
Submitted:
28 August 2024
Posted:
28 August 2024
You are already at the latest version
Abstract
Significant advancements have been made in controlled drug delivery systems in recent years, especially for oral administration. Conventional methods, although groundbreaking, encounter significant constraints when handling drugs with weak acidity or alkalinity because of their solubility being influenced by pH. The release rates of these ionizable drugs are subject to variability, which is influenced by factors such as the pH of the gastrointestinal tract (GIT), patient-specific conditions, and whether the patient is in a fed or fasted state. As a result, there is often a lack of correlation between in vitro and in vivo data. Therefore, it is imperative to develop drug delivery systems that are not affected by changes in pH in order to address these limitations. This review delves into different strategies that have been developed to achieve drug release that is not affected by changes in pH. These strategies include the utilisation of Diffucaps technology, the incorporation of pH modifiers and surfactants, the combination of non-ionic and ionic polymers, the implementation of supersaturating techniques with nucleation inhibitors, and the utilisation of osmotic drug delivery systems. We assess the efficacy of these methods in reducing the influence of pH fluctuations on the solubility and release rates of drugs. In addition, we explore the potential of these innovative techniques to enhance the reliability and predictability of drug delivery, ultimately leading to better therapeutic results. This review provides an in-depth information of various pH independent controlled drug delivery based formulation and By summarizing the existing technologies and looking into the future, the importance of innovation in pH independent delivery systems is emphasised, laying a good foundation for the future design of simple drug delivery systems, which will be conducive to achieving a wider range of applications in oral drug delivery system.
Keywords:
Dosage form
; Oral controlled delivery system
; pH independent controlled drug delivery
1. Introduction
The oral route is consistently considered the primary and most favourable method for drug delivery. Systemic administration of pharmaceutical products such as tablets, capsules, solutions, emulsions, and suspensions are widely employed due to its convenience and popularity[1]. The oral route is favoured for its widespread acceptance among patients, convenient administration, precise dosage control, cost-effective production methods, and overall extended product stability[2]. The development of a controlled release formulation of a drug aims to optimise its therapeutic benefits while minimising any potential side effects. In 1950, Smith, Kline and French, Plc. introduced the “Spansules,” a pellet filled capsule that marked the first commercially developed oral controlled release formulation[3]. The formulation involved the application of a drug onto nonpareil sugar beads, followed by an additional coating using glyceryl stearate and wax. Various strategies have been developed to achieve controlled release of drugs within the body. These pharmaceutical products range from basic matrix tablets or pellets to advanced controlled release systems that have been commercially launched[4]. Formulating a controlled release dosage form requires careful consideration of various factors, including the drug’s physicochemical properties, physiological factors, and manufacturing variables. Typically, the most prevalent method of drug administration is through the oral route. In this process, drug molecules are dissolved prior to being absorbed into the systemic circulation[1]. The concept of bioavailability refers to the proportion of a drug that enters the bloodstream without undergoing any chemical changes after administration. The rate and efficiency of absorption are contingent upon the chosen route of administration. When it comes to IV delivery, absorption is a done deal. However, for the oral route, the drug needs to be able to dissolve in the GI fluid and then make its way into the epithelial cells of the intestinal mucosa[5]. The bioavailability is influenced by a multitude of factors, including physico-chemical properties, physiological conditions, disease states, and feed composition, among others. The bioavailability of a substance is greatly influenced by its aqueous solubility, making it a crucial parameter to consider[6].
2. Controlled Drug Delivery Systems
In order to optimize the balance between efficacy and safety, controlled drug delivery systems (or CDDS) are designed to release therapeutic substances in a precisely regulated manner over lengthy periods of time [7].These systems regulate the rate at which medicines are released via a variety of ways. Drugs in diffusion-controlled systems are gradually released through a polymer matrix or membrane, with the rate of release being dictated by the drug’s concentration gradient and diffusion coefficient[8].Erosion-controlled systems, on the other hand, achieve drug release through the progressive degradation or erosion of the polymer matrix, with the release rate being dependent on the erosion rate and the solubility of the drug[9].Polymers in swelling-controlled systems swell when they absorb water, increasing the surface area accessible for drug release and hence the rate of drug release [10].The purpose of pH-independent drug delivery systems is to guarantee uniform medication release irrespective of the variations in pH within the gastrointestinal tract. This is especially advantageous for medications whose solubility fluctuates with pH since these systems sustain consistent drug release profiles under various pH ranges [11]. Future developments in CDDS are expected to focus on advanced materials such as smart polymers that respond to specific physiological triggers and nanotechnology-based systems for more targeted and efficient drug delivery[12].
3. A pH-Independent Controlled Drug Delivery System
The primary focus of formulation scientists is the development of controlled drug delivery systems that are not affected by pH levels. These systems have numerous advantages over other controlled drug delivery systems. The release of active ingredients from diffusion-controlled dosage forms in different areas of the gastrointestinal tract can vary due to the pH-dependent solubility of weak acids, weak bases, and their salts[6]. The presence of gastrointestinal fluids can lead to the transformation of a highly ionizable drug into a less soluble form, thereby reducing the rate at which the drug can diffuse through the matrix. Varying rates of drug release may lead to inconsistencies in oral absorption and potential challenges in achieving optimal bioavailability. Hence, the development of a sustained release dosage form that is not affected by pH variations is highly sought after in order to ensure consistent and effective drug treatment[13]. In recent times, the prevailing trends in the pharmaceutical industry indicate a clear shift towards the development of personalised medications. Nevertheless, there remains a demand for the development of medications that can be accessed by a wider population, are reasonably priced, and fulfil the criteria of both safety and effectiveness. Controlled release in pharmaceutics is a highly significant and innovative field, where pH independence plays a crucial role. Delivery systems are commonly utilised to incorporate commercially available drugs. This approach has the potential to significantly prolong the duration of patented medications as a component of life cycle management, thereby safeguarding the market dominance against generic drug manufacturers. Nevertheless, these innovative drug delivery systems play a crucial role in enhancing patient compliance and improving the bioavailability of pH dependent soluble drugs[14]. The solubility of a drug and its tendency to precipitate can pose significant challenges during the clinical development process, particularly when it is influenced by changes in pH. Most oral sustained/controlled drug delivery products, such as matrix tablets, beads or microcapsules, and liquid orals, typically contain an initial dose that quickly reaches maximum peak plasma concentration in the blood. These products also provide a sustained therapeutic dose to maintain steady drug plasma levels within a therapeutic range.[15]. Optimising the release of drugs from oral sustained/controlled release formulations poses a significant challenge for formulators. Modifying the approaches of drug administration is a complex task that requires careful consideration. Hence, the development of a sustained release dosage form that is not affected by pH levels is highly sought after in order to ensure consistent and effective drug therapy[16].
3.1. Advantages of pH-Independent Controlled Drug Delivery System
pH-independent controlled drug delivery systems have many benefits, especially when it comes to improving drug release uniformity and dependability in different physiological conditions. Preserving a consistent drug release profile in the face of pH variations throughout the gastrointestinal (GI) tract is one of the main advantages[17]. This is especially crucial for drugs that are sensitive to the acidic environment of the stomach or the more alkaline conditions of the intestines. By ensuring a stable release mechanism, these systems can improve therapeutic efficacy and reduce the frequency of dosing, thereby enhancing patient compliance[18].They also lessen the possibility of dosage dumping and lessen medication absorption variability, which results in pharmacokinetic profiles that are more predictable. Because of its stability at various pH levels, the drug delivery system can be used for a wider variety of drugs with various physicochemical characteristics[19].
3.2. Disadvantages of pH-Independent Controlled Drug Delivery System
pH-independent controlled drug delivery systems have several benefits, but they also have certain disadvantages. A notable drawback is the possible intricacy and expense linked to their creation. Creating a system that can reliably release a medication regardless of pH changes frequently calls for sophisticated materials and production techniques, which can be costly and time-consuming[20]. Furthermore, there can be issues with the medication’s stability within the delivery matrix over time, which could lower the medication’s effectiveness before it reaches the intended spot. One further concern pertains to the possibility of restricted control over the release rate, as the mechanisms intended to provide pH-independence may potentially impede the capacity to precisely regulate drug release in reaction to particular physiological circumstances. The creation and widespread use of pH-independent controlled drug delivery devices may be severely hampered by these constraints [21].
3.3. Factors That Influence the pH-Independent Controlled Drug Delivery System
The efficiency and operation of pH-independent controlled drug delivery systems are influenced by a number of parameters. The polymer or material selection in the formulation is one of the main determinants. These substances need to be able to hold their integrity and reliably regulate the release of the drug at various pH levels[22]. The physicochemical properties of the drug, such as solubility and stability, also play a crucial role in determining the release kinetics and overall efficacy of the delivery system[23].Additionally, the size, shape, and surface properties of the delivery system can have a big impact on the drug’s release profile and bioavailability. The effectiveness of these systems can also be impacted by external variables that interact with the delivery matrix or change the local pH environment, such as the presence of food or other drugs. Comprehending and refining these variables is imperative for the efficacious creation and implementation of pH-independent controlled medication delivery methodologies [24,25].
3.3.1. The pH of the Stomach
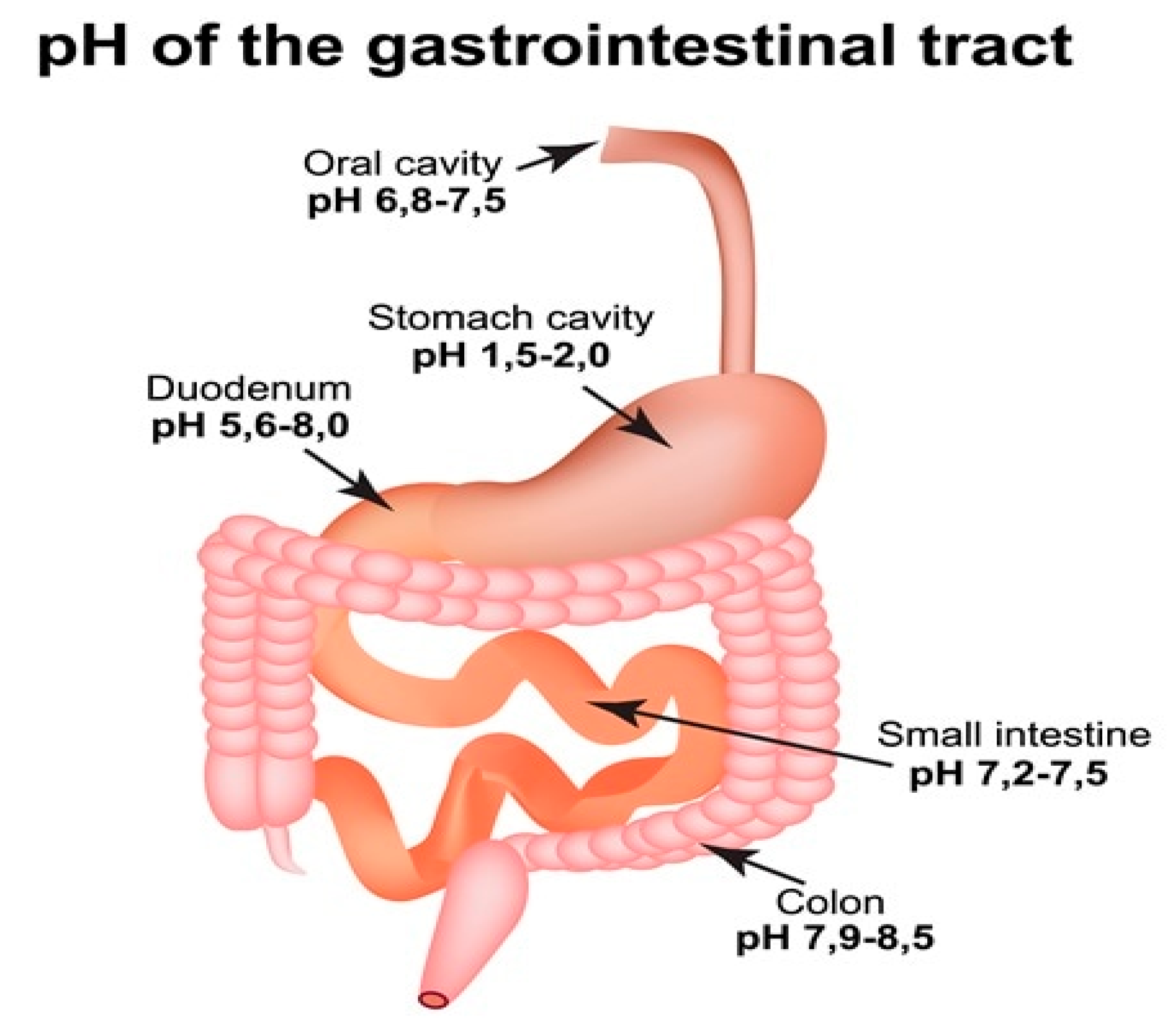
One of the key factors that significantly impact the bioavailability of a drug is the gastrointestinal pH. This pH level plays a crucial role in determining the extent of ionisation of the drug, which subsequently affects its solubility and absorption into the body[26].The drug’s unionised form demonstrates superior membrane permeability compared to its ionised counterpart[27]. The presence of an acidic environment in the stomach has a significant impact on the ionisation of both acidic and basic drugs, consequently influencing their absorption[28]. It is important to acknowledge that the intestine continues to play a significant role in the absorption of drugs from oral dosage forms[29]. This is primarily due to its larger surface area, which allows for more efficient drug absorption within the realm of the BCS class II, there exists a category of drugs characterised by their low solubility and high permeability[30]. Several drugs in this category exhibit solubility that is dependent on pH, with both weakly basic and acidic properties. A crucial obstacle in developing an effective controlled release oral formulation lies in the requirement to align the solubility and dissolution rate of the drug with that of the dosage form[31]. While the pH levels in different regions of the stomach and intestine can vary, drugs that are affected by changes in pH can pose a greater challenge[32]. When a controlled release oral dosage form of a weakly basic drug interacts with stomach fluid, it readily dissolves due to the low pH. However, when it reaches the small intestine with a higher pH, the drug precipitates out due to its low solubility. Therefore, it becomes necessary to absorb the entire drug from the stomach itself. However, this is not feasible according to the pH partition theory and stomach transit time. Similarly, weakly acidic drugs exhibit lower solubility in acidic pH due to their unionised form. However, once they enter the basic pH environment of the intestine, their solubility increases rapidly[33,34]. The impact of gastrointestinal pH on drug release from the dosage form is highly significant and is regarded as a crucial factor in formulation[35].
Figure 1.
Gastro intestinal tract system.
3.3.2. The Gastric Emptying
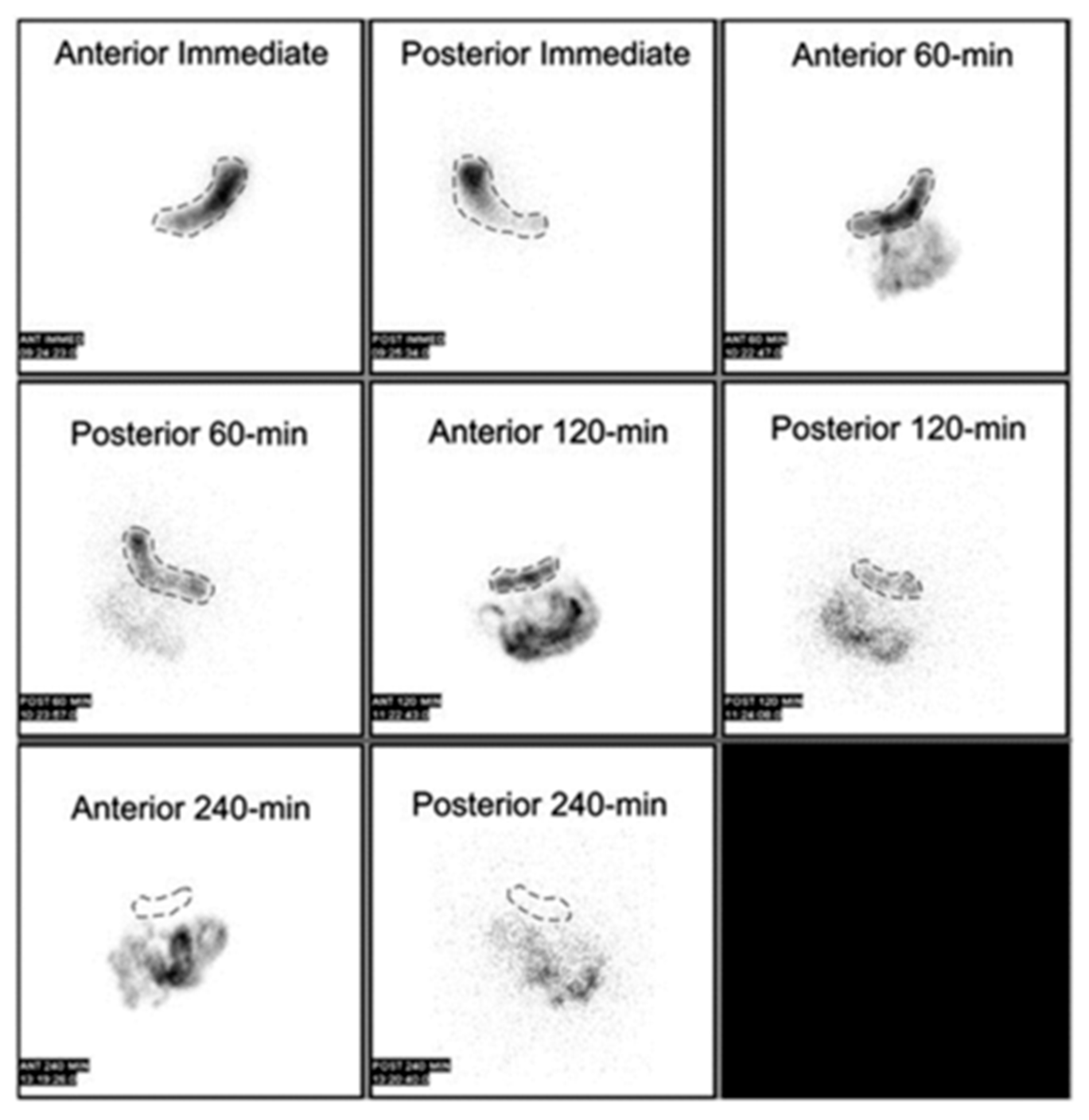
The size, shape, and density of the dosage form, as well as the simultaneous ingestion of food, its nature, caloric content, and frequency of intake, have been the focus of numerous studies[36]. Interestingly, most research on the effects of food on gastric residence time of floating systems agrees that food intake is the primary factor influencing gastric emptying[37]. However, it is worth noting that specific gravity only has a minor impact on the emptying process[38]. It is important to consider that various factors can lead to changes in gastric emptying, which can significantly affect the release of a drug from its drug delivery system[39]. Therefore, there is a need to develop a drug delivery system that can provide an extended gastrointestinal residence and a drug release profile that is not influenced by patient-related variables[36].
Figure 2.
Normal gastric emptying study demonstrating correct regions of interest in both the anterior and posterior projections on initial, 1-hour, 2-hour, and 4-hour images. This image was originally published in JNMT. Vijayakumar V. Assessment of the Practical Role of a Radionuclide Low-Fat-Meal Solid Gastric Emptying Study. J Nucl Med Technol. 2006; 34:82–85. © SNMMI.
Figure 2.
Normal gastric emptying study demonstrating correct regions of interest in both the anterior and posterior projections on initial, 1-hour, 2-hour, and 4-hour images. This image was originally published in JNMT. Vijayakumar V. Assessment of the Practical Role of a Radionuclide Low-Fat-Meal Solid Gastric Emptying Study. J Nucl Med Technol. 2006; 34:82–85. © SNMMI.
3.3.3. Drug Structure
The nature of a drug is greatly influenced by its chemical structure and functional groups. This includes factors such as pH dependence or independence, hydrophobic or hydrophilic properties, and whether the drug is charged or uncharged[40]. The partition coefficient of the compound and its subsequent bioavailability are greatly influenced by the structural modifications resulting from the substitution of various chemical groups in the drug[41,42]
3.3.4. Drug’s Nature
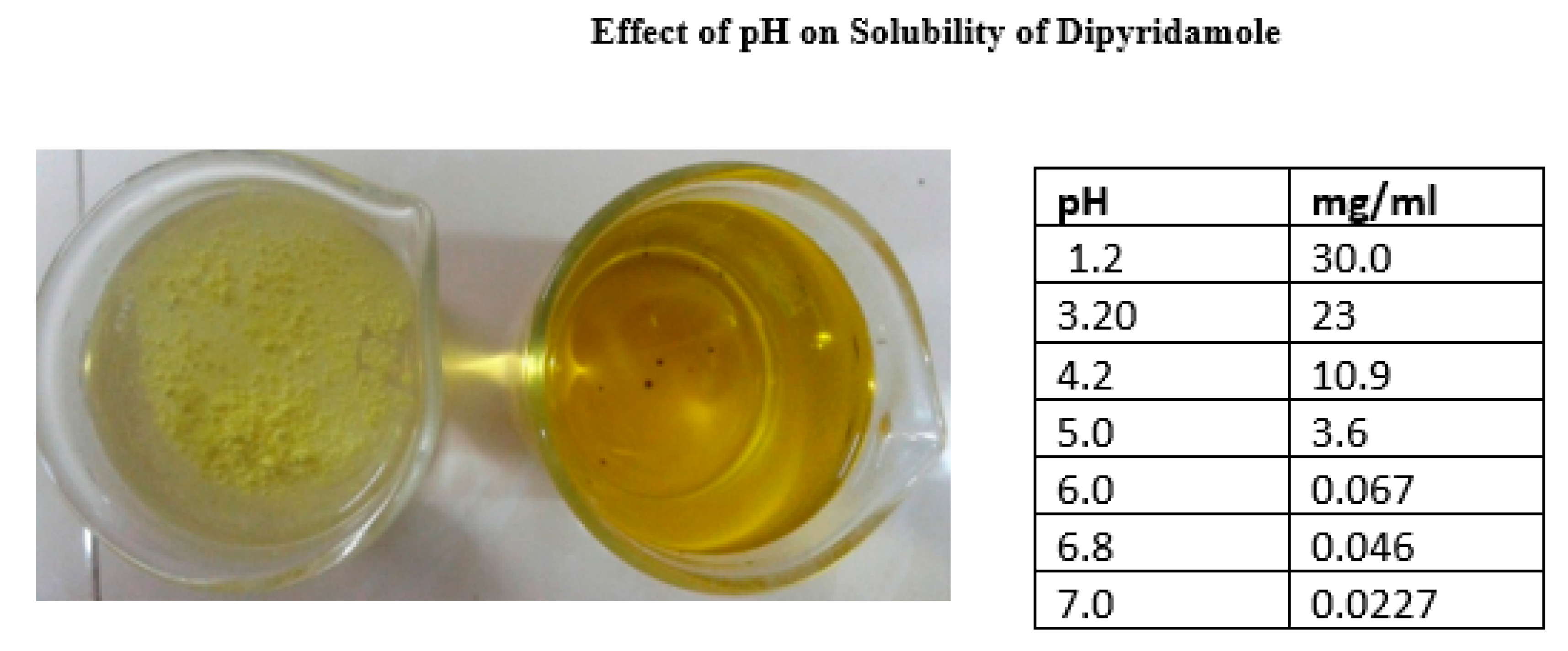
Poor absorption of highly hydrophilic drugs is attributed to their limited ability to traverse cell membranes. Drugs with high lipophilicity exhibit poor absorption due to their complete insolubility in aqueous body fluids. Consequently, they are unable to penetrate the cell surface[43]. In order for a drug to be easily absorbed, it needs to have a high degree of lipophilicity. This means it should have some solubility in water-based solutions, which is further affected by the pH levels of the gastrointestinal fluids[44].The impact of the fasted and fed states on gastrointestinal pH has been extensively studied. The relationship between food and the oral bioavailability of drugs is a highly intricate phenomenon. The bioavailability of drugs can be influenced by the physiological changes in gastric pH caused by the intake of food, which is determined by the physicochemical properties of the compounds[45] The pH variations in the upper GI tract under different feeding conditions can impact the way weakly acidic and basic drugs dissolve and get absorbed. The increase in gastric pH that occurs after a meal can have a positive effect on the solubility of a weak acid medication in the stomach, while simultaneously hindering the dissolution of a weak base drug. Carbonated beverages have been found to enhance the solubility of weakly basic drugs in the stomach, potentially hindering the absorption of acidic drugs when consumed together[46]. The dissociation constant (pKa) is a fundamental parameter in chemistry. Drug molecules can be classified as either weak acids or weak bases, and their degree of ionisation depends on the compound’s pKa and the pH of the surrounding biological fluid. In general, drugs are absorbed in their un-ionized state, a process that is influenced by the pH of the gastrointestinal tract and the drug’s lipophilicity[47]. Based on the principles of pH partition theory, it is observed that weakly basic drugs exhibit higher ionisation (greater solubility) at lower pH levels. Consequently, the absorption of these drugs is primarily influenced by their lipophilicity and solubility at the molecular level[48].
Figure 3.
Laboratory Comparison of solubility Dipyridamole in pH 1.2 and pH 6.8 phosphate buffer medium.
Figure 3.
Laboratory Comparison of solubility Dipyridamole in pH 1.2 and pH 6.8 phosphate buffer medium.
4. Suitable Drug Candidate for pH Independent Controlled Release Drug Delivery System
Therapeutic agents with pH-dependent aqueous solubility, such as weak acids or bases, are commonly formulated into matrix tablets. These tablets are designed to release the drug in a manner that is dependent on the pH of the surrounding environment[49]. Developing controlled release formulations for drugs can result in decreased drug release when the dosage form is exposed to higher pH levels in the gastrointestinal tract. To address this issue, pH independent matrices were created for weakly basic drugs by including acidic excipients that reduce the micro environmental pH within the gel layer[50]. It is feasible to create matrices that are not affected by pH for weakly acidic drugs by including non-polymeric bases or salts of strong bases, along with polymeric pH modifiers, in the controlled release dosage form[51]. Previous studies have proposed the use of weak acids or salts of strong acids as stabilizers in the formulation[52]. Drug delivery systems that can maintain a consistent drug release regardless of pH levels are of great significance for the following drug candidates[53]:
- Drugs that are soluble in a pH-dependent manner
- Drugs with a moderate level of basicity
- Incompletely absorbed as a result of a relatively limited absorption window in the gastrointestinal tract
- Drug precipitation occurs when a solid substance forms from a solution due to various factors. This phenomenon can have significant implications in pharmaceutical formulations and drug delivery systems. Understanding the mechanisms and conditions that lead to drug precipitation is crucial for ensuring the stability and efficacy of medications. By investigating the physicochemical properties of drugs and
- A highly potent pharmaceutical compound.
- Long-term treatment necessitates the use of medications.
- Therapeutic agents with a low half-life
5. Disease Targeting pH Independent Controlled Release Drug Delivery System
Pharmaceutical delivery systems that target specific disease locations and minimize systemic side effects through pH-independent controlled release are a key achievement in personalized medicine. These devices can be especially helpful in treating conditions like cancer, gastrointestinal disorders, and inflammatory diseases where the target region is subjected to a great deal of pH change. For example, in cancer treatment, tumors frequently have an acidic microenvironment in comparison to healthy tissues. Drugs can be reliably delivered at therapeutic concentrations despite these pH variations by utilizing pH-independent mechanisms, guaranteeing the drug’s continued efficacy during the course of treatment[54,55].Furthermore, these delivery systems can maintain a consistent release profile in chronic inflammatory diseases, where the inflammatory tissues may change the local pH, improving therapy efficacy and lowering administration frequency. Through the integration of pH-independent drug release with targeting mechanisms, including ligands or antibodies that identify particular markers on sick cells, these systems can greatly enhance therapy accuracy and efficacy, resulting in improved patient outcomes and decreased side effects[56,57].
6. Approaches of pH Independent Drug Delivery Techniques
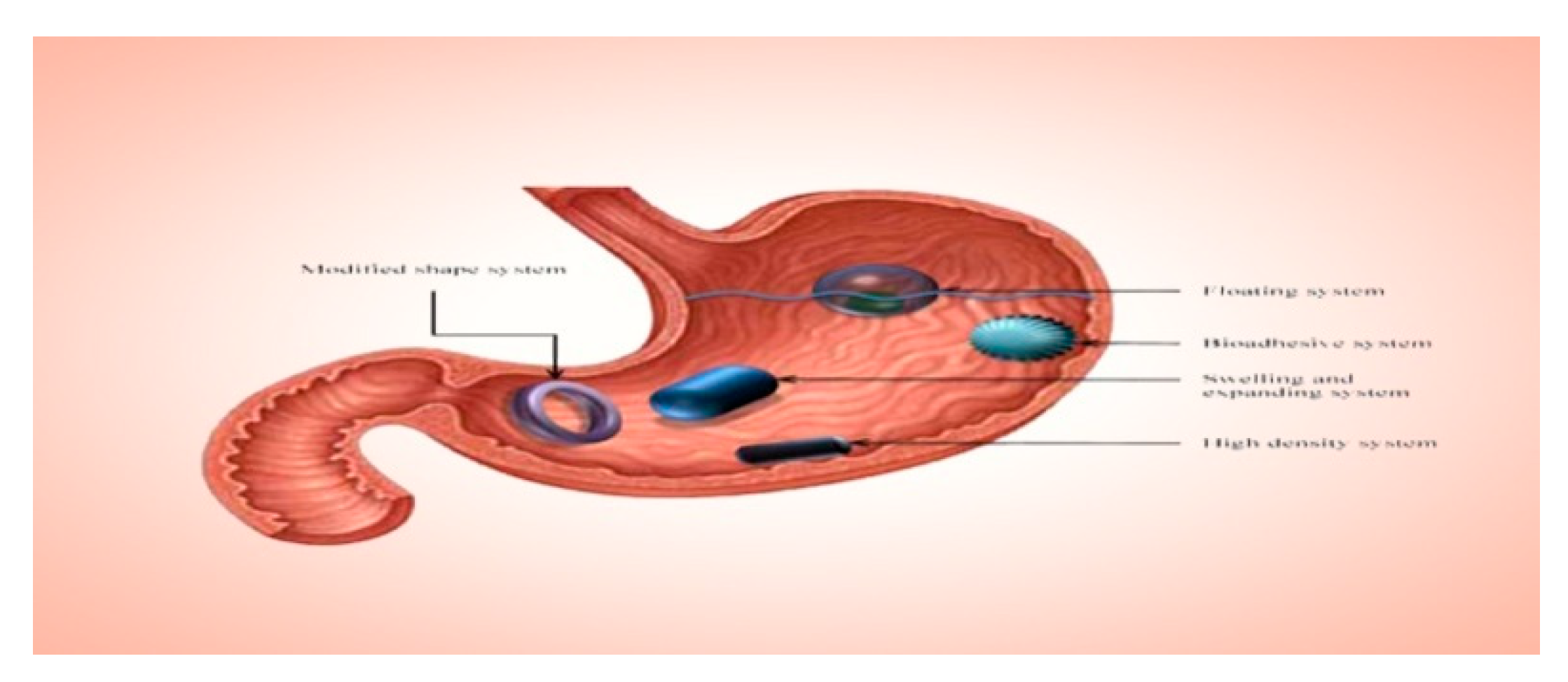
6.1. Floating Drug Delivery Systems Demonstrate the Following Characteristics
Controlled drug release plays a crucial role in the effectiveness of pH-dependent weakly basic drugs. These drugs have high solubility in the acidic environment of the stomach but tend to precipitate in the alkaline environment of the intestines due to their non-ionized nature. To overcome this challenge, floating drug delivery is an effective approach for designing pH-independent drug release. For weakly basic drugs, low density drug delivery systems are ideal, while high density systems are more suitable for weakly acidic drugs[58,59]. It is evident from the availability of previous literature that certain techniques have been developed and reported for pH-independent drug release. One interesting area of study involves the development of a gastro retentive drug delivery system. This system allows the drug to remain afloat for an extended period of time, which presents an intriguing question[10,60,61].Additionally, there is a significant issue with the correlation between in-vitro and in-vivo results, indicating a need for further investigation[62].
Figure 4.
floating drug delivery system.
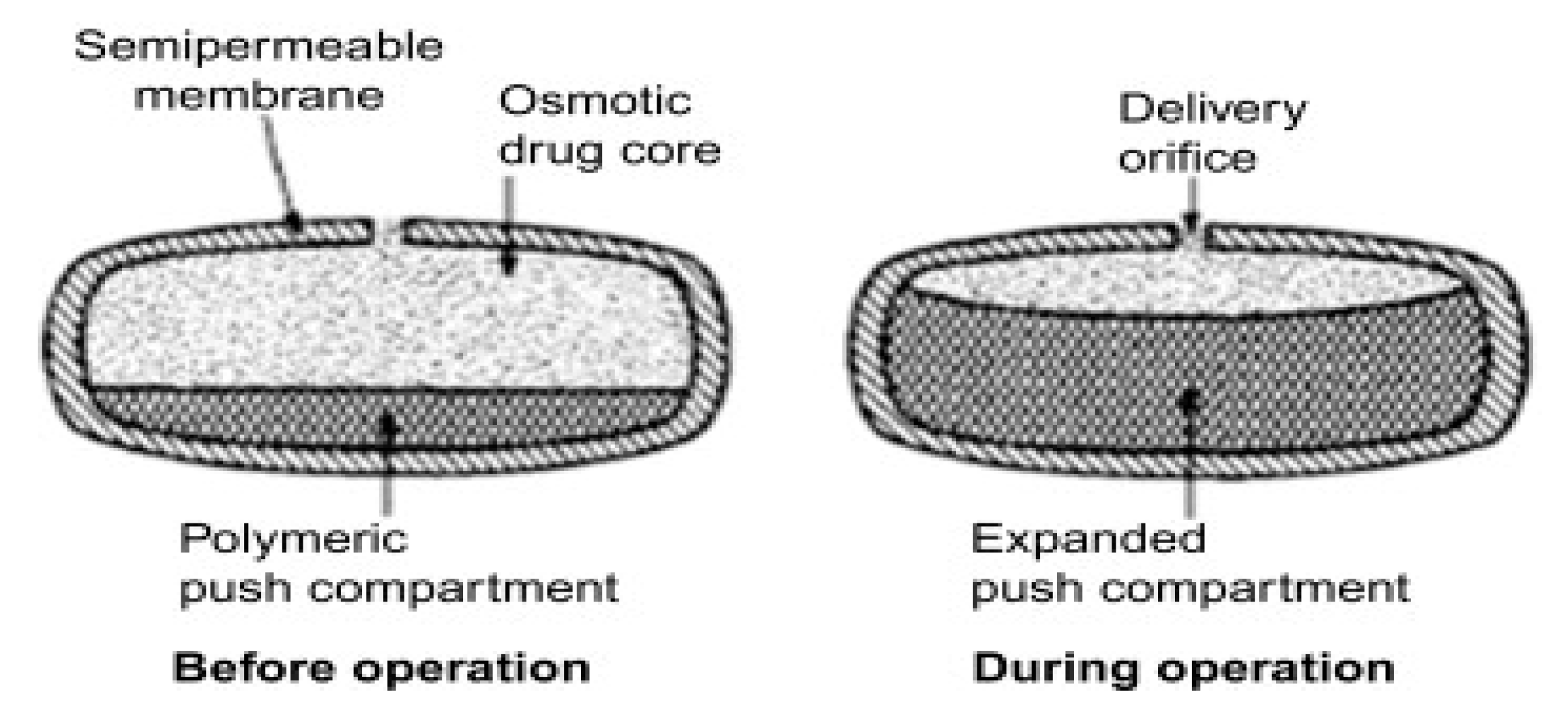
6.2. Osmotic Drug Delivery System
The field of controlled drug delivery systems has become crucial in the advancement of pharmaceutical development. While polymer-based systems are commonly used, researchers have also explored alternatives to minimise the impact of physiological factors such as pH variations caused by food intake or influenced by patient age[63]. An intriguing technology that shows great promise is the oral somatically driven system (OODS). An oral osmotic drug delivery system has been effectively developed and brought to market to prolong the release of compounds with low solubility and for drugs that demonstrate solubility dependent on pH.The push-pull osmotic pump is a modified version of the EOP[64].
Limitations
- i.
- Several parameters, such as the thickness of the membrane, osmotic pressure, the type of membrane and its characteristics, and solubility, play a crucial role in this context.
- ii.
- Drugs that possess high permeability, lack an absorption window, and do not undergo significant first-pass metabolism are more likely to succeed when formulated in osmotic drug delivery systems. Ideally, these drugs should also exhibit dose-proportional and linear pharmacokinetic profiles.
Figure 5.
osmotic drug delivery system.
6.3. pH Modifiers
The addition of pH modifiers is a widely used technique to improve the rate at which weakly acidic or basic drugs dissolve, especially when the drug’s solubility is influenced by pH. By adjusting the micro environmental pH (pHM) both inside and around the dissolving substance, these modifiers can create an ideal pH for achieving controlled solubility[65].
6.3.1. Organic Acids
When dealing with weakly basic drugs, the addition of organic acids helps maintain a low pH within the system, specifically within the intestinal pH range. This, in turn, leads to an increase in the solubility of the drug[55]. The inclusion of organic acids such as Citric, Tartaric, fumaric, succinic, or adipic acid in the formulation can establish a consistent acidic micro-environment within the gel layer, regardless of the surrounding dissolution medium[66]. Organic acids with high acidic strength, characterised by low pKa values and relatively low solubility, are ideally suited for the task. These acids can effectively maintain a low pH in the matrix for extended periods, even when present in low proportions[67].
6.3.2. Alkalizers
In most cases, a drug with weak acidity tends to have limited solubility in an acidic environment, but it exhibits better solubility in a basic pH.The pH modifiers, commonly known as alkalizers, are typically favoured for this purpose. Some commonly used alkalizers include sodium carbonate (Na2CO3), sodium bicarbonate, meglumine, arginine, Magnesium oxide, Calcium carbonate (CaCO3), bentonite, disodium hydrogen phosphate (Na2HPO4), and dipotassium hydrogen phosphate (K2HPO4). As the dissolution fluid permeated the tablets/capsules, alkalizers were released, resulting in a consistent increase in the pH of the surrounding drug particles[68,69].
Limitations
Nevertheless, determining the suitable pH modifier for a particular drug is not as simple as it may seem. Most commonly used pH modifiers exhibit greater solubility at higher pH levels in comparison to basic drug compounds. Given the assumption that pH modifiers diffuse out at a faster rate than the drug itself, it is expected that the drug delivery system will experience a complete loss of pH modifier.Through the utilisation of enteric polymers, a number of significant advancements can be achieved[70,71].
6.4. By Using Enteric Polymers
Formulating pH dependent solubility drugs as controlled release dosage forms can lead to issues with in-vivo variability and bioavailability. An enteric polymer is utilised to address the challenge of pH-dependent solubility exhibited by weakly basic drugs. The enteric polymer acts as an acidifying agent, maintaining a low pH within the system in the intestinal pH range. Alternatively, it can enhance the release of the drug from the delivery system by leaching out at higher pH values. This ensures that the release rate of the drug remains constant throughout. In the second approach, the enteric polymer is applied to both the upper and lower sides of the Matrix tablet, while the remaining sides are left uncoated[72,73].
6.5. Combination of Non-Ionic and Anionic Polymers
The combination of non-ionic and anionic polymers is a topic of great interest in scientific research. This unique blend of polymers has the potential to yield fascinating results and unlock new possibilities in various applications. Researchers have been exploring the properties and interactions of these polymers to better understand their behaviour and potential benefits[74]. By combining non-ionic and anionic polymers, scientists aim to harness the strengths of both types of polymers and create innovative solutions that can have a significant impact in various fields.A pH independent delivery can be achieved by formulating a matrix that consists of two distinct polymers, namely sodium alginate (an anionic polymer) and HPMC (a non-ionic polymer). When the matrix is subjected to an acidic environment, the HPMC, a pH independent polymer, undergoes hydration and forms a gel layer. Meanwhile, the sodium alginate precipitates and remains insoluble, effectively acting as a barrier to the diffusion of the drug[75]. As the pH rises during the tablets’ journey from the stomach to the intestinal tract, the sodium alginate in the matrix starts to expand and absorb water, resulting in the formation of a soluble salt. This process leads to erosion, which plays a crucial role in both hindering drug diffusion and causing matrix erosion. Therefore, the mechanism of release transitions from being primarily governed by diffusion to being primarily governed by erosion. Consequently, the increased permeability of the gel layer at elevated pH levels counterbalances the reduced solubility of the drug[76]. It has been asserted that the release of drugs from this system remains unaffected by changes in pH. The effectiveness of this method has been proven in a study involving a Verapamil hydrochloride matrix tablet[77].
Limitations
Sodium alginate matrices have a tendency to undergo lamination and develop cracks when exposed to low pH levels (<3). This can potentially lead to the sudden release of drugs in the gastric environment. Nevertheless, this issue can be mitigated by incorporating HPMC into the mixture[73].
6.6. Supersaturation That Is Independent of Ph
A compelling approach to improve the absorption of drugs through the oral route involves the generation of super saturation within the gastrointestinal milieu. When drug concentrations are consistently kept significantly above the thermodynamic solubility for a prolonged duration, one can anticipate an increase in absorption. When it comes to drugs that are weak bases, an acidic environment plays a crucial role in improving dissolution by causing protonation. This helps prevent crystal precipitation by creating electrostatic repulsion and increasing solubility in acidic media[78]. After undergoing a change in pH upon reaching the small intestine, specifically to a neutral pH, it is possible that maintaining a supersaturated state could potentially enhance the absorption of the compound with low water solubility. There has been speculation among authors regarding the microenvironment formed by the gradual dissolution of HPMC and the inclusion of polymeric precipitation/nucleation inhibitors. This microenvironment is believed to provide protection to the drug, preventing its precipitation upon exiting the stomach[79]. It is believed that supersaturated concentrations persist in the small intestine for a sufficient duration following a significant decrease in equilibrium solubility. This ultimately leads to an enhanced oral bioavailability. It has been suggested that incorporating nucleation inhibitors and pH modifiers into the tablet could potentially improve the dissolution rate and maintain the extent of dissolution for weak acidic and basic drugs with poor solubility[80,81].
Limitations
When there are physiological malfunctions related to Hypochlorhydria and Achlorhydria, the initial acidic environment needed to dissolve basic drugs is not present. As a result, this has a notable impact on the oral bioavailability of poorly water-soluble compounds. Furthermore, depending solely on the gastro-intestinal acid–base sequence to enhance bioactivity also carries the potential for uncontrolled precipitation of the drug compound at the absorption site[82,83].
6.7. Diffcore Technology
The Diffcore technology developed by GSK utilises a method of mechanically drilling functional film-coated tablets to create apertures with precise size and position in the film coat[84]. The release rate of weakly basic drugs can be modified and controlled by adjusting the exposed surface area and composition of the tablet core[85]. Upon ingestion, the tablet is exposed to gastrointestinal fluids which permeate through the opening in the coat and reach the core, resulting in the release of the drug[86]. The rate of release is contingent upon the constitution and arrangement of the internal matrix[84]. Weak bases exhibit a characteristic behaviour where the coating applied to them initially slows down the release of the active material into the drilled apertures. This phenomenon occurs specifically when the weak bases are exposed to the high-solubility gastric environment. Once it reaches the higher pH of the intestine, the coating undergoes dissociation and becomes soluble. The dissolution of the coat results in an expansion of the core’s surface area[85]. This expansion, in turn, enhances the accessibility of the drug substance that is now exposed. Consequently, this compensates for the reduced solubility that occurs in the intestinal pH. This phenomenon has been documented in previous studies[87,88].
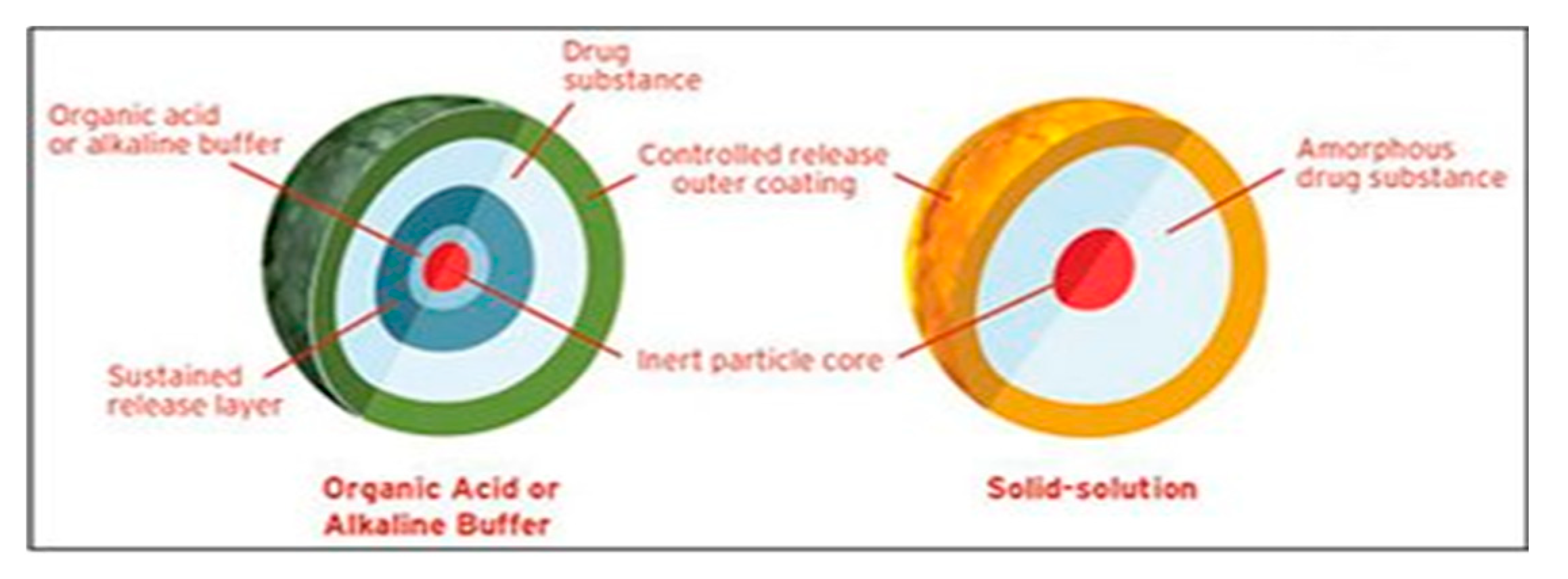
6.8. Diffucaps® Technology
Eurand, a US-based company, has successfully developed a unique technology that effectively addresses solubility issues dependent on pH. In addition, they have integrated this breakthrough with their controlled release technologies[89]. The Diffucaps® technology is composed of a series of sequential steps. The product can be formulated to contain precise quantities of both immediate release (IR) and multiple timed-release (TPR) bead populations with varying lag times[90]. The beads consist of a layer of organic acid or alkaline buffer on 25-30 mesh sugar spheres. This layer serves to regulate the solubility of a drug by establishing an ideal pH microenvironment for drugs with low solubility. In the case of basic drugs, a method commonly employed involves the creation of IR beads. This is achieved by layering the API, which contains a weakly basic nitrogen moiety, and then applying a protective seal-coat using a water soluble polymer[91]. Another technique used is the application of an SR coating on beads that have been layered with an acid or alkaline buffer. This coating consists of a water-insoluble polymer and serves to regulate the release rate of the acid. Ultimately, a combination of IR beads and one or more TPR bead populations is carefully introduced into capsules in specific proportions, aiming to attain a desired pharmacokinetics profile that is well-suited for a once-daily dosing schedule. Applying a sustained-release (SR) coating to acid or alkaline buffer layered beads using a water-insoluble polymer allows for precise control over the release rate of the acid[92].
Figure 6.
Diffucaps® Technology.
7. Novel Dosage Forms and Its Applications in pH Independent Dosage Delivery Systems
The pH-independent controlled drug delivery systems that use novel dosage forms include transdermal patches, matrix tablets, reservoir systems, and microemulsion-based systems. The gel-forming polymers in matrix tablets, such as Hydroxypropyl Methylcellulose (HPMC), allow the medicine to be released under regulated conditions regardless of changes in the pH of the gastrointestinal tract[93]. Transdermal patches, often made of acrylate polymers, deliver drugs through the skin over extended periods of time, avoiding the gastrointestinal tract and its pH fluctuations[94]. Reservoir systems encompass a drug core encircled by a rate-controlling membrane composed of pH-independent polymers such as Eudragit or Ethylcellulose[95].Furthermore, drug stability and solubility are improved by microemulsion-based systems, which offer reliable drug release under a range of pH conditions[96]. With their increased therapeutic results and patient compliance, these innovative dosage forms mark a significant leap in the development of pH-independent controlled drug delivery systems[97].
Challenges and Future Prospective
- Formulating drugs with weakly basic pH-dependent soluble drugs, such as Ondansetron HCl and Dipyridamole, presents several significant challenges. According to the literature, the major challenges can be explained as follows.
- Several drugs, such as weakly acidic and basic drugs, exhibit solubility that varies depending on the pH of the gastrointestinal tract. The rate of dissolution of a drug in a medium is directly proportional to its solubility in that medium. Consequently, the solubility of a substance varies depending on the pH of the gastrointestinal tract, resulting in varying rates of dissolution in different parts of the tract[98].
- The solubility of the drug is affected by pH, which poses challenges for conventional dosage. When the drug comes into contact with stomach fluid (which has a low pH), it easily dissolves. However, when it is transferred to the small intestine with a higher pH, it precipitates out due to its low solubility. These precipitates do not easily dissolve at the intestinal pH. Therefore, it becomes necessary to absorb the entire drug from the stomach itself, which is not feasible according to the pH partition theory. On the other hand, when this drug is included in an extended-release dosage form, the unabsorbed drug interacts with the pH of the gastrointestinal fluids, which gradually change as the dosage is processed. Therefore, the impact of GI fluid pH on drug release from the dosage form is not substantial while it resides in the stomach[99,100].
- However, as the dosage form is transferred to the intestine, the drug release is observed to decrease.
- The solubility variations caused by the drug’s pH dependence can result in either sub-therapeutic doses or toxic doses of certain potent drugs.
- The solubility patterns of pH dependent soluble drugs exhibit variations that have an impact on their absorption and, consequently, their bioavailability.
- Inter-subject variability is a phenomenon that is often observed in scientific studies. It refers to the differences or variations that exist among individuals who are part of a study or experiment. This variability can arise from a variety of factors, such as genetic differences, environmental influences, or even random chance. Understanding and accounting
- ‘Inadequate correlation between in-vitro and in-vivo data;
- Sub-therapeutic doses have no therapeutic action.
- Variation in diseased conditions
Future Directions
- Based on future perspectives, the following recommendations are proposed.
- Extensive research is required for the development of pH independent extended-release formulations for different categories of drugs. These formulations show great potential for pH dependent weakly soluble drugs. It is imperative to develop a novel technique for non pH modulating agents in order to address the limitations of current pH modulating agents.
- There has been a surge of interest in the development of pH independent extended release (ER) drug delivery systems. These systems have garnered attention for their versatility and potential in creating complex formulations, particularly for oral tablet dosage forms of pH dependent soluble drugs. There are no concerns regarding the scale-up process for the production of pH-independent extended-release tablets.
- There is potential for developing formulations utilising various multifunctional polymers, both individually and in combination. Further investigation is required to explore the impact of factors such as pH medium, polymer ratio, tablets geometric, and other formulation parameters
- It is imperative to develop methods for scaling up that can be applied in an industrial setting.
- It is essential to develop in-vitro models that can accurately replicate the in-vivo performance of pH independent controlled release tablets. An innovative compression coating technique was effectively employed and optimisation was also carried out. Therefore, further research is required in this field.
- The design and fabrication of novel extended-release formulations of Dipyridamole, which are not affected by changes in pH, have been thoroughly investigated. The study successfully implemented compression coating technology to maintain the controlled release of pH dependent soluble drugs. In order to attain optimal desirability values during the process of formulation development, it is imperative to utilise advanced tabletting equipment. This will effectively minimise both within batch and batch-batch variations, resulting in superior outcomes.
8. Conclusions
The pH-independent controlled drug release systems represent a significant advancement in pharmaceutical technology, offering consistent therapeutic outcomes irrespective of the gastrointestinal tract’s varying pH conditions. These systems enhance the bioavailability of drugs, particularly those with pH-sensitive solubility profiles, by employing polymers and other excipients that modulate drug release across a broad pH range. The development of these systems requires a thorough understanding of drug properties, excipient interactions, and the physiological environment to optimize formulation performance. Despite the progress in this field, challenges such as ensuring uniform drug release, scalability of production processes, and regulatory hurdles remain. Future research should focus on the design of novel polymers, the integration of nanotechnology, and the exploration of alternative excipients to further enhance the efficacy and versatility of pH-independent controlled drug delivery systems. Continued innovation in this area holds promise for improved patient compliance and therapeutic efficacy, especially in the treatment of chronic conditions requiring long-term medication.
References
- Rathbone, M.J., et al., Modified-release drug delivery technology. Vol. 1. 2003: Marcel Dekker New York.
- Sastry, S.V., J.R. Nyshadham, and J.A. Fix, Recent technological advances in oral drug delivery–a review. Pharmaceutical science & technology today, 2000. 3(4): p. 138-145.
- Langer, R.S. and D.L. Wise, Medical applications of controlled release. 2019: CRC Press LLC Boca Raton, FL, USA:.
- Siepmann, J., R.A. Siegel, and M.J. Rathbone, Fundamentals and applications of controlled release drug delivery. Vol. 3. 2012: Springer.
- Silvestri, L.J. and H.R. Pyle, Sustained release dosage form. 1991, Google Patents.
- Welling, P.G. and M. Dobrinska, Dosing considerations and bioavailability assessment of controlled drug delivery systems. Chapter, 1987. 7: p. 254.
- Bhat, B.B., et al., Controlled release technologies for chronotherapy: current status and future perspectives. Current Pharmaceutical Design, 2023. 29(14): p. 1069-1091.
- Adepu, S. and S. Ramakrishna, Controlled drug delivery systems: current status and future directions. Molecules, 2021. 26(19): p. 5905.
- Freichel, O.L. and B.C. Lippold, A new oral erosion controlled drug delivery system with a late burst in the release profile. European journal of pharmaceutics and biopharmaceutics, 2000. 50(3): p. 345-351.
- Keskar, S. and V. Kumar, Journal of Population Therapeutics & Clinical Pharmacology.
- BODKE, V., et al., PULSATILE DRUG DELIVERY SYSTEMS THE NOVEL APPROACH. 2024.
- Negut, I. and B. Bita, Polymeric micellar systems—a special emphasis on “smart” drug delivery. Pharmaceutics, 2023. 15(3): p. 976.
- Smith, A.A., A.K. Muthu, and R. Manavalan, Formulation development and evaluation of ondansetron hydrochloride sustained release matrix tablets. J. Pharma Sci. & Res, 2009. 1(4): p. 48-54.
- Streubel, A., et al., pH-independent release of a weakly basic drug from water-insoluble and-soluble matrix tablets. Journal of controlled release, 2000. 67(1): p. 101-110.
- Savjani, K.T., A.K. Gajjar, and J.K. Savjani, Drug solubility: importance and enhancement techniques. International Scholarly Research Notices, 2012. 2012(1): p. 195727.
- Siepmann, J. and N.A. Peppas, Modeling of drug release from delivery systems based on hydroxypropyl methylcellulose (HPMC). Advanced drug delivery reviews, 2012. 64: p. 163-174.
- Indurkhya, A., et al., Influence of drug properties and routes of drug administration on the design of controlled release system, in Dosage form design considerations. 2018, Elsevier. p. 179-223.
- Hoare, T.R. and D.S. Kohane, Hydrogels in drug delivery: Progress and challenges. polymer, 2008. 49(8): p. 1993-2007.
- Kopeček, J., Smart and genetically engineered biomaterials and drug delivery systems. European Journal of Pharmaceutical Sciences, 2003. 20(1): p. 1-16.
- Pillai, A., D. Bhande, and V. Pardhi, Controlled Drug Delivery System, in Advanced Drug Delivery: Methods and Applications. 2023, Springer. p. 267-289.
- Tang, B., et al., Development of solid self-emulsifying drug delivery systems: preparation techniques and dosage forms. Drug discovery today, 2008. 13(13-14): p. 606-612.
- Nakamura, K., E. Nara, and Y. Akiyama, Development of an oral sustained release drug delivery system utilizing pH-dependent swelling of carboxyvinyl polymer. Journal of controlled release, 2006. 111(3): p. 309-315.
- Wenande, E., R.R. Anderson, and M. Haedersdal, Fundamentals of fractional laser-assisted drug delivery: an in-depth guide to experimental methodology and data interpretation. Advanced drug delivery reviews, 2020. 153: p. 169-184.
- Fassihi, R.A. and W.A. Ritschel, Multiple-layer, direct-compression, controlled-release system: In vitro and in vivo evaluation. Journal of pharmaceutical sciences, 1993. 82(7): p. 750-754.
- Lee, P.I. and J.X. Li, Evolution of oral controlled release dosage forms. Oral controlled release formulation design and drug delivery: theory to practice, 2010: p. 21-31.
- Higuchi, T., Mechanism of sustained-action medication. Theoretical analysis of rate of release of solid drugs dispersed in solid matrices. Journal of pharmaceutical sciences, 1963. 52(12): p. 1145-1149.
- Amidon, G.L., et al., A theoretical basis for a biopharmaceutic drug classification: the correlation of in vitro drug product dissolution and in vivo bioavailability. Pharmaceutical research, 1995. 12: p. 413-420.
- Dressman, J.B., et al., Dissolution testing as a prognostic tool for oral drug absorption: immediate release dosage forms. Pharmaceutical research, 1998. 15: p. 11-22.
- Kesisoglou, F., S. Panmai, and Y. Wu, Nanosizing—oral formulation development and biopharmaceutical evaluation. Advanced drug delivery reviews, 2007. 59(7): p. 631-644.
- Lindenberg, M., S. Kopp, and J.B. Dressman, Classification of orally administered drugs on the World Health Organization Model list of Essential Medicines according to the biopharmaceutics classification system. European Journal of Pharmaceutics and Biopharmaceutics, 2004. 58(2): p. 265-278.
- Ghebre-Sellassie, I., et al., Pharmaceutical extrusion technology. 2003: CRC Press.
- Qiu, Y. , et al., Developing solid oral dosage forms: pharmaceutical theory and practice. 2016: Academic press.
- Huang, Y. and W.-G. Dai, Fundamental aspects of solid dispersion technology for poorly soluble drugs. Acta Pharmaceutica Sinica B, 2014. 4(1): p. 18-25.
- Charman, W. and V. Stella, Transport of lipophilic molecules by the intestinal lymphatic system. Advanced drug delivery reviews, 1991. 7(1): p. 1-14.
- Dahan, A. and A. Hoffman, Rationalizing the selection of oral lipid based drug delivery systems by an in vitro dynamic lipolysis model for improved oral bioavailability of poorly water soluble drugs. Journal of controlled release, 2008. 129(1): p. 1-10.
- Singh, B.N. and K.H. Kim, Floating drug delivery systems: an approach to oral controlled drug delivery via gastric retention. Journal of Controlled release, 2000. 63(3): p. 235-259.
- Hwang, S.-J., H. Park, and K. Park, Gastric retentive drug-delivery systems. Critical Reviews™ in Therapeutic Drug Carrier Systems, 1998. 15(3).
- Menon, A., W.A. Ritschel, and A. Sakr, Development and evaluation of a monolithic floating dosage form for furosemide. Journal of pharmaceutical sciences, 1994. 83(2): p. 239-245.
- Sathish, D., et al., Floating drug delivery systems for prolonging gastric residence time: a review. Current drug delivery, 2011. 8(5): p. 494-510.
- Oprea, T.I., Current trends in lead discovery: are we looking for the appropriate properties? Molecular diversity, 2000. 5: p. 199-208.
- Veber, D.F., et al., Molecular properties that influence the oral bioavailability of drug candidates. Journal of medicinal chemistry, 2002. 45(12): p. 2615-2623.
- Hansch, C., J. Björkroth, and A. Leo, Hydrophobicity and central nervous system agents: on the principle of minimal hydrophobicity in drug design. Journal of pharmaceutical sciences, 1987. 76(9): p. 663-687.
- Dobetti, L., Fast-melting tablets: Developments and technologies. Pharmaceutical technology, 2001: p. 44-44.
- Lipinski, C.A., et al., Experimental and computational approaches to estimate solubility and permeability in drug discovery and development settings. Advanced drug delivery reviews, 1997. 23(1-3): p. 3-25.
- Kalantzi, L., et al., Characterization of the human upper gastrointestinal contents under conditions simulating bioavailability/bioequivalence studies. Pharmaceutical research, 2006. 23: p. 165-176.
- Dressman, J.B., et al., Upper gastrointestinal (GI) pH in young, healthy men and women. Pharmaceutical research, 1990. 7: p. 756-761.
- Avdeef, A., Absorption and drug development: solubility, permeability, and charge state. 2012: John Wiley & Sons.
- Akiyama, Y., et al., Prediction of oral drug absorption in rats from in vitro data. Pharmaceutical Research, 2023. 40(2): p. 359-373.
- Khalid, G.M., EXTEMPORANEOUS PREPARATIONS IN PERSONALIZED THERAPY: THE DESIGN OF ORODISPERSIBLE DOSAGE FORMS. 2021.
- dos Santos, J., et al., Eudragit®: A Versatile Family of Polymers for Hot Melt Extrusion and 3D Printing Processes in Pharmaceutics. Pharmaceutics 2021, 13, 1424. 2021, s Note: MDPI stays neutral with regard to jurisdictional claims in published.
- Kim, C.-j., Advanced pharmaceutics: physicochemical principles. 2004: CRC press.
- Robinson, J.R., Sustained and controlled release drug delivery systems. (No Title), 1978.
- Aulton, M.E. and K. Taylor, Aulton’s pharmaceutics: the design and manufacture of medicines. 2013: Elsevier Health Sciences.
- Teruel, A.H., et al., New insights of oral colonic drug delivery systems for inflammatory bowel disease therapy. International journal of molecular sciences, 2020. 21(18): p. 6502.
- Wang, L., et al., Porous and responsive hydrogels for cell therapy. Current Opinion in Colloid & Interface Science, 2018. 38: p. 135-157.
- Li, W., et al., Polyelectrolyte-based physical adhesive hydrogels with excellent mechanical properties for biomedical applications. Journal of Materials Chemistry B, 2018. 6(29): p. 4799-4807.
- Bahadır, E.B. and M.K. Sezgintürk, Poly (amidoamine)(PAMAM): An emerging material for electrochemical bio (sensing) applications. Talanta, 2016. 148: p. 427-438.
- Bindu, H.A., G. Bhavya, and K. Padmalatha, Floating drug delivery system: an overview. 2021.
- Si, X., et al., Hypoxia-sensitive supramolecular nanogels for the cytosolic delivery of ribonuclease A as a breast cancer therapeutic. Journal of Controlled Release, 2020. 320: p. 83-95.
- Gupta, P., P.K. Gnanarajan, and P. Kothiyal, Floating drug delivery system: a review. International Journal of Pharma Research & Review, 2015. 4(8): p. 37-44.
- Kumar, M.R., et al., A comprehensive review on gastro retentive drug delivery system. Acta Chimica Pharmaceutica Indica, 2013. 3(2): p. 149-164.
- Azevedo, C., et al., The effect of hypergravity in intestinal permeability of nanoformulations and molecules. European Journal of Pharmaceutics and Biopharmaceutics, 2021. 163: p. 38-48.
- Siepe, S., et al., Microenvironmental pH and microviscosity inside pH-controlled matrix tablets: an EPR imaging study. Journal of controlled release, 2006. 112(1): p. 72-78.
- Company, D.C., Methocel cellulose ethers technical handbook. 2002, Dow Chemical Co Midland, MI.
- Brahmankar, D. and S.B. Jaiswal, Biopharmaceutics and pharmacokinetics. 2019: Vallabh prakashan.
- Gaber, M., et al., Protein-polysaccharide nanohybrids: Hybridization techniques and drug delivery applications. European Journal of Pharmaceutics and Biopharmaceutics, 2018. 133: p. 42-62.
- JS, P., et al., Inclusion complex system; a novel technique to improve the solubility and bioavailability of poorly soluble drugs: A review. Int. J. Pharm. Sci. Rev. Res, 2010. 2: p. 29-34.
- Bharate, S.S., S.B. Bharate, and A.N. Bajaj, Interactions and incompatibilities of pharmaceutical excipients with active pharmaceutical ingredients: a comprehensive review. International Journal of Pharmaceutical Excipients, 2016. 1(3).
- Loftsson, T. and M.E. Brewster, Pharmaceutical applications of cyclodextrins: basic science and product development. Journal of pharmacy and pharmacology, 2010. 62(11): p. 1607-1621.
- Narasimhan, B., Macromolecular dynamics during polymer dissolution: Molecular modeling and experimental characterization. 1996, Purdue University.
- Rashid, M., et al., Bioavailability enhancement of poorly soluble drugs: the holy grail in pharma industry. Current Pharmaceutical Design, 2019. 25(9): p. 987-1020.
- Anilkumar, A., T.E.G. Krishna Murthy, and A.P. Rani, Design and development of ondansetron hydrochloride pH independent control released matrix tablets. Pakistan Journal of Pharmaceutical Sciences, 2020. 33(2).
- Chen, L. and Y. Chien, Development of a skin permeation cell to simulate clinical study of iontophoretic transdermal delivery. Drug development and industrial pharmacy, 1994. 20(6): p. 935-945.
- Ron, E., et al., Controlled release of polypeptides from polyanhydrides. Proceedings of the National Academy of Sciences, 1993. 90(9): p. 4176-4180.
- Al-Zoubi, N., et al., Optimization of pH-independent chronotherapeutic release of verapamil HCl from three-layer matrix tablets. International Journal of Pharmaceutics, 2015. 494(1): p. 296-303.
- Liechty, W.B., et al., Polymers for drug delivery systems. Annual review of chemical and biomolecular engineering, 2010. 1(1): p. 149-173.
- Taniguchi, C., et al., Novel formulations of dipyridamole with microenvironmental pH-modifiers for improved dissolution and bioavailability under hypochlorhydria. International journal of pharmaceutics, 2012. 434(1-2): p. 148-154.
- Tran, P.H.-L., et al., Dissolution-modulating mechanism of pH modifiers in solid dispersion containing weakly acidic or basic drugs with poor water solubility. Expert opinion on drug delivery, 2010. 7(5): p. 647-661.
- Kandukuri, J.M., et al., Pelletization techniques for oral drug delivery. Int J Pharm Sci Drug Res, 2009. 1(2): p. 63-70.
- Mehta, D.M., et al., Investigation of the drug release modulating effect of acidifiers in modified release oral formulation of cinnarizine. Asian Journal of Pharmaceutical Sciences, 2012. 7(3).
- Jayanthi, R.M., et al., pH-independent controlled release swellable matrix tablets. IJRAP, 2011. 2: p. 577-80.
- Williams, H.D., et al., Strategies to address low drug solubility in discovery and development. Pharmacological reviews, 2013. 65(1): p. 315-499.
- Sutton, S.C., Role of physiological intestinal water in oral absorption. The AAPS journal, 2009. 11: p. 277-285.
- Siewert, M., et al., FIP/AAPS guidelines to dissolution/in vitro release testing of novel/special dosage forms. Aaps Pharmscitech, 2003. 4: p. 43-52.
- Bose, A., T.W. Wong, and N. Singh, Formulation development and optimization of sustained release matrix tablet of Itopride HCl by response surface methodology and its evaluation of release kinetics. Saudi Pharmaceutical Journal, 2013. 21(2): p. 201-213.
- Nagendrakumar, D., G. Keshavshetti, and A. Shardor, An overview: Matrix tablets as sustained release. Recent Research in Science and Technology, 2014. 5(4).
- Carlert, S., Investigation and prediction of small intestinal precipitation of poorly soluble drugs: a study involving in silico, in vitro and in vivo assessment. 2012, Acta Universitatis Upsaliensis.
- Nikam, V.K., et al., Eudragit a versatile polymer: a review. Pharmacologyonline, 2011. 1(5): p. 152-164.
- Deguchi, S., et al., Solvent Dependence of Optical Rotation of (S)-N-[1-(2-Fluorophenyl)-3, 4, 6, 7-tetrahydro-4-oxo-pyrrolo-[3, 2, 1-jk][1, 4] benzodiazepine-3-yl]-1 H-indole-2-carboxamide. Journal of pharmaceutical sciences, 1993. 82(7): p. 734-736.
- Kranz, H., V. Le Brun, and T. Wagner, Development of a multi particulate extended release formulation for ZK 811 752, a weakly basic drug. International journal of pharmaceutics, 2005. 299(1-2): p. 84-91.
- Schoen, J.C., K.M. Erlandson, and P.L. Anderson, Clinical pharmacokinetics of antiretroviral drugs in older persons. Expert opinion on drug metabolism & toxicology, 2013. 9(5): p. 573-588.
- Ching, A.L., et al., Modifying matrix micro-environmental pH to achieve sustained drug release from highly laminating alginate matrices. European journal of pharmaceutical sciences, 2008. 33(4-5): p. 361-370.
- Alderman, D., A review of cellulose ethers in hydrophilic matrices for oral controlled-release dosage forms. Int J Pharm Tech Prod Mfr, 1984. 5(3): p. 1-9.
- Prausnitz, M.R. and R. Langer, Transdermal drug delivery. Nature biotechnology, 2008. 26(11): p. 1261-1268.
- Lecomte, F., et al., pH-sensitive polymer blends used as coating materials to control drug release from spherical beads: elucidation of the underlying mass transport mechanisms. Pharmaceutical research, 2005. 22: p. 1129-1141.
- Lawrence, M.J. and G.D. Rees, Microemulsion-based media as novel drug delivery systems. Advanced drug delivery reviews, 2000. 45(1): p. 89-121.
- Amsden, B., A model for osmotic pressure driven release from cylindrical rubbery polymer matrices. Journal of controlled release, 2003. 93(3): p. 249-258.
- Li, N. and L.S. Taylor, Tailoring supersaturation from amorphous solid dispersions. Journal of Controlled Release, 2018. 279: p. 114-125.
- Hsieh, Y.-L., et al., pH-induced precipitation behavior of weakly basic compounds: determination of extent and duration of supersaturation using potentiometric titration and correlation to solid state properties. Pharmaceutical research, 2012. 29: p. 2738-2753.
- Huang, S., et al., Solubility advantage (and disadvantage) of pharmaceutical amorphous solid dispersions. Journal of pharmaceutical sciences, 2016. 105(12): p. 3549-3561.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



