
Submitted:
30 August 2024
Posted:
03 September 2024
You are already at the latest version
Abstract
Background:
Bacterial resistance to several antibiotic classes is seen as a grave threat worldwide. Bacterial resistance to antibiotics was mostly caused by the abuse and overuse of antibiotics, particularly penicillins and first-generation cephalosporins, in Egypt's primary healthcare facilities.
Aim of the study:
To investigate the main resistant bacteria to a few chosen penicillins and first-generation cephalosporins, as well as the characterization of these antibiotics' resistant genes and their detrimental effects in Egypt's main medical facilities.
Methodology:
Two hundred respiratory and urinary tract infection (RTI and UTI) specimens were gathered from Egyptian primary medical center patients. The turbidimetric assay at 630 nm wavelength, the broth dilution technique, and the nanopore sequencing homology approach were used to characterize the major resistant pathogenic bacteria and their resistant genes to cefadroxil (first generation cephalosporins) and nafcillin (antipseudomonal penicillin). Moreover, adverse outcomes resulting from antibiotic resistance were noted.
Results:
Out of 200 specimens with RTI and UTI, 186 samples showed the proliferation of resistant bacteria isolates. Enterococcus faecium strain NFC and Staphylococcus aureus strain CDX were among them. Nanopore sequencing confirmed that the antibiotic-resistant gene in Enterococcus faecium was the NFC gene, whereas the antibiotic-resistant gene in Staphylococcus aureus was the CDX gene.
Penicillin-binding proteins with modest affinity were encoded by both genes. These bacterial resistance patterns were linked to a low death rate of 5% and a high morbidity rate of 47%.
Conclusion:
By expressing low-affinity penicillin-binding proteins through resistant NFC and CDX genes, Enterococcus faecium strain NFC and Staphylococcus aureus strain CDX were found to be the predominant bacterial isolates that cause antibiotic resistance to first-generation cephalosporins and penicillins.
Keywords:
Antibiotic
; Resistance
; Infection
; bacteria
; Nanopore sequencing technique
Introduction
Worldwide, antibiotics are posing a major threat to several bacterial infectious diseases [1]. One of Egypt’s biggest problems is antibiotic resistance. [2]. The primary cause was found to be the overuse and abuse of various antibiotics, particularly penicillins and first-generation cephalosporins [3]. There exist four principal pathways that facilitate bacterial resistance to the various kinds of antibiotics [4].
First, the antibiotic is rendered inactive by deactivating enzymes, such as beta-lactamase enzymes, which break down the beta-lactam ring to render penicillins and cephalosporins inactive. [5]
The second approach involves creating new targets that the antibiotics are less effective against. [6]
The other two primary ways that bacteria become resistant to antibacterials in general are decreased permeability to the antibiotic [7] and the use of multidrug resistant pumps to the various classes of antibiotics. [8]
A genetic change in the bacterial pathogen results in major antibiotic resistance. [9] Either a plasmid is acquired, [10] transponson, [11] or a genetic mutation causes this. [12]
When glycoside antibiotics are used often, a mutation in the protein containing the 30S ribosomal subunit arises, leading to bacterial resistance. [13]
In addition, mutations in DNA gyrase result in antibiotic resistance to quinolones. [14] Conversely, it was observed that the bacterial multidrug resistant pump led to resistance against tetracyclines and sulfa medicines. [15]
The main factor leading to bacterial resistance to glycopeptide antibiotics was also found to be the substitution of lactate for alanine in the peptidoglycan of the bacterial cell wall. [16] Using third-generation high-throughput sequencing techniques like nanopore sequencing, the current study set out to investigate the bacterial resistant isolates and the genes responsible for their resistance to penicillins like nafcillin and first-generation cephalosporins like cefadroxil in primary medical centers in Egypt.
Methodology
- Ethical statement:
Priority was given in the current study to all pertinent institutional, national, and international regulations dealing with the use and care of persons. All study procedures involving human participants have been approved by Cairo University’s Ethical Committee for Human Handling (ECHCU), located in the Faculty of Pharmacy (permission number WTG479/2024). The research aimed to reduce the pain experienced by human subjects. With informed consent, the use of human subjects or samples in studies was authorized. The World Medical Association’s rule of ethics for human research, the Declaration of Helsinki, was followed in the conduct of the current investigation.
- Type of the study:
Screening experimental study.
- Place and date of the study:
The study was completed at Cairo University’s pharmacy faculty in Egypt between January 2024 and August 2024.
- Collection of the samples:
Two hundred urine samples from adult male and female patients with urinary tract infections (30–65 years old, weighing approximately 70 kg) were randomly collected in sterile urine bags. Additionally, 200 respiratory swabs from patients with respiratory tract infections (20–60 years old, weighing approximately 70 kg) were randomly collected from adult male and female patients with respiratory tract infections (RTIs) in primary medical centers in various locations in Egypt (Menofia, Cairo, Fayoum, and Qalyobia). Before being processed, the obtained samples were kept in sterile containers at 4 °C.
- Detection of resistant patterns to the test antibiotics:
A test group consisting of 200 volunteer patients were received the test antibiotics ( cefadroxil and nafcillin) where each antibiotic was given alone to 100 candidates in a concentration of 500 mg every 8 hours for one week. A standard antibiotic was administered to a positive control group consisting of 200 human volunteers where a standard vancomycin antibiotic was given in a concentration 500 mg every 8 hours for one week to 100 individuals infected with urinary tract infections. As well as the same standard antibiotic was received to 100 candidates infected with respiratory tract infections in a concentration of 500 mg every 8 hours for 7 days.
After one week, respiratory and urine samples were withdrawn from all the participants in the present study.
To help with their identification, the pathogenic bacterial isolates were first screened for growth on nutrition agar and blood agar plates. Subsequently, Gram staining and biochemical reactions were conducted.
To ascertain whether bacteria were resistant to the test antibiotics, the broth dilution antibiotic susceptibility test was used. [17]
Utilizing a 190-1100nm Ultraviolet visible spectrophotometer, model UV1600PC, that was acquired from China, the bacterial count spectrophotometric turbidimetric assay at 630 nm was performed to confirm the existence of antibiotic resistance. [18]
ThermoFisher Scientific, USA supplied the GeneJET Genomic DNA Purification Kit, Catalog number K0721, which was used to extract DNA samples from the resistant bacterial isolates. The process was completed in compliance with the DNA extraction kit’s manufacturer’s instructions.
Later, using the Ultra-Long DNA Sequencing Kit V14 with Catalog number SQK-UK114 bought from Oxford Nanopore Technologies, UK, third-generation high throughput sequencing technology (nanopore sequencing technique) was used to determine the resistant bacterial isolates and their antibiotic-resistant genes to the test antibiotics. The process was completed in accordance with the manufacturer’s instructions for the kit.
- Detection of impact of antibiotic resistance:
This was noted in order to ascertain the detrimental effect that bacterial resistance had on the rate of morbidity and mortality.
- In Silico analysis of the test antibiotics:
By using bioinformatics and docking studies with the test antibiotics, this was accomplished.
- Statistical Analysis
All cultures were conducted in triplets. Their presentation was by means and standard deviation. One-way analysis of variance (p value≤ 0.05) was used as means for performing statistical analysis. The F statistical test was used in the present study.
Results
Only 7% of the test group treated with cefadroxil and nafcillin medicines exhibited traces of bacterial resistance.
In contrast, 93 percent of test group applicants exhibited various degrees of bacterial resistance.
As demonstrated by broth dilution, spectrophotometric turbidimetric techniques, Gram staining, biochemical reactions, and nanopore sequencing technique, 51% of the 93% test candidates were impacted by the resistant strains of Staphylococcus aureus strain CDX, while 42% of the test human subjects showed resistance from Enterococcus faecium strain NFC to the test antibiotics.
Bacterial resistance to cefadroxil and nafcillin, the test antibiotics, was shown to be caused by low affinity penicillin binding proteins produced by the NFC gene of Enterococci and the CDX gene of Staphylococcus aureus, according to the results of the nanopore sequencing homology approach.
The fact that the standard group, which was given vancomycin as a normal antibiotic, did not develop any antibacterial resistance was fascinating. Utilizing BLASTn software, the results in Table 1 indicated the molecular homology of the antibiotic-resistant bacterial isolates to cefadroxil.
Under a standard light microscope, Figure 1 displayed the Gram staining of Staphylococcus aureus resistant to the drug cefadroxil.
The molecular docking of nafcillin with PBP utilizing SWISS-MODEL software is shown in Figure 4.
The biochemical process involving coagulase that Staphylococcus aureus induced in the top tube is depicted in Figure 6.
The calculation of the resistant bacterial count against various nafcillin concentrations is shown in Figure 7. P value was found to be at p≤ 0.05.
Table 4 displays the biochemical reaction profile of the antibiotic-resistant bacterial isolates.
Using the spectrophotometric turbidimetric test at 630 nm, the bacterial counts of the resistant bacterial isolates to cefadroxil were displayed in Table 3.
Table 2 provided further clarity on the molecular similarity analysis of the antibiotic-resistant bacterial isolates using BLASTn software.
Figure 2 demonstrated the Gram staining of resistant Enterococcus faecium to nafcillin antibiotic under the standard light microscope.
Docking and bioinformatic studies carried out in Silico indicate that shifting cefadroxil to position three enhanced antibiotic activity by around 17%±2% and decreased bacterial resistance by more than 25%±1%. Additionally, the docking research results showed that the antibiotic nafcillin and the aromatic compound lysidicichin together had a synergistic effect with minimal bacterial resistance.
Figure 3 revealed the 3D structure of Enterococcus faecium NFC, whereas Figure 5 showed the PBP of Staphylococcus aureus CDX.
A low mortality rate of 5%± 1% and a high morbidity rate of 47%± 3% were associated with the bacterial resistance patterns.
Discussion
Finding the antibiotic-resistant genes encoding low-affinity penicillin-binding proteins was the goal of the current investigation.
Antibiotic resistances to cefadroxil (cephalosporin) and nafcillin (penicillin) were verified during the antibiotic sensitivity test using the broth dilution technique and the measurement of the bacterial counts using the spectrophotometric turbidity assay at 630 nm wavelength.
The primary bacterial isolates in this investigation that showed resistance to the test drugs were Staphylococcus aureus strain CDX and Enterococcus faecium strain NFC, according to Gram staining, biochemical responses, and nanopore sequencing homology method.
Using a nanopore sequencing approach, the genes NFC and CDX encoding the low affinity penicillin binding proteins in the strains of Enterococcus faecium NFC and Staphylococcus aureus CDX were found to be responsible for mediating the bacterial resistance to the test antibiotics.
Since the low affinity of PBPs results in minimal antibiotic resistance, as was mentioned in a previous study, this pattern of bacterial antibiotic resistance might be overcome by raising the dose of the test antibiotics. [19] A prior investigation also verified that synergism was demonstrated when an amino-glycoside antibiotic was added to any of the test antibiotics. [20]
In the present study, low-level bacterial resistance to the test antibiotics was found to be caused by Staphylococcus aureus strain CDX and Enterococcus faecium strain NFC. In the Cabellos C et al study, 2022, high-level bacterial resistance to many penicillins and cephalosporins in hospitals was attributed to pneumococci containing bla gene encoding beta-lactamase. [21]
A change of cefadroxil at the third position increased antibiotic activity by around 17%±2%, while bacterial resistance was lowered by more than 25%±1%, according to docking and bioinformatic investigations conducted in silico. Furthermore, when the aromatic chemical lysidicichin was combined with the antibiotic nafcillin, it had a synergistic impact with very little bacterial resistance, as demonstrated by the docking experiment.
The patterns of bacterial resistance to the test antibiotics were associated with a high morbidity rate of 47%± 3% and a low death rate of 5%± 1%.
Conclusion
The present study stated the detection of novel bacterial isolates containing antibiotic resistance genes encoding low affinity penicillin binding proteins thus it was a promising one. It is recommended in the future to new sources of antibiotics to aid in overcoming the overwhelming bacterial resistance challenge in primary medical centers in Egypt.
Funding
This study was funded by the single author, Prof. Mohammed Kassab.
Conflict of interest/Competing of interests
There is no conflict of interest; as well as no competing of interests exist.
Ethics approval and consent to participate
All relevant institutional, national, and/or international regulations pertaining to the use and care of persons were given priority in the current study. The Ethical Committee for Human Handling at Cairo University (ECHCU), which is housed in the Faculty of Pharmacy, Cairo University, Egypt, approved all study procedures involving human subjects (approval number WTG479/2024). The goal of the study was to lessen the pain of human participants as much as possible. The use of human individuals or samples in experiments was approved with informed permission. The current study was conducted in accordance with the Declaration of Helsinki, the World Medical Association’s code of ethics for human experimentation.
Consent for publication
Not applicable.
Authors’ contributions
This study was performed completely by the single author, Prof. Mohammed Kassab.
Data availability and material
Datasets and material used and/or analyzed in the present study are deposited in GenBank at NCBI with accession numbers: BankIt2862892 NFC, PQ219932 and BankIt2862930 CDX, PQ219933.
Acknowledgement
The Cairo University and the Faculty of Pharmacy, Cairo University are acknowledged for their support.
References
- Lim JM, Singh SR, Duong MC, Legido-Quigley H, Hsu LY, Tam CC. Impact of national interventions to promote responsible antibiotic use: a systematic review. J Antimicrob Chemother. 2020 Jan 1;75(1):14-29. PMID: 31834401; PMCID: PMC6910191. [CrossRef]
- Baquero F, Martínez JL, F Lanza V, Rodríguez-Beltrán J, Galán JC, San Millán A, Cantón R, Coque TM. Evolutionary Pathways and Trajectories in Antibiotic Resistance. Clin Microbiol Rev. 2021 Dec 15;34(4):e0005019. Epub 2021 Jun 30. PMID: 34190572; PMCID: PMC8404696. [CrossRef]
- Iwu CD, Korsten L, Okoh AI. The incidence of antibiotic resistance within and beyond the agricultural ecosystem: A concern for public health. Microbiologyopen. 2020 Sep;9(9):e1035. Epub 2020 Jul 25. PMID: 32710495; PMCID: PMC7520999. [CrossRef]
- Larsson DGJ, Flach CF. Antibiotic resistance in the environment. Nat Rev Microbiol. 2022 May;20(5):257-269. Epub 2021 Nov 4. PMID: 34737424; PMCID: PMC8567979. [CrossRef]
- Muteeb G, Rehman MT, Shahwan M, Aatif M. Origin of Antibiotics and Antibiotic Resistance, and Their Impacts on Drug Development: A Narrative Review. Pharmaceuticals (Basel). 2023 Nov 15;16(11):1615. PMID: 38004480; PMCID: PMC10675245. [CrossRef]
- Bengtsson-Palme J, Kristiansson E, Larsson DGJ. Environmental factors influencing the development and spread of antibiotic resistance. FEMS Microbiol Rev. 2018 Jan 1;42(1):fux053. PMID: 29069382; PMCID: PMC5812547. [CrossRef]
- Jaén-Luchoro D, Busquets A, Karlsson R, Salvà-Serra F, Åhrén C, Karami N, Moore ERB. Genomic and Proteomic Characterization of the Extended-Spectrum β-Lactamase (ESBL)-Producing Escherichia coli Strain CCUG 73778: A Virulent, Nosocomial Outbreak Strain. Microorganisms. 2020 Jun 13;8(6):893. PMID: 32545759; PMCID: PMC7355845. [CrossRef]
- Karkman A, Pärnänen K, Larsson DGJ. Fecal pollution can explain antibiotic resistance gene abundances in anthropogenically impacted environments. Nat Commun. 2019 Jan 8;10(1):80. PMID: 30622259; PMCID: PMC6325112. [CrossRef]
- Yu D, Ryu K, Zhi S, Otto SJG, Neumann NF. Naturalized Escherichia coli in Wastewater and the Co-evolution of Bacterial Resistance to Water Treatment and Antibiotics. Front Microbiol. 2022 May 30;13:810312. PMID: 35707173; PMCID: PMC9189398. [CrossRef]
- Martínez JL, Baquero F. What are the missing pieces needed to stop antibiotic resistance? Microb Biotechnol. 2023 Oct;16(10):1900-1923. Epub 2023 Jul 7. PMID: 37417823; PMCID: PMC10527211. [CrossRef]
- Emgård M, Mwangi R, Mayo C, Mshana E, Nkini G, Andersson R, Msuya SE, Lepp M, Muro F, Skovbjerg S. Tanzanian primary healthcare workers’ experiences of antibiotic prescription and understanding of antibiotic resistance in common childhood infections: a qualitative phenomenographic study. Antimicrob Resist Infect Control. 2021 Jun 27;10(1):94. PMID: 34176486; PMCID: PMC8237496. [CrossRef]
- Selvarajan R, Obize C, Sibanda T, Abia ALK, Long H. Evolution and Emergence of Antibiotic Resistance in Given Ecosystems: Possible Strategies for Addressing the Challenge of Antibiotic Resistance. Antibiotics (Basel). 2022 Dec 24;12(1):28. PMID: 36671228; PMCID: PMC9855083. [CrossRef]
- Smith DR, Temime L, Opatowski L. Microbiome-pathogen interactions drive epidemiological dynamics of antibiotic resistance: A modeling study applied to nosocomial pathogen control. Elife. 2021 Sep 14;10:e68764. PMID: 34517942; PMCID: PMC8560094. [CrossRef]
- Gwenzi W. The ‘thanato-resistome’ - The funeral industry as a potential reservoir of antibiotic resistance: Early insights and perspectives. Sci Total Environ. 2020 Dec 20;749:141120. Epub 2020 Jul 25. PMID: 32836113; PMCID: PMC7381411. [CrossRef]
- Noel HR, Petrey JR, Palmer LD. Mobile genetic elements in Acinetobacter antibiotic-resistance acquisition and dissemination. Ann N Y Acad Sci. 2022 Dec;1518(1):166-182. Epub 2022 Oct 31. PMID: 36316792; PMCID: PMC9771954. [CrossRef]
- Alves G, Ogurtsov A, Karlsson R, Jaén-Luchoro D, Piñeiro-Iglesias B, Salvà-Serra F, Andersson B, Moore ERB, Yu YK. Identification of Antibiotic Resistance Proteins via MiCId’s Augmented Workflow. A Mass Spectrometry-Based Proteomics Approach. J Am Soc Mass Spectrom. 2022 Jun 1;33(6):917-931. Epub 2022 May 2. PMID: 35500907; PMCID: PMC9164240. [CrossRef]
- Smart JI, Corey GR, Stryjewski ME, Wang W, Barriere SL. Assessment of Minimum Inhibitory Concentrations of Telavancin by Revised Broth Microdilution Method in Phase 3 Hospital-Acquired Pneumonia/Ventilator-Associated Pneumonia Clinical Isolates. Infect Dis Ther. 2016 Dec;5(4):535-544. Epub 2016 Oct 7. PMID: 27718118; PMCID: PMC5125136. [CrossRef]
- Mira P, Yeh P, Hall BG. Estimating microbial population data from optical density. PLoS One. 2022 Oct 13;17(10):e0276040. PMID: 36228033; PMCID: PMC9562214. [CrossRef]
- Ciorba V.; Odone A.; Veronesi L.; Pasquarella C.; Signorelli C. Antibiotic resistance as a major public health concern: epidemiology and economic impact. Ann. Ig 2015, 27 (3), 562–579.
- Darwish RM, Matar SG, Snaineh AAA, Alsharif MR, Yahia AB, Mustafa HN, Hasabo EA. Impact of antimicrobial stewardship on antibiogram, consumption and incidence of multi drug resistance. BMC Infect Dis. 2022 Dec 7;22(1):916. PMID: 36476448; PMCID: PMC9730561. [CrossRef]
- Cabellos C, Guillem L, Pelegrin I, Tubau F, Ardanuy C, Gudiol F, Ariza J, Viladrich PF. Penicillin- and Cephalosporin-Resistant Pneumococcal Meningitis: Treatment in the Real World and in Guidelines. Antimicrob Agents Chemother. 2022 Dec 20;66(12):e0082022. Epub 2022 Nov 3. PMID: 36326246; PMCID: PMC9764967. [CrossRef]
Figure 1.
shows the Gram staining of resistant Staphyllococcus aureus to cefadroxil antibiotic under the normal light microscope.
Figure 1.
shows the Gram staining of resistant Staphyllococcus aureus to cefadroxil antibiotic under the normal light microscope.
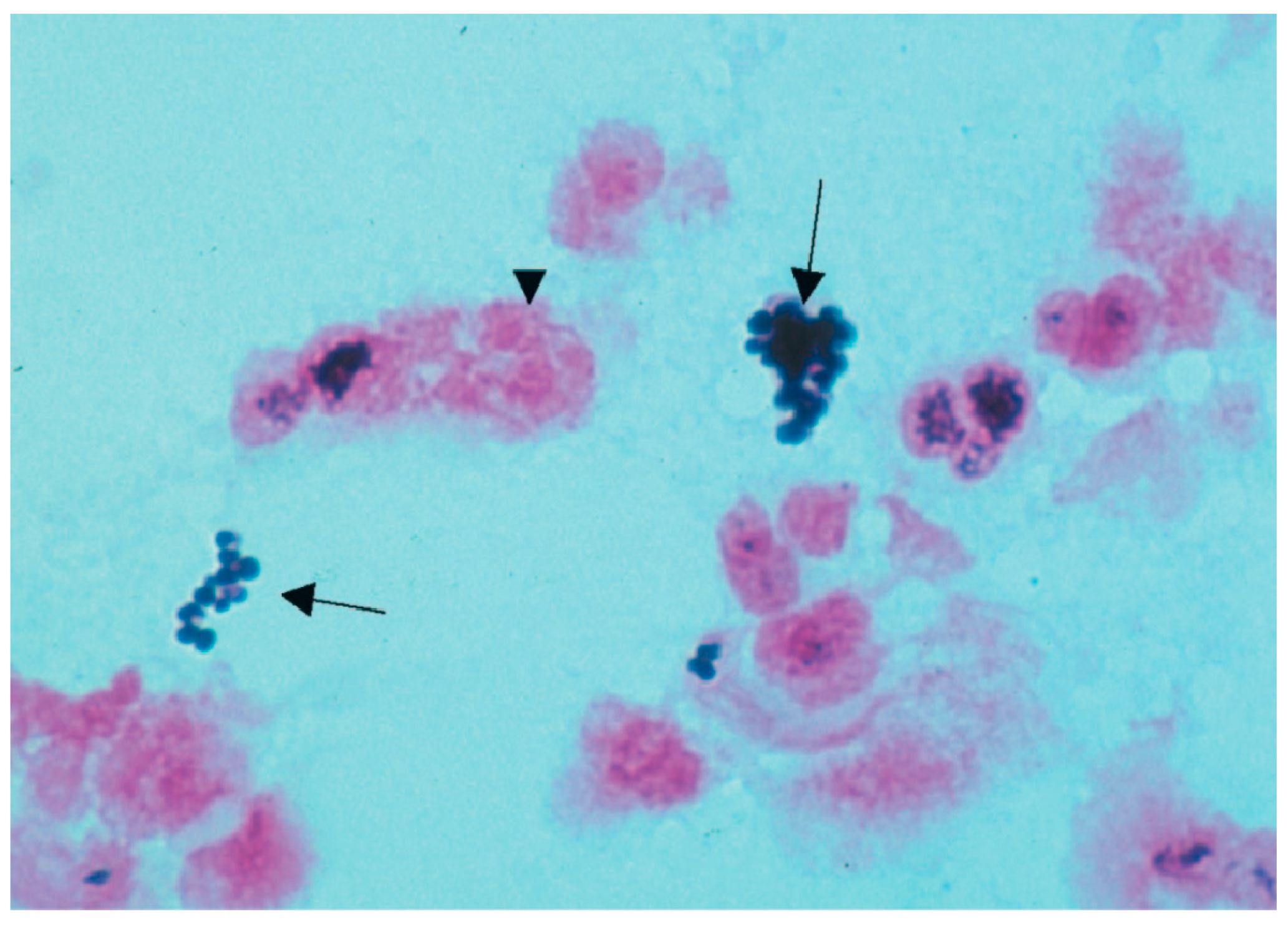
Figure 2.
displays the Gram staining of resistant Enterococcus faecium to nafcillin antibiotic under the normal light microscope.
Figure 2.
displays the Gram staining of resistant Enterococcus faecium to nafcillin antibiotic under the normal light microscope.
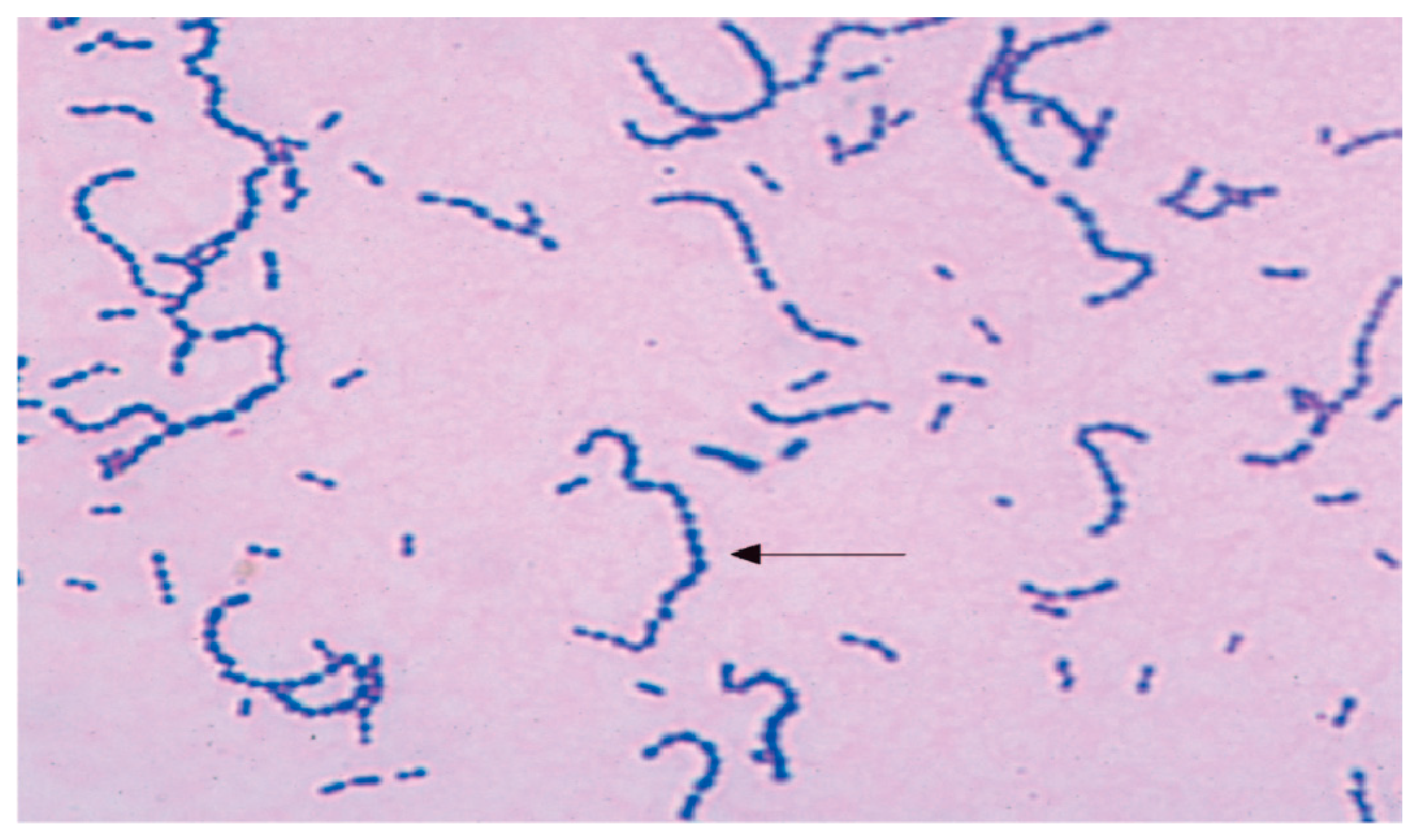
Figure 3.
shows 3Dstructure of PBP of Enterococcus faecium NFC.

Figure 4.
presents the molecular docking of nafcillin with low affinity PBP using SWISS-MODEL software. Gibbs free energy (ΔG) = 7.3 kcal/mol.
Figure 4.
presents the molecular docking of nafcillin with low affinity PBP using SWISS-MODEL software. Gibbs free energy (ΔG) = 7.3 kcal/mol.

Figure 5.
shows the 3Dstructure of PBP of Staphyllococcus aureus CDX.
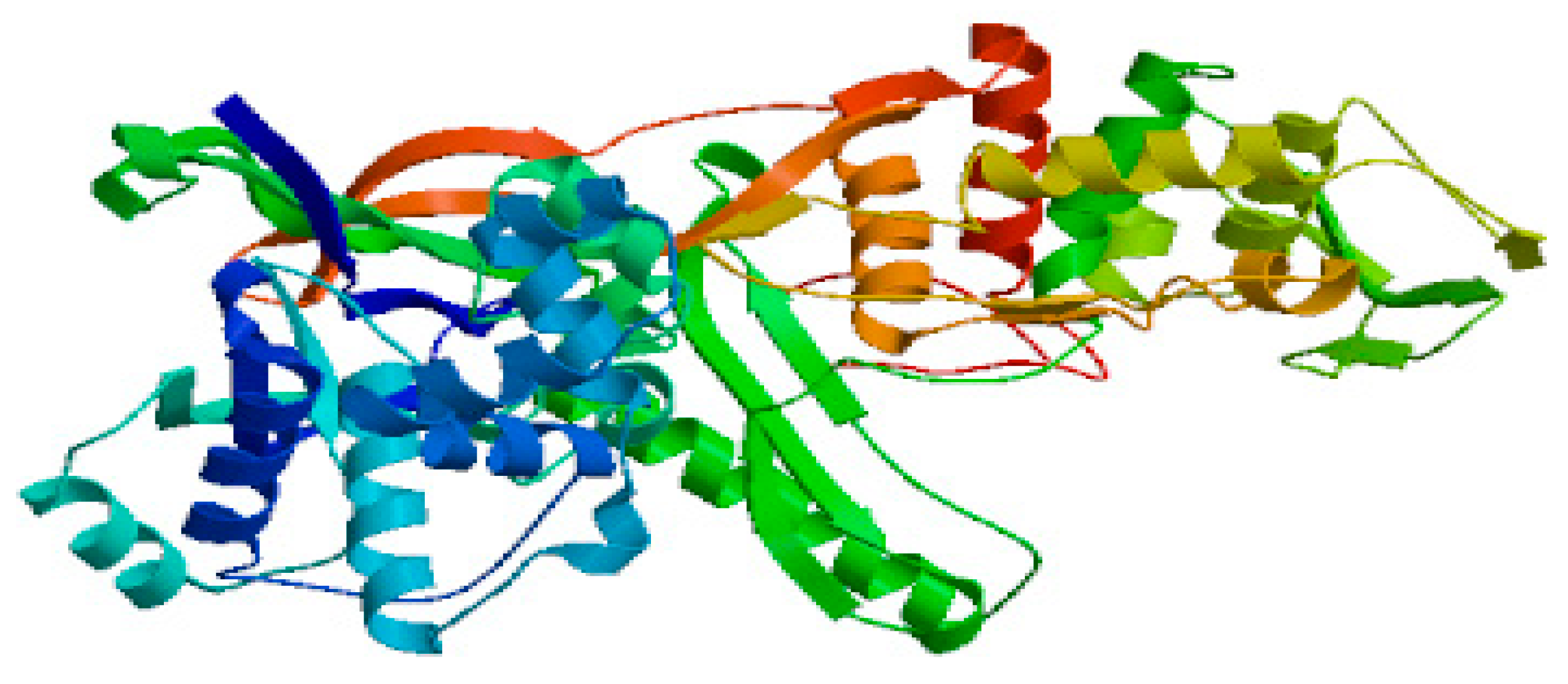
Figure 6.
demonstrates the coagulase biochemical reaction caused by Staphyllococcus aureus in the upper tube.
Figure 6.
demonstrates the coagulase biochemical reaction caused by Staphyllococcus aureus in the upper tube.
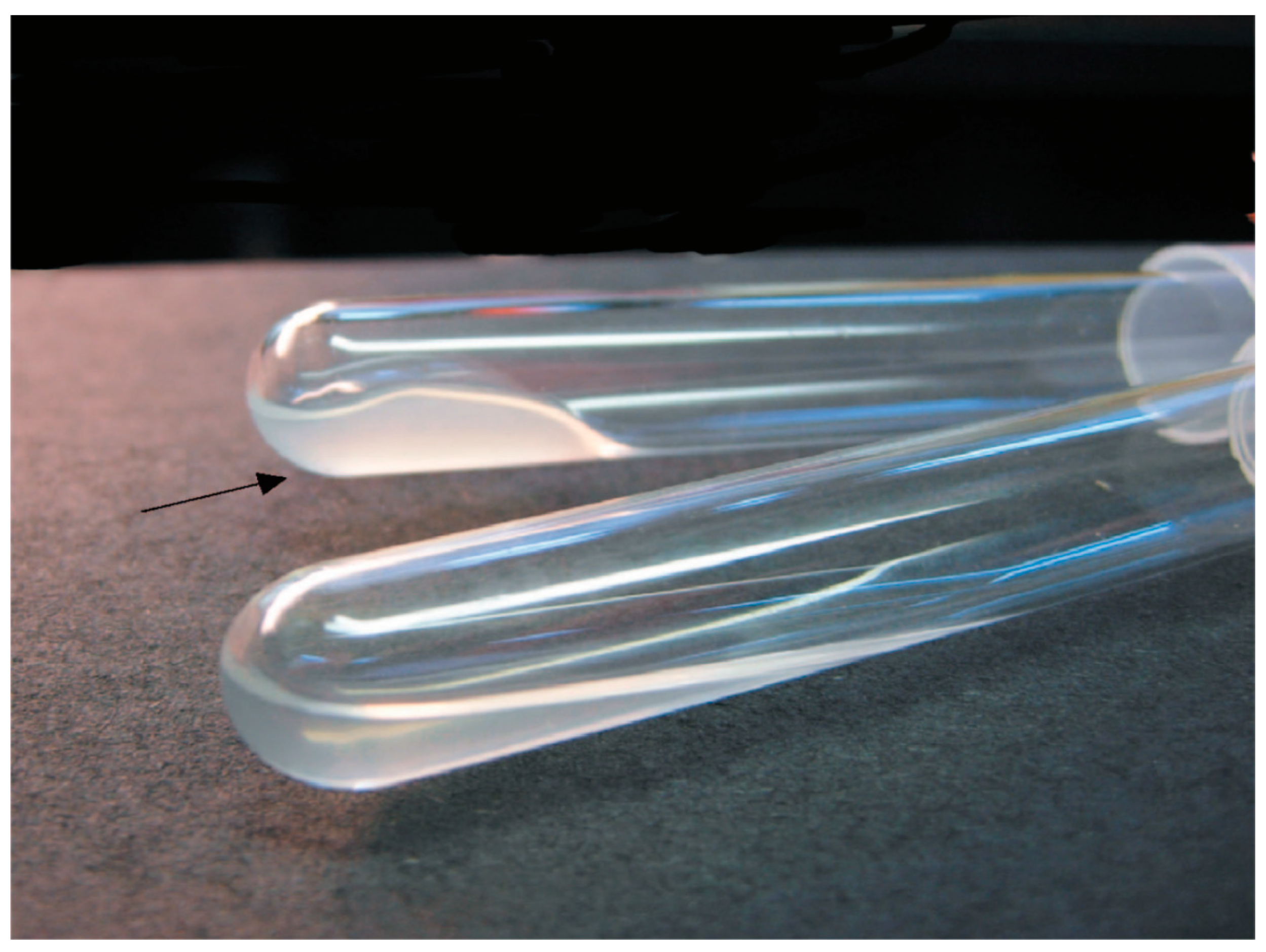
Figure 7.
demonstrates the resistant bacterial count estimation against different concentrations of nafcillin. P value was at p≤ 0.05.
Figure 7.
demonstrates the resistant bacterial count estimation against different concentrations of nafcillin. P value was at p≤ 0.05.
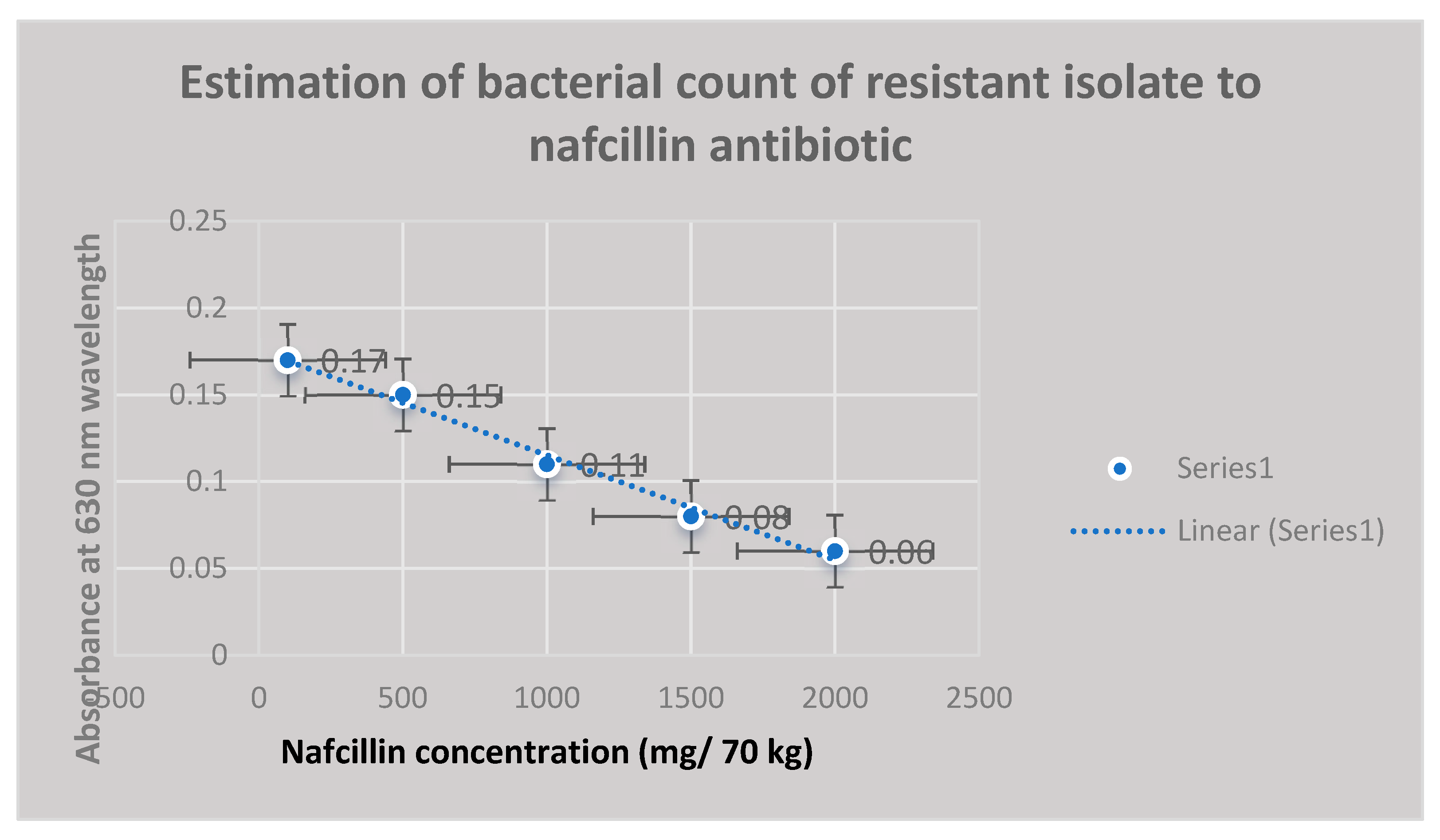

Table 1.
It demonstrates the molecular homology of the resistant bacterial isolates to cefadroxil antibiotic using BLASTn software:.
Table 1.
It demonstrates the molecular homology of the resistant bacterial isolates to cefadroxil antibiotic using BLASTn software:.
| Description | Scientific Name | Max Score | Per. Ident |
|---|---|---|---|
| Staphylococcus aureus DNA, complete genome, strain: GN3 | Staphylococcus aureus | 1188 | 99.69 |
| Staphylococcus aureus DNA, complete genome, strain: GN1 | Staphylococcus aureus | 1188 | 99.69 |
| Staphylococcus aureus strain SR434 chromosome, complete genome | Staphylococcus aureus | 1188 | 99.69 |
| Staphylococcus aureus strain Sau37 chromosome, complete genome | Staphylococcus aureus | 1188 | 99.69 |
| Staphylococcus aureus strain Sau59 chromosome, complete genome | Staphylococcus aureus | 1188 | 99.69 |
| Staphylococcus aureus strain Sau92 chromosome, complete genome | Staphylococcus aureus | 1188 | 99.69 |
| Staphylococcus aureus strain UNC_SA56 chromosome, complete genome | Staphylococcus aureus | 1188 | 99.69 |
| Staphylococcus aureus subsp. aureus Tager 104 chromosome, complete genome | Staphylococcus aureus subsp. aureus Tager 104 | 1188 | 99.69 |
| Staphylococcus aureus strain 16CS0209 chromosome, complete genome | Staphylococcus aureus | 1188 | 99.69 |
| Staphylococcus aureus strain SCAID OTT1-2022 (150) chromosome, complete genome | Staphylococcus aureus | 1188 | 99.69 |
| Staphylococcus aureus strain TCD14 chromosome | Staphylococcus aureus | 1188 | 99.69 |
| Staphylococcus aureus strain TCD9 chromosome | Staphylococcus aureus | 1188 | 99.69 |
| Staphylococcus aureus strain TCD17 chromosome | Staphylococcus aureus | 1188 | 99.69 |
| Staphylococcus aureus strain TCD15 chromosome | Staphylococcus aureus | 1188 | 99.69 |
Table 2.
It establishes the molecular similarity of the insusceptible bacterial isolates to nafcillin antibiotic exploiting BLASTn software:.
Table 2.
It establishes the molecular similarity of the insusceptible bacterial isolates to nafcillin antibiotic exploiting BLASTn software:.
| Description | Scientific Name | Total Score | Per. Ident |
|---|---|---|---|
| Enterococcus faecium strain JE1 | Enterococcus faecium | 2116 | 98.66 |
| Enterococcus lactis strain J-1-A | Enterococcus lactis | 2116 | 98.66 |
| Enterococcus lactis strain J-3-A | Enterococcus lactis | 2116 | 98.66 |
| Enterococcus lactis strain J-4-A | Enterococcus lactis | 2116 | 98.66 |
| Enterococcus lactis strain IDCC 2105 | Enterococcus lactis | 2919 | 98.66 |
| Enterococcus faecium T110 | Enterococcus faecium T110 | 2116 | 98.66 |
| Enterococcus lactis strain KCTC 21015 | Enterococcus lactis | 3218 | 98.66 |
| Enterococcus faecium strain TK-P5D | Enterococcus faecium | 2116 | 98.66 |
| Enterococcus faecium strain 642 | Enterococcus faecium | 1584 | 98.64 |
| Enterococcus lactis strain DH9003 | Enterococcus lactis | 3522 | 98.64 |
| Enterococcus lactis strain HJS001 | Enterococcus lactis | 1913 | 98.39 |
| Enterococcus faecium strain FB-1 | Enterococcus faecium | 1998 | 96.47 |
| Enterococcus faecium strain DB-1 | Enterococcus faecium | 1998 | 96.47 |
| Enterococcus faecium strain ww_sludge_ent_V1_zoecandies_230529 | Enterococcus faecium | 1639 | 95.3 |
| Enterococcus faecium isolate E4239 | Enterococcus faecium | 1162 | 95.02 |
| Enterococcus faecium isolate E4227 | Enterococcus faecium | 1162 | 95.02 |
| Enterococcus faecium strain T17-1 | Enterococcus faecium | 1754 | 97.07 |
| Enterococcus faecium strain AD21B | Enterococcus faecium | 1053 | 92.34 |
Table 3.
It shows the bacterial counts of the resistant bacterial isolates to cefadroxil using the spectrophotometric turbidimetric assay 630 nm:.
Table 3.
It shows the bacterial counts of the resistant bacterial isolates to cefadroxil using the spectrophotometric turbidimetric assay 630 nm:.
| Bacterial Count (CFU/ml) | Antibiotic Concentration (mg/70 kg) | UV Absorbance at 630 nm Wavelength | P Value |
|---|---|---|---|
| 4*105 | 500 | 0.21 | 0.05 |
| 3*104 | 750 | 0.18 | 0.01 |
| 2*104 | 900 | 0.12 | 0.05 |
| 2*103 | 1000 | 0.09 | 0.02 |
| 102 | 1500 | 0.05 | 0.01 |
Table 4.
Biochemical reactions profile of the resistant bacterial isolates to the test antibiotics:.
Table 4.
Biochemical reactions profile of the resistant bacterial isolates to the test antibiotics:.
| Characteristic Biochemical Reactions of Resistant Staphyllococcus aureus Isolates | Characteristic Biochemical Reactions of Resistant Enterococcus faecium Isolates |
|---|---|
| Grape-like clusters of Gram-positive cocci were shown by staphylococcal isolates that were resistant. Golden-yellow colonies with remarkable β-hemolysis were proven to be produced by S. aureus cultures. A coagulase positive strain of Staphylococcus aureus was found. The fermentation of mannitol was detected in Staphylococcus aureus isolates on mannitol-salt agar. Agar became yellow as a result of this action, which decreased pH. | Gram-positive streptococci were found in smears from isolates of resistant enterococci. When bile was present, these bacterial isolates were shown to hydrolyze esculin. On bile-esculin agar, they generated a black pigment. Furthermore, in a hypertonic 6.5% NaCl saline solution, it was shown that bacterial isolates of Enterococcus faecium were growing. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



