
Submitted:
03 September 2024
Posted:
04 September 2024
You are already at the latest version
Abstract
Purpose: Our aim in this case is to report a new finding regarding Nutcracker syndrome (NCS), which is a variation of the left renal vein.
Methods: We present a very rare anatomical variant of the left renal vein(LRV), with a preliminary diagnosis made by ultrasound and NCS as a differential diagnosis with computed tomography (CT) and diagnostic CT angiography.
Results: The patient in our case was a 30-year-old woman with chronic abdominal and flank pain and increased sensitivity in the flank area. Neither hematuria nor proteinuria was detected in the urinalysis. Contrast-enhanced computed tomography(CT) showed that there were two separate LRVs draining the lower and upper poles. It was observed that the vein draining the lower pole narrowed significantly between superior mesenteric artery and abdominal aorta and then continued to widen. This view showed that we were faced with a typical NCS. What made our case different and unique from typical NCS was that it had renal intraparenchymal varicose veins. Treatment of NCS includes open, laparoscopic and robotic surgical repair and endovascular/extravascular stent placement. Treatment of symptomatic NCS includes open, laparoscopic, and robotic surgical repair and endovascular/extravascular stent placement. Except for the presence of hematuria causing severe anemia, deterioration in kidney functions and serious pain, patients are followed conservatively, and our patient is also followed conservatively.
Conclusion: This case we present is the first case accompanied by renal parenchymal varices in the literature.
Keywords:
Nutcracker syndrome
; Intraparenchymal
; Renal vein
Introduction
Nutcracker syndrome(NCS) is a condition with typical clinical findings that occurs secondary to compression of the left renal vein(LRV) between the abdominal aorta(AA) and superior mesenteric artery(SMA) [1]. In the presence of the same anatomical variation but no clinical symptoms or signs, this situation is called Nutcracker phenomenon(NCP) [2,3]. Although hematuria(microscopic or macroscopic) is most commonly observed in patients, chronic abdominal or flank pain, hypertension and proteinuria may be observed. Depending on the severity of venous congestion, it may cause varicocele in men and pelvic congestion syndrome(PCS)(dyspareunia, dysmenorrhea, chronic pelvic pain) in women [2,4]. According to our research, this case, which we followed conservatively with a diagnosis of NCS, is the first case in the literature accompanied by renal intraparenchymal varicose veins.
Case Report
The physical examination of a 30-year-old female patient with no abnormal personal or family history, who applied to the urology outpatient clinic with complaints of chronic abdominal and flank pain, was unremarkable except for minimal increased tenderness in the flank area. Our patient’s height, weight and blood pressure were 1.6 m, 60 kg and 110/70 mmHg, respectively. In laboratory tests, the creatinine value was 0.66 mg/dl. No hematuria or proteinuria was detected in the urinalysis. In abdominal ultrasonography (US), the size of the left kidney increased compared to the right, and tubular appearances, the largest of which were 22x8 mm, were observed in the lower pole of the left kidney, and venous bleeding encoding was observed in color Doppler ultrasonography(RDU). Thereupon, contrast-enhanced computed tomography(CT) showed that there were two LRVs draining the lower and upper poles. It was observed that the vein draining the lower pole narrowed significantly between SMA and AA and then continued to widen, while the vein draining the upper pole was normal. The renal vein draining the lower pole was wide and tortuous in appearance and had extrarenal and parenchymal components(Figure 1). On CT, the segment diameter of the LRV between SMA and AA was 1.5 mm, and the diameter in the hilar region was 15.7 mm and the ratio was 1/10(Figure 2). Aorto-mesenteric angle(AMA) was 24º(Figure 3). It was stated that the veins containing extrarenal and parenchymal components in a dilated, tortuous appearance secondary to venostasis in the renal vein draining the lower pole showed intraparenchymal extension and showed endophytic mass formation in the first US examination, which was suspicious for angiomyolipoma(Figure 1). It was observed that this venous stasis extended to the left ovarian and parauterine veins and caused varicose dilatation(Figure 3). Although many cases similar to ours have been reported in the literature, the fact that it is the first case with renal intraparenchymal varicose veins makes this case privileged in the sense of the literature.
Discussion
LRV compression was first described anatomically by Grant in 1937. The clinical importance of this phenomenon was revealed by El-Sadr and Mina in 1950. Schepper was the first author to use NCS terminology in 1972 [3,5,6,7,8,9]. According to its morphological characteristics, there are two types: anterior NCS(ANCS) and posterior NCS(PNCS) [3,9]. In ANCS, which is the most common type, LRV is subjected to compression between AA and SMA, while in PNCS, retroaortic or circumaortic variation can be seen, caused by compression of LRV between AA and vertebral column. Although the prevalence of NCS is not known exactly because the symptoms are variable and not specific to NCS, the incidence of ANCS and PNCS is 3.2% and 0.1%, respectively [2,10]. In a study, it was found that NCP was seen at a rate of 4.1% [8,11]. While there are patients diagnosed in all age groups, it is most common in the third and fourth decades in female gender [3]. It has been stated that thin and tall people are more affected than overweight people, and that weight gain provides relief in symptoms by increasing retroperitoneal fat tissue [3,8,12]. Symptoms vary depending on the severity of venous stasis and the organs where the stasis occurs. In addition to fatigue, flank pain, macroscopic or microscopic hematuria (after rupture of venous structures into the collecting system due to high venous pressure), proteinuria, it can cause varicocele in men, PCS and chronic pelvic pain in women[3,5,6,8,12]. The most common symptom has been reported to be hematuria [3,5,9]. Our patient had no symptoms or signs other than flank painFlank pain may mimic stone-related colic pain in some patients, and the diagnosis may be missed because stones are not seen on non-contrast CT. Hematuria and colic pain may increase with exertion, and the patients’ anamnesis indicating this is very meaningful to us [13]. NCS should be among the diagnoses that should be considered in these patients. For diagnosis, the first thing that needs to be done is a good medical history and detailed physical examination. Then, complete blood count, kidney function tests, urine analysis, urine cytology, cystourethrography, US and CT urography are examined in certain steps [5]. In these evaluations, when malignancies, stones, arteriovenous malformations are excluded and NCS is considered, it is recommended to first perform RDU, which has a sensitivity and specificity of 69-90% and 89-100%, respectively, due to its non-invasive nature [1,3,6,14]. CT and magnetic resonance imaging (MRI) are useful because they provide simultaneous condition of surrounding tissues and anatomical correlation. A hilar to aorto-mesenteric segment ratio of LRV≥4.9 is the most important CT finding (100% specificity) [6,9,12]. The highest diagnostic accuracy observed in axial CT is the “beak sign” and LRV diameter [6,12]. Another diagnostic criterion is that the aortomesenteric angle (AMA), which normally varies between 38º and 56º, is less than 35º[2,3,6,9]. In our case, the aorto-mesenteric segment ratio was >10 and AMA was 24º, which was typical for NCS. In cases where radiation exposure and contrast allergy are to be avoided, MRI can also be used, which provides evidence with similar accuracy as CT [6,12]. If we look at what the gold standard method is, we see that there is a method of measuring the pressure gradient between the inferior vena cava and LRV (normal is 0-1 mmHg, >3 mmHg has diagnostic value in terms of NCS) with venography and endovascular US [2,6,8,9]. These two invasive methods are used when there is doubt in the diagnosis of NCS [3]. Recently, owing to innovations such as 3D reconstructions provided by CT or MRI technologies, it is possible to obtain axial, coronal and sagittal images with high diagnostic value, so there is no need for invasive methods. There is no clear algorithm for the treatment of NCS, and decisions are made on a patient-by-patient basis, depending on the severity of the symptom. While conservative follow-up is performed in patients without very serious symptoms, active treatment is performed in the presence of hematuria causing significant anemia, deterioration in renal functions and serious pain [3,5,6,8,9]. Medical treatment also has a place in patients at risk of venous thrombosis [13]. Treatment of NCS includes open, laparoscopic and robotic surgical repair and endovascular/extravascular stent placement [1,3]. Endovascular stent placement is the most common and first choice [9,11]. Open, laparoscopic and robotic, LRV repositioning and renal auto-transplantation are other surgical treatments [2,6,14]. We are conservatively following our patient, who does not have any serious symptoms.
Conclusion
Due to nonspecific symptoms, NCS is often not the first diagnosis that comes to mind, and there is a risk of missing a diagnosis in these patients. For this reason, the patient’s anamnesis, examination findings, laboratory and radiological imaging should be evaluated holistically. Patients diagnosed with NCS should receive follow-up or treatment modalities appropriate to the severity of NCS and the patient’s symptoms.
Financial Disclosure
The authors declared that this study has received no financial support.
Informed Consent Statement
Informed consent was obtained from the patient in reporting this case.
Conflict of Interest
No conflict of interest was declared by the authors.
References
- de Los Reyes T, Keefe DT, Rickard M, Lorenzo AJ (2021) Diagnosis and therapeutic strategies for nutcracker syndrome. Curr Opin Urol 31:135–137. https://doi.org/10.1097/MOU.0000000000000831. [CrossRef]
- Dieleman F, Hamming JF, Erben Y, Van Der Vorst JR (2023) Nutcracker Syndrome: Challenges in Diagnosis and Surgical Treatment. Annals of Vascular Surgery 94:178–185. https://doi.org/10.1016/j.avsg.2023.03.030. [CrossRef]
- Kurklinsky AK, Rooke TW (2010) Nutcracker phenomenon and nutcracker syndrome. Mayo Clin Proc 85:552–559. https://doi.org/10.4065/mcp.2009.0586. [CrossRef]
- Bookwalter CA, VanBuren WM, Neisen MJ, Bjarnason H (2019) Imaging Appearance and Nonsurgical Management of Pelvic Venous Congestion Syndrome. RadioGraphics 39:596–608. https://doi.org/10.1148/rg.2019180159. [CrossRef]
- Chait J, Sen I, Kalra M (2021) Nutcracker Syndrome: How to Diagnose It and When/How Should It Be Treated in the Pelvic Venous Disease Population. Tech Vasc Interv Radiol 24:100734. https://doi.org/10.1016/j.tvir.2021.100734. [CrossRef]
- Ananthan K, Onida S, Davies AH (2017) Nutcracker Syndrome: An Update on Current Diagnostic Criteria and Management Guidelines. Eur J Vasc Endovasc Surg 53:886–894. https://doi.org/10.1016/j.ejvs.2017.02.015. [CrossRef]
- Wang R-F, Zhou C-Z, Fu Y-Q, Lv W-F (2021) Nutcracker syndrome accompanied by hypertension: a case report and literature review. J Int Med Res 49:300060520985733. https://doi.org/10.1177/0300060520985733. [CrossRef]
- Ismailoglu T (2022) The Nutcracker Syndrome. J Radiol Case Rep 16:17–23. https://doi.org/10.3941/jrcr.v16i5.4339. [CrossRef]
- Granata A, Distefano G, Sturiale A, Figuera M, Foti PV, Palmucci S, Basile A (2021) From Nutcracker Phenomenon to Nutcracker Syndrome: A Pictorial Review. Diagnostics (Basel) 11:101. https://doi.org/10.3390/diagnostics11010101. [CrossRef]
- Kaur R, Airey D (2022) Nutcracker syndrome: A case report and review of the literature. Front Surg 9:984500. https://doi.org/10.3389/fsurg.2022.984500. [CrossRef]
- Berthelot J-M, Douane F, Maugars Y, Frampas E (2017) Nutcracker syndrome: A rare cause of left flank pain that can also manifest as unexplained pelvic pain. Joint Bone Spine 84:557–562. https://doi.org/10.1016/j.jbspin.2016.10.006. [CrossRef]
- Kolber MK, Cui Z, Chen CK, Habibollahi P, Kalva SP (2021) Nutcracker syndrome: diagnosis and therapy. Cardiovasc Diagn Ther 11:1140–1149. https://doi.org/10.21037/cdt-20-160. [CrossRef]
- Nakashima T, Sahashi Y, Kanamori H, Ohno Y, Okura H (2020) Localized solitary left renal vein thrombus complicating nutcracker syndrome: a case report and review of the literature. CEN Case Rep 9:252–256. https://doi.org/10.1007/s13730-020-00467-9. [CrossRef]
- Muheilan M, Walsh A, O’Brien F, Tuite D (2022) Nutcracker syndrome, conservative approach: a case report. J Surg Case Rep 2022:rjac423. https://doi.org/10.1093/jscr/rjac423. [CrossRef]
Figure 1.
The renal vein draining the lower pole was wide and tortuous in appearance and had extrarenal and parenchymal components (Fig. A-F).
Figure 1.
The renal vein draining the lower pole was wide and tortuous in appearance and had extrarenal and parenchymal components (Fig. A-F).

Figure 2.
The segment diameter of the LRV between SMA and AA was 1.5 mm, and the diameter in the hilar region was 15.7 mm and the ratio was. A “beak sign” is shown at the tip of the white arrow.
Figure 2.
The segment diameter of the LRV between SMA and AA was 1.5 mm, and the diameter in the hilar region was 15.7 mm and the ratio was. A “beak sign” is shown at the tip of the white arrow.
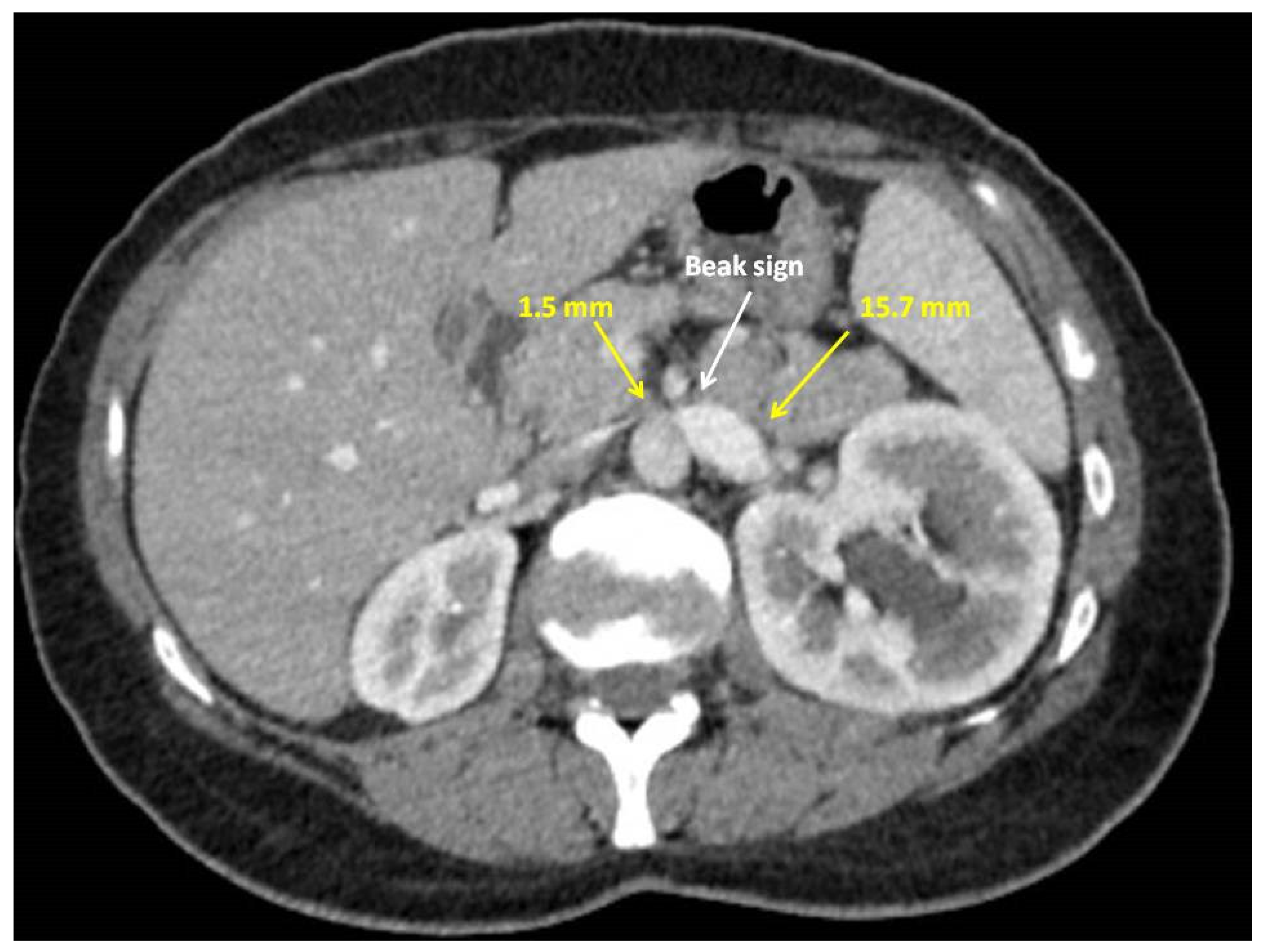
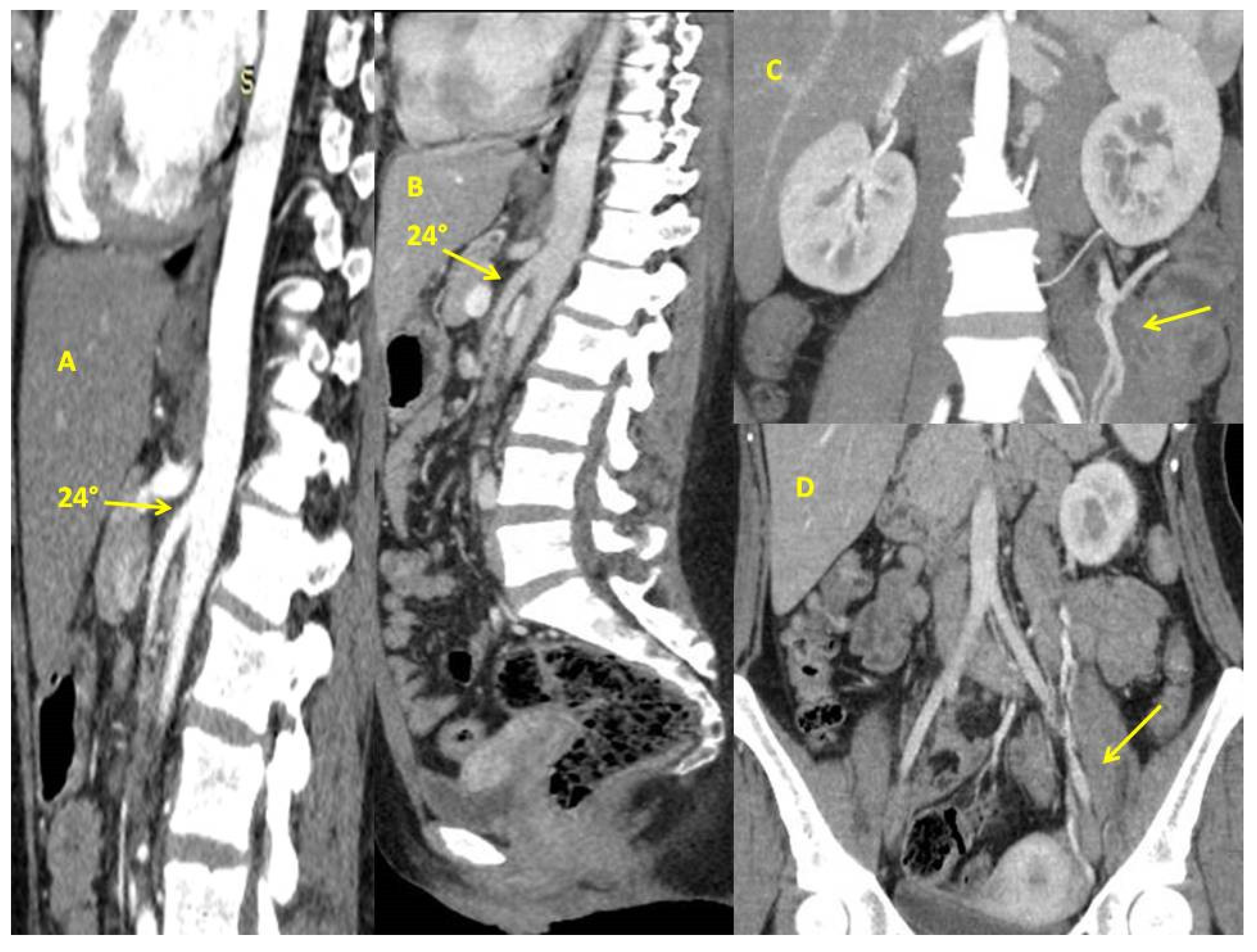
Figure 3.
Aorto-mesenteric angle(24º).Fig. A, arterial phase; Fig. B, venous phase B. Varicose dilatation in the left ovarian vein and parauterine veins(Fig. C and D).
Figure 3.
Aorto-mesenteric angle(24º).Fig. A, arterial phase; Fig. B, venous phase B. Varicose dilatation in the left ovarian vein and parauterine veins(Fig. C and D).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



