Submitted:
27 August 2024
Posted:
29 August 2024
You are already at the latest version
Abstract
Patients with heart failure (HF) with improved LVEF (HFimpEF) demonstrate better clinical outcomes when compared with individuals without restoration of cardiac function. Identification of predictors for HFimpEF may play a crucial role in individual management of HF with reduced EF (HFrEF). Cell-free nuclear (cf-nDNA) DNA are released from damaged cells and contribute to adverse cardiac remodeling, cardiac dysfunction and inflammation. The purpose of the study was to elucidate whether cf-nDNAs are associated with HFimpEF. It has been prescreened 1416 patients with HF using local database. Between October 2021 and August 2022 we included 452 patients chronic HFrEF after prescription of optimal guideline-based therapy and identified HFimpEF in 177 individuals from them according to the criteria of European Society of Cardiology. Measurements of circulating biomarkers were performed at baseline and in 6 months. Detection of cf-nDNA was executed with real time quantitative PCR (qPCR) using NADH dehydrogenase, ND2 and beta-2-microglobulin. We found that HFimpEF was associated with a significant decrease in the levels of cf-nDNA when compared with the patients from persistent HFrEF cohort. Presence of ischemia-induced cardiomyopathy (odds ration [OR] = 0.75; confidence interval [CI] = 0.62 – 0.88; p = 0.044), type 2 diabetes mellitus (OR = 0.77; CI = 0.71 – 0.82; p = 0.042) and digoxin administration (OR = 0.85; CI = 0.72-0.97; p = 0.042) were negative factors for HFimpEF, whereas NT-proBNP ≤1940 pmol/mL (OR = 1.42; 95% CI = 1.19-1.98, p = 0.001), relative decrease in NT-proBNP levels (>35% vs. ≤35%) from baseline (OR = 1.52; 95% CI = 1.38-0.69, p = 0.001) and cf-nDNA ≤7.5 μmol/L (OR = 1.56; 95% CI = 1.07-2.94, p = 0.001) were positive predictors for HFimpEF. Multivariate logistic regression adjusted to ischemia-induced cardiomyopathy, IV HF NYHA class, and digoxin use yielded that NT-proBNP ≤1940 pmol/mL (OR = 1.43; 95% CI = 1.21-1.88, p = 0.001) and cf-nDNA ≤7.5 μmol/L (OR = 1.64; 95% CI = 1.19-2.15, p = 0.001) independently predicted HFimpEF. In conclusions: we established that the levels of cf-nDNA≤7.5 μmol/L independently predicted HFimpEF and improved discriminative ability of as single measured NT-proBNP as well as relative decrease in NT-proBNP levels ≤35% from baseline.
Keywords:
heart failure with improved ejection fraction
; heart failure with reduced ejection fraction
; cell-free nuclear DNA
; biomarkers
1. Introduction
Heart failure (HF) is defined as a clinical syndrome resulting from numerous myocardial diseases leading to an structural and/or functional cardiac abnormality including reduced cardiac output and / or increased intracardiac pressure at rest or during physical exercise and associated with elevated circulating levels of natriuretic peptides and/or evident systemic or pulmonary congestion [1]. Regardless of its etiology, HF is related to poor 5-year mortality rate ranging from 50% to almost 70% depending on staging, age, and comorbidity signatures [2,3,4]. Traditionally HF is classified based on the left ventricular (LV) ejection fraction (LVEF) and consequently divided into three phenotypes - HF with preserved ejection fraction (HFpEF, LVEF ≥50%), HF with mildly reduced ejection fraction (HFmrEF, LVEF 41% to 49%), and HF with reduced ejection fraction (HFrEF, LVEF ≤40%) [5]. Although these three phenotypes exerted a strict similarity in 5-year mortality in HF patients, cardiovascular and HF rehospitalization rates were sufficiently higher in those with HFrEF and HFmrEF compared with those with HFpEF [6].
Recent clinical trials have been confirmed the improvement of HF clinical outcomes and prognosis in case of transiting reduced / mildly reduced LVEF to preserved LVEF [7,8,9]. This fact has led to the determination of a new HF subgroup with an improved LVEF (HFimpEF) that is defined as LVEF >40% at ≥3 months or ≥10% increase from baseline LVEF and which became a clinical biomarker of favorable HF-related outcomes [1]. However, causative factors contributing to HFimpEF remain unclear and what remains especially important is that a persistence of HFrEF / HFmrEF retains to be associated with poor clinical outcomes and elevated mortality rate [10,11]. However, current recommendations from the European Society of Cardiology and the American Heart Association do not provide comprehensive information on how to manage patients with HFimpEF, and are limited to stating that guideline-directed medical therapy that has led to improvement of LVEF should be maintained further [1,5]. In this connection, prediction of LVEF trajectories seems to be promising approach in management of HFrEF / HFmrEF. Indeed, there is a large body of evidence that aging, ischemic etiology, comorbidities including diabetes mellitus, atrial fibrillation, chronic kidney disease, as well as LV diameter, diastolic blood pressure, the levels of natriuretic peptides and no digoxin use could incorporate into predictive model for occurrence of HFimpEF, while this has so far lacked an individualized approach [12,13,14,15].
Cell-free deoxyribonucleic acid (cf-DNA) fragments are released into circulation from various bodily tissues following non-selective cellular membrane permeability, cellular damage or death [16]. However, profiling of cfDNA is associated with various pathological conditions including neutrophil extracellular traps (NETs), oxidative stress, mitochondrial dysfunction, apoptosis, ferroptosis and necrosis [17,18]. Fragmentation and clearance of DNA may relate to initial triggers of cellular damage (ischemia / hypoxia, infections, inflammation, immune / autoimmune reactions), physical exercise and concomitant comorbidities [19]. Two main circulating subpopulations of cfDNAs, i.e. nuclear-derived DNA (cf-nDNA) and mitochondrial-derived DNA (cf-mtDNA), which characterize cellular damage and non-selective cellular membrane permeability following oxidative stress respectively, seem to non-invasively and dynamically assess disease status in patients with acute coronary artery disease, HF, acute kidney injury, chronic kidney disease, allograft rejection, cancer, and sepsis [20,21,22,23,24]. Although circulating cfDNAs mainly cf-nDNAs were found to be a reliable biomarker of myocardial injury with possible predictive value in acute and chronic HF [25,26], there are no data about discriminative potency of cf-DNAs in HFimpEF patients with HF. The purpose of the study was to elucidate whether cf-nDNAs are associated with HFimpEF.
2. Materials and Methods
2.1. Study Patients
A total of 1416 patients with HF were prescreened using local database of the “Vita Center” (Zaporozhye, Ukraine). Using criteria of inclusion (male / female with age of ≥18 years, established HFrEF, informed consent to participate in the study) we enrolled 452 patients chronic HFrEF between October 2021 and August 2022. The patient selection process and clinical characteristics are summarized in Figure 1. All patients were included in the study at admission to the hospital with the aim of initiating optimal guideline-directed medical therapy, which has been continued after discharge. In 6 months, the patients were divided into two cohorts depending on a trajectory of LVEF: with criteria of HFimpEF (n=177) and without evidence of HFimHF (n=275).
2.2. Determination of LVEF Improvement
HFimpEF was defined as an increase of baseline LVEF≥10% over ≥3 months of guideline-directed medical therapy and a follow-up measurement >40% according to the 2021 Universal Definition and Classification of Heart Failure [1].
2.3. Medical Information Collection
Basic patient information included age, gender, height, weight, body mass index (BMI), and body surface area (BSA), NYHA HF functional class. Past history included smoking, hypertension, diabetes history, atrial fibrillation, coronary artery disease, dyslipidemia.
T2DM was diagnosed according to American Diabetes Association [27]. The European Society of Cardiology (ESC) clinical guidelines were utilized to determine HF [28], hypertension [29], dyslipidemia [30] and coronary artery disease [31]. Chronic kidney disease was detected in accordance with Kidney Disease Improving Global Outcomes (KDIGO) Consensus Report [32].
Utilization of drugs included diuretics, angiotensin-II receptor blockers (ARBs), angiotensin-converting enzyme inhibitors (ACEI), angiotensin receptor/neprilysin inhibitor (ARNI), sodium glucose co-transporter-2 inhibitors (SGLT2i), beta-blockers, antiplatelet agents, anticoagulants, statins, digoxin, calcium channel blockers and mineralocorticoid receptor antagonists.
2.3. Examination of Hemodynamics
All patients underwent echocardiographic and Doppler examinations performed by two blinded, highly experienced echocardiographers according to the guidelines of the American Society of Echocardiography [33]. The standard apical 2- and 4-chamber views were acquired at baseline and at the end of the study using a GE Healthcare Vivid E95 scanner (General Electric Company, Horton, Norway). The conventional hemodynamic parameters included LVEF by using Simpson’s method, LV end-diastolic (LVEDV) and end-systolic (LVESV) volumes, left atrial volume index (LAVI), early diastolic blood filling (E) and mean longitudinal strain ratio (e`). The estimated E/e` ratio was expressed as the ratio of the E wave velocity to the averaged medial and lateral e’ velocities. LV hypertrophy was defined as a LV mass index (LVMI) ≥95 g/m2 in women or ≥115 g/m2 in men. Data were stored in DICOM format for further analysis.
2.4. Glomerular Filtration Rate Calculation
We used CKD-EPI formula to estimate glomerular filtration rate (GFR) [34]
2.5. Blood Sampling
Venous blood samples were taken in the morning before breakfast after an overnight fast. After centrifugation at 3000 rpm for 10 min, the supernatant was collected and stored at -70°C until analysis.
2.6. Biomarker Evaluation
Conventional biochemical parameters were routinely measured in the local biochemical laboratory of the Vita Centre (Zaporozhye, Ukraine) using a Roche P800 analyzer (Basel, Switzerland). Serum concentrations of NT-proBNP, tumor necrosis factor-alpha (TNF-alpha), and high-sensitivity C-reactive protein (hs-CRP) were determined using commercially available enzyme-linked immunosorbent assay (ELISA) kits (Elabscience, Houston, Texas, USA) according to the manufacturer's instructions at baseline and in 6 months after initiation of optimal guideline-based therapy. All ELISA data were analyzed according to the standard curve, each sample was measured in duplicate, and the mean value was used for final analysis. Both intra- and inter-assay coefficients of variability for each marker were < 10%.
2.7. Cell-Free DNA Extraction
Cell-free DNA was isolated from 4 mL plasma samples using the Biosystems MagMAX Cell-Free DNA Kit (Thermo Fisher Scientific, Vienna, Austria) according to the manufacturer's instructions. Plasma samples were obtained from EDTA whole blood samples by two centrifugation steps at 4°C each. The first step involved centrifugation at 2000 × g for 10 min. Plasma samples were collected and transferred to silicone tubes for a further second centrifugation step (20,000 × g, 4 °C, within 5 min) to thoroughly remove cell debris. The supernatant was pooled and eluted in 2 mL Tris-EDTA buffer and quantified with a Nanodrop (ND-1000 Spectrophotometer v 3.7.1, Waltham, MA, USA) using spectrophotometric analysis at 260/280 nm.
2.6. Measurement of Cell-Free DNAs in Plasma Samples
Measures of cf-nDNA was performed with real time quantitative PCR (qPCR) using NADH dehydrogenase, ND2 and beta-2-microglobulin. The qPCR reactions were carried out using SYBR Green Technology (Thermo Fisher Scientific, Waltham, MA, USA).
The sequences of the primers for n-DNA and were the following: Forward primer – CCCCACACACATGCACTTACC, Reverse primer – ATCAAACTCAAAGGGCAGGA.
We used in total 20 μL of reaction volume, which composed of 0.1 mL TaqMan1Universal PCR Master Mix (Applied Biosystems, Branchburg, New Jersey, USA), 0.5 mL ultra-clear water, and 0.25 μL of each of the primers (Sigma-Aldrich, St. Louis, Missouri, USA), 1 μL of a FAM-labeled MT-ATP 8-probe, 1 μL of a MVIC-labeled GAPDH probe, 2 μL of Tris–EDTA buffer containing cell-free DNA isolated from plasma. The concentrations of primers and probes in the reaction volume were 0.6 μmol/L and 0.4 μmol/L, respectively. Negative control was 2 μL of Tris–EDTA buffer. The measures were provided with the 7500 HT Real-time PCR System (Applied Biosystems, Branchburg, New Jersey, USA) using the high resolution melt software v. 2.0 (Applied Biosystems, Branchburg, New Jersey, USA) according to conventional method [35].
2.7. Statistical Analysis
Statistical analysis was executed using SPSS 11.0 for Windows and v. 9 Graph Pad Prism (Graph Pad Software, San Diego, CA, USA). Continuous variables were expressed as means ± SD for parametric data and median and interquartile range [IQR] according to whether they were normally distributed or not. Kolmogorov–Smirnov test was used to test for normal distribution. The distribution of dichotomous values was assessed with Chi-square test. We performed One-way Analysis of Variance (ANOVA) and Tukey test for comparisons of variables between cohorts. Spearman’s correlation coefficient (r) was used for correlations between the levels of cf-nDNA and other parameters. The reliability of the predictive models was determined by receiver operating curve (ROC) analysis, with further calculation of area under the curve (AUC), its 95% confidence interval (CI), sensitivity (Se), specificity (Sp) and likelihood ratio (LR) for each predictor. The Youden test was used to estimate the cut-off points for cf-nDNA. Predictors of HFimpEF were determined by univariate and multivariate logistic regression analysis. We reported odds ratio (OR), 95% CI for each variable included in regression analysis. Predictive value of cf-nDNA for HFimpEF was reclassified using the integrated discrimination indices (IDI) and net reclassification improvement (NRI). Differences were considered significant at the level of statistical significance p < 0.05.
3. Results
3.1. General Clinical Characteristics of the Patients
There were 452 patients enrolled in this study, 177 of whom met criteria of HFimpEF events and 275 did not (Table 1). Patients were on average 59 years old, of which 266 were male, accounting for 58.9%. Mean values of body mass index (BMI) were 25.8±3.5 kg/m2. Comorbidity profile included dyslipidemia (63.2%), hypertension (15.7%), stable coronary artery disease (31.2%), dilated cardiomyopathy (15.0%), paroxysmal, persistent or permanent forms of atrial fibrillation (30.3%), smoking (37.2%), abdominal obesity (24.8%), LV hypertrophy (69.9%), and chronic kidney disease 1-3 grades (29.2%). Among entire patient population, 31.9% had I/II NYHA HF class, 50.8% had III NYHA HF class, 17.3% had IV NYHA HF class. Patients had an average of LVEF equal 32% (29%-39%), LVMMI was 226±15 g/m2, LAVI was 46 mL/m2 (39 mL/m2-52 mL/m2), circulating level of NT-proBNP and hs-CRP were 3228 pmol/mL and 9.68 mg/L respectively.
There were no significant differences between both cohorts in age, gender, BMI, as well as in a presence of dyslipidemia, hypertension, smoking, abdominal obesity, atrial fibrillation, T2DM, LV hypertrophy, CKD 1-3 grades, III and IV NYHA HF class, systolic and diastolic blood pressure, LVMMI, LAVI, E/e`, fasting glucose, total cholesterol and high-density lipoprotein cholesterol (HDL-C), hs-CRP, NT-proBNP and concomitant medication apart from digoxin. On the contrary, patients from HFimpEF cohort had often I/II HF NYHA class, whereas individuals from persistent HFrEF cohort had frequently ischemia-induced cardiomyopathy and IV HF NYHA class. Aline with it, they had significantly higher LVEDV and LVESV, lower LVEF, eGFR and also levels of creatinine, low-density lipoprotein cholesterol (LDL-C), TNF-alpha and cf-nDNA than those with HFimpEF. Patients from both cohorts received conventional therapies that was adjusted accordingly concomitant disease presence.
3.2. The Dynamics of Circulating Biomarkers Levels
In HFimpEF cohort there was a decline of NT-proBNP levels from 3015 (1780 – 5220) pmol/mL to 1940 (1220 – 2580) pmol/mL (Δ% = -35.6%; p = 0.01), whereas in those who had persistent HFrEF the levels of NT-proBNP did not exert sufficient changes. However, in persistent HFrEF cohort there was a trend to an increase from 3290 (1820 – 5470) pmol/mL at baseline up to 3515 (1380 – 6152) pmol/mL at 6 month (Δ% = 0.6%; p = 0.48).
The levels of hs-CRP demonstrated a trend to a decrease in both cohorts: from 9.25 (3.45 – 12.70) mg/L to 7.02 (3.45 – 10.20) mg/L in HFimpEF (Δ% = -24.1%, p = 0.20) and from 10.70 (5.80 – 17.50) to 9.50 (4.90 – 15.10) mg/L (Δ% = -11.2%, p = 0.20) in persistent HFrEF.
In HFimpEF patients, TNF-alpha levels decreased from 3.11 (2.62-3.69) pg/mL to 2.88 (2.53-3.27) pg/mL (Δ% = -7.4%, p = 0.04), whereas in persistent HFrEF patients, TNF-alpha levels remained unchanged over the observation period (Δ% = -0.9%, p = 0.62).
In 6 month of the observation period, the patients who met criteria of HFimpEF demonstrated a significant decrease in the levels of cf-nDNA (Δ% = -19.4%, p = 0.01) when compared with the patients from persistent HFrEF cohort (Δ% = -14.0%, p = 0.66). However, patents with HFimpEF had significantly lower 6-month levels of cf-nDNA than those without these criteria: 8.3 (5.9 – 10.6) μmol/L versus 13.4 (10.3 - 16.5) μmol/L, p = 0.01).
3.3. Spearman’s Correlation between Circulating Levels of Cell-Free DNA and Other Parameters
We found positive correlations between levels of cf-nDNA and presence of ischemia-induced cariomyopathy (r = 0.46; p = 0.001), chronic kidney disease (r = 0.29, p = 0.01), NYHA HF class (r = 0.28, p = 0.001), and T2DM (r = 0.31; p = 0.001), LAVI (r = 0.38; p = 0.001), NT-proBNP (r = 0.36; p = 0.001), LVEDV (r = 0.34; p = 0.001), TNF-alpha (r = 0.29; p = 0.001), hs-CRP (r = 0.28; p = 0.001), creatinine (r = 0.23; p = 0.02), left bundle branch block on ECG (r = 0.22; p = 0.04) and negative correlation with LVEF (r = -0.36; p = 0.001). There were not association of the levels of cf-nDNA with BMI, fasting glucose, LDL-C, TG as well as concomitant medications apart from digoxin.
3.4. The Reliability of Circulating Levels of cf-nDNA: The Results of the ROC Curve Analysis
We found that circulating levels of cf-nDNA <7.5 µmol/L (area under curve [AUC] = 0.875; 95% confidence interval [CI] = 0.795–0.950; sensitivity = 87.0%, specificity = 73.5%; likelihood ratio = 3.288; p = 0.001) were associated with HFimpEF (Figure 2).
3.5. The Predictors of HFimpEF: The Univariate and Multivariate Logistic Regression
We identified several factors with plausible predictive values for HFimpEF using the univariate logistic regression model (Table 2). For this analysis we used median levels of NT-proBNP (1940 pmol/mL), TNF-alpha (2.88 pg/mL), hs-CRP (7.02 mg/L) in HFimpEF as cut-offs. Along with it, a relative decrease in NT-proBNP levels 35% was added to the regression analysis. In rough regression analysis we established that a presence of ischemia-induced cardiomyopathy (OR = 0.75; CI = 0.62 – 0.88; p = 0.044), IV HF NYHA class (OR = 0.71; CI = 0.57 – 0.92; p = 0.044), T2DM (OR = 0.77; CI = 0.71 – 0.82; p = 0.042), CKD (OR = 0.89; CI = 0.84 – 0.96; p = 0.048), and digoxin administration (OR = 0.85; CI = 0.72-0.97; p = 0.042) were negative factors for HFimpEF, whereas NT-proBNP ≤1940 pmol/mL (OR = 1.42; 95% CI = 1.19-1.98, p = 0.001), relative decrease in NT-proBNP levels (>35% vs. ≤35%) from baseline (OR = 1.67; CI = 1.51-1.82; p = 0.001) and cf-nDNA ≤7.5 μmol/L (OR = 1.56; 95% CI = 1.07-2.94, p = 0.001) were positive predictors for HFimpEF. Multivariate logistic regression yielded that ischemia-induced cardiomyopathy (OR = 0.77; CI = 0.60 – 0.90; p = 0.042), IV HF NYHA class (OR = 0.76; CI = 0.63 – 0.87; p = 0.001), T2DM (OR = 0.84; CI = 0.62 – 0.92; p = 0.046) NT-proBNP ≤1940 pmol/mL (OR = 1.35; 95% CI = 1.12-1.76, p = 0.001), relative decrease in NT-proBNP levels (>35% vs. ≤35%) from baseline (OR = 1.70; CI = 1.61-1.83; p = 0.001) and cf-nDNA ≤7.5 μmol/L (OR = 1.64; 95% CI = 1.10-2.07, p = 0.001) remained independent predictors for HFimpEF.
After adjustment to ischemia-induced cardiomyopathy, IV HF NYHA class, and digoxin use multivariate logistic regression showed that NT-proBNP ≤1940 pmol/mL (OR = 1.43; 95% CI = 1.21-1.88, p = 0.001), relative decrease in NT-proBNP levels (>35% vs. ≤35%) from baseline (OR = 1.52; 95% CI = 1.38-0.69, p = 0.001) and cf-nDNA ≤7.5 μmol/L (OR = 1.64; 95% CI = 1.19-2.15, p = 0.001) independently predicted HFimpEF.
3.5. Comparison of the Models for HFimpEF
To compare the models, we used area under the curve (AUC) estimation, which showed superiority of the discriminatory value of relative decrease in NT-proBNP levels ≤35% from baseline and cf-nDNA ≤7.5 μmol/L over NT-proBNP ≤1940 pmol/mL (p = 0.001) (Table 3). Nevertheless, cf-nDNA ≤7.5 μmol/L improved the risk stratification by increasing the prognostic impact of NT-proBNP level and its dynamic on HFimpEF independently. However, we found that the predictive value of model 4 (NT-proBNP levels ≤1940 pmol/mL + cf-nDNA) was not better than model 3 (cf-nDNA ≤7.5 μmol/L), whereas it was better than the reference model, whereas model 5 (relative decrease in NT-proBNP levels ≤35% from baseline + cf-nDNA) exerted superiority over model 1 (NT-proBNP ≤1940 pmol/mL) and model 2 (relative decrease in NT-proBNP levels ≤35% from baseline).
4. Discussion
The results of our investigation showed that the level of cf-nDNA ≤7.5 μmol/L is associated with a presence of HFimpEF and seems to improve a risk stratification by increasing the prognostic value of NT-proBNP≤1940 pmol/mL and relative decrease in NT-proBNP levels ≤35% from baseline on HFimpEF. Along with it, combined model composed of relative decrease in NT-proBNP levels ≤35% from baseline + cf-nDNA demonstrated the best discriminative value om dependent variable when compared with NT-proBNP ≤1940 pmol/mL and relative decrease in NT-proBNP levels ≤35% from baseline alone.
These findings can demonstrate how to predict LVEF improvement and improve the prognosis of persistent HFrEF. Indeed, recent meta-analysis revealed that HFimpEF compared with HFpEF was associated with a moderately lower risk of mortality and hospitalization [36]. Moreover, based on different evidence, from 23% to 61% of patients with HFrEF would be effectively treated to reach criteria of HFimpEF and thereby improved their prognosis [13,36,37,38]. However, ischemic cardiomyopathy, T2DM, E/e`, LAVI, left bundle branch block, higher platelet count, implantable cardioverter-defibrillator therapy were found to be negative predictive factors for HFimpEF [13,39,40]. Although single measured values of NT-proBNP >5000 pg/mL and > 1000 pg/mL predicted a worse outcome in hospitalized and at discharge patients with HFrEF, there is serious concerns about the predictive ability of NT-proBNP to be associated with HFimpEF [41,42]. Indeed, elevated baseline NT-proBNP was detected as the powerful prognostic factor associated with increased risk of CV events in HFrEF patients regardless of improved EF, independent of age, sex, duration of HFrEF and other clinical risk factors [42]. On the other hand, a trajectory of NT-proBNP in patients with HFrEF corresponded to the dynamic in LVEF and reduction in NT-proBNP concentration was related to reverse of LV remodeling during HF management [43]. Finally, NT-proBNP and the trend to a decrease in the levels of NT-proBNP seem to be obvious biomarkers of LVEF restoration.
In our study, we found that HFimpEF was associated with a significant decrease in NT-proBNP (>35% from baseline), whereas circulating levels of NT-proBNP remained unchanged in patients with persistent HFimpEF. Similarly, cf-DNA levels ≤7.5 μmol/L were associated with the occurrence of recovery of LVEF, whereas levels of pro-inflammatory cytokines were not. Although the baseline levels of c-fib DNA in patients with HFrEF differed significantly from the cut-off point obtained by ROC analysis, we acknowledge that the trend towards a decrease in its concentration more accurately characterizes the likelihood of LVEF recovery than the baseline concentration of NT-proBNP. However, the models constructed from cf-nDNA showed strict similarity in their predictive ability for HFimpEF.
These findings partially agree with some previous studies, in which optimal guideline-based therapy improved patients' clinical status, cardiohemodynamic parameters and prognosis irrespective of baseline NT-proBNP level, although reduced NT-proBNP concentration was frequently associated with restoring of LVEF [44,45]. In fact, the proportion of HFrEF patients with meaningful improvement of HF-related health status or NT-proBNP level did not exceed 62% in actively treated patient cohort [45,46]. It supports to mean that NT-proBNP dynamics is probably a sufficient argument in favor of a high probability of LVEF recovery, but not for all cases. To improve the predictive ability of a decrease in NT-proBNP on HFimpEF we used the measurement of cf-nDNA levels, which reflect either cellular damage or impaired permeability of cell membranes [47,48].
Non-specific circulating molecular pattern of cf-DNA fragments are considered the biomarker of inflammation and immune reaction including neutrophil extracellular traps [49,50]. On the other hand, cf-DNA can modulate intra- and intercellular signaling cascades to upregulate the transcriptional expression of pro-inflammatory genes, inflammasome synthesis and induce oxidative stress within cells leading to increase a susceptibility to CVD including HF [51,52]. Although in this study, we did not evaluate circulating cardiomyocyte-specific cf-DNA, elevated levels of cf-nDNA derived from other cells, such as adult hematopoietic cells, is common for the patients with HF. They may be associated with transforming growth factor-beta-1/Smad-dependent activation of cardiac fibroblasts, macrophages and other immune cells, which intervene in cardiac remodeling through activation of apoptosis, necrosis, extracellular matrix accumulation, autophagy alteration resulted in myocardial stiffness and reduced LVEF [53]. Predictably, circulating cf-nDNA fragments may play a pivotal role in the progression to HFrEF during pathological insults to the heart via interstitial fibrosis and cardiomyocyte cell death.
The results of this study revealed that circulating pool of cf-nDNA fragments was negatively correlation with LVEF and positively associated with ischemic etiology of HFrEF, several concomitant comorbidities including chronic kidney disease and T2DM, severity of HFrEF, hemodynamic performances reflection fluid overload (LAVI, LVEDV), as well as conventional biomarkers of biomechanical stress (NT-proBNP) and inflammation (TNF-alpha, hs-CRP). Interestingly, individuals with wide QRS on ECG (with left or right bundle branch block) exhibited mild positive association with the levels of cf-nDNA. These findings indicate that cf-nDNA may correspond to previously establish non-specific predictor for HFimpEF that has been detected in previous studies on this issue [11,36,55,56].
In contrast to these studies, we were able to establish the fact that a decrease in NT-proBNP concentration is inferior in its predictive value to cf-nDNA concentration in the blood of patients with HFrEF receiving optimal therapy with the aim of reaching HFimpEF. Thus, it can be hypothesized that serial measurements of not only NT-proBNP, but also cf-nDNA, are likely to apply more individualized approach in respect to the risk stratification and management among patients with HFrEF and thereby to decrease the proportion of those who have persistent HFrEF. At least avoiding the use of digoxin, extending the implementation of beta-blockers, ARNIs, SGLT2 inhibitors is probably the simplest solution to increase the likelihood of achieving LVEF reversal. Nevertheless, the identification of a target cohort of patients with the highest probability of LV function improvement may be encouraging.
Another aspect of the potential application of the results obtained is the prospect of monitoring the risk of a decline in the previously improved LVEF and timely individual correction of treatment. Although this idea may have serious practical value, further research is needed to clarify the situation and to develop and validate an effective predictive model.
5. Study Limitations
The study has several limitations, the first of which concerns the origin of the DNA molecules. Although some molecular features, such as the pattern of methylation, the proportion of circular and single-stranded form, and the distribution of cell-free DNA fragments provide important information about their tissue sources, reflecting the severity of target organ damage, we studied a circulating pool of cf-nDNA without categorizing its correspondence to cardiac myocytes. A second limitation may be due to the study design, in which patients were enrolled according to the presence of HFrEF, but not randomized. Nevertheless, a respectively small sample size can be considered as one of the limitations of the study. In the future, we will extend our investigation by randomizing a larger population of HF patients. We believe that these limitations do not have a serious impact on the interpretation of the results of our study, but highlight the possibilities to investigate our hypothesis in the future.
6. Conclusions
In this study, we established that the levels of cf-nDNA≤7.5 μmol/L independently predicted HFimpEF and improved discriminative ability of as single measured NT-proBNP as well as relative decrease in NT-proBNP levels ≤35% from baseline in individuals with HFrEF.
Author Contributions
Conceptualization, A.E.B.; methodology, M.L. and A.E.B.; software, A.E.B. and O.O.B.; validation, T.A.B., A.E.B., M.L.; formal analysis, O.O.B., T.A.B. and A.E.B.; investigation, O.O.B. and T.A.B.; resources, T.A.B. and O.O.B.; data curation, A.E.B. and T.A.B.; writing—original draft preparation, T.A.B., O.O.B., M.L. and A.E.B.; writing—review and editing, T.A.B., O.O.B., M.L. and A.E.B.; visualization, O.O.B. and T.A.B.; supervision, A.E.B.; project administration, T.A.B. and O.O.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Ethics Committee of Zaporozhye Medical Academy of Post-graduate Education (protocol number: 8; date of approval: 10 October 2020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author due to privacy restrictions.
Acknowledgments
We would like to thank all patients who gave their consent to participate in the study and all administrative staff and doctors of Private Hospital “Vita-Centre LTD” for study assistance.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Bozkurt B, Coats AJS, Tsutsui H, Abdelhamid CM, Adamopoulos S, Albert N, Anker SD, Atherton J, Böhm M, Butler J, Drazner MH, Michael Felker G, Filippatos G, Fiuzat M, Fonarow GC, Gomez-Mesa JE, Heidenreich P, Imamura T, Jankowska EA, Januzzi J, Khazanie P, Kinugawa K, Lam CSP, Matsue Y, Metra M, Ohtani T, Francesco Piepoli M, Ponikowski P, Rosano GMC, Sakata Y, Seferović P, Starling RC, Teerlink JR, Vardeny O, Yamamoto K, Yancy C, Zhang J, Zieroth S. Universal definition and classification of heart failure: a report of the Heart Failure Society of America, Heart Failure Association of the European Society of Cardiology, Japanese Heart Failure Society and Writing Committee of the Universal Definition of Heart Failure: Endorsed by the Canadian Heart Failure Society, Heart Failure Association of India, Cardiac Society of Australia and New Zealand, and Chinese Heart Failure Association. Eur J Heart Fail. 2021; 23(3):352-380. [CrossRef]
- Keshvani N, Shah S, Ayodele I, Chiswell K, Alhanti B, Allen LA, Greene SJ, Yancy CW, Alonso WW, Van Spall HG, Fonarow GC, Heidenreich PA, Pandey A. Sex differences in long-term outcomes following acute heart failure hospitalization: Findings from the Get With The Guidelines-Heart Failure registry. Eur J Heart Fail. 2023 Sep;25(9):1544-1554. [CrossRef]
- Chimed S, Stassen J, Galloo X, Meucci MC, van der Bijl P, Knuuti J, Delgado V, Marsan NA, Bax JJ. Impact of Worsening Heart Failure on Long-Term Prognosis in Patients With Heart Failure With Reduced Ejection Fraction. Am J Cardiol. 2022 Dec 1;184:63-71. [CrossRef]
- Chen S, Huang Z, Liang Y, Zhao X, Aobuliksimu X, Wang B, He Y, Kang Y, Huang H, Li Q, Yao Y, Lu X, Qian X, Xie X, Liu J, Liu Y. Five-year mortality of heart failure with preserved, mildly reduced, and reduced ejection fraction in a 4880 Chinese cohort. ESC Heart Fail. 2022;9(4):2336-2347. [CrossRef]
- McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Bohm M, et al; ESC Scientific Document Group. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021; 42(36):3599-3726. [CrossRef]
- Shah KS, Xu H, Matsouaka RA, Bhatt DL, Heidenreich PA, Hernandez AF, Devore AD, Yancy CW, Fonarow GC. Heart Failure With Preserved, Borderline, and Reduced Ejection Fraction: 5-Year Outcomes. J Am Coll Cardiol. 2017;70(20):2476-2486. [CrossRef]
- Tang J, Wang P, Liu C, Peng J, Liu Y, Ma Q. Pharmacotherapy in patients with heart failure with reduced ejection fraction: A systematic review and meta-analysis. Chin Med J (Engl). 2024. Epub ahead of print. [CrossRef] [PubMed]
- Mo X, Lu P, Yang X. Efficacy of sacubitril-valsartan and SGLT2 inhibitors in heart failure with reduced ejection fraction: A systematic review and meta-analysis. Clin Cardiol. 2023;46(10):1137-1145. [CrossRef]
- Rosano GMC, Vitale C, Spoletini I. Precision Cardiology: Phenotype-targeted Therapies for HFmrEF and HFpEF. Int J Heart Fail. 2024;6(2):47-55. [CrossRef]
- Romero E, Baltodano AF, Rocha P, Sellers-Porter C, Patel DJ, Soroya S, Bidwell J, Ebong I, Gibson M, Liem DA, Jimenez S, Bang H, Sirish P, Chiamvimonvat N, Lopez JE, Cadeiras M. Clinical, Echocardiographic, and Longitudinal Characteristics Associated With Heart Failure With Improved Ejection Fraction. Am J Cardiol. 2024; 211:143-152. [CrossRef]
- Solymossi B, Muk B, Sepp R, Habon T, Borbély A, Heltai K, Majoros Z, Járai Z, Vágány D, Szatmári Á, Sziliczei E, Bánfi-Bacsárdi F, Nyolczas N. Incidence and predictors of heart failure with improved ejection fraction category in a HFrEF patient population. ESC Heart Fail. 2024; 11(2):783-794. [CrossRef]
- Su K, Li M, Wang L, Tian S, Su J, Gu J, Chen S. Clinical characteristics, predictors, and outcomes of heart failure with improved ejection fraction. Int J Cardiol. 2022;357:72-80. [CrossRef]
- Ho LT, Juang JJ, Chen YH, Chen YS, Hsu RB, Huang CC, Lee CM, Chien KL. Predictors of Left Ventricular Ejection Fraction Improvement in Patients with Early-Stage Heart Failure with Reduced Ejection Fraction. Acta Cardiol Sin. 2023;39(6):854-861. [CrossRef]
- Segev A, Avrahamy B, Fardman A, Matetzky S, Freimark D, Regev O, Kuperstein R, Grupper A. Heart failure with improved ejection fraction: patient characteristics, clinical outcomes and predictors for improvement. Front Cardiovasc Med. 2024;11:1378955. [CrossRef]
- Si J, Ding Z, Hu Y, Zhang X, Zhang Y, Cao H, Liu Y. Predictors and prognostic implications of left ventricular ejection fraction trajectory improvement in the spectrum of heart failure with reduced and mildly reduced ejection fraction. J Cardiol. 2024;83(4):250-257. [CrossRef]
- Lo YMD, Han DSC, Jiang P, Chiu RWK. Epigenetics, fragmentomics, and topology of cell-free DNA in liquid biopsies. Science. 2021;372(6538):eaaw3616. [CrossRef]
- Cahilog Z, Zhao H, Wu L, Alam A, Eguchi S, Weng H, Ma D. The Role of Neutrophil NETosis in Organ Injury: Novel Inflammatory Cell Death Mechanisms. Inflammation. 2020;43(6):2021-2032. [CrossRef]
- Stanley KE, Jatsenko T, Tuveri S, Sudhakaran D, Lannoo L, Van Calsteren K, de Borre M, Van Parijs I, Van Coillie L, Van Den Bogaert K, De Almeida Toledo R, Lenaerts L, Tejpar S, Punie K, Rengifo LY, Vandenberghe P, Thienpont B, Vermeesch JR. Cell type signatures in cell-free DNA fragmentation profiles reveal disease biology. Nat Commun. 2024;15(1):2220. [CrossRef]
- Oellerich M, Sherwood K, Keown P, Schütz E, Beck J, Stegbauer J, Rump LC, Walson PD. Liquid biopsies: donor-derived cell-free DNA for the detection of kidney allograft injury. Nat Rev Nephrol. 2021;17(9):591-603. [CrossRef]
- Tan E, Liu D, Perry L, Zhu J, Cid-Serra X, Deane A, Yeo C, Ajani A. Cell-free DNA as a potential biomarker for acute myocardial infarction: A systematic review and meta-analysis. Int J Cardiol Heart Vasc. 2023;47:101246. [CrossRef]
- Antonatos D, Patsilinakos S, Spanodimos S, Korkonikitas P, Tsigas D. Cell-free DNA levels as a prognostic marker in acute myocardial infarction. Ann N Y Acad Sci. 2006; 1075(1):278–281. [CrossRef]
- Medina JE, Dracopoli NC, Bach PB, Lau A, Scharpf RB, Meijer GA, Andersen CL, Velculescu VE. Cell-free DNA approaches for cancer early detection and interception. J Immunother Cancer. 2023; 11(9):e006013. [CrossRef]
- Berezina TA, Berezin AE. Cell-free DNA as a plausible biomarker of chronic kidney disease. Epigenomics. 2023;15(17):879-890. [CrossRef]
- Mansueto G, Benincasa G, Della Mura N, Nicoletti GF, Napoli C. Epigenetic-sensitive liquid biomarkers and personalised therapy in advanced heart failure: a focus on cell-free DNA and microRNAs. J Clin Pathol. 2020;73(9):535-543. [CrossRef]
- Yokokawa T, Misaka T, Kimishima Y, Shimizu T, Kaneshiro T, Takeishi Y. Clinical Significance of Circulating Cardiomyocyte-Specific Cell-Free DNA in Patients With Heart Failure: A Proof-of-Concept Study. Can J Cardiol, 2020; 36(6):931-935. [CrossRef]
- Berezina, T.A.; Kopytsya, M.P.; Petyunina, O.V.; Berezin, A.A.; Obradovic, Z.; Schmidbauer, L.; Lichtenauer, M.; Berezin, A.E. Lower Circulating Cell-Free Mitochondrial DNA Is Associated with Heart Failure in Type 2 Diabetes Mellitus Patients. Cardiogenetics 2023, 13, 15–30. [Google Scholar] [CrossRef]
- American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2021. Diabetes Care. 2021; 44(Suppl 1):S15-S33. [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, et al; ESC Scientific Document Group. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur Heart J. 2018; 39(33):3021-3104. [CrossRef]
- Mach F, Baigent C, Catapano AL, Koskinas KC, Casula M, Badimon L, et al; ESC Scientific Document Group. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J. 2020; 41(1):111-188. [CrossRef]
- Knuuti J, Wijns W, Saraste A, Capodanno D, Barbato E, Funck-Brentano C, Prescott E, Storey RF, Deaton C, Cuisset T, Agewall S, Dickstein K, Edvardsen T, Escaned J, Gersh BJ, Svitil P, Gilard M, Hasdai D, Hatala R, Mahfoud F, Masip J, Muneretto C, Valgimigli M, Achenbach S, Bax JJ; ESC Scientific Document Group. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. 2020;41(3):407-477. Erratum in: Eur Heart J. 2020 Nov 21;41(44):4242. 10.1093/eurheartj/ehz825. [CrossRef]
- Inker LA, Astor BC, Fox CH, Isakova T, Lash JP, Peralta CA, Kurella Tamura M, Feldman HI. KDOQI US commentary on the 2012 KDIGO clinical practice guideline for the evaluation and management of CKD. Am J Kidney Dis. 2014;63(5):713-35. [CrossRef]
- Mitchell, C.; Rahko, P.S.; Blauwet, L.A.; Canaday, B.; Finstuen, J.A.; Foster, M.C.; Horton, K.; Ogunyankin, K.O.; Palma, R.A.; Velazquez, E.J. Guidelines for Performing a Comprehensive Transthoracic Echocardiographic Examination in Adults: Recommendations from the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2018, 32, 1–64. [Google Scholar] [CrossRef] [PubMed]
- Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF 3rd, Feldman HI, et al; CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration). A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009; 150(9):604-12. [CrossRef]
- Hasenleithner SO, Speicher MR. A clinician's handbook for using ctDNA throughout the patient journey. Mol Cancer. 2022; 21(1):81. [CrossRef]
- He Y, Ling Y, Guo W, Li Q, Yu S, Huang H, Zhang R, Gong Z, Liu J, Mo L, Yi S, Lai D, Yao Y, Liu J, Chen J, Liu Y, Chen S. Prevalence and Prognosis of HFimpEF Developed From Patients With Heart Failure With Reduced Ejection Fraction: Systematic Review and Meta-Analysis. Front Cardiovasc Med. 2021; 8:757596. [CrossRef]
- Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, Deswal A, Drazner MH, Dunlay SM, Evers LR, Fang JC, Fedson SE, Fonarow GC, Hayek SS, Hernandez AF, Khazanie P, Kittleson MM, Lee CS, Link MS, Milano CA, Nnacheta LC, Sandhu AT, Stevenson LW, Vardeny O, Vest AR, Yancy CW. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022;145(18):e895-e1032. [CrossRef]
- Zamora E, González B, Lupón J, Borrellas A, Domingo M, Santiago-Vacas E, Cediel G, Codina P, Rivas C, Pulido A, Crespo E, Velayos P, Diaz V, Bayes-Genis A. Quality of life in patients with heart failure and improved ejection fraction: one-year changes and prognosis. ESC Heart Fail. 2022;9(6):3804-3813. [CrossRef]
- Yoshimura R, Hayashi O, Horio T, Fujiwara R, Matsuoka Y, Yokouchi G, Sakamoto Y, Matsumoto N, Fukuda K, Shimizu M, Izumiya Y, Yoshiyama M, Fukuda D, Fujimoto K, Kasayuki N. The E/e' ratio on echocardiography as an independent predictor of the improvement of left ventricular contraction in patients with heart failure with reduced ejection fraction. J Clin Ultrasound. 2023;51(7):1131-1138. [CrossRef]
- Cao TH, Tay WT, Jones DJL, Cleland JGF, Tromp J, Emmens JE, Teng TK, Chandramouli C, Slingsby OC, Anker SD, Dickstein K, Filippatos G, Lang CC, Metra M, Ponikowski P, Samani NJ, Van Veldhuisen DJ, Zannad F, Anand IS, Lam CSP, Voors AA, Ng LL. Heart failure with improved versus persistently reduced left ventricular ejection fraction: A comparison of the BIOSTAT-CHF (European) study with the ASIAN-HF registry. Eur J Heart Fail. 2024. Epub ahead of print. [CrossRef] [PubMed]
- Lam CSP, Li YH, Bayes-Genis A, Ariyachaipanich A, Huan DQ, Sato N, Kahale P, Cuong TM, Dong Y, Li X, Zhou Y. The role of N-terminal pro-B-type natriuretic peptide in prognostic evaluation of heart failure. J Chin Med Assoc. 2019; 82(6):447-451. [CrossRef]
- Liu D, Hu K, Schregelmann L, Hammel C, Lengenfelder BD, Ertl G, Frantz S, Nordbeck P. Determinants of ejection fraction improvement in heart failure patients with reduced ejection fraction. ESC Heart Fail. 2023;10(2):1358-1371. [CrossRef]
- Yamamoto M, Ishizu T, Sato K, Minami K, Terauchi T, Nakatsukasa T, Kawamatsu N, Machino-Ohtsuka T, Ieda M. Longitudinal Changes in Natriuretic Peptides and Reverse Cardiac Remodeling in Patients with Heart Failure Treated with Sacubitril/Valsartan Across the Left Ventricular Ejection Traction Spectrum. Int Heart J. 2023 Nov 30;64(6):1071-1078. [CrossRef]
- Butt JH, Adamson C, Docherty KF, de Boer RA, Petrie MC, Inzucchi SE, Kosiborod MN, Maria Langkilde A, Lindholm D, Martinez FA, Bengtsson O, Schou M, O'Meara E, Ponikowski P, Sabatine MS, Sjöstrand M, Solomon SD, Jhund PS, McMurray JJV, Køber L. Efficacy and Safety of Dapagliflozin in Heart Failure With Reduced Ejection Fraction According to N-Terminal Pro-B-Type Natriuretic Peptide: Insights From the DAPA-HF Trial. Circ Heart Fail. 2021;14(12):e008837. [CrossRef]
- Nassif ME, Windsor SL, Tang F, Khariton Y, Husain M, Inzucchi SE, McGuire DK, Pitt B, Scirica BM, Austin B, Drazner MH, Fong MW, Givertz MM, Gordon RA, Jermyn R, Katz SD, Lamba S, Lanfear DE, LaRue SJ, Lindenfeld J, Malone M, Margulies K, Mentz RJ, Mutharasan RK, Pursley M, Umpierrez G, Kosiborod M. Dapagliflozin Effects on Biomarkers, Symptoms, and Functional Status in Patients With Heart Failure With Reduced Ejection Fraction: The DEFINE-HF Trial. Circulation. 2019 Oct 29;140(18):1463-1476. [CrossRef]
- Martinsson A, Oest P, Wiborg MB, Reitan Ö, Smith JG. Longitudinal evaluation of ventricular ejection fraction and NT-proBNP across heart failure subgroups. Scand Cardiovasc J. 2018;52(4):205-210. [CrossRef]
- Dutta A, Das M, Ghosh A, Rana S. Molecular and cellular pathophysiology of circulating cardiomyocyte-specific cell free DNA (cfDNA): Biomarkers of heart failure and potential therapeutic targets. Genes Dis. 2022 Aug 31;10(3):948-959. PMCID: PMC10308167. [CrossRef] [PubMed]
- Ren J, Jiang L, Liu X, Liao Y, Zhao X, Tang F, et al. Heart-specific DNA methylation analysis in plasma for the investigation of myocardial damage. J Transl Med. 2022; 20(1):36. [CrossRef]
- Berezin A. Neutrophil extracellular traps: The core player in vascular complications of diabetes mellitus. Diabetes Metab Syndr. 2019; 13(5):3017-3023. [CrossRef]
- Thorsen SU, Moseholm KF, Clausen FB. Circulating cell-free DNA and its association with cardiovascular disease: what we know and future perspectives. Curr Opin Lipidol. 2024;35(1):14-19. [CrossRef]
- Vulesevic B, Lavoie SS, Neagoe PE, Dumas E, Räkel A, White M, et al. CRP Induces NETosis in Heart Failure Patients with or without Diabetes. Immunohorizons. 2019;3(8):378-388. [CrossRef]
- Liu LP, Cheng K, Ning MA, Li HH, Wang HC, Li F, et al. Association between peripheral blood cells mitochondrial DNA content and severity of coronary heart disease. Atherosclerosis. 2017; 261:105-110. [CrossRef]
- Frangogiannis, NG. The inflammatory response in myocardial injury, repair, and remodelling. Nat Rev Cardiol. 2014; 11(5):255-65. [CrossRef]
- Liu Q, Wu J, Zhang X, Li X, Wu X, Zhao Y, Ren J. Circulating mitochondrial DNA-triggered autophagy dysfunction via STING underlies sepsis-related acute lung injury. Cell Death Dis. 2021;12(7):673. [CrossRef]
- Oommen SG, Man RK, Talluri K, Nizam M, Kohir T, Aviles MA, Nino M, Jaisankar LG, Jaura J, Wannakuwatte RA, Tom L, Abraham J, Siddiqui HF. Heart Failure With Improved Ejection Fraction: Prevalence, Predictors, and Guideline-Directed Medical Therapy. Cureus. 2024;16(6):e61790. [CrossRef]
- Kim KA, Kim SH, Lee KY, Yoon AH, Hwang BH, Choo EH, Kim JJ, Choi IJ, Kim CJ, Lim S, Park MW, Yoo KD, Jeon DS, Ahn Y, Jeong MH, Chang K. Predictors and Long-Term Clinical Impact of Heart Failure With Improved Ejection Fraction After Acute Myocardial Infarction. J Am Heart Assoc. 2024;13(16):e034920. [CrossRef]
Figure 1.
Study design and patients selections for study procedures. Abbreviations: HF, heart failure; HFrEF, heart failure with reduced ejection fraction; HFimpEF, heart failure with improved LVEF; eGFR, estimated glomerular filtration rate; cf-nDNA, cell-free nuclear-derived DNA; TIA, transient ischemic attack; NT-proBNP, N-terminal brain natriuretic pro-peptide.
Figure 1.
Study design and patients selections for study procedures. Abbreviations: HF, heart failure; HFrEF, heart failure with reduced ejection fraction; HFimpEF, heart failure with improved LVEF; eGFR, estimated glomerular filtration rate; cf-nDNA, cell-free nuclear-derived DNA; TIA, transient ischemic attack; NT-proBNP, N-terminal brain natriuretic pro-peptide.
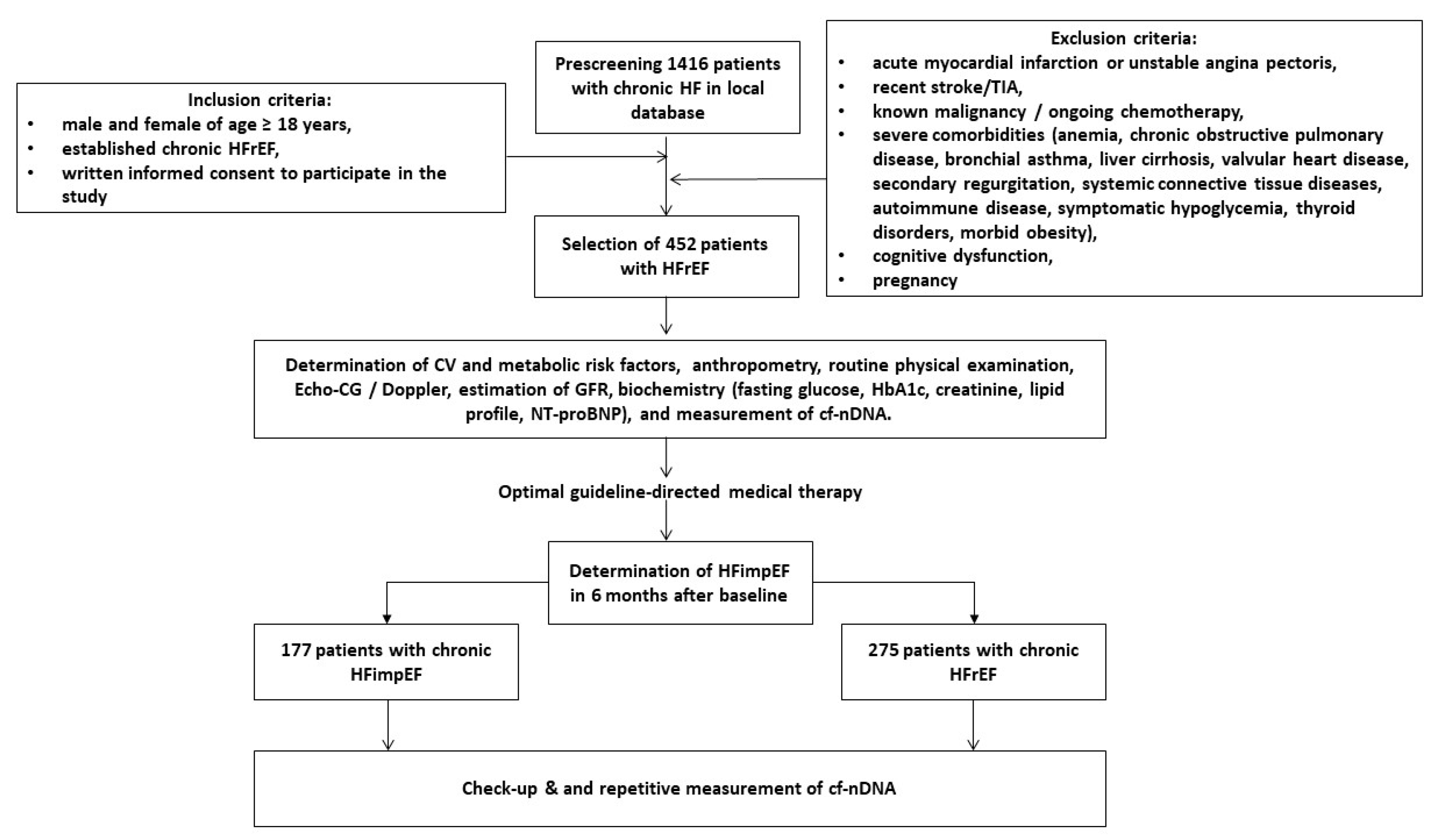
Figure 2.
Dynamic changes of circulating biomarkers during period of observation. Abbreviations: HF, heart failure; cf-nDNA, cell-free nuclear DNA; hs-CRP, high-sensitive C-reactive protein; TNF-alpha, tumor necrosis factor alpha; NT-proBNP, N-terminal brain natriuretic pro-peptide; *, a significant difference between variables at baseline and at 6 month.
Figure 2.
Dynamic changes of circulating biomarkers during period of observation. Abbreviations: HF, heart failure; cf-nDNA, cell-free nuclear DNA; hs-CRP, high-sensitive C-reactive protein; TNF-alpha, tumor necrosis factor alpha; NT-proBNP, N-terminal brain natriuretic pro-peptide; *, a significant difference between variables at baseline and at 6 month.
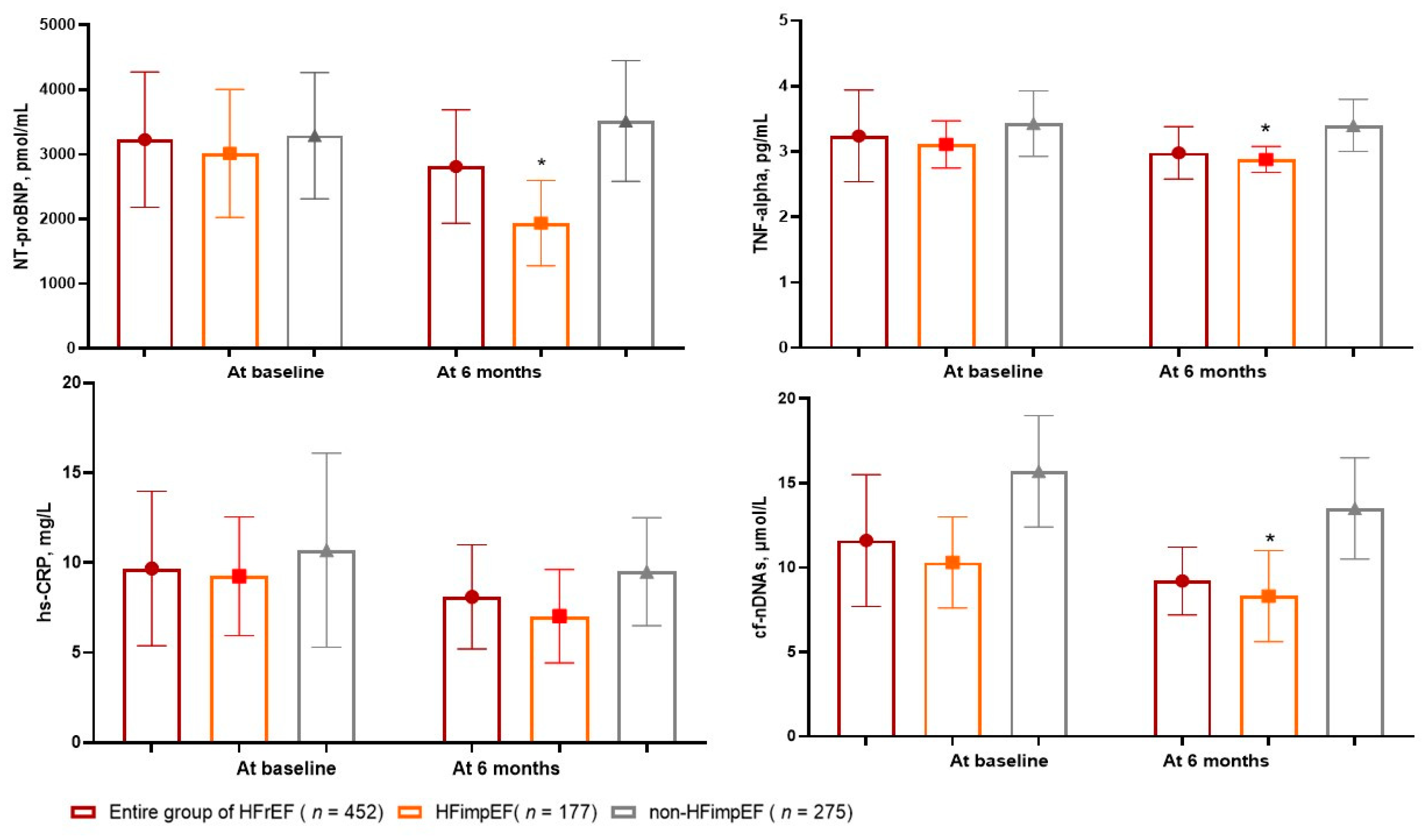
Figure 3.
Receiver operation curve analysis for HFimpEF: the well-balansed cut-off points of cf-nDNA. Abbreviations: AUC, area under curve; CI, confidence interval; LR, likelihood ratio.
Figure 3.
Receiver operation curve analysis for HFimpEF: the well-balansed cut-off points of cf-nDNA. Abbreviations: AUC, area under curve; CI, confidence interval; LR, likelihood ratio.
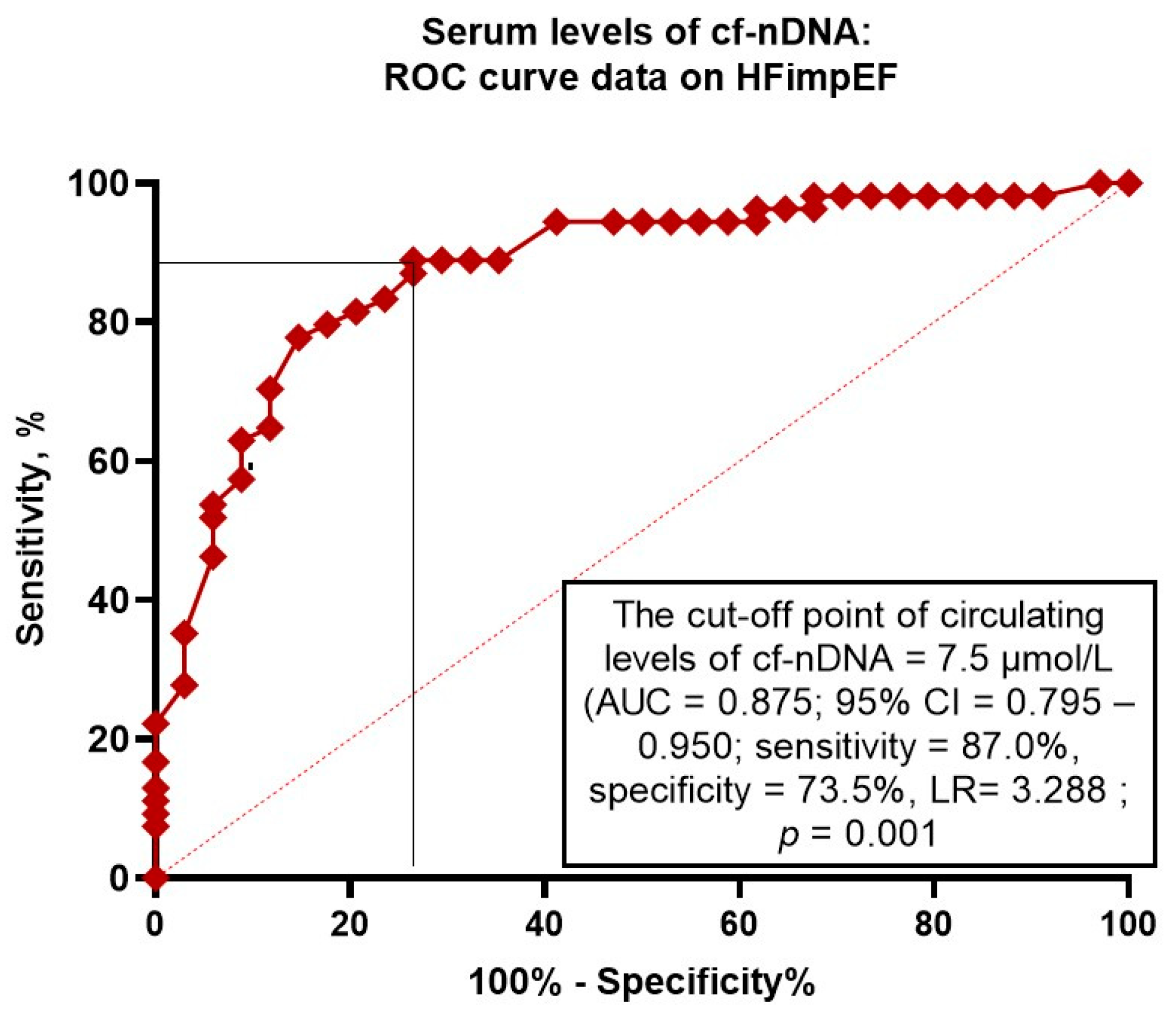

Table 1.
Baseline general characteristics of eligible T2DM patients.
| Variables | Entire patient cohort ( n = 452) |
Patients with HFimpEF ( n = 177) |
Patients with persistent HFrEF ( n = 275) |
P value |
|---|---|---|---|---|
| Demographics and anthropomorphic parameters | ||||
| Age, year | 59 (50-68) | 59 (52-65) | 60 (49-72) | 0.48 |
| Male / female n (%) | 266 (58.9) / 186 (41.2) | 102 (57.6) / 75 (42.3) | 164 (59.6) / 111 (40.4) | 0.36 |
| BMI, kg/m2 | 25.8±3.5 | 25.1±2.9 | 26.1±2.7 | 0.44 |
| Comorbidities and CV risk factors | ||||
| Dyslipidemia, n (%) | 286 (63.2) | 115 (64.5) | 171 (62.2) | 0.77 |
| Hypertension, n (%) | 71 (15.7) | 28 (15.8) | 43 (15.6) | 0.88 |
| Ischemia-induced cardiomyopathy, n (%) | 141 (31.2) | 44 (24.9) | 97 (35.3) | 0.04 |
| Dilated cardiomyopathy, n (%) | 68 (15.0) | 21 (11.9) | 47 (17.1) | 0.52 |
| AF, n (%) | 137 (30.3) | 47 (26.6) | 90 (32.7) | 0.28 |
| Smoking, n (%) | 168 (37.2) | 65 (36.7) | 103 (37.5) | 0.88 |
| Abdominal obesity, n (%) | 112 (24.8) | 46 (26.0) | 66 (24.0) | 0.87 |
| T2DM, n (%) | 146 (32.3) | 54 (30.5) | 92 (33.5) | 0.26 |
| LVH, n (%) | 316 (69.9) | 120 (67.8) | 196 (71.3) | 0.44 |
| CKD 1-3 grades, n (%) | 132 (29.2) | 45 (25.4) | 87 (31.6) | 0.42 |
| Complete LBBB / RBBB on ECG, n (%) | 98 (21.7) | 35 (19.8) | 63 (22.9) | 0.18 |
| NYHA functional classification | ||||
| I/II HF NYHA class, n (%) | 144 (31.9) | 71 (40.1) | 73 (26.6) | 0.001 |
| III HF NYHA class, n (%) | 230 (50.8) | 85 (48.0) | 145 (52.7) | 0.06 |
| IV HF NYHA class, n (%) | 78 (17.3) | 21 (11.9) | 57 (20.7) | 0.036 |
| Hemodynamics performances | ||||
| SBP, mm Hg | 128±11 | 129±9 | 125±10 | 0.22 |
| DBP, mm Hg | 78±10 | 77±8 | 74±9 | 0.64 |
| LVEDV, mL | 171 (149-192) | 168 (136-188) | 181 (150-202) | 0.04 |
| LVESV, mL | 115 (89-127) | 109 (87-124) | 126 (90-131) | 0.01 |
| LVEF, % | 32 (29-39) | 35 (31-39) | 30 (27-34) | 0.02 |
| LVMMI, g/m2 | 226±15 | 218±15 | 234±13 | 0.46 |
| LAVI, mL/m2 | 46 (39-52) | 44 (35-51) | 47 (39-54) | 0.12 |
| E/e`, unit | 17.3±5.4 | 16.6±4.1 | 19.1±3.3 | 0.56 |
| Biochemistry parameters | ||||
| eGFR, mL/min/1.73 m2 | 72 ± 11 | 80 ± 9 | 65 ± 7 | 0.04 |
| Fasting glucose, mmol/L | 5.11 ± 0.77 | 5.06 ± 0.60 | 5.19 ± 1.1 | 0.66 |
| Creatinine, µmol/L | 99.6±12.8 | 78.9±9.1 | 115.2±8.2 | 0.04 |
| TC, mmol/L | 5.88±0.90 | 5.61±0.52 | 5.92±0.70 | 0.62 |
| HDL-C, mmol/L | 0.97±0.14 | 0.97±0.15 | 0.98±0.18 | 0.68 |
| LDL-C, mmol/L | 3.93±0.18 | 3.80±0.17 | 4.00±0.12 | 0.02 |
| TG, mmol/L | 1.98±0.17 | 1.90±0.12 | 2.03±0.15 | 0.64 |
| hs-CRP, mg/L | 9.68 (4.31 – 13.70) | 9.25 (3.45 – 12.70) | 10.70 (5.80 – 17.50) | 0.22 |
| TNF-alpha, pg/mL | 3.24 (2.70–3.98) | 3.11 (2.62–3.69) | 3.43 (2.95–4.12) | 0.04 |
| NT-proBNP, pmol/mL | 3228 (1910 – 5215) | 3015 (1780 – 5220) | 3290 (1820 – 5470) | 0.44 |
| cf-nDNA, μmol/L | 11.6 (7.68 - 15.7) | 9.8 (7.2 – 12.2) | 14.1 (11.8 – 16.5) | 0.02 |
| Concomitant medications | ||||
| ACEI, n (%) | 198 (43.8) | 79 (44.6) | 119 (43.3) | 0.88 |
| ARNI, n (%) | 134 (29.6) | 53 (29.9) | 81 (29.5) | 0.90 |
| ARB, n (%) | 86 (19.0) | 35 (19.7) | 51 (18.5) | 0.82 |
| Ivabradine, n (%) | 78 (17.3) | 28 (15.8) | 50 (18.2) | 0.56 |
| Calcium channel blocker, n (%) | 67 (14.8) | 23 (13.0) | 44 (16.0) | 0.44 |
| MRA, n (%) | 405 (89.6) | 161 (91.0) | 244 (88.7) | 0.86 |
| Digoxin, n (%) | 51 (11.3) | 14 (7.9) | 37 (13.5) | 0.010 |
| Loop diuretic, n (%) | 412 (91.2) | 159 (89.8) | 253 (92.0) | 0.46 |
| Antiplatelet, n (%) | 141 (31.2) | 54 (30.5) | 87 (31.6) | 0.84 |
| Anticoagulants, n (%) | 139 (30.8) | 55 (31.1) | 84 (30.5) | 0.82 |
| Metformin, n (%) | 138 (30.5) | 54 (30.5) | 84 (31.0) | 0.86 |
| SGLT2 inhibitors, n (%) | 434 (96.0) | 175 (98.9) | 259 (94.2) | 0.86 |
| Statins, n (%) | 350 (77.4) | 139 (78.5) | 211 (76.7) | 0.88 |
Notes: data of variables are given mean ± SD and median (25%-75% interquartile range); P value, a difference between patient cohorts. Abbreviations: ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin-II receptor blockers; ARNI, angiotensin receptor neprilysin inhibitor; CKD, chronic kidney disease; BMI, body mass index; DBP, diastolic blood pressure; E/e`, early diastolic blood filling to longitudinal strain ratio; GFR, glomerular filtration rate; HDL-C, high-density lipoprotein cholesterol; hs-CRP, high-sensitivity C-reactive protein; LVEDV, left ventricular end-diastolic volume; LVESV, left ventricular end-systolic volume; LVEF, left ventricular ejection fraction; LVMMI, left ventricle myocardial mass index, left atrial volume index, LAVI; left atrial volume index; LDL-C, low-density lipoprotein cholesterol; LBBB, left bundle branch block; LVH, left ventricular hypertrophy; RBBB, right bundle branch block; MRA, mineralocorticoid receptor antagonist; NT-proBNP, N-terminal brain natriuretic pro-peptide; SBP, systolic blood pressure; SGLT2, sodium glucose linked transporter 2; TG, triglycerides; TC, total cholesterol; T2DM, type 2 diabetes mellitus.
Table 2.
Predictors for HFimpEF in study population. The results of the univariate and multivariate logistic regression analysis.
Table 2.
Predictors for HFimpEF in study population. The results of the univariate and multivariate logistic regression analysis.
| Dependent variable: HFimpEF | ||||
| Variables | Univariate logistic regression | Multivariate logistic regression | ||
| OR (95% CI) | P-value | OR (95% CI) | P-value | |
| Rough regression models | ||||
| Ischemia-induced cardiomyopathy (presence vs. absent) | 0.75 (0.62-0.88) | 0.044 | 0.77 (0.60-0.90) | 0.042 |
| IV HF NYHA class | 0.71 (0.57-0.92) | 0.001 | 0.76 (0.63-0.87) | 0.001 |
| T2DM (presence vs. absent) | 0.77 (0.71-0.82) | 0.040 | 0.84 (0.62-0.92) | 0.042 |
| CKD (presence vs. absent) | 0.89 (0.84-0.96) | 0.048 | 0.88 (0.80-0.10) | 0.050 |
| AF (presence vs. absent) | 0.94 (0.80-1.09) | 0.064 | - | |
| LVEDV | 0.93 (0.90-1.01) | 0.052 | - | |
| LAVI | 0.95 (0.92-0.98) | 0.042 | 0.96 (0.90-1.00) | 0.050 |
| E/e` | 0.92 (0.89-0.97) | 0.080 | - | |
| NT-proBNP (≤1940 pmol/mL vs. >1940 pmol/mL) | 1.42 (1.19-1.98) | 0.001 | 1.35 (1.12-1.76) | 0.001 |
| Relative decrease in NT-proBNP levels (>35% vs. ≤35%) from baseline | 1.67 (1.51-1.82) | 0.001 | 1.70 (1.61-1.83) | 0.001 |
| TNF-alpha (≤2.88 pg/mL vs. >2.88 pg/mL) | 1.06 (1.00-1.12) | 0.48 | - | |
| hs-CRP (≤7.02 mg/L vs. >7.02 mg/L) | 1.08 (1.00-1.17) | 0.60 | - | |
| cf-nDNA (≤7.5 μmol/L vs. >7.5 μmol/L) | 1.56 (1.07-2.94) | 0.001 | 1.64 (1.10-2.07) | 0.001 |
| Digoxin (presence vs. absent) | 0.85 (0.72-0.97) | 0.042 | 0.93 (0.86-1.00) | 0.052 |
| Adjustment to ischemia-induced cardiomyopathy, IV HF NYHA class, and digoxin use | ||||
| T2DM (presence vs. absent) | 0.84 (0.76-0.95) | 0.040 | 0.88 (0.74-1.01) | 0.12 |
| CKD (presence vs. absent) | 0.94 (0.90-1.02) | 0.46 | - | |
| AF (presence vs. absent) | 0.92 (0.80-1.12) | 0.52 | - | |
| LVEDV | 0.98 (0.92-1.14) | 0.66 | - | |
| LAVI | 0.97 (0.91-1.05) | 0.52 | - | |
| E/e` | 0.92 (0.84-1.03) | 0.14 | - | |
| NT-proBNP (≤1940 pmol/mL vs. >1940 pmol/mL) | 1.55 (1.23-2.06) | 0.001 | 1.43 (1.21-1.88) | 0.001 |
| Relative decrease in NT-proBNP levels (>35% vs. ≤35%) from baseline | 1.63 (1.53-0.74) | 0.001 | 1.52 (1.38-0.69) | 0.001 |
| TNF-alpha (≤2.88 pg/mL vs. >2.88 pg/mL) | 1.03 (1.00-1.07) | 0.56 | - | |
| hs-CRP (≤7.02 mg/L vs. >7.02 mg/L) | 1.06 (1.00-1.12) | 0.66 | - | |
| cf-nDNA (≤7.5 μmol/L vs. >7.5 μmol/L) | 1.64 (1.10-2.33) | 0.001 | 1.64 (1.19-2.15) | 0.001 |
Abbreviations: AF, atrial fibrillation; OR, odds ratio; CI, confidence interval; cf-nDNA, cell-free nuclear DNA; E/e`, early diastolic blood filling to longitudinal strain ratio; LVEF, left ventricular ejection fraction; hs-CRP, high-sensitive C-reactive protein; LAVI; left atrial volume index; LVEDV, left ventricular end-diastolic volume; NT-proBNP, N-terminal brain natriuretic pro-peptide; HFimpEF, heart failure with improved ejection fraction; NYHA, New York Hear Association; TNF-alpha, tumor necrosis factor-alpha.
Table 3.
The comparisons of NT-proBNP, its respective decrease and cf-nDNA discriminative potencies for HFimpEF.
Table 3.
The comparisons of NT-proBNP, its respective decrease and cf-nDNA discriminative potencies for HFimpEF.
| Predictive models | AUC | NRI | IDI | |||
| M (95% CI) | P-value | M (95% CI) | P-value | M (95% CI) | P-value | |
| Model 1 (NT-proBNP ≤1940 pmol/mL) | 0.783 (0.700–0.840) | - | Reference | - | Reference | - |
| Model 2 (relative decrease in NT-proBNP levels ≤35% from baseline) | 0.795 (0.745–0.861) | 0.06 | 0.23 (0.17–0.30) | 0.170 | 0.21 (0.18–0.25) | 0.240 |
| Model 3 (cf-nDNA ≤7.5 μmol/L) | 0.875 (0.795–0.950) | 0.001 | 0.54 (0.43–0.67) | 0.001 | 0.51 (0.45–0.58) | 0.001 |
| Model 4 (NT-proBNP levels ≤1940 pmol/mL + cf-nDNA) | 0.872 (0.820–0.941) | 0.001 | 0.48 (0.42–0.55) | 0.001 | 0.49 (0.41–0.56) | 0.001 |
| Model 5 (relative decrease in NT-proBNP levels ≤35% from baseline + cf-nDNA) | 0.893 (0.844–0.962) | 0.001 | 0.58 (0.45–0.72) | 0.001 | 0.55 (0.49–0.62) | 0.001 |
Note: P value estimated in comparison with Reference model (NT-proBNP). Abbreviations: AUC, area under curve; NT-proBNP, N-terminal brain natriuretic pro-peptide; cf-nDNA, cell-free nuclear DNA; CI, confidence interval; M, median; IDI, integrated discrimination indices; NRI, net reclassification improvement.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



