
Submitted:
05 September 2024
Posted:
06 September 2024
You are already at the latest version
Abstract
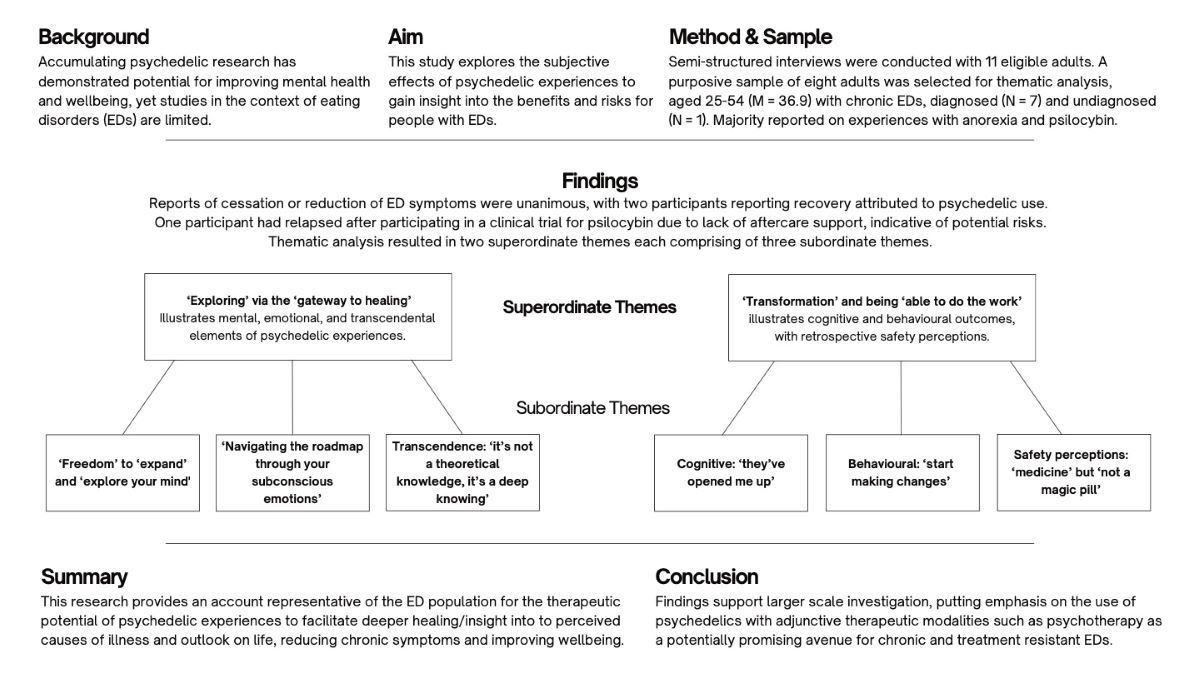
Accumulating psychedelic research has demonstrated potential for improving mental health and wellbeing, yet studies in the context of eating disorders (EDs) are limited. This study explores the subjective effects of psychedelic experiences to gain insight into the benefits and risks for people with EDs. Semi-structured interviews were conducted with 11 eligible adults. A purposive sample of eight adults aged 25-54 (M = 36.9) with chronic EDs, diagnosed (N = 7) and undiagnosed (N = 1) were thematically analysed. Reports of cessation or reduction of ED symptoms were unanimous, with two participants reporting recovery, attributed to psychedelic use. Thematic analysis resulted in two superordinate themes, each comprising three subordinate themes. The first superordinate theme, ‘Exploring’ via the ‘gateway to healing’, illustrates mental, emotional, and transcendental elements of psychedelic experiences. The second superordinate theme, ‘Transformation’ and being ‘able to do the work’, illustrates cognitive and behavioural outcomes, with retrospective safety perceptions. This research presents an account representative of the ED population for the therapeutic potential for psychedelic experiences to reduce symptoms and improve wellbeing. Findings provide evidence of therapeutic feasibility to support larger scale research, emphasising the therapeutic use of psychedelics as a potentially promising avenue for chronic and treatment resistant EDs.
Keywords:
Psychedelics
; eating disorders
; anorexia
; chronic
; qualitative
; mystical experience
; psilocybin
; ayahuasca
; psychedelic experience
; psychedelic assisted therapy
; treatment resistant
1. Introduction
Eating disorders (EDs) are serious and often chronic health conditions, characterised by abnormal eating behaviour, nutritional imbalances, persistent cognitive inflexibility and emotional distress (Smink et al., 2013; Svaldi et al., 2012; Frank et al., 2019). Marked by the highest risk of suicide and mortality rates of any psychiatric disorder, EDs are associated with a wide array of health complications (van Eeden et al., 2021; Ahn, Lee & Jung, 2019). With healthcare costs at 48% higher than the general population, EDs are among the most difficult to treat despite having high worldwide prevalence (van Hoeken & Hoek, 2020; Strober & Johnson, 2012; Cooper et al., 2016; Galmiche et al., 2019). Life-threatening inequalities, delays and failings in adult ED services leave many to rely on potentially dangerous, inadequate resources and significantly hampered wellbeing (Streatfield et al., 2021; Schmidt et al., 2016; Beat, 2019; Parliament Publications, 2019). Urgent calls have been made to investigate new interventions while effective treatment options are limited and long-term remission remains difficult to achieve (Moessner & Bauer, 2017; Solmi et al., 2021; Treasure et al., 2015; Wilson et al, 2007).
Simultaneously, there has been a renewed interest in the therapeutic potential of psychedelic drugs, with accumulating clinical evidence for safety and treatment efficacy across a range of prevalent mental disorders. Most notably, serotonergic psychedelics for illnesses characterised by rigid thought patterns and treatment resistance (Nutt, Erritzoe & Carhartt-Harris, 2020; Nutt, 2022). Central to this revival is the re-emergence of a psychedelic-assisted therapy paradigm, emphasising the therapeutic support, patient mind set, and setting for positive outcomes (Tupper et al., 2015).
Psychedelic therapies have been identified as a possible avenue for novel ED treatments, and while efficacy research is in its infancy, preliminary findings have so far been promising (Cuerva et al., 2024). Multiple clinical trials are currently underway, including one proof of concept and two pilot studies (Williams et al., 2023). Preliminary research has so far demonstrated marked reductions in ED symptoms and improvements in wellbeing following experiences with ceremonial psychedelics (LaFrance et al., 2017; Renelli et al., 2018; 2020), long-term psychedelic use (LaFrance et al., 2021) and short-term (Spriggs et al., 2021b), notably via spiritual and emotional pathways that facilitate healing. However, data is insufficient to draw firm conclusions. A recent preliminary paper reviews the hypothesis that psilocybin may be an effective adjunctive treatment for EDs, based on biological plausibility, transdiagnostic evidence and preliminary results (Koning & Brietzke, 2023). Adding weight to this hypothesis and extant preliminary evidence, this study explores the subjective effects of past psychedelic experiences on individuals with chronic EDs to elucidate potential benefits and risks associated with their wellbeing and symptoms.
The present findings delineate unanimous reports of significantly improved wellbeing and cessation or reduction of ED symptoms, with two participants reporting full recovery attributed to psychedelic use. One participant with psychedelic experiences limited to a clinical trial had reported relapsing after-the-fact and attributed this to a lack of support, with a key barrier being accessibility, rather than the psychedelic experiences themselves. Findings therefore provide an account of the therapeutic potential for psychedelic experiences to reduce symptoms and improve wellbeing for people with chronic, life enduring EDs, further supporting larger scale research.
2. Literature Review
2.1. Eating Disorders
A core feature of all EDs is the disruption of eating behaviour and nutritional regulatory systems (Himmerich et al., 2018). One aspect of ED pathology is the dysregulation of serotonergic signalling, such as in regions involved with appetite and reward, associated with mood instability, body image distortion and impulsivity (Frank, 2013; Foldi et al., 2020). It is thought that complex genetic and environmental factors contribute to ED pathology, alterations in emotional-cognitive function and interoception (Frank et al., 2019).
For example, anorexia nervosa (AN) is characterised by extreme dietary restrictions and an inability to maintain adequate healthy body weight (Arcelus et al., 2011). Orthorexia nervosa (ON) is marked by maladaptive and extreme obsession with health and restrictive diets (Dunn & Bratman, 2016). Binge eating disorder (BED) is characterised by episodes of binge eating, and bulimia nervosa (BN) combines BED with extreme compensatory behaviours, such as purging by vomiting (Berkman, Lohr & Bulik, 2007).
2.2. Theoretical Underpinning
The transdiagnostic theory underpinning EDs derives from the cognitive behavioural model, delineating core low self-esteem with clinical perfectionism, mood intolerance and interpersonal and emotional difficulties (Cooper et al., 2016; Svaldi et al., 2012). These beliefs and altered brain reward circuits lead to harmful maladaptive behaviours resulting in a cycle of comorbid issues, malnutrition, and physical consequences (Frank et al., 2019; Strober & Johnson, 2012; Himmerich et al., 2021). The wide array of comorbid conditions and psychological symptoms include poor concentration, impulse control, emotional dysregulation, depression, anxiety, obsessive compulsive disorder (OCD), post-traumatic stress disorder (PTSD), body dysmorphic disorder (BDD) and substance use problems or addictions (SUD) (Hudson et al., 2007; Ruffolo et al., 2006; Root et al., 2010; Spence & Courbasson, 2012; Anderson et al., 2002; Pisetsky et al., 2013).
Specifically, PTSD is associated with intense reactions to reminders of trauma, imminent threat and hypervigilance (Shalev, Liberzon & Marmar, 2017). OCD is marked by distressing intrusive thoughts (obsessions) and extreme avoidant and impulsive ritualistic behaviours (compulsions) (Abramowitz & Reuman, 2020), while BDD consists of distressing intrusive preoccupations with imagined or slight defects in appearance. The high comorbidity emphasises the complex aetiology and heterogeneous trajectories of EDs (Bjornsson, Didie & Phillips, 2022; Eskander, Limbana & Khan, 2020).
2.3. Treatments
The leading empirically supported psychotherapeutic treatment for EDs is cognitive behavioural psychotherapy (CBT), which rectifies dysfunctional ED thoughts and reduces ED behaviours (Fairburn et al., 2003; Dahlenburg et al., 2019). However, with less than 50% achieving remission, CBT is associated with high relapse (>30%) and dropout rates (>24%) (Waller, 2016; Södersten, 2017; Linardon, 2017; 2018). While recovery rates are still low, recent meta-analyses and multivariable meta-regression analysis of current treatments confirm that CBT enhanced for EDs, family-based therapy (in adolescents) and psychodynamic therapy (treatments based on an interpretive-supportive continuum) are associated with better outcomes (Leichsenring et al., 2015; Monteleone et al., 2022; Solmi et al., 2024).
Psychotherapy is often combined with pharmacological treatments, primarily selective serotonin reuptake inhibitors (SSRIs) as antidepressants. However, pharmacotherapy for EDs have overall failed to demonstrate significant benefit in effect sizes (Himmerich et al., 2021; Cipriani et al., 2018; Davies & Attia, 2019). A recent review suggests that pharmacological treatments may aid psychotherapy in BN and BED, but are associated with higher mortality and lower recovery in AN (Solmi et al., 2024). Moreover, a key debate argued by patients, carers, and researchers is that current treatments focus on the normalisation of weight, or cognitive behavioural aspects that are more likely consequences than causes, highlighting a crucial gap in leading treatments (Dessain et al., 2019; Strober & Johnson, 2012).
To date, evidence-based treatments are limited in efficacy, there is no specific drug to treat EDs, and new treatment data are scarce (Himmerich & Treasure, 2018; Mind, 2021). Addressing the urgency for new approaches is deemed to have the largest potential effect on the population’s disease burden (Moessner & Bauer, 2017; Solmi et al., 2021). Given the high comorbidity and genetic correlations, some experts have suggested that novel research and pharmacological developments, particularly the adjunctive use of psychedelic drugs that enhance effects of psychotherapeutic approaches (psychedelic-assisted psychotherapy), may extend future options for ED treatments (Nutt, 2020; Himmerich et al., 2021).
2.4. Psychedelics
Psychedelics are powerful psychoactive substances that produce altered states of consciousness (ASC), characterised by alterations in perception, mood and numerous cognitive processes including the sense of self, emotional state, and reality (Nichols, 2016; Preller & Vollenwieder, 2016). Psychedelics of plant extraction (serotonergic hallucinogens), now referred to as ‘classic psychedelics’, have an ancient history of medicinal use. These substances have demonstrated strong psychopharmacological properties and therapeutic efficacy, particularly during psychedelic-assisted psychotherapy (PAP) (see Table 1) (Nutt, 2022). These compounds work by stimulating brain serotonin receptors, primarily the serotonin 5-hydroxytryptamine 2A (5-HT2A) receptor, known to produce the psychedelic effects during ASCs (Nicholls, 2016). The other class of hallucinogenic substances are dissociative psychedelics, which typically cause detaching effects.
In clinical contexts, these substances are known to promote robust functional and structural neural plasticity, particularly in the prefrontal cortex of the brain which modulates cognitive control (Carhart-Harris et al., 2017; Ly et al., 2018). For example, increased global brain integration can be demonstrated in patients with depression after psilocybin therapy, shown to induce rapid and persistent cell growth in the frontal cortex with decreased amygdala reactivity, thus enhancing positive mood (Daws, Timmerman, Giribaldi et al., 2022; Shao, Liao, Gregg et al., 2021; Kreahenmann, Preller & Scheidegger., 2015). Behavioural and neuroimaging data further emphasise that they are among the most effective chemical modulators of neural plasticity to date, with potential to produce significant and sustained reductions in symptoms of mood and affective disorders (Lowe et al., 2022; Vargas et al., 2021; Muttoni et al., 2019).
Furthermore, positive psychology research (i.e., of healthy functioning and wellbeing) has provided strong evidence for positive effects on wellbeing, prosocial behaviours, creativity, personality, values, and mindfulness from 77 clinical trials and epidemiological studies (N = 9876) using psychedelics (Jungaberle, 2018). Altogether, amassing research has led to the general acceptance that psychedelic compounds are clinically and physiologically safe, with low abuse liability and low potential for dependence and medical harms (Nutt, 2015; Rucker, Illif & Nutt, 2018; Nutt & Carhart-Harris, 2021; Schlag et al., 2022). The influx of renewed research interest constitutes a uniquely promising avenue for future healthcare developments.
To date, the most significant database now exists for classic compounds psilocybin (the active compound in “magic mushrooms”) and MDMA (a synthetic psychostimulant otherwise known as “ecstasy”) (Nicholls, 2016), approved by the FDA as “breakthrough therapies” for treatment-resistant depression and PTSD (Reiff et al., 2020). Additionally, synthetic dissociative drug ketamine (an old established anaesthetic and glutamate receptor agonist) has shown antidepressant properties, resulting in its licensing in the USA and Europe (Nutt, Erritzoe & Carhart-Harris, 2020).
As stated previously, there has been increasing clinical evidence supporting the transdiagnostic effects of psychedelic-assisted therapies (PAT) for disorders of restrictive or maladaptive habitual patterns of cognition, emotion, and behaviour, including EDs (Kelly et al., 2021). Furthermore, PAT is emerging as a radical innovation to meet the decline in novel psychiatric medications amidst the rise in mental disorders, linked to debates criticising current symptom-focused approaches (Schenberg, 2018).
Emphasising these criticisms are the pharmacological properties and therapeutic efficacy continually present in clinical studies for depression, anxiety, addictions, OCD and PTSD (Tupper et al., 2015; Nutt, 2022; Lowe, Toyang, Steele et al., 2022). Meta-analysis of psychedelic-assisted randomised placebo-controlled trials for treating these disorders provide further evidence of feasibility and early efficacy data for therapeutic effects, lasting weeks to months in majority of patients (Anderson et al., 2021), including patients with PTSD, and for anxiety among adults with autism (Luoma et al., 2020). Furthermore, large scale study of biochemical mechanisms underlying classic psychedelic induced neuroplasticity, and the non-addictive nature add weight to their therapeutic potential (Olsen, 2022; Canal & Murnane, 2017).
Simply put, the primary shared feature among the conditions listed is their internalising nature, characterised by negative rumination, intrusive thoughts, and high comorbidity with EDs. The brain activity control systems and circuits that encode these habits, particularly the default mode network (DMN), are thought to be dysregulated by psychedelics via receptor agonism, allowing them to recalibrate thereafter as the acute effects subside (Nutt, Erritzoe & Carhart-Harris, 2020; Romeo et al., 2021).
Specifically, this modulation of the serotonergic system is thought to be associated with the anxiolytic and antidepressant effects with lasting mental health improvements. This suggests potential to normalise dysfunctional neurobiological systems via the global increase of brain network integration, thus becoming more functionally interconnected and flexible (Carhart-Harris & Friston, 2019; Rodan et al., 2021; Knudsen, 2022; Daws et al., 2022). Such hypotheses have long been supported by numerous scientific reviews (Carhart-Harris et al, 2014; Dos Santos et al., 2016; Johnson et al., 2019; De Vos et al., 2021).
2.5. Theoretical Underpinning
To further understand how psychedelics alter brain function and consciousness, a unified model has been proposed, called the relaxed beliefs under psychedelics (REBUS) and the anarchic brain model (Carhart-Harris & Friston, 2019). The key principle is that the action of psychedelics, via entropic effects on spontaneous cortical activity, liberate bottom-up information flow (often overweighted in contexts of mental illnesses) by relaxing the precision of high-level priors/beliefs (instantiated by the DMN) via intrinsic control systems in the brain. The result is heightened sensitivity of high-level priors to bottom-up signalling from intrinsic sources such as the limbic system, rather than top-down processes, thus enabling the revision of pathologically rigid or conditioned beliefs and emotion. This key assumption is consistent with empirical evidence that relaxation and revision of negative self-belief confidence mediates positive psychological and wellbeing outcomes (Zeifman et al., 2022).
Similarly, both naturalistic and lab studies indicate mediating roles of anxious ego dissolution, spirituality, and boundlessness on symptoms of anxiety, depressed mood, and disordered eating (Preller & Vollenweider, 2016; LaFrance et al., 2021) via acute effects on emotion, cognition, creativity, and sensory perception, with notably limited aversive side effects (Orlowski et al., 2022; Aday et al., 2020). Such findings add depth to population studies linking lifetime psychedelic use to significantly elevated mental health symptoms and wellbeing than non-users, highlighting untapped therapeutic potential (Krebs & Johansen, 2013; Hendricks et al., 2015).
Also of importance is the acute psychedelic experience itself, thought to be the main contributing factor of enduring therapeutic effects (Griffiths et al., 2006; 2008; Uthaug et al., 2018; 2019). The best outcomes with psilocybin for example, have been demonstrated in patients experiencing breakthrough, peak or mystical experiences; in other words, the most powerful psychedelic effects (Roseman et al., 2018b). This coincides with clinical, neuroimaging, naturalistic and population studies emphasising the relationship between mystical or subjective effects, insight, and therapeutic outcomes on brain network function (Johnson et al., 2019). These findings are further supported in the most recent comprehensive population survey of psychedelic drug users to date, the Canadian Psychedelic Survey. Additionally, significant correlates of ‘intense positive experiences’ included higher perceived psychedelic experience, with fun and self-exploration as motivations for use (Lake & Lucas, 2023).
More specifically, mystical and insight effects are thought to be a necessary counterpart to positive enduring outcomes (Yaden & Griffiths, 2020). Supportive neurobiological evidence demonstrates that key contributors to the therapeutic effects of psychedelic experiences are changes in self-experience, emotional processing and social cognition (Vollenweider & Preller, 2020). Furthermore, closer inspection of PAT analyses emphasises the key role of connectedness, spirituality and meaningfulness from mystical experiences to improved and sustained outcomes (Moro, 2011; Johnson et al., 2019; Carhart Harris & Erritzoe et al., 2018). Consequently, experiencing ‘emotion awe’ has been hypothesised as an underlying mechanism that fosters a sense of oneness and connectedness with others (Hendricks, 2018). Taken together, insight correlating with mystical experiences are suggested catalysts for change (Davis, Barrett & Griffiths, 2020).
2.6. Risks of Harm/Adverse Effects
A final aspect to consider regarding safety and risks is the adverse effects and challenging psychedelic experiences that are relatively unexplored (Evans & Robinson et al., 2023). In the recent Canadian Psychedelic Survey (N = 2045), half reported challenging psychedelic experiences, 56% of which said ‘some good’ came from the experience thereafter (Lake & Lucas, 2023). To be more specific, Evans and Robinson’s (2023) study recruited 608 participants reporting extending difficulties following psychedelic experiences. Feelings of anxiety and fear, existential struggle, social disconnection, depersonalisation and derealisation were the most frequently reported forms of extended difficulty. These problems persisted for over a year in one third of the sample and were endured for more than three years for ~16.6%. Importantly, knowledge of dose, drug type and lower levels of difficulty during the trip predicted a shorter duration of difficulties, while taking the drug in a guided setting predicted a lower range of difficulties, thus pointing towards the importance of education, support and harm reduction (McNamee et al., 2023).
3. Psychedelics and Eating Disorders
It is now plausible to consider the application of psychedelic therapy for those suffering from EDs and the caveats associated with psychedelic therapy trials (Borgland & Neyens, 2022; Rodan et al., 2021; Himmerich et al., 2021). Psilocybin, for example, has shown promise for alleviating depressive symptoms by enhancing cognitive flexibility. This could be applicable in the case of breaking down cognitive inflexibility associated with AN (Conn, Milton, Huang et al., 2024).
The few extant clinical and naturalistic reports of psychedelic use and EDs have so far demonstrated long and short-term cessation or reductions of ED and mental health symptoms, most notably with ayahuasca and psilocybin (LaFrance et al., 2017; Renelli et al., 2018; 2020; Spriggs et al., 2021a; 2021b). Additionally, due to the high comorbidity of EDs with PTSD, one clinical trial investigating MDMA-assisted psychotherapy as a treatment for comorbid ED-PTSD (N=82) showed promising results with significant reductions in ED symptoms (Brewerton et al., 2021).
To summarise the paucity of research on the present topic, a single scoping review exists on outcomes of psychedelic use for people reporting an eating disorder, comprising six clinical and non-clinical studies (including psilocybin, ayahuasca, DMT/5-MEO-DMT, LSD, mescaline and ketamine), reporting diminished and reduced symptoms of the ED, of anxiety, self-harm and suicidality, with some showing complete remission (Valdiviezo-Ona et al., 2023). Improvements in wellbeing and depression were also reported, along with changes in self-perception and several reports of profound spiritual healing or deep insights into the origins of their ED.
When looking at specific effects of ayahuasca on EDs, LaFrance’s (2017) investigation of ceremonial ayahuasca (a traditional Amazonian tea used in sacred healing rituals) reported significant improvements in emotional regulation and processing, linked to decreased symptom engagement or sustained remission in 11 out of 16 participants with AN and BN diagnoses. Furthermore, Renelli’s (2020) investigation reported that ayahuasca experiences were more effective than conventional ED treatments in a sample of 13, primarily by enabling the processing of intense emotions or memories, thus deeper healing via a spiritual component that enhanced recovery progression.
Importantly, both studies found that the psychedelic experiences provided tangible emotional insights about causes of illness, self-love, care, and acceptance; altogether allowing for the revision of core ED beliefs. Revisions of self-compassion, criticism and emotional regulation are consistent with reports on ayahuasca and wellbeing (Dominguez-Clave et al., 2022). Data on the potential for ayahuasca-assisted therapy as a healing tool for treating EDs are summarised and reviewed in LaFrance’s 2021 paper, detailing associated perceived risks and recommendations for integrating ayahuasca into a Western context.
Furthermore, these findings add weight to numerous reviews of broader psychedelic research which demonstrate that emotional breakthroughs, release, revision of core beliefs, mindfulness and cognitive flexibility are key mechanisms associated with classic psychedelic use and enduring changes in wellbeing and psychological functioning (Nutt, Erritzoe & Carhart-Harris, 2019; Roseman et al., 2019; Murphy-Beiner & Soar, 2020).
Emotional aspects are particularly pertinent, given that a central function of EDs is an attempt to manage difficult emotions, often manifesting as high avoidance or low emotional awareness and low motivation (Svaldi et al., 2012; Espel et al., 2016). It is therefore important to reiterate that psychedelic emotional breakthroughs are known to catalyse significantly increased psychological/cognitive flexibility, openness and connectedness associated with neural plasticity, as demonstrated in fMRI studies of brain mechanisms in patients with treatment resistant depression (Carhart-Harris et al., 2017). Furthermore, the first quantitative demonstration of positive psychological aftereffects in those with an ED planning to take a psychedelic drug has provided overwhelming evidence for improvements in depression and wellbeing scores thereafter (Spriggs et al., 2021b).
Subsequently, the first clinical trials for AN using psilocybin (National Library of Medicine, NCT04052568, 2019; NCT04505189, 2021; NCT04661514, 2022) and BED have begun. Furthermore, the protocol for a pilot study on psilocybin-assisted therapy for AN to assess feasibility, brain mechanisms and preliminary outcomes (Spriggs et al., 2021a), integrates the voices of those with lived experiences using Public Patient Involvement (PPI) focus groups that incorporate patient opinions to inform research directions (Close et al., 2021). The authors emphasised the importance and benefit of PPI to the study, participants, and psychedelic research, by integrating information rich qualitative accounts to inform future trials.
Finally, from the perspective of individuals with EDs themselves, Harding’s (2022) survey (N = 200) found that nearly 70% used complementary spiritual treatments such as yoga, meditation, and relaxation techniques to manage their ED, and believed psychedelic research to be worthwhile. Only 29.5% felt they would never participate in a clinical trial using psychedelics, with the main concern being weight gain (74%), and although not associated with weight gain, psychedelics are suggested to induce self-care effects that could facilitate healthy lifestyles, exercise and diet (Watts et al., 2017; Machek, 2019; Teixeira et al., 2021). Participants expressed ‘education around psychedelics’ and ‘endorsement from professionals’ as solutions to their concerns (Harding et al., 2022). When considering the overlaps between the phenomenology and neurophysiology of meditation practices with psychedelic ASCs associated with improved wellbeing (Milliere et al., 2018) and the demand for effective ED treatments, further research could indeed benefit this population.
4. Aims
The urgent need for novel ED treatments is growing, alongside clinical evidence supporting the transdiagnostic therapeutic potential of serotonergic psychedelics (Himmerich et al., 2021). Small-scale preliminary studies have so far demonstrated marked reductions in ED symptoms and improvements in wellbeing following experiences with ceremonial ayahuasca (LaFrance et al., 2017; Renelli et al, 2018; 2020), long-term psychedelic use (LaFrance et al., 2021) and short-term (Spriggs, 2021b), via spiritual and emotional pathways that facilitate healing. However, data is insufficient to draw firm conclusions.
As abnormal serotonin functioning and high emotional avoidance are associated with EDs (Kaye, 2008; Cowdrey & Park, 2011), there is mechanistic grounding warranting further investigation of psychedelics in the context of EDs (Spriggs, 2021a; Koning & Biretzke, 2023). The present study therefore seeks to build upon extant research and investigate how people with EDs make sense of the psychedelic phenomenon and the factors that influence perceived outcomes, benefits and risks.
5. Method
5.1. Sampling: Recruitment and Participants
A purposive sample of eight participants was recruited via social media advertisements for volunteers who could talk about their experiences of both EDs and psychedelics. Out of the total 14 respondents, 11 were interviewed according to protocol. Information-rich cases were then sought during screening using “criterion-based sampling” (Patton, 2002), aiming to yield insight and understanding of the participant so that the highest quality explorations could be analysed. Three of 11 interviewees were excluded, due to the remaining eight fitting the following inclusion criterion to a stronger degree: (1) reporting to have had a prior diagnosis of an ED, or suffered symptoms without professional diagnosis, (2) have at least one psychedelic experience.
The final sample (N = 8) included one non-binary and seven female participants, with ages ranging between 25-54 years old (M = 36.9). The age for onset of ED symptomology was between 12-16 years old (M = 13.4), meaning all participants had suffered chronic, life enduring EDs for the duration of 11-42 years (M = 23.5) (Table 2).
Seven participants had multiple ED diagnoses and had used multiple modes of conventional therapy. Five participants had used antidepressants with poor outcomes. Only one participant (P6) had never received ED treatment (besides a diet plan) and was the only participant to report lifetime recreational psychedelic use. P6 and P8 were the only participants to have reported full recovery (attributed to psychedelic use). Three participants were current users of private therapy (P2, P3, P5), P1 was back on the NHS waiting list. Further sample characteristics and outcome information are presented in Table 3.
5.2. Data Collection: Semi-Structured Interview and Procedure
Following ethics approval from the university Research Ethics Committee and recruitment, advertisement respondents were contacted via email and sent further information. Having read and signed the information and consent form, participants were interviewed for 30-90 minutes (M = 57). Data were collected using a self-report method with semi-structured online interviews using Microsoft Teams (audio only) and recorded.
At the start of the interview, consent was reconfirmed, and participants were reminded of their rights to omit questions, stop the interview, and withdraw. The interview schedule was then administered, using probes to explore psychedelic phenomena and relevant aspects. The interviewing style was flexible with open questions allowing participants to elaborate on details important to them. Participants were made aware of the interview schedule ahead of time to strengthen the quality of recall. At the end of the interview, participants provided a personal code which was attached to their debriefing form containing additional information for support services. Interview recordings were transcribed verbatim and uploaded to qualitative data software, Nvivo, for analysis.
5.3. Design: Qualitative Analysis
Eight interviews were analysed using reflexive thematic analysis (TA) (Braun & Clarke, 2022). Analysis and coding efforts were conducted in accordance with guidelines provided by Braun & Clarke (2006). This approach allowed for a flexible exploration into participants’ reality regarding the psychedelic phenomenon, and therefore conducted within a realist/essentialist paradigm. Its epistemology assumes a unidirectional relationship between experience, meaning and language, thus the analysis methodology was inductive with codes and themes identified at a semantic level, elicited by the interview data alone.
The primary goal of analysis was to systematically organise what participants reported about their psychedelic experiences and perceived effects on wellbeing and ED symptoms into themes, answering specifically to the research question. Overarching categories were pre-determined to classify findings: the context, the experience, and the aftereffects. Themes were created in terms of coding and prevalence patterns. A theme was defined as a pattern in the data if it occurred for more than half of the transcripts.
The start of the thematising process involved re-reading transcripts to familiarise with the data. The second phase involved a cyclical coding process. Initial open coding was based on participant perspectives without finite interpretations from the researcher, and relationship codes that broke data down into various incidents/events. These were then subject to pattern coding by identifying patterns across and within transcripts to condense data into more manageable segments as analytic concepts, thus in line with a more nomothetic approach typical of TA (Bingham & Witkowsky, 2022; Vaismoradi et al., 2016).
Codes were then clustered by thematic similarity into provisional subthemes and iteratively reviewed and refined, allowing for clearer identification of initial themes. This led to the construction of superordinate themes that subsumed subthemes, followed by further analysis to determine the significance of patterns, prevalence, and broader meanings. Initial themes were then reviewed by project supervision and defined to ensure a thorough capturing of explored content, before names were finalised. Nvivo provided the prevalence of each code and theme, highlighting the repetitions of specific themes across the dataset which guided the final process of writing up the results.
5.4. Ethics Commentary
No physical or emotional harm was caused, measures to avoid risk were implemented throughout all online procedures for safety. This includes disclosing the interview schedule and clarifying aims to only assess perceptions of the psychedelic experiences, their meaning, and effects deemed relevant by the participant. Efforts were maintained to avoid prying into more personal and potentially triggering aspects, unless initiated by the participant. Participants were treated according to BPS guidelines. Interview questions were considerate of risk of emotional harm in discussing participants’ personal experiences. Strict participant anonymity and confidentiality was maintained throughout.
5.5. Results and Discussion
Following thematic analysis, two superordinate themes each comprising three subordinate themes were identified, presented in Table 4. The following sections unpack each theme to provide a deeper understanding of the experiences reported.
5.6. Superordinate Theme 1
Exploring via ‘the Gateway to Healing’
Participants unanimously discussed the significant ‘catalysing’ role of their psychedelic experiences, describing how it ‘opened’ their minds, or ‘doors that needed opening’ having ‘kick started something, quite heavily’:
“Until you’ve actually tried them, you don’t really understand like, how life changing it can be and how it can free your mind to kind of see other possibilities and other pathways that you could choose to reinforce if you wanted to. So, like, once I had my first couple of psychedelic experiences, I got excited about what I might be able to do with it.” (P5)
This action enabled positive change in participants’ lives by providing renewed abilities, insights, and perspectives:
“...my brain was a lot more open and available to think, and, there was more possibility and hope” (P1)
These experiences encompassed mental, emotional, and transcendental aspects presented as subthemes that facilitated healing from ED causes by addressing ‘things that blocked having a full life and being healthy’:
“...these are concepts I’ve been working on my whole life, but I’ve not been able to put into practice... So, I think that when I took the psilocybin, I was able to put into practice all the work that I’ve been doing. I realised that it wasn’t for nothing, it wasn’t lost, and that I was working, I was fighting like hell. And um, psilocybin opened the door.” (P8)
This theme therefore unpacks the ‘profound’, ‘unimaginable’ ways that psychedelic ASCs were experienced, as essential precursors to positive outcomes.
5.7. Subordinate Theme 1. ‘Freedom’ to ‘Expand’ and ‘Explore Your Mind’
All participants described being given ‘freedom’ or ‘space’ to explore their thoughts, and ‘choose to do something else rather than just going through the same habits’, whereby detaching from ‘habitual judgemental views’ and ‘obsessive thoughts’ enabled connections to new insights about their ED:
“They help me realise why I’m having these urges, why I’m feeling that way. But also showed me that the eating disorder is part of something bigger, something deeper, which I need to go back and look at.” (P3)
This process was frequently referred to as being ‘present’. Participants unanimously described a more rational and relaxed state, giving them the ‘ability to focus’ and ‘realise’ faulty thinking, leading to resolutions and new approaches towards self-reflection:
“... I could focus my mind, which was brand new to me. I could choose, if I didn't want to think about something, I could just let it go. It, it was brilliant... That’s what I noticed first. That I could observe my thoughts, and see what was going on in my mind...
I could not before, I could know what I was thinking, but wasn’t able to... Place myself, like see myself as the observer, other than the person wrapped up in the thoughts. And I thought, wow, so this is how I’m thinking... And most importantly without judgement, my judgements, criticisms, self-criticisms... Just turned into real curiosity and wonder... And admiration for how truly, sneaky my mind is.” (P8)
The consistent reports of therapeutic effects (relaxed thinking, improved focus and cognitive flexibility) that helped alleviate habitual negative ruminations and intrusive thoughts are consistent with research suggesting that the brain circuits encoding these habits, particularly the DMN, is dysregulated during psychedelic ASCs (Nutt, Erritzoe & Carart-Harris, 2020; Romeo et al. 2021). This is particularly relevant given that many with EDs (~70%) use complementary meditative relaxation modalities to manage their EDs and are in support of psychedelic research for future treatment avenues, indicating therapeutic value (Harding et al., 2022).
Importantly, participants signalled the fact that psychedelics facilitate meditative and therapeutic processes as an adjunctive tool for self-healing. Specifically, their accounts reference the five facets of mindfulness (observe, describe, act with awareness, non-judging, and non-reactivity of inner experience) (Baer et al., 2006). As mindfulness is broadly defined as paying attention in a purposeful way, present and non-judgingly (Katbat-Zinn, 2003), findings therefore coincide with research suggesting mindfulness and cognitive flexibility to be potential mechanisms for therapeutic effects of classic psychedelics (Murphy-Beiner & Soar, 2020).
This subtheme is therefore synthesised by the unanimous notion of mental clarity that enhanced self-awareness, allowing participants to separate from and challenge the ‘oppressive’, ‘harsh’, or ‘anxious’ inner ‘critic’ dictating their ‘reality’, linked to their ED. This enabled progress towards recovery by re-approaching aversive, more challenging stimuli, ‘drawn out into the light to be looked at’ with a more ‘forgiving’, ‘relaxed’, ‘accepting and carefree’ mindset.
Aversive stimuli that presented reportedly stemmed from compulsive thoughts, unresolved trauma contributing to or ‘realised’ as the ED root cause, or loss of control (challenging experience) during the trip. One participant from a clinical trial described somatic distortions and muscle clenching that became throat tightness, triggering an ‘oh god, what’s happening, maybe it’s doing something bad and I’m gonna die’ reaction, followed by an automatic ‘oh well, I’m sure it’s safe, they’ll sort it, if this is what happens, this is what’s happening’ response, and then insight:
“...I noticed with the muscle clenching, when I relaxed, and noticed it was clenching, I realised it was me clenching it? So, I could relax... As soon as I realised that, and I relaxed, that sort of went? Almost made me realise a lot of the pressure, I think, kind of indicated to me a lot of the pressure is my own doing... And it’s my own tension, it’s like... Yeah, like just, under my control? If that makes sense. Like I’m doing all the pressure, if I relax into things, and just, loosen up a bit, things get easier...”
She then recalled ‘lots of fighting’ in her mind over compulsions to overcome inhibitions with the therapists, like asking to dance or hold her hand, ‘because I’d never normally ask or know what I need’:
“It was weird. And it felt bad, like awkward and silly, but it got easier and... They were doing it as well, and it felt kind of alright by the end... Just like, trying things and... Tryna get out of this... Control... and everything.” (P1)
This unanimously reported ability to detach from and question their usual ED selves provides a compelling instance of change in self-experience through anxious ego-dissolution, bolstered by more neutral approaches via acute effects on cognition, sensory perception, and creativity of thought, thus consistent with findings regarding the dynamics of psychedelic experiences facilitating therapeutic outcomes (Preller & Vollenweider, 2016; 2020).
Altogether, participant accounts can be explained using Carhart-Harris & Friston’s (2019) REBUS model. Overweighted high-level priors and beliefs, such as compulsive ED thoughts and criticisms stemming from participants’ anxious-ego, seem relaxed. This would coincide with neuroimaging evidence of brain function alterations, particularly in the DMN, consistent with anxiolytic and antidepressant effects (Carhart-Harris et al., 2012). Potential alteration of DMN function could explain the intercepted high-level cortex constraining influences on participants’ perception, cognition, and emotion with spontaneous cortical activity. This possible explanation for participants’ creative approaches towards self-reflection and their ability to revise pathologically rigid beliefs in relaxed states suggests a key pathway through which PAT may hold relevance to EDs, by decompressing the mind.
Five participants linked this to ‘being able to establish’ ‘much healthier relationships with food’. P5 emphasised ‘becoming really interested in food and nourishing myself’ near the end of a trip, recalling how food became ‘absolutely incredible on acid’:
“I really got to explore something that was usually a very scary, threatening, complicated... Stressful thing in my life, in a totally new way and developing my relationship to it” (P5)
Taken together, the significant change in approach to food, a typically aversive stimuli, emphasised by five participants in addition to unanimous relaxed beliefs and ego-dissolution, these findings point towards the modulation of cognitive control and psychological flexibility delineated in Kelly’s (2021) review, congruent with the REBUS model. The example of food further supports the notion of psychedelic effects recalibrating hyper responsiveness in valence systems, responsible for emotional responses, often a ‘trigger’ reported by participants. Importantly, this finding is pertinent to both the nutritional and emotional dysregulation aspects of EDs, particularly since naturalistic psychedelic use is associated with relaxed emotional reactivity which could also translate towards food (Orlowski et al., 2022).
5.8. Subordinate Theme 2. ‘Navigating the Roadmap through Your Subconscious Emotion’
Participants unanimously emphasised abilities to access and ‘reprocess’ or ‘re-experience’ ‘buried’ or ‘blocked’ intense negative and/or positive emotions. This then enabled ‘forgiving’, ‘releasing’ and ‘letting go’ of ‘strong emotions’ from the source they linked to their ED or a ‘trigger’. This was a central process associated with emotional insight, enabling a ‘deeper healing’ than their usual ‘numb’, ‘critical’ or ‘serious’ states would allow:
“I was able to heal, a lot of the childhood trauma that led to the eating disorder, and... Understand, where it originated ... I just, was able to go back to being a child... Um, being traumatised by my mum, and, able to see her as a little girl, being traumatised by her mum. So, I was able to understand that this is generational trauma... And, I was able to just forgive, so much of that, and release it. And, I was angry, I was angry, a lot. And, and I took that anger out on myself, by, just punishing myself. But I don’t have any anger about that, anymore.” (P7)
P7 explained how ‘being shown the parts that are broken’ from ‘the shadows’ of her ‘subconscious’, and ‘seeing them in a different way’ enabled resolving trauma and releasing ‘all of that toxic negativity’, which gave her a ‘new sense of love’ for herself and ‘everything she had survived’:
“You know, making poor choices because I, I didn’t have any self-confidence, I had no self-esteem, I had no self-worth. And, it helped me to... Find, those parts of me that are there, and embrace them. And, love myself, more fully” (P7)
Participants demonstrated how their significant psychedelic experiences facilitated emotional processing and release, via visceral changes in self-experience of strong emotions, typically avoided by default and blocked out of conscious awareness. This finding is consistent with Vollenweider & Preller’s (2020) neurobiological evidence for contributing factors to therapeutic effects from the experience itself. This process circles back to traditional PAT assumptions that emotional insight is facilitated by relaxed ego defences, allowing unconscious material to transpire into awareness, reinstating its clinical relevance.
The ability to access, experience and reprocess supressed emotions is especially interesting, particularly where findings portray insights as to the root causes of EDs, accompanied with greater self-love and acceptance, consistent with ED and ayahuasca studies (Lafrance et al., 2017; Renelli, 2018; 2020). Given that high emotional avoidance associated with EDs (Cowdrey & Park, 2011) is overlooked in primary treatments (Dessain et al., 2019), this finding supports the clinical application of PAT for EDs.
Importantly, participants unanimously described being ‘able to feel’ or ‘realise’ ‘love’, ‘compassion’, ‘joy’ or ‘gratitude’ towards themselves or others as a significant experience, symbiotic with that of emotional pain coming into awareness. Five participants summarised love as the source of its healing effects. The ‘very strong emotional reactions’ were automatic, as P3 described, having ‘no control over’ journaling sources of ‘resentment and pain’, but was able to forgive, she ‘had to process it, and let it do its own thing’:
“Another thing was, if you don’t mind me sharing, when I was younger, I had an abortion. Um, and I was still holding on to the pain of that, that I didn’t, sorry *crying* I didn’t know that I was holding on to? Uh, and I forgave myself, during that trip. Which was very beautiful... I think, it just brings about more love. And therefore, you start to see the fears and illusions etc... To be honest, to summarise, I think it brings you closer to yourself... It helps you, love yourself, which then helps you love everyone else around you” (P3)
The notion of heightened emotional awareness and self-experience of unfamiliar positive emotions is further consistent with Kelly’s (2021) description of psychedelic action mechanisms that recalibrate deficiencies in emotional valence systems. This is significant given that a central function of EDs is to manage emotions via low emotional awareness or avoidance, addressing challenges faced by current treatments aiming to normalise behaviour and thought processes (Svaldi et al. 2012; Espel et al., 2016).
Additionally, six participants emphasised the challenge of having to ‘trust’ or ‘surrender’ as an essential precursor to the aforementioned ‘emotional insight’, amidst personal difficulties with ‘letting go’. P8 described ‘one of the most beautiful experiences’ ever had, explaining how grief had been ‘a real issue’ in her life that psilocybin allowed her to reexperience. She described ‘drowning’ in the trip due to ‘resisting’, before deciding to ‘surrender to the experience’ by allowing herself to drown:
“... wave after wave, as I fell into the grief, and I'm crying, I also accessed this profound love. And I realise that it's like the same thing. I'm grieving because I love, and then I felt elated and joy, gratitude, incredible gratitude. And just the gratitude in the surprise, wonder, ah, that holy cow, this is what I've been avoiding my whole life... Grieving.
And grief, surrender, letting go of what I thought was, true? It’s really a jumping off point, it’s really um, terrifying, and I was afraid of the pain of it, and I didn’t want to let go. I guess. It felt like I was letting go of the person... But. I found that when I let go of things... I was present. And my presence enabled me to... Well, my presence enabled everything.” (P8)
These findings demonstrate experiences of ego-dissolution, spiritual boundlessness and their effects on reducing anxious and fearful avoidant symptoms via acute effects on emotion and sensory perception (Preller & Vollenweider, 2016; 2020). This further supports the REBUS model assumption of disrupted DMN high-level behaviours, such as perspective taking, paired with significant notions of ‘letting go’ of control, allowing for spontaneous emotional insights that therapeutically influenced and relaxed participants’ long-held beliefs.
Taken together, participants’ accounts coincide with reports of ayahuasca experiences that enable intense root cause or emotional memory processing, leading to deeper ED healing of a spiritual nature, and improved emotional regulation (LaFrance et al., 2017; Renelli et al., 2018). The magnitude of emotional significance with positive affect, reported by five participants using psilocybin, further supports research suggesting that the most powerful (breakthrough or mystical) effects are associated with greater therapeutic outcomes (Roseman et al., 2018). Findings therefore demonstrate the importance of emotional breakthroughs and release during classic psychedelic experiences, as symbiotic with the revision of core beliefs that are inextricably linked to participants’ emotions and ED sypmtoms, thus serving to catalyse improved psychological functioning (Nutt, Erritzoe & Carhart-Harris, 2019; Roseman et al., 2019).
5.9. Subordinate Theme 3. Transcendence: ‘it’s Not a Theoretical Knowledge, It’s a Deep Knowing’
All participants experiences were transcendent in nature, five reported connecting to a loving, ‘supporting’ ‘higher power’ or ‘oneness’, providing insight and new views of life and death, existence and meaning, synonymous with profound feelings of ‘joy’ and ‘elation’.
“... they’re also really, like fun, and... Put you back in touch with what’s really, really beautiful about the world and people, and can be an incredibly moving, kind of connecting thing” (P5)
These accounts therefore reflect the occasioning and significant role of mystical experiences and subjective effects demonstrated in Johnson’s (2019) integrative review of meaningful therapeutic outcomes associated with psychedelics.
Participants’ experiences were accompanied by profound positive emotions that provided a sense of ‘reassurance’ and ‘hope’ behind ‘motivation’, frequently described as ‘putting things into perspective’. One participant described this as ‘very securing’, despite having ‘just died and come back’. She explained how this ‘deep knowing’, being ‘part of a bigger consciousness’ changes ‘self-perception’:
“...when you know that, all your, like your problems kind of pale into insignificance... A little bit, or they get put into perspective... A bit more... Like let go. Chill out, I’m self-sufficient, I’ll be fine whatever happens. I have so much life left, so make the most of it, don’t die early because of bulimia. I’m human, I don’t need perfection.” (P4)
One participant ‘in the heart of it’, recalled the effect of ‘full connection to a higher power’, telling her ‘it’s okay to be happy’, in reference to her depression as she broke into tears:
“And I think that was really, really powerful... But I feel like, it was less direct insight and more just a feeling of like... Connection, and unity, and things that... I feel like it helped... *crying*, my depression, more than it helped my eating disorder, but because they’re like comorbid, I feel like, it helped in turn”
She summarised the insight and impact on her perspective, influencing her ED symptoms:
“I think, its... To do with, joy, and... There’s so much, I think, it’s to do with the feeling of um... Life is so big, and I am so small, like, the things that I think really matter, don’t matter? Like, what I look like in a pair of jeans or like, if I’ve eaten like x, y, and z today... Like those things really don’t fucking matter in comparison to like the... Largeness of the universe, and the part that I have to play in it, and what matters is... Relationship, and connection, and... Making meaning of the things that happen to us... And I felt as though... That place, will always be there for me, but I still have work to do here... and that’s okay?” (P2)
P2’s emotional breakthrough and mood improvements induced by connecting to a higher power are consistent with fMRI studies on psilocybin and brain mechanisms in depression, indicating its role as a catalyst for notably enhanced psychological flexibility, openness, and connectedness (Carhart-Harris et al., 2017). Participants’ profundities and strong sense of unity experienced further relate to that of emotional ‘awe’, a discrete emotion analogous to mystical qualities and ego-dissolution, suggested to catalyse change (Hendricks, 2018).
Participants illustrated the downstream effects of mystical experiences, relative to their EDs and beliefs about domain-general narratives on the world, self, and states of being (Ruffini, 2017), having fostered a transcendental sense of connection to a higher oneness, others, and the world as a transformation point. The personal meaning participants attached to such transcendent experiences, in view of healing, may represent trickle-down effects on functional brain organisation systems. Therefore, positioning acute subjective effects of connectedness associated with mystical experiences as a potentially key mediator for psychological wellbeing, responsible for effective and enduring therapeutic outcomes (Cervinka et al., 2012; Carhart-Harris et al., 2018).
A reverend recalled emasculating a formation of cartoon men with a giant sword, which she connected to having ‘suffered a lot of abuse at the hands of men’, before ‘giving them their hearts back’, so they were ‘whole people, not the version of them that was horrible’ then seeing herself as a ‘goddess’, perceived as ‘being able to take her power back’:
“I think it was me, being able to understand that my experience of men has been, the ego aspect of men, and, this just showed me that you know, they have a higher self too, this isn’t who they really are? Um, and that they are shaped by a society that diminishes women, and... I don’t know, just helped me to... Forgive that. You know, to forgive the abuse that I’ve suffered, because ultimately, it’s all led me to this... This healing journey...
And, there’s just not, there’s just not a reality that I want to live in where I can’t forgive people. I don’t want to hold on to... Anger, and resentment, and, I think by, yes, castrating them and giving their heart back, was... A way for me to... Acknowledge that they are better than the person that they are in this lifetime.” (P7)
The reverends experience of empowering compassion and forgiveness from initial ‘resentful’ and ‘angry’ attitudes, further depicts the REBUS explanations for psychedelic enabled revision of core beliefs and emotions from a qualitative and subjective lens. These findings directly support Renelli’s (2018) findings of a deeper healing enabled via spiritual components and LaFrance’s (2021) of spirituality and emotional processing as mediators for ED, anxious and depressive symptoms - particularly when used intentionally to promote self- development by revising personal coping strategies and enhancing self-knowledge, as was the case for seven participants (Moro, 2011).
These findings illustrate how participants’ transcendent mystical experiences combined with ego- dissolution can shift beliefs towards the notion of spirituality, emphasised as a mediator for deeper healing and improved wellbeing by reducing emotional reactivity and self- consciousness (Orlowski et al., 2022). This translates into participants’ reduced symptom engagement and negative emotional reactivity, consistent with reports from life-time psychedelic users (LaFrance et al., 2021).
5.10. Superordinate Theme 2
‘Transformation’ and Being ‘Able to Do the Work’
All participants explicitly linked their psychedelic experiences to improved wellbeing. Effects were enduring for six participants and emphasised as more effective that any ED treatment previously received:
“...working with the medicine has really helped me a lot to release that (trauma), and I honestly feel better than I have... Since, before I can remember... Physically, mentally, emotionally, just all of it.”
‘Hard work’ was emphasised unanimously, varying between ‘support’ from peers, professionals, spiritual or creative therapeutic outlets:
“You still have to... Integrate those lessons, and... Catch yourself when you’re falling back into old negative thinking patterns, but it has certainly been a catalyst... To a deeper kind of heeling than I have ever experienced before, through any kinds of conventional methods” (P7)
Major personal shifts resulting in cessation or reduction of ED symptoms were described by seven as ‘profoundly’ ‘life changing’ and ‘transformative’:
“...My life has meaning. I connected with meaning that there was meaning even in my suffering itself, I think this was probably the most significant factor... I saw that I really needed to change. And what I didn't realise was, how much I would change. I'm not that person anymore. I see a thread to that person, but I cannot. I can't go back. Like I'm not worried that my depression or my eating disorder will remerge because I feel like I can't even find those pathways.” (P8)
This theme unpacks cognitive and behavioural ways such outcomes manifested, including safety perceptions, each presented as subthemes.
5.11. Subordinate Theme 1. Cognitive: ‘They’ve Opened Me Up’
Unanimous increased ‘motivation’, ‘hope’ and improved mental health was reported to varying degrees and durations following the ‘visceral experience’ that personal change was not ‘impossible’ or ‘unimaginable’ as participants believed, linked to mood improvements:
“They give me hope, which when... I’ve been struggling with addictions and bulimia for, so long, like hope, is... So cool to have, and is so important. Because, before I tried psychedelics, I was just hopeless, like I had no hope, I wanted to die, I really didn’t give a shit. And now, like, they’ve opened my life up, they’ve opened me up spiritually, which is incredibly important. They give me hope that one day recovery, like I know, that one day I will recover. And, they’ve also, given me a lot of really cool friends. Which is great. So, yeah, I’m very, very grateful.” (P4)
The notion of improved mood further highlighted the mediating role of spirituality reported by participants with significantly more positive outlooks is consistent with Spriggs (2021) quantitative data for lower depression and improved wellbeing scores following psychedelic experiences in people reporting to have had an ED. Key character changes around spirituality, emotional attitudes and creativity were also reported, supporting their roles in decreased symptom engagement or sustained remission demonstrated by LaFrance (2017). Altogether providing supportive evidence for psychedelic use, congruent with positive psychology studies, shifting domains such as personality, values, and mindfulness towards spirituality (Jungerbele, 2018).
This was symbiotic with internalising a ‘changed perspective on life’ and ‘priorities’, informed by ‘a sense of knowing as opposed to might be’ and the renewed possibility to ‘do the work’, thus facilitating healing for seven participants:
“I think for the first time, everything else in my brain got shut off, and I got to just actually just be there and feel it, and I think that sensation is sort of what motivates me in that, I sort of know what it feels like... Before, because I’d never felt like that, it was like not plausible, it was incomprehensible... And because I was allowed to have a taste of it, I now feel like I have something to work towards, whereas before it felt like impossible.” (P2)
This notion of actualising a broader perspective with motivating effects is an important illustration of how major changes in self-experience from psychedelic experiences can produce enduring improvements to mental health via revision of core beliefs (Roseman et al., 2019; Vollenweider & Preller, 2020). This renewed possibility of recovery reported by participants suggests the recalibration of highly weighted compressive functions associated with the maintenance of internalising disorder pathology (Carhart-Harris & Friston, 2019). Consistent with neurobiological evidence, this finding is clinically significant when considering the low motivational aspect of EDs in response to difficult emotions and the comorbid depressive symptoms associated with negative beliefs (Espel, 2016; Pisetsky et al, 2013).
Participant 5, who was more experienced with naturalistic psychedelic use, built on the notion of ‘seeing’ progressive outcomes and why this was so significant:
“Seeing that I have changed over time is really encouraging and encourages you to carry on trying because you know that like, even if progress is going to be slow, it does happen if you work at it, because when you've never experienced that kind of change before then it feels impossible. Because it's so relentless sometimes the thoughts so, the urges....” (P5)
They described how it helped them feel ‘very much more comfortable’ with their body and ‘finally got on top of bingeing’ after one particularly significant at-home ketamine experience four years ago. They did this with therapeutic intent to address their EDs, and went on to describe how LSD/acid had further contributed to nurturing aspects of their healing journey:
“Acid kind of..., sort of gave me permission to just like, be at home in my body, appreciate like, looking after myself and feeding myself and, it's hard to put into words, but you’re really kind of confronted by what you are... Which is a creature, like this weird, complicated, miraculous thing that that needs to absorb stuff from other stuff to exist” (P5)
P5’s account reflects extant reports of feeling more attuned to internal needs and inherent worth as a central process behind transformative experiences (Watts et al., 2017). Furthermore, the enduring positive effects resulting from participants naturalistic use, ‘integrated’ into their lives, indicates sustained mechanisms of divergent/creative thinking (Kuypers, 2016). This notion towards the long-lasting nature of improvements in wellbeing and mental health is also emphasised by population studies, whereby lifetime psychedelic users typically report significantly lower emotional difficulties, depressive, suicidal, and anxious tendencies, with greater life satisfaction than non-users (Krebs & Johansen, 2013; Hendricks et al., 2015) and reduced ED symptoms (LaFrance, 2021).
In terms of reduced symptomology, five participants reported ‘significant reductions’ in ‘intrusive thoughts’, ‘emotions’ and ‘urges’ that ‘would often lead’ to ED behaviours, or described it being ‘a lot easier to rationalise them’, which ‘changes everything’. This process reportedly facilitated the ‘healing’ that participants had been working on, which were previously challenging:
“My thoughts are not obsessive. And if they do get obsessive, I notice it. And I’m like oh... that’s interesting... wonderfully interesting. And then I move on... It’s... The ability to notice, it’s a DBT skill, notice, describe and participate... I would practice the skills, but they just didn’t click in a way that seemed like they should be... And I wasn’t present, I was avoiding. Yeah, I have to be present to experience, you have to be present to observe, and to participate... And I didn’t know how to bring myself present, I did everything I could think of.” (P8)
Obsessive-compulsive symptoms, anxiety and perfectionism are closely tied together with EDs (Frost & Dibartolo, 2002). The reductions in intrusive and compulsive cognitions reported are indicative of symptom decreases for EDs and the comorbid psychiatric disorders participants suffered, such as depression, anxiety, OCD, PTSD and SUD which in turn, hampered their ability to engage in conventional treatments. The positive effects of alleviating cognitive barriers on participants’ personal growth are consistent with therapeutic transdiagnostic outcomes lasting weeks-months for these comorbid internalising disorders (Anderson et al., 2020; Nutt, 2022).
In summary, the transdiagnostic healing effects described by participants suggest that Kelly’s (2021) proposal of PAPs transdiagnostic mechanisms from a research domain criteria framework (RDoc) has grounds for being developed further, using an integrative approach for understanding mental illness (Insel et al., 2010). Moreover, the fact that ED cognitions were reduced following participants’ emotional experiences perceived as relevant to the root causes of illness, emphasises criticisms of current symptom-focused treatments (Schenberg, 2018). Altogether, suggesting that the use of psychedelics combined with therapeutic work may incite more cognitive flexibility that allows for deeper personal insights, possibly enhancing traditional methods and adding weight to extant reports looking specifically at comparing conventional therapies with psychedelics (Renelli et al., 2020; LaFrance et al., 2021).
5.12. Subordinate Theme 2. Behavioural: ‘Start Making Changes’
All participants described behavioural changes resulting from feeling ‘able’ to ‘make changes’, ‘break habits’ and ‘do things differently’. Summarised by P7 as being able to ‘manage things in life I can control and letting go of things I can’t’. A recovered participant shared details of this process:
“... not just having the experience with psilocybin, but putting it into practice, in their lives. Start making changes, do a lot of writing, figure out what you need to transform and um the psilocybin will help the person to do that, and to be just completely honest. With themselves. I know that when it becomes chronic it’s learned, and you can unlearn it” (P8)
The notable improvements in psychological flexibility and cognitive symptoms facilitated participants’ active role in their personal development and wellbeing. This again reflects the notion of control circuits recalibrating as acute effects of the dysregulation of self-limiting beliefs and narratives subside (Nutt et al., 2020; Romeo et al., 2021). It suggests the modulation of participants’ serotonergic systems could be at play, associated with normalising dysfunctional systems by increasing brain network integration and manifesting in behavioural changes (Daws et al., 2022). That participants were significantly more able to change their habitual behaviours indicates major shifts from ED pathology.
When describing their outcomes, each brought up examples of personally meaningful behaviour changes to signal the extent of motivation they had to maintain wellbeing and manage their ED, with reduced ‘compulsive symptoms’ weeks/months onwards:
“After that journey, I just noticed that... Some of my compulsive um, symptoms, had dramatically reduced, as far as just obsessing about my weight...
...there were times when I would weigh myself 20, times a day *laughs* and that just seemed to... Kind of, evaporate. The need, to do that just, really was greatly diminished... So, I continued, using psilocybin mushrooms from then, about 7 times, and I had just... Been able to get to the point where I don’t weigh myself at all... Anymore.” (P7)
The enduring nature of reduced behavioural symptoms and improved wellbeing reported indicates significant potential for clinical use and is consistent with meta-analytic efficacy data for PAT, producing similarly long-lasting transdiagnostic therapeutic effects for all comorbid disorders that participants reported (Anderson et al., 2021; Luoma et al., 2020). This provides further preliminary evidence that transdiagnostic effects of PAT, capable of catalysing cognitive behavioural changes via spiritually emotionally meaningful pathways encompass EDs with sustaining outcomes, and should not be overlooked (Hendricks, 2018; Kelly et al., 2021).
Enduring effects were summarised by P4 as being ‘so full inside of like, good juju’ that the ‘urges are so much diminished’, having engaged in prosocial behaviours upon her return from psychedelic rehab. Her report also points towards the healing effects of community:
“I started getting involved with like, I went to Breaking Convention, and a couple of psychedelic meetups, and it was just like, eye opening, like it was a whole new world... I started volunteering for Psycare, and felt like I had found my tribe. Like, for the first time, in a long time. And my symptoms were just fine, I was completely normal... It was beyond, like words. I couldn’t even, like I’d never had that before. I was just absolutely okay?” (P4)
Despite relapsing six months later with comorbid SUD and ED symptoms after ‘a long string of very stressful events’, she described still finding it ‘easy just to eat’ normally, emphasising the importance of nutrition:
“... normally my body will feel quite stressed, and I’m rushing around, finding it quite hard to stay grounded, and... Connected, in the moment... But now, I just don’t put much drama into, like oh no, it has to be perfect, or has to be at a certain time, like I’m a lot more flexible with my food.”
Similarly, six participant reports pertaining to healthier lifestyles and/or diets, coinciding with suggestions of psychedelics inciting health behaviour changes (Teixeira et al., 2022) and alleviating ED symptoms. Furthermore, reports of reduced social anxiety and increased motivation to engage in activities and connect with external environments are consistent with findings of relaxed social information processing and beliefs that reduce prior inhibitory notions of social isolation, leading to prosocial effects associated with 5HT2A activity (Preller et al., 2016). Similarly, participants’ accounts involve interest in others and enhanced awareness of self-schemas, emotion, and interpersonal relationships (Pollan et al., 2018), altogether highlighting an important pathway through which wellbeing, lifestyle and support networks could be actively improved for people with EDs, following psychedelic experiences.
Moreover, six participants reported sustained outcomes and new prosocial commitments, ‘just doing things, meeting people, making friends, joining activities’ of meditative, spiritual, or creative natures. An art psychotherapist attributed her recovery from AN to recreational psychedelic use, which also catalysed her ‘creative process’ as an artist by ‘helping to connect to people’ and herself. She described psychedelics as a ‘meditative practice’:
“...after having this experience with my eating disorder, and being sort of more withdrawn from my creativity and my creative voice, it really connected me to that voice. And, profoundly changed um... The direction of my artwork? For quite some time, I didn’t really have the words, you know, to sort of, to really go into that process deeply, or. It didn’t flow as naturally, let’s put it that way. And it just seemed like um... Yeah, the dots were... Connected... I guess when I was battling with it, my perception was sort of more, um, introverted I guess, and then sort of expanded with the use, with the help of psychedelics” (P6)
In addition to improved social behaviours and attitudes directed towards spirituality and creativity, participant reports of behaviour changes hint towards shifts in personality, although only one participant reported lifetime psychedelic use and could signal this notion effectively. Her accounts are consistent with psychedelic induced mediating roles of anxious ego-dissolution on her personality and sustained recovery from AN, via acute effects on creativity and her sense of ‘connection’ to herself and her outer world, with no aversive side effects and overall improved wellbeing and mental health supporting the safety and value to positive psychology (LaFrance, 2021; Aday et al., 2020; Orwloski, 2022).
Taken together, seven participants reported sustained positive behaviour changes linked to psychedelic ASCs as previously discussed, encompassing mental clarity, emotional proccessing and mystical experiences. Given the similarities between experiences of change in the sense of self induced by meditation and psychedelics, it is intriguing to speculate that this disruption of self-narratives, thus control of intrusive thoughts, could mediate improved wellbeing in experienced meditators (Milliere, 2018). This is reflected in participants’ positive long-term outcomes pertaining to prosocial behaviours and individual traits, particularly increased empathy and compassion, thought to be antecedents of prosocial behaviour (Kreplin, 2018).
5.13. Subordinate Theme 3. Safety Perceptions: ‘Medicine’ but ‘Not a Magic Pill’
This theme is characterised by an overarching high regard for psychedelics that represented ‘healing’, ‘hope’ and ‘connection’ to participants, and that the ‘danger’ lies in the context of use. All participants emphasised the importance of ‘trusted’ environments and support for ‘integration’ and safety, reflecting current data and the perspectives of western ayahuasca ceremony facilitators (Murphy et al., 2022; Williams et al., 2024):
“…they mean… Healing. And they mean, medicine, and they mean connection, and they mean… Hope, and for me they feel like… A gift, that’s given to us? By like, the earth, and… I think, there’s danger of, putting all our hopes and dreams in the basket of like, if I eat this mushroom then my life is going to be like sorted and I’m gonna have no problems ever again… I think that is not what they’re there for, and I think they’re there to allow us to see some, the possibility. See possibility where we couldn’t see it before. Um, so I’d try not to put them on a pedestal, but um, I think they’re fucking cool.” (P2)
Seven participants expressed the importance of ‘respect’ for the ‘medicines’, ‘research’, ‘educating’ and ‘preparing’ themselves to appropriately ‘get the most’ of the ‘healing potential’ safely, while emphasising the important role of external support.
“The caution would be, make sure you do your research, and be with people that, you know you can trust… Um, and if somebody has severe mental or psychological problems, they need to work with a therapist or a doctor to make sure they’re gonna be safe doing that...” (P7)
The overall perception was that hazards lie in drug ‘abuse’, ‘mixing’ recreational drugs, or ‘trying to take medicine in a chaotic environment’ and without any support, inviting the risk of unmanageable outcomes that ‘could be traumatic for someone’. Although not personally experienced by participants, their safety perceptions coincide with current understandings that the same uncontrolled variables can result in adverse reactions and psychological distress (Ona, 2018). Participants’ emphasis on education and understanding of the ‘medicines’ reflect data on adverse effects, demonstrating that knowledge of the drug and dose predict a smaller risk for experiencing extended difficulties after-the-fact (Evans & Robinson et al., 2023). Altogether, participants’ safety perceptions reflect current understandings and clinical approaches that place guided settings, participant knowledge and support at the forefront (Nutt & Carhart Harris, 2021).
Also of importance was the magnitude of ‘unexpected’ change following positive outcomes, necessitating supportive resources. A pattern could be observed whereby older participants acknowledged the general benefits of conventional therapy, but seemed to place more personal value in spiritual, meditative, and creative therapeutic modalities and communities, having reached sustained cessation of symptoms. Younger participants emphasised a higher need for professional support/‘aftercare’ to manage wellbeing and integrate their experiences, with ‘the problem’ being ‘returning to normal life’, not ‘ideally set up for aftercare’:
“If I’m going to do psychedelics on my own at home, I’ll still get lessons, but it will be more spiritual lessons, or reflective lessons around my life, but my eating disorder is still… The symptoms will still be there. You know, even though I’ll have more knowledge… There symptoms will still be there. Whereas when I go to psychedelic rehab, the symptoms are reduced, and I get more knowledge. Just cause everything’s more intense in there” (P4)
The danger of not having adequate aftercare is reflected in P1’s account, having relapsed after her first and only psychedelic experience participating a clinical trial, which she now sees as ‘a wasted opportunity’ for her to ‘change’ when ‘there was a lot more possibility and hope’:
“…it didn’t feel like I was working on, it felt like I should’ve been working on problems and thinking… Like, new ways to behave and… Putting things into action, cause I felt really… Yeah just open to things and more… Like my brain was a lot more active and hopeful and stuff. But I didn’t know what to do with that, and then it sort of trailed off… and… It just feels, I feel almost worse now… Cause I feel really disappointed.” (P1)
P1’s experience from extreme high (feeling hopeful and happy having tangibly experienced higher autonomy and reduced symptoms) to low (end of trial, no longer having access to psychedelics, disappointment) raises an important risk of the hope and opportunity that clinical trials could represent for patients mid-trial, necessitating further aftercare, particularly with a MDD diagnosis. A review by Zeifman et al. (2021) suggests that recent clinical trials provide no evidence of increased suicidality but rather the contrary, however, McNamee et al. (2023) found increases of suicidal ideation and self-injury in over 7% of trial participants using MDMA and psilocybin. Consistent with research, P1 was the only participant reporting adverse effects and difficulties linked with feelings of anxiety, fear and existential struggle (Lake & Lucas, 2023). Interestingly, P1’s psychedelic experiences were notably darker, more fear/anxiety inducing and isolating than the rest, she frequently credited the support from trial therapists. Taken together, all participants and P1’s higher levels of difficulty during her trips and extended difficulty thereafter, reflect Evans & Robinson’s (2023) findings on difficulties after psychedelic use, that shorter duration of difficulties were predicted by lower levels of difficulty reported during the trip. P1’s case points towards the importance of aftercare/support, harm reduction and the need for further research into harms and mitigating risk (McNamee et al., 2023).
The other participants acknowledged the risk of ‘disappointment’, but from unrealistic expectations of a ‘magic pill’ outcome, without appreciating ‘it’s hard’ and ‘requires so much more than just taking a drug’. As P3 explained, ‘they showed me where I need to do the work, at its core, in order to tackle the ED’ rather than directly alleviating symptoms:
“So, if people take a psychedelic and think, oh I’m gonna be cured, then they’re in for a very rude awakening, because that’s not the way it works. You have to be determined to commitment. Determined to work hard.” (P3)
The therapeutic safety of psychedelics was confidently expressed. As was the case for seven, approaching psychedelics with clear therapeutic intention has long been associated with positive mental health outcomes (Haijen et al., 2018). Participants emphasis on the need for ‘doing the work’ outside of the psychedelic experience, this seems to refer to the critical therapeutic modalities and support they had referenced throughout. The psychotherapies and therapists that added to their sustained positive outcomes coincides with evidence that stronger therapeutic alliance may predict greater emotional breakthrough and mystical experiences, which in turn is associated with more positive and sustained therapeutic outcomes in patients with depression (Murphy et al., 2022). Taken together, findings reflect population studies supporting the general safety and benefit of use in both naturalistic and lab settings with participants further emphasising the importance of mind set, trusted settings and additional support (Johnson, 2019).
6. Summary
This research provides a supportive account of extant literature for the transdiagnostic therapeutic potential of psychedelics in the context of EDs and wellbeing, contributing to preliminary research and future clinical trials that address the urgency for novel treatment options (Spriggs et al., 2021; LaFrance, 2021; Himmerich et al., 2021). The present findings are most generalisable to people with AN and the therapeutic use of psilocybin due to majority of the sample having chronic AN, ranging from 11 to 42 years (M = 23.5). Findings suggest that psychedelic experiences hold significant therapeutic value, and that PAT could be a promising treatment to alleviate ED symptoms. These findings reflect current understandings that serotonergic psychedelics work via acute effects on cognitive and emotional controls, consequently facilitating higher motivation and efforts towards therapeutic engagement and improved wellbeing thereafter (Yaden & Griffiths, 2020; Roseman et al., 2018b; Renelli et al., 2020; Orlowski et al. 2022).
To be more specific, participants’ unanimous reductions or cessation of symptoms were largely connected to profound insights about their illness, life, and process of recovery during mystical experiences. This was followed by a seemingly automatic alleviation of compulsive cognitive and behavioural symptoms that could be maintained with consistent therapeutic and prosocial activity, coinciding with current understandings (LaFrance et al., 2017; Davis, Barrett & Griffiths, 2020; Nutt, 2022). These changes in self-experience were central to shifting rigid cognitions, attitudes and habits that were perpetuating participants’ symptoms. Such experiences bear important implications for therapeutic use, having enabled greater autonomy, positivity, self-love, compassion, and acceptance (Vollenweider & Preller, 2020; Carhartt-Harris & Friston, 2019).
Furthermore, the role and meaningfulness of the psychedelic phenomena itself seemed to be an important precursor to therapeutic outcomes via cognitive, emotional, and spiritual pathways that are typically constrained in EDs, as emphasised by present findings (Johnson et al., 2019; Svaldi et al., 2012; LaFrance, 2017). The fact such potential exists to experience dramatic changes in these domains provides strong grounding for further exploration to understand and develop scalable and accessible psychedelic healing modalities for EDs in the future.
The unanimous phenomenological accounts pertaining to emotional deficits, cognitive inflexibility, deeply ingrained behavioural patterns and perceived source of illness, emphasise the unique mechanisms of psychedelics in contrast to traditional interventions. This implicates the untapped potential for PAT modalities to address theoretical gaps and longstanding criticisms of symptom-focused ED treatments with low efficacy rates (Schenberg, 2018; Himmerich et al., 2021). These findings contribute to the emerging paradigm shift in psychiatry towards transdiagnostic therapeutic effects of psychedelics, postulated by accumulating research (Anderson et al., 2021; Luoma et al., 2020).
Consistent with the literature, it is clear that psychedelics have potential to induce enduring positive effects on mood, wellbeing, psychological flexibility, and personality traits (openness, spirituality, connectedness, mindfulness, creativity, and prosocial behaviours) for people with EDs as well as the wider populations studied (Jungarberle, 2018). Given the scope for meditative and spiritual complementary treatments for this population (Harding, 2022), the combined evidence suggests major potential for psychedelic use in facilitating the necessary cognitive, behavioural and lifestyle changes that could greatly enhance therapeutic effects of current interventions such as CBT or acceptance and commitment therapy (ACT) frequently used in PAT trials (Sloshower et al., 2019).
Moreover, that EDs are highly challenging to treat with complex aetiologies and trajectories, as reflected in our sample, Kelly’s (2021) transdiagnostic review delineating mechanisms through which psychedelic-assisted therapies may modulate cognitive control, psychological flexibility, and emotional valence systems from an RDoC perspective, further implies that integrating approaches to understand how psychedelics improve mental health may benefit understandings and future treatments for EDs and underlying causes.
7. Limitations
This study is not without limitations. Firstly, given the voluntary recruitment method, self-selection may have resulted in biased participant reports of positive effects. Although one participant did volunteer to report her adverse experiences, relapsing and being worse off after-the-fact, others that may have had inconsequential or negative experiences may choose to avoid the topic completely. Second, participants were relatively well-educated and emphasised the importance of ‘research’ before use, thus, insights may have been gleaned from personal reading, potentially inviting placebo effects. Third, the semi-structured interview prompts may have influenced participants’ reflections or prevented discussion of potentially relevant information, possibly resulting in demand characteristics. Additionally, due to the small sample size, subthemes for the wide breadth of content covered were kept relatively broad and may be reductive. Finally, that the study aimed to explore the range of psychedelics and EDs, the generalisability of findings is predominantly limited to AN and the psilocybin experiences of women.
8. Conclusions
This research supports current understandings about the therapeutic use of psychedelics. Importantly, findings shed light on the positive role that psychedelic experiences can play for people with chronic EDs along their recovery journey.
These preliminary findings indicate that a focus on more rigid and larger scale study into the effects of psychedelic experiences on ED symptoms would largely benefit future directions, clinical trials, and conclusions as to their unique therapeutic value. A particular focus on psilocybin and AN has emerged within this study, consistent with the literature and subsequent focus of clinical trials currently underway. It is also important to note that other EDs should not be excluded or overlooked from such study, given that they fit the same transdiagnostic research domain criteria (RDoC) systems perspective, and are frequently comorbid with AN, as reflected in the present sample which encompasses the full range of EDs (Kelly et al., 2021).
Overall, the data suggests that two serotonergic hallucinogens, psilocybin and ayahuasca, may hold the most clinical relevance to the potential treatment of EDs, along with the psychedelic experience itself as central to the healing process. The role of the psychedelic experience itself emerges as source of deep emotional insight and reflection that can catalyse significant cognitive and behavioural changes, manifesting as significantly reduced symptoms and more positive outlook on life. It is also important to note the critical role of additional support as an adjunctive to the sustained therapeutic outcomes observed in both extant and the present research on EDs and psychedelics. Put simply, the psychedelic experiences enabled more cognitive flexibility and presence, which in turn enabled participants to engage in established therapeutic modalities and prosocial behaviours that enhanced their lifestyles and wellbeing.
That all participants referenced psychedelics as an adjunctive modality to spiritual, meditative, creative, social and/or conventional therapeutic outlets, it is worth investigating how these modalities could integrate into current evidence-based treatments, such as CBT and ACT, adopting a more holistic approach to better suit this population's needs.
Additional attention can be drawn towards ayahuasca and DMT (the active compound within), considering extant evidence of ceremonial ayahuasca’s potential to alleviate or remit symptoms of various EDs (LaFrance et al., 2017; Renelli et al., 2018; 2020). This was consistent with three participants who were able to provide data on the compounds, seemingly with great therapeutic effect. P7 credits her ongoing sustained remission to ayahuasca ceremonies and psilocybin use, P6 credits her full recovery to her recreational use of DMT, psilocybin and MDMA, and P4 credits her 6-month sustained remission from her EDs and SUD to her experiences in psychedelic rehab using ayahuasca, 5-MEO-DMT and Ibogaine. The future study of both psilocybin and ayahuasca experiences in ED contexts could therefore enable more focused assessments of feasibility and application.
While this topic area is in its infancy and much remains to be explored, the unanimous reports of improved wellbeing, ranging between relief and full remission from chronic ED symptoms or lifelong recovery, is reason for optimism. Particularly for individuals that have not obtained effective results from standard treatments and have suffered for most of their adult lives, as was the case for this sample who suffered their EDs for 11-42 years (M = 23.5). This research therefore provides insight into some of the lived experiences of those suffering from EDs and the therapeutic role psychedelic experiences have played.
These findings are timely and relevant, warranting further inquiry for innovative treatment approaches using psychedelics. Most importantly, to inform future applications of psychedelic-assisted modalities, harm reduction, and aftercare developments.
9. Reflexivity Statement
I acknowledged my position as a qualitative researcher and wish to signal the subjective context of the study findings (Levitt et al., 2018). First, I must express my view that people with EDs are marginalised and stigmatised by society, thus the feasibility of attaining support and efficient treatment is extremely challenging, further perpetuating the vicious subjugation of the disease. Similarly, psychedelics are poorly understood, and people who use drugs are marginalised by drug prohibition. The overarching stigma poses a barrier to progression. I believe that people with lived experiences of EDs and psychedelics are of great value to research and should be empowered to influence novel treatments in a way that can benefit the population's unmet needs.
My pursuit of the study topic stemmed from epistemological values of intuitive inquiry that ‘incorporates intuitive and compassionate ways of knowing’, where ‘researchers listen to the prompting of their hearts about what to study and then listen with open hearts to the experiences relayed by others, attending to what speaks to them individually and collectively in the hope that their findings will serve the greater good’ (Anderson, 2019). I therefore acknowledged that my role, situated from an interpretivist ontology construing people, the world and reality as dialogically interrelated (Shaw, 2010), could have shaped the data more favourably towards the therapeutic potential of psychedelics for EDs, and thus registered any prior assumptions I held about the subject matter throughout the study.
I recognised that my perception of psychedelics was skewed towards assumptions based on the research followed and my own personal experiences that influenced my inquiry. I therefore maintained intentions to adopt a neutral stance to appropriately explore the variation in reports and effectively draw out any limitations and risks throughout data collection without projecting my own thoughts and emotions, in attempt to mitigate bias.
My interactions with the participants who spoke generously of their personal experiences had vibrantly informed my understanding of psychedelics in a therapeutic context for EDs. This was coloured by participant testimonies and unique insights into the various ways that psychedelics can take effect, that largely varied in relation to their lived experiences and perceived causes of suffering, all whilst headed in the direction of personal healing.
My assumption of PAT was directly challenged in discovering that, while professional support is indeed crucial, it is not essential for sustained ED remission or recovery with psychedelics, which is pertinent to the issue of affordability and access. I also noted challenges to my prior understanding of EDs through listening to the complex stories of others, some which resonated deeply and cast insight into my own experiences, for which I am grateful.
I acknowledge that this adds a personal dimension to the study, and therefore note that my interests and observations beyond the study partly informed my incentive to research this area and add weight to my support for continued research towards the application and accessibility of psychedelics in therapeutic contexts.
References
- Abramowitz, J.S.; Reuman, L. Obsessive compulsive disorder. Encyclopedia of personality and individual differences 2020, 3304–3306. [Google Scholar]
- Aday, J.S.; Mitzkovitz, C.M.; Bloesch, E.K.; Davoli, C.C.; Davis, A.K. Long term effects of psychedelic drugs: A systematic review. Neuroscience & Biobehavioral Reviews 2020, 113, 179–189. [Google Scholar]
- Ahn, J.; Lee, J.H.; Jung, Y.C. Predictors of suicide attempts in individuals with eating disorders. Suicide and Life-Threatening Behavior 2019, 49, 789–797. [Google Scholar] [CrossRef] [PubMed]
- Alonso, J.F.; Romero, S.; Mañanas M, À.; Riba, J. Serotonergic psychedelics temporarily modify information transfer in humans. International Journal of Neuropsychopharmacology 2015, 18, pyv039. [Google Scholar] [CrossRef]
- American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental Disorders, 5th edn. American Psychiatric Association, Washington.
- American Psychiatric Association (2013). Highlights of Changes from DSM-IV-TR to DSM 5. In Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: American Psychiatric Association.
- Anderson, C.B.; Carter, F.A.; McIntosh, V.V.; Joyce, P.R.; Bulik, C.M. Self harm and suicide attempts in individuals with bulimia nervosa. Eating Disorders 2002, 10, 227–243. [Google Scholar] [CrossRef] [PubMed]
- Andersen, K.A.; Carhart-Harris, R.; Nutt, D.J.; Erritzoe, D. Therapeutic effects of classic serotonergic psychedelics: A systematic review of modern-era clinical studies. Acta Psychiatrica Scandinavica 2021, 143, 101–118. [Google Scholar] [CrossRef]
- Anderson, R. Intuitive inquiry: Inviting transformation and breakthrough insights in qualitative research. Qualitative Psychology 2019, 6, 312–319. [Google Scholar] [CrossRef]
- Arcelus, J.; Mitchell, A.J.; Wales, J.; Nielsen, S. Mortality rates in patients with anorexia nervosa and other eating disorders: a meta-analysis of 36 studies. Archives of general psychiatry 2011, 68, 724–731. [Google Scholar] [CrossRef]
- Artin, H.; Zisook, S.; Ramanathan, D. How do serotonergic psychedelics treat depression: The potential role of neuroplasticity. World Journal of Psychiatry 2021, 11, 201. [Google Scholar] [CrossRef]
- Baer, R.A.; Smith, G.T.; Hopkins, J.; Krietemeyer, J.; Toney, L. Using self-report assessment methods to explore facets of mindfulness. Assessment 2006, 13, 27–45. [Google Scholar] [CrossRef]
- Beating Eating Disorders (BEAT) (2019). Lives at risk: The state of NHS adult community eating disorder services in England. Beating Eating Disorders (BEAT) & Maudsley Charity. https://beat.contentfiles.net/media/documents/lives-at-risk.pdf.
- Ben-Porath, D.; Duthu, F.; Luo, T.; Gonidakis, F.; Compte, E.J.; Wisniewski, L. Dialectical behavioral therapy: an update and review of the existing treatment models adapted for adults with eating disorders. Eating Disorders 2020, 28, 101–121. [Google Scholar] [CrossRef] [PubMed]
- Berkman, N.D.; Lohr, K.N.; Bulik, C.M. Outcomes of eating disorders: a systematic review of the literature. international Journal of Eating disorders 2007, 40, 293–309. [Google Scholar] [CrossRef] [PubMed]
- Bingham, A.J.; Witkowsky, P. (2022). Deductive and inductive approaches to qualitative data analysis. In C. Vanover, P. Mihas, & J. Saldaña (Eds.), Analyzing and interpreting qualitative data: After the interview (pp. 133-146). SAGE Publications.
- Bjornsson, A.S.; Didie, E.R.; Phillips, K.A. Body dysmorphic disorder. Dialogues in clinical neuroscience. 2022, 12, 221–232. [Google Scholar] [CrossRef] [PubMed]
- Bodell, L.P.; Joiner, T.E.; Keel, P.K. Comorbidity-independent risk for suicidality increases with bulimia nervosa but not with anorexia nervosa. Journal of psychiatric research 2013, 47, 617–621. [Google Scholar] [CrossRef]
- Bratland-Sanda, S.; Sundgot-Borgen, J. Eating disorders in athletes: overview of prevalence, risk factors and recommendations for prevention and treatment. European journal of sport science 2013, 13, 499–508. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qualitative research in psychology 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Conceptual and design thinking for thematic analysis. Qualitative Psychology 2022, 9, 3. [Google Scholar] [CrossRef]
- Breeksema, J.J.; Niemeijer, A.R.; Krediet, E.; Vermetten, E.; Schoevers, R.A. Psychedelic treatments for psychiatric disorders: a systematic review and thematic synthesis of patient experiences in qualitative studies. CNS drugs 2020, 34, 925–946. [Google Scholar] [CrossRef]
- Brewerton, T.D. Eating disorders, trauma, and comorbidity: Focus on PTSD. Eating disorders 2007, 15, 285–304. [Google Scholar] [CrossRef] [PubMed]
- Brewerton, T.D.; Wang, J.B.; Lafrance, A.; Pamplin, C.; Mithoefer, M.; Yazar-Klosinki, B.; Doblin, R. MDMA-assisted therapy significantly reduces eating disorder symptoms in a randomized placebo-controlled trial of adults with severe PTSD. Journal of Psychiatric Research 2022, 149, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Brown, T.A.; Wisniewski, L.; Anderson, L.K. Dialectical behavior therapy for eating disorders: State of the research and new directions. Eating Disorders 2020, 28, 97–100. [Google Scholar] [CrossRef] [PubMed]
- Callon, C.; Williams, M.; Lafrance, A. “Meeting the Medicine Halfway”: Ayahuasca Ceremony Leaders’ Perspectives on Preparation and Integration Practices for Participants. Journal of Humanistic Psychology 2021, 00221678211043300. [Google Scholar] [CrossRef]
- Campbell, K.; Peebles, R. Eating disorders in children and adolescents: state of the art review. Pediatrics 2014, 134, 582–592. [Google Scholar] [CrossRef]
- Carhart-Harris, R.L.; Bolstridge, M.; Rucker, J.; et al. (2016) Psilocybin with psychological support for treatment-resistant depression: an open-label feasibility study. Lancet Psychiatry. 2016, 3, 619–627. [Google Scholar] [CrossRef]
- Carhart-Harris, R.L.; Bolstridge, M.; Day CM, J.; Rucker, J.; Watts, R.; Erritzoe, D.E. , .. & Nutt, D.J. Psilocybin with psychological support for treatment-resistant depression: six-month follow-up. Psychopharmacology 2018, 235, 399–408. [Google Scholar]
- Carhart-Harris, R.L.; Erritzoe, D.; Haijen EC, H.M.; Kaelen, M.; Watts, R. Psychedelics and connectedness. Psychopharmacology 2018, 235, 547–550. [Google Scholar] [CrossRef]
- Carhart-Harris, R.L.; Erritzoe, D.; Williams, T.; et al. (2012) Neural correlates of the psychedelic state as determined by fMRI studies with psilocybin. Proc Natl Acad SciUSA. 2012, 109, 2138–2143. [Google Scholar] [CrossRef]
- Carhart-Harris, R.L.; Friston, K. REBUS and the anarchic brain: toward a unified model of the brain action of psychedelics. Pharmacological reviews 2019, 71, 316–344. [Google Scholar] [CrossRef]
- Carhart-Harris, R.; Giribaldi, B.; Watts, R.; Baker-Jones, M.; Murphy-Beiner, A.; Murphy, R. ,... & Nutt, D.J. Trial of psilocybin versus escitalopram for depression. New England Journal of Medicine 2021, 384, 1402–1411. [Google Scholar] [PubMed]
- Carhart-Harris, R.L.; Goodwin, G.M. The therapeutic potential of psychedelic drugs: past, present, and future. Neuropsychopharmacology 2017, 42, 2105–2113. [Google Scholar] [CrossRef]
- Carhart-Harris, R.L.; Leech, R.; Hellyer, P.J.; Shanahan, M.; Feilding, A.; Tagliazucchi, E. ,... & Nutt, D. The entropic brain: a theory of conscious states informed by neuroimaging research with psychedelic drugs. Frontiers in human neuroscience 2014, 20. [Google Scholar]
- Carhart-Harris, R.L.; Nutt, D.J. (2017) Serotonin and brain function: a tale of two receptors. J Psychopharmacol. 2017, 31, 1091–1120. [Google Scholar] [CrossRef]
- Carhart-Harris, R.L.; Roseman, L.; Bolstridge, M.; Demetriou, L.; Pannekoek, J.N.; Wall, M.B. ,... & Nutt, D.J. Psilocybin for treatment-resistant depression: fMRI measured brain mechanisms. Scientific reports 2017, 7, 1–11. [Google Scholar]
- Cervinka, R.; Röderer, K.; Hefler, E. Are nature lovers happy? On various indicators of well-being and connectedness with nature. Journal of health psychology 2012, 17, 379–388. [Google Scholar] [CrossRef] [PubMed]
- Cipriani, A.; Furukawa, T.A.; Salanti, G.; Chaimani, A.; Atkinson, L.Z.; Ogawa, Y. ,... & Geddes, J. R. Comparative efficacy and acceptability of 21 antidepressant drugs for the acute treatment of adults with major depressive disorder: a systematic review and network meta-analysis. Focus 2018, 16, 420–429. [Google Scholar]
- Close, J.B.; Bornemann, J.; Piggin, M.; Jayacodi, S.; Luan, L.X.; Carhart-Harris, R. , & Spriggs, M. J. Co-design of guidance for Patient and Public Involvement in Psychedelic Research. Frontiers in Psychiatry 2021, 1696. [Google Scholar]
- Cooper, Z.; Allen, E.; Bailey-Straebler, S.; Basden, S.; Murphy, R.; O’Connor, M.E.; Fairburn, C.G. Predictors and moderators of response to enhanced cognitive behaviour therapy and interpersonal psychotherapy for the treatment of eating disorders. Behaviour Research and Therapy 2016, 84, 9–13. [Google Scholar] [CrossRef]
- Cuerva, K.; Spirou, D.; Cuerva, A.; Delaquis, C.; Raman, J. Perspectives and preliminary experiences of psychedelics for the treatment of eating disorders: A systematic scoping review. European Eating Disorders Review. 2024. [Google Scholar] [CrossRef]
- Dahlenburg, S.C.; Gleaves, D.H.; Hutchinson, A.D. Treatment outcome research of enhanced cognitive behaviour therapy for eating disorders: a systematic review with narrative and meta-analytic synthesis. Eating Disorders 2019, 27, 482–502. [Google Scholar] [CrossRef]
- Davis, A.K.; Barrett, F.S.; Griffiths, R.R. Psychological flexibility mediates the relations between acute psychedelic effects and subjective decreases in depression and anxiety. Journal of contextual behavioral science 2020, 15, 39–45. [Google Scholar] [CrossRef]
- Davis, L.E.; Attia, E. (2019) Recent advances in therapies for eating disorders. F1000Research. [CrossRef]
- Daws, R.E.; Timmermann, C.; Giribaldi, B.; Sexton, J.D.; Wall, M.B.; Erritzoe, D. ,... & Carhart-Harris, R. Increased global integration in the brain after psilocybin therapy for depression. Nature medicine 2022, 28, 844–851. [Google Scholar] [PubMed]
- Dessain, A.; Bentley, J.; Treasure, J.; Schmidt, U.; Himmerich, H. Patients’ and Carers’ perspectives of psychopharmacological interventions targeting anorexia nervosa symptoms. Anorexia and Bulimia Nervosa 2019, 103. [Google Scholar]
- De Vos, C.M.; Mason, N.L.; Kuypers, K.P. Psychedelics and neuroplasticity: a systematic review unraveling the biological underpinnings of psychedelics. Frontiers in psychiatry 2021, 1575. [Google Scholar] [CrossRef] [PubMed]
- Domínguez-Clavé, E.; Soler, J.; Elices, M.; Franquesa, A.; Álvarez, E.; Pascual, J.C. Ayahuasca may help to improve self-compassion and self-criticism capacities. Human Psychopharmacology: Clinical and Experimental 2022, 37, e2807. [Google Scholar] [CrossRef]
- Dos Santos, R.G.; Osorio, F.L.; Crippa JA, S.; Hallak, J.E. Classical hallucinogens and neuroimaging: A systematic review of human studies: Hallucinogens and neuroimaging. Neuroscience & Biobehavioral Reviews 2016, 71, 715–728. [Google Scholar]
- Drummond, E.; McCulloch, W.; Knudsen, G.M.; Barrett, F.S.; Doss, M.K.; Carhart-Harris, R.L. ,... & Fisher, P.M. Psychedelic resting-state neuroimaging: a review and perspective on balancing replication and novel analyses. Neuroscience & Biobehavioral Reviews 2022, 104689. [Google Scholar]
- Dunn, T.M.; Bratman, S. On orthorexia nervosa: A review of the literature and proposed diagnostic criteria. Eating Behaviors 2016, 21, 11–17. [Google Scholar] [CrossRef]
- Dyck, E.; Elcock, C. Reframing bummer trips: scientific and cultural explanations to adverse reactions to psychedelic drug use. The Social History of Alcohol and Drugs 2020, 34, 271–296. [Google Scholar] [CrossRef]
- Eskander, N.; Limbana, T.; Khan, F. Psychiatric comorbidities and the risk of suicide in obsessive-compulsive and body dysmorphic disorder. Cureus 2020, 12. [Google Scholar] [CrossRef] [PubMed]
- Espel, H.M.; Goldstein, S.P.; Manasse, S.M.; Juarascio, A.S. Experiential acceptance, motivation for recovery, and treatment outcome in eating disorders. Eating and Weight Disorders-Studies on Anorexia, Bulimia and Obesity 2016, 21, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Fairburn, C.G.; Cooper, Z.; Shafran, R. Cognitive behaviour therapy for eating disorders: A “transdiagnostic” theory and treatment. Behaviour research and therapy 2003, 41, 509–528. [Google Scholar] [CrossRef] [PubMed]
- Fassino, S.; Pierò, A. , … & Tomba, E. Factors associated with dropout from treatment for eating disorders: a comprehensive literature review. BMC Psychiatry 2009, 9, 67. [Google Scholar] [CrossRef]
- Flanagan, T.W.; Nichols, C.D. Psychedelics as anti-inflammatory agents. International Review of Psychiatry 2018, 30, 363–375. [Google Scholar] [CrossRef] [PubMed]
- Foldi, C.J.; Liknaitzky, P.; Williams, M.; Oldfield, B.J. Rethinking therapeutic strategies for anorexia nervosa: insights from psychedelic medicine and animal models. Frontiers in Neuroscience 2020, 14, 43. [Google Scholar] [CrossRef] [PubMed]
- Frank GK, W. Altered brain reward circuits in eating disorders: chicken or egg? Current Psychiatry Reports 2013, 15. [Google Scholar] [CrossRef]
- Frank, G.K.; Shott, M.E.; DeGuzman, M.C. The Neurobiology of eating disorders. Child and Adolescent Psychiatric Clinics of North America 2019, 28, 629–640. [Google Scholar] [CrossRef]
- Frost, R.O.; DiBartolo, P.M. (2002). Perfectionism, anxiety, and obsessive-compulsive disorder. In G. L. Flett & P. L. Hewitt (Eds.), Perfectionism: Theory, research, and treatment (pp. 341–371). American Psychological Association. [CrossRef]
- Galmiche, M.; Déchelotte, P.; Lambert, G.; Tavolacci, M.P. Prevalence of eating disorders over the 2000–2018 period: a systematic literature review. The American journal of clinical nutrition 2019, 109, 1402–1413. [Google Scholar] [CrossRef]
- Galvão-Coelho, N.L.; Marx, W.; Gonzalez, M.; Sinclair, J.; de Manincor, M.; Perkins, D.; Sarris, J. Classic serotonergic psychedelics for mood and depressive symptoms: a meta-analysis of mood disorder patients and healthy participants. Psychopharmacology 2021, 238, 341–354. [Google Scholar] [CrossRef]
- Gill, H.; Puramat, P.; Patel, P.; Gill, B.; Marks, C.A.; Rodrigues, N.B. ,... & McIntyre, R.S. The Effects of Psilocybin in Adults with Major Depressive Disorder and The General Population. Psychiatry Research 2022, 114577. [Google Scholar]
- Griffiths, R.R.; Hurwitz, E.S.; Davis, A.K.; Johnson, M.W.; Jesse, R. Survey of subjective" God encounter experiences": Comparisons among naturally occurring experiences and those occasioned by the classic psychedelics psilocybin, LSD, ayahuasca, or DMT. PloS one 2019, 14, e0214377. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, R.R.; Johnson, M.W.; Carducci, M.A.; Umbricht, A.; Richards, W.A.; Richards, B.D. ,... & Klinedinst, M.A. Psilocybin produces substantial and sustained decreases in depression and anxiety in patients with life-threatening cancer: A randomized double-blind trial. Journal of psychopharmacology 2016, 30, 1181–1197. [Google Scholar] [PubMed]
- Griffiths, R.R.; Richards, W.A.; Johnson, M.W.; McCann, U.D.; Jesse, R. Mystical-type experiences occasioned by psilocybin mediate the attribution of personal meaning and spiritual significance 14 months later. Journal of psychopharmacology 2008, 22, 621–632. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, R.R.; Richards, W.A.; McCann, U.; Jesse, R. Psilocybin can occasion mystical-type experiences having substantial and sustained personal meaning and spiritual significance. Psychopharmacology 2006, 187, 268–283. [Google Scholar] [CrossRef]
- Harding, F.; Seynaeve, M.; Keeler, J.; Himmerich, H.; Treasure, J.; Kan, C. Perspectives on psychedelic treatment and research in eating disorders: a web-based questionnaire study of people with eating disorders. Journal of integrative neuroscience 2021, 20, 551–560. [Google Scholar]
- Hartogsohn, I. The meaning-enhancing properties of psychedelics and their mediator role in psychedelic therapy, spirituality, and creativity. Frontiers in neuroscience 2018, 12, 129. [Google Scholar] [CrossRef]
- Hendricks, P.S. Awe: A putative mechanism underlying the effects of classic psychedelic-assisted psychotherapy. International Review of Psychiatry 2018, 30, 331–342. [Google Scholar] [CrossRef]
- Hendricks, P.S.; Copes, H.; Family, N.; Williams, L.T.; Luke, D.; Raz, S. Perceptions of safety, subjective effects, and beliefs about the clinical utility of lysergic acid diethylamide in healthy participants within a novel intervention paradigm: Qualitative results from a proof-of-concept study. Journal of Psychopharmacology 2022, 36, 337–347. [Google Scholar] [CrossRef]
- Himmerich, H.; Bentley, J.; Kan, C.; Treasure, J. Genetic risk factors for eating disorders: an update and insights into pathophysiology. Therapeutic advances in psychopharmacology 2019, 9, 2045125318814734. [Google Scholar] [CrossRef]
- Himmerich, H.; Kan, C.; Au, K.; Treasure, J. Pharmacological treatment of eating disorders, comorbid mental health problems, malnutrition and physical health consequences. Pharmacology & therapeutics 2021, 217, 107667. [Google Scholar]
- Himmerich, H.; Treasure, J. Psychopharmacological advances in eating disorders. Expert review of clinical pharmacology 2018, 11, 95–108. [Google Scholar] [CrossRef] [PubMed]
- Hoek, H.W. Incidence, prevalence and mortality of anorexia nervosa and other eating disorders. Current opinion in psychiatry 2006, 19, 389–394. [Google Scholar] [CrossRef] [PubMed]
- Hudson, J.I.; Hiripi, E.; Pope Jr, H.G.; Kessler, R.C. The prevalence and correlates of eating disorders in the National Comorbidity Survey Replication. Biological psychiatry 2007, 61, 348–358. [Google Scholar] [CrossRef] [PubMed]
- Insel, T.; Cuthbert, B.; Garvey, M.; Heinssen, R.; Pine, D.S.; Quinn, K. ,... & Wang, P. Research domain criteria (RDoC): toward a new classification framework for research on mental disorders. American Journal of psychiatry 2010, 167, 748–751. [Google Scholar]
- Ioannidis, J. Effectiveness of antidepressants: an evidence myth constructed from a thousand randomized trials? Philosophy, Ethics, and Humanities in Medicine 2008, 3, 1–9. [Google Scholar] [CrossRef]
- Johnson, M.W.; Garcia-Romeu, A.; Griffiths, R.R. Long-term follow-up of psilocybin-facilitated smoking cessation. The American Journal of Drug and Alcohol Abuse 2017, 43, 55–60. [Google Scholar] [CrossRef]
- Johnson, M.W.; Hendricks, P.S.; Barrett, F.S.; Griffiths, R.R. Classic psychedelics: An integrative review of epidemiology, therapeutics, mystical experience, and brain network function. Pharmacology & therapeutics 2019, 197, 83–102. [Google Scholar]
- Jungaberle, H.; Thal, S.; Zeuch, A.; Rougemont-Bücking, A.; von Heyden, M.; Aicher, H.; Scheidegger, M. Positive psychology in the investigation of psychedelics and entactogens: A critical review. Neuropharmacology 2018, 142, 179–199. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. Mindfulness-based interventions in context: Past, present, and future. Clinical Psychology: Science and Practice 2003, 10, 144–156. [Google Scholar] [CrossRef]
- Karjalainen, L.; Gillberg, C.; Råstam, M.; Wentz, E. Eating disorders and eating pathology in young adult and adult patients with ESSENCE. Comprehensive Psychiatry 2016, 66, 79–86. [Google Scholar] [CrossRef]
- Kelly, J.R.; Gillan, C.M.; Prenderville, J.; Harkin, A.; Clarke, G.; O'Keane, V. Psychedelic therapy's Transdiagnostic effects: A Research Domain Criteria (RDoC) Systems Perspective. Frontiers in Psychiatry 2021, 2295. [Google Scholar] [CrossRef] [PubMed]
- Knudsen, G.M. Sustained effects of single doses of classical psychedelics in humans. Neuropsychopharmacology 2022, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Koning, E.; Brietzke, E. Psilocybin-Assisted Psychotherapy as a Potential Treatment for Eating Disorders: a Narrative Review of Preliminary Evidence. Trends in Psychiatry and Psychotherapy. 2023. [Google Scholar] [CrossRef] [PubMed]
- Krebs, T.S.; Johansen P, Ø. Psychedelics and mental health: a population study. PloS one 2013, 8, e63972. [Google Scholar] [CrossRef]
- Kreplin, U.; Farias, M.; Brazil, I.A. The limited prosocial effects of meditation: A systematic review and meta-analysis. Scientific reports 2018, 8, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Lafrance, A.; Loizaga-Velder, A.; Fletcher, J.; Renelli, M.; Files, N.; Tupper, K.W. Nourishing the spirit: exploratory research on ayahuasca experiences along the continuum of recovery from eating disorders. Journal of psychoactive drugs 2017, 49, 427–435. [Google Scholar] [CrossRef]
- Lafrance, A.; Strahan, E.; Bird, B.M.; St Pierre, M.; Walsh, Z. Classic Psychedelic Use and Mechanisms of Mental Health: Exploring the Mediating Roles of Spirituality and Emotion Processing on Symptoms of Anxiety, Depressed Mood, and Disordered Eating in a Community Sample. Journal of Humanistic Psychology 2021. [Google Scholar] [CrossRef]
- Lebedev, A.V.; Lövdén, M.; Rosenthal, G.; Feilding, A.; Nutt, D.J.; Carhart-Harris, R.L. Finding the self by losing the self: Neural correlates of ego-dissolution under psilocybin. Human brain mapping 2015, 36, 3137–3153. [Google Scholar] [CrossRef]
- Leichsenring, F.; Luyten, P.; Hilsenroth, M.J.; Abbass, A.; Barber, J.P.; Keefe, J.R.; Leweke, F.; Rabung, S.; Steinert, C. Psychodynamic therapy meets evidence-based medicine: a systematic review using updated criteria. The Lancet Psychiatry 2015, 2, 648–660. [Google Scholar] [CrossRef]
- Levitt, H.M.; Bamberg, M.; Creswell, J.W.; Frost, D.M.; Josselson, R.; Suárez-Orozco, C. Journal article reporting standards for qualitative primary, qualitative meta analytic, and mixed methods research in psychology: The APA Publications and Communications Board task force report. American Psychologist 2018, 73, 26–46. [Google Scholar] [CrossRef]
- Linardon, J.; Fairburn, C.G.; Fitzsimmons-Craft, E.E.; Wilfley, D.E.; Brennan, L. The empirical status of the third-wave behaviour therapies for the treatment of eating disorders: A systematic review. Clinical psychology review 2017, 58, 125–140. [Google Scholar] [CrossRef] [PubMed]
- Linardon, J.; Hindle, A.; Brennan, L. Dropout from cognitive-behavioral therapy for eating disorders: A meta-analysis of randomized, controlled trials. International Journal of Eating Disorders 2018, 51, 381–391. [Google Scholar] [CrossRef] [PubMed]
- Luoma, J.B.; Chwyl, C.; Bathje, G.J.; Davis, A.K.; Lancelotta, R. A meta analysis of placebo-controlled trials of psychedelic-assisted therapy. Journal of Psychoactive Drugs 2020, 52, 289–299. [Google Scholar] [CrossRef] [PubMed]
- Ly, C.; Greb, A.C.; Cameron, L.P.; Wong, J.M.; Barragan, E.V.; Wilson, P.C. ,... & Olson, D. E. Psychedelics promote structural and functional neural plasticity. Cell reports 2018, 23, 3170–3182. [Google Scholar]
- Machek, S.B. Psychedelics: Overlooked Clinical Tools with Unexplored Ergogenic Potential. Journal of Exercise and Nutrition 2019, 2. [Google Scholar]
- Malcolm, B.; Thomas, K. Serotonin toxicity of serotonergic psychedelics. Psychopharmacology 2021, 1–11. [Google Scholar] [CrossRef]
- McElroy, S.L.; Guerdjikova, A.I.; Mori, N.; Keck, P.E. Psychopharmacologic treatment of eating disorders: emerging findings. Current Psychiatry Reports 2015, 17, 1–7. [Google Scholar] [CrossRef]
- Michael, P.; Luke, D.; Robinson, O. An encounter with the other: A thematic and content analysis of DMT experiences from a naturalistic field study. Frontiers in psychology 2021, 5731. [Google Scholar] [CrossRef]
- Millière, R.; Carhart-Harris, R.L.; Roseman, L.; Trautwein, F.M.; Berkovich-Ohana, A. Psychedelics, meditation, and self-consciousness. Frontiers in psychology 2018, 9, 1475. [Google Scholar] [CrossRef]
- Mind. Treatment and support for eating problems. https://www.mind.org.uk/information-support/types-of-mental-healthproblems/eating-problems/treatment-support/ 2021.
- Moessner, M.; Bauer, S. (2017). Maximizing the public health impact of eating disorder services: a simulation study. International Journal of Eating Disorders 2021, 50, 1378–1384. [Google Scholar] [CrossRef]
- Monge, M.C.; Forman, S.F.; McKenzie, N.M.; Rosen, D.S.; Mammel, K.A.; Callahan S, T. ,... & Woods, E.R. Use of psychopharmacologic medications in adolescents with restrictive eating disorders: analysis of data from the National Eating Disorder Quality Improvement Collaborative. Journal of Adolescent Health 2015, 57, 66–72. [Google Scholar]
- Monteleone, A.M.; Pellegrino, F.; Croatto, G.; Carfagno, M.; Hilbert, A.; Treasure, J.; Wade, T.; Bulik, C.M.; Zipfel, S.; Hay, P.; Schmidt, U.; Castellini, G.; Favaro, A.; Fernandez-Aranda, F.; Shin, J.I.; Voderholzer, U.; Ricca, V.; Moretti, D.; Busatta, D. ,... Solmi, M. Treatment of eating disorders: A systematic meta-review of meta-analyses and network meta-analyses. Neuroscience & Biobehavioral Reviews 2022, 142, 104857. [Google Scholar] [CrossRef]
- Moreton, S.G.; Burden-Hill, A.; Menzies, R.E. Reduced death anxiety and obsessive beliefs as mediators of the therapeutic effects of psychedelics on obsessive compulsive disorder symptomology. Clinical Psychologist 2022, 1–16. [Google Scholar] [CrossRef]
- Murphy, R.; Kettner, H.; Zeifman, R.; Giribaldi, B.; Kartner, L.; Martell, J.; Read, T.; Murphy-Beiner, A.; Baker-Jones, M.; Nutt, D.; Erritzoe, D.; Watts, R.; Carhart-Harris, R. Therapeutic Alliance and Rapport Modulate Responses to Psilocybin Assisted Therapy for Depression. Frontiers in pharmacology 2022, 12, 788155. [Google Scholar] [CrossRef] [PubMed]
- Murphy-Beiner, A. , & Soar, K. Ayahuasca’s ‘afterglow’: improved mindfulness and cognitive flexibility in ayahuasca drinkers. Psychopharmacology 2020, 237, 1161–1169. [Google Scholar]
- Muttoni, S.; Ardissino, M.; John, C. Classical psychedelics for the treatment of depression and anxiety: A systematic review. Journal of affective disorders 2019, 258, 11–24. [Google Scholar] [CrossRef]
- National Library of Medicine (U.S.). (2019, August). Effects of Psilocybin in Anorexia Nervosa. Identifier NCT04052568. https://clinicaltrials.gov/ct2/show/NCT04052568.
- National Library of Medicine (U.S.). (2021, May). Psilocybin as a Treatment for Anorexia Nervosa: A Pilot Study. Identifier NCT04505189. https://clinicaltrials.gov/ct2/show/NCT04505189.
- National Library of Medicine (U.S.). (2022, August). Efficacy and Safety of COMP360 Psilocybin Therapy in Anorexia Nervosa: A Proof-Of-Concept Study. Identifier NCT05481736. https://clinicaltrials.gov/ct2/show/NCT05481736.
- Nichols, D.E. Psychedelics. Pharmacological reviews 2016, 68, 264–355. [Google Scholar] [CrossRef] [PubMed]
- Nichols, D.E.; Johnson, M.W.; Nichols, C.D. Psychedelics as medicines: an emerging new paradigm. Clinical Pharmacology & Therapeutics 2017, 101, 209–219. [Google Scholar]
- Nutt, D. Illegal drugs laws: clearing a 50-year-old obstacle to research. PLoS biology 2015, 13, e1002047. [Google Scholar] [CrossRef]
- Nutt, D. Psychedelic drugs—a new era in psychiatry? Dialogues in clinical neuroscience. 2022, 21, 139–147. [Google Scholar] [CrossRef]
- Nutt, D.; Carhart-Harris, R. The current status of psychedelics in psychiatry. JAMA psychiatry 2021, 78, 121–122. [Google Scholar] [CrossRef] [PubMed]
- Nutt, D.; Erritzoe, D.; Carhart-Harris, R. Psychedelic psychiatry’s brave new world. Cell 2020, 181, 24–28. [Google Scholar] [CrossRef]
- Olson, D.E. The subjective effects of psychedelics may not be necessary for their enduring therapeutic effects. ACS Pharm Trans Sci 2020, 4, 563–567. [Google Scholar] [CrossRef]
- Ona, G. Inside bad trips: Exploring extra-pharmacological factors. Journal of Psychedelic Studies 2018, 2, 53–60. [Google Scholar] [CrossRef]
- Orłowski, P.; Ruban, A.; Szczypiński, J.; Hobot, J.; Bielecki, M.; Bola, M. Naturalistic use of psychedelics is related to emotional reactivity and self consciousness: The mediating role of ego-dissolution and mystical experiences. Journal of Psychopharmacology 2022, 02698811221089034. [Google Scholar] [CrossRef] [PubMed]
- Parliament Publications. House of Commons Public Administration and Constitutional Affairs Committee. (2019). Ignoring the Alarms follow-up: Too many avoidable deaths from eating disorders (Seventeenth Report of Session 2017–19). https://publications.parliament.uk/pa/cm201719/cmselect/cmpubadm/855/855.pdf.
- Patton, M.Q. (2002). Qualitative research & evaluation methods. SAGE Publications.
- Preller, K.H.; Vollenweider, F.X. Phenomenology, structure, and dynamic of psychedelic states. Behavioral neurobiology of psychedelic drugs 2016, 221–256. [Google Scholar]
- Pisetsky, E.M.; Thornton, L.M.; Lichtenstein, P.; Pedersen, N.L.; Bulik, C.M. Suicide attempts in women with eating disorders. Journal of abnormal psychology 2013, 122, 1042. [Google Scholar] [CrossRef]
- Reiff, C.M.; Richman, E.E.; Nemeroff, C.B.; Carpenter, L.L.; Widge, A.S.; Rodriguez C, I. ,... & Work Group on Biomarkers and Novel Treatments, a Division of the American Psychiatric Association Council of Research. Psychedelics and psychedelic-assisted psychotherapy. American Journal of Psychiatry 2020, 177, 391–410. [Google Scholar]
- Renelli, M.; Fletcher, J.; Loizaga-Velder, A.; Files, N.; Tupper, K.; Lafrance, A. (2018). Ayahuasca and the healing of eating disorders. In Embodiment and eating disorders (pp. 214-230). Routledge.
- Renell, M.; Fletcher, J.; Tupper, K.W.; Files, N.; Loizaga-Velder, A.; Lafrance, A. An exploratory study of experiences with conventional eating disorder treatment and ceremonial ayahuasca for the healing of eating disorders. Eating and Weight Disorders-Studies on Anorexia,Bulimia and Obesity 2020, 25, 437–444. [Google Scholar] [CrossRef]
- Renelli, M.; Fletcher, J.; Tupper, K.W.; Files, N.; Loizaga-Velder, A.; Lafrance, A. An exploratory study of experiences with conventional eating disorder treatment and ceremonial ayahuasca for the healing of eating disorders. Eating and Weight Disorders-Studies on Anorexia, Bulimia and Obesity 2018, 1–8. [Google Scholar] [CrossRef]
- Renelli, M.; Fletcher, J.; Tupper, K.W.; Files, N.; Loizaga-Velder, A.; Lafrance, A. An exploratory study of experiences with conventional eating disorder treatment and ceremonial ayahuasca for the healing of eating disorders. Eating and Weight Disorders-Studies on Anorexia, Bulimia and Obesity 2020, 25, 437–444. [Google Scholar] [CrossRef] [PubMed]
- Rome, E.S.; Ammerman, S. Medical complications of eating disorders: an update. Journal of adolescent health 2003, 33, 418–426. [Google Scholar] [CrossRef]
- Romeo, B.; Hermand, M.; Pétillion, A.; Karila, L.; Benyamina, A. Clinical and biological predictors of psychedelic response in the treatment of psychiatric and addictive disorders: A systematic review. Journal of Psychiatric Research 2021, 137, 273–282. [Google Scholar] [CrossRef]
- Romeo, B.; Karila, L.; Martelli, C.; Benyamina, A. Efficacy of psychedelic treatments on depressive symptoms: A meta-analysis. Journal of Psychopharmacology 2020, 34, 1079–1085. [Google Scholar] [CrossRef] [PubMed]
- Root, T.L.; Pisetsky, E.M.; Thornton, L.; Lichtenstein, P.; Pedersen, N.L.; Bulik, C. Patterns of co-morbidity of eating disorders and substance use in Swedish females. Psychological medicine 2010, 40, 105–115. [Google Scholar] [CrossRef]
- Roseman, L.; Haijen, E.; Idialu-Ikato, K.; Kaelen, M.; Watts, R.; Carhart-Harris, R. Emotional breakthrough and psychedelics: validation of the emotional breakthrough inventory. Journal of Psychopharmacology 2019, 33, 1076–1087. [Google Scholar] [CrossRef]
- Roseman, L.; Nutt, D.J.; Carhart-Harris, R.L. Quality of acute psychedelic experience predicts therapeutic efficacy of psilocybin for treatment-resistant depression. Frontiers in pharmacology 2018, 8, 974. [Google Scholar] [CrossRef]
- Ross, S.; Bossis, A.; Guss, J.; Agin-Liebes, G.; Malone, T.; Cohen, B. ,... & Schmidt, B.L. Rapid and sustained symptom reduction following psilocybin treatment for anxiety and depression in patients with life-threatening cancer: a randomized controlled trial. Journal of psychopharmacology 2016, 30, 1165–1180. [Google Scholar]
- Rucker, J.J.; Iliff, J.; Nutt, D.J. Psychiatry & the psychedelic drugs. Past, present & future. Neuropharmacology 2018, 142, 200–218. [Google Scholar]
- Rucker, J.J.; Marwood, L.; Ajantaival RL, J.; Bird, C.; Eriksson, H.; Harrison, J. ,... & Young, A. H. The effects of psilocybin on cognitive and emotional functions in healthy participants: results from a phase 1, randomised, placebo-controlled trial involving simultaneous psilocybin administration and preparation. Journal of Psychopharmacology 2019, 02698811211064720. [Google Scholar]
- Schenberg, E.E. Psychedelic-assisted psychotherapy: a paradigm shift in psychiatric research and development. Frontiers in pharmacology 2018, 9, 733. [Google Scholar] [CrossRef] [PubMed]
- Schimmel, N.; Breeksema, J.J.; Smith-Apeldoorn, S.Y.; Veraart, J.; van den Brink, W.; Schoevers, R.A. Psychedelics for the treatment of depression, anxiety, and existential distress in patients with a terminal illness: a systematic review. Psychopharmacology 2021, 1–19. [Google Scholar]
- Schlag, A.K.; Aday, J.; Salam, I.; Neill, J.C.; Nutt, D.J. Adverse effects of psychedelics: From anecdotes and misinformation to systematic science. Journal of Psychopharmacology 2022, 36, 258–272. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, U.; Adan, R.; Böhm, I.; Campbell, I.C.; Dingemans, A.; Ehrlich, S. ,... & Zipfel, S. Eating disorders: the big issue. The Lancet Psychiatry 2016, 3, 313–315. [Google Scholar] [PubMed]
- Shalev, A.; Liberzon, I.; Marmar, C. Post-traumatic stress disorder. New England journal of medicine 2017, 376, 2459–2469. [Google Scholar] [CrossRef]
- Smink, F.R.; van Hoeken, D.; Hoek, H.W. Epidemiology, course, and outcome of eating disorders. Current opinion in psychiatry 2013, 26, 543–548. [Google Scholar] [CrossRef]
- Södersten, P.; Bergh, C.; Leon, M.; Brodin, U.; Zandian, M. Cognitive behavior therapy for eating disorders versus normalization of eating behavior. Physiology & behavior 2017, 174, 178–190. [Google Scholar]
- Solmi, M.; Monaco, F.; Højlund, M.; Monteleone, A.M.; Trott, M.; Firth, J.; Carfagno, M.; Eaton, M.; De Toffol, M.; Vergine, M.; Meneguzzo, P.; Collantoni, E.; Gallicchio, D.; Stubbs, B.; Girardi, A.; Busetto, P.; Favaro, A.; Carvalho, A.F.; Steinhausen, H.; Correll, C.U. Outcomes in people with eating disorders: a transdiagnostic and disorder-specific systematic review, meta-analysis and multivariable meta-regression analysis. World Psychiatry 2024, 23, 124–138. [Google Scholar] [CrossRef]
- Solmi, M.; Wade, T.D.; Byrne, S.; Del Giovane, C.; Fairburn, C.G.; Ostinelli, E.G.; De Crescenzo, F.; Johnson, C.; Schmidt, U.; Treasure, J.; Favaro, A.; Zipfel, S.; Cipriani, A. Comparative efficacy and acceptability of psychological interventions for the treatment of adult outpatients with anorexia nervosa: a systematic review and network meta-analysis. The Lancet Psychiatry 2021, 8, 215–224. [Google Scholar] [CrossRef]
- Spence, S.; Courbasson, C. The role of emotional dysregulation in concurrent eating disorders and substance use disorders. Eating behaviors 2012, 13, 382–385. [Google Scholar] [CrossRef]
- Spriggs, M.J.; Douglass, H.M.; Park, R.J.; Read, T.; Danby, J.L.; de Magalhães, F.J. ,... & Carhart-Harris, R. L. Study Protocol for “Psilocybin as a Treatment for Anorexia Nervosa: A Pilot Study”. Frontiers in Psychiatry 2021, 1770. [Google Scholar] [CrossRef]
- Spriggs, M.J.; Kettner, H.; Carhart-Harris, R.L. Positive effects of psychedelics on depression and wellbeing scores in individuals reporting an eating disorder. Eat Weight Disord 2021, 26, 1265–1270. [Google Scholar] [CrossRef] [PubMed]
- Streatfeild, J.; Hickson, J.; Austin, S.B.; Hutcheson, R.; Kandel, J.S.; Lampert, J.G. ,... & Pezzullo, L. Social and economic cost of eating disorders in the United States: Evidence to inform policy action. International Journal of Eating Disorders 2021, 54, 851–868. [Google Scholar]
- Strober, M.; Johnson, C. The need for complex ideas in anorexia nervosa: Why biology, environment, and psyche all matter, why therapists make mistakes, and why clinical benchmarks are needed for managing weight correction. The International Journal of Eating Disorders 2012, 45, 155–178. [Google Scholar] [CrossRef] [PubMed]
- Svaldi, J.; Griepenstroh, J.; Tuschen-Caffier, B.; Ehring, T. Emotion regulation deficits in eating disorders: A marker of eating pathology or general psychopathology? Psychiatry Research 2012, 197, 103–111. [Google Scholar] [CrossRef]
- Teixeira, P.J.; Johnson, M.W.; Timmermann, C.; Watts, R.; Erritzoe, D.; Douglass, H. ,... & Carhart-Harris, R. L. Psychedelics and health behaviour change. Journal of Psychopharmacology 2022, 36, 12–19. [Google Scholar]
- Tupper, K.W.; Wood, E.; Yensen, R.; Johnson, M.W. Psychedelic medicine: a re emerging therapeutic paradigm. Cmaj 2015, 187, 1054–1059. [Google Scholar] [CrossRef] [PubMed]
- Uthaug, M.V.; Van Oorsouw, K.; Kuypers KP, C.; Van Boxtel, M.; Broers, N.J.; Mason, N.L. ,... & Ramaekers, J. G. Sub-acute and long-term effects of ayahuasca on affect and cognitive thinking style and their association with ego dissolution. Psychopharmacology 2018, 235, 2979–2989. [Google Scholar]
- Uthaug, M.V.; Lancelotta, R.; Van Oorsouw, K.; Kuypers KP, C.; Mason, N.; Rak, J. ,... & Ramaekers, J. G. A single inhalation of vapor from dried toad secretion containing 5-methoxy-N, N-dimethyltryptamine (5-MeO-DMT) in a naturalistic setting is related to sustained enhancement of satisfaction with life, mindfulness related capacities, and a decrement of psychopathological symptoms. Psychopharmacology 2019, 236, 2653–2666. [Google Scholar]
- Vaismoradi, M.; Jones, J.; Turunen, H.; Snelgrove, S. Theme development in qualitative content analysis and thematic analysis. Journal of Nursing Education and Practice 2016, 6, 100–108. [Google Scholar] [CrossRef]
- van Eeden, A.E.; van Hoeken, D.; Hoek, H.W. Incidence, prevalence and mortality of anorexia nervosa and bulimia nervosa. Current Opinion in Psychiatry 2021, 34, 515–524. [Google Scholar] [CrossRef] [PubMed]
- van Hoeken, D.; Hoek, H.W. Review of the burden of eating disorders: mortality, disability, costs, quality of life, and family burden. Current opinion in psychiatry 2020, 33, 521. [Google Scholar] [CrossRef]
- Vargas, M.V.; Meyer, R.; Avanes, A.A.; Rus, M.; Olson, D.E. Psychedelics and other psychoplastogens for treating mental illness. Frontiers in Psychiatry 2021, 1691. [Google Scholar] [CrossRef] [PubMed]
- Vollenweider, F.X.; Preller, K.H. Psychedelic drugs: neurobiology and potential for treatment of psychiatric disorders. Nature Reviews Neuroscience 2020, 21, 611–624. [Google Scholar] [CrossRef]
- Waller, G. Recent advances in psychological therapies for eating disorders. F1000 Research 2016, 5, 702. [Google Scholar] [CrossRef]
- Treasure, J.; Cardi, V.; Leppanen, J.; Turton, R. New treatment approaches for severe and enduring eating disorders. Physiology & Behavior, 2015; 152(Pt B), 456–465. [Google Scholar] [CrossRef]
- Watts, R.; Day, C.; Krzanowski, J.; Nutt, D.; Carhart-Harris, R. Patients’ accounts of increased “connectedness” and “acceptance” after psilocybin for treatment-resistant depression. Journal of humanistic psychology 2017, 57, 520–564. [Google Scholar] [CrossRef]
- Wheeler, S.W.; Dyer, N.L. A systematic review of psychedelic-assisted psychotherapy for mental health: An evaluation of the current wave of research and suggestions for the future. Psychology of Consciousness: Theory, Research, and Practice 2020, 7, 279–315. [Google Scholar] [CrossRef]
- Williams, M.; Crotty, S.; Callon, C.; Lafrance, A. Ceremony Leaders’ Perspectives on the Good, the Bad, and the Ugly of Ayahuasca Drinking in Ceremonial Contexts. The Journal 2022, 54, 142. [Google Scholar]
- Williams, M.; Miller, A.K.; Lafrance, A. Ayahuasca ceremony leaders’ perspectives on special considerations for eating disorders. Eating Disorders 2023, 32, 120–139. [Google Scholar] [CrossRef]
- Wilson, T.G.; Grilo, C.M.; Vitousek, K.M. Psychological treatment of eating disorders. American Psychologist 2007, 62, 199–216. [Google Scholar] [CrossRef]
- Wu, D.; Wang, K.; Wei, D.; Chen, Q.; Du, X.; Yang, J.; Qiu, J. Perfectionism mediated the relationship between brain structure variation and negative emotion in a nonclinical sample. Cognitive, Affective, & Behavioral Neuroscience 2017, 17, 211–223. [Google Scholar]
- Yaden, D.B.; Griffiths, R.R. The subjective effects of psychedelics are necessary for their enduring therapeutic effects. ACS Pharmacology & Translational Science 2020, 4, 568–572. [Google Scholar]
- Zeifman, R.; Spriggs, M.J.; Kettner, H.; Lyons, T.; Rosas, F.; Mediano, P. ,...Carhart-Harris, R. (2022, July 7). From Relaxed Beliefs Under Psychedelics (REBUS) to Revised Beliefs After Psychedelics (REBAS): Preliminary Development of the RElaxed Beliefs Questionnaire (REB-Q). [CrossRef]
- Zimmerman, J.; Fisher, M. Avoidant/restrictive food intake disorder (ARFID). Current problems in pediatric and adolescent health care 2017, 47, 95–103. [Google Scholar] [CrossRef] [PubMed]

Table 1.
Examples of classic psychedelics under investigation for potential benefits as adjuncts to psychotherapy. .
Table 1.
Examples of classic psychedelics under investigation for potential benefits as adjuncts to psychotherapy. .
| Substance | Derivation or chemical analogues | General effects and properties | Potential harms* | Potential therapeutic use |
| LSD | Ergot fungus (Claviceps purpurea); morning glory (Turbina corymbosa); Hawaiian baby woodrose (Argyreia nervosa) - sources of ergine or lysergic acid amide | - 5-HT2A (serotonin) agonist of pyramidal neurons - Dizziness, weakness, tremors, paresthesia - Altered consciousness (visions, auditory distortions, ideations) - Altered mood (happy, sad, fearful, irritable) - Distorted sense of space, time |
- Psychosis - Hallucinogen persisting perception disorder |
- Addiction (e.g., alcohol) - Anxiety associated with terminal illness |
| Psilocybin | Psilocybe and other genera of mushroom (various species) | - 5-HT2A (serotonin) agonist of pyramidal neurons - Dizziness, weakness, tremors, paresthesia - Altered consciousness (visions, auditory distortions, ideations) - Altered mood (happy, sad, fearful, irritable) - Distorted sense of space, time |
- Psychosis - Hallucinogen persisting perception disorder |
- Addiction (e.g., tobacco, alcohol) - Anxiety associated with terminal illness |
| Ayahuasca brew (admixtures contain DMT) | Chacruna leaf (Psychotria viridis); Chagropanga vine (Diplopterys cabrerana); ayahuasca vine (Banisteriopsis caapi); assorted other admixture plants | - 5-HT2A (serotonin) agonist of pyramidal neurons - Dizziness, weakness, tremors, paresthesia - Nausea, emesis - Altered consciousness (visions, auditory distortions, ideations) - Altered mood (happy, sad, fearful, irritable) - Distorted sense of space, time |
- Psychosis - Serotonin syndrome and other dangers from medication interactions due to monoamine oxidase inhibitory activity |
- Addiction (alcohol, cocaine, tobacco) - Depression, anxiety |
| Mescaline | Peyote cactus (Lophophora williamsii); San Pedro cactus (Echinopsis pachanoi) | - 5-HT2A (serotonin) agonist of pyramidal neurons - Dizziness, weakness, tremors, paresthesia - Altered consciousness (visions, auditory distortions, ideations) - Altered mood (happy, sad, fearful, irritable) - Distorted sense of space, time |
- Psychosis | - Addiction (alcohol) |
| MDMA | Sassafras tree (Sassafras albidum) - source of safrole, precursor chemical | - Serotonin, dopamine and noradrenaline agonist - Euphoria - Arousal - Perceptual alteration - Enhanced empathy and sociability |
- Potential neurocognitive deficits (e.g. memory impairment) - Sleep disruption - Short-term depression |
- PTSD |
| Note: DMT = dimethyltryptamine, LSD = lysergic acid dimethylamide, MDMA = Methylenedioxymethamphetamine, PTSD = posttraumatic stress disorder. *Potential harms identified here are associated with unsupervised uses of psychedelic substances (often in the context of polysubstance use); current clinical studies on psychedelic agents have not reported such chronic adverse sequelae. Potential therapeutic uses are identified based on evidence from past (i.e., 1950s-1960s) and current research of psychedelic drugs. | ||||
Note. From “Psychedelic medicine: a re-emerging therapeutic paradigm” by Tupper, K. W., Wood, E., Yensen, R., & Johnson, M. W., 2015.. Cmaj, 187(14), 1054-1059.
Table 2.
Sample Demographics .
| M (SD) | Range | N (%) | |
| Age | 36.9 (11.33) | 25-54 | 8 |
| Gender | |||
| Female | 7 (87.5%) | ||
| Non-binary (NB) | 1 (12.5%) | ||
| Education (highest level completed) | |||
| GCSEs | 1 (12.5%) | ||
| A level | 1 (12.5%) | ||
| Undergraduate degree | 2 (25%) | ||
| Postgraduate degree | 4 (50%) | ||
| Eating disorder (multiple diagnosis) | |||
| Anorexia nervosa | 7 (87.5%) | ||
| Bulimia nervosa | 2 (25%) | ||
| Other specified feeding or eating disorder | 1 (12.5%) | ||
| Orthorexia nervosa | 1 (12.5%) | ||
| Binge eating disorder | 1 (12.5%) | ||
| Disordered eating | 1 (12.5%) |
Note. Other specified feeding or eating disorder (OSFED) is diagnosed when symptoms do not fit a specific ED. Orthorexia nervosa (ON) is marked by extreme avoidance of perceived unhealthy foods (American Psychiatric Association, 2013).
Table 3.
Participant and Outcome Information.
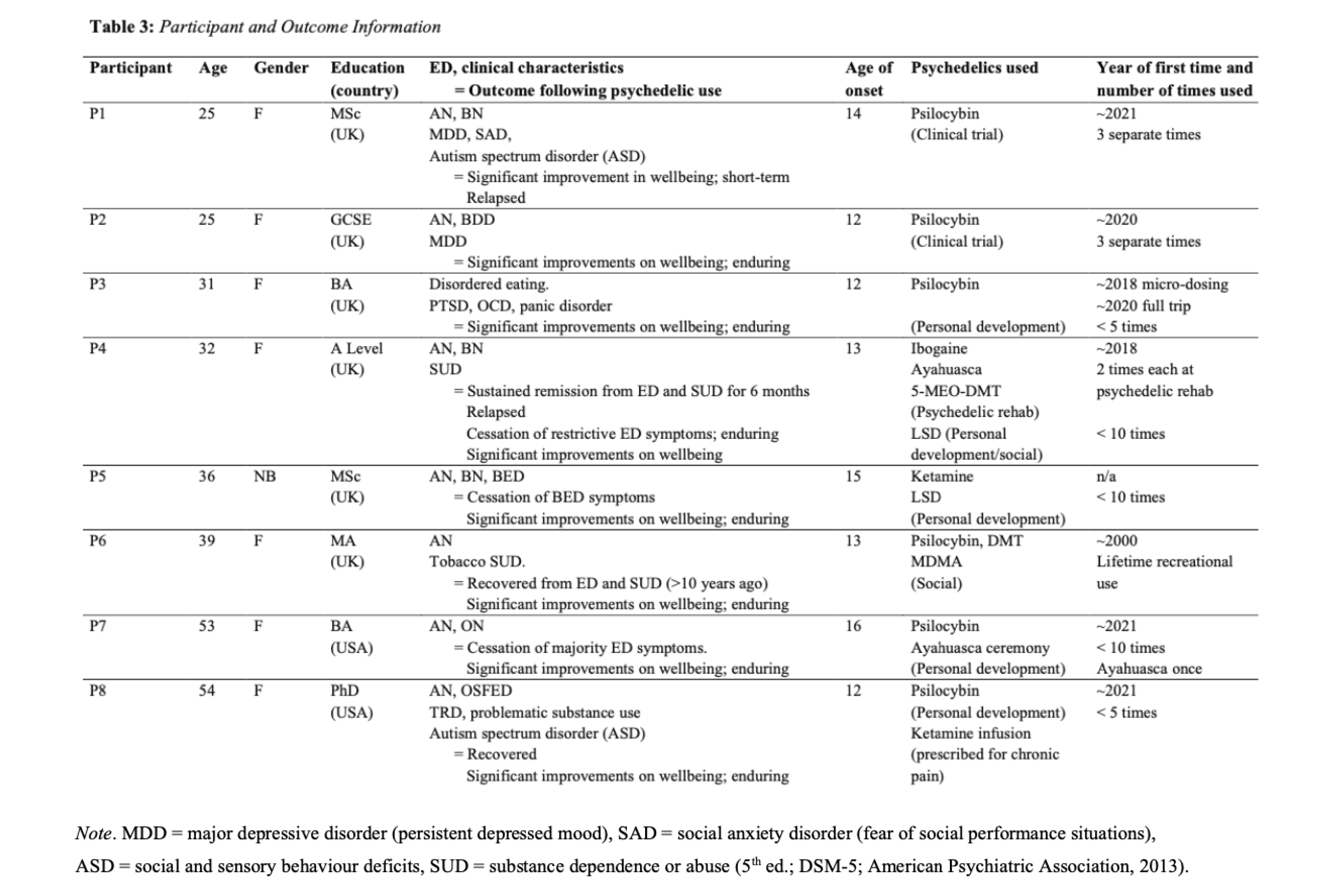 |
Table 4.
Superordinate and subordinate themes.
| Superordinate themes | Subordinate themes |
|---|---|
| ‘Exploring’ via ‘the gateway to healing’ |
‘Freedom’ to ‘expand’ and ‘explore your mind' |
| ‘Navigating the roadmap through your subconscious emotions’ | |
| Transcendence: ‘it’s not a theoretical knowledge, it’s a deep knowing’ | |
| ‘Transformation’ and being ‘able to do the work’ |
Cognitive: ‘they’ve opened me up’ |
| Behavioural: ‘start making changes’ | |
| Safety perceptions: ‘medicine’ but ‘not a magic pill’ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



