
Submitted:
02 September 2024
Posted:
03 September 2024
You are already at the latest version
Abstract
Despite the existing effective treatment methods, tuberculosis (TB) is the second most deadly infectious disease globally, its carriers in the latent and active phases accounting for more than 20% of the world population. An effective method to control TB and reduce the mortality is regular population screening and diagnosis of the latent form of TB in order to take preventive and curative measures. Numerous methods allow diagnosing TB and directly detecting Mycobacterium tuberculosis (M.tb) biomarkers, including M.tb DNA, proteins, and specific metabolites, as well as antibodies produced by the host immune system in response to M.tb. PCR, ELISA, immunofluorescence and immunochemical analyses, flow cytometry, and other methods allow the detection of M.tb biomarkers or the host immune response to M.tb by recording the optical signal of fluorescent or colorimetric dyes included in the diagnostic tools. Current research in biosensors is aimed at increasing the sensitivity of detection, which can be achieved by using brighter and more photostable optical tags containing fluorescent quantum dots. Here, we review current methods for detection of M.tb biomarkers using optical sensor systems, primarily quantum dot–based nanosensors, and summarize M.tb biomarkers whose detection can be made significantly more sensitive by using quantum dot–based nanosensors.
Keywords:
quantum dot
; nanosensor
; tuberculosis
; diagnostics
1. Introduction
Tuberculosis (TB) is an infectious disease caused by Mycobacterium tuberculosis and most often affecting the lungs. In 2022, there were 10.6 million TB cases worldwide, including 5.8 million men, 3.5 million women, and 1.3 million children; a total of 1.3 million people died from TB (including 167,000 people with concomitant HIV infection). Globally, TB is the second leading cause of death among infectious diseases after COVID-19, with death rates higher than those of AIDS [1]. TB can have particularly severe consequences for women, especially those of reproductive age and during pregnancy, and is one of the top five killers of women aged 20–59 years [2]. Recent estimates demonstrate that about 1.7 billion people are latently infected by M.tb [3]. At the same time, traditional diagnostic methods, such as chest X-ray and tuberculosis skin tests, do not have a sufficient level of sensitivity and specificity to reliably diagnose latent forms of TB [4], especially against the background of other diseases or pathological conditions [5]. The risk of progression of latent TB infection to the active form is estimated at 10% [6]. One of the health-related targets of the United Nations Sustainable Development Goals (SDGs) is to end the TB epidemic by 2030 [1]. To attain this goal, it is necessary not only to combat active forms of TB, but also to carry out prevention and therapy for patients with latent TB, which requires methods for diagnosing M.tb infection at the earliest stages.
2. Current Tuberculosis Diagnostic Methods
TB can be diagnosed in two ways: direct detection of M.tb in a clinical specimen or detection of the biomarkers associated with M.tb infection. Currently, numerous methods are widely used for TB diagnosis [7,8,9]. At the moment, there are four major groups of routine clinical methods used for this purpose: rapid molecular diagnostic tests, cultural methods, provocation tests, and diagnosis using optical methods. The characteristics of these groups of methods are presented in Table 1. With exception of skin tests, all the procedures are performed in vitro.
2.1. Molecular Diagnostic Tests
Polymerase chain reaction (PCR) is a molecular biology technique based on amplification and further analysis of specific DNA fragments. The amplification involves several cycles of heating and cooling, causing a DNA fragment to be duplicated many times to reach a detectable amount. PCR can detect the presence of a DNA fragment specific for M.tb [10]. This method is effective for early TB diagnosis when the number of the microorganisms is insufficient for detection by classical methods. PCR tests also allow analyzing drug resistance of specific M.tb strains. The PCR tests have strict requirements for laboratory room purity and personnel skills because their high sensitivity entails their downside related to the high risk of engaging contaminants in the reaction. PCR tests are suitable for detecting TB sepsis and disseminated TB but not for population screening for TB, where the results could be false negative.
LF-LAM is a lateral flow urine test for diagnosis of TB through the detection of lipoarabinomannan, a mycobacterial cell wall lipoglycan. A disadvantage of the LF-LAM method is its low sensitivity [13]. Because lateral flow tests are cheap and easy to perform, they are often used in diagnosis of TB by detecting IgG antibodies against TB-specific proteins in blood and serum samples [14]. Simultaneous detection of IgG and IgM antibodies has also been reported [25]. In this case, the test band contained a proprietary mixture of recombinant TB antigens that ensured a diagnostic sensitivity of 94.4% in a sample of 125 microbiologically or clinically diagnosed TB patients and a diagnostic specificity of 98.3% in a sample of 400 subjects who were healthy or had respiratory conditions other than TB.
Loop-mediated isothermal amplification (LAMP) uses special primers to amplify DNAs forming loop-shaped intermediates of different sizes, which can be detected using fluorescence measurements or agarose gel electrophoresis [26]. WHO recommends the use of TB-LAMP as a replacement for microscopy for the diagnosis of pulmonary TB [42].
Xpert MTB/RIF Ultra is an improved version of the Xpert MTB/RIF test [28,29]. Xpert MTB/RIF Ultra (in vitro) and Truenat can also identify mutations of the rpoB gene associated with rifampicin resistance [12,28,29,30]. Xpert MTB/RIF Ultra and Truenat have a higher sensitivity and a shorter time of analysis than conventional PCR tests.
Serological tests detecting antibodies against specific protein antigens of the recombinant M.tb complex have a high specificity but variable sensitivity [14]. The control of multiple M.tb complex antigens increases the sensitivity [14]. It should be pointed out that these methods may give false positive results because specific antibodies can occur in the human body for a long time after recovery from TB.
2.2. Tuberculosis Tests Based on T-Cell Analysis
Interferon-gamma release assay (IGRA) is a group of laboratory tests that evaluate the release of interferon-gamma (INF-γ) by human immune blood cells (T cells) and are performed in vitro [15]. There are two different types of blood tests based on this principle approved by FDA: QuantiFERON-TB Gold Plus (QFT) and T-SPOT.TB (T-SPOT). The QFT test is a whole-blood-based enzyme-linked immunosorbent assay (ELISA) measuring the amount of IFN-γ produced in response to two M.tb antigens (ESAT-6 and CFP-10). The T-SPOT test measures the number of T cells that produce INF-γ after stimulation with ESAT-6 and CFP-10. These methods may give false positive results because T cells have a long memory of an M.tb invasion that might have occurred a long time ago.
2.3. Cultural Methods
Cultural method remains the gold standard of TB diagnosis confirmation. They consist in inoculation of biological material on solid or liquid differential diagnostic nutrient media for growing mycobacterial colonies. In practice, several cultural methods are used: acid-fast mycobacteria (AFB) [16], BАСТЕС (with different parameters of MGIT, usually 460 and 960) [31], and BacT/ALERT 3D [18].
The AFB method involves examining human sputum or other samples stained to detect acid-fast bacteria. The latest experimental study using this method dates back to 1997 [31,32], which may be due to the extremely long time of analysis. The sample to be tested is inoculated into one or more vials with a specific growth medium and inserted into the instrument for incubation and periodic fluorescent reading. Each vial contains a chemical sensor detecting an increase in the amount of carbon dioxide produced by the growth of microorganisms. The instrument monitors the sensor every 10 min for an increase in its fluorescence, which is proportional to the amount of CO₂, a positive reading indicating the presence of viable microorganisms in the vial. BACTEC is a fully automated system not only for M.tb detection, but also for the analysis of M.tb sensitivity to all the first-line drugs, including pyrazinamide. BACTEC is a reference method with high sensitivity and specificity, but it takes about 10 days to obtain the result [33]. BacT/ALERT 3D allows automated monitoring the culture medium to detect the growth of microorganisms via monitoring CO2 release by an increase in reflectance. It has a high sensitivity with a shorter culturing time. BacT and BACTEC have similar operating principles but differ in the details of technology and design.
The key limitation of these methods is a too long time of analysis.
2.4. Skin Tests
In vivo tuberculin skin tests are based on provocation of the body immune response to TB-associated molecules [19]. For example, the Mantoux test uses a tuberculin solution administered via intradermal injection. All these tests suffer from frequent false positive and false negative results. The point is that the immune system responds to tuberculin if there are mycobacteria in the body, and the majority of people receive the bacteria in the form of the BCG vaccine back in the maternity hospital. Recently, WHO included Diaskintest, which is an advanced and more accurate variant of the Mantoux tuberculin test [34], into the list of recommended TB skin tests.
2.5. Tests Based on Mycobacterium Staining
Staining methods identify acid-fast mycobacteria, actinomycetes, and other acid-fast microorganisms by means of their staining and then analyzing using optical microscopy. These methods differ in the staining solution, which determines the sensitivity and specificity of analysis. The weak point of this group of TB tests is a complex procedure of analysis that requires considerable time and highly skilled personnel.
2.6. Other Methods
Chest X-rays are commonly used in the TB diagnosis. They can help identify abnormalities in the lungs that may be indicative of TB infection, such as nodules, cavities, or infiltrates. However, it should be noted that chest X-rays alone cannot definitively diagnose TB.
Matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS) is based on an ionization technique that allows the ionization of biological macromolecules, such as peptides, proteins, DNA, oligonucleotides, and lipopolysaccharides, in the presence of a special matrix under laser irradiation [35]. Wang et al. [36] have evaluated MALDI-TOF MS as a means of M.tb nucleic acid detection for rapid diagnosis of TB and drug resistance. The effectiveness of the MALDI-TOF MS can be improved by using the protocol of destruction of mycobacterium cells and protein extraction [37].
Liquid chromatography–tandem mass spectropmetry (LC-MS/MS) is based on coupling mass spectrometers in series to analyze complex mixtures [38]. For example, liquid–liquid extraction and LC-MS analysis were used to determine the pretomanid concentrations in 40 mL of human plasma [39]. The method was proven to be reliable and reproducible for pharmacokinetic analysis of samples in a clinical trial involving TB patients. Another study used the LC-MS technique to detect specific M.tb peptides in mouse blood serum. Sixty-five peptides from four recombinant M.tb proteins were identified in the mouse blood [40]. This method is not used to directly detect M.tb, but it is useful in the monitoring of TB treatment [41].
Scrutiny of the above TB diagnostic methods shows that all of them have disadvantages and limitations. Therefore, development of new simple and effective methods of TB diagnosis is an urgent task.
3. Quantum Dot–Based Nanosensors for M. Tuberculosis Detection and Tuberculosis Diagnosis
Most of the detection methods discussed above are in some way or another related to the detection of an optical signal, be it molecular detection methods based on PCR with fluorescent probes, lateral flow tests that use colloidal gold nanoparticles or colored latex microparticles, methods based on ELISA and ELISPOT tests, tests for CO2 accumulation, or specific M.tb staining. Traditionally, all commercial products for MTB detection and TB diagnosis use organic fluorescent or colorimetric dyes, which have recently been increasingly replaced with fluorescent quantum dots (QDs) [42].
QDs are inorganic semiconductor nanocrystals 2–10 nm in size with a high fluorescence quantum yield due to a high molar absorption coefficient and a high efficiency of internal conversion of the absorbed photon energy into fluorescence [43]. Another benefit of QDs is their extremely long luminescence lifetime compared to fluorescent biomolecules. This allows time-resolved detection with an increased useful signal-to-noise ratio, which enhances the detection sensitivity [44,45]. The narrow emission peak and wide absorption spectrum make it possible to excite QDs of different colors with a single broad-spectrum source and perform multiplexed measurements. QDs usually have a semiconductor core (CdSe, CdS, CdTe, InP, InAs, AgInS2, CuInS2, PbSe, etc.), often coated with a shell to passivate the surface trap states and protect the core from aggressive environment and photo-oxidative degradation, as well as to meet biosafety requirements [46,47,48]. The typical structure of QD-based nanosensors is shown in Figure 2.
An ideal QD-based fluorescence nanosensor should combine a bright fluorescent label and a highly specific recognition ligand or capture molecule [49]. This capture molecule can be a protein (e.g., an antibody or recombinant antigen), peptide, oligonucleotide, etc. [43,48,49]. After the QD-based nanosensor has bound the target biomolecule, the QD fluorescence signal can be detected and quantified [52,53,54]. Numerous methods for covalent and noncovalent conjugation of ligands to the QD surface (e.g., electrostatic interaction and metal ion chelation) have been developed [42,55,56]. The possibility of using multiple QDs with different emission spectra enables simultaneous detection of several biomarkers, which increases the diagnostic accuracy [57,58,59].
A total of 28 articles retrieved by the keywords quantum dot, tuberculosis, and Mycobacterium tuberculosis and 43 articles retrieved by the keywords quantum dot and tuberculosis have been found in the PubMed database. Of these publications, 37 dealt with TB diagnosis using QD-based nanosensors, 18 of them published in the past five years (including six reviews published in the past four years [7,8,9,60,61,62,63]). The number of these publications by year is shown in Figure 3. In total, 116 articles are cited in this review, 95 of them published in the past 10 years.
The methods of M.tb detection and TB diagnosis using QD-based nanosensors are shown in Table 2.
Not all of the biomarkers described above are completely specific, because their occurrence may be related to concomitant diseases, body conditions, etc. Currently, there is no biomarker or combination of biomarkers that allows diagnosing active forms of TB with an accuracy close to 100%. Thus, the search for a combination of biomarkers with a high specificity is an urgent task. New potential M.tb biomarkers that can be detected by new QD-based fluorescent nanosensors are listed in Table 3.
Host transcript RNA/DNA signatures is a group of biomarkers associated with the host gene expression in response to M.tb infection. For some markers listed in Table 3, there are suitable QD-based nanosensors presented in Table 2 (GBP2 [64,87], GBP5 [64,87], GBP6 [64,87], IS6110 gene [77], rpoB531 gene [72], and katG315gene [72]). Regarding PRDM1, it is also associated with lymphoma [116]. To date, there is no QD-based nanosensor for arginase 1 detection. The group of acids and their derivatives consists of two important TB biomarkers: MN [81] and MAs [69,70]. For both markers, sets of QDs and conjugates that can be used for TB diagnosis are shown in Table 2. Three most common enzymes can be used for TB diagnosis: MNAzymes, ADA, and KatG. To date, QDs functionalized with MNAzymes [68] have been proposed as TB diagnostic agents. Regarding KatGs, there are methods for detecting the encoding genes, but there are no biosensors for detecting the enzymes themselves. No nanosensors for ADA detection have been reported to date.
The groups of specific surface protein and mycobacterial antigen biomarkers can be pooled because both include specific proteins and other antigens associated with M.tb. At the moment, three main protein antigens from this group have been studied for TB diagnosis using nanosensors: CFP-10, ESAT-6, and Ag85B [71,78,80,86].
4. Summary and Outlook
TB remains a major global health problem, with millions of new cases and significant mortality every year. Early and accurate diagnosis is crucial for effective treatment and control of this disease. Traditional methods of TB diagnosis, such as PCR tests, immunofluorescence and immunochemical analyses, flow cytometry, cell culture tests, and microscopic analysis can be improved by the use of optical tags based on fluorescent QDs. Some alternative nanomaterials, such as other nanoparticles [114,115,116], graphene [88], and graphene-like 2D-materials (trans-graphenes) [113,117,118,119,120,121,122], can also be used for the development of nanosensors solving similar tasks and based on the same physical principles. QDs have already established themselves as promising constituent elements of biosensors providing increased sensitivity and specificity of detection than routinely used assays and allowing the development of multiplexed assays for early, more detailed detection of M.tb and diagnosis of TB. Despite the undoubtedly high potential, several challenges need to be addressed for enabling widespread use of QD-based nanosensors for TB diagnosis, such as the search for new suitable conjugates and available highly specific biomarkers, standardization and validation of diagnostic protocols, and advanced cost- and time-reducing solutions. However, the data reviewed here show that the unique properties of QDs make the QD-based nanosensors promising candidates for biosensing applications, including in vitro M.tb diagnosis. The use of QDs makes it possible to increase the sensitivity and speed of analysis, which is important for point-of-care diagnosis of TB and wider coverage of diagnostic procedures. The possibility of excitation of QD fluorescence in a wide range of wavelengths and a long fluorescence lifetime allow reducing the requirements for fluorescence detectors and, hence, the cost of their manufacture, as well as designing more compact devices for reading the fluorescent signal. This could ensure their wider use of these tools in diagnostic practice, thus decreasing the morbidity and mortality from TB.
Author Contributions
Conceptualization, Yu.V.K. and I.R.N.; writing—original draft preparation, V.V.N and P.M.S.; writing—review and editing, T.B.L, A.S.A., E.B.; data validation and general revision, P.M.S.; supervision, I.R.N. and Yu.V.K.; funding acquisition, Yu.V.K. and I.R.N. All authors have read and agreed to the published version of the manuscript.
Funding
The part of the study related to design of the quantum sensors was funded by the Russian Science Foundation (RSF) grant number 21-79-30048. The part of the study related to the quantum sensors biomedical applications was funded by the RSF grant number 23-75-30016.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
We thank Vladimir Ushakov for proofreading the manuscript and Maria Ya. Stoyanova for assistance in filling in the data on the standard methods for tuberculosis diagnosis.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results. The company Life Improvement by Future Technologies (LIFT) Center had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- The Global Health Observatory: SDG Target 3.3 Communicable diseases. Available online: https://Www.Who.Int/Data/Gho/Data/Themes/Topics/Sdg-Target-3_3-Communicable-Diseases.
- Tuberculosis in Women, World Health Organization, Fact Sheet October 2016. Available online: http://Www.Who.Int/Tb/Areas-of-Work/Population-Groups/Gender/En/.
- Chakaya, J.; Khan, M.; Ntoumi, F.; Aklillu, E.; Fatima, R.; Mwaba, P.; Kapata, N.; Mfinanga, S.; Hasnain, S.E.; Katoto, P.D.M.C.; et al. Global Tuberculosis Report 2020 – Reflections on the global TB burden, treatment and prevention efforts. Int. J. Infect. Dis. 2021, 113, S7–S12. [CrossRef]
- Maddineni, M.; Panda, M. Pulmonary tuberculosis in a young pregnant female: Challenges in diagnosis and management. Infect. Dis. Obst. Gynecol. 2008, 2008, 1–5. [CrossRef]
- Liu, Q.; Yang, X.; Wen, J.; Tang, D.; Qi, M.; He, J. Host factors associated with false negative results in an interferon-γ release assay in adults with active tuberculosis. Heliyon 2023, 9, e22900. [CrossRef]
- World Health Organization. Guidelines on the Management of Latent Tuberculosis Infection. World Health Organization, 2015.
- Yang, X.; Fan, S.; Ma, Y.; Chen, H.; Xu, J.-F.; Pi, J.; Wang, W.; Chen, G. Current progress of functional nanobiosensors for potential tuberculosis diagnosis: The novel way for TB control? Front. Bioeng. Biotechnol. 2022, 10, 1036678. [CrossRef]
- Mukherjee, S.; Perveen, S.; Negi, A.; Sharma, R. Evolution of tuberculosis diagnostics: From molecular strategies to nanodiagnostics. Tuberculosis 2023, 140, 102340. [CrossRef]
- Gupta, A.K.; Singh, A.; Singh, S. Diagnosis of tuberculosis: Nanodiagnostics approaches. In NanoBioMedicine; Saxena, S.K., Khurana, S.M.P., Eds.; Springer: Singapore, 2020; pp. 261–283 ISBN 978-981-329-897-2.
- Jin, T.; Fei, B.; Zhang, Y.; He, X. The diagnostic value of polymerase chain reaction for Mycobacterium tuberculosis to distinguish intestinal tuberculosis from Crohn’s disease: A meta-analysis. Saudi J Gastroenterol. 2017, 23, 3. [CrossRef]
- Steingart, K.R.; Schiller, I.; Horne, D.J.; Pai, M.; Boehme, C.C.; Dendukuri, N. Xpert MTB/RIF assay for pulmonary tuberculosis and rifampicin resistance in adults. In: Cochrane Database of Systematic Reviews 2014. [CrossRef]
- Ssengooba, W.; Katamba, A.; Sserubiri, J.; Semugenze, D.; Nyombi, A.; Byaruhanga, R.; Turyahabwe, S.; Joloba, M.L. Performance evaluation of Truenat MTB and Truenat MTB-RIF DX assays in comparison to Gene XPERT MTB/RIF Ultra for the diagnosis of pulmonary tuberculosis in Uganda. BMC Infect. Dis. 2024, 24, 190. [CrossRef]
- Bjerrum, S.; Schiller, I.; Dendukuri, N.; Kohli, M.; Nathavitharana, R.R.; Zwerling, A.A.; Denkinger, C.M.; Steingart, K.R.; Shah, M. Lateral flow urine lipoarabinomannan assay for detecting active tuberculosis in people living with HIV. In: Cochrane Database of Systematic Reviews 2019, 2019. [CrossRef]
- Manga, S.; Perales, R.; Reaño, M.; D’Ambrosio, L.; Migliori, G.B.; Amicosante, M. Performance of a lateral flow immunochromatography test for the rapid diagnosis of active tuberculosis in a large multicentre study in areas with different clinical settings and tuberculosis exposure levels. J. Thorac. Dis. 2016, 8, 3307–3313. [CrossRef]
- Chen, H.; Nakagawa, A.; Takamori, M.; Abe, S.; Ueno, D.; Horita, N.; Kato, S.; Seki, N. Diagnostic accuracy of the interferon-gamma release assay in acquired immunodeficiency syndrome patients with suspected tuberculosis infection: A meta-analysis. Infection 2022, 50, 597–606. [CrossRef]
- Tortoli, E.; Mandler, F.; Tronci, M.; Penati, V.; Sbaraglia, G.; Costa, D.; Montini, G.; Predominato, M.; Riva, R.; Passerini Tosi, C.; et al. Multicenter evaluation of mycobacteria growth indicator tube (MGIT) compared with the BACTEC radiometric method, BBL biphasic growth medium and Löwenstein—Jensen medium. Clin. Microbiol. Infect. 1997, 3, 468–473. [CrossRef]
- Cruciani, M.; Scarparo, C.; Malena, M.; Bosco, O.; Serpelloni, G.; Mengoli, C. Meta-analysis of BACTEC MGIT 960 and BACTEC 460 TB, with or without solid media, for detection of mycobacteria. J. Clin. Microbiol. 2004, 42, 2321–2325. [CrossRef]
- Martinez, M.R.; Sardiñas, M.; Garcia, G.; Mederos, L.M.; Díaz, R. Evaluation of BacT/ALERT 3D system for mycobacteria isolates. J. Tuberc. Res. 2014, 2, 59–64. [CrossRef]
- Rose, D.N.; Schechter, C.B.; Adler, J.J. Interpretation of the tuberculin skin test. J. Gen. Intern. Med. 1995, 10, 635–642. [CrossRef]
- Abdelaziz, M.M.; Bakr, W.M.K.; Hussien, S.M.; Amine, A.E.K. Diagnosis of pulmonary tuberculosis using Ziehl–Neelsen stain or cold staining techniques? J. Egypt. Pub. Health Assoc. 2016, 91, 39–43. [CrossRef]
- Cattamanchi, A.; Davis, J.L.; Worodria, W.; den Boon, S.; Yoo, S.; Matovu, J.; Kiidha, J.; Nankya, F.; Kyeyune, R.; Byanyima, P.; et al. Sensitivity and specificity of fluorescence microscopy for diagnosing pulmonary tuberculosis in a high HIV prevalence setting. Int. J. Tuberc. Lung Dis. 2009, 13, 1130–1136.
- Pinto, L.M.; Pai, M.; Dheda, K.; Schwartzman, K.; Menzies, D.; Steingart, K.R. Scoring systems using chest radiographic features for the diagnosis of pulmonary tuberculosis in adults: A systematic review. Eur. Respir. J. 2013, 42, 480–494. [CrossRef]
- Wang, Y.; Xu, Q.; Xu, B.; Lin, Y.; Yang, X.; Tong, J.; Huang, C. Clinical performance of nucleotide MALDI-TOF-MS in the rapid diagnosis of pulmonary tuberculosis and drug resistance. Tuberculosis 2023, 143, 102411. [CrossRef]
- Metcalfe, J.; Bacchetti, P.; Esmail, A.; Reckers, A.; Aguilar, D.; Wen, A.; Huo, S.; Muyindike, W.R.; Hahn, J.A.; Dheda, K.; et al. Diagnostic accuracy of a liquid chromatography-tandem mass spectrometry assay in small hair samples for rifampin-resistant tuberculosis drug concentrations in a routine care setting. BMC Infect. Dis. 2021, 21, 99. [CrossRef]
- Nsubuga, G.; Kennedy, S.; Rani, Y.; Hafiz, Z.; Kim, S.; Ruhwald, M.; Alland, D.; Ellner, J.; Joloba, M.; Dorman, S.E.; et al. Diagnostic accuracy of the NOVA tuberculosis total antibody rapid test for detection of pulmonary tuberculosis and infection with Mycobacterium tuberculosis. J. Clin. Tuberc. Other Mycobacter. Dis. 2023, 31, 100362. [CrossRef]
- Sharma, G.; Tewari, R.; Dhatwalia, S.K.; Yadav, R.; Behera, D.; Sethi, S. A loop-mediated isothermal amplification assay for the diagnosis of pulmonary tuberculosis. Lett. Appl. Microbiol. 2019, 68, 219–225. [CrossRef]
- The Use of Loop-Mediated Isothermal Amplification (TB-LAMP) for the Diagnosis of Pulmonary Tuberculosis: Policy Guidance; WHO Guidelines Approved by the Guidelines Review Committee; World Health Organization: Geneva, 2016; ISBN 978-92-4-151118-6.
- Horne, D.J.; Kohli, M.; Zifodya, J.S.; Schiller, I.; Dendukuri, N.; Tollefson, D.; Schumacher, S.G.; Ochodo, E.A.; Pai, M.; Steingart, K.R. Xpert MTB/RIF and Xpert MTB/RIF Ultra for pulmonary tuberculosis and rifampicin resistance in adults. In: Cochrane Database of Systematic Reviews 2019. [CrossRef]
- Aainouss, A.; Momen, Gh.; Belghiti, A.; Bennani, K.; Lamaammal, A.; Chetioui, F.; Messaoudi, M.; Blaghen, M.; Mouslim, J.; Khyatti, M.; et al. Performance of GeneXpert MTB/RIF in the diagnosis of extrapulmonary tuberculosis in Morocco. Rus. J. Infect. Immun. 2021, 12, 78–84. [CrossRef]
- Ngangue, Y.R.; Mbuli, C.; Neh, A.; Nshom, E.; Koudjou, A.; Palmer, D.; Ndi, N.N.; Qin, Z.Z.; Creswell, J.; Mbassa, V.; et al. Diagnostic accuracy of the Truenat MTB Plus assay and comparison with the Xpert MTB/RIF assay to detect tuberculosis among hospital outpatients in Cameroon. J. Clin. Microbiol. 2022, 60, e00155-22. [CrossRef]
- Sevastyanova, E.V.; Smirnova, T.G.; Larionova, E.E.; Chernousova, L.N. Detection of mycobacteria by culture inoculation. Liquid media and automated systems. Bulle. TsNIIT 2020, 88–95. [CrossRef]
- Lee, H.S.; Park, K.U.; Park, J.O.; Chang, H.E.; Song, J.; Choe, G. Rapid, sensitive, and specific detection of Mycobacterium tuberculosis complex by real-time PCR on paraffin-embedded human tissues. J. Mol. Diagn. 2011, 13, 390–394. [CrossRef]
- Itani, L.Y.; Cherry, M.A.; Araj, G.F. Efficacy of BACTEC TB in the rapid confirmatory diagnosis of mycobacterial infections: A Lebanese tertiary care center experience. J. Med. Liban. 2005, 53, 208–212.
- Campelo, T.A.; Cardoso De Sousa, P.R.; Nogueira, L.D.L.; Frota, C.C.; Zuquim Antas, P.R. Revisiting the methods for detecting mycobacterium tuberculosis: What has the new millennium brought thus far? Access Microbio. 2021, 3. [CrossRef]
- Szewczyk, R.; Kowalski, K.; Janiszewska-Drobinska, B.; Druszczyńska, M. Rapid method for Mycobacterium tuberculosis identification using electrospray ionization tandem mass spectrometry analysis of mycolic acids. Diagn. Microbiol. Infect. Dis. 2013, 76, 298–305. [CrossRef]
- El Khéchine, A.; Couderc, C.; Flaudrops, C.; Raoult, D.; Drancourt, M. Matrix-assisted laser desorption/ionization time-of-flight mass spectrometry identification of mycobacteria in routine clinical practice. PLoS ONE 2011, 6, e24720. [CrossRef]
- Bacanelli, G.; Araujo, F.R.; Verbisck, N.V. Improved MALDI-TOF MS identification of Mycobacterium tuberculosis by use of an enhanced cell disruption protocol. Microorganisms 2023, 11, 1692. [CrossRef]
- Thomas, S.N.; French, D.; Jannetto, P.J.; Rappold, B.A.; Clarke, W.A. Liquid chromatography–tandem mass spectrometry for clinical diagnostics. Na.t Rev. Meth. Primers 2022, 2, 96. [CrossRef]
- Malo, A.; Kellermann, T.; Ignatius, E.H.; Dooley, K.E.; Dawson, R.; Joubert, A.; Norman, J.; Castel, S.; Wiesner, L. A Validated liquid chromatography tandem mass spectrometry assay for the analysis of pretomanid in plasma samples from pulmonary tuberculosis patients. J. Pharmac. Biomed. Anal. 2021, 195, 113885. [CrossRef]
- Chen, H.; Li, S.; Zhao, W.; Deng, J.; Yan, Z.; Zhang, T.; Wen, S.A.; Guo, H.; Li, L.; Yuan, J.; et al. A peptidomic approach to identify novel antigen biomarkers for the diagnosis of tuberculosis. Infect. Dis. Rep. 2022, 15, 4617–4626. [CrossRef]
- Chen, X.; Song, B.; Jiang, H.; Yu, K.; Zhong, D. A liquid chromatography/tandem mass spectrometry method for the simultaneous quantification of isoniazid and ethambutol in human plasma. Rapid Commun. Mass Spectrom. 2005, 19, 2591–2596. [CrossRef]
- He, X.; Ma, N. An overview of recent advances in quantum dots for biomedical applications. Colloids Surf. B Biointerfaces 2014, 124, 118–131. [CrossRef]
- Medintz, I.L.; Uyeda, H.T.; Goldman, E.R.; Mattoussi, H. Quantum dot bioconjugates for imaging, labelling and sensing. Nat. Mat. 2005, 4, 435–446. [CrossRef]
- Brkić, S. Applicability of quantum dots in biomedical science. In Ionizing Radiation Effects and Applications; Djezzar, B., Ed.; InTech, 2018. ISBN 978-953-51-3953-9.
- Samokhvalov, P.S.; Karaulov, A.V.; Nabiev, I.R. Control of the photoluminescence lifetime of quantum dots by engineering their shell structure. Opt. Spektrosc. 2023, 131, 1262–1267 [in Russian]. [CrossRef]
- Bilan, R.; Nabiev, I.; Sukhanova, A. quantum dot-based nanotools for bioimaging, diagnostics, and drug delivery. ChemBioChem 2016, 17, 2103–2114. [CrossRef]
- Sukhanova, A.; Ramos-Gomes, F.; Chames, P.; Sokolov, P.; Baty, D.; Alves, F.; Nabiev, I. Multiphoton deep-tissue imaging of micrometastases and disseminated cancer cells using conjugates of quantum dots and single-domain antibodies. In Multiplexed Imaging; Zamir, E., Ed.; Methods in Molecular Biology; Springer: New York, NY, 2021; Volume 2350, pp. 105–123 ISBN 978-1-07-161592-8.
- Sokolov, P.; Samokhvalov, P.; Sukhanova, A.; Nabiev, I. Biosensors based on inorganic composite fluorescent hydrogels. Nanomaterials 2023, 13, 1748. [CrossRef]
- Hafian, H.; Sukhanova, A.; Turini, M.; Chames, P.; Baty, D.; Pluot, M.; Cohen, J.H.M.; Nabiev, I.; Millot, J.-M. Multiphoton imaging of tumor biomarkers with conjugates of single-domain antibodies and quantum dots. Nanomedicine: NBM 2014, 10, 1701–1709. [CrossRef]
- Bilan, R.; Fleury, F.; Nabiev, I.; Sukhanova, A. Quantum dot surface chemistry and functionalization for cell targeting and imaging. Bioconjugate Chem. 2015, 26, 609–624. [CrossRef]
- Sukhanova, A.; Even-Desrumeaux, K.; Kisserli, A.; Tabary, T.; Reveil, B.; Millot, J.-M.; Chames, P.; Baty, D.; Artemyev, M.; Oleinikov, V.; et al. Oriented conjugates of single-domain antibodies and quantum dots: Toward a new generation of ultrasmall diagnostic nanoprobes. Nanomedicine: NBM 2012, 8, 516–525. [CrossRef]
- Lee, J.S.; Youn, Y.H.; Kwon, I.K.; Ko, N.R. Recent advances in quantum dots for biomedical applications. J. Pharmac. Invest. 2018, 48, 209–214. [CrossRef]
- Han, X.; Xu, K.; Taratula, O.; Farsad, K. Applications of nanoparticles in biomedical imaging. Nanoscale 2019, 11, 799–819. [CrossRef]
- Zhang, Y.; Cai, N.; Chan, V. Recent advances in silicon quantum dot-based fluorescent biosensors. Biosensors 2023, 13, 311. [CrossRef]
- Brazhnik, K.; Nabiev, I.; Sukhanova, A. Oriented conjugation of single-domain antibodies and quantum dots. In Quantum Dots: Applications in Biology; Fontes, A., Santos, B.S., Eds.; Methods in Molecular Biology; Springer: New York, NY, 2014; Volume 1199, pp. 129–140 ISBN 978-1-4939-1279-7.
- Brazhnik, K.; Nabiev, I.; Sukhanova, A. Advanced procedure for oriented conjugation of full-size antibodies with quantum dots. In Quantum Dots: Applications in Biology; Fontes, A., Santos, B.S., Eds.; Methods in Molecular Biology; Springer: New York, NY, 2014; Volume 1199, pp. 55–66 ISBN 978-1-4939-1279-7.
- Biju, V. Chemical modifications and bioconjugate reactions of nanomaterials for sensing, imaging, drug delivery and therapy. Chem. Soc. Rev. 2014, 43, 744–764. [CrossRef]
- Bilan, R.S.; Krivenkov, V.A.; Berestovoy, M.A.; Efimov, A.E.; Agapov, I.I.; Samokhvalov, P.S.; Nabiev, I.; Sukhanova, A. Engineering of optically encoded microbeads with FRET-free spatially separated quantum-dot layers for multiplexed assays. ChemPhysChem 2017, 18, 970–979. [CrossRef]
- Rousserie, G.; Sukhanova, A.; Even-Desrumeaux, K.; Fleury, F.; Chames, P.; Baty, D.; Oleinikov, V.; Pluot, M.; Cohen, J.H.M.; Nabiev, I. Semiconductor quantum dots for multiplexed bio-detection on solid-state microarrays. Crit. Rev. Oncol. Hematol. 2010, 74, 1–15. [CrossRef]
- Sarkar, L.H.; Kumari, S. Nanocarriers for Mycobacterium tuberculosis. J. Sci. Res. 2021, 65, 33–37. [CrossRef]
- El-Shabasy, R.M.; Zahran, M.; Ibrahim, A.H.; Maghraby, Y.R.; Nayel, M. Advances in the fabrication of potential nanomaterials for diagnosis and effective treatment of tuberculosis. Mater. Adv. 2024, 5, 1772–1782. [CrossRef]
- Ahmad, F.; Pandey, N.; Singh, K.; Ahmad, S.; Khubaib, M.; Sharma, R. Recent advances in nanocarrier based therapeutic and diagnostic approaches in tuberculosis. Prec. Nanomed. 2023, 6. [CrossRef]
- Pati, R.; Sahu, R.; Panda, J.; Sonawane, A. Encapsulation of zinc-rifampicin complex into transferrin-conjugated silver quantum-dots improves its antimycobacterial activity and stability and facilitates drug delivery into macrophages. Sci. Rep. 2016, 6, 24184. [CrossRef]
- Gliddon, H.D.; Howes, P.D.; Kaforou, M.; Levin, M.; Stevens, M.M. A nucleic acid strand displacement system for the multiplexed detection of tuberculosis-specific mRNA using quantum dots. Nanoscale 2016, 8, 10087–10095. [CrossRef]
- Huang, H.; Li, J.; Shi, S.; Yan, Y.; Zhang, M.; Wang, P.; Zeng, G.; Jiang, Z. Detection of interferon-gamma for latent tuberculosis diagnosis using an immunosensor based on CdS quantum dots coupled to magnetic beads as labels. Int. J. Electrochem. Sci. 2015, 10, 2580–2593. [CrossRef]
- Januarie, K.C.; Oranzie, M.; Feleni, U.; Iwuoha, E. Quantum dot amplified impedimetric aptasensor for interferon-gamma. Electrochim. Acta 2023, 463, 142825. [CrossRef]
- Zhou, B.; Zhu, M.; Hao, Y.; Yang, P. Potential-resolved electrochemiluminescence for simultaneous determination of triple latent tuberculosis infection markers. ACS Appl. Mater. Interfaces 2017, 9, 30536–30542. [CrossRef]
- Hu, O.; Li, Z.; Wu, J.; Tan, Y.; Chen, Z.; Tong, Y. A multicomponent nucleic acid enzyme-cleavable quantum dot nanobeacon for highly sensitive diagnosis of tuberculosis with the naked eye. ACS Sens. 2023, 8, 254–262. [CrossRef]
- Kabwe, K.P.; Nsibande, S.A.; Pilcher, L.A.; Forbes, P.B.C. Development of a mycolic acid-graphene quantum dot probe as a potential tuberculosis biosensor. Luminescence 2022, 37, 1881–1890. [CrossRef]
- Kabwe, K.P.; Nsibande, S.A.; Lemmer, Y.; Pilcher, L.A.; Forbes, P.B.C. Synthesis and characterisation of quantum dots coupled to mycolic acids as a water-soluble fluorescent probe for potential lateral flow detection of antibodies and diagnosis of tuberculosis. Luminescence 2022, 37, 278–289. [CrossRef]
- Zou, F.; Zhou, H.; Tan, T.V.; Kim, J.; Koh, K.; Lee, J. Dual-mode SERS-fluorescence immunoassay using graphene quantum dot labeling on one-dimensional aligned magnetoplasmonic nanoparticles. ACS Appl. Mater. Interfaces 2015, 7, 12168–12175. [CrossRef]
- Hu, O.; Li, Z.; He, Q.; Tong, Y.; Tan, Y.; Chen, Z. Fluorescence biosensor for one-step simultaneous detection of Mycobacterium tuberculosis multidrug-resistant genes using nanoCoTPyP and double quantum dots. Anal. Chem. 2022, 94, 7918–7927. [CrossRef]
- Shi, T.; Jiang, P.; Peng, W.; Meng, Y.; Ying, B.; Chen, P. Nucleic acid and nanomaterial synergistic amplification enables dual targets of ultrasensitive fluorescence quantification to improve the efficacy of clinical tuberculosis diagnosis. ACS Appl. Mater. Interfaces 2024, 16, 14510–14519. [CrossRef]
- Yang, H.; Qin, L.; Wang, Y.; Zhang, B.; Liu, Z.; Ma, H.; Lu, J.; Huang, X.; Shi, D.; Hu, Z. Detection of Mycobacterium tuberculosis based on H37Rv binding peptides using surface functionalized magnetic microspheres coupled with quantum dots—A Nano detection method for Mycobacterium tuberculosis. Int. J. Nanomed. 2014, 77. [CrossRef]
- Ma, H.; Hu, Z.; Wang, Y.; Qing, L.; Chen, H.; Lu, J.; Yang, H. [Methodology research and preliminary assessment of Mycobacterium tuberculosis detection by immunomagnetic beads combined with functionalized fluorescent quantum dots]. Zhonghua Jie He He Hu Xi Za Zhi (Chin. J. Tuberc. Resp. Dis.) 2013, 36, 100–105 [in Chinese].
- Shojaei, T.R.; Mohd Salleh, M.A.; Tabatabaei, M.; Ekrami, A.; Motallebi, R.; Rahmani-Cherati, T.; Hajalilou, A.; Jorfi, R. Development of sandwich-form biosensor to detect mycobacterium tuberculosis complex in clinical sputum specimens. Braz. J. Infect. Dis. 2014, 18, 600–608. [CrossRef]
- Liang, L.; Chen, M.; Tong, Y.; Tan, W.; Chen, Z. Detection of Mycobacterium tuberculosis IS6110 gene fragment by fluorescent biosensor based on FRET between two-dimensional metal-organic framework and quantum dots-labeled DNA probe. Anal. Chim. Acta 2021, 1186, 339090. [CrossRef]
- Kim, E.J.; Kim, E.B.; Lee, S.W.; Cheon, S.A.; Kim, H.-J.; Lee, J.; Lee, M.-K.; Ko, S.; Park, T.J. An easy and sensitive sandwich assay for detection of Mycobacterium tuberculosis Ag85B antigen using quantum dots and gold nanorods. Biosens. Bioelectron. 2017, 87, 150–156. [CrossRef]
- Huang, Z.; Huang, H.; Hu, J.; Xia, L.; Liu, X.; Qu, R.; Huang, X.; Yang, Y.; Wu, K.; Ma, R.; et al. A novel quantitative urine LAM Antigen strip for point-of-care tuberculosis diagnosis in non-HIV adults. J. Infect. 2024, 88, 194–198. [CrossRef]
- Tufa, L.T.; Oh, S.; Tran, V.T.; Kim, J.; Jeong, K.-J.; Park, T.J.; Kim, H.-J.; Lee, J. Electrochemical immunosensor using nanotriplex of graphene quantum dots, Fe3O4, and Ag nanoparticles for tuberculosis. Electrochim. Acta 2018, 290, 369–377. [CrossRef]
- Bhattacharyya, D.; Sarswat, P.K.; Free, M.L. Quantum dots and carbon dots based fluorescent sensors for TB biomarkers detection. Vacuum 2017, 146, 606–613. [CrossRef]
- He, Q.; Cai, S.; Wu, J.; Hu, O.; Liang, L.; Chen, Z. Determination of tuberculosis-related volatile organic biomarker methyl nicotinate in vapor using fluorescent assay based on quantum dots and cobalt-containing porphyrin nanosheets. Microchim. Acta 2022, 189, 108. [CrossRef]
- Gazouli, M.; Liandris, E.; Andreadou, M.; Sechi, L.A.; Masala, S.; Paccagnini, D.; Ikonomopoulos, J. Specific detection of unamplified mycobacterial DNA by use of fluorescent semiconductor quantum dots and magnetic beads. J. Clin. Microbiol. 2010, 48, 2830–2835. [CrossRef]
- Cimaglia, F.; Aliverti, A.; Chiesa, M.; Poltronieri, P.; De Lorenzis, E.; Santino, A.; Sechi, L.A. Quantum dots nanoparticle-based lateral flow assay for rapid detection of mycobacterium species using anti-FprA antibodies. Nanotechnol. Dev. 2012, 2, 5. [CrossRef]
- Jiang, X.; Zeng, H.; Duan, C.; Hu, Q.; Wu, Q.; Yu, Y.; Yang, X. One-pot synthesis of stable and functional hydrophilic CsPbBr3 perovskite quantum dots for “turn-on” fluorescence detection of Mycobacterium tuberculosis. Dalton Trans. 2022, 51, 3581–3589. [CrossRef]
- Mohd Bakhori, N.; Yusof, N.A.; Abdullah, J.; Wasoh, H.; Ab Rahman, S.K.; Abd Rahman, S.F. Surface enhanced CdSe/ZnS QD/SiNP electrochemical immunosensor for the detection of Mycobacterium tuberculosis by combination of CFP10-ESAT6 for better diagnostic specificity. Materials 2019, 13, 149. [CrossRef]
- Gliddon, H.D.; Kaforou, M.; Alikian, M.; Habgood-Coote, D.; Zhou, C.; Oni, T.; Anderson, S.T.; Brent, A.J.; Crampin, A.C.; Eley, B.; et al. Identification of reduced host transcriptomic signatures for tuberculosis disease and digital PCR-based validation and quantification. Front. Immunol. 2021, 12, 637164. [CrossRef]
- Boyle, D.S.; McNerney, R.; Teng Low, H.; Leader, B.T.; Pérez-Osorio, A.C.; Meyer, J.C.; O’Sullivan, D.M.; Brooks, D.G.; Piepenburg, O.; Forrest, M.S. Rapid detection of Mycobacterium tuberculosis by recombinase polymerase amplification. PLoS ONE 2014, 9, e103091. [CrossRef]
- Verma, S.; Dubey, A.; Singh, P.; Tewerson, S.; Sharma, D. Adenosine deaminase (ADA) level in tubercular pleural effusion. Lung India 2008, 25, 109. [CrossRef]
- DeVito, J.A.; Morris, S. Exploring the structure and function of the mycobacterial KatG protein using trans -dominant mutants. Antimicrob. Agents Chemother. 2003, 47, 188–195. [CrossRef]
- Clifford, V.; Tebruegge, M.; Zufferey, C.; Germano, S.; Forbes, B.; Cosentino, L.; Matchett, E.; McBryde, E.; Eisen, D.; Robins-Browne, R.; et al. Cytokine biomarkers for the diagnosis of tuberculosis infection and disease in adults in a low prevalence setting. Tuberculosis 2019, 114, 91–102. [CrossRef]
- Zhou, B.; Hao, Y.; Chen, S.; Yang, P. A Quartz crystal microbalance modified with antibody-coated silver nanoparticles acting as mass signal amplifiers for real-time monitoring of three latent tuberculosis infection biomarkers. Microchim. Acta 2019, 186, 212. [CrossRef]
- Parate, K.; Rangnekar, S.V.; Jing, D.; Mendivelso-Perez, D.L.; Ding, S.; Secor, E.B.; Smith, E.A.; Hostetter, J.M.; Hersam, M.C.; Claussen, J.C. Aerosol-jet-printed graphene immunosensor for label-free cytokine monitoring in serum. ACS Appl. Mater. Interfaces 2020, 12, 8592–8603. [CrossRef]
- Renshaw, P.S.; Panagiotidou, P.; Whelan, A.; Gordon, S.V.; Hewinson, R.G.; Williamson, R.A.; Carr, M.D. Conclusive evidence that the major T-cell antigens of the Mycobacterium tuberculosis complex ESAT-6 and CFP-10 form a tight, 1:1 complex and characterization of the structural properties of ESAT-6, CFP-10, and the ESAT-6·CFP-10 complex. Journal of Biological Chemistry 2002, 277, 21598–21603. [CrossRef]
- Welin, A.; Björnsdottir, H.; Winther, M.; Christenson, K.; Oprea, T.; Karlsson, A.; Forsman, H.; Dahlgren, C.; Bylund, J. CFP-10 from Mycobacterium tuberculosis selectively activates human neutrophils through a pertussis toxin-sensitive chemotactic receptor. Infect. Immun. 2015, 83, 205–213. [CrossRef]
- Chai, Q.; Wang, X.; Qiang, L.; Zhang, Y.; Ge, P.; Lu, Z.; Zhong, Y.; Li, B.; Wang, J.; Zhang, L.; et al. A Mycobacterium tuberculosis surface protein recruits ubiquitin to trigger host xenophagy. Nat. Commun. 2019, 10, 1973. [CrossRef]
- P, M.; Ahmad, J.; Samal, J.; Sheikh, J.A.; Arora, S.K.; Khubaib, M.; Aggarwal, H.; Kumari, I.; Luthra, K.; Rahman, S.A.; et al. Mycobacterium tuberculosis specific protein Rv1509 evokes efficient innate and adaptive immune response indicative of protective Th1 immune signature. Front. Immunol. 2021, 12, 706081. [CrossRef]
- Lakshmipriya, T.; Gopinath, S.C.B.; Tang, T.-H. Biotin-streptavidin competition mediates sensitive detection of biomolecules in enzyme linked immunosorbent assay. PLoS ONE 2016, 11, e0151153. [CrossRef]
- Omar, R.A.; Verma, N.; Arora, P.K. Development of ESAT-6 based immunosensor for the detection of Mycobacterium tuberculosis. Front. Immunol. 2021, 12, 653853. [CrossRef]
- Diouani, M.F.; Ouerghi, O.; Refai, A.; Belgacem, K.; Tlili, C.; Laouini, D.; Essafi, M. Detection of ESAT-6 by a label free miniature immuno-electrochemical biosensor as a diagnostic tool for tuberculosis. Mater. Sci. Eng. C 2017, 74, 465–470. [CrossRef]
- Arora, J.; Kumar, G.; Verma, A.; Bhalla, M.; Sarin, R.; Myneedu, V. Utility of MPT64 antigen detection for rapid confirmation of Mycobacterium tuberculosis complex. J. Global Infect. Dis. 2015, 7, 66. [CrossRef]
- Saengdee, P.; Chaisriratanakul, W.; Bunjongpru, W.; Sripumkhai, W.; Srisuwan, A.; Hruanun, C.; Poyai, A.; Phunpae, P.; Pata, S.; Jeamsaksiri, W.; et al. A silicon nitride ISFET based immunosensor for Ag85B detection of tuberculosis. Analyst 2016, 141, 5767–5775. [CrossRef]
- Xu, J.-N.; Chen, J.-P.; Chen, D.-L. Serodiagnosis efficacy and immunogenicity of the fusion protein of Mycobacterium tuberculosis composed of the 10-kilodalton culture filtrate protein, ESAT-6, and the extracellular domain fragment of PPE68. Clin. Vaccine Immunol. 2012, 19, 536–544. [CrossRef]
- Wang, Q.; Boshoff, H.I.M.; Harrison, J.R.; Ray, P.C.; Green, S.R.; Wyatt, P.G.; Barry, C.E. PE/PPE proteins mediate nutrient transport across the outer membrane of Mycobacterium tuberculosis. Science 2020, 367, 1147–1151. [CrossRef]
- García, J.; Puentes, A.; Rodríguez, L.; Ocampo, M.; Curtidor, H.; Vera, R.; Lopez, R.; Valbuena, J.; Cortes, J.; Vanegas, M.; et al. Mycobacterium tuberculosis Rv2536 protein implicated in specific binding to human cell lines. Protein Sci. 2005, 14, 2236–2245. [CrossRef]
- Shirshikov, F.V.; Bespyatykh, J.A. TB-ISATEST: A diagnostic LAMP assay for differentiation of Mycobacterium tuberculosis. Rus. J. Bioorg. Chem. 2023, 49, 1279–1292. [CrossRef]
- Jackett, P.S.; Bothamley, G.H.; Batra, H.V.; Mistry, A.; Young, D.B.; Ivanyi, J. Specificity of antibodies to immunodominant mycobacterial antigens in pulmonary tuberculosis. J. Clin. Microbiol. 1988, 26, 2313–2318. [CrossRef]
- Verbon, A.; Hartskeerl, R.A.; Moreno, C.; Kolk, A.H.J. Characterization of B cell epitopes on the 16K antigen of Mycobacterium tuberculosis. Clini. Exp. Immunol. 2008, 89, 395–401. [CrossRef]
- Salata, R.A.; Sanson, A.J.; Malhotra, I.J.; Wiker, H.G.; Harboe, M.; Phillips, N.B.; Daniel, T.M. Purification and characterization of the 30,000 dalton native antigen of Mycobacterium tuberculosis and characterization of six monoclonal antibodies reactive with a major epitope of this antigen. J. Lab. Clin. Med. 1991, 118, 589–598.
- Andersen, A.B.; Hansen, E.B. Structure and mapping of antigenic domains of protein antigen b, a 38,000-molecular-weight protein of Mycobacterium tuberculosis. Infect. Immun. 1989, 57, 2481–2488. [CrossRef]
- Attallah, A.M.; Osman, S.; Saad, A.; Omran, M.; Ismail, H.; Ibrahim, G.; Abo-Naglla, A. Application of a circulating antigen detection immunoassay for laboratory diagnosis of extra-pulmonary and pulmonary tuberculosis. Clin. Chim. Acta 2005, 356, 58–66. [CrossRef]
- Hunter, S.W.; Gaylord, H.; Brennan, P.J. Structure and antigenicity of the phosphorylated lipopolysaccharide antigens from the leprosy and tubercle bacilli. J. Biol. Chem. 1986, 261, 12345–12351.
- Cocito, C.; Vanlinden, F. Preparation and properties of antigen 60 from Mycobacterium bovis BCG. Clin. Exp. Immunol. 1986, 66, 262–272.
- Hendrickson, R.C.; Douglass, J.F.; Reynolds, L.D.; McNeill, P.D.; Carter, D.; Reed, S.G.; Houghton, R.L. Mass spectrometric identification of Mtb81, a novel serological marker for tuberculosis. J. Clin. Microbiol. 2000, 38, 2354–2361. [CrossRef]
- Arend, S.M.; Ottenhoff, T.H.; Andersen, P.; van Dissel, J.T. Uncommon presentations of tuberculosis: The potential value of a novel diagnostic assay based on the Mycobacterium tuberculosis-specific antigens ESAT-6 and CFP-10. Int. J. Tuberc. Lung Dis. 2001, 5, 680–686.
- Wilkinson, S.T.; Vanpatten, K.A.; Fernandez, D.R.; Brunhoeber, P.; Garsha, K.E.; Glinsmann-Gibson, B.J.; Grogan, T.M.; Teruya-Feldstein, J.; Rimsza, L.M. Partial plasma cell differentiation as a mechanism of lost major histocompatibility complex class II expression in diffuse large B-cell lymphoma. Blood 2012, 119, 1459–1467. [CrossRef]
Figure 1.
Sensitivity and specificity of tuberculosis diagnostic methods shown in Table 1.
Figure 1.
Sensitivity and specificity of tuberculosis diagnostic methods shown in Table 1.
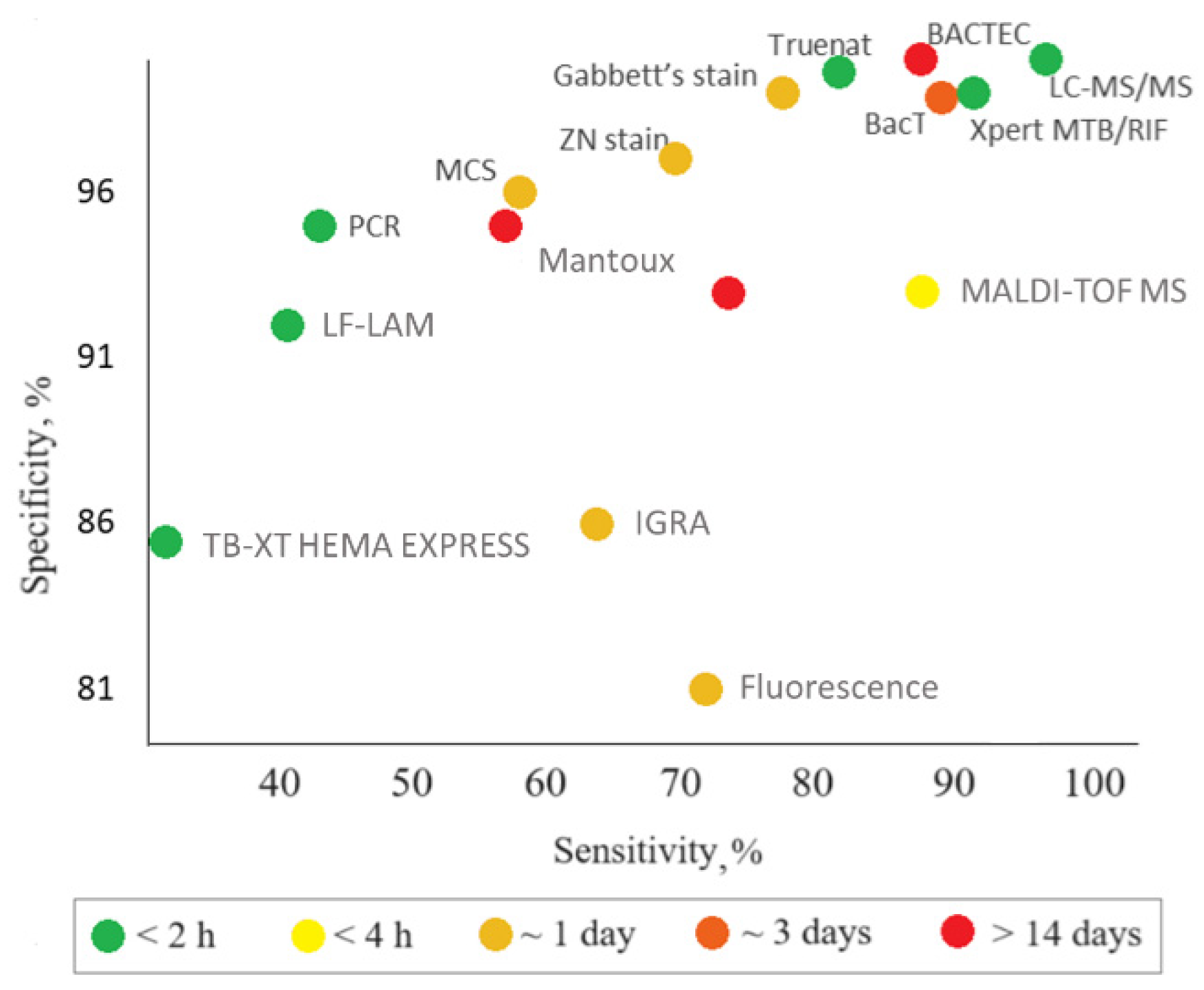
Figure 2.
Schematics of a quantum dot–based nanosensor. Abbreviations: M.tb, M. tuberculosis; TB, tuberculosis.
Figure 2.
Schematics of a quantum dot–based nanosensor. Abbreviations: M.tb, M. tuberculosis; TB, tuberculosis.
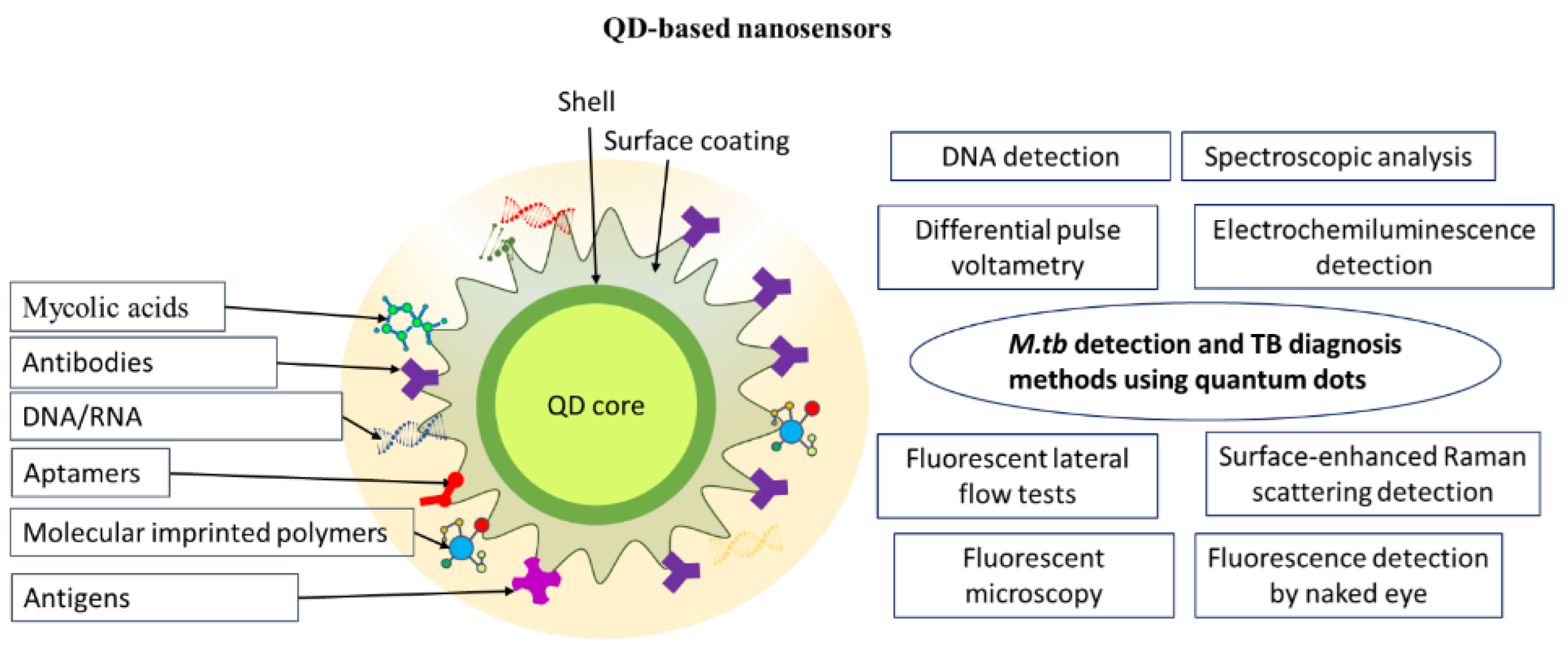
Figure 3.
Numbers of analyzed publications by year. Abbreviations: TB, tuberculosis; QDs, quantum dots.
Figure 3.
Numbers of analyzed publications by year. Abbreviations: TB, tuberculosis; QDs, quantum dots.
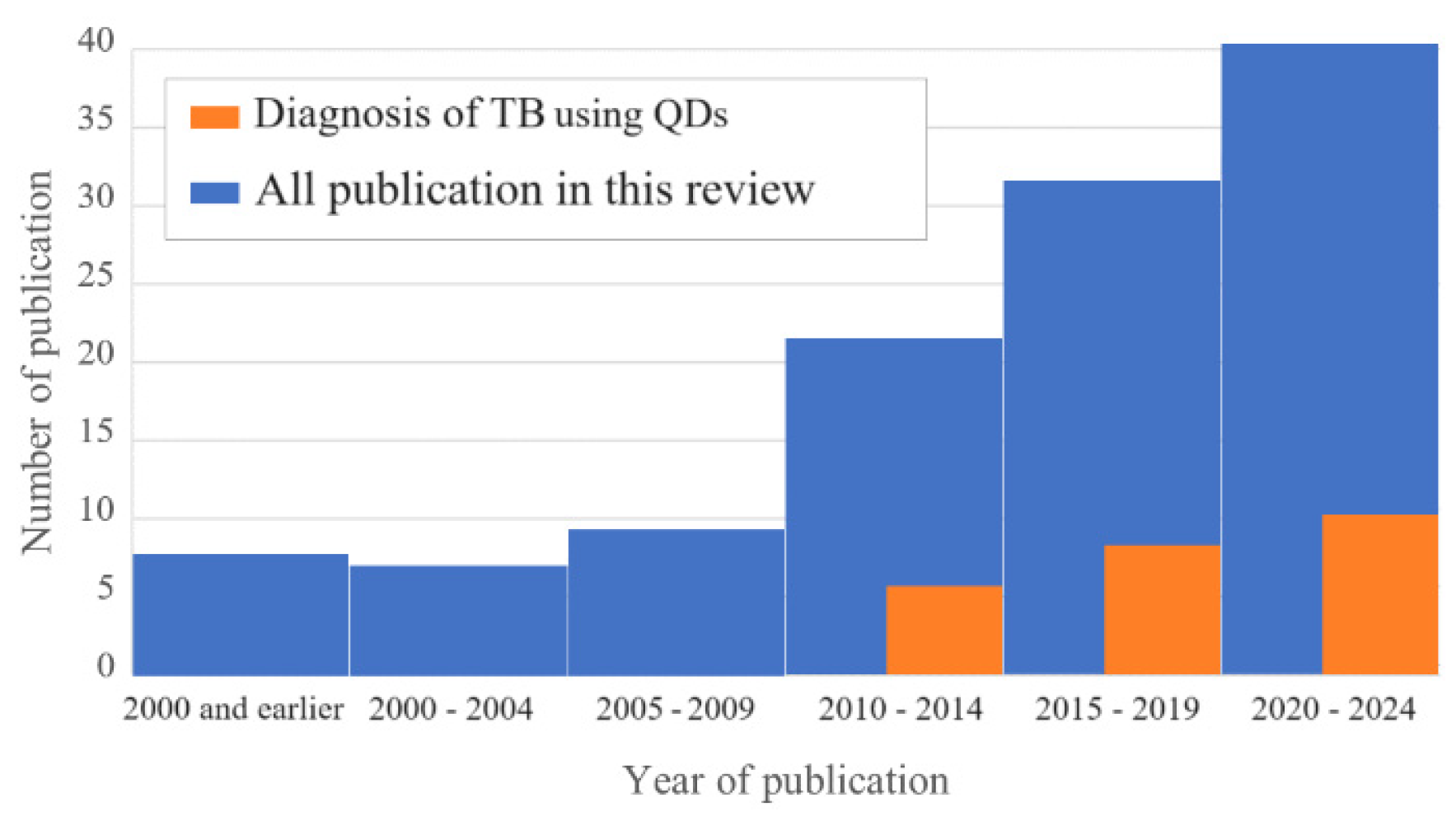

Table 1.
The major groups of routine clinical methods used for tuberculosis diagnosis.
| Assay | Biomaterial analyzed | Time of analysis | Advantages | Disadvantages | Sensitivity, specificity | Ref. | Comments |
|---|---|---|---|---|---|---|---|
| Molecular diagnostic tests | |||||||
| Polymerase chain reaction (PCR) | Serum, urine, blood, sputum, saliva, lung biopsy samples, BALF, pleural fluid | 4–5 h | High specificity, quickness, and informativeness | High cost, limited availability, low sensitivity for non-respiratory samples; detection of DNA only | Sensitivity: 47% (42–51%) Specificity: 95% (93–97%) CrI: 95% |
[10] | The sensitivity and specificity are averaged results of 9 studies in 709 subjects |
| Xpert MTB/RIF Ultra | Raw sputum or concentrated sediment | 1.5 h | Detection of rpoB gene mutations associated with rifampicin resistance | High cost | Sensitivity: 89% (85–92%) Specificity: 99% (98–99%) CrI: 95% |
[11] | The sensitivity and specificity are averaged result of 22 studies in 8998 subjects, including 2953 confirmed TB cases and 6045 cases without TB |
| Truenat | Raw sputum | 1 h | Use of a portable, chip-based and battery-operated device. Suitability for laboratories with technical equipment | Lower accuracy compared to Xpert MTB/RIF Ultra | Sensitivity: 80% (70.2–88.4%) Specificity: 98% (94.5–99.6%) |
[12] | The sensitivity and specificity have been estimated in tests in 250 subjects |
| LF-LAM | Urine | 0.5 h | High efficiency, ease of use, low cost, simple technology, no special equipment. Detection of TB in patients for whom other diagnostic methods cannot be used (e.g., HIV patients) | Lower sensitivity compared to Xpert MTB/RIF (though higher compared to microscopy methods). Suitability for a limited group of patients only. Impossibility to distinguish M. tb. from other mycobacteria, which requires using other diagnostic methods after the test | Sensitivity: 45% (29–63%) Specificity: 92% (80–97%) CrI: 95% |
[13] | The sensitivity and specificity are averaged results of 5 studies in 2313 subjects, including 35% of TB cases |
| TB-XT HEMA EXPRESS | Blood, serum | 0.5 h | Quickness, relatively low cost | Low sensitivity, suboptimal performance in the case of high TB prevalence | Sensitivity: 31% (3.9–78%) Specificity: 85% так (52–93%) |
[14] | The sensitivity and specificity have been estimated in tests in 1386 subjects, including 290 TB cases |
| TB tests based on T-cells analysis | |||||||
| IGRA, (T-SPOT.TB, QuantiFERON-TB Gold (QFT)) | Blood, serum | up to 2 days | Insensitivity to BCG vaccination or contact with atypical mycobacteria; one-time tests; high efficiency. T-SPOT.TB is less susceptible to immunosuppression than other TB tests and is preferable for the examination of HIV-infected or autoimmunity patients during treatment with immunosuppressants; can be used before starting therapy with biological drugs | Low specificity and sensitivity; high cost; impossibility to distinguish between the active and latent forms of TB and unsuitability as a primary diagnostic test for LTBI or active TB. The bacterium itself is not determined; the result depends on the state of the patient’s immune system |
QFT Sensitivity: 66% (47–81%) Specificity: 87% (68–94%) T-SPOT Sensitivity: 60% (48–72%) Specificity: 86% (65–95%) |
[15] | The sample consisted of 6,525 HIV-positive patients, including 3,467 TB cases, 806 of them with LTBI and 2,661 with active TB |
| Cultural methods | |||||||
| BBL Septi-Chek AFB | Sputum | Up to 23 days | Higher M.tb growth rate compared to methods using an isolated dense medium | Low sensitivity, long time of analysis | Sensitivity: 73% Specificity: 93% |
[16] | The sensitivity and specificity have been estimated in studies on 274 specimens |
| BАСТЕС (with different parameters of MGIT 460, 960) | Sputum | Up to 14 days | Rapid identification of M.tb and its drug sensitivity; accelerated culture testing of all first-line drugs | High cost, justified only for large laboratories. Semi-automatic monitoring of bacterium growth; many labor-intensive operations; use of radioisotopes and the need for disposal of radioactive waste; long time of analysis |
MGIT 960 Sensitivity: 81.5% Specificity: 99.6% MGIT 460 Sensitivity: 85.8% Specificity: 99.9% |
[17] | The sensitivity and specificity have been estimated in studies on ~8,000 clinical specimens per year. The number after MGIT is the number of wells in the plate. |
| BacT/ALERT 3D | Sputum | 24–72 h | Detection of M.tb growth; detection of M.tb and fungi in blood cultures. Full automation; no radioactive waste | Long time, high cost | Sensitivity: 87.80% Specificity: 99.21% |
[18] | The sensitivity and specificity have been estimated in studies on 2659 clinical specimens |
| Skin tests | |||||||
| Tuberculin skin tests, Mantoux tests, and Diaskintest (in vivo) | Skin tests | 72 h | Availability; low cost; ease of use | Low specificity and sensitivity; unsuitability for diagnosing active TB forms; false positive results in those who have been infected with M.tb in the past because their memory T cells still secrete interferon; impossibility to distinguish the active and latent forms of TB | Sensitivity: 59% Specificity: 95% |
[19] | The sensitivity and specificity have been estimated in tests in 643,694 U.S. Navy recruits |
| Tests based on mycobacterium staining | |||||||
| Gabbett's stain, Ziehl–Neelsen stain, modified cold stain (MCS) | Sputum | ~24 h | Simplicity, quickness, ease of use, low cost | Low sensitivity and specificity; suitability for pulmonary tuberculosis only; inaccuracy in children and HIV-infected persons; multistage and complex procedure. Impossibility to distinguish between different mycobacteria |
Gabbett’s stain Sensitivity: 77% Specificity: 98% Ziehl–Neelsen stain Sensitivity: 70% Specificity: 97% MCS Sensitivity: 60% Specificity: 96% |
[20] | The sensitivity and specificity have been estimated in tests in 100 patients |
| Fluorescence microscopy | Sputum | ~24 h | Quickness, ease of use, specificity | High cost, frequent burn-out of expensive mercury vapor lamps, need for continuous power supply, need for a dark room | Sensitivity: 72% Specificity: 81% |
[21] | The sensitivity and specificity have been estimated in tests in 426 patients |
| Other methods | |||||||
| X-ray | Radiographic test | 1 h | Quickness | High cost; low specificity | Sensitivity: 96% Specificity: 46% |
[22] | The sensitivity and specificity are averaged results of 13 studies |
| MALDI-TOF MS | BALF, sputum | 2.5 h | Rapid, reliable, cost-effective method | Method requires sample preprocessing to generate high-quality proteomic profiles, especially for proteins/peptides or other low-abundance analytes in which MS spectra are obscured by more abundant/high-molecular-weight species. This method is not highly specific because of the matrix proteins and noise issues | Sensitivity: 83%; Specificity: 93%; CrI: 95% |
[23] | The sensitivity and specificity have been estimated in tests in 214 patients |
| LC-MS/MS | Urine, blood | 1 h | Proteomic analysis of urine; identification of proteins characteristic of TB with high molecular specificity and sensitivity; simultaneous diagnosis of HIV-1 and TB using a blood sample. Structural identity of individual components | Changes in ionization efficiency in the presence of not only proteins, phospholipids, and salts, abut also reagents and contaminants | Sensitivity: 94% Specificity: 100% |
[24] | The sensitivity and specificity have been estimated in tests in 57 patients |
* Abbreviations: LF-LAM, lipoarabinomannan lateral shift test; LTBI, latent tuberculosis infection; MGIT, mycobacteria growth indicator tube; IGRA, interferon-gamma release assay; CrI, credible interval; BALF, bronchoalveolar lavage fluid; MALDI-TOF MS, matrix-assisted laser desorption ionization time-of-flight mass spectrometry; LC-MS, liquid chromatography tandem mass spectrometry; MS, mass spectrometry.
Table 2.
Quantum dot–based nanosensors for M. tuberculosis detection and tuberculosis diagnosis.
| No. | Biomaterial analyzed | Biomarker | Capture molecule | Nanosensor | Method of detection | Wavelength, nm (where relevant) | LOD | Ref. |
|---|---|---|---|---|---|---|---|---|
| 1 | Blood | TMCC1, GBP6 | Oligonucleotides specific for M.tb mRNA biomarkers | QD655 and QD525 conjugated with the capture molecules | Toehold-mediated strand displacement with fluorescence quenching by FRET | Emission: 525 Emission: 655 Excitation: 480 |
GBP6: 1.6 nM TMCC1: 6.4 nM |
[64] |
| 2 | Blood | IFN-γ | Anti-human IFN-γ antibodies | CdS QDs coupled to magnetic beads conjugated with the capture molecules. Sandwich-type sensor is fabricated on a glassy carbon electrode covered with a well-ordered gold nanoparticle monolayer, which offers a solid support to immobilize the capture molecules | Square wave anodic stripping voltammetry to quantify the metal cadmium, which indirectly reflects the amount of the analyte | N/A | 0.34 pg/mL | [65] |
| 3 | Serum | IFN-γ | IFN-γ aptamer | Gold electrode covered with L-cysteine-SnTeSe QDs functionalized with the capture molecules | Electrochemical impedance spectroscopy detection of the change in the electron transfer resistance upon IFN-γ binding | N/A | 0.151 pg/mL | [66] |
| 4 | Serum | IFN-γ, TNF-α, IL-2 | Antibody pairs for IFN-γ-, TNF-α and IL-2 | Sandwich immunoassay sensor consisting of luminol and carbon and CdS QDs integrated with gold nanoparticles and magnetic beads functionalized with the capture molecules, as well as the same capture molecules separately immobilized on three spatially resolved areas of a patterned indium tin oxide electrode to capture the corresponding triple latent TB biomarkers | Electrochemiluminescence detection | N/A | 1.6 pg/mL | [67] |
| 5 | Sputum | DNA IS1081 | Specific DNA nanobeacon | QD-based nanobeacon fluorescence probes containing QDs and black hole quenchers. After the target DNA hybridizes with the nanobeacon, the nanobeacon is cleaved into two DNA fragments, and the QDs fluoresce upon moving away from the black hole quenchers | Fluorescence detection by naked eye | Excitation: 280 Emission: 330 |
3.3 amol/L (2 copies/μL) |
[68] |
| 6 | N/A | Anti-MA antibodies | MAs | Graphene QDs covalently functionalized with MAs as detection tags for anti-MA antibodies | Fluorescent lateral flow assay | Excitation: 360 Emission: 470 |
N/A | [69] |
| 7 | N/A | Anti-MA antibodies | Mas | CdSe/ZnS QDs covalently functionalized with MAs as detection tags for anti-MA antibodies | Fluorescent lateral flow assay | Excitation: 390 Emission: 474 |
N/A | [70] |
| 8 | Pure CFP-10 solution | CFP-10 | Pair of anti-CFP-10 antibodies (G2 and G3) | Glass slide coated with magnetoplasmonic core/shell nanoparticles (Fe3O4/Au) functionalized with G2. Graphene QDs functionalized with conjugate of gold-binding protein with G3. Upon binding of CFP-10 by a G2–G3 sandwich, immunoassay is formed | Dual metal-enhanced fluorescence and surface-enhanced Raman scattering detection | Excitation: 320 Emission: 436, 516 |
0.0511 pg/mL | [71] |
| 9 | Pure DNA | rpoB531, katG315 | ssDNA specific for target DNA | QD535 and QD648 functionalized with specific ssDNA. When the target DNA is absent, the nanosensor is attached to a quencher. Binding with the target DNA leads to detachment of the nanosensor and recovery of fluorescence | Fluorescence measurement | Excitation: 380 Emission (rpoB531): 535 Emission (katG315): 648 |
rpoB531: 24 pM; katG315: 20 pM |
[72] |
| 10 | Blood | IFN-γ, IP-10 | Aptamers specific for IFN-γ and IP-10 | Cytosine–Ag+–cytosine and thymine-Hg2+–thymine hairpin structures releasing the metal ions upon specific interaction with different biomarker–aptamer complexes. Ag+ and Hg2+ are bound by CdTe and carbon QDs, which are detected by fluorescence | Fluorescence measurement | - | IP-10: 0.3×10-6 pg/mL; IFN-γ: 0.5×10-6 pg/mL |
[73] |
| 11 | Sputum | M.tb cell | M.tb-binding peptide H8, anti-M.tb polyclonal antibodies, and anti-HSP65 monoclonal antibodies | QDs conjugated with H8 or anti-HSP65 antibodies and MMS conjugated with H8 or anti-M.tb polyclonal antibodies. Magnetic separation of the QD–M.tb–MMS complex | Fluorescence microscopy | Excitation: 405 Emission: 610 |
103 CFU/mL | [74] |
| 12 | M.tb suspension and sputum | M.tb cell | M.tb-binding peptide H8 | Magnetic beads and QDs conjugated with H8. Magnetic separation of the QD–M.tb–magnetic bead complex | Fluorescence microscopy | N/A | 103 CFU/mL | [75] |
| 13 | Sputum | ESAT-6 | Oligonucleotides specific for ESAT-6 | FRET-based sandwich biosensor containing CdTe QDs and gold nanoparticles (quencher) conjugated with the capture molecules (obtained by PCR). When the marker id bound, QD fluorescence is quenched via FRET to gold nanoparticles | Fluorescence detection | Excitation: 370 Emission: 400–680 |
10 fg | [76] |
| 14 | Sputum | IS6110 DNA | ssDNA complementary to the IS6110 gene fragment | FRET-based biosensor in which CdTe QDs conjugated with the capture molecule serves as a donor and Cu-TCPP, which is more affine for ssDNA than double-stranded DNA, serves as an acceptor. In the absence of the marker, the QD fluorescence is quenched. Interaction of the ssDNA. Hybridization of the ssDNA with the marker results in fluorescence , whose intensity depends on the marker concentration | Fluorescence detection | Excitation: 365 Emission: 586 |
35 pM | [77] |
| 15 | Urine | Secretory antigen Ag85B | Anti-Ag85B antibodies (GBP-50B14 and SiBP-8B3) | FRET based biosensor in which gold nanorods conjugated with GBP-50B14 serve as acceptors and silica-coated CdTe QDs conjugated with SiBP-8B3 serve as donors. When both tags bind Ag85B, FRET between the QDs and nanorods quenches the QD fluorescence | Fluorescence detection | Excitation: 350 Emission: 630 |
13 pg/mL | [78] |
| 16 | Urine | LAM | Pair of anti-LAM recombinant monoclonal antibodies | Lateral flow test using CdSe/ZnS QDs encapsulated in polymeric bead conjugated with the capture molecules; test strip with the immobilized capture molecules | Portable fluorescence detector | Excitation: 375 Emission: 620 |
50 pg/mL | [79] |
| 17 | Urine | CFP-10 | Pair of anti-CFP-10 antibodies | Glassy carbon electrode modified with graphene quantum dot–coated Fe3O4@Ag nanoparticles and gold nanoparticles conjugated to the capture antibody. Binding of CFP-10 to the electrode results in an immune sandwich, gold nanoparticles conjugated with the detection antibody serving as signal-amplification labels | Differential pulse voltammetry | N/A | 330 pg/mL | [80] |
| 18 | Exhaled air | TB related volatile organic biomarkers | No | Suspension of CdSe or carbon QDs. The biomarker causes changes in the absorbance and fluorescence spectra. | Spectroscopic analysis | Excitation: 360–650 Emission: 300–800 |
N/A | [81] |
| 19 | Exhaled air | MN | Co ion | CoTCPP nanosheets with attached CdTe QDs. The QD fluorescence is quenched in the absence of MN and is recovered upon MN binding to CoTCPP causing QD release | Fluorescence detection | Excitation: 370 Emission: 658 |
0.59 µM | [82] |
| 20 | BALS, feces, paraffin-embedded tissues | IS6110 and IS900 DNA | Mycobacterium-specific oligonucleotides | CdSe QDs conjugated with streptavidin and species-specific probes and magnetic beads conjugated with streptavidin and genus-specific probes. Sandwich hybridization is used to bind the biomarkers and subsequent magnet separation, to concentrate the biomarker | Fluorescence detection | Excitation: 260 Emission: 655 |
12.5 ng | [83] |
| 21 | Pure fprA | fprA | Anti-fprA antibodies | Direct and double antibody sandwich lateral flow tests with CdSe/ZnS QDs conjugated with the capture molecule | Fluorescence detection | Emission: 565 | 12.5 pg/mL | [84] |
| 22 | M.tb strains | M.tb DNA | ssDNA specific for M.tb | FRET-based sensor composed of water-stable CsPbBr3 perovskite QDs conjugated to DNA probe serving as a donor and MoS2 nanosheets serving as acceptor | Fluorescence detection | N/A | 51.9 pM | [85] |
| 23 | Pure antigens | CFP10-ESAT6 | Anti-CFP10–ESAT6 monoclonal antibody | Electrochemical immunosensor consisting of SPCE functionalized with Si nanoparticles and CdSe/ZnS QDs. The target biomarker is adsorbed on the electrode and then captured by the primary antibody, the secondary antibody being labeled with catalase, whose activity is detected electrochemically | Differential pulse voltammetry | N/A | 15 pg/mL | [86] |
* Abbreviations: TMCC1, transmembrane and coiled-coil domain family 1; GBP6, guanylate binding protein family member 6; QD, quantum dot; IFN-γ, interferon gamma; TNF-α, tumor necrosis factor alpha; IL-2, interleukin-2; MAs, mycolic acids; CFP-10, culture filtrate protein 10; ssDNA, single-strand DNA; IP-10, IFN-γ-induced protein 10; MMS, magnetic microsphere; HSP65, heat shock protein 65; ESAT-6, early secretory antigenic target 6; FRET, Förster resonance energy transfer; Cu-TCPP, two-dimensional metal-organic framework; LAM, lipoarabinomannan; MN, methyl nicotinate; CoTCPP, cobalt-metalized tetrakis (4-carboxyphenyl) porphyrin; BALS, bronchoalveolar lavage specimens; fprA, flavoprotein reductase; SPCE, screen-printed carbon electrode; DPV, differential pulse voltammetry.
Table 3.
Potential M. tuberculosis biomarkers.
| Biomarker | Already detected with QD-based nanosensors | Comment | Ref. |
|---|---|---|---|
| Host RNA transcript/DNA signatures | |||
| GBP2, GBP5, GBP6, TMCC1 | + | Oligonucleotides (RNA, DNA) | [64,87] |
| PRDM1 | - | PR domain zinc finger protein 1 gene | [87] |
| ARG1 | - | Arginase 1 gene (encoding the arginase enzyme) | [87] |
| IS6110 | + | IS6110 gene | [77] |
| IS1081 | - | IS1081 gene | [88] |
| rpoB531 | + | rpoB531 gene | [72] |
| katG315 | + | katG315gene | [72] |
| Acids and their derivatives | |||
| MN | + | Menthyl nicotinate | [81] |
| MAs | + | Mycolic acids | [69,70] |
| Enzymes | |||
| MNAzymes | + | Multicomponent nucleic acid enzyme | [68] |
| ADA | - | Adenosine deaminase (enzyme of purine metabolism) | [89] |
| KatGs | - | Catalase-peroxidase enzymes (responsible for the activation of the antituberculosis drug isoniazid) | [90] |
| Сytokines | |||
| IL-1ra | Interleukin-1 receptor antagonist | [91] | |
| IL-2 | + | Interleukin-2 | [91,92] |
| IL-10 | + | Interleukin-10 | [91,93] |
| IL-13 | Interleukin-13 | [91] | |
| INF-y | + | Interferon gamma | [65,92,93] |
| TNF-α | + | Tumor necrosis factor alpha | [92] |
| INF-y IP-10 | + | Interferon-gamma-inducible protein 10 | [25] |
| MIP-1β | - | Macrophage inflammatory protein | [91] |
| Specific surface proteins | |||
| CFP-10 | + | 10-kDa culture-filtered protein | [86,94,95] |
| Mtb Rv1468c (PE_PGRS29) | - | M.tb surface protein | [96] |
| Rv1509 | - | M.tb-specific protein | [97] |
| ESAT-6 | - | 6-kDa early secreted antigenic target | [94,98,99,100] |
| MPT-64 | - | M.tb protein 64 | [101] |
| Ag85B | + | Secreted protein antigen 85 complex B | [78,102] |
| PPE-68 | - | Proline-proline-glutamic acid | [103,104] |
| Rv2536 | - | Potential membrane protein | [105] |
| Rv2341 | Probable conserved lipoprotein LppQ | [106] | |
| Mycobacterial antigens | |||
| 14-kDa antigen | - | 14-kDa protein antigen | [107] |
| 16-kDa antigen | - | M.tb-specific antigens | [108] |
| 19-kDa antigen | - | 19-kDa lipoprotein | [107] |
| 30-kDa antigen | - | Immunodominant phosphate-binding protein | [109] |
| 38-kDa antigen | - | Immunodominant lipoprotein antigen | [110] |
| 55-kDa antigen | - | M.tb-specific antigens | [111] |
| LAM | - | A glycolipid and a virulence factor associated with M.tb | [112] |
| A60 | - | Tuberculosis antigen | [113] |
| Mtb81 | - | Recombinant protein | [114] |
| ESAT-6 | + | M.tb-specific antigens | [86,115] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



