
Submitted:
04 September 2024
Posted:
06 September 2024
You are already at the latest version
Abstract
Background/Objectives: interpretation of evidence on de-escalation of triple therapy with with-drawal of inhaled corticosteroids (ICS) to dual bronchodilator therapy with a long-acting musca-rinic antagonist (LAMA) and a long-acting beta-agonist (LABA) in patients with chronic obstruc-tive pulmonary disease (COPD) is conflicting. We evaluated the efficacy and safety of ICS discon-tinuation from LABA-LAMA-ICS triple therapy compared to its continuation. Methods: we searched PubMed, Embase, Scopus, Web Of Science, clinicaltrial.gov and CENTRAL for RCTs and observational studies from inception to March 22, 2024, investigating the effect of triple therapy de-escalation with withdrawal of ICS to dual therapy on the risk of COPD exacerbation, pneumonia and lung function. This study was registered with PROSPERO, CRD42024527942. Results: 3335 studies were screened; three RCTs and three real-world non-interventional studies were ultimately identified as eligible. Analysis of the time to the first moderate or severe exacerbation showed a pooled HR of 0.96 (95% CI, 0.80 to 1.15; I²=77%) for ICS withdrawal compared with triple therapy continuation. Analysis according eosinophil levels showed that COPD subjects with ≥300 eosino-phils/µL had a significant increase in the incidence of moderate or severe exacerbations when de-escalated from ICS/LABA/LAMA to LABA/LAMA (pooled HR: 1.35, 95% CI 1.00-1.82; I2: 56%). The ICS withdrawal in favour of LABA/LAMA did not significantly affect the risk of mortality and pneumonia. Conclusions: the main findings of this meta-analysis are consistent with current recommendations and suggest that the use of eosinophil counts may be of help in guiding maintenance therapy. However, methodological heterogeneity between the included studies is evident.
Keywords:
Chronic Obstructive Pulmonary Disease (COPD)
; inhaled corticosteroids (ICS)
; de-escalation therapy
; Acute Exacerbation of COPD (AECOPD)
; pneumonia
; eosinophils
1. Introduction
Chronic Obstructive Pulmonary Disease (COPD) is a progressive respiratory disease characterized by airflow limitation and persistent respiratory symptoms[1]. According to the most important consensus documents[1], the management of stable COPD mainly consists of the use of inhaled medications which have been shown to relieve symptoms, reduce exacerbations and improve the quality of life[2]. One of the leading treatment strategies is the concept of triple therapy, which combines an inhaled corticosteroid (ICS), a long-acting muscarinic antagonist (LAMA), and a long-acting beta-agonist (LABA). Triple therapy is currently indicated for maintenance treatment in patients experiencing frequent exacerbations and in patients with a significant symptomatic burden despite dual bronchodilator therapy [1,2]. Randomized clinical trials have shown that triple therapy can improve lung function, quality of life and reduce exacerbations compared to dual therapy [3,4,5,6].
Despite the widely accepted role of triple therapy, concerns have been raised about the safety of long-term ICS use, such as the potential risk of adverse events, particularly pneumonia. A systematic review and meta-analysis of three RCTs found a higher incidence of pneumonia in those who were randomized to triple therapy compared with the LABA/LAMA group (Risk ratio: 1.53; 95% confidence interval (CI) 1.25-1.87; I2=19.7%) [7]. Conversely, another meta-analysis by Calzetta et al. [8] indicated that ICS discontinuation may result in an increased risk of severe exacerbations, impairment of lung function, and worsened quality of life, although the impact may not be clinically significant [8].
The current indication for ICS withdrawal from triple therapy to LABA-LAMA is limited to COPD patients with no history of exacerbations in the past year, and the recommendation had only moderate certainty of evidence [2]. Many authors question the rationale for changing a therapy that provides significant patient benefit: there is a considerable lack of evidence on the effects of de-escalating from triple therapy to LABA/LAMA, and the available data paint an unclear picture. One of the main issues leading to the tapering of ICS and the step-down to LABA/LAMA may be the need to balance the benefits of inhaled steroids against their potential risks, particularly pneumonia. Interestingly, evidence from “real-world” studies suggests that dual bronchodilator therapy is as effective as triple therapy for many patients, particularly those without a history of frequent exacerbations, but with a better safety profile [9,10].
In summary, given the conflicting evidence and the availability of different treatment combinations, the main goal of this systematic review and meta-analysis is to analyze the evidence from clinical trials that have investigated the efficacy and safety of the de-escalation strategy discontinuing ICS compared to the continuation of LABA/LAMA/ICS in subjects with COPD.
2. Materials and Methods
2.1. Search Strategy and Selection Criteria
The inclusion criteria for this systematic review with meta-analysis were limited to studies that met all of the following eligibility criteria: 1) RCTs or observational studies that enrolled adults aged ≥ 40 years with a diagnosis of COPD; 2) those comparing ICS withdrawal from triple therapy with LABA/LAMA regimen versus the continuation of LABA/LAMA/ICS; 3) follow-up period of at least of six months; and 4) those reporting any of the outcomes of interest. We excluded studies that met at least one of the following exclusion criteria: 1) no control group; 2) overlapping study population. We systematically searched MEDLINE (via PubMed), Embase, Scopus, Web Of Science and Cochrane Central Register of Controlled Trials (CENTRAL) for eligible studies from inception to 22 March 2024. The search term strategy included a combination of synonyms of “COPD”, “glucocorticoid”, “inhaled” and “withdrawal”. The complete electronic search strategy is reported in the Supplementary appendix 1. Only publications in English were considered. E.P. and D.D.R. independently reviewed each title and abstract for potential eligibility. Disagreements were resolved by consensus among the three authors. Finally, we report the results of the search strategy according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement guidelines [11].
For the purpose of this meta-analysis, we extracted and evaluated data for the following: 1) moderate or severe COPD exacerbation; 2) change from baseline in forced espiratory volume in the first second (FEV1) recorded anytime and the “trough FEV1” (i.e. the FEV1 measurement before the next inhalation of study drug and ~24 h after the last inhalation was evaluated); 3) incidence of pneumonia; 4) incidence of all-cause mortality. A detailed definition of the outcomes of interest is provided in the Supplementary appendix 2. Additionally, we evaluated the effects of the de-escalation strategy compared to the continuation of LABA/LAMA/ICS in specific subgroups of COPD patients. Specifically, we performed subgroup analyses according to different blood eosinophil thresholds: 1) <2%; 2) ≥2%; 3) <150 cells/µL; 4) ≥150 cells/µL and <300 cells/µL; 5) ≥300 cells/µL.
2.2. Data Analysis
E.P. and D.D.R. independently extracted baseline data for the studies included in the meta-analysis. Summary estimates for binary outcomes were reported as pooled hazard ratio (HR) or rate-ratio (RR) with 95% of confidence intervals for time-to-event and event-rate data, respectively. For pooled continuous data, we reported the treatment effect as the mean difference. Dichotomous outcomes were reported as risk ratios with 95% confidence intervals. All analyses were performed using the random-effects model and heterogeneity was tested using the Cochran Q test and I2 statistics. RevMan Web (Nordic Cochrane centre, The Cochrane collaboration, Copenhagen, Denmark) was used for statistical analysis. The quality assessment of RCT was evaluated using “The Cochrane tool for assessing risk of bias in randomised trials” (RoB2) [12] and for non-randomised trials we used the “Risk Of Bias In Non-randomised Studies - of Interventions” (ROBINS-I) [13]. To evaluate the robustness and conclusiveness of the findings, sensitivity analyses using the jackknife method were conducted using R 4.4.0 (Foundation for Statistical Computing, Vienna, Austria). This involved systematically excluding individual studies and recalculating the meta-analysis using the remaining pooled estimates. By iteratively omitting each study and re-evaluating the pooled estimates, we aimed to determine if any single study disproportionately influenced the overall results [14]. This systematic review and meta-analysis was registered on PROSPERO, CRD42024527942. There was no funding source for this study.
3. Results
Our literature search initially yielded 3335 results. We subsequently excluded 3317 records after removing duplicates (n: 756) and after the title/abstract inspection (n: 2554). A total of 25 articles were fully reviewed (Supplementary appendix 3). Ultimately, the results were extracted from three RCTs [15,16,17,18] and three “real-world” non-interventional studies [19,20,21]. Two separate reports from “Withdrawal of Inhaled Steroids during Optimized Bronchodilator Management” (WISDOM) trial were included in our meta-analysis: Magnussen et Al[15] reporting on the full study population and Watz et Al[16] presenting a post-hoc subgroup analysis based on eosinophil count. Figure 1 shows the PRISMA flow-diagram of the systematic literature search, study selection and reasons for exclusion.
3.1. Characteristics of the Studies Included in this Meta-Analysis
Table 1 lists the main characteristics of the studies included in this meta-analysis. All participants were at least 40 years of age (mean age 63.8 to 70.8 years) and were current or former smokers. In four studies [15,16,17,18,19], a history of exacerbations in the previous year was required. Given the non-interventional design of the three “real-world” studies [19,20,21], participants continued triple therapy or de-escalated to a LABA/LAMA depending on physician judgment or randomly allocated in the three RCTs [15,16,17,18]. Finally, one study [19] included three different COPD cohorts in the analysis: 1) Cohort 1 that specifically met the inclusion and exclusion criteria of the WISDOM trial [15]; 2) a “real-world” COPD cohort aged 35 or older (Cohort 2); 3) Cohort 3 consisting of COPD patients aged 35 or older that met at least one exclusion criteria of WISDOM trial [15]. The full inclusion and exclusion criteria of WISDOM [15] have been reported elsewhere. According to our pre-defined inclusion criteria, only Cohort 1 was eligible for inclusion in our meta-analysis. All participants received a COPD diagnosis confirmed by spirometry and a post-bronchodilator ratio of FEV1 and FVC <0.7.
3.2. Pooled Analysis of Time to the First Moderate or Severe Exacerbation and Event Rate for ICS Withdrawal Compared with Continuation of Triple Therapy
A pooled analysis of time-to-event data for "moderate or severe acute exacerbations" that included 9,735 participants is showed in Figure 2. The analysis of time to the first moderate or severe exacerbation showed a pooled HR of 0.96 (95% CI, 0.80 to 1.15; I² = 77%) for ICS withdrawal compared with continuation of triple therapy.
A further analysis of the event rate in 6,911 patients yielded an RR of 0.97 with substantial heterogeneity (95% CI, 0.69 to 1.35; I² = 94%; see Figure 3).
Subgroup analysis according to the eosinophil count and including 1,662 participants from two RCTs [16,18] and one observational study [21], showed a significant increase in the incidence of moderate or severe exacerbations among COPD patients with a blood eosinophil counts ≥300 cells/µL who underwent de-escalation from triple therapy to LABA/LAMA (Figure 4). The pooled HR was 1.35 (95% CI 1.00-1.82), with an I2 of 56% indicating moderate heterogeneity. Conversely, the same intervention did not yield a statistically significant difference in exacerbation rates among COPD patients with eosinophil counts <300 cells/μL (pooled HR: 1.05, 95% CI 0.96-1.15; I2: 0%).
Same results emerged from the subgroup analysis according to the percentage of eosinophil count (<2% vs. ≥2%). Data are available in the Supplementary Appendix 4.1.
In COPD patients with low circulating eosinophils, the same intervention did not show a significant difference in exacerbation rates as showed in Figure 5: Eos<150 cell/μL: RR of 1.01 (95% CI 0.80-1.26; I² = 21%); Eos≥150 cell/μL and <300 cell/μL: RR of 1.03 (95% CI 0.84-1.27; I² = 0%); ≥300 cells/µL: RR 1.63 (95%CI 1.24-2.14; I²:0%). The test for subgroup differences between the three absolute eosinophil count thresholds suggests that there is a statistically significant subgroup effect (p interaction=0.01, I2:76.5%), suggesting that COPD patients with an absolute eosinophils count ≥300 cell/μL may have a greater clinical benefit continuing ICS/LABA/LAMA rather than de-escalating to LABA/LAMA.
3.3. Pooled Analysis of FEV1 Variation
Data from two RCTs [15,18] were extracted for the pooled analysis of trough FEV1 variation between the two therapeutic strategies. The analysis showed a statistically significant differences toward the ICS/LABA/LAMA group with a mean difference of 34.7 ml (95% CI 15.84 to 3.57 ml) and low heterogeneity (I2: 0%).
Subgroup analysis according to eosinophil count showed no statistically significant decrease in trough FEV1 for COPD patients with circulating eosinophils (<150 cell/μL: mean difference: -9.36, 95%CI -51.47 to 32.74; I² = 56%; ≥150 cell/μL and <300 cell/μL: mean difference: -42.00, 95%CI -86.35 to 2.35) but a significant reduction for those with circulating eosinophil count ≥300 cells/µL (mean difference: -50.77 ml, 95%CI -91.32 to -10.23; I² = 0%) (data displayed in Figure 6). The test for subgroup differences indicated that there was no statistically significant subgroup effect (p interaction = 0.35).
Similar results were found according to percentage of eosinophil count (<2% vs. >2%). Data are available in the Supplementary appendix 4.2.
For the meta-analysis of change from baseline in FEV1 recorded anytime, data from two observational studies were extracted [19,21]. No significant differences were observed between those who continued triple therapy and those who descaled to LABA/LAMA. Full data are reported in Supplementary appendix 4.3.
3.3. Evaluation of Safety Outcomes: Risk of Pneumonia and All Cause Mortality
For the safety outcomes, we included three studies [15,18,20] for “all-cause mortality” and four studies [15,18,20,21] for the risk of pneumonia with 4,662 and 9,892 participants, respectively. “All-cause mortality” occurred in 49 patients in the ICS withdrawal group (2.3%) and in 51 patients in the ICS/LABA/LAMA group (2%). Compared to ICS withdrawal, ICS/LABA/LAMA showed no increase in the risk of “all-cause mortality” (pooled risk ratio: 1.05, 95%CI 0.71-1.56; I2: 0%; Figure 7A) with low heterogeneity among studies (I²: 0%). Pneumonia occurred in 102 patients in the ICS withdrawal group (3.2%) and in 214 patients in the ICS/LABA/LAMA group (3.1%). Withdrawal of ICS in favour of LABA/LAMA did not significantly affect the risk pneumonia (pooled risk ratio: 0.88, 95%CI 0.69-1.12; I2: 0%; Figure 7B).
3.4. Sensitivity Analyses and Risk of Bias Assessment
The jackknife sensitivity analysis showed that one study excessively affected the pooled estimates by introducing heterogeneity into the meta-analysis. Specifically, by omitting the “Outpatient care with long-acting bronchodilators: COPD register in Germany” (DACCORD) study [20], we observed a trend toward the reduction of exacerbation rates in COPD patients who discontinued ICS compared to those who continued triple therapy, although this did not reach statistical significance (pooled HR: 1.05, 95% CI 0.97- 1.14; I2: 0% vs I2: 77%; pooled RR: 1.18, 95% CI 0.93-1.50; I2: 88% vs I2: 94%). Finally, the pooled estimate remained consistent for all-cause mortality and pneumonia rates when the meta-analysis was repeated by omitting one study at a time, indicating the robustness of our results (see full analysis in Supplementary Appendix 5).
4. Discussion
In the current meta-analysis, we systematically evaluated the efficacy and safety of de-escalation with ICS withdrawal from ICS/LABA/LAMA to LABA/LAMA compared to continuation of triple therapy. The main findings of our meta-analysis are that no significant increase in moderate or severe exacerbations may be attributed to ICS withdrawal, whilst critical evidence emerges upon examining patients with different eosinophil thresholds. Specifically, those with ≥300 eosinophil/µL or greater than 2% experienced a significant increase in exacerbations and a greater decline in lung function when de-escalating from ICS/LABA/LAMA to LABA/LAMA, suggesting that ICS should be continued in this subgroup. Moreover, no significant differences were observed in our safety outcome analysis, including data on all-cause mortality and pneumonia risk.
We found only one meta-analysis similar to this one in a systematic review of the literature [22]. Our paper extends the quantitative analysis by Koarai et al. [22] and is, to our knowledge, the first comprehensive analysis attempting to summarize the existing evidence on the de-escalation strategy from ICS/LABA/LAMA to LABA/LAMA in the treatment of stable COPD, including a subgroup analysis according to the eosinophil count. While individual studies have previously investigated de-escalation therapy in COPD, a comprehensive synthesis of findings from randomized controlled trials and real-world studies was absent.
It should be emphasized that despite the importance of the clinical problem addressed in this meta-analysis and the very large number of patients potentially involved, our literature search found a limited number of studies and a significant methodological heterogeneity among them, encompassing variations in study design, patient populations and ICS withdrawal protocols. Patients' current smoking status is a significant factor in COPD prognosis and treatment response [23]. However, across the included studies, data on this variable were highly heterogeneous. For instance, in the WISDOM trial [15,16], 66.6% of the total sample were current smokers, whereas in the DACCORD trial [20] a small percentage had no smoking history. A notable degree of heterogeneity was evident in the duration of triple therapy prior to enrollment across the studies considered. Participants had been on triple therapy before baseline for at least three months in four studies [17,18,19,20], six weeks in the WISDOM trial [15,16]. In one “real-world” study [21], patients were included irrespective of their time on triple therapy but reported a small percentage of participants that had generically been on ICS/LABA/LAMA for less than 12 months. In addition, the studies considered as "triple therapy" both when ICS, LABA and LAMA were administered in a single inhaler and in separate inhalers, nevertheless, this issue has been reported by several authors as a potential determinant of differential benefits for subjects [24,25].
As enlightened by our jackknife sensitivity analysis, such notable variance in pooled estimates was predominantly attributable to the inclusion of one study characterized by distinct methodological approaches. Regarding the analysis of the exacerbation rates, exclusion from the meta-analysis of the DACCORD trial [20] yielded a substantial change in the pooled estimates. The DACCORD trial was a longitudinal, non-interventional “real-world” study conducted in three different cohorts [20,26]. Only cohort 3 met our inclusion criteria (received triple therapy for ≥ 6 months), and then each patient's physician decided to continue triple therapy or switch to a LABA/LAMA, so the data were included in this meta-analysis and discussed here. Briefly, patients de-escalated to LABA/LAMA had a lower incidence of both moderate and severe exacerbations compared with those in the ICS/LABA/LAMA group (HR: 0.58, 95% CI 0.42-0.79), improved in symptoms (absolute change from baseline in CAT score -2.0 for LABA/LAMA group and -1.0 for ICS/LABA/LAMA group, p=0.003) and had a lower incidence of adverse events. These results from the DACCORD trial [20] differ significantly from the other available evidence and need to be interpreted with caution. First, the “non-interventional” design could significantly contribute to the observed results. Second, the observed differences may be due to the severity of COPD in the patient population treated with ICS/LABA/LAMA. In fact, the mean predicted percentage of FEV1 (57.7%) was lower in the triple therapy group than in the LABA/LAMA group (66.9%), indicative of more severe disease at baseline. This severity is further highlighted by the higher frequency of exacerbations in the 12 months prior to study entry in the ICS/LABA/LAMA group (48.9%) than in the LABA/LAMA cohort (43.5%). Despite the methodological limitations of the non-interventional design, the DACCORD trial probably more closely reflects the “real-world” clinical management of patients with COPD on long-term triple therapy and demonstrates the clinical propensity of physicians to continue triple therapy for patients with unstable disease. This clinical decision-making is logically consistent with a cautious approach to managing patients who are more prone to exacerbations. Consequently, non-frequently exacerbating COPD patients were considered suitable candidates for ICS withdrawal and clinicians were dissuaded from de-escalating treatment in patients with a history of frequent exacerbations prioritizing disease control and prevention of further exacerbations. Of note, there is no mention of whether eosinophil counts had a role in de-escalating to LABA/LAMA or remaining on triple therapy.
Also in consideration of the extensive debate over the past years regarding the role of ICS in COPD [27,28,29,30,31], the analysis of data elaborated in the present meta-analysis suggests several considerations of potential interest for clinicians.
1) the actual relevance of using trough FEV1 as an outcome measure in COPD patients may be questionable. Data from different studies appear to be influenced by the methodology used and, most importantly, no variation reaches the 100 ml target, which is the well-recognized “minimal clinically important difference” (MCID) [32,33]. Therefore, although the assessment of this measure could be of relevance to demonstrate the therapeutic effect, it does not necessarily translate for the patients in a clinical improvement, not leading to a significant improvement in perceived quality of life.
2) In accordance with established protocols, five of the six studies included in our meta-analysis excluded only patients with a “current” diagnosis of asthma, whereas in the “Study to Understand the Safety and Efficacy of ICS Withdrawal from Triple Therapy in COPD” (SUNSET) study [18] subjects with a history of asthma were excluded a priori (see Table 1). The lack of a precise definition of asthma history can result in a wide range of patient profiles, from well-controlled patients with asthma to those with active asthma symptoms. Thus, the difference between protocols that exclude subjects with “current asthma” or with “history of asthma” raises methodological considerations because of the different role covered by ICS therapy in COPD subjects versus those with asthma-COPD overlap (ACO) [34]. Although ICS withdrawal may be feasible in certain asthma phenotypes [35], the possible inclusion of patients with ACO in studies primarily targeting COPD can significantly affect the generalizability of the findings, leading to an overestimation of the benefits of ICS therapy or an underestimate of the risks associated with discontinuation.
3) Our findings provide a small but perhaps significant addition to the debate regarding the long-term safety of ICS in COPD subjects. Previous meta-analyses have found a strong association between ICS use and the risk of pneumonia [7,36]. With the limitations imposed by the paucity of available studies, we found no safety concern for triple therapy versus LABA-LAMA de-escalation. This may be an important issue that needs to be further addressed in the future, especially in more targeted populations, including those with varying disease severity and exacerbation patterns. Our divergent results with the existing literature denote an urgent need for well-powered trials to identify COPD patients in whom the advantages of ICS substantially outweigh the risks.
4) The clinical significance of blood eosinophil levels in COPD is a subject of ongoing debate. Since the 2019 GOLD report [37] to the latest [1], the peripheral blood eosinophil count has been stated as a parameter for guiding or modifying COPD treatment, including the use of ICS-based regimens. As observed in RCTs, in COPD patients not receiving ICS-containing regimens, the likelihood of exacerbation increases with increasing eosinophil blood counts [38,39]. Conversely, in the FLAME study, the correlation between ICS therapeutic response and blood eosinophil level was not significant in COPD patients when comparing ICS/LABA to LABA/LAMA regimens in terms of exacerbation reduction. The LABA/LAMA combination was as effective as ICS/LABA in reducing exacerbation rates, regardless of the baseline eosinophil count (<2% or ≥2%) [40,41]. This is in contrast to the results of our quantitative analysis aggregating the results of the WISDOM and SUNSET trials [16,18], which form the basis of the most recent recommendations. For example, the European Respiratory Society (ERS) indicates a conditional recommendation for the withdrawal of ICS in patients with COPD without a history of frequent exacerbations and a strong recommendation not to withdraw ICS in patients who have a blood eosinophil count ≥ 300 eosinophils/μL, irrespective of the history of exacerbations [42]. Analogously, the American Thoracic Society’s guidelines do not advocate for or against the use of inhaled corticosteroids as an add-on therapy to long-acting bronchodilators for COPD patients with blood eosinophilia, except for those with a history of exacerbations [2]. The absence of a definitive recommendation underscores the need for further research in this area.
This study has several limitations. First, there is significant methodological heterogeneity among the included studies such as protocols of ICS withdrawal (abrupt or stepwise), inclusion of subject with history of asthma and history of exacerbations in the previous 12 months. Second, the non-interventional design of the real-world studies included introduces potential biases that could influence outcomes, such as physician judgment in continuing or withdrawing ICS. Third, the varying duration of triple therapy prior to study enrollment and differences in the administration of ICS, LABA, and LAMA—whether in single or separate inhalers—could contribute to differential benefits observed across studies. Fourth, the varying duration of follow-up ranging from six and 12 months which may have been inadequate to observe the outcomes. These limitations highlight the need for greater methodological consistency in future research to facilitate more reliable comparisons and robust conclusions.
5. Conclusions
A small body of evidence suggests that de-escalation of triple therapy with ICS withdrawal to dual bronchodilator therapy in patients with COPD does not affect the main outcomes (moderate or severe exacerbations, change from baseline to in trough FEV1). COPD patients with high blood eosinophils, namely 2% and ≥300 cells/µL, are most likely to benefit from continuing triple therapy and should not de-escalate to LABA/LAMA, as we found a greater risk of exacerbation and FEV1 decline, although the magnitude of change was far from the MCID threshold of 100 ml. In terms of adverse outcomes, including mortality and the risk of pneumonia, these events do not appear to be affected by ICS withdrawal. This suggests that there is no evidence that long-term use of ICS is unsafe in this category of patients. The results of this meta-analysis support the current approach of consensus documents and ongoing clinical recommendations [1,2,41], which advocate the use of eosinophil counts to guide COPD maintenance therapy to provide a more precise and individualized therapeutic approach, including de-escalation treatments for patients with lower exacerbation risk profiles. Further research toward tailoring the inhaler strategy according to patient characteristics are needed.
Supplementary Materials
The following supporting information can be downloaded at: Preprints.org, Appendix 1: Search and study selection strategy. Appendix 2: Definition of the outcomes of interest in the studies included in the meta-analysis. Appendix 3: List of studies excluded at the full-text screening stage with the reason for exclusion. Appendix 4: Forest plot of additional data from analyzed outcomes. Appendix 5: Jackknife sensitivity analyses. Appendix 6: Risk of bias assessment.
Author Contributions
EP was responsible for conceptualization, development of the study methodology and performed the formal statistical analysis. EP and DDR contributed to the screening process of the literature search. EP, DDR and AT interpreted the data and wrote the first draft of the manuscript. All authors had full access to all data, had final responsibility for the decision to submit for publication and ultimately approved the final draft to be published.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Conflicts of Interest
The authors declare no conflicts of interest.
References
- 2024 GOLD Report Available online: https://goldcopd.org/2024-gold-report/ (accessed on 17 April 2024).
- Nici, L.; Mammen, M.J.; Charbek, E.; Alexander, P.E.; Au, D.H.; Boyd, C.M.; Criner, G.J.; Donaldson, G.C.; Dreher, M.; Fan, V.S.; et al. Pharmacologic Management of Chronic Obstructive Pulmonary Disease. An Official American Thoracic Society Clinical Practice Guideline. Am. J. Respir. Crit. Care. Med. 2020, 201, e56–e69, doi:10.1164/rccm.202003-0625ST. [CrossRef]
- Rabe, K.F.; Martinez, F.J.; Ferguson, G.T.; Wang, C.; Singh, D.; Wedzicha, J.A.; Trivedi, R.; St Rose, E.; Ballal, S.; McLaren, J.; et al. Triple Inhaled Therapy at Two Glucocorticoid Doses in Moderate-to-Very-Severe COPD. N. Engl. J. Med. 2020, 383, 35–48, doi:10.1056/NEJMoa1916046. [CrossRef]
- Lipson, D.A.; Barnhart, F.; Brealey, N.; Brooks, J.; Criner, G.J.; Day, N.C.; Dransfield, M.T.; Halpin, D.M.G.; Han, M.K.; Jones, C.E.; et al. Once-Daily Single-Inhaler Triple versus Dual Therapy in Patients with COPD. N. Engl. J. Med. 2018, 378, 1671–1680, doi:10.1056/NEJMoa1713901. [CrossRef]
- Ferguson, G.T.; Rabe, K.F.; Martinez, F.J.; Fabbri, L.M.; Wang, C.; Ichinose, M.; Bourne, E.; Ballal, S.; Darken, P.; DeAngelis, K.; et al. Triple Therapy with Budesonide/Glycopyrrolate/Formoterol Fumarate with Co-Suspension Delivery Technology versus Dual Therapies in Chronic Obstructive Pulmonary Disease (KRONOS): A Double-Blind, Parallel-Group, Multicentre, Phase 3 Randomised Controlled Trial. Lancet Respir. Med. 2018, 6, 747–758, doi:10.1016/S2213-2600(18)30327-8. [CrossRef]
- Papi, A.; Vestbo, J.; Fabbri, L.; Corradi, M.; Prunier, H.; Cohuet, G.; Guasconi, A.; Montagna, I.; Vezzoli, S.; Petruzzelli, S.; et al. Extrafine Inhaled Triple Therapy versus Dual Bronchodilator Therapy in Chronic Obstructive Pulmonary Disease (TRIBUTE): A Double-Blind, Parallel Group, Randomised Controlled Trial. Lancet. 2018, 391, 1076–1084, doi:10.1016/S0140-6736(18)30206-X. [CrossRef]
- Zheng, Y.; Zhu, J.; Liu, Y.; Lai, W.; Lin, C.; Qiu, K.; Wu, J.; Yao, W. Triple Therapy in the Management of Chronic Obstructive Pulmonary Disease: Systematic Review and Meta-Analysis. BMJ. 2018, 363, k4388, doi:10.1136/bmj.k4388. [CrossRef]
- Calzetta, L.; Matera, M.G.; Braido, F.; Contoli, M.; Corsico, A.; Di Marco, F.; Santus, P.; Scichilone, N.; Cazzola, M.; Rogliani, P. Withdrawal of Inhaled Corticosteroids in COPD: A Meta-Analysis. Pulm. Pharmacol. Ther. 2017, 45, 148–158, doi:10.1016/j.pupt.2017.06.002. [CrossRef]
- Suissa, S.; Dell’Aniello, S.; Ernst, P. Single-Inhaler Triple versus Dual Bronchodilator Therapy in COPD: Real-World Comparative Effectiveness and Safety. Int. J. Chron. Obstruct. Pulmon. Dis. 2022, 17, 1975–1986, doi:10.2147/COPD.S378486. [CrossRef]
- Suissa, S.; Dell’Aniello, S.; Ernst, P. Triple Inhaler versus Dual Bronchodilator Therapy in COPD: Real-World Effectiveness on Mortality. COPD 2022, 19, 1–9, doi:10.1080/15412555.2021.1977789. [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. BMJ 2009, 339, b2535, doi:10.1136/bmj.b2535. [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898, doi:10.1136/bmj.l4898. [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A Tool for Assessing Risk of Bias in Non-Randomised Studies of Interventions. BMJ 2016, 355, i4919, doi:10.1136/bmj.i4919. [CrossRef]
- Miller, R.G. The Jackknife--A Review. Biometrika 1974, 61, 1–15, doi:10.2307/2334280. [CrossRef]
- Magnussen, H.; Disse, B.; Rodriguez-Roisin, R.; Kirsten, A.; Watz, H.; Tetzlaff, K.; Towse, L.; Finnigan, H.; Dahl, R.; Decramer, M.; et al. Withdrawal of Inhaled Glucocorticoids and Exacerbations of COPD. New. Engl. J. Med. 2014, 371, 1285–1294, doi:10.1056/NEJMoa1407154. [CrossRef]
- Watz, H.; Tetzlaff, K.; Wouters, E.F.M.; Kirsten, A.; Magnussen, H.; Rodriguez-Roisin, R.; Vogelmeier, C.; Fabbri, L.M.; Chanez, P.; Dahl, R.; et al. Blood Eosinophil Count and Exacerbations in Severe Chronic Obstructive Pulmonary Disease after Withdrawal of Inhaled Corticosteroids: A Post-Hoc Analysis of the WISDOM Trial. Lancet Respir. Med. 2016, 4, 390–398, doi:10.1016/S2213-2600(16)00100-4. [CrossRef]
- Han, M.; Criner, G.; Dransfield, M.; Halpin, D.; Jones, C.; Kilbride, S.; Lange, P.; Lettis, S.; Lipson, D.; Lomas, D.; et al. The Effect of Inhaled Corticosteroid Withdrawal and Baseline Inhaled Treatment on Exacerbations in the IMPACT Study A Randomized, Double-Blind, Multicenter Clinical Trial. Am. J. Respir. Crit. Care. Med. 2020, 202, 1237–1243, doi:10.1164/rccm.201912-2478OC. [CrossRef]
- Chapman, K.R.; Hurst, J.R.; Frent, S.-M.; Larbig, M.; Fogel, R.; Guerin, T.; Banerji, D.; Patalano, F.; Goyal, P.; Pfister, P.; et al. Long-Term Triple Therapy De-Escalation to Indacaterol/Glycopyrronium in Patients with Chronic Obstructive Pulmonary Disease (SUNSET): A Randomized, Double-Blind, Triple-Dummy Clinical Trial. Am. J. Respir. Crit. Care. Med. 2018, 198, 329–339, doi:10.1164/rccm.201803-0405OC. [CrossRef]
- Whittaker, H.; Wing, K.; Douglas, I.; Kiddle, S.; Quint, J. Inhaled Corticosteroid Withdrawal and Change in Lung Function in Primary Care Patients with Chronic Obstructive Pulmonary Disease in England. Ann. Am. Thorac. Soc. 2022, 19, 1834–1841, doi:10.1513/AnnalsATS.202111-1238OC. [CrossRef]
- Vogelmeier, C.; Worth, H.; Buhl, R.; Criée, C.; Gückel, E.; Kardos, P. Impact of Switching from Triple Therapy to Dual Bronchodilation in COPD: The DACCORD “real World” Study. Respir. Res. 2022, 23, doi:10.1186/s12931-022-02037-2. [CrossRef]
- Magnussen, H.; Lucas, S.; Lapperre, T.; Quint, J.; Dandurand, R.; Roche, N.; Papi, A.; Price, D.; Miravitlles, M.; REG Withdrawal of Inhaled Corticosteroids versus Continuation of Triple Therapy in Patients with COPD in Real Life: Observational Comparative Effectiveness Study. Respir. Res. 2021, 22, doi:10.1186/s12931-021-01615-0. [CrossRef]
- Koarai, A.; Yamada, M.; Ichikawa, T.; Fujino, N.; Kawayama, T.; Sugiura, H. Triple versus LAMA/LABA Combination Therapy for Patients with COPD: A Systematic Review and Meta-Analysis. Respir. Res. 2021, 22, doi:10.1186/s12931-021-01777-x. [CrossRef]
- Bjermer, L.H.; Boucot, I.H.; Vogelmeier, C.F.; Maltais, F.; Jones, P.W.; Tombs, L.; Compton, C.; Lipson, D.A.; Kerwin, E.M. Efficacy and Safety of Umeclidinium/Vilanterol in Current and Former Smokers with COPD: A Prespecified Analysis of The EMAX Trial. Adv. Ther. 2021, 38, 4815–4835, doi:10.1007/s12325-021-01855-y. [CrossRef]
- Cho, E.E.; Gershon, A.S. Single vs Multiple Inhaler Triple Therapy in the COPD Population. CHEST 2022, 162, 947–948, doi:10.1016/j.chest.2022.09.004. [CrossRef]
- Ferguson, G.T.; Brown, N.; Compton, C.; Corbridge, T.C.; Dorais, K.; Fogarty, C.; Harvey, C.; Kaisermann, M.C.; Lipson, D.A.; Martin, N.; et al. Once-Daily Single-Inhaler versus Twice-Daily Multiple-Inhaler Triple Therapy in Patients with COPD: Lung Function and Health Status Results from Two Replicate Randomized Controlled Trials. Respir. Res. 2020, 21, doi:10.1186/s12931-020-01360-w. [CrossRef]
- Buhl, R.; Criée, C.-P.; Kardos, P.; Vogelmeier, C.; Lossi, N.; Mailänder, C.; Worth, H. A Year in the Life of German Patients with COPD: The DACCORD Observational Study. Int. J. Chron. Obstruct. Pulmon. Dis.2016, 11, 1639–1646, doi:10.2147/COPD.S112110. [CrossRef]
- Park, J.; Hong, Y.; Rhee, C.; Choi, H.; Kim, K.; Ha Yoo, K.; Jung, K.; Park, J. The Impact of Inhaled Corticosteroids on the Prognosis of Chronic Obstructive Pulmonary Disease. Int. J. Chron. Obstruct. Pulmon. Dis. 2023, 18, 733–743, doi:10.2147/COPD.S388367. [CrossRef]
- Agusti, A.; Fabbri, L.M.; Singh, D.; Vestbo, J.; Celli, B.; Franssen, F.M.E.; Rabe, K.F.; Papi, A. Inhaled Corticosteroids in COPD: Friend or Foe? Eur. Respir. J. 2018, 52, doi:10.1183/13993003.01219-2018. [CrossRef]
- Chen, D.; Restrepo, M.I.; Fine, M.J.; V. Pugh, M.J.; Anzueto, A.; Metersky, M.L.; Nakashima, B.; Good, C.; Mortensen, E.M. Observational Study of Inhaled Corticosteroids on Outcomes for COPD Patients with Pneumonia. Am. J. Respir. Crit. Care Med. 2011, 184, 312–316, doi:10.1164/rccm.201012-2070OC. [CrossRef]
- Singanayagam, A.; Chalmers, J.D.; Akram, A.R.; Hill, A.T. Impact of Inhaled Corticosteroid Use on Outcome in COPD Patients Admitted with Pneumonia. Eur. Respir. J. 2011, 38, 36–41, doi:10.1183/09031936.00077010. [CrossRef]
- Harries, T.H.; Gilworth, G.; Corrigan, C.J.; Murphy, P.B.; Hart, N.; Thomas, M.; White, P.T. Inhaled Corticosteroids Prescribed for Copd Patients with Mild or Moderate Airflow Limitation: Who Warrants a Trial of Withdrawal? Int. J. COPD 2019, 14, 3063–3066, doi:10.2147/COPD.S238239. [CrossRef]
- Calverley, P.M.A. Minimal Clinically Important Difference - Exacerbations of COPD. COPD. 2005, 2, 143–148. doi: 10.1081/copd-200050647. [CrossRef]
- Jones, P.W.; Beeh, K.M.; Chapman, K.R.; Decramer, M.; Mahler, D.A.; Wedzicha, J.A. Minimal Clinically Important Differences in Pharmacological Trials. Am. J. Respir. Crit. Care Med. 2014, 189, 250–255, doi:10.1164/rccm.201310-1863PP. [CrossRef]
- Maselli, D.J.; Hanania, N.A. Management of Asthma COPD Overlap. Ann. Allergy Asthma Immunol. 2019, 123, 335–344, doi:10.1016/j.anai.2019.07.021. [CrossRef]
- Demarche, S.F.; Schleich, F.N.; Henket, M.A.; Paulus, V.A.; Van Hees, T.J.; Louis, R.E. Effectiveness of Inhaled Corticosteroids in Real Life on Clinical Outcomes, Sputum Cells and Systemic Inflammation in Asthmatics: A Retrospective Cohort Study in a Secondary Care Centre. BMJ Open. 2017, 7, doi:10.1136/bmjopen-2017-018186. [CrossRef]
- Miravitlles, M.; Auladell-Rispau, A.; Monteagudo, M.; Vázquez-Niebla, J.C.; Mohammed, J.; Nuñez, A.; Urrútia, G. Systematic Review on Long-Term Adverse Effects of Inhaled Corticosteroids in the Treatment of COPD. Eur. Respir. Rev. 2021, 30, doi:10.1183/16000617.0075-2021. [CrossRef]
- GOLD-2019-v1.7-FINAL-14Nov2018-WMS.Pdf.
- Pascoe, S.; Locantore, N.; Dransfield, M.T.; Barnes, N.C.; Pavord, I.D. Blood Eosinophil Counts, Exacerbations, and Response to the Addition of Inhaled Fluticasone Furoate to Vilanterol in Patients with Chronic Obstructive Pulmonary Disease: A Secondary Analysis of Data from Two Parallel Randomised Controlled Trials. Lancet Respir. Med. 2015, 3, 435–442, doi:10.1016/S2213-2600(15)00106-X. [CrossRef]
- Bafadhel, M.; Peterson, S.; De Blas, M.A.; Calverley, P.M.; Rennard, S.I.; Richter, K.; Fagerås, M. Predictors of Exacerbation Risk and Response to Budesonide in Patients with Chronic Obstructive Pulmonary Disease: A Post-Hoc Analysis of Three Randomised Trials. Lancet Respir. Med. 2018, 6, 117–126, doi:10.1016/S2213-2600(18)30006-7. [CrossRef]
- Roche, N.; Chapman, K.R.; Vogelmeier, C.F.; Herth, F.J.F.; Thach, C.; Fogel, R.; Olsson, P.; Patalano, F.; Banerji, D.; Wedzicha, J.A. Blood Eosinophils and Response to Maintenance Chronic Obstructive Pulmonary Disease Treatment. Data from the FLAME Trial. Am. J. Respir. Crit. Care Med. 2017, 195, 1189–1197, doi:10.1164/rccm.201701-0193OC. [CrossRef]
- Wedzicha, J.A.; Banerji, D.; Chapman, K.R.; Vestbo, J.; Roche, N.; Ayers, R.T.; Thach, C.; Fogel, R.; Patalano, F.; Vogelmeier, C.F. Indacaterol-Glycopyrronium versus Salmeterol-Fluticasone for COPD. New Engl. J. Med. 2016, 374, 2222–2234, doi:10.1056/NEJMoa1516385. [CrossRef]
- Chalmers, J.D.; Laska, I.F.; Franssen, F.M.E.; Janssens, W.; Pavord, I.; Rigau, D.; McDonnell, M.J.; Roche, N.; Sin, D.D.; Stolz, D.; et al. Withdrawal of Inhaled Corticosteroids in COPD: A European Respiratory Society Guideline. Eur. Respir. J. 2020, 55, doi:10.1183/13993003.00351-2020. [CrossRef]
Figure 1.
PRISMA flow-diagram of the systematic literature search, study selection and reasons for exclusion.
Figure 1.
PRISMA flow-diagram of the systematic literature search, study selection and reasons for exclusion.
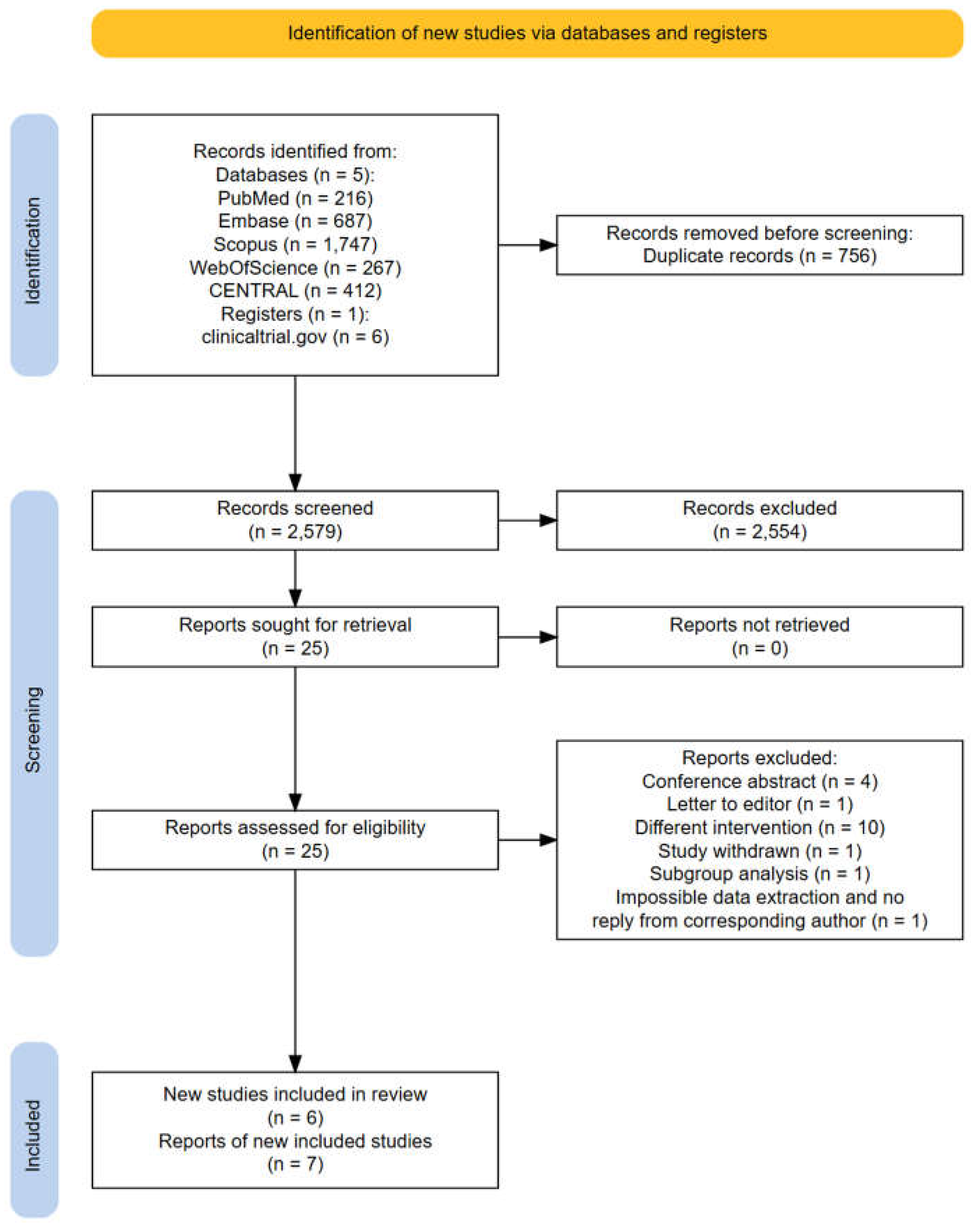
Figure 2.
Analysis of the time to the first moderate or severe exacerbation for ICS withdrawal compared with triple therapy continuation. ICS: inhaled corticosteroid; LABA: long-acting beta-agonist; LAMA: long-acting muscarinic antagonist; HR: hazard ratio; RCTs: randomized controlled trials; SE: standard error; 95% CI: 95% confidence interval;.
Figure 2.
Analysis of the time to the first moderate or severe exacerbation for ICS withdrawal compared with triple therapy continuation. ICS: inhaled corticosteroid; LABA: long-acting beta-agonist; LAMA: long-acting muscarinic antagonist; HR: hazard ratio; RCTs: randomized controlled trials; SE: standard error; 95% CI: 95% confidence interval;.
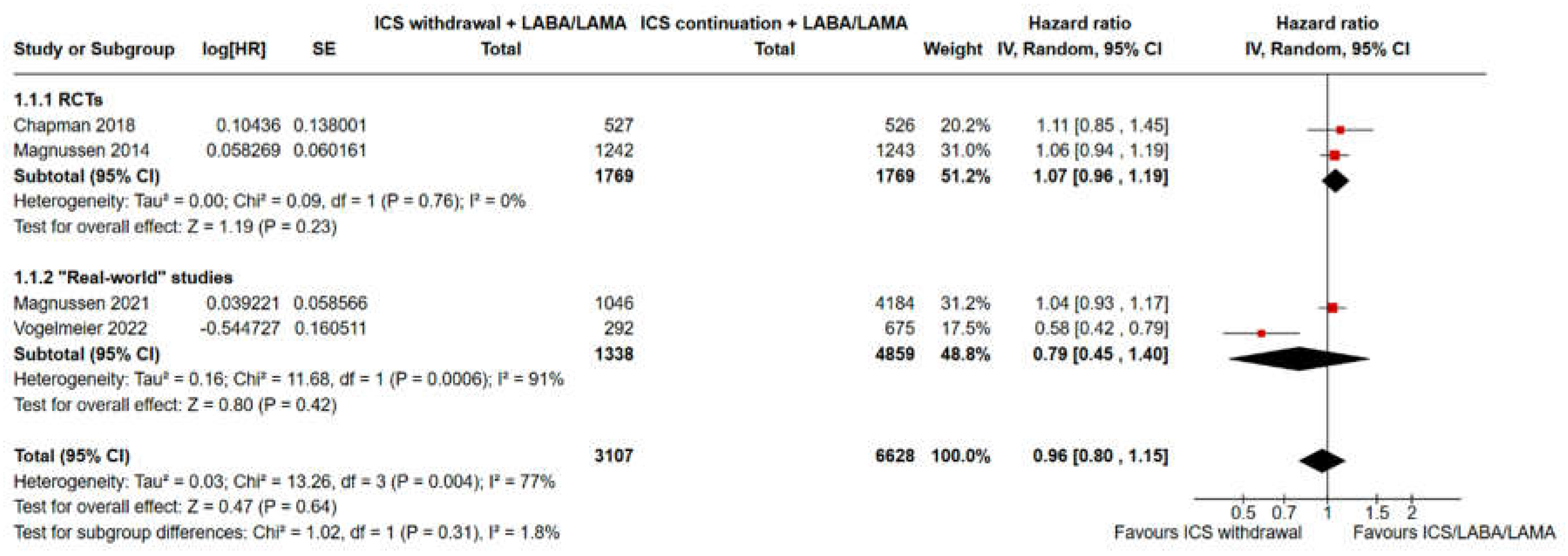
Figure 3.
Forest plot of meta-analysis comparing event rate for severe acute exacerbations in de-escalation from triple therapy with ICS withdrawal vs triple therapy continuation. ICS: inhaled corticosteroid; LABA: long-acting beta-agonist; LAMA: long-acting muscarinic antagonist; RCTs: randomized controlled trials; SE: standard error; 95% CI: 95% confidence interval;.
Figure 3.
Forest plot of meta-analysis comparing event rate for severe acute exacerbations in de-escalation from triple therapy with ICS withdrawal vs triple therapy continuation. ICS: inhaled corticosteroid; LABA: long-acting beta-agonist; LAMA: long-acting muscarinic antagonist; RCTs: randomized controlled trials; SE: standard error; 95% CI: 95% confidence interval;.
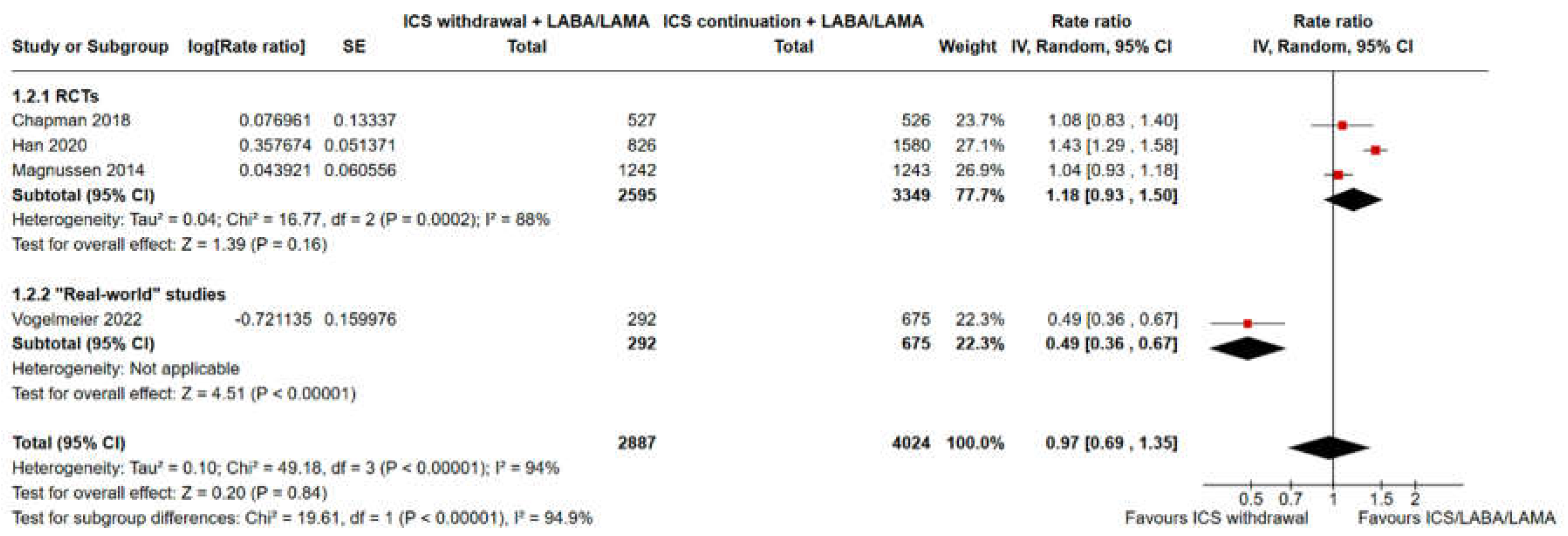
Figure 4.
Analysis of the time to the first moderate or severe exacerbation for ICS withdrawal compared with triple therapy continuation for COPD subjects with ≥300 eosinophils/µL vs < 300 eosinophils/µL. ICS: inhaled corticosteroid; LABA: long-acting beta-agonist; LAMA: long-acting muscarinic antagonist; HR: hazard ratio; SE: standard error; 95% CI: 95% confidence interval;.
Figure 4.
Analysis of the time to the first moderate or severe exacerbation for ICS withdrawal compared with triple therapy continuation for COPD subjects with ≥300 eosinophils/µL vs < 300 eosinophils/µL. ICS: inhaled corticosteroid; LABA: long-acting beta-agonist; LAMA: long-acting muscarinic antagonist; HR: hazard ratio; SE: standard error; 95% CI: 95% confidence interval;.
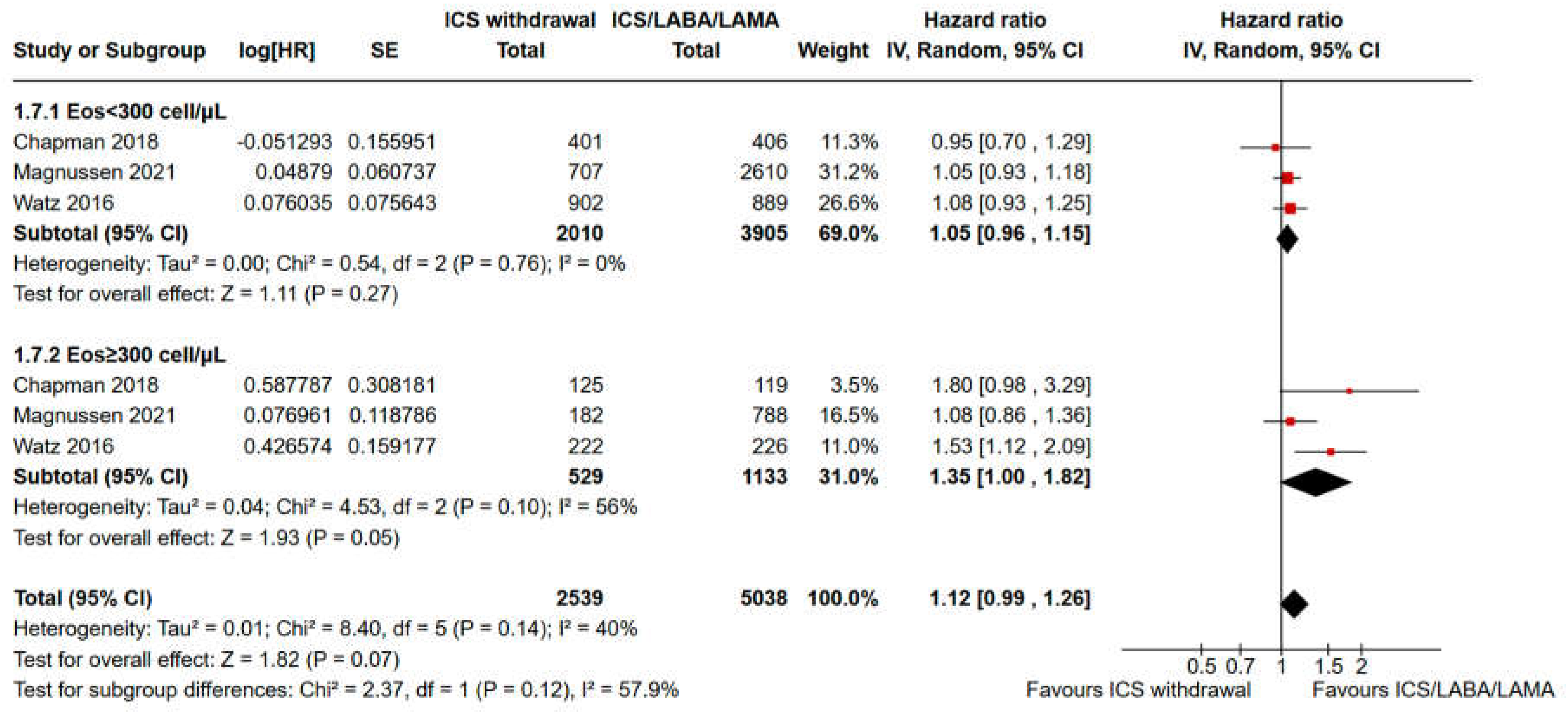
Figure 5.
Analysis of moderate or severe exacerbation rates for ICS withdrawal compared with triple therapy continuation for COPD subjects with < 150 eosinophils/µL vs ≥300 eosinophils/µL vs intermediate eosinophils levels (≥ 150 and < 300/µL). ICS: inhaled corticosteroid; LABA: long-acting beta-agonist; LAMA: long-acting muscarinic antagonist; SE: standard error; 95%CI: 95% confidence interval;.
Figure 5.
Analysis of moderate or severe exacerbation rates for ICS withdrawal compared with triple therapy continuation for COPD subjects with < 150 eosinophils/µL vs ≥300 eosinophils/µL vs intermediate eosinophils levels (≥ 150 and < 300/µL). ICS: inhaled corticosteroid; LABA: long-acting beta-agonist; LAMA: long-acting muscarinic antagonist; SE: standard error; 95%CI: 95% confidence interval;.
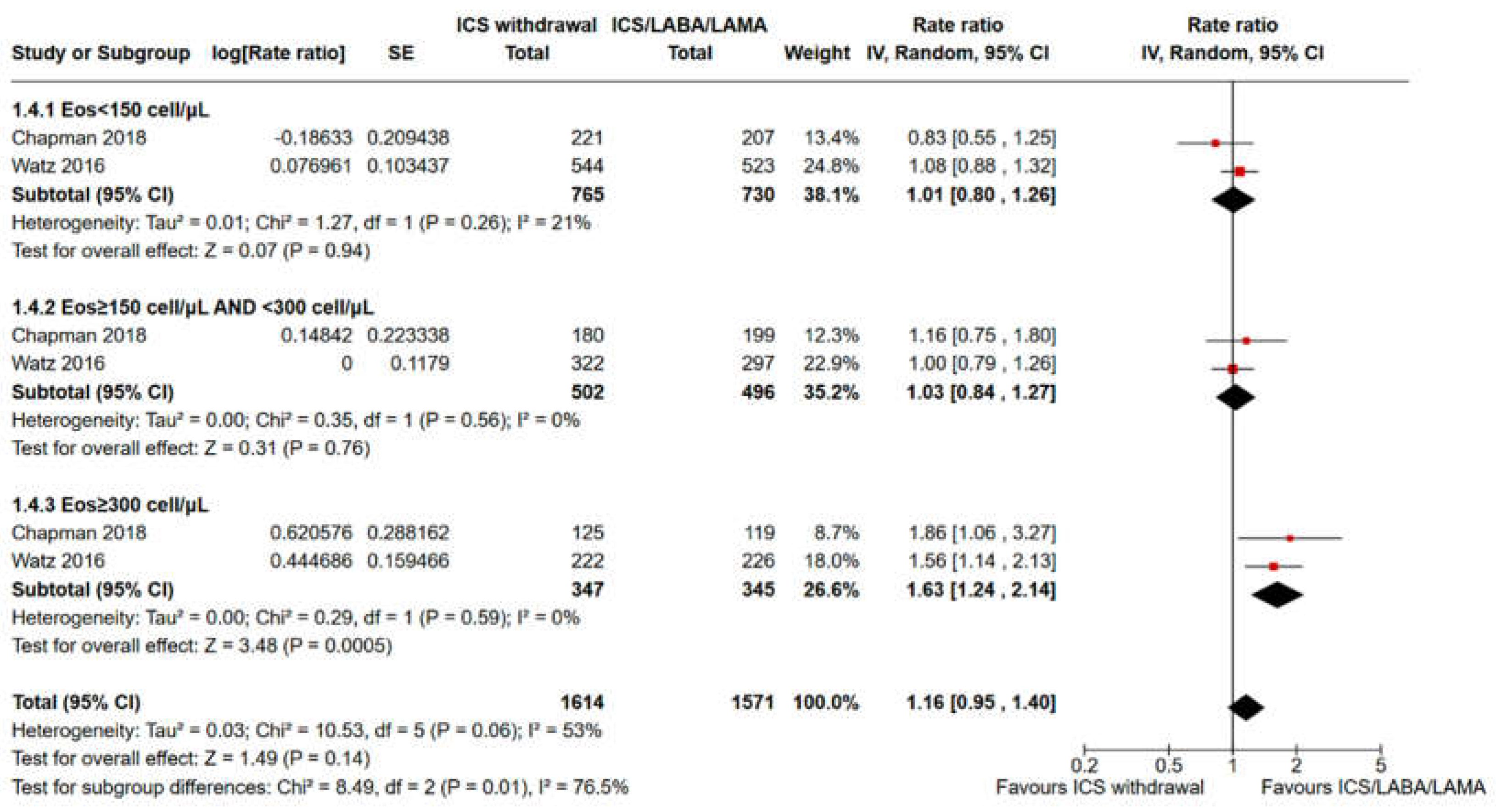
Figure 6.
Analysis of the trough FEV1 variation for ICS withdrawal compared with triple therapy continuation for COPD subjects with < 150 eosinophils/µL vs ≥300 eosinophils/µL vs intermediate eosinophils levels (≥ 150 and < 300/µL). ICS: inhaled corticosteroid; LABA: long-acting beta-agonist; LAMA: long-acting muscarinic antagonist; MD: mean difference; SE: standard error;.
Figure 6.
Analysis of the trough FEV1 variation for ICS withdrawal compared with triple therapy continuation for COPD subjects with < 150 eosinophils/µL vs ≥300 eosinophils/µL vs intermediate eosinophils levels (≥ 150 and < 300/µL). ICS: inhaled corticosteroid; LABA: long-acting beta-agonist; LAMA: long-acting muscarinic antagonist; MD: mean difference; SE: standard error;.
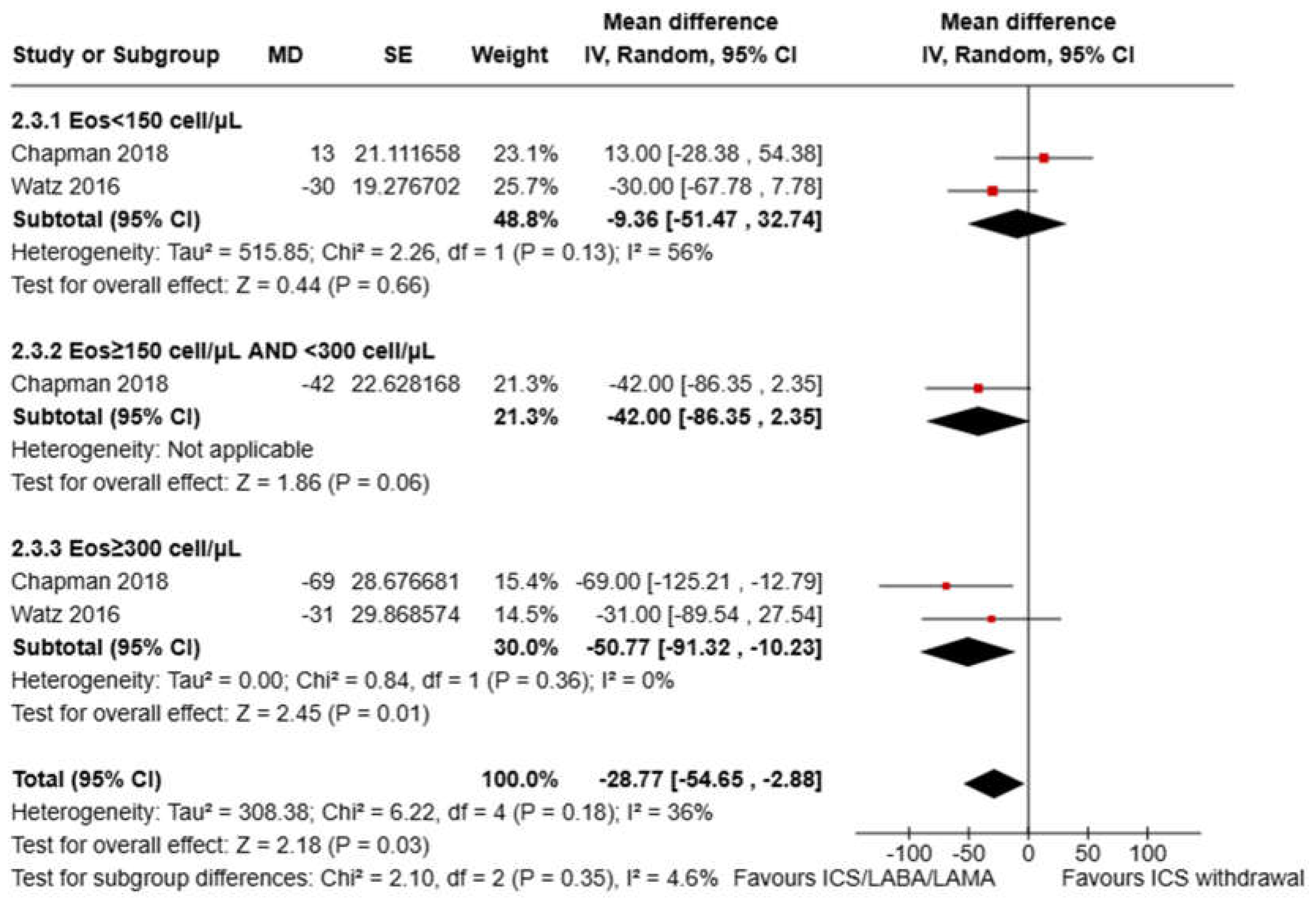
Figure 7.
(A) Forest plot of meta-analysis for all-cause mortality in de-escalation from triple therapy with ICS withdrawal group vs triple therapy continuation group. ICS: inhaled corticosteroid; LABA: long-acting beta-agonist; LAMA: long-acting muscarinic antagonist; RCTs: randomized controlled trials; 95% CI: 95% confidence interval; (B) Forest plot of meta-analysis for risk of pneumonia in de-escalation from triple therapy with ICS withdrawal group vs triple therapy continuation group. ICS: inhaled corticosteroid; LABA: long-acting beta-agonist; LAMA: long-acting muscarinic antagonist; RCTs: randomized controlled trials; 95% CI: 95% confidence interval.
Figure 7.
(A) Forest plot of meta-analysis for all-cause mortality in de-escalation from triple therapy with ICS withdrawal group vs triple therapy continuation group. ICS: inhaled corticosteroid; LABA: long-acting beta-agonist; LAMA: long-acting muscarinic antagonist; RCTs: randomized controlled trials; 95% CI: 95% confidence interval; (B) Forest plot of meta-analysis for risk of pneumonia in de-escalation from triple therapy with ICS withdrawal group vs triple therapy continuation group. ICS: inhaled corticosteroid; LABA: long-acting beta-agonist; LAMA: long-acting muscarinic antagonist; RCTs: randomized controlled trials; 95% CI: 95% confidence interval.
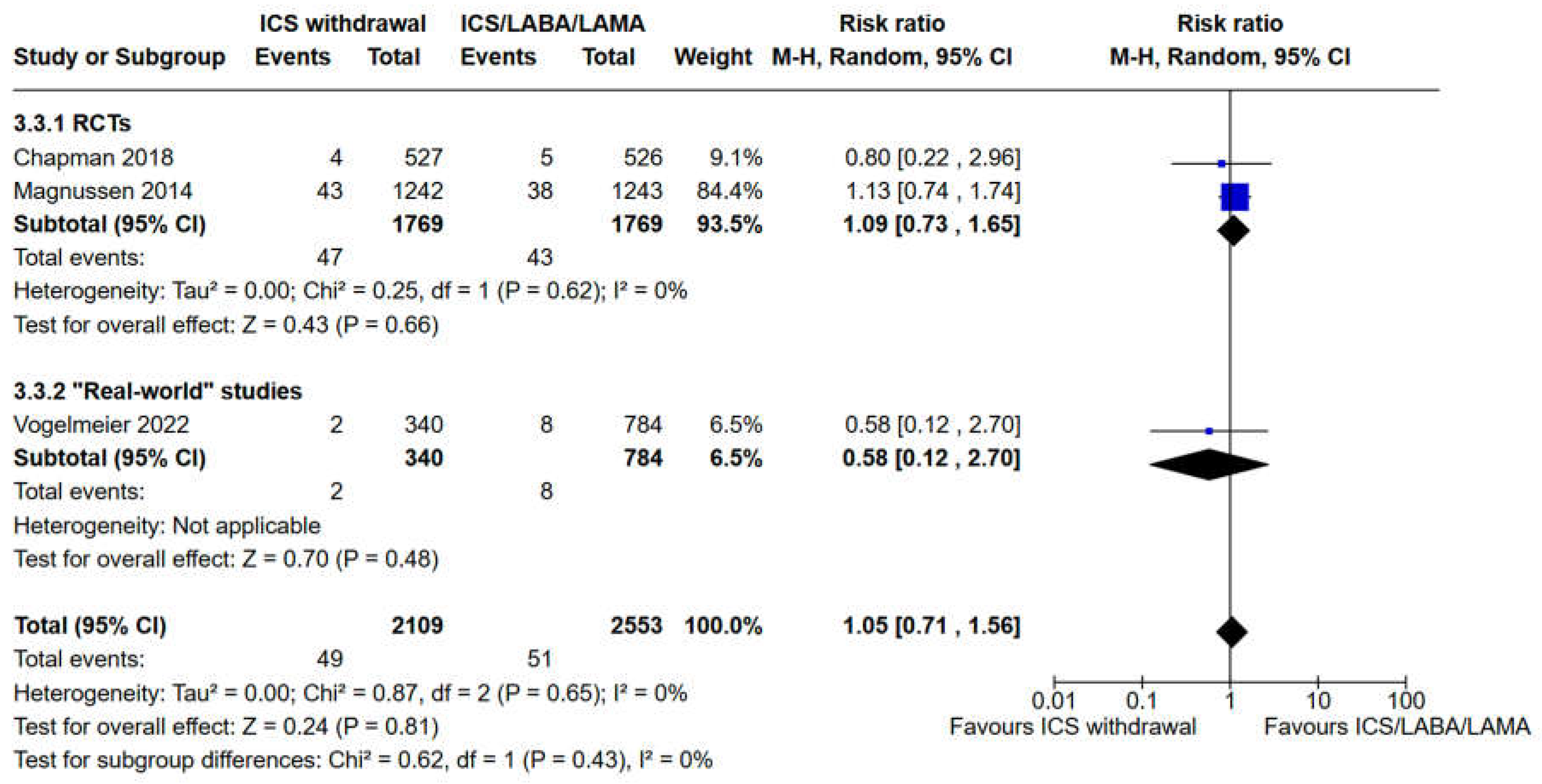
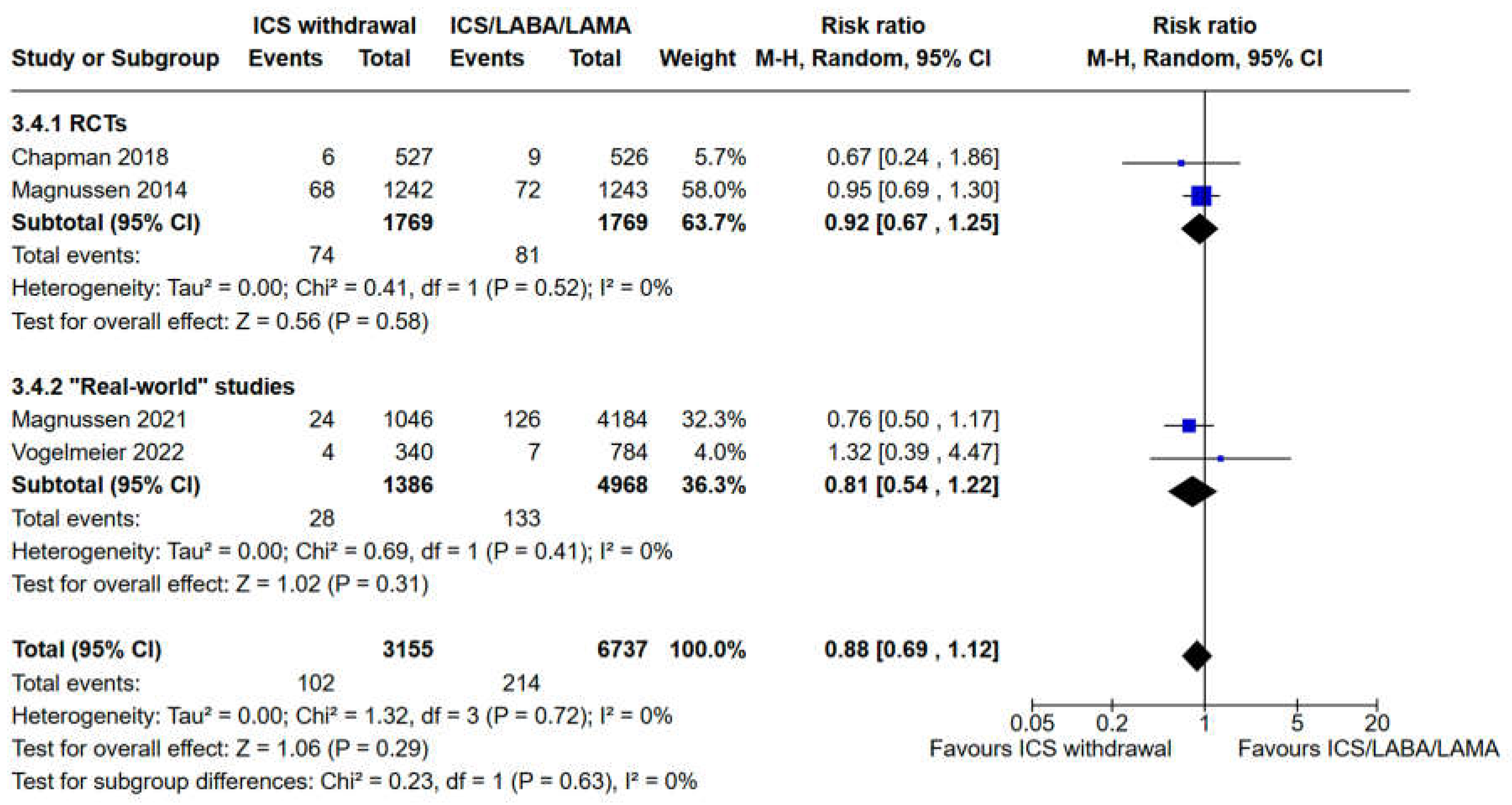

Table 1.
Baseline characteristics of included studies.
|
Study Duration (weeks) |
52 weeks | 52 weeks | 24 weeks | 52 weeks | 52 weeks | At least six months |
| Postbronchodilator FEV1 (% predicted) | 34,2±11,0 | N/A | 56,6±9,97 | 54,8±22,2 | 60,5±23,7 | N/A |
| Current Smoker (%) | 66,6 | N/A | N/A | 34,7 | 31,13 | 50,5 |
|
Male (%) |
82,5 | N/A | 70,6 | 55,4 | 57,7 | 61,2 |
|
Age (mean±SD) |
63,8±8,5 | N/A | 65,3±7,80 | 70,8±9,9 | 69,13±9,42 | 67,9±9,1 |
| Asthma | History: not reported; Current: Excluded; |
History: Included; Current: Excluded; |
History: Excluded; Current: Excluded; |
History: Included; Current: Included; |
History: Excluded; Current: Excluded; |
History: not reported; Current: Excluded; |
|
History of Exacerba-tion |
≥1 AE in the 12 months before screening |
≥1 AE in the 12 months before screening | ≤1 moderate or severe AE in the previous year |
N/A | N/A | Same as WISDOM; |
|
Patients Characteri- stics |
40 years old with FEV1<50% and FVC<70% | 40 years old with FEV1<50% and ≥1 moderate or severe AE or 50%≤FEV1<80% and ≥ 2 moderate or ≥ 1 severe AE | 40 years old with moderate to severe COPD | 40 years old with COPD | 40 years old with COPD | Same as WISDOM; |
| Control Group | Tiotropium 18µg OD Salmeterol 50µg BID (Separate inhalers) |
Umeclidinium 62,5µg Vilanterol 25µg OD (Fixed inhaler) |
Glycopyrronium 50µg OD Indacaterol 110µg BID (Separate inhalers) |
LABA/LAMA | LABA/LAMA | LABA/LAMA |
| Intervention | Tiotropium 18µg OD Salmeterol 50µg BID Formoterol 500µg BID (Separate inhalers) |
Fluticasone furoate 100µg Umeclidinium 62,5µg Vilanterol 25µg OD (Fixed inhaler) |
Fluticasone furoate 500µg BID Tiotropium 18µg OD Salmeterol 50µg BID (Separate inhalers) |
ICS/LABA/LAMA | ICS/LABA/LAMA | ICS/LABA/LAMA |
|
Total population (n) |
2485 | 2406 | 1053 | 5230 | 1124 | 6008 |
| Design | RCT | RCT | RCT | Non-RCT | Non-RCT | Non-RCT |
| Identifier | WISDOM, NCT00975195 | IMPACT, NCT02164513 | SUNSET, NCT02603393 | EUPAS30851 | DACCORD EUPAS4207 | N/A |
| 1st Author, year, Ref | Magnussen, 2014 Watz, 2016 [15,16] |
Han, 2020 [17] | Chapman, 2018 [18] | Magnussen, 2021 [21] | Vogelmaier, 2022 [20] | Whittaker, 2022 [19] |
N/A: not available, applicable or stated; ICS: Inhaled Corticosteroid; LAMA: long-acting muscarinic antagonist; LABA: long-acting beta-agonist; OD: omni die; BID: bis in die; FEV1: forced espiratory volume in the 1st. second; FVC: forced vital capacity; AE: acute exacerbation; RCT: randomized controlled trial; SD: standard deviation;.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



