
Submitted:
29 August 2024
Posted:
29 August 2024
Read the latest preprint version here
Abstract
Background/Objectives: This study aimed to evaluate compliance and accuracy in comparison with traditional PD diaries for tracking motor symptoms using a new smartphone application (My Parkinson’s) and paper diary strategies. Parkinson's disease (PD) is a neurodegenerative disorder with progressive motor symptoms. Treatment becomes more challenging as PD progresses, motor complications in the form of wearing-off phenomenon and levodopa-induced dyskinesia develop. Traditional paper diaries and clinical scales used to evaluate patients may be inadequate in assessing whether the patient is “on” or “off,” resulting in less-than-ideal treatment changes. Methods: A randomized crossover design was utilized to examine 22 advanced PD patients who underwent symptomatic assessment with both diaries during two separate 24-hour periods seven days apart. The compliance and accuracy of data were assessed by comparing diary entries with the clinical examination notes and WhatsApp queries. Latterly, patients' diary preferences were also evaluated.; Results: The digital diary had significantly better compliance and accuracy than the paper diaries, with substantial/almost perfect levels of agreement (κ = 0·615 to 0·818) between logged symptoms and clinical examination notes. 65% of patients preferred the digital diary for follow-ups, and there was no significant difference in ease of use compared to paper diaries. Conclusions: Digital diaries are helpful in the clinical management of PD patients as they minimize recall bias and reduce data errors in appropriately selected patients. Our study suggests a broader adoption of digital health technologies in PD management. Still, additional research is necessary to improve the tools and assess long-term patient outcomes.
Keywords:
Parkinson’s Disease
; Mobile Applications
; Parkinson’s disease digital diary
1. Introduction
Parkinson’s disease (PD) is the second most common neurodegenerative disorder in the elderly, affecting approximately 10 million individuals globally[1]. It is characterized by a progressive loss of dopaminergic neurons in the substantia nigra, leading to a range of motor symptoms, such as bradykinesia, rigidity, rest tremor, and postural instability. In addition, patients often experience non-motor symptoms, including sleep disturbances, orthostatic hypotension, and cognitive decline[2]. Above all the dopaminergic treatments, Levodopa remains the cornerstone of PD treatment, effectively managing motor symptoms in the early stages of the disease [3]. However, as PD progresses, patients frequently encounter motor fluctuations, especially wearing-off and levodopa-induced dyskinesia, that complicate disease management and affect their daily living quality of life [4]. These motor fluctuations can occur at varying intervals weekly, daily, or even within the same day. However, PD symptoms are usually evaluated with anamnesis and clinical scales in clinical studies and daily practice, like a snapshot examination[5]. In this examination, patients may not recall symptoms, especially the exact time of their ‘‘on’‘ and ‘‘off’‘ periods in a limited time, potentially hindering the main problems, so the optimal treatment of the disease may not be provided. Therefore, accurate and consistent self-reporting of patient data is vital in a personalized approach to tailor treatment targeting each patient’s specific needs and adjusting medication regimens more effectively [5,6]. Several paper-based patient diaries are specifically designed for patients with PD to help them track their motor symptoms [7]. They are generally used in clinical practice for documenting patients’ motor complications or ‘‘on’‘ and ‘‘off’‘ periods within a specific time frame (e.g., hourly, every 30 min) for a day or a week in a structured manner. The most widely used paper diary for tracking motor symptoms was developed by Hauser et al.[8]. Other paper diaries for PD have also been published [9,10,11]. These diaries used to be a standard follow-up method, providing valuable insights into experiences and motor fluctuations throughout the day. Still, their reliability and accuracy are uncertain for a few reasons. Foremost, it is unclear if the paper diaries were completed on time, which could impact the results. In addition, issues like low adherence, multiple entries for the same time interval (data duplication), diary fatigue, filling in the retrospectively at once, and incomplete-missing-illegible diaries can undermine the quality of the data and potentially lead to suboptimal treatment decisions[12].
Thus, digital health technologies have introduced wireless electronic diaries (e-diaries) as a contemporary approach to monitoring PD symptoms and overcoming these challenges. Available on multiple platforms, including tablets, smartphone apps, and the web, these e-diaries have several advantages over paper diaries[13]. Among them, smartphone app e-diaries stand out as they are convenient and easy to use. In response, these digital tools improve the timeliness of data entry (with alerts prompting patients to enter answers on time) and improve the accuracy of responses[7], which ensures data quality and helps improve patient compliance and retention[12]. Although smartphone-based diaries hold promise for monitoring PD symptoms, only a few studies have been published to evaluate their use in monitoring PD symptoms. Since the adoption of these digital tools continues to develop, it becomes increasingly important to assess their utility.
This study aims to evaluate the effectiveness, compliance, accuracy, and patient preferences between traditional paper diaries and our new smartphone application (My Parkinson’s) in tracking motor symptoms in PD and evaluate the agreement between clinical examination notes and patient-reported data.
2. Materials and Methods
2.1. Study Design and Participants
This single-center, prospective, randomized cross-over study enrolled 22 patients with advanced PD from June 2022 to January 2023. The UK Parkinson’s Disease Society Brain Bank criteria were used by one[14], and all participants who met these diagnostic criteria and had motor fluctuations and dyskinesias were enrolled in the study.
The study adhered to the principles of the Helsinki Declaration and received approval from the local Institutional Review Board (Approval No. 23/24.05.2022). Written informed consent was obtained from all participants before their inclusion in the study. Inclusion criteria were as follows: a baseline Mini-Mental State Examination (MMSE) score of at least 25 to ensure sufficient cognitive function, which could interfere with the results[15]. For this study, we sought at least primary school graduates to enable comprehension of the instructions and effectively use mobile applications. In addition, Internet accessibility and smartphone use in this study were prerequisites because all motor symptom assessments of the patient were digitally monitored.
Participants had to maintain a stable antiparkinsonian medication regimen for at least one month before and during the study to remove potential confounding effects possibly related to medication changes on the study outcomes. Individuals who took medications that might have altered their parkinsonism or dyskinesias and those with major depression, psychosis, or other severe medical conditions that could affect the results were excluded from the study.
All participants’ demographic and clinical characteristics, including age, gender, education, disease duration, motor complication duration, and Levodopa equivalent daily doses (LEDD)[16], were recorded. Motor symptoms of PD were assessed using the UPDRS Part III [17]and staged according to the Hoehn and Yahr (H&Y) scale [18].
2.2. Procedures
This study uses a randomized cross-over design to investigate compliance, accuracy, and patient preferences between traditional paper diaries and the electronic diary application My Parkinson’s for tracking motor symptoms in PD.
2.3. Randomization and Group Assignment
The participants were randomly allocated into one of two groups with Random.org.[19]
Group 1:
First Phase (Phase I):
Day 1: Participants in this group were initially given a paper diary. At home, they were instructed to record their PD-related symptoms (on-off fluctuations, dyskinesia, and tremors) by self-reporting every hour over 24 hours to capture their motor fluctuations.
Day 2: First Clinic Visit The day after the 24-hour monitoring period at home, patients attended a clinic visit. During their follow-up visit, a movement disorders specialist evaluated their motor symptoms according to anamnestic data (interview in the medical routine without access to recorded diaries). We included this step to replicate the circumstance of a typical clinic evaluation, which is based on patient recall and clinician judgment.
Second Phase (Phase II):
1 Week later (Day 7-Cross-over): Following a 1-week washout period to mediate any effects due to carry-over from Phase I, the PD patients were introduced, this time with access to My Parkinson’s digital diary. They downloaded apps on their smartphones and received standardized training in Turkish for using this system with a train-the-trainer model. They went on to track their motor symptoms every hour for 24 hours
Day 8 –Second Clinic Visit (Cross-over): On the second day, motor symptoms were re-evaluated by the movement disorders specialist blindly (NDC, author) using a similar method to the first clinic visit to analyze and compare symptom data collected by paper diary vs. digital diary computed at home as a direct comparison of last measurement results from patient diaries.
Group 2:
First Phase (Phase I): This group of participants started the study with a My Parkinson’s digital diary. They followed the exact same protocols as Group 1. They tracked their symptoms for 24 hours, followed by a clinic visit the next day.
Second Phase (Phase II): (Cross-over): Like in Group 1, these participants switched to using the paper diary for another 24-hour symptom-tracking after the one-week washout period. During a second clinic visit, their symptoms were then assessed blindly by the same movement disorders specialist (NDC, author).
Compliance and Data Analysis Patient compliance with the diaries was evaluated by retrospectively comparing the recorded status with the WhatsApp records at documented hours. This analysis helped to identify discrepancies between what patients recorded in their diaries and what they reported in real-time, providing insight into the reliability of each diary method
End of Study Evaluation Participants were asked to rate the paper and digital diaries in preference and convenience after the study. This charting is a subjective assessment that allowed us to estimate patient satisfaction as well as ease of usability
Randomization and Group Assignment are summarized in Figure 1.
Features of the Paper Diary
This paper chart is a 24-hour diary for movement tracking designed explicitly for PD patients. With this diary, patients can systematically record and monitor their motor symptoms and medication usage (Figure 2). The diary is divided into hourly intervals between the starting point of 06:00 am and the ending point of 04:00 am (4:00 am of the following day), allowing for continuous observation throughout the day and night whenever the patient is awake. The essential columns in the chart are “On” and “Off,” which may indicate periods of the patient’s motor state. Columns such as “Tremor” and” Involuntary Movements” can track the most common symptoms of tremors and a side effect of dyskinesia caused by medication or a symptom of the disease. Finally, the record can be made in the column “Medication Use” to write which drug was taken at each hour. This Turkish chart is a revised form of Hauser et al.’s[8]. This diary is more detailed to provide more understandable patient fluctuations daily and optimize treatment.
Features of the Smartphone Application Digital Diary (My Parkinson’s)
“My Parkinson’s” is a smartphone application developed by a movement disorders specialist (SO, author). The app is free to download from Google Play on Android and the app store on iOS. This novel digital motor tracking app for patients with PD provides a real-time, remote monitoring and quantification tool empowering physicians to optimize care. The app is like a diary that allows users to enter information about their motor condition, appear “On” and “Off” throughout the day, and involuntary movements such as tremors or dyskinesia typically occur in PD.
The app’s interface is designed with simplicity and accessibility, especially to make it easy for users to input their symptoms with just a few taps, considering it will be used mainly by older people. Once patients register in the app’s patient section, they will receive an ID on their screen. They should then share this ID with their clinician so the clinician can access the patient’s data in real-time using this code. The question ‘How is my Parkinson’s today?’’ pops up on the phone screen every hour or at the desired interval (from 15 min to every four hours) as a reminder. When they tap the question button, the patient is directed to the application and a page where the patient is prompted with the question, “How are you feeling now?” and is presented with three options: ‘‘off’‘, ‘‘on’‘ and ‘‘involuntary movements’‘ Figure 3 This functionality enables real-time tracking, allowing the clinician to monitor the patient’s condition continuously. The data on the server can be accessed only by using an access code (handed to a physician by his patient), and this access does not work forever, as each report has its unique one-time code. This information is immediately shared with their clinician, with whom they have previously shared a unique patient code.
If the patient forgets to answer or cannot answer the question, they can only respond to the next question. They are not allowed to go back and answer the previous question/s to ensure the integrity of the tracking system and prevent retrospective adjustments, changes in current data, or multiple entries at once. The app collects these entries into a single timeline and visually organizes them chronologically over numerous days. It then reviews detailed graphs displaying data over various intervals and adjusts treatments as needed (Figure 4). This feature has been added to be useful for patients and clinicians in determining when exactly symptoms are getting worse or when medication works best.
24-Hour Parkinson’s Disease Motor Symptom Monitoring Chart:
This chart is designed for clinic visits in our department. During the visit, the clinician records motor fluctuations in dyskinesias and “on” and” off” periods based on the patient’s anamnesis. The timeline at the top of the chart spans from 6:00 am to 2:00 am the following day, with annotations marking the patient’s motor status at different times. Medication names are noted along the left side, with an arrow indicating when the patient took each medication. The chart visually represents the correlation between medication administration and the patient’s motor fluctuations, providing valuable data for clinicians to adjust treatment plans. The precise identification of” on” and” off” periods, along with times of dyskinesia, allows for a more tailored and effective management of Parkinson’s Disease symptoms (Figure 5).
2.4. Statistical Analyses
All statistical analyses were conducted using SPSS software, version 22. Descriptive statistics were presented as frequencies (n) and percentages (%) for categorical variables and as medians with corresponding minimum and maximum values for continuous variables. The weighted Kappa (κ) statistic assessed inter-rater agreement for each bias risk assessment tool domain and the overall evaluation.
3. Results
This section may be divided by subheadings. It should provide a concise and precise description of the experimental results, their interpretation, and the experimental conclusions that can be drawn.
3.1. Demographic and Clinical Characteristics of the Study Cohort
Twenty-two patients were enrolled in the study; however, one patient was excluded due to inconsistent internet access, and another was excluded for not using the internet daily during the study period. Of the last cohort of 20 patients, 60% were female (n=12). The mean age was 56.8 ± 10.2 years (range 34-70), and the mean Hoehn and Yahr (H&Y) score was 2.95 ± 0.65 (range 2-4). The mean levodopa equivalent daily dose (LEDD) was 1017.05 ± 461.5 mg (range 275-1997 mg), and the mean educational level was 9.15 ± 4.2 years (range 5-15 years). The mean duration of motor complications was 6.3 ± 3.06 years (range 3-6 years). The mean Mini-Mental Status Examination score was 27.8 ± 1.9 (range 25-30). No statistically significant differences were observed between the two groups with respect to age (p=0.07), LEDD (p=0.08), sex (p=0.20), educational status (p=0.22), or disease duration (p=0.10)
3.2. Comparative Analysis of Paper and Digital Diaries in Parkinson’s Disease Management
3.2.1. Patient Enrollment and Baseline Characteristics
To measure compliance and agreement with clinical examination notes with diary entries, we use paper diaries compared to a smartphone application (My Parkinson’s) with a Turkish interface. The results of the patients who were first given paper diaries and those who began with a digital diary are shown separately. Patients who received a paper diary first were compared to those with their second phase (My Parkinson’s app stage) compliance characteristics and agreement between clinical examination notes, separately for each outcome. A detailed description of the agreement between clinical examination notes and diary entries in patients initially receiving paper diaries is shown in Table 1. A comparison of patients starting with the paper diary showed a significant discrepancy in compliance; poor adherence occurred more frequently in the paper diary group versus the digital diary (My Parkinson’s) group. In the paper diary group, 37.5% of entries had no agreement; this percentage was only 6.25 in the digital diary arm. The digital diary had substantial and almost perfect compliance rates of 18.75% and 12.5 %, respectively, compared to paper, which remains the lowest in the tier of substantial compliance (6.25%). In all 16 hourly timings, the digital diary had a better crude agreement with clinical examination than paper diaries (Table 2). During measurements 2,3 and 16, the digital diary showed substantial to almost perfect agreement (κ = 0.615., κ = 0.818, κ = 815, respectively); however, for these periods, this was not observed using only paper diaries independently, no /slight agreement existed. This firm trend illustrates the true nature of digital diaries, which capture patient data accurately and reliably over time.
3.2.2. Compliance and Agreement Analysis
In contrast, for the patients who received digital diaries first (Table 3), paper diaries continued to maintain significantly lower rates, even if less pronounced than those with paper diaries up front. However, the compliance shown with digital diary, in this case, presents a muddy picture showcasing poor overall compliance (25% entries). Significant proportions are compliant to different extents - 50% with slight and 18.75 % with fair adherence.
3.2.3. Detailed Evaluation of Compliance across Diary Formats
The hourly comparison in Table 4 reflected that, when first implemented, the digital diary did not agree well with measurements. At this time, the overall agreement level of digital compared to paper print diary was still more vigorous in most cases for the original work.
3.2.4. User Preferences and Diary Usability
Regarding diary preference, 65% (n=13) of patients preferred to use the digital diary for future follow-ups, most often due to simple accessibility. In contrast, challenges, including lack of understanding (n=2), limited internet access (n=1), and functionality issues of the digital diary, were recognized as limitations for participants using this app. On the other hand, negative experiences of using paper diaries were tiredness throughout the day to complete (n=4), difficulty carrying a pen and scrap of paper around during study visits (n=3) and forgetting to fill the diary each hour. and keeping up to date with the diary on time, reported by six participants. Regarding the ease-of-use scale, there was no significant difference between the two diaries (p=0.430).
3.2. Figures, Tables, and Schemes
4. Discussion
This study results show that the electronic diary was rated better for overall patient adherence and accuracy among patients who initiated paper diaries. Higher compliance is observed with the digital diary compared to other measures, and there is more significant agreement with clinical notes. Electronic diaries offer advantages by improving compliance through reminders and reducing recall bias, but they also present challenges, especially in extensive multicenter studies [12].
In our study, paper diaries provided worse compliance and accuracy to real-time data than digital diaries in monitoring motor symptoms of PD. While conventional paper diaries have been widely used, they face compliance issues and recall bias. Löhle et al. assessed the validity of the Parkinson’s disease (PD) home diary (paper diary) for quantifying motor states by comparing it to direct clinical observation. The results indicate that the diary often inaccurately reflects actual motor states, with overall agreement at 59.8% (Cohen’s Kappa 0.387) and significant discrepancies in documenting “On” without dyskinesia (52.3% vs. 38.9%) and “On” with dyskinesia (21.5% vs. 34.2%), suggesting it may be an unreliable tool for assessing motor fluctuations in advanced PD [21].
The digital world is evolving, especially after the COVID-19 pandemic; telemedicine and digital tools have become an irreplaceable part of life [22]. Marxreiter et al. evaluated the use of digital technologies among Parkinson’s disease (PD) patients across different age groups. The study surveyed 190 Parkinson’s disease (PD) patients and found that 75% accessed disease-related information online, with digital technology use comparable to the general population. However, smartphone usage decreased in advanced PD patients due to motor impairments, suggesting that while PD patients are adopting digital tools, future healthcare technologies must account for motor difficulties in smartphone use [23]. Habets et al. developed and validated an electronic diary that monitors Parkinson’s disease symptoms during daily life. In this study, 20 patients used the developed eDiary for 14 days. The results indicated moderate-to-strong relationships between mood, motor symptom severity, and motor performance slowness of the implemented eDiary, demonstrating the validity of psychometric properties. This study also implies the importance of carefully developing the eDiary and patient selection for successful routine application [24]. Lakshminarayana et al. assessed the effect of using a smartphone-based Parkinson’s Tracker App (PTA) for people with PD on enhancing medication adherence and clinical consultation experience by conducting multicenter RCT in England and Scotland. The trial included 215 participants and found that the PTA more than doubled medication adherence, and patients reported quality of consultation compared to usual care.
Furthermore, 72% of participants used the app weekly for all four months, reflecting a high level of patient engagement. This was consistent with the results in that improvements were seen in non-motor symptoms and QOL but did not reach statistical significance. This study concluded that the PTA assists self-management and improves clinical care for Parkinson’s disease; however, further research is needed on the long-term outcome of using the tool [25].
Previous studies comparing smartphone and paper diaries for chronic diseases show varying results [26,27,28]. Regarding digital diaries, Lyons et al. evaluated the feasibility and compliance of electronic diaries in PD patients. Over seven days, 12 patients recorded their motor function every half hour, with the diary sending alarms for missed entries. The compliance rate was exceptionally high at 99.98% within 24 hours, with an average response time of 63 minutes during waking hours. Patients successfully operated the electronic diaries, achieving over 89% acquisition compliance, and the average response compliance was around one hour, providing valuable data on response patterns. In the questionnaire conducted after using the electronic diary in the study, half of the patients preferred the electronic diary over the paper diary, and 83% of the patients stated they would use this device to evaluate a new therapy for PD [29]. Reimer et al.[10] examined the utility and reliability of a CAPSIT-PD on/off diary using a four-point scale to measure fluctuations in Parkinson’s disease. Although agreement between patients and clinicians was good overall, the study showed that the CAPSIT-PD diary needed to be administered for too long a duration (> seven days) because shorter periods (one to three days) did not predict motor fluctuations over time. Our study’s relatively higher compliance with the digital diary is consistent with other up-to-date studies examining digital health tools within PD. Chuapakdee et al. developed a simplified, symptom-based, and electronic Parkinson’s disease (PD) diary as part of monitoring motor complications (MCs) in advanced PD. They compared it with traditional paper diaries regarding feasibility and critical outcomes. The electronic diary (e-PD) was created using a smartphone application with alarms and a picture response option to record in real-time ON/OFF states and dyskinesias. Seventeen non-demented PD patients with stable medication regimens used electronic and paper diaries simultaneously for at least one week. There was no significant difference in the time of ON/OFF/dyskinesia recorded by each method, although an 80.2% coefficient existed for functional state crossed between two diaries. The new method, the e-PD diary, had an accuracy of 81.1% with a sensitivity and specificity of 89.8% and 68.5%, respectively. Additionally, patients reported superior compliance and satisfaction with the e-PD diary. Conclusions: the e-PD diary is a feasible and accurate tool that could optimize motor complications management in PD[30].
The higher data accuracy from the digital diary application used in our study is consistent with the findings by Ossig et al., who compared paper diaries to sensor-based digital monitoring systems [11]. Interestingly, digital monitoring devices even detected subtle motor fluctuations not otherwise captured by traditional diaries[7]. On the other hand, the study by Nyholm et al. compares the effectiveness of conventional paper diaries and electronic diaries for tracking Parkinson’s disease (PD) symptoms, particularly in the presence of motor fluctuations. Twenty patients with PD, diagnosed for at least five years, were randomly assigned to use either a paper or electronic diary over eight days within a month. Patients answered questions every two hours for 12 hours. The results showed that median compliance was slightly higher with the paper diary (98%) than the electronic diary (88%). However, strict compliance linked to the scheduled times was lower in the paper diary. Age and prior computer experience did not influence the ability to use the electronic diary. The study concludes that electronic diaries effectively assess PD symptoms, offering real-time data capture and accurate compliance tracking[31]. Like many digital diaries in the literature, we also observed high-performance variability by supporting the idea that digital diaries improve patients’ contribution by allowing patients to receive self-reports in real-time and create a better understanding of their state as said states are affected by interventions. However, there are challenges to be overcome; for example, patient adherence is shaped by technology-related barriers such as those described in Terroba-Chambi et al.’s paper [32]. Riggare et al. mentioned despite the potential of digital health to revolutionize Parkinson’s care, existing solutions frequently fall short of addressing their specific needs [33]. Espay et al. stated that while technology captures more detailed data on Parkinson’s disease, it hasn’t yet improved diagnosis or treatment. Challenges include incompatible platforms, the need for widespread sensor use, and the gap between large data sets and clinical applications. A task force is working to develop open-source platforms for personalized treatment, early detection, and better management of tools that may struggle to have the same transformative impact on PD without managing usability and patient education [34]. Arora et al. highlight the need for patient education and support in implementing digital tools. Digital diaries were generally more acceptable, but acceptability depended on patients’ experience with this technology, as the study showed [35]. In chronic disease management, patient engagement is essential as the care needs to be monitored regularly and requires the participation of patients themselves. Since the number of patients was small and the ages of the patients were quite similar, we could not analyze the effect of age in our study. Age and education level may affect the preference for using a digital app rather than keeping a written track of symptoms in patients with Parkinson’s disease (PD). Research indicates that given the proper education and familiar interface, older patients can use digital tools for symptom tracking[36,37]. Mobile Apps for PD have demonstrated increased usability with familiarity and support; they apply even to an aging population[26]. People with higher levels of education are more knowledgeable about PD and accept digital health technologies with technical skills and an orientation toward using new tools [38]
The results of our study bear clinical relevance, as they imply an ability for digital diaries to shape how PD is managed in the future due to their potential for integrating more precise symptomatology that occurs on a day-to-day basis. This is consistent with the observations of Dorsey et al.’s [39], who noted the potential for digital tools to enhance clinical decision-making by reinforcing data available with greater granularity and immediacy than that within traditional methods. Moreover, incorporating digital tools in day-to-day clinic practice is a game-changer, allowing new possibilities for 24/7 monitoring and truly patient-centered proactive care[40].
Limitations:
This study has several limitations that are kept in mind while proposing potential solutions. Insufficient sample size is a limiting factor in this study of only 20 patients. Hence, it will affect the generalizability of results as we lack an adequate cohort or numbers to support robust analysis. Moreover, the need for familiarity with smartphones and internet access to participate introduces selection bias. A limitation of this study is that the short follow-up duration (24 hours) may not capture complete long-term use and compliance with diaries. Patients ‘ experience with technology was ignored; some might have had little familiarity with how to use the digital diary.
5. Conclusions
Our study strongly supports that a smartphone-based digital diary is adequate compared to traditional paper in terms of compliance and data accuracy of motor symptom recording for Parkinson’s Disease (PD). Digital diaries allow immediate data collection, decrease recall bias, and enhance patient involvement, making them an essential part of the multidisciplinary team managing PD. These benefits are core to broader trends in the shift towards digital health solutions for chronic disease care, mapping a pathway that eventually leads to personalized and proactive management for patients with PD. User-friendly digital technologies have a considerable potential to boost patient adherence and symptom-tracking accuracy, potentially revolutionizing Parkinson’s Disease clinical management
Author Contributions
In this study, N.D.C., S.O., N.M. carried out conceptualization, and A.Y.K. Methodology was developed by N.D.C., S.O., and N.M., who also handled the software aspects. Validation and formal analysis were performed by N.D.C. and N.M., who also led the investigation and data curation efforts. Resources were provided by N.D.C., S.O., A.T. and A.Y.K. The original draft of the manuscript was written by N.D.C., S.O., A.T, and A.Y.K., while review and editing were done by N.D.C., N.M., S.O., A.T, and A.Y.K. Visualization was managed by N.D.C. and S.O., with supervision provided by S.O. Project administration was undertaken by N.D.C. and S.O.
Funding
The study did not require any funding.
Institutional Review Board Statement
The study adhered to the principles of the Helsinki Declaration and received approval from the Eskisehir Osmangazi University Institutional Review Board (Approval Protocol code. 23/24.05.2022).
Informed Consent Statement
Written informed consent was obtained from all subjects involved in the study before participation.
Data Availability Statement
We can confirm that the data supporting the findings of this study are available and can be shared.
Acknowledgments
We would like to express our sincere gratitude to our Parkinson’s nurse, Nazan Korul, for her invaluable support and contributions to this study. Her assistance with collecting data, communication with patients, and data collection were instrumental in the successful completion of this research.
Conflicts of Interest
The authors declare no conflicts of interest. This study was conducted without any external funding. The authors independently designed the study, collected and analyzed the data, and made the decision to publish the result.
References
- Dorsey ER, Sherer T, Okun MS, Bloem BR. The Emerging Evidence of the Parkinson’s Pandemic. J Parkinsons Dis. 2018;8(s1):S3-S8. [CrossRef]
- Raza C, Anjum R, Shakeel NUA. Parkinson’s disease: Mechanisms, translational models and management strategies. Life Sci. 2019;226:77-90. [CrossRef]
- Poewe W, Antonini A, Zijlmans JC, Burkhard PR, Vingerhoets F. Levodopa in the treatment of Parkinson’s disease: an old drug still going strong. Clin Interv Aging. 2010;5:229-38. [CrossRef] [PubMed]
- Isaacson SH. Effective Treatment Strategies for Motor and Nonmotor Symptoms of Parkinson’s Disease. J Clin Psychiatry. 2020;81(1). [CrossRef] [PubMed]
- Kanellos FS, Tsamis KI, Rigas G, Simos YV, Katsenos AP, Kartsakalis G, et al. Clinical Evaluation in Parkinson’s Disease: Is the Golden Standard Shiny Enough? Sensors (Basel). 2023;23(8). [CrossRef]
- Peasgood T, Caruana JM, Mukuria C. Systematic Review of the Effect of a One-Day Versus Seven-Day Recall Duration on Patient Reported Outcome Measures (PROMs). Patient. 2023;16(3):201-21. [CrossRef]
- Vizcarra JA, Sánchez-Ferro Á, Maetzler W, Marsili L, Zavala L, Lang AE, et al. The Parkinson’s disease e-diary: Developing a clinical and research tool for the digital age. Mov Disord. 2019;34(5):676-81. [CrossRef] [PubMed]
- Hauser RA, Friedlander J, Zesiewicz TA, Adler CH, Seeberger LC, O’Brien CF, et al. A home diary to assess functional status in patients with Parkinson’s disease with motor fluctuations and dyskinesia. Clin Neuropharmacol. 2000;23(2):75-81. [CrossRef]
- Marinus J, Visser M, Stiggelbout AM, Rabey JM, Bonuccelli U, Kraus PH, et al. Activity-based diary for Parkinson’s disease. Clin Neuropharmacol. 2002;25(1):43-50. [CrossRef]
- Reimer J, Grabowski M, Lindvall O, Hagell P. Use and interpretation of on/off diaries in Parkinson’s disease. J Neurol Neurosurg Psychiatry. 2004;75(3):396-400. [CrossRef]
- Ossig C, Sippel D, Fauser M, Gandor F, Jost WH, Ebersbach G, et al. Assessment of Nonmotor Fluctuations Using a Diary in Advanced Parkinson’s disease. J Parkinsons Dis. 2016;6(3):597-607. [CrossRef]
- Papapetropoulos SS. Patient diaries as a clinical endpoint in Parkinson’s disease clinical trials. CNS Neurosci Ther. 2012;18(5):380-7. [CrossRef] [PubMed]
- Deb R, An S, Bhat G, Shill H, Ogras UY. A Systematic Survey of Research Trends in Technology Usage for Parkinson’s Disease. Sensors (Basel). 2022;22(15). [CrossRef] [PubMed]
- Hughes AJ, Daniel SE, Kilford L, Lees AJ. Accuracy of clinical diagnosis of idiopathic Parkinson’s disease: a clinicopathological study of 100 cases. J Neurol Neurosurg Psychiatry. 1992;55(3):181-4. [CrossRef] [PubMed]
- Arevalo-Rodriguez I, Smailagic N, Roqué I Figuls M, Ciapponi A, Sanchez-Perez E, Giannakou A, et al. Mini-Mental State Examination (MMSE) for the detection of Alzheimer’s disease and other dementias in people with mild cognitive impairment (MCI). Cochrane Database Syst Rev. 2015;2015(3):CD010783.
- Tomlinson CL, Stowe R, Patel S, Rick C, Gray R, Clarke CE. Systematic review of levodopa dose equivalency reporting in Parkinson’s disease. Mov Disord. 2010;25(15):2649-53. [CrossRef] [PubMed]
- Akbostanci MC, Bayram E, Yilmaz V, Rzayev S, Özkan S, Tokcaer AB, et al. Turkish Standardization of Movement Disorders Society Unified Parkinson’s Disease Rating Scale and Unified Dyskinesia Rating Scale. Mov Disord Clin Pract. 2018;5(1):54-9. [CrossRef]
- Hoehn MM, Yahr MD. Parkinsonism: onset, progression and mortality. Neurology. 1967;17(5):427-42.
- RANDOM.ORG: True Random Number Service [ONLINE] [Internet]. 2023. Available from: https://www.random.org.
- Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159-74.
- Löhle M, Bremer A, Gandor F, Timpka J, Odin P, Ebersbach G, et al. Validation of the PD home diary for assessment of motor fluctuations in advanced Parkinson’s disease. NPJ Parkinsons Dis. 2022;8(1):69. [CrossRef]
- Cubo E, Delgado-López PD. Telemedicine in the Management of Parkinson’s Disease: Achievements, Challenges, and Future Perspectives. Brain Sci. 2022;12(12).
- Marxreiter F, Buttler U, Gassner H, Gandor F, Gladow T, Eskofier B, et al. The Use of Digital Technology and Media in German Parkinson’s Disease Patients. J Parkinsons Dis. 2020;10(2):717-27. [CrossRef]
- Habets J, Heijmans M, Herff C, Simons C, Leentjens AF, Temel Y, et al. Mobile Health Daily Life Monitoring for Parkinson’s Disease: Development and Validation of Ecological Momentary Assessments. JMIR Mhealth Uhealth. 2020;8(5):e15628. [CrossRef]
- Lakshminarayana R, Wang D, Burn D, Chaudhuri KR, Galtrey C, Guzman NV, et al. Using a smartphone-based self-management platform to support medication adherence and clinical consultation in Parkinson’s disease. NPJ Parkinsons Dis. 2017;3:2. [CrossRef]
- Stone AA, Shiffman S, Schwartz JE, Broderick JE, Hufford MR. Patient compliance with paper and electronic diaries. Control Clin Trials. 2003;24(2):182-99. [CrossRef]
- Broderick JE, Stone AA. Paper and electronic diaries: Too early for conclusions on compliance rates and their effects--Comment on Green, Rafaeli, Bolger, Shrout, and Reis (2006). Psychol Methods. 2006;11(1):106-11; discussion 23-5. [CrossRef] [PubMed]
- Palermo TM, Valenzuela D, Stork PP. A randomized trial of electronic versus paper pain diaries in children: impact on compliance, accuracy, and acceptability. Pain. 2004;107(3):213-9. [CrossRef] [PubMed]
- Lyons KE, Pahwa R. Electronic motor function diary for patients with Parkinson’s disease: a feasibility study. Parkinsonism Relat Disord. 2007;13(5):304-7. [CrossRef]
- 30. Chuapakdee O, Punyakaew P, Ratanasirisawad V, Kongdachalert S, Winyooviji C, Bhidayasiri R. Feasibility of a simplified, symptom-based electronic diary to improve evaluation of motor and non-motor complications in Parkinson’s disease [abstract]. Mov Disord. 2020;35.
- Nyholm D, Kowalski J, Aquilonius SM. Wireless real-time electronic data capture for self-assessment of motor function and quality of life in Parkinson’s disease. Mov Disord. 2004;19(4):446-51. [CrossRef] [PubMed]
- Terroba-Chambi C, Bruno V, Medina-Escobar A, Nanni F, Cerquetti D, Rossi M, et al. Open-Access Electronic Diary for Motor Fluctuation and Dyskinesia Evaluation in Parkinson Disease: Comparison With Paper Diary. Clin Neuropharmacol. 2018;41(1):20-2. [CrossRef] [PubMed]
- Riggare S, Stamford J, Hägglund M. A Long Way to Go: Patient Perspectives on Digital Health for Parkinson’s Disease. J Parkinsons Dis. 2021;11(s1):S5-S10. [CrossRef]
- Espay AJ, Bonato P, Nahab FB, Maetzler W, Dean JM, Klucken J, et al. Technology in Parkinson’s disease: Challenges and opportunities. Mov Disord. 2016;31(9):1272-82. [CrossRef] [PubMed]
- Arora S, Venkataraman V, Zhan A, Donohue S, Biglan KM, Dorsey ER, et al. Detecting and monitoring the symptoms of Parkinson’s disease using smartphones: A pilot study. Parkinsonism Relat Disord. 2015;21(6):650-3. [CrossRef]
- Tsukita K, Sakamaki-Tsukita H, Takahashi R. Long-term Effect of Regular Physical Activity and Exercise Habits in Patients With Early Parkinson Disease. Neurology. 2022;98(8):e859-e71. [CrossRef]
- Viwattanakulvanid P, Somrongthong R, Vankwani M, Kavita FN, Kumar R. Predictors and Level of Knowledge Regarding Parkinson’s Disease among Patients: A Cross-sectional Study from Thailand. Int J Prev Med. 2020;11:25. [CrossRef]
- Tennigkeit J, Feige T, Haak M, Hellqvist C, Seven Ü, Kalbe E, et al. Structured Care and Self-Management Education for Persons with Parkinson’s Disease: Why the First Does Not Go without the Second-Systematic Review, Experiences and Implementation Concepts from Sweden and Germany. J Clin Med. 2020;9(9).
- Dorsey ER, Topol EJ. State of Telehealth. N Engl J Med. 2016;375(2):154-61.
- Luis-Martínez R, Monje MHG, Antonini A, Sánchez-Ferro Á, Mestre TA. Technology-Enabled Care: Integrating Multidisciplinary Care in Parkinson’s Disease Through Digital Technology. Front Neurol. 2020;11:575975. [CrossRef] [PubMed]
Figure 1.
Flowchart of study design comparing paper diary and digital diary (My Parkinson’s) in Parkinson’s disease symptom tracking.
Figure 1.
Flowchart of study design comparing paper diary and digital diary (My Parkinson’s) in Parkinson’s disease symptom tracking.
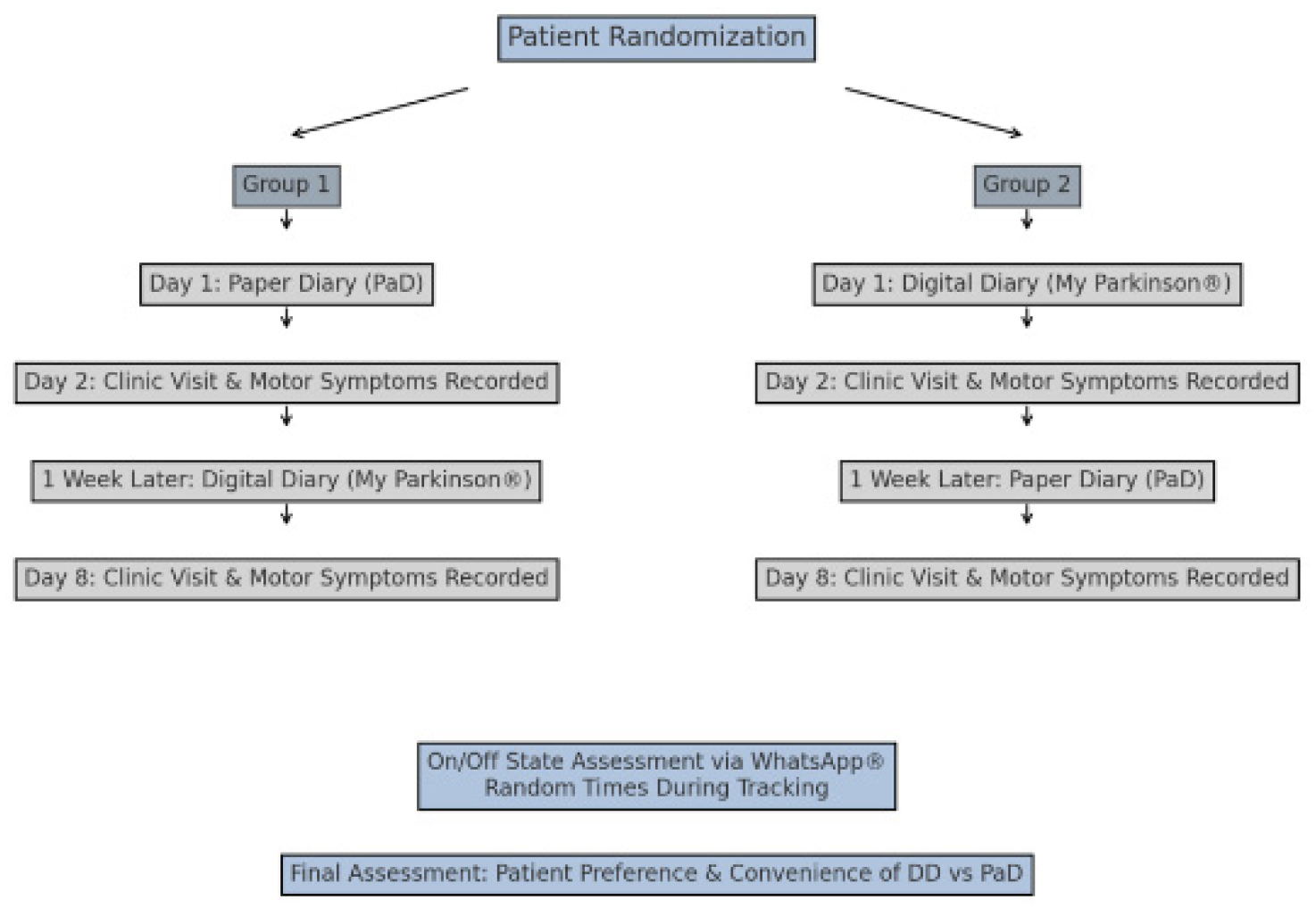
Figure 2.
The paper diary is used to track Parkinson’s disease symptoms and medication usage over 24 hours.
Figure 2.
The paper diary is used to track Parkinson’s disease symptoms and medication usage over 24 hours.
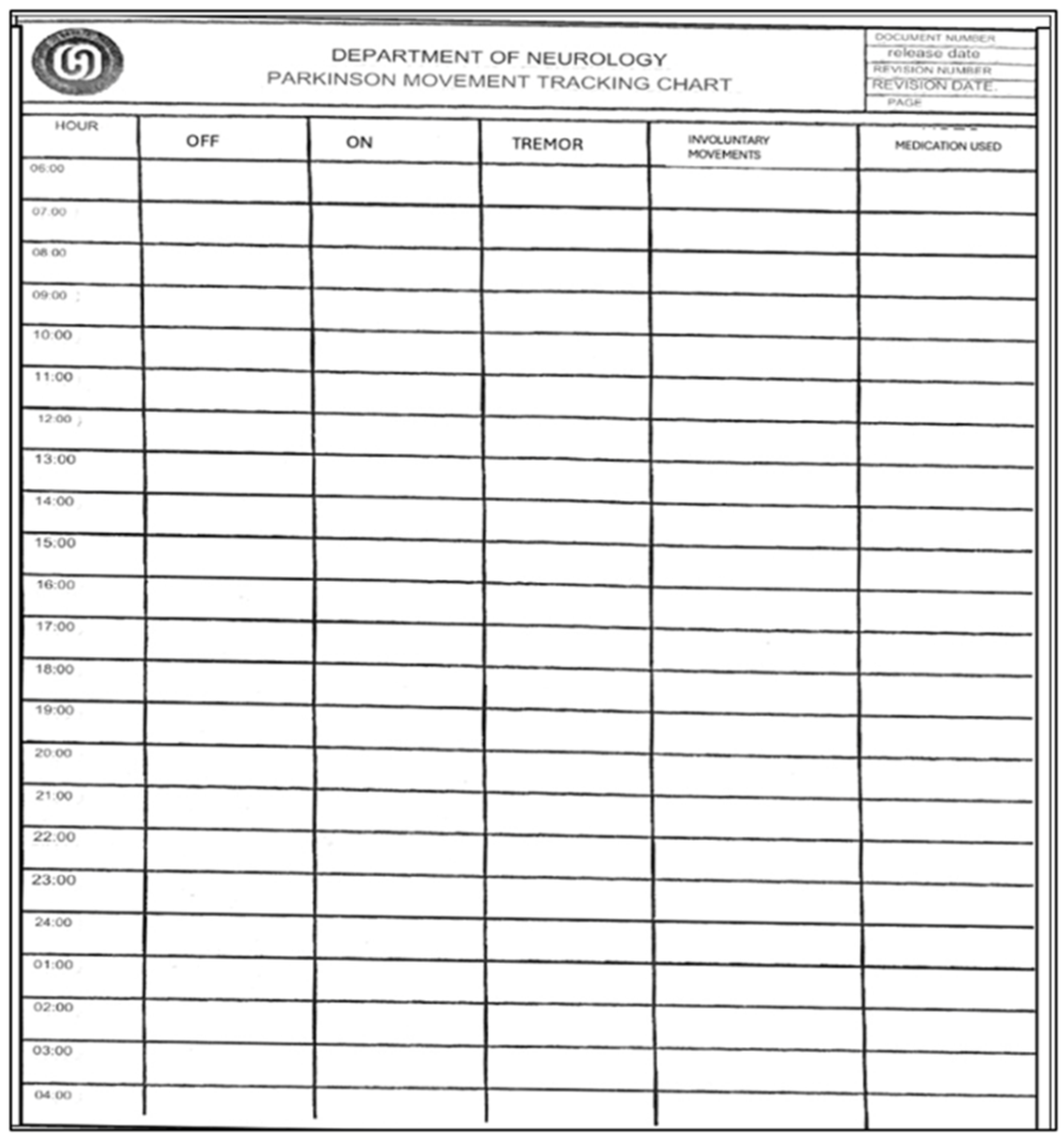
Figure 3.
User interface of the ‘MyParkinson’s app for real-time symptom tracking and status reporting in Parkinson’s disease.
Figure 3.
User interface of the ‘MyParkinson’s app for real-time symptom tracking and status reporting in Parkinson’s disease.
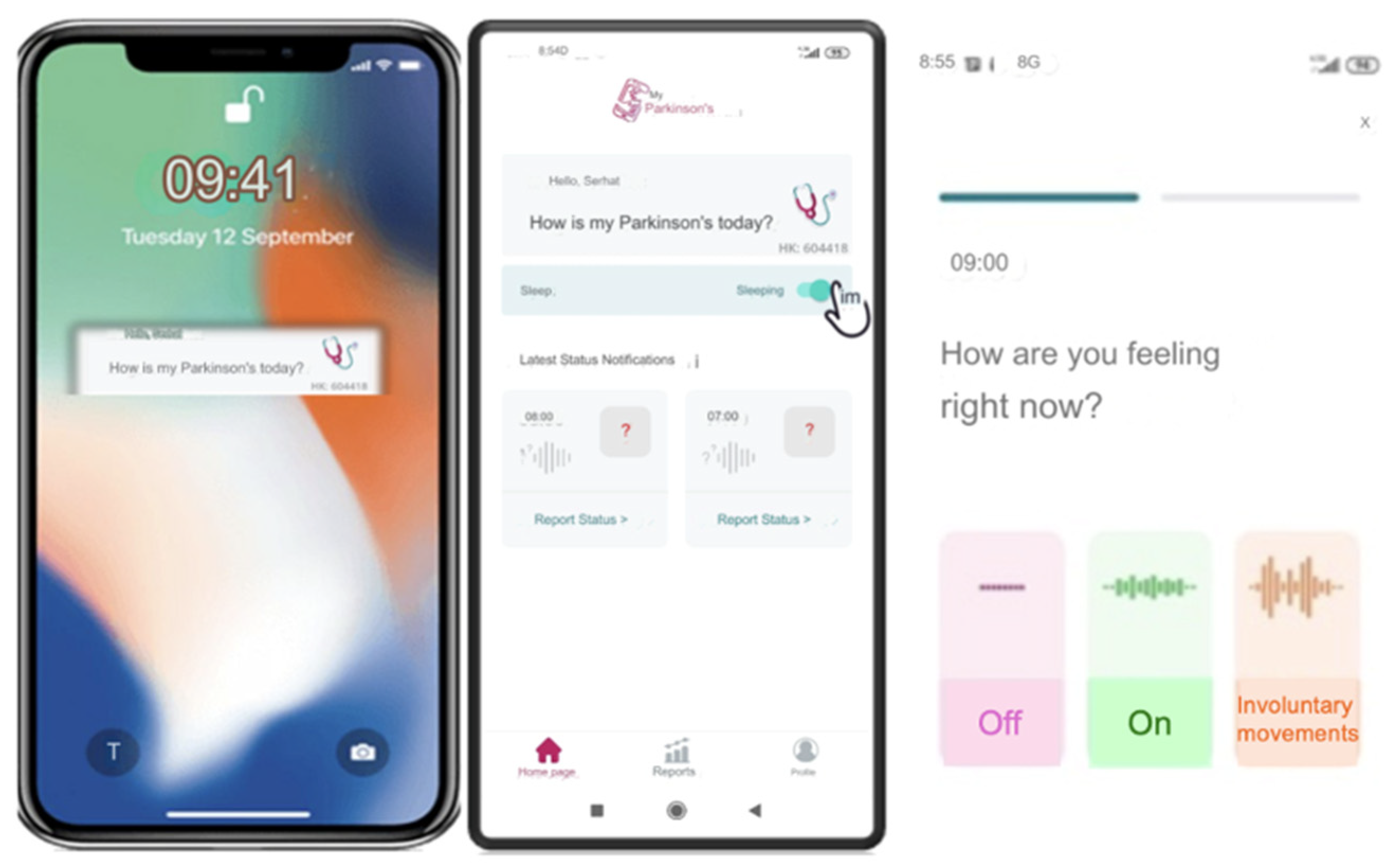
Figure 4.
Digital tracking of Parkinson’s disease symptoms: 24-hour report and dyskinesia monitoring of the ‘MyParkinson’s’ app.
Figure 4.
Digital tracking of Parkinson’s disease symptoms: 24-hour report and dyskinesia monitoring of the ‘MyParkinson’s’ app.
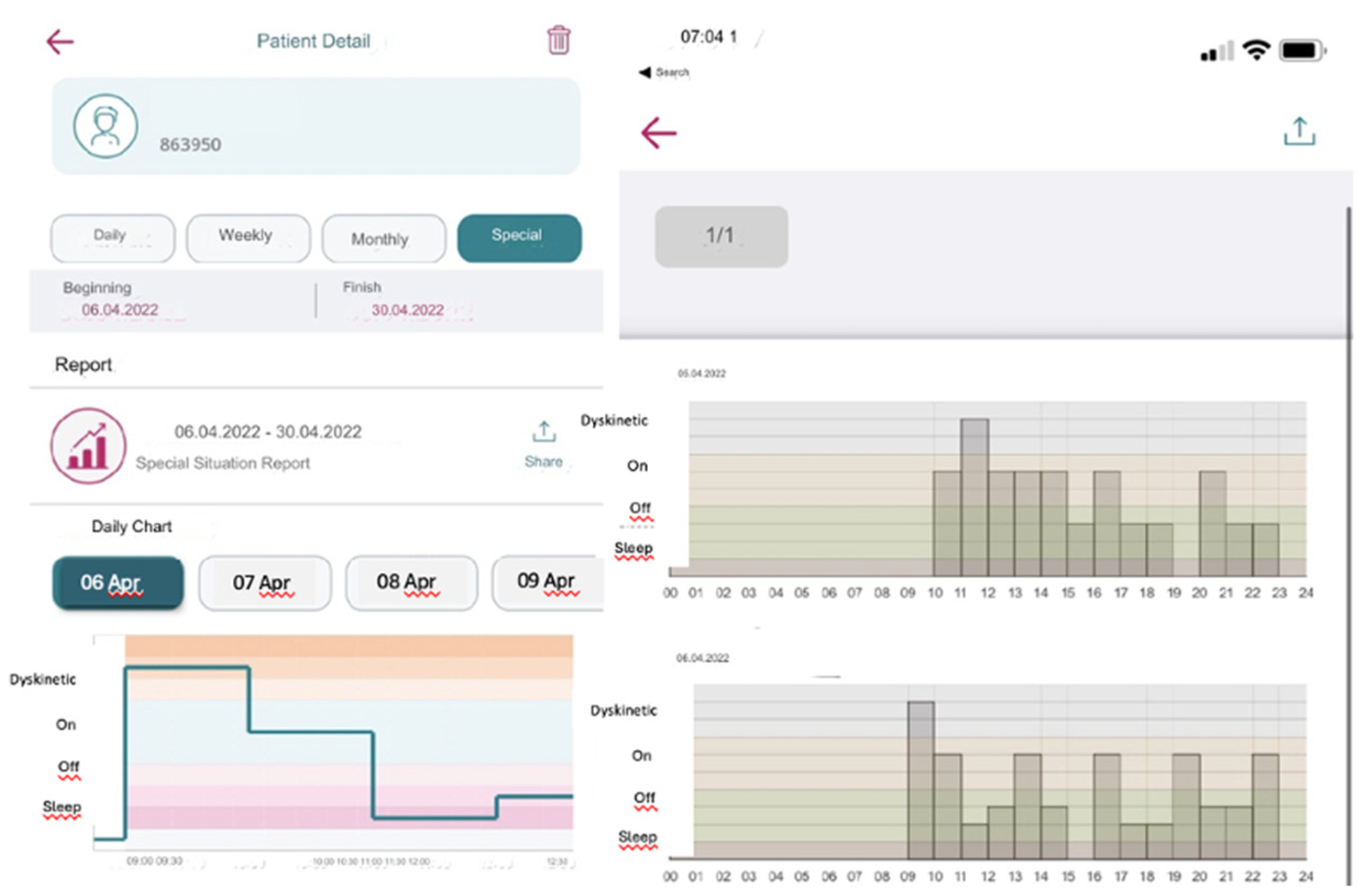
Figure 5.
24-hour Parkinson’s disease motor symptom monitoring chart.
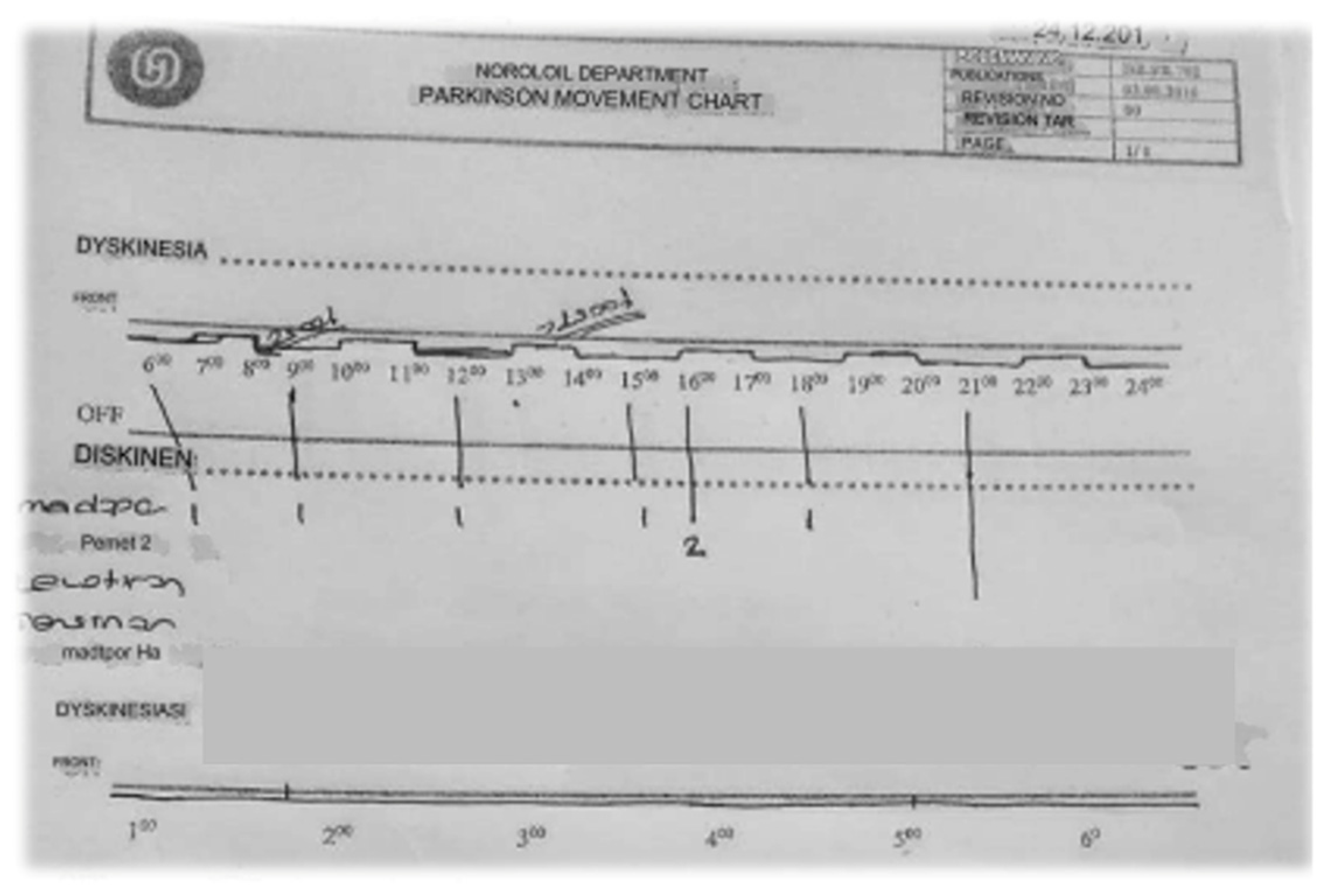

Table 1.
Distribution of agreement between clinical examination notes and both diaries in patients who were first given paper diaries.
Table 1.
Distribution of agreement between clinical examination notes and both diaries in patients who were first given paper diaries.
| n | % | |
|---|---|---|
| Paper | ||
| No agreement | 6 | 37,5 |
| Slight | 2 | 12,5 |
| Fair | 4 | 25 |
| Moderate | 3 | 18,75 |
| Substantial | 1 | 6,25 |
| Almost Perfect | 0 | 0 |
| Application | ||
| No agreement | 1 | 6,25 |
| Slight | 4 | 25 |
| Fair | 4 | 25 |
| Moderate | 2 | 12,5 |
| Substantial | 3 | 18,75 |
| Almost Perfect | 2 | 12,5 |
*The agreement was measured via Cohen’s kappa.
Table 2.
The hourly comparison of the compliance characteristics of the clinical examination notes is a table. Tables should be placed in the main text near the first time they are cited.
Table 2.
The hourly comparison of the compliance characteristics of the clinical examination notes is a table. Tables should be placed in the main text near the first time they are cited.
| Paper diary*( )κ | Digital diary*( )κ | Paper diary | Digital diary | |
|---|---|---|---|---|
| Measurement 1 | 0,574 | 0,483 | Moderate | Moderate |
| Measurement 2 | 0,000 | 0,615 | Slight | Substantial |
| Measurement 3 | -0,071 | 0,818 | No agreement | Almost Perfect |
| Measurement 4 | 0,524 | 0,259 | Moderate | Fair |
| Measurement 5 | -0,042 | -0,143 | No agreement | No agreement |
| Measurement 6 | 0,661 | 0,556 | Substantial | Moderate |
| Measurement 7 | 0,500 | 0,623 | Moderate | Substantial |
| Measurement 8 | 0,091 | 0,091 | Slight | Slight |
| Measurement 9 | 0,000 | 0,388 | Slight | Fair |
| Measurement 10 | 0,388 | 0,423 | Fair | Moderate |
| Measurement 11 | -0,111 | 0,783 | No agreement | Substantial |
| Measurement 12 | -0,111 | 0,123 | No agreement | Slight |
| Measurement 13 | -0,071 | 0,545 | No agreement | Moderate |
| Measurement 14 | 0,583 | 0,388 | Moderate | Fair |
| Measurement 15 | -0,111 | 0,231 | No agreement | Fair |
| Measurement 16 | 0,286 | 0,815 | Fair | Almost Perfect |
*κ : Kappa test, Table column presents the corresponding data for the row.
Table 3.
Distribution of agreement between clinical examination notes and both diaries in patients who were first given digital paper.
Table 3.
Distribution of agreement between clinical examination notes and both diaries in patients who were first given digital paper.
| n | % | |
|---|---|---|
| Paper | ||
| No agreement | 2 | 12,5 |
| Slight | 3 | 18,75 |
| Fair | 6 | 37,5 |
| Moderate | 5 | 31,25 |
| Substantial | 0 | 0 |
| Almost Perfect | 0 | 0 |
| Application | ||
| No agreement | 4 | 25 |
| Slight | 8 | 50 |
| Fair | 3 | 18,75 |
| Moderate | 1 | 6,25 |
| Substantial | 0 | 0 |
| Almost Perfect | 0 | 0 |
*The agreement was measured via Cohen’s kappa.
Table 4.
Hourly comparison of the compliance characteristics of the clinical examination notes and 16-hourly measurements of both diaries in patients who were first given a digital diary.
Table 4.
Hourly comparison of the compliance characteristics of the clinical examination notes and 16-hourly measurements of both diaries in patients who were first given a digital diary.
| Paper diary*( κ) | Digital diary* ( κ) | Paper diary | Digital diary | |
|---|---|---|---|---|
| Measurement 1 | 0,265 | 0,136 | Fair | Slight |
| Measurement 2 | 0,524 | 0,000 | Middle | Slight |
| Measurement 3 | 0,107 | 0,206 | Slight | Fair |
| Measurement 4 | 0,524 | -0,212 | Middle | No agreement |
| Measurement 5 | 0,123 | 0,000 | Slight | Slight |
| Measurement 6 | 0,219 | 0,000 | Fair | Slight |
| Measurement 7 | -0,111 | 0,184 | No agreement | Slight |
| Measurement 8 | 0,206 | -0,029 | Fair | No agreement |
| Measurement 9 | 0,268 | 0,153 | Fair | Slight |
| Measurement 10 | 0,474 | 0,231 | Middle | Fair |
| Measurement 11 | 0,545 | 0,492 | Middle | Middle |
| Measurement 12 | -0,029 | 0,032 | No agreement | Slight |
| Measurement 13 | 0,231 | 0,038 | Fair | Slight |
| Measurement 14 | 0,000 | -0,296 | Slight | No agreement |
| Measurement 15 | 0,250 | -0,167 | Fair | No agreement |
| Measurement 16 | 0,464 | 0,231 | Middle | Fair |
*κ : Kappa test, Table column presents the corresponding data for the row.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



