
Submitted:
26 August 2024
Posted:
26 August 2024
You are already at the latest version
Abstract
Background: Staphylococcus aureus is a major contributor to biofilm-associated infections, which complicate the treatment of chronic conditions like osteomyelitis and prosthetic infections. Bio-films, characterized by bacterial communities encased in a protective matrix, hinder the effec-tiveness of antimicrobial agents and contribute to persistent infections. Objective: This study aimed to evaluate the activity of delafloxacin, a novel fluoroquinolone, against biofilm-forming S. aureus strains, including methicillin-resistant (MRSA) and methicillin-sensitive (MSSA) isolates. Methods: Delafloxacin’s efficacy was compared with traditional antibiotics (vancomycin, line-zolid, doxycycline, sulfamethoxazole/trimethoprim, and rifampicin) using minimal inhibitory concentration (MIC) assays, including testing at different pH levels to simulate acidic biofilm conditions. Synergistic interactions between delafloxacin and other antimicrobials were assessed using the checkerboard method. Biofilm eradication was tested through minimal biofilm eradi-cation concentration (MBEC) assays, biomass quantification, and cell viability (MTT assay). Re-sults: The results showed that all isolates were susceptible to vancomycin and linezolid, with varying resistance to other antibiotics. Delafloxacin demonstrated potent activity, with MIC re-ductions observed in acidic conditions. Synergistic effects were minimal, with only a few isolates showing synergy with vancomycin and doxycycline. Biofilm eradication tests revealed limited success in eradicating biofilms at breakpoint concentrations. However, rifampicin in combination with delafloxacin significantly reduced biofilm biomass in some isolates. No significant changes in cell viability were noted across treatments. Conclusion: This study highlights delafloxacin's potential against biofilm-associated infections, particularly in acidic environments. Despite the challenges in biofilm eradication, delafloxacin combined with rifampicin shows promise for im-proved treatment strategies.
Keywords:
Staphylococcus aureus
; biofilm
; delafloxacin
; rifampicin
1. Introduction
Staphylococcus aureus plays a significant role in biofilm production, contributing to its persistence and pathogenicity, especially in chronic infections [1]. Biofilms are structured communities of bacterial cells enclosed in a self-produced polymeric matrix that adhere to surfaces and protect S. aureus from antimicrobial agents. The matrix limits the penetration of antibiotics, and the slow growth rate of bacteria within the biofilm further enhances resistance [2].
The leading cause of chronic osteomyelitis and prosthetic infections is S. aureus. Its ability to form biofilms significantly contributes to the persistence and difficulty in treating these conditions [3]. Surgical removal of the infected prosthetic device and debridement of infected bone tissue are necessary to manage these infections followed by long-term antibiotic therapy [4].
Treatment typically involves a combination of antibiotics, including those that can penetrate biofilms and target dormant bacteria [5]. Prolonged antibiotic therapy is often required to fully eradicate the infection [6]. The best antibiotics against S. aureus biofilm are rifampicin and daptomycin, although other antibiotics have variable activity [7,8]. Although rifampicin is highly effective against biofilm-embedded S. aureus due to its ability to penetrate biofilms and target dormant bacteria, it should not be used as monotherapy because resistance can develop quickly [9]. Daptomycin is effective against biofilms, especially when used in combination with other antibiotics, including rifampicin [10].
Fluoroquinolones can be effective against S. aureus. However, their effectiveness against biofilm-associated infections can vary [11]. They have good tissue penetration and can reach biofilm-embedded bacteria [12]. However, the biofilm matrix can still limit their penetration to some extent. The mechanism of action on DNA gyrase and topoisomerase IV is effective against actively growing bacteria but less so against dormant cells within biofilms. To improve efficacy, quinolones are often used in combination with other antibiotics. For instance, combining quinolones with rifampicin can enhance the overall antibacterial effect and help prevent resistance [12,13].
Delafloxacin is a newer fluoroquinolone with promising activity against Methicillin-resistant S. aureus (MRSA), including biofilm-associated infections [14]. Delafloxacin even seems to be more active than daptomycin against the MRSA strain at equipotent concentrations [15]. Delafloxacin can be used orally, making it a very attractive drug in the treatment of orthopedic infections that require prolonged treatment, an advantage over daptomycin, vancomycin and other anti-MRSA drugs. Furthermore, delafloxacin shows greater activity in acidic environments, a common condition in biofilm [16]. Considering these aspects and the recommendations for combined therapy in the treatment of infections associated with biofilm, the objective of this study was to evaluate the activity of delafloxacin combined with other drugs in a biofilm model.
The introduction should briefly place the study in a broad context and highlight why it is important. It should define the purpose of the work and its significance. The current state of the research field should be carefully reviewed and key publications cited. Please highlight controversial and diverging hypotheses when necessary. Finally, briefly mention the main aim of the work and highlight the principal conclusions. As far as possible, please keep the introduction comprehensible to scientists outside your particular field of research. References should be numbered in order of appearance and indicated by a numeral or numerals in square brackets—e.g., [1] or [2,3], or [4,5,6]. See the end of the document for further details on references.
2. Results
2.1. MIC Determination by Broth Microdilution and E-Test
Among the 12 S. aureus isolates, 10 were MRSA and 2 were MSSA. The MIC results are detailed in Table 1. All isolates were susceptible to vancomycin and linezolid. One isolate was resistant to doxycycline, while two isolates exhibited resistance to both SMX-TMP and rifampicin. Delafloxacin was tested using broth microdilution and E-test, and evaluated at different pH levels (7.4 and 5.5) (Table 1). In the E-test, 4 isolates were susceptible to delafloxacin, and the results were consistent with those obtained by broth microdilution. In 4 of the 12 isolates, the E-test showed a 1 dilution decrease in MIC compared to the broth microdilution at pH 7.4. At pH 5.5, there was a significant reduction in MIC compared to pH 7.4. The MIC decrease ranged from none (1 isolate), 1-fold (1 isolate), 2-fold (8 isolates), 3-fold (1 isolate), to 4-fold (1 isolate).
2.2. Synergism Test
The synergy between delafloxacin and other antimicrobials was assessed using the checkerboard method. Minimal synergy was observed among the tested isolates. Only one isolate showed synergy with vancomycin, and two isolates demonstrated synergy with doxycycline. Specifically, two isolates that were susceptible to doxycycline and the tested antibiotics (isolates 41 and 132) were identified. No antagonism was observed between the drug combinations, suggesting that these combinations may be additive or synergistic (Table 2).
2.3. Biofilm Test, Biomass, and MTT
For biofilm analysis, the four delafloxacin-sensitive isolates (41, 130, 132, and 136) were selected. In the MBEC (Minimum Biofilm Eradication Concentration) test, no complete eradication of biofilm was achieved even at antibiotic breakpoint concentrations. However, two isolates demonstrated significant anti-biofilm activity, with a two-log reduction in biofilm biomass when rifampicin was combined with delafloxacin (isolates 130 and 132). Additionally, isolate 132 showed anti-biofilm activity with the combination of delafloxacin and doxycycline (see Figure 1 and Figure 2).
The biomass assessment was conducted for each antibiotic individually as well as in combination with delafloxacin. Generally, there was a reduction in biomass with most single antibiotics, except for doxycycline with isolate 41, and rifampicin and SMX-TMP with isolate 132, where no reduction in biomass was observed. In the combinations of antibiotics with delafloxacin, no significant reduction in biomass was noted (see Figure 3 and Figure 4).
3. Discussion
Staphylococcus aureus is renowned for its ability to form biofilms, a trait that significantly contributes to its pathogenicity, particularly in chronic infections such as osteomyelitis and prosthetic infections [2,5,17,18,19]. The biofilm structure, a complex community of bacterial cells embedded in a self-produced matrix, offers robust protection against both host immune responses and antimicrobial agents [6]. This matrix impedes the penetration of antibiotics and the slow growth of bacteria within the biofilm further exacerbates resistance, making these infections particularly challenging to treat [8,20,21].
The persistence of S. aureus biofilms in medical devices and bone tissues often necessitates surgical intervention coupled with prolonged antibiotic therapy [3,22,23,24,25,26]. Despite the use of advanced antibiotics and the removal of infected devices, the treatment of biofilm-associated infections remains difficult due to the inherent resistance mechanisms of biofilm-embedded bacteria [15,27,28,29].
The management of biofilm-associated infections often involves a combination of antibiotics. Rifampicin and daptomycin are frequently used due to their efficacy against biofilm-embedded bacteria [8,30,31,32,33]. Rifampicin, in particular, is known for its ability to penetrate biofilms and target dormant bacteria effectively. However, its use as monotherapy is limited due to the rapid development of resistance [9,34,35]. Daptomycin, another potent antimicrobial, is effective against biofilms, especially when used in combination with rifampicin, enhancing its overall efficacy [3].
Fluoroquinolones, including delafloxacin, represent another class of antibiotics with potential efficacy against S. aureus. Their mechanism of action involves inhibition of DNA gyrase and topoisomerase IV, enzymes crucial for bacterial DNA replication and repair. Although fluoroquinolones have demonstrated good tissue penetration and some ability to reach biofilm-embedded bacteria, their effectiveness against dormant cells within biofilms is limited [8]. As a result, fluoroquinolones are often used in combination with other agents to improve treatment outcomes [11,13].
Delafloxacin, a newer fluoroquinolone, has shown promising activity against MRSA, including biofilm-associated infections [14]. It has demonstrated superior activity compared to daptomycin against MRSA at equipotent concentrations, making it a valuable option for treating resistant strains [36,37]. Additionally, delafloxacin's oral availability presents a significant advantage over other anti-MRSA agents like daptomycin and vancomycin, which are typically administered intravenously. This oral formulation is particularly beneficial for treating orthopedic infections that require prolonged therapy [38,39].
The unique advantage of delafloxacin lies in its enhanced activity in acidic environments, which is a common condition in biofilms [15,16]. This characteristic suggests that delafloxacin could be more effective in disrupting biofilm matrices and targeting embedded bacteria than other fluoroquinolones.
In this study, the MIC of delafloxacin was assessed alongside other antibiotics using the broth microdilution method and the Etest gradient strip method. All isolates were susceptible to vancomycin and linezolid. However, resistance to doxycycline, SMX-TMP, and rifampicin was observed in some isolates. Delafloxacin showed consistent results across both methods, confirming its effectiveness against the tested strains [40,41,42].
Interestingly, the MIC of delafloxacin decreased significantly at a lower pH of 5.5 compared to the neutral pH of 7.4. This finding highlights delafloxacin's enhanced activity in acidic environments, a common feature of biofilm-associated infections [43,44]. The observed decrease in MIC, ranging from none to four-fold reductions, underscores delafloxacin’s potential effectiveness in acidic biofilm conditions.
The checkerboard method was employed to assess the synergistic effects of delafloxacin in combination with other antibiotics. Minimal synergy was observed overall. Synergy was noted with vancomycin in one isolate and with doxycycline in two isolates, suggesting that while delafloxacin has potential in combination therapies, the extent of synergy varies among different antibiotic pairs [45]. No antagonistic effects were detected, indicating that the combinations of delafloxacin with other drugs could be additive or synergistic, which is valuable information for designing effective treatment regimens.
Biofilm disruption was evaluated using various methods, including the MBEC, crystal violet staining, and the MTT assay. The MBEC test demonstrated that complete eradication of biofilm was not achieved even at breakpoint concentrations of the antibiotics. However, significant anti-biofilm activity was observed when rifampicin was combined with delafloxacin, resulting in a two-log reduction in biofilm biomass for two isolates. This result aligns with the known effectiveness of rifampicin against biofilms and suggests that combining it with delafloxacin can enhance biofilm disruption [9,11,24].
The crystal violet staining method, used to quantify biomass, revealed a reduction in biomass with most single antibiotics. However, no significant reduction in biomass was noted when delafloxacin was combined with other antibiotics. This finding suggests that while delafloxacin alone or in combination can impact biofilm biomass, the effect might not be as pronounced when compared to other antimicrobial agents [46].
Cell viability within biofilms was assessed using the MTT assay. The results showed no significant changes in cell viability across individual antibiotics and their combinations with delafloxacin. This indicates that while some antibiotics, like rifampicin, show effectiveness in reducing biofilm biomass, they may not significantly impact the overall viability of the biofilm cells. This discrepancy highlights the complexity of biofilm-associated infections and the need for comprehensive evaluation of both biomass reduction and cell viability to fully assess treatment efficacy [47].
This study underscores the potential of delafloxacin as an effective treatment option for MRSA biofilm-associated infections. Its enhanced activity in acidic environments and oral availability make it a promising candidate for treating chronic infections, particularly in orthopedic settings. The combination of delafloxacin with rifampicin shows promise in disrupting biofilms, though further research is needed to optimize treatment regimens and fully understand the mechanisms of synergy and resistance. The findings emphasize the importance of continued research into new antimicrobial agents and combination therapies to combat biofilm-associated infections effectively. By expanding our understanding of how different antibiotics interact and impact biofilm structures, we can develop more effective strategies for managing these challenging infections.
4. Materials and Methods
4.1. Isolates
A total of twelve S. aureus strains were selected from a high-complexity hospital (Curitiba, Paraná, Brazil), ten MRSA and two MSSA. These isolates were randomly chosen from blood cultures obtained from different patients over a span of three months.
4.2. Minimal Inhibitory Concentration (MIC)
The antimicrobial susceptibility of the isolates to delafloxacin (DLX), vancomycin, linezolid, sulfamethoxazole/trimethoprim (SMX-TMP), doxycycline (DOX), and rifampicin (RIF) was assessed using the broth microdilution method, following CLSI M7-A9 guidelines [48]. The MIC was determined as the lowest concentration that prevented visible growth. To verify the MIC for delafloxacin, the Etest gradient strip method (Liofilchem, Waltham, MA) was used, with interpretation based on the point where the inhibition zone intersected the Etest scale. MIC interpretations were aligned with EUCAST 2024 guidelines [49]. Delafloxacin susceptibility was also tested at different pH levels. The experiments were conducted at pH 7.4, as recommended by CLSI M7-A9, and at pH 5.5 to evaluate the strains' behavior in an acidic environment.
4.3. Synergism Test
The checkerboard method was employed to evaluate the synergy between delafloxacin and other antimicrobials [50]. In this assay, one antibiotic was serially diluted along the ordinate, while the second antibiotic was diluted along the abscissa. A concentration of 105 CFU/mL was used for the strains [51]. The MIC was defined as the lowest concentration showing no turbidity or growth. Synergism was quantified using the sum of the fractional inhibitory concentrations (ƩFIC), calculated as ƩFIC = FIC A + FIC B, where FIC A is the MIC of antimicrobial A in combination divided by its MIC when used alone, and FIC B is the MIC of antimicrobial B in combination divided by its MIC when used alone. Synergism was indicated by ƩFIC < 0.5, indifference by ƩFIC between 0.5 and 4.0, and antagonism by ƩFIC > 4.0 [52].
4.4. Biofilm Test, Biomass, and MTT
Based on results of the synergism observed between the proposed antimicrobials against S. aureus strains, the antimicrobials were tested both individually and in combination using in vitro biofilm models. For the analysis, the concentrations were determined according to the sensitivity breakpoints established by EUCAST 2024. In a 96-well microplate, samples were added at a concentration of 106 CFU/mL in TSB broth and incubated at 37°C for 24 hours. After incubation, the liquid was removed and replaced with 100 µL of TSB broth plus 100 µL of antimicrobial solution, either individually or in combination. The plates were incubated at 37°C for an additional 24 hours. Then, three different methods were used, which included the minimal biofilm eradication concentration (MBEC) , biomass (crystal violet), and cell viability (MTT).
4.5. MBEC
After the antibiotic treatment and washing step, 200 µL of PBS (pH 7.5) was added to each well, and the 96-well microplates were sonicated in an ultrasonic bath for 5 min at 37 °C and 40 kHz (Sanders Medical, Santa Rita do Sapucaí, Minas Gerais, Brazil) to disrupt the biofilm matrix cells. Serial dilutions were made using sterile saline, which was poured onto TSA plates. The plates were then incubated for 24 h at 36 °C. The CFU count was determined and the results were calculated as CFU/mL, where MBEC is the minimum concentration in milligram per liter of each antifungal capable of reducing biofilm cells by 2 log10 [53].
4.6. Estimation of Metabolic Activity by the MTT Reduction Assay
The biofilms were incubated in a 96-well microplate filled with 200 µL MTT [3-(4,5-dimethylthiazol-2yl)-2,5-diphenyl tetrazolium bromide] (Sigma-Aldrich, St. Louis, MO, USA) at a concentration of 1 mg/mL at 36 °C for 2 h. After incubation, MTT was aspirated, and the wells were washed thrice using PBS (pH 7.5). The resulting product (formazan) formed inside the cells was dissolved in 200 µL of isopropanol and homogenized. Next, 100 µL of this solution was transferred to a new 96-well microplate. Absorbance was measured using a Versa-Max microplate ELISA reader adjusted to a wavelength of 570 nm [54]. Biofilm classification was based on optical density (OD) according to a previous criteria [55]. The results of the MTT assay were expressed as a percentage relative to the positive control (PC), which was considered 100%.
4.7. Biomass
For the crystal violet technique, after incubating the microplate, all the liquid content was removed and 200 µL of methanol peroxide was added to fix the remaining bacteria at the bottom of the wells. After 20 minutes, the content was discarded and allowed to dry at room temperature. Then, 200 µL of 1% crystal violet was added for 5 minutes. After this time, the plate was washed with deionized water, and then 200 µL of 33% glacial acetic acid was added to resuspend the biofilm formed at the bottom of the wells. Optical density readings were taken using an automated ELISA reader at a wavelength of 480 nm.
4.8. Statistical Analysis
All tests were performed in triplicates. Qualitative data are described as percentages, and quantitative data are expressed as medians with 10% and 90% percentiles. To compare the results among antibiotics, the Mann-Whitney U test was used to compare medians (one by one). Statistical significance was set at p < 0.05. The Shapiro-Wilk normality test showed a non-normal distribution of data, justifying the usage of a non-parametric test.
Author Contributions
Conceptualization, F.T. and J.M.; methodology, A.A. and G.O.; formal analysis, F.T. and P.S. ; investigation, A.A.; resources, J.M.; writing—original draft preparation, X.X.; writing—review and editing, F.T.; visualization, J.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by EUROFARMA and The APC was funded by EUROFARMA.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data Availability as requested.
Conflicts of Interest
F.T. received financial supported by Eurofarma to develop this study. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Pedroni, M.A.; Ribeiro, V.S.T.; Cieslinski, J.; Lopes, A.P.A.; Kraft, L.; Suss, P.H.; Tuon, F.F. Different concentrations of vancomycin with gentamicin loaded PMMA to inhibit biofilm formation of Staphylococcus aureus and their implications. J Orthop Sci 2024, 29, 334–340. [Google Scholar] [CrossRef]
- Soni, J.F.; Ribeiro, V.S.T.; Cieslinski, J.; de Andrade, A.P.; Dantas, L.R.; Pereira, B.Z.; de Almeida, B.; Suss, P.H.; Tuon, F.F. Evaluation of silver nanoparticle-impregnated PMMA loaded with vancomycin or gentamicin against bacterial biofilm formation. Injury 2023, 54 Suppl 6, 110649. [Google Scholar] [CrossRef]
- Telles, J.P.; Cieslinski, J.; Tuon, F.F. Daptomycin to bone and joint infections and prosthesis joint infections: a systematic review. Braz J Infect Dis 2019, 23, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Haidar, R.; Der Boghossian, A.; Atiyeh, B. Duration of post-surgical antibiotics in chronic osteomyelitis: empiric or evidence-based? Int J Infect Dis 2010, 14, e752–758. [Google Scholar] [CrossRef]
- Tuon, F.F.; Suss, P.H.; Telles, J.P.; Dantas, L.R.; Borges, N.H.; Ribeiro, V.S.T. Antimicrobial Treatment of Staphylococcus aureus Biofilms. Antibiotics (Basel) 2023, 12. [Google Scholar] [CrossRef]
- Tuon, F.F.; Dantas, L.R.; Suss, P.H.; Tasca Ribeiro, V.S. Pathogenesis of the Pseudomonas aeruginosa Biofilm: A Review. Pathogens 2022, 11. [Google Scholar] [CrossRef]
- Koch, J.A.; Pust, T.M.; Cappellini, A.J.; Mandell, J.B.; Ma, D.; Shah, N.B.; Brothers, K.M.; Urish, K.L. Staphylococcus epidermidis Biofilms Have a High Tolerance to Antibiotics in Periprosthetic Joint Infection. Life (Basel) 2020, 10. [Google Scholar] [CrossRef] [PubMed]
- Yee, R.; Yuan, Y.; Tarff, A.; Brayton, C.; Gour, N.; Feng, J.; Zhang, Y. Eradication of Staphylococcus aureus Biofilm Infection by Persister Drug Combination. Antibiotics (Basel) 2022, 11. [Google Scholar] [CrossRef] [PubMed]
- Brinkman, C.L.; Schmidt-Malan, S.M.; Mandrekar, J.N.; Patel, R. Rifampin-Based Combination Therapy Is Active in Foreign-Body Osteomyelitis after Prior Rifampin Monotherapy. Antimicrob Agents Chemother 2017, 61. [Google Scholar] [CrossRef]
- Mandell, J.B.; Orr, S.; Koch, J.; Nourie, B.; Ma, D.; Bonar, D.D.; Shah, N.; Urish, K.L. Large variations in clinical antibiotic activity against Staphylococcus aureus biofilms of periprosthetic joint infection isolates. J Orthop Res 2019, 37, 1604–1609. [Google Scholar] [CrossRef]
- Melendez-Carmona, M.A.; Mancheno-Losa, M.; Ruiz-Sorribas, A.; Munoz-Gallego, I.; Viedma, E.; Chaves, F.; Van Bambeke, F.; Lora-Tamayo, J. Strain-to-strain variability among Staphylococcus aureus causing prosthetic joint infection drives heterogeneity in response to levofloxacin and rifampicin. J Antimicrob Chemother 2022, 77, 3265–3269. [Google Scholar] [CrossRef]
- Melendez-Carmona, M.A.; Munoz-Gallego, I.; Viedma, E.; Lora-Tamayo, J.; Chaves, F. Intraosteoblastic activity of levofloxacin and rifampin alone and in combination against clinical isolates of meticillin-susceptible Staphylococcus aureus causing prosthetic joint infection. Int J Antimicrob Agents 2019, 54, 356–360. [Google Scholar] [CrossRef] [PubMed]
- Lora-Tamayo, J.; Euba, G.; Cobo, J.; Horcajada, J.P.; Soriano, A.; Sandoval, E.; Pigrau, C.; Benito, N.; Falgueras, L.; Palomino, J.; et al. Short- versus long-duration levofloxacin plus rifampicin for acute staphylococcal prosthetic joint infection managed with implant retention: a randomised clinical trial. Int J Antimicrob Agents 2016, 48, 310–316. [Google Scholar] [CrossRef] [PubMed]
- Turban, A.; Guerin, F.; Dinh, A.; Cattoir, V. Updated Review on Clinically-Relevant Properties of Delafloxacin. Antibiotics (Basel) 2023, 12. [Google Scholar] [CrossRef]
- Bauer, J.; Siala, W.; Tulkens, P.M.; Van Bambeke, F. A combined pharmacodynamic quantitative and qualitative model reveals the potent activity of daptomycin and delafloxacin against Staphylococcus aureus biofilms. Antimicrob Agents Chemother 2013, 57, 2726–2737. [Google Scholar] [CrossRef]
- Lemaire, S.; Tulkens, P.M.; Van Bambeke, F. Contrasting effects of acidic pH on the extracellular and intracellular activities of the anti-gram-positive fluoroquinolones moxifloxacin and delafloxacin against Staphylococcus aureus. Antimicrob Agents Chemother 2011, 55, 649–658. [Google Scholar] [CrossRef]
- Cieslinski, J.; Ribeiro, V.S.T.; Kraft, L.; Suss, P.H.; Rosa, E.; Morello, L.G.; Pillonetto, M.; Tuon, F.F. Direct detection of microorganisms in sonicated orthopedic devices after in vitro biofilm production and different processing conditions. Eur J Orthop Surg Traumatol 2021, 31, 1113–1120. [Google Scholar] [CrossRef]
- da Rocha, L.; Ribeiro, V.S.T.; de Andrade, A.P.; Goncalves, G.A.; Kraft, L.; Cieslinski, J.; Suss, P.H.; Tuon, F.F. Evaluation of Staphylococcus aureus and Candida albicans biofilms adherence to PEEK and titanium-alloy prosthetic spine devices. Eur J Orthop Surg Traumatol 2022, 32, 981–989. [Google Scholar] [CrossRef] [PubMed]
- Mendonca, J.R.; Dantas, L.R.; Tuon, F.F. Activity of multipurpose contact lens solutions against Staphylococcus aureus, Pseudomonas aeruginosa, Serratia marcescens and Candida albicans biofilms. Ophthalmic Physiol Opt 2023, 43, 1092–1099. [Google Scholar] [CrossRef]
- Sikdar, R.; Elias, M.H. Evidence for Complex Interplay between Quorum Sensing and Antibiotic Resistance in Pseudomonas aeruginosa. Microbiol Spectr 2022, 10, e0126922. [Google Scholar] [CrossRef]
- Ranjbar, R.; Farahani, A. Study of genetic diversity, biofilm formation, and detection of Carbapenemase, MBL, ESBL, and tetracycline resistance genes in multidrug-resistant Acinetobacter baumannii isolated from burn wound infections in Iran. Antimicrob Resist Infect Control 2019, 8, 172. [Google Scholar] [CrossRef] [PubMed]
- Ueda, N.; Oe, K.; Nakamura, T.; Tsuta, K.; Iida, H.; Saito, T. Sonication of Extracted Implants Improves Microbial Detection in Patients With Orthopedic Implant-Associated Infections. J Arthroplasty 2019, 34, 1189–1196. [Google Scholar] [CrossRef]
- Valour, F.; Trouillet-Assant, S.; Riffard, N.; Tasse, J.; Flammier, S.; Rasigade, J.P.; Chidiac, C.; Vandenesch, F.; Ferry, T.; Laurent, F. Antimicrobial activity against intraosteoblastic Staphylococcus aureus. Antimicrob Agents Chemother 2015, 59, 2029–2036. [Google Scholar] [CrossRef]
- Lora-Tamayo, J.; Parra-Ruiz, J.; Rodriguez-Pardo, D.; Barberan, J.; Ribera, A.; Tornero, E.; Pigrau, C.; Mensa, J.; Ariza, J.; Soriano, A. High doses of daptomycin (10 mg/kg/d) plus rifampin for the treatment of staphylococcal prosthetic joint infection managed with implant retention: a comparative study. Diagn Microbiol Infect Dis 2014, 80, 66–71. [Google Scholar] [CrossRef]
- Molina-Manso, D.; del Prado, G.; Ortiz-Perez, A.; Manrubia-Cobo, M.; Gomez-Barrena, E.; Cordero-Ampuero, J.; Esteban, J. In vitro susceptibility to antibiotics of staphylococci in biofilms isolated from orthopaedic infections. Int J Antimicrob Agents 2013, 41, 521–523. [Google Scholar] [CrossRef] [PubMed]
- Seaton, R.A.; Malizos, K.N.; Viale, P.; Gargalianos-Kakolyris, P.; Santantonio, T.; Petrelli, E.; Pathan, R.; Heep, M.; Chaves, R.L. Daptomycin use in patients with osteomyelitis: a preliminary report from the EU-CORE(SM) database. J Antimicrob Chemother 2013, 68, 1642–1649. [Google Scholar] [CrossRef]
- Boles, B.R.; Horswill, A.R. Staphylococcal biofilm disassembly. Trends Microbiol 2011, 19, 449–455. [Google Scholar] [CrossRef] [PubMed]
- Sampedro, M.F.; Huddleston, P.M.; Piper, K.E.; Karau, M.J.; Dekutoski, M.B.; Yaszemski, M.J.; Currier, B.L.; Mandrekar, J.N.; Osmon, D.R.; McDowell, A.; et al. A biofilm approach to detect bacteria on removed spinal implants. Spine (Phila Pa 1976) 2010, 35, 1218–1224. [Google Scholar] [CrossRef] [PubMed]
- Marques, S.C. Formation of biofilms by Staphylococcus aureus on stainless steel and glass surfaces and its resistance to some selected chemical sanitizers. Braz J Microbiol 2007, 38, 6. [Google Scholar] [CrossRef]
- Thompson, J.M.; Saini, V.; Ashbaugh, A.G.; Miller, R.J.; Ordonez, A.A.; Ortines, R.V.; Wang, Y.; Sterling, R.S.; Jain, S.K.; Miller, L.S. Oral-Only Linezolid-Rifampin Is Highly Effective Compared with Other Antibiotics for Periprosthetic Joint Infection: Study of a Mouse Model. J Bone Joint Surg Am 2017, 99, 656–665. [Google Scholar] [CrossRef]
- Herrera, S.; Sorli, L.; Horcajada, J.P. High-dose daptomycin together with rifampin as salvage therapy for prosthetic joint infections. Med Clin (Barc) 2017, 149, 223–224. [Google Scholar] [CrossRef] [PubMed]
- Boudjemaa, R.; Briandet, R.; Revest, M.; Jacqueline, C.; Caillon, J.; Fontaine-Aupart, M.P.; Steenkeste, K. New Insight into Daptomycin Bioavailability and Localization in Staphylococcus aureus Biofilms by Dynamic Fluorescence Imaging. Antimicrob Agents Chemother 2016, 60, 4983–4990. [Google Scholar] [CrossRef]
- Stein, C.; Makarewicz, O.; Forstner, C.; Weis, S.; Hagel, S.; Loffler, B.; Pletz, M.W. Should daptomycin-rifampin combinations for MSSA/MRSA isolates be avoided because of antagonism? Infection 2016, 44, 499–504. [Google Scholar] [CrossRef]
- Saleh-Mghir, A.; Muller-Serieys, C.; Dinh, A.; Massias, L.; Cremieux, A.C. Adjunctive rifampin is crucial to optimizing daptomycin efficacy against rabbit prosthetic joint infection due to methicillin-resistant Staphylococcus aureus. Antimicrob Agents Chemother 2011, 55, 4589–4593. [Google Scholar] [CrossRef] [PubMed]
- Forrest, G.N.; Tamura, K. Rifampin combination therapy for nonmycobacterial infections. Clin Microbiol Rev 2010, 23, 14–34. [Google Scholar] [CrossRef] [PubMed]
- Vlachaki, I.; Vacchelli, M.; Zinzi, D.; Falla, E.; Jiang, Y.; Mantopoulos, T.; Nathwani, D. Comparative efficacy of delafloxacin for complicated and acute bacterial skin and skin structure infections: results from a network meta-analysis. BMC Infect Dis 2021, 21, 1036. [Google Scholar] [CrossRef]
- Saravolatz, L.D.; Pawlak, J.M.; Wegner, C. Delafloxacin activity against Staphylococcus aureus with reduced susceptibility or resistance to methicillin, vancomycin, daptomycin or linezolid. J Antimicrob Chemother 2020, 75, 2605–2608. [Google Scholar] [CrossRef] [PubMed]
- Cruz, J.A.W.; da Cunha, M.; de Moraes, T.P.; Marques, S.; Tuon, F.F.; Gomide, A.L.; de Paula Linhares, G. Brazilian private health system: history, scenarios, and trends. BMC Health Serv Res 2022, 22, 49. [Google Scholar] [CrossRef]
- Loesch, G.H.; Cruz, J.A.W.; Gasparetto, J.; Oliveira, D.D.S.; Telles, J.P.; Tuon, F.F. Cost minimization analysis of outpatient parenteral/oral antibiotic therapy at a trauma hospital: Public health system. Infect Control Hosp Epidemiol 2021, 42, 1445–1450. [Google Scholar] [CrossRef]
- Coustilleres, F.; Renault, V.; Corvec, S.; Dupieux, C.; Simoes, P.M.; Lartigue, M.F.; Plouzeau-Jayle, C.; Tande, D.; Lamoureux, C.; Lemarie, C.; et al. Clinical, Bacteriological, and Genetic Characterization of Bone and Joint Infections Involving Linezolid-Resistant Staphylococcus epidermidis: a Retrospective Multicenter Study in French Reference Centers. Microbiol Spectr 2023, 11, e0419022. [Google Scholar] [CrossRef]
- Gomez-Zorrilla, S.; Sendra, E.; Horcajada, J.P. A profile of delafloxacin in the treatment of adults with community-acquired bacterial pneumonia. Expert Rev Clin Pharmacol 2022, 15, 671–688. [Google Scholar] [CrossRef]
- Fan, K.C.; Lin, J.; Yannuzzi, N.A.; Al-Khersan, H.; Patel, N.A.; Maestre-Mesa, J.; Zaidi, M.; Miller, D.; Flynn, H.W., Jr. In vitro Susceptibilities of Methicillin-Susceptible and Resistant Staphylococci to Traditional Antibiotics Compared to a Novel Fluoroquinolone. J Ophthalmic Inflamm Infect 2020, 10, 9. [Google Scholar] [CrossRef] [PubMed]
- Mechmechani, S.; Yammine, J.; Alhuthali, S.; El Mouzawak, M.; Charvourou, G.; Ghasrsallaoui, A.; Chihib, N.E.; Doulgeraki, A.; Karam, L. Study of the Resistance of Staphylococcus aureus Biofilm, Biofilm-Detached Cells, and Planktonic Cells to Microencapsulated Carvacrol Used Alone or Combined with Low-pH Treatment. Int J Mol Sci 2024, 25. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Grajera, M.; Pacha-Olivenza, M.A.; Fernandez-Calderon, M.C.; Gonzalez-Martin, M.L.; Gallardo-Moreno, A.M. Dynamic Adhesive Behavior and Biofilm Formation of Staphylococcus aureus on Polylactic Acid Surfaces in Diabetic Environments. Materials (Basel) 2024, 17. [Google Scholar] [CrossRef]
- Rios, E.; Perez, M.; Sanz, J.C.; Delgado-Iribarren, A.; Rodriguez-Avial, I. Efficacy of delafloxacin alone and in combination with cefotaxime against cefotaxime non-susceptible invasive isolates of Streptococcus pneumoniae. Rev Esp Quimioter 2024, 37, 158–162. [Google Scholar] [CrossRef] [PubMed]
- Siala, W.; Mingeot-Leclercq, M.P.; Tulkens, P.M.; Hallin, M.; Denis, O.; Van Bambeke, F. Comparison of the antibiotic activities of Daptomycin, Vancomycin, and the investigational Fluoroquinolone Delafloxacin against biofilms from Staphylococcus aureus clinical isolates. Antimicrob Agents Chemother 2014, 58, 6385–6397. [Google Scholar] [CrossRef]
- Gasparetto, J.; Bressianini Jurkonis, L.; Ramos Dantas, L.; Hansen Suss, P.; Francisco Tuon, F. Low-cost antiseptic-impregnated tracheostomy tube for the prevention of ventilator-associated pneumonia caused by multidrug-resistant bacteria: In vitro and pilot study in humans. Rev Argent Microbiol 2024. [Google Scholar] [CrossRef]
- CLSI. Clinical Laboratory Standard Insitute - M07 - A10 - Methods for Dilution Antimicrobial Suceptibility Tests for Bacteria that Grow Aerobically. 2015.
- EUCAST. Clinical breakpoint. European Committee on Antimicrobial Susceptibility Testing 2021, Version 11.
- Orhan, G.; Bayram, A.; Zer, Y.; Balci, I. Synergy tests by E test and checkerboard methods of antimicrobial combinations against Brucella melitensis. J Clin Microbiol 2005, 43, 140–143. [Google Scholar] [CrossRef]
- Chaiben, V.; Yamada, C.H.; Telles, J.P.; de Andrade, A.P.; Arend, L.; Ribeiro, V.S.T.; Dantas, L.R.; Suss, P.H.; Tuon, F.F. A carbapenem-resistant Acinetobacter baumannii outbreak associated with a polymyxin shortage during the COVID pandemic: an in vitro and biofilm analysis of synergy between meropenem, gentamicin and sulbactam. J Antimicrob Chemother 2022, 77, 1676–1684. [Google Scholar] [CrossRef]
- Chadwick, E.G.; Shulman, S.T.; Yogev, R. Correlation of antibiotic synergy in vitro and in vivo: use of an animal model of neutropenic gram-negative sepsis. J Infect Dis 1986, 154, 670–675. [Google Scholar] [CrossRef]
- Rodrigues, C.F.; Henriques, M. Liposomal and Deoxycholate Amphotericin B Formulations: Effectiveness against Biofilm Infections of Candida spp. Pathogens 2017, 6, 62. [Google Scholar] [CrossRef] [PubMed]
- Traba, C.; Liang, J.F. Susceptibility of Staphylococcus aureus biofilms to reactive discharge gases. Biofouling 2011, 27, 763–772. [Google Scholar] [CrossRef] [PubMed]
- Christensen, G.D.; Simpson, W.A.; Younger, J.J.; Baddour, L.M.; Barrett, F.F.; Melton, D.M.; Beachey, E.H. Adherence of coagulase-negative staphylococci to plastic tissue culture plates: a quantitative model for the adherence of staphylococci to medical devices. J Clin Microbiol 1985, 22, 996–1006. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
MBEC (Minimum Biofilm Eradication Concentration) test of antibiotics against MRSA susceptible to delafloxacin. The dashed line represents the 2 logs decrease in comparison with positive control. The number is the top represent the name of the isolate. SMX-TMP = Sulfamethoxazole / trimethoprim; DOX - Doxycycline; RIF - Rifampicin; DLX - Delafloxacin; VAN - Vancomycin; LNZ – Linezolid.
Figure 1.
MBEC (Minimum Biofilm Eradication Concentration) test of antibiotics against MRSA susceptible to delafloxacin. The dashed line represents the 2 logs decrease in comparison with positive control. The number is the top represent the name of the isolate. SMX-TMP = Sulfamethoxazole / trimethoprim; DOX - Doxycycline; RIF - Rifampicin; DLX - Delafloxacin; VAN - Vancomycin; LNZ – Linezolid.
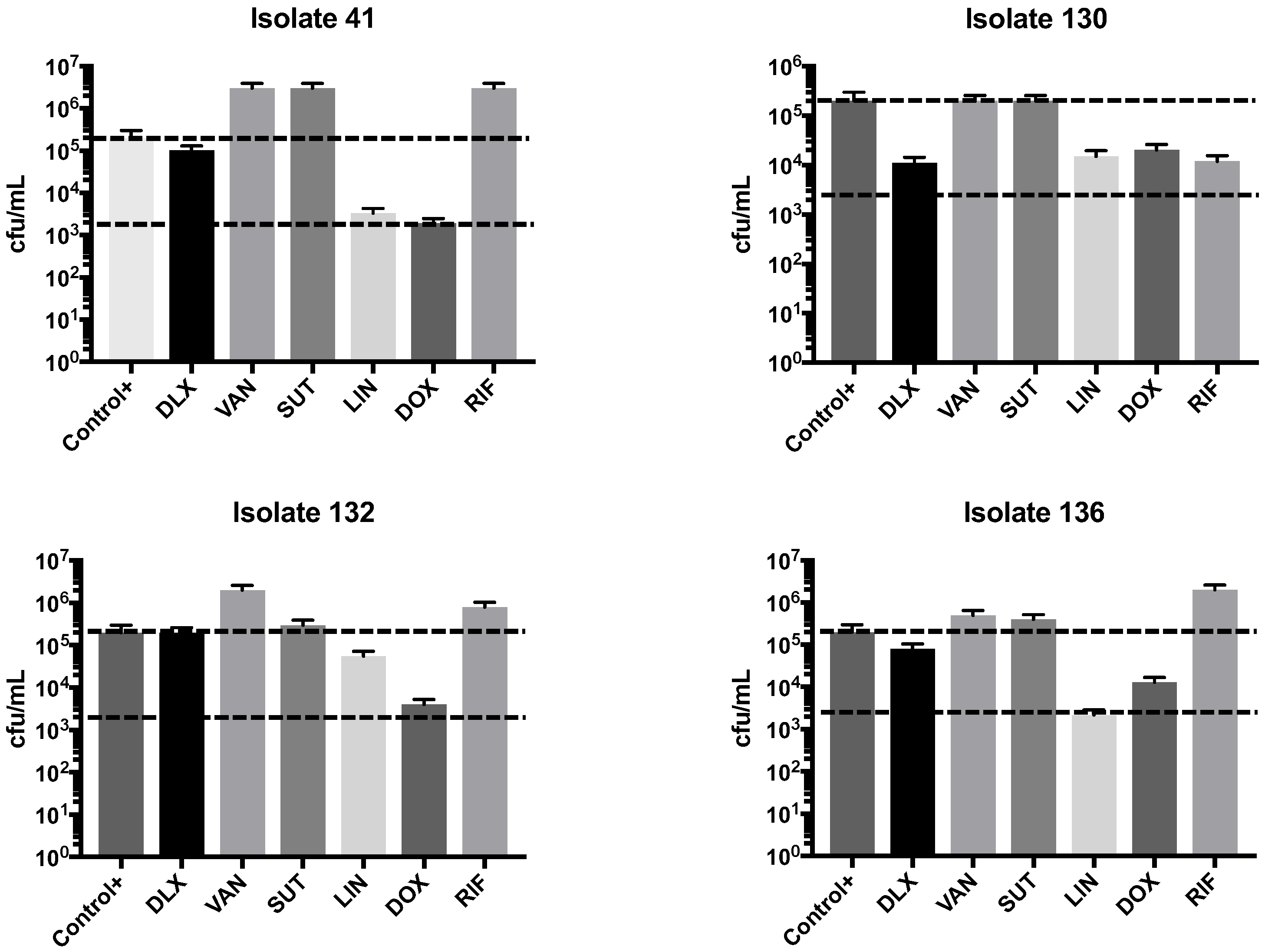
Figure 2.
MBEC (Minimum Biofilm Eradication Concentration) test of antibiotics against MRSA susceptible to delafloxacin in combinations. The dashed line represents the 2 logs decrease in comparison with positive control. The number is the top represent the name of the isolate. SMX-TMP = Sulfamethoxazole / trimethoprim; DOX - Doxycycline; RIF - Rifampicin; DLX - Delafloxacin; VAN - Vancomycin; LNZ - Linezolid.
Figure 2.
MBEC (Minimum Biofilm Eradication Concentration) test of antibiotics against MRSA susceptible to delafloxacin in combinations. The dashed line represents the 2 logs decrease in comparison with positive control. The number is the top represent the name of the isolate. SMX-TMP = Sulfamethoxazole / trimethoprim; DOX - Doxycycline; RIF - Rifampicin; DLX - Delafloxacin; VAN - Vancomycin; LNZ - Linezolid.
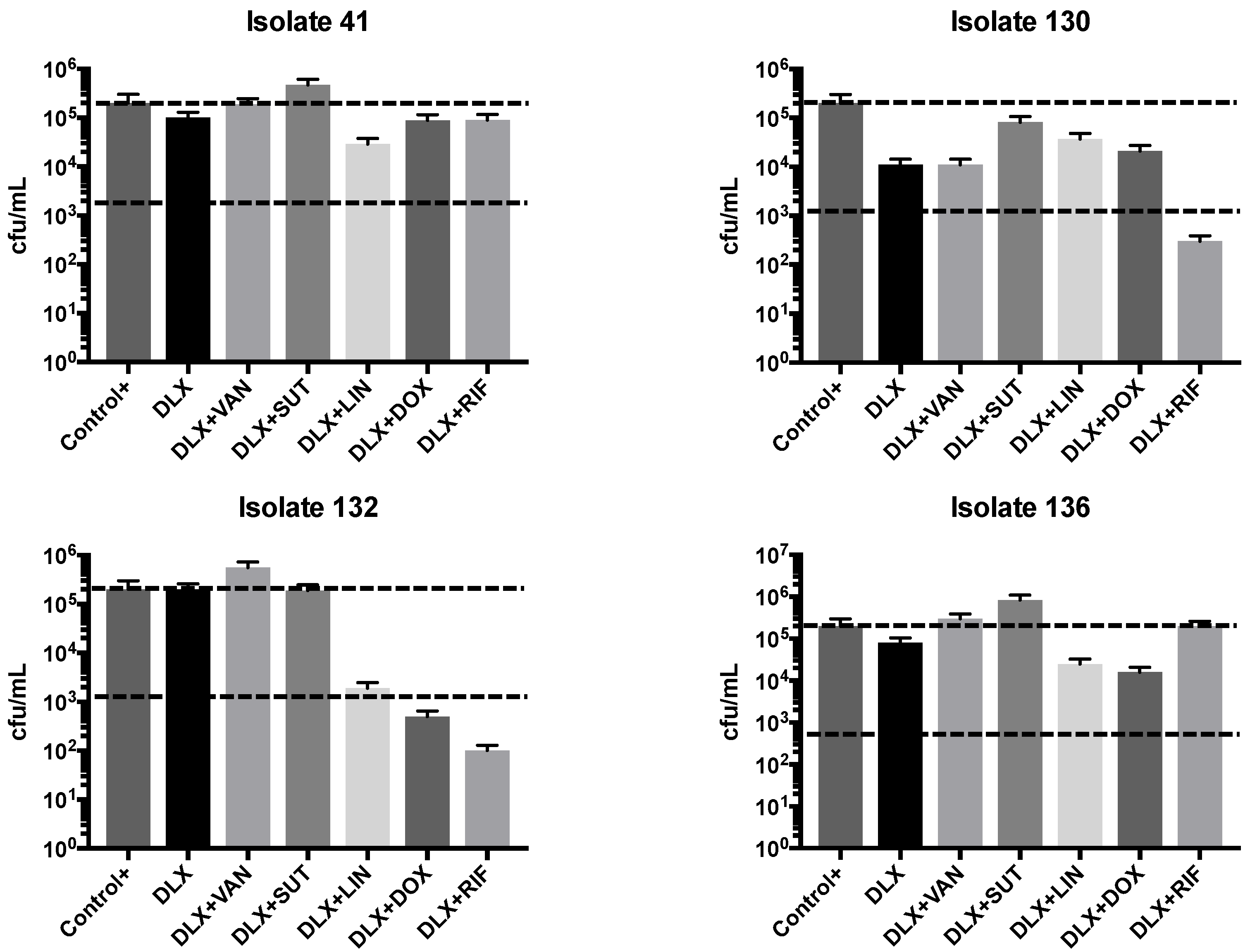
Figure 3.
Biomass (by crystal violet) test of antibiotics against MRSA susceptible to delafloxacin. The dashed line represents the positive control and negative control. The number is the top represent the name of the isolate. SMX-TMP = Sulfamethoxazole / trimethoprim; DOX - Doxycycline; RIF - Rifampicin; DLX - Delafloxacin; VAN - Vancomycin; LNZ – Linezolid.
Figure 3.
Biomass (by crystal violet) test of antibiotics against MRSA susceptible to delafloxacin. The dashed line represents the positive control and negative control. The number is the top represent the name of the isolate. SMX-TMP = Sulfamethoxazole / trimethoprim; DOX - Doxycycline; RIF - Rifampicin; DLX - Delafloxacin; VAN - Vancomycin; LNZ – Linezolid.
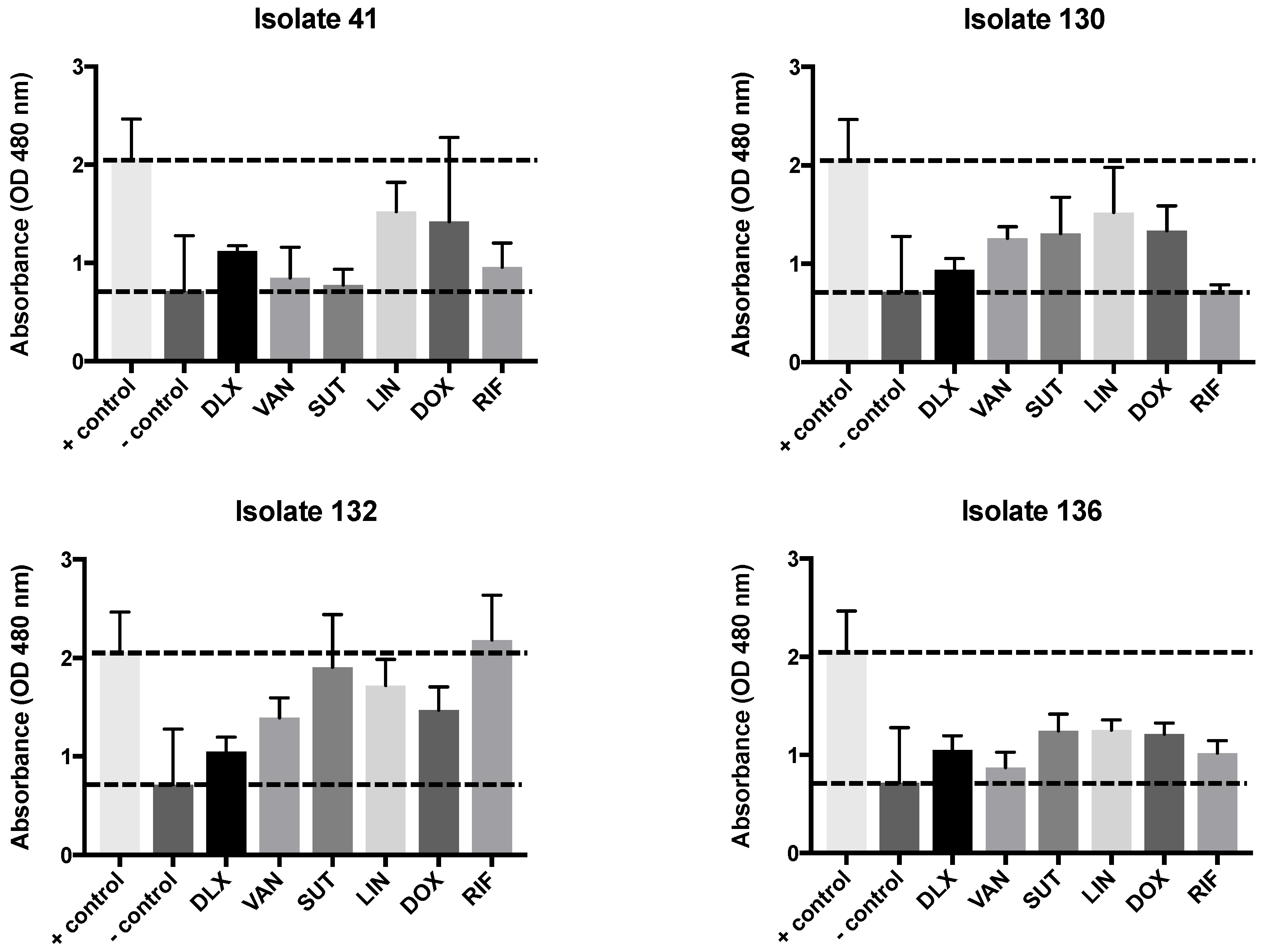
Figure 4.
Biomass (by crystal violet) test of antibiotics against MRSA susceptible to delafloxacin in combinations. The dashed line represents the positive control and negative control. The number is the top represent the name of the isolate. SMX-TMP = Sulfamethoxazole / trimethoprim; DOX - Doxycycline; RIF - Rifampicin; DLX - Delafloxacin; VAN - Vancomycin; LNZ - Linezolid
Figure 4.
Biomass (by crystal violet) test of antibiotics against MRSA susceptible to delafloxacin in combinations. The dashed line represents the positive control and negative control. The number is the top represent the name of the isolate. SMX-TMP = Sulfamethoxazole / trimethoprim; DOX - Doxycycline; RIF - Rifampicin; DLX - Delafloxacin; VAN - Vancomycin; LNZ - Linezolid
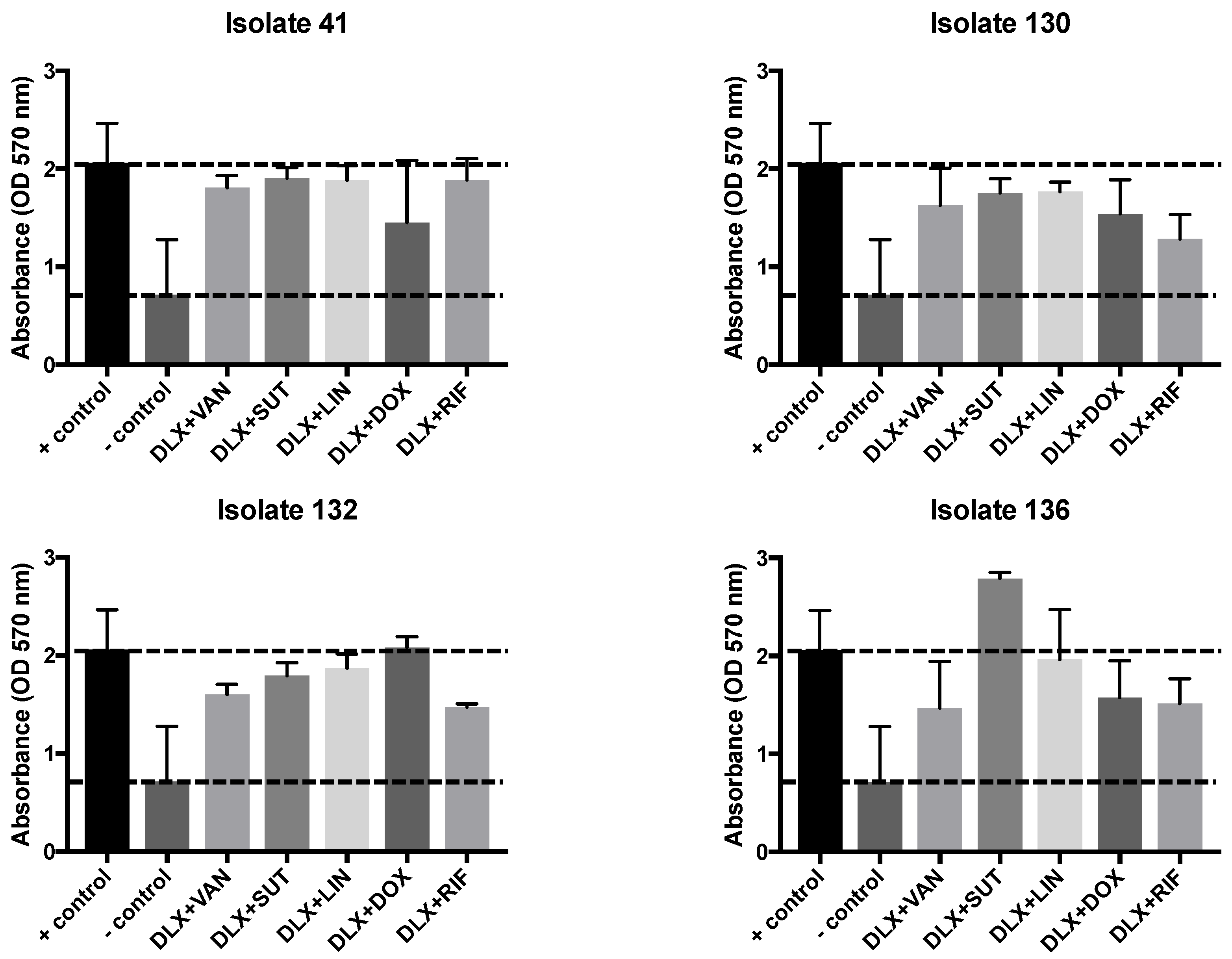
Figure 5.
MTT in biofilm with antibiotics against MRSA susceptible to delafloxacin. The dashed line represents the positive control and negative control. The number is the top represent the name of the isolate. SMX-TMP = Sulfamethoxazole / trimethoprim; DOX - Doxycycline; RIF - Rifampicin; DLX - Delafloxacin; VAN - Vancomycin; LNZ – Linezolid.
Figure 5.
MTT in biofilm with antibiotics against MRSA susceptible to delafloxacin. The dashed line represents the positive control and negative control. The number is the top represent the name of the isolate. SMX-TMP = Sulfamethoxazole / trimethoprim; DOX - Doxycycline; RIF - Rifampicin; DLX - Delafloxacin; VAN - Vancomycin; LNZ – Linezolid.
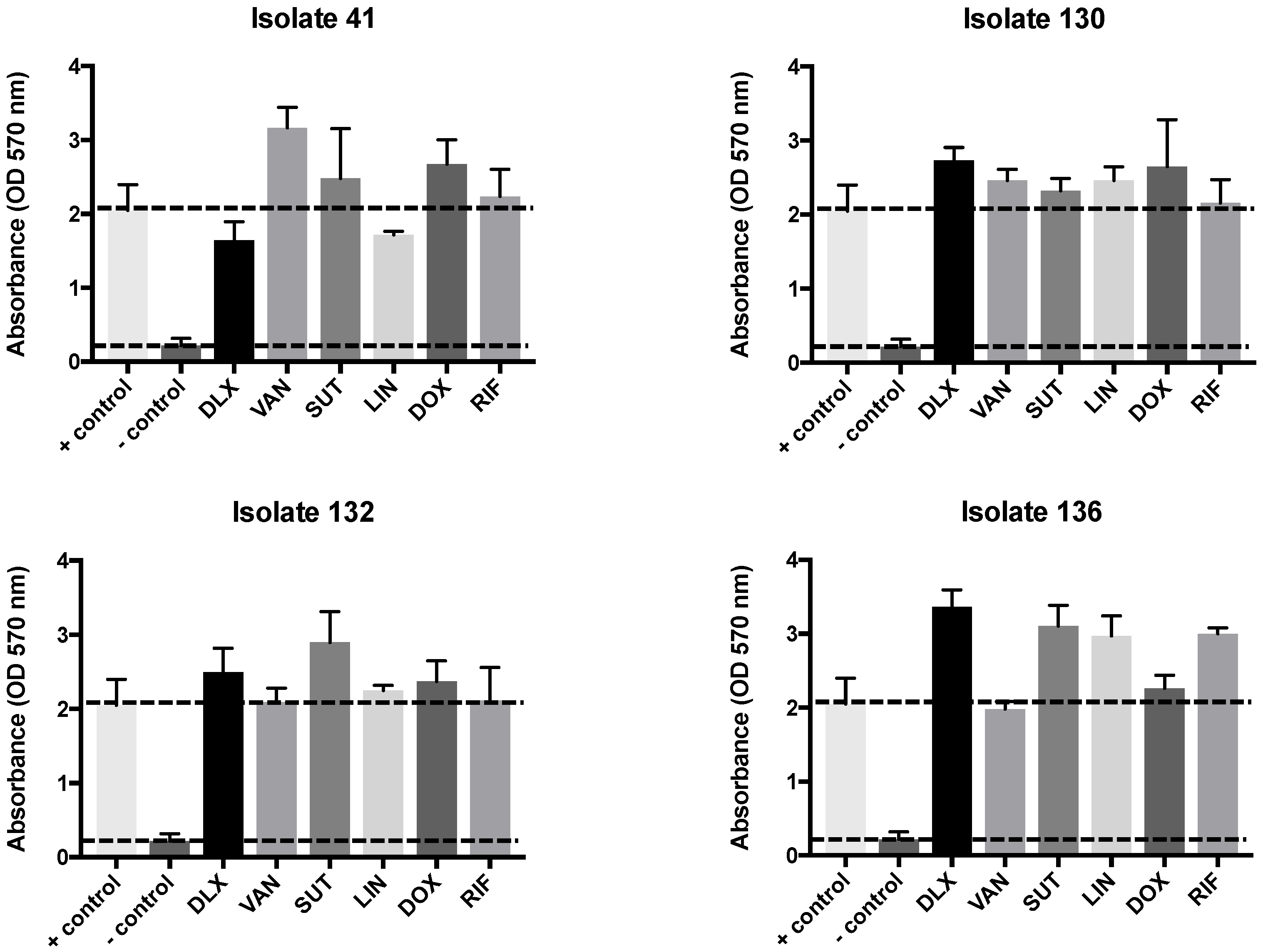
Figure 6.
MTT in biofilm with antibiotics against MRSA susceptible to delafloxacin in combinations. The dashed line represents the positive control and negative control. The number is the top represent the name of the isolate. SMX-TMP = Sulfamethoxazole / trimethoprim; DOX - Doxycycline; RIF - Rifampicin; DLX - Delafloxacin; VAN - Vancomycin; LNZ - Linezolid.
Figure 6.
MTT in biofilm with antibiotics against MRSA susceptible to delafloxacin in combinations. The dashed line represents the positive control and negative control. The number is the top represent the name of the isolate. SMX-TMP = Sulfamethoxazole / trimethoprim; DOX - Doxycycline; RIF - Rifampicin; DLX - Delafloxacin; VAN - Vancomycin; LNZ - Linezolid.
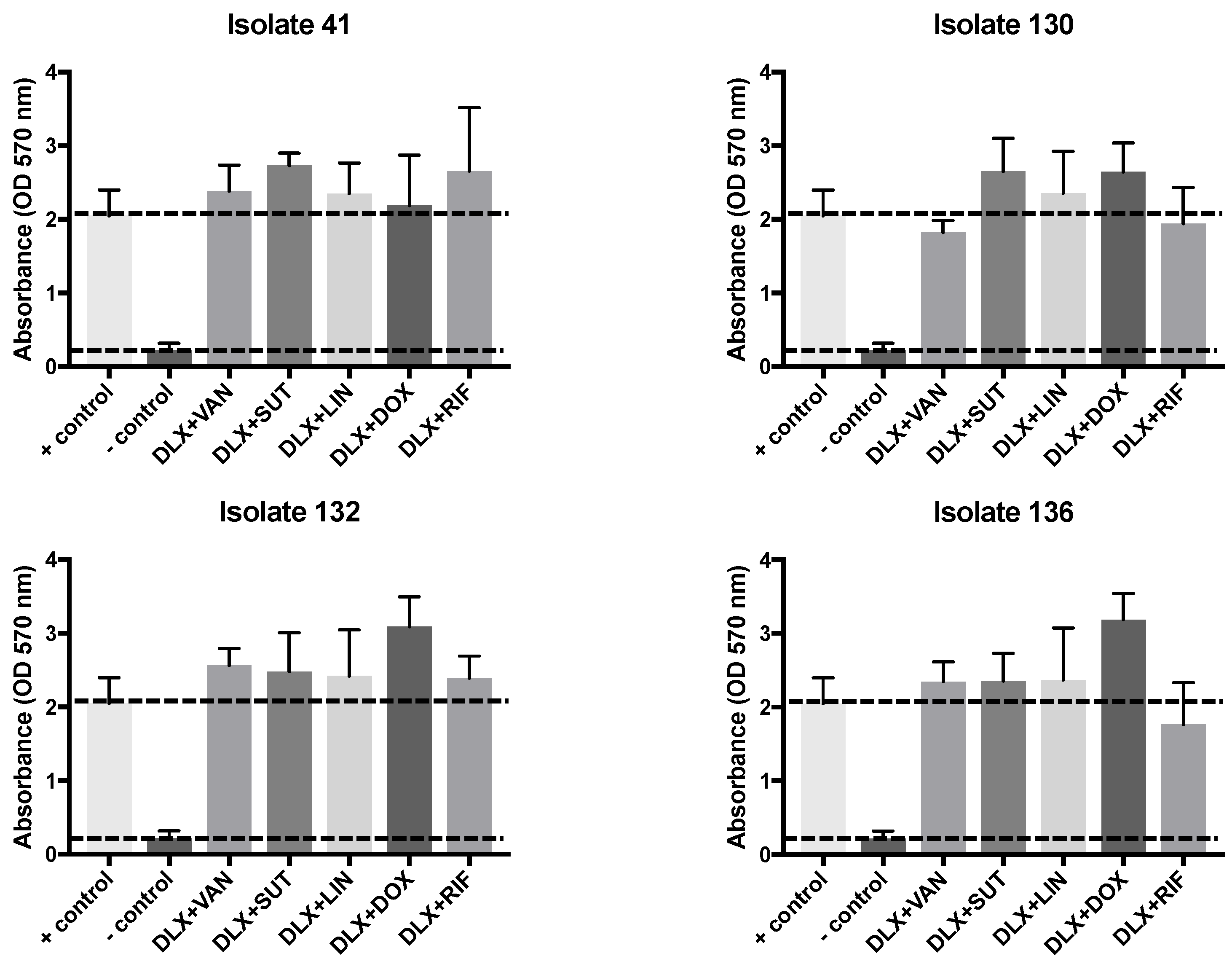

Table 1.
Minimal inhibitory concentration (MIC) of several antibiotics, including delafloxacin with different pH of the medium, and E-test. The comparison of pH 7.4 with 5.5 is described as “number of dilutions” in times (1x, 2x, 3x and 4x).
Table 1.
Minimal inhibitory concentration (MIC) of several antibiotics, including delafloxacin with different pH of the medium, and E-test. The comparison of pH 7.4 with 5.5 is described as “number of dilutions” in times (1x, 2x, 3x and 4x).
| Clinical Isolates | VAN | LNZ | SMX-TMP | DOX | RIF | DLX pH 7.4 | DLX pH 5.5 | DLX Etest | Dilutions pH 7.4 to 5.5 |
| (µg/mL) | (µg/mL) | (µg/mL) | (µg/mL) | (µg/mL) | (µg/mL) | (µg/mL) | (µg/mL) | ||
| 2 | 0.5 (S) | 2.0 (S) | 0.5 (S) | 0.125 (S) | 0.03 (S) | 2.0 (R) | 0.5 (R) | 2.0 (R) | 2x |
| 3 | 0.5 (S) | 2.0 (S) | 1.0 (S) | 0.125 (S) | 0.03 (S) | 2.0 (R) | 0.5 (R) | 2.0 (R) | 2x |
| 49 | 0.5 (S) | 2.0 (S) | 0.5 (S) | 0.125 (S) | 0.03 (S) | 2.0 (R) | 0.5 (R) | 2.0 (R) | 2x |
| 41 | 0.5 (S) | 1.0 (S) | 32 (R) | 4.0 (R) | 2.0 (R) | 0.25 (S) | 0.03 (S) | 0.125 (S) | 3x |
| 57 | 0.5 (S) | 2.0 (S) | 0.5 (S) | 0.125 (S) | 0.03 (S) | 2.0 (R) | 1.0 (R) | 2.0 (R) | 1x |
| 71 | 0.5 (S) | 4.0 (S) | 0.5 (S) | 0.125 (S) | 0.03 (S) | 2.0 (R) | 0.5 (R) | 2.0 (R) | 2x |
| 80 | 0.5 (S) | 2.0 (S) | 0.5 (S) | 0.125 (S) | 0.03 (S) | 2.0 (R) | 0.5 (R) | 2.0 (R) | 2x |
| 102 | 0.5 (S) | 4.0 (S) | 0.5 (S) | 0.25 (S) | 0.03 (S) | 2.0 (R) | 0.5 (R) | 2.0 (R) | 2x |
| 130 | 0.5 (S) | 4.0 (S) | 0.5 (S) | 0.125 (S) | 0.03 (S) | 0.004 (S) | 0.004 (S) | 0.002 (S) | 0 |
| 132 | 1.0 (S) | 2.0 (S) | 1.0 (S) | 0.5 (S) | 0.03 (S) | 0.25 (S) | 0.03 (S) | 0.19 (S) | 2x |
| 136 | 0.5 (S) | 2.0 (S) | 32 (R) | 1.0 (S) | 2.0 (R) | 0.25 (S) | 0.015 (S) | 0.125 (S) | 4x |
| 156 | 0.5 (S) | 2.0 (S) | 0.5 (S) | 0.125 (S) | 0.03 (S) | 2.0 (R) | 0.5 (R) | 2.0 (R) | 2x |
*SMX-TMP = Sulfamethoxazole / trimethoprim; DOX - Doxycycline; RIF - Rifampicin; DLX - Delafloxacin; VAN - Vancomycin; LNZ – Linezolid; S - Susceptible; R - Resistant.
Table 2.
Analysis of synergism by checkerboard of different antibiotics associated with delafloxacin. In gray the results showing potential synergism. ƩFIC is the sum of the fractional inhibitory concentrations. Synergism was indicated by ƩFIC < 0.5, indifference by ƩFIC between 0.5 and 4.0, and antagonism by ƩFIC > 4.0.
Table 2.
Analysis of synergism by checkerboard of different antibiotics associated with delafloxacin. In gray the results showing potential synergism. ƩFIC is the sum of the fractional inhibitory concentrations. Synergism was indicated by ƩFIC < 0.5, indifference by ƩFIC between 0.5 and 4.0, and antagonism by ƩFIC > 4.0.
| VAN | LNZ | SMX-TMP | DOX | RIF | |
| Isolate | ∑CIF | ∑CIF | ∑CIF | ∑CIF | ∑CIF |
| 2 | 1.5 | 1 | 1 | 1 | 1 |
| 3 | 0.75 | 1 | 1 | 1 | 1 |
| 49 | 1 | 1 | 1 | 1 | 1 |
| 41 | 0.5 | 1.25 | 1 | 1 | 1 |
| 57 | 1 | 1 | 1 | 0.4 | 1 |
| 71 | 1 | 1 | 1 | 1 | 1 |
| 80 | 1 | 1 | 1 | 1 | 1 |
| 102 | 1 | 1 | 1 | 1 | 1 |
| 130 | 1.25 | 1 | 2 | 1.5 | 2 |
| 132 | 1 | 1 | 2 | 0.5 | 1 |
| 136 | 1.25 | 1 | 1 | 1.5 | 1 |
| 156 | 1 | 1 | 1 | 1 | 1 |
*SMX-TMP = Sulfamethoxazole / trimethoprim; DOX - Doxycycline; RIF - Rifampicin; DLX - Delafloxacin; VAN - Vancomycin; LNZ - Linezolid.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



