
Submitted:
04 September 2024
Posted:
05 September 2024
You are already at the latest version
Abstract
Introduction
Sepsis-associated encephalopathy (SAE) is common in sepsis and is linked to high mortality and impaired neurologic outcome. Brain ultrasonography (US), including transcranial Doppler (TCD) and transcranial color-coded duplex sonography (TCCS), is a non-invasive tool for cerebral monitoring and might be useful in sepsis. The aims of this review are: 1) to explore whether brain perfusion is altered in sepsis, 2) to determine the role of brain US in guiding resuscitation, and 3) its ability to predict neurological outcomes in septic patients.
Materials and methods
This scoping review adhered to the PRISMA-ScR protocol and JBI methodology. A comprehensive literature search was conducted across MEDLINE, Scopus, and Web of Science. The review included studies on adults with sepsis or septic shock in the ICU. Randomised controlled trials, clinical trials, observational studies and systematic reviews were included. All the data related to the review's key questions were extracted and charted independently by two authors.
Results
625 articles were screened, and 34 were ultimately included after application of exclusion criteria. 85% of the studies were observational 15% were systematic reviews with or without meta-analysis. The studies primarily focused on cerebral blood flow (CBF) alterations in sepsis, reporting variable results. Findings showed variable cerebral autoregulation (CAR) impairment, with higher incidence in the early stages of sepsis and associations with poor neurological outcomes. However, while alterations in CAR and CBF are common in septic patients, their impact on neurological outcomes and mortality is not clear. Regarding resuscitation, only a paucity of studies were found and no conclusions can be drawn.
Conclusions
The current body of evidence has a poor grade, but it is possible to say that brain US can identify cerebral perfusions alterations. Its usage during resuscitation is feasible and warrants further investigations. Use of brain US during resuscitation and for prediction of outcome is not currently supported by evidence. Further studies on brain perfusion, acquisition of 2D images of parenchyma (TCCS) and application of a multimodal brain monitoring might be useful in these contexts.
Keywords:
Brain ultrasound
; TCCS
; transcranial doppler
; sepsis
; multimodal monitoring
; POCUS
Introduction
Sepsis-associated encephalopathy (SAE) is a widespread brain dysfunction that results from an infection located outside of the central nervous system. This condition is a serious acute neurological disorder that ranging from delirium to a state of coma [1,2]. It is a common syndrome affecting up to 50-70% of patients with sepsis impairing the neurologic outcome; patients with acute brain dysfunction have higher mortality and morbidity, with reduced quality of life and long-term cognitive impairment [3,4,5,6]. Moreover, some patients present with unexplained delayed awakening or persistent coma [7]. Still, knowledge of the brain complications in sepsis is limited, especially in deeply sedated patients, and brain monitoring is frequently neglected [8,9].
In this scenario, the introduction of brain ultrasonography (US), either blind (transcranial Doppler, TCD) or with 2D images integration (transcranial colour-coded duplex sonography, TCCS), offers as a proxy for neuromonitoring in intensive care unit (ICU), with several advantages: wide availability, possibility to assess multiple organs with the same instrument, and rapid responses at the bedside (point of care ultrasound, POCUS) [10,11]. Brain US can be used to monitor cerebral blood flow (CBF), evaluate non-invasive intracranial pressure (nICP), estimate midline shift, assess ventricles’ enlargement, and the eventual presence of masses or blood within the brain parenchyma. Thus, the use of brain US can give a panoramic overview of the brain parenchyma and its vessels [12,13].
However, evidence about the use of brain US in sepsis is limited. The aim of this scoping review is to summarise the current state of literature focusing on three main questions: 1) is brain perfusion altered in sepsis? And if so, how is it altered? 2) Can we use brain US to guide sepsis resuscitation? 3) Can brain US predict the neurologic outcome of septic patients?
Materials and Methods
This scoping review follows the Preferred Reporting Items for Systematic Reviews and Meta-analysis protocol for scoping reviews (PRISMA-ScR) methods [14]. Furthermore, the proposed scoping review will be conducted in accordance with the JBI methodology for scoping reviews [15].
Search Strategy
The literature search was performed on 9th June 2024 in MEDLINE via PubMed, Scopus and Web of Science. A combination of “sepsis” OR “septic encephalopathy” OR “sepsis associated encephalopathy” AND “brain ultrasound” OR “transcranial doppler” OR “transcranial colour-coded doppler” OR “TCCS” was used. The same search strategy, including all identified keywords and indexed terms, has been adapted for each included database and/or information source. Other papers were retrieved from cited or related articles to these results. The full search syntax used for each database can be found in the supplementary materials (Attachment 1).
Eligibility Criteria
Types of Participants
Studies on adults (>18 yo) were included. Articles on paediatric population, animal studies and experimental sepsis studies were excluded. Studies regarding populations with intracranial infections were excluded.
Concept
This review aims to assess the usefulness of brain US in critically ill septic patients, to determine if CBF alterations exist and can be used to predict the neurologic outcome or guide resuscitation. All the brain US metrics useful to answer the review questions will be taken into account and described.
Context
Critically ill patients admitted to ICU for sepsis or septic shock regardless the sex, geographic location or cultural differences.
Type of Sources
All the articles in English published until 9th June 2024 were considered eligible for the review. Articles with full text not in English were excluded. Based on the study design, randomised controlled trials, clinical trials, and observational studies were included. Literature reviews were included only if systematic reviews with or without meta-analysis. Expert opinions, letters to the editor, guidelines, consensus and editorials were excluded.
Source of Evidence Screening and Selection
All the articles were imported after search in an Excel® spreadsheet (Microsoft Corporation). Duplicates were removed, and articles were progressively included or excluded blindly by two authors (GC and IC) in accordance with the previously cited criteria. Screening was based on a first round on titles and abstracts reading, and then on full text of the papers identified as potentially relevant. Any controversies between authors were resolved by discussion and opinion of a third author (FC). The inclusion process is shown in Figure 1.
Data Extraction Process
Data were extracted from the included papers by two independent reviewers, using a data extraction form independently developed by the authors. For each article we extracted aims, characteristics of the studied population (e.g. patients, age, setting), sample size, study design, methods, brain US metrics analysed, time of observation and the key findings and conclusions in terms of the previously mentioned outcomes.
Descriptive tables were used to summarize all the retrieved information from each study (supplementary materials, Attachment 2). Articles were tagged for subtopics basing on the review questions and summary tables were created for each subtopic. The authors discussed the results and updated the tables where needed in a continuous process.
Results
A total of 625 articles were scrutinized, of which 208 resulted duplicated. After application of the exclusion criteria 34 articles were included for data extraction (Figure 1). The type of evidence of the 34 included articles is illustrated in Figure 2. 85% of the articles were observational studies and 15% systematic reviews with or without meta-analysis. No RCTs were found.
Perfusion Abnormalities in Sepsis
Cerebral Blood Flow, Pulsatility Index, Resistance Index, Cerebrovascular Resistances and Other Intracranial Haemodynamics Indexes Alterations
Many studies evaluated CBF velocity in septic patients, highlighting various changes. The feasibility of TCD insonation during sepsis was demonstrated by Pierrakos et al [16] in a cohort of 20 patients where TCD was used for estimation of CBF velocities, cerebrovascular resistances (CVR) and pulsatility index (PI) with a feasibility of 91% through the acoustic bone window.
Baseline middle cerebral artery velocities (MCAv) were reported either lower [17], non-different [18] or higher [19] in respect to healthy controls or other anesthetised patients. Regarding CVR, these might be affected by multiple factors, but they were reported as reduced [20], but still functionally [21], even if the vasoconstrictor response might be reduced and slower with a difficulty in decreasing after the vasoconstrictor stimulus has ceased [17,18].
Straver et al [22] observed an inverse relationship between the systemic vascular resistance index and MCAv, with abnormalities in middle cerebral artery (MCA) and internal carotid artery (ICA) flow velocities being more pronounced in severe sepsis. These abnormalities were especially notable in non-survivors, who exhibited higher CBF and ICA velocities, in addition to an MCA/ICA index often >2, suggesting that a mild vasospasm can occur in basal cerebral arteries.
Pierrakos et al [16] further supported the observation that cerebral vascular constriction occurs early in sepsis and is detectable by TCD. This constriction, reflected in elevated PI and Resistance Index (RI), suggests that CBF alterations are a common feature in the early stages of sepsis. PI and RI were analysed in multiple studies, reporting that its value is often higher in patients with sepsis [Table 1]. In comparison to healthy controls, Szatmàri et al [17] reported higher PI in accordance with two following studies [16,18], even if the PI values were within the normality ranges (<1.3). In accordance with these findings, additional studies reported higher but <1.3 PI in sepsis than in controls [23,24] with the most frequent alterations in the first stages of sepsis [25,26]. PI was identified as a predictor of SAE in two studies, reporting high sensitivity and specificity for the presence of confusion when PI was high on the first day of admission [25]. However, it is important to notice that PI is not only a CVR estimator but is influenced by multiple vessel properties such as compliance, perfusion pressure and heart rate [27].
A systematic review and meta-analysis from 2017 [28] evaluated TCD studies in septic patients to identify the cerebral hemodynamic course of the disease and analyse the cerebral hemodynamic parameters. They found that in early sepsis, median MCAv and PI were increased, while cerebral autoregulation (CAR) remained unchanged. In later sepsis, median MCAv normalized, PI reduced, and CAR became impaired. In addition, they stated that increased PI may indicate higher CVR in sepsis, which is associated with a higher prevalence of sepsis associated delirium (SAD).

Table 1.
Summary of findings for studies regarding cerebral perfusion alterations. CBFi: cerebral blood flow index. CCP: critical closing pressure. CCT: cerebral circulation time. CD: cognitive decline. CO2R: CO2 reactivity. CRC: cerebrovascular reserve capacity. CVR: cerebrovascular resistances. ICA: internal carotid artery. MAP: mean arterial pressure. MCAv: middle cerebral artery velocities. PI: pulsatility index. RI: resistance index. SAD: sepsis associated delirium. SAE: sepsis associated encephalopathy. TCD: transcranial doppler.
Table 1.
Summary of findings for studies regarding cerebral perfusion alterations. CBFi: cerebral blood flow index. CCP: critical closing pressure. CCT: cerebral circulation time. CD: cognitive decline. CO2R: CO2 reactivity. CRC: cerebrovascular reserve capacity. CVR: cerebrovascular resistances. ICA: internal carotid artery. MAP: mean arterial pressure. MCAv: middle cerebral artery velocities. PI: pulsatility index. RI: resistance index. SAD: sepsis associated delirium. SAE: sepsis associated encephalopathy. TCD: transcranial doppler.
| Study | Main findings | Metric used | Sample size (septic patients) |
|---|---|---|---|
| Straver 1996 [22] | Inverse relationship between systemic vascular resistance index and mean and diastolic MCAv. MCA/ICA index and MAP showed an inverse relationship (changes in MCAv more pronounced than changes in ICA). MCA and ICA flow velocities abnormalities are more pronounced in severe disease and in non-survivors. | MCAv; PI; MCA/ICA index | 20 |
| Thees 2007 [29] | CO2R seemed not to be impaired. They didn't observe abnormal findings explaining neurological abnormalities. CCP increased as expected during hyperventilation (25±11 to 39±15mmHg). | CO2R, CCP; CBF calculated with thermodiluition and indocyanine green dye; CMRO2 | 10 |
| Pfister 2008 [30] | 12/16 patients presented SAD. No differences in CBF between SAD and non-SAD groups. | MCAv, Mx | 16 |
| Szatmàri 2010 [17] | PI was higher in the group with sepsis. Vasomotor response was slower and lower in sepsis (less CRC and lower systolic MCAv). | PI, acetazolamide test, cerebrovascular reactivity, CRC | 14 |
| Fülesdi 2012 [18] | PI was higher in septic patients. CRC was similar in the two groups while cerebrovascular reactivity decreased slower in the septic group (more prolonged vasodilatory response). | Acetazolamide test, cerebrovascular reactivity, CRC | 16 |
| Pierrakos 2013 [16] | TCD has a feasibility of 91% vs. 85%, p = 0.89 (septic vs controls) due to acoustic bone window. PI and RI were higher in patients with sepsis than controls and higher in the first day. Cerebral vascular constriction is detectable by TCD in the early stage of sepsis. | MCAv, PI, RI, eCBF | 20 |
| Pierrakos 2014 [25] | PI on the first day was a good predictor of the presence of confusion (AUC = 0.908, 95%, CI 0.80-0.98, p < 0.01). For a cut-off value of 1.3, there was a 95% sensitivity and an 88% specificity. | PI | 40 |
| Toksvang 2014 [31] | The increase in MAP with noradrenaline generated a mean increase in MCAv of 14% (2-22%). There was poor agreement between TCD and NIRS for CBF estimation. | MCAv | 8 |
| Berg and Plovsing 2016 [21] | Hyperventilation was associated with a 36% increase in CVR, and a consequent 22% reduction in MCAv. CO2R is preserved in septic patients. | CVR, CO2R | 16 (only 7 underwent hyperventilation) |
| Pierrakos 2017 [26] | PI was higher in patients with CD (2.2 ± 0.7 vs. 1.4 ± 0.5, p = 0.02) and CBFi was lower (363±170 vs. 499±133, p = 0.03). In univariate analysis, delirium and PI on the first day of the study were related to CD but in the multivariate analysis PI was not found to be related to CD independently of the presence of delirium. | PI, CBFi | 28 |
| Le Dorze 2018 [19] | Baseline CO and HR were higher, and MAP lower in the sepsis group when compared to a brain injury and an anesthetised group of patients (controls). PSV, was higher in the sepsis group than in the control group but not with BI group. After a fluid challenge PSV and EDV increased significantly only in the sepsis group. No significant correlations between systemic and cerebral hemodynamic changes were observed in any group. | PSV, EDV | 38 |
| Feng 2021 [23] | The SAD group exhibited lower levels of EDV and a higher PI but all within normal range (0.98±0.19 vs. 0.84±0.20, p=0.019). | MCAv, CBFi, PI, THRR | 51 |
| Zheng 2023 [20] | Patients with SAE showed significantly elevated PSV (107 [69–138] cm/s vs 85 [69–101] cm/s, P=.002) and mean MCAv (57 [37–93] vs 54 [42–66], P=.045) even if only in the left MCA and with mean MCAv within the normal range. The PI and RI were significantly higher in the SAE group than in the non-SAE group (even if the values were within the normal range). Patients with agitation had higher MCAv and lower PI and RI than patients with decreased consciousness, suggesting lower CVR. | MCAv, PSV, EDV, PI, RI, FV, CBF volume | 198 |
| Mei 2024 [24] | The SAE group displayed significantly elevated levels of PI, RI, and CCT, while EDV was lower. CCT emerged as the most efficacious predictor for SAE, with an AUC of 0.846. S100β, PI, and CCT were identified as the independent predictors for SAE. | PI, RI, CCT | 67 |
A particular note must be given to the cerebral circulation time (CCT), that uses contrast enhanced ultrasound to calculate the transition time from the internal carotid artery to the internal jugular vein. This time has been identified as an independent predictor for SAE with an AUC of 0846. Its calculation, however, requires a specific software and a trained US operator.
Autoregulation Estimation and Other Forms of Vessels’ Reactivity
When a single method to estimate CAR was used, septic patients variably presented altered or impaired autoregulation. Some studies reported near a half probability to find an altered CAR [32,33,34] while others reported normal CAR [35] [Table 2]. Interestingly, altered CAR was associated with delirium and SAEin a couple of studies, where CAR impairment was a SAD predictor (OR=5.77, 95% CI: 1.222–27.255, p=0.027) [Feng2021] or able to predict SAE (sensitivity 79%, specificity 47%) [32].
Some studies pointed out the role of the timing from sepsis onset to justify different states of autoregulation. A systematic review and meta-analysis conducted in 2017 [28] concluded that CAR remains unchanged in early sepsis, while became impaired later. However, this study drawn its conclusion from 4 studies evaluating CAR in the first 24 [35], 48 [30], 72 hours [36] and in an undetermined time from admission [37]. Unfortunately, the exact time of the measurements within those time spans were not reported. Conversely, a study by Schramm et al [38] measured CAR throughout the first 4 days from admission and reported a decreasing incidence of impairment with a percentage going from 60% at day 1 to 46% at day 4. In this study CAR impairment in the first day was associated with development of SAD at day 4.
Concerning the causative agents of CAR impairment a study by Pfister et al [30] found a significant association between delirium, elevated C-reactive protein and impaired CAR, suggesting that inflammation could impede cerebrovascular endothelial function thus impairing CAR. Endothelial function was addressed as the translation causative mechanism, as inflammation “per sè” was not associated with CAR impairment when measured by interleukin-6. On the other hand, two studies pinpointed the relevance of the mean arterial blood pressure (ABP) or arterial partial pressure of CO2 during CAR estimation stating that a weaker autoregulation might be detected when a low ABP or a high CO2 are present, since it is reached the lower limit of autoregulation [36,37]. As hypotension is a common clinical feature in sepsis, reduction of cerebral perfusion pressure (CPP) with consequent overtaking of the lower limit of autoregulation might be a frequent event that increases the chances to observe an impaired CAR.
Table 2.
studies regarding autoregulation in septic patients. CAI: cerebral autoregulation index. CAR: cerebral autoregulation. IOR: index of autoregulation. Mx, Mxa: mean flow index. THRR, THRT: transient hyperemia response ratio or transient hyperemia response test. SAE: sepsis associated brain dysfunction. SAD: sepsis associated delirium.
Table 2.
studies regarding autoregulation in septic patients. CAI: cerebral autoregulation index. CAR: cerebral autoregulation. IOR: index of autoregulation. Mx, Mxa: mean flow index. THRR, THRT: transient hyperemia response ratio or transient hyperemia response test. SAE: sepsis associated brain dysfunction. SAD: sepsis associated delirium.
| Study | Main findings | Metric used | Sample size (septic patients) |
|---|---|---|---|
| Matta and Stow 1996 [35] | Mean IOR was 0.92 (intact autoregulation). | IOR | 10 |
| Pfister 2008 [30] | CAR was altered in the SAD patients, with no differences on perfusion in respect to the non-SAD group. | Mx | 16 |
| Steiner 2009 [37] | Correlation between Mx and another index of autoregulation from near infrared spectroscopy showed a strong positive association (R = 0.81; P < 0.0001). PaCO2-induced dilatation of flow-regulating vessels was associated with worse autoregulation. | Mx | 23 |
| Taccone 2010 [36] | CAR was impaired in 66% of patients, and impairment increased for higher PaCO2 values. | CAI | 21 |
| Schramm 2012 [38] | CAR was impaired in 88% of the patients, with a decreasing prevalence during the days (day1 - 60%, day2 - 59%, day3 - 41%, day4 - 46%). The status of CAR at day 1 was related to SAD development at day 4. SAD was associated with age. | Mx | 30 |
| Crippa 2018 [32] | 50% of patients presented impaired CAR. There was no difference in Mxa between survivors and non-survivors (at ICU discharge). Mxa was higher in patients with SAE. The best Mxa cut-off to predict SAE was 0.18 (sensitivity 79%, specificity 47%). | Mxa | 100 |
| Feng 2021 [23] | The SAD group had a significantly higher level of cerebrovascular dysfunction (THRR index < 1.09, 40 vs. 10%, p=0.01). THRR index<1.09 was a SAD predictor (OR=5.77, 95% CI: 1.222–27.255, p=0.027). | THRR | 51 |
| Crippa 2022 [33] | 53% patients had impaired CA. | THRT | 40 |
| Caldas 2022 [34] | Median ARI and Mxa values were 4.38 [2.83–6.04] and 0.32 [0.14–0.59], respectively. Impaired CAR according to the ARI threshold was observed in 42% of patients; impaired CAR according to Mxa threshold was observed in 53% patients. Mx and ARI had a weak correlation and a poor agreement to classify CAR. |
ARI, Mx | 95 |
Regarding CO2 reactivity (CO2R) some studies reported an impaired value [39,40], while other a normal value [29,35] [Table 3]. Interestingly, one study reporting an impaired CO2R did not found a relationship with mortality, while in another study where CO2R was not impaired reported a pathological neurologic exam in all the survived patients enrolled [29].
In summary, variable rates of impaired CAR are reported in literature. Even if some studies report normal CAR, the majority of studies report frequent CAR alterations and highlight the association of CAR impairment with SAD or other forms of impaired neurologic outcome in sepsis. Destruction of CAR is probably a phenomenon that comes and goes with different incidence during the course of the illness, with a high probability of alterations during the earlier and more severe phases. In addition, typical features of sepsis as hypotension or a high arterial CO2 might influence observations increasing the rate of impaired CAR measures.
Resuscitation
Noteworthy a study by De Goede et al [41] compared the MCA flow waveform between septic non-resuscitated patients and controls. Non-resuscitated patients presented lower diastolic and peak systolic MCAv, with a decreased acceleration time from baseline to the systolic peak. In addition, the absence of a secondary systolic peak, that progressively reappeared during resuscitation, was noticed. The acceleration time as well as the first and second systolic peak velocities increased significantly after resuscitation. The authors stated that brief repetitive TCD measurement during resuscitation were feasible and reappearance of the second systolic peak could be used as an hemodynamic monitoring metric.
Another study [19] evaluated the CBF modifications induced by fluid challenge in fluid responders. A comparison was made between septic patients, anesthetised patients and brain injured patients. They found an increase in peak systolic velocity (PSV) and end diastolic velocity (EDV) of MCA only in the sepsis group with no significant correlations between systemic and cerebral hemodynamic changes in any group, drawing to the conclusion that the increase in cardiac output after a fluid challenge elicit an increase in MCAv only in patients with severe acute systemic inflammation. This might be due to the sepsis-induced impairment of CAR or because the lower limit of autoregulation is often undertaken in this population. However, since CBF changes were not linked to systemic hemodynamics, direct CBF monitoring during resuscitation may be crucial to provide an adequate brain perfusion.
Regarding the possibility of an increase in cerebral edema due to aggressive fluid resuscitation, Pfister et al [42] observed no correlation between the nICP estimation with TCD and the daily fluid administration or balance.
Non-Invasive Cerebral Perfusion Pressure and Estimation of Intracranial Pressure
Only three studies regarding nICP and estimated cerebral perfusion pressure (eCPP) assessment in sepsis were found (Table 4). Unfortunately, ICP can’t be directly measured in these patients as considered too harmful. Reliability of ICP estimation with TCD, however, has been demonstrated to be low on the absolute value, but very good to reflect the general trend in comparison with the invasive ICP [43]. However, considering the incidence of hypotension and hypoperfusion occurring during sepsis and septic shock, estimation of non-invasive cerebral perfusion pressure (eCPP) by the mean of brain US can be a useful monitoring tool.
Feasibility of monitoring changes in cerebral perfusion with TCD during sepsis, was assessed by Pierrakos et al in 2013 [16]. A study by Pfister et al [42] evaluated eCPP and therefore nICP in 16 septic patients, with daily repeated measures, hypothesising that aggressive fluid administration with a derangement of vascular permeability could have provoked cerebral edema and increased ICP. However, the nICP was always below 20mmHg, and the absolute value of nICP was not related to mortality. Nevertheless, patients with low eCPP presented higher level of S-100β protein, suggesting that brain damage was directly related to hypoperfusion rather than intracranial hypertension. Another study [33] estimated eCPP and nICP in 40 septic patients. 55% of patients presented an eCPP below 60mmHg with a nICP greater than 16mmHg. Some patients in the study presented a nICP around 40mmHg, and a higher value of nICP was related to a lower neurological pupil index. The same group of researchers analysed eCPP and nICP in a cohort of 132 patients [Crippa 2023], highlighting again that even if the majority of septic patients (63%) presented with normal eCPP and nICP, nearly one third had low eCPP values. No differences were found on incidence of SAE between patients with abnormal eCPP or nICP and who had normal values.
Evaluation of the Neurologic Outcome
SAE has classically been associated with delirium during its acute phases. The majority of studies evaluated delirium in ICU using the CAM-ICU scale; for what concern long-term neurologic outcome there is a paucity of studies, and we identified only one cognitive decline (CD) related study [26] (Table 5).
A study by Feng et al [23] evidenced how an altered transient hyperemia response test (THRT) evaluated with TCCS in the first 6 hours after resuscitation in patients with septic shock, was an independent predictor of SAD [OR 5.77]; patients with delirium presented a poorer outcome (survival at 28 days), a higher APACHE II score, increased biomarkers for neuronal damage (NSE, neurospecific enolase), increased ICU length of stay and more days of ventilation. In a similar study [38], daily evaluation of CAR during the first 4 days after sepsis was assessed; patients that presented impaired autoregulation (Mx>0,3) at day 1, had a higher incidence of delirium at day 4. However, in this case, association with severity of the illness (APACHE II) or neuronal damage markers (NSE) was not evidenced. Another study, in accordance with the precedents, demonstrated that CAR derangement was associated with delirium, independently of APACHE II score, MAP, CBF velocity and catecholamine requirements [Pfister 2008].
Interestingly, in a study by Pierrakos et al [26] ROC curve analysis showed that PI on the first day (but not on the third day) was a good predictor of the presence of confusion (AUC = 0.908, 95%, CI 0.80-0.98, p < 0.01). PI was related to confusion independently from age or APACHE II score. In another study from the same group [26], 50% of patients that presented CD or persistent coma at ICU discharge presented an elevated PI and a lower CBFi on the first day of admission for sepsis (PI 2.2±0.7 vs. 1.4±0.5, p=0.02); PI increase was persistent in patients with persistent coma, while the alterations of PI were momentaneous in the other patients. Crippa et al [32] identified as SAE independent predictors an impaired CAR (evaluated with Mxa), vascular diseases and mechanical ventilation. The best Mxa cut-off to predict SAE was 0.18 (sensitivity 79%, specificity 47%). However, Mxa was not different between survivors and non survivors.
Regarding possible increases in nICP, two studies failed in proving its role for SAE and mortality prediction [44,45]. Even if Czempik et al [45] found a high probability of measuring a ONSD >5.7 at least once during the ICU stay, these high measurements were not related to CRP concentrations, highest daily lactate, or SOFA; assuming that a dilated ONSD could be related to SAE the authors concluded that ONSD measurement has to be used cautiously for SAE screening. In the other study by Crippa et al [44] patients with normal and high nICP or normal and low eCPP presented no difference in SAE occurrence or mortality.
A recent study [24] tried to use a composite TCD and biohumoral input to predict SAE. After analysing various metrics as inputs, they concluded that S100β, PI and CCT measured in the first 24h from ICU admission were independent predictors for SAE.
Finally, three systematic review and meta-analysis that investigated if delirium was related to microvascular damage in sepsis, concluded that cerebral perfusion disturbances might be associated with SAD. However, heterogeneity in delirium definitions and assessment in addition to different TCD metrics analysed can be confounding factors [46]. In the same way, another systematic review concluded that the reviewed studies indicate a link between impaired CAR and poor outcomes, but due to variations in study design and methodological limitations, further research is needed [47]. Heterogeneity in neuromonitoring tools in sepsis was also found in another study [48].
Discussion
The main findings of the present manuscript are: 1) CBF alterations are common in septic patients and 2) might be related to sepsis severity. 3) TCD metrics can be used to predict neurologic impairment and 4) brain perfusion monitoring during resuscitation is feasible.
The body of evidence we found was constituted only by observational studies (85%) or systematic reviews with/without meta-analysis (15%), often with small sample sizes and with very heterogeneous methodologies. Regarding studies heterogeneity we found some main criticalities regarding sepsis definition (i.e. study populations), time of observation, and metrics considered. An overview of the sepsis definitions used, and distribution of studies is available in the supplementary material, Attachment 3. The different sepsis definition has influenced the composition of the study cohorts, modifying inclusion criterions. Nevertheless, even if sepsis definition might have had a minor impact on patients’ selection, the presence of shock might have had more influence on the observed cerebral perfusion abnormalities, as highlighted in one of the included studies [37]. In fact, the cohorts of the studies were often composed by a mix of septic and shock septic patients.
The time of observation varied among studies, with studies observing patients within 24, 48 or 72 hours, or in a not specified timeframe; even the relationship between observation and time 0 was different, with some studies referring to symptoms’ onset and others to ICU admission. The observation time represents a crucial methodological issue because CBF alterations might present at different timepoints during the illness as presented in the study by Schramm et al [38]. The possibility to have multiple observations during the days or even multiple observations in the same day, could thus be a big improvement for results interpretation.
Concerning the metrics analysed, discussion of multiple ways of calculating similar indexes is beyond the aim of the manuscript and has been addressed elsewhere [54]. An overview of all the brain US metrics used by authors of the 34 included papers is available in Table 7. However, readers should have in mind that there’s a huge difference in the way of calculating indexes of autoregulation and non-invasive ICP or CPP. In respect to CAR metrics, we can divide these indexes in qualitative and quantitative, that are typically either snapshot (the former) or continuously calculated metrics (the later). In addition, indexes can measure the static or dynamic autoregulation, that measure the response of flow to steady state or rapid changes of ABP (e.g. ABP challenges versus spontaneous oscillations in ABP - Table 7). The concordance of different indexes is anything but obvious, with some studies demonstrating poor agreement between different indexes. In a study by Caldas et al [34], when different types of indices were compared in the same 95 patients, they were concordant only in a minority of patients, with 24% of patients presenting impaired autoregulation with both Mxa and ARI (autoregulation index), 29% of patients presenting intact CAR, and the remaining alternatively classified as impaired or intact CAR based on the index used. It remains unclear whether the poor correlation between CAR metrics is due to inherent differences in the various algorithmic models or if it results from unidentified external 'noise' present in the real-world data, such as unrelated components in ABP and CBF [55]. This uncertainty complicates meaningful comparisons. To see an overview of how the authors calculated different TCD metrics please see Table 6.
Table 6.
Overview of the brain US metrics used by authors and their reported definitions. CAR: cerebrovascular autoregulation. CBF: cerebral blood flow. dCA: dynamic cerebral autoregulation. EDV: end diastolic velocity. FV: flow velocity. MCAv: middle cerebral artery flow velocity. MAP: mean arterial pressure. PSV: peak systolic velocity.
Table 6.
Overview of the brain US metrics used by authors and their reported definitions. CAR: cerebrovascular autoregulation. CBF: cerebral blood flow. dCA: dynamic cerebral autoregulation. EDV: end diastolic velocity. FV: flow velocity. MCAv: middle cerebral artery flow velocity. MAP: mean arterial pressure. PSV: peak systolic velocity.
| TCD/TCCS metrics | Acronym | Index explanation | Reference for calculation | Article |
|---|---|---|---|---|
| Acceleration | acc | Acceleration is defined as the maximal increase in FV per second during the systolic upstroke and was obtained by taking the maximum of the first order derivative of the ensemble average during the period lasting from systolic onset until first local maximum. | Schaafsma A. Improved parameterization of the transcranial Doppler signal. Ultrasound Med Biol 2012;38:1451–1459. |
De Goede 2017 |
| Autoregulation index | ARI | The signals were filtered, interpolated and resampled at 5Hz. Then the Welch method was used for smoothing spectral estimates derived from the fast Fourier transform (FFT) over segments of 102.4 seconds with 50% overlap. ARI values were obtained by fitting a second-order polynomial to minimize the error, using neighboring integer ARI values as a reference. ARI ranges from 0 (absent dynamic cerebral autoregulation, dCA) to 9 (most efficient dCA). | Caldas et al, Dynamic autoregulation is impaired in circulatory shock. Shock Augusta Ga. (2020) 54:183–9. Czosnyka et al, Monitoring of cerebral autoregulation. Neurocrit Care. (2014) 21(Suppl. 2):S95–102. Panerai RB. Transcranial Doppler for evaluation of cerebral autoregulation. Clin Auton Res Off J Clin Auton Res Soc. (2009) 19:197–211. |
Caldas 2022 |
| Cerebral autoregulation index | CAI | Ratio of the relative changes in cerebrovascular resistances (CVR) and MAP Normal value: 0-2. |
Bouma GJ, Muizelaar JP. Cerebral blood flow, cerebral blood volume, and cerebrovascular reactivity after severe head injury. J Neurotrauma. 1992 Mar;9 Suppl 1:S333-48. | Taccone 2010 |
| Cerebral capillary closing pressure | CCP | Zero-flow velocity pressure as extrapolated by regression analysis of arterial pressure/MCAV plots, averaged over two respiratory cycles. | Thees et al, Anesthesiology. 2002 Mar;96(3):595-9 | Thees 2007 |
| Cerebral circulation time (assessed via contrast enhanced ultrasound) | CCT | Similarly to TCD, CCT measures the interval between the entry of arterial blood in the internal carotid artery (ICA) and its exit through the internal jugular vein (IJV). Utilizing a C5-1 convex array transducer, both the ICA and IJV were visualized in a transverse cross-sectional plane, specifically at a location 1.5 cm superior to the bifurcation of the common carotid artery. settings were switched to “contrast mode” with reduced mechanical and thermal indices. An FDA-approved microbubble contrast agent (SonoVue, Bracco, Milan, Italy) was prepared in 5mL of isotonic saline and rapidly administered via the median cubital vein, followed by a 5mL saline flush. Bolus administration and subsequent CCT assessments were performed on the side demonstrating higher blood flow velocity in earlier TCD measurements. Analysis of the imaging data was executed through uninterrupted video capture, with time-intensity curves being isolated post-recording by a seasoned ultrasonographer. The inbuilt software automatically processed these curves after targeting the ICA and IJV. | Liu X, et al. A new method of measurement of cerebral circulation time: contrast-enhanced ultrasonography in healthy adults and patients with intracranial shunts. Ultrasound Med Biol. (2014) 40:2372–8. | Mei 2024 |
| Cerebral metabolic rate of oxygen | CMRO2 |
With PvO2 as the pressure of oxygen in the jugular vein. |
- | Thees 2007 |
| Cerebrovascular reserve capacity | CRC | The maximal % increase of the blood flow velocity after acetazolamide administration. |
- | Szatmári 2010, Fülesdi 2012 |
| CO2 reactivity | CRCO2 | Difference between the MCAv at hypocapnia and hypercapnia expressed as a percentage of the baseline MCAv per kPa change in ETCO2. | - | Bowie 2003 |
| Absolute CO2R: change in MCAv per kPa change in PaCO2 Relative CO2R: percentage change in MCAv at PaCO2 5.3 kPa per kPa change in PaCO2 |
Matta and Stow 1996 | |||
| Percentage change in MCAv per kPa change in PaCO2 | Thees 2007 | |||
| CO2 reactivity, normalised | NCR | % change in CBF velocity per 1% increase in EtCO2 | Terborg 2001 | |
| Cerebrovascular resistances | CVR | CVR = MAP/MCAv | - | Taccone 2010, Berg 2016 |
| Cerebrovascular reactivity | CVR | CVR = (MCAacz - MCAv rest)/MCAv rest ; MCAvacz is the MCA mean blood flow velocity measured at 5, 10, 15 and 20 minutes after acetazolamide, and MCAvrest is the MCA mean blood flow velocity measured at rest. | - | Szatmári 2010, Fülesdi 2012 |
| Diastolic FV | Dias@560 | Dias@560 was obtained by calculating the mean blood FV during the interval 520–600 ms after stroke onset. Finally, the acc, sys1 and sys2 values were divided by the dias@560 value for normalization. | Schaafsma A. Improved parameterization of the transcranial Doppler signal. Ultrasound Med Biol 2012;38:1451–1459. |
De Goede 2017 |
| Estimated CBF (CBF index) | CBFi or CBF | - | Pierrakos 2013 | |
| Pierrakos 2013 | Pierrakos 2014 | |||
| Pierrakos 2013 | Pierrakos 2016 | |||
| - | Feng 2019 | |||
| A 25 mg dose of indocyanine green dye, dissolved in 40 ml of iced 5% glucose solution, was used as a double-indicator and injected into the right atrium through a central venous line. Dilution curves for both the dye and temperature were recorded simultaneously using thermistor-tipped fiber-optic catheters placed in the aorta (via a 30 cm catheter inserted into the femoral artery) and the jugular bulb. All measurements were taken from the sonographically controlled dominant (right) internal jugular vein. CBF was calculated based on the mean transit time of the first pass of the thermal and dye indicators using a specialized computer system. | Wietasch GJK, et al. Bedside assessment of cerebral blood flow by double-indicator dilution technique. Anesthesiology 2000, 92:367-375.13. Mielck F, et al. Reliability of cerebral blood flow measurements by transcerebral double-indicator dilution technique. Eur J Anaesth 2001, 18:653-661. |
Thees 2007 | ||
| Estimated CPP | eCPP | Czosnyka et al, Cerebral perfusion pressure in head-injured patients: A noninvasive assessment using transcranial Doppler ultrasonography. J. Neurosurg. 1998, 88, 802–808. | Crippa 2022, Crippa 2024 | |
| Schmidt et al, Adaptive noninvasive assessment of intracranial pressure and cerebral autoregulation. Stroke. 2003 Jan;34(1):84-9. | Pfister 2008 | |||
| Intravascular flow volume | FV | For a defined vessel, FV was defined as the product of time-averaged flow velocity (TAV) and its cross-sectional area (A) according to the formula: D= diameter. The CBF volume was determined as the sum of the FVs of the internal carotid artery and vertebral artery of both sides. |
Scheel et al, Color duplex measurement of cerebral blood flow volume in healthy adults. Stroke 2000; 31:147–150 | Zheng 2024 |
| Index of autoregulation | IOR | Ratio of percentage change in estimated cerebral vascular resistance (CVRe) to percentage change in MAP, using the equations CVRe = MAP/MCAv and IOR =%∂CVRe/ %∂ MAP, where MAP at the time of MCAv measurement | Matta BF, Lam AM, Strebel S, Mayberg TS. Cerebral pressure autoregulation and CO2-reactivity during propofolinduced EEG suppression. British Journal of Anaesthesia 1995; 74: 159–163. | Matta and Stow 1996 |
| Mean flow index | Mx or Mxa | General definition: the Mx or Mxa index is calculated as a moving correlation coefficient between short-term fluctuations in two signals over a specific time window (e.g., 5-10 seconds). Mx usually refers to a calculated index between CPP and MCAv, conversely Mxa refers to ABP and MCAv. In septic patients, thus, Mxa is used, even if in the papers is commonly referred as Mx or Mxa alternatively. A positive correlation suggests that increases in blood pressure lead to increases in MCAv, indicating impaired autoregulation (Mxa>0.3). In contrast, a near-zero or negative correlation indicates effective autoregulation, where CBF remains stable despite changes in MAP. |
||
| In this article: values of MAP and FV averaged every 10”. Mx is calculated every 60“ as the moving linear correlation coefficient between the last 30 consecutive values of MAP and FV (5 minutes). | Piechnik SK, et al. The continuous assessment of cerebrovascular reactivity: a validation of the method in healthy volunteers. Anesth Analg 1999, 89:944-949. |
Pfister 2008 (2) | ||
| In this article: values of MAP and FV averaged every 6”. Mx is calculated every 60” as the moving linear correlation coefficient between the last 30 consecutive values of MAP and FV (3 minutes). | Czosnyka et al, Monitoring of cerebral autoregulation in head-injured patients. Stroke. 1996;27:1829–34. Piechnik SK et al, The continuous assessment of cerebrovascular reactivity: a validation of the method in healthy volunteers. Anesth Analg. 1999;89:944–9. | Schramm 2012 | ||
| In this article: values of MAP and FV averaged every 10”. Mx is calculated every 60“ as the moving linear correlation coefficient between the last 30 consecutive values of MAP and FV (5 minutes). | Czosnyka et al, Monitoring of cerebral autoregulation in head-injured patients. Stroke. 1996;27:1829–34. Piechnik SK et al, The continuous assessment of cerebrovascular reactivity: a validation of the method in healthy volunteers. Anesth Analg. 1999;89:944–9. | Steiner 2009, Caldas 2022, Crippa 2022 (2), Crippa 2024 | ||
| The Pearson’s correlation coefficient between the averaged ABP and flow velocity averaged on 10s-consecutive windows with 50% overlap. | Czosnyka et al, Monitoring of cerebral autoregulation in head-injured patients. Stroke. 1996;27(10):1829–34. | Crippa 2018 | ||
| Non-invasive ICP or estimated ICP | nICP or eICP (Crippa 2022, Crippa 2024) | Mathematical algorithm built up starting from various TCD waveform parameters and ABP, that aims to estimate with precision the nICP. | Schmidt et al, Adaptive noninvasive assessment of intracranial pressure and cerebral autoregulation. Stroke. 2003 Jan;34(1):84-9. | Pfister 2008 |
| Czosnyka, M. et al. Cerebral perfusion pressure in head-injured patients: A noninvasive assessment using transcranial Doppler ultrasonography. J. Neurosurg. 1998, 88, 802–808. Rasulo FA, et al. The accuracy of transcranial Doppler in excluding intracranial hypertension following acute brain injury: a multicenter prospective pilot study. Crit Care. 2017;21(1):44. |
Crippa 2022, Crippa 2024 | |||
| Resistance index | RI | RI = (PSV – EDV)/PSV | Berg 2015, Berg and Plovsing 2016, Caldas 2022, Zheng 2023, Mei 2024 | |
| Systolic component 1 and 2 | Sys1 and Sys2 | Sys1 and sys2 are the maximal flow velocities within the first and second systolic peaks and were obtained by taking the zero-line crossing of the first (if necessary second) order derivative of the ensemble average during the first 100ms and during the remaining part of systole, respectively. | Schaafsma A. Improved parameterization of the transcranial Doppler signal. Ultrasound Med Biol 2012;38:1451–1459. |
De Goede 2017 |
| Percentage of waveforms without the second systolic peak | %no_sys2 | Percentage of 10-s intervals in which no sys2 was detected. | Schaafsma A. Improved parameterization of the transcranial Doppler signal. Ultrasound Med Biol 2012;38:1451–1459. |
De Goede 2017 |
| Transient hyperemia response ratio or Transient hyperemia response test | THRR (Feng 2021) or THRT (Crippa 2022) | CBF is analysed before, during and after the ipsilateral compression of the carotid artery at the neck level. Flow must undergo a reduction of 30-50% from baseline to ensure a proper compression. Compression duration is between 3 and 9s. After the occlusion is released, blood flow rapidly increases (hyperemia) and velocity is usually higher than the baseline due to a vasodilation occurring during compression. Ratio between maximal post-release (5 heartbeats) and baseline PSV is measured. A THRR index above 1.09 (>10% increase) is regarded as indicating dynamic cerebral vascular autoregulation function; if the level falls below 1.09, this is regarded as indicating impairment of CAR. | Cavill et al Factors affecting assessment of cerebral autoregulation using the transient hyperaemic response test. Br J Anaesth. (1998) 81:317–21 |
Feng 2021 |
| Zeileret et al, Pressure Autoregulation Measurement Techniques in Adult Traumatic Brain Injury, Part I: A Scoping Review of Intermittent/Semi-Intermittent Methods. J. Neurotrauma 2017, 34, 3207–3223. | Crippa 2022 | |||
| Gain, phase, coherence | - | Gain phase and coherence are transfer function analysis metrics that compare two signals in their spectrum frequency (ABP and MCAv). They quantify the effectiveness of dynamic CAR as a filter that dampens MAP-induced changes in CBF. In particular, gain compares the amplitude of the signals hypothesising that high amplitude oscillations in ABP should be dampened in CBF. Phase refers to the displacement of the CBF signal relative to the MAP signal, which reflects the response time of dynamic CAR. Coherence quantifies the linearity between the spectral power of CBF and the spectral power of MAP, assuming that when signals are highly related changes in ABP are passively transmitted to CBF and CAR is impaired. | Zhang R, Zuckerman JH, Giller CA, Levine BD. Transfer function analysis of dynamic cerebral autoregulation in humans. Am J Physiol 1998;274:H233–41. Panerai RB, Dawson SL, Potter JF. Linear and nonlinear analysis of human dynamic cerebral autoregulation. Am J Physiol 1999;277:H1089–99. Meel-van den Abeelen AS, van Beek AH, Slump CH, Panerai RB, Claassen JA. Transfer function analysis for the assessment of cerebral autoregulation using spontaneous oscillations in blood pressure and cerebral blood flow. Med Eng Phys 2014;36:563–75. |
Berg 2015, Berg and Plovsing 2016 |
| Optic nerve sheet diameter | ONSD | Wang, L.J.; et al. Non-invasive and quantitative intracranial pressure estimation using ultrasonographic measurement of optic nerve sheath diameter. Sci. Rep.2017, 7, 42063 | Czempik 2020 |
Table 7.
Indexes used for autoregulation estimation in the body of evidence analysed. To note that this is note the complete list of all the ways to estimate autoregulation.
Table 7.
Indexes used for autoregulation estimation in the body of evidence analysed. To note that this is note the complete list of all the ways to estimate autoregulation.
| Dynamic AR | Static AR | |
|---|---|---|
| Snapshot metrics, qualitative | THRT - Transient hyperemia response test | - |
| Prolonged monitoring required, quantitative | ARI – Autoregulation index Mxa – Mean flow index (assessed between ABP and MCAv) Transfer function analysis indexes (Phase, gain, coherence) |
CAI – Cerebral autoregulation index IOR – Index of autoregulation |
Other sources of heterogeneity must be cited for what concerns nICP estimation. In this case not only different methods of estimating it were used, but one of the most used ways of calculation is able to reflect with high reliability the trend of the real ICP, but it has a high confidence interval in estimating the absolute value [43].
Some limitations of the present manuscript are intrinsically related to the nature of scoping reviews, which try to answer to broad spectrum questions with highly heterogeneous studies. In addition, the low quality of evidence (observational studies only) represents another limitation.
Research Gaps, Awaited Studies, and Future Directions
More efforts need to be done in establishing with certainty cerebral haemodynamic alterations in sepsis, and how they may change during the critical illness course. In addition, there is a lack of studies on resuscitation and non-invasive ICP and CPP estimation, that could be useful in a systematic assessment of brain health and might contribute to ruling out intracranial pathologies whenever neurologic impairment is present.
In addition to studies evaluating multiple timeframes, implementation of 2D brain images retrievable with TCCS (ONSD, midline shift, direct visualization of third and lateral ventricles) might be a valuable addition to the nICP and eCPP estimation when a proper acoustic bone window is available [56]. Even if these techniques have been extensively described, at the moment no studies have systematically evaluated their usefulness and impact on the management of septic patients in ICU [57].
Concerning resuscitation only general protocol for patients with shock [10,58], or POCUS protocols not involving the brain have been published [59]. Thus, a study about a comprehensive brain US protocol in sepsis and septic shock is awaited. In fact, an expanding field of research regards peripheral perfusion-guided resuscitation, and multiorgan perfusion assessment [60,61]. The basic principle that guides researchers in this direction is that if the peripheral organs are adequately perfused, resuscitation can have success and vice-versa [62]. So, as long as each organ have its own autoregulation range that changes dynamically, if autoregulation is impaired perfusion will be totally dependent on perfusion pressure. Evaluation of the actual perfusion is crucial to guarantee ad adequate oxygen supply. In this perspective, some studies assessing brain perfusion in traumatic brain injured patients demonstrated that targeting a perfusion pressure within the range of autoregulation is feasible, and can be done at the bedside with proper instrumentations and the aid of a bedside software (ICM+, Cambridge enterprise, Ltd) [63]. However, the benefit of MAP titration to fit into the range of autoregulation has not yet clearly established, and further research is needed to clarify the advantages.
For certain, tailoring of therapies and titration of drugs based not only on central haemodynamics but also on peripheral perfusion is promising, and could be one of the critical interventions that dramatically improves the outcome of septic patients. In fact, it is emerging from literature that one MAP target is not always adequate for all [61,64,65]. Implementation of brain multimodal evaluation including brain US and other non-invasive neuromonitoring tools (i.e. near infrared spectroscopy, pupillometry and EEG), may give additional information about brain hypoperfusion, electric malfunctioning (i.e. epilepsy), sedation adequacy, and prediction of outcome, and might be useful in clinical practice [66,67].
Conclusions
The current body of evidence regarding brain US in patients with sepsis and septic shock has a poor grade, but it is possible to say that brain US can identify cerebral perfusions alterations. Its usage during resuscitation is feasible and warrants further investigations. Use of brain US during resuscitation and for prediction of outcome is not currently supported by evidence. However, further studies on brain perfusion, acquisition of 2D images of parenchyma (TCCS) and application of a multimodal brain monitoring might be useful in these contexts. Further studies are warranted regarding the possibility of using brain US for tailored resuscitation and to establish the usefulness of a complete brain US evaluation and its capacity of modifying the clinical management.
Funding sources/sponsors
None to declare.
Conflicts of interest
Authors have no conflicts of interest, related to this review, to declare.
Abbreviations
ABP: arterial blood pressure
APACHE: Acute Physiology and Chronic Health Evaluation
ARI: autoregulation index
BBB: blood brain barrier
CAR: cerebral autoregulation
CBF: cerebral blood flow
CPP: cerebral perfusion pressure
eCPP: estimated cerebral perfusion pressure
EEG: electro encephalogram
ICP: intracranial pressure
ICU: intensive care unit
MAP: mean arterial pressure
Mx and Mxa: mean flow index
nICP: non-invasive intracranial pressure
PI: pulsatility index
POCUS: point of care ultrasound
RI: resistance index
SAD: sepsis-associated delirium
SAE: sepsis-associated encephalopathy
TCD: transcranial doppler
TCCS: transcranial color-coded sonography
THRT: transient hyperemia response test
References
- Sonneville R, Benghanem S, Jeantin L, de Montmollin E, Doman M, Gaudemer A, et al. The spectrum of sepsis-associated encephalopathy: a clinical perspective. Crit Care. 2023 Oct 5;27(1):386. [CrossRef]
- Czempik PF, Pluta MP, Krzych ŁJ. Sepsis-Associated Brain Dysfunction: A Review of Current Literature. Int J Environ Res Public Health. 2020 Aug;17(16):5852. [CrossRef]
- Eidelman LA, Putterman D, Putterman C, Sprung CL. The spectrum of septic encephalopathy. Definitions, etiologies, and mortalities. JAMA. 1996 Feb 14;275(6):470–3. [PubMed]
- Semmler A, Widmann CN, Okulla T, Urbach H, Kaiser M, Widman G, et al. Persistent cognitive impairment, hippocampal atrophy and EEG changes in sepsis survivors. J Neurol Neurosurg Psychiatry. 2013 Jan;84(1):62–9. [CrossRef]
- Sprung CL, Peduzzi PN, Shatney CH, Schein RM, Wilson MF, Sheagren JN, et al. Impact of encephalopathy on mortality in the sepsis syndrome. The Veterans Administration Systemic Sepsis Cooperative Study Group. Crit Care Med. 1990 Aug;18(8):801–6. [CrossRef]
- Chung HY, Wickel J, Brunkhorst FM, Geis C. Sepsis-Associated Encephalopathy: From Delirium to Dementia? J Clin Med [Internet]. 2020 Mar;9(3). Available from: https://pubmed.ncbi.nlm.nih.gov/32150970/. [CrossRef]
- Calviello LA, Cardim D, Czosnyka M, Preller J, Smielewski P, Siyal A, et al. Feasibility of non-invasive neuromonitoring in general intensive care patients using a multi-parameter transcranial Doppler approach. J Clin Monit Comput. 2022 Dec;36(6):1805–15. [CrossRef]
- Klawitter F, Jager M, Klinkmann G, Saller T, Söhle M, von Möllendorff F, et al. Sepsis-assoziierte Enzephalopathie. Anaesthesist. 2021 Feb 1;70(2):112–20. [CrossRef]
- Battaglini D, Pelosi P, Robba C. The Importance of Neuromonitoring in Non Brain Injured Patients. Crit Care Lond Engl. 2022 Mar 22;26(1):78. [CrossRef]
- Robba C, Wong A, Poole D, Al Tayar A, Arntfield RT, Chew MS, et al. Basic ultrasound head-to-toe skills for intensivists in the general and neuro intensive care unit population: consensus and expert recommendations of the European Society of Intensive Care Medicine. Intensive Care Med. 2021 Dec;47(12):1347–67. [CrossRef]
- Tavazzi G, Spiegel R, Rola P, Price S, Corradi F, Hockstein M. Multiorgan evaluation of perfusion and congestion using ultrasound in patients with shock. Eur Heart J Acute Cardiovasc Care. 2023 May 4;12(5):344–52. [CrossRef]
- Bertuetti R, Gritti P, Pelosi P, Robba C. How to use cerebral ultrasound in the ICU. Minerva Anestesiol [Internet]. 2020 Mar [cited 2024 Sep 3];86(3). Available from: https://pubmed.ncbi.nlm.nih.gov/31922373/. [CrossRef]
- Lau VI, Arntfield RT. Point-of-care transcranial Doppler by intensivists. Crit Ultrasound J. 2017 Oct 13;9(1):21. [CrossRef]
- Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med. 2018 Oct 2;169(7):467–73. [CrossRef]
- Peters MDJ, Godfrey C, McInerney P, Khalil H, Larsen P, Marnie C, et al. Best practice guidance and reporting items for the development of scoping review protocols. JBI Evid Synth. 2022 Apr 1;20(4):953–68. [CrossRef]
- Pierrakos C, Antoine A, Velissaris D, Michaux I, Bulpa P, Evrard P, et al. Transcranial doppler assessment of cerebral perfusion in critically ill septic patients: a pilot study. Ann Intensive Care. 2013;3:28. [CrossRef]
- Szatmári S, Végh T, Csomós A, Hallay J, Takács I, Molnár C, et al. Impaired cerebrovascular reactivity in sepsis-associated encephalopathy studied by acetazolamide test. Crit Care Lond Engl. 2010;14(2):R50. [CrossRef]
- Fülesdi B, Szatmári S, Antek C, Fülep Z, Sárkány P, Csiba L, et al. Cerebral vasoreactivity to acetazolamide is not impaired in patients with severe sepsis. J Crit Care. 2012 Aug;27(4):337–43. [CrossRef]
- Le Dorze M, Huché F, Coelembier C, Rabuel C, Payen D. Impact of fluid challenge increase in cardiac output on the relationship between systemic and cerebral hemodynamics in severe sepsis compared to brain injury and controls. Ann Intensive Care. 2018 Jun 28;8(1):74. [CrossRef]
- Zheng Y, Shen M, Xuan L, Pan S, Chen S, Zhong M, et al. Cerebral Blood Flow Alterations in Sepsis-Associated Encephalopathy: A Prospective Observational Study. J Ultrasound Med Off J Am Inst Ultrasound Med. 2023 Aug;42(8):1829–39. [CrossRef]
- Berg RMG, Plovsing RR. Effects of short-term mechanical hyperventilation on cerebral blood flow and dynamic cerebral autoregulation in critically ill patients with sepsis. Scand J Clin Lab Invest. 2016;76(3):226–33. [CrossRef]
- Straver JS, Keunen RW, Stam CJ, Tavy DL, De Ruiter GR, Smith SJ, et al. Transcranial Doppler and systemic hemodynamic studies in septic shock. Neurol Res. 1996 Aug;18(4):313–8. [CrossRef]
- Feng Q, Ai M, Huang L, Peng Q, Ai Y, Zhang L. Relationship Between Cerebral Hemodynamics, Tissue Oxygen Saturation, and Delirium in Patients With Septic Shock: A Pilot Observational Cohort Study. Front Med. 2021;8:641104. [CrossRef]
- Mei J, Zhang X, Sun X, Hu L, Song Y. Optimizing the prediction of sepsis-associated encephalopathy with cerebral circulation time utilizing a nomogram: a pilot study in the intensive care unit. Front Neurol. 2024 Jan 11;14:1303075. [CrossRef]
- Pierrakos C, Attou R, Decorte L, Kolyviras A, Malinverni S, Gottignies P, et al. Transcranial Doppler to assess sepsis-associated encephalopathy in critically ill patients. BMC Anesthesiol. 2014;14:45. [CrossRef]
- Pierrakos C, Attou R, Decorte L, Velissaris D, Cudia A, Gottignies P, et al. Cerebral perfusion alterations and cognitive decline in critically ill sepsis survivors. Acta Clin Belg. 2017 Feb;72(1):39–44. [CrossRef]
- de Riva N, Budohoski KP, Smielewski P, Kasprowicz M, Zweifel C, Steiner LA, et al. Transcranial Doppler pulsatility index: what it is and what it isn’t. Neurocrit Care. 2012 Aug;17(1):58–66. [CrossRef]
- de Azevedo DS, Salinet ASM, de Lima Oliveira M, Teixeira MJ, Bor-Seng-Shu E, de Carvalho Nogueira R. Cerebral hemodynamics in sepsis assessed by transcranial Doppler: a systematic review and meta-analysis. J Clin Monit Comput. 2017 Dec;31(6):1123–32. [CrossRef]
- Thees C, Kaiser M, Scholz M, Semmler A, Heneka MT, Baumgarten G, et al. Cerebral haemodynamics and carbon dioxide reactivity during sepsis syndrome. Crit Care Lond Engl. 2007;11(6):R123. [CrossRef]
- Pfister D, Siegemund M, Dell-Kuster S, Smielewski P, Rüegg S, Strebel SP, et al. Cerebral perfusion in sepsis-associated delirium. Crit Care Lond Engl. 2008;12(3):R63. [CrossRef]
- Toksvang LN, Plovsing RR, Petersen MW, Møller K, Berg RMG. Poor agreement between transcranial Doppler and near-infrared spectroscopy-based estimates of cerebral blood flow changes in sepsis. Clin Physiol Funct Imaging. 2014 Sep;34(5):405–9. [CrossRef]
- Crippa IA, Subirà C, Vincent JL, Fernandez RF, Hernandez SC, Cavicchi FZ, et al. Impaired cerebral autoregulation is associated with brain dysfunction in patients with sepsis. Crit Care Lond Engl. 2018 Dec 4;22(1):327. [CrossRef]
- Crippa IA, Alvaro Quispe Cornejo A, Taccone FS. Changes in Arterial Carbon Dioxide Partial Pressure Do Not Affect Cerebral Autoregulation in Septic Patients. Neurocrit Care. 2022 Oct;37(2):572–4. [CrossRef]
- Caldas J, Quispe-Cornejo AA, Crippa IA, Subira C, Creteur J, Panerai R, et al. Cerebral Autoregulation Indices Are Not Interchangeable in Patients With Sepsis. Front Neurol. 2022;13:760293. [CrossRef]
- Matta BF, Stow PJ. Sepsis-induced vasoparalysis does not involve the cerebral vasculature: indirect evidence from autoregulation and carbon dioxide reactivity studies. Br J Anaesth. 1996;76(6):790–4. [CrossRef]
- Taccone FS, Castanares-Zapatero D, Peres-Bota D, Vincent JL, Berre’ J, Melot C. Cerebral autoregulation is influenced by carbon dioxide levels in patients with septic shock. Neurocrit Care. 2010 Feb;12(1):35–42. [CrossRef]
- Steiner LA, Pfister D, Strebel SP, Radolovich D, Smielewski P, Czosnyka M. Near-infrared spectroscopy can monitor dynamic cerebral autoregulation in adults. Neurocrit Care. 2009;10(1):122–8. [CrossRef]
- Schramm P, Klein KU, Falkenberg L, Berres M, Closhen D, Werhahn KJ, et al. Impaired cerebrovascular autoregulation in patients with severe sepsis and sepsis-associated delirium. Crit Care Lond Engl. 2012 Oct 4;16(5):R181. [CrossRef]
- Terborg C, Schummer W, Albrecht M, Reinhart K, Weiller C, Röther J. Dysfunction of vasomotor reactivity in severe sepsis and septic shock. Intensive Care Med. 2001 Jul;27(7):1231–4. [CrossRef]
- Bowie RA, O’Connor PJ, Mahajan RP. Cerebrovascular reactivity to carbon dioxide in sepsis syndrome. Anaesthesia. 2003 Mar;58(3):261–5. [CrossRef]
- de Goede AA, Loef BG, Reidinga AC, Schaafsma A. Fluid Resuscitation in Septic Patients Improves Systolic but not Diastolic Middle Cerebral Artery Flow Velocity. Ultrasound Med Biol. 2017 Nov;43(11):2591–600. [CrossRef]
- Pfister D, Schmidt B, Smielewski P, Siegemund M, Strebel SP, Rüegg S, et al. Intracranial pressure in patients with sepsis. Acta Neurochir Suppl. 2008;102:71–5. [CrossRef]
- Czosnyka M, Matta BF, Smielewski P, Kirkpatrick PJ, Pickard JD. Cerebral perfusion pressure in head-injured patients: a noninvasive assessment using transcranial Doppler ultrasonography. J Neurosurg. 1998 May;88(5):802–8. [CrossRef]
- Crippa IA, Vincent JL, Zama Cavicchi F, Pozzebon S, Gaspard N, Maenhout C, et al. Estimated Cerebral Perfusion Pressure and Intracranial Pressure in Septic Patients. Neurocrit Care. 2023 Jul 7; [CrossRef]
- Czempik PF, Gąsiorek J, Bąk A, Krzych ŁJ. Ultrasonic Assessment of Optic Nerve Sheath Diameter in Patients at Risk of Sepsis-Associated Brain Dysfunction: A Preliminary Report. Int J Environ Res Public Health. 2020 May 22;17(10):3656. [CrossRef]
- Wood MD, Boyd JG, Wood N, Frank J, Girard TD, Ross-White A, et al. The Use of Near-Infrared Spectroscopy and/or Transcranial Doppler as Non-Invasive Markers of Cerebral Perfusion in Adult Sepsis Patients With Delirium: A Systematic Review. J Intensive Care Med. 2022 Mar;37(3):408–22. [CrossRef]
- Longhitano Y, Iannuzzi F, Bonatti G, Zanza C, Messina A, Godoy D, et al. Cerebral Autoregulation in Non-Brain Injured Patients: A Systematic Review. Front Neurol. 2021 Nov 16;12:732176. [CrossRef]
- Fan TH, Premraj L, Roberts J, Lydston M, Robba C, Hager D, et al. In-Hospital Neurologic Complications, Neuromonitoring, and Long-Term Neurologic Outcomes in Patients With Sepsis: A Systematic Review and Meta-Analysis. Crit Care Med. 2024 Mar;52(3):452–63. [CrossRef]
- Bone RC, Fisher CJ, Clemmer TP, Slotman GJ, Metz CA, Balk RA. Sepsis syndrome: a valid clinical entity. Methylprednisolone Severe Sepsis Study Group. Crit Care Med. 1989 May;17(5):389–93. [PubMed]
- Bone RC, Balk RA, Cerra FB, Dellinger RP, Fein AM, Knaus WA, et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest. 1992 Jun;101(6):1644–55. [CrossRef]
- Levy MM, Fink MP, Marshall JC, Abraham E, Angus D, Cook D, et al. 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Intensive Care Med. 2003 Apr;29(4):530–8. [CrossRef]
- Calandra T, Cohen J, International Sepsis Forum Definition of Infection in the ICU Consensus Conference. The international sepsis forum consensus conference on definitions of infection in the intensive care unit. Crit Care Med. 2005 Jul;33(7):1538–48. [CrossRef]
- Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016 Feb 23;315(8):801–10. [CrossRef]
- Kostoglou K, Bello-Robles F, Brassard P, Chacon M, Claassen JA, Czosnyka M, et al. Time-domain methods for quantifying dynamic cerebral blood flow autoregulation: Review and recommendations. A white paper from the Cerebrovascular Research Network (CARNet). J Cereb Blood Flow Metab Off J Int Soc Cereb Blood Flow Metab. 2024 Apr 30;271678X241249276. [CrossRef]
- Liu X, Czosnyka M, Donnelly J, Cardim D, Cabeleira M, Lalou DA, et al. Assessment of cerebral autoregulation indices – a modelling perspective. Sci Rep. 2020 Jun 15;10(1):9600. [CrossRef]
- Caldas J, Rynkowski CB, Robba C. POCUS, how can we include the brain? An overview. J Anesth Analg Crit Care. 2022 Dec 27;2(1):55. [CrossRef]
- Alonso JV, Turpie J, Farhad I, Ruffino G. Protocols for Point-of-Care-Ultrasound (POCUS) in a Patient with Sepsis; An Algorithmic Approach. Bull Emerg Trauma. 2019 Jan;7(1):67–71.
- Perera P, Mailhot T, Riley D, Mandavia D. The RUSH exam: Rapid Ultrasound in SHock in the evaluation of the critically lll. Emerg Med Clin North Am. 2010 Feb;28(1):29–56, vii. [CrossRef]
- Sweeney DA, Wiley BM. Integrated Multiorgan Bedside Ultrasound for the Diagnosis and Management of Sepsis and Septic Shock. Semin Respir Crit Care Med. 2021 Oct;42(5):641–9. [CrossRef]
- Corradi F, Via G, Tavazzi G. What’s new in ultrasound-based assessment of organ perfusion in the critically ill: expanding the bedside clinical monitoring window for hypoperfusion in shock. Intensive Care Med. 2020 Apr;46(4):775–9. [CrossRef]
- Noitz M, Szasz J, Dünser MW. Regional perfusion monitoring in shock. Curr Opin Crit Care. 2020 Jun;26(3):281–8. [CrossRef]
- Corradi F, Brusasco C, Via G, Tavazzi G, Forfori F. Renal Doppler-Based Assessment of Regional Organ Perfusion in the Critically Ill Patient. Shock Augusta Ga. 2021 Jun 1;55(6):842–3. [CrossRef]
- Tas J, Beqiri E, van Kaam CR, Ercole A, Bellen G, Bruyninckx D, et al. An Update on the COGiTATE Phase II Study: Feasibility and Safety of Targeting an Optimal Cerebral Perfusion Pressure as a Patient-Tailored Therapy in Severe Traumatic Brain Injury. Acta Neurochir Suppl. 2021;131:143–7. [CrossRef]
- Tamagnone FM, Cheong I, Luna E, Previgliano I, Otero Castro V. Ultrasound-guided cerebral resuscitation in patients with severe traumatic brain Injury. J Clin Monit Comput. 2023 Apr;37(2):359–63. [CrossRef]
- Aries MJH, Czosnyka M, Budohoski KP, Steiner LA, Lavinio A, Kolias AG, et al. Continuous determination of optimal cerebral perfusion pressure in traumatic brain injury. Crit Care Med. 2012 Aug;40(8):2456–63. [CrossRef]
- Bögli SY, Cucciolini G, Cherchi MS, Motroni V, Olakorede I, O’Leary R, et al. Feasibility and Safety of Integrating Extended TCD Assessments in a Full Multimodal Neuromonitoring Protocol After Traumatic Brain Injury. Ultrasound Med Biol. 2024 Aug;S0301562924002710. [CrossRef]
- Rasulo FA, Togni T, Romagnoli S. Essential Noninvasive Multimodality Neuromonitoring for the Critically Ill Patient. Crit Care Lond Engl. 2020 Mar 24;24(1):100. [CrossRef]
Figure 1.
Quorum Flowchart for articles selection.
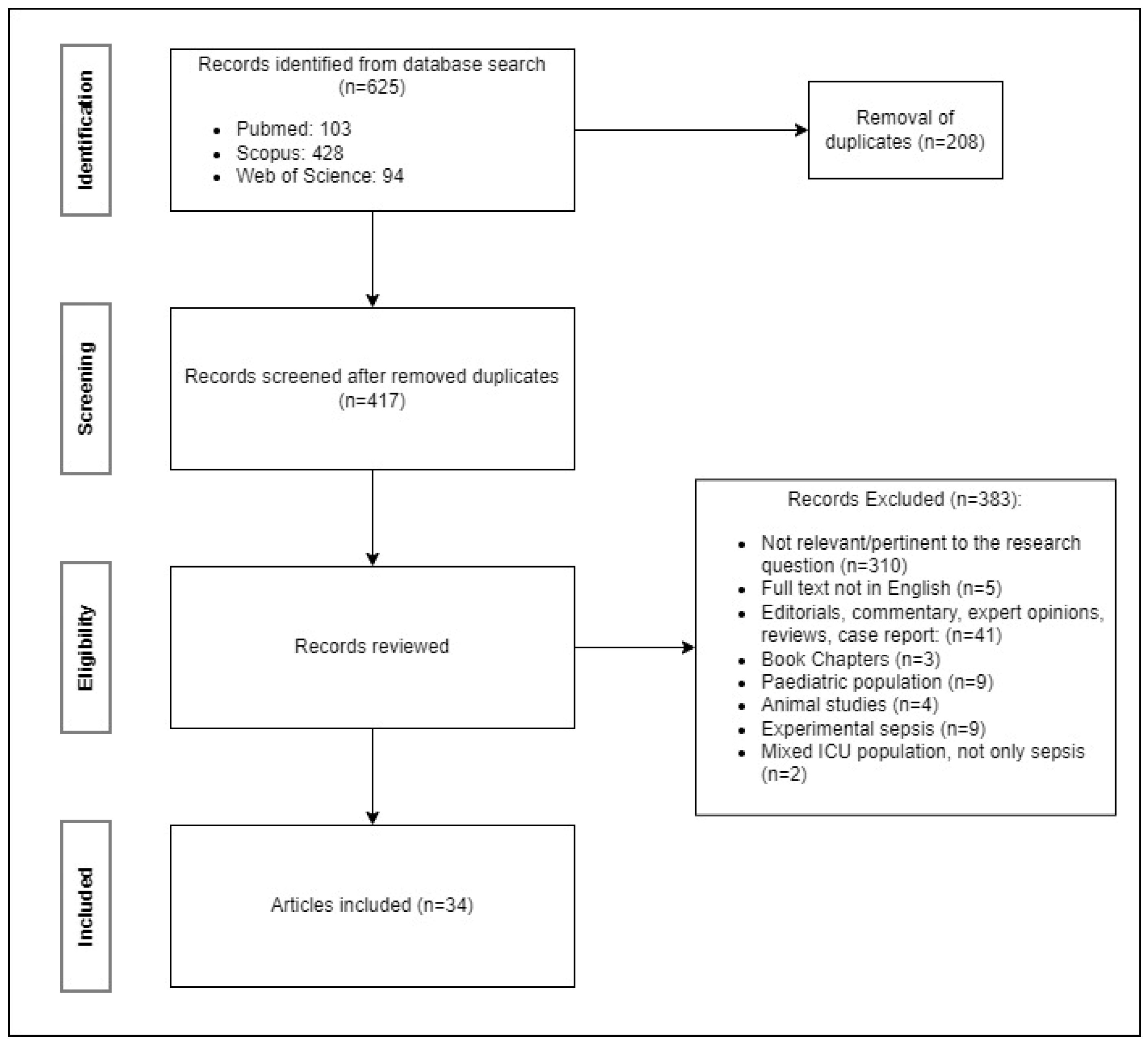
Figure 2.
Type of evidences included for the review. For each type of article is shown the total number and percentage.
Figure 2.
Type of evidences included for the review. For each type of article is shown the total number and percentage.
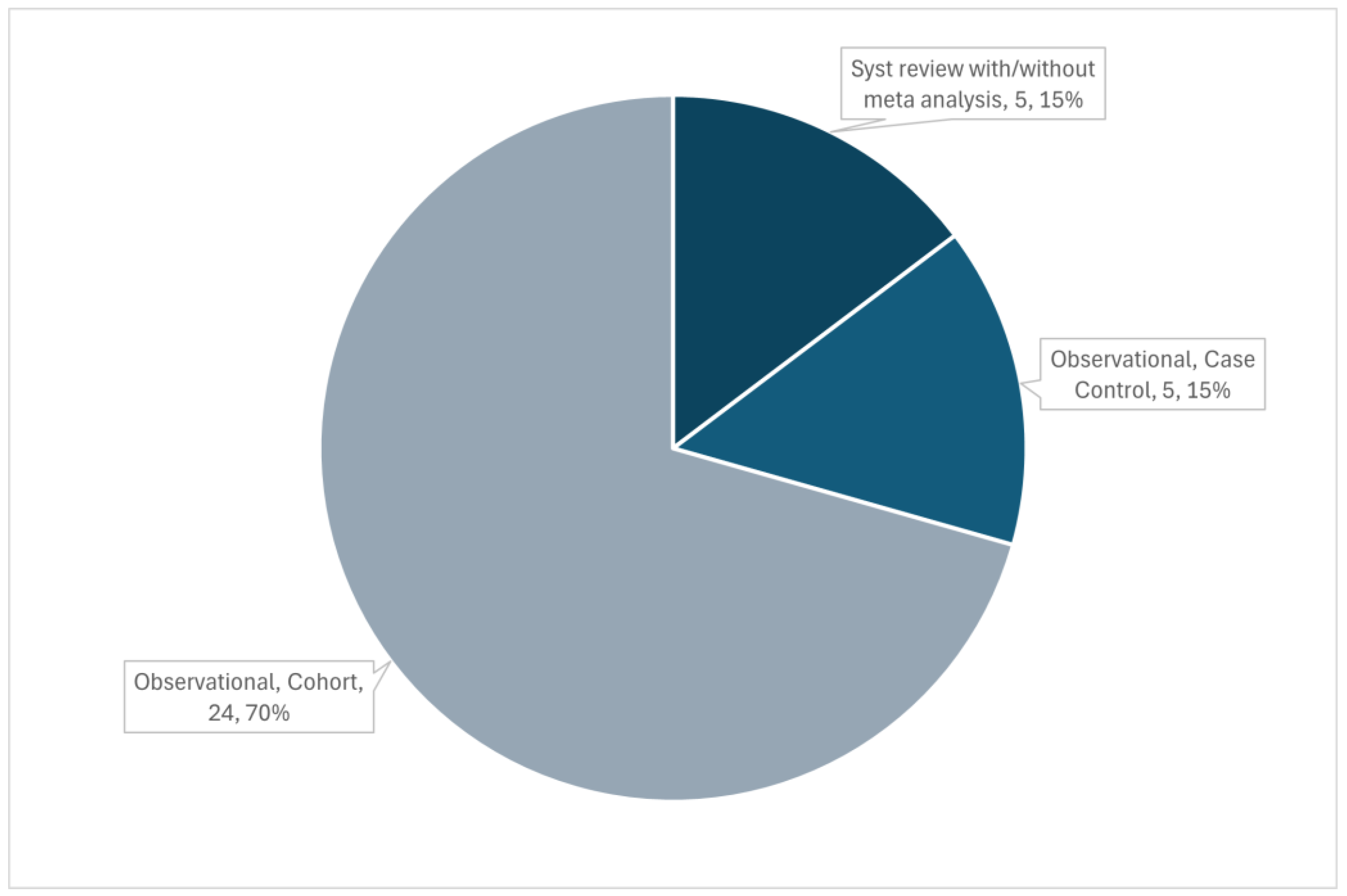
Table 3.
Summary of findings for studies regarding CO2 reactivity and and acetazolamide test. CO2R: CO2 reactivity. NCR: normalised CO2 reactivity. CAR: cerebral autoregulation. CRC cerebrovascular reserve capacity.
Table 3.
Summary of findings for studies regarding CO2 reactivity and and acetazolamide test. CO2R: CO2 reactivity. NCR: normalised CO2 reactivity. CAR: cerebral autoregulation. CRC cerebrovascular reserve capacity.
| Study | Main findings | Metric used | Sample size (septic patients) |
|---|---|---|---|
| Matta and Stow 1996 [35] | CO2R was within normal limits for all patients. | CO2R | 10 |
| Terborg 2001 [39] | During septic shock NCR was significantly reduced. | NCR | 8 |
| Bowie 2003 [40] | CO2R was abnormal in 10/12 patients. This was not related to mortality or other clinical parameters. | CO2R | 12 |
| Thees 2007 [29] | CO2R was not impaired. However, the survivors showed a pathologic neurological examination. | CO2R | 10 |
| Berg and Plovsing 2016 [21] | CO2R is preserved in sepsis. Short term hyperventilation does not necessarily enhance CAR. | Phase, gain, coherence | 16 (only 7 underwent hyperventilation) |
| Szatmàri 2010 [17] | Vasomotor response was slower and lower in sepsis (less CRC and lower systolic MCAv). | Acetazolamide tes, CVR, CRC | 14 |
| Fülesdi 2012 [18] | CRC was similar in the two groups while CVR decreased slower in the septic group (more prolonged vasodilatory response). | Acetazolamide tes, CVR, CRC | 16 |
Table 4.
Summary of results of studies regarding non invasive ICP (nICP) and estimated cerebral perfusion pressure (eCPP). THRT: transient hyperemia response test.
Table 4.
Summary of results of studies regarding non invasive ICP (nICP) and estimated cerebral perfusion pressure (eCPP). THRT: transient hyperemia response test.
| Study | Main findings | Metric used | Sample size (septic patients) |
|---|---|---|---|
| Pfister 2008 [42] | 47% of patients showed nICP>15 mmHg in at least one day. nICP increases were moderate and never exceeded 20 mmHg. nICP was strongly correlated with MAP but did not differ between survivors and non-survivors. 73% of patients had eCPP<60 mmHg (20% falling <50 mmHg). Low eCPP was associated with high S-100β levels. There was no link between nICP and fluid administration. | nICP, eCPP | 16 |
| Crippa 2022 [33] | 53% of patients had impaired CAR, 55% had low eCPP, and 38% had high nICP. Low eCPP and high nICP was seen in 35% of patients. Pupillary dilation velocity was significantly lower in those with impaired CAR. Patients with low eCPP or high nICP had lower Neurological Pupil index (NPi) values. | THRT, nICP, eCPP | 40 |
| Crippa 2023 [44] | The median eCPP was 63 mmHg, with 33% having low eCPP. The median nICP was 8 mmHg, with 4% having high nICP. Most patients (65%) had normal eCPP and nICP. 31% had low eCPP with normal nICP. 2% had low eCPP and high nICP. 2% had normal eCPP and high nICP. There were no significant differences in SAE occurrence or in-hospital mortality between patients with altered eCPP or nICP compared to those with normal values. |
eCPP, nICP, Mxa. | 132 |
Table 5.
Summary of studies for neurologic outcome prediction. CAR: cerebral autoregulation. CBFi: cerebral blood flow index. CCT: cerebral circulation time. CD: cognitive decline. CRP: C reactive protein. eCPP: estimated cerebral perfusion pressure. nICP: non invasive intracranial pressure. MCAv: middle cerebral artery velocities. Mx: mean flow index. ONSD: optic nerve sheet diameter. PI: pulsatility index. SAD: sepsis associated delirium.
Table 5.
Summary of studies for neurologic outcome prediction. CAR: cerebral autoregulation. CBFi: cerebral blood flow index. CCT: cerebral circulation time. CD: cognitive decline. CRP: C reactive protein. eCPP: estimated cerebral perfusion pressure. nICP: non invasive intracranial pressure. MCAv: middle cerebral artery velocities. Mx: mean flow index. ONSD: optic nerve sheet diameter. PI: pulsatility index. SAD: sepsis associated delirium.
| Study | Main findings | Metric used | Sample size (septic patients) |
|---|---|---|---|
|
Pfister 2008 [42] |
No significant correlations between nICP, daily change in nICP or relative change in nICP and overall or daily fluid administration or balance. | MCAv, nICP, eCPP | 16 |
|
Pfister 2008 [30] |
Mx was altered in SAD patients. No differences in CBF between the SAD and non-SAD group. | MCAv, Mx | 16 |
|
Schramm 2012 [38] |
25 patients (88%) showed impaired CAR during the four days with a decreasing prevalence during days (day1 - 60%, day2 - 59%, day3 - 41%, day4 - 46%). Delirium developed in 76% of patients. The status of CAR at day 1 was related to development of delirium at day 4. | Mx | 30 |
|
Pierrakos 2014 [25] |
Twenty-one patients (55%) presented delirium (positive CAM-ICU test). ROC curve analysis showing only PI on the first day and not the third day was a good predictor of the presence of confusion (AUC = 0.908, 95%, CI 0.80-0.98, p < 0.01). PI was related to confusion independently from age or APACHE II score. | MCAv, PI, CBFi | 40 |
|
Pierrakos 2017 [26] |
Fourteen patients (50%) presented CD at the time of discharge. Only on the first day of the study PI was higher in patients with CD (2.2 ± 0.7 vs. 1.4 ± 0.5, p = 0.02) and CBFi was lower (363 ± 170 vs. 499 ± 133, p = 0.03). In univariate analysis, delirium and PI on the first day were related to CD (OR: 36.1, 95%CI 4.3–299.1, p = 0.01, OR:4.1, 95%CI 1.1–15.2, p = 0.03), but in the multivariate analysis PI was not found to be related to CD independently of the presence of delirium. | MCAv. PI, CBFi | 28 |
|
Crippa 2018 [32] |
There was no difference in Mxa between survivors and non-survivors at ICU discharge. SAE was more common in patients with altered CAR than in those with intact CAR (34 of 50 [68%] vs 23 of 50 [46%]; p = 0.04), and Mxa was higher in patients with SAE (0.47 [0.21–0.64] vs 0.23 [- 0.12–0.52]; p <0.01). In multivariable analysis, higher Mxa, vascular disease and mechanical ventilation were independent predictors of SAE. The best Mxa cut-off to predict SAE was 0.18 (sensitivity 79%, specificity 47%). | Mxa | 100 |
|
Czempik 2020 [45] |
49/80 ONSD measurements exceeded 5.7 mm. No correlations between ONSDs and CRP concentrations, highest daily lactate, or SOFA. ONSD measurement should be applied for screening of SAE cautiously. | ONSD | 10 |
| Feng 2021 [23] | The logistic regression analysis demonstrated that several independent risks were SAD predictors: rSO2 <55% [OR=3.864, 95% CI: 1.026-14.550, p=0.046] and the THRR index<1.09 [OR=5.77, 95% CI: 1.222–27.255, p=0.027]. Patients with SAD have a close correlation with poor outcomes. | MCAv, CBFi, PI, THRR | 51 |
|
Crippa 2023 [44] |
SAE occurrence and mortality did not differ between patients with low and normal eCPP or between patients with high and normal nICP. | eCPP, nICP, Mxa | 132 |
| Mei 2024 [24] | The SAE group displayed significantly elevated levels of NSE, S100β, PI, RI, and CCT, while EDV was lower (all P-values < 0.05). CCT emerged as the most efficacious predictor for SAE, with an AUC of 0.846. S100β, PI, and CCT were identified as independent predictors for SAE. | MCAv, PSV, EDV, PI, RI, CCT | 67 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



