
Submitted:
06 September 2024
Posted:
06 September 2024
You are already at the latest version
Abstract
Recent mental health research has highlighted inflammation's critical role in conditions like depression and bipolar disorder, examining correlations with markers such as calcium levels, thyroid function, and inflammatory markers. The study aims to compare unipolar and bipolar d depression samples in terms of socio-demographic and clinical features. Prospective enrollment of patients hospitalized at the University of Insubria Psychiatric Unit. Patients were administered psychometric questionnaires (Beck Depression Inventory-II, Mental Pain Questionnaire, Beck Anxiety Inventory, Clinical Global Impressions Severity scale, and Reasons for Living Inventory). Thirty-six patients (17 males, 19 females) were enrolled. A statistically significant association emerged between calcium levels and bipolar depression (Pearson Chi square=0.050) and between CRP and bipolar depression (Pearson Chi-square=0.017). Additionally, a statistically significant association was observed between the unipolar and bipolar depression subgroups and current substance abuse (p=0.0275) A statistically significant difference between the BRLF scores and UDD subgroup emerged (p=0.0126). The results of the pilot study revealed significant associations between calcium/CRP levels with depressive symptoms, particularly in bipolar depression. Further research on inflammatory markers is needed to refine diagnostic subtypes and therapeutic strategies.
Keywords:
depression
; calcium
; thyrotropin
; inflammatory biomarkers
; mental health
1. Introduction
In recent decades, mental health research has increasingly emphasized the role of inflammation in the pathogenesis, course, and treatment of mental disorders such as depression and affective disorders [1]. Several studies outlined recent developments and provided an overview of the inflammatory profiles associated with depression, psychosis, and bipolar disorder, including variations within these conditions [2,3]. Furthermore, factors such as social environment and childhood experiences have been examined for their potential to clarify the intricate interplay between inflammation and other closely related biological systems, while also considering the potentially confounding influence of various lifestyle factors. Several dietary compounds have been implicated in the onset, persistence, and severity of depressive disorders and related conditions such as obesity and diabetes [4]. Unipolar and bipolar depression are prevalent and recurrent mental illnesses affecting millions worldwide. Recently, ketamine has demonstrated a unique rapid neuroprotective and antidepressant effect through its action on the glutamatergic system. Consequently, there has been a growing body of evidence supporting the role of the excitatory amino acid neurotransmitter glutamate in depression treatment in recent years. Emerging research indicates that N-methyl-D-aspartate (NMDA) receptor antagonists, group 1 metabotropic glutamate receptor antagonists, and α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid (AMPA) receptor agonists possess antidepressant properties. NMDA receptor antagonists have been shown to promote synaptic plasticity and reverse neuronal changes induced by stress [5]. Recent research has identified new mediators involved in both energy balance and mood regulation, including insulin growth hormone (IGF-1), neuropeptide Y (NPY), brain-derived neurotrophic factor (BDNF), ghrelin, leptin, cholecystokinin (CCK), glucagon-like peptide 1 (GLP-1), advanced glycosylation end-products (AGEs), glucose metabolism, and the gut microbiota [6]. Changes in inflammatory markers, calcium levels, and thyroid function have been noted in patients experiencing symptoms such as anxiety, depression, fluctuations in thymic axis toward both ends, mental pain and suicidal thoughts [7]. Several studies have investigated the potential interconnections among these factors, impacting both physical homeostasis and mental well-being [2]. Inflammation plays a critical role in defense mechanisms. However, there are hypotheses suggesting that chronic inflammation could disrupt calcium metabolism, affecting neuronal function and contributing to the development of psychiatric disorders such as mood disorders and depression. Elevated levels of pro-inflammatory cytokines, such as interleukin-6 (IL-6) and tumor necrosis factor alpha (TNF-α), observed in individuals with major depression, lend support to the notion that these cytokines might influence brain function through mechanisms such as altering neurotransmission, reducing neurogenesis, and increasing oxidative stress [8]. Furthermore, inflammation has been associated with an increased risk of anxiety and suicidal thoughts. This inflammatory response may impact brain function and behavior through the gut-brain axis, altering neurotransmitter production and the permeability of the blood-brain barrier. Calcium is essential for various bodily functions, including the regulation of nerve transmission and neurotransmitter activity. Abnormal levels of calcium in the blood or brain have been linked to neuropsychiatric disorders. Research indicates that intracellular calcium levels may be disrupted in patients with depression or mood disorders, potentially affecting the release of neurotransmitters like serotonin and norepinephrine, which are critical for mood regulation. Moreover, calcium plays a fundamental role in brain neuroplasticity, known as the brain's ability to adapt and reorganize in response to experiences and learning. Imbalances in calcium levels can disrupt synaptic plasticity and brain function, potentially contributing to conditions such as anxiety and depression. The potential correlation between inflammation, calcium metabolism, and mental disorders suggests promising avenues for diagnostic and therapeutic interventions. For example, emerging research is exploring the use of anti-inflammatory treatments to manage depression and other mood disorders. Additionally, identifying and correcting imbalances in calcium metabolism could lead to targeted strategies aimed at improving mental health outcomes. Any therapeutic approach should be grounded in a comprehensive understanding of the underlying biological mechanisms and supported by robust clinical evidence. A multidisciplinary approach to these complex pathologies, integrating clinical and laboratory data, is essential for clinicians to develop precise hypotheses and effectively manage these conditions, enhancing both prevention and treatment strategies. In this context, our focus has been on observing patients with symptoms across the spectrum of unipolar and bipolar depressive disorders, assessing them clinically and based on bio-humoral indicators. The prospective study aimed to compare unipolar and bipolar depression samples in terms of socio-demographic and clinical characteristics, evaluating potential correlations with calcium levels, thyrotropin (TSH), erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP) values. Specifically, the study aims to:
- -
- Evaluate potential correlations between unipolar and bipolar depression with total calcium and thyrotropin (TSH) levels, free T4, (FT4; thyroxine), erythrocyte sedimentation rate (ESR), and reactive C protein (CRP) values in patients accessing the University Psychiatry Unit of Varese (ASST, Azienda Socio-Sanitaria Territoriale Sette Laghi-Varese) and Como (ASST, Azienda Socio-Sanitaria Territoriale Lariana);
- -
- Compare two patient subgroups (unipolar depression vs. bipolar depression) in terms of alterations in calcium, TSH, ESR, and CRP levels;
- -
- Assess potential correlations between suicidal ideation and calcium levels, TSH, ESR, and CRP in patients accessing the University Psychiatry Unit of Varese and Como.
2. Materials and Methods
2.1. Study Design
This prospective observational study involved the collection of data on hospitalized patients in the University Psychiatric Unit of Varese, ASST Sette Laghi-Varese (N=28) and in the Psychiatric Unit of Como, Lariana (N=8). Subjects were recruited consecutively between October 11, 2022 and June 11, 2023. Prior to the participation, all individuals were duly informed about the study’s objectives and procedures and provided written informed consent for the use and analysis of the data.
2.2. Inclusion and Exclusion Criteria
Patients had to fulfil the following inclusion criteria:
- -
- Diagnosis of major depressive disorder and bipolar disorder in the depressive phase according to the diagnostic criteria of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5);
- -
- Age ≥ 18 years;
- -
- Provision of written informed consent for the use of anonymous data for scientific scope;
- -
- CGIs ≥ 3.
- -
- Patients were excluded from the study based on the following exclusion criteria:
- -
- Age < 18 years;
- -
- Refusal to participate in the study;
- -
- Neurocognitive deficits that impair the understanding of assessment tools;
- -
- Inflammatory diseases and current infectious;
- -
- Language barriers that impair the understanding of assessment tools.
Socio-demographic and clinical characteristics were recorded at recruitment. Laboratory tests were performed at ASST Sette Laghi in Varese and ASST Lariana in Como and retrieved through Intranet systems.
2.3. Assessment Tools
The assessment was conducted at recruitment by Clinicians using the following tools:
- -
- Patient demographic form: standardized instrument to collect essential information from patients and clarify the demographic profile (age, gender, marital status, education level, employment status, and other relevant demographic details). Collected information can be used to identify potential correlations between demographic factors and health outcomes;
- -
- Beck Depression Inventory-II (BDI-II): widely used self-report questionnaire designed to assess the severity of depression. Developed by Aaron T. Beck and colleagues, the BDI-II consists of 21 items, each rated on a 4-point scale, which reflects the intensity of depressive symptoms experienced over the past two weeks. It covers various aspects of depression, including mood, cognitive function, physical symptoms, and behavior. The BDI-II is a reliable and valid tool for both clinical and research settings [9];
- -
- The Orbach & Mikulincer Mental Pain Questionnaire (OMMP): used to measure psychological pain or mental anguish, distinct from physical pain. It assesses intensity, frequency, and duration of mental pain, including feelings of hopelessness, loss, and emotional turmoil. The OMMP helps clinicians identify the depth of mental suffering that may not be captured by traditional measures of depression or anxiety [10];
- -
- Beck Anxiety Inventory (BAI): 21-item self-report inventory designed to measure the severity of an individual's anxiety. Each item describes a common symptom of anxiety, which the respondent rates based on their experience over the past week. The BAI covers various domains of anxiety, including physiological, cognitive, and affective symptoms, and is useful in both clinical and research contexts for diagnosing and monitoring treatment progress [11];
- -
- Reasons for Living Inventory (RFL): self-report instrument developed to assess cognitive and motivational factors that prevent individuals from attempting suicide. It includes a series of statements reflecting reasons for living, such as fear of social disapproval, moral objections, and survival and coping beliefs. The RFL helps identify protective factors that may mitigate the risk of suicidal behavior [12,13].
- -
- Clinical Global Impressions Severity (CGIs): used to assess the severity of a patient's mental illness. It involves a single-item rating, where the clinician evaluates the patient’s current state on a scale from 1 (normal, not at all ill) to 7 (among the most extremely ill patients). The CGIs is widely used in clinical practice and research due to its simplicity and effectiveness in providing a global assessment of patient severity [14,15].
2.4. Laboratory Tests
Serum TSH (reference range: 0.27-4.2 mU/liter) and FT4 (9.3-17 pg/ml) levels were measured by electrochemiluminescence immunoassay (Analytical Unit for immunochemistry Cobas e801, Roche). Normal values for chemistry determination were as follows: calcium 8.8-10.2 mg/dl, CRP 0-5 mg/l, ESR 0-15 mm, albumin 3.57-5.49 g/dl.
2.5. Statistical Analysis
Descriptive statistics were reported as mean and standard deviation for continuous variables or frequency and percentage for qualitative variables. The sample size was estimated based on other similar studies on correlations between serum calcium levels and psychopathology [16,17]. The Chi-square test with Fisher's correction when necessary was used to evaluate the association between two qualitative variables. For better data interpretation, Cramer's V derivation index was used. The following values were considered for Cramer's V: 0.00-0.30 "weak association", 0.30-0.60 "good association", 0.60-0.90 "strong association", > 0.9 "excellent association". Statistical significance has been established for a p-value ≤ 0.05. Statistical analyses were performed using SPSS statistics software [18].
The Chi-square Test was used to analyze the associations between calcium, TSH, ESR, and CRP levels with the diagnosis of Unipolar Depression (UD), combining patients diagnosed with Major Depressive Disorder (MDD), Reactive Depression, and Adjustment Disorder with Anxiety and Depressed Mood, and the diagnosis of Bipolar Depression (BD), including Bipolar I and II Disorders (BDI, BDII) based on DSM-5 criteria. Chi-square values are expressed as bilateral asymptotic significance, and the P-value is always expressed as bilateral exact significance in the presence of Fisher's Exact Test or approximated to the value of Cramer's V in the absence of Fisher's Test.
2.6. Data Protection
Data were recorded anonymously in a dedicated Excel database, access to which was restricted to the physicians involved in the study, thus maintaining patient confidentiality. This study did not incur any additional costs and did not interfere with routine clinical activities. The handling of data –personal, demographic, and clinical – was solely for scientific research purposes, and any dissemination of results will be done anonymously and/or in aggregate form for scientific purposes. The material is and will be used exclusively for scientific research purposes, never for profit and/or commercial purposes. The study was conducted by taking into account regulatory requirements and legal requirements [19] and in accordance with the ethical principles of the Declaration of Helsinki.
3. Results
3.1. Socio-Demographic and Clinical Characteristics of the Sample
The sample consists of 17 males and 19 females, totaling 36 patients. Most patients fall within the age range of 18 to 49 years, with a higher percentage between 18 to 29 years (25.0%; N=9) and 40 to 49 years (22.2%; N=8). Socio-demographic characteristics of the sample are shown in Table 1.
Regarding family history, 52.8% (N=19) of the sample has no significant family history; 22.2% (N=8) have a family history of anxiety disorder, 8.3% (N=3) of schizophrenia spectrum disorder, 5.6% (N=2) of substance abuse, 2.8% (N=1) of affective disorders, and 8.3% (N=3) of other psychiatric disorders.
Regarding endocrinological and organic and comorbidities, 63.9% of the sample (N=23) have no medical comorbidities. 2.8% (N=1) report hypothyroidism, and the same percentage applies to diagnoses of thyroid nodule and osteoporosis. As regards as cardiometabolic comorbidities, 2.8%(N=1) has hypercholesterolemia; 11% (N=4) has diabetes, 8.3% (N=3) suffer from obesity, and 5.6% (N=2) have hypertension (Figure 1).
The only identified case of hypothyroidism is undergoing treatment with levothyroxine. 13.9% of the patients (5 out of 36) are undergoing treatment with lithium salts, which has an impact on the morpho-structural thyroid profile.
Table 2 shows data on the primary psychiatric diagnosis and psychiatric comorbidities, expressed as frequency (N) and percentage (%).
The onset age of psychopathological symptoms mainly falls between 10 and 39 years, with a higher percentage between 10 and 19 years (32.0%; N=8) and between 30 and 39 years (28.0%; N=7). One patient had an onset before the age of 10, and six patients had an onset between 40 and 79 years. Regarding psychopharmacological therapy at the time of recruitment, the percentages are as follows: 19.4% (N=7) of the total sample is not on any drug therapy, 8.3% (N=3) is on monotherapy, and 72.2% (N=26) is on polypharmacotherapy.
Regarding substance abuse, 22.9% (N=8) of the sample has a positive history of alcohol abuse, 5.7% (N=2) has a history of abuse of substances other than alcohol (one substance), and 5.7% (N=2) has a history of poly-substance abuse. At the time of recruitment, 68.6% (N=24) had no substance abuse, 22.9% (N=8) had alcohol abuse, 5.7% (N=2) abused a substance other than alcohol, and 2.9% (N=1) show poly-substance abuse. The 16.7% (N=6) regularly consume coffee, 16.7% (N=6) smoke cigarettes, 22.2% (N=8) both, and 44.4% (N=16) report neither habit.
The 58.3%3 of the sample had lifetime suicidal ideation, while 50% recurrent suicidal ideation. A history of attempted suicide was found in 63.9% of cases, and a recent suicide attempt was identified in 72.2% of cases.
3.2. Data Analysis
A weak statistically significant association between calcium levels and unipolar depression (Chi-square=0.233; Cramer's V=0.229; p=0.532) and a good statistically significant association between calcium levels and bipolar depression emerged (Chi-square=0.050; Cramer's V=0.378; p=0.115). A good statistically significant association between CRP and Bipolar Depression (Chi-square=0.017; Cramer's V=0.470; p=0.028) emerged. The data concerning the associations between inflammatory markers, TSH, and Calcium with different groups within the total sample have been reported in Table 3. A weak statistically significant association between TSH and both unipolar (Chi-square=0.212; Cramer's V=0.255; p=0.493) and bipolar depression (Chi-square=0.289; Cramer's V=0.217; p=0.380) emerged. A weak statistically significant association between both ESR and Unipolar Depression (Chi-square=0.488; Cramer's V=0.126; p=0.640) and ESR and Bipolar Disorder (Chi-square=0.125; Cramer's V=0.280; p=0.183) emerged. The data concerning CRP and Unipolar Depressive Disorder did not show a significant statistical association (Chi-square=0.592; Cramer's V=0.105; p=0.661).
Values were calculated using Fisher's exact test. Regarding the association between inflammatory markers (ESR and CRP) and current suicidal ideation, no statistically significant difference was found. White blood cell abnormalities were also found to be homogeneous across the two diagnostic subgroups (BD and UDD), as were alterations in calcium levels in relation to the presence or absence of suicidal ideation, with a corresponding p-value of p=0.4328 in the latter case. Regarding psychopharmacological therapy, the Fisher's exact test was used to assess associations between the population receiving therapy (monotherapy or polytherapy) at the time of hospitalization versus those not receiving any psychotropic medication, concerning inflammatory markers (VES and PCR), TSH, and Calcium values. In none of the examined cases did a statistically significant difference emerge that would suggest a potentially clinically relevant interaction. Regarding organic and endocrinological conditions, the two diagnostic subgroups (UD and BD) were evenly distributed (p=0.1590). Considering current suicidal ideation, reported by the patient during the clinical interview, although it was present in 50% of the total sample, it was found to be consistent between the population with Unipolar Depression (n=10) and the population diagnosed with Bipolar Depression (n=8). However, a statistically significant association (p=0.0275) was observed between the two analyzed subgroups and current substance abuse (single substance or polysubstance abuse), highlighting how this behavior served as a protective factor against suicidal ideation (Table 4).
To assess whether there was a significant association between the two diagnostic subgroups (UD and BD) and the scores obtained from the assessment scales, we considered potential associations between the mean total scores obtained from the psychometric scales with Unipolar Depressive Disorder and Bipolar Depression, using the Student's t-test as a tool to determine potential statistical significance. Regarding the association between BRLF scores and the total population divided into the two diagnostic subgroups of Unipolar Depression (UD) and Bipolar Disorder (BD), a statistically significant difference emerges, particularly in the group of patients with Unipolar Depressive Disorder (p=0.0126) (Table 5).
No statistically significant difference was observed from the associations with the other assessment scales and the two psychopathological groups. Furthermore, the association between current suicidal thoughts and the Mental Pain Questionnaire (OMMP) was investigated to assess suicide risk levels in a considered high-risk population. The presence or absence of suicidal ideation in the examined sample did not show any significant correlation with the results obtained from the assessment scale (p=0.4027).
4. Discussion
The relationship between the immune system and alterations in the thymic axis has long been recognized, particularly the immune system's role in depressive spectrum disorders. This prospective study aimed to evaluate the relationship between several biomarkers which are routinely investigated in clinical settings, depressive symptoms and suicidal ideation, highlighting potential differences between patients with unipolar spectrum disorders and those with bipolar depression. This study was designed to assess a potential correlation between inflammation indices (ESR and CRP), TSH, and calcium, and the manifestation of depressive symptoms with or without suicidal ideation. Additionally, interactions with sociodemographic, clinical, and psychometric factors were evaluated to better understand the applicability of these biomarkers as screening methods in the context of differential diagnosis, suicide prevention, and personalized treatment strategies. The sample was evenly distributed between the sexes, with a low number of married and employed patients. This could be attributed to the predominantly young age group (N=17) and the fact that depressive symptoms often lead to relational poverty and reduced socio-occupational functioning [20]. A noteworthy observation was the early onset of mood disorders reported by patients (N=15), consistent with current literature describing an increasingly earlier onset of mood disorders, especially bipolar spectrum disorders [21]. About 30% of patients had organic and endocrinological comorbidities, predominantly type II diabetes, obesity, and hypertension. Considering the young age of the sample, this high frequency is significant. Extensive literature exists on comorbidities in psychiatric and mood disorders, suggesting multifactorial etiopathogenic mechanisms, including lifestyle habits, sedentary behavior, smoking, poor diet, and the role of polypharmacotherapy or inadequate hormonal treatments that can induce psychiatric symptoms. The role of glucocorticoids produced by the adrenal gland in regulating immune processes and metabolism is well documented. Dysregulation of the hypothalamic-pituitary-adrenal (HPA) axis has been noted in mood disorders, with chronic stress leading to elevated glucocorticoid levels, particularly cortisol, triggering an inflammatory response mediated by pro-inflammatory cytokines, especially IL-1β. This HPA axis hyperactivation, potentially due to defective neuroendocrine control, could explain the increased prevalence of metabolic disorders and central obesity in bipolar patients [8]. Half of the sample had a positive family history of psychiatric disorders, particularly anxiety disorders, especially among bipolar patients. Familial predisposition is common in mood disorders, particularly in the bipolar spectrum, where patients often have a positive family history of psychiatric conditions [22]. Polypharmacotherapy was more prevalent than monotherapy, suggesting more severe and complex psychopathological conditions often necessitate the use of multiple psychotropic drugs, despite potential side effects and drug-drug interactions that can negatively impact patient compliance [23]. Suicidal ideation was present in 50% of the total population at recruitment, with 72.2% having attempted suicide before admission. The strong association between suicidal ideation and depression, particularly bipolar spectrum depression and mixed states, is well-documented [24]. Interestingly, suicidal ideation negatively correlated with substance abuse, suggesting those with current suicidal ideation were less likely to engage in substance abuse (p=0.0275). This relationship is complex and varies with individual patient contexts and substance use patterns [25]. Comparing unipolar and bipolar depression, significant alterations in calcium levels were observed in bipolar patients (p=0.050). Calcium role in the pathogenesis of bipolar spectrum disorders is acknowledged but not fully understood, with alterations linked to hypervigilance and thymic axis oscillations [26]. TSH levels showed weak alterations across both patient groups, without significant differences, reflecting the well-known relationship between thyroid hormones and mood disorders [27]. CRP levels were significantly altered, particularly in bipolar depression (p=0.028), supporting existing literature on immune system alterations in bipolar disorder [8]. The primary limitation of this study is the small sample size, which may not be representative of the broader population and lacks statistical power. Additionally, the inability to follow up with patients for repeated psychometric assessments and biochemical evaluations limits the study to a cross-sectional analysis. By integrating sociodemographic, clinical, and biomarker data, this study underscores the importance of a multidisciplinary approach in understanding and treating mood disorders, aiming to improve diagnostic precision and therapeutic outcomes.
5. Conclusions
In conclusion, this work highlights the comprehensiveness of the psychophysical aspects of the patient, moving towards an increasingly comprehensive approach to psychopathological disorders and the individual. This approach, increasingly present in international literature, aims to enhance understanding of physio-pathogenetic processes, as well as progress in diagnostic framing, differential diagnoses, and greater accuracy and personalization of therapeutic approaches. The primary endpoint of the study was to evaluate potential correlations between unipolar and bipolar depression and suicidal ideation with levels of calcium, TSH, ESR, and CRP. The results demonstrated that calcium and CRP levels are correlated with depressive symptoms, predominantly within the bipolar spectrum. Furthermore, based on the results, it is reasonable to state that among the psychometric scales used, the BRLF was the most effective in identifying patients at higher suicidal risk at the time of evaluation, particularly those with bipolar depression. The second endpoint was to compare the two subgroups of patients with unipolar and bipolar depression and analyze potential differences in clinical and socio-demographic characteristics, highlighting the main etiopathogenic factors and associated risk factors. Among these socio-demographic and clinical characteristics, current substance abuse emerged as the most interesting and worthy of further investigation, having a protective role against suicidal ideation within the sample. However, this data should be interpreted cautiously, as the tendency to deny the problem, factors related to social tolerance of alcohol consumption, and the mode of alcohol intake might have led to underestimating the phenomenon. These preliminary results need further investigation to clarify the underlying biochemical mechanisms and the clinical implications. Understanding these phenomena is crucial for developing effective preventive and therapeutic strategies and reducing the resulting individual and social burden. Future perspectives emphasize the importance of confirming our findings, enriching them with second-level investigations on inflammatory parameters such as IL-1B, IL-6, and IL-2 to identify factors useful in differential diagnosis and the identification of additional diagnostic subtypes and increasingly targeted therapeutic frameworks.
Author Contributions
Conceptualization, MI and DG; Formal analysis, MI; Investigation, MI; Methodology, IC; Supervision, MLT, EP and CC; Writing – original draft, IC; Writing – review & editing, DG.
Funding
This research received no external funding.
Acknowledgments
None
Conflicts of Interest
None of the authors have potential conflicts of interest to be disclosed.
References
- Teraiza, E.; Meza, R. Depression as a Medical-Psychiatric Entity. Rev colomb psiquiatr 2008, 37, 220–235. [Google Scholar]
- Baumeister, D.; Russell, A.; Pariante, C.M.; Mondelli, V. Inflammatory biomarker profiles of mental disorders and their relation to clinical, social and lifestyle factors. Soc Psychiatry Psychiatr Epidemiol 2014, 49, 841–849. [Google Scholar] [CrossRef] [PubMed]
- Gasparini, A.; Callegari, C.; Lucca, G.; Bellini, A.; Caselli, I.; Ielmini, M. Inflammatory Biomarker and Response to Antidepressant in Major Depressive Disorder: A Systematic Review and Meta-Analysis. Psychopharmacol Bull 2022, 52, 36–52. [Google Scholar] [PubMed]
- Lang, U.E.; Beglinger, C.; Schweinfurth, N.; Walter, M.; Borgwardt, S. Nutritional aspects of depression. Cell Physiol Biochem 2015, 37, 1029–1043. [Google Scholar] [CrossRef]
- Deutschenbaur, L.; Beck, J.; Kiyhankhadiv, A.; Mühlhauser, M.; Borgwardt, S.; Walter, M.; Hasler, G.; Sollberger, D.; Lang, U.E. Role of calcium, glutamate and NMDA in major depression and therapeutic application. Prog Neuropsychopharmacol Biol Psychiatry 2016, 4, 325–33. [Google Scholar] [CrossRef]
- Lang, U.E.; Borgwardt, S. Molecular mechanisms of depression: Perspectives on new treatment strategies. Cell Physiol Biochem 2013, 31, 761–777. [Google Scholar] [CrossRef]
- Ielmini, M.; Lucca, G.; Trabucchi, E.; Aspesi, G.L.; Bellini, A.; Caselli, I.; Callegari, C. Assessing Mental Pain as a Predictive Factor of Suicide Risk in a Clinical Sample of Patients with Psychiatric Disorders. Behav Sci (Basel) 2022, 12, 111. [Google Scholar] [CrossRef]
- Barbosa, I.G.; Machado-Vieira, R.; Soares, J.C.; Teixeira, A.L. The immunology of bipolar disorder. Neuroimmunomodulation 2014, 21, 117–122. [Google Scholar] [CrossRef]
- Beck, A. T.; Steer, R. A.; Brown, G. Beck Depression Inventory–II (BDI-II), 1996.
- Orbach, I.; Mikulincer, M.; Sirota, P.; Gilboa-Schechtman, E. Mental Pain: A Multidimensional Operationalization and Definition. Suicide and Life-Threatening Behavior 2003, 33, 219–230. [Google Scholar] [CrossRef]
- Beck, A. T.; Steer, R. A. Beck Anxiety Inventory manual. Psychological Corporation, San Antonio, TX, 1993.
- Linehan, M.M.; Goodstein, J.L.; Nielsen, S.L.; Chiles, J.A. Reasons for Staying Alive When You Are Thinking of Killing Yourself: The Reasons for Living Inventory. Journal of Consulting and Clinical Psychology 1983, 51, 276–286. [Google Scholar] [CrossRef]
- Osman, A. , Jones, K., & Osman, J. R. The Reasons for Living Inventory: Psychometric Properties. Psychological Reports 1991, 69, 271–278. [Google Scholar] [PubMed]
- Guy, W. Assessment Manual for Psychopharmacology. Editor. ECDE, 1976.
- Busner, J.; Targum, S.D. The clinical global impressions scale: Applying a research tool in clinical practice. Psychiatry (Edgmont) 2007, 4, 28–37. [Google Scholar] [PubMed]
- Stern, J.E.; Guinjoan, S.M.; Cardinali, D.P. Correlation between serum and urinary calcium levels and psychopathology in patients with affective disorders. Short communication. J Neural Transm (Vienna) 1996, 103, 509–13. [Google Scholar] [CrossRef]
- Steardo, L., Jr.; Luciano, M.; Sampogna, G.; Carbone, E.A.; Caivano, V.; Di Cerbo, A., Giallonardo; Palummo, C.; Vece, A. Del Vecchio, V.; De Fazio, P.; Fiorillo, A. Clinical Severity and Calcium Metabolism in Patients with Bipolar Disorder. Brain Sci 2020, 10, 417. [Google Scholar] [CrossRef]
- IBM Corp. IBM SPSS Statistics for Windows, Version 28.0. Armonk, NY, IBM Corp. (SCIRP), 2021.
- DL n.211 of 24 June 2003 (and DM 17 December 2004).
- Bosc, M. Assessment of social functioning in depression. Compr Psychiatry 2000, 41, 63–69. [Google Scholar] [CrossRef]
- NIHM, 2020. Available online: https://www.nimh.nih.gov/.
- Köhler-Forsberg, O.; Sylvia, L.G.; Ruberto, V.L.; Kuperberg, M.; Shannon, A.P.; Fung, V.; Overhage, L.; Calabrese, J.R.; Thase, M.; Bowden, C.L.; Shelton, R.C.; McInnis, M.; Deckersbach, T.; Tohen, M.; Kocsis, J.H.; Ketter, T.A.; Friedman, E.S.; Iosifescu, D.V.; McElroy, S.; Ostacher, M.J.; Nierenberg, A.A. Familial severe psychiatric history in bipolar disorder and correlation with disease severity and treatment response. J Affect Disord 2020, 1, 131–137. [Google Scholar] [CrossRef]
- Moncrieff, J.; Cohen, D.; Porter, S. The psychoactive effects of psychiatric medication: The elephant in the room. J Psychoactive Drugs 2013, 45, 409–415. [Google Scholar] [CrossRef] [PubMed]
- Dome, P.; Rihmer, Z.; Gonda, X. Suicide Risk in Bipolar Disorder: A Brief Review. Medicina (Kaunas) 2019, 55, 403. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, H.C.; Conner, K.R.; Caine, E.D. Association of Alcohol and Drug Use Disorders and Completed Suicide: An Empirical Review of Cohort Studies. Drug and Alcohol Dependence 2004, 76, 9–11. [Google Scholar] [CrossRef]
- D’Onofrio, S.; Mahaffey, S.; Garcia-Rill, E. Role of calcium channels in bipolar disorder. Curr Psychopharmacol 2017, 6, 122–135. [Google Scholar] [CrossRef]
- Talaei, A.; Rafee, N.; Rafei, F.; Chehrei, A. TSH cut off point based on depression in hypothyroid patients. BMC Psychiatry 2017, 17, 327. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Endocrinological comorbidities.
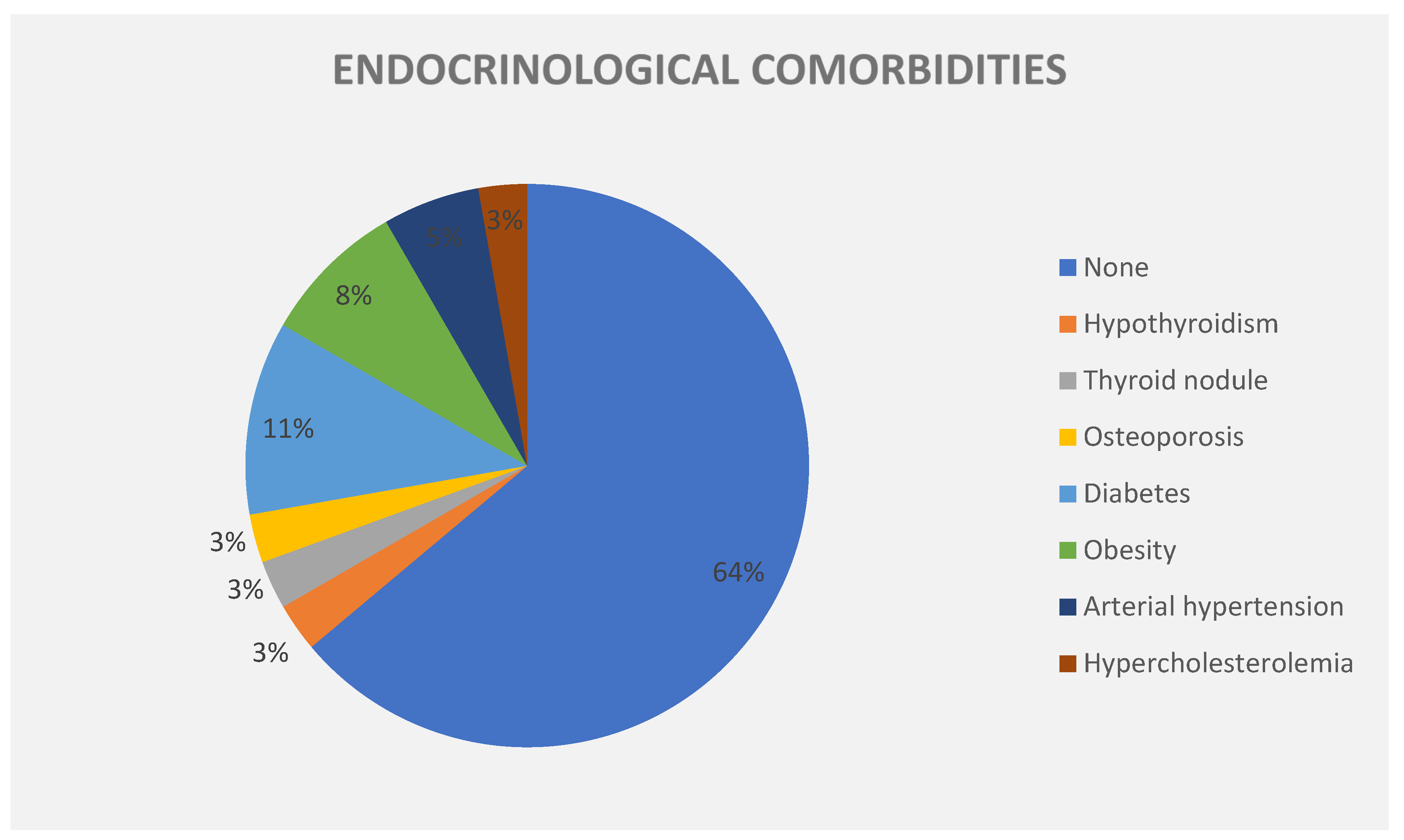

Table 1.
Socio-demographic characteristics of the sample.
| Male (N) | Female (N) | Total (N) | |
|---|---|---|---|
| 17 | 19 | 36 | |
| Marital status | |||
| Married Single Divorced Widowed |
7 4 3 3 |
12 3 4 - |
19 (58.2%) 7 (19.4%) 7 (19.4%) 3 (8.3%) |
| Education | |||
| Elementary school Middle school High school Degree Missing data |
2 9 3 2 1 |
- 7 7 5 - |
2 (5.7%) 16 (45.7%) 10 (28.6%) 7 (20%) - |
| Employment | |||
| Occupied Unoccupied Retired Invalid Missing data |
5 4 6 1 1 |
8 3 5 2 1 |
13 (38.2%) 7 (20.6%) 11 (32.4%) 3 (8.8%) - |
Table 2.
Frequencies of primary psychiatric diagnosis.
| Main psychiatric diagnosis | N (%) | Psychiatric comorbidities | N (%) |
| Major Depressive Disorder | 16 (45%) | None | 22 (61.1%) |
| Reactive Depression with Adjustment Disorder and Adjustment Disorder with depressive mood | 5 (14%) | Substance abuse | 3 (8.3%) |
| Bipolar Disorder Type 1 | 3 (8%) | Adjustment Disorder | 1 (2.8%) |
| Bipolar Disorder Type 2 | 12 (33%) | Personality disorder NOS | 9 (25.0%) |
| Eating disorder | 1 (2.8%) | ||
| Total | 36 (100.0%) | Total | 36 (100.0%) |
Table 3.
Association between Calcium levels and CPR and unipolar and bipolar depression.
| Pearson chi-square | Exact Fisher test | Cramer V | |
| Calcium and UD | 0.233 | 0.233 | 0.233 |
| Calcium and BD | 0.050 | 0.115 | 0.378 |
| CPR and UD | 0.592 | 0.592 | 0.592 |
| CPR and BD | 0.017 | 0.017 | 0.017 |
Table 4.
Significance between current substance abuse and suicidal intention.
| Actual substance abuse | No actual substance abuse | Total | P value | |
| Current suicidal intention |
2 |
16 |
18 |
=.0275 |
| No current suicidal intention |
9 |
9 |
18 |
|
| Total | 11 | 25 | 36 |
Table 5.
Association between Brief Reasons for Living Inventory (BRLF) and DUU and DB.
| Group | DDU BRLF | DB BRLF | P value |
| Media | 45.52 | 35.47 |
=.0126 |
| SD | 12.36 | 9.55 | |
| SEM | 2.70 | 2.47 | |
| N | 21 | 15 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



