
Submitted:
06 September 2024
Posted:
06 September 2024
You are already at the latest version
Abstract
Introduction: Arterial hypertension and obesity are two major risk factors for cardiovascular morbidity and mortality closely linked. The objective of this study was to describe the epidemiological and clinical characteristics of hypertensive patients according to their level of obesity as proposed by the classification of the World Health Organization (WHO). Patients and Methods: Retrospective study (January 2022-April 2023) involving 230 hypertensive and obese adult patients whose mean age was 52.5 ± 12.05 years [Extremes: 24-85 years] followed on an outpatient basis and classified into 3 Classes according to their body mass index (BMI). Epidemiological, clinical parameters and cardiovascular risk stratification were analyzed. The relevance of the risk stratification method was analyzed by area under the curve (AUC). Statistical analysis was performed using SPPS version 26 software (SPSS Inc., Chicago, IL, USA). Results: Classes 1 (n=170; 73.9%), 2 (n=43; 18.7%) and 3 (n=17; 7.4%) were identified. There were significantly more women than men in Class 3 (9.7% versus 2.7%; p=0.001). The risk of being diabetic (OR=0.135;95%CI=0.034–0.541;p=0.005), of having angina pain (OR=0.084;95%CI=0.009–0.790;p=0.030) or developing chronic renal failure (OR=2.416;95%CI=1.471–85.268;p=0.020) was significantly higher in Class 3 than in Class 1. According to cardiovascular risk stratification, 152 patients (66.1%) were at high and very high risk. The level of cardiovascular risk of our patients was not related to the degree of obesity based on body mass index (p=0.32). The risk stratification method was relevant (AUC˃0.70;p˂0.001). Conclusion: Morbid obesity exposes hypertensives more to cardiovascular, renal and metabolic complications.
Keywords:
Obesity
; Hypertension
; risk factor
; Cardiology
Introduction
Arterial hypertension and obesity are 2 major risk factors for cardiovascular morbidity and mortality which are closely linked [1,2,3]. According to current global statistics, these 2 conditions are on the rise with forecasts of approximately 30% of hypertensives by 2025 [1] and 1.12 billion obese people in 2030 out of the entire world population [4,5]. The arterial hypertension-obesity association known from the literature since the 20th century [6] therefore represents a veritable pandemic and remains a major public health problem [7]. According to the literature, there is a strong relationship between body mass index, variation in blood pressure and the occurrence of cardiovascular disease [7,8,9]. Indeed, an increase of 1.71 mm Hg per 1 kg of weight/m2 in systolic BP has been clearly described in West Africa [1]. Also, a weight gain of 10 kg was associated with an increase of 3 mm Hg for systolic blood pressure and 2.3 mm Hg for diastolic blood pressure, resulting in an increased risk of occurrence of cardiovascular diseases such as coronary artery disease and cerebrovascular accident (CVA) [10,11]. Several other studies [12,13,14] also demonstrated that obese subjects have a 2 to 3 times greater risk of developing arterial hypertension and approximately 60% of the incidence of arterial hypertension is attributable to the increase in fat reserves. This epidemiological and clinical observation suggests a more in-depth analysis of these 2 conditions within our populations. It is in this perspective that we carried out this study which aimed to describe the epidemiological and clinical characteristics of hypertensives according to their level of obesity according to the WHO classification.
Patients and Methods
Population and Study Period
This is a study conducted over a period of 16 months involving 230 adult, hypertensive and obese patients followed on an outpatient basis in the Cardiology department of the Bouake University Hospital. The following inclusion criteria were applied to select the participants in the study: Were included, adult patients over the age of 18, all hypertensive under treatment and followed by Medical Specialists in Cardiology and presenting obesity whatever either the grade, with a BMI ≥ 30 kg/m². Pregnant women were not included. These patients have been grouped into 3 categories according to the classification of the World Health Organization (WHO) [15] which designates obesity as a complex and multifactorial disease due to an abnormal or excessive accumulation of fat capable of altering the health of individuals [15,16,17,18]. Thus, three levels of obesity severity were distinguished: People with a BMI of 30.0 to 34.9 kg/m² were considered to have class I obesity, those with a BMI of 35 to 39, 9 kg/m² corresponding to class II obesity, and those with a BMI of 40 kg/m² and more corresponding to class III obesity, ie severe obesity, formerly called morbid obesity. Abdominal obesity, the best reflection of the risk, is generally assessed using a tape measure graduated in cm, by measuring the waist circumference (WC) or the abdominal perimeter [19,20] while considering abdominal obesity such as a Waist Circumference ≥ 102 cm for men and a WC ≥ 88 cm for women) [21,22].
Methodology
This is a retrospective, cross-sectional study with a descriptive and analytical purpose. We analyzed the variation in the epidemiological and clinical parameters of our patients according to their level of obesity in univariate and multivariate analysis. We then studied cardiovascular risk stratification of our patients according to grade and stage of hypertension as proposed by the ESH 2023. The study of the area under the curve (AUC) allowed us to analyze the relevance of the quantitative parameters used for this risk stratification (systolic blood pressure (SBP), diastolic blood pressure (DBP) and Cardiovascular risk (CVRF) number) for our population.
Measures
Mass anthropometric parameters (height and weight) were measured separately in patients wearing more or less light clothing [23] and barefoot for the calculation of BMI. The abdominal circumference was also measured. Body mass index (BMI) was calculated as weight in kilograms divided by the square of height in meters [19,20,23,24,25,26], is used to screen for obesity in adults, with a threshold set at 30 kg/m² in adults by the Centers for Disease Control and Prevention (CDC) [19,27].
Assessment of Blood Pressure and Hypertension
Blood pressure was measured using an electronic tensiometer based on American and European International recommendations [28,29,30]. Arterial hypertension was defined as systolic blood pressure ≥ 140 mm Hg and/or diastolic blood pressure ≥ 90 mm Hg. We analyzed epidemiological and clinical characteristics in obesity subgroups.
Cardiovascular Risk Level Stratification [30]
To perform the cardiovascular risk stratification, we used the 2023 ESH Cardiovascular risk according to grade and stage of hypertension which classifies patients into 4 groups namely Low Risk, Moderate Risk, High Risk and Very High Risk. This classification is based on the grade of hypertension, the number of risk factors, Hypertension-mediated organ damage (HMOD), Diabetes mellitus and established cardiovascular and kidney disease.
Statistical Analysis
Statistical analysis was performed using IBM SPSS Statistics software, version 26 (SPSS Inc., Chicago, IL, USA). P values (two-sided) <0.05 were considered statistically significant. Continuous variables were expressed as mean ± standard deviation (SD) or median with interquartile range (25%, 75%) and categorical variables were presented as percentages (%). Student’s t-test and Chi-square test were used for continuous and dichotomous variables, respectively. Regression tests were used to analyze associations between variables. Data were summarized as Odd Ratio (95% CI). To assess the discriminating power of the cardiovascular risk classification model for our population, we constructed the Receiver -operating curve (ROC) and calculated the area under the curve (area under the curve=AUC). Discriminatory power was defined as acceptable if the AUC ≥ 0.5 [31].
Ethics
This research followed the ethical guidelines established in the Declaration of Helsinki [32].
Results
We collected 230 patients including 75 (32.61%) male patients and 155 (67.39%) female patients. The average age was 52.5 ± 12.05 years [Extremes: 24-85 years] with 93 (40.4%) patients from rural areas and 137 (59.6%) patients from urban areas. The Body Mass Index (BMI) and abdominal circumference were, respectively, on average 33.59 ± 4.20 Kg/m² [Extremes: 30-53.99 Kg/m²] and 103, 71± 10.66 cm [Extremes: 69-150 cm]. These patients were all hypertensives Grade 1 (n= 123; 53.5%) or Grade 2 (n= 47; 20.4%) or Grade 3 (n= 60; 26.1%). These hypertensives had an average of 2.8 ± 0.81 cardiovascular risk factors [Extremes: 2-6]. We counted 28 (12.2%) type 2 diabetic patients; 10 (4.3%) smoking patients and 37 (16.1%) patients with dyslipidemia. Seventeen (7.4%) patients presented with anginal chest pain on admission and twenty-nine patients (12.60%) presented with dyspnea. The mean abdominal circumference was 103.71±10.66cm [ Extremes: 69-150]. One hundred and eighty-nine patients (82.17%) presented with abdominal obesity and 18 (7.8%) patients presented with left ventricular hypertrophy on electrocardiographic evaluation. Heart failure, Chronic Kidney Failure and stroke were 19 (8.26%), 5 (2.2%) and 18 (7.82%) respectively (Table 1). In univariate analysis, Classes 1 (n=170;73.9%), 2 (n=43;18.7%) and 3 (n=17;7.4%) were identified. There were significantly more women than men in Class 3 (9.7% versus 2.7%; p=0.001). There were more diabetic patients (29.4% versus 10%; p=0.048) and renal failure patients (11.8% versus 1.2%; p=0.035) in Class 3 than in Class 1. Class 3 patients have more angina pain (23.5% versus 7.1%; p=0.017) compared to Class 1 patients. In multivariate analysis, the risk of being diabetic (OR=0.135; 95% CI=0.034–0.541; p=0.005), of having angina pain (OR=0.084; 95% CI=0.009–0.790; p=0.030) and developing chronic renal failure (OR=2.416; 95% CI=1.471–85.268; p=0.020) was significantly higher in Class 3 than in Class 1 (Table 2). According to cardiovascular risk stratification (Table 3), 152 patients (66.1%) were at high and very high risk. The level of cardiovascular risk of our patients was not related to the degree of obesity based on body mass index (p=0.32). The quantitative parameters used to classify the cardiovascular risk within our study population were relevant for systolic blood pressure (AUC=0.830; 95%CI=0.776–0.883; p˂0.001), diastolic blood pressure (AUC=0.724; 95%CI=0.659–0.790; p˂0.001) and the number of cardiovascular risk factors (AUC=0.710; 95%CI=0.642–0.779; p˂0.001) (Figure 1).
Discussion
Epidemiology and Prevalence of Obesity-Related Hypertension
Data from the literature confirm a close link between obesity and hypertension [1,33,34]. This link was demonstrated in 1960 prospectively in the Framingham study [6,32]. Indeed, 40-67.3% of hypertensives worldwide are obese [1,6,13,33]. This hypertension-obesity association is stronger in women than in men in our study (67.39% versus 32.61%; p=0.001). This finding was corroborated by Zhang et al. [13] in 2022 in China who reported a higher prevalence of obese hypertensives in women than in men (26.2% versus 18.8%; P < 0.001). In our series, around 59.6% versus 40.4% of obese hypertensive patients come from urban areas (p= 0.25). These results, even if not significant, were confirmed by the work of Zhang et al. [13] in 2022 in China who found a higher prevalence of obese hypertensive patients in urban areas (26.5% versus 21.5%; P <0.001), this could be explained by the fact that patients in cities would be more sedentary living with socio-professional stress.
The Pathophysiology of Obesity-Related Hypertension [6,12,36]
Obesity-related hypertension results from several complex mechanisms: insulin resistance, alteration of adipokines; dysfunction of the Sympathetic Nervous System and the Renin Angiotensin Aldosterone system; metabolic, endothelial and vascular dysfunctions, neuroendocrine imbalances, sodium retention, glomerular hyperfiltration, proteinuria and inappropriate immune and inflammatory responses. These mechanisms will be responsible for two consequences: on the one hand, high cardiovascular morbidity and mortality, due to the occurrence of coronary heart disease, congestive heart failure, sudden cardiac death, chronic renal failure (CRI), and strokes and on the other hand, resistant hypertension.
Joint Effects of Obesity and Hypertension on Cardiovascular Risk
In our study, class 3 obese hypertensives had a 3 times greater risk of developing type 2 diabetes (Table II). This observation is consistent with data from the literature [6]. Obesity associated with type 2 diabetes and hypertension increases the risk of occurrence of cardiovascular diseases [37–39]. In addition, hypertensive patients with morbid obesity in our series were more likely to present with angina pain or chronic renal failure. This would be explained by the pathophysiological disorders [10,12,33] due to the “cursed couple” hypertension-obesity and also confirmed by data from the literature [40,41]. The level of cardiovascular risk of our patients was not related to the degree of obesity based on body mass index (p=0.32). This surprising result seems to be explained by the fact that the WHO classification of obesity used in our study was based on the measurement of BMI. However, the best predictive factor of cardiovascular risk is Waist circumference and not BMI [42–45]. Hence the absence of relation between the level of cardiovascular risk of our patients and their degree of obesity. Indeed, body mass index (BMI) is the most widely used method to determine the prevalence of overweight and classify obesity. However, in recent years it has been suggested that primarily waist circumference is higher closely associated with cardiovascular morbidity and mortality [42].
Therapeutic Implications
The therapeutic management of obese hypertensives is based on lifestyle and dietary measures and pharmacological means.
Hygieno-Dietary Measures [6]
It consists of lifestyle changes including: the (DASH) Dietary Approaches to Stop Hypertension diet, weight loss, weight loss diet low in saturated fat, low sodium diet, regular physical activity, reduction of alcohol and smoking cessation.
Pharmacological Means
Target blood pressure should be <140/90 [28]. To achieve this blood pressure target, antihypertensive treatment will be based on angiotensin-converting enzyme inhibitors, angiotensin receptor blockers and thiazide diuretics, while β-blockers should be avoided unless specifically cardiac indicated. This antihypertensive treatment will be combined with bariatric medical treatment and bariatric surgery [6].
Conclusion
Hypertensives with class 3 obesity have a higher risk of developing type 2 diabetes, presenting with angina pain or chronic renal failure with, therefore, a higher risk of cardiovascular disease. The cardiovascular risk was not related to the degree of obesity based on body mass index.
Conflicts of Interest
no-financial interests that are directly or indirectly related to this manuscript.
References
- Akpa OM, Made F, Ojo A, Ovbiagele B, Adu D, Motala AA, Mayosi BM, Adebamowo SN, Engel ME, Tayo B, Rotimi C, Salako B, Akinyemi R, Gebregziabher M, Sarfo F, Wahab K, Agongo G , Alberts M, Ali SA, Asiki G, Boua RP, Gómez-Olivé FX, Mashinya F, Micklesfield L, Mohamed SF, Nonterah EA, Norris SA, Sorgho H, Tollman S, Parekh RS, Chishala C, Ekoru K, Waddy SP , Peprah E, Mensah GA, Wiley K, Troyer J, Ramsay M, Owolabi MO; as members of the CVD Working Group of the H3Africa Consortium. Regional Patterns and Association between Obesity and Hypertension in Africa: Evidence from the H3Africa CHAIR Study. Hypertension. 2020; 75:1167-78. [CrossRef]
- El Meouchy P, Wahoud M, Allam S, Chedid R, Karam W, Karam S. Hypertension Related to Obesity: Pathogenesis, Characteristics and Factors for Control. Int J Mol Sci. 2022; 23:12305. [CrossRef]
- Fahed G, Aoun L, Bou Zerdan M, Allam S, Bou Zerdan M, Bouferraa Y, Assi HI Metabolic Syndrome: Updates on Pathophysiology and Management in 2021. Int. J.Mol. Science. 2022; 23:786. [CrossRef]
- Kearney PM, Whelton M, Reynolds K, Muntner P, Whelton PK, He J. Global burden of hypertension: analysis of worldwide data. Lancet. 2005; 365:217–23. [CrossRef]
- Kelly T, Yang W, Chen CS, Reynolds K, He J. Global burden of obesity in 2005 and projections to 2030. Int J Obes (Lond). 2008; 32:1431-7. [CrossRef]
- Landsberg L, Aronne LJ, Beilin LJ, Burke V, Igel LI, Lloyd-Jones D, Sowers J. Obesity-related hypertension: pathogenesis, cardiovascular risk, and treatment: a position paper of The Obesity Society and the American Society of Hypertension. J Clin Hypertens (Greenwich). 2013; 15:14-33. [CrossRef]
- Dalichaouch-Benchaoui, Souhaila, and Noureddine Abadi. “Variables of adiposity related to obesity and morbid states of a population of eastern Algeria.” Metabolic Disease Medicine 15.8.2021:809-17.
- Alberti KG, Zimmet P, Shaw J; IDF Epidemiology Task Force Consensus Group. The metabolic syndrome--a new worldwide definition. Lancet. 2005;366:1059-62. [CrossRef]
- El Rhazia, K., et al. “Prevalence of obesity and the main socio-demographic factors associated in Morocco.” Papers 57.2009: S3-S59.
- Pathak, A., Rouet, P., Despas, F., Jourdan, G., Verwaerde, P., Galinier, M., & Senard, JM Obesity and arterial hypertension: epidemiology, pathophysiology and management. mt cardio.2007; 3 :169-177. [CrossRef]
- Clinical Guidelines on the Identification. Evaluation, and Treatment of Overweight and Obesity in Adults--The Evidence Report.National Institutes of Health.Obes Res.1998; 62: 51S-209S.
- Seravalle G, Grassi G. Obesity and hypertension. Pharmacol Res. 2017; 122:1-7. [CrossRef]
- Zhang Y, Zhang WQ, Tang WW, Zhang WY, Liu JX, Xu RH, Wang TD, Huang XB. The prevalence of obesity-related hypertension among middle-aged and older adults in China. Front Public Health. 2022; 10:865870. [CrossRef]
- Okosun IS, Prewitt TE, Cooper RS. Abdominal obesity in the United States: prevalence and attributable risk of hypertension. J Hum Hypertens. 1999; 13:425–30. [CrossRef]
- Hebebrand J, Holm JC, Woodward E, Baker JL, Blaak E, Durrer Schutz D, Farpour-Lambert NJ, Frühbeck G, Halford JGC, Lissner L, Micic D, Mullerova D, Roman G, Schindler K, Toplak H, Visscher TLS , Yumuk V. A Proposal of the European Association for the Study of Obesity to Improve the ICD-11 Diagnostic Criteria for Obesity Based on the Three Dimensions Etiology, Degree of Adiposity and Health Risk. Obese Facts. 2017; 10:284-307. [CrossRef]
- World Health Organization Obesity: Preventing and Managing the Global Epidemic. Report of a WHO Consultation (WHO Technical Report Series 894). 2000. www.who.int/nutrition/publications/obesity/WHO_TRS_894/en/ (last accessed on August 10, 2023).
- Available online: https://www.who.int/health-topics/obesity#tab=tab_1 (last accessed on August 10, 2023).
- Lauby-Secretan B, Dossus L, Marant-Micallef C, His M. Obésité et cancer [Obesity and Cancer]. Bull Cancer. 2019; 106:635-46. [CrossRef]
- El Meouchy P, Wahoud M, Allam S, Chedid R, Karam W, Karam S. Hypertension Related to Obesity: Pathogenesis, Characteristics and Factors for Control. Int J Mol Sci. 2022; 23:12305. [CrossRef]
- Ross, R.; Neeland, IJ; Yamashita, S.; Shai, I.; Seidell, J.; Magni, P.; Santos, RD; Arsenault, B.; Cuevas, A.; Hu, FB; et al. Waist circumference as a vital sign in clinical practice: A Consensus Statement from the IAS and ICCR Working Group on Visceral Obesity. Nat. Rev. Endocrinol. 2020; 16: 177–18. [CrossRef]
- Wang Y, Beydoun MA, Min J, Xue H, Kaminsky LA, Cheskin LJ. Has the prevalence of overweight, obesity and central obesity leveled off in the United States? Trends, patterns, disparities, and future projections for the obesity epidemic. Int J Epidemiol. 2020; 49:810-23. [CrossRef]
- National Institutes of Health (NIH) National Heart L, and Blood Institute’s (NHLBI) North American Association for the Study of Obesity (NAASO). The practical guide: identification, evaluation, and treatment of overweight and obesity in adults In. National Institutes of Health , 2000. Vol Publication no. 00-4084. Rockville, MD.
- Köchli S, Endes K, Steiner R, Engler L, Infanger D, Schmidt-Trucksäss A, Zahner L, Hanssen H. Obesity, High Blood Pressure, and Physical Activity Determine Vascular Phenotype in Young Children. Hypertension. 2019; 73:153-61. [CrossRef]
- Ma S, Xi B, Yang L, Sun J, Zhao M, Bovet P. Trends in the prevalence of overweight, obesity, and abdominal obesity among Chinese adults between 1993 and 2015. Int J Obes. 2021; 45:427–37. [CrossRef]
- Finkelstein, MM Body mass index and quality of life in a survey of primary care patients. J.Fam. Practice 2000; 49:734–37. [PubMed]
- Fujioka, S.; Matsuzawa, Y.; Tokunaga, K.; Tarui, S. Contribution of intra-abdominal fat accumulation to the impairment of glucose and lipid metabolism in human obesity. Metabolism. 1987; 36:54–59. [CrossRef]
- CDC. Available online: https://www.cdc.gov/obesity/basic/adult-defining.html?CDC_AA_refVal=https%3A%2%2Fwww.cdc.gov%2Fobesity%2Fadult%2Fdefining.html (last accessed on 4 July 2023).
- Cheung AK, Whelton PK, Muntner P, Schutte AE, Moran AE, Williams B, Sarafidis P, Chang TI, Daskalopoulou SS, Flack JM, Jennings G, Juraschek SP, Kreutz R, Mancia G, Nesbitt S, Ordunez P, Padwal R , Persu A, Rabi D, Schlaich MP, Stergiou GS, Tobe SW, Tomaszewski M, Williams KA Sr, Mann JFE. International Consensus on Standardized Clinic Blood Pressure Measurement - A Call to Action. Am J Med. 2023; 136:438-45. [CrossRef]
- Flack JM, Adekola B. Blood pressure and the new ACC/AHA hypertension guidelines. Trends Cardiovascular Med. 2020; 30:160-64. [CrossRef]
- Mancia Chairperson G, Kreutz Co-Chair R, Brunström M, Burnier M, Grassi G, Januszewicz A, Muiesan ML, Tsioufis K, Agabiti-Rosei E, Algharably EAE, Azizi M, Benetos A, Borghi C, Hitij JB, Cifkova R , Coca A, Cornelissen V, Cruickshank K, Cunha PG, Danser AHJ, de Pinho RM, Delles C, Dominiczak AF, Dorobantu M, Doumas M, Fernández-Alfonso MS, Halimi JM, Járai Z, Jelaković B, Jordan J, Kuznetsova T, Laurent S, Lovic D, Lurbe E, Mahfoud F, Manolis A, Miglinas M, Narkiewicz K, Niiranen T, Palatini P, Parati G, Pathak A, Persu A, Polonia J, Redon J, Sarafidis P, Schmieder R, Spronck B, Stabouli S, Stergiou G, Taddei S, Thomopoulos C, Tomaszewski M, Van de Borne P, Wanner C, Weber T, Williams B, Zhang ZY, Kjeldsen SE; Authors/Task Force Members:. 2023 ESH Guidelines for the management of arterial hypertension The Task Force for the management of arterial hypertension of the European Society of Hypertension Endorsed by the European Renal Association (ERA) and the International Society of Hypertension (ISH). J Hypertens. 2023 Jun 21. Epub ahead of print. [CrossRef] [PubMed]
- Wan H, Wang Y, Xiang Q, Fang S, Chen Y, Chen C, Zhang W, Zhang H, Xia F, Wang N, Lu Y. Associations between abdominal obesity indices and diabetic complications: Chinese visceral adiposity index and neck circumference. Cardiovasc Diabetol. 2020; 19:118. [CrossRef]
- Múzquiz-Barberá P, Ruiz-Cortés M, Herrero R, Vara MD, Escrivá-Martínez T, Baños RM, Rodilla E, Lisón JF. “Own doctor” presence in a web-based lifestyle intervention for adults with obesity and hypertension: A randomized controlled trial. Front Public Health. 2023; 11:1115711. [CrossRef]
- Leggio M, Lombardi M, Caldarone E, Severi P, D’Emidio S, Armeni M, Bravi V, Bendini MG, Mazza A. The relationship between obesity and hypertension: an updated comprehensive overview on vicious twins. Hypertens Res. 2017; 40:947-63. [CrossRef]
- Wang Y, Wang QJ. The prevalence of prehypertension and hypertension among US adults according to the new joint national committee guidelines: new challenges of the old problem. Arch Intern Med. 2004; 164:2126-34. [CrossRef]
- Kannel WB, Brand N, Skinner JJ Jr, Dawber TR, McNamara PM. The relation of adiposity to blood pressure and development of hypertension. The Framingham study. Ann InternMed. 1967; 67:48-59. [CrossRef]
- DeMarco VG, Aroor AR, Sowers JR. The pathophysiology of hypertension in patients with obesity. Nat Rev Endocrinol. 2014; 10:364-76. [CrossRef]
- Stamler J, Dyer AR, Shekelle RB, Neaton J, Stamler R. Relationship of baseline major risk factors to coronary and all-cause mortality, and to longevity: findings from long-term follow-up of Chicago cohorts. Cardiology. 1993; 82:191-222. [CrossRef]
- Haffner SM, Lehto S, Rönnemaa T, Pyörälä K, Laakso M. Mortality from coronary heart disease in subjects with type 2 diabetes and in nondiabetic subjects with and without prior myocardial infarction. N Engl J Med. 1998; 339:229-34. [CrossRef]
- Juutilainen A, Lehto S, Rönnemaa T, Pyörälä K, Laakso M. Type 2 diabetes as a “coronary heart disease equivalent”: an 18-year prospective population-based study in Finnish subjects. Diabetes Care. 2005; 28:2901-7. [CrossRef]
- Chi JH, Lee BJ. Association of myocardial infarction and angina pectoris with obesity and biochemical indices in the South Korean population. Sci Rep. 2022; 12:13769. [CrossRef]
- Wilson PW, Bozeman SR, Burton TM, Hoaglin DC, Ben-Joseph R, Pashos CL. Prediction of first events of coronary heart disease and stroke with consideration of adiposity. Traffic. 2008; 118 :124–30. [CrossRef]
- Huxley R, Mendis S, Zheleznyakov E, Reddy S, Chan J. Body mass index, waist circumference and waist:hip ratio as predictors of cardiovascular risk--a review of the literature. Eur J Clin Nutr. 2010; 64:16-22. [CrossRef]
- Staiano AE, Reeder BA, Elliott S, Joffres MR, Pahwa P, Kirkland SA, Paradis G, Katzmarzyk PT. Body mass index versus waist circumference as predictors of mortality in Canadian adults. Int J Obes (Lond). 2012; 36:1450-4. [CrossRef]
- Ashwell M, Gunn P, Gibson S. Waist-to-height ratio is a better screening tool than waist circumference and BMI for adult cardiometabolic risk factors: systematic review and meta-analysis. Obes Rev. 2012; 13:275-86. [CrossRef]
- Janssen I, Katzmarzyk PT, Ross R. Waist circumference and not body mass index explains obesity-related health risk. Am J Clin Nutr. 2004; 79:379-84. [CrossRef]
Figure 1.
Plots of Receiver operating curve (ROC) curves for analyzing the performance of quantitative cardiovascular risk stratification parameters according to the 2023 ESH, namely systolic blood pressure (SBP), diastolic blood pressure (DBP) and Cardiovascular risk number (CVRF). These parameters classify patients according to whether or not they belong to the class of patients at high cardiovascular risk.
Figure 1.
Plots of Receiver operating curve (ROC) curves for analyzing the performance of quantitative cardiovascular risk stratification parameters according to the 2023 ESH, namely systolic blood pressure (SBP), diastolic blood pressure (DBP) and Cardiovascular risk number (CVRF). These parameters classify patients according to whether or not they belong to the class of patients at high cardiovascular risk.
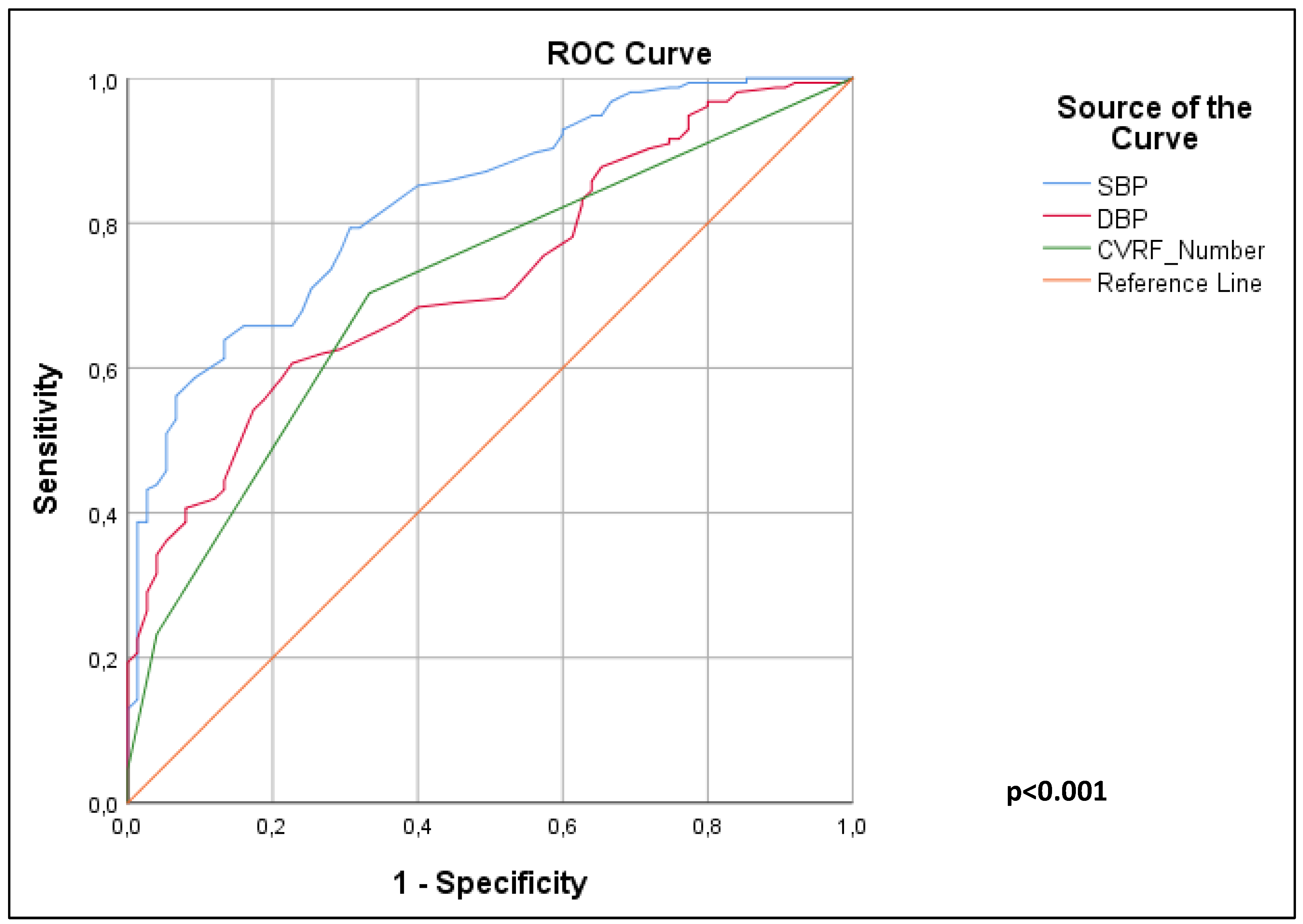

Table 1.
Epidemiological and clinical characteristics of obese hypertensives in univariate analysis.
Table 1.
Epidemiological and clinical characteristics of obese hypertensives in univariate analysis.
| Variables | Average values (N=230) |
Class 1 obesity (n=170) | Class 2 obesity (n=43) | Class 3 obesity (n=17) | p-value |
|---|---|---|---|---|---|
| Age, years | 52.5 ± 12.05 [Extremes: 24-85] | 51 | 50 | 56.5 | 0.77 |
| Sex Male Female |
75(32.61%) 155 (67.39%) |
67(39.4%) 103 (60.6%) |
6(14%) 37 (86%) |
2(11.8%) 15 (88.2%) |
0.001 |
| Origin rural Urban |
93(40.4%) 137(59.6%) |
74(43.5%) 96(56.5%) |
13(30.2%) 30(69.8%) |
06(35.3%) 11(64.7%) |
0.25 |
| CVRF | 2.8±0.81 [Extremes:2-6] | 2.6 | 2.8 | 3 | 0.82 |
| Type 2 diabetes | 28 (12.2%) | 17 (10%) | 6 (14%) | 5 (29.4%) | 0.048 |
| Dyslipidemia Active smoking |
37(16.1%) 10(4.3%) |
26(15.3%) 7(4.11%) |
6(14%) 3(6.97%) |
5(29.4%) 00(0%) |
0.29 0.506 |
| Angina Pain Dyspnea |
17(7.4%) 29(12.60) |
12(7.1%) 16(9.41) |
1(2.3%) 7(16.27) |
4 (23.5%) 3(17.64) |
0.017 0.577 |
| Arterial hypertension Grade 1 Grade 2 Grade 3 |
123(53.5%) 47(20.4%) 60(26.1%) |
91(53%) 33(19.4%) 46(27.1%) |
22(51.2%) 10(23.3%) 11(25.6%) |
10(58.8%) 4(23.5%) 3(17.6%) |
0.913 |
| BMI, Kg/m² | 33.59± 4.20 [Extremes: 30-53.99] | - | - | - | - |
| Abdominal perimeter, cm Abdominal Obesity |
103.71± 10.66[Extremes: 69-150] 189(82.17) |
- - |
- - |
- - |
- - |
| CKF | 5 (2.2%) | 2 (1.2%) | 1 (2.3%) | 2 (11.8%) | 0.035 |
| HVG Stroke Heart failure Cancer |
18(7.82%) 18(7.82%) 19(8.26%) 02(0.86%) |
13(7.6%) 15(8.82) 15(8.82%) 2(1.17%) |
4(9.3%) 3(6.97) 2(4.65%) 0(00%) |
1(5.9%) 0(0%) 2(11.76%) 0(00%) |
0.90 0.63 0.54 0.99 |
CVRF: Cardio-Vascular Risk Factor; BMI: Body Mass Index; CKF: Chronic Kidney Failure; LVH: Left Ventricular Hypertrophy.
Table 2.
Epidemiological and clinical characteristics of obese hypertensives in multivariate analysis.
Table 2.
Epidemiological and clinical characteristics of obese hypertensives in multivariate analysis.
| Variables | Average values (N=230) |
Grade 1 obesity (n=170) |
Grade 3 obesity (n=17) |
odds ratio | 95% CI | p-value |
|---|---|---|---|---|---|---|
|
Abdominal Obesity Type 2 diabetes |
189(82.17) 28 (12.2%) |
132(77.64%) 17(10%) |
16(94.11%) 5 (29.4%) |
0.135 |
0.034–0.541 |
0.005 |
| Dyslipidemia | 37 (16.1%) | 26(15.3%) | 5 (29.4%) | 0.458 | 0.052-4.063 |
0.48 |
| Angina Pain | 17 (7.4%) | 12(7.1%) | 4 (23.5%) | 0.084 | 0.009–0.790 |
0.030 |
|
Arterial hypertension Grade 1 Grade 2 Grade 3 |
123(53.5%) 47 (20.4%) 60 (26.1%) |
91(53%) 33(19.4%) 46(27.1%) |
10(58.8%) 4(23.5%) 3(17.6%) |
0.602 | 0.157–2.305 | 0.45 |
|
Chronic Kidney Failure |
5 (2.2%) | 2 (1.2%) | 2 (11.8%) | 2,416 | 1.471–85.268 | 0.020 |
|
LVH |
18 (7.8%) | 13 (7.6%) | 1(5.9%) | 1,255 | 0.152–10.389 | 0.83 |
| LVH: Left ventricular hypertrophy. | ||||||
Table 3.
Cardiovascular risk stratification according to ESH.
| Variables | Average values (N=230) |
Grade 1 obesity (n=170) | Grade 2 obesity (n=43) | Grade 3 obesity (n=17) | p-value |
|---|---|---|---|---|---|
| Cardiovascular Risk Stratification | 0.32 | ||||
| Low Risk | 28(12.2) | 20(11.76%) | 5(11.62) | 3(17.64) | |
| Moderate Risk | 50(21.7) | 41(24.11%)) | 9(20.93) | 0(0%) | |
| High Risk | 103(44.8) | 73(42.94%) | 20(46.51) | 10(58.82) | |
| Very High Risk | 49(21.3) | 36(21.17%) | 9(20.93) | 4(23.52) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



