil, 17.5% positivity was found in children aged 0–12 years between 2009 and 2013 and a higher viral load was detected in hospitalized cases [16]. Likewise, our findings are consistent with previously reports from the United States on RSV ARI in this age group [17].
The frequency of co-infections (41.7%) found in our study was similar to that described in other studies [18,19] and significantly higher than that described in a study in Santander, Colombia [20] and one in Santiago, Chile [21]. Some authors suggest that viral co-infections occurring in ARI cases in children are associated with exacerbated symptoms and require longer hospital and/or ICU intensive care unit stays [22,23]. Despite this finding, Asner et al. and other systematic reviews indicate that the presence of two or more respiratory viruses is not associated with ARI-SARI severity or its clinical course [24,25,26]. Coinfection of hMPV with other viruses has been previously reported, and the associated agents are usually PIV, RSV, and HRV [21,23].
For the purposes of INS surveillance, influenza virus (Flu) was not detected in the samples based on the operational definition of ILI, suggesting a low prevalence. This finding aligns with another study reporting Flu only in a coinfection with SARS-CoV-2 and RSV [27].
Our study had several limitations. Although RT-qPCR was used, not all samples from hospitalized patients with ARIs were screened owing to limitations in reagent availability. A larger sample size would be needed to make broader inferences about the general population. Additionally, our study captured virus behavior during a specific time period, which may have been influenced by serotypes and environmental variations, among other factors.
Despite SARS-CoV-2 being the predominant virus in ARI-SARI during the pandemic, our findings suggest that surveillance of other viruses as potential etiologic agents of SARI should continue. This should be supported by both the reference laboratory and the national network laboratories. Further studies in other territories are necessary to characterize circulating viruses and develop effective prevention and promotion measures.
Author Contributions
Conceptualization, Lisandro Pacheco-Lugo and Antonio Acosta-Hoyos; Data curation, Leonardo Arrieta-Rangel and Ibeth Luna-Rodriguez; Formal analysis, Leonardo Arrieta-Rangel, Yesit Bello-Lemus, Ibeth Luna-Rodriguez, Elkin Navarro Quiroz and Antonio Acosta-Hoyos; Funding acquisition, Lisandro Pacheco-Lugo and Antonio Acosta-Hoyos; Investigation, Leonardo Arrieta-Rangel, Yesit Bello-Lemus and Martha Guerra-Simanca; Methodology, Yesit Bello-Lemus, Martha Guerra-Simanca, Lisandro Pacheco-Lugo and Antonio Acosta-Hoyos; Project administration, Antonio Acosta-Hoyos; Supervision, Antonio Acosta-Hoyos; Validation, Ibeth Luna-Rodriguez and Elkin Navarro Quiroz; Visualization, Valmore Bermúdez; Writing – original draft, Leonardo Arrieta-Rangel; Writing – review & editing, Valmore Bermúdez, Yirys Díaz-Olmos and Antonio Acosta-Hoyos.
Funding
This study was funded with resources from the general royalty system (BPIN Project # 2021000100270).
Institutional Review Board Statement
Our Laboratory is part of the Colombian Network of Diagnostic Laboratories created at the beginning of the pandemic to mitigate COVID-19 and is coordinated by the Instituto Nacional de Salud (INS), which is the reference lab and health authority of Colombia and the Network according to the national law 9/1979, decrees 786/1990 and 2323/2006. Under the cooperation agreement 16/2020, the INS authorizes the use of biological material for research purposes without informed consent in cases of a public health emergency or those in which scientific research for public health purposes is required, including or assuring the anonymous disclosure of results. This study was performed following the ethical standards of the Declaration of Helsinki 1964 and its later amendments. The information herein does not represent a risk to the community as its data comes from secondary sources that were previously anonymized. The Laboratory internal protocol code is OT-ME-03-LT.
Acknowledgments
We thank Secretaría de Salud of Barranquilla and all the members of the COVID group of Universidad Simón Bolívar for their support during the pandemic.
Declaration of conflict of interest
The authors do not state any conflicts of interest.
References
- Charlton CL, Babady E, Ginocchio CC, Hatchette TF, Jerris RC, Li Y, et al. Practical guidance for clinical microbiology laboratories: Viruses causing acute respiratory tract infections. Clin Microbiol Rev 2019;32:e00042-18. [CrossRef]
- Fernandes-Matano L, Monroy-Muñoz IE, Angeles-Martínez J, Sarquiz-Martinez B, Palomec-Nava ID, Pardavé-Alejandre HD, et al. Prevalence of non-influenza respiratory viruses in acute respiratory infection cases in Mexico. PLOS ONE 2017;12:e0176298. [CrossRef]
- Sánchez DCM, Domínguez PAP, Ira E. Vigilancia Y ANÁLISIS del Riesgo en SALUD PÚBLICA PROTOCOLO DE VIGILANCIA. EN Salud Publ INFECCIÓN Respir AGUDA (IRA) 2017.
- Stockwell MS, Reed C, Vargas CY, Wang L, Alba LR, Jia H, et al. Five-year community surveillance study for acute respiratory infections using text messaging: Findings from the MoSAIC study. Clin Infect Dis 2022;75:987–95. [CrossRef]
- Bello-Lemus Y, Anaya-Romero M, Gómez-Montoya J, Árquez M, González-Torres HJ, Navarro-Quiroz E, et al. Comparative analysis of in-house RT-qPCR detection of SARS-CoV-2 for resource-constrained settings. Diagnostics 2022;12:2883. [CrossRef]
- Guia para la Vigilancia por Laboratorio de Virus Respiratorios.pdf n.d.
- Respiratory viruses identified from hospitalized patients in an institution of higher complexity. Interdisciplinary Journal of Epidemiology and Public Health n.d. Available online: https://revistas.unilibre.edu.co/index.php/iJEPH/article/view/5056 (accessed on 31 January 2023).
- Suryadevara M, Domachowske JB. Epidemiology and seasonality of childhood respiratory syncytial virus infections in the tropics. Viruses 2021;13:696. [CrossRef]
- Darniot M, Pitoiset C, Millière L, Aho-Glélé LS, Florentin E, Bour J-B, et al. Different meteorological parameters influence metapneumovirus and respiratory syncytial virus activity. J Clin Virol 2018;104:77–82. [CrossRef]
- Instituto Nacional de Salud. Infeccion respiratoria aguda PE IX 2021. Available online: https://www.minsalud.gov.co/salud/Paginas/Infecciones-Respiratorias-Agudas-(IRA).aspx (accessed on 31 January 2023).
- Instituto Nacional de Salud. Infeccion respiratoria aguda PE IX 2021. Available online: https://www.minsalud.gov.co/salud/Paginas/Infecciones-Respiratorias-Agudas-(IRA).aspx (accessed on 31 January 2023).
- Instituto Nacional de Salud. Infeccion respiratoria aguda PE IX 2021. Available online: https://www.minsalud.gov.co/salud/Paginas/Infecciones-Respiratorias-Agudas-(IRA).aspx (accessed on 31 January 2023).
- Sánchez DC, Fuentes SMA Informe DE evento infeccion respiratoria AGUDA, Colombia 2020 2019.
- PortalSivigila. Indicadores COVID-19. Available online: http://portalsivigila.ins.gov.co/ (accessed on 31 January 2023).
- Londono-Avendano MA, Peláez-Moreno M, López Medina E, Moreno Turriago MS, Parra Patiño B. Transmission of respiratory syncytial virus genotypes in Cali, Colombia. Influenza Other Respir Viruses 2021;15:521–8. [CrossRef]
- Cruz JS, de Souza Luna LK, Alves VRG, Conte DD, Bellei NC. Viral load of respiratory syncytial virus among children from primary care and hospital settings admitted to a university hospital in Brazil (2009–2013). J Med Virol 2021;93:3397–400. [CrossRef]
- Jain S, Williams DJ, Arnold SR, Ampofo K, Bramley AM, Reed C, et al. Community-acquired pneumonia requiring hospitalization among U.S. children. N Engl J Med 2015;372:835–45. [CrossRef]
- Benavides Osorio J Etiología viral y factores de riesgo asociados a las infecciones respiratorias agudas en niños menores de 5 años ingresados al hospital Universidad del Norte entre 2016 Y 2017. Master’s thesis. Universidad del Norte.
- Co-infección viral respiratoria en niños hospitalizados por infección respiratoria aguda y su impacto en la gravedad clínica. Rev Chil Infect 2012; 29 (2): 169-174. [CrossRef]
- García Corzo JR, Niederbacher Velasquez J, González Rugéles CI, Rodríguez Villamizar LA, Machuca Pérez M, Torres Prieto A, et al. Etiología viral de infección respiratoria aguda en niños menores de 5 años en las provincias comunera y García Rovira de santander. Revista de la Universidad Industrial de Santander Salud 2016;48:240–5. [CrossRef]
- Le-Corre N, Pérez R, Vizcaya C, Martínez-Valdebenito C, López T, Monge M, et al. Relevance of codetection of respiratory viruses in the severity of acute respiratory infection in hospitalized children. Andes Pediatr 2021;92:349–58. [CrossRef]
- Chauhan JC, Slamon NB. The impact of multiple viral respiratory infections on outcomes for critically ill children. Pediatr Crit Care Med 2017;18:e333–8. [CrossRef]
- Rehder KJ, Wilson EA, Zimmerman KO, Cunningham CK, Turner DA. Detection of multiple respiratory viruses associated with mortality and severity of illness in children. Pediatr Crit Care Med 2015;16:e201–6. [CrossRef]
- Asner SA, Science ME, Tran D, Smieja M, Merglen A, Mertz D. Clinical disease severity of respiratory viral co-infection versus single viral infection: A systematic review and meta-analysis. PLOS ONE 2014;9:e99392. [CrossRef]
- Scotta MC, Chakr VC, de Moura A, Becker RG, de Souza APD, Jones MH, et al. Respiratory viral coinfection and disease severity in children: A systematic review and meta-analysis. J Clin Virol 2016;80:45–56. [CrossRef]
- Meskill SD, O’Bryant SC. Respiratory virus co-infection in acute respiratory infections in children. Curr Infect Dis Rep 2020;22:3. [CrossRef]
- PAHO. Influenza regional Update EW 38, 2021 /actualización regional de Influenza SE 38 de 2021. Available online: https://www.paho.org/es/documentos/actualizacion-regional-influenza-semana-epidemiologica-38-octubre-6-2021 (accessed on 31 January 2023).
Figure 1.
Flow chart used for the selection and screening of respiratory samples.
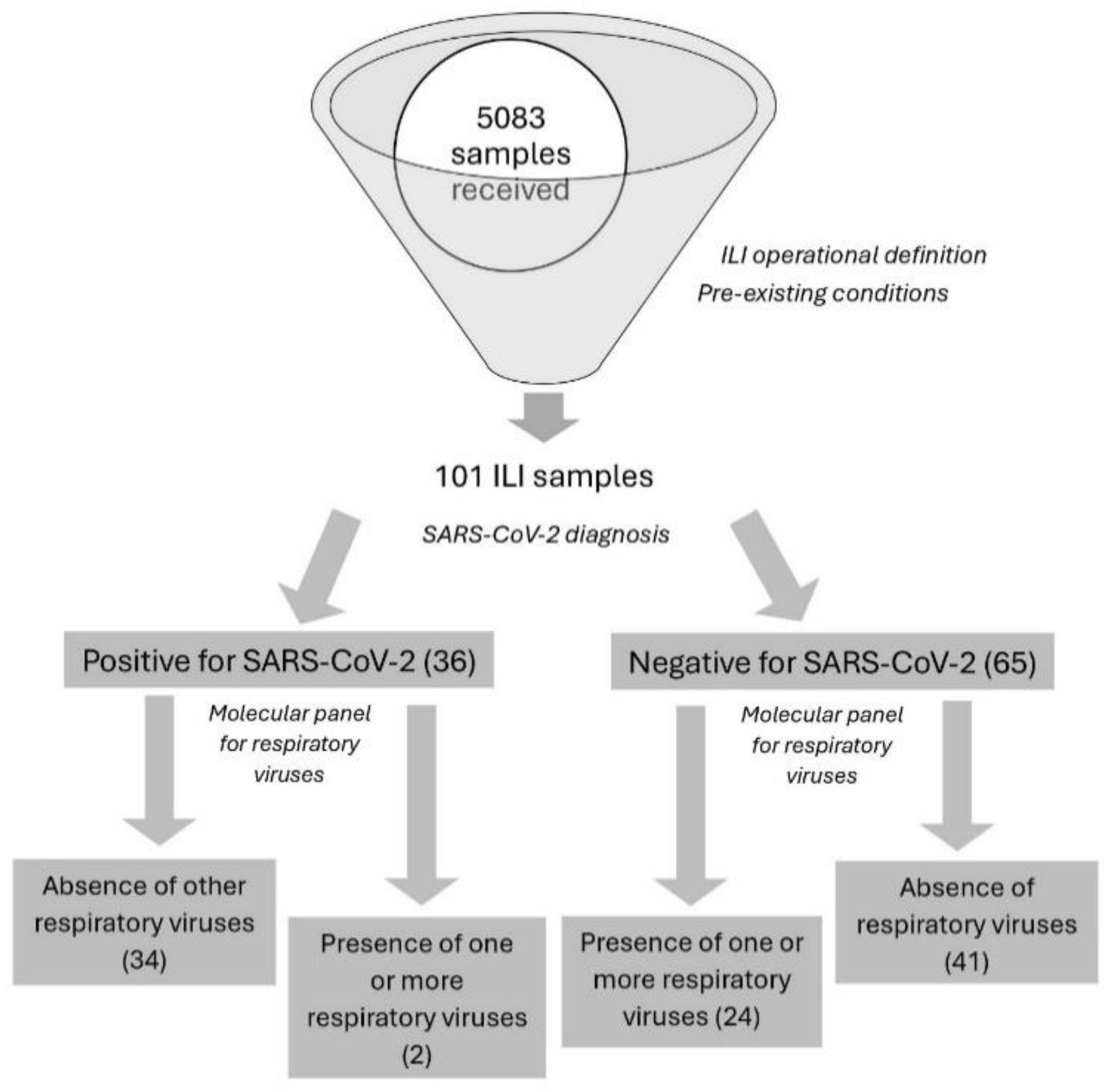

Table 1.
Respiratory viruses screened in the study.
| Allplex™ Respiratory Panel 1 | Allplex™ Respiratory Panel 2 | Allplex™ Respiratory Panel 3 |
|---|---|---|
| Influenza A (Flu A) | Human adenovirus (AdV) | Bocavirus 1/2/3/4 (BoV) |
| Influenza B (Flu B) | Human metapneumovirus (hMPV) | Human rhinovirus A/B/C (HRV) |
| Respiratory Syncytial Virus A (RSV A) | Human enterovirus (hEV) | Coronavirus 229E |
| Respiratory Syncytial Virus B (RSV B) | Parainfluenza 1 (PIV-1) | Coronavirus NL63 |
| Influenza A-H1N1 (Flu A-H1pdm09) | Parainfluenza 2 (PIV-2) | Coronavirus OC43 |
| Parainfluenza 3 (PIV-3) | ||
| Parainfluenza 4 (PIV-4) |
Table 2.
Sociodemographic variables and comorbidities in patients positive for SARS-CoV-2.
| Variables | POSITIVE SARS-CoV-2 DIAGNOSIS | |||||||
|---|---|---|---|---|---|---|---|---|
| No hospitalization | Hospitalization | Intensive care unit admission | Deaths | |||||
| n | % | n | % | n | % | n | % | |
| Sex | ||||||||
| Male | 6 | 5.94% | 1 | 0.99% | 1 | 0.99% | - | - |
| Female | 13 | 12.87% | 11 | 10.89% | 2 | 1.98% | 2 | 1.98% |
| Age (years) | ||||||||
| 0 - 5 | 1 | 0.99% | - | - | - | - | - | - |
| 6-11 | - | - | - | - | - | - | - | - |
| 12-18 | 1 | 0.99% | - | - | - | - | - | - |
| 19 - 27 | 8 | 7.92% | - | - | - | - | - | - |
| 28 - 59 | 7 | 6.93% | 3 | 2.97% | 2 | 1.98% | 2 | 1.98% |
| 60 - 80 | 2 | 1.98% | 8 | 7.92% | 1 | 0.99% | - | - |
| >80 | - | - | 1 | 0.99% | - | - | - | - |
| Comorbidities | ||||||||
| Autoimmune disease | - | - | - | - | - | - | - | - |
| Diabetes | - | - | - | - | - | - | - | - |
| Immunosuppressed individuals | 1 | 0.99% | - | - | - | - | - | - |
| Digestive system diseases | 1 | 0.99% | - | - | - | - | - | - |
| Cardiovascular system diseases | - | - | 2 | 1.98% | - | - | - | - |
| Nervous system diseases | - | - | - | - | - | - | - | - |
| Respiratory system diseases | 1 | 0.99% | 1 | 0.99% | 1 | 0.99% | 1 | 0.99% |
| Urinary system diseases | - | - | - | - | - | - | - | - |
| Various comorbidities | 1 | 0.99% | - | - | 1 | 0.99% | 1 | 0.99% |
| Human Immunodeficiency virus | - | - | - | - | - | - | - | - |
| None | 15 | 14.85% | 9 | 8.91% | 1 | 0.99% | - | - |
| Molecular diagnosis (respiratory panels) | ||||||||
| Negative | 17 | 16.83% | 12 | 11.88% | 3 | 2.97% | 2 | 1.98% |
| Positive | 2 | 1.98% | - | - | - | - | - | - |
Table 3.
Sociodemographic variables and comorbidities in patients negative for SARS-CoV-2.
| Variables | No hospitalization | Hospitalization | Intensive care unit admission | |||
|---|---|---|---|---|---|---|
| n | % | N | % | n | % | |
| Sex | ||||||
| Male | 13 | 20.0% | 12 | 18.5% | 12 | 18.5% |
| Female | 8 | 12.3% | 11 | 16.9% | 9 | 13.8% |
| Age groups (years) | ||||||
| 0 - 5 | 5 | 7.7% | 11 | 16.9% | 10 | 15.4% |
| 6 - 11 | 6 | 9.2% | 1 | 1.5% | 1 | 1.5% |
| 12 - 18 | 3 | 4.6% | 1 | 1.5% | 1 | 1.5% |
| 19 - 27 | 1 | 1.5% | 1 | 1.5% | 2 | 3.1% |
| 28 - 59 | 3 | 4.6% | 4 | 6.2% | 5 | 7.7% |
| 60 - 80 | 2 | 3.1% | 3 | 4.6% | 2 | 3.1% |
| >80 | 1 | 1.5% | 2 | 3.1% | - | - |
| Comorbidities | ||||||
| Autoimmune disease | - | - | - | - | 1 | 1.5% |
| Diabetes | 2 | 3.1% | - | - | - | - |
| Immunosuppressed individuals | 1 | 1.5% | 1 | 1.5% | 1 | 1.5% |
| Cardiovascular system diseases | 2 | 3.1% | 1 | 1.5% | ||
| Nervous system diseases | - | - | 1 | 1.5% | 1 | 1.5% |
| Respiratory system diseases | 1 | 1.5% | 3 | 4.6% | 3 | 4.6% |
| Urinary system diseases | - | - | - | - | 1 | 1.5% |
| Human Immunodeficiency virus | - | - | 1 | 1.5% | - | - |
| Various comorbidities | - | - | 3 | 4.6% | 1 | 1.5% |
| Autoimmune disease | - | - | - | - | 1 | 1.5% |
| None | 15 | 23.1% | 14 | 21.5% | 12 | 18.5% |
| Molecular diagnosis (respiratory panels) | ||||||
| Negative | 19 | 29.2% | 9 | 13.8% | 13 | 20.0% |
| Positive | 2 | 3.1% | 14 | 21.5% | 8 | 12.3% |
Table 4.
Global distribution of respiratory viruses found in the study.
| Etiological agent | n | % |
|---|---|---|
| RSV A | 4 | 15.38% |
| RSV B | 4 | 15.38% |
| PIV 2 | 1 | 3.85% |
| PIV 3 | 2 | 7.69% |
| HRV | 4 | 15.38% |
| > 1 respiratory virus | 11 | 42.31% |
| AdV, HEV, HRV | 1 | 3.85% |
| RSV A, AdV, HEV | 1 | 3.85% |
| RSV B, HRV | 1 | 3.85% |
| PIV 2, HRV | 1 | 3.85% |
| PIV 4, MPV | 4 | 15.38% |
| PIV 4, MPV, HRV | 1 | 3.85% |
| HRV, Coronavirus subtype 229E, Coronavirus subtype NL63 | 1 | 3.85% |
| HRV, Coronavirus subtype OC43 | 1 | 3.85% |
| Total | 26 | |
| Note: All abbreviations referred in the table stand for the viruses studied as follows, RSV: Respiratory Syncytial Virus; PIV: parainfluenza virus; HRV: human rhinovirus; AdV: Adenovirus; HEV: Human enterovirus; MPV: human metapneumovirus | ||
Table 5.
Respiratory virus distribution by age group.
| Etiological agent | SARS-CoV-2 negative | SARS-CoV-2 positive | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0-5 | 6-11 | 19-27 | 28-59 | 60-80 | >80 | Total | 19-27 | 28-59 | Total | |||||||||
| n | % | n | % | n | % | n | % | n | % | n | % | n | % | n | % | |||
| RSV A | 3 | 11.54 | - | - | 1 | 3.85 | - | - | - | - | - | - | 4 | - | - | - | - | |
| RSV B | 3 | 11.54 | 1 | 3.85 | - | - | - | - | - | - | - | - | 4 | - | - | - | - | |
| PIV 2 | 1 | 3.85 | - | - | - | - | - | - | - | - | - | - | 1 | - | - | - | - | |
| PIV 3 | 1 | 3.85 | - | - | - | - | - | - | - | - | 1 | 3.85 | 2 | - | - | - | - | |
| HRV | 1 | 3.85 | - | - | 1 | 3.85 | - | - | 1 | 3.85 | - | - | 3 | - | - | 1 | 3.85 | 1 |
| >1 respiratory virus | 6 | 23.08 | - | - | - | - | 3 | 11.54 | 1 | 3.85 | - | - | 10 | - | - | - | - | |
| AdV, HEV, HRV | 1 | 3.85 | - | - | - | - | - | - | - | - | - | - | 1 | - | - | - | - | |
| RSV A, AdV, HEV | 1 | 3.85 | - | - | - | - | - | - | - | - | - | - | 1 | - | - | - | - | |
| RSV B, HRV | - | - | - | - | - | - | 1 | 3.85 | - | - | - | - | 1 | - | - | - | - | |
| PIV 2, HRV | 1 | 3.85 | - | - | - | - | - | - | - | - | - | - | 1 | - | - | - | - | |
| PIV 4, MPV | 2 | 7.69 | - | - | - | - | 1 | 3.85 | 1 | 3.85 | - | - | 4 | - | - | - | - | |
| PIV 4, MPV, HRV | 1 | 3.85 | - | - | - | - | - | - | - | - | - | - | 1 | - | - | - | - | |
| HRV, Coronavirus subtype 229E, Coronavirus subtype 229E | - | - | - | - | - | - | - | - | - | - | - | - | - | 1 | 3.85 | - | - | 1 |
| HRV, Coronavirus subtype OC43 | - | - | - | - | - | 1 | 3.85 | - | - | - | - | 1 | - | - | - | - | ||
| 24 | 2 | |||||||||||||||||
| Note: All abbreviations referred in the table stand for the viruses studied as follows, RSV: Respiratory Syncytial Virus; PIV: parainfluenza virus; HRV: human rhinovirus; AdV: Adenovirus; HEV: Human enterovirus; MPV: human metapneumovirus | ||||||||||||||||||
Table 6.
Respiratory virus distribution in patients with comorbidities.
| Comorbidity/ etiological agent | No hospitalization | General hospitalization | Intensive care unit admission | Total | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Immunosuppressed | 1 | ||||||
| RSV A | - | - | - | - | 1 | 3.8 | |
| Nervous system diseases | 1 | ||||||
| PIV 2 | - | - | 1 | 3.8 | - | - | |
| Respiratory system diseases | 4 | ||||||
| PIV 4, MPV | - | - | - | - | 1 | 3.8 | |
| HRV, Coronavirus subtype OC43 | - | - | - | - | 1 | 3.8 | |
| RSV B | - | - | 1 | 3.8 | - | - | |
| HRV | - | - | 1 | 3.8 | - | - | |
| Urinary system diseases | 1 | ||||||
| HRV | - | - | - | - | 1 | 3.8 | |
| Various comorbidities | 2 | ||||||
| PIV 4, MPV | - | - | 1 | 3.8 | - | - | |
| PIV 3 | - | - | 1 | 3.8 | - | - | |
| None | 4 | 15.4 | 9 | 34.6 | 4 | 15.4 | 17 |
| 24 | |||||||
| Note: All abbreviations referred in the table stand for the viruses studied as follows, RSV: Respiratory Syncytial Virus; PIV: parainfluenza virus; HRV: human rhinovirus; AdV: Adenovirus; HEV: Human enterovirus; MPV: human metapneumovirus | |||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



