
Submitted:
27 August 2024
Posted:
27 August 2024
You are already at the latest version
Abstract
Bioimpedance analysis (BIA) is a validated non-invasive technique already proven to be useful for the diagnosis, prognosis, and management of body fluids in subjects with heart failure (HF) and chronic kidney disease (CKD). Although BIA has been widely employed for research purposes, its clinical application is still not fully widespread. The aim of this review is to provide a comprehensive overview of the state of art of BIA utilization by analysing the clinical benefits, limitations, and the potential future developments in this clinically unexplored field.
Keywords:
Bioimpedance Analysis
; Heart Failure
; Kidney Disease
; Chronic Patients
; Cardiology
; Nephrology
; Diagnostics
; Prognosis
1. Introduction
The human body behaves like a complex electric circuit [1,2]. This concept has been at the base of extensive research to understand how biological tissues respond to electrical stimuli and various models have been developed with the purpose to estimate the body composition [1,2,3,4]. A promising scientific area of research has emerged in the past 20 years, leading to the development of “Bioimpedance Analysis” (BIA) [3,4,5]. BIA exploits the set of electrical properties that characterizes the opposition to an electric current flowing through the biological tissue [3,4,5].
The main principle of BIA is based on building models that approximate the human body to an electric circuit with resistors and capacitors, studying the relationship between alternating electrical currents at different frequencies (i.e. single or multiple), body volume, and hydration status (HS) [3,6]. The raw measures of Resistance (R), Reactance (Xc) and Phase Angle (PA) are then employed to estimate the distribution of total body water (TBW) composition, comprising the measurements of intracellular water (ICW) and extracellular water (ECW) but also, fat mass (FM) and fat free mass (FFM) [6,7,8]. Additionally, a set of hemodynamic parameters such as cardiac output and systemic vascular resistance can also be estimated with BIA [9].
BIA holds the potential to improve patient care, especially for conditions such as heart failure (HF) and end-stage kidney disease (ESKD), by supporting in the assessment of the health status (HS) of such patients [10,11]. In facts, even if the two conditions often exhibit a different etiology or initial presentation, their clinical course is similar, presenting recurrent decompensation events caused by episodes of congestion or at the opposite volume depletion [12]. The two diseases coexist in almost 40-60% of the cases and in many situations those patients are affected by the so called cardiorenal syndrome (CRS), leading to poor prognosis and repeated unplanned hospitalizations [13]. In detail, CRS is a complex pathophysiological disorder involving the heart and kidneys in which either an acute or chronic dysfunction of one organ may induce dysfunction of the other [13].
Cardiovascular diseases are the leading cause of mortality in chronic kidney disease (CKD) patients, reaching 9-fold increased risk in hemodialysis (HD) patients compared to age-matched in general population [14]. Moreover, patients affected by CRS are more prone to worsening renal function and acute kidney injury (AKI) than CKD patients without cardiovascular disease [14,15].
Although BIA technology has been widely investigated, its application is still limited due to many factors and far from being integrated in the clinical routine setting [12,16].
The aim of this narrative review is to revise the current clinical benefits of using BIA in HF and CKD patients by first investigating studies exploring the hardest endpoints, such as the prediction of mortality and acute decompensation events, then addressing the main pitfalls of BIA technique.
Therefore, our review will not focus in detail on the technical aspects and methodologies of BIA as this information has been previously and extensively published [10,11,17].
Finally, we aim to identify what could be improved or changed considering future paths of development in the field.
2. BIA Methods
BIA techniques differ on the number of frequencies employed, being either single or multiple, so that they are commonly classified into single frequency (SF-BIA), generally measured at 50 kHz, and multiple frequency (MF-BIA), ranging between 5 and 1000 kHz [11]. An in-depth description of these methods is beyond the scope of our narrative review; therefore, in this section, we will briefly describe the main concepts to highlight the technical advantages and disadvantages of the techniques.
Single Frequency-BIA (SF-BIA) and BIVA
SF-BIA is based on the inverse relationship between the measured impedance and TBW, which serves as the conductive pathway for the electric current [11].
Among the SF-BIA method, bioimpedance vectorial analysis (BIVA) approach have attracted the attention of the clinicians due to the ability of accurately classify the hydration status (expressed as normohydration or overhydration) [3]. By measuring the R and Xc of the current, BIVA can generate a vector in a two-dimensional impedance plane [3] which is then analyzed in respect to population-specific reference ellipses to infer information about an individual’s body composition and hydration status [3]. The process is non-invasive, quick, and can be performed in various settings, making it a versatile tool for the diagnosis and risk stratification of chronic and acute patients at higher risk of dehydration [3].
Multiple Frequency-BIA (MF-BIA) and BIS
The examination of BIA acquired at more than two frequencies is referred to as MF-BIA. This method relies on the observation that extracellular fluid (ECF) and TBW can be evaluated by subjecting them to low and high-frequency electric currents, respectively [11].
In case 50 frequencies are applied, it is referred to as bioimpedance spectroscopy (BIS). The values obtained are translated onto a so-called Cole-Cole plot, allowing the extrapolation of resistances at zero (R0) and infinite (R∞) frequency. This assumes that at the lowest frequencies, the current primarily flows through the ECF, while at high frequencies, it traverses ICW and ECW [11].
While SF-BIA is highly accurate for the assessment of TBW, for patients with highly altered hydration status, MF-BIA has been shown to provide a more accurate prediction of ECF compared to the SF-BIA [17]. Nevertheless, among elderly individuals, the MF-BIA method exhibits reduced sensitivity in identifying fluid shifts between ECF and intracellular fluid (ICF) [17].
The Devices
In clinical practice, two BIA measuring methods have been primarily developed: the “external band electrode method” and the “implanted device lead method” [10]. The prevailing approach for measuring total body compartments is the hand-to-foot external band method [10] which was originally introduced by Hoffer and revised by Nyboer [18,19]. The approach aims to decrease the contact impedance between the skin and the electrodes and was validated or the first time by Lukaski on 140 healthy adults [2]. In this pioneer study, the authors avoided electrode polarization and reduced the effects of skin impedance by employing four electrodes: one pair for passing the current through the body and the other to detect the resulting voltage [20]. In detail, the electrodes are placed on the dorsal side of the hands and feet, with a distance of at least 3-5 cm between the signaling and detection electrodes [20]. Tetra-polar measurements are taken on a supine subject for generally 15 minutes to allow the stabilization of the body fluids [20]. Ideally, before placing the electrodes, the surface should be cleaned with alcohol to avoid measurement bias [20].
Another way to utilize the external band electrode method is through thoracic BIA, which uses two pairs of external electrodes placed on the body surface on the thorax [21]. This method exploits the phenomenon whereby variations in fluid volume and blood flow determine changes in the frequency of propagating waves rather than in the amplitude of the signal [21,22]. Therefore, detecting the phase shift of electrical currents (known as bioreactance) also allows the assessment of cardiac output and vascular resistance [21,22]. The method is also known as impedance cardiography (ICG) [22].
A different method is based on the assessment of intrathoracic impedance by measuring the impedance between the device case, typically implanted in the left pectoral region, and the lead in the right ventricle [23]. Impedance has long been used to check for lead integrity in pacemakers or defibrillator devices and intrathoracic bioimpedance measurements have been also developed and integrated into cardiac implantable electronic devices (CIED) to check volume status [24]. In fact, changes in impedance can be determined across two relatively fixed points, thus minimizing distortion, or variations in electrode placement. Therefore, the primary purpose of implanted device–based BIA is to monitor over time the clinical status in chronically ill patients as an additional function of the implanted device [24,25].
Although BIA technology has been widely investigated, its application is, to this day, still limited due to many factors and far from being integrated in the clinical routine setting [26].
In the following article we will refer generally to the term BIA for what concerns the bioimpedance analysis technology, nonetheless we will specify for each study the type of technique (e.g. MF-BIA, BIVA, BIS) that has been used.
Clinical Relevance of BIA in HF Patients
HF presents the highest rate of hospitalizations among 65-year-old patients [27], with high morbidity and mortality, consuming vast resources of the public health system around the world [28]. The projected absolute number of people suffering from HF is approximately 26 million worldwide, and it is considered a growing epidemic with increasing incidence and prevalence [5,29]. In patients with acute decompensated HF (ADHF), body fluid congestion, presenting different clinical degrees of dyspnea, orthopnea, fatigue, jugular venous distension, rales, and edema, was demonstrated to be associated with re-hospitalization and high mortality rate [30]. Moreover, it is widely recognized that the pathophysiological determinant of the worsening of the patient’s state is caused by increased left ventricular filling pressures, dysregulation of the effective circulatory volume, and consequent extracellular fluids retention and mostly intravascular congestion [31] that, if left untreated, leads to pulmonary edema [32]. It is known that approximately 90% of patients admitted to the emergency department exhibit signs of fluid overload [33], and as indicated by another study, about 50% of them are discharged with some degree of congestion [34].
When patients are admitted to the hospital with excessive edema, intravenous diuretic therapy is commonly administered; however, since the monitoring is mostly performed through clinical observations, physical examination, or evaluation of the diuresis, the overall body volume assessment is not precise [35,36].
Determining diuretic therapy efficacy also depends on the patient’s diuretic resistance, which often makes the in-hospital assessment of the body volume challenging. These difficulties are also quite expected in home-setting conditions [37].
In many peripheral wards, body weight changes are utilized to evaluate the performance of diuretic therapy, assuming that a deterioration of HF has been defined as an increase of 2 kg in 48/h [38]. Nonetheless, different studies have shown that body weight monitoring presents a low sensitivity for the timely detection of congestive events and does not completely correlate with the process of a patient’s decompensation [39,40].
Body volume assessment is critical at home since preventing acute decompensation events is an unmet necessity [41]. Therefore, many studies have investigated how to manage the volume status of HF patients by the time they leave the hospitals to predict and avoid re-hospitalizations [38]. Although the cardioMEMS system, in which a small sensor is implanted the pulmonary artery to measure the pulmonary artery pressure, has been proven to be an effective method to prevent re-hospitalizations and reduce mortality in this set of patients, its use is limited by the invasiveness, costs, market penetration and potential complications [42,43,44]. Non-invasive methods or devices, employed mostly for regularly checking the patient’s body weight and congestion symptoms, have been studied to identify timely a potential heart failure decompensation event [45]. BIA has emerged to detect accurately the level of body fluids, and it has been studied as a potentially earlier predictor for decompensation events rather than an increase in body weight [30].
A selection of the most relevant prospective clinical studies in HF patients studying hard endpoints that showed a beneficial or a neutral effect of BIA in both intra-hospital and homecare settings are summarized in Table 1.
One of the earlier studies on BIA performed by Packer et al, also known as the Prospective Evaluation and Identification of Cardiac Decompensation by ICG Test (PREDICT), was conducted to assess the feasibility of ICG in predicting clinical deterioration in ambulatory patients with HF [46]. In detail, the study prospectively evaluated 212 stable patients with chronic HF (CHF) who presented a recent episode of clinical decompensation; patients underwent clinical evaluation and blinded ICG testing every 2 weeks for 26 weeks and were followed up for the occurrence of death or hospitalization [46]. The study combined clinical parameters such as NYHA class and blood pressure with ICG parameters such as velocity index, thoracic fluid content (TFC) index, and left ventricular ejection time, producing a composite score. The score showed to predict with good accuracy an HF event during the next 14 days of follow-up (p = 0.0002). Moreover, visits with a high-risk ICG score presented an 8.4% event rate during the next 14 days and predicted 41.6% of the events [46].
In 2010 the group of Di Somma et al aimed to verify whether BIVA could be a valid methodology for the assessment of fluid overload in ADHF, if there was a correlation with BNP, and if BIVA could be used in the management of the diuretic therapy in acute settings [47]. A total of 51 patients were enrolled, and their hydration state, BNP level, and caval index were evaluated at the following time points: at admission, after 24 and 72 hours, and at discharge. Moreover, a follow-up by phone was performed after 3 months. BIOVA measured higher values of hydration state in ADHF patients compared to controls. The most interesting result was that patients with an average hydration value >80.5% had a correlation with events at 3 months (death or rehospitalization for cardiogenic event) with a sensitivity of 22% and specificity of 94.2% [47].
In 2017, a prospective, multicenter, observational study by Santarelli et al. investigated the prognostic role of quantitative reduction of congestion during hospitalization by using BIVA serial evaluations in patients admitted for ADHF [48]. Both clinical and BIVA evaluations were performed at admission and discharge. A follow-up phone call was carried out at 90 days, and the primary endpoint was a composite of re-hospitalizations for HF or all-cause mortality. BIVA correctly predicted the primary endpoint at both admission (area under the curve (AUC) 0.56, p<0.04) and discharge (AUC 0.57, p<0.03). When combined with clinical evaluation, the prediction of the primary endpoint significantly increased for all-cause mortality or re-hospitalizations at 90 days (AUC 0.97, p<0.0001). Noteworthy, an increase of in-hospital resistance variation (dR/H) of more than 11 Ohm/m was associated with overall survival [48]. No significant results were found about the in-hospital reactance variation (dXc/H), underlining the concept that R is primarily influenced by changes in hydration status [48]. Furthermore, AHF patients discharged with the presence of at least one congestion sign were experiencing a lower survival [48].
BIA external devices have also been studied to assess their potential utilization for remote management in HF patients. The MUSIC study (Multisensor Monitoring in Congestive Heart Failure) was conducted to develop and validate an algorithm for predicting impending acute HF decompensation using a multi-parameter approach, including BIA obtained from an external device adhered to the chest [49]. This study found that the multisensor algorithms which included ICG as one of its sensors could accurately predict HF exacerbations with a sensitivity of 87% and a specificity of 87%. The algorithm also predicted HF aggravations an average of 6 days before clinical events occurred [49]. Moreover, BIA-derived measures of TFC were sensitive for predicting HF decompensation 9 to 11 days in advance. The study found that a TFC increase of 7.5% from baseline could predict clinical events with a sensitivity of 77% and a specificity of 64% [49].
Furthermore, in a prospective study by Gyllensten et al., 91 patients with CHF were monitored for an average of 10 months using a weight scale and a wearable BIA vest in home settings to predict HF exacerbations. One of the most important results was that BIA algorithms could better predict impending decompensation within 2 weeks compared to changes in weight (cross-validation estimate was 60% for BIA vs 33% for body weight). However, the authors noted that many alerts detected through the BIA device and its algorithms were not associated with clinically overt decompensation and related HF hospitalizations [50].
The SENTINEL-HF study, instead, tested a wearable BIA device called a fluid accumulation vest. This device is noninvasive, capable of transmitting data via a mobile phone, and employs an automated algorithm to predict recurrent HF events. Among the study participants with sufficient data (n=57), an algorithm analyzing thoracic BIA showed 87% sensitivity (95% CI 82-92), 70% specificity (95% CI 68-72), and 72% accuracy (95% CI 70-74) in the identification of HF events [51].
Different studies concentrated on analyzing intrathoracic congestion by applying BIA to the current generated from the pacing wires of pacemakers and defibrillators. One of the first studies on an ICD equipped with intrathoracic impedance monitoring was conducted by Wang et al. in a canine model [23,26,52]. The study demonstrated that impedance to electrical flow on the lead of these devices can reveal changes in thoracic congestion, mainly due to impending HF [23].
A study performed by Check-Man Yu et al. estimated that an implantable system capable of measuring intrathoracic impedance could identify fluid overload in patients before HF hospitalization and determine its correlation with standard measures of fluid status during hospitalization [26]. In detail, the automated detection of decreases in intrathoracic impedance via pacemaker and implantable cardioverter-defibrillator devices alerted in advance of the beginning of decompensation due to volume overload, providing timely information for titration of the medication [26]. Therefore, internal impedance-meter-equipped CIEDs have been developed with the product most known as Opti-Vol. In the DOT-HF trial, Opti-Vol affected the clinical outcomes of CHF patients, most likely due to additional data obtained from this method [53]. In the study, the number of deaths was comparable (p=0.54), while the number of outpatient visits was higher in the access arm (250 versus 84; p<0.0001). Interestingly, the intervention was associated with a borderline statistically significant increase in the primary endpoint of all-cause mortality and HF hospitalizations. This increase was mostly due to increased HF-related admissions caused by the Opti-Vol method, which led to an increase in unneeded hospitalizations, thus not addressing the authors’ main hypothesis [53].
Eventually, a recent multi-centric study performed by Anshory et al. investigated the role of a non-invasive method to assess hemodynamic parameters and total body congestion via BIA (NICaS)[54]. In this work, the authors aimed to evaluate the above-mentioned technology in a cohort of Asian and Caucasian AHF patients predicting mortality and re-hospitalization for HF within 30 days. As a main result, data at admission significantly predicted 30-day cardiovascular mortality and rehospitalization. Moreover, at discharge, a value of cardiac output obtained using NICaS predicted significantly a 30-day rehospitalization. Noteworthy, total peripheral resistance index on admission and during 48–72 hours showed each an AUC > 0.70 in predicting mortality and rehospitalization compared to clinical congestion score and NT-proBNP. These findings underline the importance of the role of combined methodologies, such as total body water and hemodynamics, to better understand the patients’ clinical status.
Clinical Relevance of BIA in CKD Patients
Chronic kidney disease (CKD) is defined as a reduction in kidney function that persists for more than 3 months, with leading causes including diabetes and hypertension, as well as infectious glomerulonephritis, vasculitis, congenital anomalies of the kidney and urinary tract (CAKUT), inherited and autoimmune diseases. Regardless of the etiology, CKD is characterized by progressive and accelerating loss of renal function caused by self-maintaining processes of fibrosis and atrophy of kidney tissues. Throughout the years, CKD can lead to end-stage kidney disease (ESKD), leading to potential kidney transplant or dialysis. The prevalence of CKD in the USA is as high as 40% among people over 70 years, with most patients having CKD stage 3 (GFR 30-59 ml/min/1.73 m2) [55]. The main clinical manifestations are caused by the accumulation of uremic toxins, anemia, metabolic acidosis, malnutrition, altered electrolytes, and impaired water homeostasis, leading to volume expansion, hypertension, and peripheral/pulmonary edema. Chronic fluid overload is experienced by 40-50% of hemodialysis (HD) patients [55].
The volume status of a patient is a crucial parameter in the nephrology clinical practice, especially for those with concomitant renal and heart failure, in which both fluid overload and volume depletion events are frequent and are associated with CKD progression and poor outcomes [56,57].
A selection of the most relevant prospective clinical studies in CKD patients studying hard endpoints that showed a beneficial or neutral effect of BIA is presented in Table 2.
It has become clear that BIA (i.e. BIS) is the most widely used method to evaluate volume status and guide fluid management in nephrological patients [58,59]. In HD, BIS is already employed to assess the overhydration state, enabling clinicians to evaluate the amount of fluid that ultrafiltration should remove [58,59].
Hur et al performed a well-structured randomized trial to investigate the effect of BIS-guided fluid management on cardiovascular outcomes in hemodialysis patients [60]. The authors used time-averaged fluid overload (TAFO) as a more accurate variable of the fluid status of patients. TAFO, calculated on pre-dialysis fluid overload (FO) and interdialytic weight gain (IDWG) (TAFO = FOpre – IDWG/2) was used to increase or decrease post-dialytic weight. Authors showed that bioimpedance fluid management significantly reduced left ventricular mass index (LVMI) and improved systolic and diastolic blood pressure pre- and post-dialysis compared to standard care [60].
Onofriescu et al showed in a randomized trial that a strict BIA-based (BIS) fluid management not only improved survival by reducing mortality significantly (Hazard ratio (HR) = 0.100 (95% CI, 0.013-0.805; p=0.03)), but also surrogated endpoints such as arterial stiffness, relative fluid overload and systolic BP improved [61].
In another randomized trial, ABISAD-III researchers provided an algorithm to determine post-dialysis weight based on the evaluation of fluid status by Body Composition Monitor [62]. Incidence of acute fluid overload (AFO), cardiovascular events, hypertension, or intradialytic complications were significantly reduced in the intervention group [62].
Other works and specific metanalysis studies have confirmed that excessive hydration defined by bioimpedance is an independent predictor of mortality in patients with ESKD [63,64].
A recent detailed methodological review and meta-analysis study on the use of whole-body BIA in dialysis patients was conducted on 46 manuscripts on the ESKD population; these studies were sub-grouped according to whether they used phase angle (PA)/BIVA, normalized ECW (ECW/TBW) or the overhydration index (OHI) [65]. The work evidenced that OHI is an independent predictor of mortality in ESKD patients independent of the influence of comorbidity and that different parameters, such as PA and OHI, act as similar predictors of outcome [65].
Another meta-analysis investigated the impact of bioimpedance-guided fluid management on two separated subsets of patients: CKD stage 3-5 and ESKD dialysis-dependent patients [66]. To our knowledge, this is the largest meta-analysis published on BIA-based monitoring of fluid management in dialysis patients. The authors analyzed hard and secondary outcomes, and they showed a significantly reduced all-cause mortality (HR = 0.64, 95% CI: 0.41, 0.99) and lower blood pressure with the use of BIA [66].
A systematic review and meta-analysis conducted by the NHS on more than 5,000 patients showed that BIA may lower overhydration in HD patients and improve blood pressure control, but it did not definitively prove a reduction in overall mortality [67]. The authors suggested that the difference could be due to the new studies in the meta-analysis and the increased number of peritoneal dialysis (PD) patients. Indeed, patients with residual renal function usually have a lower risk of mortality. Thus, the inclusion of more studies with PD may have led to a significant difference [67]. Differently, another recent study failed to demonstrate an improvement in short term clinical outcomes [68]. Nevertheless, results were not discordant in finding a significant reduction in hospitalization rate and an impressive, although not statistically significant, trend in the improvement of the primary composite endpoint consisting of death, acute myocardial infarction, cerebral infarction, cerebral hemorrhage, and peripheral vascular disease (HR = 0.487, 95% CI 0.217-1.091, P = 0.08) [68,69].
Diagnosis, Therapy, and Risk Stratification in HF and CKD
BIA measurements can provide valuable information to clinicians for the diagnosis, treatment, and risk stratification of HF and CKD patients. Figure 1A,B show a visual representation of the most relevant clinical benefits of BIA for HF and CKD patients, respectively.
ADHF = acute decompensated heart failure; BIA = bioimpedance analysis; CKD = chronic kidney disease; HF = heart failure; LVMI = left ventricular mass index
Various studies have repeatedly shown that BIA aids in the diagnostic assessment of the hydration status of HF and CKD patients.
Velazquez-Cecena et al. aimed to evaluate the correlation of low-, intermediate-, and high-risk groups for ADHF as determined by ICG parameters with LVEDP and serum BNP. The study’s main outcome was that patients considered at high risk for ADHF as determined by ICG presented significantly higher levels of LVEDP and BNP compared to lower-risk groups [70].
A study by Parrinello et al was designed to evaluate the diagnostic role of segmental and whole-BIA in the differential diagnosis of ADHF from the other causes of acute dyspnea across a broad population presenting to the emergency department [71]. One of the study’s main results revealed that whole body and segmental BIA were strong predictors of ADHF alone or in combination with BNP at the multiple regression analysis (AUC 0.989). Moreover, ROC curves were significantly higher (P < 0.0001) for segmental BIA (AUC = 0.963; CI: 0.935 - 0.982) and whole-body BIA (AUC = 0.934; CI: 0.902 - 0.961) than for LVEF (AUC = 0.814; CI: 0.764 - 0.857) and Framingham score (AUC = 0.681; CI: 0.625 - 0.734) [71].
In a study of ambulatory patients with HF by Gastelurrutia et al., BIVA was utilized instead to successfully differentiate between stable and unstable HF; stable patients were found to have a significantly lower impedance-measured fluid load ratio and lower nt-proBNP than the unstable ones [72].
Many studies concentrated on the role of BIA to guide and assess the efficacy of diuretic therapy in ADHF.
In a study by Zink et al., segmental BIA measurement was employed for the in-hospital monitoring of cardiac re-compensation in HF patients, which revealed the location of fluid accumulation and shift within the body during diuretic treatment [73].
In the study by Di Somma et al., the authors demonstrated a direct correlation between BIVA and urine output at 72 hours, showing how the efficacy of diuretic therapy and the effectiveness of these measurements go hand in hand with the normalization of BNP and caval index values at discharge. Thus, the authors suggested that BIVA could be more useful than clinical signs in managing diuretic therapy in ADHF patients [47].
Concerning CKD, a study aimed to evaluate the clinical usefulness of BIA in assessing volume status in patients receiving maintenance dialysis. The results indicated that BIA can accurately assess fluid volume status in patients receiving maintenance dialysis as measured by ECW and it can predict volume overload and hypertension in patients with end-stage renal disease. Lastly, it pointed out that BIA can be used to monitor changes in volume status over time and to guide clinical decision-making in managing fluid volume in patients receiving maintenance dialysis [74].
The group of Khan et al. demonstrated the efficacy of BIS in the stratification of CKD patients based on their volemic status and therefore randomized them to different diuretic therapy approaches, with good results compared to controls [58].
Detecting body fluids congestion in HF is challenging and many patients are discharged from the hospitals in a still congested state [75,76]. In a study on hospitalized ADHF patients, Massari et al demonstrated that BIVA could predict the total length of hospital stay independently. In other words, the more congested the patients were, the longer the staying in the hospital [76].
Other studies investigated the role of BIA (i.e. BIVA) and BNP or NTproBNP for risk stratification of HF patients [47,77,78]. In the study by Massari et al, BIVA was more accurate than BNP in the detection of peripheral congestion in both ADHF (AUC was 0.88 vs. 0.57 respectively; P < 0.001) and in chronic HF (AUC was 0.89 vs. 0.68, respectively; P < 0.001). Algorithms that include BIVA together with NTproBNP or BNP showed to be extremely accurate for patients´ prognosis assessment [77].
Eventually, a metanalysis on the role of BIA (leg bioimpedance) in relation to incident HF in the general population, with more than 50.0000 patients, was presented by Lindholm et al. in 2018.[79] This multivariable model that included leg bioimpedance, age, sex, and self-reported prior myocardial infarction showed good discrimination for future HF hospitalization, highlighting the potential benefits of adopting this simple, non-invasive, and cost-effective measure [79].
Advantages of BIA
In this narrative review, we presented a generalized beneficial effect of BIA for both HF and CKD patients in predicting hard endpoints such as ADHF, re-hospitalizations, and mortality.
BIA is a safe and affordable technique whose utilization is not operator-dependent due to its highly proven accuracy and repeatability [11]. Due to its non-invasiveness, it can be adapted to different clinical settings [11]. Figure 2 depicts the potential clinical benefits of utilizing BIA in acute and chronic care settings.
Moreover, BIA has been shown to provide many advantages, and its utilization can theoretically span from the emergency room to the bedside clinical ward assessment up to remote monitoring.
While we currently describe its role in the assessment of hydration, a great amount of evidence is also present regarding the role of BIA in assessing the nutrition status of chronic patients [11].
Limitations of BIA
Even if the advantages of BIA are clear, the technique has some limitations. Body composition assessment through BIA is highly reproducible in ideal conditions. However, the correct positioning and adherence of the electrodes to the skin need to be considered a potential confounding factor. A supine condition with a hand-to-foot configuration is considered the most accurate as it estimates the whole-body surface but may be difficult to obtain with certain patients, especially if they are acutely decompensated or during an HD procedure [80].
One of the main limitations is that BIA mostly uses regression models derived from healthy people to predict body composition [81]. While BIA has been validated in conditions such as HF and CKD and in different population subsets, it is relevant to constantly study and adapt novel dedicated equations for an accurate estimation of the body composition in specific pathological conditions [11]. For instance, BIA is inaccurate for morbidly obese patients because excess of adipose tissue can overestimate FFM while underestimating FM values. This is mainly caused by the different distribution between body mass and body conductivity, reducing the accuracy detection of BIA [11,17].
CKD is associated with fluid retention, which increases total body water (TBW) and leads to changes in intracellular water (ICW) and ECW. Other confounders such as ethnicity, gender, body mass index, and estimated glomerular filtration rate, may affect BIA accuracy and outcome prediction [11].
A theoretical limitation of BIA regards its utilization in patients carrying cardiac implantable electronic devices (CIED) due to potential electromagnetic interference. Nonetheless, different studies approached the problem, showing that neither BIA nor the implantable devices interfered or provided any risks to the functioning and measurement of the other method [82].
Future Perspectives
Although the clinical relevance of BIA has been repeatedly demonstrated in the past years, its everyday utilization in the clinical wards or for remote monitoring remains limited.
One of the main problems regarding BIA adoption is the lack of large, randomized trials that could justify a complete reimbursement of the solution. Further studies should question the benefits of BIA, comparing the scenarios in which it is employed against those in which it is not applied, with the hypothesis that it can improve the current standard of care. This holds true for in-hospital use, but it is even more relevant for home settings.
Another point that needs to be addressed when considering its adoption is the complete integration of the measurement of HS into the clinical work routine.
Currently, the assessment of HS in the hospital is still mostly based on physical examination by the medical doctor, while patients use only weight scales at home. Therefore, the detection of HS should be accessible not only at the patient’s bedside but also at the patient’s home.
Hydration status should be an easily visualizable and actionable parameter, similar to blood pressure, blood glucose, or temperature, and channelled into a clinical decision tree.
Thus, it is crucial to have dedicated and instructed personnel collecting and interpreting the information. However, future solutions should focus on automatizing the information workflow and introducing smart sensors.
A recent study showed that a handheld bioimpedance system for the assessment of body fluid status could be used to assist the patient in home-based ESKD treatments [83]. This device consisted of a custom-made handheld tetrapolar bioimpedance spectrometer and a textile-based electrode garment for total body fluid assessment [83]. Future solutions should follow those developments.
We believe optimizing processes and improving clinical outcomes should drive HS adoption, with patients’ needs as the focus of our attention.
Another extremely relevant aspect concerns the creation of personalized pathology parameters that, through AI and the analysis of large datasets, should guide the personalization of treatments. Indeed, combining different biomarkers with BIA has been shown to be very promising for prognostic purposes. For this reason, our study group recently finalized a study currently under revision to assess the role of BIA, biomarkers, and other vital parameters to create a risk prediction algorithm that could detect mortality and re-hospitalizations within 6 months.
3. Conclusions
The importance of BIA in detecting and predicting the clinical course of patients has been demonstrated. A fundamental step is needed to integrate hydration status assessment into the everyday routine for the management of CKD and HF patients. Further randomized trials are needed to prove that using BIA compared to standard care may reduce re-hospitalizations and mortality, especially in remote monitoring settings.
Author Contributions
For research articles with several authors, a short paragraph specifying their individual contributions must be provided. The following statements should be used “Conceptualization, X.X. and Y.Y.; methodology, X.X.; software, X.X.; validation, X.X., Y.Y. and Z.Z.; formal analysis, X.X.; investigation, X.X.; resources, X.X.; data curation, X.X.; writing—original draft preparation, X.X.; writing—review and editing, X.X.; visualization, X.X.; supervision, X.X.; project administration, X.X.; funding acquisition, Y.Y. All authors have read and agreed to the published version of the manuscript.” Please turn to the CRediT taxonomy for the term explanation. Authorship must be limited to those who have contributed substantially to the work reported.
Funding
Please add: “This research received no external funding” or “This research was funded by NAME OF FUNDER, grant number XXX” and “The APC was funded by XXX”. Check carefully that the details given are accurate and use the standard spelling of funding agency names at https://search.crossref.org/funding. Any errors may affect your future funding.
Institutional Review Board Statement
In this section, you should add the Institutional Review Board Statement and approval number, if relevant to your study. You might choose to exclude this statement if the study did not require ethical approval. Please note that the Editorial Office might ask you for further information. Please add “The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of NAME OF INSTITUTE (protocol code XXX and date of approval).” for studies involving humans. OR “The animal study protocol was approved by the Institutional Review Board (or Ethics Committee) of NAME OF INSTITUTE (protocol code XXX and date of approval).” for studies involving animals. OR “Ethical review and approval were waived for this study due to REASON (please provide a detailed justification).” OR “Not applicable” for studies not involving humans or animals.
Informed Consent Statement
Any research article describing a study involving humans should contain this statement. Please add “Informed consent was obtained from all subjects involved in the study.” OR “Patient consent was waived due to REASON (please provide a detailed justification).” OR “Not applicable.” for studies not involving humans. You might also choose to exclude this statement if the study did not involve humans.
Written informed consent for publication must be obtained from participating patients who can be identified (including by the patients themselves). Please state “Written informed consent has been obtained from the patient(s) to publish this paper” if applicable.
Data Availability Statement
We encourage all authors of articles published in MDPI journals to share their research data. In this section, please provide details regarding where data supporting reported results can be found, including links to publicly archived datasets analyzed or generated during the study. Where no new data were created, or where data is unavailable due to privacy or ethical restrictions, a statement is still required. Suggested Data Availability Statements are available in section “MDPI Research Data Policies” at https://www.mdpi.com/ethics.
Acknowledgments
In this section, you can acknowledge any support given which is not covered by the author contribution or funding sections. This may include administrative and technical support, or donations in kind (e.g., materials used for experiments).
Conflicts of Interest
Declare conflicts of interest or state “The authors declare no conflicts of interest.” Authors must identify and declare any personal circumstances or interest that may be perceived as inappropriately influencing the representation or interpretation of reported research results. Any role of the funders in the design of the study; in the collection, analyses or interpretation of data; in the writing of the manuscript; or in the decision to publish the results must be declared in this section. If there is no role, please state “The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results”.
References
- Bioelectrical impedance analysis in body composition measurement: National Institutes of Health Technology Assessment Conference Statement. The American journal of clinical nutrition. 1996;64(3 Suppl):524S-32S.
- Lurefkaskis HC, Bolonchuk WW, Hall CB, Siders WA. Validation of tetrapolar bioelectrical impedance method to assess human body composition. 1986;60(4):1327-32.
- Lukaski HC, Vega Diaz N, Talluri A, Nescolarde L. Classification of Hydration in Clinical Conditions: Indirect and Direct Approaches Using Bioimpedance. Nutrients. 2019;11(4).
- Lukaski HC, Talluri A. Phase angle as an index of physiological status: validating bioelectrical assessments of hydration and cell mass in health and disease. Rev Endocr Metab Disord. 2023;24(3):371-9.
- Baumgartner RN, Chumlea WC, Roche A. Estimation of body composition from bioelectric impedance of body segments. The American journal of clinical nutrition. 1989;50(2):221-6.
- Kotanko P, Levin NW, Zhu F. Current state of bioimpedance technologies in dialysis. Nephrology Dialysis Transplantation. 2008;23(3):808-12.
- Thomas BJ, Ward LC, Cornish BH. Bioimpedance spectrometry in the determination of body water compartments: accuracy and clinical significance. Appl Radiat Isot. 1998;49(5-6):447-55.
- Chamney PW, Krämer M, Rode C, Kleinekofort W, Wizemann V. A new technique for establishing dry weight in hemodialysis patients via whole body bioimpedance. Kidney Int. 2002;61(6):2250-8.
- Charra, B. Fluid balance, dry weight, and blood pressure in dialysis. Hemodial Int. 2007;11(1):21-31.
- Khalil SF, Mohktar MS, Ibrahim F. The theory and fundamentals of bioimpedance analysis in clinical status monitoring and diagnosis of diseases. Sensors. 2014;14(6):10895-928.
- Kyle UG, Bosaeus I, De Lorenzo AD, Deurenberg P, Elia M, Gómez JM, et al. Bioelectrical impedance analysis--part I: review of principles and methods. Clin Nutr. 2004;23(5):1226-43.
- La Porta E, Lanino L, Calatroni M, Caramella E, Avella A, Quinn C, et al. Volume Balance in Chronic Kidney Disease: Evaluation Methodologies and Innovation Opportunities. Kidney & blood pressure research. 2021;46(4):396-410.
- Ronco C, Haapio M, House AA, Anavekar N, Bellomo R. Cardiorenal syndrome. Journal of the American College of Cardiology. 2008;52(19):1527-39.
- de Jager DJ, Grootendorst DC, Jager KJ, van Dijk PC, Tomas LM, Ansell D, et al. Cardiovascular and noncardiovascular mortality among patients starting dialysis. Jama. 2009;302(16):1782-9.
- Deferrari G, Cipriani A, La Porta E. Renal dysfunction in cardiovascular diseases and its consequences. J Nephrol. 2021;34(1):137-53.
- Faragli A, La Porta E, Campana C, Pieske B, Kelle S, Koehler F, et al. Out-of-Hospital Care of Heart Failure Patients During and After COVID-19 Pandemic: Time for Telemedicine? 2020;2.
- Kyle UG, Bosaeus I, De Lorenzo AD, Deurenberg P, Elia M, Manuel Gómez J, et al. Bioelectrical impedance analysis—part II: utilization in clinical practice. Clinical Nutrition. 2004;23(6):1430-53.
- Hoffer EC, Meador CK, Simpson DC. Correlation of whole-body impedance with total body water volume. Journal of applied physiology. 1969;27(4):531-4.
- Lukaski, HC. Evolution of bioimpedance: a circuitous journey from estimation of physiological function to assessment of body composition and a return to clinical research. European journal of clinical nutrition. 2013;67(1):S2-S9.
- Lukaski HC, Bolonchuk WW, Hall CB, Siders WA. Validation of tetrapolar bioelectrical impedance method to assess human body composition. Journal of applied physiology. 1986;60(4):1327-32.
- Bera, TK. Bioelectrical impedance methods for noninvasive health monitoring: a review. Journal of medical engineering. 2014;2014.
- Keren H, Burkhoff D, Squara P. Evaluation of a noninvasive continuous cardiac output monitoring system based on thoracic bioreactance. 2007;293(1):H583-H9.
- Wang, L. Fundamentals of intrathoracic impedance monitoring in heart failure. The American journal of cardiology. 2007;99(10):S3-S10.
- Yang X-W, Hua W, Ding L-G, Wang J, Zheng L-H, Li C-Q, et al. OptiVol fluid index predicts acute decompensation of heart failure with a high rate of unexplained events. Journal of Geriatric Cardiology: JGC. 2013;10(3):253.
- Tang WH, Tong W. Measuring impedance in congestive heart failure: current options and clinical applications. American heart journal. 2009;157(3):402-11.
- Yu C-M, Wang L, Chau E, Chan RH-W, Kong S-L, Tang M-O, et al. Intrathoracic impedance monitoring in patients with heart failure: correlation with fluid status and feasibility of early warning preceding hospitalization. Circulation. 2005;112(6):841-8.
- Felker GM, Lee KL, Bull DA, Redfield MM, Stevenson LW, Goldsmith SR, et al. Diuretic strategies in patients with acute decompensated heart failure. The New England journal of medicine. 2011;364(9):797-805.
- Savarese G, Lund LH. Global public health burden of heart failure. Cardiac failure review. 2017;3(1):7.
- Roger, VL. Epidemiology of heart failure. Circulation research. 2013;113(6):646-59.
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JG, Coats AJ, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. European journal of heart failure. 2016;18(8):891-975.
- Boorsma EM, Ter Maaten JM, Damman K, Dinh W, Gustafsson F, Goldsmith S, et al. Congestion in heart failure: a contemporary look at physiology, diagnosis and treatment. Nature reviews Cardiology. 2020;17(10):641-55.
- Ishikawa S-e. Hyponatremia associated with heart failure: pathological role of vasopressin-dependent impaired water excretion. Journal of clinical medicine. 2015;4(5):933-47.
- Palazzuoli A, Evangelista I, Nuti R. Congestion occurrence and evaluation in acute heart failure scenario: time to reconsider different pathways of volume overload. Heart failure reviews. 2020;25(1):119-31.
- Gheorghiade M, Filippatos G, De Luca L, Burnett J. Congestion in acute heart failure syndromes: an essential target of evaluation and treatment. Am J Med. 2006;119(12 Suppl 1):S3-S10.
- Pellicori P, Kaur K, Clark AL. Fluid Management in Patients with Chronic Heart Failure. Card Fail Rev. 2015;1(2):90-5.
- O’Connor CM, Stough WG, Gallup DS, Hasselblad V, Gheorghiade M. Demographics, clinical characteristics, and outcomes of patients hospitalized for decompensated heart failure: observations from the IMPACT-HF registry. J Card Fail. 2005;11(3):200-5.
- Neuberg GW, Miller AB, O’Connor CM, Belkin RN, Carson PE, Cropp AB, et al. Diuretic resistance predicts mortality in patients with advanced heart failure. Am Heart J. 2002;144(1):31-8.
- Lewin J, Ledwidge M, O’Loughlin C, McNally C, McDonald K. Clinical deterioration in established heart failure: What is the value of BNP and weight gain in aiding diagnosis? European journal of heart failure. 2005;7(6):953-7.
- Chaudhry SI, Mattera JA, Curtis JP, Spertus JA, Herrin J, Lin Z, et al. Telemonitoring in patients with heart failure. The New England journal of medicine. 2010;363(24):2301-9.
- Evangelista LS, Lee JA, Moore AA, Motie M, Ghasemzadeh H, Sarrafzadeh M, et al. Examining the effects of remote monitoring systems on activation, self-care, and quality of life in older patients with chronic heart failure. The Journal of cardiovascular nursing. 2015;30(1):51-7.
- Faragli A, Abawi D, Quinn C, Cvetkovic M, Schlabs T, Tahirovic E, et al. The role of non-invasive devices for the telemonitoring of heart failure patients. Heart Fail Rev. 2021;26(5):1063-80.
- Abraham WT, Adamson PB, Bourge RC, Aaron MF, Costanzo MR, Stevenson LW, et al. Wireless pulmonary artery haemodynamic monitoring in chronic heart failure: a randomised controlled trial. Lancet. 2011;377(9766):658-66.
- Vaduganathan M, DeFilippis EM, Fonarow GC, Butler J, Mehra MR. Postmarketing Adverse Events Related to the CardioMEMS HF System. JAMA Cardiol. 2017;2(11):1277-9.
- Singh R, Varjabedian L, Kaspar G, Zughaib M. CardioMEMS in a Busy Cardiology Practice: Less than Optimal Implementation of a Valuable Tool to Reduce Heart Failure Readmissions. Cardiol Res Pract. 2018;2018:4918757.
- Koehler F, Koehler K, Deckwart O, Prescher S, Wegscheider K, Winkler S, et al. Telemedical Interventional Management in Heart Failure II (TIM-HF2), a randomised, controlled trial investigating the impact of telemedicine on unplanned cardiovascular hospitalisations and mortality in heart failure patients: study design and description of the intervention. Eur J Heart Fail. 2018;20(10):1485-93.
- Packer M, Abraham WT, Mehra MR, Yancy CW, Lawless CE, Mitchell JE, et al. Utility of impedance cardiography for the identification of short-term risk of clinical decompensation in stable patients with chronic heart failure. Journal of the American College of Cardiology. 2006;47(11):2245-52.
- Di Somma S, De Berardinis B, Bongiovanni C, Marino R, Ferri E, Alfei B. Use of BNP and bioimpedance to drive therapy in heart failure patients. Congest Heart Fail. 2010;16 Suppl 1:S56-61.
- Santarelli S, Russo V, Lalle I, De Berardinis B, Vetrone F, Magrini L, et al. Prognostic value of decreased peripheral congestion detected by Bioelectrical Impedance Vector Analysis (BIVA) in patients hospitalized for acute heart failure: BIVA prognostic value in acute heart failure. Eur Heart J Acute Cardiovasc Care. 2017;6(4):339-47.
- Anand IS, Tang WW, Greenberg BH, Chakravarthy N, Libbus I, Katra RP, et al. Design and performance of a multisensor heart failure monitoring algorithm: results from the multisensor monitoring in congestive heart failure (MUSIC) study. Journal of cardiac failure. 2012;18(4):289-95.
- Gyllensten IC, Bonomi AG, Goode KM, Reiter H, Habetha J, Amft O, et al. Early indication of decompensated heart failure in patients on home-telemonitoring: a comparison of prediction algorithms based on daily weight and noninvasive transthoracic bio-impedance. JMIR medical informatics. 2016;4(1):e4842.
- Darling CE, Dovancescu S, Saczynski JS, Riistama J, Sert Kuniyoshi F, Rock J, et al. Bioimpedance-Based Heart Failure Deterioration Prediction Using a Prototype Fluid Accumulation Vest-Mobile Phone Dyad: An Observational Study. JMIR Cardio. 2017;1(1):e1.
- Wang L, Lahtinen S, Lentz L, Rakow N, Kaszas C, Ruetz L, et al. Feasibility of using an implantable system to measure thoracic congestion in an ambulatory chronic heart failure canine model. Pacing and Clinical Electrophysiology. 2005;28(5):404-11.
- van Veldhuisen DJ, Braunschweig F, Conraads V, Ford I, Cowie MR, Jondeau G, et al. Intrathoracic impedance monitoring, audible patient alerts, and outcome in patients with heart failure. Circulation. 2011;124(16):1719-26.
- Anshory M, Kuan WS, Rohman MS, Waranugraha Y, Kamila PA, Iskandar A, et al. Can non-invasive cardiac hemodynamics and fluid content system (NICaS) parameters predict Acute Heart Failure outcomes in Caucasian and Asian patients in the emergency department? Advances in medical sciences. 2024;69(1):81-9.
- McCullough K, Sharma P, Ali T, Khan I, Smith WC, MacLeod A, et al. Measuring the population burden of chronic kidney disease: a systematic literature review of the estimated prevalence of impaired kidney function. Nephrology Dialysis Transplantation. 2012;27(5):1812-21.
- McCullough PA, Chan CT, Weinhandl ED, Burkart JM, Bakris GL. Intensive Hemodialysis, Left Ventricular Hypertrophy, and Cardiovascular Disease. Am J Kidney Dis. 2016;68(5s1):S5-s14.
- Soi V, Yee J. Sodium Homeostasis in Chronic Kidney Disease. Adv Chronic Kidney Dis. 2017;24(5):325-31.
- Khan YH, Sarriff A, Adnan AS, Khan AH, Mallhi TH. Diuretics prescribing in chronic kidney disease patients: physician assessment versus bioimpedence spectroscopy. Clin Exp Nephrol. 2017;21(3):488-96.
- Davies SJ, Caskey FJ, Coyle D, Lindley E, Macdonald J, Mitra S, et al. Rationale and design of BISTRO: a randomized controlled trial to determine whether bioimpedance spectroscopy-guided fluid management maintains residual kidney function in incident haemodialysis patients. BMC Nephrol. 2017;18(1):138.
- Hur E, Usta M, Toz H, Asci G, Wabel P, Kahvecioglu S, et al. Effect of fluid management guided by bioimpedance spectroscopy on cardiovascular parameters in hemodialysis patients: a randomized controlled trial. Am J Kidney Dis. 2013;61(6):957-65.
- Onofriescu M, Hogas S, Voroneanu L, Apetrii M, Nistor I, Kanbay M, et al. Bioimpedance-guided fluid management in maintenance hemodialysis: a pilot randomized controlled trial. Am J Kidney Dis. 2014;64(1):111-8.
- Huan-Sheng C, Yeong-Chang C, Ming-Hsing H, Fan-Lieh T, Chu-Cheng L, Tsai-Kun W, et al. Application of bioimpedance spectroscopy in Asian dialysis patients (ABISAD-III): a randomized controlled trial for clinical outcomes. Int Urol Nephrol. 2016;48(11):1897-909.
- Zoccali C, Moissl U, Chazot C, Mallamaci F, Tripepi G, Arkossy O, et al. Chronic Fluid Overload and Mortality in ESRD. J Am Soc Nephrol. 2017;28(8):2491-7.
- Dekker M, Konings C, Canaud B, Carioni P, Guinsburg A, Madero M, et al. Pre-dialysis fluid status, pre-dialysis systolic blood pressure and outcome in prevalent haemodialysis patients: results of an international cohort study on behalf of the MONDO initiative. Nephrol Dial Transplant. 2018;33(11):2027-34.
- Tabinor M, Elphick E, Dudson M, Kwok CS, Lambie M, Davies SJ. Bioimpedance-defined overhydration predicts survival in end stage kidney failure (ESKF): systematic review and subgroup meta-analysis. Scientific reports. 2018;8(1):4441.
- Horowitz L, Karadjian O, Braam B, Mavrakanas T, Weber C. Bioimpedance-Guided Monitoring of Volume Status in Patients With Kidney Disease: A Systematic Review and Meta-Analysis. Can J Kidney Health Dis. 2023;10:20543581231185433.
- Scotland G, Cruickshank M, Jacobsen E, Cooper D, Fraser C, Shimonovich M, et al. Multiple-frequency bioimpedance devices for fluid management in people with chronic kidney disease receiving dialysis: a systematic review and economic evaluation. Health Technol Assess. 2018;22(1):1-138. [CrossRef]
- Liu L, Sun Y, Chen Y, Xu J, Yuan P, Shen Y, et al. The effect of BCM guided dry weight assessment on short-term survival in Chinese hemodialysis patients : Primary results of a randomized trial - BOdy COmposition MOnitor (BOCOMO) study. BMC Nephrol. 2020;21(1):135. [CrossRef]
- Stigger K, Ribeiro LR, Cordeiro FM, Böhlke M. Incidence of hospital admissions in bioimpedance-guided fluid management among maintenance hemodialysis patients-Results of a randomized controlled trial. Hemodial Int. 2023;27(3):318-25. [CrossRef]
- Velazquez-Cecena JL, Sharma S, Nagajothi N, Khraisat A, Khosla S, Arora RR, et al. Left ventricular end diastolic pressure and serum brain natriuretic peptide levels in patients with abnormal impedance cardiography parameters. Arch Med Res. 2008;39(4):408-11.
- Parrinello G, Paterna S, Di Pasquale P, Torres D, Fatta A, Mezzero M, et al. The usefulness of bioelectrical impedance analysis in differentiating dyspnea due to decompensated heart failure. Journal of cardiac failure. 2008;14(8):676-86.
- Gastelurrutia P, Nescolarde L, Rosell-Ferrer J, Domingo M, Ribas N, Bayes-Genis A. Bioelectrical impedance vector analysis (BIVA) in stable and non-stable heart failure patients: a pilot study. Int J Cardiol. 2011;146(2):262-4.
- Zink MD, König F, Weyer S, Willmes K, Leonhardt S, Marx N, et al. Segmental bioelectrical impedance spectroscopy to monitor fluid status in heart failure. Scientific Reports. 2020;10(1):3577.
- Park JH, Jo YI, Lee JH. Clinical usefulness of bioimpedance analysis for assessing volume status in patients receiving maintenance dialysis. Korean J Intern Med. 2018;33(4):660-9.
- Maddox TM, Januzzi JL, Jr., Allen LA, Breathett K, Butler J, Davis LL, et al. 2021 Update to the 2017 ACC Expert Consensus Decision Pathway for Optimization of Heart Failure Treatment: Answers to 10 Pivotal Issues About Heart Failure With Reduced Ejection Fraction: A Report of the American College of Cardiology Solution Set Oversight Committee. J Am Coll Cardiol. 2021;77(6):772-810.
- Massari F, Scicchitano P, Ciccone MM, Caldarola P, Aspromonte N, Iacoviello M, et al. Bioimpedance vector analysis predicts hospital length of stay in acute heart failure. Nutrition. 2019;61:56-60.
- Massari F, Iacoviello M, Scicchitano P, Mastropasqua F, Guida P, Riccioni G, et al. Accuracy of bioimpedance vector analysis and brain natriuretic peptide in detection of peripheral edema in acute and chronic heart failure. Heart Lung. 2016;45(4):319-26.
- Massari F, Scicchitano P, Iacoviello M, Passantino A, Guida P, Sanasi M, et al. Multiparametric approach to congestion for predicting long-term survival in heart failure. J Cardiol. 2020;75(1):47-52.
- Lindholm D, Fukaya E, Leeper NJ, Ingelsson E. Bioimpedance and new-onset heart failure: a longitudinal study of> 500 000 individuals from the general population. Journal of the American Heart Association. 2018;7(13):e008970.
- Montalibet A, Rastel D, Chaigneau C, Grenier E, McAdams E. Comparison between bioelectrical impedance spectroscopy measurements and water volume displacement of ankle oedema variations during the course of a day. Physiol Meas. 2020;41(8):085004.
- Sun SS, Chumlea WC, Heymsfield SB, Lukaski HC, Schoeller D, Friedl K, et al. Development of bioelectrical impedance analysis prediction equations for body composition with the use of a multicomponent model for use in epidemiologic surveys. The American journal of clinical nutrition. 2003;77(2):331-40.
- Chabin X, Taghli-Lamallem O, Mulliez A, Bordachar P, Jean F, Futier E, et al. Bioimpedance analysis is safe in patients with implanted cardiac electronic devices. Clin Nutr. 2019;38(2):806-11.
- Ferreira J, Pau I, Lindecrantz K, Seoane F. A Handheld and Textile-Enabled Bioimpedance System for Ubiquitous Body Composition Analysis. An Initial Functional Validation. IEEE journal of biomedical and health informatics. 2017;21(5):1224-32.
Figure 1.
Graphical representation of the most relevant clinical results obtained with BIA in HF and CKD patients. In each figure the most relevant clinical results obtained in the selected studies are summarized for HF (A) and CKD (B) groups. The size of the bubble is directly proportional to the number of patients in which the results have been obtained. For each parameter the first Author and the number of patients studied are shown.
Figure 1.
Graphical representation of the most relevant clinical results obtained with BIA in HF and CKD patients. In each figure the most relevant clinical results obtained in the selected studies are summarized for HF (A) and CKD (B) groups. The size of the bubble is directly proportional to the number of patients in which the results have been obtained. For each parameter the first Author and the number of patients studied are shown.
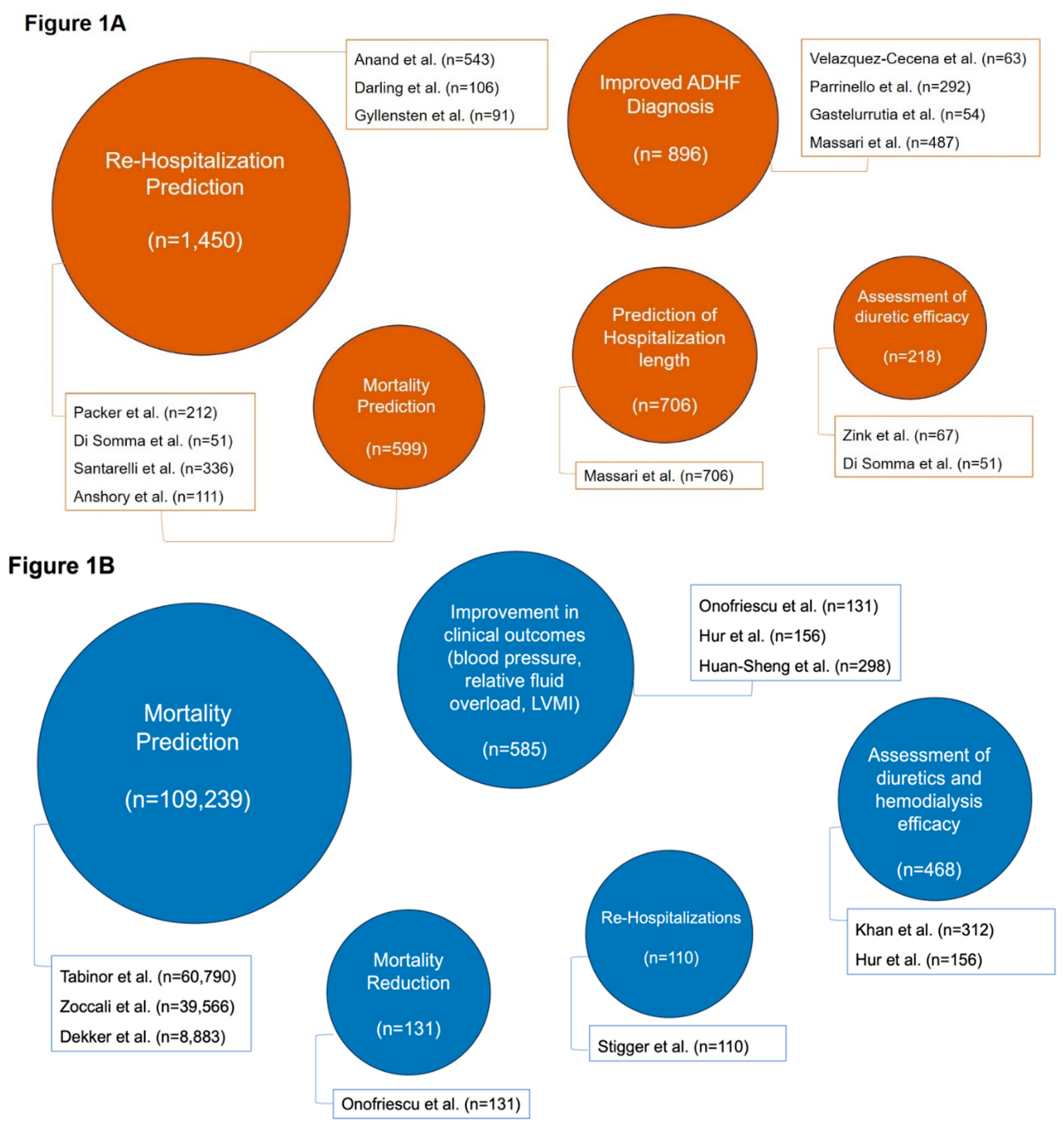
Figure 2.
Graphical representation of the proven clinical benefits of BIA in acute and chronic care settings. The usual clinical course of CKD and HF patients from acute to chronic care is displayed. The studied role of BIA for diagnosis, risk stratification and therapy in each settings are written in blue. The clinical benefit of using BIA in each setting is shown in green. For each step the citations are written in parentheses. BIA = bioimpedance analysis; CKD = chronic kidney disease; HF = heart failure.
Figure 2.
Graphical representation of the proven clinical benefits of BIA in acute and chronic care settings. The usual clinical course of CKD and HF patients from acute to chronic care is displayed. The studied role of BIA for diagnosis, risk stratification and therapy in each settings are written in blue. The clinical benefit of using BIA in each setting is shown in green. For each step the citations are written in parentheses. BIA = bioimpedance analysis; CKD = chronic kidney disease; HF = heart failure.
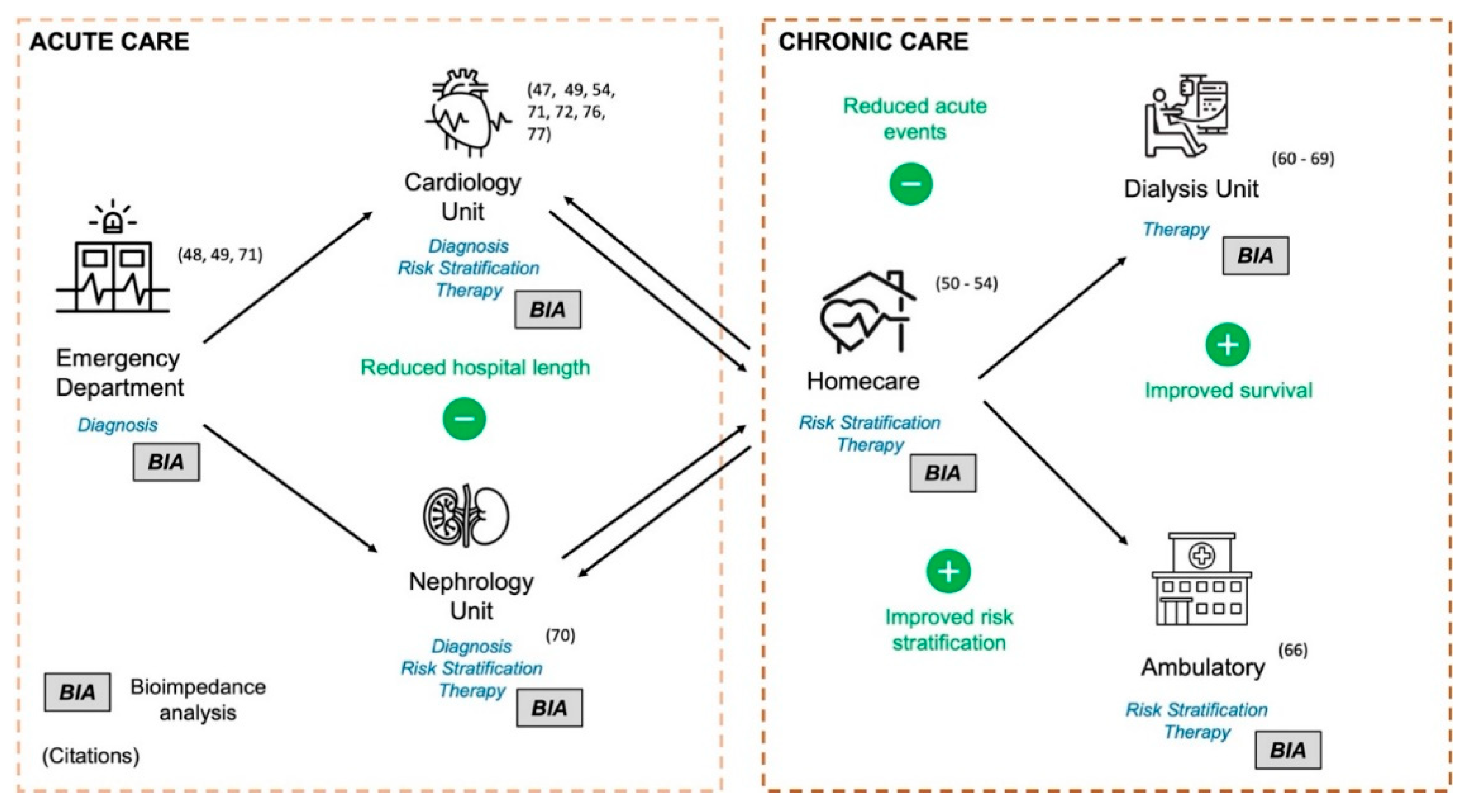

Table 1.
Comparative analysis of BIA studies in HF patients. A selection of the studies exploring the hardest endpoints in HF patients is summarized in the table.
Table 1.
Comparative analysis of BIA studies in HF patients. A selection of the studies exploring the hardest endpoints in HF patients is summarized in the table.
| Author | Year | Journal | Type of study | Patients | BIA Method | Endpoints | Limitations | Main Results |
|---|---|---|---|---|---|---|---|---|
| Packer - (PREDICT) |
2006 | Journal of the American College of Cardiology |
Prospective non-randomized study |
212 | Non-invasive transthoracic impedance |
All-cause mortality or HF hospitalizations in 14 days | Small sample size |
BENEFICIAL EFFECTS Clinical and ICG parameters predict HF at 14 days (p = 0.0002). High-risk ICG score presents an 8.4% event rate at 14 days (Accuracy: 41.6%) |
| Di Somma |
2010 | Congestive Heart Failure | Prospective non-randomized study |
51 | BIVA | All-cause mortality or HF hospitalizations in 90 days | Small sample size |
BENEFICIAL EFFECTS Overhydration >80.5% measured with BIVA correlated with primary endpoint at 3 months (Sensitivity: 22%; Specificity: 94.2%) |
| van Veldhuisen - (DOT-HF) | 2011 | Circulation | Randomized trial - Remote Monitoring |
335 | Intrathoracic impedance monitoring | All-cause mortality or HF hospitalizations in 15 months | Terminated prematurely due to slow enrollment |
NEUTRAL EFFECTS No difference in mortality between groups (p=0.54); number of outpatient visits was higher in the intervention group (250 versus 84; p<0.0001). |
| Anand - (MUSIC Study) |
2012 | Journal of Cardiac Failure |
Prospective non-randomized study - Remote Monitoring |
543 | Non-invasive transthoracic impedance |
ADHF event in 90 days | High exclusion rate due to device failure or withdrawal of consent |
BENEFICIAL EFFECTS Thoracic fluid content (TFC) found sensitive for predicting HF decompensation up to 9-11 days in advance. TFC increase of 7.5% from baseline was found to predict the primary endpoint (Sensitivity: 77%; Specificity: 64%). |
| Gyllensten | 2016 | JMIR Med Inform. |
Prospective non-randomized study - Remote Monitoring |
91 | Non-invasive transthoracic impedance | ADHF event in 14 days | Possibility of early intervention affecting results, small sample size |
BENEFICIAL EFFECTS Non-invasive transthoracic BIA predicts a decompensation event 2 weeks in advance (P<.001). NEUTRAL EFFECTS Non-invasive transthoracic BIA and its algorithms had a low positive predictive value for overt HF decompensation events. |
| Darling - (SENTINEL -HF) |
2017 | JMIR Cardio | Prospective non-randomized study - Remote Monitoring |
16 | Non-invasive transthoracic impedance |
ADHF event in 45 days | Small sample size, specificity was affected by false postives, homogeneous cohort |
BENEFICIAL EFFECTS An algorithm utilizing non-invasive thoracic BIA is highly predictive for the identification of recurrent HF events at 45 days (Accuracy: 72%) |
| Santarelli |
2017 | Eur Heart J – Acute Cardiovascular Care | Prospective non-randomized study |
336 | BIVA | All-cause mortality or HF hospitalizations in 90 days | Higher accuracy if BIVA is utilized with clinical signs |
BENEFICIAL EFFECTS BIVA predicts the primary endpoints at admission (area under the curve (AUC) 0.56, p<0.04) and at discharge (AUC 0.57, p<0.03). By combining BIVA with clinical signs, a high predictive value for cardiovascular events at 90 days (AUC 0.97, p<0.0001) was observed. |
| Anshory | 2024 | Advances in Medical Sciences | Prospective non-randomized study |
111 | Non-invasive transthoracic impedance + BIVA |
All-cause mortality or HF hospitalizations in 30 days | Drugs used in patient treatment and inotropic usage may have conditioned the results |
BENEFICIAL EFFECTS Hemodynamic and TBW data significantly predicted 30-day cardiovascular mortality and rehospitalization. At discharge, a value of cardiac output was a significant predictor for 30-day rehospitalization. |
ADHF = acute decompensated heart failure; AUC = area under the curve; BIA = bioimpedance analysis; BIVA = bioimpedance vectorial analysis; CI = confidence interval; ECW = extracellular water; HF = heart failure; ICG = impedance cardiography; ICW = intracellular water; TFC = thoracic fluid content.
Table 2.
Comparative analysis of BIA studies in CKD patients. A selection of the studies exploring the hardest endpoints in HF patients is summarized in the table.
Table 2.
Comparative analysis of BIA studies in CKD patients. A selection of the studies exploring the hardest endpoints in HF patients is summarized in the table.
| Author | Year | Journal | Type of study | Patients |
BIA Method | Endpoints | Limitations | Main Results |
|---|---|---|---|---|---|---|---|---|
| Onofriescu |
2014 | American Journal of Kidney Diseases |
Prospective randomized controlled trial - Hemodialysis |
131 | BIS |
All-cause mortality | Underpowered regarding mortality outcomes due to younger cohort and less diabetes rate |
BENEFICIAL EFFECTS BIA-based fluid management significantly reduced mortality in HD patients (HR=0.100 95% CI, 0.013-0.805). |
| Huan-Sheng – (ABISAD III) |
2016 | International Urolology and Nephrology | Prospective randomized controlled trial - Hemodialysis |
298 | BIS | All-cause hospitalizations AFO |
This study focused on FO post HD, further studies are needed to show whether other interventions besides weight adjustment play a role in this improvement. |
BENEFICIAL EFFECTS AFO incidence, cardiovascular events, or intradialytic complications were significantly reduced in the intervention group. NEUTRAL EFFECTS All-cause hospitalization rate was not different between groups. |
| Zoccali |
2017 | Journal of the American Society of Nephrology | Prospective non-randomized study - Hemodialysis |
39,566 | BIS |
All-cause mortality at 1 and 4 years | Purely observational nature of the study |
BENEFICIAL EFFECTS Baseline OHI/ECW >15% in men and >13% in women at baseline were independent predictors of mortality in HD patients (HR = 1.26, 95% CI 1.19–1.33). |
| Tabinor |
2018 | Scientfic report | Meta-analysis - Hemodialysis |
60,790 | Various BIA methods |
Mortality | Methodological heterogeneity, inadequately reported demographics and report of endpoints |
BENEFICIAL EFFECTS Baseline pre-dialysis OHI>15% is predictive for mortality in HD patients (HR = 2.28, 95% CI 1.56-3.34). |
| Dekker |
2018 | Nephrology Dialysis Transplantation. | Prospective study - Hemodialysis |
8,883 | BIS |
Mortality | No documentation of antihypertensive medications, echocardiographic results are not available and cardiac failure is likely underreported |
BENEFICIAL EFFECTS Pre-dialysis FO (>+1.1 to +2.5 L) together with pre-SBP <110 mmHg was associated with an increased mortality (HR = 1.52; 95% CI 1.06–2.17) |
| Liu - (BOCOMO Study) |
2020 | BMC Nephrology | Prospective randomized controlled trial - Hemodialysis |
445 | BIS |
All-cause mortality, myocardial infarction, cerebral infarction, cerebral hemorrhage, and peripheral vascular disease | Small cohort and limited follow up period |
NEUTRAL EFFECTS An increasing trend of survival rates in patients with BIA guided HD was observed, however no significant difference observed. (log-rank test, p= 0.07). |
| Horowitz |
2023 | Canadian Journal of Kidney Health and Disease | Systematic Review and Meta-Analysis - Hemodialysis |
2,420 | Various BIA methods |
All-cause mortality, blood pressure control, all-cause hospitalization, major adverse cardiovascular events, and change in left ventricular mass index | Heterogenity in reported endpoints/outcomes |
BENEFICIAL EFFECTS In HD patients using BIA decreases all-cause mortality and blood pressure. NEUTRAL EFFECTS No significant difference in all-cause hospitalization, major adverse cardiac event, or change in left ventricular mass index was observed. |
| Stigger |
2023 | Hemodialysis International | Prospective randomized controlled trial - Hemodialysis |
110 | BIS |
All-cause mortality, blood pressure control, all-cause hospitalization | Small sample size |
BENEFICIAL EFFECTS BIA utilization significantly reduced the incidence rate of hospital admissions in HD patients. |
AFO = average fluid overload; BIA = bioimpedance analysis; BIS = bioimpedance spectroscopy; CI = confidence interval; ECW = extracellular water; FO = fluid overload; HD = hemodialysis; HR = hazard ratio; OHI = overhydration index.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



