
Submitted:
04 September 2024
Posted:
04 September 2024
You are already at the latest version
Abstract
Chemical plants are characterized by the management and operation of various hazardous materials; thus, accident risk is inherently high. Nevertheless, the incidence of chemical accidents in Korea has effectively stabilized, with no marked increase attributable to the implementation of systematic safety management procedures based on process safety management system principles. In June 2023, the Ministry of Employment and Labor in Korea unveiled the Serious Injury and Fatality (SIF) report, meticulously cataloging 4,432 instances of grave accidents spanning six years (2016–2021). The compilation comprises 1,834 and 2,574 cases within the manufacturing and affiliated sectors and the construction sector, respectively. This study provides an overview of each accident, and elucidates the causes, and recommends preventative strategies. The objective was to galvanize companies across various industrial landscapes and fortify their intrinsic safety management protocols by using accident data delineated per sector. Sixteen specific accident cases from the SIF report, all of which occurred in facilities regulated by process safety management (PSM), were investigated. Technical analysis was conducted, focusing on explosion accidents within the organic catalyst packaging process, notable for their unique patterns of occurrence. This analysis extended to an examination of the reproducibility of such accidents. Employing two system analysis methodologies, system theoretic accident model and process and barrier-based systemic cause analysis technique, this study provides insights into the causative factors of the accidents and formulates comprehensive strategies for the prevention of future accidents. The findings will contribute significantly to reducing the risk of accidents within the catalyst packaging domain and assist in the development of robust recurrence prevention measures.
Keywords:
process safety management
; System Theoretic Accident Model and Process (STAMP)
; Barrier based Systemic Cause Analysis Technique (BSCAT)
1. Introduction
Various chemical substances have been produced with the advancement of science and technology and the expansion of chemical plants, leading to a transformation of the industrial structure towards the production of essential products using these chemicals. Consequently, the proportion of chemical substances used by humans has increased, increasing human dependence on these substances [1]. According to the American Chemistry Council, the global production of chemical substances exceeds 400 million tons annually, and the demand for chemical and petrochemical products is increasing annually [2,3]. Thus, the careless/unsafe production, use, storage, and transportation of chemical substances may result in accidents such as fires and explosions. In particular, fires and explosions can negatively affect human health, and in extreme cases, lead to large-scale fatal accidents [4,5]. Owing to some of the properties of chemical substances, such as flammability, reactivity, and toxicity, they are also considered potential threats to human life and the natural environment [6,7]. For example, the nitrocellulose cotton fire leading to an ammonium nitrate explosion at Tianjin Port, China in 2015, and the ammonium nitrate explosion at the Port of Beirut, Lebanon in 2020, resulted in massive casualties and economic damages [8,9]. Generally, chemical accidents occur at a larger scale compared to general industrial accidents, and potentially pose a greater risk to public safety; thus, it is imperative to establish and maintain safety rules based on the hazardous nature of chemicals to safely manage and operate processes in the chemical industry [10,11]. Additionally, although extensive preventative activities have been applied, such as developing technologies to enhance safety for the prevention of chemical accidents, introducing changes to the role of safety departments within organizations, and setting systematic chemical accident prevention standards by creating chemical accident databases, along with providing incentives, most countries focus their policies on strengthening regulations and systems related to the safe management of chemical substances for the prevention of chemical accidents [12].
Process safety management (PSM) is a highly representative systemic chemical safety management system and is administered by the Occupational Safety and Health Administration (OSHA) in the United States. PSM includes safety regulations necessary for the operation of chemical plants, such as safe operating procedures; education for employees, including workers; management measures to ensure the mechanical integrity of equipment; process hazard analysis; and process safety management. The PSM system in the U.S. has been criticized for primarily focusing on workplace safety and worker protection; however, additional systems are being implemented by the Environmental Protection Agency (EPA), including off-site consequence analysis (OCA) related to chemical accident simulation and the risk management plan (RMP) for accident risk analysis and response [13].
The Korean process safety management (K-PSM) ) system (based on the U.S. system) is composed of 12 elements and was first established and operated in 1996 in accordance with the Industrial Safety and Health Act. The hydrofluoric acid accident that occurred in Gumi in 2015 was a turning point, as it highlighted that accidents caused by chemical substances impact not only the individuals within the factory, but can also significantly contaminate the surrounding environment and negatively affect nearby residents. Consequently, the Ministry of Environment in Korea introduced the OCA and RMP systems from the U.S. and established and operated the Chemical Substance Management Act. Owing to the various chemical accidents that have occurred in Korea, regulations and legal provisions related to chemical substances have been continuously strengthened. However, this has led to criticisms regarding the imposition of excessive administrative regulations [14]. The reason why accidents are difficult to prevent, despite the strengthening of various regulations and laws, is that most of the causes of safety accidents in factories are associated with human error [22]. Therefore, accident investigation researchers have recognized human error and accident models as the key factors for the safe operation of the system, and have conducted many related studies [18].
Dr. Leveson from the Massachusetts institute of technology (MIT) proposed that, as activities within organizations have expanded into more complex relationships than in the past, a comprehensive and integrated systemic analysis is required in addition to sequential analysis methods from various perspectives, including social, technical, and organizational, to prevent accidents within organizations [15,16]. There are various systems thinking analyses and investigation techniques (Figure 3), and they are generally categorized into three generations based on their thinking model [23].
The first-generation accident survey model was based on linear cause-effect models, such as the well-known domino and FTA models. In this model, accidents occur in a linear causal relationship with a root cause of the accident [24]. Accordingly, the model demonstrates that accidents can be prevented by eliminating only their root causes However, as more accidents occurred later, it became necessary to expand human and organizational factors and identify potential accident factors, thus the second-generation accident investigation model was created in the 1990s.
The second-generation model is known as the Swiss cheese model, which is based on an epidemiological model. In the first-generation accident investigation model, when the cause of the accident was identified as human error, no further accident analysis was conducted. However, the second-generation model included the behavioral factors of the accident victims and the management problems in the organization. The second-generation model was more effective than the first in investigating accidents caused by various and complex factors, but the second-generation model also assumed a linear causal relationship, which limited its ability to clearly analyze accidents caused by complex interactions [23].
The third-generation accident investigation model is a systemic investigation technique based on the systemic model, in which accidents are caused by emergent properties, where various factors in an organization interact in an unexpected and nonlinear manner [25,26]. Of these systematic accident investigation techniques, AcciMap was applied in the 1990s, and the system theoretic accident model and processes (STAMP), CREAM, and functional resonance analysis method (FRAM) have been used for accident investigations and research since the 2000s [27].
The STAMP model is an analysis method released in 2004 to overcome the limitations of the sequential accident analysis of the first- and second-generation accident investigation models [28]. This model consists of a hierarchy of control structures for each stage, including system development and operation structures. The upper structure of the model determines safety-related policies, internal standards, and procedures, and the lower structure includes procedures or controls that must be operated to realize the policies and procedures [15,16]. STAMP is a top-down analysis model, which has the advantage of enabling various analyses of accident-related causes by including software, people, organization, procedures, and safety culture as the main factors for accident occurrence even in complex structures [29,30]. Therefore, STAMP can be applied to various types of accident analyses [20].
The FRAM models the nonlinear interaction of system functions during the accident process under the premise that accidents occur when normal variable factors in the system form unexpected combinations. Although it is a functional model that helps analysts understand the functionality of the entire system, it is also applied to safety models because such models can be used for accident analysis and risk assessment. FRAM is based on the concepts and principles of Safety II and resilience engineering, a new safety paradigm [25,31].
Various models can be used for accident investigation depending on their characteristics. Of the 216 accident investigation reports written in the past 20 years, 63 were conducted using accident investigation methods, including STAMP, AcciMap, HFACS, FRAM, and FTA [33]. STAMP is the most commonly used model for systemic accident investigations, as it is useful for analyzing accidents caused by complex systems and the relationships between stakeholders involved in the decision-making process. FRAM is useful for job analysis, function assignment, accident analysis, hazard/risk assessment, and impact analysis of changes such as design alterations and improvements [32]. In South Korea, various systematic accident investigation studies have been conducted using the STAMP model. This technique is mainly used to determine organizational and systematic recurrence prevention measures by analyzing the lack of legal obligation measures, incorrect decisions and defects, and policy errors for each function of the government, original contractors, suppliers, production departments, workers, production processes, and facilities involved in accidents related to chemical handling in plants [34].
In this study, based on the technical analysis results of fire and explosion accidents that occurred during the packaging of organic catalysts in a chemical plant, we further analyzed the causes of accidents from a barrier perspective using the barrier-based systematic cause analysis technique (BSCAT), an accident investigation technique provided by DNV. The BSCAT is based on the systematic cause analysis technique (SCAT), an accident investigation technique introduced by Dr. Bird in 1985. This accident investigation technique focuses on identifying the basic/root cause of accidents and control areas for improvement actions based on the direct cause identified by the accident investigator [21]. BSCAT analyzes accidents based on the barriers involved in preventing the spread of chemical accidents in factories with complexities among various causes and factors related to their occurrence, and the barrier is the concept of containment of threat factors [35].
The organic catalysts involved in this accident investigation are classified as Class 3 dangerous goods (spontaneously combustible and water- reactive chemicals) under Korea's Dangerous Goods Act, and there have been numerous fires involving these materials in South Korea and Japan. In Korea, there were a total of 104 fires caused by water reactive chemical between 2013 and 2017 [36]. In Japan, a numerous accidents caused by alkyl aluminum, a water-reactive chemical, occurred between 2000 and 2016, and more than a dozen of these accidents are well known, thus the National Fire Research Institute of Japan established technical standards for extinguishing alkyl aluminum-induced fires. Most of the alkyl aluminum-induced fire accidents in Japan were the result of a leakage inside the facilities related to the handling of the substance, internal explosions due to abnormal reactions during processing, or leakage during packaging [37]. Because prevention and response are important for incidents involving spontaneous combustion and water-reactive chemicals, identifying the barriers involved in blocking and responding to accident threats that can cause such accidents is important [35]. Based on technical analysis of accidents and results of a BSCAT analysis, this study aimed to conduct a systematic analysis of the relationship between various factors such as safety policies, internal standards, procedures, workers, and organizational structure related to organic catalyst explosion accidents using the STAMP model [19]. In addition, the relationship and role complementarities between various departments involved from the research stage to the process establishment, risk assessment, and work procedure establishment stages through the step-by-step application of various analysis models was demonstrated, and comprehensive appropriate recurrence prevention measures are proposed.
2. Materials and Methods
2.1. Materials
A comprehensive analysis was conducted on a dataset comprising 4,432 severe accidents identified over six years from 2016 to 2021. These data were extracted from the Serious Injury and Fatality (SIF) report that was publicly released by the Ministry of Employment and Labor in South Korea in June 2023. The dataset included 1,834 cases related to manufacturing and associated industries and 2,574 cases associated with the construction sector. The initial phase of the analysis involved categorizing accidents associated with the handling of specific hazardous materials, namely explosive, water-reactive, spontaneously ignitable liquid/solid, and flammable liquid materials. Following this categorization, a subset of 62 cases in which the causative agent was identified as a flammable material was further delineated for a more detailed investigation. Among these 62 cases, 16 occurred within chemical and rubber product, active pharmaceutical ingredients, and petroleum product manufacturing plants. These industries fall under the jurisdiction of Process Safety Management (PSM) workplaces, thus warranting an additional layer of scrutiny. An in-depth examination of these 16 cases was subsequently undertaken to gain insight into the summaries of the accidents and their underlying causes, the findings of which are presented in Table 1. Table 1 illustrates that a significant proportion of accidents related to the handling of hazardous materials predominantly occurred during raw material input, cleaning processes, and equipment cutting. However, a particular fire/explosion accident in the catalytic process in May 2020, was uniquely identified as having occurred during the product packaging process. This anomaly prompted a more focused analysis.
In May 2020, an accident occurred during the packaging of catalyst products at a PSM facility, and the analysis data from the Occupational Safety and Health Agency were documented by KOSHA-MIA-202014. summary of the accident is presented in Table 2.
The Occupational Safety and Health Agency analyzed the accident in which a worker died due to an explosion during the operation. The accident occurred as a sequential occurrence of two events (Table 3). The first event was as follows: during the packaging process, in a state where the catalyst transfer pipe and catalyst packaging container were not properly connected, external air flowed into the packaging container through the gap between the pipe and container. Subsequently, a reaction occurred between the catalyst inside the container and air (Figure 1). Because of this reaction, high pressure formed inside the packaging container, which is relieved through the process safety valve (PSV), and catalyst dust burst into the packaging room, causing a dust explosion in the room.
To clearly analyze the cause of the accident and establish effective recurrence prevention measures, we applied the research methodology described in Section 2.2.
2.2. Methods
2.2.1. Procedure
To dissect the intricacies of this fire/explosion accident, a dual-pronged approach, encompassing both technical and systemic analyses, was adopted. As shown in Figure 2, the framework for this analysis was meticulously followed by using accident data compiled by the Occupational Safety and Health Agency (KOSHA), a premier national safety organization. Using this methodological approach, the complex interplay of factors that culminated in the accident was determined, providing a holistic understanding of the causative elements and potential preventive measures.
2.2.2. Systematic Accident/Accident Analysis
Accident investigation techniques have been developed in the order of technology, human factors, and sociotechnical systems (Figure 3), and are applied to accident investigations according to the characteristics of these techniques.
In this study, the STAMP (Figure 4) and the (BSCAT methods (Figure 5) were applied for the systemic analysis of the accident and were technically scrutinized. The interrelationships among various elements such as accident-related safety policies, internal standards, procedures, personnel, and organizational structures were analyzed based on systemic components of the two methods.
Based on the accident scenarios derived from the technical analysis results, a root cause analysis of the accidents was conducted using the BSCAT method. Subsequently, the focus was placed on identifying the barriers that could prevent progression to the next stage during the accident, and analyzing the root causes of the barriers’ failure to operate.
3. Results
3.1. Technical Analysis Results
The details of the investigation are provided in the KOSHA-MIA-202014, conducted by the KOSHA, postulates that the accident was caused by the unintended introduction of external substances (e.g., air or water) into the catalyst packaging container. Considering the manufacturing and facility attributes prevailing at the time of the accident, potential scenarios facilitating the ingress of material into the packaging container were meticulously analyzed and are presented in Table 4. This comprehensive analysis revealed that the entry of external substances into the packaging container was a circumstance unique to the catalyst packaging process. Following this revelation, a technical verification plan was formulated to evaluate the feasibility of external substances penetrating packaging containers. The failure to implement safety location at the discharge section of the PSV, is implicated as the cause of the second event (Table 3), which is a transgression of domestic safety regulations. Consequently, this aspect was omitted from the technical verification elements examined in this study. The primary objective of the technical verification conducted in this study was two-fold. First, we aimed to determine whether external substances such as air or water could potentially infiltrate the container via minor leaks stemming from imperfect connections between the packaging container and attached pipes. This scenario was evaluated during the procedure of infusing nitrogen at a pressure of 5 barg through pipes connected to a packaging container. Second, we sought to ascertain the reaction time between the substances that had entered and the catalyst chamber. This dual approach was key in unearthing the causative factors of the accident and propelling the study towards achieving a holistic understanding of the event.
3.1.1. Material Characteristics/ Properties Analysis
According to KOSHA-MIA-202014 from the Occupational Safety and Health Agency in South Korea, the substance related to the accident is methylaluminoxane (MAO), which is an iso-Bu Me, branched, cyclic, and linear aluminoxane. This substance is classified as a Class 3 hazardous material according to the national criteria for dangerous materials classification. Its molecular weights and structural formulae are listed in Table 5. Class 3 dangerous materials are spontaneously combustible and water-reactive chemicals that react upon contact with air or moisture.
In polymer-producing petrochemical processes, the methylaluminoxane (MAO) is used as a co-catalyst that aids in the activity of metallocene, the primary catalyst used in polymer manufacturing, which, when combined, creates a supported catalyst (Figure 6).
3.1.2. Evaluation on Reactivity with Air
MAO is categorized as a Class 3 hazardous material with a propensity to react with air or water. To determine the thermodynamic nature of this reaction (exothermic or endothermic) a detailed analysis of the reaction heat was performed using computational chemistry tools (Table 6).
For this analysis, the enthalpies of formation for both the reactants and products involved in the chemical reaction were theoretically computed and juxtaposed for predictive insight. Table 6 shows that the enthalpies of the products, resulting from reaction of MAO with oxygen or water are significantly more stable than those of the reactants.
This revelation conclusively confirms that the interaction between MAO and water or air is exothermic. Considering this thermodynamic characterization, the actual reactive behavior of MAO in conjunction with the metallocene-supported catalysts in the presence of air was observed. In a controlled environment within a fume hood, 100 g of the supported catalyst was transferred to a stainless-steel carrier. Adorned in flame-retardant apparel and equipped with essential safety gear, a researcher ensured thorough mixing of the supported catalyst and air by agitating the carrier. The ensuing reactive behavior between the supported catalyst and air was monitored at 1-s intervals.
As shown in Figure 7, upon exposure to air, the MAO+metallocene-supported catalyst exhibited a noticeable increase in temperature after 20 s, indicated by the color change. Subsequently, at the 30-s mark, smoke was observed, accompanied by ignition. Table 6 and Figure 7 corroborate that in the event of air infiltration during the catalyst packaging process, the exothermic reaction could potentially yield the reactants and generate carbon monoxide and water within the container. This comprehensive analysis underscores the importance of maintaining an air-tight environment during catalyst packaging to pre-emptively mitigate the risk of hazardous reactions.
3.1.3. Assessment on Air Introduction during Packaging Process
Upon exposure to air, the MAO+metallocene-supported catalyst reaction initiated after 20 s. This finding highlights the need for stringent preventive measures against air entering the packaging container throughout the packaging process. The risk assessment report related to this accident, which was associated with the catalyst packaging operation, failed to adequately address the potential hazards stemming from air infiltration during the packaging stage. After the accident, a thorough site investigation revealed that the bolts connecting the piping to the packaging container were not secured according to the prescribed torque standards; therefore, we hypothesized that air entered through a gap between the packaging container and piping. To validate this hypothesis, the packaging equipment was reassembled to replicate the conditions and status at the time of the accident, and an experiment was performed to evaluate the possibility of air entry through the identified gap. By leveraging the principles of Bernoulli's equation, as shown in Figure 8. The experiment was conducted to investigate whether the pressure changes occurring around the gap could facilitate external air entry into the packaging container.
Two methodologies were considered: employing actual packaging equipment and applying simulation techniques using computational fluid dynamics (CFD). However, in this study, a deliberate gap was introduced at the connection point on top of the packaging container, using the same equipment used during the accident, as shown in Figure 9. The aim was to determine whether air can infiltrate through this specific area.
The catalyst manufacturing process concludes with the packaging phase, where the discharge line from the vessel containing the final product, after drying, is connected to the connection point (Figure 9). An inert gas line (N2) is also connected to the discharge line during the packaging operation to mitigate the risk of a reaction between the catalyst and oxygen within the packaging container. While the N2 line maintains a pressure of 5 barg, the structure of the packaging container permits the release of N2 through the upper vent line, maintaining the pressure of the packaging container below 0.5 barg.
For the experimental analysis of air infiltration, an artificial gap was created between the piping and upper part of the packaging container. By intentionally under-tightening the four bolts on the flange and connecting the piping to the packaging container, a gap of approximately 1 mm was maintained, as shown in Figure 10. By maintaining the N2 pressure at 5 barg, the product input valve on top of the packaging container was opened by approximately 30%. From the observations, we observed that smoke from the smoke stick entered the flange gap swiftly. Based on the experimental results, the pressure change inside the pipe was simulated using the Ansys fluent simulation software (version 11.0) (Figure 11). As shown in Figure 11, a negative pressure was formed in a certain section around the gap between the flanges, and a flow rate of approximately 20 m/s was created in this section. Ansys fluent simulation software was used to accurately reflect the flow and pressure formation process of gas supplied in a high-pressure state within a pipe with a complex structure, and to calculate numerous finely divided cells simultaneously. After 3D modeling the pipe, its volume was divided into 1,000,000 cells based on a volume of 0.003m3 for accurate calculation, and each cell was calculated separately. As this did not consider CFD analysis, the CFD calculations are not included.
This reconstruction test and analysis of the CFD experiment conclusively demonstrated that if the internal structure of the packaging container’s piping is similar to the conditions necessitated by Bernoulli's equation, the external air has the potential to infiltrate through minute gaps. Therefore, it is important, especially when dealing with products that are sensitive to air, to ensure airtight connections and eliminate even the smallest gaps. Furthermore, if any small gaps arise between the piping and packaging container, considering a straight piping design without changes in the inner diameter of the piping is crucial to prevent the infiltration of external air into the packaging container.
3.2. Systematic Analysis by Accident
The technical analysis of accidents that occurred within the PSM facility was conducted using the STAMP and BSCAT methods. Systematic recurrence prevention measures have been established based on the fundamental causes of accidents identified through these methods.
3.2.1. BSCAT Analysis
To prevent the recurrence of this accident, the design and management of manufacturing facilities from the research phase to the construction of production equipment in the plant must be done with the utmost care to ensure that there is no air infiltration. Accordingly, using BSCAT, an analysis was conducted sequentially from the causes of improper connection between the packaging containers and piping, up to the barriers identified at the time of the accident.
Figure 12.
A flow chart showing the barrier-based systematic cause analysis technique (BSCAT) analysis of the accident.
Figure 12.
A flow chart showing the barrier-based systematic cause analysis technique (BSCAT) analysis of the accident.
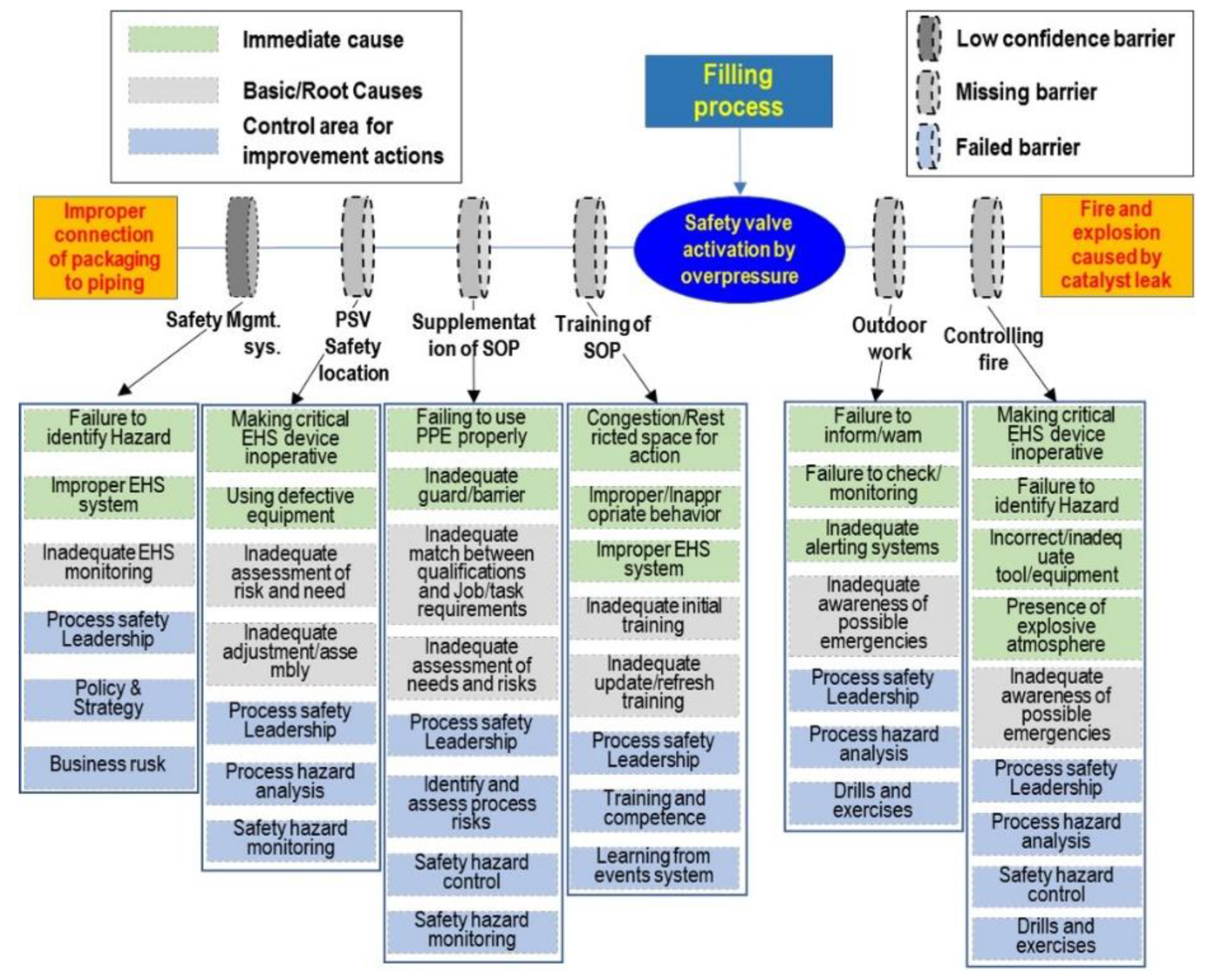
The prevention controls identified using BSCAT analysis included education on standard operating procedures (SOP), supplementation of SOP, safety location of PSV, and the “safety mgmt. system”. The accident could have been prevented if the prevention controls were properly executed before the workers performed the task. In addition, even if various prevention control items were not properly executed, the packaging process would have been organized as outside work when designing the process from the mitigation control perspective, or if the indoor fire protection facilities were properly configured, the accident would not have caused significant losses.
The barriers identified through BSCAT analysis are listed in Table 7. Predominantly, there was no connection between the safety valve discharge line and the combustion/absorption/capture/recovery facilities (no barrier was present), and the safety management system was an unreliable Barrier. Furthermore, there were no additions to the work procedure documents (a barrier that did not exist) and education on work procedures (another nonexistent barrier). From the onset of the accident to the spread of damage, the analyzed barriers were outdoor operations (barrier was not present) and fire safety facilities (barrier was not present).
The BCSAT analysis identified the following areas for improvement to prevent accident recurrence: process safety leadership, hazard assessment, risk management, emergency response, and risk monitoring (Figure 13).
3.2.2. STAMP Analysis
Through meticulous technical analysis and the application of BSCAT, the causes of the accident, along with managerial lapses and deficiencies present at the time of the accident were identified. The roots of these managerial shortcomings can be traced back to the initial phases of chemical process research and development, extending to the pre-commissioning stage. During these critical periods, the identification and subsequent assessment of risk factors associated with materials, processes, and equipment were inadequate, resulting in the oversight of potential hazards. These risk factors necessitate vigilant management, either by designated personnel at each stage of the process or through comprehensive reviews conducted by pertinent departments. However, even in moments leading to the accident, these overlooked risk factors remain undetected, culminating in an unfortunate event. Ensuring a proper connection between the packaging container and piping is a seemingly straightforward and crucial process during product packaging operations; it is imperative that this is systematically evaluated during the risk assessment phase. The lack of a secure connection could allow air to infiltrate the packaging container, posing a significant risk of fire and explosion. Additionally, a comprehensive preoperative safety check should be an integral part of the procedures leading up to the commencement of work. By dissecting the identified factors through the lens of work stages and inter-organizational relationships, we created a visual representation (Figure 14). This approach not only clarifies the causative factors but also emphasizes the pivotal role of rigorous managerial oversight in preventing such accidents in the future.
4. Discussion
The analysis of the safety control structure model included stages from early research and development (R&D), scale-up operations, and design and installation associated with new factory establishments, including the production team, safety and environment team, company management, Ministry of Employment and Labor, Occupational Safety and Health Agency, and research institutes. Using this model, communication strategies and necessary internal organizational improvements for the prevention of recurring similar accidents can be established (Table 8).
The data presented in Table 7 and Table 8 highlights the need to meticulously design chemical processes that minimize the potential influx of external substances into the system. This necessitates integration of the identified reaction requirements and associated hazards, as discussed during the research phase, into the reactor design stage. Subsequently, it becomes the duty of the controller to proactively identify potential risk factors during the scale-up phase and throughout the establishment and operation of the actual production process, ensuring that these risk factors are considered in the risk assessment. In the permitting stage, it is crucial to compile a comprehensive checklist of items that require review in accordance with the regulations governing the establishment of new processes. A safety design, conceived from a foolproof perspective and informed by the KOSHA Guidelines and other relevant technical materials, should be executed, considering the most unforeseeable circumstances. As demonstrated in this study, the use of systematic analysis methods, such as BSCAT and STAMP, can significantly enhance the precision and clarity in identifying and understanding the root causes of accidents, especially in complex scenarios where various factors are interwoven. This approach not only facilitates a more thorough and specific root cause analysis but also contributes to the prevention of similar accidents in the future.
5. Conclusions
By investigating the technical intricacies of the causes of an accident during the catalyst packaging process, this study has successfully elucidated the immediate cause and further subjected it to a meticulous re-analysis employing systematic analytical methods. The accident analysis outcomes highlight the importance of recognizing the potential for substances to mix inadvertently during both the process design and stable operational stages, potentially resulting in an accident. It is of the utmost importance to distinctly identify these considerations during the risk assessment phase and establish, within the organization, a procedure to seamlessly incorporate risk mitigation measures for each identified risk factor into the design stage. Even if the respective risk factors are meticulously reflected in work procedures, it is crucial to adopt a 'worker-centric risk assessment' approach to mitigate the risk of accidents owing to human error. When examining chemical accidents within a PSM framework, it is easy to mistakenly attribute them to a single causative factor when solely evaluating the outcomes. However, this study showed that a systematic analysis can reveal the complex web of underlying causes that lead to these accidents. This highlights that beyond conventional accident prevention measures, such as securing additional devices and functions within the manufacturing process, there is a need for proactive management and vigilance, underpinned by clearly defined roles and responsibilities (R&R) across the departments involved in process design, operation, safety environment, and R&D. The onus is on the production and safety departments within the factory to internalize these considerations to ensure their systematic application and operation in the field, bolstered by dual or even triple verification processes, extending beyond the R&D phase. This study validated the applicability of a systematic analysis method integrating BSCAT and STAMP for both direct and root-cause analyses of chemical accidents. Moreover, it suggests that the adoption of such systematic techniques for process risk evaluation and preoperative inspections of newly established plants hold significant promise for reducing the risks associated with accidents.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
References
- Winterton, N. Green Chemistry: Deliverance or distraction? Clean Technol. Environ. Policy 2016, 18, 991–1001. [Google Scholar] [CrossRef]
- Liu, T.; Zhang, H.; Li, X.; Zhang, H. Individual factors influencing risk perceptions of hazardous chemicals in China. Environ Res. 2020, 186, 109523. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Ma, X.; Zhang, J.; Yang, Q.; Wei, K. Identifying the Weaker Function Links in the Hazardous Chemicals Road Transportation System in China. Int. J. Environ. Res. Public Health. 2021, 18, 7039. [Google Scholar] [CrossRef] [PubMed]
- Carson, P.; Mumford, C. Hazardous Chemicals Handbook, 1st ed.; Butterworth-Heinemann: Clifton Park, NY, USA, 2013; pp. 11–30. [Google Scholar]
- Li, X.; Liu, T. Community participation effects on preparedness behaviour through risk perception: Empirical data of hazardous chemicals from China. Int. J. Disaster Risk Reduct. 2020, 44, 101421. [Google Scholar] [CrossRef]
- Carpenter, D.O.; Arcaro, K.; Spink, D.C. Understanding the human health effects of chemical mixtures. Environ. Health Perspect. 2002, 110, 25–42. [Google Scholar] [CrossRef]
- Lee, D.J.; Lee, T.H.; Shin, C.H. Study on Improvement Measures for Prevention and Countermeasure of Chemical Accident. Fire Sci. Eng. 2016, 30, 137–143. [Google Scholar] [CrossRef]
- Hua, W.; Chen, J.; Qin, Q.; Wan, Z.; Song, L. Causation analysis and governance strategy for hazardous cargo accidents at ports:Case study of Tianjin Port’s hazardous cargo explosion accident. Mar. Pollut. Bull. 2021, 173 Pt B, 113053. [Google Scholar] [CrossRef]
- Samar, A.H.; Hassan, R.D.; Stefania, M.; Haytham., K.; Firas, K.; Ralph, G.D. Beirut Ammonium Nitrate Blast: Analysis, Review, and Recommendations. Policy and Practice Reviews article 2021, 9, 1–11. [Google Scholar]
- Hartmann, S.; Klaschka, U. Interested consumers’ awareness of harmful chemicals in everyday products. Environ. Sci. Eur. 2017, 29, 29. [Google Scholar] [CrossRef]
- Dong, R.; Wang, J.; Weng, S.; Yuan, H.; Yang, L. Field determination of hazardous chemicals in public security by using a hand-held Raman spectrometer and a deep architecture-search network. Spectrochim. Acta Part A Mol. Biomol. Spectrosc. 2021, 258, 119871. [Google Scholar] [CrossRef]
- White-Hunt, K.; Makower, M. The Encouragement of Technological Change; Technological Economics Research Unit, University of Stirling: Stirling, Scotland, 1981. [Google Scholar]
- Belke, J.C.; Dietrich, D.Y. The post-Bhopal and post-9/11 transformations in chemical emergency prevention and res/ponse policy in the United States. J. Loss Prev. Process Ind. 2005, 18, 375–379. [Google Scholar] [CrossRef]
- Wang, W.S.; Jeonggue, P.; Sun-yeong, G. A Study on Improvement Plans for Chemical Accident Policies and Industry Support Plans in the Chemicals Control Act (II). Basic Res. Rep. 2017, 2017, 1–163. [Google Scholar]
- Leveson, N.; Daouk, M.; Dulac, N.; Marais, K. Applying STAMP in Accident Analysis, Massachusetts Institute of Technology. Engineering Systems Division, 2003, ESD-WP-2003-02.
- Leveson, N. A New Accident Model for Engineering safer Systems. Safety Science 2004, 42, 237–270. [Google Scholar] [CrossRef]
- Lundberg, J.; Rollenhagen, C.; Hollnagel, E. The Consequences of Underlying Accident Models in Eight Accident Investigation Manuals. Safety science 2009, 47, 1297–1311. [Google Scholar] [CrossRef]
- Qureshi, Z.H. A Review of Accident Modelling Approaches for Complex Critical Sociotechnical Systems, DSTO-TR-2094, Defence Science and Technology Organization, 2008.
- Meng, X.; Chen, G.; Shi, J.; Zhu, G.; Zhu, Y. STAMP-based analysis of deepwater well control safety. Journal of loss prevention in the process industries 2018, 55, 41–52. [Google Scholar] [CrossRef]
- Zhang, Y.; Dong, C.; Guo, W.; Dai, J.; Zhao, Z. Systems theoretic accident model and process (STAMP): A literature review. Safety science. 2022, 152, 105596. [Google Scholar] [CrossRef]
- Erick, H.; Josephine, S. Study on Developments in Accident Investigation Methods: A Survey of the “State-of-the-Art”. SKI Report 2008, 2008, 50. [Google Scholar]
- Reason, J. Human error: models and management. British Medical Journal. 2000, 320, 768–770. [Google Scholar] [CrossRef]
- Hollnagel, H. Understanding accidents-from root causes to performance variability. Proceedings of the IEEE 7th Conference on Human Factors and Power Plants:1-6. 2002.
- Underwood, P.; Waterson, P. Accident analysis models and methods: guidance for safety professionals, Loughborough University. 2013.
- Hollnagel, H. FRAM: The Functional Resonance Analysis Method. Farnham, UK: Ashgate. 2012.
- Belmonte, F.; Schoen, W.; Heurley, L.; Capel, R. Interdisciplinary safety analysis of complex socio-technological systems based on the functional resonance accident model: An application to railway traffic supervision. Reliability Engineering and System Safety. 2011, 96, 237–249. [Google Scholar] [CrossRef]
- Waterson, P.; Robertson, M.M.; Cooke, N.J.; Militello, L.; Roth, E.; Stanton, N.A. Defining the methodological challenges and opportunities for an effective science of sociotechnical systems and safety. Ergonomics. 2015, 58, 565–599. [Google Scholar] [CrossRef]
- Seo, D.H.; Gae, G.W.; Choi, Y.R.; Han, O.S. Analysis of a Fire Accident during a Batch Reactor Cleaning with AcciMap, STAMP and FRAM. Journal of the Korean Society of Safety. 2021, 36, 62–70. [Google Scholar]
- Koo, C.C.; Seo, D.H.; Lee, P. H. Analysis of Explosion Accidents in a Chemical Plant using STAMP, a Systematic Cause-and-effect Analysis Technique. Korean Institute of Fire Science & Engineering 2021, 35, 17–23. [Google Scholar]
- Kee, D.H. Review and Comparison of Systemic Accident Analysis Techniques based on Literature Survey. Journal of the Ergonomics Society of Korea. 2021, 40, 55–63. [Google Scholar] [CrossRef]
- Patriarca, R.; Bergstrőm, J.; Di Gravio, G. Defining the functional resonance analysis space: Combining Abstraction Hierarchy and FRAM. Reliability Engineering and System Safety. 2017, 165, 34–46. [Google Scholar] [CrossRef]
- Cho, C.H.; Choi, S.W.; Kim, I.K.; Lee, S.H.; Kim, T.W. Study on the Chemical Accidents Investigation and Effective Response System in Korea 2020. Korean Journal of Hazardous Materials. 2020, 9, 68–75. [Google Scholar] [CrossRef]
- Wienen, H.C.A.; Bukhsh, F.A.; Vriezekolk, E.; Wieringa., R.J. Accident Analysis Methods and Models - A Systematic Literature Review, 2017.
- SEO, D.H.; Park, J.H.; Hyun, J.S.; Kim, J.H. Application Review of a Systemic Accident Analysis Method in the Field of Occupational Health -Focused on the Analysis of Methanol Poisoning Accidents Using STAMP-. Journal of Korean Society of Occupational and Environmental Hygiene. 2023, 33, 188–205. [Google Scholar]
- Robin, P.; Tony, P.; Mark, F.; Stuart, G.F. A Method for Barrier-Based Incident Investigation. Process Safety Progress. 2015, 34, 328–334. [Google Scholar]
- National Fire Information Center E-Fire Statistics. 2018.
- Report of national research institue of fire and disaster. National Research Institute of Fire and Disaster. Japan. 2018. No.124.
Figure 1.
Diagram illustrating the accident.
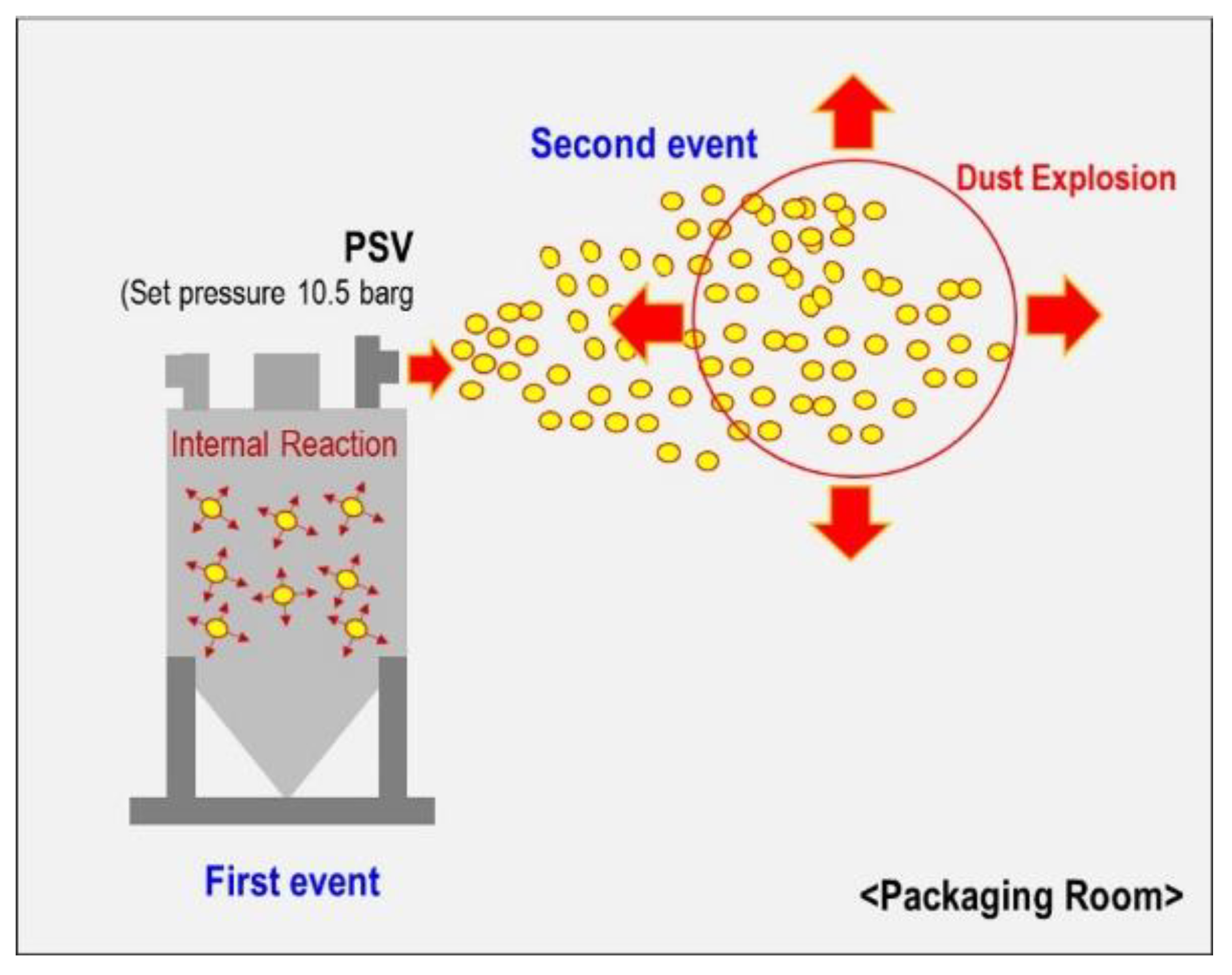
Figure 2.
Flow chart showing the accident analysis procedure.
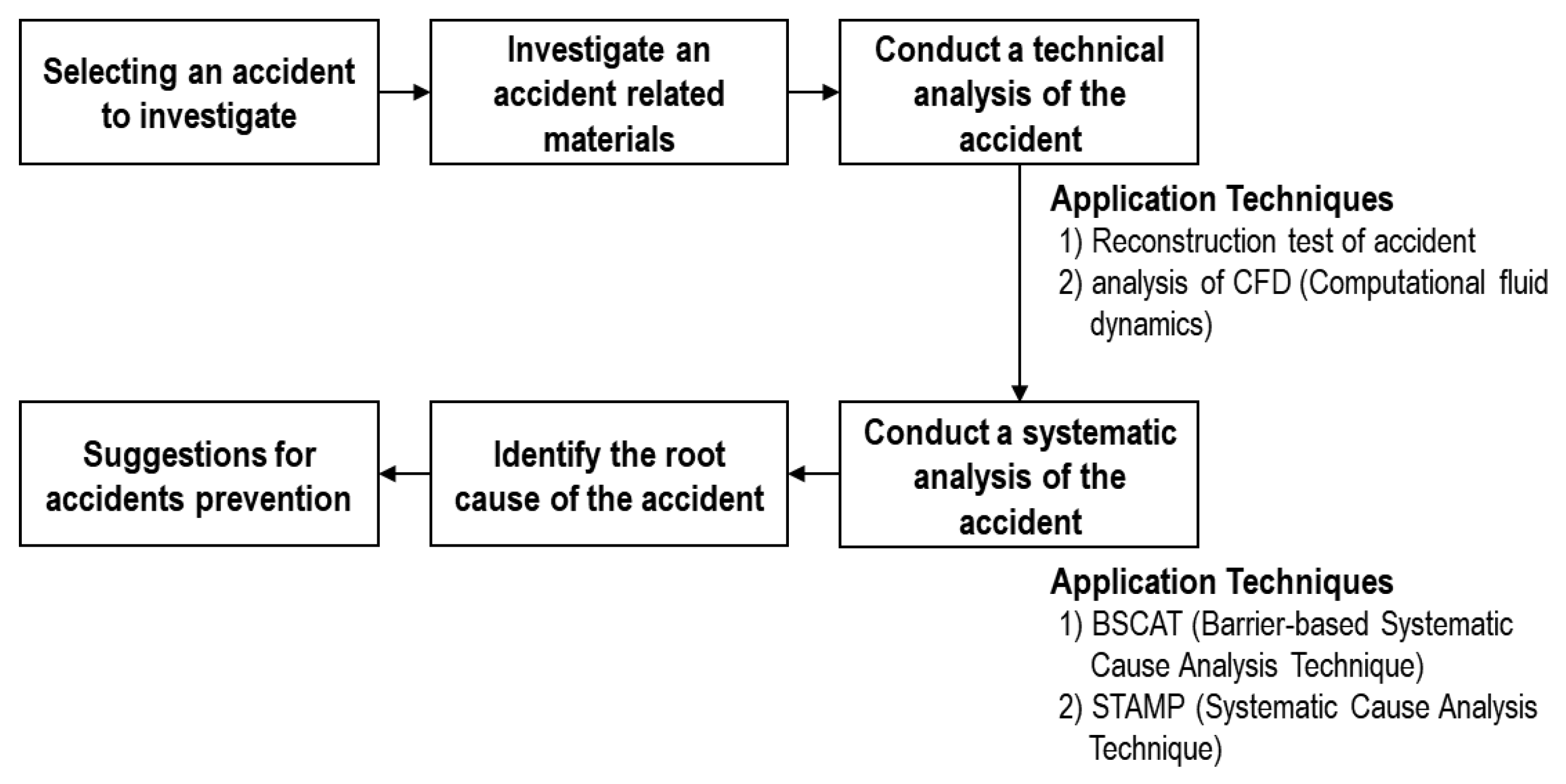
Figure 3.
A timeline of the development of methods for sociotechnical systems and safety [21].
Figure 3.
A timeline of the development of methods for sociotechnical systems and safety [21].
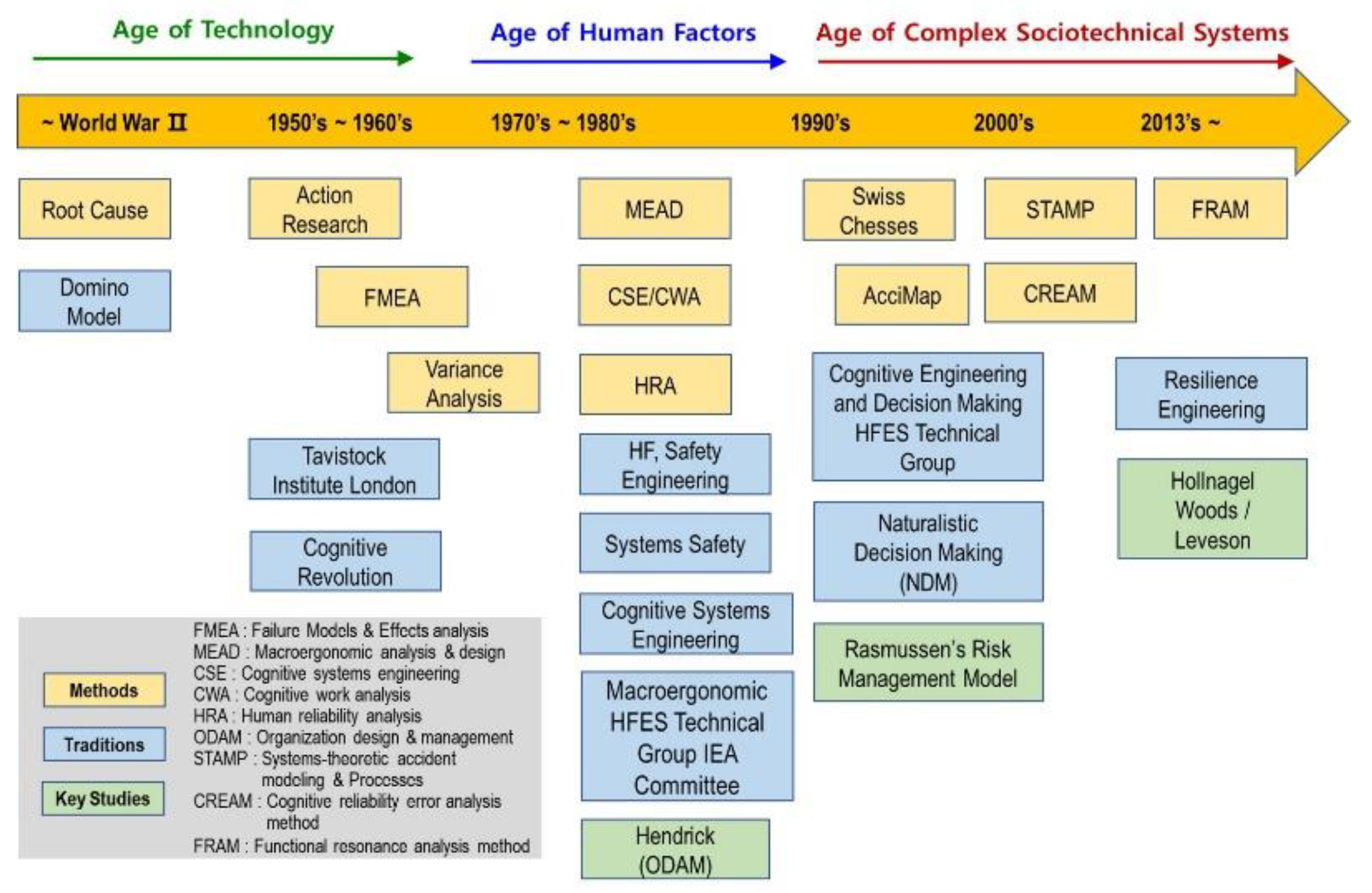
Figure 4.
Typical socio-technical control model of the system theoretical accident model and processes (STAMP) method.
Figure 4.
Typical socio-technical control model of the system theoretical accident model and processes (STAMP) method.
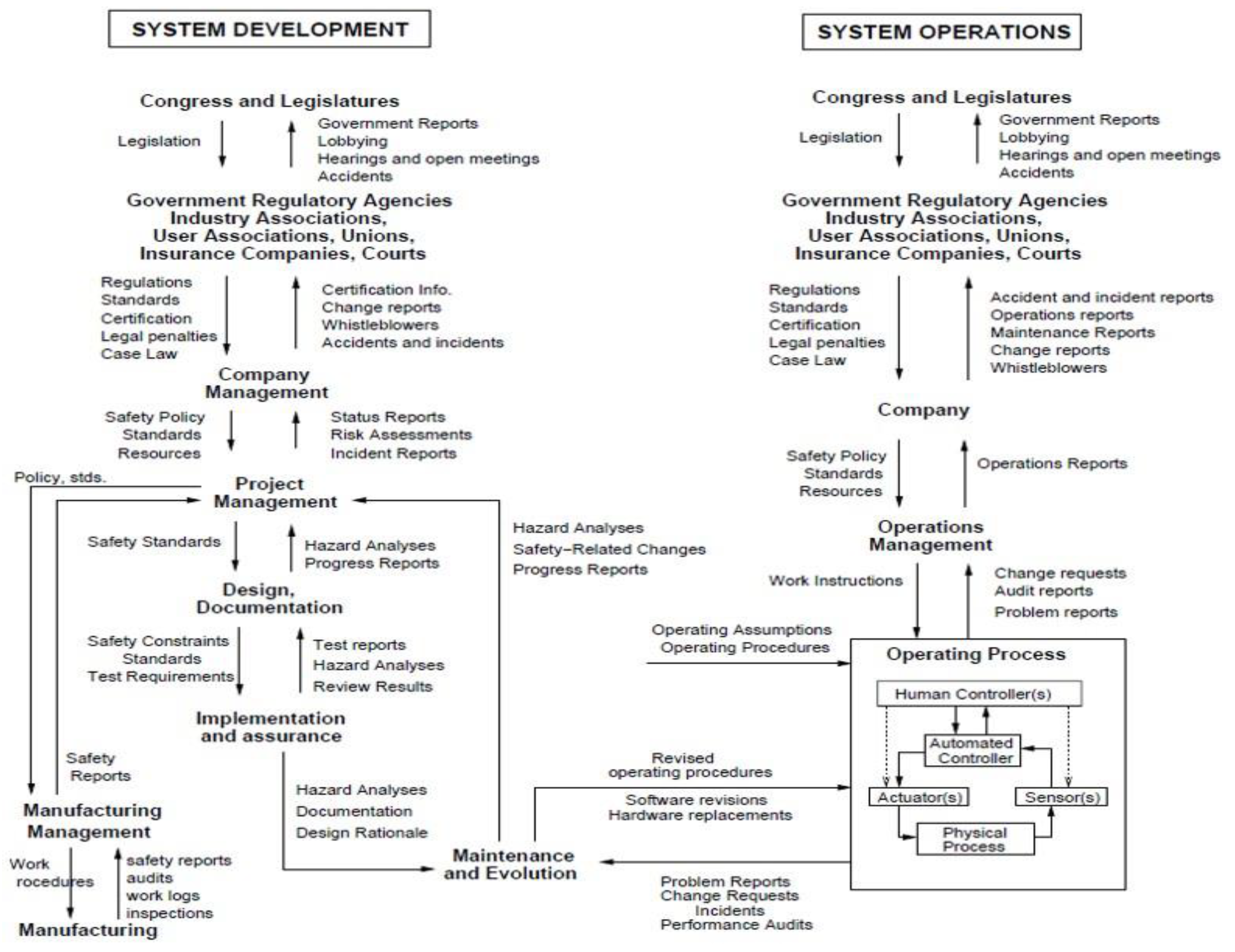
Figure 5.
Flow chart illustrating the accident root cause analysis model of barrier-based systematic cause analysis technique (BSCAT). (DNV SCAT 8.2 ver.).
Figure 5.
Flow chart illustrating the accident root cause analysis model of barrier-based systematic cause analysis technique (BSCAT). (DNV SCAT 8.2 ver.).
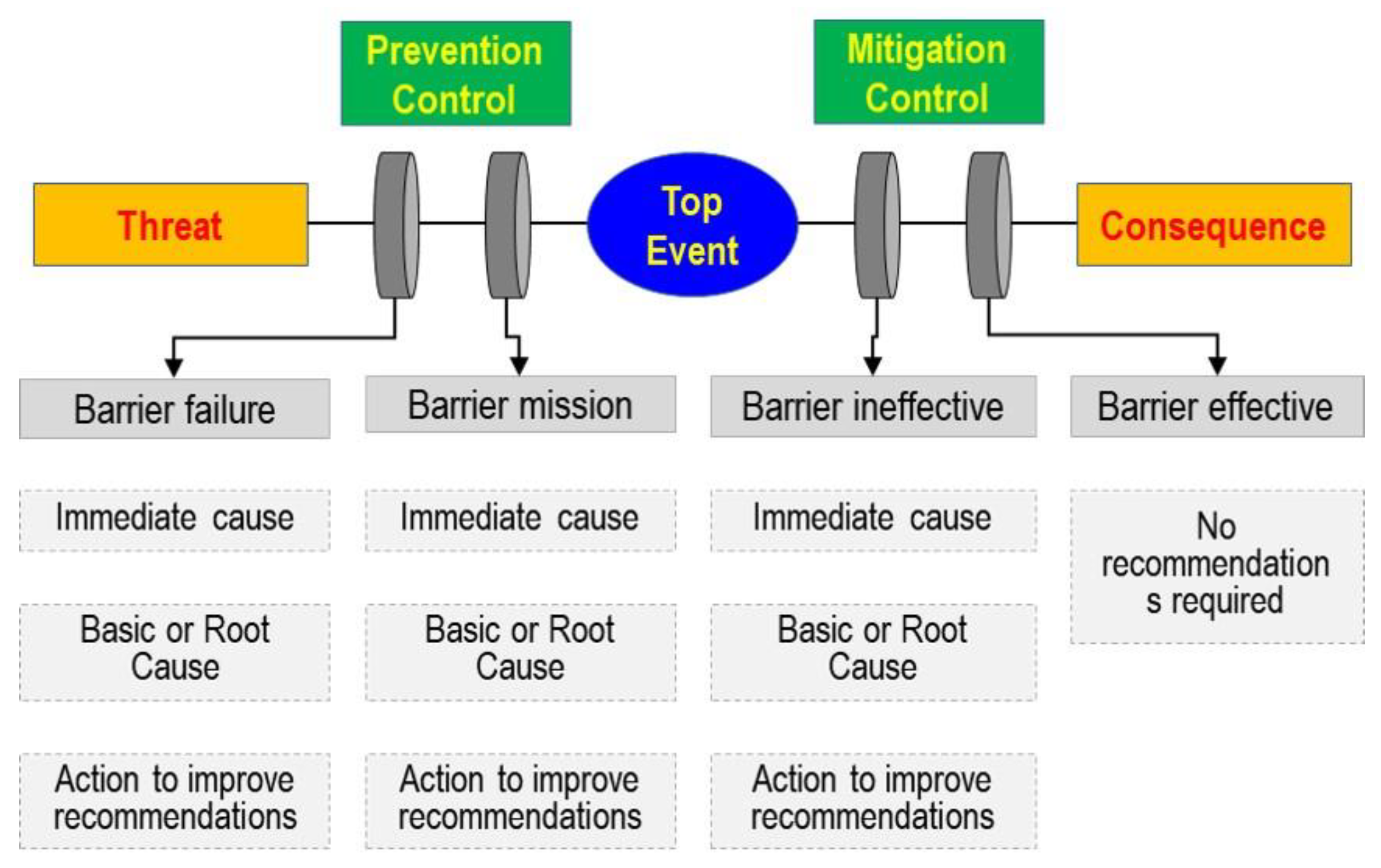
Figure 6.
Structure of supported catalyst.
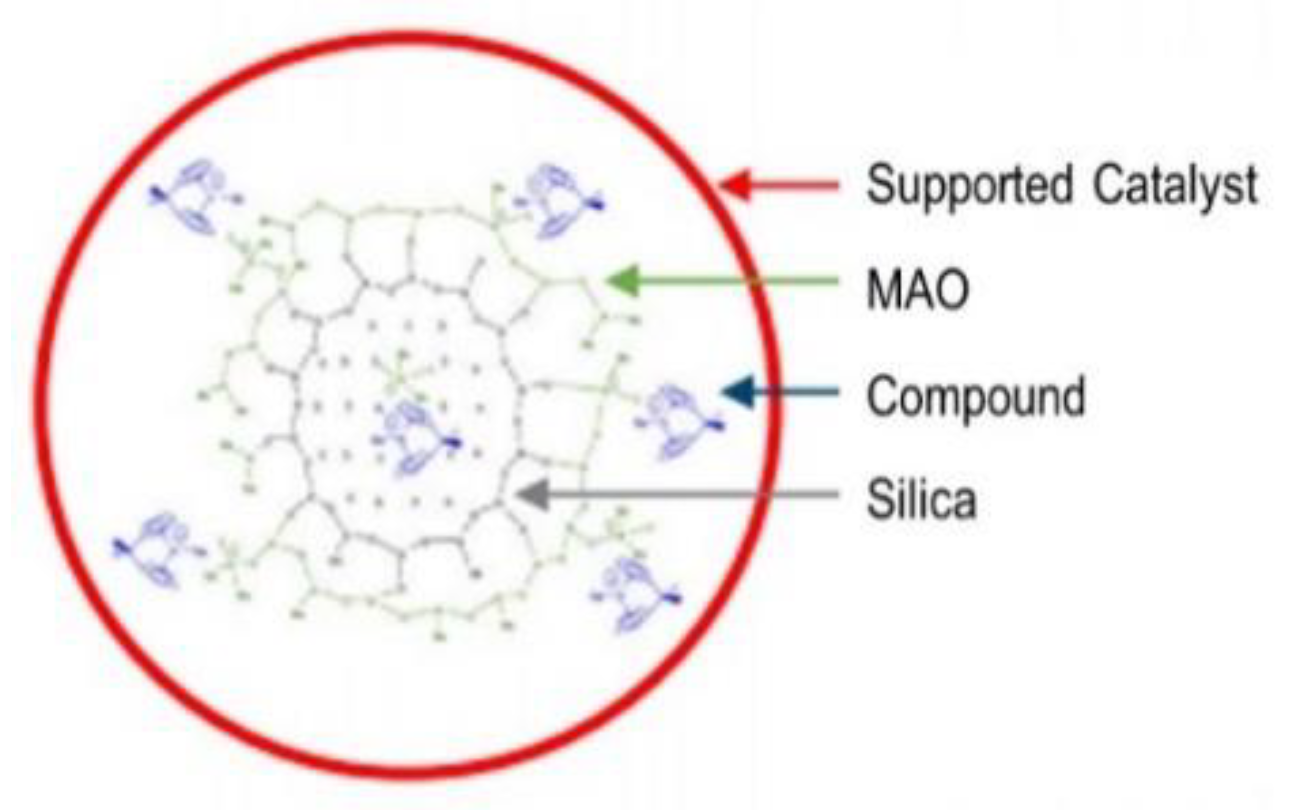
Figure 7.
Airborne exposure testing of MAO+metallocene supported catalyst (heat is generated 20 s after reacting with air). (a) Start of the experiment; (b) 20 s elapsed; (c) 33 s elapsed.
Figure 7.
Airborne exposure testing of MAO+metallocene supported catalyst (heat is generated 20 s after reacting with air). (a) Start of the experiment; (b) 20 s elapsed; (c) 33 s elapsed.
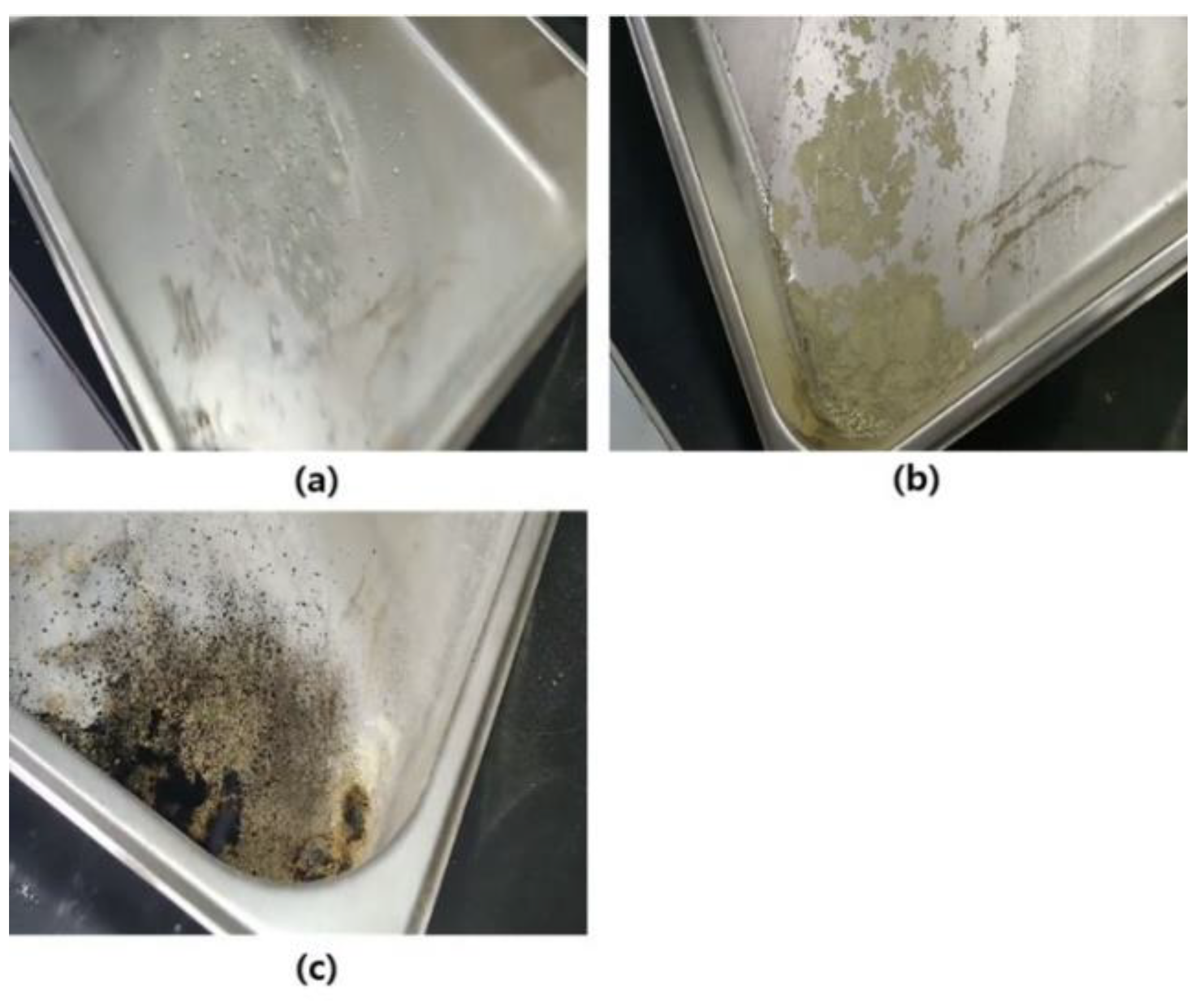
Figure 8.
Illustration of Bernoulli's equation (P1 > P2).
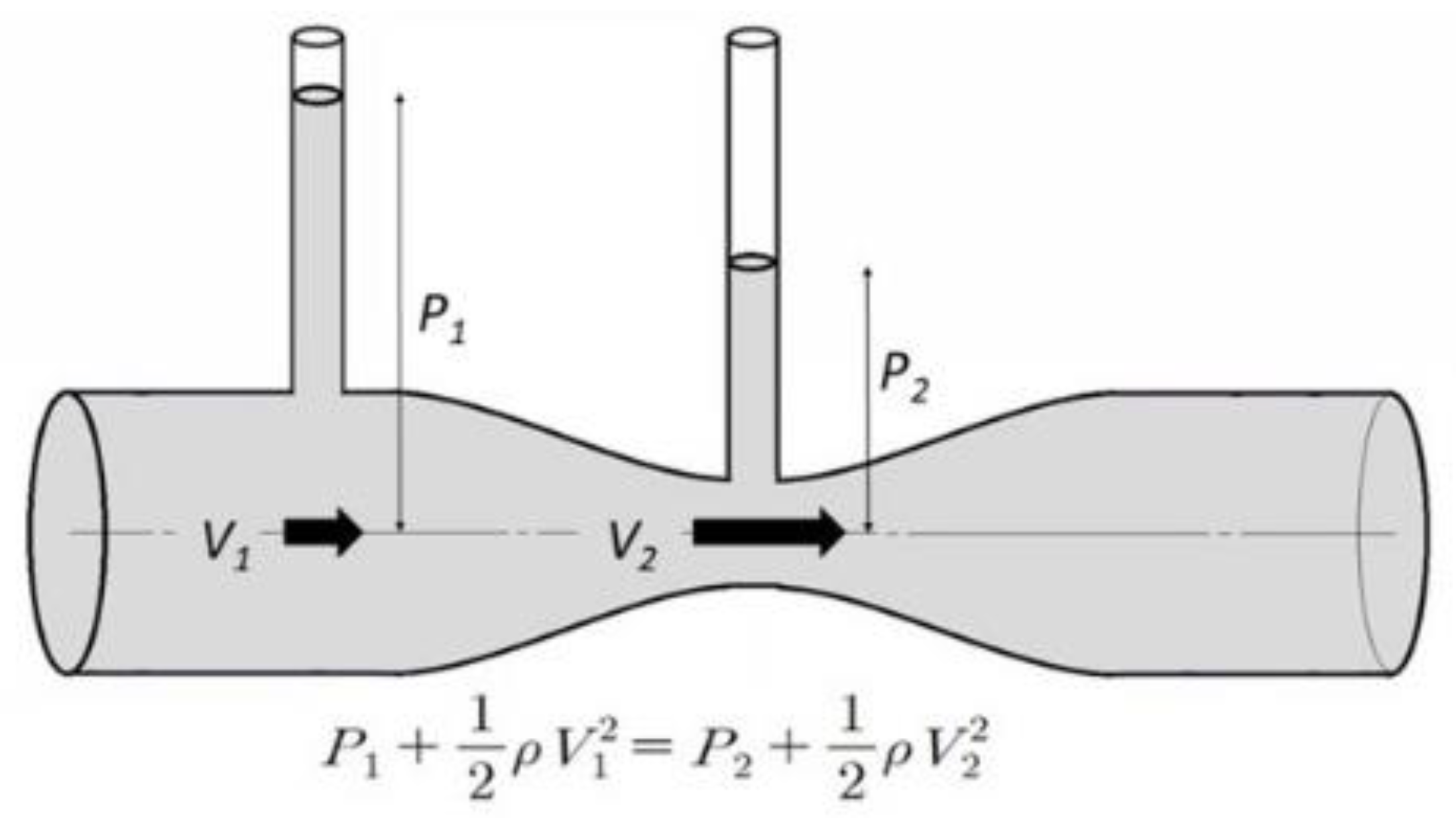
Figure 9.
A schematic drawing of the packaging container (PSV, connection point, and vent line are outlined).
Figure 9.
A schematic drawing of the packaging container (PSV, connection point, and vent line are outlined).
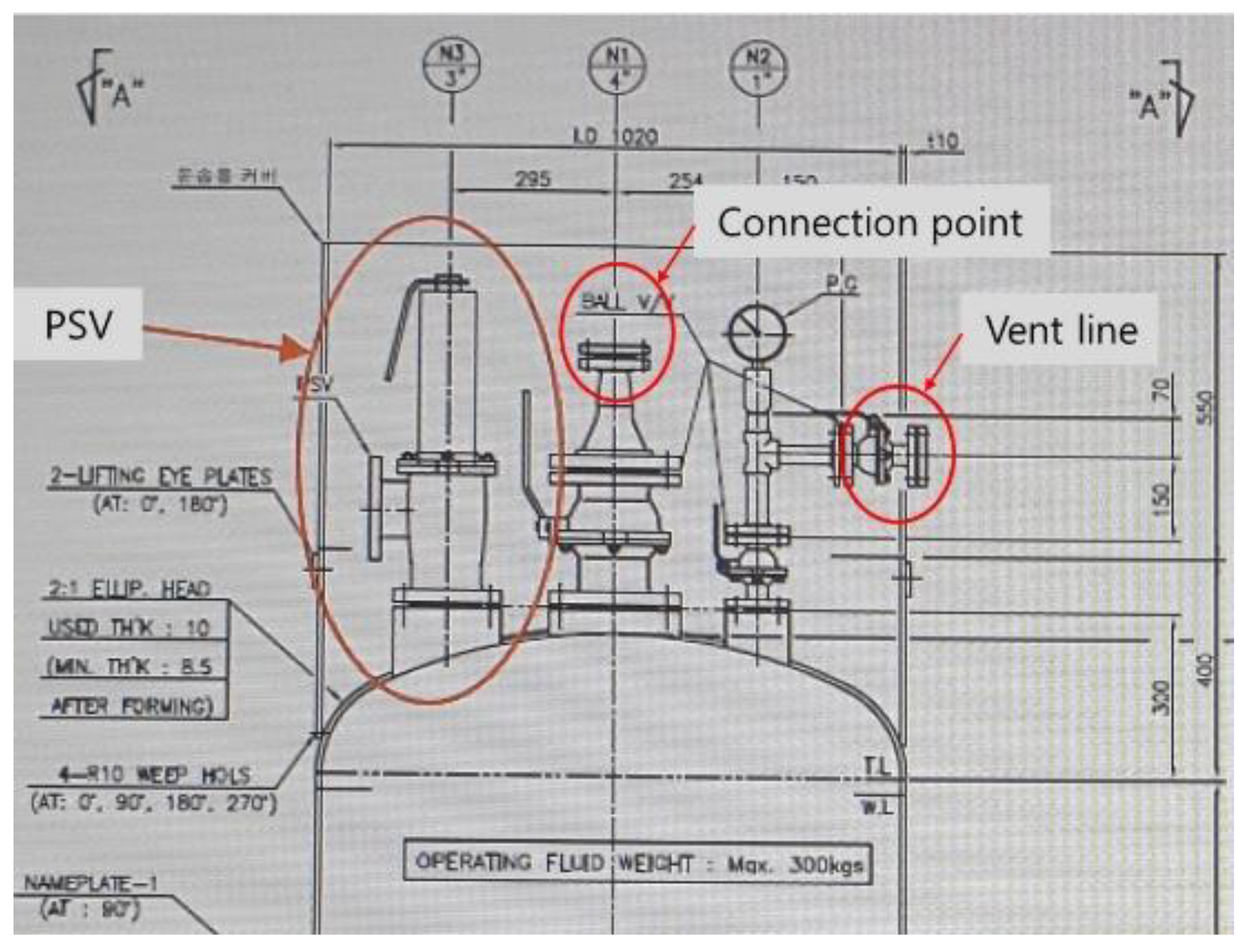
Figure 10.
Outside air entering the leak point when valve is open. (a) Start of the experiment; (b) N2 line valve open (red arrow indicates the smoke endpoint).
Figure 10.
Outside air entering the leak point when valve is open. (a) Start of the experiment; (b) N2 line valve open (red arrow indicates the smoke endpoint).
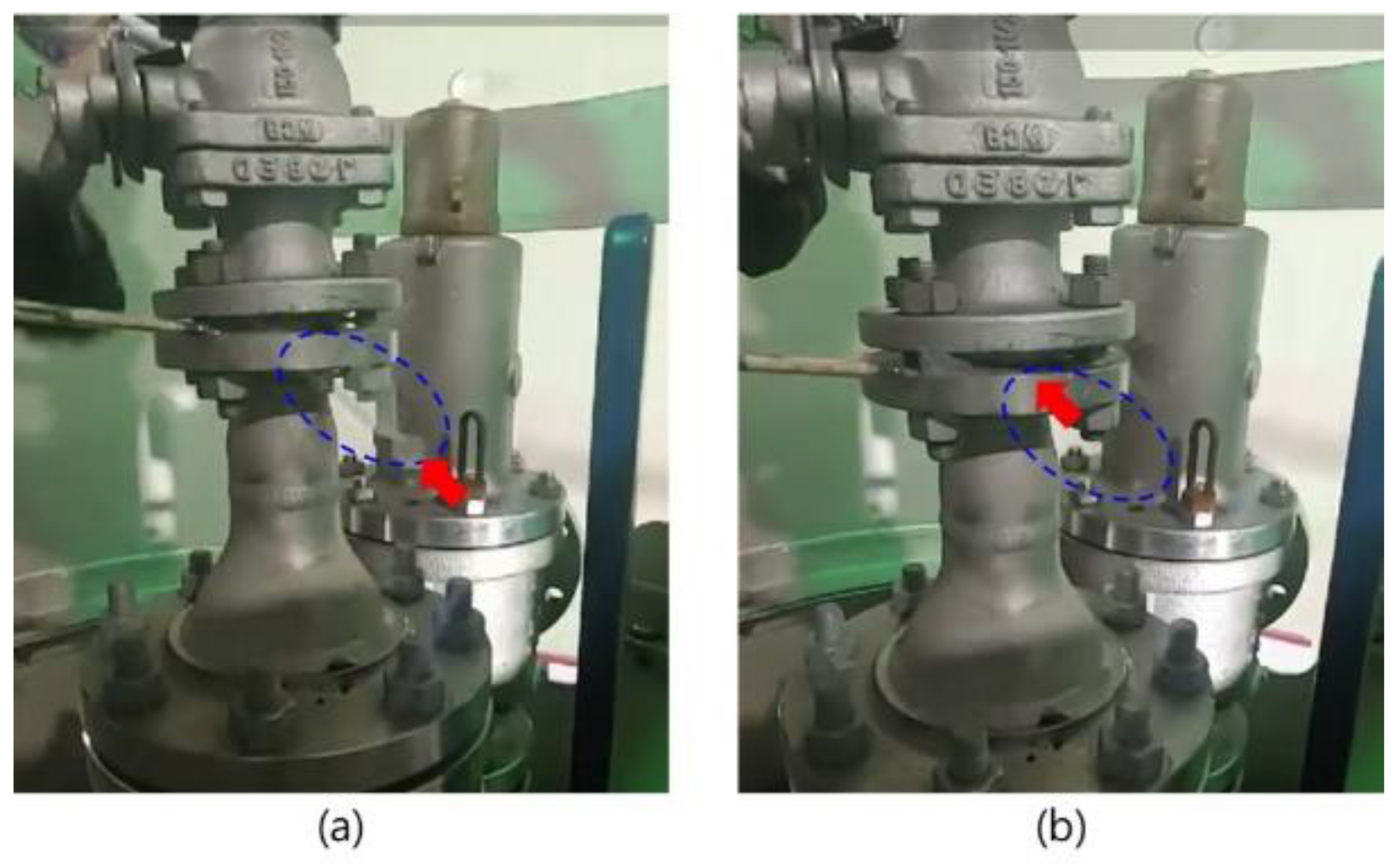
Figure 11.
Pressure changes in a packaging filling line (valve is 30% open and leak gap is 5 mm).

Figure 13.
Action required to improve risk management.
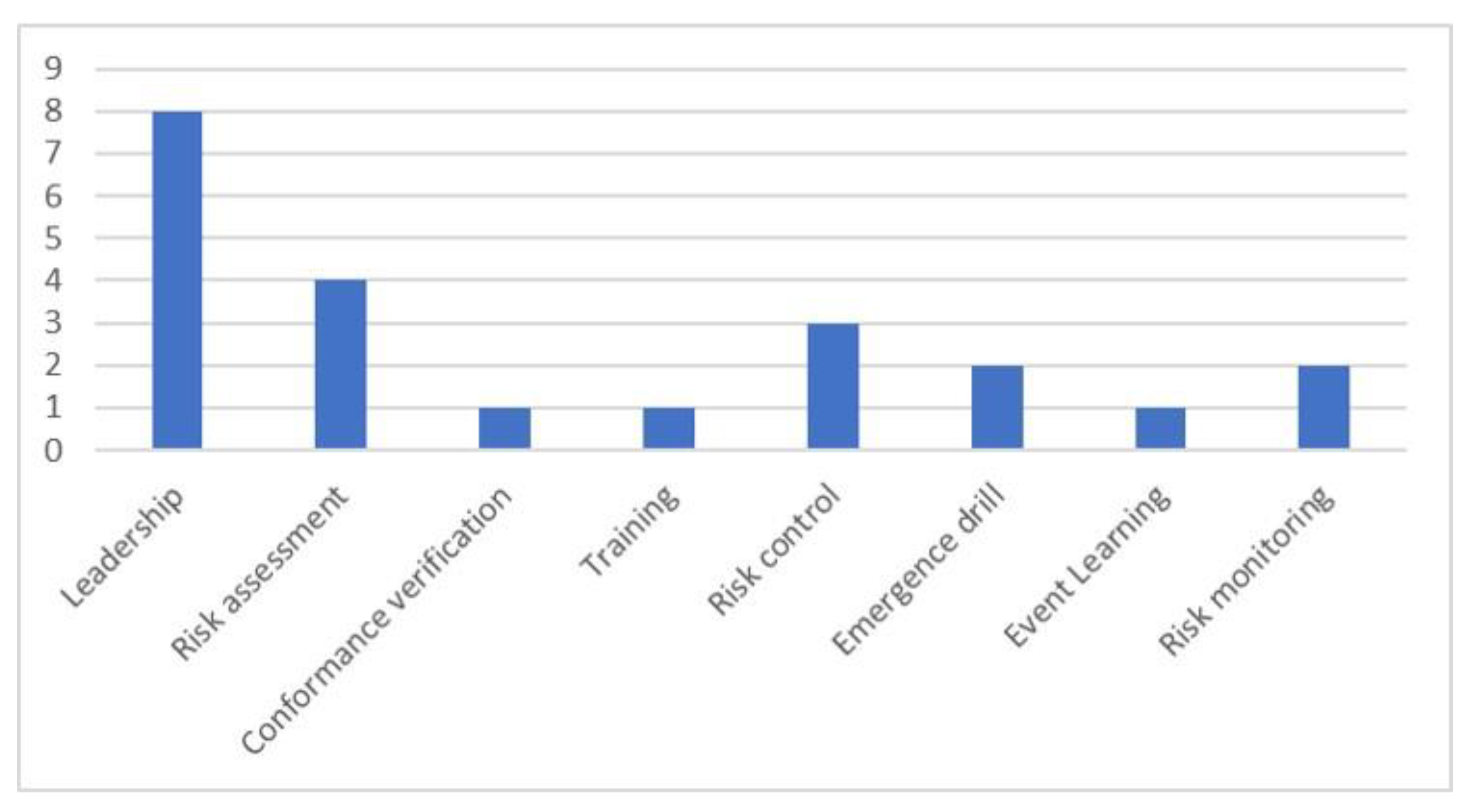
Figure 14.
Flow chart showing the procedures and related departments from the research and development (R&D) stage to commissioning organic catalytic processes.
Figure 14.
Flow chart showing the procedures and related departments from the research and development (R&D) stage to commissioning organic catalytic processes.
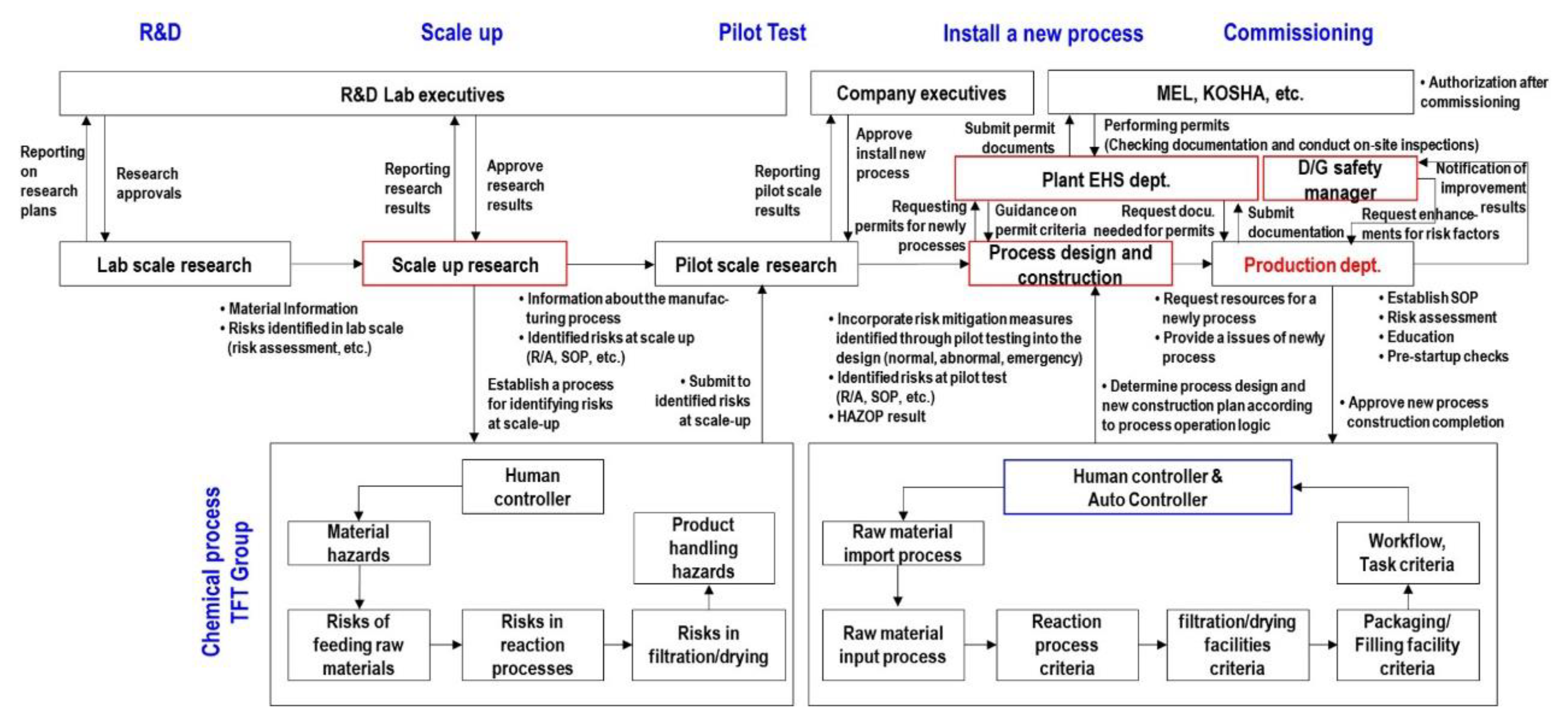

Table 1.
History of accidents involving hazardous materials in process safety management (PSM) plants in South Korea (2016–2021).
Table 1.
History of accidents involving hazardous materials in process safety management (PSM) plants in South Korea (2016–2021).
| No. | Industries | Accident Date | Process categorization | Disaster |
|---|---|---|---|---|
| 1 | Pharmaceutical raw materials, petroleum products manufacturing | January. 2016 | Fire in a cleaning process of a raw material concentrator | Death |
| 2 | Pharmaceutical raw materials, petroleum products manufacturing | January. 2016 | Fire in the process of feeding raw materials into a reactor | Death |
| 3 | Chemical and rubber products manufacturing | July. 2016 | Fire from a chemical leak in a reactor | Death |
| 4 | Chemical and rubber products manufacturing | October. 2017 | Dust explosion in a facility during pre-operational inspection | Death |
| 5 | Chemical and rubber products manufacturing | November. 2018 | Fire in the process of adding filler to the mixer | Death |
| 6 | Chemical and rubber products manufacturing | August. 2018 | Fire caused by oil vapor in the process of feeding raw materials into an agitator | Serious injury |
| 7 | Chemical and rubber products manufacturing | November. 2019 | Fire during a chemical splay operation | Serious injury |
| 8 | Chemical and rubber products manufacturing | December. 2019 | Explosion during a reactor internal cleaning | Death |
| 9 | Pharmaceutical raw materials, petroleum products manufacturing | May. 2019 | Fire during filtration of chemicals | Serious injury |
| 10 | Pharmaceutical raw materials, petroleum products manufacturing | February. 2020 | Explosion during a reactor internal cleaning | Serious injury |
| 11 | Chemical and rubber products manufacturing | March. 2020 | Explosion during welding on top of reactor | Death |
| 12 | Chemical and rubber products manufacturing | March. 2020 | Fire while cutting piping connected to a storage tank | Death |
| 13 | Pharmaceutical raw materials, petroleum products manufacturing | April. 2020 | Fire during powder feeding operation | Serious injury |
| 14 | Chemical and rubber products manufacturing | May. 2020 | Fire during flange bolt cutting operation | Serious injury |
| 15 | Chemical and rubber products manufacturing | May. 2020 | Fires and explosions in organocatalyst product packaging operations | Death |
| 16 | Chemical and rubber products manufacturing | June. 2021 | Fire during powdered chemical feed operation | Serious injury |
Table 2.
Accident overview.
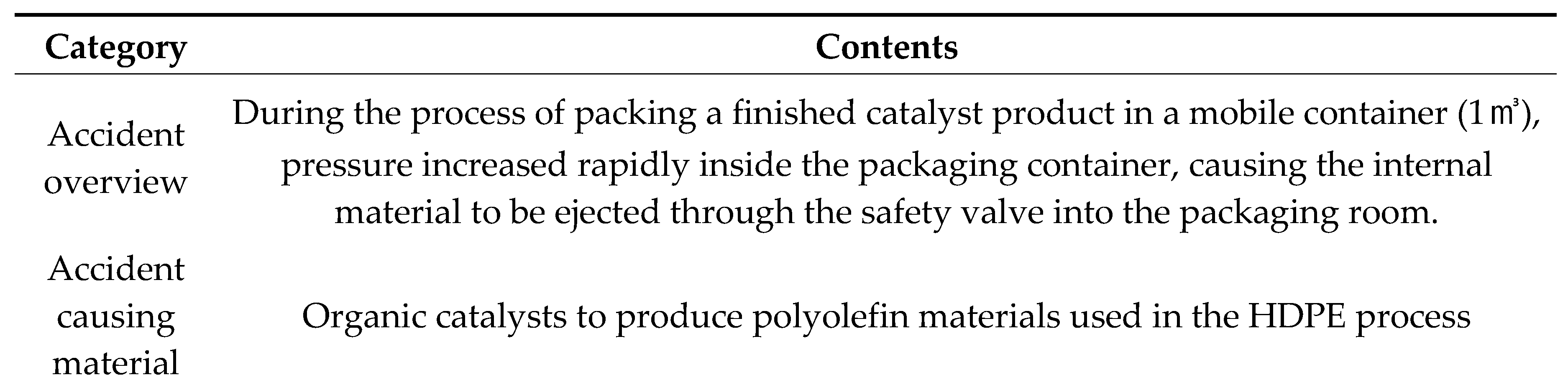

Table 3.
Estimated cause and result of the accident by the Korean Occupational Safety and Health Agency (KOSHA).
Table 3.
Estimated cause and result of the accident by the Korean Occupational Safety and Health Agency (KOSHA).
| Sequence of events | Accident cause | Reason for accident | Result |
|---|---|---|---|
| First Event | Improper connection between container and flange | Air enters between improperly connected flanges and reacts with the catalyst inside the container | Pressure builds up inside the vessel, causing the internal pressure to blow out through the process safety valve (PSV). |
| Second Event | safety valve outlet is not connected to a safety location | Catalyst dust is blowing into the room because the PSV outlet is not connected to a safety location | “Dust explosion” caused by dust released into the packing room |
Table 4.
Possible scenarios that could lead to an accident.
| Classification | Possible scenario | Investigation result |
|---|---|---|
| Packaging containers |
Moisture residue due to poor container cleaning | Internal analysis of identically handled containers shows no moisture residue |
| Moisture ingress due to improper container storage | ||
| Nitrogen Inlet Line |
Moisture content in nitrogen | The issue did not occur with other products packaged under the same conditions. |
| Moisture in the nitrogen supply line | ||
| Catalyst Filling Line |
Entry of air or moisture during the catalyst packaging line connection process | Nitrogen purging for 5 minutes after packaging line connection removes internal residue |
| Entry of air or moisture during catalyst packaging operations | Need technical analysis | |
| Vent Line | Debris blocks the vent pipe releasing pressure from the packaging container | The pressure inside the packaging container (5 barg) is expelled through the vent pipe during the packing operation |
| Oil inside the pressure gauge installed at the end of the container discharge line enters the packaging container. | Even if oil leaks, it is structured in a way that prevents oil from entering inside the packaging container. | |
| Foreign matter present in the raw material | Foreign matter (such as moisture) in the raw material was mixed in during manufacturing. | The issue did not occur with other products packaged under the same conditions. |
Table 5.
Information on methylaluminoxane (MAO).

Table 6.
the measurement of enthalpy change (∆E) in MAO reactions with air and water.
| Reaction Case | Chemical equation | ∆E (kcal/mol) |
비고 |
|---|---|---|---|
| MAO+O2 | 2(CH3AlO) + 3O2 → Al2O3 + 2CO + 3H2O | -55.2 | O2 1 mol |
| MAO+H2O | 2(CH3AlO) + H2O → Al2O3 + 2CH4 | -30.5 | H2O 1 mol |
| <Calculation Tool> ① Software Operations Center : lg chem R&D Center ② Method : Density Functional Theory (DFT) , Becke Exchange Functional & Perdew-Wang 91 Correlation Functional ③ Basis Set : DND(Double-numerical + d Polarization Basis Set) ④ Calculation formula : ΔE°_rxn = [Sum of products for ΔH°_f] – [Sum of reactants for ΔH°_f] | |||
Table 7.
Status of different barriers that could have prevented the accident.
| No. | Barrier | Status | Confidence | Challenge | Performance |
|---|---|---|---|---|---|
| 1 | Safety Mgmt. Sys. | Low | Contains regulations on procedures and work permits for safe process management | Not working properly |
|
| 2 | Safety valve discharge line connected to combustion/ absorption/capture/recovery facilities. | Missing | Dangerous substances discharged from safety valves must be treated by combustion, absorption, capture, and recovery. | Not operational |
|
| 3 | Supplementation of SOP | Missing | 1) In case the piping is not connected properly, the operator should reconfirm the piping connection on his own or have another operator reconfirm the piping connection Establish a procedure for waiting a certain amount of time after packaging to work on a product because adverse events may occur during packaging |
Not operational |
|
| 4 | Education on standard of procedure (SOP) | Missing | Prevent similar accidents from occurring by training workers on work procedures | Not operational |
|
| 5 | Packaging process organized as an outside work | Missing | Operate catalyst packaging outside to ensure that catalyst dust does not reach explosive dust concentrations even if it is blown outside | Not operational |
|
| 6 | Properly configured fire protection facilities | Missing | Prevent secondary accidents such as fires and explosions by eliminating flammable materials near the workplace or establishing facilities indoors to prevent or respond to dust explosions | Not operational |
Table 8.
Management requirements for each department to prevent accidents during chemical processes.
Table 8.
Management requirements for each department to prevent accidents during chemical processes.
| Group | Safety requirements | Improper decision | Defect in organization |
|---|---|---|---|
| MEL/ KOSHA |
1) Enforcement of the safety & health Act 2) Thoroughly review a PSM document |
- | - |
| R&D Center |
1) Establishing safety standards & risk assessment criteria in R&D 2) Establish a safety training program for researchers 3) Establish procedures to identify the risks involved before transferring R&D products to production. |
Underestimating the risk of chemicals and failing to consider the safeguards that should be in place during the scale-up phase. | Enhance the ability to list risks identified in the research phase and clearly communicate them to production and design teams. |
| Production team | 1) Establish procedures to identify key risks before transferring R&D products to production 2) Establish procedures for training workers on key points related to manufacturing new products |
1) Performing piping connections in unsafe locations and conditions without a worker-centric risk assessment. 2) Lack of understanding of what happens when foreign objects are introduced during the packaging process |
Lack of procedure regarding what needs to be reviewed when introducing new products and the ability to worker-centric risk assessments and manage incident cases. |
| EHS Team | 1) Clear cross-functional R&R by PSM element 2) Inventory legal requirements about PSM |
Determined that indoor emissions from PSV lines are not in violation of the law | It is necessary to supplement the function that lists relevant laws and regulations when introducing new products and periodically check them during the construction process. |
| D/G safety manager |
Perform safety management tasks to meet legal requirements when handling hazardous materials | Determining the risk of the pack aging step as low and not participating in the packaging process. | Establish a system to ensure that safety managers are involved in all hazardous materials work |
| Process design team | 1) Establish procedures to incorporate risk factors identified in the research phase into the design. 2) Establish procedures to incorporate accident cases into design |
1) Failure to clearly review legislation during process design 2) Failure to account for human error in process design |
Internal criteria for safe design guidelines (KOSHA Guidelines) must be clarified |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



