Submitted:
30 August 2024
Posted:
02 September 2024
You are already at the latest version
Abstract
Cardiovascular diseases (CVDs) and their risk factors are a major cause of illness and death worldwide, especially in low- and middle-income countries like Cameroon. Physiotherapist-led health promotion (PLHP) has proven effective in improving health and reducing CVD risks. Understanding patient perspectives is crucial for designing effective, context-specific PLHP interventions. This study explored patients' views, experiences, perceived usefulness, acceptability, and preferred methods of PLHP through a sequential explanatory mixed-methods approach. The quantitative data highlights a significant burden of CVD conditions and risk factors among patients seen in physiotherapy services. Qualitatively, three themes were identified and included: 1) perspectives and experiences of people at risk or with CVDs (pwCVDs) on PLHP; 2) Perceived usefulness and acceptability of PLHP; 3) Preferred delivery methods of PLHP. Participants reported positive feedback on PLHP and physiotherapy services. Barriers to effective PLHP included high workloads for physiotherapists, limited service access in rural areas, and prohibitive costs. Despite these challenges, participants expressed strong confidence in physiotherapists' competence, though they also called for improved regulation and ongoing professional development. PLHP components, especially physical treatment and dietary advice, were deemed highly useful and acceptable. Patients suggested various delivery methods, including peer support groups, home visits, and mass media interventions. This study highlights the need to improve the scope of practice, competence of physiotherapists and accessibility of physiotherapy services in Cameroon for pwCVDs. It is necessary to adopt multidisciplinary approaches to achieve better outcomes for risk factors like diabetes and hypertension in context.
Keywords:
Cardiovascular diseases
; risk factors
; physiotherapist-led health promotion
; Cameroon
1. Introduction
Cardiovascular disease (CVD) and associated risk factors are responsible for a significant proportion of morbidity and mortality burden of all non-communicable diseases (NCDs) globally [1]. The global prevalence of CVD increased from 271 million in 1990 to 523 million in 2019 with an associated increase in deaths from 12.1 million to 18.6 million over the same period [2]. The majority of all CVD mortality occurs in people under 70 years of age, with Low- and Medium-Income Countries (LMIC) accounting for over 85% of these deaths [2]. This suggests that effective, context-specific interventions are still required to reduce this burden in LMIC [3].
In many LMICs, health systems are highly strained due to the double burden of infectious diseases and rising incidence of NCDs [4]. CVD account for approximately 10% of all hospital admissions in Sub-Saharan Africa [5]. One African study demonstrated an increase in the trend of CVD admission from 4.6% to 8.2% over a decade (2004-2015), representing a 78% increase over this period [6]. The increasing burden is associated with concurrent increases of modifiable risk factors such as tobacco use, unhealthy diet, overweight and obesity, physical inactivity and harmful use of alcohol in LMIC [7].
The burden of NCDs in Cameroon is rising, with risk factors overtaking some regional and global prevalence statistics. For example, 30.8% of Cameroonian women were living with high blood pressure in 2015 compared to 20.1% of women globally [8]. The prevalence of diabetes in Cameroon is estimated at 6% higher than in Africa at 3.85% prevalence [9,10]. Approximately 43.8% of Cameroonians use tobacco, compared with global figures of 36.1% [8]. An estimated 26% of Cameroonians live with hypercholesteremia compared to 25.5% among adults in Africa [11,12]. Hypertension is responsible for 41.3-54.49% of heart diseases in Cameroon [13,14]. CVD accounted for 10-16% of all hospitalisations in Cameroon, with the most prevalent CVDs being heart failure (38.5%), stroke (33.3%) and uncontrolled hypertension (22.4%) [15].
Healthcare providers in Cameroon need to address the challenge of avoidable risk factors to decrease the prevalence of CVD. There are limited effective Health Promotion (HP) strategies and implementation programmes, and this, coupled with an undeveloped and fragile health system, is contributing to the rising risk factors and CVD [15,16]. There is increasing evidence that public health interventions are cost-effective and that secondary prevention models such as cardiac rehabilitation (CR) provide several benefits to patients [17,18]. Despite these benefits, promotive and preventive intervention programs such as HP and CR uptake and adherence in resource-limited settings like Cameroon remain poor. This is due to various factors, including a lack of trained health personnel, limited resources, competing priorities, affordability, accessibility issues and lack of insurance coverage [19]. While there are extensive HP and prevention programs for people at risk or with CVD (pwCVDs) in High-Income Countries (HICs), they are either limited or completely absent in low-resource settings such as Cameroon [18].
With the absence of established HP and prevention programs in Cameroon, physiotherapists, with their core knowledge of physical interventions, exercise and health education, are well placed to assume this role [20,21]. Physiotherapist-Led Health Promotion (PLHP) may be a viable way to introduce or augment promotive and preventive interventions for pwCVDs. Physiotherapists manage a wide range of these patients and can engage them in HP and disease prevention through brief interventions (opportunistic advice, discussion, negotiation or encouragement on various key public health issues) [22,23]. Enabling meaningful patient involvement results in better-informed decisions regarding care choices and aligns patient preferences with the resources at hand, which is crucial for successful lifestyle interventions [24]. This can improve understanding of health issues, context, surrounding circumstances, relevant health needs, personal values, preferences and concerns about the proposed course of action [24]. As patient engagement becomes more effective, it fosters shared decision-making among practitioners and patients, thereby enhancing patient's long-term adherence to interventions. [25,26]. Patients' perceptions of healthcare providers significantly impact their adoption and adherence to lifestyle changes [27,28]. Having real patients articulate their fears and concerns about PLHP may allow physiotherapists to appreciate their patients' perspectives, build trust and provide care and education with better outcomes [24].
There is a lack of data on patient preferences and acceptability of HP interventions [29]. Closing this evidence gap is crucial for delivering quality, compassionate, and safe care, particularly in Cameroon, with its rising prevalence and burden of pwCVDs. Therefore, the aim of this mixed-methods study was to explore the perspectives of Cameroonian pwCVDs' experiences, needs, and preferences regarding a PLHP intervention and its delivery.
2. Materials and Methods
2.1. Study Design and Theoretical Underpinning
This study employed a two-part, sequential explanatory mixed-methods design following guidelines and recommendations for conducting and reporting mixed-methods studies [19,30]. This mixed-methods study was underpinned by a pragmatic paradigm and conducted in two phases [30]. In the first phase, a descriptive, cross-sectional survey was conducted to assess pwCVD views on PLHP in Cameroon. The specific objectives were, i) to investigate the experiences of pwCVDs regarding their health and PLHP, ii) to establish which components of PLHP pwCVDs they might find useful and acceptable. Data was collected from October 2nd, 2023, to December 29th, 2023. In the second phase, semi-structured interviews were conducted with a purposive sample of the surveyed participants to develop an in-depth understanding of their views of PLHP in Cameroon from January 15th, 2024, to February 16th, 2024. The specific objectives of the qualitative study were i) to explore the experiences and concerns of pwCVDs on PLHP, ii) to gain an in-depth understanding of which components pwCVDs find useful and acceptable, iii) to explore the preferred methods of PLHP delivery among pwCVDs
2.2. Study Setting
Physiotherapy practice in Cameroon lacks specialist physiotherapy services in either the public or private sectors [31]. Patients access physiotherapy services directly from home (self-referral), through referral by other healthcare providers in hospital settings, or through referrals from healthcare institutions without physiotherapy services. A small number of physiotherapists also work in private practice. The majority of physiotherapists are concentrated in urban areas, with very little formal provision of physiotherapy services in rural areas [32]. Therefore, patients in many rural areas who need physiotherapy services may need to travel to urban areas to access these services in established clinics and hospitals.
The study was conducted in physiotherapy services across four cities in Cameroon, namely, Bamenda, Buea, Douala and Yaoundé, to enhance access to an optimal number and diversity of pwCVDs. The physiotherapy services of the following hospitals were used: Regional Hospital Bamenda, Military Regional Hospital Yaoundé, Laquintinie Hospital Douala, Buea Regional Hospital, Idimed Polyclinic Douala, Yaoundé General Hospital, National Centre for the Rehabilitation of Persons with Disabilities, Yaoundé University Teaching Hospital, Bamenda Regional Hospital and Limbe Regional Hospital.
2.3. Study Population
All participants were pwCVDs accessing physiotherapy services for management of their condition and other related health concerns or complications. To be included in the study, participants had to be: Eighteen years or older, present with at least one risk factor for CVD (hypertension, diabetes, overweight and obesity, dyslipidaemia) OR present with a diagnosis of CVDs which may include heart failure, surgical heart condition, coronary artery disease, coronary heart disease, stroke or myocardial infarction [7]. All participants received physiotherapy for at least two weeks and could communicate well in French or English. Exclusion criteria included people with long-term cognitive or communication impairments preventing them from providing informed consent, for example, people living with Alzheimer’s disease and dysphasia. People who live with a pre-existing psychotic illness, such as schizophrenia, or those receiving end-of-life care were also not eligible to take part in the study.
2.4. Recruitment
Practising physiotherapists in participating services identified all eligible participants. Trained data collectors, i.e. physiotherapists, students on placement or the investigator (EN), then contacted the potential participant to explain the objectives of the study and procedure. A screening form with the inclusion and exclusion criteria for the study was used to assess participant eligibility. Each eligible participant, depending on his/her preference, was given an information sheet in English or French for the study. When consent was granted, the survey instrument was then administered electronically (Phase 1). During this phase, all consenting participants were asked whether they would be willing to take part in a follow-up interview (Phase 2). Participants provided their preferred contact details for later use in arranging the interview.
2.5. Phase 1: Quantitative
2.5.1. Patient Survey
The survey instrument was designed to collect the following data (supplementary file S1): Section A; demographic information, Section B; perception of pwCVDs towards PLHP and Section C; acceptability and usefulness of PLHP. The survey instrument took approximately 10-15 minutes to complete. The completed survey instrument was piloted, and all feedback was used to improve on the survey instrument before final administration.
2.5.2. Training of Data Collectors
Data collectors were trained by the lead author (ENN) in the selected hospital establishments. This constituted two physiotherapists and three physiotherapy students on clinical placement to enhance the continuity of data collection in the absence of the principal investigator. The training was directed towards understanding the purpose of the study, how to deliver the information sheet and seek consent, and how to access the survey tool, complete it and submit it electronically.
2.5.3. Sample Size Calculations
Calculator.net was used to estimate the sample size for the survey [33]. We used an estimated annual population size of 2000 pwCVDs across the participating hospitals and a population proportion of 90% with an eligible condition. With a significance level set at 0.05 and a margin of error of 5%, the sample size for this study was estimated to be approximately 130 participants. Other similar patient surveys examining patient preferences for treatment of LBP, inflammatory bowel disease, spinal surgery, and diabetes have recruited 130 – 170 participants [34,35,36]. To consider errors within estimates, the target sample was set at an upper limit of 170 participants.
2.5.4. Data Collection
The survey instrument was administered electronically via a link using mobile phones, tablets, iPads and laptops, independently by the patient or with the aid of a data collector. Where participants consented but had no means to complete the survey, the investigator or trained data collector facilitated completion on electronic devices dedicated to the study.
2.5.5. Data Analysis
Data were checked in Qualtrics. The data were then downloaded in Microsoft Excel format and transferred to SPSS (IBM SPSS Statistical Software, version 26.0) for statistical analysis. Descriptive statistics (frequencies, central tendency, dispersion/variation, and percentages) were used to present the demographic information and pattern of practice among participants. All data were considered in the analysis regardless of missing responses.
2.6. Phase 2: Qualitative Interviews
2.6.1. Sampling and Recruitment
Participants were selected purposively from those who provided preliminary consent to follow-up interviews as part of completing the survey (phase 1). This was based on gender, level of education, duration of receiving physiotherapy, various characteristics typical of pwCVDs and geographical locations of the patients. All participants were contacted via their preferred contact details, which they provided in Phase 1. Recruitment was done through telephone and in-person communication. Once participants provided written consent, arrangements were made to conduct the interview in a mutually convenient place, considering the participant and investigator's safety. For consistency, before each interview started, the investigator read a script that explained the purpose of the study, that participation was voluntary, that there were no known risks for participation, and what to expect in terms of content and duration of the interview.
2.6.2. Data Collection
Interviews were conducted face-to-face using individual semi-structured questionnaires. Permission was obtained from each participant to record the interview to ensure the accuracy of the resulting transcripts [37]. A topic guide (Supplementary file S2), informed by previous literature, facilitated the interviews [38]. The investigator used a general warm-up question specific to the patient's condition before addressing all central questions to build rapport in the presence of the audio recording device [39]. The interview recording was transcribed verbatim, including verbal expressions and body language that revealed considerable emotions and or expressions of feeling on specific issues [40]. A field diary was kept with comments and explanation of description and interpretation of patients’ responses.
2.6.3. Sample Size Determination
While a range of 3 to 10 participants is considered appropriate for qualitative studies using semi-structured interviews [41], a similar physiotherapy qualitative study used 13 participants [42]. We aimed for an upper limit of 20 participants as recommended for studies of lived experience or without a well-defined cultural domain [43]. This upper limit was assumed to provide adequate information based on the aims and the underdeveloped nature of the PLHP for pwCVDs [44]. However, data collection was stopped at 13 interviews as data saturation occurred and no further additional themes emerged from the dataset [45].
2.6.4. Data Analysis
The qualitative data collected was analysed using a two-stage reflective thematic analysis [46,47]. The first stage employed the 6-step thematic approach recommended by Braun and Clarke [46], and the second stage was a methodological reflection to understand and derive meaning from the generated data in context [47]. The interviews were transcribed and coded using NVivo 12 [48]. The results of the first interviews were used by the reviewers (ENN, BS) to develop common categories and subcategories, which were then clarified and supported with quotes from an interview transcript. The general categorisation evolved until the end of the analysis [46].
The methodological reflection was based on the categories obtained from the descriptive analysis, and conceptual categories were developed beyond merely describing the themes and subthemes to give interpretation to the thematic descriptions that emerged from the interviews [47].
A joint analysis was conducted by two researchers (ENN and BS) after they had analysed each interview separately. The interpretation of the interviews was verified by two co-investigators (RY and SM). The findings were written according to guidelines for reporting qualitative research [49].
2.7. Reflexivity
Engaging in reflexive thematic analysis requires researchers to acknowledge and express the underlying assumptions guiding their approach and interpretation of qualitative data [50]. In this study, coders practised reflexivity during the coding process by considering their professional role and research biases that could impact the interpretation of qualitative responses. The two qualitative coders in this study (ENN and BS) identify as black and white males, emerging and early middle-aged adults, with an interest in health promotion. Throughout the coding process, they remained mindful of their biases and endeavoured to assign themes based on data rather than their own biases informed by previous research and knowledge [50].
2.8. Triangulation and Integration of Findings
This study adopted and reported triangulation of data during data analysis and interpretation based on the methods (survey and qualitative findings), investigators (multiple observations) and data source (pwCVDs) at the end of the study [51]. The triangulation process involved the initial sorting of themes and categories from the qualitative data and relating it to the quantitative findings to create a coding matrix. The data was then analysed to see if there was agreement, dissonance, or partial agreement between the data sets [51].
3. Results
3.1. Participant Characteristics
A total of 146 respondents and 13 participants in phases 1 and 2, respectively, were included in the final analysis, with the characteristics summarised in Table 1. In phase 1, most of the respondents were females (52.7%), with the average mean age of all participants being 46.18±14.77 years. Respondents with primary education (29.0%, n=42) and undergraduate degrees (20.7%, n=30) constituted the higher proportions for education levels. Most respondents (68.4%, n=100) had multiple risk factors, with hypertension (60.9%, n=89) and overweight (56.8%, n=83) being the most prevalent. Stroke (45.2%, n=66) was the most prevalent CVD and was associated with multiple risk factors. Swelling of arms and legs (38.3%, n=56) and poor sleep (34.2%, n=50) were the most prevalent symptoms. The greatest challenges for pwCVDs included taking part in physical activity or exercise (56.8%, n=83), doing usual activities of daily living (56.0%, n=80) and making hospital visits (31.0%, n=44). The majority of respondents on medications (73.3%, n=117) followed medical recommendations for either health promotion or medical management of chronic conditions.
Semi-structured interviews were conducted with 13 participants, including males (n=7, 53.8%) and females (n=6, 46.2%) with a mean age of 56.31±12.11years ranging from 37 to 79 years. Participants had established CVD and multiple risk factors. Detailed characteristics of interviewed participants can be found in Table 2. Interviews took between 21 minutes and 38 minutes. By comparing interview data throughout the analysis process and observing that no new aspects, dimensions, or nuances of codes were emerging, we concluded that data saturation had been achieved.
3.2. Synthesised Findings
Analyses of the transcripts generated three themes, which included 1) perspectives and experiences of pwCVDs on PLHP; 2) Perceived usefulness of PLHP by pwCVDs; 3) Preferred delivery methods of PLHP (Figure 1). Complete and independent results of both the quantitative and qualitative phases can be found in supplementary file S3.
3.3. Perspectives and Experiences of pwCVDs on PLHP
3.3.1. Reasons for Attending Physiotherapy
The quantitative findings demonstrated a diverse range of CVDs and risk factors, with stroke as the leading CVD (93.0%, n=66), hypertension (36.77%, n=89) and overweight (34.30%, n=83) as the leading CVD risk factors. The leading symptoms among respondents were swelling of the limbs (38.36%, n=56) and poor sleep (34.25% n=50). The qualitative findings demonstrate that some participants access physiotherapy services primarily due to a cardiovascular condition or risk factors, while others had cardiovascular issues identified as a secondary concern, such as being overweight, having diabetes and hypertension. This could be following traumatic incident or low back pain among others.
“I started physiotherapy because of insomnia and being overweight” P3
“I was a victim of an accident. I was operated upon, and I was unable to move. I was bedridden. So, after the operation, the doctor advised that I could go for physiotherapy to help speed up the recovery. So, just like a week after the operation, I started physiotherapy” P7
3.3.2. Scope of PLHP Practice
The quantitative findings demonstrate that 58.9%, (n=86) of the respondents believe that the role of physiotherapist is not limited to exercise prescription. Qualitative findings also demonstrated that patients felt that although physiotherapists emphasised the importance of exercise and physical activity, they could also have a wider role in delivering other relevant aspects of HP. The majority of participants reported that they had received and appreciated information on a range of different PH topics related to alcohol (n=3), diet (n=8), etc, even though PTs might not be experts in these areas. Physiotherapists less frequently and more superficially covered HP activities related to sleep and lifestyle, etc. The majority of participants felt that physiotherapists could be delivering more strongly in a greater number of HP activities.
“What they do is just exercise, but as concerns nutrition and other health issues. I think no one has ever told me about it, regarding stress management, nothing.” P11
"I don't really know some areas of the therapist's scope of work, but they can advise us on diet which is good" P10
3.3.3. Relationship with Physiotherapists
The majority of the respondents indicated that their physiotherapists have never made them uncomfortable (81.4%, n=118) and can form good relationships with patients (79.45%, n=116). Qualitatively the majority of participants (12/13) reported to having very healthy and supportive relationships with physiotherapists, although 1/13 participant reported that not all physiotherapists form good and healthy relationships with their patients.
“No, there are very interesting people, "he laughs" for my own sessions that I had were very interesting, very interesting. A lot of encouragement and you could see results” P3
“But others look a little bit, more of military kind of harsh to patients, some of them, but not all. Others are wonderful” P12
3.3.4. Practice of Physiotherapy
The quantitative data shows less than half of respondents had discussions around treatment goals and objectives (47.9%, n=69). The qualitative findings also complemented this result. Three participants (3/13) were aware of the importance of goal setting in physiotherapy practice and acknowledged that they have yet to have discussions around treatment goals with their physiotherapist. Some participants were not aware of this, but some were aware that it is part of the approaches to physiotherapy practice.
“The first thing I would like to know from the physiotherapist is to know about my goals, which I never had. I have a problem with my lower back. At the end of the therapy, I should be able to do what I was unable to do before starting the therapy. So, that should be my goal at the end of my treatment. If I achieve my goal, then I know that things went well. Yes!” P10
Participants also perceived that the physiotherapy profession is not well regulated, and the training facilities are limited. Consequently, leading to a shortage of physiotherapists in many hospitals. Participants hold the view that physiotherapists should be professional in their approach and obtain contemporary and standardised training to be effective practitioners.
“First of all, I must say that what I've noticed that they are charlatan physiotherapists” P1
“So they really need to increase the number of people that are training in this area because you go to some hospitals, and you hardly find a physiotherapist. Then most of the time you have nursing aid assistant that have been trained informally in hospital settings, and they are handling this type of issues” P3
3.3.5. Need for a Multidisciplinary Approach to Health
The majority of respondents on medications (73.3%, n=117) followed medical recommendations for either health promotion or medical management of chronic conditions. The swelling of arms and legs (38.3%, n=56) and poor sleep (34.2%, n=50) were the most prevalent symptoms amongst the respondents. Qualitatively, participants held the view that physiotherapists cannot treat and manage all conditions and risk factors, such as diabetes and hypertension, independently and should work in synergy with other relevant clinicians.
“But in the real treatment, I think that the specialists of this area are more competent if they want to take it as a disease to treat. But for the physiotherapists, I see him handling it as something resulting from his own specialty and something which his advice can equally help to check. But for treatment per say, I don't think so” P1
3.3.6. Factors Affecting PLHP Practice
Our quantitative data shows only 18.6% of respondents (n=27) think that the workload of the physiotherapists limits their engagement in HP. The majority (40.6%, n=59) think workload has no impact on physiotherapists engagement in HP. The qualitative data suggests that participants believe the workload for the physiotherapy service was too much and may impact the ability of the physiotherapist to deliver HP messages. This then also translated to prolonged waiting time for the patients.
“So I just felt that they have a lot of work because the person that comes here is working elsewhere. He has full-time work. So when he comes here, maybe he has to rush to his office or has other patients to see, I just feel like they are not putting enough time” P4
“I think everything boils down to time. Sometimes I feel that I don't have enough time, the workload at the level of the physiotherapist (long waiting time)” P2
In addition, some participants (12/13) believe there is a significant demand for physiotherapy services, and people are suffering unnecessarily because they are unaware of the service's role and importance. They expressed concerns about limited access, especially for patients in rural areas, as services are primarily available in urban areas with a limited workforce. The number of physiotherapists needs to be increased to meet the growing demand. Participants suggested that, in addition to increasing the number and quality of physiotherapists, the government should provide subsidies and insurance policies to help citizens access these services, as the cost of physiotherapy sessions was identified as a major barrier to accessing the services, limiting the number of sessions for some and rendering therapy ineffective for others.
"Well, for the cost. I won't say it is quite affordable because someone who has to do physiotherapy, let's say, for 2 months, 3 months, and people go even beyond that. If you have to pay because, at the beginning, I had to come every day. So considering the standard of living here in our country, I think that the cost is not quite affordable for everyone" P7
“Subvention for citizens, the government chooses to subsidise this issue, if they want the improvement of their citizens, it's not all about money the government rules citizens. It doesn't rule people. People pay taxes because of their health care" P11
There is a belief among some participants that the government should implement policies for public awareness and education on health issues based on national statistics, emphasising that public health intervention should be strengthened rather than leaving health issues to individual patients.
“You know things that come from the government media is valued by the populace, where people believe that if they're saying this thing now and bring it out, you see the specialists coming to talk, people are taking more seriously because they are giving statistics, national statistics. At the macro level, what is happening in the nation with this and the consequences? People will take it more seriously rather than me going informally and doing my Google search and checking on it; when they start talking like that, it becomes a policy issue. Yes, and people will take it more seriously” P11
Most respondents (66.67%, n=96) reported that physiotherapists always praise and motivate them to reach their goals. Qualitative findings indicate that some participants (3/13) found visiting physiotherapy services more beneficial than joining sports clubs or exercising independently, as they struggled to maintain motivation on their own. They also noted that the lack of equipment and inadequate investment and training in physiotherapy services by hospital administrations contribute to the poor performance of these services.
“So I feel better here. If they can make it more frequent per client, it will be nice. I come and exercise, somebody follows me, is very nice, in the club is not the same. People are doing it their own and, in the club, you may injure one part of your body. Just because they just do their business you know, they are not specialists most of the time" P3
"Alone I cannot do it but when I come here, they are very specific. And I do not really like it alone because whenever I'm tired, I just get up and go. But here they say, no, 15 minutes, you still have 3 minutes and I make the effort" P13
Additionally, participants (3/13) felt that some of the education and advice from physiotherapists were unclear and not patient-centred, making them difficult to follow. The advice sometimes seemed passive, as patients felt instructed to follow it without understanding its importance. Participants expressed a desire for PLHP services to be extended to home visits or self-delivery.
“Yeah, because what I’m saying is that when you tell him to do some physical exercise, which by his very nature, he cannot do it, it means nothing. So, it is good to tell somebody what he can do. I've had the experience where I'm told what to do, which I cannot do" P1.
"I would love that. But because I am having challenges, I think that doing it in a group might not be very comfortable working in a group. That's why I always like home visits; I'm still striving for home visits" P5
3.3.7. Confidence in Physiotherapists
Quantitatively, 60% of respondents (n=87) believe that physiotherapists have the skills to assist them with their conditions. This was further supported by the qualitative findings as the majority of the participants expressed strong confidence and trust in the physiotherapy workforce. While some participants (4/13) expressed reservations about fully trusting their physiotherapist, they still found them to be very helpful in their practice. Regarding training and competence, participants acknowledged that physiotherapists are generally competent but noted there is room for improvement. Some participants (7/13) felt that, regardless of their perception of competence, the managers of physiotherapy establishments should ensure competence and standards of practice. Also, some participants believe that physiotherapists need ongoing support and supervision in their practice.
“The physiotherapist wants me to be well. So, I don't think that is any advice or restrictions that they can give me, which can be contrary to essence, I don't think so. What I got, help me and for me, what they do, I don't see anything to object” P4
“Most of the time they are lacking, and they need somebody who should be overseeing them, who is actually very professional overseeing them, especially in the government settings” P3
3.4. Perceived Usefulness and Acceptability of PLHP
3.4.1. Components Found to Be Useful
The quantitative data shows that the majority of the respondents perceived PLHP to be very useful with a mean score of 86.8% (n=124) across all components (i.e. diet, sleep, stress management etc). The component with the highest proportion of perceived usefulness was dietary advice on fruits (91.6%, n=132), and the lowest was advice or education to stop smoking (75.35%, n=107). The qualitative data revealed that participants viewed diet and nutrition as a crucial aspect of PLHP, recognising the importance of combining it with other components. Some participants also deemed physical treatment essential, including exercises on the treatment bed. Most participants found the education and interventions provided by physiotherapists to be universally useful, without a preference for specific components.
“What I know is that their advice, in general, is useful. Yes, I know that is useful, but to say, I can choose one for the other, no” P1
“No, no, "Nodding in disagreement" they should talk about everything. They should talk of everything that will help me. That is it” P 6
3.4.2. Components Found to More Acceptable
The majority of the respondents found PLHP advice/education acceptable across multiple components with a mean score of 94.65% (n=131). Increasing general physical activity advice was the component that was most acceptable (95.80%, n=137). Conversely, advice on alcohol consumption had the highest rate of unacceptability, with 4.8% (n=7) of respondents. This is because respondents not drinking alcohol do not value such counsel. Qualitative findings indicated that participants viewed these interventions and educational efforts as highly beneficial and essential for managing their conditions. They emphasised that such resources should be publicly accessible, with physiotherapists playing a key role in leading exercises, planning, and educating the public, given their crucial impact on health outcomes.
“When I suddenly had a stroke in 2013, it was necessary for me to get to physiotherapy for treatment. Well, I can say that was an important element in my treatment because they said it. Yes, I was heavily encouraged to do that. Let me add that it helped me a lot" P1
“Physiotherapists hold a transformational position in people's health” P9
3.5. Preferred Methods of PLHP Delivery
This aspect was only explored during the qualitative phase of the study. Participants proposed and justified a variety of delivery methods based on their experiences, conditions, circumstances, or observations of the physiotherapy service. Patient peer support groups were considered beneficial for sharing experiences and challenges to improve adherence with PH interventions. Some participants, due to personal challenges such as communication or mobility issues, valued privacy and preferred home visits, although they acknowledged that arranging and maintaining these visits can be costly. Participants also advocated for one-on-one discussions or education, citing reasons such as mobility issues, different pathologies, and the need to clarify doubts. Some participants preferred group discussions and lectures with physiotherapists, as this saves time and ensures effective communication, especially for people with similar conditions. Others suggested that regular audiovisual or mass media slots could have a broader impact on disease prevention and health promotion. Some preferred workshops, seminars, or regular talks, provided they are invited in advance, either free or at a minimal cost. Participants also mentioned positive experiences with using apps and expressed interest in having access to them. Participants also highlighted that written or printed information is helpful for various reasons, though a few found it challenging due to reduced vision. A few participants expressed no preference for the delivery method but valued any information that could potentially improve their health (Sample quotes can be found in supplementary file S3, qualitative results).
4. Discussion
This mixed-methods study aimed to provide a comprehensive overview of patients' experiences, perceptions, and preferences of PLHP for pwCVDs in Cameroon to inform intervention development. Our data reflects participants' views of multiple risk factors and challenges and demonstrates positive perceptions of PLHP delivered via multiple methods. There was good agreement of the qualitative and quantitative data across the study elements.
Consistent with previous research from Ghana among stroke patients [52], approximately two-thirds (68.4%) of our respondents had multiple CVD risk factors. They, however, reported a higher prevalence for hypertension (85%) and obesity (58%) compared with 60.9% and 56.8% in our study, respectively. These differences could be explained by their study being conducted among stroke survivors [52]. Conversely, Mastwyk and colleagues in Australia reported a 37% and 58% prevalence of metabolic syndrome and hypertension among clients attending private practice physiotherapy with predominantly musculoskeletal conditions (94%). The differences could be attributed to their study population of musculoskeletal patients with potentially lower levels of CVD markers than in our study population on CVD [53]. The high levels of varied CVD risk factors reported in our study and in the general Cameroon population highlight the need for PLHP strategies adopting multimodal strategies to address this complex problem in Cameroon [5,6,9]. Physiotherapists are well-placed to deliver these HP interventions for pwCVD, other clinical populations and the general population [21,54].
Consistent with previous research on patients' experiences with physiotherapy services from Kenya and Spain [55,56], our participants reported excellent/good cordial relationships with physiotherapists and perceived PLHP interventions as useful and effective for managing their condition and improving their health. Despite positive perceptions, participants presented challenges related to the competence and scope of practice of physiotherapists, demonstrating the need for comprehensive training and skill development beyond exercise and physical activity to better address their needs. This supports the findings of Severin and colleagues that only 14.8% of physical therapists measure blood pressure and pay attention to examining and educating patients on CVD risk factors in the USA [57]. This may be because of the existence of specialist respiratory therapists in the USA, who tend to deal with patients who have complex cardiac and pulmonary conditions [58]. Physiotherapists' workloads due to a lack of staff and equipment resulting from prolonged waiting time were reported in our study. This is consistent with previous data reporting 0.92 physiotherapists per 100000 population in Cameroon and similar across many African countries [55,59], which compares less than favourably with other countries such as South Africa and Germany with 13 and 234.4 physiotherapists per 100000 respectively [58]. For participants with high levels of disability coupled with challenges to accessing physiotherapy services may mandate a shift towards community-based services to facilitate access. Facilitating community-based programs necessitates collaboration and empowerment of community-based workers and expert patient groups to increase access and sustainability through affordable mechanisms and provide effective health education [21,55].
Contrary to growing evidence that written prescription is more effective and motivating than oral advice for improving lifestyle changes such as physical activity [60,61], the majority of our participants expressed a preference for individual discussions and, to a lesser extent, regular planned educational sessions, group discussions, lectures, printed information, use of apps among others. This could be explained by the degree to which resources are available in Cameroon including relevant evidence, internet and printers. Patient-related factors were also highlighted by our participants, including loss of eyesight with aging, making reading challenging. Oral advice was preferred because of the advantage of clarifying doubts following relevant questioning. This highlights and emphasises the need for context and patient-centred considerations in clinical practice.
In summary, the findings of this study suggest that pwCVD perceives PLHP delivery across many components as useful and acceptable. Many positive and some negative patient' experiences of physiotherapists delivering PH interventions were identified. Positive and negative experiences also facilitated or limited access to PH information or affected the quality of PLHP interventions. This, coupled with the high prevalence of CVDs and risk factors for CVD, creates an imperative for a more systematic and comprehensive approach to PLHP in Cameroon [62].
4.1. Implications for Practice, Training and Research
Practice
All Physiotherapists should understand how risk factors influence the development and progression of CVD and be competent in delivering lifestyle education, diet, stress management, and sleep hygiene interventions, in addition to exercise and physical activity. Therefore, there is a mandate for the Cameroon Society of Physiotherapy (CASP), the Ministry of Public Health, and relevant stakeholders to organise professional development training that covers this wide range of HP activities for practising physiotherapists. Community-based initiatives and collaboration with community-based health workers and expert patient groups may also be valuable options [63]. A variety of flexible PH delivery methods would support physiotherapists in delivering PH messages to a larger population that may improve compliance and adherence, leading to better health outcomes. Mass media and community outreach may also facilitate patient education and behaviour change. Collaboration with other healthcare professionals is crucial to enhance the delivery of PLHP intervention and improve patient outcomes.
Training
The undergraduate physiotherapy training courses need to be comprehensive, covering key aspects of HP, such as relevant assessment tools on lifestyle-related behaviours, counselling skills, and the use of behaviour change strategies for specific HP components [21]. This will enable qualified physiotherapists to be confident in delivering HP interventions.
Research
Additional research is needed to explore the long-term impacts of PLHP interventions for pwCVDs management and outcomes in the Cameroonian context. Therefore, to allocate limited resources effectively, it is necessary to investigate the effectiveness of different PLHP components (e.g., dietary advice and stress management) in improving cardiovascular health. Research should focus on developing and testing patient-centred PLHP models considering individual preferences and barriers.
4.2. Strengths and Limitations
The use of both quantitative and qualitative methods provided a comprehensive understanding of pwCVDs' perceptions and experiences in physiotherapy services. We also included a diverse sample of participants from four regions of Cameroon across several physiotherapy services, enhancing the generalizability of the findings. Qualitative interviews offered great depth and insights into patients' personal experiences and perceptions of our findings.
The relatively small sample size, particularly for the qualitative component, may limit the generalizability of the findings. However, the recruitment of all participants in the qualitative phase was based on criteria that represented the sample, including gender, condition, and duration of exposure to physiotherapists. Secondly, reliance on self-reported data might have introduced bias, as participants might overestimate or underestimate their experiences and perceptions.
5. Conclusions
The findings demonstrate positive perceptions and experiences of physiotherapists delivering a variety of PH information and advice in Cameroon with wide acceptance of PLHP interventions. However, pwCVDs also report unmet needs related to service provision, personalisation and tailoring of PLHP interventions. This finding resonates with prior literature on disciplinary workforce development for wider HP intervention engagement and delivery. This underscores the need to enhance physiotherapy entry-level training in Cameroon. Additionally, relevant stakeholders must develop strategies to extend the delivery of PLHP interventions beyond urban areas to rural and remote settings.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Supplementary files S1: The survey, S2: Topic guide for the second phase, and S3: The complete Quantitative and Qualitative results
Author Contributions
Conceptualisation, E.N.N. and S.M.; methodology E.N.N., S.M, C.K. R.Y and J.L.; validation, E.N.N., S.M, C.K. R.Y, B.S., and J.L; formal analysis, E.N.N, and B.S.; data curation, E.N.N and S.M; writing—original draft preparation, E.N.N..; writing—review and editing, E.N.N., S.M, C.K. R.Y and J.L.; supervision, S.M, C.K. R.Y and J.L project administration, E.N.N.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study received ethics approval from Sheffield Hallam University research committee (ER47597467) and from the Cameroon National Ethics Committee for Human Health Research (2023/10/1595/CE/CNERSH/SP). Administrative authorisation was obtained from all participating institutions.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the corresponding authors on request.
Acknowledgments
The authors acknowledged the substantial contributions of these two physiotherapists, Gina Sandra Talongwa Pokam and Vanheime Kom Fokou in making the survey data collection successful in the Litorral Region of Cameroon.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Liu, J.; Bu, X.; Wei, L.; Wang, X.; Lai, L.; Dong, C.; Ma, A.; Wang, T. Global Burden of Cardiovascular Diseases Attributable to Hypertension in Young Adults from 1990 to 2019. J. Hypertens. 2021, 39, 2488–2496. [Google Scholar] [CrossRef]
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef]
- Druetz, T. Integrated Primary Health Care in Low- and Middle-Income Countries: A Double Challenge. BMC Med. Ethics 2018, 19, 48. [Google Scholar] [CrossRef]
- Mudie, K.; Jin, M.M.; Tan; Kendall, L.; Addo, J.; dos-Santos-Silva, I.; Quint, J.; Smeeth, L.; Cook, S.; Nitsch, D.; et al. Non-Communicable Diseases in Sub-Saharan Africa: A Scoping Review of Large Cohort Studies. J. Glob. Health 2019, 9, 020409. [Google Scholar] [CrossRef]
- Nkoke, C.; Jingi, A.M.; Makoge, C.; Teuwafeu, D.; Nkouonlack, C.; Dzudie, A. Epidemiology of Cardiovascular Diseases Related Admissions in a Referral Hospital in the South West Region of Cameroon: A Cross-Sectional Study in Sub-Saharan Africa. PLOS ONE 2019, 14, e0226644. [Google Scholar] [CrossRef]
- Appiah, L.T.; Sarfo, F.S.; Agyemang, C.; Tweneboah, H.O.; Appiah, N.A.B.A.; Bedu-Addo, G.; Opare-Sem, O. Current Trends in Admissions and Outcomes of Cardiac Diseases in Ghana. Clin. Cardiol. 2017, 40, 783–788. [Google Scholar] [CrossRef]
- Keates, A.K.; Mocumbi, A.O.; Ntsekhe, M.; Sliwa, K.; Stewart, S. Cardiovascular Disease in Africa: Epidemiological Profile and Challenges. Nat. Rev. Cardiol. 2017, 14, 273–293. [Google Scholar] [CrossRef]
- Dzudie, A.; Fourie, J.M.; Scholtz, W.; Scarlatescu, O.; Nel, G.; Kingue, S. PASCAR and WHF Cardiovascular Diseases Scorecard Project. 2020, 31, 8. [Google Scholar] [CrossRef]
- Dessie, G.; Mulugeta, H.; Amare, D.; Negesse, A.; Wagnew, F.; Getaneh, T.; Endalamew, A.; Adamu, Y.W.; Tadesse, G.; Workineh, A.; et al. A Systematic Analysis on Prevalence and Sub-Regional Distribution of Undiagnosed Diabetes Mellitus among Adults in African Countries. J. Diabetes Metab. Disord. 2020, 19, 1931–1941. [Google Scholar] [CrossRef]
- IDF Atlas 9th Edition and Other Resources. Available online: https://www.diabetesatlas.org/en/resources/ (accessed on 14 August 2020).
- Noubiap, J.J.; Bigna, J.J.; Nansseu, J.R.; Nyaga, U.F.; Balti, E.V.; Echouffo-Tcheugui, J.B.; Kengne, A.P. Prevalence of Dyslipidaemia among Adults in Africa: A Systematic Review and Meta-Analysis. Lancet Glob. Health 2018, 6, e998–e1007. [Google Scholar] [CrossRef]
- WHO | World Health Statistics 2016: Monitoring Health for the SDGs. Available online: http://www.who.int/gho/publications/world_health_statistics/2016/en/ (accessed on 15 August 2020).
- Akono, M.N.; Simo, L.P.; Agbor, V.N.; Njoyo, S.L.; Mbanya, D. The Spectrum of Heart Disease among Adults at the Bamenda Regional Hospital, North West Cameroon: A Semi Urban Setting. BMC Res. Notes 2019, 12, 761. [Google Scholar] [CrossRef]
- Nkoke, C.; Makoge, C.; Dzudie, A.; Mfeukeu, L.K.; Luchuo, E.B.; Menanga, A.; Kingue, S. A Predominance of Hypertensive Heart Disease among Patients with Cardiac Disease in Buea, a Semi-Urban Setting, South West Region of Cameroon. BMC Res. Notes 2017, 10, 684. [Google Scholar] [CrossRef]
- Nkoke, C.; Jingi, A.M.; Makoge, C.; Teuwafeu, D.; Nkouonlack, C.; Dzudie, A. Epidemiology of Cardiovascular Diseases Related Admissions in a Referral Hospital in the South West Region of Cameroon: A Cross-Sectional Study in Sub-Saharan Africa. PLOS ONE 2019, 14, e0226644. [Google Scholar] [CrossRef]
- Global Action Plan for the Prevention and Control of NCDs 2013-2020. Available online: https://www.who.int/publications-detail-redirect/9789241506236 (accessed on 8 March 2022).
- Owen, L.; Pennington, B.; Fischer, A.; Jeong, K. The Cost-Effectiveness of Public Health Interventions Examined by NICE from 2011 to 2016. J. Public Health 2018, 40, 557–566. [Google Scholar] [CrossRef]
- Supervia, M.; Turk-Adawi, K.; Lopez-Jimenez, F.; Pesah, E.; Ding, R.; Britto, R.R.; Bjarnason-Wehrens, B.; Derman, W.; Abreu, A.; Babu, A.S.; et al. Nature of Cardiac Rehabilitation Around the Globe. EClinicalMedicine 2019, 13, 46–56. [Google Scholar] [CrossRef]
- Meissner, H.; Creswell, J.; Klassen, A.C.; Plano, V.; Smith, K.C. Best Practices for Mixed Methods Research in the Health Sciences. 61.
- Dean, E.; Greig, A.; Murphy, S.; Roots, R.; Nembhard, N.; Rankin, A.; Bainbridge, L.; Anthony, J.; Hoens, A.M.; Garland, S.J. Raising the Priority of Lifestyle-Related Noncommunicable Diseases in Physical Therapy Curricula. Phys. Ther. 2016, 96, 940–948. [Google Scholar] [CrossRef]
- Dean, E.; Skinner, M.; Myezwa, H.; Mkumbuzi, V.; Mostert, K.; Parra, D.C.; Shirley, D.; Söderlund, A.; de Andrade, A.D.; Abaraogu, U.O.; et al. Health Competency Standards in Physical Therapist Practice. Phys. Ther. 2019, 99, 1242–1254. [Google Scholar] [CrossRef]
- McLean, S.; Charlesworth, L.; May, S.; Pollard, N. Healthcare Students’ Perceptions about Their Role, Confidence and Competence to Deliver Brief Public Health Interventions and Advice. BMC Med. Educ. 2018, 18, 114. [Google Scholar] [CrossRef]
- Rawlinson, G. Health Promotion in Physiotherapy Services Using NHS Health and Diabetes Checks. Br. J. Healthc. Manag. 2019, 25, 22–31. [Google Scholar] [CrossRef]
- Bombard, Y.; Baker, G.R.; Orlando, E.; Fancott, C.; Bhatia, P.; Casalino, S.; Onate, K.; Denis, J.-L.; Pomey, M.-P. Engaging Patients to Improve Quality of Care: A Systematic Review. Implement. Sci. 2018, 13, 98. [Google Scholar] [CrossRef]
- Hargraves, I.; LeBlanc, A.; Shah, N.D.; Montori, V.M. Shared Decision Making: The Need For Patient-Clinician Conversation, Not Just Information. Health Aff. (Millwood) 2016, 35, 627–629. [Google Scholar] [CrossRef]
- Puhl, R.; Peterson, J.L.; Luedicke, J. Motivating or Stigmatizing? Public Perceptions of Weight-Related Language Used by Health Providers. Int. J. Obes. 2013, 37, 612–619. [Google Scholar] [CrossRef]
- Allison, K.; Delany, C.; Setchell, J.; Egerton, T.; Holden, M.; Quicke, J.; Bennell, K. A Qualitative Study Exploring the Views of Individuals with Knee Osteoarthritis on the Role of Physiotherapists in Weight Management: A Complex Issue Requiring a Sophisticated Skill Set. Musculoskeletal Care 2019, 17, 206–214. [Google Scholar] [CrossRef]
- Berry, L.L.; Parish, J.T.; Janakiraman, R.; Ogburn-Russell, L.; Couchman, G.R.; Rayburn, W.L.; Grisel, J. Patients’ Commitment to Their Primary Physician and Why It Matters. Ann. Fam. Med. 2008, 6, 6–13. [Google Scholar] [CrossRef]
- Heine, M.; Fell, B.L.; Robinson, A.; Abbas, M.; Derman, W.; Hanekom, S. Patient-Centred Rehabilitation for Non-Communicable Disease in a Low-Resource Setting: Study Protocol for a Feasibility and Proof-of-Concept Randomised Clinical Trial. BMJ Open 2019, 9, e025732. [Google Scholar] [CrossRef]
- University of Arkansas; Venkatesh, V.; Brown, S.; University of Arizona; Sullivan, Y.; State University of New York, Binghamton. Guidelines for Conducting Mixed-Methods Research: An Extension and Illustration. J. Assoc. Inf. Syst. 2016, 17, 435–494. [Google Scholar] [CrossRef]
- Cameroon Society of Physiotherapy. Available online: https://world.physio/membership/cameroon (accessed on 20 June 2022).
- Physiotherapy Practice Start up, Cameroon. Available online: https://www.indiegogo.com/projects/1307213 (accessed on 8 July 2022).
- Sample Size Calculator. Available online: https://www.calculator.net/sample-size-calculator.html?type=1&cl=95&ci=5&pp=50&ps=400&x=44&y=23 (accessed on 15 August 2023).
- Gogovor, A.; Visca, R.; Ware, M.A.; Valois, M.-F.; Bartlett, G.; Hunt, M.; Ahmed, S. Determinants Of Patient Experience With Low Back Pain Interdisciplinary Care: A Pre-Post Interventional Study. J. Pain Res. 2019, Volume 12, 3203–3213. [Google Scholar] [CrossRef]
- Kariburyo, M.F.; Xie, L.; Teeple, A.; Tan, H.; Ingham, M. Predicting Pre-Emptive Discussions of Biologic Treatment: Results from an Openness and Preference Survey of Inflammatory Bowel Disease Patients and Their Prescribers. Adv. Ther. 2017, 34, 1398–1410. [Google Scholar] [CrossRef]
- Knisely, B.M.; Vaughn-Cooke, M. A Comprehensive Survey of Preference for Personal Health Record Features in Patients with Diabetes. Proc. Int. Symp. Hum. Factors Ergon. Health Care 2020, 9, 171–175. [Google Scholar] [CrossRef]
- Rutakumwa, R.; Mugisha, J.O.; Bernays, S.; Kabunga, E.; Tumwekwase, G.; Mbonye, M.; Seeley, J. Conducting In-Depth Interviews with and without Voice Recorders: A Comparative Analysis. Qual. Res. 2020, 20, 565–581. [Google Scholar] [CrossRef]
- Ngeh, E.N.; Lowe, A.; Garcia, C.; McLean, S. Physiotherapy-Led Health Promotion Strategies for People with or at Risk of Cardiovascular Diseases: A Scoping Review. Int. J. Environ. Res. Public. Health 2023, 20, 7073. [Google Scholar] [CrossRef]
- DiCicco-Bloom, B.; Crabtree, B.F. The Qualitative Research Interview. Med. Educ. 2006, 40, 314–321. [Google Scholar] [CrossRef]
- McLellan, E.; MacQueen, K.M.; Neidig, J.L. Beyond the Qualitative Interview: Data Preparation and Transcription. Field Methods 2003, 15, 63–84. [Google Scholar] [CrossRef]
- Smith, J.; Flowers, P.; Larkin, M. Interpretative Phenomenological Analysis: Theory, Method and Research; 2009; Vol. 6, ISBN 978-1-4129-0834-4. [Google Scholar]
- Sadler, E.; Wolfe, C.D.A.; Jones, F.; McKevitt, C. Exploring Stroke Survivors’ and Physiotherapists’ Views of Self-Management after Stroke: A Qualitative Study in the UK. BMJ Open 2017, 7, e011631. [Google Scholar] [CrossRef]
- Bernard, H. Social Research Methods : Qualitative and Quantitative Approaches, 2nd ed.; Sage: Thousand Oaks CA, 2013; ISBN 978-1-4129-7854-5. [Google Scholar]
- Malterud, K.; Siersma, V.D.; Guassora, A.D. Sample Size in Qualitative Interview Studies: Guided by Information Power. Qual. Health Res. 2016, 26, 1753–1760. [Google Scholar] [CrossRef]
- Guest, G.; Namey, E.; Chen, M. A Simple Method to Assess and Report Thematic Saturation in Qualitative Research. PLOS ONE 2020, 15, e0232076. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using Thematic Analysis in Psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Reflecting on Reflexive Thematic Analysis. Qual. Res. Sport Exerc. Health 2019, 11, 589–597. [Google Scholar] [CrossRef]
- Best Qualitative Data Analysis Software for Researchers | NVivo. Available online: https://www.qsrinternational.com/nvivo-qualitative-data-analysis-software/home (accessed on 24 April 2022).
- O’Brien, B.C.; Harris, I.B.; Beckman, T.J.; Reed, D.A.; Cook, D.A. Standards for Reporting Qualitative Research: A Synthesis of Recommendations. Acad. Med. 2014, 89, 1245–1251. [Google Scholar] [CrossRef]
- Olmos-Vega, F.M.; Stalmeijer, R.E.; Varpio, L.; Kahlke, R. A Practical Guide to Reflexivity in Qualitative Research: AMEE Guide No. 149. Med. Teach. 2023, 45, 241–251. [Google Scholar] [CrossRef]
- Carter, N.; Bryant-Lukosius, D.; DiCenso, A.; Blythe, J.; Neville, A.J. The Use of Triangulation in Qualitative Research. Oncol. Nurs. Forum 2014, 41, 545–547. [Google Scholar] [CrossRef]
- Sarfo, F.; Acheampong, J.; Appiah, L.; Oparebea, E.; Akpalu, A.; Bedu-Addo, G. The Profile of Risk Factors and In-Patient Outcomes of Stroke in Kumasi, Ghana. Ghana Med. J. 2014, 48, 127. [Google Scholar] [CrossRef]
- Mastwyk, S.; Taylor, N.F.; Lowe, A.; Dalton, C.; Peiris, C.L. Metabolic Syndrome Is Prevalent and Undiagnosed in Clients Attending Private Practice Physiotherapy: A Cross-Sectional Study. Physiotherapy 2024, 124, 116–125. [Google Scholar] [CrossRef]
- Dean, E.; Moffat, M.; Skinner, M.; Dornelas de Andrade, A.; Myezwa, H.; Söderlund, A. Toward Core Inter-Professional Health Promotion Competencies to Address the Non-Communicable Diseases and Their Risk Factors through Knowledge Translation: Curriculum Content Assessment. BMC Public Health 2014, 14, 717. [Google Scholar] [CrossRef]
- Gona, J.; Newton, C.R.; Geere, J.-A.; Hartley, S. Users’ Experiences of Physiotherapy Treatment in a Semi-Urban Public Hospital in Kenya. Available online: https://www.rrh.org.au/journal/article/2210/ (accessed on 9 July 2024).
- Del Baño-Aledo, M.E.; Medina-Mirapeix, F.; Escolar-Reina, P.; Montilla-Herrador, J.; Collins, S.M. Relevant Patient Perceptions and Experiences for Evaluating Quality of Interaction with Physiotherapists during Outpatient Rehabilitation: A Qualitative Study. Physiotherapy 2014, 100, 73–79. [Google Scholar] [CrossRef]
- Severin, R.; Wang, E.; Wielechowski, A.; Phillips, S.A. Outpatient Physical Therapist Attitudes Toward and Behaviors in Cardiovascular Disease Screening: A National Survey. Phys. Ther. 2019, 99, 833–848. [Google Scholar] [CrossRef]
- Physicians and Physiotherapists in the EU: How Many? Available online: https://ec.europa.eu/eurostat/web/products-eurostat-news/w/ddn-20230818-1 (accessed on 14 August 2024).
- Kossi, O. Training, Care Delivery, and Research in Physiotherapy in Sub-Saharan French-Speaking Africa. South Afr. J. Physiother. 2023, 79. [Google Scholar] [CrossRef]
- Elley, C.R. Effectiveness of Counselling Patients on Physical Activity in General Practice: Cluster Randomised Controlled Trial. BMJ 2003, 326, 793–793. [Google Scholar] [CrossRef]
- Grandes, G. Effectiveness of Physical Activity Advice and Prescription by Physicians in Routine Primary CareA Cluster Randomized Trial. Arch. Intern. Med. 2009, 169, 694. [Google Scholar] [CrossRef]
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and Evaluating Complex Interventions: The New Medical Research Council Guidance. BMJ 2008, a1655. [Google Scholar] [CrossRef]
- Griffiths, C.; Foster, G.; Ramsay, J.; Eldridge, S.; Taylor, S. How Effective Are Expert Patient (Lay Led) Education Programmes for Chronic Disease? BMJ 2007, 334, 1254–1256. [Google Scholar] [CrossRef]
Figure 1.
Summary of the qualitative findings showing the first and second-order themes of phase 2. *PLHP: Physiotherapist-led health promotion, pwCVDs: People at risk or with cardiovascular diseases, PT: physiotherapist.
Figure 1.
Summary of the qualitative findings showing the first and second-order themes of phase 2. *PLHP: Physiotherapist-led health promotion, pwCVDs: People at risk or with cardiovascular diseases, PT: physiotherapist.
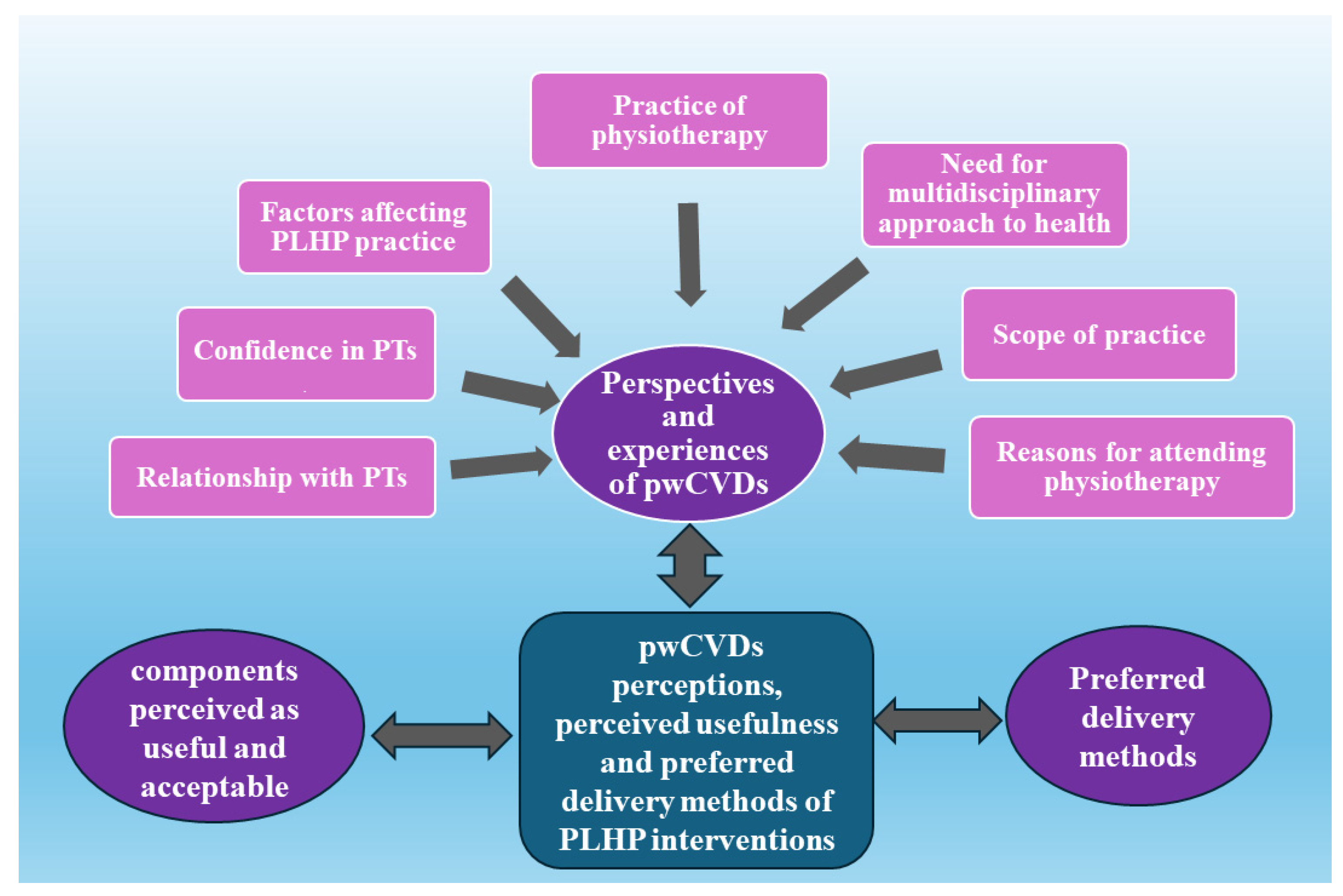

Table 1.
Sociodemographic and clinical characteristics of the participants enrolled in the study (n=146)
Table 1.
Sociodemographic and clinical characteristics of the participants enrolled in the study (n=146)
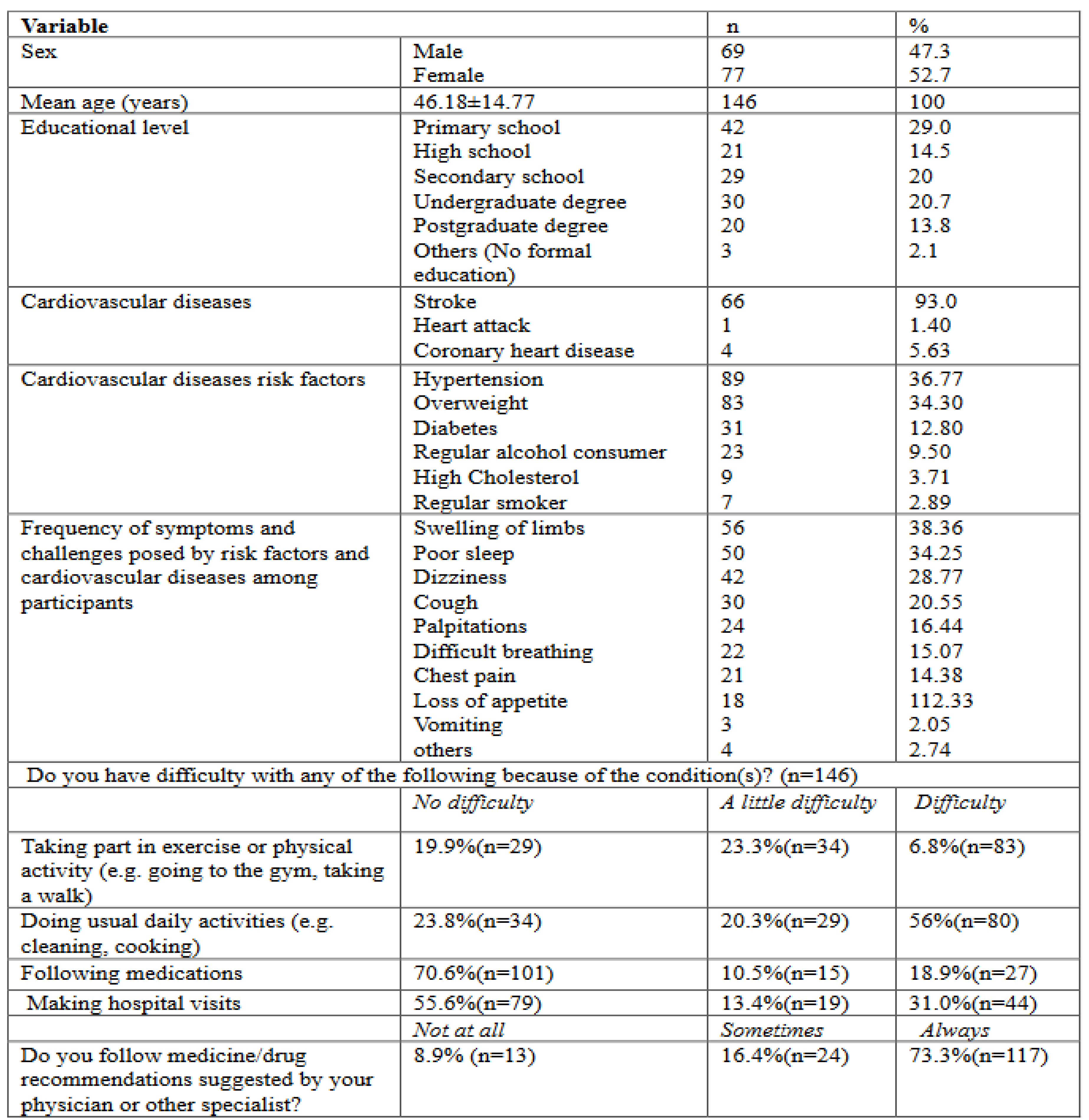
Table 2.
Characteristics of participants interviewed for PLHP (n=13).
| Participants | Age/years | Gender | Profession | Academic Qualification | Risk Factor (S) and/or Cardiovascular Condition |
|---|---|---|---|---|---|
| P1 | 79 | M | Retired School Administrator | Postgraduate Degree | Hypertension, Diabetes, Stroke, High Cholesterol, CHD |
| P2 | 49 | F | Agricultural engineer | Postgraduate degree | Overweight |
| P3 | 64 | M | Community development Officer | Undergraduate Degree | Insomnia, hypertension and overweight |
| P4 | 68 | F | Retired Civil Servant | Undergraduate Degree | Stroke, Hypertension, Overweight, High Cholesterol |
| P5 | 37 | M | Unemployed | No formal Education | Stroke, hypertension |
| P6 | 56 | M | Business | High School | Hypertension, Overweight, Stroke and High Cholesterol |
| P7 | 39 | F | Translator | Postgraduate degree | Overweight |
| P8 | 65 | M | Business | High School | Overweight |
| P9 | 46 | F | Teacher | Postgraduate degrees | Overweight |
| P10 | 60 | F | Retired nurse | Undergraduate Degree | Hypertension, Diabetes, Overweight, High Cholesterol |
| P11 | 46 | M | Business | Diploma | Overweight |
| P12 | 63 | M | Retired physical education and sport teachers | Undergraduate Degree | Hypertension, Diabetes, Overweight |
| P13 | 60 | F | Retired civil servant | Undergraduate degrees | Overweight, Diabetes, hypertension, physical inactivity, Stroke |
*P: Participants, M: Male, F: Female, CHD: Coronary Artery Disease.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



