
Submitted:
28 August 2024
Posted:
29 August 2024
You are already at the latest version
Abstract
This study aims to investigate whether 16 weeks of High-Intensity Interval Training (HIIT) implemented on Physical Education classes (PEC), can improve physical fitness in high-school adolescents This study was a two-arm randomized controlled trial design with adolescents (15-17 years old). Twelve classes were randomized to either a 16 weeks of HIIT (HIIT-G, n = 106 students) implemented on PEC warm-up or a control group (CG, n = 123 students) of usual PEC warm-up. The HIIT sessions ranged from 14 to 20 all-out bouts intervals, adopting a 2:1 work-to-rest ratio. Post-intervention measures revealed a significant difference between groups in CRF and girls from HIIT-G increased their cardiorespiratory fitness (CRF) with significant difference between female groups and a medium to large effect size. The main findings from this study indicate that brief whole-body HIIT of an extremely low volume, over 16 weeks, can improve CRF in adolescent girls.
Keywords:
Health
; cardiorespiratory fitness
; muscular fitness
; body composition
1. Introduction
Low cardiorespiratory fitness (CRF), measured by maximal oxygen consumption (VO2max), is a powerful predictor of all-cause mortality and morbidity in young people [1]. Insufficient physical exercise (PE) but also other factors, such as overweight and obesity, and poor diet, are increasingly evident in the adolescent population, and could be decisive both for low CRF and the increasing incidence of different pathologies [2]. Over 50% of obese children will become obese adults, with a significant increase in the risk of developing asymptomatic diseases, including cardiovascular diseases, cancer, and type 2 diabetes mellitus [3]. Despite the numerous benefits of regular PE, western children and adolescents spend too much time in sedentary behaviors, which is worsening every decade [2,4,5,6]. Data related to Health Behavior in School-Aged Children (HBSC) associate a sedentary lifestyle with headaches, sadness, irritability, and nervousness [6]. Moreover, adolescents tend to become more inactive as their age increases [7]. Short leisure time, reduced access to facilities and low motivation to engage in physical activities, are frequently reported barriers to poor adherence to exercise programs [8,9,10]. In modern society, it is unlikely that individuals will ever return to the high average PE levels of the past. In any case, higher amounts of sedentary behavior are associated with increased adiposity, poorer cardiometabolic health and fitness in children and adolescents, and the World Health Organization (WHO) stated that this population should achieve at least an average of 60 minutes per day of moderate-to-vigorous PE (MVPE) and must limit sedentary time [11]. Notwithstanding the limited number of people willing to engage in MVPE and the high attrition of those who participate [12], the evidence shows high effectiveness of MVPE in reducing mortality, even considering a long lifespan [13].
Therefore, High-Intensity Interval Training (HIIT) is presented as a time-efficient alternative to aerobic training [2,14,15,16], as it leverages the number of exercise participants, resulting in improvements in health outcomes, mainly from adolescents [5,17,18,19]. HIIT is characterized by relatively short periods of very intense exercise, interspersed with periods of pause or low-intensity exercise [20,21]. The purpose of HIIT is that physiological systems may perform exercises of higher intensity than those achieved during a gradual maximal test [22]. HIIT is a powerful stimulus in improving body composition and preventing cardiometabolic risk in adults [23]. Preliminary studies conducted with adolescents have shown promising results on body composition and cardiometabolic health and more effective and time-efficient interventions for improving blood pressure and aerobic capacity levels [4,7,17,24,25]. According to Bond et al. [26], time spent in high-intensity activities is the most relevant factor in promoting vascular health and autonomic cardiac modulation. Children and adolescents have expressed a clear preference for time efficiency and pleasure, and the “stop-start” nature of HIIT seems to reflect the activities traditionally observed in childhood [2,3,4,16]. No harmful associations in recent studies applying intense efforts are also encouraging [27,28]. Furthermore, adolescents seem to be more enthusiastic about resistance training, whereas aerobic training is found to be boring [29]. Other studies, besides aerobic and resistance training groups, included a variety of activities to enhance motivation and appeal to the interest of older adolescents, improving aspects of adolescents’ cardiometabolic health [30], fitness and body composition, despite the lowest dose among groups [5]. Interventions designed to increase MVPE in Physical Education classes (PEC) indicate that programs could increase the proportion of time students spend in higher intensities and reduce sedentary behavior, since motivational climates that emphasize effort and improvement and provide opportunities to demonstrate leadership and make decisions have a positive impact on PA [31].
Adolescents, especially older ones, are underrepresented in studies implemented in the school context [28]. Despite the widespread interest in the advantages that the HIIT methodology reveals, there is a lack of randomized controlled studies investigating the impact on adolescents [2,28], mainly addressing adolescents’ environments, such as schools [5,18]. It is known that the school and PEC are privileged spaces and promoters of positive changes for the rest of life [32], in which time-efficient approach interventions have a prominent role. Recently, some studies present HIIT programs targeting school-aged children [33,34,35,36], and in a scope of 10 years, we find dozens of works with students aged 10-19 years, but only a few were implemented in the school setting (manly extracurricular activity). Of them, just a few [9,27,35,36,37,38,39,40] were implemented in PEC, replacing the entire session with the intervention [9,40]. Most protocols in the literature opted for 1:1 density and SPRINT as modality [25]. Some, recording large effect sizes on CRF [9,40], PA [9], strength, power, and speed [41], needed only six minutes three [9,40] and four times [41] a week, and chose to use all-out bouts instead of a percentage of Maximal Aerobic Speed (MAS). In adults, previous findings suggest that a 2:1 work-to-rest ratio is optimal during HIIT for both men and women [42]. We aim to provide novel HIIT protocols for schools with less volume (only twice a week) and higher density (less rest in each interval), implement PA interventions that retain the health-enhancing effects and satisfy the adolescents’ desire for enjoyment and variety. This study aims to investigate whether 16 weeks of HIIT implemented on PEC, compared to 16-weeks of usual PEC, can improve body composition and physical fitness in high-school adolescents, and determine the gender differences among the participants.
2. Materials and Methods
2.1. Study Design
This project was registered on ClinicalTrials.gov (ID: NCT04022642) and approved by the Ethics Committee of the University of Évora (doc. 19017). In all aspects, this trial was conducted according to the Declaration of Helsinki on Human Research. Apart public schools in the city of Beja (Portugal) were invited to participate, but only one consented to participate. Written consent was obtained before participation from the school principal and parents.
2.2. Participants
This study was a two-arm randomized controlled trial design with adolescents from the 10th to 12th grades (15-17 years old). Twelve from a total of 18 classes with an average of 25 students each, recruited from a public school (Figure 1), were randomized to either 16 weeks of HIIT (HIIT-G, n = 106 students) implemented on PEC warm-up or a control group (CG, n = 123 students) of usual PEC warm-up. After an invitation, the researchers met with the school principal to provide information on the whole project. After accepting to participate, adolescents and their parents were informed of a detailed description of the scientific background, objectives, and safety.
2.3. Randomization
The school principal, as a person independent of the study, concealed participant allocation by shaking a bag with all 18 classes before baseline testing. Classes were randomized so that two classes from each grade were allocated to the intervention condition and the other two were used as control group. Using this approach, each class had an equal chance of being allocated to the intervention condition while maintaining an appropriate balance of grades across the two conditions. Students were ineligible if they did not provide parental consent to participate, had physical limitations or revealed intellectual disabilities.
2.4. Sample Size
Power calculations were based on the primary outcome of CRF, assessed using the 20-m Progressive Aerobic Cardiovascular Endurance Run (PACER; Henriques-Neto, et al. [43]). To detect a clinically meaningful baseline-adjusted between-group difference of seven laps [28] with 80% power at a 5% significance level, 58 students per treatment group were required (i.e., four classes of 15 students), for a potential drop-out rate of 15% at our primary study end point (i.e., 16 weeks).
On 13 March 2020, the Portuguese Government adopted strict containment measures to avoid the new coronavirus (SARS-CoV-2) spread, and the student population was placed in home confinement, with permission only to leave home for limited and documented purposes (e.g., for health reasons or buying food), and several activities were temporarily prevented, including schools. Many students stayed at home in the first few days of March, even before the formal lockdown, and didn't finish the entire intervention program or post-tests. These global preventive strategies posed unprecedented challenges and obstacles for our research, experiencing lower follow-up rates in the ongoing trial. As a negative consequence of home confinement, we experienced a high number of dropouts in several outcomes (Figure 1).
2.5. Intervention Program
Throughout the 16-week intervention period, the HIIT-G took part in the regular 90min PEC twice a week, conducted by the schools’ PEC teachers following the regular curriculum. The HIIT-G replaced the warm-ups established in the PEC curriculum with the proposed HIIT training sessions. After the HIIT sessions, students completed the planned PEC.
The HIIT sessions were applied in the first 10-15 minutes of each PEC and ranged from 14 to 20 all-out bouts intervals, adopting a 2:1 work-to-rest ratio, involving a combination of aerobic and body weight muscle-strengthening exercises, and designed to be fun and engaging, as well as vigorous in nature (Figure 2).
To promote exercise adherence, sessions were designed progressively from four minutes in week zero to 10 minutes in week three using the Tabata, et al. [44] protocol (20s intense work, followed by 10s rest). From week four to week seven, the same volume but using 30s-intense work, followed by 15s rest. From weeks nine to 15, sessions were completed in pairs (Figure 3). Participants gave additional elements of choice, such as music, exercises, and workouts.
A cut-point of 90% of HRmax was a criterion for satisfactory compliance to high-intensity exercise. HR has become one of the most used outcomes to assess the intensity, and several authors suggest that each interval corresponds to a value equal to or greater than 90%HRmax [45,46,47]. An optimal stimulus that promotes cardiovascular and peripheral adaptations implies several minutes per session in the so-called red zone, which usually means a minimum intensity of 90%VO2max [48]. It is expected that HR reaches maximum values (>90-95% HRmax) close to the speed/power associated with VO2max, which does not always happen, especially in very short exercises (<30 seconds) [45,46]. It may be related to the known delay in HR response at the beginning of exercise, which is slower than the VO2 response. During the supervised intervention, the researchers recorded HR using the Heart Zones Move™ software application which uses a forearm wearable plethysmography heart rate sensor (Scosche Industries, CA, USA) to ensure compliance with the exercise stimulus at the predetermined target HR zone. Besides, rating perceived exertion (RPE) was also measured in each exercise session to estimate effort, fatigue, and training load, targeting >17 on the 6−20 Borg scale [49,50].
Throughout the 16-week intervention period, the CG took part in the regular 90min PEC twice a week, conducted by the schools’ PEC teachers following the regular curriculum.
2.6. Measures
All primary and secondary outcomes were measured at baseline two weeks prior the intervention and after 16 weeks after the HIIT program (Figure 4). CRF was the primary outcome, and secondary outcomes includes muscular fitness and body composition. All assessments were conducted by the Principal Investigator. Anthropometric assessments were conducted sensitively with the presence of a same-sex research staff when possible. The Principal Investigator provided a brief verbal description and demonstration of each fitness test before evaluation. Before the exercise intervention, both group teachers and participants were instructed to follow the regular curriculum and maintain their regular dietary and lifestyle behaviors during the intervention period. The authors evaluated measures and data collection, not blinded for group allocation. Different tests were conducted on different days to ensure sure that all interventions and assessments were implemented in PEC.
2.7. Physical Fitness Assessment
2.8. Body Composition Assessment
Participants’ body composition was measured to the nearest 0.1 kg in light sportswear on a bioelectrical impedance scale (Tanita MC -780), and height was measured to the nearest 1 mm using a portable stadiometer (Seca 213 Portable Height Measuring Rod Stadiometer). Body composition measurements (body fat, lean body mass and basal metabolic rate) were performed by bioelectrical body impedance analysis (BIA). Measurements were performed according to Jackson, et al. [52].
2.9. Data Analysis
All statistical analyses were performed with the Statistical Package for the Social Sciences v.24 (SPSS Inc., Chicago, IL, USA). The normality of data distribution was tested using the Kolmogorov-Smirnov test. When normality was observed, data were checked for significant differences between baseline and post-intervention applying student’s t-test for paired samples and for significant differences between the two groups applying student’s t-test for unpaired samples. Where the analysis suggested non-normality, simple effects were examined using the non-parametric Wilcoxon’s signed ranks test for differences between baseline and post-intervention and the Mann-Whitney U test for significant differences between the two groups and genders.
To estimate effect sizes, Hedge’s g was calculated for normally distributed measurements (one of the means from the two distributions is subtracted from the other, and the result is divided by the pooled sample standard deviation) and interpreted as follows: d = 0.2, d = 0.5, and d = 0.8, considered as small, medium, and large effect sizes, respectively [53]. For non-normal distributions, the z value was used to calculate the effect size, such as the r proposed by Cohen (1988, cit in Fritz et al., 2012) [53]; Cohen’s guidelines for r are that a large effect is .5, a medium effect is .3, and a small effect is .1. Significance was set at p < 0.05.
3. Results
The mean training load response and volume during HIIT intervention are displayed in Table 1. Descriptive statistics and the effects of the intervention on physical fitness and body composition measures are displayed in Table 2. Due to activities and teaching breaks or climate condition, each class of HIIT-G participated on an average of 16.4 ± 1.3 (63%) of the 26 scheduled exercise sessions. The mean attendance for participants involved in the intervention was 12.2 ± 3.5 (47%). Absences were due to illness, medical appointments, lack of appropriate clothing or work placement attendance and, near the end of the intervention, home confinement.
Post-intervention measures revealed a significant difference between groups in CRF (U = 5313.5; p < 0.05; ES = 0.16) mainly because of the girls, since girls from CG lowered their CRF (Z = -2.1; p < 0.05; ES = 0.25) and girls from HIIT-G increased their CRF (t = 2.6; 0.5 to 3.9 95%IC; p < 0.05; ES = 0.35), with significant difference between female groups and a medium to large ES (t = -3.6; -5.9 to -1.7 95%IC; p < 0.001; ES = 0.65). Within groups, HIIT-G increased muscular fitness (t = 3.2; 1.7 to 7.8 95%IC; p < 0.005; ES = 0.43), again mainly because of the girls (t = 2.4; 0.8 to 9.9 95%IC; p < 0.05; ES = 0.45) since boys did not reach significance (t = 2.0; -0.1 to 8.0 95%IC; p = 0.005; ES = 0.40).
There was no significant difference in body composition between groups post-intervention. All groups and genders increased their lean body mass and lowered body fat; however, regarding body fat, only HIIT-G boys did not reach significance (Z = -1.6; p = 0.12; ES = 0.25).
4. Discussion
The aim of this study was to investigate whether 16 weeks of HIIT implemented on PEC, compared to 16 weeks of usual PEC warm-up, can improve physical fitness in high-school adolescents, and determine the gender differences among the participants. The main findings from this study indicate that brief whole-body HIIT (10 min) of an extremely low volume, over 16 weeks (on average, 0.8 sessions per week), can improve CRF and muscular fitness in adolescent girls. Our study registered an increase of 9% in CRF in HITT-G girls and a decrease of 4% in CG girls, representing a medium to large ES (t = -3.6; -5.9 to -1.7 95%IC; p < .001; ES = 0.65). Within a 10-year scope, we find dozens of works with students aged 15-17 years, but only a few were implemented in the school setting. Notwithstanding some studies have been implemented in the school setting, only a few were implemented in PEC. Along this line of results, at the end of the seventh week, Alonso-Fernández, Fernández-Rodríguez, Taboada-Iglesias and Gutiérrez-Sánchez [38], in a similar intervention with only 8 min twice a week, registered an increase of 10% in VO2max to baseline (p < .001; ES = 0.33), with only 13 female adolescents distributed by intervention and CG. Also in a seven week intervention, but with three sessions/week, using six min SPRINT as modality and only two female adolescents in HIIT-G, Buchan, Young, Simpson, Thomas, Cooper and Baker [37] observed, compared to CG, a significant increase of seven laps in PACER (p < .005), and a significant decrease in muscular fitness of CG (p < .005). Martin-Smith, Buchan, Baker, Macdonald, Sculthorpe, Easton, Knox and Grace [9], using three sessions/week for only four weeks, replaced the entire PEC session with six min HIIT intervention, with nine female adolescents in HIIT-G, increased CRF 5 ml/kg/min with large ES (p < .05, ES = 0.92). Years earlier, the same researchers [40], with seven girls in HIIT-G, reached a large ES in intervention (0.93) due to the significant decrease in CRF of CG (p < .05) in a seven week intervention, three sessions/week. Costigan, Eather, Plotnikoff, Taaffe and Lubans [24] also did not reach significance in CRF and muscular fitness improvements in an eight week intervention, 10min/session, three sessions/week, with 12 female adolescents distributed in two HIIT-G. An increase in mitochondrial content and induced higher increases in citrate synthase maximal activity [54], type II fiber activation, and adenosine monophosphate-activated protein kinase activity [55] can be some of the physiological mechanisms explaining why HIIT may improve CRF. According to Bond et al. [26], time spent in high-intensity activities is the most important factor in promoting vascular health and autonomic cardiac modulation. Moreover, this could explain the absence of improvements in CRF observed in males. Because this is a high-intensity methodology, it is necessary to regulate the intensity to ensure that subjects hit a high enough threshold in their exercises. The difference in the findings between girls and boys may be a consequence of the higher average intensity, represented as the average time in seconds above 90%HRmax/session, of the girls observed in this study compared with the boys (222s vs 133s, respectively; t = 3.8; 42.0 to 135.5 95%IC; p < .000; ES = 0.74). Despite men's ability to produce more power, some studies reveal that women may have a higher resistance to exhaustion and/or better recovery during bouts of repetitive activity [42]. These data support the idea that women may recover faster from high-intensity exercise because they self-select intensities that put their hearts under more pressure. Although VO2max is frequently used to determine the intensity of HIIT, this method ignores the subjects' anaerobic characteristics, which are critical for HIIT [56]. Likewise, it seems unlikely that teachers would have access to those technologies in PEC real-world contexts. The use of all-out bouts and plyometrics are also simple and effective approaches since some studies that record Large Effect Sizes chose to use all-out bouts instead of a percentage of MAS [9,40,41].
Regarding body composition, in our study, all groups and genders increased their lean body mass and lowered body fat. Alonso-Fernández, Fernández-Rodríguez, Taboada-Iglesias and Gutiérrez-Sánchez [38] registered a decrease of 8% in % of body fat to baseline (p < .001; ES = 0.58) and an increase of 6% in lean body mass (p < .001; ES = 0.15). In Buchan, Young, Simpson, Thomas, Cooper and Baker [37] intervention, there were no significant changes in body composition in both groups, and Martin-Smith, Buchan, Baker, Macdonald, Sculthorpe, Easton, Knox and Grace [9] did not reach significance in the waist and hip circumference. Costigan, Eather, Plotnikoff, Taaffe and Lubans [24] reduced significantly compared to CG 2 cm in waist circumference (p < .05; ES = 0.70).
Physical fitness is considered a significant health indicator, as well as a predictor of cardiovascular disease morbidity and mortality [1]. Given the time limits of school curricula, adding a HIIT protocol to the PEC curriculum may help students increase their fitness levels and enhance their health.
Strengths and Limitations
This study has several strengths, including the randomized design, intervention applied to older adolescents, objectively and subjectively measured internal load and in a PEC real context without, interfering with other aspects of the curriculum. Adolescents, especially older ones, are underrepresented in studies implemented in the school context [28]. Notwithstanding the fact that some studies have been implemented in the school setting, only a few [9,27,35,36,37,38,39,40] were implemented in PEC, some of which replaced the entire session with the intervention [9,40]. Adjusting exercise intensity using HR has been a valid option, mainly in prolonged and submaximal periods. Few studies have objectively measured internal load by monitoring HR [9,10,28,38,39,57,58] or RPE [38,41]. HR has become one of the most used outcomes to assess intensity. Optimal exercise duration and rest intervals remain ambiguous and dose-response relationships of HIIT volume and intensity are unsettled. On adolescents, despite differences in protocols on intensity like all-out bouts or % of MAS, modality (sprints vs calisthenics), and volume (6min-35min/session), most of them opted for 1:1 density [25]. With this study, the authors aim to provide novel HIIT protocols for schools with less volume (only twice a week) and higher density (less rest in each interval), which include resistance exercises through calisthenic exercises and plyometrics that retain the health-enhancing effects and satisfy the adolescents’ desire for enjoyment and variety.
However, some limitations should also be acknowledged, such as the high missing values due to school activities, teaching breaks, weather conditions and lockdown, or the absence of a detailed evaluation to determine intervention fidelity to confirm treatment/protocol adherence. Due to the negative consequences of home confinement, we experienced a significant number of dropouts in several outcomes, so the primary analysis of the data set was not carried out according to the ‘intention to treat’ principle. These simple effects were examined either using separate independent repeated measurement analysis, such as t-tests or – where the analysis of the residuals suggested non-normality – using the non-parametric Wilcoxon’s signed ranks test. The mean attendance for participants involved in the intervention was 12.2 ± 3.5 (47%) of the 26 scheduled exercise sessions. If there had been a higher participation rate, perhaps the differences between baseline and post-intervention and between groups would have been more pronounced as was noted in other studies [9,24,37,38,40]. One of the gaps in HIIT research is the small number of volunteers and the short duration of interventions so that significant impacts on public health can be inferred [59]. However, in a school context, more than seven weeks can be problematic due to activities and teaching breaks provided for in planning and the school calendar [9]. Although we planned to include a pre- and post-nutrition control and a PA enjoyment scale, home confinement did not allow that assessment.
5. Conclusions
Despite the extremely low volume (on average, 10 min/week), brief whole-body HIIT over 16 weeks can improve CRF and muscular fitness in adolescent girls. It should be noted that there is no need for external loads to implement these protocols; the use of all-out bouts and plyometrics are also simple approaches. The actual PEC time is still restricted due to activities and teaching breaks, as well as absences due to illness, medical appointments, and a lack of appropriate clothing, making it difficult to find content that can positively influence healthy physical fitness in students due to an objective lack of time. Replacing the traditional warm-up without interfering with other curricular content provided in PEC with this time-efficient approach could have a prominent role in improving female students’ CRF. Investigations of dose-response relationships and the potential upper limits of HIIT volume and intensity are unsettled and highly relevant for healthy and clinical populations. Since HIIT did not improve CRF in boys, we recommend increasing the intensity and frequency of this type of exercise.
Author Contributions
Conceptualization, A.B., L.C. and A.R.; methodology, L.C. and A.R.; software, A.B. validation, A.B. and A.R.; formal analysis, A.B. and L.C. investigation, A.B. and A.R.; resources, A.B. and L.C.; data curation, A.B. and A.R.; writing original draft preparation, A.B.; writing review and editing, A.B., L.C. and A.R.; visualization, A.B., L.C. and A.R.; supervision, L.C. and A.R.; project administration, A.B., L.C. and A.R.; funding acquisition, A.B., L.C. and A.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Portuguese national funding agency for science, research, and technology, Fundação para a Ciência e Tecnologia, grant number SFRH/BD/136869/2018.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Ethics Committee of the University of Évora (doc. 19017, 10 June 2019).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are not publicly available due to participants privacy protection but are available from the corresponding author on reasonable request.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
References
- Carnethon, M.R.; Gidding, S.S.; Nehgme, R.; Sidney, S.; Jacobs, J., David R.; Liu, K. Cardiorespiratory Fitness in Young Adulthood and the Development of Cardiovascular Disease Risk Factors. JAMA 2003, 290, 3092–3100. [CrossRef]
- Logan, G.R.; Harris, N.; Duncan, S.; Schofield, G. A review of adolescent high-intensity interval training. Sports Med 2014, 44, 1071–1085. [Google Scholar] [CrossRef] [PubMed]
- Dias, K.A.; Coombes, J.S.; Green, D.J.; Gomersall, S.R.; Keating, S.E.; Tjonna, A.E.; Hollekim-Strand, S.M.; Hosseini, M.S.; Ro, T.B.; Haram, M.; et al. Effects of exercise intensity and nutrition advice on myocardial function in obese children and adolescents: a multicentre randomised controlled trial study protocol. BMJ Open 2016, 6, e010929. [Google Scholar] [CrossRef] [PubMed]
- Herget, S.; Reichardt, S.; Grimm, A.; Petroff, D.; Kapplinger, J.; Haase, M.; Markert, J.; Bluher, S. High-Intensity Interval Training for Overweight Adolescents: Program Acceptance of a Media Supported Intervention and Changes in Body Composition. Int J Environ Res Public Health 2016, 13. [Google Scholar] [CrossRef]
- Logan, G.R.; Harris, N.; Duncan, S.; Plank, L.D.; Merien, F.; Schofield, G. Low-Active Male Adolescents: A Dose Response to High-Intensity Interval Training. Med Sci Sports Exerc 2016, 48, 481–490. [Google Scholar] [CrossRef] [PubMed]
- Marques, A.; Calmeiro, L.; Loureiro, N.; Frasquilho, D.; de Matos, M.G. Health complaints among adolescents: Associations with more screen-based behaviours and less physical activity. J Adolesc 2015, 44, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Bluher, S.; Kapplinger, J.; Herget, S.; Reichardt, S.; Bottcher, Y.; Grimm, A.; Kratzsch, J.; Petroff, D. Cardiometabolic risk markers, adipocyte fatty acid binding protein (aFABP) and the impact of high-intensity interval training (HIIT) in obese adolescents. Metabolism 2017, 68, 77–87. [Google Scholar] [CrossRef] [PubMed]
- Lau, P.W.C.; Wong, D.P.; Ngo, J.K.; Liang, Y.; Kim, C.G.; Kim, H.S. Effects of high-intensity intermittent running exercise in overweight children. European Journal of Sport Science 2015, 15, 182–190. [Google Scholar] [CrossRef] [PubMed]
- Martin-Smith, R.; Buchan, D.S.; Baker, J.S.; Macdonald, M.J.; Sculthorpe, N.F.; Easton, C.; Knox, A.; Grace, F.M. Sprint Interval Training and the School Curriculum: Benefits Upon Cardiorespiratory Fitness, Physical Activity Profiles, and Cardiometabolic Risk Profiles of Healthy Adolescents. Pediatric exercise science 2019, 31, 296–305. [Google Scholar] [CrossRef]
- Cvetkovic, N.; Stojanovic, E.; Stojiljkovic, N.; Nikolic, D.; Scanlan, A.T.; Milanovic, Z. Exercise training in overweight and obese children: Recreational football and high-intensity interval training provide similar benefits to physical fitness. Scand J Med Sci Sports 2018, 28 Suppl 1, 18–32. [Google Scholar] [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports Med 2020, 54, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Courneya, K.S. Efficacy, effectiveness, and behavior change trials in exercise research. International Journal of Behavioral Nutrition and Physical Activity 2010, 7, 81. [Google Scholar] [CrossRef]
- Wen, C.P.; Wai, J.P.; Tsai, M.K.; Yang, Y.C.; Cheng, T.Y.; Lee, M.C.; Chan, H.T.; Tsao, C.K.; Tsai, S.P.; Wu, X. Minimum amount of physical activity for reduced mortality and extended life expectancy: a prospective cohort study. Lancet 2011, 378, 1244–1253. [Google Scholar] [CrossRef]
- Kong, Z.; Sun, S.; Liu, M.; Shi, Q. Short-Term High-Intensity Interval Training on Body Composition and Blood Glucose in Overweight and Obese Young Women. Journal of diabetes research 2016, 2016, 4073618. [Google Scholar] [CrossRef]
- Zhang, H.; Tong, T.K.; Qiu, W.; Zhang, X.; Zhou, S.; Liu, Y.; He, Y. Comparable Effects of High-Intensity Interval Training and Prolonged Continuous Exercise Training on Abdominal Visceral Fat Reduction in Obese Young Women. Journal of diabetes research 2017, 2017, 9. [Google Scholar] [CrossRef]
- Kilian, Y.; Engel, F.; Wahl, P.; Achtzehn, S.; Sperlich, B.; Mester, J. Markers of biological stress in response to a single session of high-intensity interval training and high-volume training in young athletes. Eur J Appl Physiol 2016, 116, 2177–2186. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Hermoso, A.; Cerrillo-Urbina, A.J.; Herrera-Valenzuela, T.; Cristi-Montero, C.; Saavedra, J.M.; Martinez-Vizcaino, V. Is high-intensity interval training more effective on improving cardiometabolic risk and aerobic capacity than other forms of exercise in overweight and obese youth? A meta-analysis. Obes Rev 2016, 17, 531–540. [Google Scholar] [CrossRef]
- Harris, N.K.; Dulson, D.K.; Logan, G.R.M.; Warbrick, I.B.; Merien, F.L.R.; Lubans, D.R. Acute Responses to Resistance and High-Intensity Interval Training in Early Adolescents. J Strength Cond Res 2017, 31, 1177–1186. [Google Scholar] [CrossRef]
- Lazzer, S.; Tringali, G.; Caccavale, M.; De Micheli, R.; Abbruzzese, L.; Sartorio, A. Effects of high-intensity interval training on physical capacities and substrate oxidation rate in obese adolescents. J Endocrinol Invest 2017, 40, 217–226. [Google Scholar] [CrossRef]
- Fisher, G.; Schwartz, D.D.; Quindry, J.; Barberio, M.D.; Foster, E.B.; Jones, K.W.; Pascoe, D.D. Lymphocyte enzymatic antioxidant responses to oxidative stress following high-intensity interval exercise. J Appl Physiol (1985) 2011, 110, 730–737. [Google Scholar] [CrossRef]
- Gibala, M.J.; Jones, A.M. Physiological and performance adaptations to high-intensity interval training. Nestle Nutrition Institute workshop series 2013, 76, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Stuckey, M.I.; Tordi, N.; Mourot, L.; Gurr, L.J.; Rakobowchuk, M.; Millar, P.J.; Toth, R.; MacDonald, M.J.; Kamath, M.V. Autonomic recovery following sprint interval exercise. Scand J Med Sci Sports 2012, 22, 756–763. [Google Scholar] [CrossRef]
- Sim, A.Y.; Wallman, K.E.; Fairchild, T.J.; Guelfi, K.J. Effects of High-Intensity Intermittent Exercise Training on Appetite Regulation. Med Sci Sports Exerc 2015, 47, 2441–2449. [Google Scholar] [CrossRef] [PubMed]
- Costigan, S.A.; Eather, N.; Plotnikoff, R.C.; Taaffe, D.R.; Lubans, D.R. High-intensity interval training for improving health-related fitness in adolescents: a systematic review and meta-analysis. Br J Sports Med 2015, 49, 1253–1261. [Google Scholar] [CrossRef] [PubMed]
- Eddolls, W.T.B.; McNarry, M.A.; Stratton, G.; Winn, C.O.N.; Mackintosh, K.A. High-Intensity Interval Training Interventions in Children and Adolescents: A Systematic Review. Sports medicine (Auckland, N.Z.) 2017, 47, 2363–2374. [Google Scholar] [CrossRef]
- Bond, B.; Cockcroft, E.J.; Williams, C.A.; Harris, S.; Gates, P.E.; Jackman, S.R.; Armstrong, N.; Barker, A.R. Two weeks of high-intensity interval training improves novel but not traditional cardiovascular disease risk factors in adolescents. Am J Physiol Heart Circ Physiol 2015, 309, H1039–H1047. [Google Scholar] [CrossRef]
- Costigan, S.A.; Eather, N.; Plotnikoff, R.C.; Taaffe, D.R.; Pollock, E.; Kennedy, S.G.; Lubans, D.R. Preliminary efficacy and feasibility of embedding high intensity interval training into the school day: A pilot randomized controlled trial. Preventive medicine reports 2015, 2, 973–979. [Google Scholar] [CrossRef]
- Leahy, A.A.; Eather, N.; Smith, J.J.; Hillman, C.H.; Morgan, P.J.; Plotnikoff, R.C.; Nilsson, M.; Costigan, S.A.; Noetel, M.; Lubans, D.R. Feasibility and Preliminary Efficacy of a Teacher-Facilitated High-Intensity Interval Training Intervention for Older Adolescents. Pediatric exercise science 2019, 31, 107–117. [Google Scholar] [CrossRef]
- Lee, S.; Bacha, F.; Hannon, T.; Kuk, J.L.; Boesch, C.; Arslanian, S. Effects of aerobic versus resistance exercise without caloric restriction on abdominal fat, intrahepatic lipid, and insulin sensitivity in obese adolescent boys: a randomized, controlled trial. Diabetes 2012, 61, 2787–2795. [Google Scholar] [CrossRef]
- Weston, K.L.; Azevedo, L.B.; Bock, S.; Weston, M.; George, K.P.; Batterham, A.M. Effect of Novel, School-Based High-Intensity Interval Training (HIT) on Cardiometabolic Health in Adolescents: Project FFAB (Fun Fast Activity Blasts) - An Exploratory Controlled Before-And-After Trial. PLoS One 2016, 11, e0159116. [Google Scholar] [CrossRef]
- Lonsdale, C.; Rosenkranz, R.R.; Peralta, L.R.; Bennie, A.; Fahey, P.; Lubans, D.R. A systematic review and meta-analysis of interventions designed to increase moderate-to-vigorous physical activity in school physical education lessons. Preventive Medicine 2013, 56, 152–161. [Google Scholar] [CrossRef]
- Mura, G.; Rocha, N.B.F.; Helmich, I.; Budde, H.; Machado, S.; Wegner, M.; Nardi, A.E.; Arias-Carrión, O.; Vellante, M.; Baum, A.; et al. Physical activity interventions in schools for improving lifestyle in European countries. Clin Pract Epidemiol Ment Health 2015, 11, 77–101. [Google Scholar] [CrossRef] [PubMed]
- Sharp, C.A.; McNarry, M.A.; Eddolls, W.T.B.; Koorts, H.; Winn, C.O.N.; Mackintosh, K.A. Identifying facilitators and barriers for adolescents participating in a school-based HIIT intervention: the eXercise for asthma with commando Joe's® (X4ACJ) programme. BMC Public Health 2020, 20, 609. [Google Scholar] [CrossRef]
- Tottori, N.; Morita, N.; Ueta, K.; Fujita, S. Effects of High Intensity Interval Training on Executive Function in Children Aged 8-12 Years. International journal of environmental research and public health 2019, 16, 4127. [Google Scholar] [CrossRef]
- Bogataj, Š.; Trajković, N.; Cadenas-Sanchez, C.; Sember, V. Effects of School-Based Exercise and Nutrition Intervention on Body Composition and Physical Fitness in Overweight Adolescent Girls. Nutrients 2021, 13. [Google Scholar] [CrossRef]
- Ketelhut, S.; Kircher, E.; Ketelhut, S.R.; Wehlan, E.; Ketelhut, K. Effectiveness of Multi-activity, High-intensity Interval Training in School-aged Children. Int J Sports Med 2020, 41, 227–232. [Google Scholar] [CrossRef]
- Buchan, D.S.; Young, J.D.; Simpson, A.D.; Thomas, N.E.; Cooper, S.M.; Baker, J.S. The effects of a novel high intensity exercise intervention on established markers of cardiovascular disease and health in Scottish adolescent youth. J Public Health Res 2012, 1, 155–157. [Google Scholar] [CrossRef]
- Alonso-Fernández, D.; Fernández-Rodríguez, R.; Taboada-Iglesias, Y.; Gutiérrez-Sánchez, Á. Impact of a HIIT protocol on body composition and VO2max in adolescents. Science & Sports 2019. [Google Scholar] [CrossRef]
- Costigan, S.A.; Ridgers, N.D.; Eather, N.; Plotnikoff, R.C.; Harris, N.; Lubans, D.R. Exploring the impact of high intensity interval training on adolescents' objectively measured physical activity: Findings from a randomized controlled trial. Journal of Sports Sciences 2018, 36, 1087–1094. [Google Scholar] [CrossRef]
- Martin, R.; Buchan, D.S.; Baker, J.S.; Young, J.; Sculthorpe, N.; Grace, F.M. Sprint interval training (SIT) is an effective method to maintain cardiorespiratory fitness (CRF) and glucose homeostasis in Scottish adolescents. Biology of sport 2015, 32, 307–313. [Google Scholar] [CrossRef]
- Engel, F.A.; Wagner, M.O.; Schelhorn, F.; Deubert, F.; Leutzsch, S.; Stolz, A.; Sperlich, B. Classroom-Based Micro-Sessions of Functional High-Intensity Circuit Training Enhances Functional Strength but Not Cardiorespiratory Fitness in School Children-A Feasibility Study. Front. Public Health 2019, 7, 9. [Google Scholar] [CrossRef]
- Laurent, C.M.; Vervaecke, L.S.; Kutz, M.R.; Green, J.M. Sex-specific responses to self-paced, high-intensity interval training with variable recovery periods. J Strength Cond Res 2014, 28, 920–927. [Google Scholar] [CrossRef]
- Henriques-Neto, D.; Minderico, C.; Peralta, M.; Marques, A.; Sardinha, L.B. Test–retest reliability of physical fitness tests among young athletes: The FITescola® battery. Clinical Physiology and Functional Imaging 2020, 40, 173–182. [Google Scholar] [CrossRef]
- Tabata, I.; Nishimura, K.; Kouzaki, M.; Hirai, Y.; Ogita, F.; Miyachi, M.; Yamamoto, K. Effects of moderate-intensity endurance and high-intensity intermittent training on anaerobic capacity and VO2max. Med Sci Sports Exerc 1996, 28, 1327–1330. [Google Scholar] [CrossRef] [PubMed]
- Hanssen, H.; Nussbaumer, M.; Moor, C.; Cordes, M.; Schindler, C.; Schmidt-Trucksass, A. Acute effects of interval versus continuous endurance training on pulse wave reflection in healthy young men. Atherosclerosis 2015, 238, 399–406. [Google Scholar] [CrossRef]
- Helgerud, J.; Hoydal, K.; Wang, E.; Karlsen, T.; Berg, P.; Bjerkaas, M.; Simonsen, T.; Helgesen, C.; Hjorth, N.; Bach, R.; et al. Aerobic high-intensity intervals improve VO2max more than moderate training. Med Sci Sports Exerc 2007, 39, 665–671. [Google Scholar] [CrossRef]
- Bonsu, B.; Terblanche, E. The training and detraining effect of high-intensity interval training on post-exercise hypotension in young overweight/obese women. Eur J Appl Physiol 2016, 116, 77–84. [Google Scholar] [CrossRef]
- Buchheit, M.; Laursen, P.B. High-intensity interval training, solutions to the programming puzzle: Part I: cardiopulmonary emphasis. Sports Med 2013, 43, 313–338. [Google Scholar] [CrossRef]
- Borg, G. Perceived exertion as an indicator of somatic stress. Scandinavian journal of rehabilitation medicine 1970, 2, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.G.; Eston, R.G.; Stretch, C. Use of the Rating of Perceived Exertion to Control Exercise Intensity in Children. 1991, 3, 21. [CrossRef]
- Krustrup, P.; Mohr, M.; Amstrup, T.; Rysgaard, T.; Johansen, J.; Steensberg, A.; Pedersen, P.K.; Bangsbo, J. The yo-yo intermittent recovery test: physiological response, reliability, and validity. Med Sci Sports Exerc 2003, 35, 697–705. [Google Scholar] [CrossRef] [PubMed]
- Jackson, A.S.; Pollock, M.L.; Graves, J.E.; Mahar, M.T. Reliability and validity of bioelectrical impedance in determining body composition. J Appl Physiol (1985) 1988, 64, 529–534. [Google Scholar] [CrossRef] [PubMed]
- Fritz, C.O.; Morris, P.E.; Richler, J.J. Effect size estimates: current use, calculations, and interpretation. Journal of experimental psychology. General 2012, 141, 2–18. [Google Scholar] [CrossRef] [PubMed]
- MacInnis, M.J.; Zacharewicz, E.; Martin, B.J.; Haikalis, M.E.; Skelly, L.E.; Tarnopolsky, M.A.; Murphy, R.M.; Gibala, M.J. Superior mitochondrial adaptations in human skeletal muscle after interval compared to continuous single-leg cycling matched for total work. The Journal of physiology 2017, 595, 2955–2968. [Google Scholar] [CrossRef]
- Kristensen, D.E.; Albers, P.H.; Prats, C.; Baba, O.; Birk, J.B.; Wojtaszewski, J.F. Human muscle fibre type-specific regulation of AMPK and downstream targets by exercise. The Journal of physiology 2015, 593, 2053–2069. [Google Scholar] [CrossRef]
- Vaccari, F.; Giovanelli, N.; Lazzer, S. High-intensity decreasing interval training (HIDIT) increases time above 90%VO2peak. Eur J Appl Physiol 2020, 120, 2397–2405. [Google Scholar] [CrossRef]
- Buchan, D.S.; Ollis, S.; Young, J.D.; Cooper, S.M.; Shield, J.P.; Baker, J.S. High intensity interval running enhances measures of physical fitness but not metabolic measures of cardiovascular disease risk in healthy adolescents. BMC Public Health 2013, 13, 498. [Google Scholar] [CrossRef]
- Racil, G.; Ben Ounis, O.; Hammouda, O.; Kallel, A.; Zouhal, H.; Chamari, K.; Amri, M. Effects of high vs. moderate exercise intensity during interval training on lipids and adiponectin levels in obese young females. Eur J Appl Physiol 2013, 113, 2531–2540. [Google Scholar] [CrossRef]
- Biddle, S.J.H.; Batterham, A.M. High-intensity interval exercise training for public health: a big HIT or shall we HIT it on the head? International Journal of Behavioral Nutrition and Physical Activity 2015, 12, 95. [Google Scholar] [CrossRef]
Figure 1.
Study design.
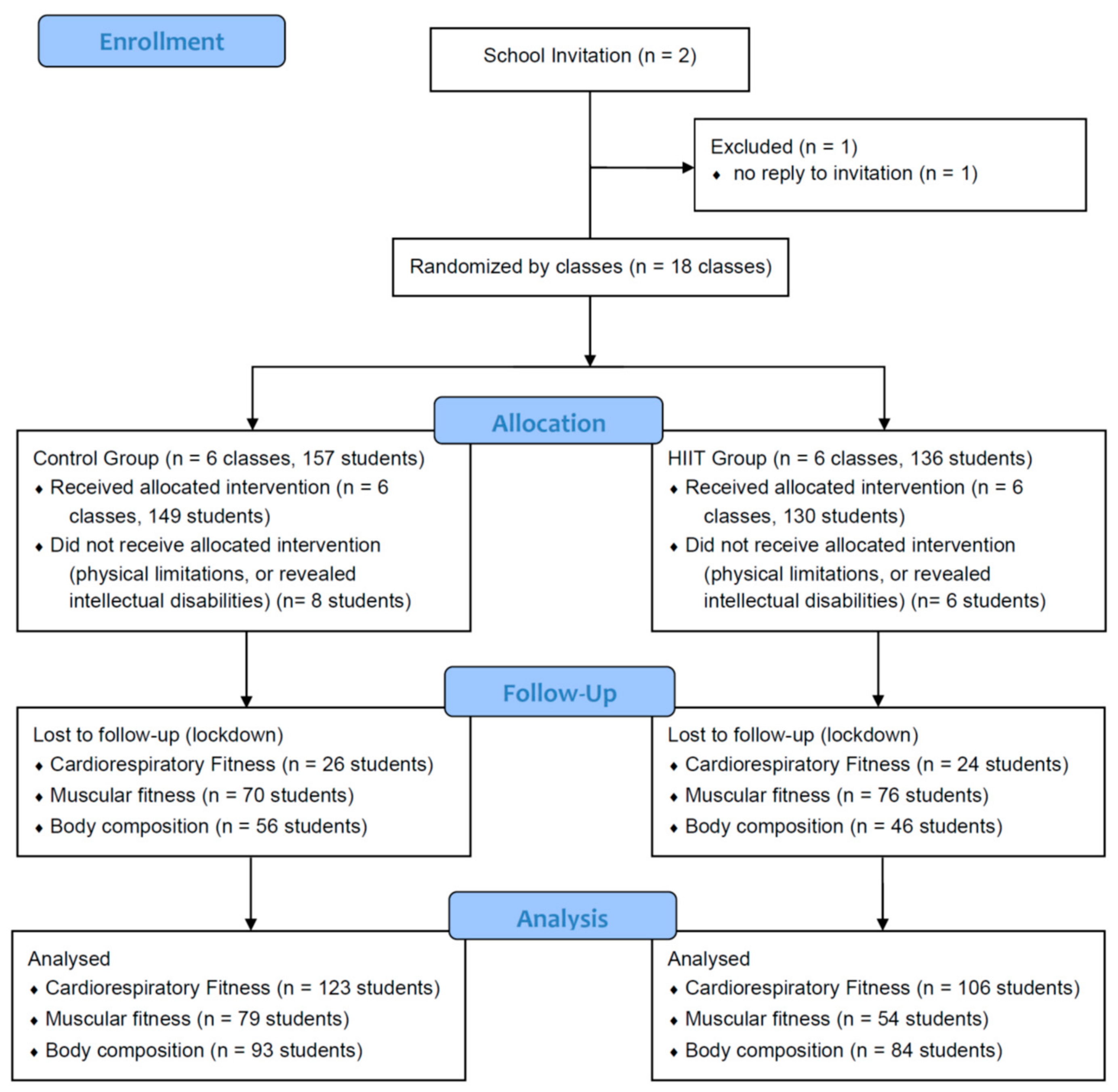
Figure 2.
Graphical description of an example session (Figure produced by the author).
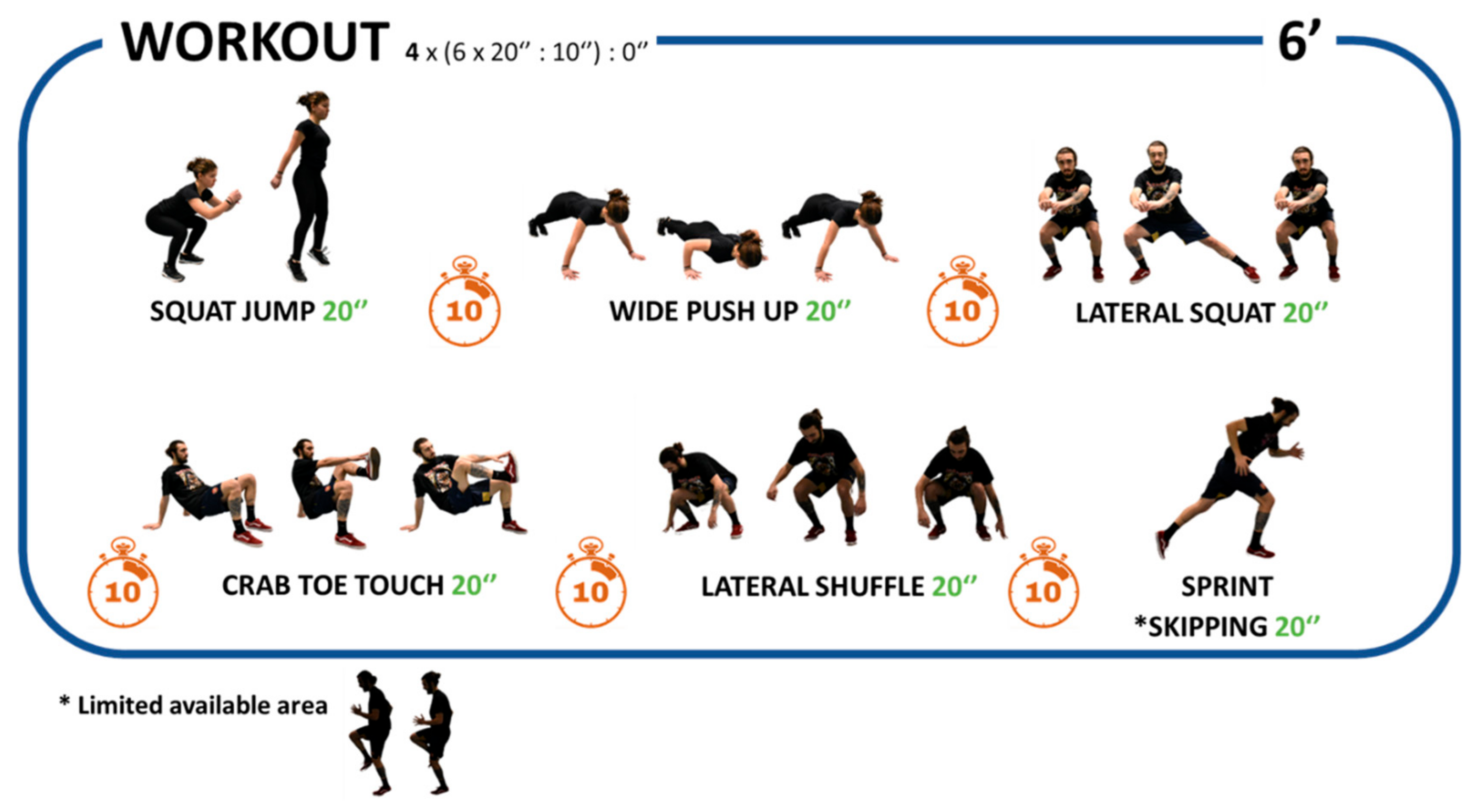
Figure 3.
Graphical description of an example session (couples) (Figure produced by the author).
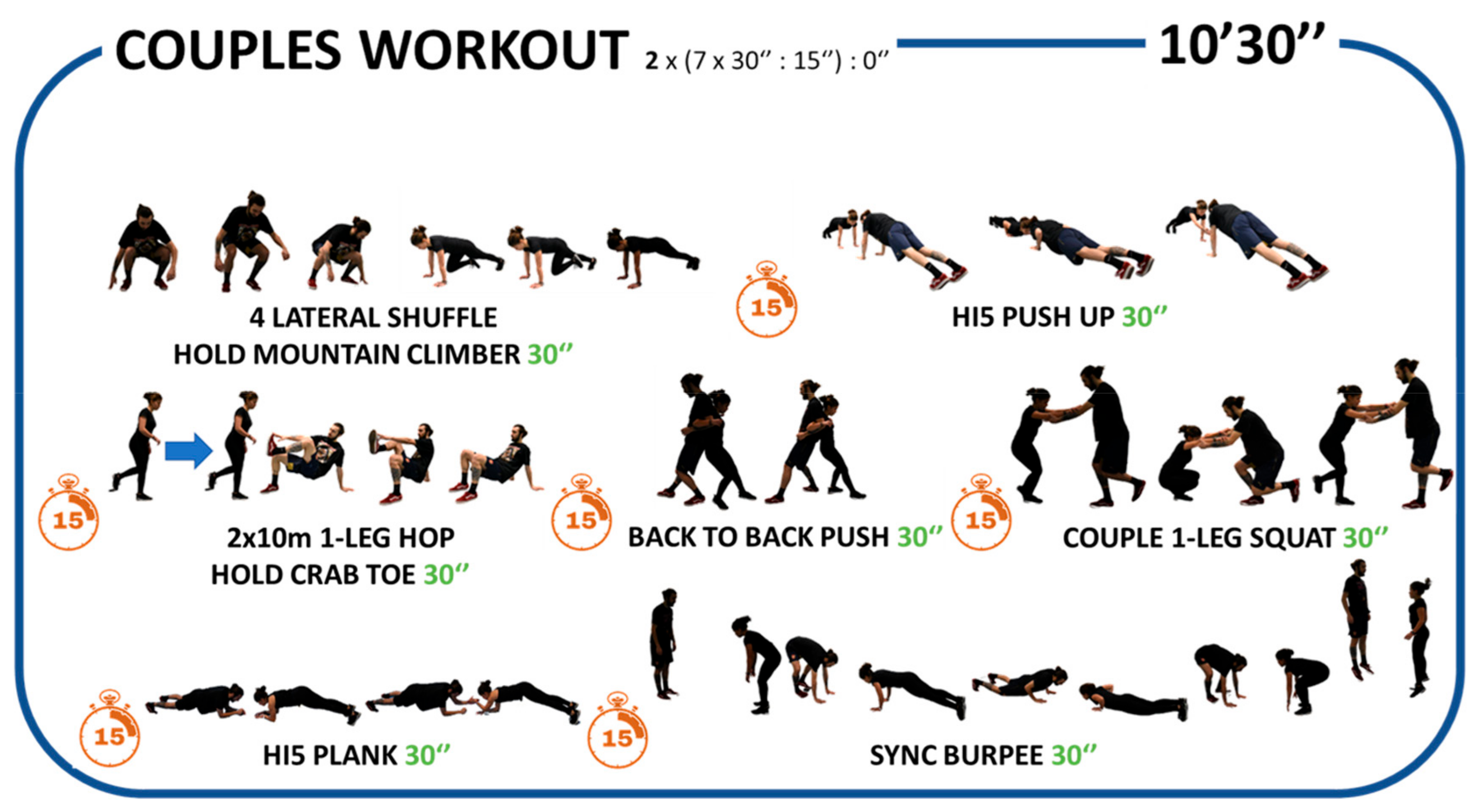
Figure 4.
Schedule of assessment and HIIT intervention. (‘) Total work in minutes, (‘’:’’) ratio ON:OFF in seconds.
Figure 4.
Schedule of assessment and HIIT intervention. (‘) Total work in minutes, (‘’:’’) ratio ON:OFF in seconds.
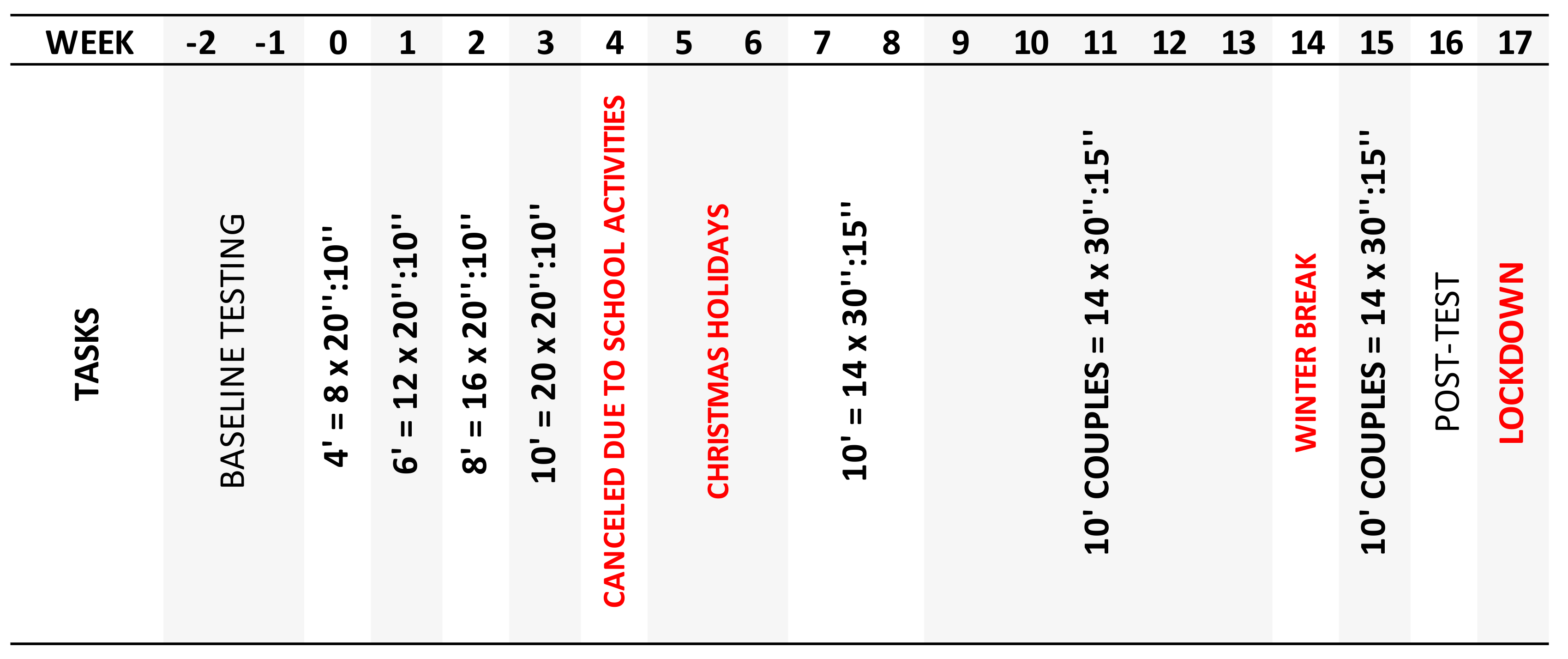

Table 1.
Training load of HIIT Intervention.
| HIIT | |||
|---|---|---|---|
| Total (n =106) |
Girls (n =55) |
Boys (n =51) |
|
| Planned Sessions (n) | 26 | ||
| Sessions, mean (sd) | 12.2 (3.5) | 12.2 (3.6) | 12.2 (3.4) |
| Time in seconds >90%HRmáx/session, mean (sd) | 179.9 (128.2)§ | 221.6 (127.8) | 132.9 (112.4) |
| RPE/session, mean (sd) | 17.4 (0.7) | 17.6 (1.5) | 17.4 (0.7) |
Abbreviations: HR: heart rate; RPE: rating perceived exertion. Note: Values are presented as mean (SD). § p < 0.001.
Table 2.
Characteristics of physical fitness and body composition variables: Control group and HIIT at baseline and post-intervention.
Table 2.
Characteristics of physical fitness and body composition variables: Control group and HIIT at baseline and post-intervention.
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



