
Submitted:
26 August 2024
Posted:
27 August 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background: Early risk stratification tools for COVID-19 patients were indicated but little is known about their ability to effectively detect clinical deterioration among COVID-19 patients. Objectives: To assess the prognostic accuracy of NEWS2 in predicting severe morbidity and mortality in hospitalization for COVID-19 patients. Methods: A prospective cohort study was performed among adult patients with a confirmed diagnosis of COVID-19 who were admitted to the inpatient units at COVID-19 Martyrs Medical Military Complex and Palestinian Red Crescent Society Hospital, located at Nablus, Palestinian Authority. NEWS2 scores were measured at admission, on 6, 12, 24, and 48 hours after their admission to the hospital using Receiver Operating Characteristic Curves (ROC). Results: Overall, 192 adult COVID-19 patients aged 25-94 years (mean=62.1, SD=13.9) were enrolled. Of those, 49.0% were males, 47.4% were vaccinated, and 53.6% were with diabetes. The mean NEWS scores during the patient’s hospital stay were excellent predictors of mechanical ventilation, admission to the ICU, and mortality, as indicated by an AUROC of 0.94 (95% CI: 0.88-1.00, P<0.001), 0.91 (95% CI: 0.87-0.96, P<0.001) and 0.96 (95% CI: 0.92-1.00, P<0.001), respectively. The classification of 192 patients into NEWS score categories indicated that 12.5% were classified as high-risk at admission. Conclusion: The NEWS2 had moderate sensitivity and specificity in predicting the deterioration of patients with COVID-19. Our findings support the utility of NEWS2 monitoring as a sensitive approach for initially assessing COVID-19 patients. It could be helpful to improve predictive performance by supplementing the score parameters with additional measures besides the clinical judgment.
Keywords:
NEWS2
; COVID-19
; Sensitivity
; Predictive
1. Introduction
COVID-19 cases have been reported in Wuhan, China since December 2019. In March 2020, due to the global spread and severity of the cases, the WHO identified the situation as a COVID-19 pandemic [1]. The National Early Warning Score 2 (NEWS2) was designed to assess patients with COVID-19 and to track the progression of the disease, as the virus has diverse clinical presentations, ranging from asymptomatic transmission to life-threatening [2,3,4]. Clinical characteristics, such as increased respiratory rate, elevated temperature, and low systolic blood pressure may require respiratory support such as non-invasive pressure support, invasive ventilation, or critical care admission, and this has threatened the capacity and workflow of emergency departments (EDs) and intensive care units (ICU) in hospitals worldwide [5,6]. Therefore, identifying the disease severity for these patients early is important, however, failure to recognize a patient's deteriorating condition in a hospital setting may result in life-threatening conditions, a lengthened hospital stay, and significant disabling consequences that may lead to unanticipated hospital admissions or readmissions, increasing hospital morbidity and mortality [7]. NEWS2 seems to be a robust predictor of COVID-19 inpatient hospital deaths [8,9,10,11,12]. This is extremely important because it validates the ability of NEWS2 to support clinical judgment while also providing a standardized communication tool in a short time frame, taking into account the limited resources and operational demands that hospitals faced during the COVID-19 pandemic outbreak in the emergency phase [11]. Consequently, patients facing clinical deterioration or at risk of deterioration would receive an initial assessment on time. NEWS2 is associated with reduced mortality rates and deferred medical interventions, however, at times numerical scores caused overestimating at the expense of holistic clinical analysis and the situational context [3,13,14].
The integration of NEWS2 scores within the broader clinical assessment is vital, considering the myriad factors influencing patient health evaluations. Such scores should be integrated with condition-specific observations that could also necessitate heightened clinical intervention. Patient engagement and understanding are fundamental in both the assessment process and in decision-making [13,15]. The use of NEWS2 has extended to emergency departments and pre-hospital settings, buoyed by growing evidence and experiential learning [16,17]. The National Institute for Health and Care Excellence recommends the recording of these vital parameters at hospital admission or during initial evaluations with a recent audit of 156 hospitals demonstrating compliance within 30 minutes in 77% of cases [13,18]. Escalation thresholds signal the need for more intensive clinical evaluation to respond to illness severity, risk of deterioration, or change in patient status. Accordingly, we explored the prognostic accuracy of NEWS2 in predicting severe morbidity and mortality in hospitalization for COVID-19 patients.
2. Materials and Methods
2.1. Study Design and Population
A prospective cohort study was performed among adult patients who were admitted to the inpatient units at COVID-19 Martyrs Medical Military Complex and Palestinian Red Crescent Society Hospital, which also functioned as a certified testing and treatment facility for COVID-19 located at Nablus, Palestinian Authority.
2.2. Inclusion and Exclusion Criteria
All adult patients (>18 years of age) with a confirmed diagnosis of COVID-19 by a positive nasal and/or oropharyngeal PCR swab were included. Patients who were younger than 18 years old, pregnant women, those with spinal cord injuries, non-COVID patients, and patients who were readmitted to the unit during the study were excluded from the study. These criteria were developed following the Royal College of Physicians' 2017 standards.
2.3. Data Collection and Clinical Definitions
We collected the patient's physiological measurements (blood pressure, heart rate, respiratory rate, oxygen saturation, temperature, and confusion level) from admission until discharge (death/alive). We defined severe morbidity by one of the following: initiation of respiratory support (low flow oxygen, high flow nasal cannula, non-invasive positive pressure ventilation, or invasive mechanical ventilation), admission to the ICU, or in-hospital death. When none of these events occurred, observations were recorded up to the point of discharge. NEWS2 scores were measured at admission, on 6, 12, 24, and 48 hours after their admission to the hospital.
2.4. Statistical Analysis
The ability of NEWS2 to predict outcomes was examined using Receiver Operating Characteristic Curves (ROC), Sensitivity, specificity, and likelihood ratios were pooled by using logistic and linear regression. ANOVA tests were conducted to evaluate how the implementation affected various outcomes. A two-sided P value <0.05 was considered statistically significant. Data were analyzed using SPSS version 28 (IBM, Armonk, New York, USA).
2.5. Ethical Consideration
The study protocol was approved by the Institutional Review Board (IRB) at An-Najah National University (protocol number 2022-25; approval date: March 2022). All procedures were performed following local guidelines and regulations. The participants signed an informed consent form, authorizing their participation in the study as well as the publication of its findings. Ethics approval and consent to participate in this study was carried out following the Declaration of Helsinki.
3. Results
Overall, 192 adult COVID-19 patients aged 25-94 years (mean=62.1, SD=13.9) were enrolled. Of those, 49.0% were males, 47.4% were vaccinated, 53.6%, 10.4%, and 5.7% were with diabetes, chronic kidney disease, and cancer, respectively.
Table 1 and Figure 1, Figure 2 and Figure 3 indicated AUROC, optimal cut-off, sensitivity, and 1-specificity values of all the NEWS scores. The mean NEWS score calculated during the patient’s hospital stay was a fair predictor of the need for low flow O2 as indicated by an AUROC of 0.74 (95% CI: 0.64-0.84, P < 0.001), with a cutoff point of 3.7 that accurately predict 52.7% of the low flow O2 cases with a probability of false-positive of 19.0%. However, the mean NEWS scores during the patient’s hospital stay were good and excellent predictors of the need for high flow o2 and mechanical ventilation, respectively as indicated by an AUROC of 0.87 (95% CI: 0.82-0.92, P < 0.001) and 0.94 (95% CI: 0.88- 1.00, P < 0.001), respectively, with cutoff points of 5.0 and 6.3 that accurately predict 56.1% and 88.2% of the high flow o2 and mechanical ventilation, respectively with a probability of false-positive of 9.6% and 10.3% (Table 1).
Using ROC curve analyses, we found that the mean NEWS scores during the patient’s hospital stay were excellent predictors of admission to the ICU (Figure 1) and mortality (Figure 2) as indicated by an AUROC of 0.91 (95% CI: 0.87-0.96, P < 0.001) and 0.96 (95% CI: 0.92-1.00, P < 0.001), respectively, with cutoff points of 4.7 and 5.9 that could accurately predict 70.2% and 87.5% of ICU admissions and mortality with a probability of false-positive of 10.4% and 8.9%, respectively. However, the mean NEWS score during the patient’s hospital stay was a fair predictor of staying in the hospital for six or more days as indicated by an AUROC of 0.78 (95% CI: 0.72-0.85, p < 0.001), with a cutoff point of 4.5 that accurately predict 55.0% of the cases with a probability of false positive of 18.8% (Figure 3).
Table 2 shows the classification of patients into NEWS score categories as low (need a monitor every 4-6 hours), medium (need a monitor every 1 hour), and high-risk (need a monitor continuously) based on their NEWS scores measured at admission, and on the other time intervals (6, 12, 24, and 48 hours) after their admission to the hospital. Of the 192 patients, 112 (58.3%) were classified as low-risk, 56 (29.2%) were classified as medium-risk, and 24 (12.5%) were classified as high-risk at admission.
4. Discussion
In the current study, we explored the prognostic accuracy of NEWS2 in predicting severe morbidity and mortality in hospitalization for COVID-19 patients. In terms of predicting the combined outcome of the requirement for intense respiratory assistance, ICU admission, or in-hospital mortality, the NEWS2 commonly displays good discrimination. To begin with the NEWS2, an updated version of the NEWS varies from the original NEWS in that it includes a new SpO2 scoring scale for use in patients with hypercapnic respiratory failure. Oxygen supplementation is a risk factor for coronaviruses [19]. Additionally, this study's results showed that the mean NEWS scores during the patient’s hospital stay were a fair predictor of the need for low-flow O2, a good predictor of the need for high-flow O2, and an excellent predictor of the need for mechanical ventilation. These findings were consistent with a 2020 study that demonstrated that the oxygen saturation level had a good prognostic performance for predicting death in patients with COVID-19 infection [20]. Thus, benefitting from adding a specific scale for patients with hypercapnic respiratory failure, the NEWS2 showed better sensitivity and discrimination than the original NEWS. The high sensitivity of the NEWS2 supports its use as an effective tool for accurately assessing COVID-19 patients upon hospital admission.
In this study, it was also found that the mean NEWS scores during the patient’s hospital stay were a fair predictor of a hospital stay of six days or more, and an excellent predictor of admission to the ICU, and mortality as indicated by an AUROC. Like worldwide hospital policies, most ICU admissions were estimated to take 2.0 days from hospital admission. These findings were in line with a few small cohort studies that looked at the predictive value of baseline NEWS2 and other clinical scoring systems in predicting clinical outcomes in COVID-19 patients based on a single measurement at the time of hospital admission. In a Chinese study of 654 COVID-19 admissions, the baseline NEWS2 had a better prediction of mortality than CURB-65 (0.85 [0.81-0.89]) and performed better than qSOFA (0.73 [0.69-0.78] with an AUROC of 0.81 (95 % CI 0.77-0.85) [21]. In a study conducted in Korea of 110 COVID-19 inpatients, using a baseline threshold of NEWS, over or equal to 5 indicated a predictive value of 0.98 but a positive predictive value of 0.59 for a future event [22]. The baseline (original) NEWS anticipated an event (defined as ICU admission and/or death) with AUROC 0.92 (95 % CI 0.84–1.00) vs 0.76 (0.62–0.90) for qSOFA.
The baseline NEWS2 had an AUROC of 0.79 (95% CI 0.66–0.91) in a Norwegian study of 66 inpatients [23]. It predicted a composite adverse outcome of inpatient death and/or ICU admission. This was in comparison with qSOFA's AUROC of 0.62 (0.45–0.81) and CURB-65's AUROC of 0.58 (0.41–0.76), respectively. The prognostic qualities of NEWS2 for admission to the intensive care unit were similarly established in 68 patients with severe COVID-19 in 2020 (AUROC = 0.90 (CI, 0.82-0.97) [24,25]. "Serious events" were classified as any of the following occurring while the patient was hospitalized: death, unexpected transfer to an ICU, or the start of non-invasive ventilation, with equivalent AUROC scores for predicting serious events of 0.837 (0.748-0.943) for admission NEWS and 0.846 (0.735-0.939) for admission using NEWS modified by age [10,24].
The main strengths of our study are: a large sample size, we have consecutively included all COVID-19 patients admitted from the start of the outbreak including all components of the NEWS2 score; the NEWS2 scores were measured at admission, on 6, 12, 24 and 48 hours after their admission to the hospital, and it is the first study in the Palestinian Authority that examine the prognostic accuracy of NEWS2 in predicting severe morbidity and mortality in hospitalization for COVID-19 patients. However, the main limitation of our study is the patients with severe disease might have been more severely ill already at admission.
5. Conclusions
The mean NEWS scores during the patient’s hospital stay were excellent predictors of admission to the ICU and mortality with a moderate sensitivity and specificity in predicting severe morbidity and mortality in hospitalization for COVID-19 patients. Our findings support the utility of NEWS2 monitoring as a sensitive approach for initially assessing COVID-19 patients. It could be helpful to improve predictive performance by supplementing the score parameters with additional measures (such as laboratory blood tests and others) besides the clinical judgment. Our findings can contribute to a better understanding of the benefits of using NEWS2 in patients with COVID-19, which could be useful for implementing its use in clinical practice.
Author Contributions
Conceptualization: M.T., J.Q., W.N.; Methodology: M.T., J.Q., I.M.T., W.N.; Formal analysis and investigation: J.Q., I.M.T., W.N.; Writing—original draft preparation: M.T., J.Q., W.N.; Writing—review and editing: W.N.; Project administration, M.T.; Supervision: W.N. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board at An-Najah National University (protocol number 2022-25; approval date: March 2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patients to publish this paper.
Data Availability Statement
All data generated or analyzed during this study are included in this article. Further inquiries can be directed to the corresponding author.
Acknowledgments
We thank the staff at An-Najah National University and the Clinical Research Center of An-Najah National University for allowing us to conduct this study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Benlghazi, A.; Benali, S.; Bouhtouri, Y.; Belouad, M.; Massoudi, H.; Kouach, J. SARS-CoV-2 infection in pregnant women; epidemiological, clinical, biological and evolutionary profile in 16 cases: the COVID-19 experience in the Moroccan Military Hospital in Benslimane. Pan Afr Med J, 2021, 38, 384. [CrossRef]
- Jebril, N. World Health Organization declared a pandemic public health menace: A systematic review of the coronavirus disease 2019 “covid-19.” 2020, Available at SSRN 3566298. [CrossRef]
- Royal College of Physicians. National Early Warning Score (NEWS) 2. Standardizing the assessment of acute-illness severity in the NHS. 2017, Available from: https://www.rcplondon.ac.uk.
- Connell, C.J.; Endacott, R.; Cooper, S. The prevalence and management of deteriorating patients in an Australian emergency department. Australas Emerg Care. 2021, 24, 112-120. [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497-506. [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet 2020, 395, 1054-1062. [CrossRef]
- Hammond, N.E.; Spooner, A.J.; Barnett, A.G.; Corley, A.; Brown, P.; Fraser, J.F. The effect of implementing a modified early warning scoring (MEWS) system on the adequacy of vital sign documentation. Aust Crit Care 2013, 26, 18-22. [CrossRef]
- Marius, M.; Hakon, I.H.; Aune, T.A.; Lyster, A.E.; Stale, N.; Arnljot, T. National Early Warning Score 2 (NEWS2) on admission predicts severe disease and in-hospital mortality from Covid-19 – a prospective cohort study. Scand J Trauma Resusc Emerg Med. 2020, 28, 66. [CrossRef]
- Sze, S.; Pan, D.; Williams, C.M.L.; Wong, N.; Sahota, A.; Bell, D.; Tang, J.W.; Wiselka, M.; Stephenson, I.; Pareek, M. Letter to the Editor: Variability but not admission or trends in NEWS2 score predicts clinical outcome in elderly hospitalized patients with COVID-19. J Infect. 2021, 82, 159-198. [CrossRef]
- Baker, K.F.; Hanrath, A.T.; Schim, van der Loeff, I.; Kay, L.J.; Back, J.; Duncan, C.J. National Early Warning Score 2 (NEWS2) to identify inpatient COVID-19 deterioration: a retrospective analysis. Clin Med (Lond). 2021, 21, 84–89. [CrossRef]
- Rigoni, M.; Torri, E.; Nollo, G.; Delle Donne, L.; Cozzio, S. NEWS2 is a valuable tool for appropriate clinical management of COVID-19 patients. Eur J Intern Med. 2021, 85, 118-120. [CrossRef]
- Robert, G.; Marie-Claire, H.; Jessie, M.; Darran, R.; Victoria, R.; Paul, M. qSOFA, SIRS and NEWS for predicting inhospital mortality and ICU admission in emergency admissions treated as sepsis. Emerg Med J. 2018, 35, 345–349. [CrossRef]
- Welch, J.; Dean, J.; Hartin, J. Using NEWS2: an essential component of reliable clinical assessment. Clin Med (Lond). 2022, 22, 509-513. [CrossRef]
- Scott, L.J.; Redmond, N.M.; Tavaré, A.; Little, H.; Srivastava, S.; Pullyblank, A. Association between National Early Warning Scores in primary care and clinical outcomes: an observational study in UK primary and secondary care. Br J Gen Pract. 2020, 70, e374–380. [CrossRef]
- Holland, M.; Kellett, J. A systematic review of the discrimination and absolute mortality predicted by the National Early Warning Scores according to different cut-off values and prediction windows. Eur J Intern Med. 2022, 98, 15–26. [CrossRef]
- Prytherch, D.R.; Smith, G.B.; Schmidt, P.E.; Featherstone, P.I. ViEWS–Towards a national early warning score for detecting adult inpatient deterioration. Resuscitation. 2010, 81, 932–937. [CrossRef]
- Kovacs, C.; Jarvis, S.W.; Prytherch, D.R.; Meredith, P.; Schmidt, P.E.; Briggs, J.S.; Smith, G.B. Comparison of the National Early Warning Score in non-elective medical and surgical patients. Br J Surg. 2016, 103, 1385–1393. [CrossRef]
- National Institute for Health and Care Excellence. Acutely ill patients in hospital: Recognition of and response to acute illness in adults in hospital: Clinical guideline [CG50]. NICE, 2007.
- Sun, Q.; Qiu, H.; Huang, M.; Yang, Y. Lower mortality of COVID-19 by early recognition and intervention: Experience from Jiangsu Province. Annals of Intensive Care. 2020, 10. [CrossRef]
- Liu, F.Y.; Sun, X.L.; Zhang, Y.; Ge, L.; Wang, J.; Liang, X.; Li, J.F.; Wang, C.L.; Xing, Z.T.; Chhetri, J.K.; et al. Evaluation of the risk prediction tools for patients with coronavirus disease 2019 in Wuhan, China: A single-centered, retrospective, observational study. Crit Care Med. 2020, 48. e1004-e1011. [CrossRef]
- Fan, G.; Tu, C.; Zhou, F.; Liu, Z.; Wang, Y.; Song, B.; Gu, X.; Wang, Y.; Wei, Y.; Li, H.; et al. Comparison of severity scores for COVID-19 patients with pneumonia: a retrospective study. Eur Respir J. 2020, 56, 2002113. [CrossRef]
- Jang, J.G.; Hur, J.; Hong, K.S.; Lee, W.; Ahn, J.H. Prognostic Accuracy of the SIRS, qSOFA, and NEWS for Early Detection of Clinical Deterioration in SARS-CoV-2 Infected Patients. J Korean Med Sci. 2020, 35, e234. [CrossRef]
- Myrstad, M.; Ihle-Hansen, H.; Tveita, A.A.; Andersen, E.L.; Nygard, S.; Tveit, A.; Berge, T. National Early Warning Score 2 (NEWS2) on admission predicts severe disease and in-hospital mortality from Covid-19 - a prospective cohort study. Scand J Trauma Resusc Emerg Med. 2020, 28, 66. [CrossRef]
- Martín-Rodríguez, F.; López-Izquierdo, R.; Del Pozo Vegas, C.; Delgado-Benito, J.F.; Carbajosa-Rodríguez, V.; Diego-Rasilla M.N.; Martín-Conty, J.L.; Mayo-Iscar, A.; Otero de la Torre, S.; Méndez-Martín, V.; et al. Accuracy of National Early Warning Score 2 (NEWS2) in Prehospital Triage on In-Hospital Early Mortality: A Multi-Center Observational Prospective Cohort Study. Prehosp Disaster Med. 2019, 34, 610-618. [CrossRef]
- Aliberti, M.J.R.; Covinsky, K.E.; Garcez, F.B.; Smith, A.K.; Curiati, P.K.; Lee, S.J.; Dias, M.B.; Melo, V.J.D.; Rego-Júnior, OFD.; Richinho, V.P.; et al. A fuller picture of COVID-19 prognosis: the added value of vulnerability measures to predict mortality in hospitalized older adults. Age Ageing. 2021, 50, 32-39. [CrossRef]
Figure 1.
ROC curve for patients admitted to the ICU using mean NEWS scores.
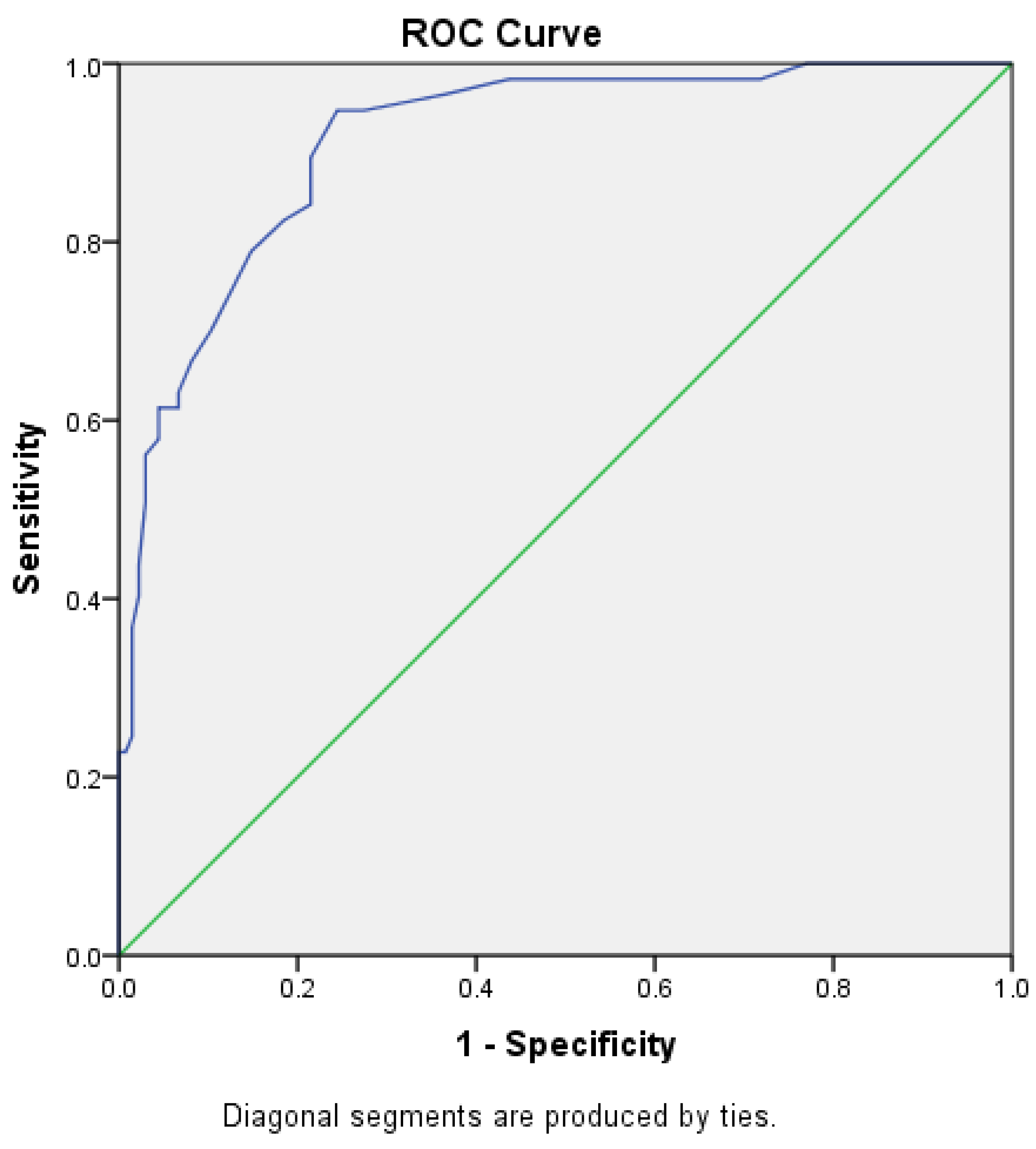
Figure 2.
ROC curve for patient's mortality using mean NEWS scores.
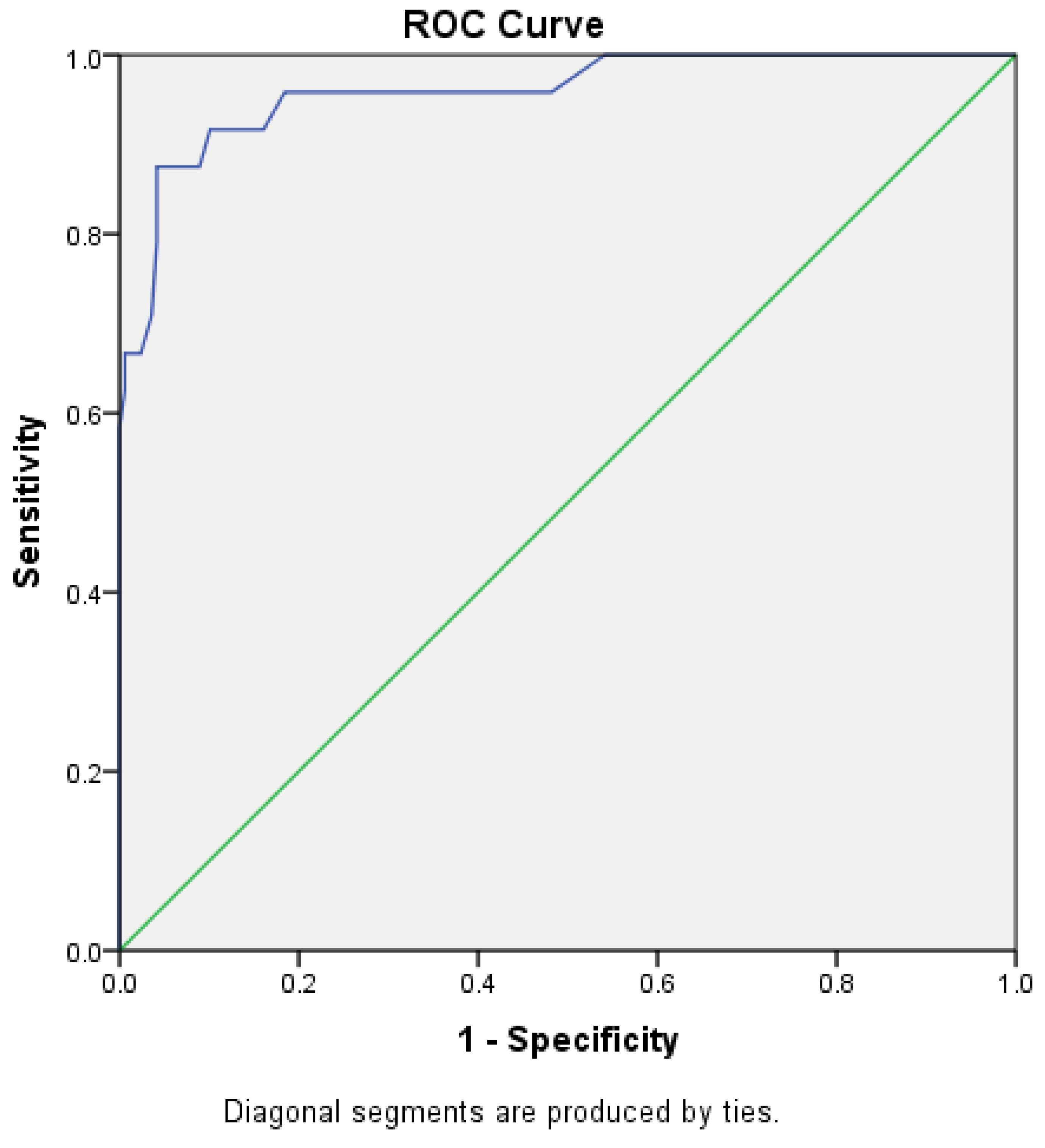
Figure 3.
ROC curve for patients staying in the hospital for 6 days or more using mean NEWS scores.
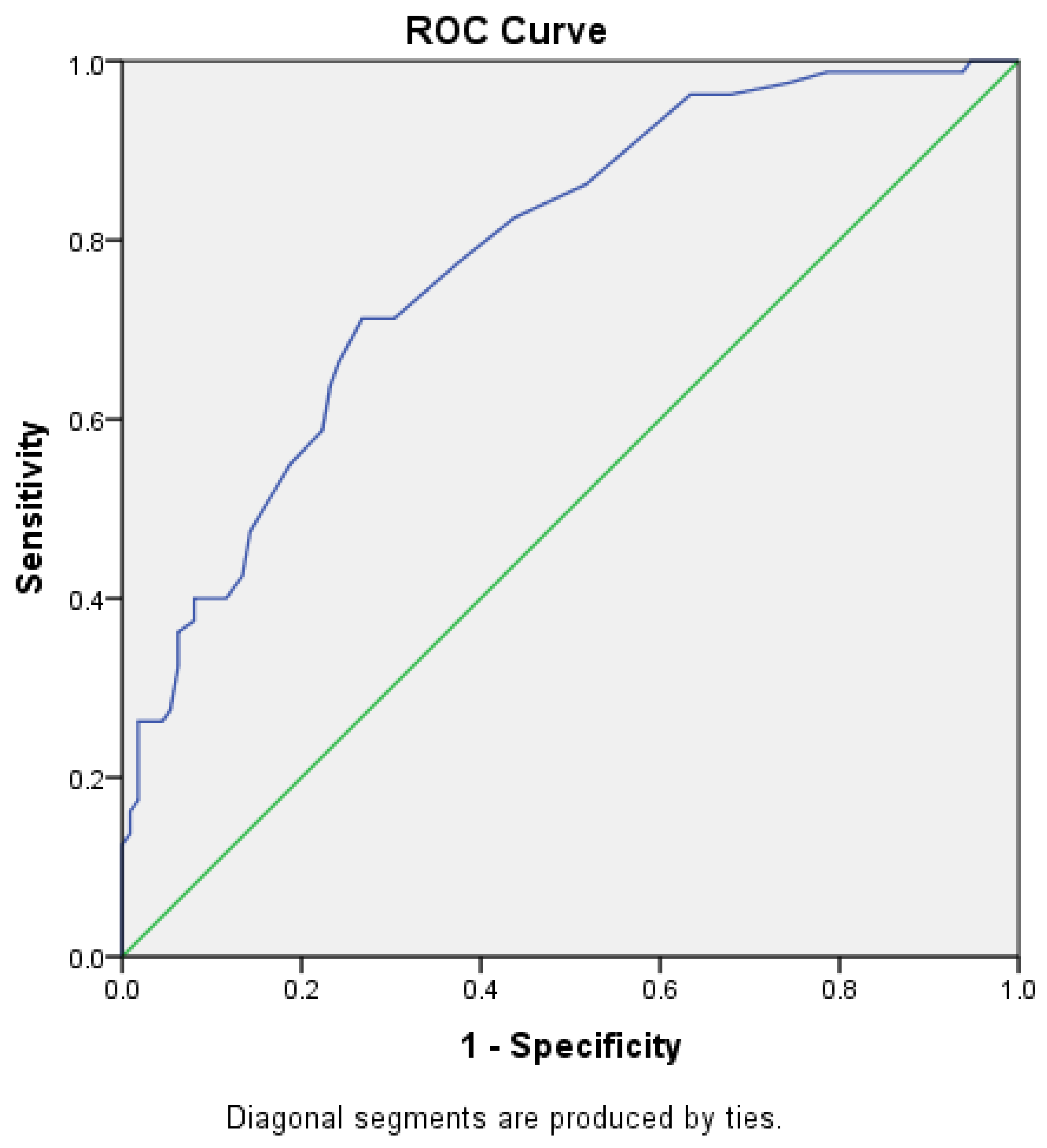

Table 1.
Early Warning Scores on predicting severe morbidity and mortality in hospitalization for COVID-19 patients-ROC curve analyses.
Table 1.
Early Warning Scores on predicting severe morbidity and mortality in hospitalization for COVID-19 patients-ROC curve analyses.
| Variable | 95% CI | |||||||
|---|---|---|---|---|---|---|---|---|
| AUC | SE | P | Lower | Upper | Proposed cutoff point | Sensitivity | 1 - specificity | |
| Low flow O2 | 0.74 | 0.05 | < 0.001 | 0.64 | 0.84 | 3.7 | 0.527 | 0.190 |
| High-flow nasal cannula | 0.87 | 0.03 | < 0.001 | 0.82 | 0.92 | 5.0 | 0.561 | 0.096 |
| Mechanical ventilation | 0.94 | 0.03 | < 0.001 | 0.88 | 1.00 | 6.3 | 0.882 | 0.103 |
| Hospital stay ≥ 6 days | 0.78 | 0.03 | < 0.001 | 0.72 | 0.85 | 4.5 | 0.550 | 0.188 |
| ICU | 0.91 | 0.02 | < 0.001 | 0.87 | 0.96 | 4.7 | 0.702 | 0.104 |
| Mortality | 0.96 | 0.02 | < 0.001 | 0.92 | 1.00 | 5.9 | 0.875 | 0.089 |
Table 2.
Classification of patients into NEWS score categories.
| NEWS2 scores measured at admission | NEWS2 scores measured at 6 hours | NEWS2 scores measured at 12 hours | NEWS2 scores measured at 24 hours | NEWS2 scores measured after 48 hours | Based on the average NEWS score | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| NEWS score category | n | % | n | % | n | % | n | % | n | % | n | % |
| Low-risk (monitor every 4-6 h) | 112 | 58.3 | 114 | 59.4 | 126 | 65.6 | 137 | 71.4 | 154 | 80.2 | 143 | 74.5 |
| Medium-risk (monitor every 1 h) | 56 | 29.2 | 45 | 23.4 | 33 | 17.2 | 28 | 14.6 | 16 | 8.3 | 26 | 13.5 |
| High-risk (monitor continuously) | 24 | 12.5 | 33 | 17.2 | 33 | 17.2 | 27 | 14.1 | 22 | 11.5 | 23 | 12.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



