
Submitted:
30 August 2024
Posted:
02 September 2024
You are already at the latest version
Abstract
Objective Hypertension is one of the most common chronic diseases, affecting more than 20 % of the population. The side effects experienced due to antihypertensive medications such as tired-ness, muscle pain, and insomnia are often a significant predictor of poor adherence to therapy. The goal of the current study is to present the frequency, type, seriousness, and severity of adverse drug reactions reported to the BDA via Individual Case Safety Reports (ICSR) and following differentiation of messages found in more than one patient. Methods We conducted a retrospective analysis of the reported adverse drug reactions (ADR) reported in the Bulgarian Drug Agency database after treatment with antihyperlipidemic medicines, angiotensin-converting enzyme (ACE) - inhibitors, and sartans for the period 2017-2021. Each ICSR form was observed and data for suspected medicine and type of adverse reaction was analyzed. Results The total number of processed notifications for adverse drug reactions (ADR) included in the database is 142. The highest number of ADRs was reported for ARB (58), followed by antihyperlipidemic medicines (55) and ACE inhibitors (29.) Most of the assessed adverse events experienced by more than one patient fall into the probable and related categories based on Global Introspection method classification. Therefore, they have been investigated and are consistent with exposure in the population. Conclusion Cardiovascular medicines from the groups of ACE inhibitors, sartans and statins are with high share of reported ADRs in the BDA system. Some of them are severe and need further investigation.
Keywords:
drug-related side effects and adverse reactions
; antihyperlipidemic medicines
; angiotensin-converting enzyme (ACE) - inhibitors
; sartans
1. Introduction
Cardiovascular diseases (CVD) are the leading cause of co-morbidity and polypharmacy due to their complex nature. Hypertension is one of the most common chronic CVD, affecting more than 20% of the population. Hypertension prevalence in Bulgaria is 48%, compared with a global average of 33%. Out of 2.4 million hypertensive patients aged 30–79 in Bulgaria only 28% of female and 18% of male successfully managed the disease. Not only morbidity but also mortality is high. The deaths due to cardiovascular disease accounted 68 900 in 2019. [1]
National programs for early hypertension diagnosis among the ageing population let to more detected co-morbid conditions compared with those 20 years ago. Extended life expectancy and longer years of life with chronic conditions increased the number of people who needed long-term therapy worldwide. Statistical data confirms that over 70% of people above 65 years of age are with cardiovascular co morbidities. [2] CVD treatment often requires more than two medications, thus enhancing the polypharmacy in this group and increasing the risk of adverse events (fall injury, heart failure, and BP exacerbation). [3] In addition to a higher risk of side effects, drug interactions are also foreseeable. About 13% of elderly people are taking over 10 medicines, thus increasing the risk and exposure to adverse events. [4] One-third of the chronic patients had concerns for the necessity of their medicines. [5] Higher number of prescribed medicines correlated with observed adverse events such as hospitalizations, mortality, side effects, and medicines interactions. [6] Some of them might be life threatening as for example bleeding and thrombotic events in patients with atrial fibrillation (AF) on polypharmacy (or complexity of major bleeding, ischemic stroke, and mortality). [7]
The increased frequency of hospitalizations and complications is the main reason for significant public expenditure. [8] The side effects experienced due to antihypertensive medications such as tiredness, muscle pain, and insomnia are often a significant predictor of poor adherence to therapy. [9] The risk for medication non-adherence depends on some therapy-related factors such as a number of prescribed medicines, prescribed drug classes and their safety profile. [10] Single-pill combination (SPC) therapy in patients suffering from hypertension and dyslipidemia is associated with systolic blood pressure reduction, reduced emergency department visits, and better clinical outcomes compared with free combination therapy (FCT). [11]
There are evidence that the adverse drug reactions (ADR) are underreported [12]. To overcome this challenge the pharmaceutical legislation, introduce the possibility of reporting ADR from patients, and all health care professionals in addition to companies' obligations to provide evidence for safety of their products [13].
This study aims to systematize ADRs for ACE-inhibitors, sartans, and antihyperlipidemic medicines reported to the Bulgarian Drug Agency (BDA) via Individual Case Safety Reports (ICSR) according to their frequency, type, seriousness, and severity. Repeating ADRs appearing in more than 1 patient were also evaluated.
2. Materials and Methods
We conducted a retrospective, descriptive analysis of the reported ADRs to the Bulgarian Drug Agency database for the period 2017-2021. Information from every ICSR was extracted and analysed according to:
- suspected medicines (international nonproprietary name (INN) and therapeutic indication,as well as concomitant therapy;
- Characteristics on the reported adverseevent as evaluated by the BDA: seriousness; expectancy; severity; type of report and reporting (spontaneous or nonspontaneous); adverse event occurred (MedDRA) related to the suspected drug, and reporter -physicians, patients, and other healthcare professionals (including experts from pharmaceutical companies, pharmacists etc).
Additionally, subgroup analysis was performed for events that occurred in more than one patient. They were analyzed according to their frequency and causality. The causal relationship of suspected ADRs was evaluated using the Global Introspection method [14] from Health Care professional point of view. The company or primary source reporters’ assessment was provided in cases of missing evaluation from the health care professionals.
3. Results
The total number of processed notifications for adverse drug reactions (ADR) included in the database during 2017 -2021is 142.Out of them reports for antihyperlipidemic medicines were 55, of which 20 were classified as serious ADRs, 28 as expected and 42 as spontaneous. Rosuvastatin is the product with the highest number of ADRs reports accounting for 45.45% of the total number of reported notifications of antilipidemics and 29.09% of them are serious.
In the group of angiotensin II receptor blockers (sartans) 58 reports were found with 46 serious, 16 expected, and 57 spontaneous ADRs. The highest number of reports was submitted for valsartan (48.28%), and the number of serious ADRs (39.66%) was also the highest. On total 29 reports for ACE inhibitors were submitted to BDA. 13 of them reported serious, 26 expected, and 25 spontaneous ADRs. The highest number of reports and the most serious ADRs were for ramipril (41.38% of which 20.6% were serious).
Table 1 presents a summary of submitted notifications for each INN.
The adverse drug reactions occurring in more than one patient along with the available data for causality included in ICSR are presented on Table 2. The categories are based on an assessment of causality provided by health professionals using the Global Introspection scaling.
ADRs occurring in more than one patient were observed for 10 out of 14 INNs included in the observation. In the group of statins atorvastatin, rosuvastatin and evolocumab ADRs affects between 2 to 5 persons with highest number of 23 patients for evolucimab. Acute myocardial infarction, acute coronary syndrome, and angina pectoris were the most often reported. Due to their probably life threatening nature there is a need for additional examination of products safety profiles.
Within the sartans group for irbesartan, olmesartan, telmisartan, and valsartan were reported ADRs in more than 1 person. Most disturbing is the highest number of manifested coetaneous malignancies such as melanoma (22 people) and squamous cell carcinoma, as well as cases of prostate carcinoma. They appear within 2 to 5 years after the beginning of drug therapy and should be carefully examined, especially those for valsartan. These adverse drug reactions are unexpected (not mentioned in the summary of product characteristics), but a possible and with suspected causal relationship, especially when more than one sartan is taken. ADRs were reported in 6 patients out of 7 treated with irbesartan, 8 out of 13 treated with olmesartan, 3 out of 7 treated with telmisartan, and 22 out of 28 treated with valsartan. The most disturbing ADR is that of melanoma and other types of malignancies as squamous cell carcinoma and prostate carcinoma.
Within the ACE-inhibitor group, adverse drug reactions occurring in more than one patient have been reported forramipril, lisinopril, and perindopril. The most severe are heart and valvular failure, cardiotoxicity, pulmonary hypertension and ventricular tachycardia. Hypo- and hyperglycemia in diabetics have been also reported.
Most of the ADRs experienced by more than one patient fall into the related and suspected categories, 17 and 7 respectively, indicating that they have been investigated and are consistent with exposure to the INN (Figure 1). Despite missing category ‘suspected’ in Global Introspection classification we found that ramipril and valsartan side effects are assessed as suspected in provided ICSR. Therefore, they are presented as suspected in the figure above.
4. Discussion
In this study we evaluated ADRs reported to BDA for 3 classes of CV medicines. We found out that there is an increase in the reporting, and the physicians are the most active reporters in the system. It is also evident that many of the reported ADRs occur in more than one patient and many of them are severe.
The polypharmacy is one of the most important factors for ADRs occurrence, and patients with CVD are among the most often affected once.[15] Factors that contribute to the development of adverse reactions may be related to the medicinal product, to the disease, or to the patient. Age, gender, and disease progression are patient-related factors that contribute significantly to the development of adverse reactions, especially among patients with CVD. [16]We still do not proceed those data and will further deeper our analysis.
Lesar et al. found that ADRs for CV medicines were 2.4 times higher compared to other products. [17]Our results confirm such a conclusion because most of the reported ADRs to the BDA were for CV medicines.
A combination of some types of antidiabetics with antihypertensive medicines could result in hypoglycemia in patients with diabetes mellitus. [18]Therefore, cardiovascular medicines which are one of the most commonly prescribed in healthcare settings can be precursor for medication errors and should be monitored for associated side effects. [19]We do have some suspicious results for probably drug interactions that needs to be further investigated.
The Danish study found that enalapril and ramipril were the most often prescribed with 40.3% and 42.6% of the market share of ACE - inhibitors, but 54.7% of adverse events were associated with enalapril, while 14.2% only concerns ramipril. [20]As it was examined in Bulgaria ramipril utilization is higher than that of enalapril (19.61 vs 12.12 reference DDD/1000 inh/day in 2019) and continues to rise in recent years. [21]The number of reported ADRs for ramipril is higher (n=12 or 41.38%), followed by perindopril (37.9%), and enalapril (10.34%). The most common ADRs for ACE inhibitors are cough, hypotension, hyperkaliemia, and acute renal failure. Similar to our results majority of ADRs were probable and assessed as moderately severe. [22]
Evolocumab often leads to flu-like conditions and general malaise, which is expected due to its affiliation with the monoclonal antibody group. It is relatively new hypolipidemic drug and needs still additional safety studies. Similar to our findings the American Heart Association published data for side effects in more than one patient exposed to statins, [23]which increased diabetes risk, risk of hemorrhagic stroke, and could also lead to back pain. The interesting fact is that muscle pain and weakness are not reported in Bulgaria.
Recent studies also discussed the cancer risk during sartans treatment, but the causal link remains uncertain. Moreover, the population-based10 years study provides the evidences that an increase in cancer risk is unlikely. [24]The nitrosamine impurities should be also examined to exclude or confirm potential relationship[25]The nitrosamines have a proven carcinogenic potential, and they can cause heterogeneous neoplasms which means that could exist possible melanoma triggers. [26,27]
The range of patient reported ADR is from 57.83% to 14.37% in five selected Western EU countries, whereas less than 1% of patients in Asia reported such. The developed feedback system, supported from patient organizations, and increasing citizens' awareness are among the leading factors for higher levels of reported by the patients ADRs. [28] Our study showed that physicians are the most active group reporting adverse events. Reports from patients are 16.2% which is the low range from EU countries. The necessity of patients' education and popularization of the BDA platform which allowed direct reporting is obvious.
This is the first descriptive study in Bulgaria focusing on the reported adverse drug reactions in cardiology patients by using the BDA database. The limitation of our study is that it is still a descriptive analysis of the reporting. We plan further studies to confirm relationships and population risk. Concomitant therapy and co-morbidities are also observed and will be a subject of further studies to explain all detected characteristics and their mutual dependencies.
5. Conclusions
Cardiovascular medicines from the groups of ACE inhibitors, sartans and statins are with high share of reported ADRs in the BDA system. Some of them are severe and needs further investigation. The highest number of ADRs reports is found for sartans, which are among the most commonly used CV medicines in Bulgaria. The side effects experienced by more than one patient were also high, but further studies are needed to identify the frequency of occurrence in the population.
Author Contributions
Conceptualization, Z.M., A.D.; methodology, M.D.; validation, Z.M., A.D; formal analysis, A.D; investigation, A.D.; data curation, M.D..; writing—original draft preparation, Z.M.; writing—review and editing, G.P.; supervision, G.P.; funding acquisition, G.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research is funded by the European Union-Next Generation EU, through the National Recovery and Resilience Plan of the Republic of Bulgaria, project № BG-RRP-2.004- 0004-C01, research group ACCOMPLISH.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data are Available after a reasonable request from the authors.
Acknowledgments
We would like to thank the Bulgarian Drug Agency for the access to reports of adverse drug reaction data and ICSR forms.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- World Health Organization. Hypertension profiles 2023 Available online: https://www.who.int/docs/default-source/ncds/ncd-surveillance/hypertension-profiles-2023.pdf [accessed on 22 July 2024].
- Guthrie, B.; Makubate, B.; Hernandez-Santiago, V.; Dreischulte, T. The Rising Tide of Polypharmacy and Drug-Drug Interactions: Population Database Analysis 1995-2010. BMC Med. 2015,13:74. [CrossRef] [PubMed]
- Mukete, B.N.; Ferdinand, K.C. Polypharmacy in Older Adults With Hypertension: A Comprehensive Review. J ClinHypertens (Greenwich). 2016, 18(1):10-8. [CrossRef] [PubMed]
- Avoidable Costs in U.S. Healthcare. IMS Institute for Healthcare Informatics; June 2013 Available: https://offers.premierinc.com/rs/381-NBB-525/images/Avoidable_Costs_in%20_US_Healthcare-IHII_AvoidableCosts_2013%5B1%5D.pdf (Accessed on 20 July 2024).
- Viktil, K.K.; Frøyland, H.; Rogvin, M.; Moger, T.A. Beliefs about medicines among Norwegian outpatients with chronic cardiovascular disease. Eur J Hosp Pharm. 2014, 21(2) pp 118-120. [CrossRef]
- Sirois, C.; Laroche, M.L.; Guénette, L.; Kröger, E.; Cooper, D.; Émond, V. Polypharmacy in multimorbid older adults: protocol for a systematic review. Syst Rev 2017, 19, 6(1):104. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Montesinos, L.; Rivera-Caravaca, J.M.; Agewall,S.; Soler, E.; Lip, G.Y.H.; Marín, F.; Roldán, V. Polypharmacy and adverse events in atrial fibrillation: Main cause or reflection of multimorbidity? Biomedicine & Pharmacotherapy 2023, 158:114064. [CrossRef] [PubMed]
- Maher, R.L.; Hanlon,J.; Hajjar, E.R.Clinical Consequences of Polypharmacy in Elderly. Expert Opin. Drug Saf. 2014, 13 (1),pp 57–65. [CrossRef]
- Gebreyohannes, E.A.; Bhagavathula, A.S.; Abebe, T.B.; Tefera, Y.G.; Abegaz, TM. Adverse effects and non-adherence to antihypertensive medications in University of Gondar Comprehensive Specialized Hospital. ClinHypertens 2019, 25, 1. [Google Scholar] [CrossRef] [PubMed]
- Gupta, P.; Patel, P.;Štrauch, B.; Lai, F.Y.; Akbarov, A.; Marešová, V.; White, C.M.J.; Petrák, O.; Gulsin, G.S.; Patel, V.; Rosa, J.; Cole, R.; Zelinka, T.; Holaj, R.; Kinnell, A.; Smith, P.R.; Thompson, J.R.; Squire, I.; Widimský, J. Jr.; Samani, N.J.; Williams, B.; Tomaszewski, M. Risk factors for nonadherence to antihypertensive treatment. Hypertension. 2017, 69(6) pp1113–1120. [CrossRef]
- Weisser, B.; Predel, H.G.; Gillessen, A.; Hacke, C.; Vor dem Esche, J.; Rippin, G.; Noetel, A,; Randerath, O. Single Pill Regimen Leads to Better Adherence and Clinical Outcome in Daily Practice in Patients Suffering from Hypertension and/or Dyslipidemia: Results of a Meta-Analysis. High Blood Press Cardiovasc Prev 2020, 27, pp 157–164. [CrossRef]
- Varallo, F.R.; Guimarães Sde, O.; Abjaude, S.A.; Mastroianni, Pde. C. Causes del subregisto de loseventosadversos de medicamentosporlosprofesionales de la salud: revision sistemática [Causes for the underreporting of adverse drug events by health professionals: a systematic review]. Rev Esc Enferm USP. 2014, 48(4) pp 739-47. Spanish. [CrossRef] [PubMed]
- Directive 2001/83/EC of the European Parliament and of the Council of 6 November 2001 on the Community code relating to medicinal products for human use. OJ L 311, 28/11/2001, p. 67–128 http://data.europa.eu/eli/dir/2001/83/oj.
- Marante, K.B. The Challenges of Adverse Drug Reaction Evaluation. J Pharmacovigil 2018, 6: 260. [CrossRef]
- Kaufman, G. Adverse drug reactions: classification, susceptibility and reporting. Nurs Stand. 2016, 30(50) pp 53-63. [CrossRef] [PubMed]
- Murphy, G.K.; McAlister, F.A.; Eurich, D.T. Cardiovascular medication utilization and adherence among heart failure patients in rural and urban areas: a retrospective cohort study. Can J Cardiol. 2015, 31(3) pp 341-7. [CrossRef] [PubMed]
- Lesar, T.S.; Lomaestro, B.M.; Pohl, H. Medication–prescribing errors in a teaching hospital: A nine year experience. Arch Intern Med. 1997,157 pp 1569–76.
- Gosho, M. Risk of Hypoglycemia After Concomitant Use of Antidiabetic, Antihypertensive, and Antihyperlipidemic Medications: A Database Study. The Journal of Clinical Pharmacology 2018, 58 pp 1324-1331. [CrossRef]
- LaPointe, N.M.; Jollis, J.G. Medication errors in hospitalized cardiovascular patients. Arch Intern Med. 2003, 163 pp 1461–66.
- Cornwall, J.E.L.; Bygum, A.; Rasmussen, E.R. ACE-Inhibitor Related Angioedema Is Not Sufficiently Reported to the Danish Adverse Drug Reactions Database. Drug, Healthcare and Patient Safety 2019, 11 pp 105–113. [CrossRef]
- Mitkova, Z.; Petrova, G. Utilization, Cost, and Affordability of Antihypertensive Therapy in Bulgaria. Iran J Pharm Res. 2021, 20(2) pp 403-416. [CrossRef] [PubMed]
- Mateti, U.V.; Nekkanti, H.; Vilakkathala, R.; Rajakannan, T.; Mallayasamy, S.; Ramachandran, P. Pattern of Angiotensin-converting enzyme inhibitors induced adverse drug reactions in South Indian teaching hospital. N Am J Med Sci. 2012, 4(4) pp 185-9. [CrossRef]
- Newman, C.B.; Preiss, D.; Tobert, J.A.; Jacobson, T.A.; Goldstein, L.B.; Chin, C.; Tannock, L.R.; Miller, M.; Raghuveer, G.; Duell, P.B.; Brinton, E.A.; Pollak, A.; Braun, L.T.; Welty, F.K.; American Heart Association Clinical Lipidology, Lipoprotein, Metabolism and Thrombosis Committee, a Joint Committee of the Council on Atherosclerosis, Thrombosis and Vascular Biology and Council on Lifestyle and Cardiometabolic Health; Council on Cardiovascular Disease in the Young; Council on Clinical Cardiology; and Stroke Council. Statin Safety and Associated Adverse Events: A Scientific Statement From the American Heart Association. ArteriosclerThrombVasc Biol. 2019 Feb; 39(2):e38-e81. doi: 10.1161/ATV.0000000000000073. Erratum in: ArteriosclerThrombVasc Biol. 2019;39(5):e158.
- Chan, T.H.; Tsoi, M.F.; Yung Cheung, B.M. Cancer Risk of Angiotensin II Receptor Blocker Valsartan: A Population-based Study. J Cardiovasc Pharmacol. 2022, 79(4) pp 577-582. [CrossRef] [PubMed]
- Berrido, A.M.; Byrd, J.B. Angiotensin Receptor Blockers and the Risk of Cancer: Insights from Clinical Trials and Recent Drug Recalls. Curr Hypertens Rep. 2020, 22(3):20. [CrossRef] [PubMed]
- Tchernev, G.; Bitolska, A.; Patterson, J.W. Telmisartan (and/or nitrosamine) - induced occult melanoma: first reported case in world literature. Expert Review of Clinical Pharmacology 2021, 14(9), pp 1075–1080. [CrossRef]
- Tchernev, G.; Kordeva, S. NITROSOGENESIS OF SKIN (HUMAN) CANCER- THE HIDDEN TRUTH OF A NEVERENDING STORY: NITROSAMINE CONTAMINATION IN OLMESARTAN, VALSARTAN AND HCT AS MAIN RISK FACTOR FOR THE DEVELOPMENT OF KERATINOCYTE CANCER. Georgian Medical News. 2023, pp 63-67. PMID: 37354675.
- Worakunphanich, W.; Youngkong, S.; Suwankesawong, W.; Anderson, C.; Thavorncharoensap, M. Comparison of Patient Adverse Drug Reaction Reporting Systems in Nine Selected Countries. Int J Environ Res Public Health. 2022, 19 (8):4447. [CrossRef] [PubMed]
Figure 1.
Distribution of causality categories of reported ADR in more than one patient.
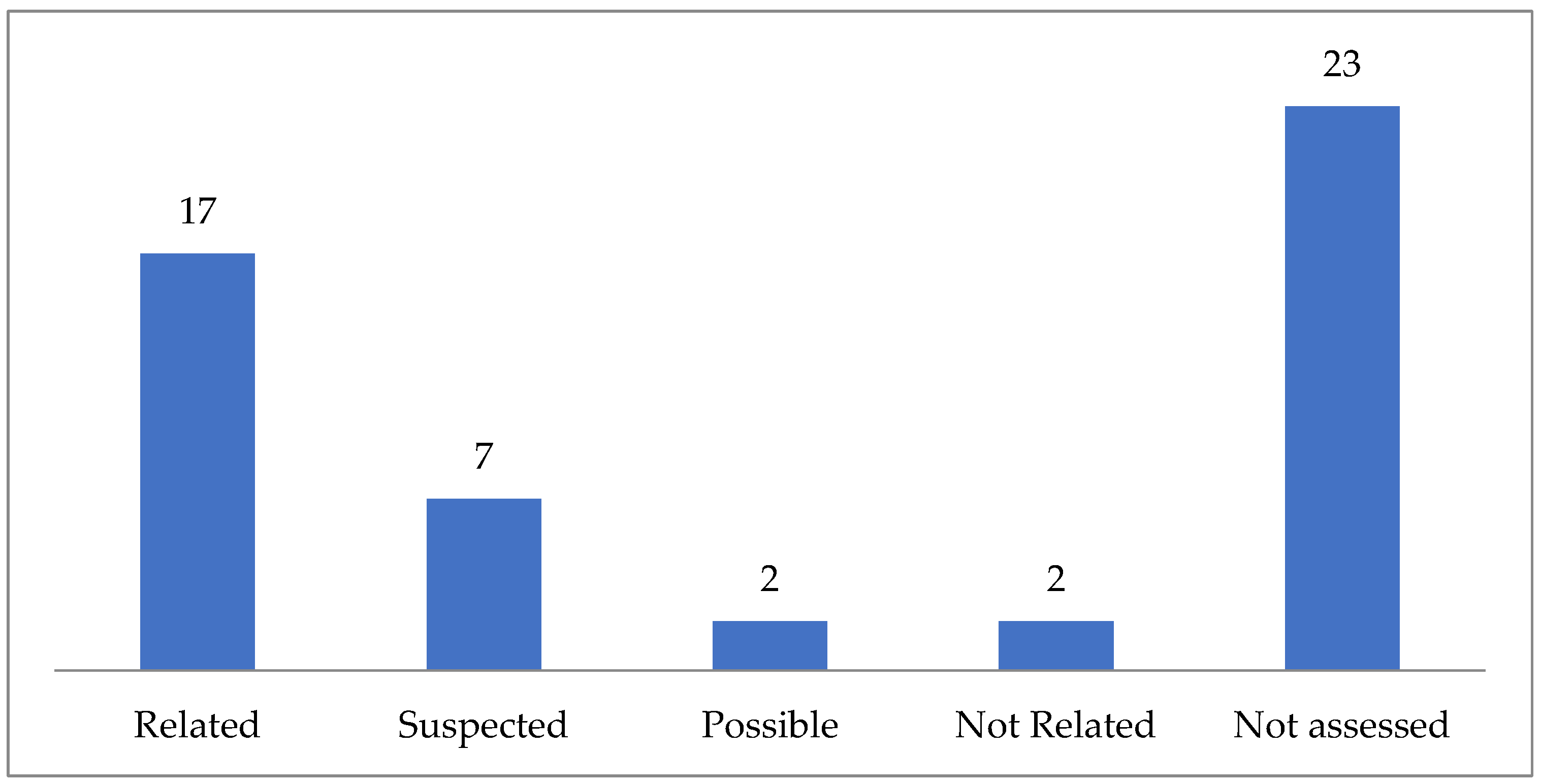

Table 1.
Distribution of ADRs by number, severity, expectancy, reporting type and person
| INN | Number (%)of reports | Number (%) of serious ADRs | Number (%)of expected ADRs | Number (%) of spontaneous reports | Number of reports submitted by | ||
| Physician | Patient | Other healthcare professional | |||||
| Atorvastatin | 7 (12.73) | 2 (3.64) | 6 (10.91) | 7 (12.73) | 5 | - | 2 |
| Simvastatin | 3 (5.45) | - | 3 (5.45) | 3 (5.45) | - | 1 | 2 |
| Rosuvastatin | 25 (45.45) | 16 (29.09) | 5 (9.09) | 25 (45.45) | 20 | 3 | 2 |
| Ezetimibe | 2 (3.64) | - | 1 (1.82) | 2 (3.64) | - | 1 | 1 |
| Evolocumab | 18 (32.73) | 2 (3.64) | 13 (23.64) | 5 (9.09) | 11 | 5 | 2 |
| Candesartan | 3 (5.17) | 2 (3.45) | 1 (1.72) | 3 (5.17) | 1 | 2 | |
| Irbesartan | 7 (12.07) | 7 (12.07) | - | 7 (12.07) | 5 | - | 2 |
| Olmesartan | 13 (22.41) | 10 (17.24) | 7 (12.07) | 13 (22.41) | 6 | 2 | 5 |
| Telmisartan | 7 (12.07) | 4 (6.90) | 4 (6.9) | 7 (12.07) | 3 | 2 | 2 |
| Valsartan | 28 (48.28) | 23 (39.66) | 4 (6.9) | 27 (46.55) | 20 | 2 | 6 |
| Ramipril | 12 (41.38) | 6 (20.69) | 11 (37.93) | 12 (41.38) | 3 | 2 | 7 |
| Enalapril | 3 (10.34) | 2 (6.90) | 3 (10.34) | 3 (10.34) | 2 | 1 | - |
| Lisinopril | 3 (10.34) | 1 (3.45) | 3 (10.34) | 3 (10.34) | 1 | - | 2 |
| Perindopril | 11 (37.93) | 4 (13.79) | 9 (31.03) | 7 (24.14) | 3 | 2 | 6 |
* The % is calculated based on a total number of reports for each pharmaco-therapeutic group (55 numbersfor antihyperlipidemics, 58 for sartans, and 29 for ACE-inhibitors).
Table 2.
ADRs occurring in more than one patient and included causality assessment in ICSR.
| INN | ADRin more than one patient | Causality assessment according to Global Introspection | Numberof patients (% fromtotal number of INN notifications)* |
|---|---|---|---|
| Atorvastatin | Increased glucose level | Related, Global Introspection, Health Care professional | 2 (28.57) |
| Hypoglycaemia | Related, Global Introspection, Health Care professional | 2 (28.57) | |
| Dry mouth | Related, Global Introspection, Health Care professional | 2 (28.57) | |
| Polydipsia | Related, Global Introspection, Health Care professional | 2 (28.57) | |
| Increased HbA1C | Related, Global Introspection, Health Care professional | 2 (28.57) | |
| Pollakiuria | Related, Global Introspection, Health Care professional | 2 (28.57) | |
| Rosuvastatin | Chest pain | not assessed | 4 (16.00) |
| Fatigue | not assessed | 3(12.00) | |
| Hypertension | not assessed | 3(12.00) | |
| Acute myocardial infarction | not assessed | 5(20.00) | |
| Acute coronary syndrome | not assessed | 3(12.00) | |
| Unstable angina | not assessed | 4(16.00) | |
| Evolocumab | Influenza like illness | not assessed | 4 (22.22) |
| Back pain | not assessed | 3(16.67) | |
| Limb pain | not assessed | 3(16.67) | |
| Vomiting | not assessed | 2(11.11) | |
| Myalgia | not assessed | 3(16.67) | |
| Rhinorhoea | not assessed | 3(16.67) | |
| Positive test for COVID-19 | not assessed | 2(11.11) | |
| Hematoma at the injection site | not assessed | 3(16.67) | |
| Irbesartan | Malignant melanoma | Related, Global Introspection, primary source reporter | 6(85.71) |
| Prostate Carcinoma Possible | not assessed | 2(28.57) | |
| Olmesartan | Malignant melanoma | not assessed | 8(61.54) |
| Squamous cell carcinoma | not assessed | 4(30.77) | |
| Headache | Related, Global Introspection Reporter | 2(15.38) | |
| Telmisartan | Malignant melanoma | Possible, Global introspection, Author | 2(28.57) |
| Hypertension | not assessed | 2(28.57) | |
| Fatigue | not assessed | 2(28.57) | |
| Chest pain | not assessed | 2(28.57) | |
| Valsartan | Malignant melanoma | Possible, Global Introspection, Author | 22(78.57) |
| Squamous cell carcinoma | not assessed | 4(14.29) | |
| Pruritus | Suspected, Global Introspection, primary source reporter | 4(14.29) | |
| Ramipril | Pulmonary hypertension | Suspected, Global Introspection, primary source reporter | 2(16.67) |
| Chest pain | Not assessed | 3(25.00) | |
| Fatigue | Suspected, Global Introspection, primary source reporter | 2(16.67) | |
| Cough | Related, Global Introspection, Health Care professional | 3(25.00) | |
| Joint swelling | Not Related, Global Introspection, Health Care professional | 3(25.00) | |
| Heart failure | Suspected, Global Introspection, primary source reporter | 2(16.67) | |
| Mitral valve incompetence | Suspected, Global Introspection, primary source reporter | 2(16.67) | |
| Tricuspid valve insufficiency | Not Related, Global Introspection, Health Care professional | 2(16.67) | |
| Cardiotoxicity | Suspected, Global Introspection, primary source reporter | 2(16.67) | |
| Dyspnoea | Suspected, Global Introspection, primary source reporter | 2(16.67) | |
| Pulmonary hypertension | Related, Global Introspection, Health Care professional | 2(16.67) | |
| Lisinopril | Hyperglycaemia | Related, Global Introspection, Health Care professional | 2(66.67 |
| Hypoglycaemia | Related, Global Introspection, Health Care professional | 2(66.67) | |
| Dry mouth | Related, Global Introspection, Health Care professional | 2(66.67) | |
| Polydipsia | Related, Global Introspection, Health Care professional | 2(66.67) | |
| Polyuria | Related, Global Introspection, Health Care professional | 2(66.67) | |
| Increased HbA1C levels | Related, Global Introspection, Health Care professional | 2(66.67) | |
| Perindopril | Ventricular tachycardia | not assessed | 3(27.27) |
| Heart failure | Related, Global Introspection, Health Care professional | 2(18.18) |
* The% is calculated fromthe total number of reports for everyINN, presented in the first column in Table 1.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



