
Submitted:
03 September 2024
Posted:
04 September 2024
You are already at the latest version
Abstract
Harms of combustible cigarette (CC) use in pregnancy for fetal development are well-studied. Less understood is potential impacts of newer non-combustible cigarette alternatives, including electronic cigarettes (EC). Our goal was to examine whether EC use during pregnancy predicts increased risk of adverse birth outcomes. This retrospective cohort study used data from the Obstetrics Initiative (OBI), a statewide collaborative of 70 maternity hospitals. OBI’s clinical registry of data on nulliparous, term, singleton, vertex fetal presentation pregnancies were from medical records. Three groups of pregnancy cigarette users (Controls (n=26,394), CC (n=2,216), EC (n=493) were compared on birth outcomes, controlling for background differences. Compared to controls, the EC group had significantly lower birth weight, while CC had reduced birthweight and greater rates of arterial cord pH < 7.1. Compared to EC, CC users had higher rates of neonates requiring antibiotics and NICU admission. Growing evidence suggests EC are not safer alternatives to CC, and use during pregnancy should be discouraged. Additional research is needed, as non-significant trends for increased risk of several adverse neonatal outcomes following EC use were found, potentially significant in larger studies with average-risk for adverse pregnancy outcomes and when frequency and timing of EC exposure are considered.
Keywords:
electronic cigarette
; combustible cigarette
; marijuana
; neonatal
; adverse effects
; birth outcomes
; birthweight
; APGAR
; arterial cord pH
; assisted ventilation
; NICU
; neonatal antibiotics
1. Introduction
Use of combustible cigarettes (CC) in pregnancy is the leading preventable cause of poor pregnancy outcomes [1]. Impacts of CC use in pregnancy are well-studied and include low birth weight (LBW), small for gestational age (SGA), preterm birth (PTB), infant lung hypoplasia, increased rates of cesarean delivery, birth defects, admission to the neonatal intensive care unit, and fetal and infant death [2,3,4]. Less understood are the effects of electronic cigarette (EC) use, which are used in up to 15% of pregnancies in the US [5]. While ACOG firmly recommends discontinuation of all forms of smoking, including EC, during pregnancy [6], studies suggest that the general public believes EC to be safer in pregnancy than CC [7].
Existing research on the use of EC in pregnancy involves mostly animal models, and relevance to human offspring is unclear due to placental differences. However, these studies have identified adverse fertility and offspring development, including deficits in bone growth following exposure to both nicotine-containing and nicotine-free EC aerosols [8]. Cinnamaldehyde flavoring, a common EC offering, was especially harmful to growth, health, and behavioral development [8]. In mammal models, studies have linked exposure to nicotine-containing EC vapor to reduced birthweight [9,10] and adult weight [11,12], while others reported pulmonary [10], and neurological effects, including impacts on motor coordination, learning, behavior, and memory into adulthood [13].
Existing human studies on birth outcomes relative to prenatal EC exposure have largely been done using the Pregnancy Risk Assessment Monitoring System (PRAMS) database. For example, third-trimester EC use was associated with increased risk for small for gestational age (SGA) [14,15]. Third trimester exposure was also associated with low birth weight (LBW) across multiple studies utilizing PRAMS [15,16,17,18]. While PRAMS is a national survey soliciting responses from a representative subset of new mothers, non-response and recall bias, as well as social-desirability responding and question formats (for example, questions about EC are limited to third trimester use) can limit the validity and generalizability of conclusions of studies using PRAMS. To date, most studies not utilizing PRAMS, have reported no differences in birthweight between neonates born to EC-only users and control groups [19,20], but have identified increased risk of preterm birth (PTB) in the EC groups [15,16,17]. Interestingly, one study found that the odds of a pregnancy impacted by use of only EC resulting in SGA or PTB were not significantly lower than the group of individuals who used CC during pregnancy, supporting that EC are not safer alternatives to CC [15]. These studies, however, are limited by smaller and more homogeneous samples. Consequently, while existing research suggests that use of EC in pregnancy may be unsafe, exact findings in relation to PTB, LBW, and SGA are inconsistent across studies. Thus, while harms of CC use in pregnancy are well-studied, data from high quality studies are lacking regarding comparative use of CC and EC on commonly studied adverse neonatal outcomes such as birth size and gestational length, as well as less frequently examined outcomes including low APGAR scores, NICU admissions, supplemental oxygen therapy at birth, infection, and metabolic acidosis.
The goal of the current study was to examine whether EC use during pregnancy increases the risk of a wide variety of birth outcomes compared to non-use, and to also examine the differences in outcomes between pregnancy EC and CC use.
2. Materials and Methods
2.1. Dataset
Data for this retrospective cohort study were obtained from the Obstetrics Initiative (OBI), a quality improvement project funded by Blue Cross Blue Shield of Michigan and Blue Care Network, currently focused on safely lowering the number of cesarean deliveries across the state of Michigan. OBI’s registry includes chart-abstracted data from approximately 70 maternity hospitals in Michigan and includes nulliparous, singleton, term delivery, and vertex (NSTV) births. OBI provided a de-identified dataset of NTSV births between January 2021 and July 2022 in the registry, and our local IRB determined the study was exempt from IRB oversight.
2.2. Exposure Definitions
Within the OBI database, EC and CC use were indicated for participants. OBI allowed the following values in their definition of EC use at any point during pregnancy: e-cigarettes, e-hookah, steam stones, pens, vape pens, and other vaping products. CC use included the following: cigarettes, hookah, chewing tobacco, or any other tobacco-based product during pregnancy. Marijuana use was categorized as positive if there was any marijuana use during pregnancy, regardless of how it was consumed.
For our sample, we excluded those for whom information was unavailable on their EC and CC use status. EC and CC users were defined as individuals who used those products for some or all of their pregnancy, and those who used both (n=134) were excluded from the current analysis. Participants in the control group were individuals who were definitively identified as non-CC or non-EC users. Patients with any documentation of alcohol or opioid use during pregnancy were excluded from this study; however, those who had indication of marijuana use, in this state where recreational use is legal and common, were retained.
2.3. Outcome Definitions
All available markers of neonatal wellbeing at birth were examined as study outcomes. Birthweight (grams) was included as a continuous outcome. LBW, arterial cord pH, 1 and 5-minute APGAR scores, neonatal assisted ventilation at birth and > 6 hours postpartum, neonatal antibiotics at birth, and NICU admission were all reported as categorical outcomes. LBW was defined as birthweight < 2500 g [21]. Low arterial cord pH was defined as pH < 7.1, indicative of neonatal metabolic acidosis. Low 1-minute APGAR scores were defined as scores < 7 and low 5-minute APGAR scores as < 8. The remaining outcomes were keyed as “yes” vs “no” depending on whether the outcome occurred. Gestational age at delivery was not examined as an outcome due to the dataset including only term births.
2.4. Additional Variables
Study population descriptors and model covariates for these first-time mothers included: maternal age at delivery, race/ethnicity, pre-pregnancy and delivery weight and BMI, gravidity, parity, diabetes (gestational and preexisting), and hypertension (pregnancy induced and chronic).
2.5. Data Analyses
Data analyses were completed using IBM SPSS Statistics version 28.0.1.0. Bivariate comparisons between exposure and control groups utilized ANOVA and chi-square analysis. Background variables significantly associated with group status were identified and included as control variables in subsequent analyses. Logistic and linear regression were performed to examine group differences on outcomes controlling for all significant background factors.
3. Results
3.1. Background Differences between Study Groups
The analytic sample contained 26,394 controls, 493 EC-only users, and 2,126 CC-only users (Table 1). All smokers were significantly more likely to be white, non-Hispanic, and gain more weight during pregnancy compared to controls. Additionally, those who smoked CC compared to other participants had a higher mean BMI pre-pregnancy and were significantly more likely to have diabetes. Those who used EC were significantly less likely to have hypertension than the remaining participants. The groups did not differ significantly on the remaining background factors, including pregnancy marijuana use.
3.2. Neonatal Outcome Differences between Study Groups
Birthweight was analyzed as both a continuous and categorical variable. All other variables were analyzed as categorical variables, and adjusted odds ratios as well as confidence intervals can be seen in Figure 1 for the between-group comparisons. Compared to the control group, EC users gave birth to babies on average 114 grams (95% CI -156 to -72) lighter than those who did not use any cigarettes during pregnancy. Participants in this group were also 60% more likely than controls to have a newborn classified as LBW. The risk for NICU admission was significantly decreased for those born to EC users. When evaluating risks of low 1- and 5-minute APGAR scores, neonatal metabolic acidosis, and necessity of neonatal antibiotics and assisted ventilation both at birth and > 6 hours postpartum, there were no statistically significant differences between EC and control groups.
In comparing the CC group to controls, those who used CC had more than double the risk of a LBW baby. The CC group was almost 50% more likely than controls to have a newborn with metabolic acidosis, which was statistically significant. Similarly, the risk of low 1- and 5-minute APGAR scores, needing neonatal antibiotics, NICU admission, and needing neonatal assisted ventilation at birth and for > 6 hours postpartum were increased for babies born to CC users, though not statistically significant.
When observing the exposure groups against one another, there was no significant difference in birthweight (adjusted mean: -44.8 g, 95% CI -91.6 to 2.0), risk of giving birth to a LBW baby, or risk of neonatal metabolic acidosis. Babies born to CC users were more than 2.5 times more likely to require neonatal antibiotics, however, and over 1.5 times more likely to get admitted to the NICU than babies born to EC users, statistically significant differences.
Panels A-C indicate risk of adverse pregnancy outcomes for the above group comparisons, where aOR >1 indicates increased risk for the EC group compared to control group, CC group compared to the control group, and CC group compared to the EC group, respectively. Results are from linear and logistic regression analyses controlled for all significant background factors in Table 1.
4. Discussion
Findings from this large population-based study of full-term infants demonstrated that use of EC during pregnancy, compared to no use of EC or CC, was associated with significantly decreased birthweight, and a trend toward increased risk of lower 1 and 5-minute APGAR scores. Use of CC in pregnancy was also associated with reduced birthweight, along with greater rates of arterial cord pH less than 7.1. When comparing CC and EC groups to one another, CC use in pregnancy was found to have significantly higher risk of neonates requiring antibiotics at birth and NICU admission, but no other significant differences were observed.
To our knowledge, this is the first large population-based analysis assessing adverse neonatal outcomes associated with use of EC in pregnancy that looked beyond gestational age and size at birth to examine other neonatal outcomes including low APGAR scores, metabolic acidosis, respiratory distress, infection, and NICU admission. Like many other studies, ours demonstrated decreased birthweight as a significant risk associated with both electronic and combustible cigarette use. While the effect was larger when quantifying average decrease in birthweight among babies born to CC users, the decrease in birthweight was still significant for babies born to EC users when compared to nonsmokers, indicating use of EC in pregnancy may be independently harmful and not an appropriate alternative to CC. The developmental sequelae for most LBW babies is poor, with increased incidence of cognitive and attentive deficits, as well as problems with neuromotor functioning into adolescence,29 indicating long-term detrimental effects that could follow EC exposure during gestation.
Our study found a trend toward increased risk for low 1 and 5-minute APGAR scores in both the EC and CC groups, with risk most elevated in the CC group. APGAR scores are generally regarded as markers for how well babies tolerated birth, and how well they are adjusting to being outside of the womb. While APGAR scores have not been clinically useful in predicting individual neonatal mortality or longer-term outcomes, a 5-minute score of 3 or less confers increased risk of neonatal mortality at the population level as well as an increased relative risk of cerebral palsy [22]. While our cutoff for defining a low APGAR score was higher, studies show that scores below 7 are concerning for neonatal hypoxic-ischemic encephalopathy, meconium aspiration, respiratory distress, and mortality, [23,24,25,26] indicating that scores below this level may have implications for longer-term detrimental effects.
Interestingly, increased risk for neonatal assisted ventilation, antibiotic administration, and NICU admission in the CC group when compared to nonsmokers was nonsignificant in this study, in contrast to some other studies where these effects have been found. Previous literature has described associations between maternal CC use in pregnancy and increased risk of neonatal NICU admission, infection requiring antibiotics, and respiratory distress requiring assisted ventilation [27,28,29,30]. Our population was inherently low risk since participants who delivered preterm, were non-NSTV, and experienced fetal death were not included in OBI’s sampling. Thus, individuals who had adverse outcomes associated with both EC and CC use may have been eliminated from the original dataset, suggesting that our findings may conservatively estimate the true effect among higher risk populations, including those with combined EC and CC use (who were excluded from the analysis) or those with prematurity (who were not included in our dataset).
Our study had many strengths. To our knowledge, it was the first large, population-based study examining birth outcomes following EC use in pregnancy using data objectively captured in electronic medical records, rather than data from those who choose to be in the study and self-report all variables, such as is the case with PRAMS. In addition, PRAMS only captures third trimester EC use, while our dataset included EC use in any part of pregnancy. Use of EC in the first trimester alone has been associated with adverse neonatal outcomes including PTB, LBW, SGA, neonatal assisted ventilation, NICU admission, and infant death. [31,32] Including individuals who used EC at any point in pregnancy, including those that quit during pregnancy, captures a more representative population of EC use in pregnancy than limiting to third trimester use, and may also lead to the discovery of more associated adverse outcomes. Further, PRAMS does not include many outcomes analyzed in this study, including arterial cord pH, APGAR scores, neonatal assisted ventilation, neonatal antibiotic administration, and NICU admission, many of which predict long-term health and developmental issues. Additionally, most published research on this topic not using PRAMS datasets is poorly generalizable due to smaller and homogenous samples [33].
A further strength of our study is that we included participants who used marijuana in pregnancy concomitantly with cigarettes. With expanding legalization, marijuana usage rates have been increasing, and research suggests that those who use EC are significantly more likely to concomitantly or later use marijuana [34,35]. Thus, we designed our study to include these individuals as more representative of the general population of EC users, adding validity to this study and increasing power by including more participants. Further, a recent study found that concomitant use of tobacco and marijuana during pregnancy was not associated with additional risks of poor neonatal outcomes compared to tobacco use alone [36], supporting that significant findings from our study are not explained by in utero marijuana exposure alone, as indeed our cigarette use groups did not differ significantly in their rates of marijuana use in pregnancy. Our study was additionally strengthened by excluding participants who used other substances beyond marijuana, including alcohol and opioids, which have well-established effects on newborn outcomes and could decrease the validity of our findings. Thus, our study utilizes a larger dataset with expanded inclusion of birth outcomes and pregnancy EC use before the third trimester, and represents concomitant use of marijuana while controlling for effects of other substances, all of which strengthen the current study and make findings more generalizable than result of previous studies.
This study should be interpreted considering some limitations. First, there were fewer EC only users in comparison to CC only and control groups. As EC are still new to the market, we expect future studies will have proportionately more EC users as sales of EC continue to grow. Further, our data were not granular enough to examine type of EC used, frequency of use, and duration and timing of use in pregnancy, which are likely relevant to the findings. Animal studies indicated potential harm to cardiovascular development from flavorings and other toxicants in nicotine-free EC [37]. Thus, there are independent harms associated with use of nicotine-free EC, which would be valuable to ascertain in a human-based study. In future studies, it would be beneficial to observe outcomes relative to type, frequency, and duration of use. Lastly, as our dataset only contained live, full-term, NSTV births, the low-risk nature of participants may have impacted findings including not being able to assess associations with preterm delivery or stillbirth. Thus, cases for whom EC use led to adverse outcomes were potentially eliminated. This low-risk sample may also be why, unlike other studies, we identified fewer adverse outcomes following tobacco use in pregnancy. This suggests EC effects may be larger in more generalized samples as well, but our study does show that EC and CC use in pregnancy predict adverse outcomes even when gestational age at delivery is not impacted.
5. Conclusions
While use of EC in pregnancy reduced birth weight in this study, most adverse newborn outcomes examined were not significantly predicted by EC use. Additional study is needed, as non-significant trends toward poorer outcomes for EC users were evident and potentially significant with larger samples that include higher risk deliveries, or when information on amount and timing of EC exposure is considered. These findings suggest detailed prospective studies, especially those that examine whether there are subsets of women for whom EC use in pregnancy is especially risky, are needed, and further reinforce that lack of significant findings related to prenatal substance exposure should be carefully scrutinized before conclusions about lack of harm are made. Finally, our findings can motivate and inform efforts to educate and counsel about EC use during prenatal care, including making sure that perinatal quality improvement initiatives focused on smoking cessation also address EC use.
Author Contributions
Conceptualization, M.A. and B.B.; methodology, M.A. and B.B.; formal analysis, M.A. and B.B.; investigation, M.A. and B.B.; resources, E.O. and B.B.; data curation, B.B.; writing—original draft preparation, M.A. and B.B.; writing—review and editing, M.A., E.O., M.M., and B.B.; supervision, B.B. All authors have read and agreed to the published version of the manuscript.
Funding
Dr. Moniz receives salary support from Blue Cross Blue Shield of Michigan for leading the Obstetrics Initiative. The other authors did not receive any sources of funding for conduct of this study.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of Covenant Medical Center (C-22-05 OBI Dataset, original approval date 4/19/2022).
Informed Consent Statement
A waiver of informed consent was approved by the IRB due to the retrospective nature of this study.
Data Availability Statement
Restrictions apply to the availability of these data. Data were obtained with written approval from OBI with the agreement that data would not be distributed without their consent. Any request for data acquisition must be placed with OBI and are only available directly from that organization.
Acknowledgments
This study included data from the Obstetrics Initiative (OBI; https://obstetricsinitiative.org/), a statewide quality improvement collaborative that maintains a clinical data registry of NTSV deliveries in Michigan. Support for the Obstetrics Initiative is provided by Blue Cross Blue Shield of Michigan and Blue Care Network as part of the BCBSM Value Partnerships program. Although Blue Cross Blue Shield of Michigan and OBI work collaboratively, the opinions, beliefs and viewpoints expressed by the author do not necessarily reflect the opinions, beliefs and viewpoints of BCBSM or any of its employees. Findings from this study were part of a poster presentation by the first author at the annual American College of Obstetricians and Gynecologists scientific meeting in May of 2023, in Baltimore, MD.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- National Center for Chronic Disease Prevention and Health Promotion (US) Office on Smoking and Health The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General; Centers for Disease Control and Prevention (US): Atlanta, 2014.
- McEvoy, C.T.; Spindel, E.R. Pulmonary Effects of Maternal Smoking on the Fetus and Child: Effects on Lung Development, Respiratory Morbidities, and Life Long Lung Health. Paediatr Respir Rev 2017, 21, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Ciobanu, A.; Rouvali, A.; Syngelaki, A.; Akolekar, R.; Nicolaides, K.H. Prediction of Small for Gestational Age Neonates: Screening by Maternal Factors, Fetal Biometry, and Biomarkers at 35-37 Weeks’ Gestation. Am J Obstet Gynecol 2019, 220, 486.e1–486.e11. [Google Scholar] [CrossRef] [PubMed]
- Ratnasiri, A.W.G.; Gordon, L.; Dieckmann, R.A.; Lee, H.C.; Parry, S.S.; Arief, V.N.; DeLacy, I.H.; Lakshminrusimha, S.; DiLibero, R.J.; Basford, K.E. Smoking during Pregnancy and Adverse Birth and Maternal Outcomes in California, 2007 to 2016. Am J Perinatol 2020, 37, 1364–1376. [Google Scholar] [CrossRef] [PubMed]
- Vilcassim, M.J.R.; Stowe, S.; Majumder, R.; Subramaniam, A.; Sinkey, R.G. Electronic Cigarette Use during Pregnancy: Is It Harmful? Toxics 2023, 11. [Google Scholar] [CrossRef]
- Tobacco and Nicotine Cessation During Pregnancy: ACOG Committee Opinion, Number 807. Obstetrics and gynecology 2020, 135, e221–e229. [CrossRef]
- Dobbs, P.D.; Lu, Y.; Maness, S.; Coleman, L.; Johnson, A.; Metz, S.; Vidal, C.; Cheney, M.K. Gestational Women’s Perceptions About the Harms of Cigarette and E-Cigarette Use During Pregnancy. Matern Child Health J 2021, 25, 1209–1220. [Google Scholar] [CrossRef]
- Bhattacharya, B.; Narain, V.; Bondesson, M. E-Cigarette Vaping Liquids and the Flavoring Chemical Cinnamaldehyde Perturb Bone, Cartilage and Vascular Development in Zebrafish Embryos. Aquat Toxicol 2021, 240, 105995. [Google Scholar] [CrossRef]
- Orzabal, M.R.; Lunde-Young, E.R.; Ramirez, J.I.; Howe, S.Y.F.; Naik, V.D.; Lee, J.; Heaps, C.L.; Threadgill, D.W.; Ramadoss, J. Chronic Exposure to E-Cig Aerosols during Early Development Causes Vascular Dysfunction and Offspring Growth Deficits. Transl Res 2019, 207, 70–82. [Google Scholar] [CrossRef] [PubMed]
- Cahill, K.M.; Gartia, M.R.; Sahu, S.; Bergeron, S.R.; Heffernan, L.M.; Paulsen, D.B.; Penn, A.L.; Noël, A. In Utero Exposure to Electronic-Cigarette Aerosols Decreases Lung Fibrillar Collagen Content, Increases Newtonian Resistance and Induces Sex-Specific Molecular Signatures in Neonatal Mice. Toxicol Res 2022, 38, 205–224. [Google Scholar] [CrossRef]
- Wetendorf, M.; Randall, L.T.; Lemma, M.T.; Hurr, S.H.; Pawlak, J.B.; Tarran, R.; Doerschuk, C.M.; Caron, K.M. E-Cigarette Exposure Delays Implantation and Causes Reduced Weight Gain in Female Offspring Exposed In Utero. J Endocr Soc 2019, 3, 1907–1916. [Google Scholar] [CrossRef]
- Chen, H.; Li, G.; Chan, Y.L.; Chapman, D.G.; Sukjamnong, S.; Nguyen, T.; Annissa, T.; McGrath, K.C.; Sharma, P.; Oliver, B.G. Maternal E-Cigarette Exposure in Mice Alters DNA Methylation and Lung Cytokine Expression in Offspring. Am J Respir Cell Mol Biol 2018, 58, 366–377. [Google Scholar] [CrossRef] [PubMed]
- Sifat, A.E.; Nozohouri, S.; Villalba, H.; Al Shoyaib, A.; Vaidya, B.; Karamyan, V.T.; Abbruscato, T. Prenatal Electronic Cigarette Exposure Decreases Brain Glucose Utilization and Worsens Outcome in Offspring Hypoxic-Ischemic Brain Injury. J Neurochem 2020, 153, 63–79. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Lee, N.L.; Burstyn, I. Smoking and Use of Electronic Cigarettes (Vaping) in Relation to Preterm Birth and Small-for-Gestational-Age in a 2016 U.S. National Sample. Prev Med (Baltim) 2020, 134, 106041. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Oancea, S.C. Electronic Cigarettes May Not Be a “Safer Alternative” of Conventional Cigarettes during Pregnancy: Evidence from the Nationally Representative PRAMS Data. BMC Pregnancy Childbirth 2020, 20, 557. [Google Scholar] [CrossRef]
- Hawkins, S.S.; Wylie, B.J.; Hacker, M.R. Associations between Electronic Nicotine Delivery Systems and Birth Outcomes. J Matern Fetal Neonatal Med 2022, 35, 6868–6875. [Google Scholar] [CrossRef]
- Regan, A.K.; Bombard, J.M.; O’Hegarty, M.M.; Smith, R.A.; Tong, V.T. Adverse Birth Outcomes Associated With Prepregnancy and Prenatal Electronic Cigarette Use. Obstetrics and gynecology 2021, 138, 85–94. [Google Scholar] [CrossRef]
- Regan, A.K.; Pereira, G. Patterns of Combustible and Electronic Cigarette Use during Pregnancy and Associated Pregnancy Outcomes. Sci Rep 2021, 11, 13508. [Google Scholar] [CrossRef]
- Froggatt, S.; Reissland, N.; Covey, J. The Effects of Prenatal Cigarette and E-Cigarette Exposure on Infant Neurobehaviour: A Comparison to a Control Group. EClinicalMedicine 2020, 28, 100602. [Google Scholar] [CrossRef]
- McDonnell, B.P.; Dicker, P.; Regan, C.L. Electronic Cigarettes and Obstetric Outcomes: A Prospective Observational Study. BJOG 2020, 127, 750–756. [Google Scholar] [CrossRef]
- Cutland, C.L.; Lackritz, E.M.; Mallett-Moore, T.; Bardají, A.; Chandrasekaran, R.; Lahariya, C.; Nisar, M.I.; Tapia, M.D.; Pathirana, J.; Kochhar, S.; et al. Low Birth Weight: Case Definition & Guidelines for Data Collection, Analysis, and Presentation of Maternal Immunization Safety Data. Vaccine 2017, 35, 6492–6500. [Google Scholar] [CrossRef]
- AMERICAN ACADEMY OF PEDIATRICS COMMITTEE ON FETUS AND NEWBORN; AMERICAN COLLEGE OF OBSTETRICIANS AND GYNECOLOGISTS COMMITTEE ON OBSTETRIC PRACTICE The Apgar Score. Pediatrics 2015, 136, 819–822. [CrossRef]
- Lai, S.; Flatley, C.; Kumar, S. Perinatal Risk Factors for Low and Moderate Five-Minute Apgar Scores at Term. Eur J Obstet Gynecol Reprod Biol 2017, 210, 251–256. [Google Scholar] [CrossRef]
- Salustiano, E.M.A.; Campos, J.A.D.B.; Ibidi, S.M.; Ruano, R.; Zugaib, M. Low Apgar Scores at 5 Minutes in a Low Risk Population: Maternal and Obstetrical Factors and Postnatal Outcome. Rev Assoc Med Bras (1992) 2012, 58, 587–593. [Google Scholar] [CrossRef]
- Thorngren-Jerneck, K.; Herbst, A. Low 5-Minute Apgar Score: A Population-Based Register Study of 1 Million Term Births. Obstetrics and gynecology 2001, 98, 65–70. [Google Scholar] [CrossRef]
- Iliodromiti, S.; Mackay, D.F.; Smith, G.C.S.; Pell, J.P.; Nelson, S.M. Apgar Score and the Risk of Cause-Specific Infant Mortality: A Population-Based Cohort Study. Lancet 2014, 384, 1749–1755. [Google Scholar] [CrossRef]
- Sun, J.; Liu, X.; Zhao, M.; Magnussen, C.G.; Xi, B. Dose-Response Association between Maternal Smoking during Pregnancy and the Risk of Infant Death: A Nationwide, Population-Based, Retrospective Cohort Study. EClinicalMedicine 2023, 57, 101858. [Google Scholar] [CrossRef] [PubMed]
- Adams, E.K.; Miller, V.P.; Ernst, C.; Nishimura, B.K.; Melvin, C.; Merritt, R. Neonatal Health Care Costs Related to Smoking during Pregnancy. Health Econ 2002, 11, 193–206. [Google Scholar] [CrossRef] [PubMed]
- De Queiroz Andrade, E.; Da Silva Sena, C.R.; Collison, A.; Murphy, V.E.; Gould, G.S.; Bonevski, B.; Mattes, J. Association between Active Tobacco Use during Pregnancy and Infant Respiratory Health: A Systematic Review and Meta-Analysis. BMJ Open 2020, 10, e037819. [Google Scholar] [CrossRef]
- Tarasi, B.; Cornuz, J.; Clair, C.; Baud, D. Cigarette Smoking during Pregnancy and Adverse Perinatal Outcomes: A Cross-Sectional Study over 10 Years. BMC Public Health 2022, 22, 2403. [Google Scholar] [CrossRef]
- Bacheller, H.L.; Chaiken, S.R.; Hersh, A.R.; Garg, B.; Caughey, A.B. Maternal Smoking Status during Pregnancy and the Effect on Adverse Maternal and Neonatal Outcomes. Am J Obstet Gynecol 2021, 224, S530–S531. [Google Scholar] [CrossRef]
- Osborne, J.B.; Bailey, B.A. Does It Matter When I Quit? Could I Just Cut down Some? Links between Trimester-Specific Smoking Amount, Preterm Birth, and Low Birth Weight. Birth Defects Res 2022, 114, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Cohn, A.M.; Elmasry, H.; Wild, R.C.; Johnson, A.L.; Abudayyeh, H.; Kurti, A.; Coleman-Cowger, V.H. Birth Outcomes Associated With E-Cigarette and Non-E-Cigarette Tobacco Product Use During Pregnancy: An Examination of PATH Data Waves 1-5. Nicotine Tob Res 2023, 25, 444–452. [Google Scholar] [CrossRef] [PubMed]
- Ksinan, A.J.; Spindle, T.R.; Thomas, N.S.; Eissenberg, T.; Spit for Science Working group; Dick, D. M. E-Cigarette Use Is Prospectively Associated with Initiation of Cannabis among College Students. Addictive behaviors 2020, 106, 106312. [Google Scholar] [CrossRef] [PubMed]
- Chadi, N.; Schroeder, R.; Jensen, J.W.; Levy, S. Association Between Electronic Cigarette Use and Marijuana Use Among Adolescents and Young Adults: A Systematic Review and Meta-Analysis. JAMA Pediatr 2019, 173, e192574. [Google Scholar] [CrossRef]
- Waddell, M.L.; Dickson, S.A.; Dodge, P.A.; Kopkau, H.E.; Nadolski, K.N.; Zablocki, V.; Forrestal, K.M.; Bailey, B.A. Birth Outcomes Following in Utero Co-Exposure to Tobacco and Marijuana. Birth Defects Res 2023. [Google Scholar] [CrossRef]
- Piechowski, J.M.; Bagatto, B. Cardiovascular Function during Early Development Is Suppressed by Cinnamon Flavored, Nicotine-Free, Electronic Cigarette Vapor. Birth Defects Res 2021, 113, 1215–1223. [Google Scholar] [CrossRef]
Figure 1.
Risk of adverse pregnancy outcomes based on type of cigarette use.
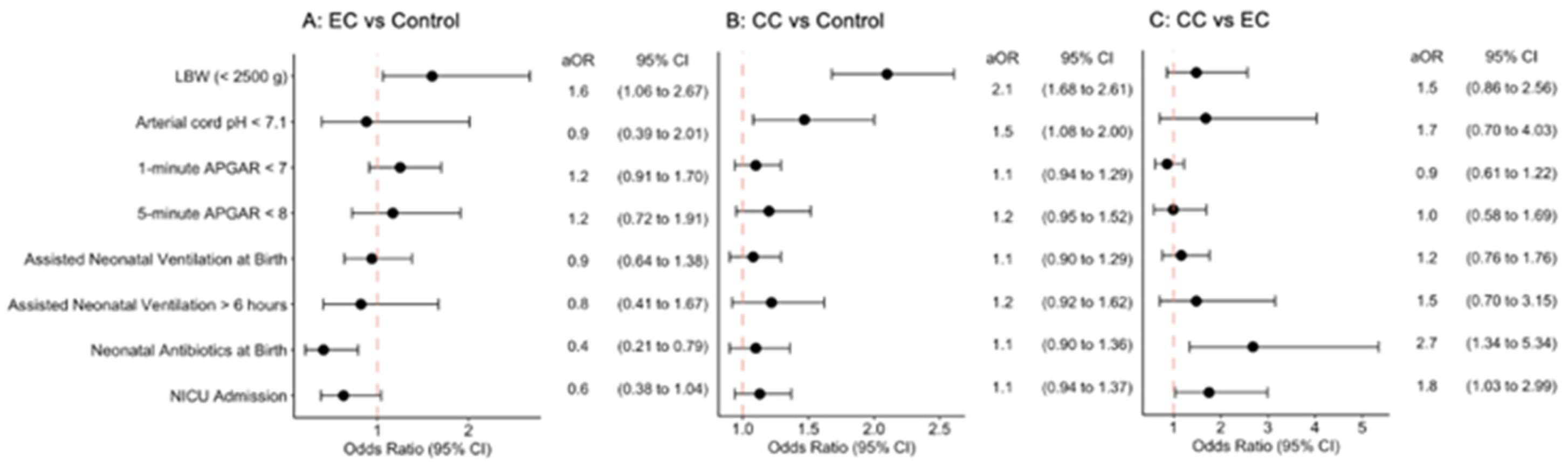

Table 1.
Participant background factors significantly associated with cigarette use.
| Controls (n=26,394) |
Electronic cigarette only (n=493) |
Combustible cigarette only (n=2,126) |
p | |
|---|---|---|---|---|
| Race (% white, non-Hispanic) | 68.5% | 84.9% | 79.5% | <.001 |
| Pre-pregnancy BMI (kg/m2) | 27.5 | 27.4 | 28.6 | <.001 |
| Pregnancy weight gain (lbs.) | 31.7 | 36.3 | 34.6 | <.001 |
| Diabetes (pre-existing or gestational, %) | 8.8% | 8.7% | 10.3% | .045 |
| Hypertension (chronic or pregnancy induced, %) | 19.8% | 16.2% | 21.9% | .009 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



