
Submitted:
06 September 2024
Posted:
09 September 2024
You are already at the latest version
Abstract
Maternal obesity and gestational diabetes mellitus (GDM) are the most common metabolic conditions with have unfavourable impact on maternal and fetal health. Key biosubtrats such as apelin, vascular endothelial growth factor (VEGF), leptin, and DNA methylation play crucial roles in these pathologic conditions.
Apelin is a peptide involved in regulating glucose metabolism and cardiovascular functions. This molecule also interacts with the apelin receptor to enhance glucose uptake, suggesting potential therapeutic implications for managing GDM and obesity.
Leptin, a hormone predominantly produced by adipose tissue, regulates appetite and energy balance. In obesity, leptin levels are often high, but a resistance to its effects develops, disrupting normal metabolic processes. Similarly, in GDM, elevated leptin may impair glucose metabolism and contribute to insulin resistance.
VEGF is critical for angiogenesis, the formation of new blood vessels, and is often found in increased concentrations in obese individuals and those with GDM. This elevation may contribute to abnormal placental function and vascular complications, exacerbating both conditions.
DNA methylation, an epigenetic modification, plays a crucial role in gene expression regulation. In both GDM and obesity, altered DNA methylation patterns have been observed, affecting genes involved in metabolism, inflammation, and insulin sensitivity. These epigenetic changes may predispose individuals to metabolic disorders.
In our study we investigated placental apelin, leptin, VEGF, and DNA methylation interconnection in the pathophysiology of GDM and obesity during gestation. They have similar or different influencing on metabolic regulation, vascular function, and gene expression in GDM and obesity? Sonogpahic examinatios supported the metabolic analyses for that understanding their roles may lead to better management and therapeutic strategies for these conditions.
Keywords:
apelin
; leptin
; VEGF
; DNA methylation
; human pregnancy
; obesity
; placenta
; diabetes
1. Introduction
Gestational diabetes mellitus (GDM) is a type of diabetes that is first recognized during pregnancy. It is characterized by high blood sugar levels that develop during pregnancy in women who did not previously have diabetes. This condition can arise because pregnancy hormones can make the body less effective at using insulin, a hormone that regulates blood sugar levels. GDM diagnosed during pregnancy is present in around 10% in Europe [Dluski 2022], making it the most common medical complications during pregnancy [Tsakiridis I 2021, Visolyi-Kun 2023, Damm P 2016]. Showed an increase in the GDM incidence in last decades. The pooled global standardized prevalence of GDM was 14.0% (95% confidence interval: 13.97-14.04%). The regional standardized prevalence of GDM were 7.1% (7.0-7.2%) in North America and Caribbean, 7.8% (7.2-8.4%) in Europe, 10.4% (10.1-10.7%) in South America and Central America, 14.2% (14.0-14.4%) in Africa, 14.7% (14.7-14.8%) in Western Pacific, 20.8% (20.2-21.4%) in South-East Asia and 27.6% (26.9-28.4%) in Middle East and North Africa. The standardized prevalence of GDM in low-, middle- and high-income countries were 12.7% (11.0-14.6%), 9.2% (9.0-9.3%) and 14.2% (14.1-14.2%), respectively. [Wang 2022 ]. Gestational Diabetes Mellitus (GDM) and obesity are interrelated conditions that pose significant health risks for both mothers and their newborns. The prevalence of maternal obesity is rising rapidly worldwide and constitutes a major obstetric problem. It is as a main risk for GDM is rising significantly on all continents, reflecting broader global trends. Increased rates of obesity among women of childbearing age are contributing to a higher incidence of GDM, mirroring patterns observed throughout Europe. Factors such as urbanization, sedentary lifestyles, and dietary changes are key contributors. This surge presents substantial public health challenges, as both obesity and GDM are linked to adverse outcomes for mothers and infants, including increased risks of metabolic disorders, cardiovascular diseases, and complications during pregnancy and delivery. [Zehravi M 2021, Patham 2015]. Annual reports from the WHO reveal that 43% of women were overweight and 16% of women were obese in 2022. [WHO 2024].
GDM and obesity conditions are influenced by a variety of biochemical and molecular factors, including apelin, leptin, vascular endothelial growth factor (VEGF), and DNA methylation. Understanding the roles of these factors can provide insight into the pathophysiology of GDM and obesity, potentially leading to improved therapeutic strategies.
Apelin
Apelin is an endogenous peptide that plays a key role in the regulation of glucose homeostasis, cardiovascular functions, and angiogenesis. It is the ligand for the G protein-coupled receptor apelin, which is expressed in various tissues, including the heart, adipose tissue, and pancreas. [Antushevich H 2018]. In the context of obesity, apelin levels are generally elevated in serum, possibly as a compensatory mechanism to counteract metabolic dysregulation. Apelin has been shown to enhance glucose uptake in skeletal muscle and adipose tissue, and it may have insulin-sensitizing effects. In GDM, the expression of apelin is also upregulated, potentially as a response to increased metabolic demands and insulin resistance. Elevated serum apelin levels in GDM may contribute to improved glucose tolerance by enhancing insulin sensitivity, though this compensatory mechanism may not always suffice to maintain normal glucose levels. [Antushevich H 2018]. Moreover, apelin is implicated in cardiovascular health, and its dysregulation can exacerbate the risk of cardiovascular complications, which are already heightened in obesity and GDM. [Antushevich H 2018]
Vascular Endothelial Growth Factor (VEGF)
VEGF is a key regulator of angiogenesis, the process of new blood vessel formation, which is crucial for tissue growth and repair. It is particularly important in the context of placental development during pregnancy.[Ballmer-Hofer 2018]. In obese individuals and those with GDM, VEGF serum levels are often elevated. This overexpression can lead to abnormal angiogenesis, contributing to complications such as preeclampsia and fetal growth restriction. In the placenta, excessive VEGF can alter vascular permeability and placental function, potentially leading to adverse pregnancy outcomes.[Bolatai 2022]. The increased expression of VEGF in obesity and GDM is thought to be driven by hypoxic conditions in adipose tissue due to inadequate blood supply. This hypoxia-induced VEGF expression may further exacerbate inflammation and insulin resistance, creating a vicious cycle that aggravates the metabolic and vascular complications associated with these conditions.[Bolatai 2022, Ballmer-Hofer 2018]
Leptin
Leptin is a hormone primarily secreted by adipocytes and is pivotal in regulating energy balance, appetite, and metabolism. It acts on the hypothalamus to suppress appetite and promote energy expenditure. However, in the state of obesity, serum leptin levels are significantly increased, but paradoxically, leptin resistance occurs, where the body's responsiveness to leptin's effects is diminished. [Obradociv 2021]. In GDM, serum leptin levels are also elevated, likely reflecting the increased adiposity and insulin resistance characteristic of the condition. Leptin resistance in GDM can contribute to the dysregulation of energy homeostasis and glucose metabolism. [Obradociv 2021] Additionally, high serum leptin levels may influence placental function and fetal growth, potentially leading to macrosomia (excessive fetal growth), which is a common complication of GDM.[Gaudix 2023]. Leptin is also involved in the regulation of inflammation, and its elevated serum levels in obesity and GDM may contribute to a chronic low-grade inflammatory state. This inflammation can further impair insulin sensitivity and exacerbate metabolic dysregulation. [Obradociv 2021]
DNA Methylation
DNA methylation is an epigenetic modification that involves the addition of a methyl group to the cytosine base of DNA, typically leading to gene repression. This process plays a critical role in regulating gene expression and is influenced by environmental factors, including diet and metabolic status. [Moor 2013]. In the context of obesity and GDM, aberrant DNA methylation patterns have been observed. These changes can affect genes involved in key metabolic pathways, such as those regulating glucose and lipid metabolism, inflammation, and insulin signalling [Heikkinen 2022]. For instance, altered methylation of genes like PPARγ (a regulator of adipogenesis) and IGF2 (involved in fetal growth) has been linked to metabolic disturbances in obesity and GDM.[Horvath 2018, Law 2019]. The changes in DNA methylation in these conditions are not only relevant for the individual but can also have transgenerational effects. Epigenetic modifications influenced by maternal obesity or GDM can impact the health of the offspring, predisposing them to metabolic disorders later in life.[Moor 2013, Heikkinen 2022].
Interactions and Implications
The interplay between apelin, VEGF, leptin, and DNA methylation creates a complex network that influences the development and progression of GDM and obesity. For instance, the inflammatory state driven by leptin and VEGF can alter DNA methylation patterns, which in turn can affect the expression of genes involved in metabolism and vascular function. Apelin’s role in modulating insulin sensitivity and glucose uptake further integrates into this network, potentially offering a protective effect against the metabolic derangements seen in these conditions [Antushevich H 2018]. Understanding these interactions is crucial for developing therapeutic strategies. For example, targeting leptin resistance or VEGF pathways could potentially ameliorate some of the complications associated with GDM and obesity. Similarly, interventions aimed at modifying epigenetic marks, such as through diet or pharmacological agents, hold promise in mitigating the long-term effects of these conditions. Potential of biomarkers in two human deasese that show rather consistent alterations in obesity and glucose imbalance.
2. Materials and Methods
2.1. Samples
A prospective, cross-sectional cohort study was conducted in the Department of Obstetrics and Gynaecology, University of Szeged, Hungary, between June 2023 and March 2024 among pregnant women who underwent elective caesarean section. Inclusion criteria for the study were singleton pregnancies, where the caesarean section was performed between 34-41 weeks of gestation. Those at 34+0 and 40+0 weeks of gestation were included in our study (N=48). Placental samples (cc. 1 cm3) were taken at caesarean section. Normal, GDM, and obese (BMI>30 kg/m2) women were enrolled in our study at the Department of Obstetrics and Gynecology, University of Szeged. The human study protocol was approved by the Clinical Research Ethics Committee of the University of Szeged (Ref. No. 57/2020-SZTE). The study was conducted according to the principles of the Declaration of Helsinki. Written informed consent was obtained from all participants. The exclusion criteria for the study included: overweighed pregnant women (BMI= 25-30 kg/m2), underweighted pregnant women (BMI<18 kg/m2) multiple pregnancies, structural or genetic abnormalities of the fetus and/or neonate, inappropriate placental localization (e.g. placenta praevia), abnormal placentation (placenta accreta spectrum), and self-reported drug, alcohol or nicotine dependence. Gestational age was determined on the basis of ultrasound biometry (coronal peak length and biparietal diameter) performed on the first day of the last menstrual period and/or at 10 weeks of pregnancy. Placental tissues were frozen immediately after collection and stored at -80 °C until examination. Forty-eight cases were included to the study: normal pregnancies (n=30), obese pregnancies (n=12) , and GDM (n=6) with placental samples.
2.2. Ultrasound Investigations
The ultrasound investigation was performed 16-48 hours before caesarean section. Standard 2D measurements were taken: fetal position and presentation, body movements and fetal heart rate, and placental localization. The factorial default setting ‘Obstetrics/2–3 trimester’ was used in 2-D mode. Then, a 3D sweep was obtained through the placenta with power Doppler settings. The 3DPD sweep was obtained through the placenta with a Voluson S10 BT2021 ultrasound machine (RAB 2-5 MHz probe and 4D View version 10.4 program; GE Healthcare, Kretztechnik, Zipf, Austria). The volume acquisition was obtained in ‘maximum’ quality and its duration was between 10 and 15 s keeping the probe perpendicular to the placental plate. The same pre-established instrument settings were used in all the cases (power 96%; frequency low; quality normal, density 6, ensemble 16; balance 150; filter 2; smooth 3/5; pulse repetition frequency 0.9 kHz, gain -0.2). Each image was recovered from the disk in succession for processing. The stored volumes were further analysed using the virtual organ computer-aided analysis (VOCAL) program pertaining to the computer software 4D VIEW (GE Medical Systems, Austria, version 10.4) , which consists of outlining the contour of the placenta repeatedly after rotating its image 6 times by 30°, with careful attention to exclude decidua and maternal vessels. After the complete rotation was finished, the placental volume was automatically calculated by the software. For each patient, placental volumes were measured 3 times by a specifically trained sonographer. The three-dimensional volume is composed of small units of volume known as "voxels." Voxels encompass all data regarding grey and colour intensity scales ranging from 0 to 100. Based on these values, three power Doppler indices can be derived from this measurement system, which are suitable for evaluating vessels and blood flow. These 3-DPD indices are employed in assessing placental perfusion, and it is widely acknowledged that they may reflect both uteroplacental and fetoplacental blood flow.
The vascularization index (VI), defined as the ratio of colour voxels to total voxels, quantifies the presence of blood vessels within a given volume of interest and is expressed as a percentage (vascularity). The flow index (FI) represents the average colour value of all colour voxels, indicating the average intensity of blood flow on a scale from 0 to 100 (unitless). The vascularization flow index (VFI), calculated as the weighted ratio of colour voxels to total voxels, combines information on vessel presence (vascularity) and the quantity of blood cells transported (unitless). The values range from 0 to 100. The VOCAL program automatically computes these indices (VI, FI, VFI) based on the collected samples.
2.3. RT-PCR Studies
2.3.1. Total RNA Preparation from Tissue
The cellular RNA was isolated using the guanidinium thiocyanate-acid-phenol-chloroform extraction method described by Chomczynski and Sacchi [Chomzynski 1997]. Following precipitation with isopropanol, the RNA underwent a wash with 75% ethanol and was then resuspended in diethylpyrocarbonate-treated water. The purity of the RNA was verified by measuring the optical density at 260/280 nm using BioSpec Nano (Shimadzu, Japan), with all samples showing an absorbance ratio within the range of 1.6-2.0. The quality and integrity of the RNA were evaluated through agarose gel electrophoresis.
2.3.2. Real-Time Quantitative Reverse Transcription-PCR (RT-PCR)
Reverse transcription and amplification of the PCR products were performed by using the TaqMan RNA-to-CT-Step One Kit (Thermo Fisher Scientific, Hungary) and an ABI StepOne Real-Time cycler. Reverse-transcriptase PCR amplifications were performed as follows: at 48 °C for 15 min and at 95 °C for 10 min, followed by 40 cycles at 95 °C for 15 sec and at 60 °C for 1 min. The generation of specific PCR products was confirmed by melting curve analysis. The following primers were used: assay ID Hs00270873_s1 for the APLNR and Hs01060665_g1 for β-actin as endogenous control (Thermo Fisher Scientific, Hungary). Each sample was analyzed in triplicate. The fluorescence intensities of the probes were graphed against the PCR cycle number. The amplification cycle at which the first significant increase in fluorescence signal was observed was designated as the threshold cycle (CT).
2.4. ELISA Assay
Following the manufacturers’ recommendations, leptin and VEGF concentrations were measured using an ELISA assay kit (Human Lep ELISA Kit, Human VEGF kit, FineTest, China). All optical density values were measured using a SPECTROStar Nano microplate spectrophotometer (BMG Labtech, Germany).
2.5. Global DNA Methylation
The DNA isolation from the placenta tissues was made by the GeneaidTM DNA Isolation Kit (Geneaid Biotech Ltd.,Taiwan), and the global DNA methylation was determined by the Methylated DNA Quantification Kit (Abnova Ltd., Taiwan).
2.6. Statistical Analysis
Statistical analyzes were performed with the Prism 10.2.1 software (Graphpad Software Inc. San Diego, CA, USA). All data were evaluated with one-way ANOVA-test (Dunett’s post hoc test) or unpaired t-test, and each is presented as the mean ±SEM. Significance was accepted at p<0.05.
3. Results
The demographical data present (see Table 1) the population studies, the GDM pregnant are older, than normal population at delivery and the gestation period is less, than normal, because fetal or maternal complication, that may require cesarean section in earlier gestational age. The obesity prevalence is high in all age group, so it compare to the normal pregnant population has no alteration in maternal age and gestational length. it is important to highlight we recruited obese cases without other health problem (e.g. diabetes or blood hypertension). Obese women who participated in our study had a mean BMI of 37.67 kg/m2 at the first medical visit. The GDM cases had BMI in the normal range: 18-25 kg/m2 at first medical visit.
Table 2 displays the 3-dimensional power Doppler indices in the placenta. The placental volumetry were prepared in 3D mode by VOCAL program (Figure 1). The in vivo vascular analyses were at umbilical insertion in the most vascularized part of the placenta (Figure 2). In the two study groups, the placental volume was significantly elevated, while the vascularization indices (VI: vascularization index, FI: flow index, and VFI: vascularization flow index) were significantly depressed in the obese and GDM cases compared to normal-weighted pregnant women. Between the obes and GDM cases were no significantly alteration in placental volume and 3-dimensional power Doppler indices.
The placental biomarker analyses present the follow data results. Apelin receptor mRNA expression was significantly decreased in the samples from women with GDM; however, it did not significantly change in the samples from obese women compared to the control samples (Figure 3.).
The VEGF concentration decreased significantly in the GDM samples, and the obese samples compared to the control in the placenta tissue (Figure 4).
Leptin concentration significantly decreased in the GDM samples, while it did not change significantly in the obese samples compared to the control samples (Figure 5).
The 5-mC (5-methylcytosine) percentage of the GDM samples increased significantly compared to the control, while the 5-mC percentage of the obese samples did not change significantly (Figure 6).
4. Discussion
Although there is a rapid increase in the prevalence of diabetes in many parts of the world, such as in Middle East Asia, global estimates and comparisons of the prevalence of diabetes, particularly GDM, are difficult to make due to the wide variation in screening strategies and diagnostic criteria used to identify the disease. Fetal abnormalities, such as cardiac abnormalities, are at least 15 times more common than in the offspring of non-diabetic pregnancies [Damm P 2016]. Aside from the short-term maternal, fetal and neonatal consequences associated with GDM, there are long-term consequences for both mother and their child [Damm P 2016].While studies in adult offspring are limited, several human studies exist in children from different populations, involving a mix of different maternal diabetes types [Fraser A 2014]. The results of these studies are in line with the animal studies, the majority finding increased risk of diabetes and obesity in children exposed to maternal diabetes. [Damm P 2016, Fraser 2024].The prevalence of GDM had been elevated in last decade, because the population BMI is elevated by 12% during fertile ages in women. [Gregory ECW 2022]. In our study we investigated these two high-risk group.
In sonography-based cohort studies of singleton pregnancies, volume and weight of placenta were higher in obese and GDM pregnancies than in normal-weight controls. Our data may be consistent with the report that obese and GDM mothers have larger placentas because vasculogenesis is impaired and edema occurs in these placentas [Musa 2024, Suranyi 2016]. The placental volume were not significantly different in GDM and obes cases.
We observed a negative correlation between 3-D power Doppler indices and maternal BMI in pregnancies with obesity and GDM. Compared to the control group, the indices were reduced, although VI, FI and VFI values overlapped in the GDM and obese groups, but all higher placental volumes were associated with worse vascular indices. Increased placental volume expansion was not only associated with BMI but also with abnormal glycation. Decreases in placental VI and VFI in obesity and GDM were associated with reduced angiogenesis and decreased arteriolar number causing placental edema. However, depressed FI may represent a narrower internal vascular diameter. Th three dimensional ultrasonography did not detect differences between the obese and GDM groups, whereas biomarkers showed characteristic shifts. [Musa 2023]. It has been suggested that the placenta plays an active role in mediating inflammation in women with obesity and GDM. Placental structure and function may be altered in an adaptive response to obesity, and the placenta may act as a target and a source of inflammatory cytokines and biomarkers in pregnancies [Patham 2015].
Obesity and gestational diabetes mellitus (GDM) share several common pathophysiological mechanisms, particularly related to insulin resistance and low-grade inflammation [Patham 2015]. These overlapping pathways contribute to the development and complications of both conditions. Obesity and gestation complicated by GDM by increasing the risk of fetal and placental growth abnormality [Pahtam 2015, Suranyi 2016]. Insulin resistance is a central feature in both obesity and GDM. In obesity the excess adipose tissue, particularly visceral fat, increases the release of free fatty acids and adipokines (hormones produced by fat cells), which can interfere with insulin signalling [Patham 2015, Zehravi 2021]. This leads to reduced glucose uptake by the cells, requiring the pancreas to produce more insulin to maintain normal blood glucose levels. Over time, the pancreas may fail to keep up with this demand, leading to hyperglycemia.[Zehravi 2021]
During pregnancy, hormonal changes naturally increase insulin resistance as a mechanism to ensure more glucose is available to the fetus. In women with pre-existing insulin resistance (often associated with obesity), this additional insulin resistance can overwhelm pancreatic insulin production capacity, leading to elevated blood glucose levels and GDM. [zehravi 2021, Ruppert 2024]. Both obesity and GDM are associated with a state of chronic low-grade inflammation [Patham 2015, Lim 2023, Ruppert 2024]. Inflammation is also characterized by an increased basal metabolic rate due to the focused and rapid response to the insult [Patham 2015].The profile of immune cells favoring a pro-inflammatory environment in tissues such as adipose, liver and pancreas; it is chronically maintained by metabolic cells such as adipocytes without resolution, and it is associated with a reduced metabolic rate [Gregor MF 2011, Ruppert 2024]. For these reasons, the term ‘metaflammation’ or ‘metainflammation’ was coined to describe this particular profile associated with obesity [Gregor MF 2011]. The link between adiposity, inflammation and insulin resistance was first identified when it was observed that levels of the proinflammatory cytokines were increased in adipose tissue of obese individuals, and that antagonism led to increased insulin sensitivity [Ruppert 2024]. Weight-loss is associated with a reduction cytokines and reversal of insulin resistance. It is now evident that, in the obese state, several adipokines, chemokines, and cytokines released from adipose tissue and immune cells may interact in an autocrine and paracrine network, causing impaired insulin sensitivity in the metabolic syndrome [Ruppert 2024]. Adipose tissue thus behaves as one of the largest endocrine organs in the body [Ahima 2000]. Insulin acts by binding to insulin receptors in muscle, liver and adipose tissue, leading to phosphorylation of insulin receptor substrates. The regulatory subunit phosphorylates Akt, resulting in translocation of the glucose transporter in adipose tissue and muscle to the plasma membrane to facilitate glucose uptake [Ruppert 2024]. Insulin-stimulated Akt phosphorylation also activates glycogen synthase and glycogen synthesis. After insulin signaling, mitogen-activated protein kinase plays a role in promoting protein synthesis and cell growth and differentiation [Cildir 2013]. Normal pregnancy is also characterized by a state of insulin resistance, with a 50% reduction in insulin-mediated glucose clearance, and a ~250% increase in insulin production to maintain maternal euglycemia [Catalano 1999].
Pregnancy itself is characterized by an altered inflammatory profile compared to the non-pregnant state. A tightly regulated balance between pro- and anti-inflammatory biosubstrats may be necessary for normal implantation, trophoblast invasion and placentation.[Mor G 2011]
Apelin receptor mRNA expression and leptin concentration was significantly decreased in the placental samples from women with GDM, compare to the normal placenta. The obesity has similar effect, but the depression of leptin and apelin receptor mRNA expression were not significat.
In women with Gestational Diabetes Mellitus (GDM), the expression of apelin receptor mRNA and leptin concentrations are often decreased due to several possible mechanisms [Musa 2023]: In GDM, serum apelin levels are typically elevated, which may contribute to insulin resistance [Zehravi 2021].
- Insulin Resistance and Hormonal Dysregulation: GDM is characterized by insulin resistance, which can affect the regulation of various hormones and receptors, including apelin and leptin. Insulin resistance may impair the signaling pathways that regulate the expression of apelin receptors and the secretion of leptin.
- Inflammation and Oxidative Stress: GDM is associated with increased inflammation and oxidative stress, which can lead to alterations in the expression of genes and proteins involved in metabolic regulation. These conditions might downregulate apelin receptor expression and leptin production.
- Placental Function: The placenta plays a significant role in hormone regulation during pregnancy. In GDM, placental function is often compromised, which can affect the production and regulation of hormones like leptin. Abnormal placental function could also influence the expression of apelin receptors in maternal tissues.
- Nutritional and Metabolic Factors: The altered metabolic environment in GDM, including changes in glucose and lipid metabolism, may impact the levels of leptin and the expression of its receptors, including the apelin receptor.
These factors together can lead to the observed decrease in apelin receptor mRNA expression and leptin concentrations in women with GDM compared to those without the condition. (Musa 2023, Musa 2024]. The change of adipokine secretion can lead to the change of glucose homeostasis during pregnancy, and adipokine is also associated with the pathogenesis of GDM and obesity, so adipokines have become a hot spot in GDM and obesity research [Ruppert 2024]. The peripheral blood changes present serum leptin concentration is elevated in obesity and GDM, while the adipokin concentration is depressed in obesity and GDM cases [Xu 2020]. The placental tissue analyses presented adipokin concentration significantly decreased both in the GDM and obes samples [Xu 2022, Ruppert 2024]. The leptin concentration significantly decreased in the GDM samples, while leptin value depressed non significantly in the obese samples. The GDM cause more severe depression in placental tissues, compare to obesity. The serum level of leptin in the early pregnancy is 2–3 times higher than that in the non-pregnancy period, and gradually increases during gestation [Xu 2022]. Therefore, we conclude that the decrease in placental leptin concentration in obese and even more pronounced in GDM patients is a placental compensatory mechanism to maintain serum leptin levels.
GDM and obesity are dysfunction of the leptin signaling pathways. Leptin appears to be a relevant key hormone that regulates placental transport, and this regulation is altered in pathophysiological conditions such as gestational diabetes and /or obesity. Adaptations in the placental capacity to transport glucose may underlie both under- or overgrowth of the fetus when maternal nutrient and hormone levels are altered due to changes in maternal obesity or metabolic disease. [Gaudix 2023]Leptin can induce phosphorylation of VEGF receptor [Lim PQ 2023] . VEGF results presented the vasculogenesis is damaged in our study. This placental depression may contribute to abnormal placental function and vascular complications, exacerbating both conditions. The effect of obesity is the same as GDM in placental vasculogenesis. Leptin concentration had correlation with VEGF value. In GDM the VEGF depression was 50 percent and Leptin concentration fall down with 64 percent compare to the normal placental tissue value. In obesity the VEGF depression was 53 percent and leptin concentration fall down with 54 percent compare to the normal placental tissue value in our study.
A decreased concentration of Vascular Endothelial Growth Factor (VEGF) in the placenta can have significant implications for pregnancy and fetal development. VEGF is a critical regulator of angiogenesis, the process by which new blood vessels form, and is essential for ensuring adequate blood supply to the developing fetus [Xu 2022].
Key implications of reduced VEGF levels in the placenta include:
- Impaired Angiogenesis: VEGF is crucial for the development of the placental vascular network. A reduction in VEGF can lead to insufficient blood vessel formation, resulting in inadequate blood flow to the placenta. This can compromise the delivery of oxygen and nutrients to the fetus, potentially leading to fetal growth restriction or intrauterine growth retardation (IUGR).
- Placental Dysfunction: Lower VEGF levels may indicate placental insufficiency, where the placenta cannot adequately support the growing fetus. This condition can increase the risk of pregnancy complications such as preeclampsia, a disorder characterized by high blood pressure and damage to organ systems, which can be life-threatening for both the mother and the baby. Maternal inflammation in obesity and GDM may not always be associated with fetal inflammation. We propose that the placenta ‘senses’ and adapts to the maternal inflammatory environment, and plays a central role as both a target and producer of inflammatory mediators.[Patham 2015]
- Hypoxia: Reduced angiogenesis and blood flow can cause a hypoxic environment in the placenta, where there is insufficient oxygen. This can further complicate fetal development and increase the risk of adverse pregnancy outcomes, including preterm birth or stillbirth.
- Potential Long-term Effects: Insufficient placental VEGF and the resulting poor placental function can also have long-term health consequences for the child, potentially predisposing them to cardiovascular and metabolic diseases later in life.
The decreased VEGF concentration in the placenta is a critical marker that can indicate underlying issues with placental function and fetal development, necessitating careful monitoring.[Xu 2022, Pantham 2016]
DNA methylation, one of the most common epigenetic modifications, has received considerable attention in last years [Xu P2022]. DNA methylation assays in the placental tissue samples represented elevation both in GDM and obesity. In our study the DNA methylation were significantly higher in GDM, than in obesity. In Gestational Diabetes Mellitus (GDM), the increase in DNA methylation compared to obesity may be due to the unique metabolic and hormonal changes that occur during pregnancy. These changes can influence gene expression differently than in obesity alone. GDM-specific factors, such as altered insulin and glucose levels, hormonal fluctuations, and inflammation, can lead to distinct epigenetic modifications. These modifications can affect genes involved in glucose metabolism, inflammation, and placental function, resulting in more pronounced DNA methylation changes in GDM compared to obesity, which primarily involves chronic metabolic stress. [Xu P 2022]. The placenta in maternal obesity and GDM may represent an adaptation, which could contribute to limit exposure of the fetus to inflammation and oxidative stress. The placental DNA methylation is moderalty higher in GDM compare to obesity in our study. The influence of DNA methylation of leptin, adipokin, insulin molecules and pathway-related genes on gene expression is also closely related to the pathogenesis of GDM.[Xu P 2022]
Systematic follow-up programmes would be ideal to prevent the progression of GDM to diabetes, but unfortunately in most countries such programmes are lacking in routine clinical practice. This study shows possible alternatives for early screening and follow-up in cases of GDM and obesity. If not managed properly, GDM and obesity can lead to complications for both the mother and the baby. For the mother, it can increase the risk of developing high blood pressure and preeclampsia. For the baby, it can lead to excessive birth weight (macrosomia), premature birth, respiratory distress syndrome, and an increased risk of fetal malforamation ( e.g. fetal heart defects) and developing obesity and/or type 2 diabetes later in life.
Limitation of the study was the small sample in study groups. Recruitment was difficult because obesity is a common underlying condition of GDM. It was considered important not to examine cases where obesity was associated with GDM. This allowed us to separate the effects of GDM and obesity as much as possible. Altough the number of GDM with normal BMI is still much lower than in cases with obesity. GDM without obesity is becoming more common, due to bad eating habits [Zehravi 2021]. The ideal dietary habit enjoy three meals a day, while some of us prefer to eat almost continuously throughout the day.
During pregnancy, especially if managing gestational diabetes mellitus (GDM), it is generally recommended to eat small, balanced meals and snacks throughout the day to help maintain stable blood glucose levels. A typical recommendation is: enjoy three meals a day and 2-3 little snacks. This results in eating around 5 to 6 times a day. The goal is to avoid large fluctuations in blood sugar levels, which can occur with irregular eating patterns or large meals. Smaller, more frequent meals can help in managing blood sugar levels effectively.
Monitoring GDM during pregnancy is crucial to manage blood sugar levels and ensure the health of both the mother and the baby. The key components of GDM monitoring is frequent monitoring of blood glucose levels helps to maintain them within a target range and prevent complications. Maintaining a balanced diet with controlled portions of carbohydrates. To monitor the baby's growth and detect any potential complications by ultrasound. Occasionally, to check long-term blood sugar control by HbA1c-test. The HbA1c-test is a useful tool in managing diabetes outside of pregnancy, there are several disadvantages to using the HbA1c test during pregnancy, particularly for diagnosing or monitoring gestational diabetes mellitus (GDM). HbA1c is not sensitive to short-term fluctuations in blood glucose, which are important to monitor in pregnancy to ensure tight glucose control and prevent complications [Stewing 2021] . Pregnant women have increased red blood cell turnover, which can lower HbA1c levels regardless of glucose levels. The increased blood volume during pregnancy can dilute red blood cells, potentially affecting HbA1c values [Nader Rifai:Tiezt 2022]. The HbA1c test reflects average blood glucose over a longer period (2-3 months), which may not capture recent changes in glucose levels, especially if GDM develops later in third trimester of pregnancy. The HbA1c test may not be sensitive enough to detect mild hyperglycemia or to differentiate between normal glucose tolerance and GDM [Nader Rifai:Tiezt 2022]. This can lead to missed diagnoses or a false sense of security if HbA1c levels appear normal while postprandial glucose levels are elevated. There is no universally accepted HbA1c cutoff for diagnosing gestational diabetes. The diagnostic thresholds used for type 2 diabetes do not directly translate to GDM, making it difficult to interpret results in a pregnancy-specific context. HbA1c levels can be influenced by factors such as ethnicity, genetic hemoglobin variants, and certain medical conditions (e.g., anemia, hemoglobinopathies). These factors can further complicate the interpretation of HbA1c results during pregnancy. [Stewing 2021, Culliney 2018].
The underlying pathogenic mechanisms behind the abnormal metabolic risk profile in offspring are unknown, but epigenetic changes induced by exposure to maternal hyperglycaemia during fetal life are implicated. Obesity during pregnancy is a significant risk factor for developing hyperglycemia, which can lead to gestational diabetes mellitus (GDM) or exacerbate pre-existing diabetes. Neither diet, physical activity, nor a combination of both offered significant benefit in preventing GDM in overweight/obese women [Lim 2023] , despite that these measures were all remarkably beneficial for gestational weight gain restriction .
This condition, characterized by elevated blood sugar levels by insulin resistance, increased insulin demand. Adipose tissue, especially in excess, can produce inflammatory cytokines and hormones like leptin and adiponectin, which can interfere with insulin action. This inflammation can exacerbate insulin resistance and contribute to hyperglycemia [Musa 2023 ].
The insulin-blood glucose balance varies from week to week in gestation and a quick response is the key to few complications. To do this, we are researching new biomarkers such as leptin, adipokin, VEGF expression and DNA metilation. Implementing new strategies to modulate placental transport may improve maternal health and prove effective in normalizing placental and fetal growth.
The identification of specific changes in the placenta can help in the development of diagnostic and therapeutic approaches to improve prenatal outcomes, with particularly significant benefits. Concerning prevention in the offspring, our knowledge is still too limited to recommend specific programmes.
Conclusions
GDM and obesity are multifactorial conditions influenced by a variety of biochemical and molecular factors, including apelin, VEGF, leptin, and DNA methylation.
This is the first complex clinical trial in which these biomarkers have been tested in parallel in placental tissue and sonographic features of placenta. A major strength of the study is that it very clearly examined obese and GDM cases in separate groups. It also defined control groups for each marker of placental concentrations at near term gestational age. These biofactors are not only crucial for understanding the pathophysiology of these conditions but also offer potential targets for therapeutic intervention. This study emphasized the importance of exploring the utility of adiposity measures (weight gain during gestation) in predicting the risk of GDM during pregnancy beyond BMI alon at first medical visit.
Continued research into the roles and interactions of these molecules will be essential for developing effective treatments and preventive strategies for GDM in obesity, ultimately improving maternal and fetal health outcomes.
Author Contributions
Kata Kemeny and Balint Kolcsár collected and prepared the human samples, clinical data and participated in the experiments. Zoltan Kozinszky prepared the data analyses and statistical investigation, write the masnuscipt. Andrea Suranyi prepared the ultrasound investigations, Eszter Ducza and Andrea Surányi supervised and organized the whole study and manuscript writing.
Funding
This work was supported by the National Research, Development and Innovation Office, Hungary (grant NKFI-FK19-132499) and "Geza Hetenyi" Grant, University of Szeged [No.:5S 724 (A202)] and by the «Azonosító1»«Azonosító2» New National Excellence Program of the Ministry for Culture and Innovation from the source of the National Research, Development and Innovation Fund.
Conflicts of Interest
“The authors declare no conflicts of interest.”.
Abbreviations
GDM gestational diabetes mellitus; VEGF vascular endothelial growth factor
References
- Ahima RS, Flier JS. Adipose tissue as an endocrine organ. Trends in endocrinology and metabolism: TEM 2000, 11, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Antushevich H, Wójcik M. Review: Apelin in disease. Clin Chim Acta 2018, 483, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Ballmer-Hofer, K. Vascular Endothelial Growth Factor, from Basic Research to Clinical Applications. Int J Mol Sci. 2018, 19, 3750. [Google Scholar] [CrossRef] [PubMed]
- Bolatai A, He Y, Wu. Vascular endothelial growth factor and its receptors regulation in gestational diabetes mellitus and eclampsia. J Transl Med. 2022, 20, 400. [Google Scholar] [CrossRef] [PubMed]
- Catalano PM, Huston L, Amini SB. Longitudinal changes in glucose metabolism during pregnancy in obese women with normal glucose tolerance and gestational diabetes mellitus. Am J Obstet Gynecol. 1999, 180, 903–914. [Google Scholar] [CrossRef]
- Chomzynski, P. Single-Step Method of RNA Isolation by Acid Guanidinium Thiocyanate–Phenol–Chloroform Extraction. Analytical Biochemistry 1987, 162, 156–159. [Google Scholar] [CrossRef] [PubMed]
- Cildir G, Akincilar SC, Tergaonkar V. Chronic adipose tissue inflammation: all immune cells on the stage. Trends in molecular medicine 2013, 19, 487–500. [Google Scholar] [CrossRef]
- Culliney K, McCowan LME, Okesene-Gafa K; HUMBA Study Group. Accuracy of point-of-care HbA1c testing in pregnant women. Aust N Z J Obstet Gynaecol. 2018, 58, 643–647. [Google Scholar] [CrossRef] [PubMed]
- Damm P, Houshmand-Oeregaard A, Kelstrup L. Gestational diabetes mellitus and long-term consequences for mother and offspring: a view from Denmark. Diabetologia 2016, 59, 1396–1399. [Google Scholar] [CrossRef] [PubMed]
- Dłuski DF, Ruszała M, Rudziński G. Evolution of Gestational Diabetes Mellitus across Continents in 21st Century. Int J Environ Res Public Health. 2022, 19, 15804. [Google Scholar] [CrossRef] [PubMed]
- Elizabeth, C.W. Gregory, M.P.H., and Danielle M. Ely, Ph.D: Trends and Characteristics in Gestational Diabetes, 2016–2020. National vital statistics reports 2022, 71. Available online: https:// cdc.gov/nhcs/data/nvsr/nvsr71/nvsr71-03.
- Fraser A, Lawlor DA. Long-term health outcomes in offspring born to women with diabetes in pregnancy. Curr Diab Rep 2014, 14, 489. [Google Scholar] [CrossRef]
- Gregor MF, Hotamisligil GS. Inflammatory mechanisms in obesity. Annual review of immunology. 2011, 29, 415–445. [Google Scholar] [CrossRef] [PubMed]
- Guadix P, Corrales I, Vilariño-García T. Expression of nutrient transporters in placentas affected by gestational diabetes: role of leptin. Front Endocrinol (Lausanne). 2023, 14, 1172831. [Google Scholar] [CrossRef] [PubMed]
- Heikkinen A, Bollepalli S, Ollikainen M. The potential of DNA methylation as a biomarker for obesity and smoking. J Intern Med. 2022, 292, 390–408. [Google Scholar] [CrossRef] [PubMed]
- Horvath S, Raj K. DNA methylation-based biomarkers and the epigenetic clock theory of ageing. Nat Rev Genet. 2018, 19, 371–384. [Google Scholar] [CrossRef] [PubMed]
- Law PP, Holland ML. DNA methylation at the crossroads of gene and environment interactions. Essays Biochem. 2019, 63, 717–726. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lim PQ, Lai YJ, Ling PY. Cellular and molecular overview of gestational diabetes mellitus: Is it predictable and preventable? World J Diabetes. 2023, 14, 1693–1709. [Google Scholar] [CrossRef] [PubMed]
- Lim PQ, Lai YJ, Ling PY. Cellular and molecular overview of gestational diabetes mellitus: Is it predictable and preventable? World J Diabetes 2023, 14, 1693–1709. [Google Scholar] [CrossRef]
- Moore LD, Le T, Fan G. DNA methylation and its basic function. Neuropsychopharmacology 2013, 38, 23–38. [Google Scholar] [CrossRef] [PubMed]
- Mor G, Cardenas I, Abrahams V. Inflammation and pregnancy: the role of the immune system at the implantation site. Ann Ny Acad Sci. 2011, 1221, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Musa E, Salazar-Petres E, Arowolo A. Obesity and gestational diabetes independently and collectively induce specific effects on placental structure, inflammation and endocrine function in a cohort of South African women. J Physiol 2023, 601, 1287–1306. [Google Scholar] [CrossRef]
- Musa E, Salazar-Petres E, Vatish M. Kisspeptin signalling and its correlation with placental ultrastructure and clinical outcomes in pregnant South African women with obesity and gestational diabetes. Placenta 2024, 154, 49–59. [Google Scholar] [CrossRef] [PubMed]
- Nader Rifai: Tietz Textbook of Laboratory Medicine, Elsevire 7th Edition, 2022. Section V Genetic Metabolic Disorders p.p886-889.
- Obradovic M, Sudar-Milovanovic E, Soskic S. Leptin and Obesity: Role and Clinical Implication. Front Endocrinol (Lausanne) 2021, 12, 585887. [Google Scholar] [CrossRef] [PubMed]
- Pantham P, Aye IL, Powell TL. Inflammation in maternal obesity and gestational diabetes mellitus. Placenta 2015, 36, 709–715. [Google Scholar] [CrossRef] [PubMed]
- Ruppert, Z., Neuperger; et al. Characterization of obesity-related diseases and inflammation using single cell immunophenotyping in two different diet-induced obesity models. Int J Obes 2024. [Google Scholar] [CrossRef] [PubMed]
- Stiewig M, Jackson DN, Howard DL. Does serum hemoglobin A1C during early pregnancy predict performance on the 1-hour glucose challenge test? J Matern Fetal Neonatal Med. 2021, 34, 1174–1176. [Google Scholar] [CrossRef] [PubMed]
- Surányi A, Kozinszky Z, Molnár A. Placental volume relative to fetal weight estimated by sonography in diabetic pregnancies. J Matern Fetal Neonatal Med. 2016, 29, 1229–1232. [Google Scholar] [CrossRef]
- Tsakiridis I, Giouleka S, Mamopoulos A. Diagnosis and Management of Gestational Diabetes Mellitus: An Overview of National and International Guidelines. Obstet Gynecol Surv. 2021, 76, 367–381. [Google Scholar] [CrossRef] [PubMed]
- Visolyi GÁ, Kun A, Szalai O. Pregnancy outcomes of women with untreated 'mild' gestational diabetes (gestational diabetes by the WHO 2013 but not by the WHO-1999 diagnostic criteria) - A population-based cohort study. Diabetes Res Clin Pract. 2023, 203, 110874. [Google Scholar] [CrossRef] [PubMed]
- Wang H, Li N, Chivese T; IDF Diabetes Atlas Committee Hyperglycaemia in Pregnancy Special Interest Group. IDF Diabetes Atlas: Estimation of Global and Regional Gestational Diabetes Mellitus Prevalence for 2021 by International Association of Diabetes in Pregnancy Study Group's Criteria. Diabetes Res Clin Pract. 2022, 183, 109050. [Google Scholar] [CrossRef] [PubMed]
- WHO report: Obesity and overwight 2024. https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.
- Xu P, Dong S, Wu L. Maternal and Placental DNA Methylation Changes Associated with the Pathogenesis of Gestational Diabetes Mellitus. Nutrients 2022, 15, 70. [Google Scholar] [CrossRef] [PubMed]
- Zehravi M, Maqbool M, Ara I. Correlation between obesity, gestational diabetes mellitus, and pregnancy outcomes: an overview. Int J Adolesc Med Health 2021, 33, 339–345. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Placenta volumetry in 3D mode. The multiplanar technique was applied and after the entire volume was scanned, the 3 orthogonal ultrasonographic sections were analyzed. The longest view of the placenta on the ‘A’ plane (green A on image) of the 3 orthogonal ultrasonographic sections was chosen as the reference image.
Figure 1.
Placenta volumetry in 3D mode. The multiplanar technique was applied and after the entire volume was scanned, the 3 orthogonal ultrasonographic sections were analyzed. The longest view of the placenta on the ‘A’ plane (green A on image) of the 3 orthogonal ultrasonographic sections was chosen as the reference image.
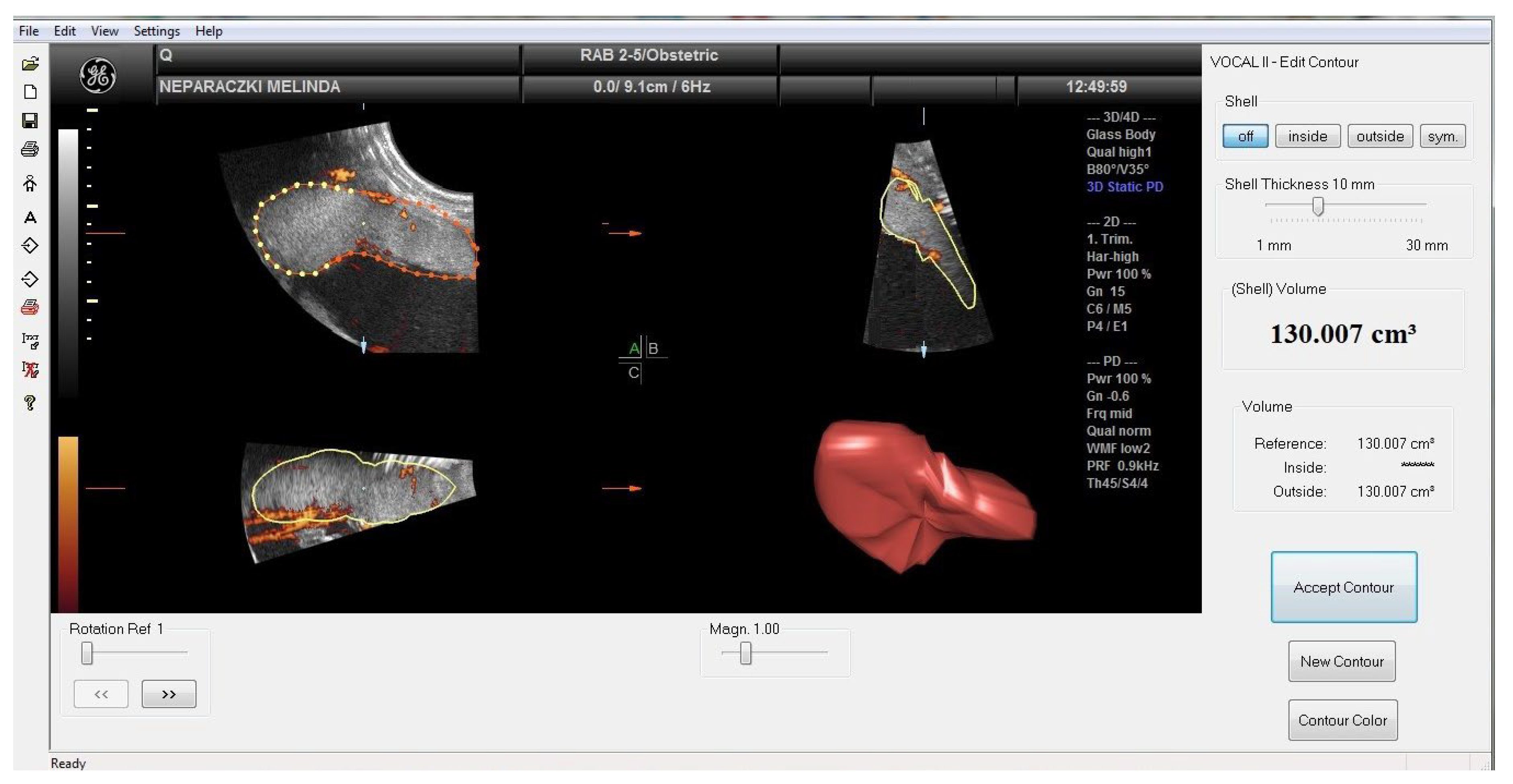
Figure 2.
Placental vessel by 3DPD mode. 3DPD allows visualization of small vessels with a relatively low velocity blood flow (in the green box).
Figure 2.
Placental vessel by 3DPD mode. 3DPD allows visualization of small vessels with a relatively low velocity blood flow (in the green box).
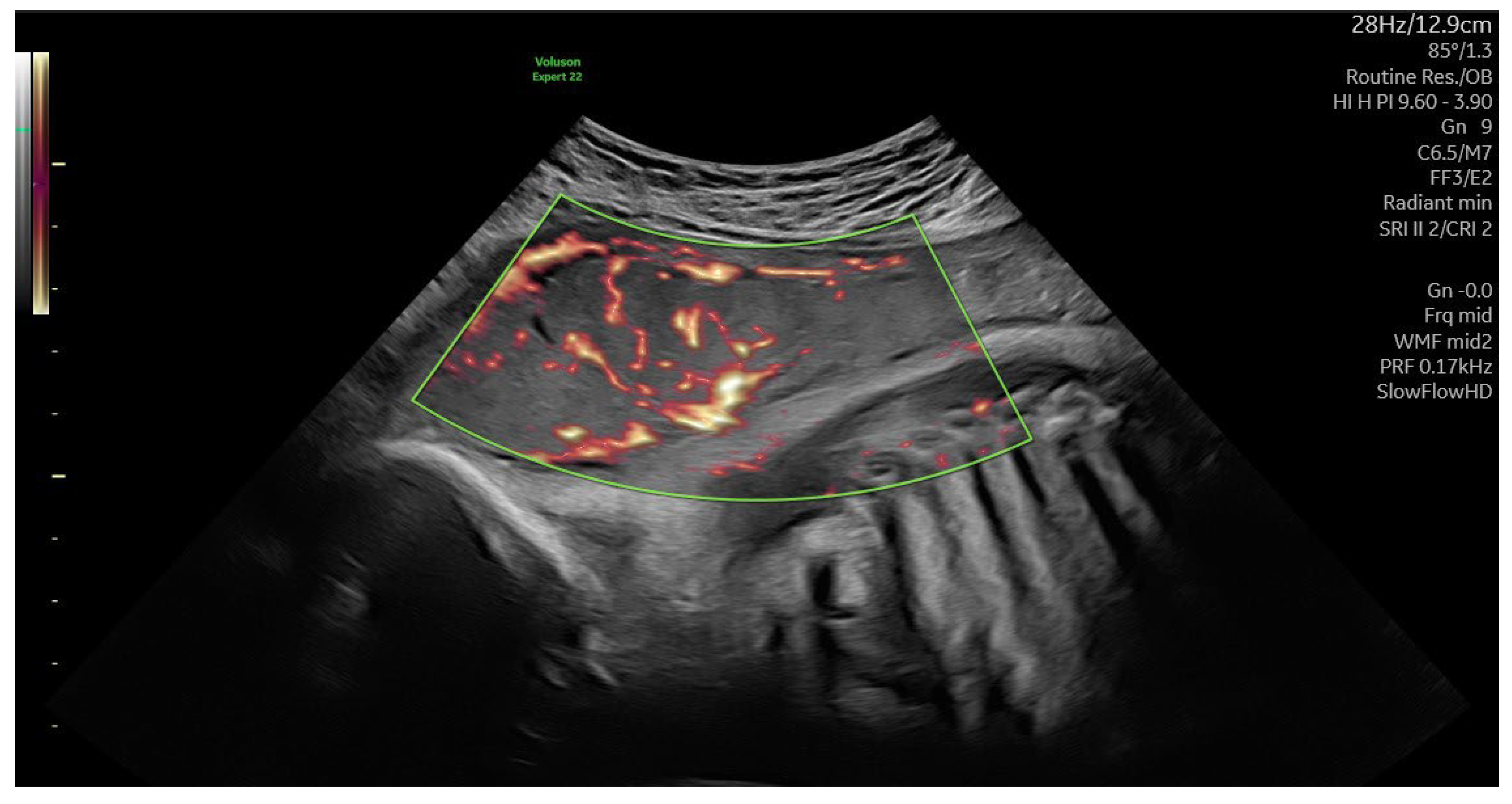
Figure 3.
Changes in the APLNR mRNA expression in the placental tissue samples collected from obese, GDM (gestational diabetes mellitus) and control women; ns: p>0.05; *: p<0.05 compared to the control.
Figure 3.
Changes in the APLNR mRNA expression in the placental tissue samples collected from obese, GDM (gestational diabetes mellitus) and control women; ns: p>0.05; *: p<0.05 compared to the control.
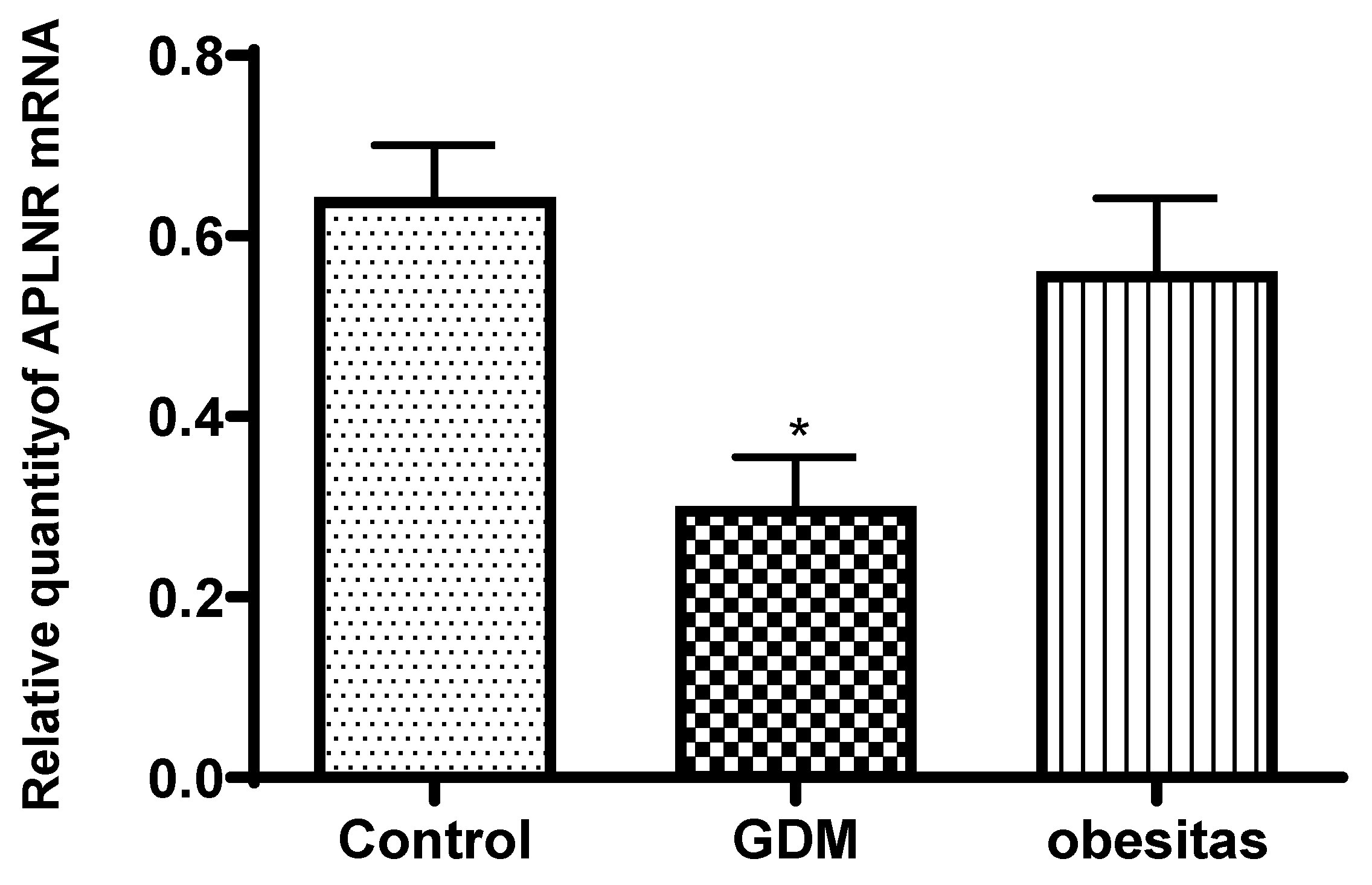
Figure 4.
Changes in the VEGF concentration (ng/ml) in the placental tissues collected from obese, GDM (gestational diabetes mellitus) and control women; *: p<0.05 compared to the control.
Figure 4.
Changes in the VEGF concentration (ng/ml) in the placental tissues collected from obese, GDM (gestational diabetes mellitus) and control women; *: p<0.05 compared to the control.
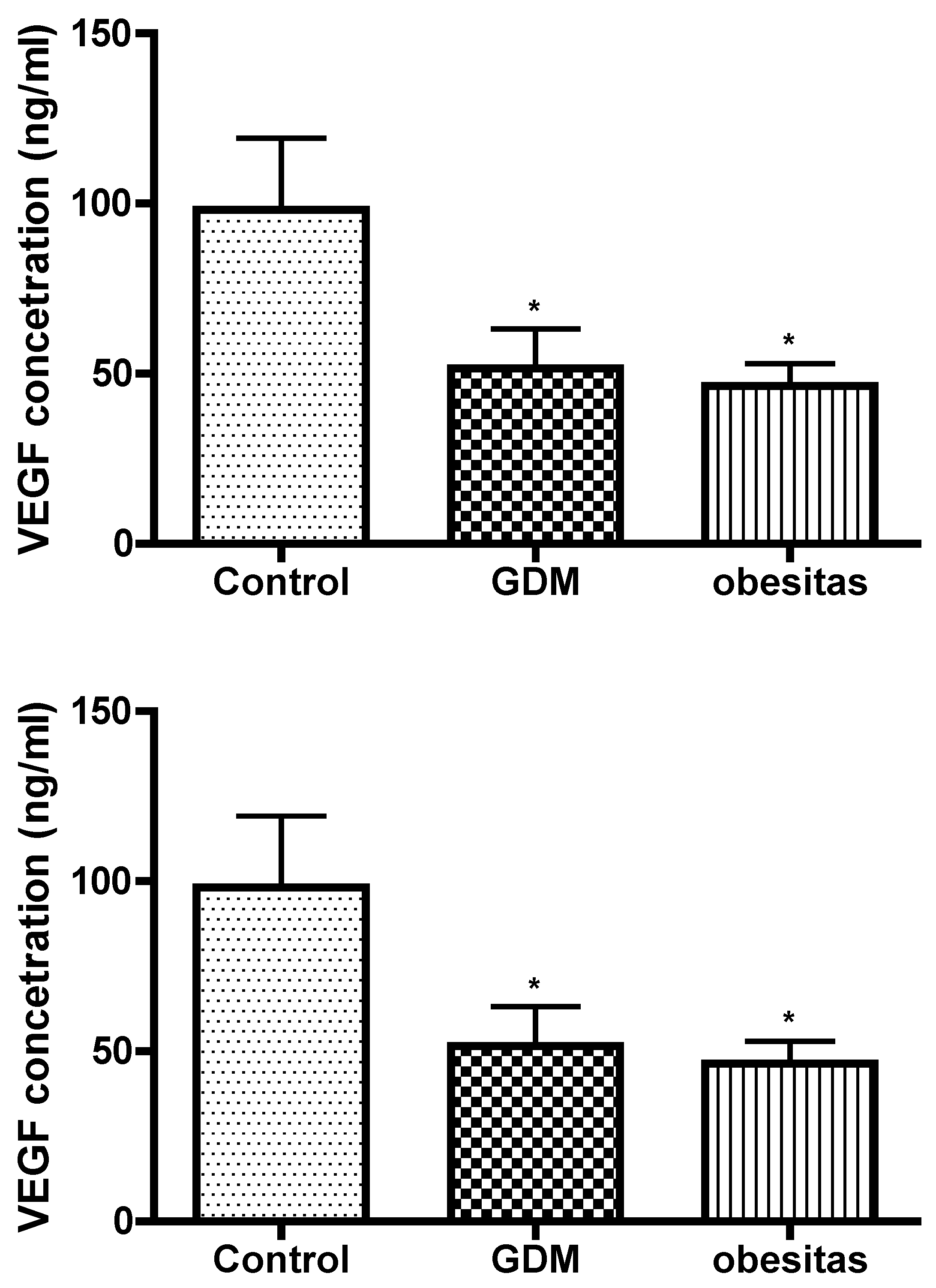
Figure 5.
Changes in the leptin concentration (ng/ml) in the placental tissue samples collected from obese, GDM and control women; ns: p>0.05; *: p<0.05 compared to the control.
Figure 5.
Changes in the leptin concentration (ng/ml) in the placental tissue samples collected from obese, GDM and control women; ns: p>0.05; *: p<0.05 compared to the control.
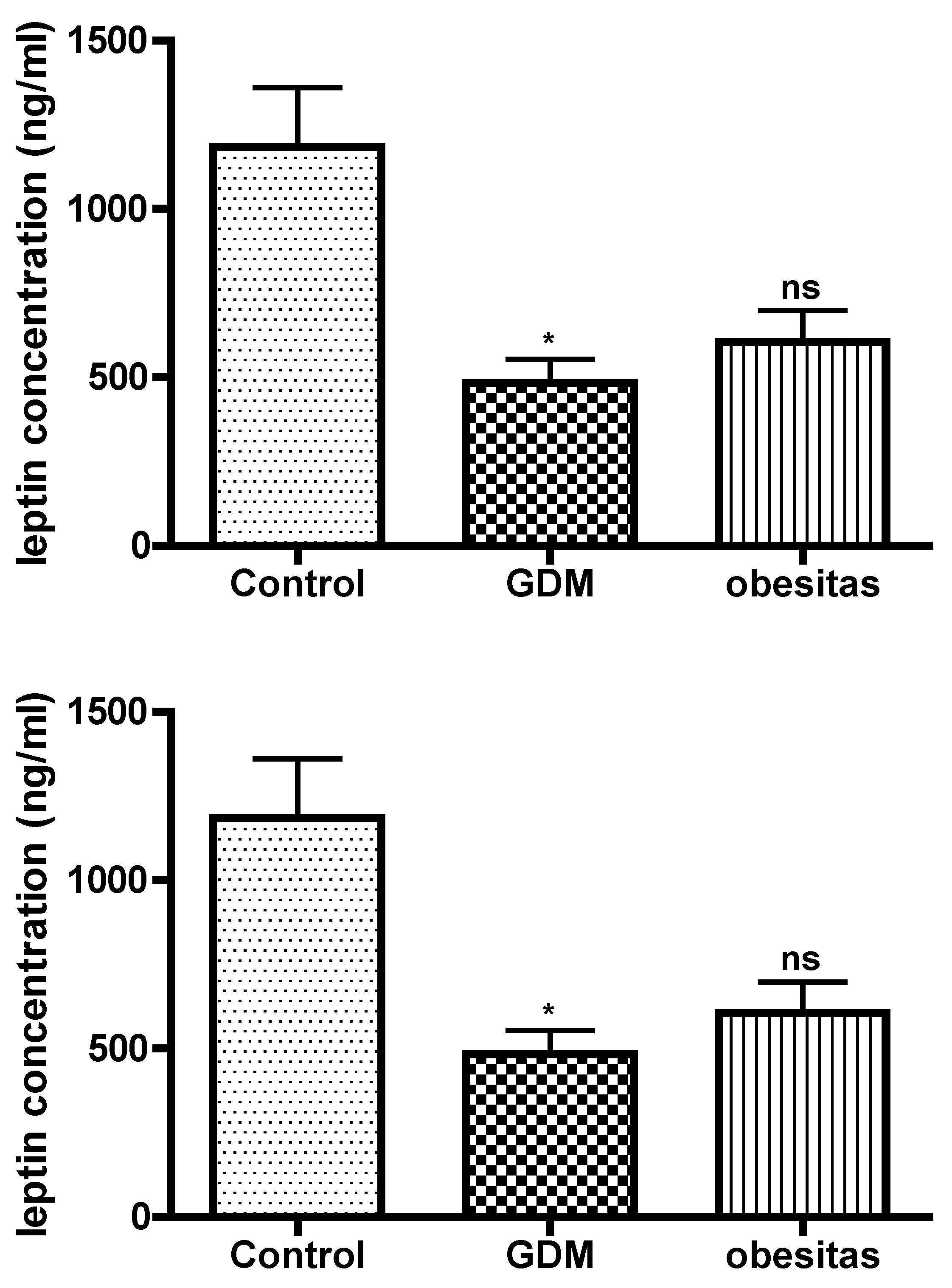
Figure 6.
Results of DNA methylation assays in the placental tissue samples collected from obese, GDM and control women; ns: p>0.05; ** p<0.01 compared to the control.
Figure 6.
Results of DNA methylation assays in the placental tissue samples collected from obese, GDM and control women; ns: p>0.05; ** p<0.01 compared to the control.
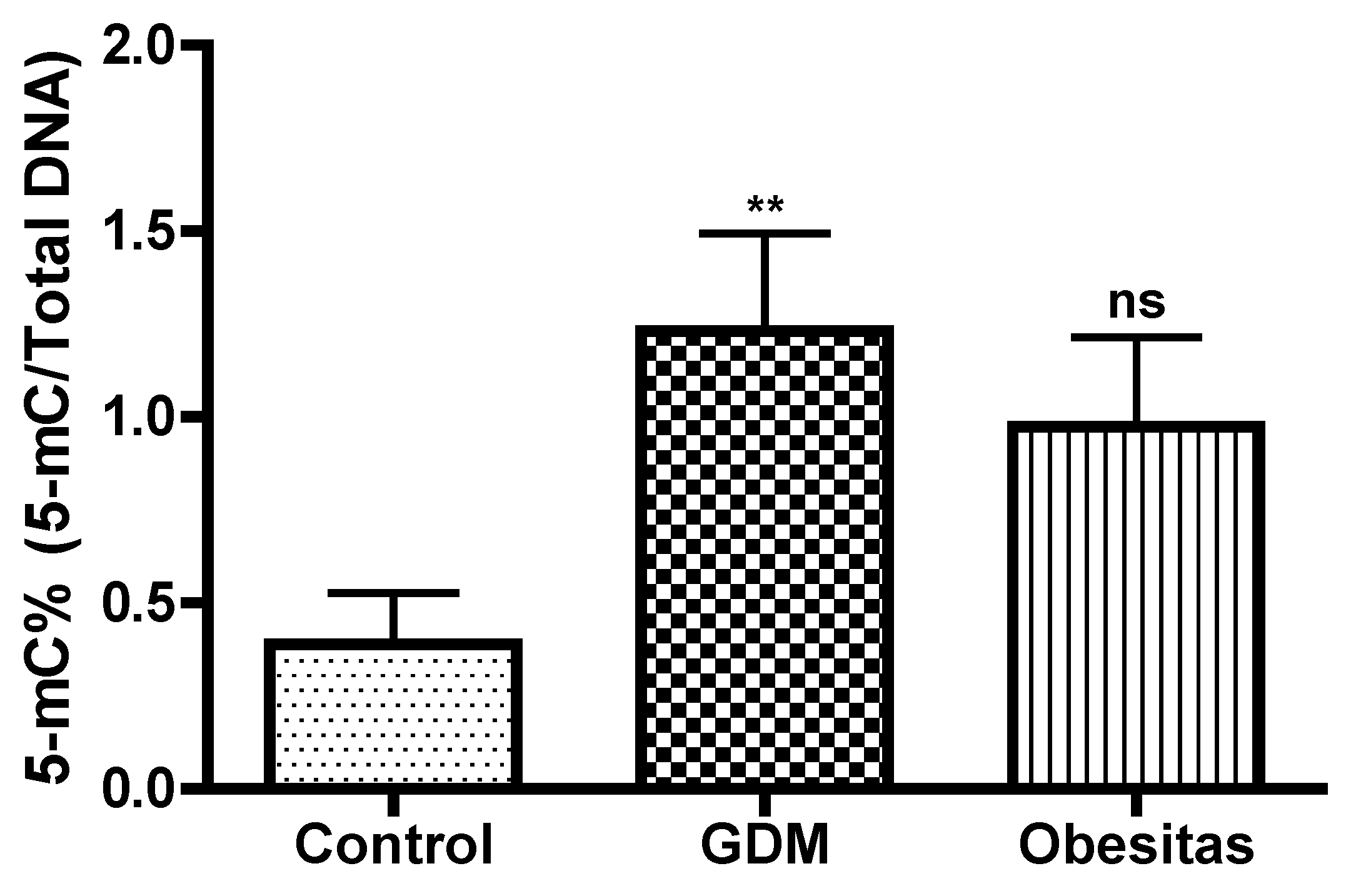

Table 1.
Maternal data.*: p<0.05; ns: p>0.05, compared to pregnant women with normal BMI.
| Pregnancy | Maternal age[mean± SD] | Gestation age[mean ±SD] |
|---|---|---|
| Normal BMI (N=30) | 26.6 ± 4 | 40.5 ± 0.84 |
| BMI>30 kg/m2 (N=12) | 29.5 ± 2.4ns | 39.5 ± 2.1 ns |
| GDM (N=6) | 35.6 ± 3.2 * | 36.9 ± 1.36* |
Table 2.
The results of placental sonography. *: p<0.05, ns: p>0.05, compared to pregnant women with normal BMI.
Table 2.
The results of placental sonography. *: p<0.05, ns: p>0.05, compared to pregnant women with normal BMI.
| Placental sonography | Normal BMI (N=30) | BMI>30 kg/m2 (N=12) | GDM (N=6) |
|---|---|---|---|
| Placental volume (ml ± SD) | 527.3 ± 93.1 | 775.6 ± 143.2 * | 754.6 ± 155.3 * |
| VI (mean ± SD) | 14.11 ± 5.1 | 8.71 ± 2.4* | 7.67 ± 3.3* |
| FI (mean ± SD) | 44.97 ± 22.64 | 37.4 ± 10.9 * | 39.4 ± 14.1 * |
| VFI (mean ± SD) | 8.21 ± 3.63 | 4.74 ± 1.34* | 3.99 ± 2.67* |
VI: vascularisation index, FI: flow index, and VFI: vascularization flow index.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



