
Submitted:
06 September 2024
Posted:
06 September 2024
You are already at the latest version
Abstract
Background: Whole-body computed tomography (WBCT) is commonly employed for primary screening in pediatric patients experiencing out-of-hospital cardiac arrest (OHCA) without prehospital return of spontaneous circulation (ROSC). This study aimed to evaluate the cause of OHCA on WBCT and compare WBCT findings between ROSC and non-ROSC groups in non-traumatic pediatric OHCA cases in an emergency department (ED) setting. Methods: A retrospective analysis was conducted on 27 pediatric patients (mean age: 32.4 months; median age: 10 months) who experienced non-traumatic OHCA without prehospital ROSC and were transported to our tertiary care hospital between January 2013 and December 2023. WBCT scans were performed to investigate the cause of OHCA, with recorded findings in the head, chest, abdomen, and subcutaneous tissues. Results: In all cases, the direct causes of OHCA were undetermined, and WBCT identified no fatal findings. Statistical comparisons of CT findings between the ROSC and non-ROSC groups revealed significant differences. The non-ROSC group had a higher incidence of brain swelling, loss of cerebral gray-white matter differentiation, symmetrical lung consolidation/ground-glass opacity, cardiomegaly, hyperdense aortic walls, narrowed aorta, gas in the mediastinum, and hepatomegaly compared to the ROSC group. Conclusions: Although WBCT did not provide the direct cause of OHCA, it clarified several indicative findings for non-ROSC. These imaging findings could support clinical decision-making, offering objective criteria for discontinuing resuscitation in pediatric OHCA cases where prehospital ROSC is absent.
Keywords:
computed tomography
; pediatric patient
; out-of-hospital cardiac arrest
; return of spontaneous circulation
1. Introduction
Out-of-hospital cardiac arrest (OHCA) in pediatric populations is a rare but critical event with significant implications for clinical outcomes and public health. As of 2024, the Tokyo metropolitan area had a population of approximately 14 million, including about 2 million individuals under the age of 19 [1]. In 2020, the incidence of OHCA in this age group accounted for just 1.3% of all emergency transport cases, reflecting its rarity (160 out of 12,338 cases) [2]. Specifically, the incidence rates were 0.9 per 10,000 for males and 0.65 per 10,000 for females.
Despite its infrequency, pediatric OHCA presents unique challenges in clinical management. In Japan, the causes of pediatric OHCA often remain undetermined, highlighting the need for a more structured approach, such as the implementation of a Child Death Review system to investigate sudden unexpected deaths in children [3]. Accurate identification of the underlying causes is crucial not only for understanding the etiology but also for informing appropriate resuscitation strategies.
A recent survey conducted between November 1 and December 12, 2022, across 502 pediatric training facilities and emergency centers in Japan, reported that 96% of these institutions performed computed tomography (CT) scans on pediatric OHCA cases they received. This rate was comparable to that of routine blood tests and blood gas analyses [4]. The use of CT, particularly whole-body CT (WBCT), has been recognized as a valuable tool in identifying abnormal findings that can guide life-saving interventions and the development of treatment plans. However, in cases where resuscitation is unlikely to succeed, CT findings may also provide essential information to support the difficult decision to cease resuscitation efforts—a decision that requires clear communication with the family, who may be in shock and struggling to comprehend the situation.
Although CT is widely utilized for screening potential causes of cardiac arrest [5,6,7,8], its specific role in pediatric OHCA cases—especially among those who did not achieve a return of spontaneous circulation (ROSC) before arriving at the emergency department (ED)—has not been fully elucidated. The clinical utility and implications of CT in these scenarios remain underexplored.
This study aims to assess the utility and clinical implications of CT, particularly WBCT, in pediatric OHCA cases where prehospital ROSC was not achieved. By investigating the WBCT findings in these cases, we seek to contribute to a better understanding of how WBCT can inform resuscitation efforts and decisions regarding the termination of resuscitation in the ED setting.
2. Materials and Methods
This retrospective study was conducted in accordance with the principles outlined in the Declaration of Helsinki. Approval was obtained from the institutional review boards (T2023-0192), and the requirement for informed consent was waived.
2.1. Subjects
We retrospectively reviewed pediatric patients who experienced non-traumatic OHCA between January 2013 and December 2023. Inclusion criteria were patients transported to the ED of our tertiary care hospital without ROSC prior to arrival. At the time of the study, the legal age of adulthood in Japan was defined as 18 years, per the Civil Code. Consequently, the study focused on individuals under 18 years of age. The determination of whether the cause of OHCA was traumatic or non-traumatic was made by emergency physicians based on physical examination and information obtained from paramedics, family members, or first responders.
2.2. CT Scanning
All patients underwent WBCT without contrast enhancement. During or after cardiopulmonary resuscitation (CPR), WBCT scanning was performed in the supine position, covering the area from just above the vertex to the toes. In scans during CPR, the duration of interruption of chest compressions was less than 10 seconds. Two types of multi-detector CT scanners were used: a 64-row scanner (Aquilion 64, Canon Medical Systems, Tokyo, Japan) until June 30, 2019, and an 80-row scanner (Aquilion Prime SP, Canon Medical Systems, Tokyo, Japan) from July 1, 2019. Helical scans were performed at a tube voltage of 120 kV. On the Aquilion 64, tube current was set at 200 mA for the head and 300 mA for the body, or 300 mA for the head and 400 mA for the body. The axial slice thickness was 4 mm for the head and 2–5 mm for the body. On the Aquilion Prime SP, tube current was regulated by automatic exposure control, with a slice thickness of 3 mm for the head and 2–5 mm for the body. Image reconstruction, when available, was performed at a thickness of 1 mm. On both scanners, the helical pitch was set at 0.625 for the head and 0.828 for the body, with a maximum field of view of 350–420 mm and a 512 × 512 image matrix.
2.3. CT Image Evaluation
WBCT images were independently reviewed via Synapse Picture Archiving and Communication System (Fujifilm, Tokyo, Japan) by two senior board-certified diagnostic radiologists with 14 and 18 years of experience, respectively. In interpreting CT images, diagnostic radiologists could access clinical information (including present illness at admission, past history, and family history), laboratory results (hematological and biochemical tests), arterial blood gas analysis, and available previous images. The radiologists specifically evaluated the WBCT images for findings that could explain the cause of OHCA. Additionally, the presence or absence of the following findings was assessed: brain swelling, loss of cerebral gray-white matter differentiation, hyperdense intracranial venous sinuses, symmetrical or asymmetrical lung consolidation/ground-glass opacity, cardiomegaly, pericardial effusion, hyperdense aortic wall, narrowed aorta, gas in the mediastinum (i.e., in the cardiac cavity, aorta, or superior vena cava), hepatomegaly, dilated inferior vena cava, dilated gastrointestinal tract, gas in upper abdominal organs (i.e., in the liver, kidney, pancreas, or spleen), and dorsal subcutaneous fatty edema. These findings are commonly observed on postmortem CT [9,10] and are therefore considered observable during the agonal stage in non-ROSC cases. Consensus was reached on the presence or absence of these findings.
2.4. Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics version 29.0. Results were considered statistically significant at p < 0.05. Patients were categorized into two groups based on whether ROSC was achieved in the ED. Differences between the ROSC and non-ROSC groups were evaluated using the Mann-Whitney U test. Differences in specific CT findings between the groups were assessed using Fisher’s exact test.
3. Results
3.1. Clinical Information
During the study period, 27 pediatric patients with non-traumatic OHCA who did not achieve prehospital ROSC were referred to the ED of our tertiary care hospital and subsequently underwent WBCT scanning. Of these, 14 were boys and 13 were girls, with a mean age of 32.4 months (median: 10 months; range: 0.4–166 months). The interval from the last sighting to discovery was estimated based on information provided by family members or the individuals who found the patients. The mean interval time was 3 hours and 4 minutes, with a median of 2 hours and 25 minutes (range: 0 to 9 hours and 20 minutes).
Cardiopulmonary resuscitation was performed in all cases, before and after arrival at the hospital. Eight patients achieved ROSC in the ED and were subsequently hospitalized, whereas 19 patients did not achieve ROSC and were pronounced dead in the ED. We analyzed differences between the non-ROSC and ROSC groups in terms of age, sex, presence of past medical history, location of discovery (home or elsewhere), whether the patient was found after bedtime, estimated time from last sighting to discovery, and the presence of bystander CPR (Table 1). There were significant differences in whether the patient was found after bedtime and estimated time from last sighting to discovery between the two groups. The non-ROSC group was significantly larger for the proportion of patients discovered after bedtime and for the estimated time from last sighting to discovery.
3.2. Evaluation of WBCT Findings
WBCT scans were performed during CPR in 25 patients and after the termination of CPR in two non-ROSC cases. In all cases, the direct cause of OHCA remained undetermined by WBCT, and no fatal findings were identified by WBCT.
Supplementary Tables S1 and S2 present clinical information and CT findings of the non-ROSC (Figure 1) and ROSC groups (Figure 2), respectively. The non-ROSC group showed significantly higher incidences of several findings compared to the ROSC group, including brain swelling (84% vs. 12.5%; p < 0.001), loss of cerebral gray-white matter differentiation (74% vs. 37.5%; p = 0.033), symmetrical consolidation/ground-glass opacity (95% vs. 50%; p = 0.017), cardiomegaly (84% vs. 25%; p = 0.006), hyperdense aortic wall (84% vs. 0%; p < 0.001), narrowed aorta (100% vs. 0%; p < 0.001), gas in the mediastinum (80% vs. 0%; p < 0.001), and hepatomegaly (79% vs. 12.5%; p = 0.002). Neither pericardial effusion nor subcutaneous fatty edema was observed in any case. There were no significant differences between the non-ROSC and ROSC groups in the incidence of loss of cerebral gray-white matter differentiation, hyperdense intracranial venous sinus, symmetrical/asymmetrical consolidation/ground-glass lung opacity, cardiomegaly, hepatomegaly, dilated inferior vena cava, dilated gastrointestinal tract, or gas in the upper abdominal organs. A summary of the differences in WBCT findings between the non-ROSC and ROSC groups is provided in Table 2.
4. Discussion
This study identifies notable differences in the frequency of certain imaging findings between pediatric OHCA patients who achieved ROSC and those who did not. Our investigation into the clinical utility of WBCT during resuscitation in the ED represents a novel approach that may have significant implications for clinical practice.
In our study, we found significant differences in the incidence of specific CT findings between the ROSC and non-ROSC groups. Findings such as brain swelling, loss of cerebral gray-white matter differentiation, hyperdense aortic wall, and narrowed aorta were more frequently observed in the non-ROSC group. These findings may represent physiological alterations during the agonal phase that are similar to normal postmortem changes [9,10,11,12,13]. Following the cessation of circulation, specific changes occur, notably the edematous alterations that elevate the water content in cerebral gray matter, blurring the distinction between gray and white matter. Additionally, there is narrowing of sulci and ventricles along with brain swelling, predominantly when vasogenic edema is evident. The narrowing of the short arterial diameter and the hyperdense arterial walls likely reflect smooth muscle contraction. These phenomena are analogous to the changes observed as rigor mortis in postmortem examinations [10].
Following circulatory arrest, the vasculature reaches a mean circulatory filling pressure, characterized by a hydrostatic pressure around 7 mmHg. This pressure exceeds the typical diastolic pressure of the right heart system, prompting a redistribution of blood volume to the right heart system post-mortem. Consequently, this can lead to dilatation of the right heart system and the superior vena cava [9,10]. Therefore, clinical signs such as cardiomegaly and hepatomegaly, indicative of blood shift and pooling in the right heart system, may signal ineffective CPR. These CT findings could inform the potential futility of ongoing resuscitation efforts in specific cases. Additionally, the pressure shift may cause aortic narrowing, whereas symmetrical consolidation or ground-glass opacity in imaging is likely indicative of pulmonary edema resulting from cardiac arrest. It was not clear that inferior vena cava dilation was significantly more frequent in the non-ROSC group in this study, as there were no reports of inferior vena cava dilation as a postmortem change.
Additionally, the primary cause of the findings of gas in the mediastinum (i.e., in the cardiac cavity, aorta, or superior vena cava) or in the upper abdominal organs (i.e., in the liver, kidney, pancreas, or spleen) may have been produced by chest compressions [14,15]. Intravascular and intra-organic gas is frequently observed after chest compressions. The causes of this observation include the vaporization of dissolved gasses in the blood, air entry through the infusion route, and the formation of broncho-vascular fistula (pressure trauma to the bronchi and pulmonary vessels) in combination with artificial ventilation [14,16]. The longer the duration of cardiopulmonary resuscitation, the more frequently gas is seen in multiple organs. As reported in postmortem CT, intravenous gas may also relate to intra-osseous needles [17]. Chest compressions can spread intravascular gasses in the arteries in a prograde fashion and the veins in a retrograde fashion. On the other hand, manual ventilation with a bag–valve–mask or similar device supplies air to the body, resulting in extensive dilation of the gastrointestinal tract. This CT finding can be observed on CT owing to manual ventilation [9,10] and there is no significant difference between the ROSC and non-ROSC groups.
On the other hand, no significant difference was found in the intracranial hyperdense venous sinus between the ROSC and non-ROSC groups. Hyperdense venous sinus occurs as a result of circulatory arrest and is known as livor mortis in the postmortem state [18]. In neonates and infants, the brain parenchyma exhibits higher water content and appears with lower attenuation on CT scans. This characteristic facilitates the contrast between the brain parenchyma and the developed intradural venous plexus. Consequently, it is plausible that the hyperdense intracranial venous sinuses represent normal physiological variations with minimal correlation to cardiac arrest. Given the challenges of pediatric imaging owing to the lower resolution inherent in pediatric CT modalities [19], radiologists must interpret the CT findings assessed in this study with caution, as their clinical significance may not always be evident.
Although our study did not establish the utility of WBCT in identifying causative factors of OHCA, one of the potential advantages of WBCT is its capacity to detect life-threatening conditions in critical organs such as the heart, brain, or lungs. Nonetheless, in this study, WBCT did not reveal definitive findings that clarified the etiology of cardiac arrest. This aligns with prior postmortem CT research, which indicates that the underlying causes of sudden cardiac arrest in pediatric cases, especially non-traumatic ones, often remain unidentified [20,21,22].
In recent years, postmortem CT has gained popularity in Japan and globally for determining the cause of death as a non-invasive complementary to traditional autopsy, particularly for detecting hemorrhagic, vascular, or other gross pathological lesions. However, its diagnostic accuracy in pediatric cases, especially in non-traumatic deaths, is limited [23]. For example, postmortem CT identified the cause of death in only 12.9% of pediatric cases in which the diagnosis was confirmed by autopsy. In contrast, in 74.1% of cases, postmortem CT did not provide additional diagnostic information, often owing to infectious or cardiovascular causes of death that are not easily identifiable via imaging [22]. Other studies have also reported low diagnostic accuracy for pediatric postmortem CT in cases of natural death, indicating that postmortem CT does not typically provide new insights when the cause of death is unexplained by pathologists [24]. Studies on pediatric postmortem CT have reported that it is often challenging to identify a definite cause of death [22,25,26,27], which is consistent with the present findings. Nevertheless, the absence of significant findings on WBCT can still be clinically valuable, especially in ruling out external causes of cardiac arrest when the circumstances are unclear. Just as postmortem CT can sometimes identify the cause of death, identifying the cause of cardiac arrest on CT could guide immediate and targeted interventions, potentially improving outcomes by preventing delays in treatment in OHCA cases. The role of technology in the management of OHCA cases remains promising and merits further investigation.
A notable concern in pediatric cardiopulmonary arrest cases is the parent's refusal to discontinue resuscitation procedures. Identification of cardiac arrest is also essential for grief care [28]. In these situations, CT may sometimes be able to explain the cardiac arrest and provide important information to help bring some closure to the grieving family. In this perspective, the timing of CT scans in OHCA cases, ideally conducted with family consent, remains a practical challenge. In the previous study, most CT scans were performed during ongoing resuscitation efforts. Previous surveys indicate that 22% of institutions perform CT scans during resuscitation [4], possibly influenced by Japan's health insurance system, which does not cover postmortem examinations. Consequently, CT scans are often performed during CPR to meet insurance requirements and ensure compensation before death is formally declared.
This study presents several limitations. Firstly, the retrospective design and the small sample size of 27 cases may limit the generalizability of our findings. OHCA without prehospital ROSC is uncommon, especially at single institutions, underscoring the necessity for larger, multi-institutional studies to corroborate our results. Secondly, the CT findings evaluated were based on known normal postmortem changes; however, other indicators that might predict non-ROSC could exist and were not captured in this study. Thirdly, variability in resuscitation practices, such as epinephrine administration, ventilation methods, and chest compression techniques, might have influenced outcomes, as CPR protocols were not standardized across all cases. Chest compressions were interrupted during WBCT scanning, but the interruption lasted less than 10 seconds, and we consider that the scanning did not affect resuscitation. Furthermore, the potential influence of other diagnostic measures immediately post-admission, such as echocardiography or abdominal ultrasound, on cardiopulmonary resuscitation procedures was not considered.
5. Conclusions
WBCT did not reveal the direct cause of OHCA in patients without prehospital ROSC. However, our evaluation of CT findings during the agonal phase in pediatric OHCA cases identified several findings that were more frequently observed in the non-ROSC group. For parents and families confronted with the sudden cardiac arrest of their child, sharing CT findings that resemble postmortem changes may help communicate the futility of continued resuscitation efforts, potentially easing the process of accepting the situation. Given the critical challenge of managing pediatric OHCA in the ED, WBCT may emerge as a valuable clinical tool in guiding decisions on whether to continue or cease resuscitative efforts in children who have experienced cardiac arrest.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Table S1: Clinical information and CT findings of 19 pediatric OHCA patients with non-ROSC; Table S2: Clinical information and CT findings of 8 pediatric OHCA patients with ROSC.
Author Contributions
Conceptualization, M.I. and S.M.; Methodology, M.I.; Validation, M.I. and T.T.; Formal Analysis, M.I. and T.T.; Investigation, M.I., H.U. and T.T.; Data Curation, M.I., T.T., and S.M.; Writing – Original Draft Preparation, M.I.; Writing – Review & Editing, M.I., S.M., H.U., H.N., S.W., and M.N.; Visualization, M.I.; Supervision, G.Y., H.H., and K.S.; Project Administration, M.I. and K.S.; Funding Acquisition, M.I.
Funding
This research was funded by the Japan Society for the Promotion of Science (JSPS) KAKENHI Grant No. 23K07202.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board of Tokyo Medical University Hospital (Approval No.: T2023-0192).
Informed Consent Statement
Informed consent was waived by the ethics committee owing to the retrospective nature of the study.
Data Availability Statement
Raw data are available upon request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Tokyo Households and Population (by town/village and age) by Basic Resident Ledger; Statistics Division, Bureau of General Affairs, Tokyo Metropolitan Government, 2024. Available online: https://www.toukei.metro.tokyo.lg.jp/juukiy/2024/jy24qf0001.pdf.
- Current status of emergency services 2022; Tokyo Fire Department, 2023. Available online: https://www.tfd.metro.tokyo.lg.jp/hp-kyuukanka/katudojitai/data/pdf/R2_2.pdf.
- Numaguchi, A.; Mizoguchi, F.; Aoki, Y.; An, B.; Ishikura, A.; Ichikawa, K.; Ito, Y.; Uchida, Y.; Umemoto, M.; Ogawa, Y.; et al. Epidemiology of child mortality and challenges in child death review in Japan: the Committee on Child Death Review: A Committee Report: The Committee on Child Death Review: a Committee Report. Pediatr Int 2022, 64, e15068. [CrossRef]
- Survey on the search for causes of pediatric out-of-hospital cardiac arrest (in Japanese); Japan Pediatric Association. Available online: https://www.jpeds.or.jp/uploads/files/20240729_ingai_hokoku.pdf.
- Adel, J.; Akin, M.; Garcheva, V.; Vogel-Claussen, J.; Bauersachs, J.; Napp, L.C.; Schäfer, A. Computed-tomography as first-line diagnostic procedure in patients with out-of-hospital cardiac arrest. Front Cardiovasc Med 2022, 9, 799446. [CrossRef]
- Chelly, J.; Mongardon, N.; Dumas, F.; Varenne, O.; Spaulding, C.; Vignaux, O.; Carli, P.; Charpentier, J.; Pène, F.; Chiche, J.D.; et al. Benefit of an early and systematic imaging procedure after cardiac arrest: insights from the PROCAT (Parisian RegionOut of Hospital Cardiac Arrest) registry. Resuscitation 2012, 83, 1444–1450. [CrossRef]
- Christ, M.; von Auenmueller, K.I.; Noelke, J.P.; Sasko, B.; Amirie, S.; Trappe, H.J. Early computed tomography in victims of non-traumatic out-of-hospital cardiac arrest. Intern Emerg Med 2016, 11, 237–243. [CrossRef]
- Viniol, S.; Thomas, R.P.; König, A.M.; Betz, S.; Mahnken, A.H. Early whole-body CT for treatment guidance in patients with return of spontaneous circulation after cardiac arrest. Emerg Radiol 2020, 27, 23–29. [CrossRef]
- Ishida, M.; Gonoi, W.; Okuma, H.; Shirota, G.; Shintani, Y.; Abe, H.; Takazawa, Y.; Fukayama, M.; Ohtomo, K. Common postmortem computed tomography findings following atraumatic death: differentiation between normal postmortem changes and pathologic lesions. Korean J Radiol 2015, 16, 798–809. [CrossRef]
- Ishida, M.; Gonoi, W.; Abe, H.; Ushiku, T.; Abe, O. Essence of postmortem computed tomography for in-hospital deaths: what clinical radiologists should know. Jpn J Radiol 2023, 41, 1039–1050. [CrossRef]
- Shiotani, S.; Kohno, M.; Ohashi, N.; Yamazaki, K.; Nakayama, H.; Ito, Y.; Kaga, K.; Ebashi, T.; Itai, Y. Hyperattenuating aortic wall on postmortem computed tomography (PMCT). Radiat Med 2002, 20, 201–206.
- Takahashi, N.; Higuchi, T.; Hirose, Y.; Yamanouchi, H.; Takatsuka, H.; Funayama, K. Changes in aortic shape and diameters after death: comparison of early postmortem computed tomography with antemortem computed tomography. Forensic Sci Int 2013, 225, 27–31. [CrossRef]
- Shirota, G.; Gonoi, W.; Ishida, M.; Okuma, H.; Shintani, Y.; Abe, H.; Takazawa, Y.; Ikemura, M.; Fukayama, M.; Ohtomo, K. Brain swelling and loss of gray and white matter differentiation in human postmortem cases by computed tomography. PLOS ONE 2015, 10, e0143848. [CrossRef]
- Shiotani, S.; Kohno, M.; Ohashi, N.; Atake, S.; Yamazaki, K.; Nakayama, H. Cardiovascular gas on non-traumatic postmortem computed tomography (PMCT): the influence of cardiopulmonary resuscitation. Radiat Med 2005, 23, 225–229.
- Ishida, M.; Gonoi, W.; Hagiwara, K.; Takazawa, Y.; Akahane, M.; Fukayama, M.; Ohtomo, K. Intravascular gas distribution in the upper abdomen of non-traumatic in-hospital death cases on postmortem computed tomography. Leg Med (Tokyo) 2011, 13, 174–179. [CrossRef]
- Yamaki, T.; Ando, S.; Ohta, K.; Kubota, T.; Kawasaki, K.; Hirama, M. CT demonstration of massive cerebral air embolism from pulmonary barotrauma due to cardiopulmonary resuscitation. J Comput Assist Tomogr 1989, 13, 313–315. [CrossRef]
- Barber, J.L.; Kiho, L.; Sebire, N.J.; Arthurs, O.J. Interpretation of intravascular gas on postmortem CT in children. J Forensic Radiol Imaging 2015, 3, 174–179. [CrossRef]
- Takahashi, N.; Satou, C.; Higuchi, T.; et al. Quantitative analysis of intracranial hypostasis: comparison of early postmortem and antemortem CT findings. AJR 2010, 195, 388–393.
- Gould, S.W.; Harty, M.P.; Givler, N.E.; Christensen, T.E.; Curtin, R.N.; Harcke, H.T. Pediatric postmortem computed tomography: initial experience at a Children’s Hospital in The United States. Pediatr Radiol 2019, 49, 1113–1129. [CrossRef]
- Krentz, B.V.; Alamo, L.; Grimm, J.; Dédouit, F.; Bruguier, C.; Chevallier, C.; Egger, C.; Da Silva, L.F.F.; Grabherr, S. Performance of post-mortem CT compared to autopsy in children. Int J Legal Med 2016, 130, 1089–1099. [CrossRef]
- Oyake, Y.; Aoki, T.; Shiotani, S.; Kohno, M.; Ohashi, N.; Akutsu, H.; Yamazaki, K. Postmortem computed tomography for detecting causes of sudden death in infants and children: retrospective review of cases. Radiat Med 2006, 24, 493–502. [CrossRef]
- van Rijn, R.R.; Beek, E.J.; van de Putte, E.M.; Teeuw, A.H.; Nikkels, P.G.J.; Duijst, W.L.J.M.; Nievelstein, R.A.; Dutch NODO Group. The value of postmortem computed tomography in paediatric natural cause of death: a Dutch observational study. Pediatr Radiol 2017, 47, 1514–1522. [CrossRef]
- Speelman, A.C.; Engel-Hills, P.C.; Martin, L.J.; van Rijn, R.R.; Offiah, A.C. Postmortem computed tomography plus forensic autopsy for determining the cause of death in child fatalities. Pediatr Radiol 2022, 52, 2620–2629. [CrossRef]
- Sieswerda-Hoogendoorn, T.; Soerdjbalie-Maikoe, V.; de Bakker, H.; van Rijn, R.R. Postmortem CT compared to autopsy in children; concordance in a forensic setting. Int J Legal Med 2014, 128, 957–965. [CrossRef]
- Proisy, M.; Marchand, A.J.; Loget, P.; Bouvet, R.; Roussey, M.; Pelé, F.; Rozel, C.; Treguier, C.; Darnault, P.; Bruneau, B. Whole-body post mortem computed tomography compared with autopsy in the investigation of unexpected death in infants and children. Eur Radiol 2013, 23, 1711–1719. [CrossRef]
- Noda, Y.; Yoshimura, K.; Tsuji, S.; Ohashi, A.; Kawasaki, H.; Kaneko, K.; Ikeda, S.; Kurokawa, H.; Tanigawa, N. Postmortem computed tomography imaging in the investigation of nontraumatic death in infants and children. BioMed Res Int 2013, 2013, 327903. [CrossRef]
- Ishida, M.; Gonoi, W.; Shirota, G.; Abe, H.; Shintani-Domoto, Y.; Ikemura, M.; Ushiku, T.; Abe, O. Utility of unenhanced postmortem computed tomography for investigation of in-hospital nontraumatic death in children up to 3 years of age at a single Japanese tertiary care hospital. Med (Baltim) 2020, 99, e20130. [CrossRef]
- Garstang, J.; Griffiths, F.; Sidebotham, P. What do bereaved parents want from professionals after the sudden death of their child: a systematic review of the literature. BMC Pediatr 2014, 14, 269. [CrossRef]
Figure 1.
Nine-month-old boy with non-ROSC (case no. 19 in Table S1). (a) Observations in the head included brain swelling, loss of cerebral gray-white matter differentiation, and hyperdense intracranial venous sinus (arrows). (b) Symmetrical consolidation/ground-glass opacity of the lungs was noted. (c) In the mediastinum, findings included cardiomegaly, a hyperdense aortic wall (arrows), and gas in the cardiac cavity (arrowheads). (d) A narrowed aorta (arrow) and hepatomegaly were observed.
Figure 1.
Nine-month-old boy with non-ROSC (case no. 19 in Table S1). (a) Observations in the head included brain swelling, loss of cerebral gray-white matter differentiation, and hyperdense intracranial venous sinus (arrows). (b) Symmetrical consolidation/ground-glass opacity of the lungs was noted. (c) In the mediastinum, findings included cardiomegaly, a hyperdense aortic wall (arrows), and gas in the cardiac cavity (arrowheads). (d) A narrowed aorta (arrow) and hepatomegaly were observed.
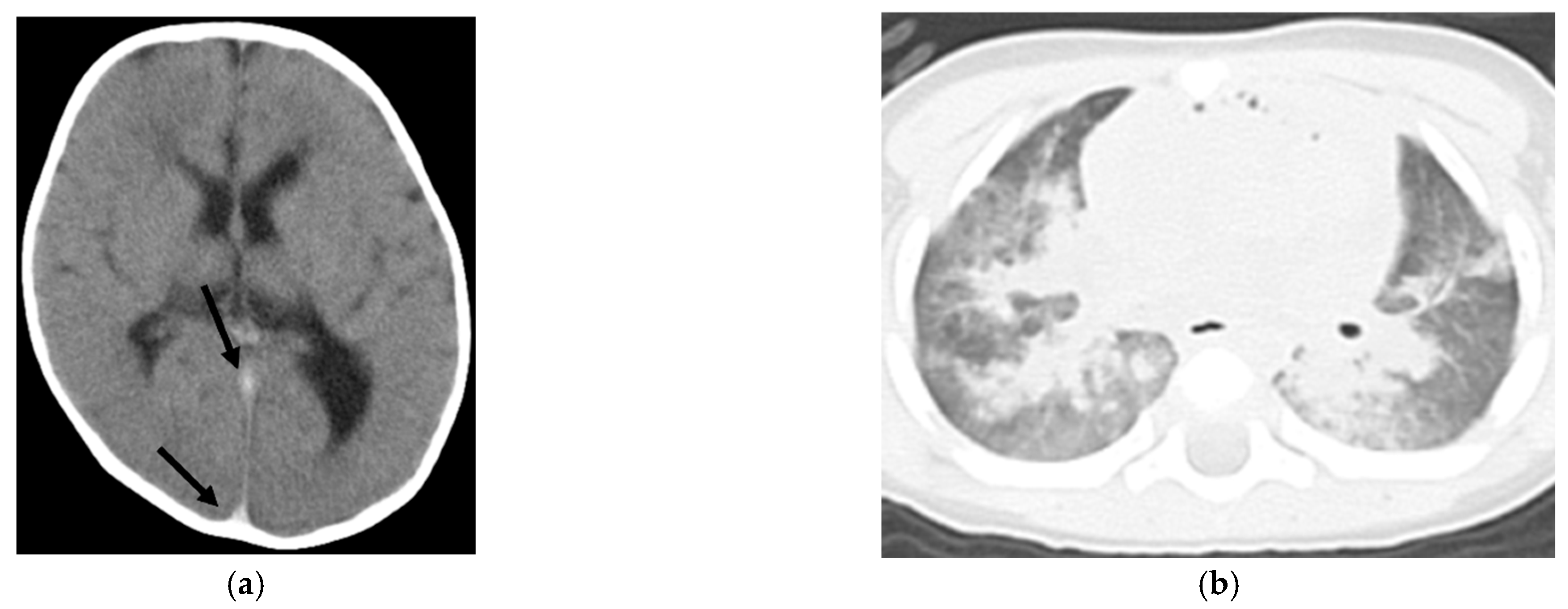
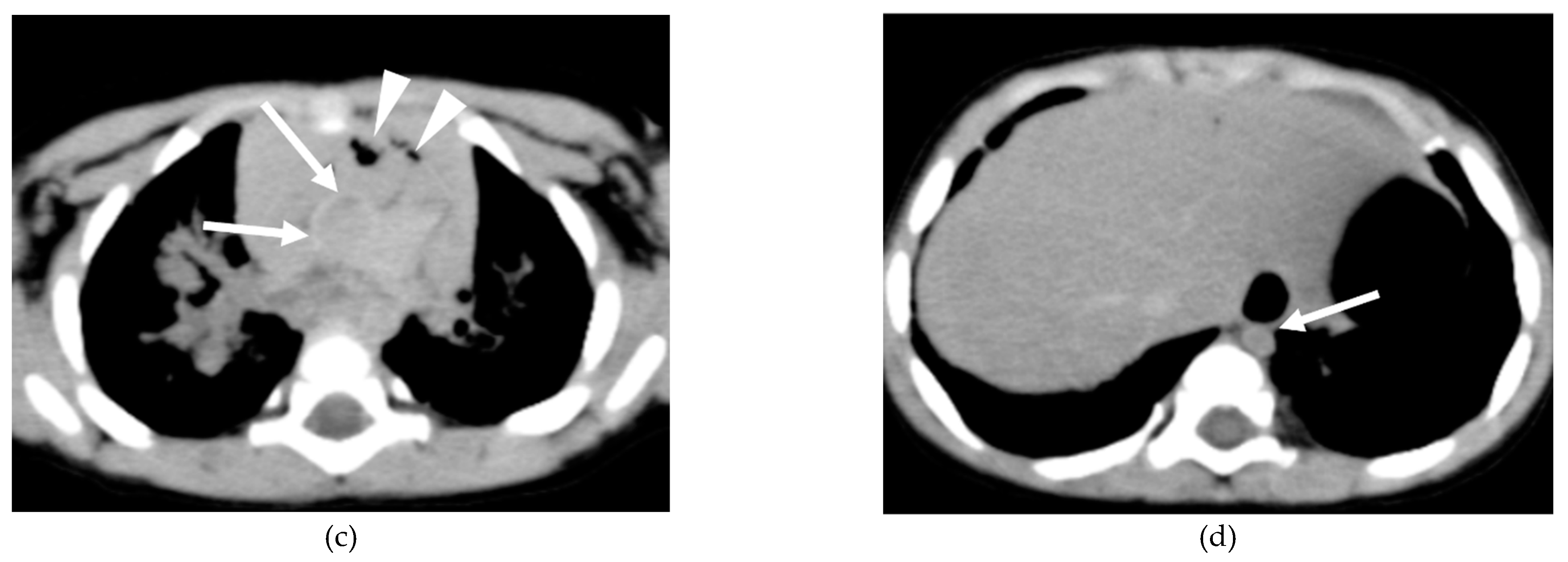
Figure 2.
Four-month-old boy with ROSC (case no. 6 in Table S2). (a) No symmetrical or asymmetrical lung consolidation/ground-glass opacity of the lungs was observed. (b) In the mediastinum, mild cardiomegaly was noted, but no hyperdense aortic wall was identified. (c) A dilated gastrointestinal tract was observed.
Figure 2.
Four-month-old boy with ROSC (case no. 6 in Table S2). (a) No symmetrical or asymmetrical lung consolidation/ground-glass opacity of the lungs was observed. (b) In the mediastinum, mild cardiomegaly was noted, but no hyperdense aortic wall was identified. (c) A dilated gastrointestinal tract was observed.
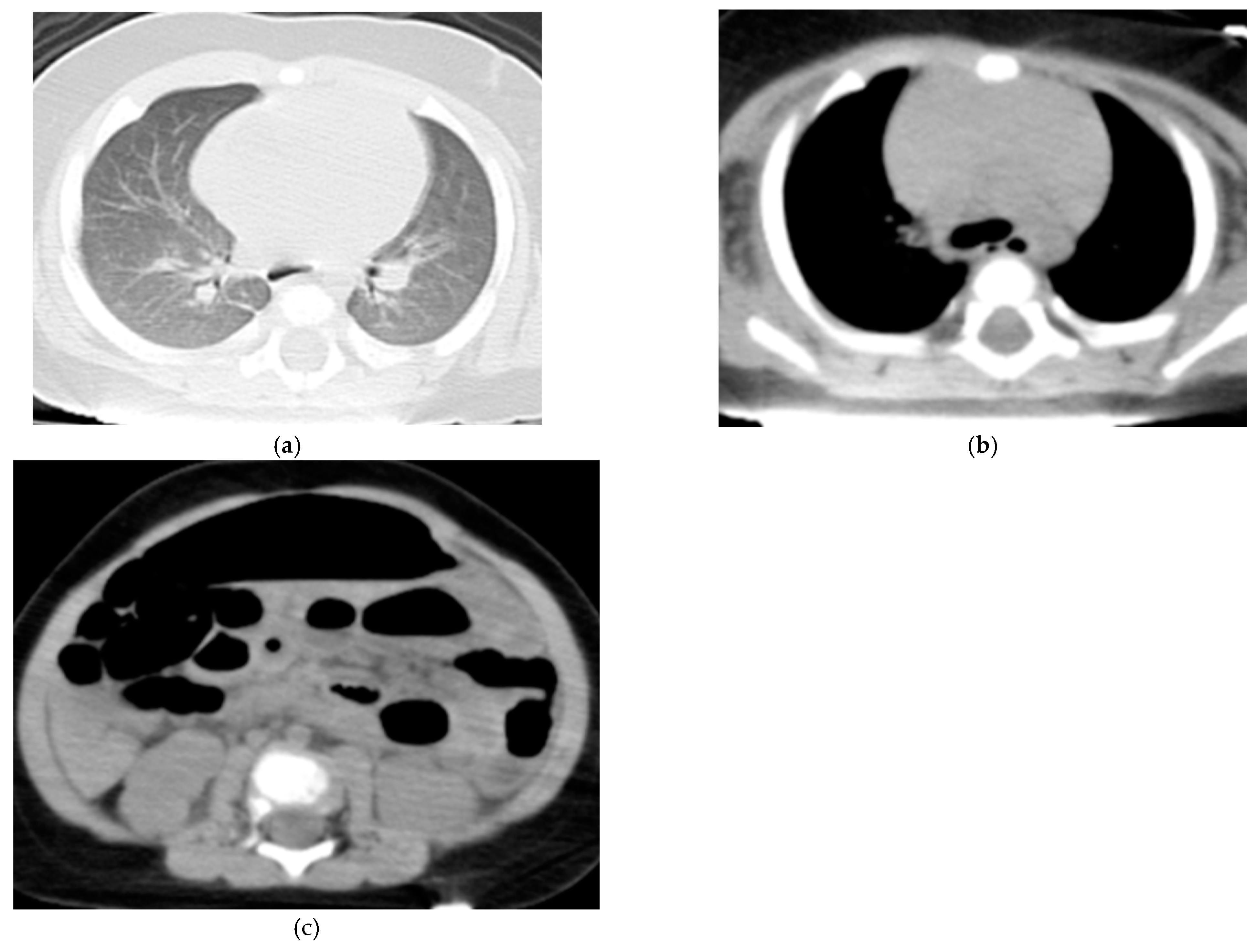

Table 1.
Patient characteristics.
| non-ROSC (n=19) | ROSC (n=8) | p (Mann–Whitney U test) | |
|---|---|---|---|
| Age (mean month, range) | 13.2 (1–108) | 14.3 (0.4–166) | 0.735 |
| Sex (m:f) | 10:9 | 4:4 | 0.938 |
| Past history (-:+) | 13:6 | 7:1 | 0.449 |
| Whether or not the home of the place of discovery (-:+) | 18:1 | 5:3 | 0.198 |
| Whether found after bedtime (-:+) | 18:1 | 1:7 | < .001 |
| Estimated time from the last sighting to discovery (mean minutes, range) | 254.8 (0–560) | 17.3 (0–115) | < .001 |
| Bystander CPR (+:-) | 7:12 | 3:5 | 0.979 |
CPR - Cardiopulmonary Resuscitation; ROSC - Return of Spontaneous Circulation.
Table 2.
Differences in CT findings of OHCA between non-ROSC and ROSC groups.
| Number of positive cases | |||
| CT findings | non-ROSC (n=19) | ROSC (n=8) | p (Fisher’s exact test) |
| Head | |||
| Brain swelling | 16 | 1 | <0.001 |
| Loss of cerebral gray-white matter differentiation | 14 | 3 | 0.033 |
| Hyperdense intracranial venous sinus | 6 | 0 | 0.136 |
| Lung | |||
| Symmetrical consolidation/ground-glass opacity | 18 | 4 | 0.017 |
| Asymmetrical consolidation/ground-glass opacity | 2 | 2 | 0.558 |
| Mediastinum | |||
| Cardiomegaly | 16 | 2 | 0.006 |
| Pericardial effusion | 0 | 0 | n/a |
| Hyperdense aortic wall | 16 | 0 | <0.001 |
| Narrowed aorta | 19 | 0 | <0.001 |
| Gas in the cardiac cavity, aorta, and superior vena cava | 15 | 0 | <0.001 |
| Abdomen and pelvis | |||
| Hepatomegaly | 15 | 1 | 0.002 |
| Dilated inferior vena cava | 3 | 2 | 0.616 |
| Dilated gastrointestinal tract | 17 | 5 | 0.136 |
| Gas in the upper abdominal organs | 8 | 0 | 0.061 |
| Soft tissue | |||
| Subcutaneous fatty edema | 0 | 0 | n/a |
CT - Computed Tomography; n – number; OHCA - Out-of-Hospital Cardiac Arrest; ROSC - Return of Spontaneous Circulation.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



