
Submitted:
05 September 2024
Posted:
06 September 2024
You are already at the latest version
Abstract
The unravelling of the human genome created new perceptions on the origin and evolution of diseases and for cancer in particular, it established the notion that neoplasia has been a companion of life since its ap-pearance on earth.
It is not surprising that neoplasms, in various forms, develop in numerous species of animals and even in plants. Unmistakable accounts of cancer with clinical features as are understood today, begin in the 5th c. B.C. The principles and practice of the Hippocratic and Galenic tradition dominated cancer care virtually into the 20th century. Advanced sequencing technologies at the dawn of the 21st century, generate new ther-apeutic opportunities with immunotherapy, oncolytic virotherapy and gene transfer, the latter especially in cases of hereditary cancer.
Keywords:
Hippocratic oncology
; Cancer
Introduction
The unravelling of the human genome [1] created new perceptions on the origin and evolution of diseases and for cancer in particular, it established the notion that neoplasia has been a companion of life since its appearance on earth.
It is not surprising that neoplasms, in various forms, develop in numerous species of animals [2,3] and even in plants, the latter when afflicted by phytoviruses or other infections, developing “unnatural growths", as Galen, the 2nd Century A.D. physician, would have articulated.
The ΤOR signalling pathway is ubiquitous in eukaryotic cells and has been evolutionarily conserved in fungi, plants, animals, and humans [4,5]. It is obvious that dysregulations of these functions by exogenous or genetic causes, can cause among others, uncontrolled cell proliferation, culminating in neoplasia.
The question, therefore, is not whether cancer existed in ancient societies – (it did!) – but whether the physicians of antiquity recognized it and described it as a distinct nosologic entity? There are inferences to growths in Egyptian papyri, variously interpreted as cancer, but the evidence is conjectural [6,7]. In Chinese language, according to Shan Jiang, of the Institute of Medical Humanities, Peking University, Beijing, China and Visiting Fellow at the Institute of Advanced Studies, University College, London (UCL), the terms zhongliu, and liu, have a broad meaning for all types of tumours, benign and malignant. On the other hand, ai, narrowly refers to malignant neoplasia. [8]. Shan Jiang’s report relates to data of the Chinese classical era (around 25-220 CE), specifically based on texts in (Yellow Emperor’s Inner Canon).
According to K.M.N. Kunzru and Radha Bhat, there is no actual concept of “Neoplasm” in Ayurveda, the ancient Indian System of Medicine. The surgeon-physician, Suśruta however, describes several tumour/neoplasm-like lesions in clinical and therapeutic detail in his monumental Compendium, Suśrutasamhitã. Suśruta trained, practised, and taught in the North Indian city Kãśi, modern Varanasi, sometime in the mid 1st Millennium BCE. [9].
Unmistakable accounts of cancer with clinical features as are understood today, begin in the 5th c. B.C. with Hippocrates of Cos, and evolve into the 7th c. A.D. with Paul of Aegina. At least fifteen physicians of this period describe the incidence of cancer predominantly in advanced age, the clinical characteristics, its life-threatening course and attempts to treat it [10].
The first thorough and systematic study of the ancient Greek literature on cancer is credited to the distinguished historian of Medicine, Aristotle P. Kouzis, who in 1902, as an Associate Professor of the History of Medicine at the National University of Athens, published a monograph entitled "CANCER AND THE ANCIENT GREEK PHYSICIANS" (O ΚAΡΚΙΝOΣ ΠAΡA ΤOΙΣ AΡΧAΙOΙΣ ΕΛΛHΣΙΝ ΙAΤΡOΙΣ) [11]. Aristotle Kouzis became later in life, President of the Academy of Athens.
In the Hippocratic Corpus, we find the terms Καρκίνος (Cancer), Καρκινοῦσθαι and Καρκινωθῆναι (becoming Cancerous) Καρκίνωμα (Carcinoma) and Καρκίνια (Small Cancers), with a clear reference to the disease as we know it today [10].
The term ὄγκος "tumour" is mentioned in at least 12 passages in the literature attributed to Hippocrates, but without an obvious association with the disease cancer.
The physician Bacchius from Tanagra in the province of Boeotia, Greece, who wrote in the 3rd century B.C., included among the Hippocratic treatises one, with the title "On Carcinosis" [10].
We may speculate that the author of this lost work would have discussed in detail the characteristics of cancer, perhaps even the etymology of the term, which, however, we find much later in Galen.
In the existing works of the Hippocratic collection, we find the description of a characteristic clinical picture of breast cancer: "The woman from Abdera developed breast cancer, and a blood-stained fluid was flowing from the nipple. When the discharge ceased, she died".
We have a clear reference to the frequency of cancer in advanced age and the fatal outcome of the disease. "In the elderly such tubercles do not develop. But deep and superficial cancers appear, from which they die" [10].
We encounter scepticism about the effectiveness of the treatment of deep-seated cancers, “These who develop deep cancers are better left untreated. Because with treatment they perish quickly, whereas without treatment they live longer."
Reference is also made to the application of thermal energy, as in our days, for the control of cancerous tumours "He, with the carcinoma in the pharynx, was cured by us with cauterization" [10].
And an observation, really admirable for the clinical acumen of the physicians of the Hippocratic era, which is often seen today in cases of immunosuppression, and which on occasions accompanies the development of neoplasia. "Of all the ulcers that spread, herpetes are the least harmful, but they are difficult to eradicate in the presence of deep-seated cancers" [10].
Some six centuries after Hippocrates, his commentator and admirer, Galen of Pergamum (120-200 A.D.?), provides a detailed clinical picture of cancer and the irrefutable testimony that the ancients knew and understood the disease, which today is diagnosed clinically, not infrequently, before the histological documentation of a carcinoma [10].
Galen informs us about the nomenclature of diseases and characteristically writes:
"Often a disease is named after the ailing part of the body, such as pleurisy, arthritis... sometimes from the symptom such as ileus, tenesmus, or spasm ... and sometimes from both, such as headache or otalgia... and sometimes when it resembles something outside the body such as elephantiasis or “cancer” or polyp...» [10].
In another passage, he provides the etymology and the definition of cancer: "Carcinoma is a malignant and indurated tumour, ulcerated or non-ulcerated. It is named after the animal cancer” [10].
Galen elaborates further on the clinical picture of breast cancer (8), arguing that the distended veins that in some cases surround the tumour, simulate in appearance the animal cancer (crab) "... He adds, “…and on the breasts we often saw tumours that looked exactly like the animal cancer. And just as the legs of the animal are lined up on either side of the body, so in this disease the distended veins of the unnatural growth form something resembling the crab (cancer)" [10].
Galen knows that cancer develops in all organs, he recognizes the high incidence of breast cancer during menopause, but he believes that as long as menstruation remains normal, women are not afflicted by the neoplasm [10].
Elsewhere, he repeats that carcinomas appear in all other parts of the body, "Cancers develop mainly in the breasts but also in the genital organs of men and women. But cancer can appear in any part of the body, occult, ulcerated, malignant." [10].
It would appear therefore that the common anatomical cancer sites observed today, were also common in antiquity.
Another term for cancer used by ancient Greek physicians is Θηρίωμα, “Therioma”.
Therion in Greek means wild beast and the word is probably used with an inference to the wild and uncontrolled nature of the disease or the monstrous appearance of some tumours [10].
Regarding the treatment of cancer, Galen boasts “…the early cancer we have cured, but the one that arose to considerable size, without surgery, no one has cured”! [10]. The position of comma after surgery is crucial, but it is uncertain if this was the case in the original text.
This dogma of convenience dominates the therapeutic philosophy of cancer even in our days!
Elsewhere, Galen advocates the complete excision of the tumour approaching normal tissues "The aim of every surgical intervention is the complete excision of the abnormal growth, in a circle, approaching the margins of normal tissue" [10].
The Alexandrian physician Leonidas or Leonides (2nd century A.D.), a contemporary of Galen, gives a detailed description of a mastectomy for cancer, followed with instructions of post-operative care. "… And in the case of carcinomas that do not adhere to the thorax, he writes, I operate in this manner. With the patient lying supine, I divide the healthy part of the breast above the carcinoma...and I cauterize the divided parts until haemostasis is achieved. Then, I incise the breast again, in depth, cauterizing the margins repeatedly until the bleeding is controlled...at the end and after the complete excision, I bring together the cauterised margins for the final reconstruction...” [10,11].
WHAT DID THE ANCIENTS KNOW ABOUT METASTASIS?
The word (μετάστασις) is found for the first time in the work of the Lyric Poet Simonides (6th–5th century B.C.). He laments the rapid and unexpected transition (μετάστασις) of man’s good fortune. Since then, the term has been used by philosophers, physicians, dramatists of comedy and tragedy, theologians, orators and others, but with meanings very different from the current use of the word for cancer dissemination.
For example, Plato and Aristotle, use metastasis when commenting on the transition, peaceful or violent, of a political system [12].
The word is introduced into the English literature for the first time towards the end of the 16th century but in a rhetorical sense, not as a medical term [12,13].
In the Hippocratic corpus, metastasis is mentioned at least nine times, in several treatises but without an apparent association with cancer!
For example, in the work ON THE SACRED DISEASE, one of the most important of the Hippocratic literature, the term metastasis is used in the discussion of pre-adolescent epilepsy (petit mal), which may cease during adulthood. In this case metastasis also means resolution of a disease or transition to health, rather than dissemination, as Galen explains in his comment on the relevant Hippocratic aphorism [12,13].
Although physicians had appreciated since the Hippocratic era that breast and uterine cancer could involve regional lymph-nodes, the word used for this development was “sympathy” (συμπάθεια), not metastasis [11,12].
The establishment of the term metastasis, in the context of cancer dissemination, must have been significantly influenced by Ashworth's publication in 1869, in which cancer cells in the bloodstream were mentioned for the first time [14]. Ashworth did not use the term metastasis but hinted at it by emphasizing that "cells observed in the blood invariably with those of cancer tend to illuminate the mode of origin of multiple tumours coexisting in the same individual" [14].
The first time that metastasis was indisputably used to mean cancer dissemination was, in all probability, in 1911; Homer Gage in his article on colon cancer, which was published in the Boston Medical and Surgical Journal, the precursor of the New England Journal of Medicine, wrote:
“It has been frequently observed that cancer of the sigmoid seems to retain its local character much longer than cancer in other parts of the large intestine and that lymphatic involvement and visceral metastases occur much later” [15].
CANCER THERAPEUTICS IN OUR ERA
The principles and practice of the Hippocratic and Galenic tradition dominated cancer care virtually into the 20th century with the precept “catch it early and cure it “, still an appealing concept repeatedly propagated in the medical literature, the press, and the media [16].
The dawn of the 20th century witnessed the emergence of a new treatment modality, radiotherapy, following the discovery of the X-rays by Wilhelm Conrad Röntgen in 1895 and of Radium by Marie Curie in 1898 [17]. Radiotherapy developed in Europe with the three major centres that pioneered and developed this new treatment modality, located in Manchester in the U.K., Villejuif (Institute Gustave Roussy) in France and the Radiumhemmet in Stockholm [17]. Early in the 20th century during the reign of King Gustav V, in Sweden, patients with cancer were entitled to free travel by train for treatment and follow up at the Radiumhemmet. This far-sighted approach, paradigmatic of Sweden’s leadership in social cohesion, was not only a humane treatment of cancer-sufferers but allowed at the same time exceptional possibilities for the documentation of treatment outcomes, both positive and negative, of radiation therapy [17]. These were, presumably, the origins of Sweden’s uniquely reliable, cancer-registry.
In the multidisciplinary approach to cancer, radiation therapy, especially with the latest developments in stereotactic radiotherapy, often referred to as radiosurgery [17], and recent advances in particle therapy, remains an important component of cancer treatment for a significant number of selected patients with this disease.
It took two World Wars in the last century and a weapon of chemical warfare, for oncology to enter the era of systemic treatment for a widely disseminated cancer. Mechlorethamine hydrochloride, also known as nitrogen mustard or mustine, targeting the cell’s DNA, in combination with vincristine, procarbazine and prednisone, launched the new approach for the conquest of widespread neoplasia, ultimately rendering Hodgkin’s lymphoma curable for the majority of patients [18]. Thomas Hodgkin (1798-1866) the pathologist at Guy’s Hospital in London, described the disease that bears his name in 1832, an incurable cancer in those days.
The introduction, in parallel, of the antimetabolite methotrexate, a folate antagonist, transformed a previously invariably lethal neoplasm, choriocarcinoma, into a treatable and eventually a highly curable cancer [19]. Anticancer drugs, derived initially from plants and subsequently produced semi -synthetically, include podophyllotoxin (etoposide), and the vinca alkaloids, vincristine, vinblastine, vindesine and vinorelbine, which interact with tubulin and prevent microtubule formation, an essential component of cellular division.
A screening programme for phytopharmaceuticals culminated in the development of Paclitaxel and Docetaxel, two of the most effective drugs against refractory cancers. Synthetic analogues of the original drugs reduced significantly the cost of production and the impact on the environment. Additional examples of anti-cancer drugs derived from plants are harringtonine, homoharringtonine and isoharringtonine, the alkaloids from Cephalotaxus harringtonia; they exert antitumour activity by interfering with protein synthesis [20].
The inhibitory activity of cis-platin on cell division was noted in 1965 by the biophysicist Barnett Rosenberg [21]. Among other actions it arrests DNA replication leading to apoptosis or cell necrosis. Cis-platin entered clinical practice in 1978 and exhibited activity in a broad spectrum of neoplasms; it proved particularly effective in testicular carcinoma, another example of a curable neoplasm for the majority of patients with widespread disease.
Cisplatin’s efficacy in a broad spectrum of malignancies is limited by its nephrotoxicity and neurotoxicity, especially ototoxicity. It is also a highly emetogenic drug; this significant toxicity which may have forced some patients to abandon an otherwise effective treatment, led to the development of new effective antiemetic agents that made treatment more tolerable [22]. The toxicity of cis-platin led also to the development of the synthetic analogues carboplatin and oxaliplatin [21].
Examples of what, in the past, could be argued constituted “palliative” chemotherapy for a tumour broadly considered, notoriously refractory to treatment, are illustrated in Figure 1, Figure 2, Figure 3 and Figure 4.
Response to the combination chemotherapy with cisplatin-vinblastine-vindesine, right, 2b.
Before and after chemotherapy.
Figure 1a,b illustrate the dramatic resolution of large subcutaneous masses in a patient with disseminated melanoma before, and after 6 courses of treatment with the Vinca alkaloid drug Vindesine, in the 1970’s.
Figure 2a,b. The target lesion in this patient progressed after Radiotherapy.
Both lesions shown, responded to the combination chemotherapy with cisplatin-vinblastine-vindesine. Chemotherapy caused complete alopecia, but hair regrew upon cessation of treatment.
Figure 3a,b. Illustrate the case of a patient with numerous visceral and cutaneous lesions, some ulcerating with odorous discharge, intolerable to the patient and the carers. This patient was referred from a Palliative Care Unit to the Westminster Hospital, in London, U.K. Figure 3a, illustrates a selected lesion before commencement of chemotherapy with the DJV3 combination, (Dacarbazine, Vincristine, Vindesine, Vinblastine, Carboplatin) and Figure 3b, after treatment, with significant palliation of the target lesion shown and complete resolution of other masses. (Image reproduced in colour from Retsas, S. et al. [23].
Figure 4a,b. This patient with disseminated melanoma with multiple pulmonary lesions and an ulcerating mass on the right knee, the site of the primary lesion. Treated in the late 1980’s with combination chemotherapy with the DJV3 combination (sse above, Fig. 3a & 3b). Resolution with treatment of pulmonary lesions and healing of the soft-tissue mass overlying the right knee. (Image reproduced and supplemeted in colour from Retsas, S. et al [23].
All pictures displayed in this communication, emanate from the archives of the Medical Illustration Department of Westminster and Chelsea and Westminster Hospitals, in London, U.K., and were obtained with the patients’ full and written consent.
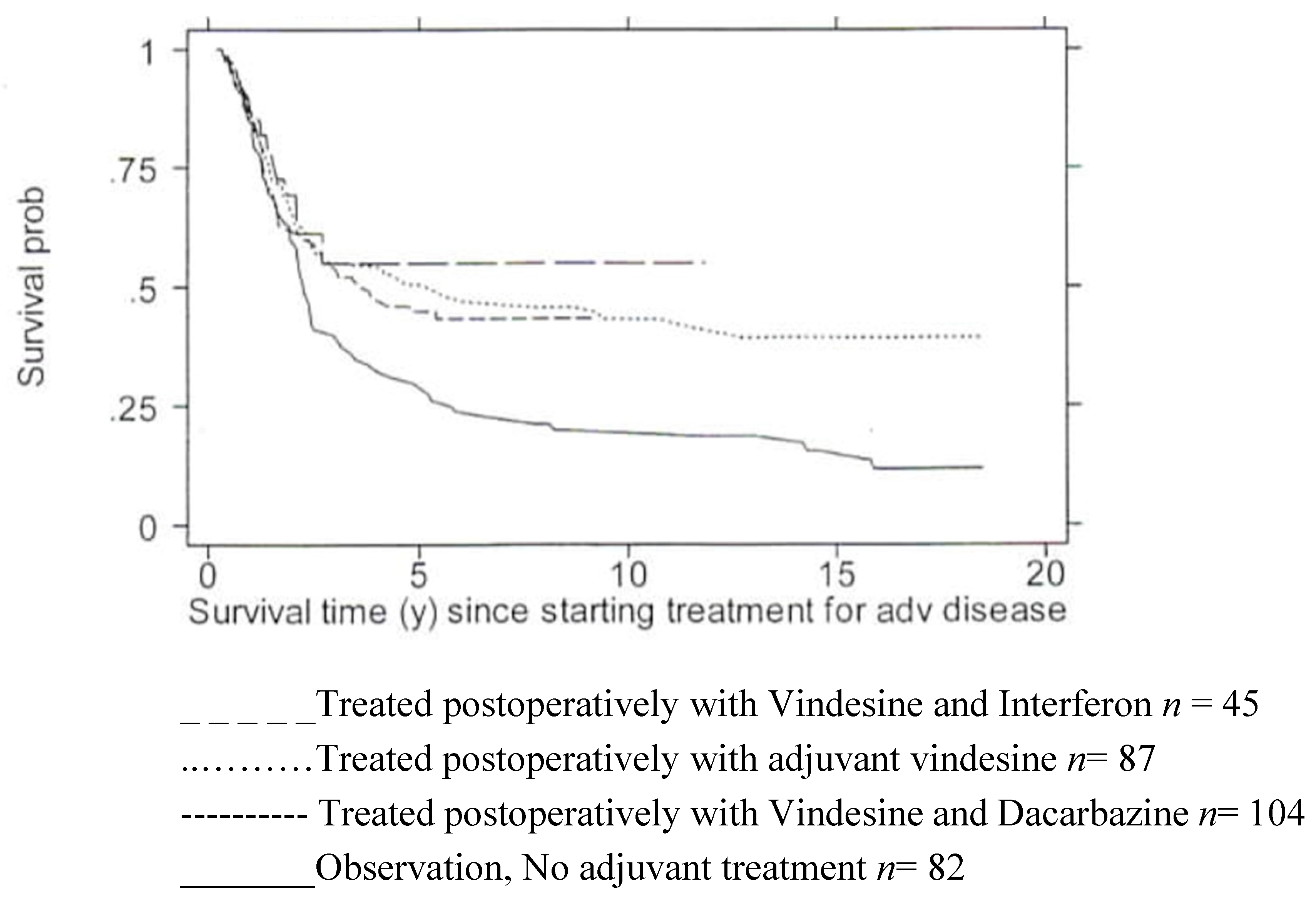
Figure 5. Shows the observed survival in years from a single institution, of 318 patients with metastatic melanoma from the time of diagnosis of clinical and pathological involvement of regional lymph nodes, AJCC Stage III disease. Survival is calculated in years, from the onset of systemic treatment with three sequential treatment protocols, following complete resection of lymph nodes in the involved basin (n = 236), or no adjuvant treatment (n=82). Treatment was not randomly allocated. Some patients who did not receive adjuvant treatment for stage III disease, may have subsequently been treated upon widespread dissemination with treatments, as described in Figure 1 & Figure 2.
The data, obtained from the melanoma Unit at Charing Cross Hospital, Chelsea and Westminster and Westminster Hospitals, in London, were independently analysed by Professor Patrick Royston (MRC Clinical Trials Unit, 18 June 2001)
These results were presented and discussed at the 4th International Conference on The Adjuvant Therapy of Malignant Melanoma, held at the Royal College of Physicians of London, in 15-16 March 2002. [24]. This analysis followed an earlier report that included the first – 169 patients of this cohort. [25]. The full MRC report of this analysis is available on request.
Despite the plethora of anticancer agents, at the end of the last century, only a small number of disseminated solid tumours was curable with the available systemic treatments; choriocarcinoma, lymphoma, and germ cell tumours mentioned above. As we approach the conclusion of the first quarter of the 21st century, endowed with new insights into the neoplastic process at the molecular and genomic level, and with indisputable improvements in the response rates and the duration of such responses, the number of curable cancers, so far, has hardly increased.
Although pre-operative systemic treatment – often referred to in the literature as neoadjuvant - had been attempted with limited success in selected tumours in the 20th century [26], the higher response rates and more durable responses with the newer treatments of the 21st century make neoadjuvant systemic treatments an increasingly appealing option for some solid neoplasms [27,28,29].
But the 20th century also witnessed the emergence of targeted therapy. By recruiting an ancient drug, arsenic trioxide, into the treatment of one of the most lethal haematological malignancies, acute promyelocytic leukaemia became curable for the majority of sufferers! [30,31,32,33]
The newer sequencing technologies at the dawn of the 21st century have opened a new era of therapeutic intervention broadly, as well as, at the personal genome.
The development and refinement of liquid biopsies taking advantage of body fluids such as blood, saliva or urine, is generating new opportunities for the non-invasive diagnosis and follow up, especially of tumours with high risk for relapse [34].
Beginning with iodine-131 for the diagnosis and treatment of Thyroid cancer, more recent application of radiopharmaceuticals - so called theranostics or theragnostics - is contributing to the management of some neuroendocrine tumours and prostate cancer [35]. Theranostics refers to a material that serves the combined diagnosis, treatment and follow up of a disease.
Gene therapy for cancer treatment, encompasses different approaches such as immunotherapy, oncolysis mediated by viruses and gene transfer [36].
Cell-based therapies using chimeric antigen receptor T cells (CAR-T) are the latest approach in the genomic era, with some notable responses in haematologic malignancies and refractory B and plasma cell lymphomata, but so far without successful application in solid tumours. This novel therapeutic approach is not without considerable toxicity which, in addition to other methodological issues, limits its application in the common solid tumours [37,38,39,40]. Concern has also been raised about the risk, albeit rare, of the development of secondary neoplasms following CAR-T cell therapy [37,38,39,40].
The recent report of restoration of hearing in a child with congenital deafness is an example of intervention with gene transfer into the personal genome [41]. We may anticipate parallel applications in oncology in the future, especially in cases of hereditary cancer [42,43].
New ethical issues are now emerging regarding hereditary cancers [44] affecting not only the patients but also close family members and relatives; their impact is being addressed and debated [44]. Time will decide about potential risks, and unanticipated long-term side-effects from the intrusion into the genome and similar interventions.
As well as spectacular advances, already seen in the treatment of cancer, puzzles in the biology of the disease await answers that will, hopefully, be provided by further advances in the study of the human genome in the near future, both in health and disease.
In our time, we wonder about the behaviour of metastasis, a biological process, characterised by some investigators, as highly inefficient since only 0.01% of circulating tumour cells eventually succeed in forming secondary tumours [45,46].
We are still puzzled by the tendency of ocular melanoma to metastasize to the liver in 95% of cases, some 20 years or very much longer, after ablation of the primary focus or enucleation of the affected eye, while the same neoplasm rarely metastasizes to the anatomically adjacent brain [47,48]. Is the metastatic behaviour of this particular cancer the result of hematogenous spread, or is it a heterotopic, after decades, revival of the neoplasm, related to some hitherto unknown tissue "sympathy" between the choroid and the hepar?
Perhaps newer advances in the biology of cancer from the study of the human genome will, one-day, decode this asymmetric relationship between the eye and the liver.
References
- Watson, J.; Crick, F. Molecular Structure of Nucleic Acids: A Structure for Deoxyribose Nucleic Acid. Nature 1953, 171, 737–738. [Google Scholar] [CrossRef] [PubMed]
- Pavlidis, N. The diachronic presence of cancer on Planet Earth. PALAEO-ONCOLOGY: Historical Review of Cancer from Antiquity to the 21st century. Proceedings of the 2nd International Symposium of the European Society for the History of Oncology. Research Centre for the Hellenic and Latin Literature. Academy of Athens, Greece, 2020; pp. 21–33, ISBN 978-960-404-367-5 (In Greek).
- Parisi, F.; Aurisicchio, L.; Pecorari, A.; Poli, A.; Millanta, F. A Preliminary Evaluation of the Prognostic Role of HER-2 and HER-3 Immunohistochemical Expression in Canine Melanomas ANIMALS 2024, 14. [CrossRef]
- Henriques, R.; Borge, L.; Horvath, B.; Magyar, Z. Balancing act: matching growth with environment by the TOR signalling Pathway. J Exp Bot. 2014, 65, 2691–2701. [Google Scholar] [CrossRef] [PubMed]
- Yang Xiong; and Jen Sheen. The role of target of Rapamycin Signalling Networks in Plant Growth and metabolism. Plant Physiology February 2014, 164, 499–512. [Google Scholar] [CrossRef] [PubMed]
- Ghalioungui, P. Malignancy in Ancient Egypt. In Palaeo-Oncology. The Antiquity of Cancer; Retsas, S., Ed.; Farrand Press: London, UK, 1986; pp. 27–33. ISBN 1-85083 006 1. [Google Scholar]
- Fawzi Sweha Boulos. Oncology in Egyptian Papyri. In Palaeo-Oncology. The Antiquity of Cancer. Retsas, S. Ed.; Farrand Press, London, UK, 1986, pp.35-40, ISBN 1-85083 006 1.
- Shan, Jiang. Naming, Explanations, Treatments: Knowledge of Tumour from Chinese Classical Era. Presented at An International Colloquium on PALAEO-ONCOLOGY, The Antiquity of Cancer, organised By the European Society for the History of Oncology and The Hellenic Medical Society – UK. November 16, 2018. Abs. No 8. At the Hellenic Centre, London, U.K. An ESO recommended Event. 16 November 2018.
- Kunzru, K.M.N.; Bhat, R. Tumours in Ancient India: A reading of Suśrutasamhitã. PALAEO-ONCOLOGY: Historical Review of Cancer from Antiquity to the 21st century. Proceedings of the 2nd International Symposium of the European Society for the History of Oncology. Research Centre for the Hellenic and Latin Literature. Academy of Athens, Greece, 2020; pp. 107–122, ISBN 978-960-404-367-5.
- Retsas, S. On the Antiquity of Cancer; from Hippocrates to Galen. In Palaeo-Oncology. The Antiquity of Cancer. Retsas, S. Ed.; Farrand Press, London, UK, 1986, pp.41-53, ISBN 1-85083 006 1.
- Kouzis, A. CANCER AND THE ANCIENT GREEK PHYSICIANS. (O ΚAΡΚΙΝOΣ ΠAΡA ΤOΙΣ AΡΧAΙOΙΣ ΕΛΛHΣΙΝ ΙAΤΡOΙΣ). Athens Medical Society, 1902. (In Greek).
- Retsas, S. Palaeo-Oncology: Diachronic perceptions of the meaning of the term Metastasis. PALAEO-ONCOLOGY: Historical Review of Cancer from Antiquity to the 21st century. Proceedings of the 2nd International Symposium of the European Society for the History of Oncology. Research Centre for the Hellenic and Latin Literature. Academy of Athens, Greece, 2020; pp. 93–106, ISBN 978-960-404-367-5 (in Greek).
- Retsas, S. Cancer and the arts: metastasis - as perceived through the ages. ESMO Open 2017, 2, e000226. [Google Scholar] [CrossRef]
- Ashworth, T.R. A case of cancer in which cells similar to those in the tumours were seen in the blood after death. Australian Medical Journal 1869, 14, 146–147. [Google Scholar]
- Gage, H. Cancer of the Colon. Boston Medical and Surgical Journal. 1911, CLXV, 474–479. [Google Scholar] [CrossRef]
- Retsas, S. COVID-19 and cancer: Revisiting "The comfort zone". Hell J Nucl Med. 2020, 23, 65–69. [Google Scholar] [PubMed]
- Ringborg, U. The Radiumhemmet – A Historic Centre for Cancer Research and Treatment. PALAEO-ONCOLOGY: Historical Review of Cancer from Antiquity to the 21st century. Proceedings of the 2nd International Symposium of the European Society for the History of Oncology. Research Centre for the Hellenic and Latin Literature. Academy of Athens, Greece, 2020; pp. 157–168, ISBN 978-960-404-367-5.
- DeVita, V.T., Jr.; Jaffe, E.S.; Hellman, S. Hodgkin’s Disease and the Non-Hodgkin’s Lymphomas. Chapter 44. In Cancer Principles and Practice of Oncology.; DeVita, V.T. Jr., Rosenberg, S.A., Hellman, S. Eds.; J.B. Lippincott Company Philadelphia. 1985. Second Edition, pp 1623-1709. ISBN 0-397-50632-5.
- Chin, A.C. Methotrexate for gestational choriocarcinoma: a paradigm shift in oncology. Nat Rev Endocrinol 2023, 19, 501. [Google Scholar] [CrossRef]
- Powell RG, Weisleder D, Smith CR Jr, Rohwedder WK. Structures of harringtonine, isoharringtonine, and homoharringtonine. Tetrahedron Lett. 1970, 815–818. [CrossRef] [PubMed]
- Monneret, C. Platinum anticancer drugs. From serendipity to rational design. Ann Pharm Fr. 2011, 69, 286–295. [Google Scholar] [CrossRef] [PubMed]
- Sagar SM, Bayliss MA, Chong SL, Retsas, S. Ondansetron; further progress in the prevention of nausea and vomiting induced by anti-cancer chemotherapy. Clin Oncol (R Coll Radiol). 1991, 3, 183. [CrossRef] [PubMed]
- Retsas, S.; Bayliss, M.; Sheikh, N.; Chong, S.L.; Bafaloukos, D. Chemotherapy of malignant melanoma: The European Experience. La Revue de Médicine Interne Mars-Avril 1990 51-58 – Tome XI (Supplément au Numéro 2).
- Retsas, S.; MacRae, K.; Henry, K. Adjuvant Treatment for clinically apparent lymph node metastases (≥N1b) from melanoma: single-institution experience from a cohort of 318 patients. Abstract 26; Melanoma Research – Vol. 12 - 2002, A15.
- Retsas S, Quigley M, Pectasides, D, Macrae, K., Henry, K. Clinical and histologic involvement of regional lymph nodes in malignant melanoma. Adjuvant vindesine improves survival. Cancer 1994, 73, 2119–2130. [CrossRef] [PubMed]
- Retsas, S. Scientific evidence and expert clinical opinion for the investigation and management of stage III malignant melanoma – medical intervention. Chapter 6. In The Effective Management of Malignant Melanoma. MacKie, R.M., Murray, D., Rosin, R.D., Hancock, B., and Miles, A. Eds. Pp 65-82. Uk key advances in clinical practice series 2001. Aesculapius Medical Press.
- Chalabi, M.; Verschoor, Y.L.; Tan, P.B.; Balduzzi, S.; Van Lent, A.U.; Grootscholten, C.; Dokter, S.; Büller, N.V.; Grotenhuis, B.A.; Kuhlmann, K.; et al. Neoadjuvant Immunotherapy in Locally Advanced Mismatch Repair-Deficient Colon Cancer. N Engl J Med. 2024, 390, 1949–1958. [Google Scholar] [CrossRef] [PubMed]
- Menzies, A.M.; Amaria, R.N.; Rozeman, E.A.; et al. Pathological response and survival with neoadjuvant therapy in melanoma: a pooled analysis from the International Neoadjuvant Melanoma Consortium (INMC). Nat Med. 2021, 27, 301–309. [Google Scholar] [CrossRef]
- Patel, S.P.; Othus, M.; Chen, Y.,; Wright, G.P. Jr; Yost, K.J.; Hyngstrom, J.R.; Hu-Lieskovan, S.; Lao, C.D.; Fecher, L.A.; Truong, T.G. Neoadjuvant-Adjuvant or Adjuvant-Only Pembrolizumab in Advanced Melanoma. N Engl J Med. 2023, 388, 813–823. [CrossRef] [PubMed] [PubMed Central]
- Lo-Coco, F.; Avvisati, G.; Vignetti, M.; Thiede, C.; Orlando, S.M.; Iacobelli, S.; Ferrara, F.; Fazi, P.; Cicconi, L.; Di Bona, E.; et al. Gruppo Italiano Malattie Ematologiche dell'Adulto; German-Austrian Acute Myeloid Leukemia Study Group; Study Alliance Leukemia. Retinoic acid and arsenic trioxide for acute promyelocytic leukemia. N Engl J Med. 2013, 369, 111–121. [Google Scholar] [CrossRef] [PubMed]
- de Thé, H. Lessons taught by acute promyelocytic leukemia cure. Lancet. 2015, 386, 247–248. [Google Scholar] [CrossRef] [PubMed]
- Ernberg, I. From the first curative targeted cancer treatment to the implementation of the most extensive healthcare reform. J Intern Med. 2015, 278, 643–644. [Google Scholar] [CrossRef] [PubMed]
- Retsas, S. Geotherapeutics: the medicinal use of earths, minerals and metals from antiquity to the twenty-first century. In Geology and Medicine: Historical Connections Duffin, C.J., Gardner-Thorpe, C., and Moody, R.T.J. Eds; 2017, 133-139. London Geological Society Special Publication No. 452. 2017. [Google Scholar]
- Yu, D. Li, Y., Wang, M. et al. Exosomes as a new frontier of cancer liquid biopsy. Mol Cancer 2022, 21, 56. [Google Scholar] [CrossRef]
- Zoi, V.; Giannakopoulou, M.; Alexiou, G.A.; Bouziotis, P.; Thalasselis, S.; Tzakos, A.G.; Fotopoulos, A.; Papadopoulos, A.N.; Kyritsis, A.P.; Sioka, C. Nuclear Medicine and Cancer Theragnostics: Basic Concepts. Diagnostics (Basel). 2023, 13, 3064. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cross, D.; Burmester, J.K. Gene therapy for cancer treatment: past, present and future. Clin Med Res. 2006, 4, 218–227. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bailey, S.R.; Berger, T.R.; Graham, C.; Larson, R.C.; Maus, M.V. Four challenges to CAR T cells breaking the glass ceiling. Eur J Immunol. 2023, 53, e2250039. [Google Scholar] [CrossRef] [PubMed]
- Abramson, J.S.; Solomon, S.R.; Arnason, J.; Johnston, P.B.; Glass, B.; Bachanova, V.; Ibrahimi, S.; Mielke, S.; Mutsaers, P.; Hernandez-Ilizaliturri, F.; et al. Plain language summary of the TRANSFORM study primary analysis results: lisocabtagene maraleucel as a second treatment regimen for large B-cell lymphoma following failure of the first treatment regimen. Future Oncol. 2024 Mar 28. [CrossRef] [PubMed]
- CAR T-cell therapy for solid tumours. Editorial. The Lancet Oncology. July 2021. [CrossRef]
- Hamilton, M.P.; Sugio, T.; Noordenbos, T.; Shi, S.; Bulterys, P.L.; Liu, C.L.; Kang, X.; Olsen, M.N.; Good, Z.; Dahiya, S.; et al. Risk of second tumours and T-Cell lymphoma after CAR T-Cell Therapy. N Engl J Med 2024, 390, 2047–2060. [Google Scholar] [CrossRef]
- Lv, J.; Wang, H.; Cheng, X.; Chen, Y.; Wang, D.; Zhang, L.; Cao, Q.; Tang, H.; Hu, S.; Gao, K.; Xun, M.; et al. AAV1-hOTOF gene therapy for autosomal recessive deafness 9: a single-arm trial. Lancet. 2024, 403, 2317–2325. [Google Scholar] [CrossRef] [PubMed]
- Samadder, N.J.; Giridhar, K.V.; Baffy, N.; Riegert-Johnson, D.; Couch, F.J. Hereditary Cancer Syndromes-A Primer on Diagnosis and Management: Part 1: Breast-Ovarian Cancer Syndromes. Mayo Clin Proc. 2019, 94, 1084–1098. [Google Scholar] [CrossRef] [PubMed]
- Samadder, N.J.; Baffy, N.; Giridhar, K.V.; Couch, F.J.; Riegert-Johnson, D. Hereditary Cancer Syndromes-A Primer on Diagnosis and Management, Part 2: Gastrointestinal Cancer Syndromes. Mayo Clin Proc. 2019, 94, 1099–1116. [Google Scholar] [CrossRef] [PubMed]
- Winkler, E.C.; Knoppers, B.M. Ethical challenges of precision cancer medicine. Seminars in Cancer Biology 2022, 84, 263–270. [Google Scholar] [CrossRef]
- Fidler, I.J. Metastasis: quantitative analysis of distribution and fate of tumor emboli labelled with 125 I-5-iodo-2'-deoxyuridine. J Natl Cancer Inst 1970, 45, 773–782. [Google Scholar]
- Langley, R.R.; Fidler, I.J. The seed and soil hypothesis revisited – the role of tumor-stroma interactions in metastasis to different organs. Int J Cancer 2011, 128, 2527–2535. [Google Scholar] [CrossRef]
- Jensen, O.A. Malignant melanomas of the human uvea: 25-year follow-up of cases in Denmark, 1943--1952. Acta Ophthalmol (Copenh). 1982, 60, 161–182. [Google Scholar] [CrossRef] [PubMed]
- Kujala, E.; Mäkitie, T.; Kivelä, T. Very long-term prognosis of patients with malignant uveal melanoma. Invest Ophthalmol Vis Sci. 2003, 44, 4651–4659. [Google Scholar] [CrossRef] [PubMed]
- Editorial. Lung Cancer Treatment: 20 years of progress. www.thelancet.com Vol 403 June 22, 2024; 2663.
- Ringborg, U.; von Braun, J.; Celis, J.; et al. Strategies to decrease inequalities in cancer therapeutics, care and prevention. Mol Oncol 2024, 18, 245–279. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
a and 1b. Multiple subcutaneous masses from metastatic melanoma. Before, 1a left. and after six courses of chemotherapy with Vindesine, 1b right.
Figure 1.
a and 1b. Multiple subcutaneous masses from metastatic melanoma. Before, 1a left. and after six courses of chemotherapy with Vindesine, 1b right.
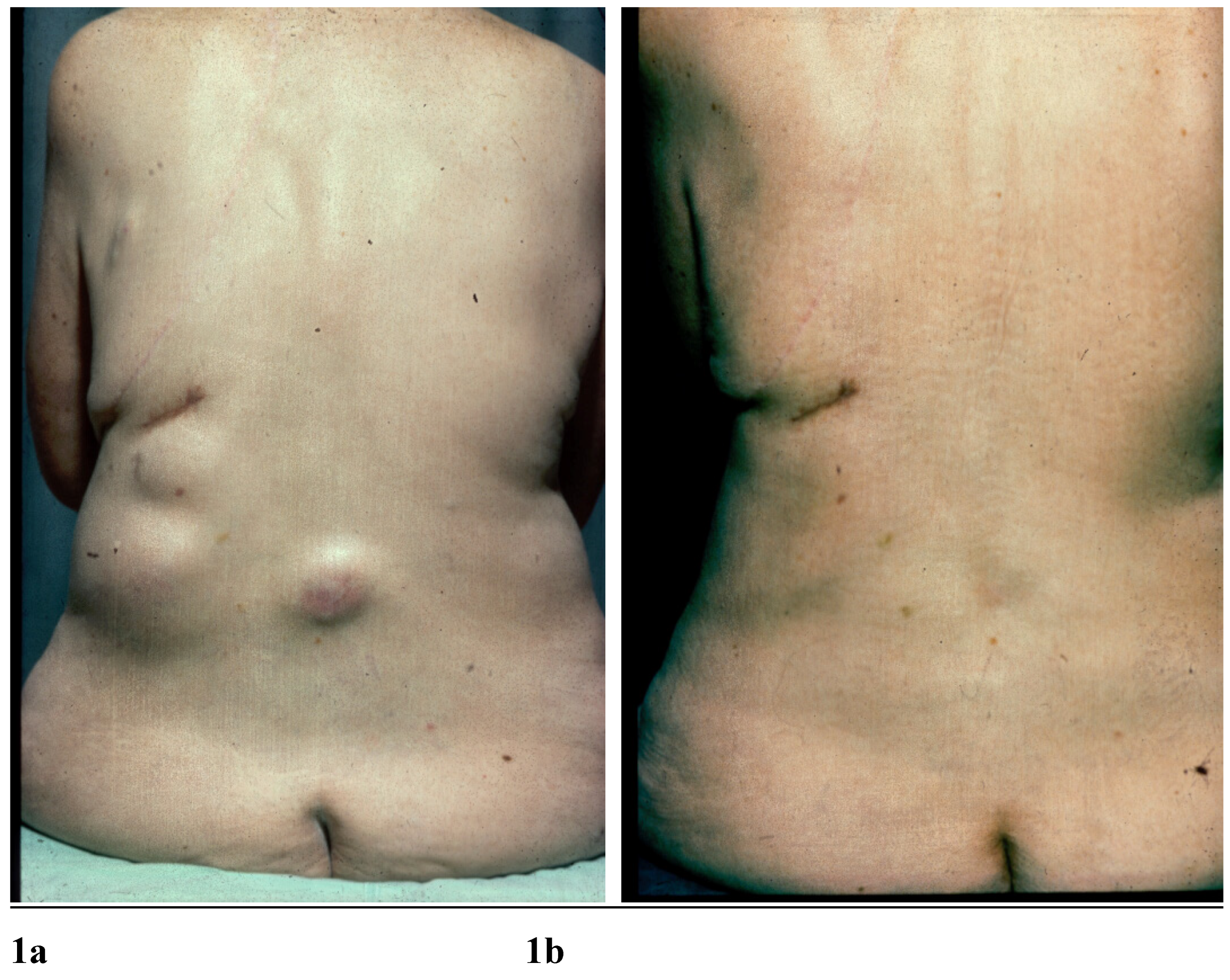
Figure 2.
a & 2b. Metastatic melanoma. Progression after Radiotherapy, left, 2a.
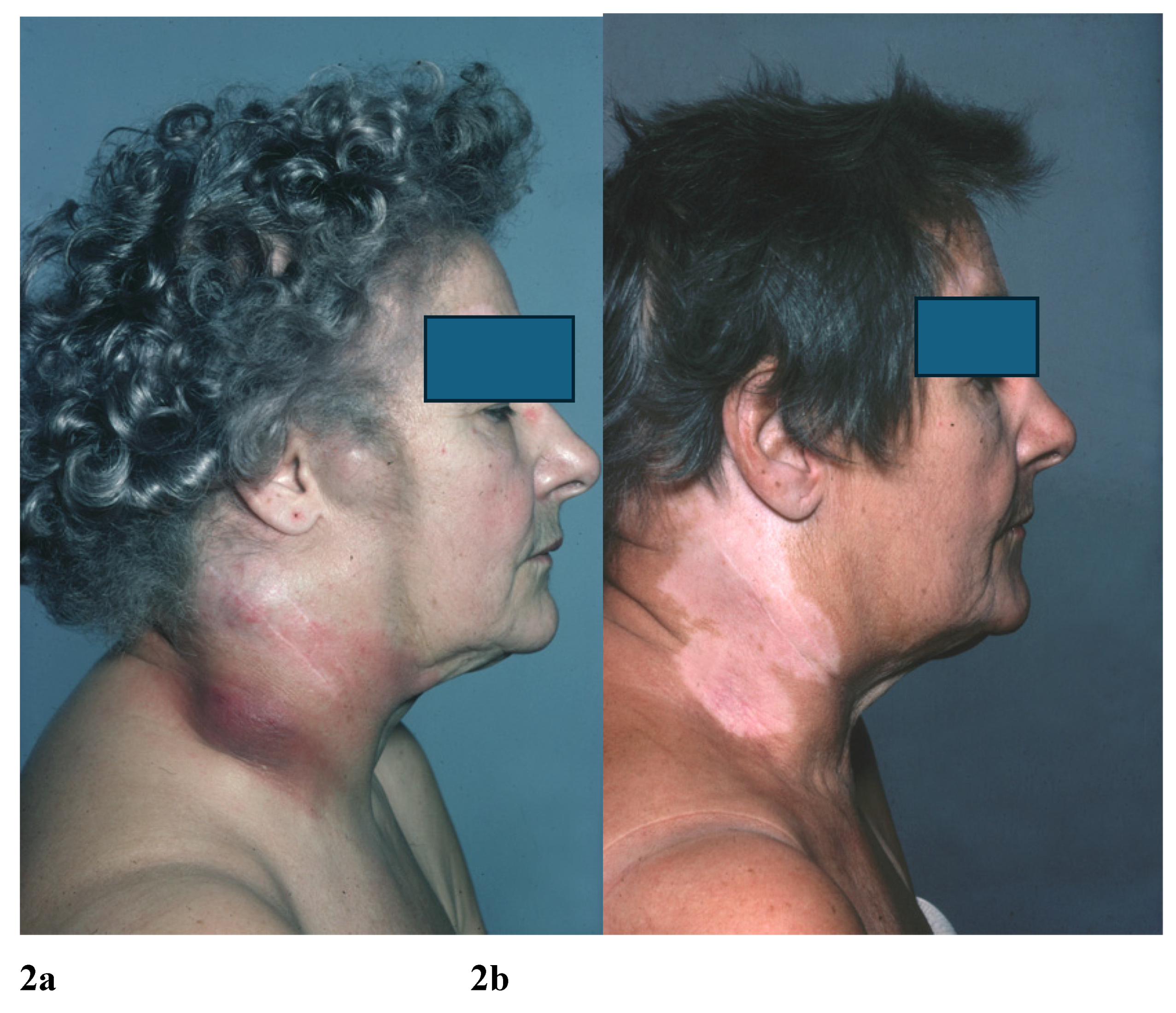
Figure 3.
a & 3b. What the ancients would have called a “Therioma”.
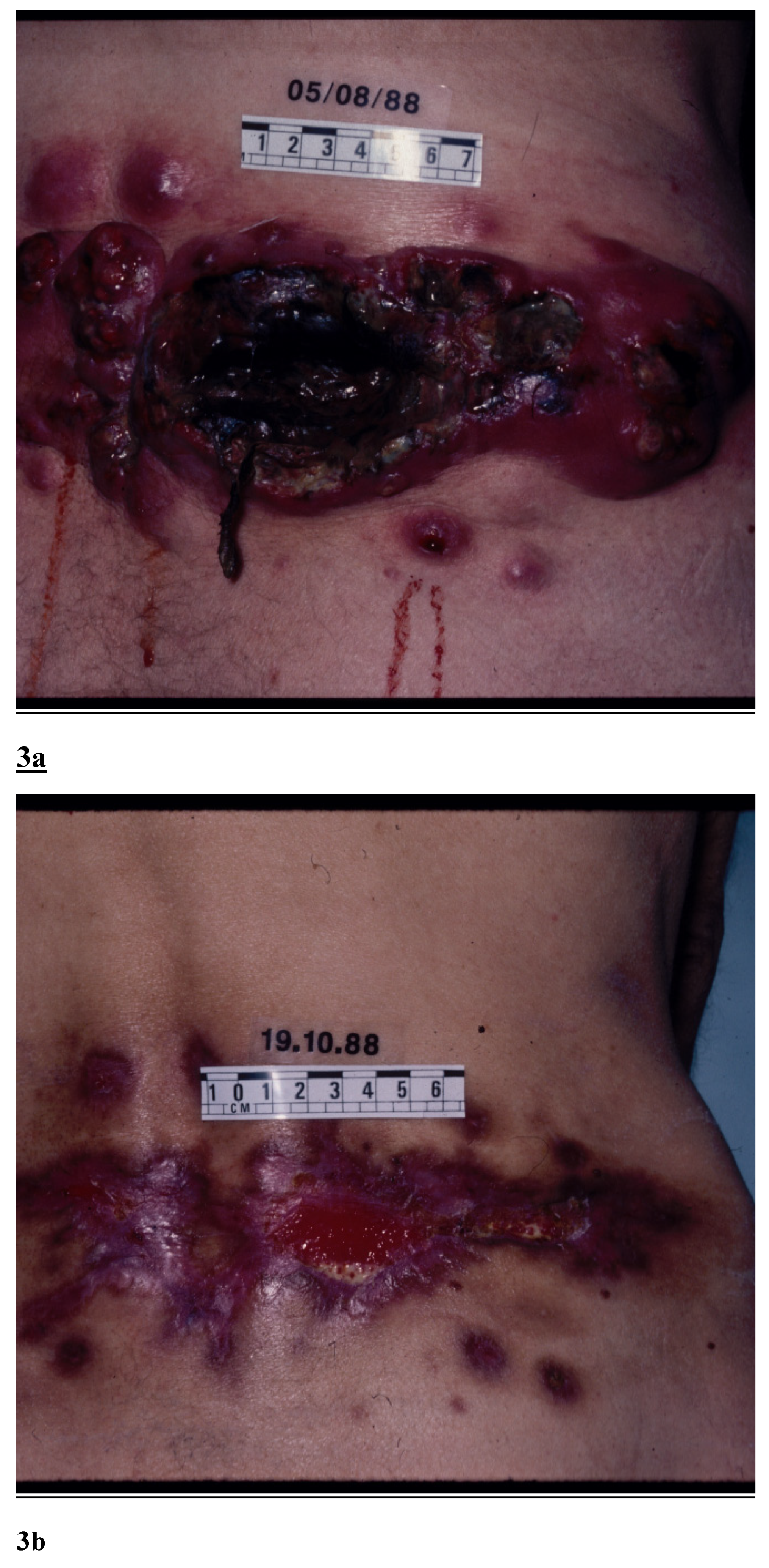
Figure 4.
a & b Before treatment. c & d after treatment.
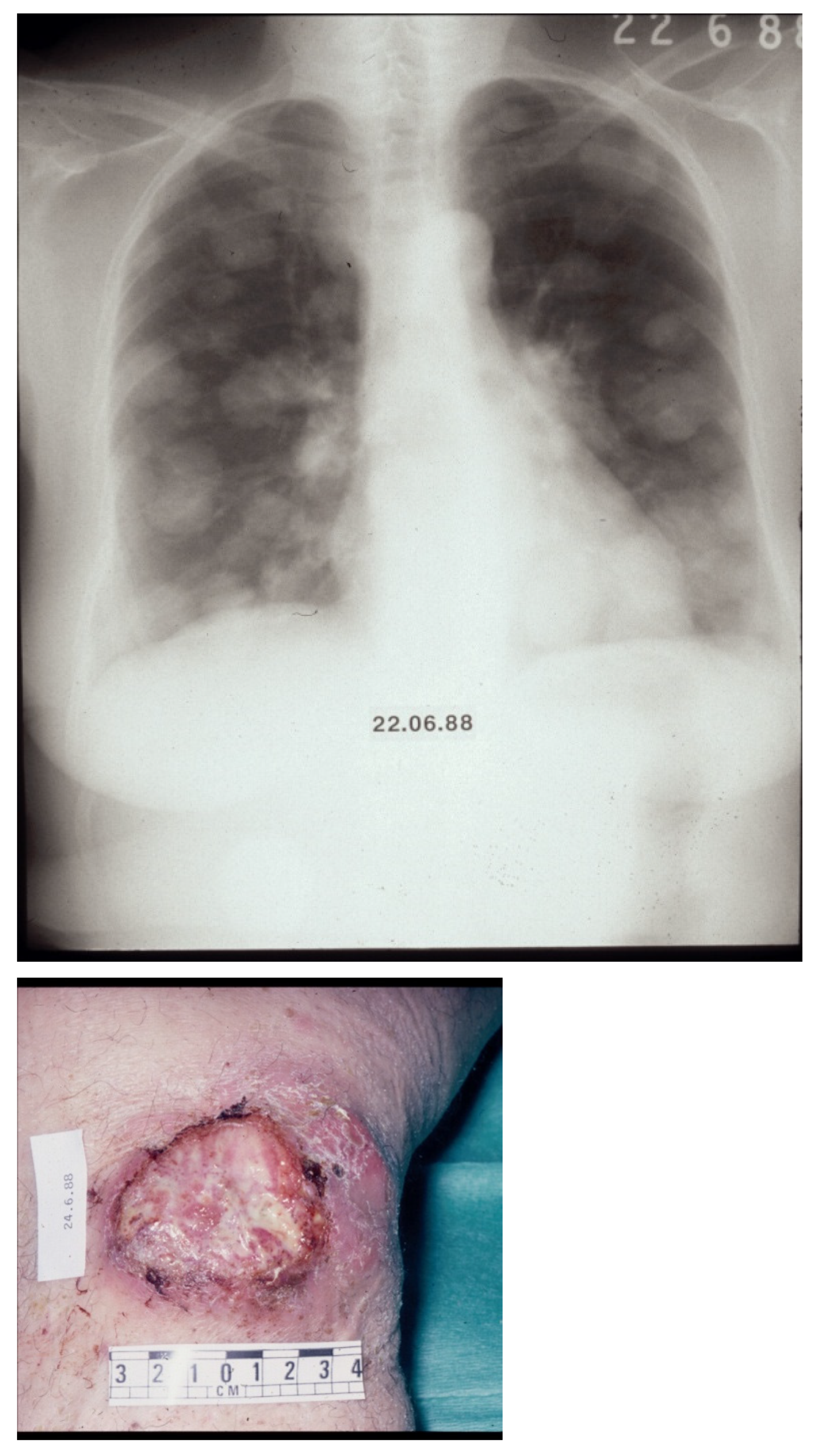
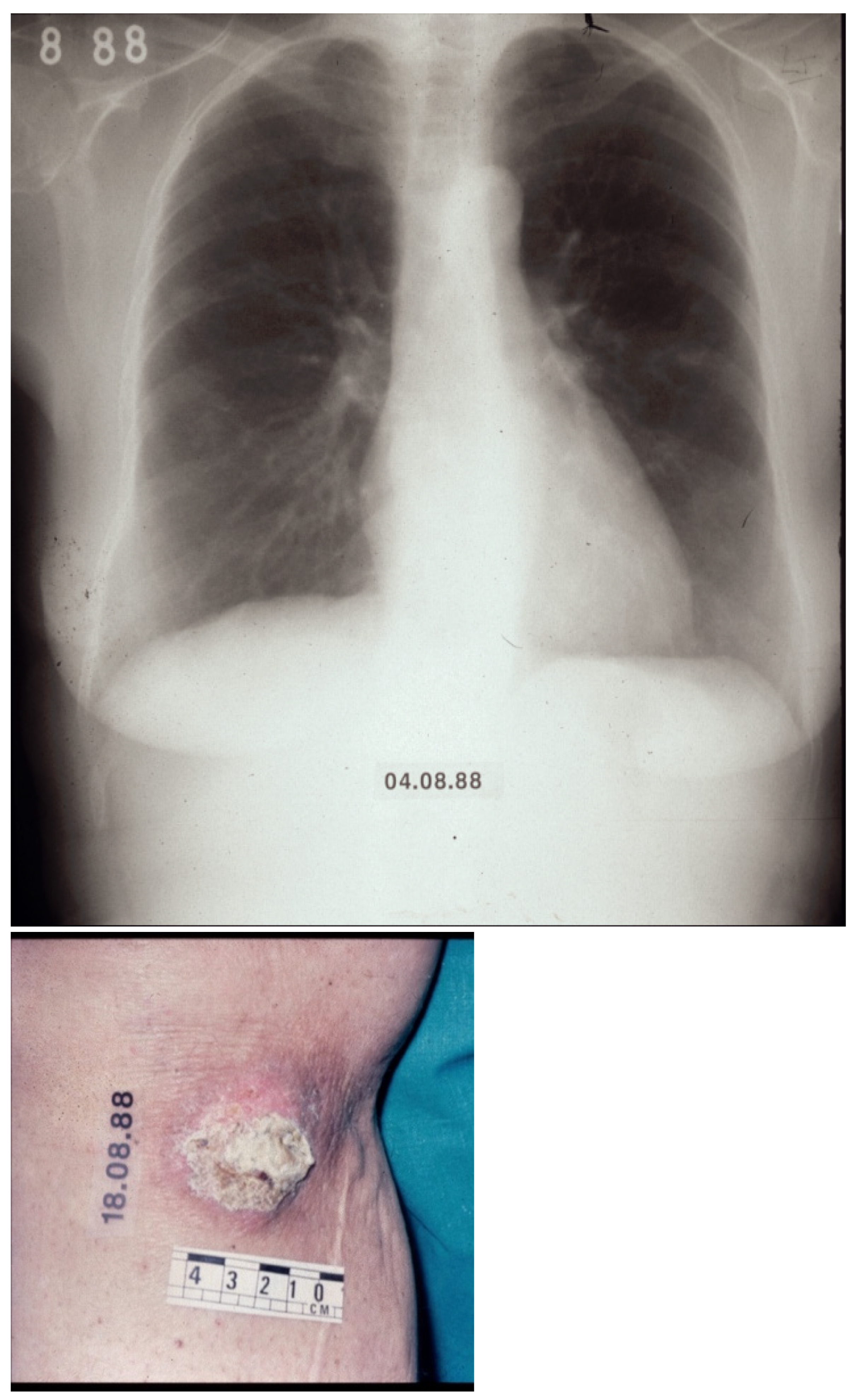
Figure 5.
Observed survival in years, of 318 patients with metastatic melanoma from diagnosis of clinical and pathological involvement of regional lymph nodes, AJCC Stage III disease. From onset of adjuvant systemic treatment following complete resection of lymph nodes (n=236) in the involved basin, or no adjuvant treatment (n=82).
Figure 5.
Observed survival in years, of 318 patients with metastatic melanoma from diagnosis of clinical and pathological involvement of regional lymph nodes, AJCC Stage III disease. From onset of adjuvant systemic treatment following complete resection of lymph nodes (n=236) in the involved basin, or no adjuvant treatment (n=82).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



