
Submitted:
29 August 2024
Posted:
29 August 2024
You are already at the latest version
Abstract
This study investigated the prevalence and associated risk factors of Lower Back Pain (LBP) among medical students of Alfaisal University, Riyadh, Saudi Arabia. A cross-sectional style was employed where 331 medical students were evaluated using the Oswestry Disability Index (ODI) supplemented with demographic and lifestyle questions. Data analysis allowed identification of LBP-risk factor relationships. The study revealed a 73.4% prevalence of LBP among Alfaisal University medical students with a 4.61 average severity. Female students, those who spent long hours on computers, and those who did not exercise were more likely to experience LBP. Higher disability degree was associated with participants aged >21, used their devices for extended periods, and insufficient sleep. LBP is highly prevalent with several risk factors existing. These findings highlight the need for targeted interventions such as ergonomic/lifestyle improvements and reduced device use.
Keywords:
Lower Back Pain
; Medical Students
; Saudi Arabia
; Prevalence
; Oswestry Disability Index
; Ergonomics
; Physical Activity
; Risk Factors
; Disability
Introduction
Lower back pain (LBP) is a highly prevalent condition that affects a large number of people around the world throughout their lifetime, including medical students. This lower back pain is defined as the pain that affects the lumbar region of the back that begins below the ribcage and ends in the buttock region, often lasting for less than three months [1,2]. This type of pain can be a significant detriment to a person's quality of life and hinder activities, work performance, and mental wellbeing.
The global impact of LBP is staggering. It is currently the leading cause of years lived with disability, affecting 619 million people and leading to almost a combined 69 million years of disability [3]. The mean prevalence of lower back pain globally ranges from 8-31% according to various studies, varying significantly with regards to age, gender, and region [4,5]. This widespread issue represents potentially massive economic losses in all sectors, especially the healthcare sector.
LBP accounted for the one of the topmost reasons workers consult their physicians for, costing both money and time [6,7]. In high-income countries, the total costs associated with LBP can be as high as €10.75 billion per population (2.6b direct and 8.15b indirect), costing individual patients up to $10,143 over the course of the pain [8]. In middle and low-income countries, these costs were found to be even higher on a per-patient basis [9].
Among specific demographic identifiers of patients, the prevalence of LBP becomes more variable. The prevalence of LBP among teenagers (years 13-18) sits at about 19%, in university students it rises to around 60-80% [10,11]. Multiple studies have seen a discrepancy among females and males–with females having higher prevalence rates than males, ranging from 1-10% higher than males across all settings [5,12]. In all, back pain is on the increase across all demographics and will continue to represent a significant cause of disability in the global population–estimated to increase by almost 36.4% new cases of lower back pain (although the total prevalence rate is expected to decrease slightly from 7.30% to 7.08) [5].
Several factors contribute to the development of LBP, with both behavioral and psychological etiologies playing a role. Interestingly, less than 1% of LBP cases presenting to primary care clinics have diagnosed pathological causes as seen in one study [13]. As such, the vast majority of LBP cases remain idiopathic and/or multifactorial rather than associated with one specific etiology [14]. The main mechanism of developing LBP is a disturbance to the natural curvature of the spine. Factors such as increased BMI, obesity, poor sitting and standing posture, poor lumbar support, sedentary lifestyle, poor exercise regime, and insufficient sleep all contribute to an increased risk of developing LBP [2,15].
The point prevalence of LBP among Saudi university students was shown to range from 22-66% in two recent studies tallying students from both province-specific universities and across Saudi Arabia [12,16]. With regards to Saudi medical students this has been seen to be anywhere from 80-94% among three studies from separate medical colleges across the Kingdom of Saudi Arabia [17,18,19].
Among the general population, medical students are particularly susceptible to LBP due to their long hours of study and sedentary lifestyle caused by the increased curriculum rigor. All being potential factors that can predispose them to developing a sedentary, study-based lifestyle that can increase the likelihood of developing back pain [20]. It is critical to further understand LBP in this cohort, as medical students are a significant part of the health system and point of access between patient and the healthcare system [21]. As such, the significant loss of productivity and gain of disability due to LBP in medical students and healthcare workers (HCWs) is critical to consider when looking at losses in the healthcare system.
However, the question of whether being a medical student itself is the factor at play or whether it is any extraneous disturbances to a normal healthy state caused by a shifting to medical curricula then arises. Medical students themselves undergo significant lifestyle changes to adapt to the curriculum which often go unexplored in a majority of studies regarding lower back pain.
Previous studies on this issue were able to reach conclusions on prevalence rates among general university students and medical students however gaps exist in understanding the exact mechanism behind high rates of LBP. Alshehri et. al’s study does not analyze medical students themselves and as such the demographic factors are limited in activities that medical students are specifically more prone to [12]. Aljohani et al. extends off of Alshehri’s study by utilizing the Oswestry Disability Index (ODI) questionnaire but again does not account for study degree [16]. Alwashmi et.al and Alrabai et. al’s studies analyzes the lifestyle factors that can affect LBP prevalence in medical students but does not extend this to the severity of this disability and the correlation of factors on degree of disability by using an index/tool like previous studies [17,18].
Given these gaps in the existing research, there remains a significant need to understand the role of various lifestyle and demographic factors on the prevalence and severity of LBP in medical university students in Saudi Arabia. This study seeks to address these knowledge gaps by examining both novel and previously studied factors implicated with LBP. By investigating the prevalence and severity of lower back pain among the medical students of Alfaisal University and its relation to various factors, this research aims to provide a more comprehensive understanding of LBP in this population. The study will employ the Oswestry Disability Index (ODI) to assess the degree of disability, coupling an examination of LBP with an analysis of its severity in the studied population.
To guide this investigation, the authors formulated the following hypotheses:
H0: There is no statistically significant association/difference between the presence of lower back pain/Oswestry Index score and the variables analyzed. This is if the p-value is found to be above or equal to 0.05.
HA: There is a statistically significant association/difference between the presence of lower back pain/Oswestry Index score and the variables analyzed. This is if the p-value is found to be below 0.05.
Through this comprehensive approach, the study aims to contribute valuable insights to the understanding of LBP among medical students, potentially informing future interventions and preventive measures in this crucial population.
2. Materials and Methods
2.1. Study Design
This cross-sectional study was conducted at Alfaisal University from March to April 2024, involving medical students from Years 1-5, if they consented to participate. The authors opted for a cross-sectional design due to its efficiency in collecting data from a large sample simultaneously, which is particularly advantageous given the busy schedules of medical students. This study utilized STROBE cross-sectional study guidelines and adhered to them.
2.2. Study Eligibility Criteria
Participants were eligible to be considered in this study if they were:
- Currently Enrolled Medical Students at Alfaisal University (Years 1-5, MBBS program)
- Consented to the study IRB disclosure agreement
2.3. Study Sample
The target population for this study comprised all medical students at Alfaisal University in Riyadh (approximately 1200 students). Multiple channels were used to maximize recruitment including emails, broadcast messages, and in-person invitations through QR codes of the study form. Reminders were sent to encourage students' participation.
2.4. Sample Size Calculation
To ensure statistical validity, the authors calculated the required sample size, for a precision of 5% and a prevalence of 50% in a population of 1200 students. A minimum required sample of 292 participants was yielded based on a 95% confidence interval (CI). This calculation was performed utilizing the sample size calculator available at https://www.calculator.net/sample-size-calculator.html. The final sample of 331 students exceeded this requirement, enhancing the study's statistical power.
2.5. Survey Instrument
The survey instrument comprised three main components:
- Author-developed questions: These were specifically designed to gather demographic information and explore factors potentially associated with lower back pain (LBP) among medical students. These questions were pilot tested on a group of 15 students which were not included in the study population and minor adjustments were done based on their feedback.
The Oswestry Disability Index (ODI) score calculation and interpretation that was applied included:
- The ODI score was calculated by summing the scores from all 10 questions, resulting in a total score ranging from 0 to 50.
- This total score was then used to determine the degree of LBP-related disability experienced by the respondent.
-
The interpretation of ODI scores is as follows:
- 0-4: No disability
- 5-14: Mild disability
- 5-24: Moderate disability
- 25-34: Severe disability
- 35-50: Complete disability
By combining these validated tools with custom questions, the authors aimed to comprehensively assess both the prevalence and severity of LBP among Alfaisal University medical students, as well as identify potential risk factors associated with this condition.
2.6. Data Collection
Data was collected via a Google form distributed to students through multiple modalities, such as in person pop-ups where participants anonymously filled out their data, through university-wide broadcast emails, and social media platforms such as WhatsApp. The data collection duration lasted approximately one month, from March to April 2024. Participants were assured of the confidentiality of their responses, which were strictly for research purposes and guided by the strict protocols by the university's ethics board. The survey automatically excluded non-medical students, ensuring that only the target population, Alfaiasl University College of Medicine students could proceed to complete the survey.
2.7. Statistical Analysis
Data was first stored, cleaned, and then imported into Google Sheets for analysis using IBM SPSS Statistics software. Responses that did not consent to the disclosure agreement in addition to improperly filled/missing responses were discarded. To conduct hypothesis testing, Chi-squared analysis was utilized to identify associations between categorical demographics and the occurrence of lower back pain (LBP) and further analysis regarding the role of gender among significant determinants of LBP. As for assessing the relationship between mean Oswestry Disability Index (ODI) scores and demographic factors, we conducted Analysis of Variance (ANOVA) and t-tests. Regression analysis was carried out on variables like age with adjustments made for variables. In this study we set an alpha value of 0.05 considering results with p<0.05 being considered as significant. This thorough analytical approach allowed us to deeply explore the associations between various factors and LBP among students.
2.8. Ethical Considerations
The respondents were surveyed through an anonymous Google Forms survey tool that did not collect any form of identifier apart from the examined variables for the study. All data was stored on a secure server only accessible to the study team and data will be destroyed following the study conclusion. This study was conducted under the oversight of the Alfaisal institutional board.
This study was not funded by any entities nor did any of the authors possess any conflicts of interests.
3. Results
3.1. Descriptive Results
Over the course of the data collection period, 338 responses were gathered with 336 respondents consented to participate and of those only 331 providing complete responses. Thus formed our final study data sample of 331 students.
The respondents were from all five years of study of Alfaisal University and ranged from ages 17 to above 22. The average age of the respondent was 20, average BMI was around 23, and the responses displayed a high female:male ratio. Most students surveyed were in the 17-21 age range (n=278), with respondents primarily being concentrated in the first two years of Alfaisal University medical school (44.7% and 25.4% for study years 1 and 2 respectively). A significant majority of respondents were in the normal BMI range (57.7%), followed by those in the overweight category (23.9%) and small amounts of underweight and obese respondents (10.3% and 8.2% respectively) (Table 1).
As for the lifestyle of the respondents, a majority (51.4%) experienced lower back pain before beginning medical school. A supermajority of surveyed students also spend long hours on their computer/laptop for various purposes (94%). Regarding phone usage, a majority of students use their phone for an average of 2-5 hours (42.9%) with a sizable minority using it 5-8 hours a day (33.8%). Additionally, the majority of students exercise (50.1%) with the largest percentage exercising for more than five hours. Most students are not smokers, do not lift weights, and commute to university in less than 30 minutes. Most respondents sleep 4-6 hours (55.0), yielding an average sleep duration of 4.45 hours. The sitting position of respondents was also questioned, which revealed that most students lean forward when they sit in any situation (39.0). Regarding backpack usage and habits, the majority of respondents do regularly wear a backpack (40.2) however the second-largest contingent of students following backpack wearers is the group of students who wear a shoulder-bag or a crossbody (34.7) (Table 1).
Regarding lower back pain data, a significant majority of students did admit to suffering from lower back pain (LBP) in any capacity (73.4%, n=253). From a scale of 1-10 where 10 is the most severe, the average LBP severity was 4.61 out of 10 (Table 2).
3.2. Analytical Results
Table 3 includes the results of the chi-square analysis of the data. Various lifestyle and demographic factors were analyzed with regards to the presence or absence of lower back in participants.
Regarding the demographic profile of the participants, analysis discerned that there exists a statistically significant relationship between gender and the presence of LBP. LBP presence seems to strongly skew towards females rather than male participants (p= <0.001). There was no other statistically significant relationship in the demographics profile of the participants.
Surrounding the lifestyle factors and behaviors of the participants, numerous statistically-significant relationships exist. For instance, exercise and LBP also display a statistically significant relationship, however the duration of that exercise does not seem to have an association (p=0.001 and 0.287 respectively). Regarding exercise, lifting weights also displayed strong significance with back pain with larger numbers of weight-ligting participants possessing back-pain than their counterparts who do not (p= <0 .001). The duration of average daily phone use is also another important lifestyle factor noted in the analysis, with a slight relationship existing (p=0.042). Regarding the sitting position of participants, there is a strong relationship between it and LBP, with most participants leaning either forward or backward (p=0.014) . Additionally, participants’ habit of wearing backpacks, similar items, or not, displays a strong relationship with LBP (p=0.001). Most participants either wear a backpack or a shoulder bag/crossbody to university.
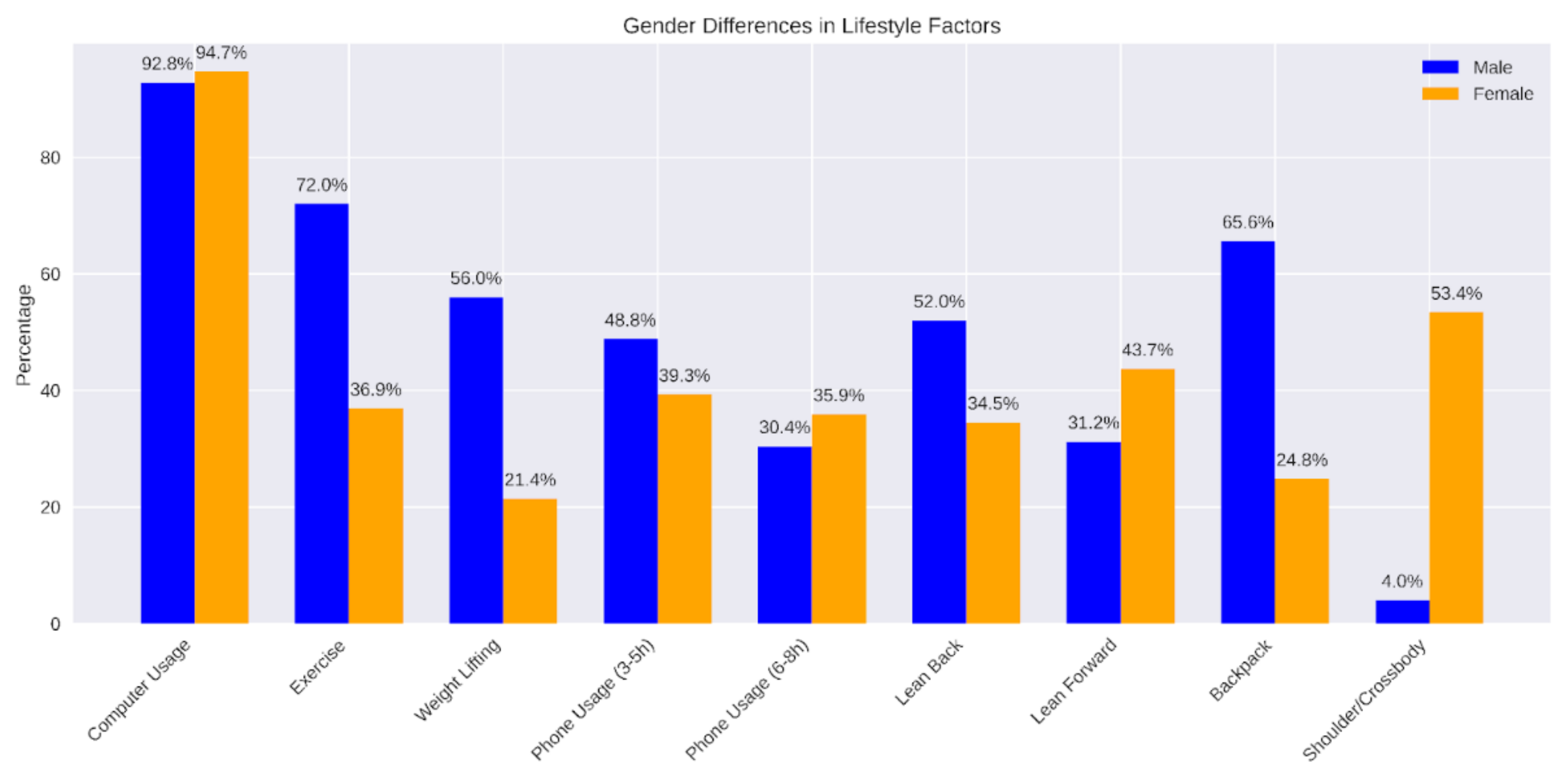
Following the chi-square analysis of how each factor relates to the presence or absence of lower back pain, a subsequent analysis focused on gender differences among the statistically-significant variables uncovered. (p<0.05). Gender was cross tabulated with factors such as exercise, lifting weights, average phone usage duration, sitting position, and backpack use. Figure 1 illustrates these gender-specific patterns.
Results revealed distinct patterns between male and female students (Table 4, Figure 1). Both genders reported high rates of long computer usage, with 92.8% of males and 94.7% of females spending extended periods on computers. However, significant disparities were observed in physical activities. Male students showed higher engagement in exercise (72.0% exercising regularly) compared to female students (only 36.9%). Similarly, weight lifting was more prevalent among males (56.0%) than females (21.4%).
Regarding daily phone usage, a higher percentage of male students (48.8%) reported using their phones for 3-5 hours compared to female students (39.3%). However, for 6-8 hours of daily usage, the trend reversed slightly with 35.9% of females versus 30.4% of males.
Sitting posture analysis indicated gender-specific preferences. Male students were more likely to lean back (52.0%) compared to female students (34.5%), while a higher proportion of female students (43.7%) tended to lean forward when seated versus male students (31.2%).
In terms of bag preferences, a stark contrast was observed. The majority of male students (65.6%) opted for backpacks, while only 24.8% of female students did so. Conversely, shoulder bags or crossbody bags were overwhelmingly preferred by female students (53.4%) compared to male students (4.0%).
Figure 2.
Gender Differences in Statistically Significant Lifestyle Factors and Behaviors.
The Oswestry Disability Index (ODI) was used to assess the level of disability that admitted to suffering from Lower back pain (LBP). As depicted in Table 5, the majority of respondents (56.9%, n=144) were classified as having "No Disability.”A substantial proportion (37.2%, n=94) fell into the "Mild Disability" category. A smaller fraction of participants were categorized with more significant impairment: 4.3% (n=11) showed "Moderate" disability, while only 1.6% (n=4) were classified with "Severe Disability". These findings suggest that while LBP was prevalent in the study population, the impact on daily functioning, as seen by the severity levels uncovered by the ODI, was relatively minimal for most participants. Over 94% of the respondents experienced either no disability or only mild disability, indicating that the majority of individuals with LBP in this study were able to manage their daily activities with little to no significant impairment (Table 5).
The respondents’ Oswestry Disability Index score (ODI scores) was also analyzed with regards to the various demographic and lifestyle factors using Analysis of Variance (ANOVA) and independent t-test statistical analyses, yielding mean ODI scores for each demographic and lifestyle factor in addition to the degree of statistical significance of those relationships. Most categories of factors were correlated with a mean ODI between 5-14 points–categorizing them as “low-disability” with small numbers of specific factors with mean scores below 5 leading to a categorization of “no-disability.”
The age range of the participants displayed statistically significant variance (p=0.08) between participants aged 17-21 and participants 22 years and over, with the former having an average ODI score of 4.86 (thus categorizing them as “No Disability” per the Oswestry Disability Index) and the latter 7.14 (“Mild Disability”). No other demographic factors displayed statistically significant variance among ODI scores.
Regarding demographic factors, a number of them displayed valid relationships with regards to average ODI scores. Firstly, participants who admitted to spending long hours on their displayed markedly higher Oswestry index scores compared to those who did not (5.47 vs. 1.57; p=0.008). Additionally, daily phone usage duration was shown to display statistically significant variance among participants–those who utilized their phones for less than an hour or more than 8 hours (10.75 for those >1 Hour and 7.21 for those 8+; p=0.28). Those who used their phones for intermediate durations had similar scores. Average sleep time of the participants was also shown to be statistically significant with regard to Mean ODI score, possessing an inverse relationship on ODI scores (p=0.023). These results are summarized in Table 6.
In order to further explore the relationship between age (as a continuous variable) and the Oswestry Disability Index (ODI) Score of the participants, a linear regression analysis was conducted with adjustment for the other statistically significant variables impacting Oswestry Disability Index Score (phone usage duration, spending long hours on devices, and sleep duration). Following adjustment of other statistically significant determinants of ODI scores uncovered through ANOVA and t-test analysis, the model displayed that age did indeed possess a statistically significant relationship on ODI score (p=0.026). Age was shown to have a positive correlation with Oswestry Disability Index score (ꞵ=.137), indicating that as age increases so too will ODI scores. Additionally, the regression model uncovered that duration of sleep had a negative relationship on the ODI score of participants (ꞵ=-.140; p=0.025), suggesting that sleeping more decreases ODI score while spending long hours increases ODI score due to the positive relationship uncovered (ꞵ=.170; p=0.006). Duration of phone usage did not meet the alpha of the study (p>0.05). These results are summarized in Table 7.
4. Discussion
4.1. General Discussion
Results of this study reveal that a significant number of students (73.4%) experience LBP, which is consistent with findings from previous studies worldwide. This discovery corresponds with research from a school in Bangladesh, where 63.3% of students reported LBP over a 12 month period [27]. Previous studies conducted in cities in Saudi Arabia have also shown a prevalence of LBP among medical students; for instance 82% at Qassim University [19]. However it is important to note that some studies have indicated rates of LBP among students, such as 33.3% and 20.8% at Taif University in Saudi Arabia and a similar study carried out in Serbia respectively [28,29]. These discrepancies could stem from the cross-sectional design of these studies potentially introducing biases along with variations in lifestyles, across different geographical regions.
This study found that among medical students, LBP is closely linked to a few factors; weightlifting (p<0.001), being female (p <0.001), physical activity (p =0.001), and carrying a backpack (p =0.001). It's noteworthy that the majority (70.8%) of students with LBP mentioned not participating in weightlifting even though some engaged in exercise. This intriguing discovery hints at an aspect of proper weightlifting against LBP. One possible explanation is that correct weightlifting techniques could help strengthen the back and core muscles potentially reducing or preventing LBP [30].
This study also revealed that most medical students suffering from LBP carry a backpack at least occasionally. This finding is consistent with a previous study on college students, which demonstrated a significant association between regular backpack use and increased chance of experiencing LBP (p =0.044) [31].
This study also indicates a strong and significant association between LBP and gender (p= <0.001), showing that more female than male medical students are affected. This is consistent with a previous study that also found a strong association between gender and LBP (p=0.000), with female students being more prone to LBP than male students [26]. Female risk factors for LBP were not examined thoroughly in the past, with previous studies stating that females could face higher risks of LBP due to the nature of the female gender (hormonal fluctuations) and bad postures [18,26]. To further understand why females are at higher risk for having LBP, the authors of this study ran a cross-tabulation between gender and all statistically significant variables. It was found that 78.8% of participants who do not exercise are females, and that 74.7% of participants who do not lift weights are also females. Regarding sitting postures, there was not a significant difference between males and females, as 90% of participants of each gender reported that they sat in wrong postures. Ultimately, insufficiency in exercise, insufficiency in weight-lifting, and hormonal fluctuations, are the main reasons as to why LBP is generally more prevalent in females.
Factors like BMI, year of study, and smoking, did not display any statistically significant correlations with LBP. Some results yielded by different studies are consistent with results of this study, while others are not. For instance, authors of a study conducted in Al-Taif university also found that BMI and smoking were not statistically significant variables; however, year of study was found to have a strong association with LBP (p= 0.002) [26].
Additionally, our analysis of the Oswestry Disability Index (ODI) scores revealed important insights. The ODI data shows that the majority of participants (56.9%) fall into the "No Disability" category, followed by 37.2% in the "Mild Disability" category. Only a small percentage of participants are classified as having "Moderate" (4.3%) or "Severe Disability" (1.6%). This distribution suggests that while LBP is prevalent among medical students, the impact on their daily activities and quality of life varies considerably, with most experiencing no or mild disability [19,32].
Furthermore, our linear regression model revealed a statistically significant relationship between age and ODI scores (p = 0.026), with a positive correlation (β = 0.137). This demonstrates that as age increases, ODI scores increase as well, suggesting that older medical students may be more susceptible to LBP-related disability. This finding was not mentioned in the original discussion and provides valuable insight into the age-related aspects of LBP among medical students.
The regression model also exhibited significant associations for other variables that were not previously discussed. Sleep duration showed a negative correlation with ODI scores (β = -0.140, p = 0.025), suggesting that longer sleep durations were associated with lower ODI scores and potentially less LBP-related disability. This demonstrates the importance of adequate sleep for medical students to decrease the chances of facing LBP [19,27].
Prolonged device use also exhibited a positive association with ODI scores (β = 0.170, p = 0.006), indicating that extended use of devices was correlated with higher ODI scores and potentially more severe LBP-related disability. This finding is particularly relevant in the context of modern medical education, where students usually spend long hours using electronic devices for studying and research [28,29,30].
Regarding study generalizability, this study entailed a strict inclusion criterion so that the population being studied was clearly defined. As such, the generalizability is limited to the studied population: medical students. Regarding this generalizability, the study yielded many results that are consistent with results of studies from all around the world (as discussed previously), suggesting that this study possesses strong external validity, and that its results are applicable to different populations of medical students in different settings. Although there could be limitations in the sense that participation in the study was completely voluntary (meaning that not everyone that matched the conditions of the inclusion criteria participated). Furthermore, the factors that were examined in the study did not include laboratory tests, and resembled real-life situations to ensure generalizability and applicability to those who didn’t participate.
4.2. Limitations and Strengths of the Study
Regarding the limitations of the study, there are several avenues that can be improved in future investigations. Firstly, the study is of a cross-sectional design and therefore could be liable to both causality bias and selection-bias. Causality bias can limit the study in that it is not possible to conclude that participants experience LBP more/less due to medical school. On the other hand, selection-bias might have affected this study in that participants who suffer from LBP might have been more open to participating in this study and those who do not to abstain from it. Aside from study design, the study also did not go over the characteristics of the lower back pain itself, such as pain duration. Temporal analysis of the pain might have uncovered further relationships with the variables evaluated with respect to LBP.
The strengths of this study primarily arise from the fact that the study examined a large sample size from Alfaisal University and the usage of a validated tool (Oswestry Disability Index) to analyze the characteristics of Lower Back Pain. Additionally, including validated questions and examining a large number of demographic and lifestyle variables allowed the exploration of numerous relationships between them and LBP.
5. Conclusions
5.1. General Conclusions
In conclusion, this study allowed a comprehensive examination of the prevalence of lower back pain and a construction of the profile of those who suffer from it among medical students in Alfaisal University. 73.4% of surveyed Alfaisal University Medical Students possessed lower back pain, averaging a severity of 4.61 from 1-10. These students are majority female, within the age of 18-21, and use their devices for long hours among other demographic trends.
Statistical analyses of the data collected uncovered numerous relationships with various demographic and behavioral factors. The profile of Alfaisal University medical students who are prone to lower back pain are those who are female, spend long hours on their computers, do not exercise, and do not lift weights. This supports the findings of previous literature which also found LBP correlated with female, sedentary, and computer-bound students [18,19]. Further analysis into gender as a factor itself following initial analysis showed that these LBP-prone female students exercise less, are less likely to lift weights, and use shoulder bags to carry their items.
Regarding the degree of disability of LBP per the Oswestry Disability Index most students who suffer from LBP can be categorized as “No Disability” followed by a sizable minority of those classified as “Mild Disability.” Factors associated with a higher degree of disability are those such as being above the age of 21, spending long hours on computers, using their phone for more than 8 hours, and sleeping very little.
Strengths of this study include a large sample size from a single institution, the usage of validated tools and questions, and a comprehensive examination of demographic and lifestyle factors.
Limitations of this study include a cross-sectional design limiting causality exploration, potential selection bias, and reliance on self-reported data. Additionally, temporal and psychosocial aspects of LBP were not explored.
As LBP is a complex and oftentimes idiopathic condition, these results hold promise in narrowing down its potential determinants–however, more studies are needed, especially in this cohort.
5.2. Future Directions
Further investigation into this topic should look to go deeper into all aspects of LBP (severity, temporal characteristics, and degree of disability) with regards to a multitude of factors. This may include studies employing approaches other than a cross-sectional one. Further investigation can also look at modalities of objective measurements such as imaging studies or physical examination to rule out any issues arising from self-reporting data. Additionally, among the Saudi medical student population, there is limited information regarding the relationship between the various characteristics of LBP and as such could be an area of further investigation.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, S1: STROBE Checklist of the study. S1: This is the STROBE checklist with the guidelines that were used to guide the composition of this manuscript.
Author Contributions
Conceptualization, M.B., S.A., S.O., S.Q., and M.M., ; Methodology, M.B. and M.T.; Software, M.B., S.O., and H.T., Validation, M.B. and S.O.; Formal Analysis, M.B., S.O., and H.T.; Investigation, M.B., S.O. and S.Q.; Resources, S.O., H.T. S.Q., and M.M.; Data Curation, M.B., S.O., M.T., and S.A.; Writing – Original Draft Preparation, M.B., S.O., M.T., and J.A.; Writing – Review & Editing, M.B., S.O., S.Q., H.T., and M.M.; Visualization, X.X.; Supervision, S.Q.; Project Administration, M.B. and S.O.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board of Alfaisal University (Protocol/Approval Code #20278, date of approval 25/02/2024). Consent was obtained prior to respondents answering the survey, detailing the nature of the project and handling of respondent information. An excerpt of the consent statement available to respondents is included below. Participants who responded YES I CONSENT had their non-identifiable data included in the study whereas those who did not had their data destroyed.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study including publication consent.
Data Availability Statement
The original contributions presented in the study are included in the article material, further inquiries can be directed to the corresponding author.
Acknowledgments
We would like to acknowledge Dr. Sadia Qazi, Dr. Muhammed Atif Mazhar, and Dr. Hani Tamim for their support of this study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- World Health Organization, “Low back pain.” Accessed: Jun. 14, 2024. Available online: https://www.who.int/news-room/fact-sheets/detail/low-back-pain.
- G. E. Ehrlich, “Low back pain,” Bull World Health Organ, vol. 81, no. 9, pp. 671–676, 2003.
- M. L. Ferreira et al., “Global, regional, and national burden of low back pain, 1990–2020, its attributable risk factors, and projections to 2050: a systematic analysis of the Global Burden of Disease Study 2021,” The Lancet Rheumatology, vol. 5, no. 6, pp. e316–e329, Jun. 2023. [CrossRef]
- D. Hoy et al., “A systematic review of the global prevalence of low back pain,” Arthritis & Rheumatism, vol. 64, no. 6, pp. 2028–2037, 2012. [CrossRef]
- Wu et al., “Global low back pain prevalence and years lived with disability from 1990 to 2017: estimates from the Global Burden of Disease Study 2017,” Annals of Translational Medicine, vol. 8, no. 6, Art. no. 6, Mar. 2020. [CrossRef]
- J. Hartvigsen et al., “What low back pain is and why we need to pay attention,” Lancet, vol. 391, no. 10137, pp. 2356–2367. [CrossRef]
- K. P. Jordan, U. T. Kadam, R. Hayward, M. Porcheret, C. Young, and P. Croft, “Annual consultation prevalence of regional musculoskeletal problems in primary care: an observational study,” BMC Musculoskeletal Disorders, vol. 11, no. 1, p. 144, Jul. 2010. [CrossRef]
- F. Fatoye, T. Gebrye, C. G. Ryan, U. Useh, and C. Mbada, “Global and regional estimates of clinical and economic burden of low back pain in high-income countries: a systematic review and meta-analysis,” Front Public Health, vol. 11, p. 1098100, Jun. 2023. [CrossRef]
- F. Fatoye, T. Gebrye, C. E. Mbada, and U. Useh, “Clinical and economic burden of low back pain in low- and middle-income countries: a systematic review,” BMJ Open, vol. 13, no. 4, p. e064119, Apr. 2023. [CrossRef]
- L. Panjaitan, W. Hon, and S. Mohd Sojran, THE INCIDENCE OF LOW BACK PAIN AMONG UNIVERSITY STUDENTS. 2018.
- de Vitta, T. P. F. Bento, G. P. Cornelio, P. D. de O. Perrucini, L. A. Felippe, and M. H. S. de Conti, “Incidence and factors associated with low back pain in adolescents: A prospective study,” Braz J Phys Ther, vol. 25, no. 6, pp. 864–873, 2021. [CrossRef]
- M. M. Alshehri et al., “Prevalence of lower back pain and its associations with lifestyle behaviors among college students in Saudi Arabia,” BMC Musculoskelet Disord, vol. 24, p. 646, Aug. 2023. [CrossRef]
- N. Henschke et al., “Prevalence of and screening for serious spinal pathology in patients presenting to primary care settings with acute low back pain,” Arthritis Rheum, vol. 60, no. 10, pp. 3072–3080, Oct. 2009. [CrossRef]
- P. Shokri et al., “Non-spinal low back pain: Global epidemiology, trends, and risk factors,” Health Sci Rep, vol. 6, no. 9, p. e1533, Sep. 2023. [CrossRef]
- H. Yang and S. Haldeman, “Behavior-Related Factors Associated With Low Back Pain in the US Adult Population,” Spine (Phila Pa 1976), vol. 43, no. 1, pp. 28–34, Jan. 2018. [CrossRef]
- A. Aljohani et al., “Prevalence of Low Back Pain Among University Attendants in Tabuk City During 2023: A Cross-Sectional Study in Saudi Arabia,” Cureus, vol. 15, no. 12, p. e50357, Dec. 2023. [CrossRef]
- H. M. Alrabai, M. H. Aladhayani, S. M. Alshahrani, Z. K. Alwethenani, M. J. Alsahil, and A. D. Algarni, “Low Back Pain Prevalence and Associated Risk Factors among Medical Students at Four Major Medical Colleges in Saudi Arabia,” Journal of Nature and Science of Medicine, vol. 4, no. 3, p. 296, Sep. 2021. [CrossRef]
- H. Alwashmi, “Prevalence of Low Back Pain and Associated Factors Among Qassim University Medical Students: A Cross-Sectional Study,” Cureus, vol. 15, no. 9, p. e44596, Sep. 2023. [CrossRef]
- Y. A. Taha et al., “The Prevalence of Low Back Pain Among Medical Students: A Cross-Sectional Study From Saudi Arabia,” Cureus, vol. 15, no. 5, p. e38997, May 2023. [CrossRef]
- Janampa-Apaza et al., “Physical activity and sedentary behavior in medical students at a Peruvian public university,” Medwave, vol. 21, no. 5, p. e8210, Jun. 2021. [CrossRef]
- J. D. Gonzalo, M. Dekhtyar, R. E. Hawkins, and D. R. Wolpaw, “How Can Medical Students Add Value? Identifying Roles, Barriers, and Strategies to Advance the Value of Undergraduate Medical Education to Patient Care and the Health System,” Academic Medicine, vol. 92, no. 9, pp. 1294–1301, Sep. 2017. [CrossRef]
- M. Davidson and J. Keating, “Oswestry Disability Questionnaire (ODQ),” Aust J Physiother, vol. 51, no. 4, p. 270, 2005. [CrossRef]
- J. C. Fairbank and P. B. Pynsent, “The Oswestry Disability Index,” Spine (Phila Pa 1976), vol. 25, no. 22, pp. 2940–2952; discussion 2952, Nov. 2000. [CrossRef]
- Maryam. Alshanqiti, Mays. Garah, KhuloodSalem. Alsenani, and SarahKhaled. Alrasheed, “PREVALENCE OF LOWER BACK PAIN AMONG TAIBAH UNIVERSITY STUDENTS.,” IJAR, vol. 5, no. 1, pp. 1304–1313, Jan. 2017. [CrossRef]
- R. K. A. Rawaf et al., “Prevalence of neck–shoulder pain and low back pain among high school students in Riyadh, Saudi Arabia,” JMSR, vol. 3, p. 279, Jul. 2019. [CrossRef]
- L. H. Alturkistani et al., “Prevalence of Lower Back Pain and its Relation to Stress Among Medical Students in Taif University, Saudi Arabia,” Int J Prev Med, vol. 11, p. 35, 2020. [CrossRef]
- K. Bintang, I. Santosa, Y. Goysal, M. Akbar, and S. Aulina, “Relationship between sleep quality and pain intensity in patients with chronic low back pain,” Med Clin Pract, vol. 4, Apr. 2021. [CrossRef]
- Kho, L. E. Henderson, D. D. Dressler, and S. Kripalani, “Use of handheld computers in medical education. A systematic review,” J Gen Intern Med, vol. 21, no. 5, pp. 531–537, May 2006. [CrossRef]
- T. J. G. Chase et al., “Mobile learning in medicine: an evaluation of attitudes and behaviours of medical students,” BMC Med Educ, vol. 18, no. 1, p. 152, Jun. 2018. [CrossRef]
- Masic, “E-learning as new method of medical education,” Acta Inform Med, vol. 16, no. 2, pp. 102–117, 2008. [CrossRef]
Figure 1.
Responses Gathered At Each Stage.
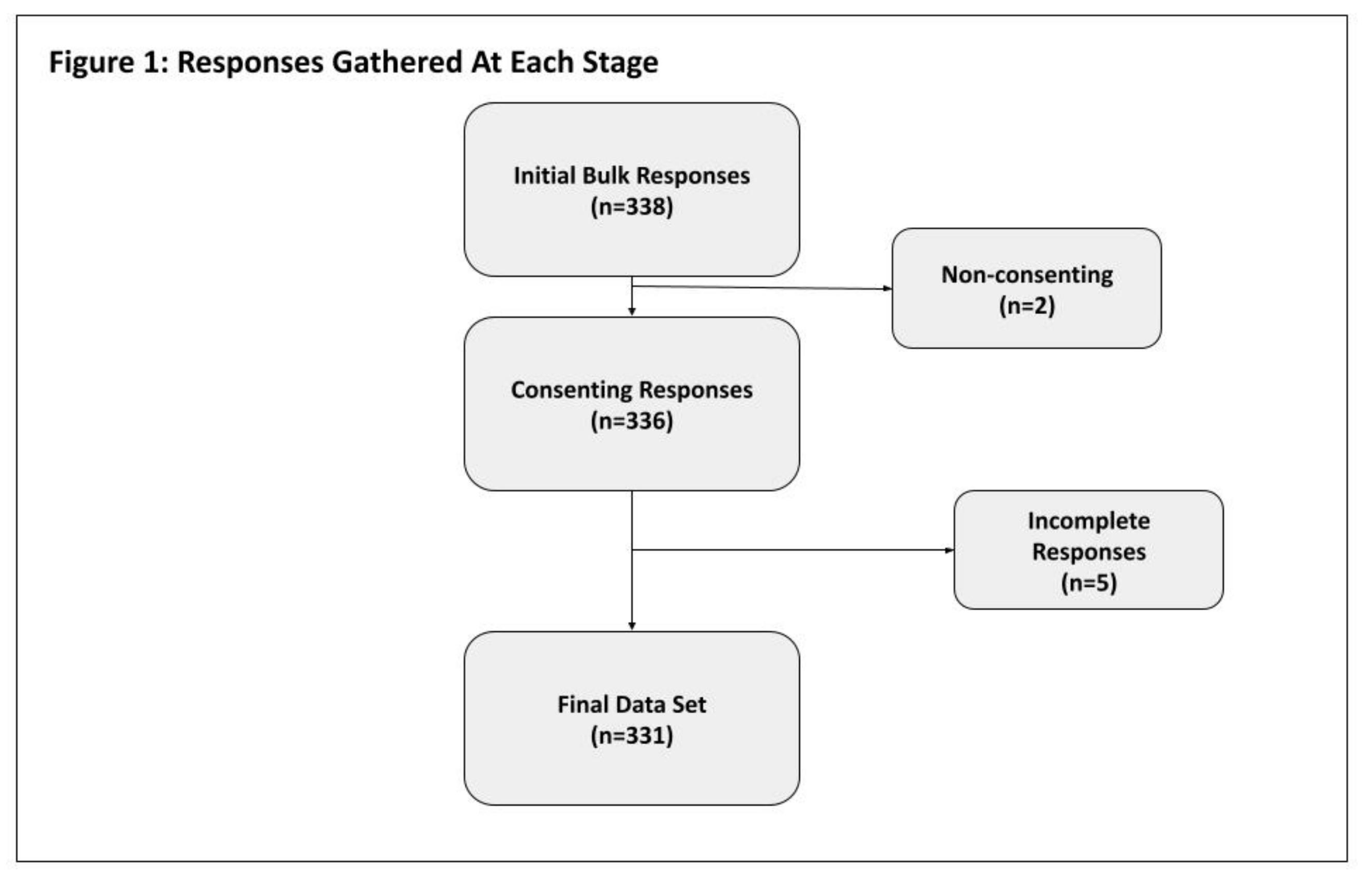

Table 1.
Demographics & Lifestyle Habits of Respondents.
| Variable | Frequency | |
|---|---|---|
| Age, mean ±sd (yrs) | 20.01 ±1.81 | |
| Age (yrs) | 17-21 | 278(84.0) |
| 22+ | 53(16.0) | |
| Gender | Female | 206(62.2) |
| Male | 125(37.8) | |
| BMI, mean ±sd (kg/m2) | 23.63 ±4.60 | |
| BMI Category | Underweight | 34 (10.3) |
| Normal | 191 (57.7) | |
| Overweight | 79 (23.9) | |
| Obese | 27 (8.2) | |
| Year In Medical School | Year 1 | 148(44.7) |
| Year 2 | 84(25.4) | |
| Year 3 | 52(15.7) | |
| Year 4 | 26(7.9) | |
| Year 5 | 21(6.3) | |
| Experienced Back Pain Before Medical School | No | 161(48.6) |
| Yes | 170 (51.4) | |
| Spend Long Hours on Computers | No | 20 (6.0) |
| Yes | 311 (94.0) | |
| Exercise | No | 165 (49.8) |
| Yes | 166 (50.2) | |
| Weekly exercise (hrs) | 1-2 | 47 (28.3) |
| 3-5 | 53 (31.9) | |
| 5+ | 66 (39.7) | |
| Lift Weights | No | 217 (65.6) |
| Yes | 114 (34.4) | |
| Smoke | No | 296 (89.4) |
| Yes | 35 (10.6) | |
| Average daily phone usage (hrs) | <1 | 4 (1.2) |
| 1-2 | 31 (9.4) | |
| 2-5 | 142 (42.9) | |
| 5-8 | 112 (33.8) | |
| 8+ | 42 (12.7) | |
| University Commute Length (Minutes) | Less than 30 | 180 (54.4) |
| More than 30 | 151 (45.6) | |
| Average sleep time (hrs) | 4> | 24 (7.3) |
| 4-6 | 182 (55) | |
| 6-8 | 103 (31.1) | |
| 8+ | 22 (6.6) | |
| Sitting Position | Upright | 33 (10) |
| Leaning Back | 136 (41.1) | |
| Leaning forward | 129 (39) | |
| Sitting at edge | 33 (10) | |
| Wear Backpack | Yes | 133 (40.2) |
| Sometimes | 57 (17.2) | |
| No | 26 (7.9) | |
| Carry shoulder bag or crossbody | 115 (34.7) |
Table 2.
Prevalence of Lower Back Pain in Alfaisal University Medical Students.
| Variable | Frequency (%) | |
|---|---|---|
| Experience Back Pain | YesNo | 78 (23.6) 253 (73.4) |
| Severity of Back Pain, mean ±sd (1-10) | 4.61 ±2.16 | |
Table 3.
Chi-Square Analysis of Lower Back Pain v. Various Factors.
| Variable | Do Not Suffer Back Pain (%) | Suffer Back Pain (%) | P-value | |
|---|---|---|---|---|
| Age | 17-21 | 50 (64.1) | 75 (29.6) | 0.218 |
| 22+ | 28 (35.9) | 178 (70.4) | ||
| Gender | Male | 69 (88.5) | 209 (82.6) | <.001 |
| Female | 9 (11.5) | 44 (17.4) | ||
| BMI | Underweight | 10 (12.8) | 24 (9.5) | 0.836 |
| Normal | 45 (57.7) | 146 (57.7) | ||
| Overweight | 17 (21.8) | 62 (24.5) | ||
| Obese | 6 (7.7) | 21(8.3) | ||
| Year of Study | Year 1 | 35 (44.9) | 113 (44.7) | 0.302 |
| Year 2 | 21 (26.9) | 63 (24.9) | ||
| Year 3 | 16 (20.5) | 36 (14.2) | ||
| Year 4 | 4 (5.1) | 22 (8.7) | ||
| Year 5 | 2 (2.6) | 19 (7.5) | ||
| Spend Long Hours on Computers | No | 6 (7.7) | 14 (5.5) | 0.484 |
| Yes | 72 (92.3) | 239 (94.5) | ||
| Exercise | No | 26 (33.3) | 139 (54.9) | 0.001 |
| Yes | 52 (66.7) | 114 (45.1) | ||
| Weekly exercise (hrs) | 1-2 | 11 (20.8) | 37 (32.5) | 0.287 |
| 3-5 | 18 (34.0) | 35 (30.7) | ||
| 5+ | 24 (45.3) | 42 (36.8) | ||
| Lift Weights | No | 38 (48.7) | 179 (70.8) | <0.001 |
| Yes | 40 (51.3) | 74 (29.2) | ||
| Smoke | No | 70 (89.7) | 226 (89.3) | 0.917 |
| Yes | 8 (10.3) | 27 (10.7) | ||
| Average daily phone usage (hrs) | <1 | 0 (0.0) | 4 (1.6) | 0.042 |
| 1-2 | 5 (6.4) | 26 (10.3) | ||
| 2-5 | 45 (57.7) | 97 (38.3) | ||
| 5-8 | 20 (25.6) | 92 (36.4) | ||
| 8+ | 8 (10.3) | 34 (13.4) | ||
| University Commute Length (Minutes) | Less than 30 | 48 (61.5) | 132 (52.2) | 0.147 |
| More than 30 | 30 (38.5) | 121 (47.8) | ||
| Average sleep time (hrs) | 4> | 2 (2.6) | 22 (8.7) | 0.272 |
| 4-6 | 46 (59.0) | 136 (53.8) | ||
| 6-8 | 26 (33.3) | 77 (30.4) | ||
| 8+ | 4 (5.1) | 18 (7.1) | ||
| Sitting Position | Upright | 7 (9.0) | 26 (10.3) | 0.014 |
| Leaning Back | 44 (56.4) | 92 (36.4) | ||
| Leaning forward | 20 (25.6) | 109 (43.1) | ||
| Sitting at edge | 7 (9.0) | 26 (10.3) | ||
| Wear Backpack | Yes | 8 (10.3) | 18 (7.1) | 0.001 |
| Sometimes | 10 (12.8) | 47 (18.6) | ||
| No | 45 (57.7) | 88 (34.8) | ||
| Carry shoulder bag or crossbody | 15 (19.2) | 100 (39.5) |
Table 4.
Further Analysis of Gender v. Factors Found Associated With Back Pain (p < 0.05).
| Variable | Frequency of Males | Frequency of Females |
|
|---|---|---|---|
| Spend Long Hours on Computers | No | 9 (7.2) | 11 (5.3) |
| Yes | 116 (92.8) | 195 (94.7) | |
| Exercise | No | 35 (28.0) | 130 (63.1) |
| Yes | 90 (72.0) | 76 (36.9) | |
| Lift Weights | No | 55 (44.0) | 162 (78.6) |
| Yes | 70 (56.0) | 44 (21.4) | |
| Average daily phone usage (hrs) | <1 | 2 (1.6) | 2 (1.0) |
| 1-2 | 9 (7.2) | 22 (10.7) | |
| 3-5 | 61 (48.8) | 81 (39.3) | |
| 5-8 | 38 (30.4) | 74 (35.9) | |
| 8+ | 15 (12.0) | 27 (13.1) | |
| Sitting Position | Upright | 13 (10.4) | 20 (9.7) |
| Leaning Back | 65 (52.0) | 71 (34.5) | |
| Leaning forward | 39 (31.2) | 90 (43.7) | |
| Sitting at Edge | 8 (6.4) | 25 (12.1) | |
| Carry a Backpack | No | 11 (8.8) | 15 (7.3) |
| Sometimes | 27 (21.6) | 30 (14.6) | |
| Yes | 82 (65.6) | 51 (24.8) | |
| Instead carry shoulder bag or crossbody | 5 (4.0) | 110 (53.4) |
Table 5.
Oswestry Disability Index Categorization of Participants Suffering from LBP.
| Oswestry Index Degree of Disability | Frequency (%) |
|---|---|
| No Disability | 144 (56.9) |
| Mild Disability | 94 (37.2) |
| Moderate | 11 (4.3) |
| Severe Disability | 4 (1.6) |
Table 6.
Comparison and Correlation of LBP-Stricken Student Oswestry Disability Index Score By Variables.
Table 6.
Comparison and Correlation of LBP-Stricken Student Oswestry Disability Index Score By Variables.
| Variable | Mean ODI Score ± SD | p | |
|---|---|---|---|
| Age | 17-21 | 4.86 ±4.87 | 0.008 |
| 22+ | 7.14 ±7.29 | ||
| Gender | Male | 4.68 ±5.65 | 0.778 |
| Female | 5.50 ±5.32 | ||
| BMI | Underweight | 5.46 ±5.84 | 0.141 |
| Normal | 4.62 ±4.76 | ||
| Overweight | 6.13 ±6.30 | ||
| Obese | 6.86 ±6.21 | ||
| Year of Study | Year 1 | 5.12 ±5.02 | 0.635 |
| Year 2 | 5.56 ±5.54 | ||
| Year 3 | 4.81 ±5.54 | ||
| Year 4 | 4.50 ±4.06 | ||
| Year 5 | 6.84 ±8.08 | ||
| Experienced Back Pain Before Medical School | No | 5.23 ±5.29 |
0.765 |
| Yes | 5.28 ±5.55 | ||
| Spend Long Hours on Computers | No | 1.57 ±1.51 | 0.008 |
| Yes | 5.47 ±5.49 | ||
| Exercise | No | 5.23 ±5.06 | 0.170 |
| Yes | 5.29±5.86 | ||
| Weekly exercise (hrs) | 1-2 | 4.62 ±3.80 | 0.054 |
| 3-5 | 7.26 ±7.30 | ||
| 5+ | 4.24 ±5.73 | ||
| Lift Weights | No | 5.46 ±5.59 | 0.573 |
| Yes | 4.77 ±5.00 | ||
| Smoke | No | 5.04 ±5.33 | 0.763 |
| Yes | 7.11 ±5.93 | ||
| Average daily phone usage (hrs) | <1 | 10.75 ±6.90 | 0.028 |
| 1-2 | 5.15 ±4.93 | ||
| 2-5 | 5.18 ±5.05 | ||
| 5-8 | 4.41 ±4.52 | ||
| 8+ | 7.21 ±7.86 | ||
| University Commute Length (Minutes) | Less than 30 | 5.08 ±5.77 | 0.388 |
| More than 30 | 5.45 ±5.03 | ||
| Average sleep time (hrs) | 4> | 8.23 ±7.13 | 0.023 |
| 4-6 | 5.37 ±5.58 | ||
| 6-8 | 4.23 ±4.35 | ||
| 8+ | 5.17 ±4.96 | ||
| Sitting Position | Upright | 4.58 ±4.53 | 0.333 |
| Leaning Back | 5.86 ±6.54 | ||
| Leaning forward | 4.70 ±4.37 | ||
| Sitting at edge | 6.15 ±5.82 | ||
| Wear Backpack | Yes | 6.61 ±6.85 | 0.337 |
| Sometimes | 5.72 ±5.38 | ||
| No | 4.49 ±4.81 | ||
| Carry shoulder bag or crossbody | 5.47 ±5.65 |
Table 7.
Regression Analysis of Participant Age on Oswestry Index Score, Adjusted for Spending Long Hours on Devices, Avg. Duration of Sleep, and Avg. Duration of Phone Usage*.
Table 7.
Regression Analysis of Participant Age on Oswestry Index Score, Adjusted for Spending Long Hours on Devices, Avg. Duration of Sleep, and Avg. Duration of Phone Usage*.
| Variable* | Beta | Std. Error | p |
|---|---|---|---|
| Constant | n/a | 4.128 | 0.207 |
| Age (cont.) | .137 | .182 | 0.026 |
| Duration of sleep (Ranges) | -.140 | .451 | 0.025 |
| Spend Long Hours on Computer (y/n) | .170 | 1.453 | 0.006 |
*Average daily phone usage duration results not included in the table as it did not meet alpha (p=0.934).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



