Submitted:
28 August 2024
Posted:
29 August 2024
You are already at the latest version
Abstract
Lupus, also known as systemic lupus erythematosus (SLE), is a chronic autoimmune disease that can lead to inflammation and damage to multiple organs and tissues in the body. The symptoms vary from patient to patient, which makes the disease manifest very differently, resulting in difficulty in diagnosing and treating patients. Some may experience fatigue, hair loss, joint pain, and more. In the past, a general approach of blanket immunosuppression was commonly used to treat lupus. These immunosuppressive drugs would broadly target the immune system and focus on reducing symptoms. However, recent research has shown that selective immunotherapies such as monoclonal antibodies (anifrolumab and belimumab) which target specific components of the immune system are more effective in managing lupus because of their ability to reach specific cells in the immune system rather than easing symptoms. Anifrolumab blocks the activity of type I interferons, while belimumab neutralizes BLyS to reduce the production of autoantibodies, the root cause of SLE.¹⁻² This paper will introduce the immunology of the disease, explore how the more traditional approach of blanket immunosuppressive drugs work compared to the newer selective immunotherapies, and review the results from the clinical trials of anifrolumab and belimumab.
Keywords:
Lupus
; Systemic Lupus Erythematosus Treatment
; Selective Immunotherapies
; Anifrolumab
; Belimumab
Introduction
Lupus is a chronic autoimmune disease that causes inflammation and damage to various organs and tissues in the body. There are four different subtypes of lupus: systemic lupus erythematosus (SLE), drug-induced lupus, cutaneous lupus, and neonatal lupus. SLE is characterized by the production of autoantibodies, proteins formed by plasma cells that specifically respond to self-antigens. In a healthy immune system, antibodies are formed in response to a foreign antigen such as a pathogen in an attempt to target and remove the pathogen. In an autoimmune disease, our immune system has mistaken our own tissues as a foreign antigen which leads to autoantibodies being generated to attack our own bodies (Figure 1).¹ As the two main white blood cell types of the adaptive immune system, B and T cells work together to protect the body from foreign pathogens. T-cells eliminate cancerous or infected cells directly, while B-cells develop into plasma cells and produce antibodies. Other immune cells produce signaling molecules such as interferon-gamma (IFNg) and B-cell lymphocyte stimulator (BLyS) which bind to B and T-cell receptors acting as inflammatory mediators. Type I interferons activate T-cells or natural killer cells which can directly kill our tissues and help activate B-cells to produce autoantibodies. BLyS binds to B-cells and promotes cell survival. When these two molecules are in excess, autoantibodies are produced, targeting specific components of the cell nucleus, creating inflammation and damage within tissues and organs.²⁻³ This occurs when cells undergo a cell death process called necrosis, in which the mitochondria and cytoplasm swell up in the presence of packaged DNA in response to uncontrolled external factors such as autoantibodies, leading to SLE.²
As a result of multiple anti-nuclear antibodies broadly targeting DNA, patients often experience a wide range of symptoms including fatigue, hair loss, and joint pain. Due to the broad nature of symptoms, lupus may be mistaken for other autoimmune diseases, making accurate diagnosis difficult. Moreover, a lack of understanding around the cause(s) of lupus has hindered development of novel treatments. In the past, a more general approach of prescribing broadly immunosuppressive drugs has been employed to manage disease. These blanketed agents work by targeting the symptoms and suppressing the immune system as a whole. Indeed, these drugs, such as non-steroidal anti-inflammatory drugs (NSAIDs), are commonly used in various medical conditions where an overactive immune system can cause harm.⁴⁻⁵
The increase in the understanding of lupus has allowed for more efficient treatment options. A new approach of selective immunotherapies such as monoclonal antibodies (mAbs) that specifically target certain parts of the immune system are proving to be more successful in treating lupus in the long term than the broadly suppressive drugs like NSAIDs.⁶⁻⁸ Recent clinical trials on anifrolumab and belimumab have shown a considerable improvement in SRI response (the decrease in the rate of SLE) when compared to standard therapy which consists of a blanket approach.⁶⁻⁷ This is due to their selective nature of earmarking specific cells and molecules that are increasing autoimmunity. The two main focuses of these drugs are: type I interferons, to which anifrolumab corresponds, and B-cell lymphocyte stimulator, which belimumab neutralizes. Limiting these molecules decreases the production of autoantibodies and activated T cells, therefore decreasing lupus activity.⁶⁻⁷
The Deficiencies of the Blanket Immunosuppressive Drugs:
Prior to 2011, all FDA-approved drugs for the treatment of lupus did not include a selective approach that focuses on improving the activity of the immune system in the long term.⁹ Unfortunately, the majority of drug development for lupus has been focused on the blanket approach method. These standard therapies known as blanket immunosuppressive drugs are a common treatment approach for managing lupus symptoms that includes the use of corticosteroids and/or antimalarial therapy.⁹ Also known as steroids, corticosteroids aim to reduce inflammation by mimicking the function of cortisol, a hormone naturally produced by the adrenal glands.¹⁰ This therapy reduces the production of cytokines and adhesion molecules that cause inflammation through deactivating inflammatory genes.¹⁰⁻¹¹ Today, nearly 88% of patients with SLE are treated with these therapies, making corticosteroids a popular form of prescription drug for lupus.¹¹ These drugs share similarities with NSAIDS such as ibuprofen and naproxen which work by suppressing the immune system's response, thereby easing general symptoms such as inflammation and joint pain. They are often supplied as tablets in over the counter and prescription form, providing short term relief from symptoms such as joint pain and fever. While naproxen provides longer lasting pain relief with fewer doses, ibuprofen requires more doses to work to its full efficacy. Ultimately, both medications work similarly and thus share similar side effects such as stomach upset, nausea, and dizziness.⁴⁻⁵ NSAIDs function to relieve pain by blocking cyclooxygenase (COX), which is an enzyme that produces prostaglandins.⁴ As a result, the prostaglandin production is reduced, which alleviates pain and inflammation. Despite their initial effectiveness, blanket immunosuppressive drugs have limitations when it comes to the long-term management of lupus. One of the key drawbacks of them is their lack of specificity in targeting the underlying causes of lupus. Although the COX enzyme is blocked, specific components of the immune system must be targeted to properly treat lupus.
Moving Beyond Blanket Approaches: Advancements in Lupus Treatments Targeting the Immune System
Recent studies have found that selective, targeted immunotherapies that modulate specific components of the immune system are more effective in treating lupus. Monoclonal antibodies are lab-generated proteins engineered to mimic the antibodies created by our own immune system, targeting single molecules or cells. They are commonly used in conditions such as cancer, covid-19, osteoporosis, etc. ⁸ Monoclonal antibodies such as Belimumab and Anifromulab have shown greater long-term effectiveness in managing lupus compared to blanket immunosuppressive drugs. Both Phase 3 and 4 clinical trials of selective immunotherapies, such as anifrolumab and belimumab, have been effective examples of these agents.⁶⁻⁷ Their efficacy lies in their ability to target and suppress precise molecules of the immune system. The binding affinity, or strength of the bond between antibody and antigen-binding, enables pharmaceutical chemists to modify antibodies to bind to a specific target, such as a lupus threatening antigen. This ensures that necessary cells or molecules are targeted.
- Anifrolumab
Anifrolumab is a monoclonal
Anifrolumab (Saphnelo), was first developed by the global biopharmaceutical company AstraZeneca to treat SLE. Anifrolumab works by blocking the activity of type I interferons (IFNs).¹²⁻¹³ In SLE, type I IFNs are produced by antigen-presenting cells (APCs), a group of immune cells in which antigens are processed and presented to T and B-cells. An increase in the exposure of inflammatory signaling molecules such as type I IFNs causes the T and B-cells to produce autoantibodies. These self-acting antibodies disrupt the homeostasis of the immune system, ultimately causing autoimmunity.¹
antibody that targets the type I interferon receptor which consists of two transmembrane proteins: IFNAR1 and IFNAR2. The success of the drug is linked to the blocking of type I interferons. Because type I interferons are cytokines involved in inflammatory pathways, the targeting of them is successful in treating lupus because they are specific to the development of inflammation, rather than the overall symptom of inflammation. Given in the form of an injection, the anifrolumab antibody binds to IFNAR1 of the receptor, blocking the activity of all type I interferons, including IFN-alpha, IFN-beta, and IFN-omega (Figure 2).¹ Although this antibody is relatively new, there has been successful trials that show its effectiveness. A randomized placebo controlled Phase III extension trial among two different studies aimed to test the long-term safety and tolerability of Anifrolumab in active SLE. Patients were given a 300mg dose of anifrolumab, which was compared to a group given the placebo drug.⁷ The SLE Disease Activity Index (SLEDAI), a system used to measure disease activity by weighing symptoms based on their severity, was used in this study. The rates from both studies were adjusted to accurately reflect the results of the scores measuring the severity of the SLE which were 8.5 with anifrolumab, while 11.2 with placebo.⁷ The combined anifrolumab 300mg group showed significant improvement in the severity scores compared to the placebo control group. Patients who were given anifrolumab had a decrease in severity from 11.4 ± 3.8, to 5.1 ± 3.5. Meanwhile, patients given placebo only decreased to 6.0 ± 4.1.⁷ This decrease in severity accounted for the decrease in symptoms such as overactive immune flare-ups. The average flare-up rate for the combined anifrolumab group was 10%, while the placebo group had a rate of 20%.⁷ This data demonstrates that the medication is aligned with a lower cumulative patient use of glucocorticoid, a common blanket immunosuppressive drug. Overall, this suggests a long-term effectiveness of anifromulab in SLE.
Belimumab
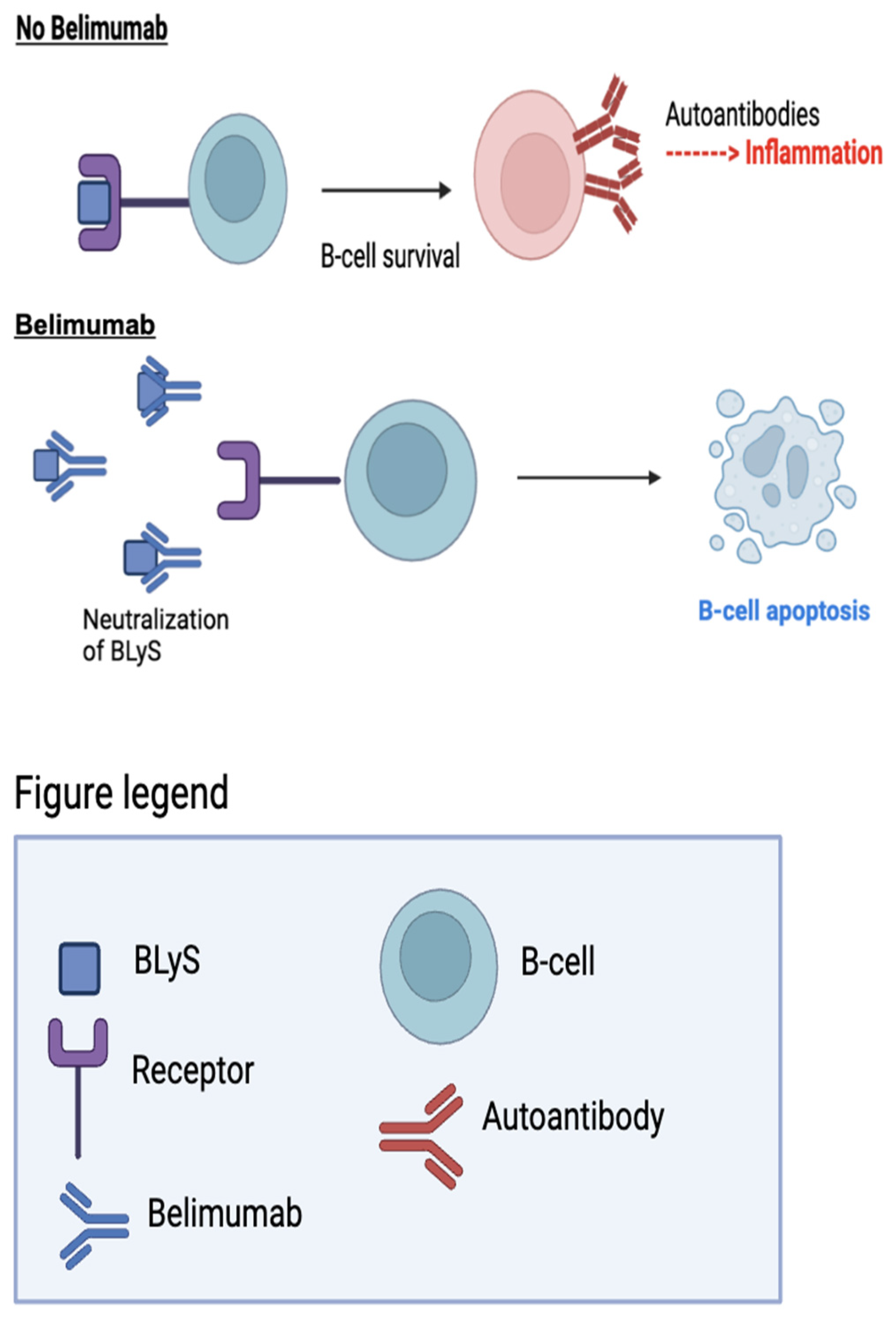
Belimumab (Benlysta) was developed to address humoral immunodeficiencies caused by failed B-cell development.² BLyS consists of ligands and receptors that act as checkpoints to regulate antibody production by B-cells. In the absence of BLyS, naive B-cells fail to develop and mature into plasma cells, which produce antibodies.¹⁴ The targeting of BLyS is necessary for treating autoimmune diseases because BLyS binds to autoreactive B-cells, promoting B-cell survival and the production of autoantibodies. This can cause inflammation and lead to autoimmune diseases like SLE.¹⁴
Belimumab neutralizes BLyS by binding to it before it reaches the B-cell, leading to cell apoptosis and the prevention of potential autoantibodies (Figure 3).¹⁴ In 2011, Belimumab gained FDA approval for its effectiveness in SLE in correspondence to its successful results in lupus patients.² In a randomized, controlled Phase III trial, the safety and efficacy of belimumab in addition to standard therapy was assessed against standard therapy alone in patients with SLE.⁶ The study randomized patients into groups receiving either 1 mg/kg or 10 mg/kg of belimumab, or the placebo control, in addition to standard therapy. The results demonstrated that patients receiving 10 mg/kg of belimumab, in combination with standard therapy, experienced the greatest improvement, with a 43% SRI response rate at week 52, compared to a 33.5% rate for the placebo.⁶ The group receiving 1 mg/kg of Belimumab plus standard therapy achieved a response rate of 40.6%. These findings highlight the superior effectiveness of belimumab compared to broad immunosuppressive drugs in treating SLE. Additionally, the use of belimumab resulted in a reduction in flare-up rates, with a decrease of 0.13% for patients receiving 10 mg/kg and 0.023% for those receiving 1 mg/kg.⁶ Overall, belimumab at 10 mg/kg in combination with standard therapy, demonstrated a favorable response, improving SRI response rate, reducing disease activity, and demonstrating tolerability in patients with SLE.
Conclusion
As a newly researched disease, lupus is often misunderstood by doctors and scientists in regards to diagnosis and treatment, which is why there must be continuous efforts to find new treatments and enhance care for all SLE patients. The discussed clinical trials of anifrolumab and belimumab demonstrate that selective immunotherapies, such as monoclonal antibodies, have greater long-term effectiveness in managing lupus when compared to the use of corticosteroids and antimalarial treatment in blanket immunosuppressive drugs. The success of anifrolumab and belimumab in treating lupus is linked to their targeting of specific molecules of the immune system to prevent further development of the disease. To limit further autoantibody production, the anifrolumab antibody binds to type I IFNs and belimumab targets BLyS. In the anifrolumab study, patients who were given anifrolumab had a significant decrease in severity rates while patients given placebo did not experience a substantial change.⁷ In the belimumab study, those who were receiving 10 mg/kg of belimumab, in combination with standard therapy, experienced the greatest improvement, with a larger overall SRI response rate at week compared to the placebo drug.⁶ These results conclude that blanket immunosuppressive drugs are not as effective in treating the activity of lupus compared to selective monoclonal antibodies. In actuality, there have been reports of adverse events with corticosteroids. A wide range of patients treated with corticosteroids experienced irreversible organ damage.¹¹ While it has been proven that monoclonal antibodies therapies are effective in treating SLE, there have been a minute but notable amount of patients that have experienced adverse events. In a double-blind Phase 4 trial of belimumab aiming to test the long term effectiveness of patients with SLE, 10 patients in the belimumab group died versus 8 patients in the placebo group.¹⁵ In addition, a higher quantity of patients in the belimumab group had infusion and hypersensitivity reactions.¹⁵ While selective immunotherapies have shown efficacy in treating lupus, it must be taken into account these treatments are not suitable for everyone. The current SRI response rates to these therapies range from 50–60%, indicating the need for ongoing research and development of better treatment options.¹⁶ Continued efforts to understand and address the complexities of lupus will ultimately lead to improved care and outcomes for patients with SLE.
References
- Ivashkiv et. al, L. B. (2015, January 1). Regulation of type I interferon responses. National Library of Medicine. Retrieved June 3, 2024, from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4084561/#:~:text=Type%20I%20IFNs%20can%20also,diseases%20such%20as%20multiple%20sclerosis.
- Stohl, W., & Hilbert, D. M. (2012, January 9). The discovery and development of belimumab: the anti-BLyS–lupus connection. National Library of Medicine. Retrieved June 3, 2024, from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3264947/.
- Tau et. al, G. (1999, December). Biologic Functions of the IFN-γ Receptors. National Library of Medicine. Retrieved June 12, 2024, from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4154595/#:~:text=IFN%E2%80%90%CE%B3%20is%20primarily%20secreted,%2C%20regulate%20Th1%2FTh2%20balance%2C.
- Medications - non-steroidal anti-inflammatory drugs. (n.d.). https://www.betterhealth.vic.gov.au/health/conditionsandtreatments/medications-non-steroidal-anti-inflammatory-drugs. Retrieved June 3, 2024.
- Medications used to treat lupus. (n.d.). Lupus Foundation of America. Retrieved June 3, 2024, from https://www.lupus.org/resources/medications-used-to-treat-lupus.
- Furie, R. (2011, August 30). A phase III, randomized, placebo-controlled study of belimumab, a monoclonal antibody that inhibits B lymphocyte stimulator, in patients with systemic lupus erythematosus†. Wiley. Retrieved June 3, 2024, from https://onlinelibrary.wiley.com/doi/ftr/10.1002/art.30613.
- Kalunian et. al, K. C. (2022, November 11). [A Randomized, Placebo-Controlled Phase III Extension Trial of the Long-Term Safety and Tolerability of Anifrolumab in Active Systemic Lupus Erythematosus]. American College of Rheumatology. https://acrjournals.onlinelibrary.wiley.com/doi/10.1002/art.42392.
- Robak et. al, E. (2011, January 10). Monoclonal antibodies in the treatment of systemic lupus erythematosus. National Library of Medicine. Retrieved June 3, 2024, from https://pubmed.ncbi.nlm.nih.gov/19149533/.
- Dennis, G. J. (2011, November 30). Belimumab: A blys-specific inhibitor for the treatment of systemic lupus erythematosus. Clinical Pharmacology & Therapeutics, 91(1), 143-149. [CrossRef]
- Corticosteroids. (2020, January 20). Cleveland Clinic. Retrieved June 17, 2024, from https://my.clevelandclinic.org/health/drugs/4812-corticosteroids.
- Katarzyna et. al, P.-B. (2023, May 12). Current treatment of systemic lupus erythematosus: a clinician's perspective. Springer Link. Retrieved June 17, 2024, from https://link.springer.com/article/10.1007/s00296-023-05306-5.
- Kemp, A. (2021, August 2). Saphnelo (anifrolumab) approved in the US for moderate to severe systemic lupus erythematosus. AstraZeneca. Retrieved June 3, 2024, from https://www.astrazeneca.com/media-centre/press-releases/2021/saphnelo-approved-in-the-us-for-sle.html#.
- Deeks, E. D. (2021, October). Anifrolumab: First Approval. Retrieved June 3, 2024, from https://pubmed.ncbi.nlm.nih.gov/34554438/.
- Cancro, M. P. (2009, May). The role of B lymphocyte stimulator (BLyS) in systemic lupus erythematosus. National Library of Medicine. Retrieved June 3, 2024, from https://pubmed.ncbi.nlm.nih.gov/19411764/.
- Sheikh MD, S. Z. Z. (2021, February). Mortality and adverse events of special interest with intravenous belimumab for adults with active, autoantibody-positive systemic lupus erythematosus (BASE): a multicentre, double-blind, randomised, placebo-controlled, phase 4 trial. ScienceDirect. Retrieved June 3, 2024, from https://www.sciencedirect.com/science/article/abs/pii/S2665991320303556.
- Khalili et. al, L. (2023, September 27). Lupus clinical trials and the promise of future therapies. National Library of Medicine. Retrieved June 17, 2024, from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10538598/#j_rir-2023-0018_ref_007.
Figure 1.
In a healthy immune system, antibodies fight foreign antigens. Cytotoxic T cells, a type of T cell that destroys virus infected cells kills foreign antigens. In an autoimmune diseases, B cells produce autoantibodies which attack self antigens and T cells directly destroy self antigens.
Figure 1.
In a healthy immune system, antibodies fight foreign antigens. Cytotoxic T cells, a type of T cell that destroys virus infected cells kills foreign antigens. In an autoimmune diseases, B cells produce autoantibodies which attack self antigens and T cells directly destroy self antigens.
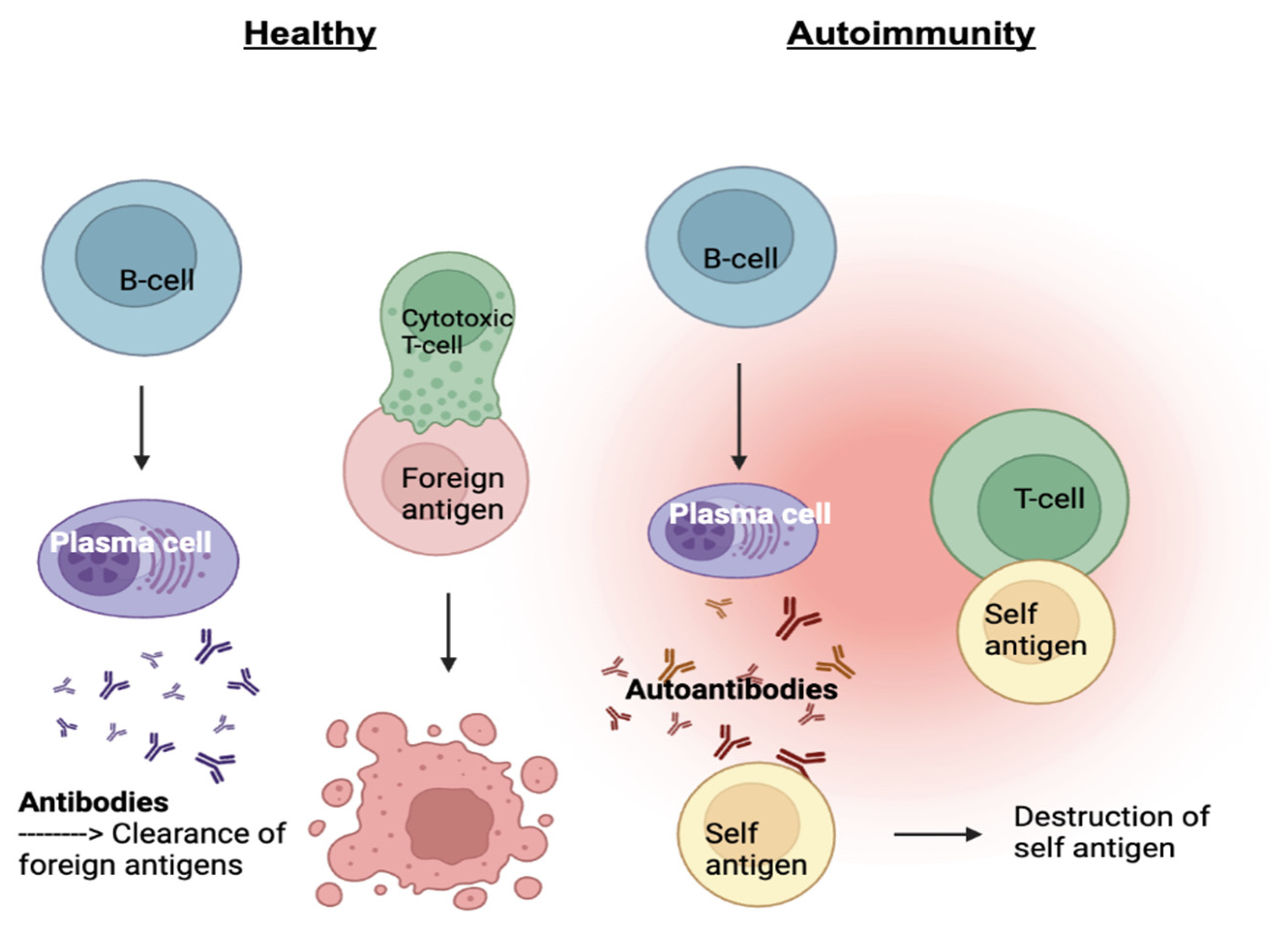
Figure 2.
In the absence of anifrolumab, type I IFNs to bind to IFNAR 1 and 2, creating inflammation. In the presence of the mAb, anifrolumab blocks type I IFNs preventing potential inflammation.
Figure 2.
In the absence of anifrolumab, type I IFNs to bind to IFNAR 1 and 2, creating inflammation. In the presence of the mAb, anifrolumab blocks type I IFNs preventing potential inflammation.
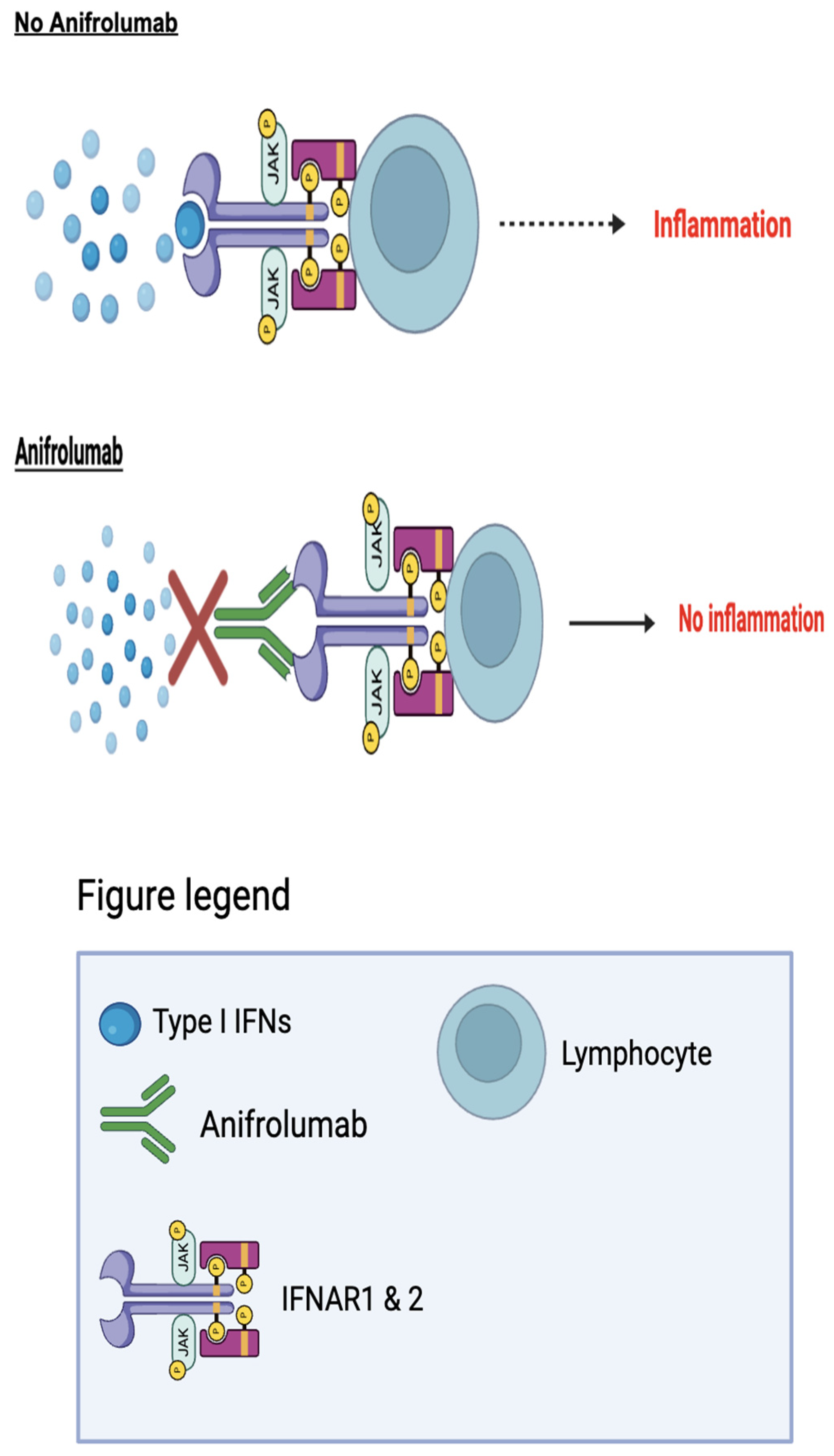
Figure 3.
In the absence of belimumab, BLyS binds to the B cell receptor, allowing the B-cell to survive and produce autoantibodies. When belimumab is in action, it will block BLyS, causing B-cell apoptosis.
Figure 3.
In the absence of belimumab, BLyS binds to the B cell receptor, allowing the B-cell to survive and produce autoantibodies. When belimumab is in action, it will block BLyS, causing B-cell apoptosis.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



