
Submitted:
02 September 2024
Posted:
03 September 2024
You are already at the latest version
Abstract
Vitamin D and iron deficiencies are the most prevalent micronutrient deficiencies among women of reproductive age (WRA) in Morocco. Recent studies suggest that Vitamin D deficiency (VDD) may reduce iron bioavailability necessary for erythropoiesis, potentially leading to iron deficiency (ID) and anemia. This study investigates the association between vitamin D status, iron levels, and anemia risk among Moroccan WRA aged 18-49 years. A cross-sectional study was conducted with 463 participants. Serum levels of 25(OH)D, blood count parameters, iron, ferritin, C-reactive protein, and creatinine were measured. Lifestyle factors, including dietary intake, sun exposure, and physical activity, were evaluated using validated questionnaires, and anthropometric data were collected. Linear and logistic regression models assessed the relationships between variables, while Receiver Operating Characteristic (ROC) curve analysis evaluated the predictive accuracy of VDD for ID and anemia. VDD (25(OH)D < 20 ng/ml) was significantly associated with lower levels of hemoglobin, hematocrit, red blood cells, and ferritin (all p < 0.01), suggesting a role of vitamin D in erythropoiesis and iron storage. Multivariate logistic regression showed that VDD increased the risk of anemia (OR: 7.17, 95% CI: 3.19-19.28, p < 0.001), ID (OR: 2.20, 95% CI: 1.32-3.77, p = 0.007), and IDA (OR: 4.10, 95% CI: 1.73-12.08, p = 0.004). Dietary iron intake was inadequate among all participants, with minimal protective effect against anemia and ID (β(SE): -0.08(0.03), p = 0.030 and β(SE): -0.05(0.02), p=0.037 respectively). ROC analysis demonstrated moderate discriminative power for VDD in diagnosing IDA and anemia (AUC: 0.643 and 0.603) but reduced accuracy for ID (AUC: 0.575). This study identifies VDD as a significant risk factor for impaired iron status and anemia among Moroccan WRA, underscoring the need for targeted nutritional interventions and further research to explore effective prevention strategies.
Keywords:
Vitamin D
; Vitamin D deficiency
; iron deficiency
; iron deficiency anemia
; anemia
; erythropoiesis
; dietary intake
; women of reproductive age
1. Introduction
VDD and anemia continue to affect millions of women worldwide, predominantly in low-and middle-income countries [1,2] resulting in impaired economic productivity [1,3], increased morbidity and all-cause mortality [4,5], and risk of adverse outcomes for mothers and newborns [6,7].
Anemia occurs when red blood cells and hemoglobin levels are too low to meet the body's oxygen needs [8,9]. It’s commonly measured in terms of blood hemoglobin content, as hemoglobin is the primary oxygen-carrying molecule within red blood cells [9]. The etiology of anemia is multifactorial caused by nutritional factors (e.g., iron, vitamins A and B12, folate, and riboflavin), genetic conditions (including sickle cell disease and thalassemia, an inherited blood disorder), or inflammation as an outcome of infectious and chronic diseases [10]. ID is the primary common cause accounting for 50% of all anemia cases among women in developed countries [9]. WRA are at particularly increased risk of ID due to physiological changes and increase nutrients requirement during pregnancy or growth periods [9]. Despite its known causes and effective treatments (e.g., eating iron-rich foods and taking iron supplements) [10], the global prevalence of anemia in WRA has remained stagnant since 2000, effecting nearly one-third of the non-pregnant WRA (15-49 years) worldwide [9]. The WHO established a Global Nutrition Target to reduce anemia in WRA by 50% by 2025, which was later extended to 2030 [9].
VDD is a global pandemic that affect one billion of the world’s population independent of age, sex, ethnicity and geographic location [11,12] Humans rely on two major sources to meet their biological requirements for vitamin D; the endogenous synthesis is initiated through photochemical and thermal conversion in skin from the cholesterol precursor 7-dehydrocholesterol in the presence of adequate solar ultraviolet B irradiation [13,14]. To a lesser extent, vitamin D can be obtained by exogenous intake from dietary sources [13,14]. VDD is defined by a serum level of 25-hydroxyvitamin D (25(OH)D) below 20 ng/mL (50 nmol/L) [12].Vitamin D functions in the human body as a fat-soluble vitamin and a prohormone nutrient with pleiotropic effects [15]. It’s essential for bone health and the metabolism of calcium and phosphate and shows substantial involvement in many gene expression pathways [16]. Vitamin D action’s through a single vitamin D receptor (VDR), which also has been identified in the ovaries and the endometrium among other human female reproductive tissues [17,18].
Likewise, vitamin D has gained attention for its potential associations with anemia and iron status. Several speculations of the biological mechanism are highlighted in studies. VDR have been discovered in the bone marrow at 100 folds higher concentration than in plasma [19], which suggested a direct effect of vitamin D on reducing anemia by stimulating erythroid precursors [20,21]. Bacchetta et al, reported a direct effect of vitamin D on downregulating hepcidin expression as they identified a VDR binding site on human hepcidin promoter [22]. Hepcidin is the hormone that regulates systemic iron homeostasis. It inhibits and ultimately degrades ferroprotein, the transmembrane protein that transports iron, and therefore controls the amount of iron absorbed in the intestine and released from cellular storage [22,23]. Moreover, vitamin D is acting indirectly on hepcidin by reducing pro- inflammatory cytokine (IL6 and IL1β) [22,24]. This latter increase hepcidin level, resulting in limited iron availability to invasive microbe [23]. Nevertheless, it also causes a decrease in hemoglobin concentrations [23]. This anti-inflammatory effect of vitamin D, is more elucidated for anemia of inflammation [25]. More recently, an animal based study, suggested that vitamin D intake have protective effect on iron metabolism trough the regulation of expression of divalent metal transporter 1(DMT1) [26], a protein that play a key role in transporting iron across the intestinal mucosa and its homeostasis [27]. As VDR have been already found highly expressed in the human intestines [28], further research may combine current evidences to extend the role of vitamin dietary intake in iron absorption.
Several observational and trials studies supported the association between low 25(OH)D concentration and disturbance in iron status and hemoglobin concentrations in different age group and population [5,29,30,31,32,33,34,35,36]. Trials results showed that vitamin D intake increase hemoglobin, erythrocyte and iron levels [37] and improvement in vitamin D status to be >20ng/ml; is positively correlated to transferrin saturation (a marker of iron supply to tissues) in women, [32]. An increase of vitamin D concentration after intramuscular iron treatment in infants was also observed in other investigation [38]. This suggested a reciprocal interplay between vitamin D and iron [35,36] that may be beneficial in both VDD and iron deficiency recovery.
Morocco is characterized by abundant sunlight throughout the year, which theoretically would mean that its population has adequate vitamin D levels. The country, has prioritized primary prevention efforts by implementing basic food fortification in vitamin D and iron to combat nutrients deficiencies [39,40]. In addition, systemic vitamin D supplementation programs primarily target children at birth and 6 months thereafter, aiming to reduce the prevalence of nutritional rickets [39]. Pregnant WRA receive iron, and vitamin D2 supplementation to decrease the incidence of maternal anemia and adverse birth outcomes [41]. Nonetheless despite these efforts, both nutrient deficiencies remain a health challenge. A high prevalence of VDD (73% in 2019) is registered in WRA [40] and the rate of anemia in WRA have increased from 32.9% in 2006 to 34.4% in 2019 with 49.7% of IDA [40]. Simultaneously, a significant prevalence of overweight and obesity coexists with micronutrient deficiencies, characterizing a national nutritional transition and triggering a double burden of malnutrition [40].
Therefore, this paper endeavors to address the current knowledge gap in Morocco by delving into the complex relationships between vitamin D levels, iron status, and anemia, with a specific focus on WRA. The effect of the lifestyle factors including dietary intake was also examined. Ultimately, elucidating whether vitamin D status can be considered a modifiable risk factor for ID or anemia will provide valuable insights for crafting more efficient preventative nutritional recommendations and guiding targeted intervention strategies.
2. Materials and Methods
2.1. Study Design and Population
This was a cross-sectional study involving WRA from the Meknes prefecture (Morocco) who presented for vitamin D blood analysis, prescribed by a clinician in a private medical clinics and certified laboratory that participated in the study. Enrolment was conducted between February and December 2022.
The sample size was obtained by the Cochran's formula n =Z2 pq/e2 [42], Where: Z is the standard normal variate at a confidence interval of 95% = 1.96 and p is the prevalence of vitamin D deficiency (25(OH)D< 20ng/ml) =78.8%, which was stated in the National Nutrition Survey (ENN 2019) [40], q is 1-p, and e is the margin of error = 0.05. Hence, the minimum number of 256 participants was required to obtain statistically representative data. To increase statistical power and considering completion of response, a total of 533 women participants were recruited for the study of which 463 consented to conclude assessments with the research team and were eligible for our inclusion criteria (Figure 1).
Women were eligible if they were aged 18 to 49 years; apparently healthy and were able to provide consent to participate in the study. Women were excluded if they reported any significant medical conditions that affect hemoglobin, iron or 25 (OH)D serum concentrations such as abnormal renal/liver function; peptic or duodenal ulcer or metabolic, cardiac, malignancy diseases autoimmune and thyroid disease, as well as disorders which cause gastrointestinal bleeding, helminthic infections or malabsorption syndromes [10,43,44,45]. Further we excluded pregnant women, women treated for abnormal uterine bleeding in particular heavy menstrual bleeding [46] and any women involved in loss weight programs, diet restriction, or under medication known to interfere with vitamin D metabolism [47]. Regular blood donors [48] that had donated blood within the previous three months, women reporting taking iron supplements, vitamin D3 supplement use in the past six months or multiple micronutrient supplements, or those with known iron deficiency or anemia were also excluded.
The ethics committee of biomedical research at Moulay Ismail University (reference; N°1/CERB-UMI/19) approved the study protocol, and all investigations were conducted under the principles of the Declaration of Helsinki. All participants signed written informed consent.
2.2. Measurements
2.2.1. Socio-Demographic Information
The socio-demographic covariates were collected by face-to-face questionnaire and included age, education level (Illiterate, ≤10years(secondary-college); ≥11years(university or higher)), marital status(Married-Unmarried),employment(employed-unemployed), and geographic localization (Urban, Rural).
2.2.3. Anthropometric Measurements
Anthropometric measurements were performed with standard procedures, while participants were minimally clothed and without shoes. The weight in kilograms was measured with a digital scale (SECA®), with a precision of 0.5Kg. Height was measured with a portable stadiometer (SECA 214) to the nearest 0.1 cm. Body Mass Index (BMI) was calculated as weight in kilograms divided by height in meters squared and expressed in Kg/m2. Anthropometric status was categorized using classification according to BMI as follows: Underweight: BMI<18.5kg/m², Normal: BMI: 18.5-24.9 kg/m², Overweight: BMI 25-29.9 kg/m², and obese ≥30 kg/m² [49].
2.2.3. Lifestyle Factors
Nutrient Intakes Estimate
Vitamin D3 dietary intakes were assessed using our self-administered and validated Vitamin D-FFQ in Moroccan WRA [50]. Briefly, the VD-FFQ include 78 items pertaining the richest vitamin D3 food consumed in the Moroccan context. Criterion validity of the FFQ showed a high validity coefficient against seven days estimated record ρQR =0.90 (95%CI: 0.89-0.92) [50]. Iron daily intake was estimated through 24-hour dietary recall. All women were asked by certified dietitian to recall all the foods and beverages consumed in the day before. Photograph aids of typical Moroccan household measurements were used to assist the participant [51]. To estimate daily nutrient (vitamin D3 and iron) intakes from diet, frequency and serving size for each food consumed were multiplied by the nutrient content of that food using the French CIQUAl food composition database [52] and the Nutrient Database for Dietary Studies 2015-2016 of the United States Department of Agriculture National Food (USDA) when values were missing in the French database [53].
Iron status is more dependent on the type of dietary iron (heminic and non heminic) than on overall intake. Because of certain hemoglobin transporters [44], heminic iron is absorbed more efficiently whereas non heminic iron, needs iron reduction prior to absorption [44]. In our estimate, the content of Heme-iron was calculated based on a commonly applied assumption that heme iron is attributed to 40% of iron derived from animal products including red meat, poultry, fish, and animal organs, and non-heme iron was calculated as the remaining portion of the total iron from all foods [54,55]. Energy intakes in Kcal/day were calculated from all participants 24H recall and nutrients estimates were adjusted for using the residual method [56]. The WHO/FAO recommended daily intakes were applied to ascertain intakes adequacy of vitamin D3 and iron [57].
Sun Exposure Behaviors
Participants' self-reported sun exposure over the previous month was assessed using our validated sun exposure score questionnaire, previously described [50,58]. Three domains relating sun exposure behaviors were reported and scored (on scale of 0 to 4);( indoor sun exposure, outdoor sun exposure, including work or routine activities, recreation or leisure activities, and sun protection practices) and then were adjusted for the participants Fitzpatrick’s skin type and the strength of UVB rays in the outside weather conditions. The estimated total sun exposure score (SES) served to categorize participant exposure levels from 0 to 30. The sun exposure level was considered as insufficient if SES < 17, moderate if SES =7.5 to 15, sufficient if SES = 15 to 30 and very sufficient or high if the score is> 30 [50,58].
Physical Activity Assessment
To assess physical activity (PA) levels, we used the short version of the International PA Questionnaire (IPAQ-SF)1 which is commonly applied in studies among adults aged 18–69 years [59,60] Participants had to reported their activities during the previous week, including walking (any type of walking), moderate activities (carrying light loads, gardening, doubles tennis, and cycling at a steady pace), and vigorous activities (carrying heavy loads, aerobics, weight training, fast cycling, or jogging at 10 km/h) [60]. Each activity (walking, moderate, and vigorous activities) converted in minutes per week were multiplied by metabolic equivalent (METs) factors as follow: (daily minutes of walking x days per week with walking x 3.3METs) + (daily minutes of moderate-intensity activity x days per week with moderate-intensity activity x 4 METs) + (daily minutes of vigorous activity x days per week with vigorous activity x 8 METs) . Score was categorized to low intensity (< 600 MET min/week), moderate PA (at least 600 MET-min/week), and Intense/vigorous PA (at least 3000 MET-min/week) [59].
Laboratory Assessment
Fasting venous blood of 10 ml were collected from each women participant and analyze on the day. Serum 25(OH) D and concentrations were performed with one-step electrochemiluminescence immunoassay according to the manufacturer’s instructions. All chemical analysis was carried out using the Abbott Architect ci4100 Chemistry Analyzer COBAS E411 analyzer. Blood count (BC) analysis was performed using automates (BC-5380). Unless otherwise specified, we use laboratory references to express the proportion of each biomarker's category concentration (low or high).
Biomarkers Cut-Off Points Definition
Anemia and severity of anemia was defined according to the WHO criteria for anemia: Hb level <12 g/dl, for The severity of anemia; Mild anemia: HB: 11-11.9; moderate anemia: HB: 11-8-10.9 severe anemia HB <8g/dl [8]. The standard for establishing iron deficiency is a bone marrow aspiration or biopsy followed by iron staining since it is unaffected by inflammation. However, the cost and invasiveness of this test make it less feasible; it is rarely performed for this reason [61] Ferritin concentration is an accurate marker of iron stores in populations and required to diagnose iron deficiency in healthy people [10,62]. However, inflammation is known to raise SF levels, which may lead to an overestimation of iron reserves and the misclassification of individuals as iron replete. Therefore, the diagnostic criteria for ID were serum ferritin concentration <15 μg/L; a threshold indicative of depleted bone marrow iron stores and absence of elevated concentrations of CRP: CRP<5mg/ml. IDA was diagnosed by the criteria for iron deficiency in addition to lower and haemoglobin less than 12 g/dl [8,10,62].
VDD was defined as serum 25(OH)D levels <20 ng/mL [12,63,64], a threshold associated with the prevention of impaired intestinal calcium absorption and for maintaining skeletal and overall health, [64,65]. Severe VDD was defined as 25(OH)D <12 ng/mL) [41,42,43], whereas vitamin D insufficiency was defined as levels between 20 and 30 ng/mL [12,64]. Women with serum 25(OH)D >30ng/mL concentrations were considered to have sufficient levels [12,64].
Statistical Analysis
Normality of the continuous data was evaluated using Kolmogorov-Smirnov and Shapiro wilk tests (n>50) respectively. All variables were not normally distributed therefore only nonparametric tests were applied. Descriptive analysis was performed, and data were expressed as median with interquartile range (IQR) for continuous variables and in frequencies and percentages for categorical variables.
Participants were classified into sub-groups according to vitamin D and anemia status. Kruskal-Wallis tests were used to compare groups of hypothesized risk factors (independent variables) according to vitamin D or anemia status sub-groups while e chi-squared or fisher’s exact test were used to measure the difference in frequency for categorical variables.
Pearson correlation coefficient and linear regression analysis were used to evaluate the relationship between continuous variables (25(OH)D and iron/anemia markers which were log-transformed for scatter plots and regression analyses.
To investigate the associations between VDD, ID, IDA and all cause anemia, we utilized a combination of logistic regression, and receiver Operating Characteristic (ROC) curve analysis.
Logistic Regression
Logistic regression models were employed to estimate the odds ratios (OR) and corresponding 95% confidence intervals (CI) for the associations between VDD and the outcomes of ID, IDA, and anemia. To ensure the accuracy of the logistic regression models, the collinearity between potential predictors was checked using the Variance Inflation Factor (VIF), with a threshold of VIF < 10 indicating acceptable collinearity [67]. Stepwise regression analysis was then applied to select significant predictors of the outcomes to be included in the multivariate models. The best model was retained based on the Akaike Information Criterion (AIC), ensuring the most parsimonious model with the best fit. The significance of the predictors was assessed using the z-values and p-values [67].
To assess the discriminative power of VDD the logistic models, ROC curve analysis was conducted [68]. The ROC curves for both the full model and the VDD-specific model were generated, providing visual representations of the sensitivity and specificity of the models. The area under the curve (AUC) was calculated to quantify the overall accuracy of the models in distinguishing between anemia, IDA, ID cases and non-cases. Commonly used values for AUC interpretation are: 0.90-1.00: Excellent, 0.80-0.89: Good, 0.70-0.79: Fair, 0.60-0.69: Poor and 0.50-0.59. A sensitivity and specificity above 0.70 regarded as acceptable [68].
All statistical analyses were performed in R version 3.4.2 (2017-09-28). A p-value of <0.05 was considered significant for this study.
3. Results
Baseline characteristics of the study participants overall and by anemia status are presented in Table 1. Anemia was present in 23.3% of women participant 76.6% were healthy. There was no statistically significant difference in terms of most sociodemographic between the healthy and anemic groups. However, urban women exhibited a significant higher prevalence of anemia (55.6%) compared to their rural counterparts (44.4%) (p=0.025).
The median BMI indicated a higher prevalence of overweight and obesity among our study participants, with 61.3% falling into this category (38.0% overweight and 23.3% obese). Anemia was associated with a higher median (IQR) BMI (p=0.001) and showed a significantly higher prevalence rate (72.2%, p=0.024) in the overweight and obese groups (39.8% and 32.4% respectively).
The PAC score median (IQR) was determined to be 1647 MET-min/week. Among the women participants, 80.7% exhibited a moderate activity level, 11.5% had a low PAC level, and 7.8% had a high PAC level. Lower median(IQR) PAC level was observed in anemic group (p<0.0001).
Regarding dietary intakes, our results showed that most women 81.2% and 100% reported inadequate intake of vitamin D and iron falling below the recommended values established by WHO and FAO. The anemic group displayed a significant lower intake in vitamin D intake compared to the healthy group (p=0.035). Non-Heme iron consumption was moreover higher in the healthy participant (p=0.012). Further, more than half of our participant (53.3%) reported an insufficient to moderat sun exposure scores with the highest proportion (55.6%) observed in the anemic women (p=0.034).
Data on biochemical parameters according to participant’s 25(OH)D(ng/ml) cut-off points are described in Table 2. The median (IQR) 25(OH)D level for the overall study population was 14.4(10.8)ng/ml within 463 women participants included in our analysis. VDD (25(OH)D3<20ng/ml) showed the highest rate with 72.1%, of which approximately one third (29.7%) having a severe VDD (25(OH)D<12ng/ml). Vitamin D insufficiency affected 17.1%( 20ng/ml ≤ 25(OH) D3<29.9ng/ml) whereas only 10.2% of our participant had sufficient 25(OH) D3 level ≥30ng/ml.
A pattern of significant increase from the deficiency to insufficiency rang was observed in almost all blood count markers, including hemoglobin (p<0.001), erythrocytes (p=0.005), hematocrit(p<0.001),MCV(p<0.001),MCH(p<0.001), and MCHC (p<0.001).WBC count seems to be inversely correlated with serum 25(OH)D concentration, as higher counts were observed in the VDD range, but this was not statistically significant (p=0.643).
Higher ferritin concentrations were observed in participants with sufficient levels of vitamin D, showing an increasing trend (p=0.002). However, the distribution of iron concentration levels did not differ significantly across vitamin D status ranges (p=0.604). Related to renal function parameters, none of our participant had a chronic kidney disease as the computed rate of eGFR<60 ml/min/1.73 m2 was site to 0. However, participants eGFR (ml/min/1.73 m2) exhibits a substantial increase(p=0.045) as the 25(OH)D levels rise while plasma creatinine remains stable. When considering the presence of inflammation (defined by CRP >5), 21.8% of all participants had an inflammation, with no significant difference in this proportion across 25(OH)D levels.
As illustrated in Figure 2, all blood count parameters, including hemoglobin, hematocrit, erythrocytes (red blood cells), MCV, MCH, and MCHC, were positively related to circulating 25(OH)D, except for white blood count, which showed no significant association with vitamin D levels. Additionally, a significant association was found between 25(OH)D and ferritin, whereas iron concentration was not related to 25(OH)D concentration. The magnitude of these relationships was weak for all indices (all r: 0.10-0.39, p<0.05) [69].
Table 3 presents a detailed distribution of anemia and iron status according to the levels of 25 (OH)D3 serum concentrations in the study participants.
The distribution of anemia varied significantly across different 25(OH)D levels (p<0.001). The highest prevalence of anemia (93.5%) was observed in participants with 25(OH)D levels indicative of VDD (25(OH)D < 20 ng/ml), compared to a proportion of 65.6% in the non-anemic women. However, anemia severity distribution was not statistically different across participants’ vitamin D status.
In addition, of the study participants, 27.6% were found to have ID. The majority (82.6%) of these women fell within the VDD range. The variations in ID rates across different 25(OH)D statuses were statistically significant (p=0.001). The rate of IDA within the anemic group was 50% (54 out of 108), while among all women participants, 11.7% (54 of 463) presented IDA. Of these, a significant proportion (90.7%) exhibited concurrent VDD (p=0.003), compared to a proportion of 69.7% in the non-anemic group (p=0.003).
The logistic regression analysis results, as presented in Table 4, indicate a significant association between VDD and anemia. Women with VDD had an odds ratio (OR) of 8.79 (95% CI: 4.06, 23.00; p<0.001) for anemia, suggesting a substantially higher likelihood of developing anemia compared to those with insufficient or sufficient vitamin D levels. After adjusting for potential confounders, the OR for the association between VDD and anemia was slightly reduced to 7.17 (95% CI: 3.19, 19.28) but remained highly significant (p<0.001).
Similar trends were observed regarding the impact of VDD on iron status. Women with VDD were found to be twice as likely to present with ID and over four times more likely to have IDA compared to those without VDD. The unadjusted OR for ID was 2.12 (95% CI: 1.28, 3.50; p=0.003), which, after adjustment for confounders, slightly increased to 2.20 (95% CI: 1.32, 3.77; p=0.007). For IDA, the unadjusted OR was 4.16 (95% CI: 1.62, 10.71; p=0.003), and the adjusted OR was 4.10 (95% CI: 1.73, 12.08; p=0.004).
Summary of ROC analysis results are presented in Table 5 and Figure 3. The AUC for VDD predicting general anemia and specific IDA were 0.643 (p < 0.001) and 0.603 (p < 0.001), respectively, indicating moderate discriminant ability. Higher sensitivity values in identifying cases were observed (0.944 for anemia and 0.833 for IDA), with Youden indexes indicating a moderate balance between sensitivity and specificity for VDD in predicting anemia and IDA (0.285 and 0.206, respectively).
The inclusion of covariates in the model, such as ID, geographic localization, dietary iron intake, sun exposure and physical activity level likely contributed to the higher accuracy and predictive power for anemia (AUC: 0.813 (95% CI: 0.768 - 0.855), p< 0.001, optimal sensitivity: 0.722, optimal specificity: 0.806, and Youden Index: 0.528).
Similar, the adjustment for covariates contributed to the balanced sensitivity and specificity and more moderate discrimination ability of VDD in predicting IDA ( AUC: 0.712 (95% CI: 0.643 - 0.776), p < 0.001, optimal sensitivity: 0.741, optimal specificity: 0.648, and Youden Index: 0.389).
Nevertheless, the accuracy of VDD in predicting ID appears low, with an AUC of 0.575 (p < 0.001), although moderate sensitivity was observed (0.833). Accounting for participants demographic characteristics including age and education level in addition to dietary intake of non heminic iron improved the accuracy of VDD to detect anemia cases with an acceptable AUC around of 0.654, specificity of 0.634 and sensitivity of 0.648.
4. Discussion
Vitamin D and iron deficiencies, and the resulting anemia, remain widespread among Moroccan WRA, despite existing health management efforts. This cross-sectional study examined, the interplay between VDD, iron status, and anemia in 463 WRA aged 18-49 from Meknes, Morocco.
The prevalence of anemia in our study (23.3%) was lower than the national rate of 34.4% [40]. This discrepancy may stem from variations in sampling methodologies, inclusion criteria, and analytical techniques used to measure hemoglobin, such as the use of Haemoglobinometer in the national nutritional survey (2019-2020).However, the prevalence rates of ID and IDA aligned with the national report [40], highlighting ongoing challenges in addressing nutritional deficiencies among premenopausal women.
We observed a high prevalence of VDD (72.1%), with approximately one-third of participants experiencing severe VDD (25(OH)D < 12 ng/mL). These findings align with national rates for VDD and severe VDD [40]. Beyond the skeletal system [41,42,43], these deficiencies may have broader health implications on our participant, potentially affecting conditions such as infertility [70], cardiovascular diseases [71],Covid-19 [72], and even breast cancer [73,74].
Regarding the impact on iron metabolism, numerous studies have investigated the relationship between VDD and poor iron status or anemia; however, the findings have been inconsistent [29,31,32,33,34,35,75,76,77] suggesting a complex interaction between vitamin D and iron. Calcitriol, the active form of vitamin D, may directly enhance erythropoiesis by stimulating erythroid progenitor cells in conjunction with erythropoietin (EPO) [21]. This mechanism could reduce dependence on erythropoiesis-stimulating agents, and decreases the amount of EPO needed to maintain optimal hemoglobin levels, as observed in conditions like kidney disease [20] and pregnancy [78]. Additionally, higher levels of vitamin D in the bone marrow, compared to serum [19], underscore its role in supporting hematopoiesis.
The suppression of hepcidin, a key hormone in iron regulation secreted by the liver, is one proposed mechanism by which vitamin D may influence iron metabolism [23]. Hepcidin controls iron release from macrophages and intestinal cells, and its expression can be downregulated through various pathways, including the direct interaction of active vitamin D (1α,25(OH)2D3) with the vitamin D receptor on the HAMP promoter gene, reducing HAMP mRNA expression [24,79]. Additionally, vitamin D has anti-inflammatory properties that can suppress pro-inflammatory cytokines, which are known to increase hepcidin production [24,79]. This dual action—direct and anti-inflammatory—suggests that vitamin D could potentially enhance iron availability for erythropoiesis and hemoglobin synthesis. However, the exact contribution of these pathways remains a topic of debate, as some studies have failed to observe a significant impact of vitamin D on hepcidin levels [80], indicating the need for further research to confirm these mechanisms in different populations and disease states.
Our analysis revealed significant, albeit weak, correlations between vitamin D levels and key biomarkers of anemia, such as hemoglobin, RBC, and hematocrit, as well as morphological indices of RBC like MCV, MCH, and MCHC (all r: 0.10-0.39, p < 0.05). This weak correlation could be attributed to the low vitamin D concentrations observed in our participants (median (IQR): 14.4 (10.8) ng/mL). However, there was a consistent pattern of increasing marker concentrations as vitamin D levels rose from deficiency to insufficiency ranges. This finding aligns with the results from a large cohort study conducted by Zhang et al., which involved a US adult population (n = 29,933, with 50.5% women). The study found that increases in RBC count and hemoglobin levels were correlated with higher serum 25(OH)D levels, specifically within the insufficiency range of 23.8-28.1 ng/mL (59.7–70.3 nmol/L) in addition to a reduced incidence of anemia [81].
Our study’s results also resonate with prior research among both healthy and patient populations of premenopausal women [29,34,76,77,82,83]. Particularly, the study by Seong et al, in a national representative survey involving 16,060 Korean adults, where severe VDD (<15.0 ng/mL) was significantly associated with lower hemoglobin, hematocrit, iron, and ferritin concentrations in premenopausal women. The risk of anemia in these women was significantly higher (OR=1.293, 95% CI: 1.105-1.513, p<0.001) [77]. At the same citing, previously, reported VDD prevalence at 94.9% in premenopausal women with an odds ratio for anemia in the lowest vitamin D quartile Q4 (≤ 11.92 ng/ml) significant at OR: 1.821 (1.240, 2.673); p = 0.009 [76]. Likewise, meta-analysis by Liu et al of five studies involving adult participant, that conclude that VDD was associated with an increased incidence of anemia in both gender (OR = 2.33; 95% CI = 1.43–3.80) [31]. In our study, VDD was more prevalent among anemic women (93.5%) compared to non-anemic women (65.6%), with the deficient group being over seven times more likely to develop anemia (adjusted OR: 7.17; 95% CI: 3.19-19.28; p<0.001). These findings suggest that maintaining adequate vitamin D levels (≥20 ng/mL) could be beneficial for effective anemia management in Moroccan WRA.
However, it is important to note the conflicting results from other studies. For instance, studies among WRA by Soepnel et al. [34] and Anya Greenwood et al. [82] found no direct associations between vitamin D levels, hemoglobin, anemia, or iron status. Additionally, Smith et al. reported in US cohort of adult men and women, a correlation between low serum 25(OH)D levels and increased odds of anemia in Black individuals but not in Whites, particularly associating it with anemia of inflammation without impacting iron status [84]. Conversely, Malczewska-Lenczowska et al. observed that VDD (<30 ng/mL) was associated with both storage and transport iron pools such in lower ferritin levels, higher Total Iron-Binding Capacity (TIBC), and elevated soluble transferrin receptor (sTfR) levels, indicating a prevalent pattern of ID in athletic female (OR: 1.75, 95% CI: 1.02–2.99, p=0.040; OR: 4.6, 95% CI: 1.81–11.65, p=0.001) [29]. Similarly, Lavoie et al. (2024) found that 25(OH)D levels were positively associated with serum ferritin (β: 12, 95% CI: 0.01-0.22, p<0.05) and inversely associated with IDA (β: 0.57, 95% CI: 0.38-0.84, p<0.01), though no association with hemoglobin levels was observed in both referred studies [85].
These discrepancies suggest that the role of vitamin D in mitigating anemia may vary depending on geographic location, population demographics, and the specific type of anemia. It’s potentially cofounded by factors such as ethnicity [25,82,84], gender [76,77], baseline health conditions (e.g., body fat percentage, inflammatory states) [25,30,34,82,85]. Besides, methodological differences in studies, in particular the thresholds of biomarkers used to define VDD and ID, could contribute to the variability in findings.
Our study investigated the relationship between VDD and iron status while carefully excluding participants with chronic diseases or infections that might confound results due to inflammatory processes. We found that VDD coexisted with impaired iron status, with vitamin D deficient women facing twice the risk of iron deficiency (ID) (adjusted OR: 2.0, 95% CI: 1.20-3.32, p=0.007) and a fourfold increase in the risk of IDA (adjusted OR: 4.10, 95% CI: 1.73-12.08, p=0.004). Notably, there was a trend of rising ferritin levels toward the normal range as vitamin D status improved from deficient to sufficient (p=0.002).This result hinting at vitamin D’s potential role in enhancing iron storage and mobilization in the study participant.
In line with this, some evidence suggests enzymes like CYP11A1 known for its role in vitamin D metabolism may mediate these interactions, influencing both vitamin D metabolism and ferritin heavy chain [86]. Additionally, CYP11A1’s involvement in steroidogenesis, particularly in synthesizing hormones such as estrogen and testosterone, could impact iron metabolism by regulating hepatic hepcidin expression [87,88]. However, these mechanisms are still under investigation, and their relevance to the observed findings in premenopausal women warrants further exploration.
Regardless, it’s established that ferritin serves as a marker of iron stores in the body, and decreased ferritin level is primary indicators of ID and IDA [89]. Typically, inflammatory states can skew ferritin levels due to the acute phase response and lead to altered iron distribution through hepcidin upregulation. [90] Vitamin D may help normalize ferritin levels and improve iron availability by reducing inflammation.
Our study did not include direct measurements of hepcidin or pro-inflammatory cytokines, which are key mediators in the relationship between vitamin D and iron metabolism. This limits our ability to fully explore whether the observed associations between VDD and iron status are indeed mediated through traditional inflammatory pathways. While we observed no correlation between general inflammatory markers (e.g., WBC and CRP) and vitamin D or iron levels, this does not rule out more subtle or specific inflammatory mechanisms that could still play a role.
The ROC analysis showed that VDD had moderate discriminative power for diagnosing general anemia (AUC: 0.643) and IDA (AUC: 0.603), with high sensitivity but low specificity (Youden index: 0.285 for anemia, 0.206 for IDA). The low specificity indicates that while VDD is useful for identifying individuals at risk of anemia, it is not sufficient as a standalone diagnostic marker due to its inability to reliably distinguish between anemia types or other causes of poor iron status. This limitation is further evidenced by the particularly weak performance of VDD in predicting iron deficiency alone (AUC: 0.575, sensitivity: 0.833). Thus, for more accurate clinical assessment and intervention planning, VDD should be evaluated in conjunction with a comprehensive profile of other diagnostic markers and patient-specific factors, especially in WRA who are susceptible to multiple nutritional deficiencies.
The influence of dietary intake and lifestyle factors on vitamin D and iron status is evident in our study. Iron deficiency among young women, particularly in middle- and low-income countries like Morocco, often results from inadequate dietary intake, poor absorption, increased physiological needs, and significant losses due to menstruation and childbirth [43,91]. For example, menstruation alone can account for a monthly loss of 25% (1 mg iron/cycle) of the total body iron in healthy women while on average women with menorrhagia would losse five-to-six times higher than normal [92]. Pregnancy can lead to a net iron deficit much higher of 580-680 mg owing to the demands of the fetus and placenta, as well as delivery-associated blood loss [93]. To maintain iron homeostasis, dietary intake must not only meet daily needs but also replenish these significant losses [94]. Given these challenges, ensuring adequate intake of bioavailable iron, particularly heme iron from animal sources, which is absorbed more efficiently than non-heme iron from plant sources [94] is crucial at this vulnerable age. Nutritional guidelines recommend daily iron intakes of 14.8 to 18 mg for WRA [95]. However, the WHO suggests a higher intake of 58.8 mg/day for premenopausal women living developing countries, accounting for the low bioavailability of iron in their typical diets [57].
In other side, despite debates about vitamin D requirements and their broader health impacts, low vitamin D levels are a concern globally. In some populations living in high latitude, resulting in inadequate sun exposure, dietary intake and body stores help maintain adequate vitamin D levels, especially during winter [96]. Inadequate vitamin D intake has also been reported in women of childbearing age in some previous Moroccan studies [50,97].
Our study revealed poor nutrient intake and overall dietary quality among the participants. Iron intake across all participants was significantly below the recommended levels, and only 18.8% of participants met the recommended daily vitamin D intake of 5 µg/day. There was no association between participant vitamin D intake and VDD (β (SE): 0.099(0.26), p= 0.705) (data not shown).Yet, anemic women were consuming significantly less iron and vitamin D than their non-anemic counterparts (p=0.011 and p=0.031, respectively). Thus, the protective effect of dietary iron intake against anemia and IDA was minimal (β(SE): -0.05(0.02), p=0.041; β(SE): -0.08(0.03), p=0.030) and non heminic iron was negatively associated to ID (β(SE): -0.05(0.02), p=0.037).
The dietary habits of Moroccan WRA, which predominantly rely on legumes, vegetables, and cereals characterized by a high intake of non-heme iron and lower amount of vitamin D [98], likely explains the observed correlation with iron deficiency and contribute to the cumulative risk of anemia. Likewise,, the strong inhibitory effect of polyphenols in tea; a widely consumed beverage amounts Moroccan population [99] would greatly reduce the amount of iron absorption from the diet and the fortified staples mainly wheat flour, even in women with IDA, who are maximally upregulating their iron absorption [90]. Given these findings, effective dietary interventions for anemic women should focus on increasing iron intake and improving its absorption through strategies like increasing vitamin C consumption, which enhances non-heme iron absorption [101,102]. The potential value of adequate vitamin D dietary intake and supplementation in iron deficiency and anemia management should be examined in broader clinical trials in Morocco. Such trials could further lead to more tailored, effective treatment strategies for vulnerable women population.
Moreover, the high rates of overweight and obesity in our sample (61.3%) could further impair the adequate evaluation of body stores of vitamin D and iron by impacting their bioavailability [103,104,105,106] and thus obscuring their interaction. Our data further revealed that higher BMI was significantly associated with anemia (p=0.001), with 72.2% of anemic women being either overweight or obese, compared to 58.1% among the non-anemic women. Obesity-related factors [107], such as chronic low-grade inflammation and elevated hepcidin levels, are well-documented contributors to iron deficiency and anemia [107]. Additionally, the sequestration of fat-soluble vitamin D in adipose tissue offers a plausible explanation for the low vitamin D levels observed, as it supported by other studies [108].
Sunlight exposure, a key source of 25(OH)D in humans [13], is consistently linked to VDD in women [58,109], although its role in anemia and iron metabolism is less understood. Emerging studies suggest that ultraviolet radiation might affect blood gene expression related to inflammatory responses, cytokine regulation, and cellular transport, potentially impacting hepcidin and iron metabolism beyond its direct effects on vitamin D synthesis and plasma 25(OH)D levels [110]. Our bivariate analysis indicates that women with insufficient to moderate sun exposure have significantly 59% higher odds of having anemia compared to those with sufficient sun exposure (p=0.034). However, when VDD and other predictors are included in the multivariate model, the effect of sun exposure on anemia risk was no longer statistically significant. We also found that women with insufficient to moderate sun exposure are about 2.6 times more likely to have VDD compared to those with sufficient sun exposure (p<0.001) (data not shown). This strong association suggests that the relationship between sun exposure and anemia may be driven largely by its impact on vitamin D levels, which could partially explain the widespread prevalence of VDD among the anemic group.
Furthermore, low physical activity and urban residency emerged as independent risk factors for anemia in our study. Urban living and sedentary lifestyles may reduce opportunities for outdoor exposure to sunlight, thereby decreasing UVB availability for vitamin D production [109,111,112,113]. This reduction in sun exposure may further exacerbate VDD and its associated anemia risk among our participants. The association between low physical activity and anemia is further supported by evidence showing that anemia can impair aerobic capacity, as indicated by decreased maximal oxygen consumption (VO2max), which affects physical fitness and endurance [114]. This could suggest a cyclical relationship where sedentary behavior contributes to anemia, which in turn exacerbates fatigue and reduces physical activity levels. However, whether sedentary behavior is primarily a cause, or a consequence of altered iron status and hemoglobin levels remains to be fully elucidated [115,116]
Taken together, these findings underscore the need for interventions focused on promoting outdoor activities, enhancing sun exposure, and improving dietary quality or supplementing vitamin D intake. Such strategies may be crucial for maintaining adequate vitamin D levels, which in turn could support hemoglobin synthesis and iron metabolism in anemic women.
This study's strengths include the use of validated questionnaires to estimate vitamin D intake and sun exposure behavior, providing detailed insights into the dietary patterns of Moroccan women. The study also adjusted for multiple relevant confounders, including BMI, lifestyle factors, and socioeconomic characteristics to improve the reliability of results. However, the use of single 24-hour recall used to estimate iron intake may not represent usual participant intake. Besides, the study's cross-sectional nature limits the ability to infer causality between VDD, iron status, and anemia risk. While associations were identified, it remains unclear whether VDD directly contributes to anemia or if other underlying factors might mediate this relationship. We conducted our analysis in a relatively modest sample size (n=463) from a single region (Meknes), which may limit the generalizability of the findings to the broader population of Moroccan WRA. Future longitudinal research with larger sample sizes and the inclusion of relevant biomarkers such as hepcidin and transferrin receptor is needed to explore the temporal dynamics of the observed associations and give more depth of the analysis. Such research would also aid in developing more targeted prevention and management strategies.
5. Conclusions
In summary, our study adds to the growing body of evidence that VDD significantly impacts iron homeostasis in premenopausal women, increasing the risk of anemia and poor iron status among Moroccan WRA. Addressing VDD in this at-risk group could not only support bone health but also enhance iron metabolism, potentially preventing iron deficiency and anemia. Clinically, recognizing that VDD and iron deficiency are interrelated and often coexist in anemic WRA is crucial. Our findings suggest that routine assessment of VDD as part of a comprehensive evaluation in anemic women could offer valuable insights into the multifactorial causes of anemia and IDA. This integrated approach may improve diagnostic precision and lead to more effective, individualized treatment strategies. Further clinical trials are sought to determine the efficacy of vitamin D supplementation as an adjunct therapy in managing ID and anemia.
In the current context, there is also an urgent need for targeted public health interventions and awareness campaigns to promote adequate dietary intake, sun exposure, and overall healthy lifestyle choices among young Moroccan women. These efforts could play a crucial role in reducing the dual burden of VDD and anemia in this vulnerable population.
Author Contributions
Conceptualization N.Z, and I.L.; Methodology, N.Z; Data collection, N.Z. and I.L.; Statistical analysis and interpretation, N.Z. and Y.F.-Z.; Drafting of the initial project, N.Z.; Scientific supervision, A.E.M., L.G., Y.F.-Z. and S.E.J.; Supervision of the study and approval of the manuscript, A.E.M., L.G., Y.F.-Z. and S.E.J. All authors have read and agreed to the published version of the manuscript.
Funding
This study was funded by the Institutional University Cooperation Program with Moulay Ismail University, which is supported by VLIR-UOS (Phase I: 2017–2021; Contract n°MA2017IUC038A104) and by the “SEBIO” Research and Development Project (Morocco, PDR-MA-SEBIO (2017–2022)).
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the ethics committee of biomedical research at Moulay Ismail University of Meknes (reference; N°1/CERB-UMI/19).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets generated and analyzed for the current study are available from the corresponding author, upon reasonable request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Kinyoki, D.; Osgood-Zimmerman, A.E.; Bhattacharjee, N.V.; Local Burden of Disease Anaemia Collaborators; Schaeffer, L.E.; Lazzar-Atwood, A.; Lu, D.; Ewald, S.B.; Donkers, K.M.; Letourneau, I.D.; et al. Anemia Prevalence in Women of Reproductive Age in Low- and Middle-Income Countries between 2000 and 2018. Nat. Med. 2021, 27, 1761–1782. [Google Scholar] [CrossRef] [PubMed]
- Cui, A.; Zhang, T.; Xiao, P.; Fan, Z.; Wang, H.; Zhuang, Y. Global and Regional Prevalence of Vitamin D Deficiency in Population-Based Studies from 2000 to 2022: A Pooled Analysis of 7.9 Million Participants. Front. Nutr. 2023, 10, 1070808. [Google Scholar] [CrossRef] [PubMed]
- Horton, S.; Ross, J. The Economics of Iron Deficiency. Food Policy 2003, 28, 51–75. [Google Scholar] [CrossRef]
- Heath, A.; Kim, I.; Hodge, A.; English, D.; Muller, D. Vitamin D Status and Mortality: A Systematic Review of Observational Studies. Int. J. Environ. Res. Public. Health 2019, 16, 383. [Google Scholar] [CrossRef]
- Liu, Z.; Sun, R.; Li, J.; Cheng, W.; Li, L. Relations of Anemia With the All-Cause Mortality and Cardiovascular Mortality in General Population: A Meta-Analysis. Am. J. Med. Sci. 2019, 358, 191–199. [Google Scholar] [CrossRef]
- Wagner, C.L.; Hollis, B.W. The Implications of Vitamin D Status During Pregnancy on Mother and Her Developing Child. Front. Endocrinol. 2018, 9, 500. [Google Scholar] [CrossRef]
- Smith, E.R.; Shankar, A.H.; Wu, L.S.-F.; Aboud, S.; Adu-Afarwuah, S.; Ali, H.; Agustina, R.; Arifeen, S.; Ashorn, P.; Bhutta, Z.A.; et al. Modifiers of the Effect of Maternal Multiple Micronutrient Supplementation on Stillbirth, Birth Outcomes, and Infant Mortality: A Meta-Analysis of Individual Patient Data from 17 Randomised Trials in Low-Income and Middle-Income Countries. Lancet Glob. Health 2017, 5, e1090–e1100. [Google Scholar] [CrossRef]
- WHO. Global nutrition targets 2025: anaemia policy brief (WHO/NMH/NHD/14.4). Geneva: World Health Organization; 2014.
- WHO. Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity. Vitamin and Mineral Nutrition Information System. Geneva, World Health Organization, 2011 (WHO/NMH/NHD/MNM/11.1) available online on:http://www.who.int/vmnis/indicators/haemoglobin. pdf, accessed on 22may2021).
- World Health Organization Nutritional Anaemias: Tools for Effective Prevention and Control; World Health Organization: Geneva, 2017; ISBN 978-92-4-151306-7.
- Holick, M.F. Vitamin D Deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef]
- Holick, M.F. The Vitamin D Deficiency Pandemic: Approaches for Diagnosis, Treatment and Prevention. Rev. Endocr. Metab. Disord. 2017, 18, 153–165. [Google Scholar] [CrossRef]
- Holick, M.F. Ultraviolet B Radiation: The Vitamin D Connection. Adv. Exp. Med. Biol. 2017, 996, 137–154. [Google Scholar] [CrossRef]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Endocrine Society Evaluation, Treatment, and Prevention of Vitamin D Deficiency: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed]
- Fleet, J.C.; Shapses, S.A. Vitamin D. In Present Knowledge in Nutrition; Elsevier, 2020; pp. 93–114. ISBN 978-0-323-66162-1. [Google Scholar]
- Dimitrov, V.; Barbier, C.; Ismailova, A.; Wang, Y.; Dmowski, K.; Salehi-Tabar, R.; Memari, B.; Groulx-Boivin, E.; White, J.H. Vitamin D-Regulated Gene Expression Profiles: Species-Specificity and Cell-Specific Effects on Metabolism and Immunity. Endocrinology 2021, 162, bqaa218. [Google Scholar] [CrossRef] [PubMed]
- Ciepiela, P.; Dulęba, A.J.; Kowaleczko, E.; Chełstowski, K.; Kurzawa, R. Vitamin D as a Follicular Marker of Human Oocyte Quality and a Serum Marker of in Vitro Fertilization Outcome. J. Assist. Reprod. Genet. 2018, 35, 1265–1276. [Google Scholar] [CrossRef]
- Pérez-Fernandez, R.; Alonso, M.; Segura, C.; Muñoz, I.; Garcia-Caballero, T.; Diéguez, C. Vitamin D Receptor Gene Expression in Human Pituitary Gland. Life Sci. 1996, 60, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Norman, A.W. Vitamin D Receptor: New Assignments for an Already Busy Receptor. Endocrinology 2006, 147, 5542–5548. [Google Scholar] [CrossRef]
- Aucella, F.; Scalzulli, R.P.; Gatta, G.; Vigilante, M.; Carella, A.M.; Stallone, C. Calcitriol Increases Burst-Forming Unit-Erythroid Proliferation in Chronic Renal Failure. A Synergistic Effect with r-HuEpo. Nephron Clin. Pract. 2003, 95, c121–127. [Google Scholar] [CrossRef]
- Alon, D.B.; Chaimovitz, C.; Dvilansky, A.; Lugassy, G.; Douvdevani, A.; Shany, S.; Nathan, I. Novel Role of 1,25(OH)(2)D(3) in Induction of Erythroid Progenitor Cell Proliferation. Exp. Hematol. 2002, 30, 403–409. [Google Scholar] [CrossRef]
- Bacchetta, J.; Zaritsky, J.J.; Sea, J.L.; Chun, R.F.; Lisse, T.S.; Zavala, K.; Nayak, A.; Wesseling-Perry, K.; Westerman, M.; Hollis, B.W.; et al. Suppression of Iron-Regulatory Hepcidin by Vitamin D. J. Am. Soc. Nephrol. 2014, 25, 564–572. [Google Scholar] [CrossRef]
- Ganz, T.; Nemeth, E. Hepcidin and Iron Homeostasis. Biochim. Biophys. Acta BBA - Mol. Cell Res. 2012, 1823, 1434–1443. [Google Scholar] [CrossRef]
- Zughaier, S.M.; Alvarez, J.A.; Sloan, J.H.; Konrad, R.J.; Tangpricha, V. The Role of Vitamin D in Regulating the Iron-Hepcidin-Ferroportin Axis in Monocytes. J. Clin. Transl. Endocrinol. 2014, 1, e19–e25. [Google Scholar] [CrossRef]
- Smith, E.M.; Tangpricha, V. Vitamin D and Anemia: Insights into an Emerging Association. Curr. Opin. Endocrinol. Diabetes Obes. 2015, 22, 432–438. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Mei, G.; Zhou, F.; Kong, B.; Chen, L.; Chen, H.; Wang, L.; Tang, Y.; Yao, P. Vitamin D Decreases Pancreatic Iron Overload in Type 2 Diabetes through the NF-κB-DMT1 Pathway. J. Nutr. Biochem. 2022, 99, 108870. [Google Scholar] [CrossRef] [PubMed]
- Shawki, A.; Knight, P.B.; Maliken, B.D.; Niespodzany, E.J.; Mackenzie, B. H+-Coupled Divalent Metal-Ion Transporter-1. In Current Topics in Membranes; Elsevier, 2012; Vol. 70, pp. 169–214. ISBN 978-0-12-394316-3. [Google Scholar]
- Fleet, J.C.; Aldea, D.; Chen, L.; Christakos, S.; Verzi, M. Regulatory Domains Controlling High Intestinal Vitamin D Receptor Gene Expression Are Conserved in Mouse and Human. J. Biol. Chem. 2022, 298, 101616. [Google Scholar] [CrossRef]
- Malczewska-Lenczowska, J.; Sitkowski, D.; Surała, O.; Orysiak, J.; Szczepańska, B.; Witek, K. The Association between Iron and Vitamin D Status in Female Elite Athletes. Nutrients 2018, 10, 167. [Google Scholar] [CrossRef]
- Sim, J.J.; Lac, P.T.; Liu, I.L.A.; Meguerditchian, S.O.; Kumar, V.A.; Kujubu, D.A.; Rasgon, S.A. Vitamin D Deficiency and Anemia: A Cross-Sectional Study. Ann. Hematol. 2010, 89, 447–452. [Google Scholar] [CrossRef]
- Liu, T.; Zhong, S.; Liu, L.; Liu, S.; Li, X.; Zhou, T.; Zhang, J. Vitamin D Deficiency and the Risk of Anemia: A Meta-Analysis of Observational Studies. Ren. Fail. 2015, 37, 929–934. [Google Scholar] [CrossRef]
- Blanco-Rojo, R.; Pérez-Granados, A.M.; Toxqui, L.; Zazo, P.; De La Piedra, C.; Vaquero, M.P. Relationship between Vitamin D Deficiency, Bone Remodelling and Iron Status in Iron-Deficient Young Women Consuming an Iron-Fortified Food. Eur. J. Nutr. 2013, 52, 695–703. [Google Scholar] [CrossRef] [PubMed]
- Mogire, R.M.; Muriuki, J.M.; Morovat, A.; Mentzer, A.J.; Webb, E.L.; Kimita, W.; Ndungu, F.M.; Macharia, A.W.; Cutland, C.L.; Sirima, S.B.; et al. Vitamin D Deficiency and Its Association with Iron Deficiency in African Children. Nutrients 2022, 14, 1372. [Google Scholar] [CrossRef]
- Soepnel, L.M.; Mabetha, K.; Draper, C.E.; Silubonde, T.M.; Smuts, C.M.; Pettifor, J.M.; Norris, S.A. A Cross-Sectional Study of the Associations between Biomarkers of Vitamin D, Iron Status, and Hemoglobin in South African Women of Reproductive Age: The Healthy Life Trajectories Initiative, South Africa. Curr. Dev. Nutr. 2023, 7, 100072. [Google Scholar] [CrossRef]
- Arabi, S.M.; Ranjbar, G.; Bahrami, L.S.; Vafa, M.; Norouzy, A. The Effect of Vitamin D Supplementation on Hemoglobin Concentration: A Systematic Review and Meta-Analysis. Nutr. J. 2020, 19, 11. [Google Scholar] [CrossRef]
- Azizi-Soleiman, F.; Vafa, M.; Abiri, B.; Safavi, M. Effects of Iron on Vitamin D Metabolism: A Systematic Review. Int. J. Prev. Med. 2016, 7, 126. [Google Scholar] [CrossRef] [PubMed]
- Toxqui, L.; Pérez-Granados, A.M.; Blanco-Rojo, R.; Wright, I.; González-Vizcayno, C.; Vaquero, M.P. Effects of an Iron or Iron and Vitamin D–Fortified Flavored Skim Milk on Iron Metabolism: A Randomized Controlled Double-Blind Trial in Iron-Deficient Women. J. Am. Coll. Nutr. 2013, 32, 312–320. [Google Scholar] [CrossRef]
- Heldenberg, D.; Tenenbaum, G.; Weisman, Y. Effect of Iron on Serum 25-Hydroxyvitamin D and 24,25-Dihydroxyvitamin D Concentrations. Am. J. Clin. Nutr. 1992, 56, 533–536. [Google Scholar] [CrossRef]
- Ministère de la Santé, M. La Lutte Contre Les Troubles Dus Aux Carences En Micronutriments. Situation et Perspectives. Rapport Ministère de La Santé 2003.
- PNN, Enquête Nationale sur la Nutrition, Diversité alimentaire, Carence en Fer, Carence en Vitamine A, Carence en Iode. 2019. Available online: https://www.sante.gov.ma/Documents/2022/07/rapport%20ENN%202019-2020%20ajout%20preface%20(1).pdf (accessed on 2 January 2022).
- Programme national de nutrition. Available online: https://www.sante.gov.ma/Documents/2019/06/Programme%20National%20de%20Nutrition.pdf (accessed on 21 April 2021).
- Glenn, D. Israel. Determining Sample Size 1. University of Florida IFAS Extension. 2012, pp. 1–5. Available online: http://Edis.Ifas.Ufl.Edu (accessed on 12 january 2021).
- Chaparro, C.M.; Suchdev, P.S. Anemia Epidemiology, Pathophysiology, and Etiology in Low- and Middle-Income Countries. Ann. N. Y. Acad. Sci. 2019, 1450, 15–31. [Google Scholar] [CrossRef]
- Briguglio, M.; Hrelia, S.; Malaguti, M.; Lombardi, G.; Riso, P.; Porrini, M.; Perazzo, P.; Banfi, G. The Central Role of Iron in Human Nutrition: From Folk to Contemporary Medicine. Nutrients 2020, 12, 1761. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Chen, W.; Li, D.; Yin, X.; Zhang, X.; Olsen, N.; Zheng, S.G. Vitamin D and Chronic Diseases. Aging Dis. 2017, 8, 346. [Google Scholar] [CrossRef]
- de Souza, S.S.; Camargos, A.F.; Ferreira, M.C.F.; de Assis Nunes Pereira, F.; de Rezende, C.P.; Araújo, C.A.A.; Silva Filho, A.L. Hemoglobin Levels Predict Quality of Life in Women with Heavy Menstrual Bleeding. Arch. Gynecol. Obstet. 2010, 281, 895–900. [Google Scholar] [CrossRef] [PubMed]
- Gröber, U.; Schmidt, J.; Kisters, K. Important Drug-Micronutrient Interactions: A Selection for Clinical Practice. Crit. Rev. Food Sci. Nutr. 2020, 60, 257–275. [Google Scholar] [CrossRef]
- Kalus, U.; Pruss, A.; Wodarra, J.; Kiesewetter, H.; Salama, A.; Radtke, H. Influence of Blood Donation on Levels of Water-soluble Vitamins. Transfus. Med. 2008, 18, 360–365. [Google Scholar] [CrossRef]
- WHO Consultation on Obesity (1997: Geneva, Switzerland)World Health Organization. Division of Noncommunicable Diseases & World Health Organization. Programme of Nutrition, Family and Reproductive Health. (1998) Obesity : Preventing and Managing the Global Epidemic : Report of a WHO Consultation on Obesity, Geneva, 3-5 June 1997.
- Zouine, N.; Lhilali, I.; Menouni, A.; Godderis, L.; El Midaoui, A.; El Jaafari, S.; Zegzouti Filali, Y. Development and Validation of Vitamin D- Food Frequency Questionnaire for Moroccan Women of Reproductive Age: Use of the Sun Exposure Score and the Method of Triad’s Model. Nutrients 2023, 15, 796. [Google Scholar] [CrossRef]
- Neve J Aliments et Préparations Typiques de La Population Marocaine: Outil Pour Estimer La Consommation Alimentaire. 2008.
- The French Agency for Food, Environmental and Occupationnal Health Safty (ANSES) Ciqual French Food Composition 2017.
- U.S. Department of Agriculture, Agricultural Research Service USDA Food and Nutrient Database for Dietary Studies 2015-2016. 2018.
- Skolmowska, D.; Głąbska, D. Analysis of Heme and Non-Heme Iron Intake and Iron Dietary Sources in Adolescent Menstruating Females in a National Polish Sample. Nutrients 2019, 11, 1049. [Google Scholar] [CrossRef] [PubMed]
- Pretorius, B.; Schönfeldt, H.C.; Hall, N. Total and Haem Iron Content Lean Meat Cuts and the Contribution to the Diet. Food Chem. 2016, 193, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Willett, W.C.; Howe, G.R.; Kushi, L.H. Adjustment for Total Energy Intake in Epidemiologic Studies. Am. J. Clin. Nutr. 1997, 65, 1220S–1228S, discussion 1229S-1231S. [Google Scholar] [CrossRef] [PubMed]
- Vitamin and Mineral Requirements in Human Nutrition; Weltgesundheitsorganisation, Ed.; 2. ed.; Geneva, 2004; ISBN 978-92-4-154612-6.
- Lhilali, I.; Zouine, N.; Menouni, A.; Godderis, L.; Kestemont, M.-P.; El Midaoui, A.; El Jaafari, S.; Filali-Zegzouti, Y. Sun Exposure Score and Vitamin D Levels in Moroccan Women of Childbearing Age. Nutrients 2023, 15, 688. [Google Scholar] [CrossRef] [PubMed]
- Forde, C. Scoring the International Physical Activity Questionnaire (IPAQ); University of Dublin: Dublin, Ireland, 2018; p. 3. [Google Scholar]
- Craig, C.; Marshall, A.; Sjostrom, M.; et al. International physical activity questionnaire-short form. J Am Coll Health 2017, 65, 492–501. [Google Scholar]
- Nairz, M.; Theurl, I.; Wolf, D.; Weiss, G. Iron Deficiency or Anemia of Inflammation?: Differential Diagnosis and Mechanisms of Anemia of Inflammation. Wien. Med. Wochenschr. 2016, 166, 411–423. [Google Scholar] [CrossRef]
- World Health Organization WHO Guideline on Use of Ferritin Concentrations to Assess Iron Status in Individuals and Populations; World Health Organization: Geneva, 2020; ISBN 978-92-4-000012-4.
- Bouillon, R.; Van Schoor, N.M.; Gielen, E.; Boonen, S.; Mathieu, C.; Vanderschueren, D.; Lips, P. Optimal Vitamin D Status: A Critical Analysis on the Basis of Evidence-Based Medicine. J. Clin. Endocrinol. Metab. 2013, 98, E1283–E1304. [Google Scholar] [CrossRef]
- Holick, M.F. Vitamin D Status: Measurement, Interpretation, and Clinical Application. Ann. Epidemiol. 2009, 19, 73–78. [Google Scholar] [CrossRef]
- Bouillon, R.; Manousaki, D.; Rosen, C.; Trajanoska, K.; Rivadeneira, F.; Richards, J.B. The Health Effects of Vitamin D Supplementation: Evidence from Human Studies. Nat. Rev. Endocrinol. 2022, 18, 96–110. [Google Scholar] [CrossRef]
- Levey, A.S. A More Accurate Method To Estimate Glomerular Filtration Rate from Serum Creatinine: A New Prediction Equation. Ann. Intern. Med. 1999, 130, 461. [Google Scholar] [CrossRef]
- Hosmer, D.W.; Lemeshow, S.; Sturdivant, R.X. Applied Logistic Regression; Wiley Series in Probability and Statistics; 1st ed.; Wiley, 2013; ISBN 978-0-470-58247-3.
- Zhou, X.; Obuchowski, N.A.; McClish, D.K. Statistical Methods in Diagnostic Medicine; Wiley Series in Probability and Statistics; 1st ed.; Wiley, 2011; ISBN 978-0-470-18314-4.
- Schober, P.; Boer, C.; Schwarte, L.A. Correlation Coefficients: Appropriate Use and Interpretation. Anesth. Analg. 2018, 126, 1763–1768. [Google Scholar] [CrossRef] [PubMed]
- Várbíró, S.; Takács, I.; Tűű, L.; Nas, K.; Sziva, R.E.; Hetthéssy, J.R.; Török, M. Effects of Vitamin D on Fertility, Pregnancy and Polycystic Ovary Syndrome—A Review. Nutrients 2022, 14, 1649. [Google Scholar] [CrossRef] [PubMed]
- Binkley, N.; Bikle, D.D.; Dawson-Hughes, B.; Plum, L.; Sempos, C.; DeLuca, H.F. Nonskeletal Effects of Vitamin D. In Principles of Bone Biology; Elsevier, 2020; pp. 757–774 ISBN 978-0-12-814841-9.
- Szarpak, L.; Feduniw, S.; Pruc, M.; Ciebiera, M.; Cander, B.; Rahnama-Hezavah, M.; Szarpak, Ł. The Vitamin D Serum Levels in Pregnant Women Affected by COVID-19: A Systematic Review and Meta-Analysis. Nutrients 2023, 15, 2588. [Google Scholar] [CrossRef] [PubMed]
- Estébanez, N.; Gómez-Acebo, I.; Palazuelos, C.; Llorca, J.; Dierssen-Sotos, T. Vitamin D Exposure and Risk of Breast Cancer: A Meta-Analysis. Sci. Rep. 2018, 8, 9039. [Google Scholar] [CrossRef] [PubMed]
- Osanai, M.; Lee, G.-H. CYP24A1-Induced Vitamin D Insufficiency Promotes Breast Cancer Growth. Oncol. Rep. 2016, 36, 2755–2762. [Google Scholar] [CrossRef]
- Suh, Y.J.; Lee, J.E.; Lee, D.H.; Yi, H.G.; Lee, M.H.; Kim, C.S.; Nah, J.W.; Kim, S.K. Prevalence and Relationships of Iron Deficiency Anemia with Blood Cadmium and Vitamin D Levels in Korean Women. J. Korean Med. Sci. 2016, 31, 25. [Google Scholar] [CrossRef]
- Shin, J.Y.; Shim, J.Y. Low Vitamin D Levels Increase Anemia Risk in Korean Women. Clin. Chim. Acta 2013, 421, 177–180. [Google Scholar] [CrossRef]
- Seong, J.M.; Park, C.E.; Gi, M.Y.; Cha, J.A.; Moon, A.E.; Lee, J.H.; Sung, H.H.; Lim, J.H.; Oh, S.H.; Chung, C.H.; et al. Gender Difference in the Relationship between Anemia and Vitamin D in Korean Adults: The Fifth Korea National Health and Nutrition Examination Survey. J. Clin. Biochem. Nutr. 2021, 69, 299–304. [Google Scholar] [CrossRef]
- Thomas, C.E.; Guillet, R.; Queenan, R.A.; Cooper, E.M.; Kent, T.R.; Pressman, E.K.; Vermeylen, F.M.; Roberson, M.S.; O’Brien, K.O. Vitamin D Status Is Inversely Associated with Anemia and Serum Erythropoietin during Pregnancy. Am. J. Clin. Nutr. 2015, 102, 1088–1095. [Google Scholar] [CrossRef]
- Bacchetta, J.; Zaritsky, J.J.; Sea, J.L.; Chun, R.F.; Lisse, T.S.; Zavala, K.; Nayak, A.; Wesseling-Perry, K.; Westerman, M.; Hollis, B.W.; et al. Suppression of Iron-Regulatory Hepcidin by Vitamin D. J. Am. Soc. Nephrol. 2014, 25, 564–572. [Google Scholar] [CrossRef]
- Smith, E.M.; Alvarez, J.A.; Kearns, M.D.; Hao, L.; Sloan, J.H.; Konrad, R.J.; Ziegler, T.R.; Zughaier, S.M.; Tangpricha, V. High-Dose Vitamin D3 Reduces Circulating Hepcidin Concentrations: A Pilot, Randomized, Double-Blind, Placebo-Controlled Trial in Healthy Adults. Clin. Nutr. Edinb. Scotl. 2017, 36, 980–985. [Google Scholar] [CrossRef]
- Zhang, Y.; Wang, X.; Wang, J.; Hu, W.; Song, X.; Yuan, D.; Yan, X. The Association between Standardized Serum 25-Hydroxyvitamin D Concentration and Risk of Anemia: A Population-Based Cross-Sectional Study. Int. J. Clin. Pract. 2022, 2022, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Greenwood, A.; von Hurst, P.R.; Beck, K.L.; Mazahery, H.; Lim, K.; Badenhorst, C.E. Relationship between Vitamin D, Iron, and Hepcidin in Premenopausal Females, Potentially Confounded by Ethnicity. Eur. J. Nutr. 2023, 62, 3361–3368. [Google Scholar] [CrossRef]
- Michalski, E.S.; Nguyen, P.H.; Gonzalez-Casanova, I.; Nguyen, S.V.; Martorell, R.; Tangpricha, V.; Ramakrishnan, U. Serum 25-Hydroxyvitamin D but Not Dietary Vitamin D Intake Is Associated with Hemoglobin in Women of Reproductive Age in Rural Northern Vietnam. J. Clin. Transl. Endocrinol. 2017, 8, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Smith, E.M.; Alvarez, J.A.; Martin, G.S.; Zughaier, S.M.; Ziegler, T.R.; Tangpricha, V. Vitamin D Deficiency Is Associated with Anaemia among African Americans in a US Cohort. Br. J. Nutr. 2015, 113, 1732–1740. [Google Scholar] [CrossRef] [PubMed]
- Lavoie, A.; Lemire, M.; Lévesque, B.; Ayotte, P. Determinants of Iron Deficiency and Anemia among Nunavimmiut: Results from the Qanuilirpitaa? 2017 Nunavik Health Survey. Can. J. Public Health Rev. Can. Sante Publique 2024, 115, 152–167. [Google Scholar] [CrossRef]
- Slominski, A.T.; Kim, T.-K.; Li, W.; Yi, A.-K.; Postlethwaite, A.; Tuckey, R.C. The Role of CYP11A1 in the Production of Vitamin D Metabolites and Their Role in the Regulation of Epidermal Functions. J. Steroid Biochem. Mol. Biol. 2014, 144 Pt A, 28–39. [Google Scholar] [CrossRef]
- Hou, Y.; Zhang, S.; Wang, L.; Li, J.; Qu, G.; He, J.; Rong, H.; Ji, H.; Liu, S. Estrogen Regulates Iron Homeostasis through Governing Hepatic Hepcidin Expression via an Estrogen Response Element. Gene 2012, 511, 398–403. [Google Scholar] [CrossRef]
- Velarde, M.C. Mitochondrial and Sex Steroid Hormone Crosstalk during Aging. Longev. Heal. 2014, 3, 2. [Google Scholar] [CrossRef]
- Toxqui, L.; Vaquero, M. Chronic Iron Deficiency as an Emerging Risk Factor for Osteoporosis: A Hypothesis. Nutrients 2015, 7, 2324–2344. [Google Scholar] [CrossRef]
- Pike, J.W.; Meyer, M.B. The Vitamin D Receptor: New Paradigms for the Regulation of Gene Expression by 1,25-Dihydroxyvitamin D3. Endocrinol. Metab. Clin. North Am. 2010, 39, 255–269. [Google Scholar] [CrossRef] [PubMed]
- Pasricha, S.-R.; Drakesmith, H.; Black, J.; Hipgrave, D.; Biggs, B.-A. Control of Iron Deficiency Anemia in Low- and Middle-Income Countries. Blood 2013, 121, 2607–2617. [Google Scholar] [CrossRef] [PubMed]
- Napolitano, M.; Dolce, A.; Celenza, G.; Grandone, E.; Perilli, M.G.; Siragusa, S.; Carta, G.; Orecchioni, A.; Mariani, G. Iron-Dependent Erythropoiesis in Women with Excessive Menstrual Blood Losses and Women with Normal Menses. Ann. Hematol. 2014, 93, 557–563. [Google Scholar] [CrossRef] [PubMed]
- Bothwell, T.H. Iron Requirements in Pregnancy and Strategies to Meet Them. Am. J. Clin. Nutr. 2000, 72, 257S–264S. [Google Scholar] [CrossRef]
- Hurrell, R.; Egli, I. Iron Bioavailability and Dietary Reference Values. Am. J. Clin. Nutr. 2010, 91, 1461S–1467S. [Google Scholar] [CrossRef]
- Milman, N.T. Dietary Iron Intake in Women of Reproductive Age in Europe: A Review of 49 Studies from 29 Countries in the Period 1993–2015. J. Nutr. Metab. 2019, 2019, 1–13. [Google Scholar] [CrossRef]
- Spiro, A.; Buttriss, J.L. Vitamin D : An Overview of Vitamin D Status and Intake in E Urope. Nutr. Bull. 2014, 39, 322–350. [Google Scholar] [CrossRef]
- Benhammou, S.; Heras-González, L.; Ibáñez-Peinado, D.; Barceló, C.; Hamdan, M.; Rivas, A.; Mariscal-Arcas, M.; Olea-Serrano, F.; Monteagudo, C. Comparison of Mediterranean Diet Compliance between European and Non-European Populations in the Mediterranean Basin. Appetite 2016, 107, 521–526. [Google Scholar] [CrossRef]
- Masella, R.; Malorni, W. Gender-Related Differences in Dietary Habits. Clin. Manag. Issues 2017, 11. [Google Scholar] [CrossRef]
- High Commission for Planning. National Survey on Household Consumption and Expenditure. [Internet]. Rabat(Morocco): High Commission for Plannig, 2013/2014. Available from: Https://Www.Hcp.Ma/Downloads/Enquete-Nationale-Sur-La-Consommation-et-Les-Depenses-Des-Menages_t21181.Html (Accessed 20 April 2020).
- Zijp, I.M.; Korver, O.; Tijburg, L.B.M. Effect of Tea and Other Dietary Factors on Iron Absorption. Crit. Rev. Food Sci. Nutr. 2000, 40, 371–398. [Google Scholar] [CrossRef]
- Thankachan, P.; Walczyk, T.; Muthayya, S.; Kurpad, A.V.; Hurrell, R.F. Iron Absorption in Young Indian Women: The Interaction of Iron Status with the Influence of Tea and Ascorbic Acid. Am. J. Clin. Nutr. 2008, 87, 881–886. [Google Scholar] [CrossRef] [PubMed]
- Skolmowska, D.; Głąbska, D.; Kołota, A.; Guzek, D. Effectiveness of Dietary Interventions to Treat Iron-Deficiency Anemia in Women: A Systematic Review of Randomized Controlled Trials. Nutrients 2022, 14, 2724. [Google Scholar] [CrossRef] [PubMed]
- Mawer, E.B.; Backhouse, J.; Holman, C.A.; Lumb, G.A.; Stanbury, S.W. The Distribution and Storage of Vitamin D and Its Metabolites in Human Tissues. Clin. Sci. 1972, 43, 413–431. [Google Scholar] [CrossRef] [PubMed]
- Pereira-Santos, M.; Costa, P.R.F.; Assis, A.M.O.; Santos, C.A.S.T.; Santos, D.B. Obesity and Vitamin D Deficiency: A Systematic Review and Meta-analysis. Obes. Rev. 2015, 16, 341–349. [Google Scholar] [CrossRef] [PubMed]
- Menzie, C.M.; Yanoff, L.B.; Denkinger, B.I.; McHugh, T.; Sebring, N.G.; Calis, K.A.; Yanovski, J.A. Obesity-Related Hypoferremia Is Not Explained by Differences in Reported Intake of Heme and Nonheme Iron or Intake of Dietary Factors That Can Affect Iron Absorption. J. Am. Diet. Assoc. 2008, 108, 145–148. [Google Scholar] [CrossRef]
- Frelut, M.-L.; Girardet, J.-P.; Bocquet, A.; Briend, A.; Chouraqui, J.-P.; Darmaun, D.; Dupont, C.; Feillet, F.; Hankard, R.; Rozé, J.-C.; et al. Impact of Obesity on Biomarkers of Iron and Vitamin D Status in Children and Adolescents: The Risk of Misinterpretation. Arch. Pédiatrie 2018, 25, 3–5. [Google Scholar] [CrossRef]
- Alshwaiyat, N.; Ahmad, A.; Wan Hassan, W.M.R.; Al-jamal, H. Association between Obesity and Iron Deficiency (Review). Exp. Ther. Med. 2021, 22, 1268. [Google Scholar] [CrossRef]
- Wortsman, J.; Matsuoka, L.Y.; Chen, T.C.; Lu, Z.; Holick, M.F. Decreased Bioavailability of Vitamin D in Obesity. Am. J. Clin. Nutr. 2000, 72, 690–693. [Google Scholar] [CrossRef]
- Santana, K.V.D.S.D.; Oliver, S.L.; Mendes, M.M.; Lanham-New, S.; Charlton, K.E.; Ribeiro, H. Association between Vitamin D Status and Lifestyle Factors in Brazilian Women: Implications of Sun Exposure Levels, Diet, and Health. eClinicalMedicine 2022, 47, 101400. [Google Scholar] [CrossRef]
- Bustamante, M.; Hernandez-Ferrer, C.; Sarria, Y.; Harrison, G.I.; Nonell, L.; Kang, W.; Friedländer, M.R.; Estivill, X.; González, J.R.; Nieuwenhuijsen, M.; et al. The Acute Effects of Ultraviolet Radiation on the Blood Transcriptome Are Independent of Plasma 25OHD3. Environ. Res. 2017, 159, 239–248. [Google Scholar] [CrossRef]
- Kift, R.; Rhodes, L.E.; Farrar, M.D.; Webb, A.R. Is Sunlight Exposure Enough to Avoid Wintertime Vitamin D Deficiency in United Kingdom Population Groups? Int. J. Environ. Res. Public. Health 2018, 15, 1624. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Vitamin D Deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Maeda, S.S.; Saraiva, G.L.; Hayashi, L.F.; Cendoroglo, M.S.; Ramos, L.R.; Corrêa, M. de P.; Henrique de Mesquita, C.; Lazaretti-Castro, M. Seasonal Variation in the Serum 25-Hydroxyvitamin D Levels of Young and Elderly Active and Inactive Adults in São Paulo, Brazil: The São PAulo Vitamin D Evaluation Study (SPADES). Dermatoendocrinol. 2013, 5, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Damian, M.-T.; Vulturar, R.; Login, C.C.; Damian, L.; Chis, A.; Bojan, A. Anemia in Sports: A Narrative Review. Life Basel Switz. 2021, 11, 987. [Google Scholar] [CrossRef] [PubMed]
- Brownlie, T.; Utermohlen, V.; Hinton, P.S.; Haas, J.D. Tissue Iron Deficiency without Anemia Impairs Adaptation in Endurance Capacity after Aerobic Training in Previously Untrained Women. Am. J. Clin. Nutr. 2004, 79, 437–443. [Google Scholar] [CrossRef]
- Haas, J.D.; Brownlie, T. Iron Deficiency and Reduced Work Capacity: A Critical Review of the Research to Determine a Causal Relationship. J. Nutr. 2001, 131, 676S–690S. [Google Scholar] [CrossRef]
Figure 1.
Participant flow chart.
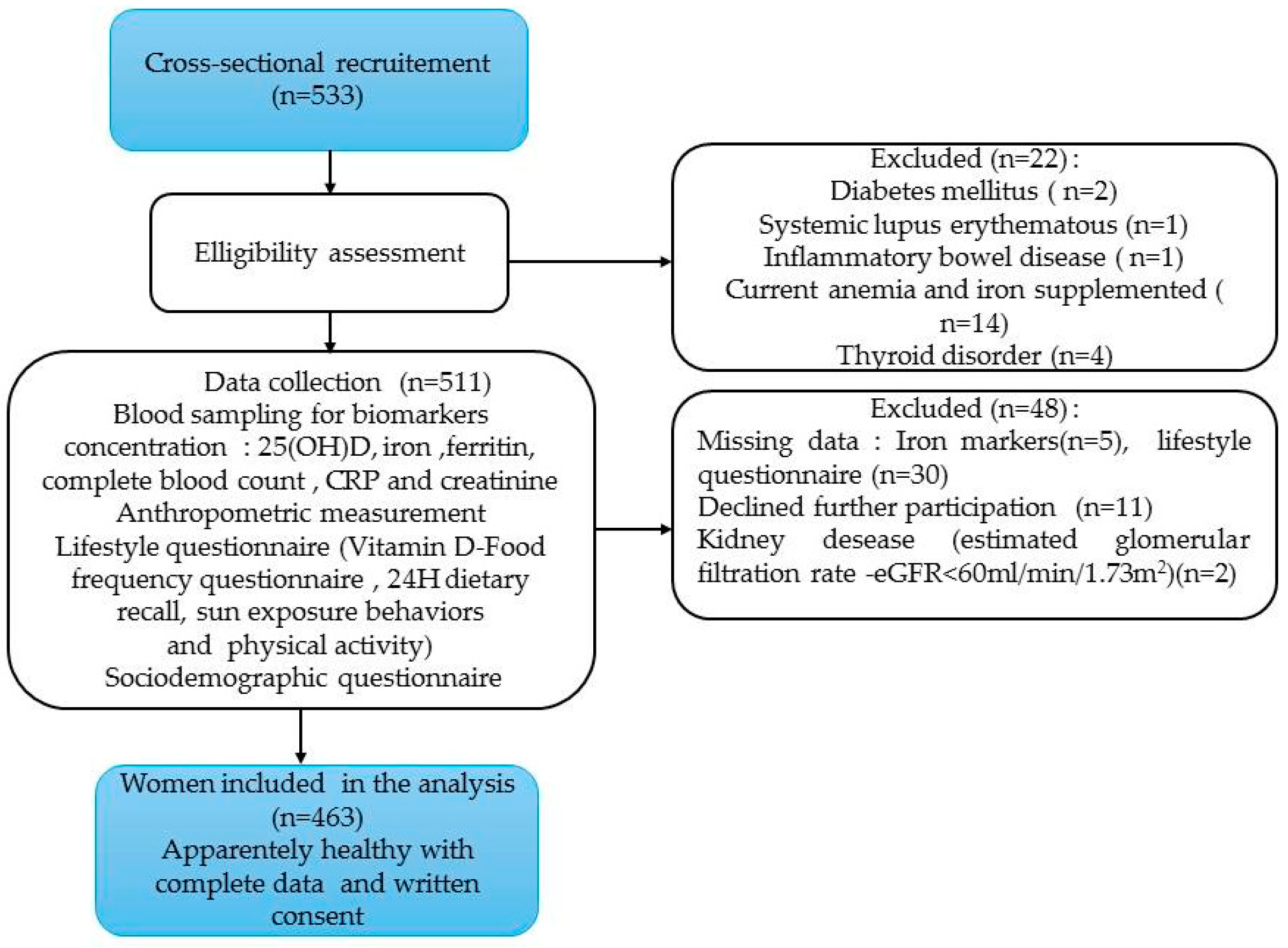
Figure 2.
Scatter and regression plots of anemia indices against log 25(OH) D3 levels. Abbreviations: 25(OH) D3: 25-hydroxyvitamin D, MCV: Mean corpuscular volume, MCH: mean corpuscular hemoglobin, MCHC: mean corpuscular hemoglobin concentration, r: Pearson correlation coefficient, Magnitude of the correlation: Negligible (r: 0.00-0.10), weak (r: 0.10-0.39), moderate (r: 0.40-0.69), strong (r: 0.70- 0.89), very strong (r:0.90-1.00) [69]. *p<0.05.
Figure 2.
Scatter and regression plots of anemia indices against log 25(OH) D3 levels. Abbreviations: 25(OH) D3: 25-hydroxyvitamin D, MCV: Mean corpuscular volume, MCH: mean corpuscular hemoglobin, MCHC: mean corpuscular hemoglobin concentration, r: Pearson correlation coefficient, Magnitude of the correlation: Negligible (r: 0.00-0.10), weak (r: 0.10-0.39), moderate (r: 0.40-0.69), strong (r: 0.70- 0.89), very strong (r:0.90-1.00) [69]. *p<0.05.
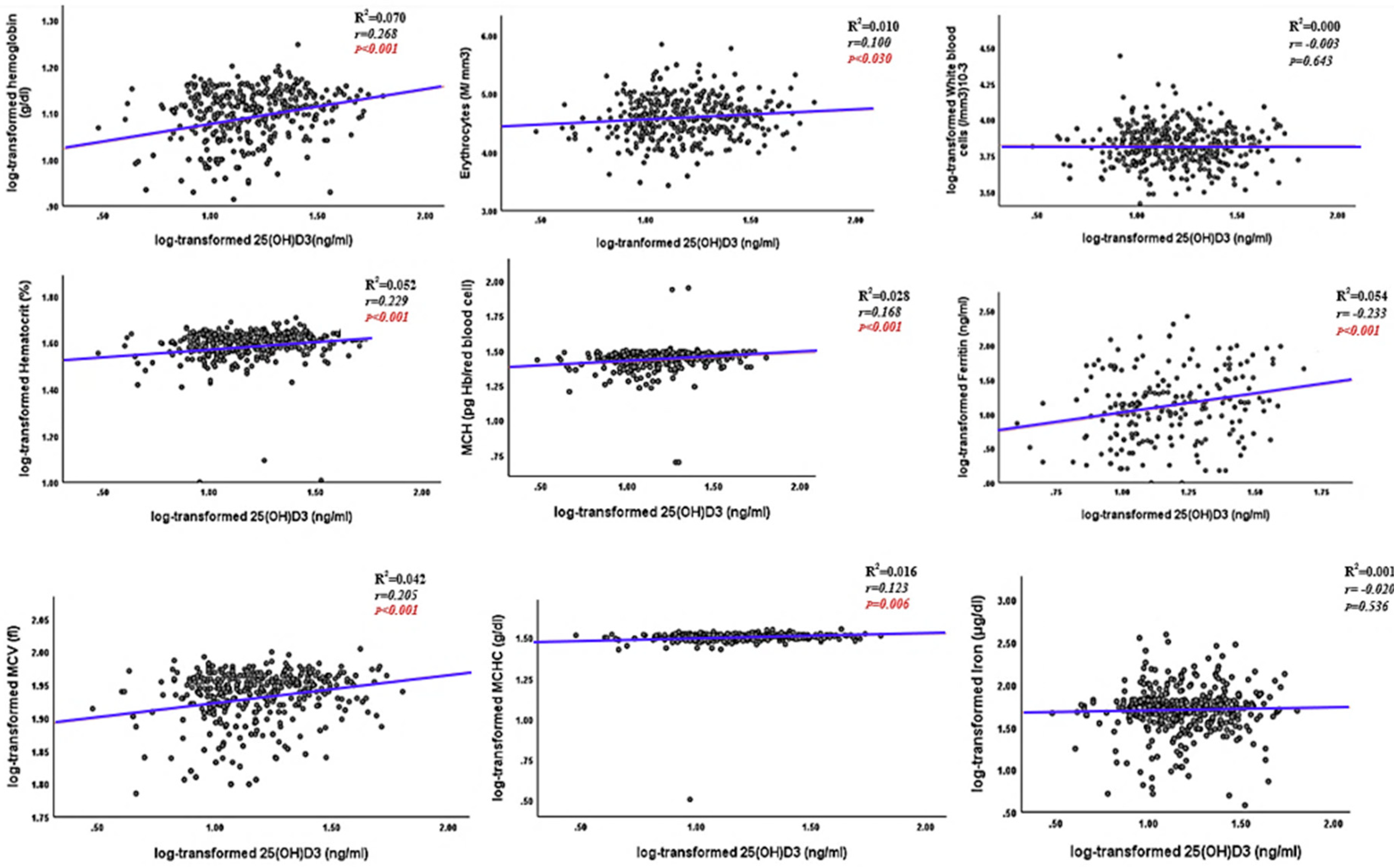
Figure 3.
Roc curves of VDD ability in predicting anemia and iron status. Abbreviations: VDD: Vitamin D deficiency, ID: iron deficiency, IDA: Iron deficiency anemia, AUC: Area under the curve, Sens: sensitivity, Spec: specificity. Statistical significance, p < 0.05.
Figure 3.
Roc curves of VDD ability in predicting anemia and iron status. Abbreviations: VDD: Vitamin D deficiency, ID: iron deficiency, IDA: Iron deficiency anemia, AUC: Area under the curve, Sens: sensitivity, Spec: specificity. Statistical significance, p < 0.05.
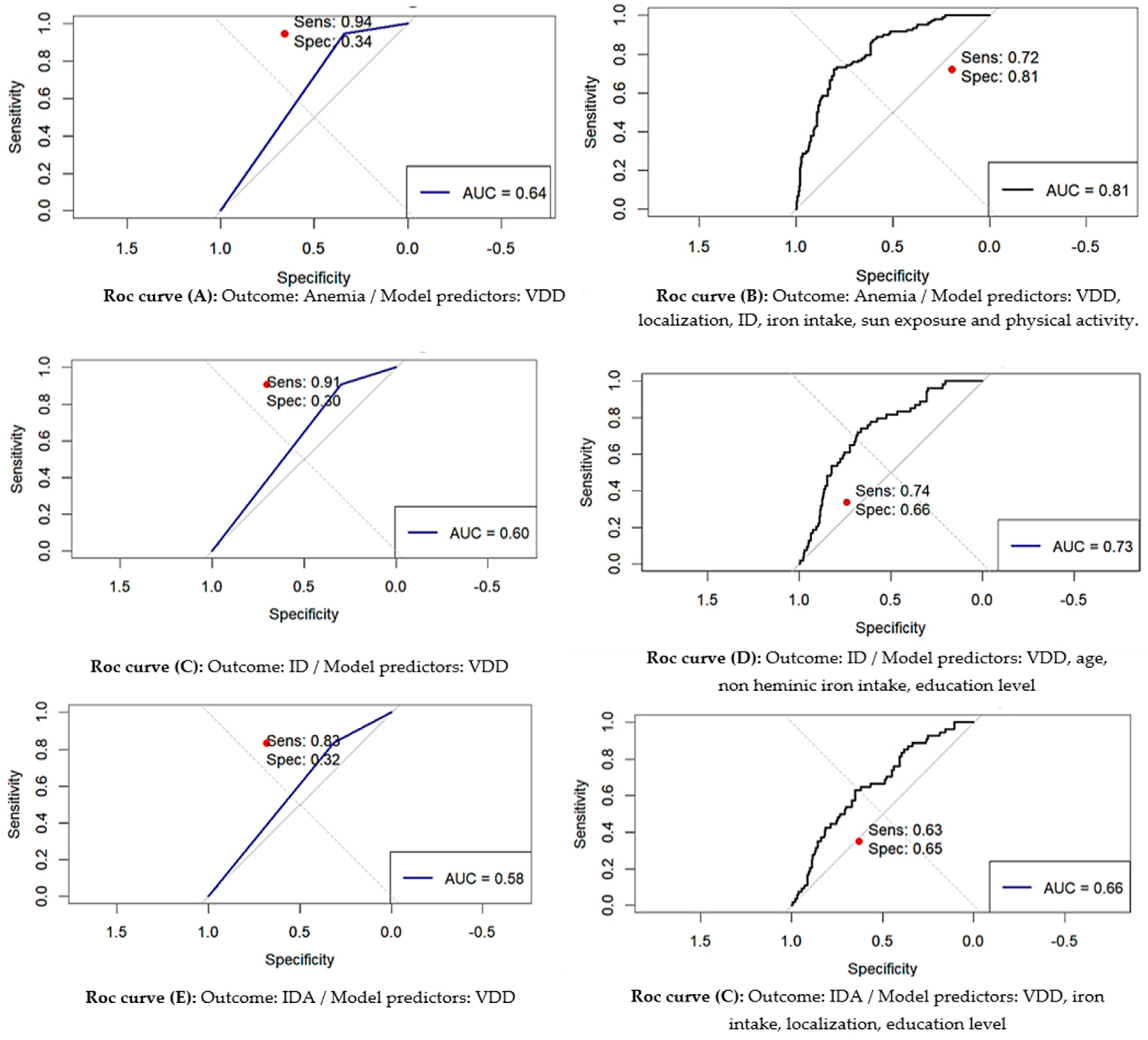

Table 1.
Characteristics of study participants by serum 25-OH) D3 and anemia status.
| Characteristics | All participant (n=463) |
Anemic (n=108) |
Non anemic (n =355) |
p-value1 |
|---|---|---|---|---|
| Median (IQR) or n (%) | ||||
| Anemia status(HB<12g/dl) | 463 (100) | 108(23.3) | 355(76.6) | <0.001 |
| Socio-demographic characteristics; | ||||
| Age, years | 29.0(11.0) | 28.0(10.0) | 29.0(11.0) | 0.639 |
| Education Illiterate ≤10 years (secondary-college) ≥11years(university or higher ) |
84(18.1) 222(47.9) 157(33.9) |
20(18.5) 56(51.9) 32(29.6) |
64(18.0) 166(46.8) 125(35.2) |
0.259 |
| Marital status Married Unmarried |
292(63.1) 171(36.9) |
65(60.2) 43(39.8) |
227(63.9) 128(36.1) |
0.479 |
| Employment Yes No |
201(43.4) 262(56.6) |
44(40.7) 64(59.3) |
157(44.2) 198(55.8) |
0.522 |
| Localization Urban Rural |
299(64.6) 164(35.4) |
60(55.6) 48(44.4) |
239(67.3) 116(32.7) |
0.025 |
| Anthropometric measures; BMI, Kg/m2 |
26.5(6.4) |
27.6(7.0) |
25.8(6.9) |
0.001 |
| BMI classification Underweight(<18kg/m2) Normal(<25kg/m2) Overweight (25 to<30 kg/m2) Obesity (≥30kg/m2) |
6(1.3) 173(37.4) 176(38.0) 108(23.3) |
1(0.9) 29(26.9) 43(39.8) 35(32.4) |
5(1.4) 144(40.6) 133(37.5) 73(20.6) |
0.024 |
| Lifestyle factors; PAC score, MET min/week |
1597.6(1892.4) | 1358.4(1178.8) |
1778.2(1765.0) |
<0.0001 |
| PAC levels (%) Low Moderate High |
53(11.5) 373(80.7) 36(7.8) |
29(12.3) 75(86.4) 3(2.8) |
24(6.8) 298(83.9) 33(9.3) |
<0.0001 |
| Dietary intake Energy, Kcal/day |
1678.4(651.3) |
1748.1(758.3) |
1652.6(596.8) |
0.295 |
| Vitamin D intake, µg/day | 2.7(2.74) | 2.3(2.3) | 2.8(2.76) | 0.035 |
| Vitamin D intake categories; Low (<5 µg /day) Adequate (≥5 µg /day) |
376(81.2) 87(18.8) |
91(84.3) 17(15.7) |
285(80.3) 70(19.7) |
0.352 |
| Iron intake, mg/day | 11.4(6.1) | 9.2(6.4) |
11.5(5.1) | 0.011 |
| Iron intake categories; Low (<(58.8 mg /day) Adequate (≥58.8 mg /day) |
463(100) 0(0.0) |
108(23.3) 0(0.0) |
355(76.7) 0(0.0) |
- |
| Heminic iron intake, mg/day | 0.5(0.2) | 0.4(0.3) | 0.5(0.2) | 0.051 |
| Non-Heminic iron intake, mg/day | 11.0(5.3) | 8.4(6.5) |
10.1(5.1) |
0.012 |
| Sun exposure behaviors; Sunscore (SES), median (IQR) Sunscore categories (%) Insufficient-Moderate Sufficient-High |
15.5(8.5) 247(53.3) 216(46.7) |
14.4(6.9) 60(55.6) 48(44.4) |
15.9(10.5) 156(43.9) 199(56.1) |
0.060 0.034 |
| Saison (%) Summer-spring Autun-winther |
281(60.69) 182 (39.30) |
72 (15.55%) 36 (7.78%) |
209 (45.14%) 146 (31.53%) |
0.180 |
Abbreviations; IQR: interquartile range, PAC: physical activity, SES: sun exposure score. 1Kruskal–Wallis test was used to compare for continuous variables and χ2 test or fisher’s exact test were used to compare qualitative variables. Significant level, p<0.05.
Table 2.
Distribution of participants biochemical parameters in the study sample by serum concentration of 25(OH) D3 (ng/ml) cut-off points.
Table 2.
Distribution of participants biochemical parameters in the study sample by serum concentration of 25(OH) D3 (ng/ml) cut-off points.
| Parameters | All participant (n=463) |
25(OH)D (ng/ml) cut-off points | P-value 1 | ||
|---|---|---|---|---|---|
| 20 (n=334) |
20-30 (n=82) |
>30 (n=47) |
|||
| Median (IQR) or n(%) | |||||
|
25(OH)D (ng/mL) Cut-off points, <12ng/ml 12-20ng/ml 20-30ng/ml >30ng/ml |
14.4(10.8) 99(29.7) 334(72.1) 82(17.1) 47(10.2) |
11.7(5.6) | 24.3(4.7) | 34.9(12.2) | <0.001 |
| BC parameters; | |||||
| Hemoglobin (g/dl) | 12.8(2.2) | 12.2(3.0) | 13.4(1.5) | 13.1(1.4) | <0.001 |
| Erythrocytes (M/ mm3) | 4.5(0.5) | 4.4(0.5) | 4.6(0.4) | 4.5(0.4) | 0.005 |
| Hematocrit (%) | 40.0(5.7) | 38.1(6.8) | 41.5(5.4) | 40.1(3.8) | <0.001 |
| MCV (fl) | 88.0(8.0) | 86.3(9.7) | 89.2(6.2) | 90.0(7.0) | <0.001 |
| MCH (pg Hb/erythrocytes ) | 28.0(3.4) | 27.3(4.8) | 29.0(2.1) | 29.0(2.0) | <0.001 |
| MCHC (g/dl) | 32.1(1.4) | 31.7(2.0) | 32.3(1.2) | 32.2(1.0) | <0.001 |
| White blood cells (/mm3)10-3 | 2.1(0.07) | 6.7 (2.6) | 6.4(3.1) | 6.6(2.8) | 0.643 |
|
Iron markers. Ferritin (µg/l) |
13.4 (20.8) |
11.4(15.5) |
14.8(29.4) |
32.8(44.9) |
0.002 |
| Iron (μg/dl) | 55.5(50.5) | 51.1(49.8) | 53.0(47.8) | 77.3(60.6) | 0.604 |
|
Renal fonction Plasma creatinine (mg/dl) |
0.7(0.1) |
0.6(0.1) |
0.7(0.1) |
0.7(0.1) |
0.231 |
| eGFR (ml/min/1.73 m2) | 196.9(96.16) | 184.5(93.7) | 215.4(94.0) | 204.8(86.3) | 0.010 |
|
Inflammatory marker CRP (mg/dl) |
3.75(4.57) |
3.8(4.3) |
3.1(4.9) |
4.1(6.7) |
0.366 |
| Inflammation present (CRP>5) Yes No |
101(21.8) 362(78.2) |
81(24.3) 253(75.7) |
12(14.6) 70(85.4) |
8(17.0) 39(17.0) |
0.118 |
Abbreviation; 25(OH) D: 25-hydroxyvitamin D, IQR: interquartile range, BC: blood count, MCV: Mean corpuscular volume, MCH: mean corpuscular hemoglobin, MCHC: mean corpuscular hemoglobin concentration, eGFR: estimated glomerular filtration rate, CRP: C-reactive protein. 1Kruskal–Wallis test was used to compare for continuous variables and χ2 test or fisher’s exact test were used to compare qualitative variables. Significant level p<0.05.
Table 3.
Anemia status, severity of anemia, and iron status according to 25(OH) D3 cut-off points.
| All Participant (n=463) |
25(OH)D (ng/ml) cut-off points | P-value1 | |||
|---|---|---|---|---|---|
| <20 (n=334) |
20-30 (n=82) |
>30 (n=47) |
|||
| n(%) | |||||
| Anemia status (HB<12mg/dl) Non anemic Anemic |
355 (76.7) 108(23.3) |
233(65.6) 101(93.5) |
46(13.0) 6(5.6) |
76(21.4) 1(11.0) |
<0.001 |
| Anemia severity (n=108) Milde to moderat(10.9<Hb<12g/dl) Severe (HB <8g/dl) |
101(93.51) 7(6.48) |
94(93.1) 7(100) |
6(5.6) 0(0.0) |
1(0.6) 0(0.0) |
0.771 |
| Iron deficiency No Yes |
331(71.5) 132(27.6) |
225(68.0) 109(82.6) |
43 (19.0) 19(14.4) |
63(13.0) 4(3.0) |
0.001 |
| Iron deficiency anemia No Yes |
409(88.3) 54(11.7) |
285(69.7) 49(90.7) |
77(18.8) 5(9.3) |
47(11.5) 0(0.0) |
0.003 |
Abbreviation; HB: hemoglobin 1 χ2 test or fisher’s exact test, significant level p<0.05.
Table 4.
Regression analysis for anemia, iron deficiency, and iron deficiency anemia according to vitamin D status.
Table 4.
Regression analysis for anemia, iron deficiency, and iron deficiency anemia according to vitamin D status.
| Unadjusted model | Adjusted model | |||||
|---|---|---|---|---|---|---|
| Β(SE) | OR (95% CI) | P-value | β(SE) | OR (95% CI) | P-value | |
| Outcome: Anemia | ||||||
|
Vitamin D status Sufficient-insufficient (>20 ng/mL) Deficient (<20 ng/mL) |
2.17(0.43) |
Reference 8.79(4.06,23.00) |
<0.001 | 1.97(0.45) |
Reference 7.17(3.19, 19.28) |
<0.001 |
| Physical activity intensity Moderate to high Low |
1.67(0.31) | Reference 5.35(2.88,9.91) |
<0.001 | 1.76(0.34) | Reference 5.80(2.96, 11.62) |
<0.001 |
| ID No Yes |
1.54 (0.23) |
Reference 4.70 (2.95, 7.49) |
<0.001 |
1.61(0.26) |
Reference 5.02(2.99,8.45) |
<0.001 |
| Localization Urbain Rural |
0.50 (0.22) |
Reference 1.64 ((1.06,2.55) |
0.026 |
0.57(0.25) |
Reference 1.77(1.07,2.94) |
0.021 |
| Sunscore categories (%): Sufficient to high SES Insufficient to moderate SES |
0.46 (0.22) |
Reference 1.59( 1.03, 2.46) |
0.034 |
0.31( 0.25) |
Reference 1.33(0.82,2.17) |
0.221 |
| Iron intake(mg/day) | -0.07(0.02) | 0.93 (0.88-0.98) | 0.008 | -0.05 (0.02) | 0.94 (0.88, 0.99) | 0.0419 |
| Outcome: Iron deficiency | ||||||
|
Vitamin D status Sufficient-insufficient (>20 ng/mL) |
Reference |
Reference |
||||
| Deficient (<20 ng/mL) | 0.75(0.25) | 2.12(1.28, 3.50) | 0.003 | 0.75(0.26 ) | 2.20(1.32, 3.77) | 0.007 |
| Age (years) | -0.04(0.01) | 0.95(0.92,0.98) | 0.009 |
-0.04(0.01) |
0.95(0.92,0.98) | 0.012 |
| Non heminic iron intake(mg/day) | -0.04(0.02) | 0.95(0.90,1.00) | 0.084 | -0.05(0.02) | 0.95(−1.10,1.00) | 0.037 |
| Education Illetrat Literate |
-0.38(0.18) |
Reference 0.67(0.46,0.97) |
0.037 |
-0.30(0.14) |
Reference 0.74(0.54,0.99) |
0.069 |
| Outcome: Iron deficiency anemia | ||||||
| Vitamin D status Sufficient -insufficient (>20ng/ml) |
Reference |
Reference |
||||
| Deficient (<20 ng/mL) | 1.42(0.48) |
4.16(1.62,10.71) |
0.003 | 1.41(0.48) | 4.10(1.73,12.08) | 0.004 |
| Iron intake (mg/day) | -0.08(0.03) | 0.92 (0.86, 0.98) | 0.013 | -0.08(0.03) | 0.91(0.85, 0.99) | 0.030 |
| Localization Rural Urban |
0.60(0.29) |
Reference 1.82(1.02,3.23) |
0.039 |
0.55(0.30) |
Reference 1.74(0.96, 3.15) |
0.084 |
| Education Illiterate Literate |
-0.397(0.20) |
Reference 0.67(0.44,1.00) |
0.052 |
-0.38(0.21) |
Reference 0.68(0.44,1.03) |
0.070 |
Table 5.
Summary of ROC Analysis for VDD and covariates predicting anemia, and iron status.
| Outcome | Predictors | AUC | 95% CI for AUC | p-value for AUC | Optimal Threshold | Youden Index | Optimal Sensitivity |
Optimal Specificity |
|---|---|---|---|---|---|---|---|---|
| Anemia | VDD | 0.643 | 0.610-0.676 | < 0.001 | 0.175 | 0.285 | 0.944 | 0.341 |
| VDD, localization, ID, iron intake and physical activity, sun exposure |
0.813 |
0.768-0.855 |
< 0.001 |
0.269 |
0.528 |
0.722 |
0.806 |
|
| ID | VDD | 0.575 | 0.535-0.616 | < 0.001 | 0.250 | 0.151 | 0.833 | 0.317 |
| VDD, age, non heminic iron intake, education level | 0.654 | 0.604-0.704 |
< 0.001 |
0.233 |
0.243 |
0.634 |
0.648 |
|
| IDA | VDD | 0.603 | 0.557-0.644 | < 0.001 | 0.093 | 0.206 | 0.907 | 0.298 |
| VDD, iron intake, localization, education level. | 0.712 | 0.643-0.776 | < 0.001 |
0.123 |
0.389 |
0.741 |
0.648 |
Abbreviations: VDD: Vitamin D deficiency, ID: iron deficiency, IDA: Iron deficiency anemia, AUC: Area under the curve, CI: confidence interval . Statistical significance, p < 0.05.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



