
Submitted:
03 September 2024
Posted:
03 September 2024
You are already at the latest version
Abstract
Medullary thyroid carcinoma (MTC) is a rare yet aggressive form of thyroid cancer, comprising a disproportionate share of thyroid cancer-related mortalities despite its low prevalence. MTC differs from other differentiated thyroid malignancies due to its heterogeneous nature, presenting complexities in both hereditary and sporadic cases. Traditional management guidelines, designed primarily for papillary thyroid carcinoma (PTC), fall short in providing the individualized care required for MTC patients. In recent years, the sheer volume of data generated from clinical evaluations, radiological imaging, pathological assessments, genetic mutations, and immunological profiles has made it humanly impossible for clinicians to simultaneously analyze and integrate these diverse data streams effectively. This data deluge necessitates the adoption of advanced technologies to assist in decision-making processes. Holomics, an integrated approach that combines various omics technologies, along with artificial intelligence (AI), emerges as a powerful solution to address these challenges. AI-driven precision oncology can significantly enhance the diagnostic work-up, staging, risk stratification, management, and follow-up care of MTC patients by processing vast amounts of complex data quickly and accurately. AI algorithms can identify patterns and correlations that may not be apparent to human clinicians, thereby improving the precision of personalized treatment plans. Moreover, the implementation of AI in MTC management enables the collation and synthesis of clinical experiences from across the globe, facilitating a more comprehensive understanding of the disease and its treatment outcomes. This global approach aligns with the United Nations Sustainable Development Goal 3, which aims to ensure healthy lives and promote well-being for all at all ages. By leveraging AI and holomics, we can strive towards making personalized healthcare accessible to every individual, regardless of their economic status, thereby improving overall survival rates and quality of life for MTC patients worldwide. In conclusion, the integration of holomics and AI in the management of medullary thyroid carcinoma represents a significant advancement in precision oncology. This innovative approach not only addresses the complexities of a rare and aggressive disease but also paves the way for global collaboration and equitable healthcare solutions, ultimately transforming the landscape of MTC treatment and care.
Keywords:
Artificial intelligence
; holomics
; medullary thyroid carcinoma
; precision oncology
1. Introduction
Medullary thyroid carcinoma (MTC) constitutes less than 5% of primary malignant tumors of the thyroid gland but more than 10% of the deaths from thyroid cancer [1]. Approximately 25% of MTC is hereditary and part of either multiple endocrine neoplasia type 2A or 2B (MEN 2A or MEN 2B) [2,3]. Eighty percent of hereditary MTC occurs in individuals with the classical variant of MEN 2A while 5% in those with MEN 2B. Close to 15% of hereditable MTC is part of familial medullary thyroid carcinoma (FMTC) variant of MEN 2A [3,4,5]. Around 53% and 20% of patients with sporadic MTC carry mutually exclusive somatic mutations of the rearranged during transfection (RET) and rat sarcoma virus (RAS) gene, respectively (Figure 1).
Aberrant splicing is a crucial factor in the development and progression of cancers, including MTC. Splicing removes introns from pre-mRNA and joins exons to form mature mRNA, a process regulated by the spliceosome and various splicing factors. Disruption of this regulation can result in abnormal mRNA isoforms that contribute to cancer [6]. The spliceosome consists of small nuclear RNAs (snRNAs) and associated proteins, with key splicing factors including serine/arginine-rich (SR) proteins and heterogeneous nuclear ribonucleoproteins (hnRNPs). The SR proteins usually promote exon inclusion, while hnRNPs can repress splicing or enhance exon skipping [7,8].
Medullary thyroid carcinoma is often associated with mutations in the RET proto-oncogene, which encodes a receptor tyrosine kinase involved in cell growth and differentiation. In addition to point mutations, alternative splicing of RET can produce different isoforms with varying oncogenic potentials. For example, the inclusion or exclusion of specific exons in the RET transcript can influence the kinase activity, cellular localization, and interaction with signaling partners [9]. In MTC, aberrant splicing of the RET gene has been observed, leading to the expression of RET isoforms that contribute to the malignancy. Studies have identified splicing variants of RET that lack the entire exon 11 or 12, resulting in constitutively active forms of the receptor that promote uncontrolled cell growth [10]. Additionally, the aberrant splicing of other genes involved in cell cycle regulation, apoptosis, and metastasis has been implicated in MTC pathogenesis [11]. Targeting aberrant splicing represents a promising therapeutic strategy for MTC. Several approaches are being explored, including small molecules that modulate splicing factor activity and antisense oligonucleotides (ASOs) that correct splicing defects. For instance, spliceosome inhibitors like spliceostatin A and E7107 have shown potential in preclinical studies by inducing apoptosis in cancer cells with splicing abnormalities [12]. ASOs can be designed to bind to specific RNA sequences and modify splicing patterns, potentially restoring normal gene expression [13].
Recent advances have also explored the use of CRISPR/Cas9 technology to target and correct splicing mutations at the genomic level, offering another potential avenue for therapeutic intervention [14]. Aberrant splicing plays a significant role in the pathogenesis of MTC, particularly through the dysregulation of the RET proto-oncogene. Understanding the mechanisms underlying splicing abnormalities in MTC can reveal novel therapeutic targets and strategies, offering hope for more effective treatments for this aggressive cancer. Diagnostic workup of patients with suspected MTC starts with clinical assessment followed by thyroid function test, ultrasound, measurement of serum level of Ctn, fine needle aspiration cytology (FNAC), CT scan and MRI [1]. The choice and timing of treatment, follow-up plans depend on the type of MTC, stage and grade of a tumor, mutational status and serum levels of Ctn and CEA, and their doubling time [1,3,15]. Chemotherapy, radiotherapy and radioactive iodine and other radionuclide therapy are not effective in the treatment of MTC [1,16]. Targeted therapy using multi- or selective tyrosine kinase inhibitors is effective in few patients with MTC.
A patient with MTC is cured if there is no structural evidence of residual disease and serum level of Ctn is normal or not detectable. The prognosis of majority of patients with MTC is poor despite the introduction of newer diagnostic modalities and targeted therapy, and the involvement of multidisciplinary teams in decision making and management. Some of the reasons for the poor outcomes associated with MTC include that majority of the patients present when the tumor is advanced. Management of patients with MTC is often not individualized and one-size-fits-all approach is followed althoMTC ugheven is known to be a highly complex and heterogenous disease. The American Joint Committee on Cancer tumor node metastasis (TNM) staging system cannot accurately quantify the volume of the disease to enable personalized management of patients with MTC [17]. The level of serum Ctn is generally useful for screening, risk-stratification and postoperative monitoring following curative resection of MTC [18,19,20,21]. Other parameters for prognostication of MTC include age and gender of the patient, size of the tumor, existence of extra-thyroidal spread, lymph node metastasis and, levels of serum Ctn and carcinoembryonic antigen (CEA) [1,22]. The mutational landscape of a tumor, alterations in the expression of non-coding RNAs and molecular profile of the tumor influence the clinical behaviour and outcome of patients with MTC [23,24,25,26,27,28,29,30,31,32]. MTC is curable if surgical treatment is instituted when it is still confined to the thyroid gland and is completely removed [21,33,34,35,36,37]. However, majority of patients with MTC present when the tumor is larger than 2cm and there are metastasis to lymph nodes, lungs, bone or liver [21,38,39,40,41,42,43,44,45]. Furthermore, MTC and its TME evolve as the tumor progresses and may acquire new mutation necessitating dynamic risk stratification.
2. Management of Medullary Thyroid Carcinoma
The mainstay of treatment of MTC is total thyroidectomy with central lymph node dissection [36,38]. Radioactive iodine, thyroid stimulating hormone (TSH) suppression, external beam radiotherapy, standard chemotherapy and immunotherapy are not effective in the treatment of MTC [16,36,38,46]. Medullary thyroid carcinoma, especially if it is larger 1cm han 1in size may overexpress programmed cell death-ligand 1 and may be amenable to treatment with PD-L1 inhibitors [47]. External beam radiotherapy is used to treat residual or recurrent disease in the neck that is not amenable to re-do surgery [1,16]. The tumor microenvironment (TME) of MTC, like of most thyroid cancers; is less immunogenic thus immunetherapy is usually not effective [44]. Similar to targeted therapy with selective tyrosine kinase (TKIs and multi-kinase inhibitors (MKIs), immunotherapy can howe slow down progression of MTC, and palliate symptoms like diarrhea in case of metastatic MTC [48,49]. Occasionally, neo-adjuvant TKIs may lead to a signficant reduction in the size of the tumor in patients with locally advanced and irresectable MTCs, and make it amenable to a resection [50].
2.1. Extent of Thyroidectomy for Medullary Thyroid Carcinoma
Total thyroidectomy is indicated in all patients with hereditary MTC as the tumor is likely to be multifocal or bilateral [51,52]. Thyroid lobectomy with prophylactic central lymph node dissection is sometimes appropriate in patients with low-risk MTC. A low-risk sporadic MTC must be unifocal, low-grade tu and less than 1cm in maximum diA low-risk MTC must also be ameter. intra-thyroidal, and not harbour high-risk mutations [36,53]. Additionally, the serum level of Ctn and/or CEA must normalize or be not detectable within 1-3 months after the lobectomy [54]. Among the concerns regarding the appropriateness of thyroid lobectomy for curative treatment of MTC include a possibility of mistaking patients with late onset hereditary MTC with those having the sporadic type. In some cases an MTCthat is less than 2cm may already have metastasized to regional lymph nodes or distant sites [53]. Furthermore, serum levels of Ctn with or without CEA is not always useful as in some patients with MTC have normal or discordant results [5].
2.2. Extent of Cervical Lymphadenectomy
Medullary thyroid carcinoma should preferably be diagnosed preoperatively and the patient offered the most appropriate surgery at first instance as completion or re-do surgery is associated with an increased rate of post-operative complications and poorer outcomes [55]. If MTC was missed during pre-operative investigation and the diagnosis is made following a diagnostic lobectomy, subsequent management may be observation with serial measurement of serum Ctn or completion thyroidectomy [33,53,54,56]. There is yet no consensus on the appropriate management of patients with sporadic MTC diagnosed following a diagnostic lobectomy. Although majority of experts would recommend completion thyroidectomy some do not deem it necessary as the incidence of bilateral disease in sporadic MTC is less than 10% [53]. The need for completion thyroidectomy is not debatable in patients with MTC if the tumor has high-risk features like lymph node metastases and markedly elevated serum level of Ctn [53]. Other markers of aggressive MTC that would strengthen the need for completion thyroidectomy include patient’s factors like male gender, older age and high-grade tumor on histology [4]. High-risk histological features include evidence of necrosis, mitotic count above 4 per 2mm2 and a Ki67 index greater than 4% [56,57]. However, majority of experts insists that total thyroidectomy with central lymph node dissection should be the minimum treatment in any patient with MTC regardless of the level of serum Ctn and, stage, grade or mutational status of the tumor [36,51].
Patients with an MTC that is less than 4cm in diameter and no clinical and/or radiological evidence of cervical lymph node involvement should have total thyroidectomy and prophylactic central lymph node neck dissection [36,52,58]. Central lymph node dissection implies the removal of lymph nodes bearing tissues from the hyoid bone to the brachiocephalic vein inferiorly and, laterally bordered by the right and left medial aspects of the internal jugular veins [51]. Clearance of central lymph nodes, even in patients with no evidence of metastatic involvement on pre-operative investigations and during surgery increases the likelihood of cure and reduces the risk of tumor recurrence and re-do surgery [51,59,60,61]. Additionally, some patients with MTC have metastasis that are missed during clinical examination and imaging with investigations [62,63]. The first surgical procedure in patients with MTC must be appropriate and definitive, as re-do surgery increases the risk of post-operative complications with no improvement in the outcome [55].
Although majority of surgeons routinely include central lymph node dissection during total thyroidectomy for MTC some omit it if serum Ctn is less than 20pg/ml in patients whose tumor is smaller than 1cm in diameter, and there is no evidence of lymph node involvement as the likelihood of occult metastasis is low [39,64]. There are surgeons who add prophylactic central and ipsilateral lateral neck dissection if preoperative Ctn level is above 20 pg/ml [20]. Prophylactic contralateral lateral cervical lymph node dissection is advised in patients with MTC and pre-operative serum Ctn is between 200pg/ml and 1000pg/ml, as the possibility of achieving biochemical cure in this group of patients is around 50% [49,50,51]. Biochemical cure is a postoperative level of serum Ctn that is not detectable or normal at least 1-3 months after surgery [65]. A normalized level of Ctn without structural evidence of disease following surgery in patients with MTC is associated with 98% 10-year survival and a recurrence rate below 5%, and even better results if Ctn level is not detectable [66].
2.3. Management of Locally Advanced or Metastatic Medullary Thyroid Carcinoma
Treatment goals in patients with irresectable MTC include locoregional control, palliation of symptoms resulting from excess hormones like Ctn, pain management and prevention or relief of airway compression [35]. Extensive surgery is generally discouraged if there is extensive extra-thyroidal extension but palliative resection of MTC may be necessary if there is impending life-threatening involvement of the upper aerodigestive tract [35,67]. Among the surgical options in patients with irresectable MTC are de-bulking thyroidectomy, laryngectomy, esophagectomy, laryngoesophagectomy and metastectomy [35,36]. Although there are isolated reports of successful use of TKIs as neo-adjuvant therapy, there is generally no role for neo-adjuvant therapy in the management of locally advanced and irresectable MTC [50]. Metastectomy for palliation is justifiable in patients with MTC and isolated but symptomatic lesions that are progressively enlarging [51,52]
Targeted therapy with for example RET or VEGFR-2 inhibitors is currently the first-line therapy for metastatic MTC [35,36,52,68]. Cabozantinib and vandetanib were the first drugs approved by the Food and Drug Administration (FDA) as first-line TKIs for managing locally advanced or metastatic MTC [67]. Both cabozantinib and vandetanib can improve progression-free survival in patients with progressive locally advanced or metastatic MTC [67]. The efficacy of XL184 (Cabozantinib) in Advanced Medullary Thyroid Cancer (EXAM) trial showed that it improved median progression-free survival of around four months in the placebo to 11.2 months in the treatment group (95% CI 0.19-0.40) [67]. Due to the high risk of adverse events and toxicity of TKIs and MKIs, patient selection is crucial. Treatment with TKIs or MKIs should be limited to patients with high tumor burden with symptomatic disease or rapidly progressing disease and favourable proteo-metabolic status [67,68,69]. Assessment of the stability of advanced MTC uses either the trend of biochemical markers like trend of serum levels of Ctn and/or the response evaluation criteria in solid tumors (RECIST) criteria [35,51,52,67,68]. Other options for the management of locally advanced or metastatic MTC include peptide receptor radionuclide therapy [56], external beam radiotherapy [57], radiofrequency ablation, cryoablation and embolization [35,36,51,52,68]. Medullary thyroid carcinoma is not sensitive to standard chemotherapeutic agents [51]. Similary, external beam radiotherapy does not improve the survival in patients with irresectable or residual tumor in patients locally advanced MTC with extra-thyroidal extension [16].
2.4. Post-Operative Follow-Up
Following surgery, patients with MTC should be assessed clinically every 3-6 months thereafter [1]. Serial serum Ctn and CEA measurement is done six-monthly for two years and yearly subsequently, if there is no evidence of recurrent disease, and ultrasound of the neck should be performed every 3 to 12 months. Persistently elevated postoperative serum calcitonin levels indicate residual disease, and the magnitude of the elevation influences further evaluation and management [44]. If after 2 to 3 months following surgery, the level of Ctn is above 150 pg/ml, there is a high likelihood that the patient has metastatic disease and would necessitate a metastatic work-up, which should include neck ultrasound and CTor MRI of the neck and abdomen [36,70,71]. Metastases from MTC are usually small and may be missed, and other imaging investigations like bone scan, MRI and 18F-FDG-PET/CT should be added if metastases are suspected but not visible on ultrasound and or CT scan [21,36,51,72,73,74]. Nevertheless, 18F-FDG-PET/CT is recommended in patients with MTC and serum level of Ctn from 500 to 1000 pg/ml but no structural evidence of metastases on ultrasound and CT scan [73,74].
2.5. Management of Persistent or Recurrent Disease Medullary Thyroid Carcinoma
Factors that influence treatment selection in patients with persistent or recurrent MTC are nature of the symptoms, sites of the disease, burden of disease including the levels of serum Ctn and CEA, and the rate of progression of structural disease [35]. Local or systemic treatment is not advised in patients in whom serum Ctn and/or CEA level remain elevated following surgery but there is no evidence of structural disease [52,68]. Patients with persistently elevated serum Ctn and/or CEA following total thyroidectomy with prophylactic or therapeutic lymphadenectomy without evidence of structural disease should undergo surveillance with measurement of serum calcitonin and CEA levels every 3-6 months to determine doubling times; and ultrasound of the neck every 6-12 months [35,38,68]. Further investigations is indicated if the Ctn or CEA doubling time is less than 24 months, as it would be suggestive of an aggressive disease [35,51,52].
Persistent or recurrent MTC include biochemical incomplete response or recurrence and structurally incomplete response or recurrence [35,52,72]. Biochemical incomplete response is characterized by a high or rising serum level of serum Ctn after at least three months post-surgical resection without anatomical evidence of the disease [35,52,68]. Patients with biochemical incomplete response need to be investigated, and the investigation’s extent depends on the extent of elevation of serum Ctn [35,51,52]. While neck ultrasound alone is adequate investigation if the level of serum Ctn is not above 150pg/ml but patients in whom the level is higher require additional investigations like CT, MRI, laparoscopy and bone scan [72]. Patients with structurally residual MTC are categorized as either stable or unstable disease, and those with stable disease should undergo active surveillance with monitoring of serum levels of Ctn and CEA with imaging by at least an ultrasound every 3-6 months [35,52]. A repeat lymph node dissection followed by external beam radiotherapy (EBRT) or intensity-modulated radiation therapy should be considered in patients with structurally residual but resectable disease if it is still localized in the neck [35]. Furthermore, patients with unstable but resectable disease may also be considered for surgical resection, followed by EBRT [35]. In patients with unstable and irresectable disease, as evidenced by worsening of symptoms and RECIST-confirmed progression, treatment modalities such as various forms of local ablative therapies like radiofrequency ablation, TKIs, cytotoxic chemotherapy and radio-immunotherapy may be trialled [35,52,68,72].
3. Challenges Associated with Management of Medullary Thyroid Carcinoma
Medullary thyroid carcinoma is a complex and highly heterogeneous disease, and its complexity spans the entire continuum from its presentation, diagnosis, staging, risk stratification, management and follow-up following treatment [21,34,49,56,75,76]. Some of the complexities of MTC are generic and applicable to all patients with MTC, while others are specific to hereditary and sporadic MTC. Generic challenges linked to evaluation of suspected or confirmed MTC include the value of routine measurement of serum Ctn level during the workup of nodular goitre, variable cut-off levels of serum Ctn used for diagnosis to guide management, inability of the TNM to quantify the amount of the disease and the justifiability of thyroid lobectomy as definitive treatment in patients with low-risk sporadic MTC [71]. Deciding on the appropriateness of a potentially debilitating surgery for locally advanced or metastatic disease is another challenge. A study by Liu et al. (2024) showed that some patients with metastatic MTC may benefit from resection of the primary tumor, but there is not as yet guidelines for selection of individuals for whom it is appropriate [77]. Other problems include how to tailure treatment and follow-up of patients with Ctn-negative MTC. Another dilemma is of patients whose serum Ctn level is persistently elevated after curative surgery without structural evidence of residual or recurrent disease.
3.1. Serum Calctonin
Normal serum Ctn level is less than 10pg/ml, and levels above 100pg/ml are diagnostic of MTC [78,79]. In a significant proportion of patients with MTC, the serum level is in the “gray-zone” of 10-100pg/ml as it may be seen healthy individuals or patients with benign diseases like chronic thyroiditis, hyperparathyroidism or kidney dysfunction [79]. The level of serum Ctn is higher in adult males compared to females and children [65]. The tumor in some patients with MTC may not secrete high levels of Ctn, even if the tumor stains positive on immunohistochemistry, and occassionally, serum levels of both Ctn and CEA may be normal [80,81,82]. In 2015, the ATA task force could not reach a consensus on the utility of serum Ctn level in the general work-up of a patient with nodular disease of the thyroid gland [65]. Trimboli et al. investigated the usefulness of routine serum Ctn levels testing during nodular goitre diagnostic work-up to exclude MTC over 14.5-years [83]. Predetermined Ctn reference ranges were stipulated for the risk of MTC and included 10-20 pg/ml, 20-100 pg/ml and greater than 100 pg/ml. The levels of serum Ctn in 170 of the patients were in the upper limit of normal and 50 underwent thyroidectomy. Final histology in the majority of the patients who had elevated serum levels of Ctn showed benign disease, a few of them had PTC, and none confirmed MTC. Preoperative FNAC is diagnostic in less than 60% of patients with MTC [84,85,86,87]. Trimboli et al. (2022) in a meta-analysis spanning over 10 years, found that FNAC on its own accurately detected MTC in 56.8 % and subsequently recommended that FNAC must be utilized in combination with other tools to improve its diagnostic value. The types of cells that constitute MTC are variable and have been described as epithelioid, plasmacytoid and spindle shape, amongst others, which may explain the high-rate of misdiagnosis [84,88].
3.2. Hereditary MTC
Decision regarding the management of patients with MEN 2B is less complex if the diagnosis is made timeously and the tumor is still intra-thyroidal, as it would be limited to a search for co-existent pheochromocytoma [72,89], the timing of total thyroidectomy and the extent of lymphadenectomy [90]. Unlike other manifestations of MEN 2B that are expected in all the affected individuals, phaeochromocytoma develops in half of the cases [89]. The genomic landscape of MEN 2B is uniform and only involves germline mutation of the RET Met918Thr. Of concern is that in some cases, mutations that drive hereditary MTC in patients with MEN2B occur de novo, and some of the individuals would have no family history and be the first to be affected [91]. Although the MTC in patients with classical MEN 2A is less aggressive compared to FMTC and MEN 2B associated variants, it is complex to manage as it is heterogeneous disease with a vast mutational landscape and variable clinical presentations [69,90,91,92,93]. Categorization of hereditary MTC into moderate, high or highest risk based on the codon of the RET proto-oncogene involved is only relevant when the tumor is early as the outcome is similar at advanced stage [94]. The occurrence of some of the manifestations of MEN 2A, such as hyperparathyroidism and phaeochromocytoma is variable, which may lead to it being mistaken with sporadic MTC [72,90,95]. The appropriate time to do thyroidectomy for the variants of MTC in patients with MEN 2A also varies, and sequencing of surgery for associated endocrinopathies is also essential [90].
3.3. Sporadic MTC
Sporadic MTC is more unpredictable than MEN 2A and MEN 2B- associated variants [53,69,84]. For still unknown reason, some cases of sporadic MTC may remain indolent and associated with a higher 10-year survival despite distant metastases [25]. The serum level of Ctn is not always useful as it is normal or marginally elevated in some patients with sporadic MTC [96,97]. Most patients with sporadic MTC present like other thyroid tumors and are subjected to the same diagnostic tests that include s-TSH, ultrasound and FNAC. Both ultrasound and FNAC are less helpful in the diagnostic work-up of sporadic MTC when compared with other malignancies of the thyroid gland except FTC [87]. Thyroid nodules in sporadic MTC may resemble benign disease on ultrasound, which may lead to an erroneous decision to observe it serially or offer an inappropriate initial surgery [98]. The staging of sporadic MTC mirrors that of PTC. Still, stage for stage MTC is more aggressive and is responsible for a disproportionate amount of deaths due to thyroid cancer, despite its relative rarity [69]. A sporadic MTC, even when less than 1cm in maximum diameter, is likely to have metastasized to lymph nodes or systemically [53]. The current TNM/AJCC staging system for differentiated thyroid cancer is not adequate as it often underestimates the extent and complexity of sporadic MTC [17].
3.4. Targeted Therapy
The other strategies which have been used to risk-stratify patients with sporadic MTC include segregating the tumors using the levels of Ctn and/or other markers such as CEA, procalcitonin, pro-gastrin releasing peptide and carbohydrate antigen 19.9 (CA 19.9) [53,71]. Other measures include detailed analysis of ultrasound images and other imaging findings such as CT results , FNAC slides and, genetic, epigenetic, proteomics and metabolomics landscapes [99,100,101]. Locally advanced or metastatic MTC cannot be cured but may sometimes require surgical intervention to prevent complications or control symptoms in a select group of patients [36]. Treatment options for stable locally advanced or metastatic disease include surgery, external beam radiotherapy, radiofrequency, ablation and stereotactic radio-guided surgery [43,46]. Surgical resection of locally advanced or metastatic MTC is however inappropriate if it leads to significant postoperative complications such as bilateral recurrent laryngeal nerve injury and permanent hypoparathyroidism without survival benefit [55,102]. The other options for advanced MTC are targeted therapy with tyrosine kinase inhibitors [44,48,100]. Targeted immunotherapies are relatively expensive and may lead to significant side effects such as nausea, diarrhoea, hypertension, bleeding, thrombosis, skin changes and weight loss [44].
4. Artificial Intelligence in the Healthcare Industry
The use of machines to simulate human actions was first proposed by Alan Turing in 1950, and John McCarthy introduced the term artificial intellegence in 1956 [103]. The subtypes of AI include machine learning (ML), artificial neural networks (ANN) and deep learning (DL) [104]. In ML, machines are trained to do what historically could only be performed by a human being. ANN and DL are more complex, and require advanced computing. In DL computers are trained to extract, analyze and interpret quantitative data with or without supervision [104]. Deep learning is more complex than ANN as it has multiple hidden layers [105,106,107,108,109]. For arrangement of AI options according to progressive level of complexity see Figure 2.
The adoption of AI in the healthcare industry has been slow and its use diagnostic investigation, risk stratification, management and follow-up of patients is limited [110,111]. The use of AI to assist decision-making is useful in managing cancer, as cancer is a heterogeneous disease, the heterogeneity and complexity of which are often missed by the traditional methods of staging the disease [110,112,113]. Interpretation of imaging and cytological or histological findings in a patient suspected to have MTC rely on expertise, which is not universally available [104,111,114]. Data collected during the evaluation of patients with suspected MTC include information on family history, lifestyle, environmental risk factors, results of imaging investigation(s), histological findings, genomics, epigenomics, transcriptomics, proteomics, metabolomics and microfluidics of cancer [107,115,116,117,118,119,120,121]. Several publications have reported on the usefulness of radiomics [122], pathomics [123], genomics [69,124] and other omics in the management of thyroid cancers [121]. ML and the convolutional neural network (CNN) version of DL are utilized extensively in other branches of medicine that rely on imaging and evaluation of pathological specimens for screening, diagnosis, staging, risk stratification, treatment selection and follow-up [109,118]. Table 1 contains other versions of AI algorithms that may be used for computer-aided decision making in the management ofpatients with MTC.
Several studies have proven the beneficial role of AI in the diagnostic work-up and management of thyroid diseases including cancer [107,108,111,114,115,118]. The majority of studies on the role of AI in thyroid cancer focused solely on PTC. The rarity of MTC and limited availability of expertise may not allow for the accumulation of enough data for training and testing of AI models [118,124]. However, fundamental to appropriate management of MTC is the diagnosis when the tumor is small and the exclusion of lymph nodes and distant metastases, determining the completeness of surgical resection and timeous detection of recurrence. The other key issues are establishing the genomic variant and molecular subtype of MTC, especially if the tumor is locally advanced or metastatic, and treatment with target therapy is being considered.
5. Application of Artificial Intelligence during the Investigation of Medullary Thyroid Carcinoma
Majority of cases of MTC present as thyroid nodules, and thyroid nodules are found in around 7% of the general population following clinical examination and up to 70% following ultrasound examination [136]. Most thyroid nodules are benign and do not require surgery unless they are toxic or causing compression symptoms [137]. MTC. Using a computer program to extract and subsequently combine demographic data, lifestyle, environmental factors, clinical findings, ultrasound results and FNAC can assist to differentiate a benign from malignant thyroid nodule [104,105,107,108,117].
5.1. Radiomics
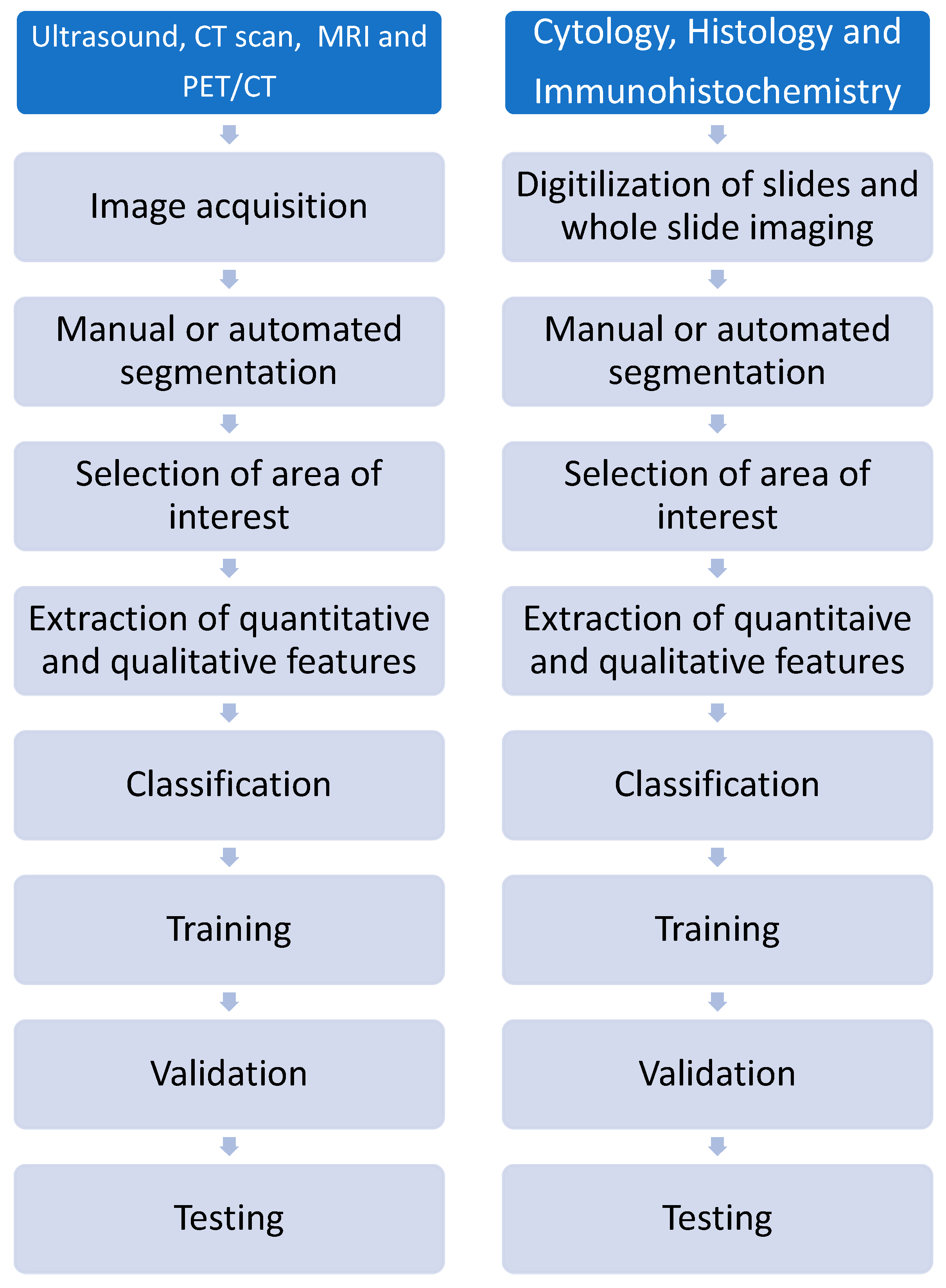
Radiomics is the process of extracting quantitative information from imaging investigations beyond the capability of a human eye. Results of radiomics alone or combined with clinical information and other omics (holomics) are useful for diagnosis, risk-stratification and prognostication in patients with cancer [109,126]. Radiomics may be applied following any imaging investigations including ultasound, CT scan, MRI and PET/CT [100,109]. The six main steps in radiomics are acquisition of an image, processing, marking of areas of interest (segmentation), extraction of key features, development of predictive model and verification [109,138]. The same steps are followed during the development of training, validation and testing models. Imaging results for training and validation may be sourced from archived results.
Interpretation of findings following ultrasound examination of the thyroid gland is influenced by the experience of the sonographer [104,116,137]. Features that are suggestive of malignancy and are assessed during ultrasound evaluation of a thyroid nodule include, among others, whether a nodule is cystic or solid, the echogenicity, vascularity, existence of calcifications, even-ness of its border, shape and stiffness [78,87,139]. Malignant nodules in MTC may appear benign or resemble PTC [32]. Changes critical for the diagnosis of MTC, may not be visible to the naked eye. ML allows for segmentation of thyroid nodules to enable detailed analysis, and outperforms less experienced radiologists in differentiating benign from malignant lesions [104,111,117,137].
Artificial intelligence-guided analysis of ultrasound images can differentiate MTC from PTC. Whereas a PTC that is less than 1cm (microcarcinoma) in maximum in low-risk patients may be observed, the same cannot be said of MTC, as it may be hereditary or harbouring aggressive features. Integration of demographic information, clinical findings, ultrasound and CT scan results using AI technology can more accurately differentiate benign from malignant nodules in patients whose FNAC results are indeterminate compared to when each is used in isolation [105,106,107,140]. Another potential benefit of digital imaging, whole slide imaging and application of AI is the ability to non-invasively identify the underlying mutation driving the cancer [141]. Radiomics may also be repeated after administration of contrast or during follow-up after initiation of treatment, the so-called delta radiomics to improve the diagnostic ability of an investigation or guide timeous adjustment of therspy [142]
Although not yet explicitly utilised in MTC, AI-guided analysis of findings from other imaging investigations can be used to characterize a thyroid nodule following a Bethesda III or IV FNAC results and predict the probability of metastasis to lymph nodes and predict the mutational status of tumor [105,140,143]. For example, AI-guided interpretation of CT scan findings is more accurate than radiologists in distinguishing benign from malignant thyroid nodules with indeterminate cytology results [118]. Using AI technology allows for segmentation of lesions and the mining of quantitative information beyond what a human can do regardless of experience even when working in a multidisciplinary team [140]. Dual-energy CT scan is among the simple versions of AI-guided analysis that is useful for differentiating benign from malignant lesion in thyroid nodules where the FNAC result is indeterminate [144].
5.2. Pathomics
The interpretation of FNAC specimens of suspected MTC may be complex and require experience. It is not uncommon for MTC to be mistaken for PTC, FTC, poorly differentiated thyroid carcinoma (PDTC), anaplastic thyroid carcinoma (ATC), lymphoma and benign conditions [114]. The ability to create digital slides and whole slide imaging allow for the application of AI-aided diagnosis of thyroid cancer [123,145]. The sequence followed during in pathomics is similar to thoat of radiomics and starts with image acquisition [138,145]. A comparison of the steps that are followed in radiomics and patholomics following identification of a tumour.
Figure 3.
Steps followed during development of training and validation model in radiomics and pathomics.
Figure 3.
Steps followed during development of training and validation model in radiomics and pathomics.
The ability to share the slides for a second opinion and segmentation of the slides with selection of region of interest is likely to lead to a more detailed assessment of a tumuor and its environment leading to accurate pre-operative grading of a cancer [101,104,146]. Artificial intelligence-aided analysis and interpretation of FNAC can accurately diagnose the subtype, differentiation, grade and of genomic profile of the cancer, and predict the likelihood of metastasis and recurrence [113,145].
5.3. Epigenomics
Application of epigenomics in work-up of thyroid cancer is firmly established. Epigenetics include histone modification among others histone modication and alteration of expression of lnRNA and miRNA. Inclusion of the pattern of change of for example miRNA may improve decision making during treatment of patients with MTC [5,30,148,149,150,151]. For a summary of changes in the levels of miRNA seen patients with MTC see Table 2.
5.4. Other Omics for Investigation and Management of Cancer
Other AI-assisted diagnostic strategies shown to be useful in patients with other malignancies of the thyroid including PTC are proteomics, metabolomics, glycomics and lipidomics [31,32,105,112,154,155,156]. Among the processes involved in post-translational modification of proteins is glycosylation, which involves the addition of a carbohydrate chains [145]. Protein which are glycosylated may be intracellular or extracellular. A change in the levels of glycosylation is seen in several cancers, including thyroid cancers. Calcitonin, CEA and CA 19.9 are among the glycosylated proteins that are relevant for screening, diagnosis and treatment of MTC. A change in the expression of genes that code glycosylated proteins, epigenetic modification or the glycans themselves may lead to a development of cancer, influence its progression or response to treatment [157]. A study of the pattern of change of the glycosylated products (glycomics) in the tumor, TME or blood is useful for screening, diagnosis, selection of treatment and prediction of response to treatment and the likelihood of recurrence in patient with various cancers, among them thyroid cancer.
Analysis of fluid (fluidomics) such as blood, saliva or ascitic fluid for molecules other than Ctn and CEA may provide valuable information for screening, diagnosis, risk stratification and follow-up of patients with MTC. Among the presdisposing factors of cancer is chronic inflammation, which does not cease to be active even after a cancer has developed but continues and has an influence on progression, metastatic potential and recurrence of the tumors [158]. Markers of inflammation that are commonly monitored include the neutrophil to lymphocte ratio (NLR), lymphocyte to monocytes ratio (LMR), mean platelet volume (MPV) and platelets distribution width (PDW). There are conflicting reports of the usefulness of NLR, LMR, PDW for prediction of the local spread, lymph node metastasis and possibility of biochemical cure of MTC [159,160].
Combining the level of inflammatory markers with results from genomics, epigenomics, metabolomics and other omics may further enhance decision making during management of MTC. There is still a paucity of evidence regarding the use of the other omics other than proteomics, metabolomics, radiomics or pathomics during investigation of patients with confirmed or suspected MTC [28,29,138,161]. Results of a study by Jajin et al using gas chromatography-mass spectrometry-based untargeted metabolomics showed that MTC is associated with a change in among others plasma levels of amino acids and lipid metabolites [154]. They found that patients with MTC had lower levels of leucine compared to healthy individuals. Table 3 is a summary of the sources of data (holomics) that would be useful for omics-guided individualized management of cancer.
6. Potential Application of Artificial Intelligence in MTC
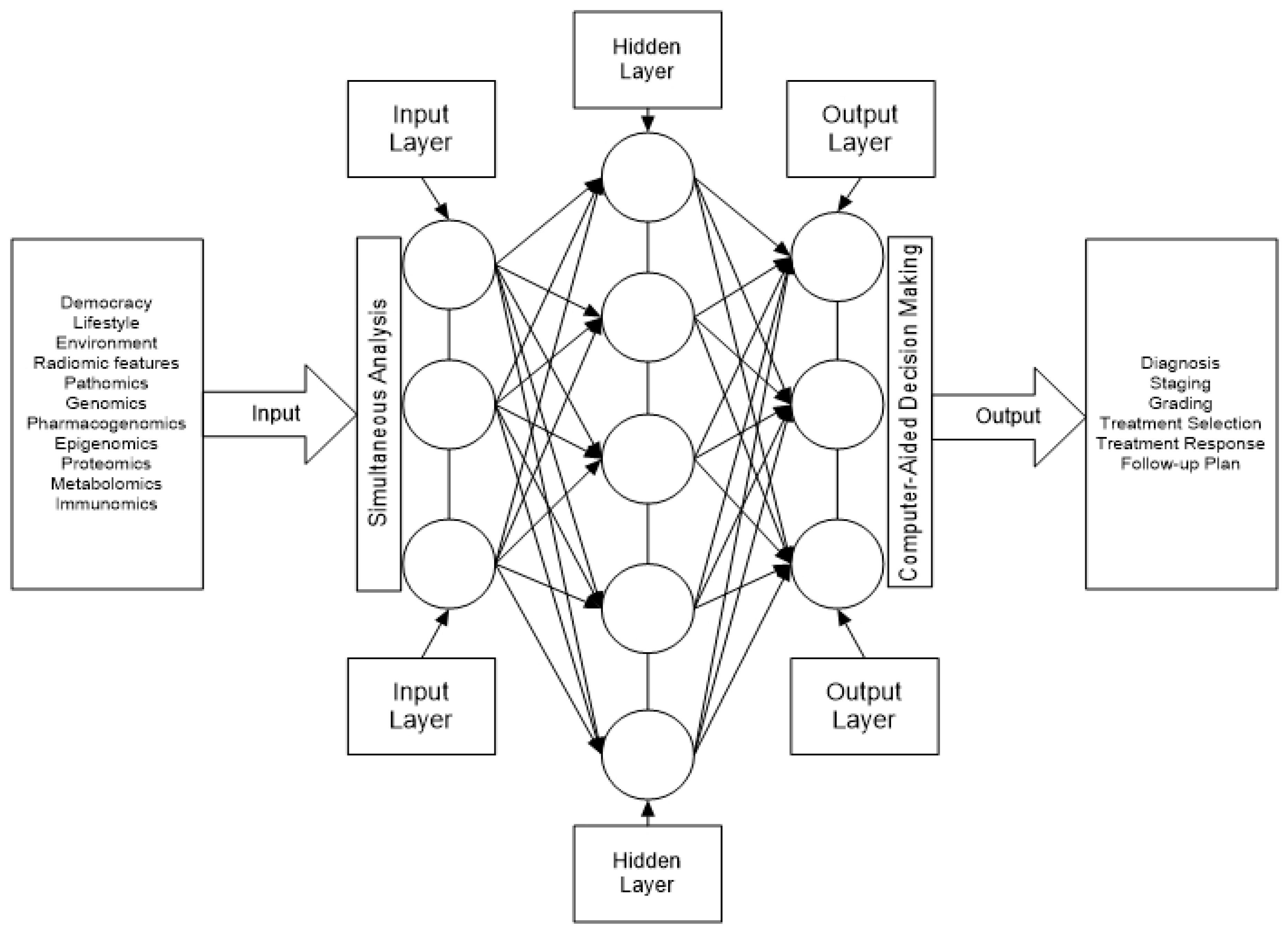
Majority of sporadic patients with MTC have metastases to central and or lateral cervical lymph nodes at presentation and are not cured if treated only with lobectomy or thyroidectomy [100,168]. The size of the primary tumor and serum level of Ctn are not always useful for predicting central, ipsilateral, and/or contralateral lateral cervical lymph node metastasis [61,169]. Application of AI facilitate structuring of big data, analysis and intergration of findings from various for improved quantification of the burden of the disease, risk-stratification and tailoring of treatment in patient with MTC (Figure 3].
Figure 3.
Process intergration, harmonization and simultaneous analysis of holomics for AI-aided decision.
Figure 3.
Process intergration, harmonization and simultaneous analysis of holomics for AI-aided decision.
6.1. Metastatic Work-Up of Medullary Thyroid Carcinoma
A study by Zhang et al. (2024) involving patients with early MTC found that AI algorithms combining clinical and ultrasound findings accurately predicted the existence of metastatic cervical lymph nodes [168]. Similarly, Li et al., (2020) reported that AI-enabled extraction of quantitative data from ultrasound image of thyroid cancer can accurately predict involvement of regional lymph nodes [105]. Computerized tomography-based AI models also accurately predict metastasis to the central and lateral cervical lymph nodes in patients with PTC [105]. Large tumor size greater than 4cm [169], high levels of Ctn, high CEA [18,100,101, high CA19.9 [53,115], high-grade tumors [115], tumors with areas of desmoplastic reaction [44,170] or lympho-vascular invasion [169] and/or RET proto-oncogene mutations increase the likelihood of distant metastasis [171]. However, distant metastasis may be small and missed during pre-operative investigations, only to be suspected when the level of Ctn does not normalize or become not detectable following curative surgery [72]. The use of various ML and CNN programs combining personal tumor location and size and ultrasound findings can accurately predict the existence of distant metastasis [106,107,108,163].
6.2. Risk Stratification of Medullary Thyroid Carcinoma
The TNM/AJCC, MTC grading system and serum levels of Ctn and CEA do not sufficiently risk-stratify MTC [4,15,17]. Furthermore, MTC is often missed during preoperative investigations and diagnosed following diagnostic lobectomy or inappropriate surgical procedures, which may negatively affect the outcome [35,71]. Locally advanced or metastatic MTC may in some patients unexpectedly be indolently and not warrant aggressive and sometimes debilitating surgery [25].
6.3. Treatment of Locally Advanced and Metastatic Medullary Thyroid Carcinoma
Application of AI can guide the extent of thyroidectomy and lymphadenectomy in patients with MTC [168]. The available treatment options are not uniformly suitable for all patients with MTC and are dependent on the genomic landscape of the tumor [173,174,175,176]. Genetic and molecular analyses are expensive and are not universally available. However, cancer’s genetic and molecular profile can be determined following liquid biopsy, virtual biopsy using ultrasound and other imaging modalities [99], and cytopathological analysis [113,139,164]. Table 3 contains a summary of areas in which AI application of AI would assist in managing a patient with MTC.

Table 4.
List of omics options available for use during screening, investigation, management and follow-up of patients with MTC.
Table 4.
List of omics options available for use during screening, investigation, management and follow-up of patients with MTC.
| Target | Omics option | References |
|---|---|---|
| Diagnosis | Fluidomics Genomics Glycomics Metabolomics Pathomics Proteomics Radiomics Trascriptomics |
[4] [165] [162] [160] [12,145] [177] [104,111] [5] |
| Staging | Fluidomics Metabolomics Radiomics Pathomics Transcriptomics |
[4,178] [155] [111,156,173] [146,147] [5] |
| Risk stratification | Epigenomics Fluidomics Genomics Glycomics Immunomics Pathomics Radiomics Transcriptomics |
[55] [4,99,173,176] [94] [177] [47,174] [146,147,156] [173] [5,12] |
| Selection of treatment | Fluidomics Genomics Immunomics Pathomics Radiomics Transcriptomics |
[176] [99] [47] [147] [141] [5,8,12] |
| Follow-up | Delta radiomics Fluidomics Genomics Metabolomics |
[143] [4] [176] [155] |
There is a need for the development of a risk stratification system that would simultaneously integrate and harmonize findings from demographic and clinical assessment [22,107,108,115], imaging [121], histopathology or cytopathology [29,113,126], genomics [29,100], epigenomics [31], proteomics and metabolomics [32,101,117], and fluidomics [4] to guide decision making to enable appropriate management of patients with MTC.
Among the limitations of AI-aided management of MTC is restricted availability due high-cost infrastructure for modern computing, especially in low- and middle-income countries. Develoing algorithms for training and testing AI models requires expertise and adequate sample size for training, validation and testing, which may be a challenge as MTC is rare, and there is not enough expertise. Small sample size for use to develop a training or validation process may lead to over-fitting and predispose to generation of models that do not accurately reflect the actual situation. The rarity of MTC, however, encourages collaboration worldwide that would augment the already available data. The challenge of being unable to scientifically explain some of the decisions after applying of ML algorithms, the so-called “blackbox”, is common to all AI programs.
7. Conclusion and Perspectives
Medullary thyroid carcinoma (MTC), despite its rarity and stable prevalence, poses a significant challenge due to its aggressive nature and high mortality rate compared to other thyroid malignancies. Its heterogeneity, whether hereditary or sporadic, complicates treatment approaches not adequately addressed by guidelines tailored for papillary thyroid carcinoma (PTC). The extensive data collected during MTC investigation and management spanning clinical, radiological, pathological, mutational, and immunological domains overwhelms manual analysis and integration capabilities. To overcome this, integrating artificial intelligence (AI) and holomics emerges as a pivotal solution. AI, in conjunction with holomics, offers a transformative approach across MTC's diagnostic, staging, risk stratification, management, and follow-up phases. By swiftly processing diverse data types and uncovering nuanced patterns, AI enhances precision in treatment planning beyond human capability. Furthermore, this approach fosters global collaboration by synthesizing worldwide clinical experiences, thereby enriching understanding and refining therapeutic strategies for MTC. Moreover, deploying AI aligns with Goal Number 3 of the United Nations Sustainable Development Goals (SDG) for 2030, aiming to ensure universal access to personalized healthcare. This synergy underscores AI's potential to revolutionize MTC management, enhancing survival rates and quality of life globally. In summary, integrating holomics and AI into MTC management represents a paradigm shift in precision oncology. This innovative approach addresses the unique challenges of MTC, promotes global healthcare equity, and promises improved outcomes for patients worldwide. As AI continues to evolve, its synergy with holomics holds promise for personalized, effective, and accessible care, setting a new standard in oncological practice.
Author Contributions
Conceptualization, TEL; resources, TEL; writing—original draft preparation, TEL, NS, LJ, MM, TM, TGM, SBK, ZD.; writing—review and editing, TEL, LJ, MSM, ZD; project administration. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were not applicable as it is a review article.
Informed Consent Statement
It is not applicable as it is a review article.
Data Availability Statement
Not applicable.
Acknowledgments
The authors sincerely appreciate the teaching from the team at the Pan African Cancer Research Institute at the University of Pretoria. We would not have been able to write this manuscript without the excellent knowledge we gained from the Genomic 101 course that the institute run annually.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Hassan, A.; Siddique, M.; Riaz, S.; Khan, A.I.; Nawaz, M.K.; Bashir, H. Medullary Thyroid Carcinoma: Prognostic Variable And Tumor Markers Affecting Survival. J Ayub Med Coll Abbottabad. 2018, 30 (Suppl. S1), S627–S632. [Google Scholar]
- Moo-Young, T.A.; Traugott, A.L.; Moley, J.F. Sporadic and Familial Medullary Thyroid Carcinoma: State of the Art. Surg. Clin. North Am. 2009, 89, 1193–1204. [Google Scholar] [CrossRef] [PubMed]
- Wells, S.A., Jr.; Pacini, F.; Robinson, B.G.; Santoro, M. Multiple Endocrine Neoplasia Type 2 and Familial Medullary Thyroid Carcinoma: An Update. J. Clin. Endocrinol. Metab. 2013, 98, 3149–3164. [Google Scholar] [CrossRef]
- Ricci, C.; Salvemini, A.; Dalmiglio, C.; Castagna, M.G.; Cantara, S. From Circulating Tumor Cells to Mirna: New Challenges in the Diagnosis and Prognosis of Medullary Thyroid Cancer. Cancers 2023, 15, 4009. [Google Scholar] [CrossRef] [PubMed]
- Shakiba, E.; Boroomand, S.; Kia, S.K.; Hedayati, M. MicroRNAs in thyroid cancer with focus on medullary thyroid carcinoma: Potential therapeutic targets and diagnostic/prognostic markers and web based tools. Oncol. Res. 2024, 32, 1011–1019. [Google Scholar] [CrossRef] [PubMed]
- Kahles, A.; Lehmann, K.-V.; Toussaint, N.C.; Hüser, M.; Stark, S.G.; Sachsenberg, T.; Stegle, O.; Kohlbacher, O.; Sander, C.; The Cancer Genome Atlas Research Network; et al. Comprehensive Analysis of Alternative Splicing Across Tumors from 8,705 Patients. Cancer Cell 2018, 34, 211–224. [Google Scholar] [CrossRef]
- Lee, Y.; Rio, D.C. Mechanisms and regulation of alternative pre-mRNA splicing. Annual Review of Biochemistry 2015, 84, 291–323. [Google Scholar] [CrossRef]
- Bonnal, S.C.; López-Oreja, I.; Valcárcel, J. Roles and mechanisms of alternative splicing in cancer — implications for care. Nat. Rev. Clin. Oncol. 2020, 17, 457–474. [Google Scholar] [CrossRef]
- Mulligan, L.M. RET revisited: Expanding the oncogenic portfolio. Nat. Rev. Cancer 2014, 14, 173–186. [Google Scholar] [CrossRef]
- Wirth, M.; Tate, J.; Capdevila, J.; Hughes, D.T. MEDULLARY THYROID CANCER: Management guidelines update. Endocrine Practice 2020, 26, 1063–1086. [Google Scholar]
- Sveen, A.; Kilpinen, S.; Ruusulehto, A.; A Lothe, R.; I Skotheim, R. Aberrant RNA splicing in cancer; expression changes and driver mutations of splicing factor genes. Oncogene 2015, 35, 2413–2427. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.C.W.; Abdel-Wahab, O. Therapeutic targeting of splicing in cancer. Nat. Med. 2016, 22, 976–986. [Google Scholar] [CrossRef] [PubMed]
- Wan, Y.; Dreyfuss, G. Splicing in disease: Disruption of the splicing code and the decoding machinery. Nature Reviews Genetics 2017, 18, 762–778. [Google Scholar]
- Khan, M.A.; Bianchi, F.; Rizzi, R.; Sakar, M.S.; Ding, X. CRISPR/Cas9-mediated cancer targeting: Applications and challenges. Theranostics 2018, 8, 2758–2772. [Google Scholar]
- Chen, Z.; Mao, Y.; You, T.; Chen, G. Establishment and validation of a nomogram model for predicting distant metastasis in medullary thyroid carcinoma: An analysis of the SEER database based on the AJCC 8th TNM staging system. Front. Endocrinol. 2023, 14, 1119656. [Google Scholar] [CrossRef]
- Barletta, J.A.; Nosé, V.; Sadow, P.M. Genomics and Epigenomics of Medullary Thyroid Carcinoma: From Sporadic Disease to Familial Manifestations. Endocr. Pathol. 2021, 32, 35–43. [Google Scholar] [CrossRef]
- Mathiesen, J.S.; Kroustrup, J.P.; Vestergaard, P.; Poulsen, P.L.; Rasmussen, K.; Feldt-Rasmussen, U.; Schytte, S.; Londero, S.C.; Pedersen, H.B.; Hahn, C.H.; et al. Replication of newly proposed TNM staging system for medullary thyroid carcinoma: A nationwide study. Endocr. Connect. 2019, 8, 1–7. [Google Scholar] [CrossRef]
- Chen, L.; Zhao, K.; Li, F.; He, X. Medullary Thyroid Carcinoma With Elevated Serum CEA and Normal Serum Calcitonin After Surgery: A Case Report and Literature Review. Front. Oncol. 2020, 10, 526716. [Google Scholar] [CrossRef]
- Giovanella, L.; Fontana, M.; Keller, F.; Verburg, F.A.; Ceriani, L. Clinical performance of calcitonin and procalcitonin Elecsys® immunoassays in patients with medullary thyroid carcinoma. Clin Chem Lab Med. 2020, 59, 743–747. [Google Scholar] [CrossRef]
- Danila, R.; Livadariu, R.; Branisteanu, D. Calcitonin Revisited in 2020. Acta Endocrinol. (Bucharest) 2019, 15, 544–548. [Google Scholar] [CrossRef]
- Matrone, A.; Gambale, C.; Prete, A.; Elisei, R. Sporadic Medullary Thyroid Carcinoma: Towards a Precision Medicine. Front. Endocrinol. 2022, 13, 864253. [Google Scholar] [CrossRef] [PubMed]
- Matrone, A.; Gambale, C.; Prete, A.; Piaggi, P.; Cappagli, V.; Bottici, V.; Romei, C.; Ciampi, R.; Torregrossa, L.; De Napoli, L.; et al. Impact of Advanced Age on the Clinical Presentation and Outcome of Sporadic Medullary Thyroid Carcinoma. Cancers 2020, 13, 94. [Google Scholar] [CrossRef] [PubMed]
- Gild, M.L.; Clifton-Bligh, R.J.; Wirth, L.J.; Robinson, B.G. Medullary Thyroid Cancer: Updates and Challenges. Endocr. Rev. 2023, 44, 934–946. [Google Scholar] [CrossRef]
- Ito, Y.; Miyauchi, A.; Kihara, M.; Higashiiyama, T.; Fukushima, M.; Miya, A. Static Prognostic Factors and Appropriate Surgical Designs for Patients with Medullary Thyroid Carcinoma: The Second Report from a Single-Institution Study in Japan. World J. Surg. 2018, 42, 3954–3966. [Google Scholar] [CrossRef] [PubMed]
- Censi, S.; Cavedon, E.; Watutantrige-Fernando, S.; Barollo, S.; Bertazza, L.; Manso, J.; Iacobone, M.; Nacamulli, D.; Galuppini, F.; Pennelli, G.; et al. Unique Case of a Large Indolent Medullary Thyroid Carcinoma: Time to Reconsider the Medullary Thyroid Adenoma Entity? Eur. Thyroid. J. 2018, 8, 108–112. [Google Scholar] [CrossRef]
- Hamdy, O.; Awny, S.; Metwally, I. Medullary thyroid cancer: Epidemiological pattern and factors contributing to recurrence and metastasis. Medullary thyroid cancer: epidemiological pattern and factors contributing to recurrence and metastasis. Ann R Coll Surg Engl 2020, 102, 1–5. [Google Scholar] [CrossRef]
- APAYDIN, T.; Imre, E.; Yavuz, D. Determinants of remission in a case series of medullary thyroid carcinoma. Turk. J. Med Sci. 2021, 51, 2050–2056. [Google Scholar] [CrossRef]
- Barletta, J.A.; Nosé, V.; Sadow, P.M. Genomics and Epigenomics of Medullary Thyroid Carcinoma: From Sporadic Disease to Familial Manifestations. Endocr. Pathol. 2021, 32, 35–43. [Google Scholar] [CrossRef]
- Romei, C.; Elisei, R. A Narrative Review of Genetic Alterations in Primary Thyroid Epithelial Cancer. Int. J. Mol. Sci. 2021, 22, 1726. [Google Scholar] [CrossRef]
- Galuppini, F.; Censi, S.; Moro, M.; Carraro, S.; Sbaraglia, M.; Iacobone, M.; Fassan, M.; Mian, C.; Pennelli, G. MicroRNAs in Medullary Thyroid Carcinoma: A State of the Art Review of the Regulatory Mechanisms and Future Perspectives. Cells 2021, 10, 955. [Google Scholar] [CrossRef]
- Yang, F.; Zhang, J.; Li, B.; Zhao, Z.; Liu, Y.; Zhao, Z.; Jing, S.; Wang, G. Identification of Potential lncRNAs and miRNAs as Diagnostic Biomarkers for Papillary Thyroid Carcinoma Based on Machine Learning. Int. J. Endocrinol. 2021, 2021, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Jiang, N.; Zhang, Z.; Chen, X.; Zhang, G.; Wang, Y.; Pan, L.; Yan, C.; Yang, G.; Zhao, L.; Han, J.; Xue, T. Plasma Lipidomics Profile Reveals Biomarkers for Papillary Thyroid Carcinoma. Frontiers in Cell and Developmental Biol 2021, 9. [Google Scholar] [CrossRef]
- Opsahl, E.M.; Akslen, L.A.; Schlichting, E.; Aas, T.; Brauckhoff, K.; Hagen, A.I.; Rosenlund, A.F.; Sigstad, E.; Grøholt, K.K.; Mæhle, L.; et al. Trends in Diagnostics, Surgical Treatment, and Prognostic Factors for Outcomes in Medullary Thyroid Carcinoma in Norway: A Nationwide Population-Based Study. Eur. Thyroid. J. 2018, 8, 31–40. [Google Scholar] [CrossRef] [PubMed]
- Weber, T. Medullary Thyroid Carcinoma: Why Is Specialization Mandatory? Visc. Med. 2018, 34, 419–421. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Kim, B.H. Current Guidelines for Management of Medullary Thyroid Carcinoma. Endocrinol. Metab. 2021, 36, 514–524. [Google Scholar] [CrossRef] [PubMed]
- Jayasinghe, R.; Basnayake, O.; Jayarajah, U.; Seneviratne, S. Management of medullary carcinoma of the thyroid: A review. J. Int. Med Res. 2022, 50, 3000605221110698. [Google Scholar] [CrossRef]
- Wu, X.; Li, B.; Zheng, C. Clinical Characteristics, Surgical Management, and Prognostic Factors of Medullary Thyroid Carcinoma: A Retrospective, Single-Center Study. Technol. Cancer Res. Treat. 2022, 21, 15330338221078435. [Google Scholar] [CrossRef]
- Aziz, A.; Khan, S.; Esbhani, U.; Masood, M. Medullary thyroid cancer: An experience from a tertiary care hospital of a developing country. Indian J. Endocrinol. Metab. 2022, 26, 68–72. [Google Scholar] [CrossRef]
- Luo, Z.; Hong, Y.; Yan, C.; Ye, Q.; Wang, Y.; Huang, P. Nomogram for preoperative estimation risk of cervical lymph node metastasis in medullary thyroid carcinoma. Front. Oncol. 2022, 12, 883429. [Google Scholar] [CrossRef]
- Beukhof, C.M.; Brabander, T.; van Nederveen, F.H.; van Velthuysen, M.-L.F.; de Rijke, Y.B.; Hofland, L.J.; Franssen, G.J.H.; Fröberg, L.A.C.; Kam, B.L.R.; Visser, W.E.; et al. Peptide receptor radionuclide therapy in patients with medullary thyroid carcinoma: Predictors and pitfalls. BMC Cancer 2019, 19, 325. [Google Scholar] [CrossRef]
- Meng, K.; Luo, H.; Chen, H.; Guo, H.; Xia, W. Prognosis value of numbers of metastatic lymph node in medullary thyroid carcinoma population-based study using the SEER 18 database. Medicine (Baltimore) 2019, 98, e13884. [Google Scholar] [CrossRef] [PubMed]
- Grossrubatscher, E.; Fanciulli, G.; Pes, L.; Sesti, F.; Dolci, C.; de Cicco, F.; Colao, A.; Faggiano, A.; NIKE Group. Advances in the Management of Medullary Thyroid Carcinoma: Focus on Peptide Receptor Radionuclide Therapy. J. Clin. Med. 2020, 9, 3507. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.; Zhong, J.; Zhang, Z.; Chen, R.; Li, J.; Sun, J.; Chen, H. Prognosis of radiotherapy in medullary thyroid carcinoma patients without distant metastasis. Transl. Cancer Res. 2021, 10, 4714–4726. [Google Scholar] [CrossRef] [PubMed]
- Kiesewetter, B.; Riss, P.; Scheuba, C.; Raderer, M. How I treat medullary thyroid cancer. ESMO Open 2021, 6, 100183. [Google Scholar] [CrossRef]
- Moses, L.E.; Oliver, J.R.; Rotsides, J.M.; Shao, Q.; Patel, K.N.; Morris, L.G.T.; Givi, B. Nodal disease burden and outcome of medullary thyroid carcinoma. Head Neck 2020, 43, 577–584. [Google Scholar] [CrossRef]
- Kukulska, A.; Krajewska, J.; Kołosza, Z.; Grządziel, A.; Gajek, M.; Paliczka-Cieślik, E.; Syguła, D.; Ficek, K.; Kluczewska-Gałka, A.; Jarząb, B. Stereotactic radiotherapy is a useful treatment option for patients with medullary thyroid cancer. BMC Endocr. Disord. 2021, 21, 1–6. [Google Scholar] [CrossRef]
- Shi, X.; Yu, P.-C.; Lei, B.-W.; Li, C.-W.; Zhang, Y.; Tan, L.-C.; Shi, R.-L.; Wang, J.; Ma, B.; Xu, W.-B.; et al. Association Between Programmed Death-Ligand 1 Expression and Clinicopathological Characteristics, Structural Recurrence, and Biochemical Recurrence/Persistent Disease in Medullary Thyroid Carcinoma. Thyroid 2019, 29, 1269–1278. [Google Scholar] [CrossRef]
- Araque, K.A.; Gubbi, S.; Klubo-Gwiezdzinska, J. Updates on the Management of Thyroid Cancer. Horm. Metab. Res. 2020, 52, 562–577. [Google Scholar] [CrossRef]
- Oczko-Wojciechowska, M.; Czarniecka, A.; Gawlik, T.; Jarzab, B.; Krajewska, J. Current status of the prognostic molecular markers in medullary thyroid carcinoma. Endocr. Connect. 2020, 9, R251–R263. [Google Scholar] [CrossRef]
- Golingan, H.; Hunis, B.; Golding, A.C.; Bimston, D.N.; Harrell, R.M. Neoadjuvant Lenvatinib in Advanced Unresectable Medullary Thyroid Carcinoma: A Case Report. AACE Clin. Case Rep. 2020, 6, e73–e78. [Google Scholar] [CrossRef]
- Wells, S.A.; Asa, S.L.; Dralle, H.; Elisei, R.; Evans, D.B.; Gagel, R.F.; Lee, N.; Machens, A.; Moley, J.F.; Pacini, F.; et al. Medullary Thyroid Carcinoma. Thyroid® 2015, 25, 567–610. [Google Scholar] [CrossRef] [PubMed]
- Filetti, S.; Durante, C.; Hartl, D.; Leboulleux, S.; Locati, L.; Newbold, K.; Papotti, M.; Berruti, A.; ESMO Guidelines Committee. Thyroid cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2019, 30, 1856–1883. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Colombo, C.; Sun, H.; Kim, H.Y.; Pino, A.; De Leo, S.; Gazzano, G.; Persani, L.; Dionigi, G.; Fugazzola, L. Unilateral Surgery for Medullary Thyroid Carcinoma: Seeking for Clinical Practice Guidelines. Front. Endocrinol. 2022, 13, 875875. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.W. A High Frequency of Lobectomy Instead of Total Thyroidectomy to Treat Medullary Thyroid Cancer in Korea: Data from the Korean National Health Insurance Service. Endocrinol. Metab. 2020, 35, 784–785. [Google Scholar] [CrossRef]
- Raffel, A.; Cupisti, K.; Krausch, M.; Wolf, A.; Schulte, K.; Röher, H. Incidentally Found Medullary Thyroid Cancer: Treatment Rationale for Small Tumors. World J. Surg. 2004, 28, 397–401. [Google Scholar] [CrossRef]
- Pelizzo, M.R.; Mazza, E.I.; Mian, C.; Boschin, I.M. Medullary thyroid carcinoma. Expert Rev. Anticancer. Ther. 2023, 23, 943–957. [Google Scholar] [CrossRef]
- Xu, B.; Fuchs, T.L.; Ahmadi, S.; Alghamdi, M.; Alzumaili, B.; Bani, M.-A.; Baudin, E.; Chou, A.; De Leo, A.; Fagin, J.A.; et al. International Medullary Thyroid Carcinoma Grading System: A Validated Grading System for Medullary Thyroid Carcinoma. J. Clin. Oncol. 2022, 40, 96–104. [Google Scholar] [CrossRef]
- Ito, Y.; Miyauchi, A.; Kihara, M.; Higashiiyama, T.; Fukushima, M.; Miya, A. Static Prognostic Factors and Appropriate Surgical Designs for Patients with Medullary Thyroid Carcinoma: The Second Report from a Single-Institution Study in Japan. World J. Surg. 2018, 42, 3954–3966. [Google Scholar] [CrossRef]
- Fleming, J.B.; Lee, J.E.; Bouvet, M.; Schultz, P.N.; Sherman, S.I.; Sellin, R.V.; Friend, K.E.; Burgess, M.A.; Cote, G.J.; Gagel, R.F.; et al. Surgical Strategy for the Treatment of Medullary Thyroid Carcinoma. Ann. Surg. 1999, 230, 697–707. [Google Scholar] [CrossRef]
- Kebebew, E.; Greenspan, F.S.; Clark, O.H.; Woeber, K.A.; Grunwell, J. Extent of Disease and Practice Patterns for Medullary Thyroid Cancer. J. Am. Coll. Surg. 2005, 200, 890–896. [Google Scholar] [CrossRef]
- Kiriakopoulos, A.; Giannakis, P.; Menenakos, E. Calcitonin: Current concepts and differential diagnosis. Ther. Adv. Endocrinol. Metab. 2022, 13, 1–16. [Google Scholar] [CrossRef]
- Xiao, J.; Jiang, J.; Chen, W.; Hong, T.; Li, B.; He, X.; Liu, W. Combination of ultrasound and serological tests for detecting occult lateral lymph node metastases in medullary thyroid cancer. Cancer Med. 2023, 12, 11417–11426. [Google Scholar] [CrossRef]
- Gan, F.-J.; Zhou, T.; Wu, S.; Xu, M.-X.; Sun, S.-H. Do medullary thyroid carcinoma patients with high calcitonin require bilateral neck lymph node clearance? A case report. World J. Clin. Cases 2021, 9, 1343–1352. [Google Scholar] [CrossRef] [PubMed]
- Machens, A.; Lorenz, K.; Weber, F.; Dralle, H. Risk Patterns of Distant Metastases in Follicular, Papillary and Medullary Thyroid Cancer. Horm. Metab. Res. 2021, 54, 7–11. [Google Scholar] [CrossRef]
- Trimboli, P.; Giannelli, J.; Marques, B.; Piccardo, A.; Crescenzi, A.; Deandrea, M. Head-to-head comparison of FNA cytology vs. calcitonin measurements in FNA washout fluid (FNA-CT) to diagnose medullary thyroid carcinoma. A systematic review and meta-analysis. Endocrine 2022, 75, 33–39. [Google Scholar] [CrossRef]
- Modigliani, E.; Cohen, R.; Campos, J.; Conte-Devolx, B.; Maes, B.; Boneu, A.; Schlumberger, M.; Bigorgne, J.; Dumontier, P.; Leclerc, L.; et al. Prognostic factors for survival and for biochemical cure in medullary thyroid carcinoma: Results in 899 patients. Clin. Endocrinol. 1998, 48, 265–273. [Google Scholar] [CrossRef] [PubMed]
- Bartz-Kurycki, M.A.; Oluwo, O.E.; Morris-Wiseman, L.F. Medullary thyroid carcinoma: Recent advances in identification, treatment, and prognosis. Ther. Adv. Endocrinol. Metab. 2021, 12. [Google Scholar] [CrossRef]
- I Haddad, R.; Bischoff, L.; Ball, D.; Bernet, V.; Blomain, E.; Busaidy, N.L.; Campbell, M.; Dickson, P.; Duh, Q.-Y.; Ehya, H.; et al. Thyroid Carcinoma, Version 2.2022. J. Natl. Compr. Cancer Netw. 2022, 20, 925–951. [Google Scholar] [CrossRef] [PubMed]
- Shi, X.; Sun, Y.; Shen, C.; Zhang, Y.; Shi, R.; Zhang, F.; Liao, T.; Lv, G.; Zhu, Z.; Jiao, L.; et al. Integrated proteogenomic characterization of medullary thyroid carcinoma. Cell Discov. 2022, 8, 1–22. [Google Scholar] [CrossRef]
- Gan, F.-J.; Zhou, T.; Wu, S.; Xu, M.-X.; Sun, S.-H. Do medullary thyroid carcinoma patients with high calcitonin require bilateral neck lymph node clearance? A case report. World J. Clin. Cases 2021, 9, 1343–1352. [Google Scholar] [CrossRef]
- Shaghaghi, A.; Salari, A.; Jalaeefar, A.; Shirkhoda, M. Management of lymph nodes in medullary thyroid carcinoma: A review. Ann. Med. Surg. 2022, 81, 104538. [Google Scholar] [CrossRef]
- Roy, M.; Chen, H.; Sippel, R.S. Current Understanding and Management of Medullary Thyroid Cancer. Oncol. 2013, 18, 1093–1100. [Google Scholar] [CrossRef] [PubMed]
- Duarte, P.S.; de Castroneves, L.A.; Sado, H.N.; Sapienza, M.T.; Hoff, A.A.F.d.O.; Buchpiguel, C.A. Bone and Calcified Soft Tissue Metastases of Medullary Thyroid Carcinoma Better Characterized on 18F-Fluoride PET/CT than on 68Ga-Dotatate PET/CT. Nucl. Med. Mol. Imaging 2018, 52, 318–323. [Google Scholar] [CrossRef]
- Rasul, S.; Hartenbach, S.; Rebhan, K.; Göllner, A.; Karanikas, G.; Mayerhoefer, M.; Mazal, P.; Hacker, M.; Hartenbach, M. [18F]DOPA PET/ceCT in diagnosis and staging of primary medullary thyroid carcinoma prior to surgery. Eur. J. Nucl. Med. Mol Imaging. 2018, 45, 2159–2169. [Google Scholar] [CrossRef] [PubMed]
- Martins, R.S.; Jesus, T.T.; Cardoso, L.; Soares, P.; Vinagre, J. Personalized Medicine in Medullary Thyroid Carcinoma: A Broad Review of Emerging Treatments. J. Pers. Med. 2023, 13, 1132. [Google Scholar] [CrossRef]
- Trimboli, P.; Ferrarazzo, G.; Cappelli, C.; Piccardo, A.; Castellana, M.; Barizzi, J. Thyroid nodules with Indeterminate FNAC According to the Italian Classification System: Prevalance, Rate of Operation, and Impact on Risk of Malignancy. . An Updated Systematic Review and Meta-analysis. Endo Pathol. 2022, 33, 457–471. [Google Scholar] [CrossRef]
- Liu, C.-Q.; Shen, C.-K.; Du, Y.-X.; Li, Z.-M.; Shi, X.; Wang, Y.; Wei, W.-J. Survival Outcome and Optimal Candidates of Primary Tumor Resection for Patients With Metastatic Medullary Thyroid Cancer. J. Clin. Endocrinol. Metab. 2024. [Google Scholar] [CrossRef] [PubMed]
- Brammen, L.; Niederle, M.B.; Riss, P.; Scheuba, C.; Selberherr, A.; Karanikas, G.; Bodner, G.; Koperek, O.; Niederle, B. Medullary Thyroid Carcinoma: Do Ultrasonography and F-DOPA-PET-CT Influence the Initial Surgical Strategy? Ann. Surg. Oncol. 2018, 25, 3919–3927. [Google Scholar] [CrossRef]
- Fan, Y.; Xu, H.; Lv, M.; Li, N. Preoperative Serum Calcitonin Level and Ultrasonographic Characteristics Predict the Risk of Metastatic Medullary Thyroid Carcinoma: Functional Analysis of Calcitonin-Related Genes. Dis. Markers 2022, 2022, 1–14. [Google Scholar] [CrossRef]
- Gambardella, C.; Offi, C.; Clarizia, G.; Romano, R.M.; Cozzolino, I.; Montella, M.; Di Crescenzo, R.M.; Mascolo, M.; Cangiano, A.; Di Martino, S.; et al. Medullary thyroid carcinoma with double negative calcitonin and CEA: A case report and update of literature review. BMC Endocr. Disord. 2019, 19, 1–8. [Google Scholar] [CrossRef]
- Gambardella, C.; Offi, C.; Patrone, R.; Clarizia, G.; Mauriello, C.; Tartaglia, E.; Di Capua, F.; Di Martino, S.; Romano, R.M.; Fiore, L.; et al. Calcitonin negative Medullary Thyroid Carcinoma: A challenging diagnosis or a medical dilemma? BMC Endocr. Disord. 2019, 19, 1–12. [Google Scholar] [CrossRef]
- Wienliang, Y.; Zhang, Y. Oncologic outcomes of calcitonin-negative medullary thyroid carcinoma. Front Endocrinol 2022, 13, 1025629. [Google Scholar] [CrossRef]
- Trimboli, P.; Camponovo, C.; Ruinelli, L. The dilemma of routine testing for calcitonin thyroid nodule’s patients to detect or exclude medullary carcinoma: One single negative test should be valuable as rule-out strategy to avoid further calcitonin measurements over time. Endocrine 2022, 77, 80–85. [Google Scholar] [CrossRef]
- Thomas, C.M.; Asa, S.L.; Ezzat, S.; Sawka, A.M.; Goldstein, D. Diagnosis and Pathologic Characteristics of Medullary Thyroid Carcinoma—Review of Current Guidelines. Curr. Oncol. 2019, 26, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Moon, W.S.; Kang, M.J.; Youn, H.J.; Kim, K.M. Diagnostic pitfall of thyroid fine-needle aspiration induced fibrosis: Follicular adenoma mimicking medullary thyroid carcinoma in frozen section. Diagn. Pathol. 2021, 16, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Ciarletto, A.M.; Narick, C.; Malchoff, C.D.; Massoll, N.A.; Labourier, E.; Haugh, K.; Mireskandari, A.; Finkelstein, S.D.; Kumar, G. Analytical and clinical validation of pairwise microRNA expression analysis to identify medullary thyroid cancer in thyroid fine-needle aspiration samples. Cancer Cytopathol. 2020, 129, 239–249. [Google Scholar] [CrossRef]
- Ferrarazzo, G.; Camponovo, C.; Deandrea, M.; Piccardo, A.; Scappaticcio, L.; Trimboli, P. Suboptimal accuracy of ultrasound and ultrasound-based risk stratification systems in detecting medullary thyroid carcinoma should not be overlooked. Findings from a systematic review with meta-analysis. Clin. Endocrinol. 2022, 97, 532–540. [Google Scholar] [CrossRef] [PubMed]
- Torresan, F.; Armellin, C.; Iacobone, M. Management of medullary carcinoma. Ann Thyroid 2020, 5, 16. [Google Scholar] [CrossRef]
- Makri, A.; Akshintala, S.; Derse-Anthony, C.; Del Rivero, J.; Widemann, B.; A Stratakis, C.; Glod, J.; Lodish, M. Pheochromocytoma in Children and Adolescents With Multiple Endocrine Neoplasia Type 2B. J. Clin. Endocrinol. Metab. 2018, 104, 7–12. [Google Scholar] [CrossRef]
- Opsahl, E.M.; Brauckhoff, M.; Schlichting, E.; Helset, K.; Svartberg, J.; Brauckhoff, K.; Mæhle, L.; Engebretsen, L.F.; Sigstad, E.; Grøholt, K.K.; et al. A Nationwide Study of Multiple Endocrine Neoplasia Type 2A in Norway: Predictive and Prognostic Factors for the Clinical Course of Medullary Thyroid Carcinoma. Thyroid® 2016, 26, 1225–1238. [Google Scholar] [CrossRef]
- Choi, Y.S.; Kwon, H.J.; Kim, B.K.; Kwon, S.K.; Park, Y.H.; Kim, J.H.; Jung, S.B.; Lee, C.H.; Lee, S.K.; Uchino, S. A Case of Medullary Thyroid Carcinoma with de novo V804M RET Germline Mutation. J. Korean Med Sci. 2013, 28, 156–159. [Google Scholar] [CrossRef] [PubMed]
- Lombardo, F.; Baudin, E.; Chiefari, E.; Arturi, F.; Bardet, S.; Caillou, B.; Conte, C.; Dallapiccola, B.; Giuffrida, D.; Bidart, J.-M.; et al. Familial Medullary Thyroid Carcinoma: Clinical Variability and Low Aggressiveness Associated withRETMutation at Codon 804. J. Clin. Endocrinol. Metab. 2002, 87, 1674–1680. [Google Scholar] [CrossRef] [PubMed]
- Dabir, T.; Hunter, S.J.; Russell, C.F.J.; McCall, D.; Morrison, P.J. The RET Mutation E768D Confers a Late-onset Familial Medullary Thyroid Carcinoma – Only Phenotype with Incomplete Penetrance: Implications for Screening and Management of Carrier Status. Fam. Cancer 2006, 5, 201–204. [Google Scholar] [CrossRef] [PubMed]
- Shirali, A.S.; I Hu, M.; Chiang, Y.-J.; Graham, P.H.; Fisher, S.B.; Sosa, J.A.; Perrier, N.; Brown, S.; Holla, V.R.; Dadu, R.; et al. Next-Generation Sequencing in Sporadic Medullary Thyroid Cancer Patients: Mutation Profile and Disease Aggressiveness. J. Endocr. Soc. 2024, 8, bvae048. [Google Scholar] [CrossRef] [PubMed]
- Al-Kurd, A.; Gross, D.J.; Zangen, A.; Atlan, K.; Mazeh, H.; Grozinsky-Glasberg, S. Bilateral Medullary thyroid carcinoma in a 3-year-old female patient with Multiple Endocrine Neoplasia 2A Syndrome Undergoing prophylactic Thyroidectomy:Should current guidelines be revised? Eur Thyroid J 2018, 79, 267–271. [Google Scholar] [CrossRef] [PubMed]
- Yue, W.; Zhang, Y. Oncologic outcomes of calcitonin-negative medullary thyroid carcinoma. Front. Endocrinol. 2022, 13, 1025629. [Google Scholar] [CrossRef]
- Murphy, D.; Johnson, S.; Aspinall, S. Calcitonin-negative medullary thyroid carcinoma: The 'triple-negative' phenotype. Ind. Mark. Manag. 2020, 102, E63–E66. [Google Scholar] [CrossRef]
- Niederle, B. Screening for medullary carcinoma of the thyroid. Br. J. Surg. 2014, 101, 1625–1626. [Google Scholar] [CrossRef]
- Yang, X.; Xu, J.; Sun, J.; Yin, L.; Guo, R.; Yan, Z. Clinical value of color Doppler ultrasound combined with serum tumor markers for the diagnosis of medullary thyroid carcinoma. Oncol. Lett. 2021, 22, 1–9. [Google Scholar] [CrossRef]
- Gild, M.L.; Clifton-Bligh, R.J.; Wirth, L.J.; Robinson, B.G. Medullary Thyroid Cancer: Updates and Challenges. Endocr. Rev. 2023, 44, 934–946. [Google Scholar] [CrossRef]
- Lang, S.; Xu, Y.; Li, L.; Wang, B.; Yang, Y.; Xue, Y.; Shi, K. Joint Detection of Tap and CEA Based on Deep Learning Medical Image Segmentation: Risk Prediction of Thyroid Cancer. J. Health Eng. 2021, 2021, 1–9. [Google Scholar] [CrossRef]
- Wilczyńska, M.; Suchmiel, M.; Sokołowski, G.; Hubalewska-Dydejczyk, A.; Trofimiuk-Müldner, M. Disseminated medullary thyroid cancer - an alternative therapeutic approach. Endokrynol. Polska 2022, 73, 909–910. [Google Scholar] [CrossRef] [PubMed]
- Kaul, V.; Enslin, S.; Gross, S.A. History of artificial intelligence in medicine. Gastrointest. Endosc. 2020, 92, 807–812. [Google Scholar] [CrossRef]
- Cao, C.L.; Li, Q.L.; Tong, J.; Shi, L.N.; Liv, W.X.; Xu, Y.; Cheng, J.; Du, T.T.; Li, J.; Cui, X.W. Artificial Intelligence in thyroid ultrasound. Front Oncol 2023, 13, 1060702. [Google Scholar] [CrossRef]
- Li, L.-R.; Du, B.; Liu, H.-Q.; Chen, C. Artificial Intelligence for Personalized Medicine in Thyroid Cancer: Current Status and Future Perspectives. Front. Oncol. 2021, 10, 604051. [Google Scholar] [CrossRef]
- Liu, T.; Meng, J.; Zhang, Y. miR-592 acts as an oncogene and promotes medullary thyroid cancer tumorigenesis by targeting cyclin-dependent kinase 8. Mol. Med. Rep. 2020, 22, 3316–3326. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Li, Z.; Luo, Z.; Liao, W.; Liu, Z.; Liu, J. Machine learning for the prediction of bone metastasis in patients with newly diagnosed thyroid cancer. Cancer Med. 2021, 10, 2802–2811. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Wang, S.; Ye, Z.; Xu, P.; Xia, X.; Guo, M. Prediction of lung metastases in thyroid cancer using machine learning based on SEER database. Cancer Med. 2022, 11, 2503–2515. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Feng, Q.; Wang, J.; Tan, Z.; Li, Q.; Ge, M. Molecular basis and targeted therapy in thyroid cancer: Progress and opportunities. Biochim. et Biophys. Acta (BBA) - Rev. Cancer 2023, 1878, 188928. [Google Scholar] [CrossRef]
- Hill, K.; Diaz, J.; Hagemann, I.S.; Chernock, R.D. Multiple Myeloma Presenting as Massive Amyloid Deposition in a Parathyroid Gland Associated with Amyloid Goiter: A Medullary Thyroid Carcinoma Mimic on Intra-operative Frozen Section. Head Neck Pathol. 2018, 12, 269–273. [Google Scholar] [CrossRef]
- Peng, S.; Liu, Y.; Lv, W.; Liu, L.; Zhou, Q.; Yang, H.; Ren, J.; Liu, G.; Wang, X.; Zhang, X.; et al. Deep learning-based artificial intelligence model to assist thyroid nodule diagnosis and management: A multicentre diagnostic study. Lancet Digit. Heal. 2021, 3, e250–e259. [Google Scholar] [CrossRef]
- Lin, Q.; Qi, Q.; Hou, S.; Chen, Z.; Jiang, N.; Zhang, L.; Lin, C. Application of Pet-CT Fusion Deep Learning Imaging in Precise Radiotherapy of Thyroid Cancer. J. Heal. Eng. 2021, 2021, 1–10. [Google Scholar] [CrossRef]
- Wang, C.-W.; Muzakky, H.; Lee, Y.-C.; Lin, Y.-J.; Chao, T.-K. Annotation-Free Deep Learning-Based Prediction of Thyroid Molecular Cancer Biomarker BRAF (V600E) from Cytological Slides. Int. J. Mol. Sci. 2023, 24, 2521. [Google Scholar] [CrossRef] [PubMed]
- Hirokawa, M.; Niioka, H.; Suzuki, A.; Abe, M.; Arai, Y.; Nagahara, H.; Miyauchi, A.; Akamizu, T. Application of deep learning as an ancillary diagnostic tool for thyroid FNA cytology. Cancer Cytopathol. 2022, 131, 217–225. [Google Scholar] [CrossRef] [PubMed]
- Xi, N.M.; Wang, L.; Yang, C. Improving the diagnosis of thyroid cancer by machine learning and clinical data. Sci. Rep. 2022, 12, 1–11. [Google Scholar] [CrossRef]
- Gao, L.; Xi, X.; Jiang, Y.; Yang, X.; Wang, Y.; Zhu, S.; Lai, X.; Zhang, X.; Zhao, R.; Zhang, B. Comparison among TIRADS (ACR TI-RADS and KWAK- TI-RADS) and 2015 ATA Guidelines in the diagnostic efficiency of thyroid nodules. Endocrine 2019, 64, 90–96. [Google Scholar] [CrossRef] [PubMed]
- Radebe, L.; van der Kaay, D.C.M.; Wasserman, J.D.; Goldenberg, A. Predicting Malignancy in Pediatric Thyroid Nodules: Early Experience With Machine Learning for Clinical Decision Support. J. Clin. Endocrinol. Metab. 2021, 106, e5236–e5246. [Google Scholar] [CrossRef]
- Zhao, H.-B.; Liu, C.; Ye, J.; Chang, L.-F.; Xu, Q.; Shi, B.-W.; Liu, L.-L.; Yin, Y.-L.; Shi, B.-B. A comparison between deep learning convolutional neural networks and radiologists in the differentiation of benign and malignant thyroid nodules on CT images. Endokrynol. Polska 2021, 72, 217–225. [Google Scholar] [CrossRef]
- Zhao, L.; Ma, B. Radiomics Features of Different Sizes of Medullary Thyroid Carcinoma (MTC) and Papillary Thyroid Carcinoma (PTC) Tumors: A Comparative Study. Clin. Med. Insights: Oncol. 2022, 16, 11795549221097675. [Google Scholar] [CrossRef]
- Wong, C.M.; Kezlarian, B.E.; Lin, O. Current status of machine learning in thyroid cytopathology. J. Pathol. Informatics 2023, 14, 100309. [Google Scholar] [CrossRef]
- Maurea, S.; Stanzione, A.; Klain, M. Thyroid Cancer Radiomics: Navigating Challenges in a Developing Landscape. Cancers 2023, 15, 5884. [Google Scholar] [CrossRef] [PubMed]
- Cordes, M.; Götz, T.I.; Coerper, S.; Kuwert, T.; Schmidkonz, C. Ultrasound characteristics of follicular and parafollicular thyroid neoplasms: Diagnostic performance of artificial neural network. Thyroid. Res. 2023, 16, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Niazi, M.K.K.; Parwani, A.V.; Gurcan, M.N. Digital pathology and artificial intelligence. Lancet Oncol. 2019, 20, e253–e261. [Google Scholar] [CrossRef] [PubMed]
- Stanzione, A.; Cuocolo, R.; Ugga, L.; Verde, F.; Romeo, V.; Brunetti, A.; Maurea, S. Oncologic Imaging and Radiomics: A Walkthrough Review of Methodological Challenges. Cancers 2022, 14, 4871. [Google Scholar] [CrossRef]
- Zhao, Z.; Ye, C.; Hu, Y.; Li, C.; Li, X. Cascade and Fusion of Multitask Convolutional Neural Networks for Detection of Thyroid Nodules in Contrast-Enhanced CT. Comput. Intell. Neurosci. 2019, 2019, 1–13. [Google Scholar] [CrossRef]
- Li, W.; Cheng, S.; Qian, K.; Yue, K.; Liu, H. Automatic Recognition and Classification System of Thyroid Nodules in CT Images Based on CNN. Comput. Intell. Neurosci. 2021, 2021, 5540186. [Google Scholar] [CrossRef]
- Guo, Z.-T.; Tian, K.; Xie, X.-Y.; Zhang, Y.-H.; Fang, D.-B. Machine Learning for Predicting Distant Metastasis of Medullary Thyroid Carcinoma Using the SEER Database. Int. J. Endocrinol. 2023, 2023, 1–10. [Google Scholar] [CrossRef]
- Krishnan, G.; Singh, S.; Pathania, M.; Gosavi, S.; Abhishek, S.; Parchani, A.; Dhar, M. Artificial intelligence in clinical medicine: Catalyzing a sustainable global healthcare paradigm. Front. Artif. Intell. 2023, 6, 1227091. [Google Scholar] [CrossRef]
- Ma, X.; Han, X.; Zhang, L. An Improved k-Nearest Neighbor Algorithm for Recognition and Classification of Thyroid Nodules. J. Ultrasound Med. 2024, 43, 1025–1036. [Google Scholar] [CrossRef]
- Habchi, Y.; Himeur, Y.; Kheddar, H.; Boukabou, A.; Atalla, S.; Chouchane, A.; Ouamane, A.; Mansoor, W. AI in Thyroid Cancer Diagnosis: Techniques, Trends, and Future Directions. Systems 2023, 11, 519. [Google Scholar] [CrossRef]
- Zhang, Z.; Zhao, Y.; Canes, A.; Steinberg, D.; Lyashevska, O.; written on behalf of AME Big-Data Clinical Trial Collaborative Group. Predictive analytics with gradient boosting in clinical medicine. Ann. Transl. Med. 2019, 7, 152. [Google Scholar] [CrossRef]
- BuHamra, S.S.; Almutairi, A.N.; Buhamrah, A.K.; Almadani, S.H.; Alibrahim, Y.A. An NLP tool for data extraction from electronic health records: COVID-19 mortalities and comorbidities. Front. Public Heal. 2022, 10, 1070870. [Google Scholar] [CrossRef] [PubMed]
- Franco, E.F.; Rana, P.; Cruz, A.; Calderón, V.V.; Azevedo, V.; Ramos, R.T.J.; Ghosh, P. Performance Comparison of Deep Learning Autoencoders for Cancer Subtype Detection Using Multi-Omics Data. Cancers 2021, 13, 2013. [Google Scholar] [CrossRef]
- Boulos, M.N.K.; Peng, G.; VoPham, T. An overview of GeoAI applications in health and healthcare. Int. J. Heal. Geogr. 2019, 18, 7. [Google Scholar] [CrossRef]
- Tseng, Y.-J.; Wang, H.-Y.; Lin, T.-W.; Lu, J.-J.; Hsieh, C.-H.; Liao, C.-T. Development of a Machine Learning Model for Survival Risk Stratification of Patients With Advanced Oral Cancer. JAMA Netw. Open 2020, 3, e2011768. [Google Scholar] [CrossRef] [PubMed]
- Rathi, R.; Vakharia, A.; Shadab, M. Lean six sigma in the healthcare sector: A systematic literature review. Mater. Today Proc. 2022, 50, 773–781. [Google Scholar] [CrossRef]
- Dean, D.S.; Gharib, H. Epidemiology of thyroid nodules. Best Pract. Res. Clin. Endocrinol. Metab. 2008, 22, 901–911. [Google Scholar] [CrossRef]
- Liu, Z.; Zhang, X.; Zhao, X.; Guo, Q.; Li, Z.; Wei, M.; Niu, L.; An, C. Combining radiomics with thyroid imaging reporting and data system to predict lateral cervical lymph node metastases in medullary thyroid cancer. BMC Med Imaging 2024, 24, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Gatta, R.; Depeursinge, A.; Ratib, O.; Michielin, O.; Leimgruber, A. Integrating radiomics into holomics for personalised oncology: From algorithms to bedside. Eur. Radiol. Exp. 2020, 4, 1–9. [Google Scholar] [CrossRef]
- Piccardo, A.; Puntoni, M.; Treglia, G.; Foppiani, L.; Bertagna, F.; Paparo, F.; Massollo, M.; Dib, B.; Paone, G.; Arlandini, A.; et al. Thyroid nodules with indeterminate cytology: Prospective comparison between 18F-FDG-PET/CT, multiparametric neck ultrasonography, 99mTc-MIBI scintigraphy and histology. Eur. J. Endocrinol. 2016, 174, 693–703. [Google Scholar] [CrossRef]
- Cao, Y.; Zhong, X.; Diao, W.; Mu, J.; Cheng, Y.; Jia, Z. Radiomics in Differentiated Thyroid Cancer and Nodules: Explorations, Application, and Limitations. Cancers 2021, 13, 2436. [Google Scholar] [CrossRef] [PubMed]
- Le, N.Q.K.; Kha, Q.H.; Nguyen, V.H.; Chen, Y.-C.; Cheng, S.-J.; Chen, C.-Y. Machine Learning-Based Radiomics Signatures for EGFR and KRAS Mutations Prediction in Non-Small-Cell Lung Cancer. Int. J. Mol. Sci. 2021, 22, 9254. [Google Scholar] [CrossRef] [PubMed]
- Nardone, V.; Reginelli, A.; Grassi, R.; Boldrini, L.; Vacca, G.; D’ippolito, E.; Annunziata, S.; Farchione, A.; Belfiore, M.P.; Desideri, I.; et al. Delta radiomics: A systematic review. La Radiol. medica 2021, 126, 1571–1583. [Google Scholar] [CrossRef] [PubMed]
- Ludwig, M.; Ludwig, B.; Mikuła, A.; Biernat, S.; Rudnicki, J.; Kaliszewski, K. The Use of Artificial Intelligence in the Diagnosis and Classification of Thyroid Nodules: An Update. Cancers 2023, 15, 708. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.H.; Lee, Y.H.; Seo, H.S.; Lee, K.Y.; Suh, S.; Ryoo, I.; You, S.; Kim, B.; Yang, K. Dual-energy CT iodine quantification for characterizing focal thyroid lesions. Head Neck 2018, 41, 1024–1031. [Google Scholar] [CrossRef]
- Gupta, R.; Kurc, T.; Sharma, A.; Almeida, J.S.; Saltz, J. The Emergence of Pathomics. Curr. Pathobiol. Rep. 2019, 7, 73–84. [Google Scholar] [CrossRef]
- Wang, Z.; Fan, X.; Zha, X.; Xu, Y.; Yin, Z.; Rixiati, Y.; Yu, F. A Proposed Modified Staging System for Medullary Thyroid Cancer: A SEER Analysis With Multicenter Validation. Oncol. 2023, 29, e59–e67. [Google Scholar] [CrossRef]
- Bera, K.; Schalper, K.A.; Rimm, D.L.; Velcheti, V.; Madabhushi, A. Artificial intelligence in digital pathology—New tools for diagnosis and precision oncology. Nat. Rev. Clin. Oncol. 2019, 16, 703–715. [Google Scholar] [CrossRef]
- Wei, S.; LiVolsi, V.A.; Montone, K.T.; Morrissette, J.J.D.; Baloch, Z.W. Detection of Molecular Alterations in Medullary Thyroid Carcinoma Using Next-Generation Sequencing: An Institutional Experience. Endocr. Pathol. 2016, 27, 359–362. [Google Scholar] [CrossRef]
- Zhang, L.; Lu, D.; Liu, M.; Zhang, M.; Peng, Q. Identification and interaction analysis of key miRNAs in medullary thyroid carcinoma by bioinformatics analysis. Mol. Med. Rep. 2019, 20, 2316–2324. [Google Scholar] [CrossRef]
- Censi, S.; Bertazza, L.; Piva, I.; Manso, J.; Benna, C.; Iacobone, M.; Mondin, A.; Plebani, M.; Faggian, D.; Galuppini, F.; et al. Serum miR-375 for Diagnostic and Prognostic Purposes in Medullary Thyroid Carcinoma. Front. Endocrinol. 2021, 12, 647369. [Google Scholar] [CrossRef] [PubMed]
- Wei, S.; LiVolsi, V.A.; Montone, K.T.; Morrissette, J.J.D.; Baloch, Z.W. Detection of Molecular Alterations in Medullary Thyroid Carcinoma Using Next-Generation Sequencing: An Institutional Experience. Endocr. Pathol. 2016, 27, 359–362. [Google Scholar] [CrossRef]
- Shabani, N.; Razaviyan, J.; Paryan, M.; Tavangar, S.M.; Azizi, F.; Mohammadi-Yeganeh, S.; Hedayati, M. Evaluation of miRNAs expression in medullary thyroid carcinoma tissue samples: miR-34a and miR-144 as promising overexpressed markers in MTC. Hum. Pathol. 2018, 79, 212–221. [Google Scholar] [CrossRef]
- Abraham, D.; Jackson, N.; Gundara, J.S.; Zhao, J.; Gill, A.J.; Delbridge, L.; Robinson, B.G.; Sidhu, S.B. MicroRNA Profiling of Sporadic and Hereditary Medullary Thyroid Cancer Identifies Predictors of Nodal Metastasis, Prognosis, and Potential Therapeutic Targets. Clin. Cancer Res. 2011, 17, 4772–4781. [Google Scholar] [CrossRef] [PubMed]
- Jajin, M.G.; Abooshahab, R.; Hooshmand, K.; Moradi, A.; Siadat, S.D.; Mirzazadeh, R.; Chegini, K.G.; Hedayati, M. Gas chromatography-mass spectrometry-based untargeted metabolomics reveals metabolic perturbations in medullary thyroid carcinoma. Sci. Rep. 2022, 12, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Krneta, M.P.; Šaranović, D.; Teodorović, L.M.; Krajčinović, N.; Avramović, N.; Bojović, Z.; Bukumirić, Z.; Marković, I.; Rajšić, S.; Djorović, B.B.; et al. Prediction of Cervical Lymph Node Metastasis in Clinically Node-Negative T1 and T2 Papillary Thyroid Carcinoma Using Supervised Machine Learning Approach. J. Clin. Med. 2023, 12, 3641. [Google Scholar] [CrossRef]
- Wang, B.; Xu, X.; Zhao, Z.Y.; Yan, J.B.; Yao, D.Y. A rare coexistence of parathyroid adenoma and medullary and papillary thyroid carcinoma. Int J Clin Exp Pathol. 2020, 13, 2387–2391. [Google Scholar]
- Innella, G.; Rossi, C.; Romagnoli, M.; Repaci, A.; Bianchi, D.; Cantarini, M.E.; Martorana, D.; Godino, L.; Pession, A.; Percesepe, A.; et al. Results and Clinical Interpretation of Germline RET Analysis in a Series of Patients with Medullary Thyroid Carcinoma: The Challenge of the Variants of Uncertain Significance. Cancers 2020, 12, 3268. [Google Scholar] [CrossRef]
- Ghazani, A.A.; Breen, K.M.; Dwan, M.; Barletta, J.A.; Vatnick, D.R.; Stokes, S.M.; Block, C.; Doherty, G.M.; Cohn, A.Y.; Marqusee, E.; et al. Unexpected Pathogenic RET p.V804M Variant Leads to the Clinical Diagnosis and Management of Medullary Thyroid Carcinoma. Am. J. Case Rep. 2020, 21, e927415. [Google Scholar] [CrossRef]
- Skalnaniak, A.; Trofimiuk-Mudldner, M.; Przybylik-Mazerek, E.; Hubalewska-Dydejczyk, A. Modifier Role of Common RET Variants in Sporadic Medullary Thyroid Carcinoma. Int J Mol Sci. 22, 11794. [CrossRef]
- Randolph, G.W.; Sosa, J.A.; Hao, Y.; Angell, T.E.; Shonka, D.C.; LiVolsi, V.A.; Ladenson, P.W.; Blevins, T.C.; Duh, Q.-Y.; Ghossein, R.; et al. Preoperative Identification of Medullary Thyroid Carcinoma (MTC): Clinical Validation of the Afirma MTC RNA-Sequencing Classifier. Thyroid® 2022, 32, 1069–1076. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Wong, C.; Li, Y.; Huang, T.; Wang, J.; Lin, C. Artificial intelligence assisted diagnosis of early tc markers and its application. Discov. Oncol. 2024, 15, 1–11. [Google Scholar] [CrossRef]
- Liao, J.; Li, X.; Gan, Y.; Han, S.; Rong, P.; Wang, W.; Li, W.; Zhou, L. Artificial intelligence assists precision medicine in cancer treatment. Front. Oncol. 2023, 12, 998222. [Google Scholar] [CrossRef] [PubMed]
- A Aksoy, Y.; Xu, B.; Viswanathan, K.; Ahadi, M.S.; Al Ghuzlan, A.; Alzumaili, B.; Bani, M.; A Barletta, J.; Chau, N.; Chou, A.; et al. Novel prognostic nomogram for predicting recurrence-free survival in medullary thyroid carcinoma. Histopathology 2024, 84, 947–959. [Google Scholar] [CrossRef] [PubMed]
- Munk, K.; Ilina, D.; Ziemba, L.; Brader, G.; Molin, E.M. Holomics - a user-friendly R shiny application for multi-omics data integration and analysis. BMC Bioinform. 2024, 25, 1–20. [Google Scholar] [CrossRef] [PubMed]
- López, D.M.; Rico-Olarte, C.; Blobel, B.; Hullin, C. Challenges and solutions for transforming health ecosystems in low- and middle-income countries through artificial intelligence. Front. Med. 2022, 9, 958097. [Google Scholar] [CrossRef]
- Ludwig, M.; Ludwig, B.; Mikuła, A.; Biernat, S.; Rudnicki, J.; Kaliszewski, K. The Use of Artificial Intelligence in the Diagnosis and Classification of Thyroid Nodules: An Update. Cancers 2023, 15, 708. [Google Scholar] [CrossRef]
- Zhang, X.; Zhao, X.; Jin, L.; Guo, Q.; Wei, M.; Li, Z.; Niu, L.; Liu, Z.; An, C. The machine learning-based model for lateral lymph node metastasis of thyroid medullary carcinoma improved the prediction ability of occult metastasis. Cancer Med. 2024, 13, e7155. [Google Scholar] [CrossRef]
- Cote, G.J.; Evers, C.; I Hu, M.; Grubbs, E.G.; Williams, M.D.; Hai, T.; Duose, D.Y.; Houston, M.R.; Bui, J.H.; Mehrotra, M.; et al. Prognostic Significance of Circulating RET M918T Mutated Tumor DNA in Patients With Advanced Medullary Thyroid Carcinoma. J. Clin. Endocrinol. Metab. 2017, 102, 3591–3599. [Google Scholar] [CrossRef]
- Gao, X.; Ran, X.; Ding, W. The progress of radiomics in thyroid nodules. Front. Oncol. 2023, 13, 1109319. [Google Scholar] [CrossRef]
- Shen, C.; Shi, X.; Wen, D.; Zhang, Y.; Du, Y.; Zhang, Y.; Ma, B.; Tang, H.; Yin, M.; Huang, N.; et al. Comprehensive DNA Methylation Profiling of Medullary Thyroid Carcinoma: Molecular Classification, Potential Therapeutic Target, and Classifier System. Clin. Cancer Res. 2023, 30, 127–138. [Google Scholar] [CrossRef]
- Minna, E.; Romeo, P.; Dugo, M.; De Cecco, L.; Aiello, A.; Pistore, F.; Carenzo, A.; Greco, A.; Borrello, M.G. Medullary Thyroid Carcinoma Mutational Spectrum Update and Signaling-Type Inference by Transcriptional Profiles: Literature Meta-Analysis and Study of Tumor Samples. Cancers 2022, 14, 1951. [Google Scholar] [CrossRef] [PubMed]
- Gumà, J.; Peña, K.B.; Riu, F.; Lucia-Gozálvez, C.; Vidaller, A.; Maldonado, V.; Parada, D. Blood Liquid Biopsy in an Advanced Medullary Thyroid Carcinoma: A Case Study with Rearranged during Transfection Heterogeneity. Pathobiology 2023, 90, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Pozdeyev, N.; Erickson, T.A.; Zhang, L.; Ellison, K.; Rivard, C.J.; Sams, S.; Hirsch, F.R.; Haugen, B.R.; French, J.D. Comprehensive Immune Profiling of Medullary Thyroid Cancer. Thyroid® 2020, 30, 1263–1279. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Zhao, H.; Li, X. Serum Biochemical Markers for Medullary Thyroid Carcinoma: An Update. Cancer Manag. Res. 2024, 16, 299–310. [Google Scholar] [CrossRef] [PubMed]
- Guo, F.; Li, L.; Gu, P.; Zhang, G.; Ruan, X.; Zhao, J.; Zheng, X.; Wei, S.; Gao, M. Changes of biochemical factors and the effect on recurrence of medullary thyroid carcinoma after surgery. Heliyon 2024, 10, e29857. [Google Scholar] [CrossRef]
- Matrone, A.; Gambale, C.; Prete, A.; Piaggi, P.; Cappagli, V.; Bottici, V.; Romei, C.; Ciampi, R.; Torregrossa, L.; De Napoli, L.; et al. Impact of Advanced Age on the Clinical Presentation and Outcome of Sporadic Medullary Thyroid Carcinoma. Cancers 2020, 13, 94. [Google Scholar] [CrossRef]
- Sahli, Z.T.; Canner, J.K.; Zeiger, M.A.; Mathur, A. Association between age and disease specific mortality in medullary thyroid cancer. Am. J. Surg. 2020, 221, 478–484. [Google Scholar] [CrossRef]
Figure 1.
Classification and mutational landscape of sporadic and hereditary medullary thyroid carcinoma.
Figure 1.
Classification and mutational landscape of sporadic and hereditary medullary thyroid carcinoma.
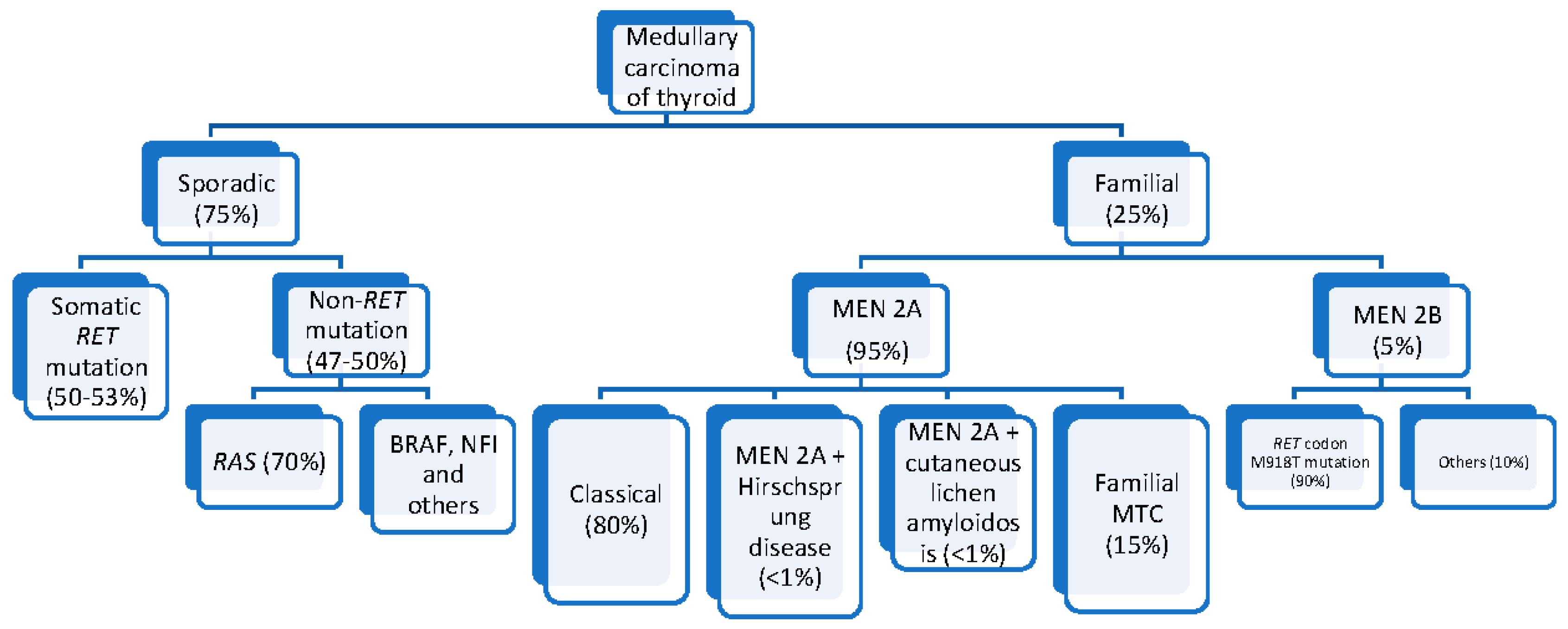
Figure 2.
Categories of artificial intelligence arranged according to their complexities.
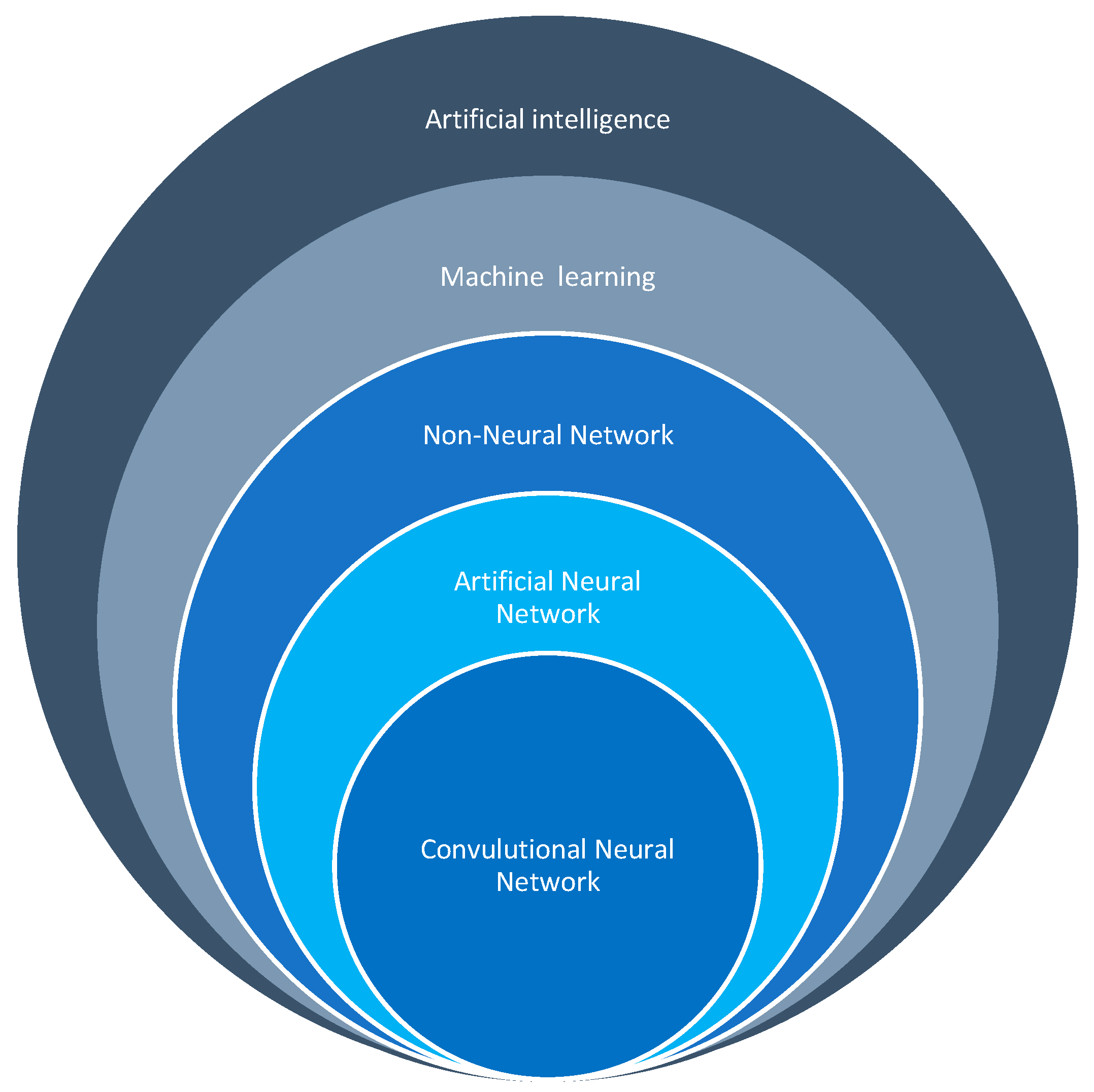
Table 1.
Artificial intelligence options for processing and integrative analysis of tumours.
| Algorithm | Application | Function | Example |
|---|---|---|---|
| Convolutional neural network [125,126] | Image analysis (ultrasound, CT, MRI) | Automatically identify features indicative of MTC | Distinguish between benign and malignant thyroid nodules with high accuracy |
| Support vector machine (SVM) [127] | Classification of thyroid lesions | Find the optimal hyperplane that separates different classes of data points | Classify MTC patients based on genetic mutations and protein expression profiles |
|
Random forest (RF) [128] |
Classification and regression | Build multiple decision trees and merge them to improve predictive accuracy | Predict patient outcomes and treatment responses based on clinical, genetic, and proteomic data |
| K-nearest Neighbours (KNN) regression [129] | Classification and regression | Classify a data point based on the classification of its neighbors | Classify thyroid nodules based on ultrasound features to determine likelihood of malignancy |
| ANN [130] | Complex pattern recognition | Process data in layers to learn intricate patterns | Integrate multi-omics data to predict disease progression and patient survival |
| Gradient bosting model (GBM) [131] | Classification and regression | Build models sequentially, each correcting errors of the previous ones | Predict recurrence risk in MTC patients by analyzing clinical and molecular data |
| Recurrent neural network (RNN) [130] | Time-series prediction and sequential data analysis | Maintain a memory of previous inputs to predict future outcomes | Analyze longitudinal patient data to predict future disease progression and treatment outcomes |
| Autoencoders [132] | Data dimensionality reduction and feature extraction | Compress data into a lower-dimensional representation and reconstruct it back | Identify key features in genetic and proteomic data that are most indicative of MTC |
|
Bayesian Networks [130] |
Probabilistic inference and decision-making | Represent variables and their conditional dependencies through directed acyclic graphs | Model relationships between genetic mutations, environmental factors, and MTC development |
| Natural language processing (NLP) [133] | Process and analyze unstructured clinical texts | Extract relevant information from EHRs, pathology reports, and scientific literature | Extract patient data and clinical outcomes related to MTC, integrating with omics data for comprehensive analysis |
| Geolocation [134] | Epidemiology and public health planning | Mapping the geographical distribution of MTC cases to identify environmental and genetic risk factors; planning targeted screening programs and resource allocation | Identifying regions with higher incidence rates of MTC to implement targeted screening programs and allocate resources effectively; correlating regional dietary habits and environmental exposures with MTC incidence |
| Survival Analysis [135] | Prognostic predictions and patient stratification | Estimating time until events (disease progression, recurrence, death) and identifying prognostic factors | Developing risk stratification models based on clinical, genetic, and demographic variables to predict patient outcomes and tailor follow-up and monitoring strategies |
|
Lean Six Sigma [136] |
Process optimization and efficiency in clinical workflows | Streamlining clinical processes, reducing diagnostic errors, and improving treatment workflows by eliminating inefficiencies | Standardizing procedures for sample collection and data integration to reduce variability and improve the reliability of holomic analyses; ensuring consistent follow-through on diagnostic and treatment protocols |
Table 2.
Change in miRNA expression in medullary carcinoma and the implications.
| Name of miRNA | Expression | Consequences | References |
|---|---|---|---|
| miR-375 | Overexpressed | Diagnosis, Lateral lymph nodes predicted, worse prognosis. Distinguishing hereditary from sporadic MTC. |
[30,149,150] |
| miR-127 | Underexpressed | Aggressive sporadic disease. | [149,151] |
| miR-429 | Overexpressed | Not yet specified | [149] |
| miR-592 | Overexpressed | Poor prognosis. | [106] |
| miR-224 | Underexpressed | Poor prognosis | [30] |
| miR-199-5p | Underexpressed | Not yet specified | [149] |
| miR-199a-3p | Underexpressed | Not yet specified | [149] |
| miR-34a | Underexpressed | Biomarker of MTC | [152] |
| miR-9 | Underexpressed | Distinguishing hereditary versus sporadic | [153] |
| miR-21 | Overexpressed | Prediction of lymph node and distant metastasis | [30] |
| miR-144 | Overexpressed | Biomarker of MTC | [152] |
| miR—183 | Overexpressed | Prediction of lateral lymph nodes involvement, distant metastasis and high mortality, and distinguishing hereditary from sporadic MTC. | [30,153] |
Table 3.
Summary of potential applications of AI in patients with MTC.
| Application | Description | Examples/Impact |
|---|---|---|
| Enhanced diagnostic accuracy [162] | AI improves diagnostic accuracy for MTC by analyzing imaging data, integrating multiple data sources including imaging, genetic and clinical, and identifying subtle features indicative of MTC. Traditional methods like ultrasound and fine-needle aspiration can be inconclusive. | AI-powered image recognition systems distinguish between benign and malignant thyroid nodules more accurately than human radiologists, leading to early and accurate diagnosis essential for effective treatment of MTC. |
| Personalized treatment plans [163] | AI personalizes treatment plans by analysing genetic and molecular data to identify specific mutations and biomarkers associated with MTC. It predicts patient responses to targeted therapies, optimizing treatment efficacy and minimizing side effects. AI updates treatment recommendations as new data become available. | AI guides the selection of targeted therapies such as tyrosine kinase inhibitors, ensuring that patients with MTC receive the most current and effective treatments based on their unique genetic profile. |
| Prognostic predictions [164] | AI develops predictive models to estimate disease progression and patient outcomes by integrating diverse data points like stage of cancer, genetic mutations and patient’s characteristics. Machine learning algorithms analyze historical patient data to identify patterns and risk factors associated with recurrence or metastasis. | AI helps clinicians stratify patients into different risk categories and tailor follow-up and monitoring strategies, providing more accurate prognostic information and improving long-term management of MTC. |
| Holomic integration [165] | Holomics integrates various omics data to provide a holistic view of MTC at the molecular level. AI analyze and interprets complex datasets to identify gene expression patterns, detect protein biomarkers, and analyze metabolic profiles, offering a more complete understanding of the disease. | AI-enabled holomics uncovers novel insights into MTC pathogenesis and identifies new therapeutic targets, leading to better diagnostic and therapeutic strategies. |
| Comparative insights in HICs versus LMICs [166] | AI application varies between high-income countries (HICs) and low- and middle-income countries (LMICs). HICs benefit from advanced healthcare infrastructure and cutting-edge technologies, while LMICs face challenges like limited resources and insufficient training. AI can bridge these gaps by deploying diagnostic tools via mobile health platforms and optimizing resource use. | AI-driven diagnostic tools enable remote diagnosis and expert consultations in resource-limited settings, making high-quality cancer care more accessible and efficient. This reduces disparities between HICs and LMICs in MTC management. |
| Future prospects [167] | The future of AI in MTC investigation is promising with continued advancements in AI algorithms and the growing availability of comprehensive holomic datasets. Collaborative efforts between researchers, clinicians, and AI experts will develop and validate tailored AI tools. The development of interpretable AI models will be crucial for clinical acceptance. | Expanding AI applications to other areas of thyroid cancer research, such as risk stratification and the discovery of novel therapeutic targets, holds great potential for improving patient outcomes. AI will play an increasingly integral role in the investigation and management of MTC, transforming the landscape of thyroid cancer care. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



