
Submitted:
28 August 2024
Posted:
28 August 2024
You are already at the latest version
Abstract
Background. National surveys reported on variable prevalence of chronic kidney disease (CKD) due to differences in characteristics of population, design, equations used to estimate glomerular filtration rate (eGFR) and definitions. The EH-UH 2 survey is the first study evaluating CKD prevalence, characteristics and awareness in Croatia. Methods. This was a cross-sectional nationwide observational study designed to assess the prevalence and cardio-kidney-metabolic risk factors in Croatia which included 1765 randomly selected subjects. We estimated the prevalence of CKD by means of albumin-to-creatinine ratio (ACR) and eGFR (CKD EPI equation). Comorbidities, anthropometric and social factors related to the prevalence of CKD were analyzed, and CV risk profile was evaluated. Results. The weighted prevalence of CKD (any stage), CKD stage ≥ G3A A2, and CKD defined only as eGFR < 60 ml/min/1.73 m2 were estimated at 17.1%, 9.8% and 7.9%, respectively. The prevalence was higher in men than in women (11.8% vs. 7.9%; p 30 mg/g was 15.1%. Older age, male gender, diabetes, ePWV, and uric acid were independently associated with CKD prevalence. The awareness of CKD of 9.5%. Unaware were older with lower income, less educated, having more frequently diabetes, hypertension (less frequently controlled) and milder renal impairment. Conclusion. In Croatia, the estimated prevalence of CKD is high, being more frequently presented in men than in women. CKD patients have unfavorable CV risk profile. The awareness of CKD is very low reflecting poor health literacy in general population but also in health care workers.
Keywords:
albuminuria
; awareness
; chronic kidney disease
; cardiovascular risk
; eGFR (CKD Epi) formula
; glomerular filtration rate
; national population survey
1. Introduction
Assessing the burden of kidney dysfunction, the prevalence of chronic kidney disease (CKD) in 2017 was estimated as 9.1% in the world’s population [1]. In this analysis age-standardized prevalence of CKD in Croatia was estimated to be 8.8%. In other analyses which included 33 population-based representative studies from around the world the age-standardized global prevalence of CKD stages 1–5 in subjects older than 20 years was 10.4% among men and 11.8% among women [2]. The current total number of individuals affected by CKD stages 1–5 worldwide was estimated to be 843.6 million, which is more people than those with diabetes, osteoarthritis, chronic obstructive pulmonary disease (COPD), asthma, or depressive disorders [3,4]. Disturbingly, the burden of kidney disease is rising worldwide. According to the Global Burden of Disease (GBD) study, the global prevalence of CKD increased by 33% between 1990 and 2017 [1]. Death and disability due to CKD also have increased as well. Globally CKD burden is mostly driven by population growth, aging, diabetes, and hypertension [5]. CKD disproportionately affects vulnerable and marginalized populations, and most of the burden was concentrated in the three lowest quintiles of socio-demographic index.
CKD has been recognized as an independent risk factor for cardiovascular disease (CVD) and was appreciated as a risk multiplier in patients with hypertension and diabetes [6,7,8,9]. In 2017, impaired kidney function resulted in 61.3 million DALYs, of which 58.4% were directly contributed by CKD whereas 41.6% were CVD DALYs [1]. Of CVD DALYs attributable to kidney dysfunction 58.8% came from ischemic heart disease and 40.2% from stroke [1]. In the 2021 European Society of Cardiology (ESC) guideline on CVD prevention individuals with moderate and severe CKD were regarded as high and very high-risk of CVD, respectively [10]. To personalize CVD preventive therapies, ESC developed and validated a new approach that allows the inclusion of information on the two CKD measures, estimated glomerular filtration rate (eGFR) and albuminuria, into existing prediction models. This approach, CKD add-on, have significantly improved CVD risk prediction beyond the Pooled Cohort Equation (PCE) and SCORE [11,12,13]. Recently, American Heart Association has launched a new holistic paradigm on cardio-kidney-metabolic health, and new predictive equation (PREVENT), also emphasizing the importance of kidney dysfunction for the global risk [14].
CKD is now the seventh most common cause of death from noncommunicable disease (NCD) worldwide. Contrary to CVD, stroke and respiratory disease, CKD mortality has been rising. Nowadays, CKD and kidney dysfunction is the third fastest-growing cause of death globally. Importantly CKD is the only NCD to exhibit a continued rise in age-adjusted mortality [15]. By 2040, CKD is projected to be the 5th highest cause of years of life lost (YLL) globally [16].
Many studies have shown a variable CKD prevalence, with significant differences in men and women in most, but not all, cases [17,18,19,20,21]. Differences in reported CKD prevalence could be explained by heterogeneity of study design, by selection bias, by equation used to estimate eGFR or variety of CKD definitions used across different studies [22]. This should be considered when interpreting and comparing results on CKD prevalence obtained in different national surveys. The other important point is the fact that the true prevalence is probably underestimated due to the lack of screening programs and early detection of kidney dysfunction which is related to the unawareness of the risk associated with the earlier stages of CKD [23]. This poor health literacy is present in general population and patients, but also in all health care workers and health-care authorities [24]. CKD is frequently undetected because of the asymptomatic nature and slow clinical course. According to most reports approximatively only 10 % of patients with CKD were aware of having kidney dysfunction, and majority were undiagnosed until the very late stages missing opportunity for interventions which could prevent disease progression before kidney injury reaches a point-of-no-return [1,25,26]. Finally, debate on how to differentiate aging kidney from true CKD in elderly is going on [27,28]. Modification of risk factors and medical treatment of diabetes, hypertension, and CKD itself can improve renal and CV outcomes and slow or prevent progression to end-stage-kidney-disease (ESKD) [29,30].
The rising burden of CKD should be seriously appreciated and included in the global and national health agendas because it is largely preventable and treatable. However, many countries have underdeveloped nephrology workforces and/or are mainly oriented on the provision of treatment for ESKD but not for early stages of CKD. In Croatia, most of nephrologists are focused on patients with ESKD, with excellent kidney transplantation program and with well-documented registries of patients undergoing renal replacement therapy. Unfortunately, interest for individuals at the earlier stages of CKD was disproportionally lower, and there were only a few preventive nephrologists. A surge of new drugs proven to be effective in preventing CKD and CVD progression (sodium-glucose transport protein 2 inhibitors, glucagon-like peptide-1 receptor agonists, finerenone) increased interest not only from nephrologists but also from cardiologists and diabetologists for CKD starting from early stages, and it is our hope that future will be better. Accurate information on both early and advanced stages of CKD in the general population is important for making proper strategies for screening, diagnosis, prevention, and treatment. Until now, we were lacking data on prevalence, characteristics, and awareness of CKD in a representative group of Croatian adults. This is particularly important because Croatia is high-middle income country ranked in the group of countries with high CV risk [31]. To obtain this valuable information we have conducted EH-UH 2 study, a nationwide, population-based survey of CKD prevalence and awareness which incorporate both albuminuria and estimates of eGFR based on the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation.
2. Materials and Methods
2.1. Study Design and Recruitment
This cross-sectional study was a part of the EH-UH 2 survey (Epidemiology of arterial hypertension and salt intake in Croatia), a nationally representative survey of non-institutionalized persons in the Croatia which involved collecting anthropometric, demographic, lifestyle, and biological marker data from the general adult population to assess risk factors for cardio-kidney-metabolic health, and the prevalence of major NCDs. A total of 2021 subjects (18 to 91 years old) were included by random selection from the general population using randomization numbers obtained from the registry of the family physician (FP) (the randomization numbers represent the ordinal numbers of the archive of each family physicians' practice). The subjects selected via the randomization list were informed about the project by telephone call from FP and were included in the study according to the exclusion and inclusion criteria. Exclusion criteria for participation in the project were persons with terminal illness, dementia, paresis, amputation or immobilization of a limb, acute illness, reconvalescent after surgery, pregnant women, lactating mothers, COVID - 19 infection within the last 3 months, those who were prescribed therapy with diuretics in the last two weeks prior to the urine sample collection date, and unsigned consent to participate in the research, while the inclusion criteria were: individuals over 18 years of age and a signed consent to participate in the research. Being on dialysis and after kidney transplantation were not exclusion criteria. However, no one reported on any type of renal replacement therapy. In the case the invited subject had one or more exclusion criteria, the FP contacted the next subject from the randomization list. Final number of subjects included in the study are shown in Figure 1. Participation rate (attending the outpatient visit) was 76%. After the subjects had been included in the study, the nurses, members of the mobile examination team (MET) made an appointment for home visit. The home visit consisted of signing the consent to participate in the study, subjects got their personal identification code and the first measurements of blood pressure (BP) and heart rate were taken. Subjects were given instruction on how to properly collect and handle urine during a 24-hour period and were instructed to fast for 12 hours prior to the examination at which blood samples would be taken. At the end of the home visits, the subjects were invited for outpatient examinations. It was carried out in three steps: (a) questionnaire survey, (b) physical measurements and (c) blood drawn, spot urine sample collections, and 24-hour urine collections. Nurses, physicians, pharmacists, fellows, residents, and medical students who were members of MET were educated to collect study and clinical data in a standardized manner (Figure 2).
2.2. Questionnaire
The questionnaire (face-to-face interview) was used to collect data on participant’s demographic (age, sex, place of residence), socio-economic status (SES), lifestyles (physical activity, smoking habit, alcohol consumption, diet, frequency of high salt food consumption, fruit and vegetable consumption, knowledge on dietary salt), personal and family history of cardio-kidney-metabolic diseases, and drug therapy. Subjects’ smoking habit was coded as current smoker, former smoker and never smoked. Pack years was calculated as the number of packs subject smoke per day multiplied by the number of years patients have smoked. Heavy alcohol use was defined as consumption of ≥8 drinks/week for women or ≥15 drinks/week for men. SES was measured by two indicators: education and occupation. By answering the question of educational attainment, subjects were coded as less than primary school (< 4 years), primary school (4 to ≤ 8 years), high school (8-12 years), university degree (> 12 years). The professional qualifications were coded as no college, college, bachelor s degree, master s degree. Physical activity was defined as active (≥75 min/week of vigorous intensity or ≥150 minutes/week of moderate or an equivalent combination of moderate and vigorous intensity activity), intermediate (5–74 min/week of vigorous intensity or 10–149 min/week of moderate or an equivalent combination of moderate and vigorous intensity activity), or inactive [32]. Poverty-income ratio (PIR) was calculated as family income was categorized as ≤130% or >130% based on commonly used thresholds. Each participant’s marital status was described by one of the following categories: married/cohabited, single, separated/divorced, and widowed.
2.3. Anthropometry (Physical Measurements)
The outpatient examinations of the subjects included: anthropometric data measurements, measurement of brachial BP, central BP and arterial stiffness i.e. pulse wave velocity (PWV), recording of electrocardiogram (ECG), metabolic scale measurements followed by fasting blood sampling and collecting of morning spot urine sample. Few days before the outpatient examinations, subjects were reminded to collect and bring 24-hor urine from the previous day. Office BP measurements were performed according to the European Society for Hypertension guidelines and recommendations of the Croatian Society for Hypertension [33,34]. BP was measured on both hands, and if there was a difference in BP over the left or right hand, as the higher value was taken as relevant, and the BP was measured on that arm. If there was no difference in BP between left and right arm, BP was measured on the non-dominant arm. BP and heart rate were measured using oscilometric device (OMRON M6 Comfort smart cuff). The first measurement was discarded, and an average of the last two readings was used. Hypertension was defined as anyone with systolic BP ≥ 140 and or diastolic BP ≥ 90 mm Hg or taking medication for hypertension. Diabetes was defined as fasting blood glucose >7 mmol/l and/or taking antidiabetic drugs. The persons’ weight and height were measured while they were clothed only in their underwear. A metabolic scale (OMRON BF511) was used for weight measurements to the nearest 100 grams, and height was measured with a height rule (stadiometer) rounded to the nearest centimeter. Body mass index (BMI) was calculated by dividing weight in kilograms by height in meters squared (kg/m2). Obesity was defined as BMI ≥30, overweight as 25 ≤ BMI < 30; overweight/obesity was defined as BMI ≥25. Waist circumference (WC) was used as a measure of central adiposity (defined as WC >88 cm for women and >102 cm for men). PWV was calculated from pulse wave obtained over brachial artery using IEM Mobil-O-Graph PWA monitor, and ePWV was calculated using validate equation (ePWV = 9.587 - (0.402 x age) + [4.560 x 0.001 x (age2)] - [2.621 x 0.00001 x (age2) x systolic AT] + (3.176 x 0.001 x age x systolic AT) - (1.832 x 0.01 x systolic AT)) [35].
2.4. Laboratory Analysis
Fasting blood samples and morning urine samples were analyzed by using standard laboratory methods. About 8.5 ml in the tube with Silica Clot Activator-SST for biochemistry tests (BD Diagnostic, Sparks, MD, USA) and 50 ml morning urine sample were collected in plastic containers for each subject. Blood samples were centrifuged for 10 minutes at 3500 rpm within 2 hours of collection. All samples were transported the same day to the Department of Laboratory Diagnostics, University Hospital Centre Zagreb where they were analyzed immediately. Serum and urine creatinine were measured on the Abbott Alinity CC analyzer using the enzymatic method with creatininase traceable to isotope dilution-mass spectrometry (IDMS) (Alinity, Abbott, USA). Calibration was performed once per lot of reagents using the same company calibrators traceable to the IDMS method and NIST reference material SRM 967 (substance creatinine purity of 99.7 ± 0.3%) for serum and the NIST reference material SRM 914a (substance creatinine purity of 99.7 ± 0.3%) for urine samples. Urinary albumin was measured in the 24-hour urine sample by immunonephelometric method on the BN II nephelometer, (Siemens Healthcare Diagnostics Inc, Tarrytown, NY, USA) standardized using primary ERM-DA470 calibrators with a method sensitivity of 3.0 mg/L. Continuous internal quality control was performed throughout the study using quality control materials provided by the respective manufacturers. In the serum samples additional tests were subsequently performed using standard laboratory methods on the Alinity analyzer (Abbott, Abbott Park, Illinois, U.S.A): triglycerides using photometry with glycerol phosphate oxidase (GPOPAP), total cholesterol using photometry with cholesterol oxidase (CHOD-PAP), HDL-cholesterol using homogeneous enzyme immunoinhibition method and LDL- cholesterol using homogeneous enzyme colorimetric method). On the same platform, with original reagents from the same manufacturer: Lp(a) using immunoturbidimetric method on polystyrene particles, NTproBNP and Troponin I hs using chemiluminescent immunochemical method (CMIA), Apo (A) and Apo (B) using immunoturbidimetric on polystyrene particles, uric acid using photometric method with uricase, glucose using UV photometry with hexokinase and serum electrolytes using indirect potentiometric method. Insulin was measured using Electro Chemi Luminescence Immunoassay (ECLIA) method on instrument Cobas e 411 (Cobas Roche, California, USA) and tTG IgA using chemiluminescence method (CLIA) on BioFlash instrument (Biokit S.A. Barcelona, Spain). Full blood count was determined according to the principle of laser light scattering technology on Sysmex XN-1000 analyzer (Sysmex Corporation, Kobe, Japan).
The eGFR was calculated for adults aged 18+ years using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation based on the serum creatinine values [36]. The values of eGFR (mL/min/1.73 m2) were grouped into six categories based on the Kidney Disease Improving Global Outcomes (KDIGO) 2012 classification recommendations as follows: G1:≥ 90 mL/min/1.73 m2 (normal or high) , G2: 60–89 mL/min/1.73 m2 (mildly decreased), G3a: 45–59 mL/min/1.73 m2 (mildly to moderately reduced), G3b: 30–44 mL/min/1.73 m2 (moderately to severely decreased), G4: 15–29 mL/min/1.73 m2 (severely decreased) and G5: < 15 mL/ mL/min/1.73 m2 (kidney failure) [29]. Categories of albuminuria based on urine albumin-to-creatinine ratio ACR were classified according to the recommendations of the KDIGO classification into three categories as follows: A1:<30 mg/g (normal to mildly increased), A2: 30–300 mg/g (moderately increased), A3:>300 mg/g (severely increased). Increased albuminuria was defined as an ACR ≥30 mg/g.
2.5. Statistical Analysis
Statistical analysis was performed using SPSS version 23.0 (IBM Corp., USA). The normality of data distribution was tested using Kolmogorov-Smirnov test. Preliminary analyses were performed to ensure no violation of the assumptions of normality, linearity, and homoscedasticity. Categorical data were expressed as numbers and frequencies. Correlations were obtained using Pearson’s test for normally distributed variables and Spearman rank correlation for non-normally distributed variables. The results were reported as mean (SD and/or 95% confidence interval CI), median and interquartile range (IQR) or percentages, as appropriate. Non-normally distributed data were expressed as median and interquartile range and Mann-Whitney U-test was used on comparison between two groups. Categorical variables were compared using χ2-test. A Pearson correlation coefficient was calculated to obtain information about the relationships between variables. Firstly, the prevalence of different stages of CKD were estimated and expressed as counts and proportions (%). To account for the stratified random sampling method, weighted statistical methods were applied to produce nationally representative CKD prevalence estimates [37]. Secondly, descriptive analyses were performed to present demographic, socio-economic, behavioral, and cardio metabolic risk factors of subjects with CKD. Univariate and multivariate logistic regression analyses were used to determine association between parameters and CKD. Results were expressed in terms of odds ratio (OR) and the respective 95% CI. Finally, multivariable logistic regression analyses were performed to identify the independent contribution of important factors to the risk of having CKD. Based on a literature review and on statistical criteria (variables showing p < 0.05 in the univariate analyses), the following variables were introduced in the multivariable models: model 1: adjusted for age and gender; model 2: further adjusted for ePWV; model 3: additionally adjusted for diabetes; model 4, model 5, model 6, and model 6: further adjusted for urea, uric acid, and serum potassium, respectively. We analyzed prevalence of aware and unaware subjects of having CKD, their characteristics and association with risk factors using regression analyses. A two-side p-value < .05 was considered statistically significant.
The survey was carried out in accordance with the Declaration of Helsinki and Good Clinical Practice [REF]. Ethical approval for the survey was obtained from the Committee of Research Ethics of the National Centre of Public Health and subjects provided written informed consent to take part.
3. Results
The estimated weighted (age standardization to the Croatian adult population) overall prevalence of CKD (any stage) was 17.1%; 95% CI 8.0-15.0, and prevalence of CKD ≥ G3A A2 was 9.8 %; 95% CI 6.6-9.5; men vs. women 11.8% ;95% CI 7.6-12.8 vs. 7.9%; 95% CI 5.2-8.4; p<0.001) (Table 1). The overall crude prevalence of CKD in population, defined as eGFR < 60 ml/ min/1.72 m2 was 9.5 % (men vs. women 12.8% vs. 7.8%; p<0.001). The weighted prevalence of CKD defined as eGFR < 60 ml/ min/1.72 m2 was lower in the whole group (7.9 %; 95% CI 6.5-9.3; men vs. women: 10.7%; 95% CI 8.0-13.3 vs. 6.5%; 95% CI 4.8-8.1; p<0.001). The weighted prevalence of albuminuria using unique ACR cut-off of 30 mg/g was 15.1% being significantly higher in men than women. Table 2 shows the percentages of subjects in KDIGO categories, i.e. estimates of the crude and weighted prevalence of subjects with cardio-renal risk based on both eGFR and ACR. Most subjects were in stages G1 and G2 (weighted prevalence 71%), and most of them (57.7%) were in stages G1A1 plus G2A1, and 11.7% and 0.6% were in stages G1A2 plus G2A2, and G1A3 plus G2A3, respectively. Based on these results we can estimate that in Croatia there is a total number of 311.441 adult persons (age 18 -90 years) having CKD stage ≥ G3A A2. Very high, high and moderate cardio-kidney risk was found in 1.7%, 4.5% and 16.6% of adult Croatian population, respectively. Differences in demographic, social, behavioral and clinical characteristics, as well as in laboratory factors between CKD and non-CKD populations are shown in Table 3. CKD group was older with more men, higher systolic BP, with more untreated and uncontrolled hypertension, and more subjects with diabetes. There were more overweight and obese subjects with higher visceral circumference, and CKD group had higher arterial stiffness estimated by PWV and ePWV. There were less smokers, but we failed to find differences in daily salt intake. Subjects with CKD had lower personal and family monthly income and were less educated with lower professional qualifications. There were more ischemic strokes, heart failure and atrial fibrillation in CKD group, but differences in prevalence of hemorrhagic stroke and myocardial infarction did not reach statistically significance. In addition to expected differences in kidney biomarkers (serum creatinine, urea, eGFR, ACR), we found higher levels of uric acid, triglycerides, potassium and cardiac biomarkers (NTproBNP, Troponin I hs), and total, HDL and LDL cholesterol in CKD group. In univariate logistic regression analysis various variables were associated with CKD. Table 4 outlines only those factors for which the association with CKD was significant. Overall, the prevalence of CKD increased significantly with age, men gender, low family income, systolic BP, obesity (particularly visceral), ePWV, presence and duration of hypertension and diabetes. Positive history for ischemic stroke, heart failure and atrial fibrillation were also significantly associated with CKD. Out of biochemical parameters, beside serum creatinine, urea and ACR, fasting blood glucose, uric acid, and lipids were significant predictors of CKD. Interestingly, we found cardiac biomarkers (NTproBNP and Troponin I hs) to be significantly associated with CKD. We failed to find significant difference according to geographical regions and urban/rural residency. In the multivariate regression analysis (Table 4) men gender (OR 4.2), older age (OR 0.82), ePWV (1.65), diabetes (2.74), urea (OR 0.64), uric acid (OR 0.99) and serum potassium (0.43) were independently associated with higher prevalence of CKD.
The awareness of CKD was 9.5 %. Unaware of having CKD were older with lower income and qualifications, less educated, having more frequently diabetes, hypertension (less frequently controlled) and milder renal impairment (Table 5).

Table 5.
Multivariate logistic regression analysis estimating independent correlates of chronic kidney disease.
Table 5.
Multivariate logistic regression analysis estimating independent correlates of chronic kidney disease.
| Model | Coef | S.E. | Odds Ratio | 95% CI | P | Nagelkerke R2 | P for change | |
|---|---|---|---|---|---|---|---|---|
| (B) | Exp (B) | Lower | Upper | |||||
| Model 1 | 0.287 | <0.001 | ||||||
| Constant | 8.554 | 0.863 | 5186.45 | <0.001 | ||||
| Gender | 1.780 | 0.258 | 5.93 | 3.58 | 9.82 | <0.001 | ||
| Age | -0.106 | 0.013 | 0.90 | 0.87 | 0.92 | <0.001 | ||
| Model 2 | 0.304 | <0.001 | ||||||
| Constant | 8.997 | 0.936 | 8075.6 | <0.001 | ||||
| Gender | 1.837 | 0.262 | 6.280 | 3.760 | 10.48 | <0.001 | ||
| Age | -0.174 | 0.029 | 0.841 | 0.794 | 0.89 | <0.001 | ||
| ePWV | 0.359 | 0.138 | 1.432 | 1.092 | 1.878 | 0.009 | ||
| Model 3 | 0.331 | 0.557 | ||||||
| Constant | 8.407 | 1.108 | 4479.2 | <0.001 | ||||
| Gender | 1.778 | 0.265 | 5.917 | 3.517 | 9.954 | <0.001 | ||
| Age | -0.181 | 0.030 | 0.834 | 0.787 | 0.885 | <0.001 | ||
| ePWV | 0.409 | 0.141 | 1.505 | 1.141 | 1.984 | 0.004 | ||
| Diabetes | 0.995 | 0.324 | 2.705 | 1.144 | 5.105 | <0.001 | ||
| Model 4 | 0.454 | <0.001 | ||||||
| Constant | 10.198 | 1.096 | 26860.47 | <0.001 | ||||
| Gender | 1.921 | 0.299 | 6.828 | 3.8 | 12.2 | <0.001 | ||
| Age | -0.158 | 0.032 | 0.854 | 0.80 | 0.91 | <0.001 | ||
| Diabetes | 0.948 | 0.290 | 2.579 | 1.46 | 4.55 | 0.001 | ||
| ePWV | 0.408 | 0.155 | 1.504 | 1.11 | 2.03 | 0.008 | ||
| urea | -0.503 | 0.071 | 0.589 | 0.51 | 0.67 | <0.001 | ||
| Model 5 | 0.496 | 0.001 | ||||||
| Constant | 13.057 | 1.358 | 468266.30 | |||||
| Gender | 1.581 | 0.315 | 4.862 | 2.64 | 9.00 | <0.001 | ||
| Age | -0.177 | 0.034 | 0.838 | 0.78 | 0.89 | <0.001 | ||
| Diabetes | 1.009 | 0.303 | 2.743 | 1.51 | 4.96 | <0.001 | ||
| ePWV | 0.501 | 0.161 | 1.650 | 1.20 | 2.26 | 0.002 | ||
| urea | -0.442 | 0.075 | 0.643 | 0.55 | 0.74 | <0.001 | ||
| Uric acid | -0.009 | 0.002 | 0.991 | 0.98 | 0.99 | <0.001 | ||
| Model 6 | 0.518 | 0.001 | ||||||
| Constant | 17 752 | 2.091 | 51240062.3 | <0.001 | ||||
| Gender | 1.445 | 0.323 | 4.240 | 2.250 | 7.991 | <0.001 | ||
| Age | -0.187 | 0.036 | 0.829 | 0.773 | 0.890 | <0.001 | ||
| Diabetes | 1.005 | 0.315 | 2.731 | 1.472 | 5.065 | 0.001 | ||
| ePWV | 0.552 | 0.171 | 1.73 | 1.242 | 2.431 | 0.001 | ||
| urea | -0.429 | 0.80 | 0.651 | 0.557 | 0.,762 | <0.001 | ||
| Uric acid | -0.11 | 0.002 | 0.989 | 0.985 | 0.993 | <0.001 | ||
| potassium | -0.837 | 0.270 | 0.433 | 0.255 | 0.735 | 0.002 | ||
Table 6.
Characteristics of subjects divided in the groups depending on CKD awareness.
| CKD aware N = 11 |
CKD unaware N = 106 |
X2; | p | |||
|---|---|---|---|---|---|---|
| Median (IQR) | 95% CI | Median (IQR) | 95% CI | |||
| Men % | 54.5 | 23.4-83.8 | 50.0 | 40.1-59.9 | 12 653; | 0.002 |
| Age (years) | 71 (62-75) | 62.51-75.68 | 72 (65-79) | 69.2-72.9 | NS | |
| Smokers % | 18.2 | 27.3-51.8 | 11.3 | 6.0-18.9 | 12 004; | <0.017 |
| Hypertension duration (years) | 15.5 (5.5-13.2) | 54.5-56.1 | 10.0 (5.0-16.0) | 10.2-14.7 | NS | |
| Systolic blood pressure (mmHg) | 138 (126-138) | 129.3-162.6 | 137.5 (124-153) | 135.5-144.2 | NS | |
| Waist circumference % | 88.9 | 51.8-99.7 | 78.4 | 68.8-86.1 | 10 222; | 0.037 |
| Personal income < 300 Eu % | 44.3 | 37.4 -54.3 | 32.4 | 1.7-35.2 | 18 169; | 0.029 |
| Family income < 300 Eu % | 22.6 | 15.1-31.8 | 10.1 | 8.4-12.6 | 39 534; | <0.001 |
| Education < 12 years % | 50.0 | 40.1-55.9 | 54.8 | 51.8-57.7 | 20 269; | 0.009 |
| No college % | 36.8 | 27.6-46.7 | 23.5 | 21.1-26.6 | 21 771; | 0.005 |
| Atrial fibrillation % | 1.8 | 0.2-5.1 | 8.5 | 4.0-15.5 | 19 446; | 0.001 |
| Hypertension % | 63.6 | 30.8-89.1 | 72.6 | 63.1-80.9 | 5583; | 0.061 |
| Controlled hypertensive % | 23.4 | 21.0-26.9 | 21.9 | 14.4-31.0 | 12 851; | 0.045 |
| Diabetes % | 27.3 | 17.6-61.0 | 29.2 | 20.8-38.9 | 18913; | <0.001 |
| ePWV (m/s) | 11.5 (10.1-13.9) | 10.4-13.4 | 12.0 (10.6-13.4) | 11.6-12.4 | NS | |
| Urea (mmol/l) | 8.2 (3.6) | 5.7-10.6 | 8.0 (3.0) | 7.4-8.6 | NS | |
| Serum creatinine (µmol/l) | 119 (106-132) | 101.5-157.0 | 110 (91.7-118) | 106.7-121.6 | NS | |
| eGFR (ml/min/1.73m2 ) | 45.2 (38.5-58.0) | 38.4-53.6 | 55.0 (44.5-58.1) | 49.5-53.3 | NS | |
| Uric acid (µmol/l) | 350 (284-475) | 287.6-482.9 | 360.0 (304-417) | 350.5-386.4 | NS | |
4. Discussion
To our best knowledge EH-UH-2 study is the first study estimating CKD prevalence in Croatia, but also in South-East Europe and Balkan region at the national level based on a large random sample of adult population according to the KDIGO guidelines using recommended measures, CKD stages defined by eGFR (CKD-EPI) and ACR. The weighted prevalence of CKD stages 1-5 was 17.1% which was higher than 10.6% and 9.1% reported in worldwide analyzes [1,38]. The weighted prevalence of CKD stages 3-5 and albuminuria (A2 plus A3) was also higher in our studied population (9.8% and 15.1%, respectively) than in this report (5.4 % and 5.4%, respectively) [38]. However, our results are much closer to the results of recent meta-analysis of 100 studies with almost 7 million patients which reported a global prevalence of 13.4% for CKD stages 1–5 and 10.6% for CKD stages 3–5 [39]. On contrary, CKD prevalence of approximatively 6% was found in Italy, Luxembourg and Poland [40,41,42]. Our finding of predominance of early stages are in concordance with all other reports. Direct comparison of various national surveys is very difficult and should be performed very vigilantly. Characteristics of enrolled population, study design, CKD definitions and used eGFR equations could be reasons of significant difference among various survey. Already in 2016, DeNicola and Zoccali pointed on this issue [43]. One of the most important causes for discrepancy in reported results is usage of different equations. Therefore, our results on CKD prevalence are much more alike results of studies which used CKD EPI equation: 9.1%, 10.0%, 11.5%, 11.9%, and 12.5% in India, Malaysia, Switzerland, Australia, England and Canada, respectively [41,44,45,46,47,48,49].
Using a single cut-off point of ACR > 30 mg/g, in our cohort weighted prevalence of albuminuria was 15.1 %, being higher in men than in women. Our results are in concordance with reports from China (19%) and Canada (20%) but were higher than results obtained in US (11.7%), Australia (6%), Italy (4.8%), Japan (4.6%) [40,50,51,52,53,54]. Observed differences in the albuminuria prevalence could be explained with different definitions and methods but it also strongly depends on characteristics of examined population. Observed higher prevalence of albuminuria in our study was related to high prevalence of diabetes, hypertension, and overweight/obesity in Croatian population. Results from Health Survey for England showed increased prevalence of albuminuria with slight J shape pattern where 88% of albuminuria was observed in people with eGFR >60 which agrees with our results [55].
In our study, estimates of the prevalence of subjects in specific KDIGO CKD GA categories showed that very few subjects have high (4.5%) or very-high (1.7%) cardio-renal risk considering combined measure of eGFR and ACR level. Most of subjects (71.9%) had normal eGFR (≥60 mL/min/1.73 m2) and normal albuminuria (ACR <30 mg/g), and 14.9% had normal eGFR, but ACR > 30 mg/g. These results are concordant with reports from other countries [40,50,51,52,53,54]. Our results on prevalence of each KDIGO category in our general population are completely in line with reported international total combined prevalence [56]. We can estimate that in Croatia more than 311.000 adults between 18 and 90 years of age have CKD stage ≥ G3A A2. High and very-high risk was estimated to be present in 177.117 and these subjects should be referred to nephrologist. However, this would be very difficult task as Croatia is lacking nephrologist as many other countries. Therefore, Croatian Renal Association and Croatian Hypertension League have started with education of family physicians preparing curriculum in nephrology and curriculum in hypertension. Furthermore, we succeeded in negotiation with national insurance company which is now fully covering costs for determination of ACR in primary, secondary and tertiary care for all subjects with high cardio-kidney-metabolic risk. This will hopefully improve earlier detection not only of patients in advanced CKD stages but also those in the beginning of the cardio-kidney-metabolic continuum who have moderate risk. According to our estimates there are 522.065 adult citizen in Croatia in this category, and they deserve particular attention. On the long-term, they can have most benefit not only from new cardio-reno protective drugs, but also from changing poor lifestyle. To increase awareness and to improve health literacy of general population, Croatian Hypertension League has established educational digital platform named Hunting the Silent Killer where one of most important tasks is education how to change poor lifestyle (https://tihiubojica.hr/)
Hypertension, diabetes and overweight/obesity were significantly more prevalent in our CKD group compared to subject not having CKD. There were significantly less controlled and much more untreated hypertensive patients in the CKD group which could contribute to higher CV risk and more CV morbidity in these patients. History of atrial fibrillation, heart failure and ischemic stroke were significantly more frequently presented in CKD than in non-CKD group. Myocardial infarction and hemorrhagic stroke were also more prevalent in CKD than in non-CKD group, but the difference was not significant. Association of CKD with CV and cerebrovascular morbidity was also reported in other studies, but wide variability in its prevalence was found which also could explain observed differences in CKD prevalence among various surveys [57]. In univariate logistic regression we found various demographic, socio-economic, behavioral and health related risk factors to be associated with CKD. In multivariate regression analysis older age, male gender, diabetes, uric acid and ePWV were independently associated with higher CKD prevalence. Similar results were reported by other authors with slight differences depending on basal characteristics of enrolled populations. In GDB study impaired fasting plasma glucose, high BP, high BMI, and diet high in sodium were risk factors for CKD, but high BP contributed mostly to CKD burden in east Asia, eastern Europe, tropical Latin America, and western sub-Saharan Africa, whereas high fasting plasma glucose was the leading risk factor for CKD in all other regions [1]. Even in non-obese individuals, clustering of CV risk factors has impact on CKD. In a Japanese study adult non-obese subject with at least three metabolic factors had an equal or slightly higher risk of renal dysfunction than obese subjects with ≥ 3 metabolic factors [58]. In our group uric acid was significantly associated with CKD prevalence. The association of uric acid with CKD and hyperuricemia with progression of disease remains controversial and debatable. Systematic review of 23 studies containing 212,740 subjects found the pooled prevalence of 43.6% hyperuricemia in patients with CKD globally, and it was reported as 67.4% and 32.6% in case of male and female patients, respectively [59]. In our population we failed to find differences in salt consumption between CKD and non-CKD population. Some other authors found sodium-to-potassium ratio to be more important risk factor for CKD than solely salt ingestion [60]. Our result on this topic will be published soon.
Low family monthly income and less education were associated with CKD prevalence in our cohort. These results are in line with reports that a significant increase in CKD DALYs globally was most pronounced in middle and low-middle SDI quintiles [1,5]. The study reported important differences by geographic region classified by income level had impact on CKD age-standardized prevalence in both men and women: 8.6% and 9.6%, respectively in high-income countries, and 10.6% and 12.5%, respectively in low- and middle-income countries [56]. In multicenter German Chronic Kidney Disease cohort, subjects with low educational attainment (vs. high) had a higher risk for mortality and kidney failure, particularly for diabetic kidney disease [61]. Although not unanimously reported, in many studies the prevalence of CKD tends to be higher in women than in men [62]. One important explanation for such finding is that a single cutoff of <60 ml/min per 1.73 m2 for CKD definition may result in over-diagnosing CKD in women [62]. Results on higher prevalence in women reported in many studies are in contrast with observations from in vitro experiments which found the protective effect of estrogen and detrimental effect of testosterone on non-diabetic CKD [21]. Beside the hormonal reasons, differences in lifestyle and socioeconomic factors were reported to be associated with such findings [63]. These results are conflicting data that indicate a higher prevalence and incidence of CKD, faster progression and higher mortality rate in men [19,38,62,63,64,65]. Overall, the decline of eGFR with age in men was 0.92 ml/min per 1.73 m2 compared with 0.75 ml/min per 1.73 m2 in women [66]. In our study, like in Italian and Spanish cohorts, the prevalence of CKD was higher in men than in women [40,67]. We failed to find differences in age or prevalence of hypertension between men and women, but men were significantly more overweight/obese and more frequently had diabetes, ingested more salt, and had higher values of BP, fasting blood glucose, uric acid and faster ePWV. All these characteristics made them more prone for CKD than women.
Only 9.5 % of our CKD patients were aware of having CKD. This is in line with other reports on only 6% of the general population and 10% of the high-risk population to be aware of their CKD [25,40,42]. In our group, unaware of having CKD were older with lower income and qualifications, less educated, having more frequently diabetes, hypertension (more uncontrolled) and milder renal impairment. The GBD Study has shown that CKD awareness is generally low worldwide, with significant disparities between high-income and low-income countries [1]. Observed association of unawareness with lower education and poorer socio-economic index is in line with general observation that CKD is particularly detrimental in vulnerable subpopulations. Patients with milder renal impairment were also less aware and our result are like results of other studies [25,26,40,42,68]. This could be explained by having less (or none) symptoms of CKD in early stages compared to more advanced CKD stages. Interestingly, in our group awareness was associated with men gender like it was reported in Poland [42]. Higher prevalence of hypertension, diabetes, atrial fibrillation and particularly lower percentage of controlled hypertensive patients in the unaware group is particularly disturbing and disappointing. This reflects not only poor awareness of patients or subjects with CKD but is also an indicator of clinical inertia and poor health literacy of physicians. Namely, most of them, at least treated hypertensive patients, were under control of physicians who obviously neither checked kidney function nor informed their patient of having CKD. The International Society of Nephrology's "Global Kidney Health Atlas" reports that many countries lack adequate CKD awareness programs, especially in regions with limited healthcare access underscoring the critical need for enhanced public health initiatives to improve CKD awareness, early detection, and management globally. Increased efforts in education, screening, and healthcare access are essential [69]. Our results confirmed that this is utmost need for Croatia where both poor awareness and clinical inertia should be improved.
5. Strengths and Limitations
This study has several important strengths. Our results are based on a large nationwide, population-based sample of general adults in Croatia. We weighted data which allowed as to estimate a population-representative prevalence of CKD. Kidney dysfunction was determined following the most recent guidelines, combining CKD EPI eGFR and ACR enabling us to define CKD GA stages. One of important strong points is fact that we determined ACR from adequate and reliable 24-hour urine sample. Furthermore, we analyzed broad set of risk factors for CKD, including demographic, socio-economic, clinical, and lifestyle variables. Obvious limitation is the cross-sectional design of the study. Secondly, we measured eGFR and ACR only once which could overestimate the prevalence. Next limitation was that we excluded subjects in residential care potentially having CKD which can underestimate the prevalence. Another important limitation was the lack of data on cystatin C-based eGFR which would increase accuracy. And finally, we did not consider aging and did not use different suggested cut offs for different age groups and/or we did not use BIS equation for elderly. The definition by eGFR <60 ml/min per 1.73 m2 may not be optimal for defining CKD in the elderly, because 50% of persons older than 70 years might be labeled as having CKD, while it is more likely that they have only physiologic aging of the kidneys [70]. In recent years, the need for an age dependent definition of CKD have been proposed, and some authors have suggested that the eGFR thresholds for defining CKD could be adapted to <75 m/min per 1.73 m2 in youth, <60 ml/min per 1.73 m2 for middle age, and <45 ml/min per 1.73 m2 for older adults [27,28]. Using various definitions and/or different equations for elderly could bring our results closer to real prevalence. However, it would disable us to compare our results with worldwide published results on CKD prevalence, while most of studies used a single cut off for CKD and in last decade majority are using the CKD EPI equation and KDIGO staging. Furthermore, large population-based studies indicate that even in older adults at lower risk for kidney failure, stage 3 CKD is associated with an elevated risk of mortality, CV events and acute kidney injury [71]. Therefore, KDIGO guidelines support the use of eGFR <60 ml/min/1.73m2 threshold to define CKD regardless of age group.
6. Conclusions
This is the first evidence-based report on the prevalence, characteristics, and awareness of CKD in Croatia, but also in this part of Europe. High prevalence of CKD and unfavorable CV risk profile associated with very poor awareness strongly point on need for systematic actions in Croatia which will ameliorate high burden of this important public health problem. Nephrology community together with hypertensiologists, diabetologist and cardiologist with strong support of national health authorities should jointly organize continuous activities which will increase awareness and improve clinical inertia helping in earlier detection, organization of primordial and primary prevention and evidence-based medical treatment also considering knowledge on epidemiology and pathophysiology. Some of first steps were already done – all physicians in Croatia can determine ACR in all subjects with high cardio-kidney-metabolic risk, and this is fully covered by the national insurance company. Additionally, we have started with education of general population (https://tihiubojica.hr/; https://www.70-26.hr/ https://www.kolesterol.hr ) and health care workers (www.healthmed; https://hdh.healthmed.hr/curriculum-hypertensiologiae/) [72]. With these actions we hope to slower progression of CKD and substantially decrease CV risk. There is no try. Failure is not an option.
Funding
This study was funded by a Croatian Science Foundation research grant (IP-06-2016), which supported the project Epidemiology of hypertension and salt intake in Croatia (EH—UH 2); unrestricted research grants from the Croatian Society of Hypertension and the Croatian Hypertension League; the Croatian Science Foundation program “Young Researchers’ Career Development Project—training of doctoral students”, which funded the work of Mihaela Marinović Glavić (PhD student), DOK-2018-09; and financial and organization help from the School of Medicine University of Zagreb and the Croatian Institute of Public Health.
Acknowledgments
We would like to thank all participants who agreed to participate, including family physicians, nurses, residents, fellows, and medical students who, as members of the MET, participated in field work. We would also like to thank the medical directors of outpatient clinics across Croatia, who allowed us to use their rooms and facilities for our field work. Warm and special thanks to Jasna Lovrić, vice-dean of the School of Medicine, and to the d8solutions company, digital partner of the Croatian Hypertension League, who helped us organize the field work.
Conflicts of Interest
On behalf of all authors, the corresponding author states that there are no conflicts of interest.
References
- GBD Chronic Kidney Disease Collaboration. Global, regional, and national burden of chronic kidney disease, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2020; 29;395(10225):709-733. [CrossRef]
- Mills K.T., Xu Y., Zhang W., et al. A systematic analysis of worldwide population-based data on the global burden of chronic kidney disease in 2010. Kidney Int. 2015;88:950–957. [CrossRef]
- GBD Mortality Causes of Death Collaborators Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;385:117–171. [CrossRef]
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392:1789–1858. [CrossRef]
- Y, Bowe B, Mokdad AH, Xian H, Yan Y, Li T, Maddukuri G, Tsai CY, Floyd T, Al-Aly Z. Analysis of the Global Burden of Disease study highlights the global, regional, and national trends of chronic kidney disease epidemiology from 1990 to 2016. Kidney Int. 2018;94(3):567-581. [CrossRef]
- Couser WG, Remuzzi G, Mendis S, Tonelli M. The contribution of chronic kidney disease to the global burden of major noncommunicable diseases. Kidney Int. 2011; 80:1258–1270. [CrossRef]
- Sarnak MJ, Levey AS, Schoolwerth AC. Kidney disease as a risk factor for development of cardiovascular disease: a statement from the American Heart Association councils on kidney in cardiovascular disease, high blood pressure research, clinical cardiology, and epidemiology and prevention. Circulation. 2003; 108:2154–2169. [CrossRef]
- Matsushita K, Coresh J, Sang Y. Estimated glomerular filtration rate and albuminuria for prediction of cardiovascular outcomes: a collaborative meta-analysis of individual participant data. Lancet Diabetes Endocrinol. 2015; 3:514–525. [CrossRef]
- Chronic Kidney Disease Prognosis Consortium Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: a collaborative meta-analysis. Lancet. 2010; 375:2073–2081. [CrossRef]
- Visseren FLJ, Mach F, Smulders YM, Carballo D, Koskinas KC, Bäck M, Benetos A, Biffi A, Boavida JM, Capodanno D, Cosyns B, Crawford C, Davos CH, Desormais I, Di Angelantonio E, Franco OH, Halvorsen S, Hobbs FDR, Hollander M, Jankowska EA, Michal M, Sacco S, Sattar N, Tokgozoglu L, Tonstad S, Tsioufis KP, van Dis I, van Gelder IC, Wanner C, Williams B; ESC National Cardiac Societies; ESC Scientific Document Group. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur Heart J. 2021 Sep 7;42(34):3227-3337. [CrossRef]
- Matsushita K, Jassal SK, Sang Y, Ballew SH, Grams ME, Surapaneni A, Arnlov J, Bansal N, Bozic M, Brenner H, Brunskill NJ, Chang AR, Chinnadurai R, Cirillo M, Correa A, Ebert N, Eckardt KU, Gansevoort RT, Gutierrez O, Hadaegh F, He J, Hwang SJ, Jafar TH, Kayama T, Kovesdy CP, Landman GW, Levey AS, Lloyd-Jones DM, Major RW, Miura K, Muntner P, Nadkarni GN, Naimark DM, Nowak C, Ohkubo T, Pena MJ, Polkinghorne KR, Sabanayagam C, Sairenchi T, Schneider MP, Shalev V, Shlipak M, Solbu MD, Stempniewicz N, Tollitt J, Valdivielso JM, van der Leeuw J, Wang AY, Wen CP, Woodward M, Yamagishi K, Yatsuya H, Zhang L, Schaeffner E, Coresh J. Incorporating kidney disease measures into cardiovascular risk prediction: Development and validation in 9 million adults from 72 datasets. EClinicalMedicine. 2020; 14; 27:100552. [CrossRef]
- Grundy SM, Stone NJ, Bailey AL, Beam C, Birtcher KK, Blumenthal RS, Braun LT, de Ferranti S, Faiella-Tommasino J, Forman DE, Goldberg R, Heidenreich PA, Hlatky MA, Jones DW, Lloyd-Jones D, Lopez-Pajares N, Ndumele CE, Orringer CE, Peralta CA, Saseen JJ, Smith SC Jr, Sperling L, Virani SS, Yeboah J. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019; 18;139(25):e1082-e1143. [CrossRef]
- Piepoli MF, Hoes AW, Agewall S, Albus C, Brotons C, Catapano AL, Cooney MT, Corrà U, Cosyns B, Deaton C, Graham I, Hall MS, Hobbs FDR, Løchen ML, Löllgen H, Marques-Vidal P, Perk J, Prescott E, Redon J, Richter DJ, Sattar N, Smulders Y, Tiberi M, van der Worp HB, van Dis I, Verschuren WMM, Binno S; ESC Scientific Document Group. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts) Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur Heart J. 2016; 1;37(29):2315-2381. [CrossRef]
- Ndumele CE, Rangaswami J, Chow SL, Neeland IJ, Tuttle KR, Khan SS, Coresh J, Mathew RO, Baker-Smith CM, Carnethon MR, Despres JP, Ho JE, Joseph JJ, Kernan WN, Khera A, Kosiborod MN, Lekavich CL, Lewis EF, Lo KB, Ozkan B, Palaniappan LP, Patel SS, Pencina MJ, Powell-Wiley TM, Sperling LS, Virani SS, Wright JT, Rajgopal Singh R, Elkind MSV; American Heart Association. Cardiovascular-Kidney-Metabolic Health: A Presidential Advisory from the American Heart Association. Circulation. 2023;14;148(20):1606-1635. [CrossRef]
- GBD. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016; 388, 1459–1544. [CrossRef]
- Foreman KJ, Marquez N, Dolgert A, Fukutaki K, Fullman N, McGaughey M, Pletcher MA, Smith AE, Tang K, Yuan CW, Brown JC, Friedman J, He J, Heuton KR, Holmberg M, Patel DJ, Reidy P, Carter A, Cercy K, Chapin A, Douwes-Schultz D, Frank T, Goettsch F, Liu PY, Nandakumar V, Reitsma MB, Reuter V, Sadat N, Sorensen RJD, Srinivasan V, Updike RL, York H, Lopez AD, Lozano R, Lim SS, Mokdad AH, Vollset SE, Murray CJL. Forecasting life expectancy, years of life lost, and all-cause and cause-specific mortality for 250 causes of death: reference and alternative scenarios for 2016-40 for 195 countries and territories. Lancet. 2018; 10;392(10159):2052-2090. [CrossRef]
- Radhakrishnan J, Remuzzi G, Saran R, Williams DE, Rios-Burrows N, Powe N; CDC-CKD Surveillance Team; Brück K, Wanner C, Stel VS; European CKD Burden Consortium; Venuthurupalli SK, Hoy WE, Healy HG, Salisbury A, Fassett RG; CKD.QLD group; O'Donoghue D, Roderick P, Matsuo S, Hishida A, Imai E, Iimuro S. Taming the chronic kidney disease epidemic: a global view of surveillance efforts. Kidney Int. 2014;86(2):246-50. [CrossRef]
- Carrero JJ, Hecking M, Chesnaye NC, Jager KJ. Sex and gender disparities in the epidemiology and outcomes of chronic kidney disease. Nat Rev Nephrol. 2018;14(3):151-164. [CrossRef]
- Bikbov B, Perico N, Remuzzi G; on behalf of the GBD Genitourinary Diseases Expert Group. Disparities in Chronic Kidney Disease Prevalence among Males and Females in 195 Countries: Analysis of the Global Burden of Disease 2016 Study. Nephron. 2018;139(4):313-318. [CrossRef]
- Bairey Merz CN, Dember LM, Ingelfinger JR, Vinson A, Neugarten J, Sandberg KL, Sullivan JC, Maric-Bilkan C, Rankin TL, Kimmel PL, Star RA; participants of the National Institute of Diabetes and Digestive and Kidney Diseases Workshop on “Sex and the Kidneys”. Sex and the kidneys: current understanding and research opportunities. Nat Rev Nephrol. 2019;15(12):776-783. [CrossRef]
- Silbiger SR, Neugarten J. The impact of gender on the progression of chronic renal disease. Am J Kidney Dis. 1995;25(4):515-33. [CrossRef]
- Noborisaka Y. Smoking and chronic kidney disease in healthy populations. Nephrourol Mon. 2013 Winter;5(1):655-67. [CrossRef]
- Centers for Disease Control and Prevention. Chronic Kidney Disease in the United States, 2021 (US Department of Health and Human Services, 2021).
- Tuot DS, Zhu Y, Velasquez A, Espinoza J, Mendez CD, Banerjee T, Hsu CY, Powe NR. Variation in Patients' Awareness of CKD according to How They Are Asked. Clin J Am Soc Nephrol. 2016; 7;11(9):1566-1573. [CrossRef]
- Ene-Iordache B, Perico N, Bikbov B, Carminati S, Remuzzi A, Perna A, Islam N, Bravo RF, Aleckovic-Halilovic M, Zou H, Zhang L, Gouda Z, Tchokhonelidze I, Abraham G, Mahdavi-Mazdeh M, Gallieni M, Codreanu I, Togtokh A, Sharma SK, Koirala P, Uprety S, Ulasi I, Remuzzi G. Chronic kidney disease and cardiovascular risk in six regions of the world (ISN-KDDC): a cross-sectional study. Lancet Glob Health. 2016;4(5):e307-19. [CrossRef]
- Florea A, Jacobs ET, Harris RB, Klimentidis YC, Thajudeen B, Kohler LN. Chronic kidney disease unawareness and determinants using 1999-2014 National Health and Nutrition Examination Survey Data. J Public Health (Oxf). 2022; 25;44(3):532-540. [CrossRef]
- Glassock RJ, Delanaye P, Rule AD. Should the definition of CKD be changed to include age adapted GFR criteria? YES. Kidney Int. 2020; 97:34-41. [CrossRef]
- Delanaye P, Jager KJ, Bökenkamp A, et al. CKD: a call for an age-adapted definition. J Am Soc Nephrol. 2019; 30:1785-1805. [CrossRef]
- Stevens PE, Levin A; Kidney Disease: Improving Global Outcomes Chronic Kidney Disease Guideline Development Work Group Members. Evaluation and management of chronic kidney disease: synopsis of the kidney disease: improving global outcomes 2012 clinical practice guideline. Ann Intern Med. 2013; 4;158(11):825-30. [CrossRef]
- Ruggenenti P, Cravedi P, Remuzzi G. Mechanisms and treatment of CKD. J Am Soc Nephrol. 2012;23(12):1917-28. [CrossRef]
- chrome-extension://.
- efaidnbmnnnibpcajpcglclefindmkaj/https://health.ec.europa.eu/system/files/2021-12/2021_chp_hr_english.pdf.
- https://www.who.int/publications/i/item/9789240015128 accessed on 26th June 2024.
- Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, Clement DL, Coca A, de Simone G, Dominiczak A, Kahan T, Mahfoud F, Redon J, Ruilope L, Zanchetti A, Kerins M, Kjeldsen SE, Kreutz R, Laurent S, Lip GYH, McManus R, Narkiewicz K, Ruschitzka F, Schmieder RE, Shlyakhto E, Tsioufis C, Aboyans V, Desormais I; ESC Scientific Document Group. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur Heart J. 2018; 1;39(33):3021-3104. [CrossRef]
- Vrdoljak A, Vrkić TZ, Kos J, Vitale K, Premuzić V, Laganović M, Jelaković B. Blood pressure measurement--do not sweat the small stuff and it is all small stuff?! Position paper of the Croatian national referral center for hypertension, center of excellence of the European Society of Hypertension. Lijec Vjesn. 2014;136(1-2):33-43.
- Greve SV, Blicher MK, Kruger R, Sehestedt T, Gram-Kampmann E, Rasmussen S, Vishram JK, Boutouyrie P, Laurent S, Olsen MH. Estimated carotid-femoral pulse wave velocity has similar predictive value as measured carotid-femoral pulse wave velocity. J Hypertens. 2016;34(7):1279-89. [CrossRef]
- Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF 3rd, Feldman HI, Kusek JW, Eggers P, Van Lente F, Greene T, Coresh J; CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration). A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009; 5;150(9):604-12. Erratum in: Ann Intern Med. 2011; 20;155(6):408. [CrossRef]
- https://dzs.gov.hr/u-fokusu/popis-2021/88 accessed on 26th June 2024.
- Mazhar F, Sjölander A, Fu EL, Ärnlöv J, Levey AS, Coresh J, Carrero JJ. Estimating the prevalence of chronic kidney disease while accounting for nonrandom testing with inverse probability weighting. Kidney Int. 2023;103(2):416-420. [CrossRef]
- Hill NR, Fatoba ST, Oke JL, Hirst JA, O'Callaghan CA, Lasserson DS, Hobbs FD. Global Prevalence of Chronic Kidney Disease - A Systematic Review and Meta-Analysis. PLoS One. 2016; 6;11(7):e0158765. [CrossRef]
- De Nicola L, Donfrancesco C, Minutolo R, Lo Noce C, Palmieri L, De Curtis A, Iacoviello L, Zoccali C, Gesualdo L, Conte G, Vanuzzo D, Giampaoli S; ANMCO-SIN Research Group. Prevalence and cardiovascular risk profile of chronic kidney disease in Italy: results of the 2008-12 National Health Examination Survey. Nephrol Dial Transplant. 2015;30(5):806-14. [CrossRef]
- Alkerwi, A., Sauvageot, N., El Bahi, I. et al. Prevalence and related risk factors of chronic kidney disease among adults in Luxembourg: evidence from the observation of cardiovascular risk factors (ORISCAV-LUX) study. BMC Nephrol. 2017; 18, 358. [CrossRef]
- Zdrojewski Ł, Zdrojewski T, Rutkowski M, Bandosz P, Król E, Wyrzykowski B, Rutkowski B. Prevalence of chronic kidney disease in a representative sample of the Polish population: results of the NATPOL 2011 survey. Nephrol Dial Transplant. 2016;31(3):433-9. [CrossRef]
- De Nicola L, Zoccali C. Chronic kidney disease prevalence in the general population: heterogeneity and concerns. Nephrology Dialysis Transplantation. 2016; 1;31(3):331-5. [CrossRef]
- Anand S, Shivashankar R, Ali MK et al. Prevalence of chronic kidney disease in two major Indian cities and projections for associated cardiovascular disease. Kidney Int 2015; 88: 178–185. [CrossRef]
- Hooi LS, Ong LM, Ahmad G et al. A population-based study measuring the prevalence of chronic kidney disease among adults in West Malaysia. Kidney Int 2013; 84: 1034–1040. [CrossRef]
- Ponte B, Pruijm M, Marques-Vidal P et al. Determinants and burden of chronic kidney disease in the population-based CoLaus study: a crosssectional analysis. Nephrol Dial Transplant 2013; 28: 2329–2339. [CrossRef]
- White SL, Polkinghorne KR, Atkins RC et al. Comparison of the prevalence and mortality risk of CKD in Australia using the CKD Epidemiology Collaboration (CKD-EPI) and Modification of Diet in Renal Disease (MDRD) Study GFR estimating equations: the AusDiab (Australian Diabetes, Obesity and Lifestyle) Study. Am J Kidney Dis 2010; 55: 660–670. [CrossRef]
- Fraser SD, Aitken G, Taal MW et al. Exploration of chronic kidney disease prevalence estimates using new measures of kidney function in the health survey for England. PLoS One 2015; 10: e0118676. [CrossRef]
- Arora P, Vasa P, Brenner D et al. Prevalence estimates of chronic kidney disease in Canada: results of a nationally representative survey. CMAJ 2013; 185: E417–E423. [CrossRef]
- Chen F, Yang W, Weng J, Jia W, Ji L, Xiao J, Shan Z, Liu J, Tian H, Ji Q, Zhu D, Ge J, Lin L, Chen L, Guo X, Zhao Z, Li Q, Zhou Z, Shan G, Lu J; China National Diabetes and Metabolic Disorders Study Group. Albuminuria: Prevalence, associated risk factors and relationship with cardiovascular disease. J Diabetes Investig. 2014;5(4):464-71. [CrossRef]
- Zacharias, J.M., Young, T.K., Riediger, N.D. et al. Prevalence, risk factors and awareness of albuminuria on a Canadian First Nation: A community-based screening study. BMC Public Health 2012; 12, 290. [CrossRef]
- J Reed III, N Kopyt. Prevalence of Albuminuria in the U.S. Adult Population Over the age of 40: Results from the National Health and Nutrition Examination Survey (1999-2008). The Internet Journal of Nephrology. 2009 Volume 6 Number 1.
- Atkins RC, Polkinghorne KR, Briganti EM, Shaw JE, Zimmet PZ, Chadban SJ. Prevalence of albuminuria in Australia: the AusDiab kidney study. Kidney International. 2004; 1;66:S22-4. [CrossRef]
- Tanaka S, Takase H, Dohi Y, Kimura G. The prevalence and characteristics of microalbuminuria in the general population: a cross-sectional study. BMC research notes. 2013;6:1-7. [CrossRef]
- Hounkpatin HO, Harris S, Fraser SDS, Day J, Mindell JS, Taal MW, O'Donoghue D, Roderick PJ. Prevalence of chronic kidney disease in adults in England: comparison of nationally representative cross-sectional surveys from 2003 to 2016. BMJ Open. 2020; 13;10(8):e038423. [CrossRef]
- Kovesdy CP. Epidemiology of chronic kidney disease: an update 2022. Kidney Int Suppl (2011). 2022;12(1):7-11. [CrossRef]
- Murton M, Goff-Leggett D, Bobrowska A, Garcia Sanchez JJ, James G, Wittbrodt E, Nolan S, Sörstadius E, Pecoits-Filho R, Tuttle K. Burden of Chronic Kidney Disease by KDIGO Categories of Glomerular Filtration Rate and Albuminuria: A Systematic Review. Adv Ther. 2021;38(1):180-200. [CrossRef]
- Nishikawa K, Takahashi K, Okutani T, Yamada R, Kinaga T, Matsumoto M, Yamamoto M. Risk of chronic kidney disease in non-obese individuals with clustering of metabolic factors: a longitudinal study. Intern Med. 2015;54(4):375-82. [CrossRef]
- Rashid I, Katravath P, Tiwari P, D’Cruz S, Jaswal S, Sahu G. Hyperuricemia—a serious complication among patients with chronic kidney disease: a systematic review and meta-analysis. Explor Med. 2022;3:249. [CrossRef]
- Kieneker L, Bakker S, de Boer R, Navis G, Gansevoort R, Joosten M. Low potassium excretion but not high sodium excretion is associated with increased risk of developing chronic kidney disease Kidney International 2016; 90: 888–896;. [CrossRef]
- Winitzki D, Zacharias HU, Nadal J, Baid-Agrawal S, Schaeffner E, Schmid M, Busch M, Bergmann MM, Schultheiss U, Kotsis F, Stockmann H, Meiselbach H, Wolf G, Krane V, Sommerer C, Eckardt KU, Schneider MP, Schlieper G, Floege J, Saritas T. Educational Attainment Is Associated With Kidney and Cardiovascular Outcomes in the German CKD (GCKD) Cohort. Kidney Int Rep. 2022; 14;7(5):1004-1015. [CrossRef]
- Neugarten J, Golestaneh L. Influence of Sex on the Progression of Chronic Kidney Disease. Mayo Clin Proc. 2019;94(7):1339-1356. [CrossRef]
- Ricardo AC, Yang W, Sha D, Appel LJ, Chen J, Krousel-Wood M, Manoharan A, Steigerwalt S, Wright J, Rahman M, Rosas SE, Saunders M, Sharma K, Daviglus ML, Lash JP; CRIC Investigators. Sex-Related Disparities in CKD Progression. J Am Soc Nephrol. 2019;30(1):137-146. [CrossRef]
- Hecking M, Bieber BA, Ethier J, Kautzky-Willer A, Sunder-Plassmann G, Säemann MD, Ramirez SP, Gillespie BW, Pisoni RL, Robinson BM, Port FK. Sex-specific differences in hemodialysis prevalence and practices and the male-to-female mortality rate: the Dialysis Outcomes and Practice Patterns Study (DOPPS). PLoS Med. 2014 Oct 28;11(10):e1001750. [CrossRef]
- Iseki K, Nakai S, Shinzato T, Nagura Y, Akiba T; Patient Registration Committee of the Japanese Society for Dialysis Therapy. Increasing gender difference in the incidence of chronic dialysis therapy in Japan. Ther Apher Dial. 2005 Oct;9(5):407-11. [CrossRef]
- van der Burgh AC, Rizopoulos D, Ikram MA, Hoorn EJ, Chaker L. Determinants of the Evolution of Kidney Function With Age. Kidney Int Rep. 2021; 16;6(12):3054-3063. [CrossRef]
- Gorostidi M, Sánchez-Martínez M, Ruilope LM, Graciani A, de la Cruz JJ, Santamaría R, Del Pino MD, Guallar-Castillón P, de Álvaro F, Rodríguez-Artalejo F, Banegas JR. Chronic kidney disease in Spain: Prevalence and impact of accumulation of cardiovascular risk factors. Nefrologia (Engl Ed). 2018;38(6):606-615. English, Spanish. [CrossRef]
- Liu Q, Li Z, Wang H et al. High prevalence and associated risk factors for impaired renal function and urinary abnormalities in a rural adult population from southern China. PLoS One. 2012; 7: e47100. [CrossRef]
- https://www.theisn.org/wp-content/uploads/media/ISN%20Atlas_2023%20Digital_REV_2023_10_03.pdf accessed on 21st June 2024.
- Hommos MS, Glassock RJ, Rule AD. Structural and Functional Changes in Human Kidneys with Healthy Aging. J Am Soc Nephrol. 2017;28(10):2838-2844. [CrossRef]
- De Nicola L, Minutolo R, Chiodini P, et al. The effect of increasing age on the prognosis of non-dialysis patients with chronic kidney disease receiving stable nephrology care. Kidney Int. 2012;82:482-488. [CrossRef]
- Jelaković B, Pećin I, Lang VB, Braš M, Capak K, Jelaković A, Kralj V, Miličić D, Soldo A, Bubaš M. Improving blood pressure and dyslipidemia control by increasing health literacy in Croatia-missions 70/26 & Do you know what is your number. Blood Press. 2024 Dec;33(1):2371863. [CrossRef]
Figure 1.
Final number of the subjects included in the study.# Either urine volume < 500 ml or urine creatinine not in ranges (5.9–26.0 mmol/24 h for men; 4.0–16.4 mmol/24 h women) or urinary tract infection
Figure 1.
Final number of the subjects included in the study.# Either urine volume < 500 ml or urine creatinine not in ranges (5.9–26.0 mmol/24 h for men; 4.0–16.4 mmol/24 h women) or urinary tract infection
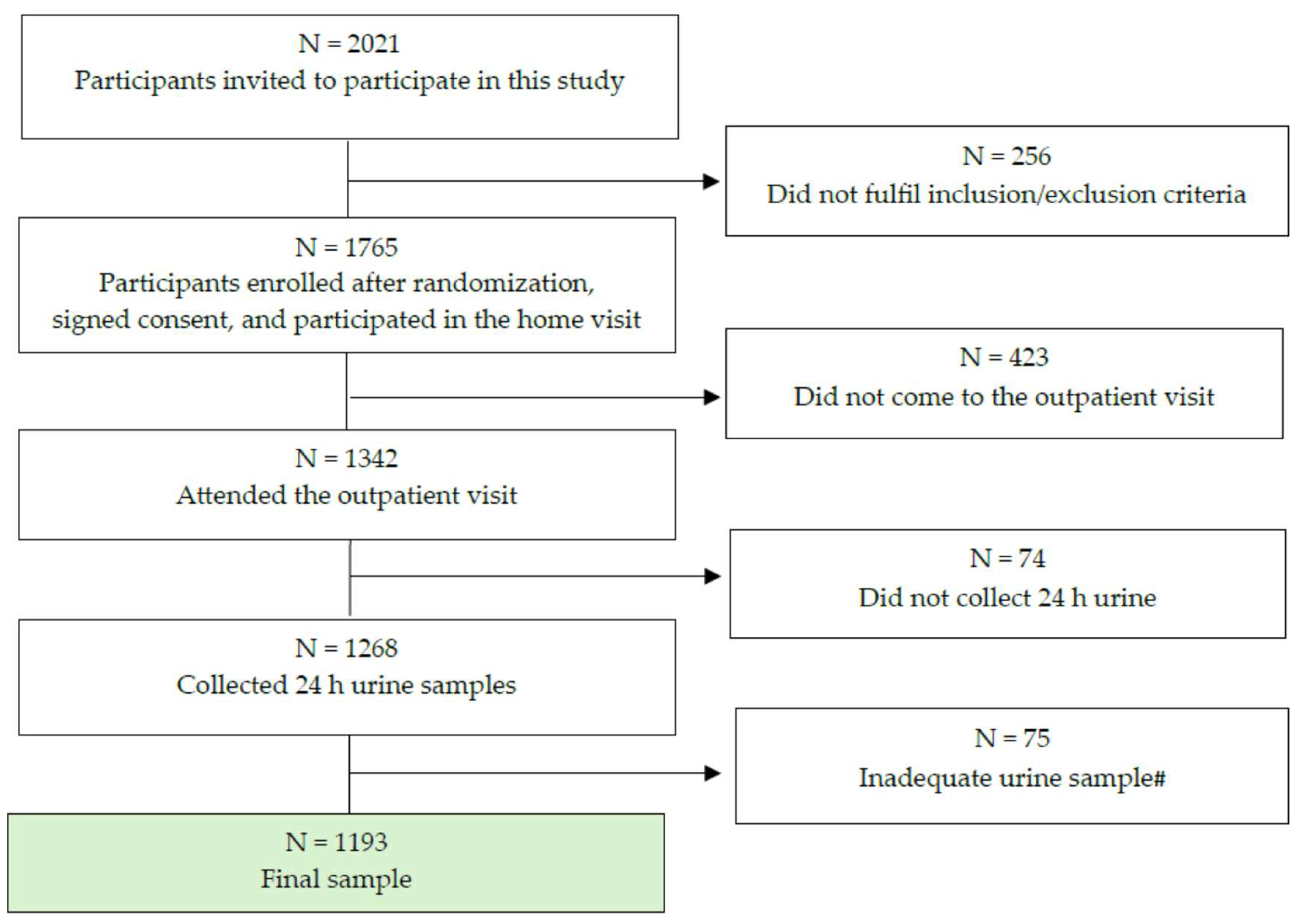
Figure 2.
Study design.
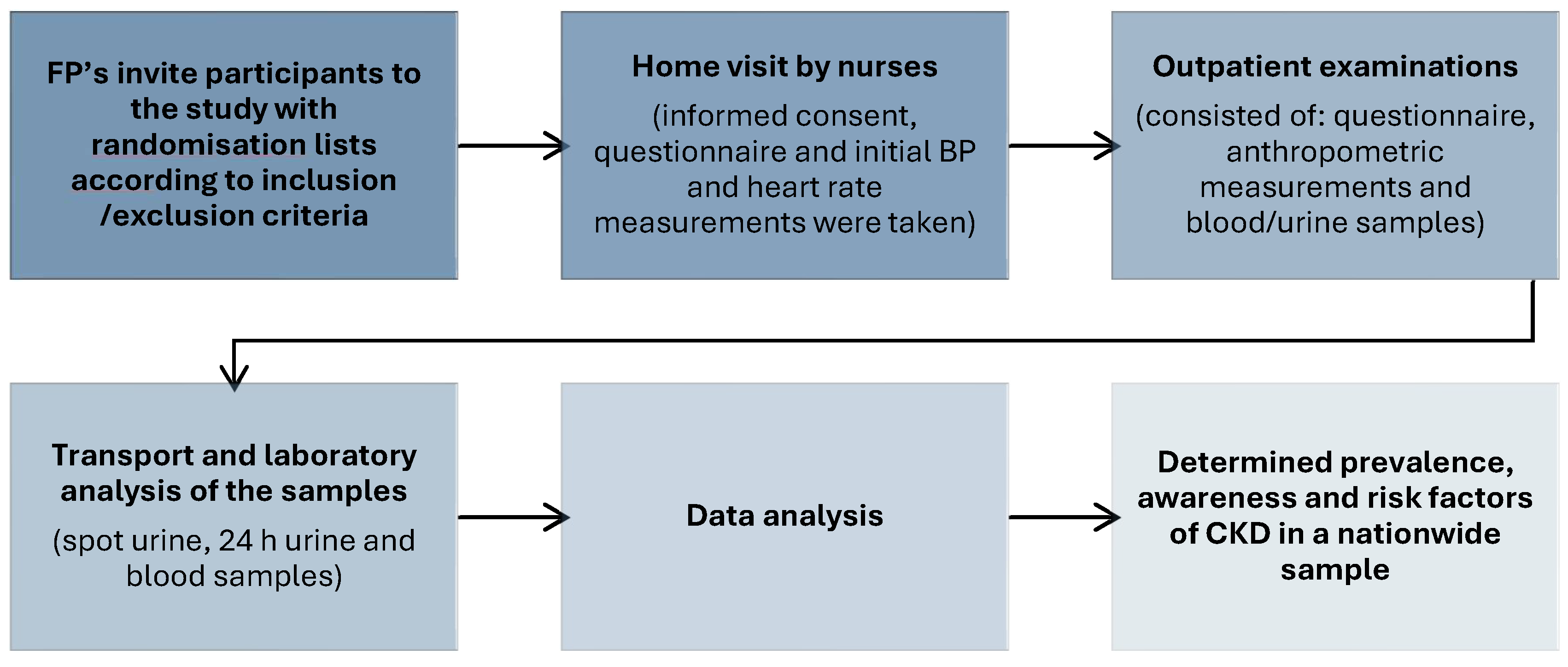
Table 1.
Weighted prevalence of chronic kidney disease in adult population using various definitions.
Table 1.
Weighted prevalence of chronic kidney disease in adult population using various definitions.
| Overall CKD (any KDIGO stage) |
CKD ≥ stage 3GA A2 |
CKD < 60 ml/min/1.73 m2 |
ACR > 30 mg/g |
|||||
|---|---|---|---|---|---|---|---|---|
| % | 95% CI | % | 95% CI | % | 95% CI | % | 95% CI | |
| All | 17.1 | 8.0-15.0 | 9.8 | 6.6- 9.5 | 7.9 | 6.5- 9.5 | 15.1 | 7.0-15.2 |
| Men | 19.3 | 8.3-17.3 | 11.8 | 7.6-12.8 | 10.7 | 8.0-13.3 | 17.5 | 6.9-16.0 |
| Women | 14.9 | 7.1-11.5 | 7.9 | 5.2- 8.4 | 6.5 | 4.8- 8.1 | 13.5 | 6.5-10.7 |
Table 2.
Distribution of adult population based on eGFR and ACR with prevalence estimates according to KDIGO chronic kidney disease risk groups.
Table 2.
Distribution of adult population based on eGFR and ACR with prevalence estimates according to KDIGO chronic kidney disease risk groups.
| Albuminuria categories | ||||||||||
| A1 | A2 | A3 | ||||||||
| ACR <30 mg/g |
ACR 30-299 mg/g |
ACR ˃300 mg/g |
Total | |||||||
| eGFR categories (ml/min/1.73 m2 | G1 | ≥ 90 | crude weighted 95% CI |
55.4 45.4 43.1-47.8 |
9.8 8.1 6.7-9.6 |
0.2 0.2 0.002-0.4 |
65.4 53.7 |
|||
| G2 | 60-89 | crude weighted 95% CI |
16.9 13.3 11.6-15.0 |
4.3 3.6 2.6-4.5 |
0.5 0.4 0.1-0.8 |
21.7 17.3 |
||||
| G3A | 45-59 | crude weighted 95% CI |
5.9 4.9 3.8-6.0 |
2.3 1.9 1.2-2.7 |
0.4 0.3 0.04-0.6 |
8.6 7.1 |
||||
| G3B | 30-44 | crude weighted 95% CI |
3.5 2.0 0.6-5.0 |
0.2 0.2 0.02-0.4 |
0 |
3.7 2.2 |
||||
| G4 | 15-29 | crude weighted 95% CI |
0.1 0.1 0,05-0.3 |
0.2 0.2 0.02-0.4 |
0.07 0.06 0.006-0.2 |
0.38 0.36 |
||||
| G5 | <15 | crude weighted 95% CI |
0.07 0.06 0.002-0.02 |
0.07 0.06 0.006-0.12 |
0.08 0.07 0.006-0.2 |
0.22 0.19 |
||||
| crude weighted |
81.87 68.37 |
16.88 14.07 |
1.25 1.04 |
100 | ||||||
| CKD risk | % | estimated number | ||||||||
| crude | weighted | of Croatian adult population | ||||||||
| Low risk | 72.3 | 58.7 | 1,846.099 | |||||||
| Moderate risk | 20.0 | 16.6 | 522.065 | |||||||
| High risk | 6.5 | 4.5 | 141.523 | |||||||
| Very high risk | 1.1 | 1.1 | 35.594 | |||||||
| CKD ≥ G3A A1 | 12.8 | 9.8 | 311.441 | |||||||
Table 3.
Characteristics of subjects with chronic kidney disease and subjects with normal kidney function.
Table 3.
Characteristics of subjects with chronic kidney disease and subjects with normal kidney function.
| CKD population (N = 117) |
Non-CKD population (N = 1076) |
X2; | P | |||||
|---|---|---|---|---|---|---|---|---|
| Mean (SD) | 95% CI | Mean (SD) | 95% CI | |||||
| Median (IQR)# | Median (IQR)# | |||||||
| Age # | 72 (65-75) | 68.3 - 72.3 | 58 (46-75) | 55.34-56.9 | <0.001 | |||
| Gender (men) % | 49.6 | 40.7 – 58.5 | 33.8 | 31.1- 36.6 | 57.42; | <0.001 | ||
| Hypertension duration (years)# | 10 (5-18) | 10.7 - 16.2 | 9.0 (4.0-14.0) | 9.9-11.5 | 0.005 | |||
| Systolic BP (mmHg) # | 137 (125-151) | 134.8 - 144.4 | 131 (120-144) | 143.0-134.1 | 0.001 | |||
| Diastolic BP (mmHg) | 79.7 (11.3) | 77.3 - 82.1 | 82.6 (10.3) | 82.2-83.2 | 0.011 | |||
| Hypertension (yes) | 72.1 | 63.5 – 79.6 | 61.6 | 58.6-64.2 | NS | |||
| Treated controlled (yes) | 20.7 | 15.7-30.9 | 23.4 | 21.0-25.9 | ||||
| Untreated (yes) | 28.9 | 21.2-37.6 | 20.9 | 18.6-23.4 | 7.57; | 0.057 | ||
| Heart rate (bpm) # | 75.3 (16-83.6) | 74.2 - 80.4 | 75.0 (67-83) | 74.8-76.1 | 0.168 | |||
| Height (cm) # | 166 (160-175) | 169.1 - 173.5 | 168 (162.0-175) | 168.3-169.4 | 0.198 | |||
| Weight (kg) # | 82 (63-93) | 81.6 - 88.8 | 80 (69.0-91.4) | 80.4 - 82.4 | 0.191 | |||
| Body mass index (kg/m2) # | 29.3 (26.2-32.5) | 27.9 - 29.9 | 27.9 (24.7-31.3) | 28.1 - 28.7 | 0.008 | |||
| BMI category (kg/m2) % | ||||||||
| 25-29.9 | 35.3 | 26.8 - 44.6 | 39.0 | 36.1 - 41.9 | ||||
| 30.0-34.9 | 36.1 | 27.5 – 45.4 | 23.1 | 20.6 – 25.6 | 14.52; | 0.013 | ||
| 35.0-39.9 | 9.2 | 4.7 – 15.9 | 7.3 | 5.9 – 9.0 | ||||
| Waist circumference (cm) # | 103.5 (95.0-110.2) | 100.5-105.2 | 97.0(87.0-108.0) | 96.7-98.5 | <0.001 | |||
| WC pathologic # | 80.5 | 72.2-87.2 | 64.9 | 62.0-67.7 | 11.69; | 0.003 | ||
| Body surface area (m2) # | 1.95 (1.180-1.95) | 1.95 - 2.05 | 1.93 (1.77-2.09) | 1.93 - 1.96 | 0.426 | |||
| Smokers (yes) | 10.9 | 6.1 – 17.5 | 26.4 | 23.9 – 29.0 | 15.04; | <0.001 | ||
| Daily salt intake (g/day) # | 7.2 (5.0-12.4) | 8.1 - 10.3 | 8.4 (5.6-11.4) | 8.5 - 9.0 | 0.234 | |||
| Daily salt intake > 5 grams % | 24.4 | 17.1-33.0 | 19.0 | 16.8-21.4 | NS | |||
| ePWV (m/s) # | 12.5 (10.6-13.7) | 11.4 - 12.3 | 9.5 (7.9-11.2) | 9.5 - 9.8 | <0.001 | |||
| Monthly income (< 300 Eu) % | 42.6 | 34.0-51.6 | 30.2 | 27.6-32.9 | 14.45; | 0.006 | ||
| Family monthly income (< 300 Eu) % | 22.5 | 15.6-30.7 | 8.4 | 6.9-10.2 | 34,8; | 0.001 | ||
| Education (years) % | ||||||||
| No school | 0.8 | 1.1-6.0 | 0.8 | 0.4-1.5 | ||||
| < 4 | 3.1 | 0.7-9.4 | 1.2 | 0.7-2.0 | ||||
| 4-8 | 27.9 | 10.5-27.3 | 15.6 | 14.7-19.0 | 16.44; | 0.002 | ||
| 8-12 | 45.1 | 41.4-62.9 | 55.4 | 51.7-57.4 | ||||
| ≥12 | 21.7 | 16.9 -35.8 | 26.9 | 24.1-29.1 | ||||
| Professional qualification % | ||||||||
| No college | 38.0 | 19.1-39.3 | 21.1 | 20.1-24.8 | ||||
| College | 38.8 | 34.0-55.3 | 42.7 | 39.3-45.0 | 21.043; | <0.001 | ||
| Bachelor’s degree | 12.4 | 7.9-23.4 | 17.1 | 14.8-18.9 | ||||
| Master’s degree | 9.3 | 5.5-19.5 | 17.3 | 14.9-19.2 | ||||
| Stroke ischemic % | 4.7 | 1.7 – 9.8 | 2.4 | 1.6-3.4 | 6.358; | 0.042 | ||
| Stroke hemorrhagic % | 0.8 | 0.0 – 4.2 | 0.3 | 0.1-0.9 | NS | |||
| Myocardial infarction % | 3.1 | 1.3 - 7.7 | 2.5 | 1.7 – 3.6 | NS | |||
| Heart failure % | 3.9 | 1.3 – 8.8 | 0.8 | 0.3 – 1.4 | 13.06; | 0.001 | ||
| Atrial fibrillation % | 10.1 | 5.5 – 16.6 | 2.8 | 1.9 – 3.9 | 10.25; | 0.006 | ||
| Fasting blood glucose (mmol/l) | 5.4 (4.7-6.7) | 5.6 - 6.6 | 4.9 (4.4-5.2) | 5.0 - 5.2 | <0.001 | |||
| Diabetes % | 29.5 | 21.8 -38.1 | 14.0 | 12.1-16.1 | 36.40; | <0.001 | ||
| Urea (mmol/l) # | 7.5 (6.2-9.2) | 7.6 - 9.3 | 5.2 (4.4-6.2) | 5.3 - 5.5 | <0.001 | |||
| Serum creatinine (µmol/min) # | 110 (92.0-120.5) | 119.6-138.7 | 68.0 (61.0-79.0) | 69.5-71.0 | <0.001 | |||
| eGFR (ml/min/1.73 m2) # | 54.7 (44.3-58.0) | 45.8 - 50.6 | 92.2 (81.7-101.4) | 90.0- 91.8 | <0.001 | |||
| Uric acid (µmol/l) # | 360 (304-422.1) | 368.2 -411.7 | 280 (234-338) | 285.8-294.4 | <0.001 | |||
| Total cholesterol (mmol/l) # | 4.9 (4.1-5.9) | 4.7 - 5.2 | 5.3 (1.1) | 5.3 -5.4 | 0.003 | |||
| Triglycerides (mmol/l ) # | 1.5 (1.1-2.1) | 1.5 - 2.2 | 1.3 (0.9-1.9) | 1.5 - 1.6 | 0.009 | |||
| LDL cholesterol (mmol/l)# | 2.8 (2.1-3.5) | 2.6 - 3.0 | 3.1 (2.4-3.9) | 3.1 -3.2 | <0.001 | |||
| HDL cholesterol (mmol/l) # | 1.3 (1.1-1.5) | 1.2 - 1.4 | 1.4 (1.1-1.6) | 1.4 - 1.5 | 0.022 | |||
| Serum potassium (mmol/l) # | 4.7 (4.3-5.6) | 4.6 - 4.9 | 4.5 (4.3-4.8) | 4.5 - 4.6 | 0.001 | |||
| NT pro BNP (mmol/l) # | 152.2 (76-358) | 324.0-781.1 | 73 (41.0-127.2) | 109.8-134.1 | <0.001 | |||
| Hs Troponin I (mmol/l) # | 5.0 (5.0-5.0) | 5.74 - 13.7 | 5.0 (5.0-5.0) | 5.7 - 6.5 | <0.001 | |||
| ACR (mg/g) # | 17.3 (5.6-44.1) | 26.7-291.19 | 9.4 (4.6-20.8) | 22.6-32.2 | <0.001 | |||
| ACR category (mg/g) % | ||||||||
| 30-299 | 25.0 | 17.3-34.1 | 16.4 | 14.2-18.8 | ||||
| <300 | 7.1 | 3.1-13.6 | 1.0 | 0.5-1.8 | 31.37; | <0.001 | ||
Table 4.
Demographic, socio-economic, behavioral and health related factors associated with chronic kidney disease in univariate logistic regression.
Table 4.
Demographic, socio-economic, behavioral and health related factors associated with chronic kidney disease in univariate logistic regression.
| Coef (B) | S.E. | Odds Ratio Exp (B) |
95% CI Lower Upper |
P | ||
|---|---|---|---|---|---|---|
| Age (years) | -1.00 | 0.012 | 0.90 | 0.88 | 0.92 | <0.001 |
| Gender (men) | 1.680 | 0.243 | 5.36 | 3.33 | 8.63 | <0.001 |
| Family income < 300 Eu | -1.03 | 0.31 | 0.35 | 0.66 | 1.80 | 0.004 |
| Systolic BP (mmHg) | 0.810 | 0.339 | 2.23 | 1.15 | 4.36 | 0.017 |
| Hypertension (no) | 0.481 | 0.205 | 1.61 | 1.08 | 2.42 | 0.019 |
| Hypertension duration (years) | -0.026 | 0.011 | 0.97 | 0.95 | 0.99 | 0.023 |
| Stroke ischemic (yes) | 1.114 | 0.464 | 3.04 | 1.27 | 7.56 | 0.016 |
| Heart failure (yes) | 1.757 | 0.603 | 5.79 | 1.77 | 18.87 | 0.004 |
| Atrial fibrillation (yes) | 1.158 | 0.407 | 3.18 | 1.43 | 7.07 | 0.004 |
| Body mass index (kg/m2) | -0.035 | 0.018 | 0.96 | 0.93 | 0.99 | 0.045 |
| Waist circumference (cm) | -0.021 | 0.006 | 0.97 | 0.96 | 0.99 | <0.001 |
| PWV (m/s) | -0.362 | 0.141 | 0.65 | 0.52 | 0.91 | 0.01 |
| ePWV (m/s) | -0.431 | 0.053 | 0.65 | 0.58 | 0.72 | <0.001 |
| Fasting blood glucose (mmol/l) | -0.197 | 0.044 | 0.82 | 0.75 | 0.89 | <0.001 |
| Diabetes (yes) | 1.32 | 0.233 | 3.76 | 2.38 | 5.93 | <0.001 |
| Uric acid umol/l) | -0.012 | 0.001 | 0.98 | 0.98 | 0.99 | <0.001 |
| Serum creatinine (µmol/l) | -0.372 | 0.051 | 0.68 | 0.62 | 0.76 | <0,001 |
| Urea (mmol/l) | -0.248 | 0.047 | 0.79 | 0.72 | 0.86 | <0.001 |
| Total cholesterol (mmol/l) | 0.258 | 0.085 | 1.29 | 1.09 | 1.53 | 0.002 |
| HDL cholesterol (mmol/l) | 0.818 | 0.312 | 2.26 | 1.22 | 4.17 | 0.009 |
| LDL cholesterol (mmol/l) | 0.373 | 0.114 | 1.45 | 1.16 | 1.81 | 0.001 |
| Triglycerides (mmol/l) | -0.017 | 0,059 | 0.89 | 0.79 | 0.99 | 0.046 |
| Potassium (mmol/l) | -0.727 | 0.189 | 0.48 | 0.33 | 0.81 | <0.001 |
| NT pro BNP (mmol/l) | -0.002 | 0.001 | 0.99 | 0.99 | 0.99 | <0.001 |
| hs Troponin I (mmol/l) | -0.004 | 0.01 | 0.95 | 0.93 | 0.98 | <0.001 |
| ACR | -1.0640 | 0.201 | 0.34 | 0.23 | 0.51 | <0.001 |
| ACR 30-299 (mg/g) | -0.745 | 0.273 | 0.47 | 0.27 | 0.81 | 0.006 |
| ACR > 300 (mg/g) | -2.742 | 0.507 | 0.06 | 0.02 | 0.17 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



