
Submitted:
09 September 2024
Posted:
10 September 2024
You are already at the latest version
Abstract
Ingestion of corrosive agents is a well-known cause of extensive and severe gastrointestinal tract injury. Acids can result in significant acute complications throughout the gastrointestinal system. Herein, we present a case of total gastrointestinal necrosis after a patient ingested a large amount of concentrated hydrochloric acid. Of note, the patient developed an intestinal fistula six days following ingestion, requiring surgical intervention. This case underscores the potential for delayed gastrointestinal necrosis with high-volume and concentrated hydrochloric acid ingestion. Early CT evaluationto and multi-organ protectionis are crucial for such patients. For patients with no signs of perforation, multidisciplinary physicians should comprehensively evaluate the necessity of surgical exploration. In such cases, comprehensive treatment strategies can significantly improve outcomes. The purpose of this case report is to highlight the complexities and challenges in managing severe hydrochloric acid ingestion, to discuss the multidisciplinary approach required for such cases, and to contribute to the existing literature by providing detailed insights into the clinical presentation, treatment, and outcomes of a rare and severe instance of concentrated HCl ingestion.
Keywords:
hydrochloric acid
; gastrointestinal tract necrosis
; caustic injury
; multiple organ dysfunction
1. Introduction
Hydrochloric acid (HCl) is a chemical that often causes swallowing injuries, 2% of which result in strictures. In the United States, as many as 5,000 cases of caustic substance ingestion are reported annually, with hydrochloric acid being one of the substances involved [1]. Injuries from these ingestions predominantly affect young children, with an incidence rate of about 80%, while the remaining cases typically involve adults who attempt suicide [2,3]. HCl is also naturally present in gastric acid, aiding in protein denaturation, protecting against microorganisms, and activating pepsin [4,5]. Accidental or deliberate intake of concentrated HCl is known to cause a range of clinical symptoms, including severe damage to the upper gastrointestinal tract and the tracheobronchial system, necessitating immediate and specialized treatment. Herein, we report a case of gastric necrosis in a patient who ingested 100 ml of HCl. We employed a multidisciplinary approach to manage this patient, combining surgery, gastroenterology, imaging, and critical care medicine. Unfortunately, the patient succumbed to his extensive injuries after a 21-day hospital stay. HCl ingestion, although relatively rare, remains a critical medical emergency due to its high morbidity and mortality rates. The severity of symptoms is influenced by the concentration and volume of the acid ingested, with outcomes ranging from mild gastrointestinal discomfort to life-threatening perforations and multi-organ failure. Fatalities from HCl poisoning have decreased with advancements in medical care, but the potential for severe complications necessitates immediate and specialized treatment. This case report documents an extreme instance of HCl ingestion, offering valuable insights into the clinical progression and management of such a severe case.
2. Case Description
A healthy 35-year-old male patient attempted suicide by ingesting 100 ml of detergent solution. The patient presented to a local hospital with nausea, vomiting, and bloody vomitus. Eleven hours later, he was transferred to the intensive care unit (ICU) of Guangzhou 12th People’s Hospital for further treatment. A bedside esophagogastroduodenoscopy (EGD) was performed in the ED, revealing Zargar grade 3B esophagitis and active bleeding from the duodenum (Figure 1). Vital signs and physical examination revealed no apparent abnormalities or abdominal tenderness. The original bottle of detergent was sent for analysis, and after being diluted 100 times, the pH test indicated a value of 2, confirming that the substance was a powerful acid. Several blood test results were elevated (Table 1), particularly lipase (4250.0 U/L), α-amylase (1315.0 U/L), creatine kinase (260 U/L and 312 U/L), creatine kinase MB isoenzyme (47.1 U/L), lactate dehydrogenase (1445 U/L), AST (345.2 U/L), and ALT (499.1 U/L) (Figure 2). Computed tomography (CT) at admission revealed a mildly enlarged pancreatic head (Figure 3A). The patient was subsequently treated with continuous venovenous hemodiafiltration (CVVHDF), continuous renal replacement therapy (CRRT), hepatoprotective medication, and trypsin inhibitors. On the fifth day, follow-up abdominal CT indicated acute pancreatitis, characterized by thickening and edema of the intestinal wall in the mid-abdomen, moderate ascites, and perirenal exudative changes (Figure 3B). On the sixth day, abdominal CT scans showed the development of an intestinal fistula, acute pancreatitis, and increased peritoneal effusion (Figure 3C). On the seventh day, an exploratory laparotomy under general anesthesia was performed, revealing a significant amount of purulent and dark brown exudate in the abdominal cavity. Intraoperative findings revealed black necrosis involving the entire upper abdominal greater omentum, duodenum, and most of the upper jejunum, including portions of the mesentery. A postoperative CT indicated no apparent signs of contrast medium leakage in the small intestine and ascending colon (Figure 3D). Postoperative pathological examination confirmed extensive hemorrhage and necrosis of the stomach, duodenum, and parts of the jejunum, as shown in Figure 4. Following surgery, the patient was returned to the ward and received personalized fluid replacement and symptomatic supportive treatment. Subsequent auxiliary examination indices gradually stabilized. Nevertheless, the patient’s gastrointestinal tract did not recover, and he succumbed to abdominal bleeding after 21 days of critical care.
3. Discussion
Hydrochloric acid is a strong and corrosive acid solution commonly used in household chemical cleaners. It has been widely abused as a means of suicide and is one of the most frequently treated causes of chemical burns. Hydrochloric acid poisoning is characterized by corrosive damage to the digestive tract [6]. To prevent misdiagnosis, radiologists should have a thorough understanding of the essential characteristics during imaging. CT has become integral in assessing acute corrosive ingestion in adult patients [7]. Notably, thoracoabdominal CT is preferred over endoscopy [8] due to its lower risk of esophageal perforation and ability to evaluate esophageal injury and surrounding tissues [9,10]. Saito et al. suggested that all patients exposed to strong acids should undergo CT imaging to detect early signs of perforation [11]. In cases involving significant ingestion of concentrated acids, especially with those presenting with signs of perforation [12], immediate surgery is necessary, with patients exhibiting a survival rate of around 50%. Additionally, patients who ingest substantial amounts of strong acid should be monitored for pancreatic head changes [13]. Due to rapid deterioration in the patient’s clinical condition after admission, an abdominal CT examination on the sixth day revealed a small intestinal fistula, acute pancreatitis, and ascites. Subsequently, the patient underwent surgery on the seventh day after admission. In a previous case report involving the ingestion of 20 ml of concentrated HCl, no imaging signs of perforation were initially observed [14]. Nonetheless, the patient underwent a partial esophagectomy and a total gastrectomy, resulting in a favorable outcome. Another published case described the initial absence of imaging signs of perforation following 150 ml of concentrated hydrochloric acid ingestion. However, total gastrectomy and partial esophagectomy were performed after free intra-abdominal gas was detected on imaging [15]. This highlights the potential benefit of delayed “on-demand” surgical intervention for patients. Masaya et al. reported that abdominal CT performed 3 to 6 hours after ingestion of a corrosive substance is superior to endoscopy for detecting permeability defects in the digestive tract [16]. Furlano found that, given the extent of the esophageal injury observed during endoscopy, the patient was not a candidate for esophagectomy and ultimately died despite aggressive medical management [17]. When determining whether patients with hydrochloric acid ingestion require surgery, relying solely on endoscopy is insufficient. Early and frequent CT is necessary to prevent secondary intestinal fistulas.
Oral ingestion of HCl often leads to complex and critical conditions, with rapid changes during treatment. Management of oral ingestion acidosis necessitates careful attention to organ protection and treatment[18].In the present case, hepatorenal failure and myocardial damage were noted, possibly due to direct corrosion from extravasation. However, there are currently no standardized treatment protocols for corrosive injuries, although clinical data typically support the use of prophylactic antibiotic therapy and parenteral nutrition [19,20]. Comprehensive diagnostic approaches and treatment strategies are essential to mitigate complications [21,22]. Patients with one or more systemic complications face a high mortality rate (45%), including conditions such as renal insufficiency, liver dysfunction, and disseminated intravascular coagulation [23].In this case, we used CRRT, liver protection, heart protection, inhibition of pancreatic enzyme secretion and other methods to protect the patient’s organs. Dalus et al. reported a 100% mortality rate among patients with perforation complicated by hypotension, high acid intake, hematemesis, metabolic acidosis, and acute respiratory distress syndrome [24]. These studies highlight renal insufficiency, liver dysfunction, and hematemesis as significant risk factors associated with a poor prognosis. Our case highlights that secondary small intestinal fistula caused by oral hydrochloric acid is one of the adverse prognostic factors. This case raises awareness of serious considerations when treating oral hydrochloric acid poisoning combined with multi-organ dysfunctionin.
4. Conclusions
In summary, we described the treatment of a patient who ingested a large amount of concentrated HCl. Early CT evaluationto and multi-organ protectionis are crucial for such patients. Meanwhile, for patients showing no signs of perforation, the timing of extensive radiological assessment and surgical intervention should be individually determined in close collaboration with ICU physicians, radiologists, and surgeons.
Author Contributions
XXZ and YCC conceptualized and wrote the draft in consultation with ZW; ZJO collected and collated the data; RCZ analyzed and visualized the data. All authors reviewed and approved the final manuscript.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
The patient provided written permission that their data might be presented anonymously for research and training purposes.
Data Availability Statement
Data are contained within the article.
Acknowledgments
This work was approved by the ethics committee institution of Guangzhou Twelfth People’s Hospital, and consent was obtained from the patient’s family.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Obarski, P.; Włodarczyk, J. Diagnosis and Management of Gastrointestinal Chemical Burns and Post-Burn Oesophageal Stenosis. Kardiochir Torakochirurgia Pol 2021, 18, 252–259. [Google Scholar] [CrossRef]
- Arnold; Marion; Alp Numanoglu. Caustic Ingestion in Children—a Review. Seminars in Pediatric Surgery 2017, 26, 95–104. [Google Scholar] [CrossRef]
- Sari; Desi Rahmah; Ismi Dian Meiliana; Sakti, D. ; Kinasih, S.; Kurniasari, H.; Rejeki, P.S. Hyperbaric Oxygen Therapy as an Adjuvant Treatment in Hydrochloric Acid Poisoning: A Literature Review. Biomorphology J. 2023, 33, 52–58. [Google Scholar]
- Schröder, W.; Brunner, S.; Bruns, C.J. Caustic Ingestion of the Upper Gastrointestinal Tract. Chirurg 2022, 93, 202–203. [Google Scholar] [CrossRef]
- Oliva, S.; Romano, C.; De Angelis, P.; Isoldi, S.; Mantegazza, C.; Felici, E.; Dabizzi, E.; Fava, G.; Renzo, S.; Strisciuglio, C.; et al. Foreign body and caustic ingestions in children: A clinical practice guideline. Dig. Liver Dis. 2020, 52, 1266–1281. [Google Scholar] [CrossRef]
- Dilawari, J.B.; Singh, S.; Rao, P.N.; Anand, B.S. Corrosive acid ingestion in man - a clinical and endoscopic study. Gut 1984, 25, 183–187. [Google Scholar] [CrossRef]
- Gill, M.; Tee, D.; Chinnaratha, M.A. Caustic Ingestion: Has the Role of the Gastroenterologist Burnt Out? Emerg Med Australas 2019, 31, 479–482. [Google Scholar] [CrossRef]
- Agarwal, A.; Srivastava, D.N.; Madhusudhan, K.S. Corrosive injury of the upper gastrointestinal tract: the evolving role of a radiologist. Br. J. Radiol. 2020, 93. [Google Scholar] [CrossRef]
- Kaewlai, R.; Noppakunsomboon, N.; Tongsai, S.; Tamrakar, B.; Kumthong, N.; Teerasamit, W.; Kongkaewpaisan, N.; Pisanuwongse, A.; Amornsitthiwat, R.; Maitriwong, W.; et al. Performance of computed tomography and its reliability for the diagnosis of transmural gastrointestional necrosis in a setting of acute ingestion of predominantly strong acid substances in adults. Clin. Toxicol. 2023, 61, 346–354. [Google Scholar] [CrossRef]
- Cutaia, G.; Messina, M.; Rubino, S.; Reitano, E.; Salvaggio, L.; Costanza, I.; Agnello, F.; La Grutta, L.; Midiri, M.; Salvaggio, G.; et al. Caustic ingestion: CT findings of esophageal injuries and thoracic complications. Emerg. Radiol. 2021, 28, 845–856. [Google Scholar] [CrossRef]
- Saito, K.; Goto, F.; Sekine, M.; Yamamoto, H.; Kaneda, S.; Sakai, A.; Ebisumoto, K.; Maki, D.; Iijima, H.; Yamauchi, M.; et al. Computed Tomography to Diagnose Paranasal Sinus Chemical Burns and Tissue Damage: A Case Report. Laryngoscope 2021, 131, E2490–E2493. [Google Scholar] [CrossRef]
- Gupta, V.; Shah, J.; Yadav, T.D.; Kumar, P.; Wig, J.D.; Kochhar, R. Emergency surgical intervention in acute corrosive ingestion: single-center experience from India. ANZ J. Surg. 2023, 93, 2864–2869. [Google Scholar] [CrossRef]
- Rasbach, E.; Schölch, S.; Reissfelder, C.; Rahbari, N.N. Successful treatment of gastric necrosis after ingestion of hydrochloric acid: a two-stage minimally invasive surgical procedure. BMJ Case Rep. 2019, 12, e231879. [Google Scholar] [CrossRef]
- Wijeratne, T.; Ratnatunga, C.; Dharrmapala, A.; Samarasinghe, T.; University of Sri Jayewardenepura; LK About T Department of Surgery; Faculty of Medical Sciences X close T Wijeratne; Peradeniya, T. H.; Ratnatunga, L.A.T.S.U.X.C.C.; LK About C Department of Surgery; et al. Corrosive acid injury of the stomach. Ceylon Med J. 2015, 60, 25. [Google Scholar] [CrossRef]
- Frank, D.B.; Fumanti, B.J.; Grossman, M.D.; Mendez, A. Suicidal ingestion of household bleach resulting in total gastrectomy. Clin. Toxicol. 2019, 58, 300–301. [Google Scholar] [CrossRef]
- Ushio, M. A case of early gastric necrosis due to ingestion of an acidic toilet cleaner. Clin. Case Rep. 2023, 11, e7481. [Google Scholar] [CrossRef]
- Furlano, E.R.; Wu, G.P.; Vosburgh, B.; Waldman, C.R.; Noonan, J.; Bracey, A. Man Presenting After Hydrochloric Acid Ingestion. Clin. Pr. Cases Emerg. Med. 2023, 8, 77–79. [Google Scholar] [CrossRef]
- Kumar, C.B.; Chowdhury, S.D.; Ghatak, S.K.; Sreekar, D.; Kurien, R.T.; David, D.; Dutta, A.K.; Simon, E.G.; Joseph, A.J. Immediate and long-term outcome of corrosive ingestion. Indian J. Gastroenterol. 2019, 38, 356–361. [Google Scholar] [CrossRef]
- Chirica, M.; Bonavina, L.; Kelly, M.D.; Sarfati, E.; Cattan, P. Caustic Ingestion. Lancet 2017, 389, 2041–2052. [Google Scholar] [CrossRef]
- Hoffman, R.S.; Burns, M.M.; Gosselin, S. Ingestion of Caustic Substances. New Engl. J. Med. 2020, 382, 1739–1748. [Google Scholar] [CrossRef]
- Singh, H.; Dhibar, D.P.; Naidu, G.S.R.S.N.K. Life-threatening corrosive injury with hepato-renal-pulmonary failure in boric acid poisoning. Postgrad. Med J. 2020, 98, 70–71. [Google Scholar] [CrossRef]
- Picciariello, A.; Papagni, V.; Martines, G.; Palasciano, N.; Altomare, D. The management of esophago-gastric necrosis due to caustics ingestion: Anastomotic reinforcement with Cyanoacrylate glue and damage control with Vacuum Assisted Closure Therapy—A case report. Int. J. Surg. Case Rep. 2019, 60, 327–330. [Google Scholar] [CrossRef]
- Huscher, C.G.; Mingoli, A.; Mereu, A.; Sgarzini, G. Laparoscopy can be Very Effective in Reducing Mortality Rate for Caustic Ingestion in Suicide Attempt. World J. Surg. 2011, 35, 2363–2364. [Google Scholar] [CrossRef]
- Yeh, I.J.; Liu, K.T. St Segment Elevation Associated with Hydrochloric Acid Ingestion: A Case Report. Medicine (Baltimore) 2017, 96, e8819. [Google Scholar] [CrossRef]
Figure 1.
Endoscopy performed within the first 24 hours after HCl intake. A: view of the proximal esophagus showing diffuse thickening and edema, with narrowed lumen from caustic esophagitis. B: view of the duodenum, with hematin and caustic injury.
Figure 1.
Endoscopy performed within the first 24 hours after HCl intake. A: view of the proximal esophagus showing diffuse thickening and edema, with narrowed lumen from caustic esophagitis. B: view of the duodenum, with hematin and caustic injury.
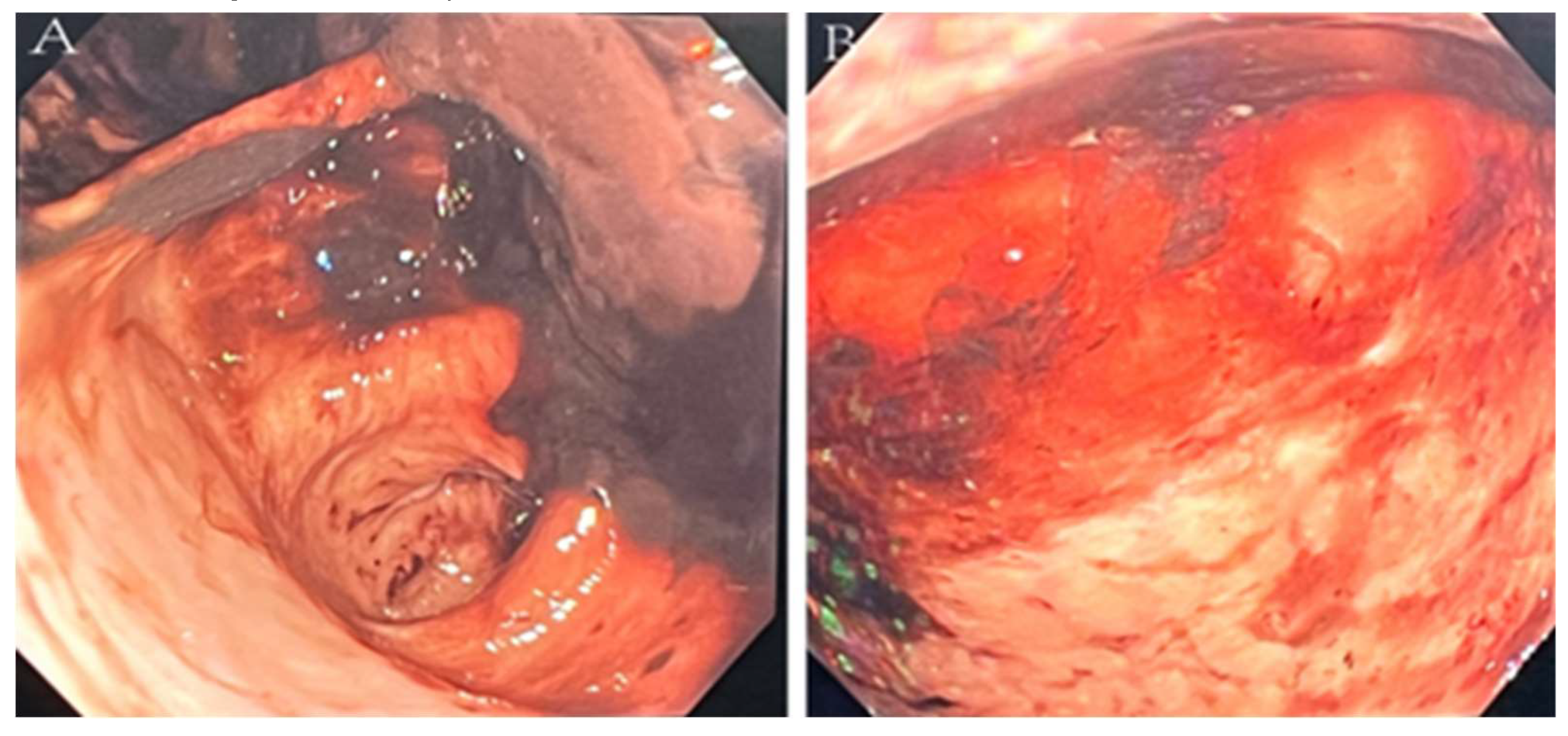
Figure 2.
Changes in the patient’s main laboratory test results following admission.
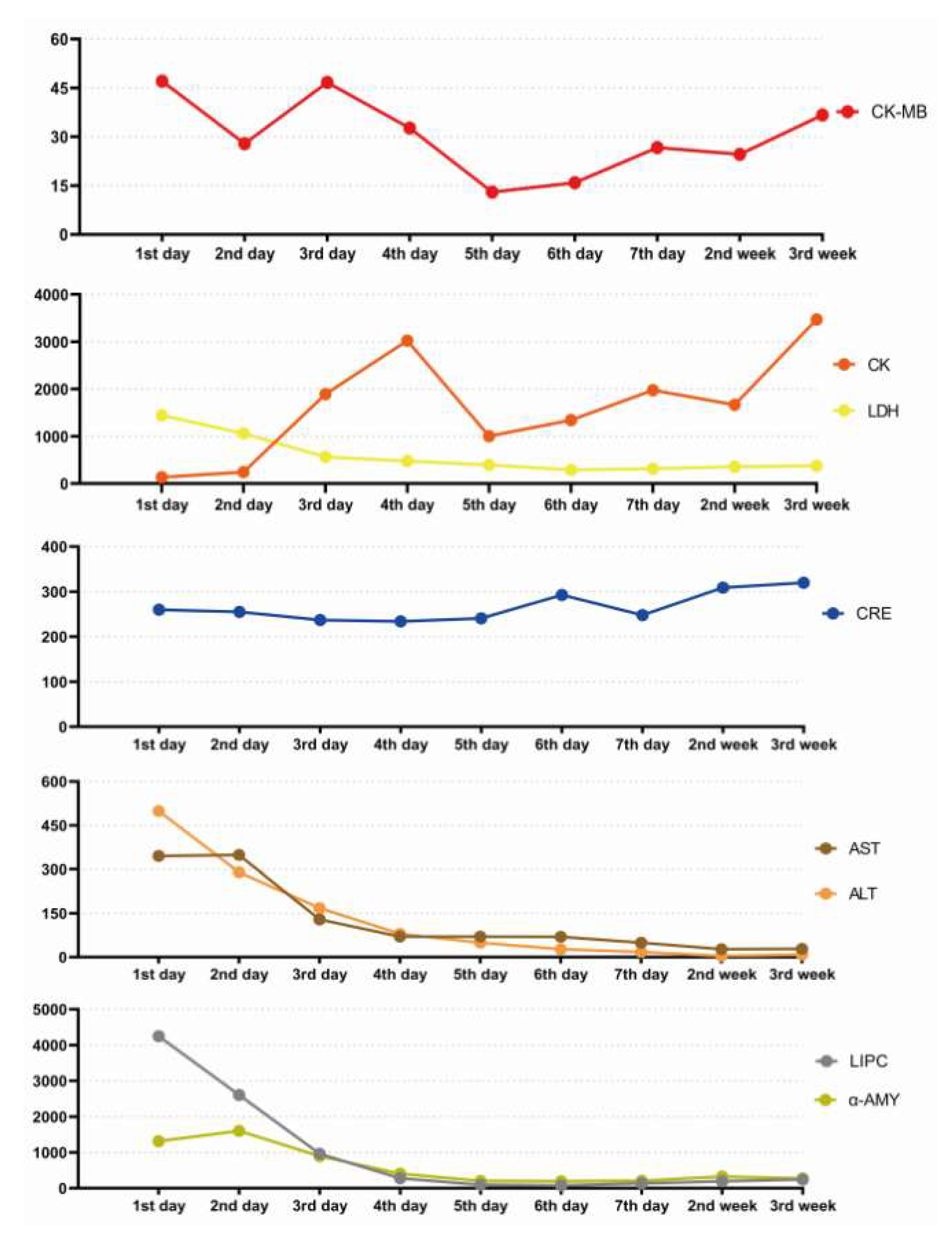
Figure 3.
Longitudinal abdominal computed tomography images. A. Admission CT indicated a slightly enlarged head of the pancreas. B. On the 5th day, abdominal CT revealed acute pancreatitis, with thickening and swelling of the intestinal wall of the middle abdomen. Moderate effusion in the abdominal cavity and perirenal lesions. C. On the 6th day, abdominal CT identified a small intestinal fistula, acute pancreatitis and peritoneal effusion. D. Postoperative CT showed no obvious signs of contrast medium leakage in the small intestine and ascending colon.
Figure 3.
Longitudinal abdominal computed tomography images. A. Admission CT indicated a slightly enlarged head of the pancreas. B. On the 5th day, abdominal CT revealed acute pancreatitis, with thickening and swelling of the intestinal wall of the middle abdomen. Moderate effusion in the abdominal cavity and perirenal lesions. C. On the 6th day, abdominal CT identified a small intestinal fistula, acute pancreatitis and peritoneal effusion. D. Postoperative CT showed no obvious signs of contrast medium leakage in the small intestine and ascending colon.
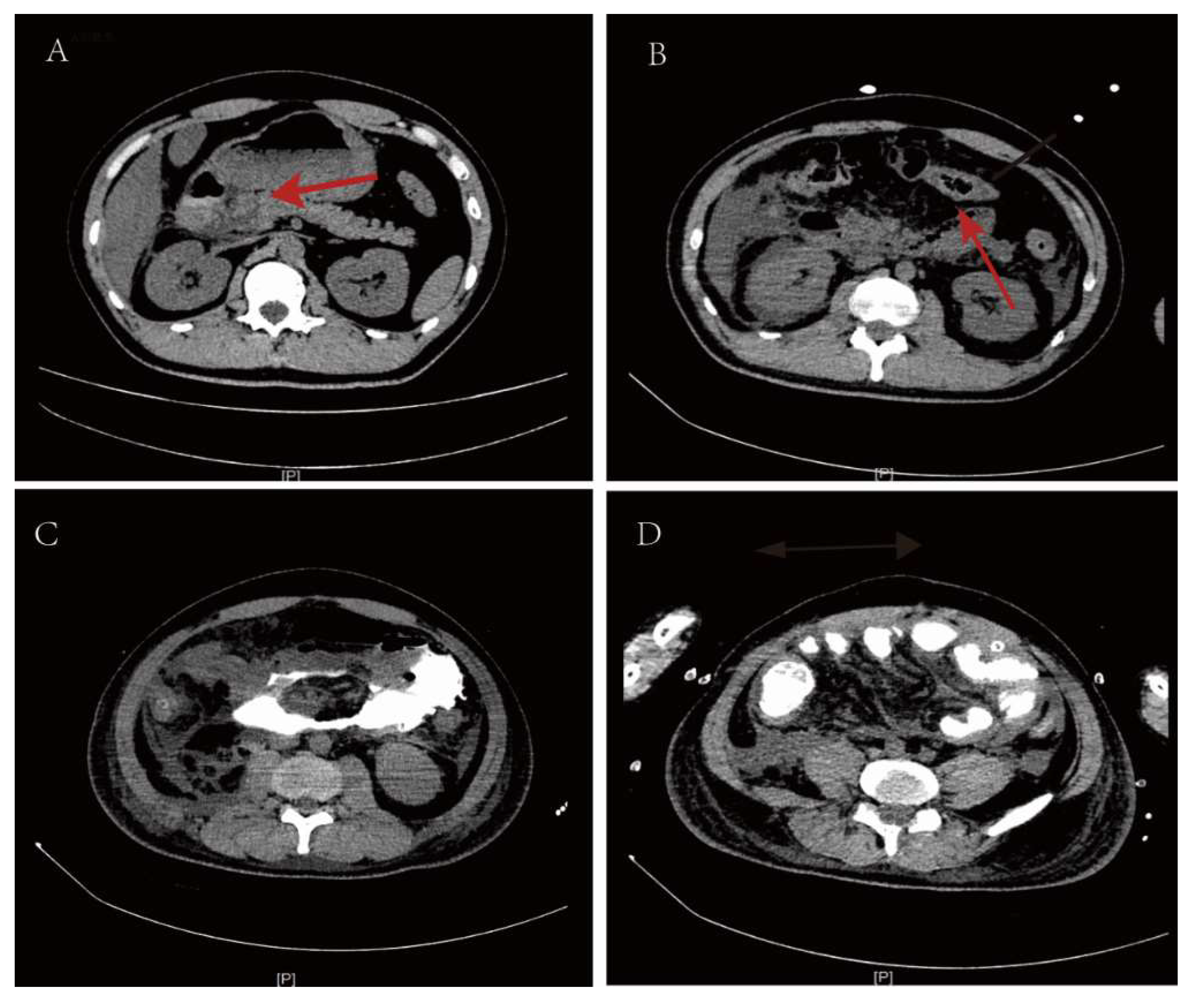
Figure 4.
Gastroduodenal bleeding and necrosis found during pathological analysis. A. Intraoperative view of showing the complete necrotic intestine. B. Pathological section diagram of necrotic intestinal fracture.
Figure 4.
Gastroduodenal bleeding and necrosis found during pathological analysis. A. Intraoperative view of showing the complete necrotic intestine. B. Pathological section diagram of necrotic intestinal fracture.
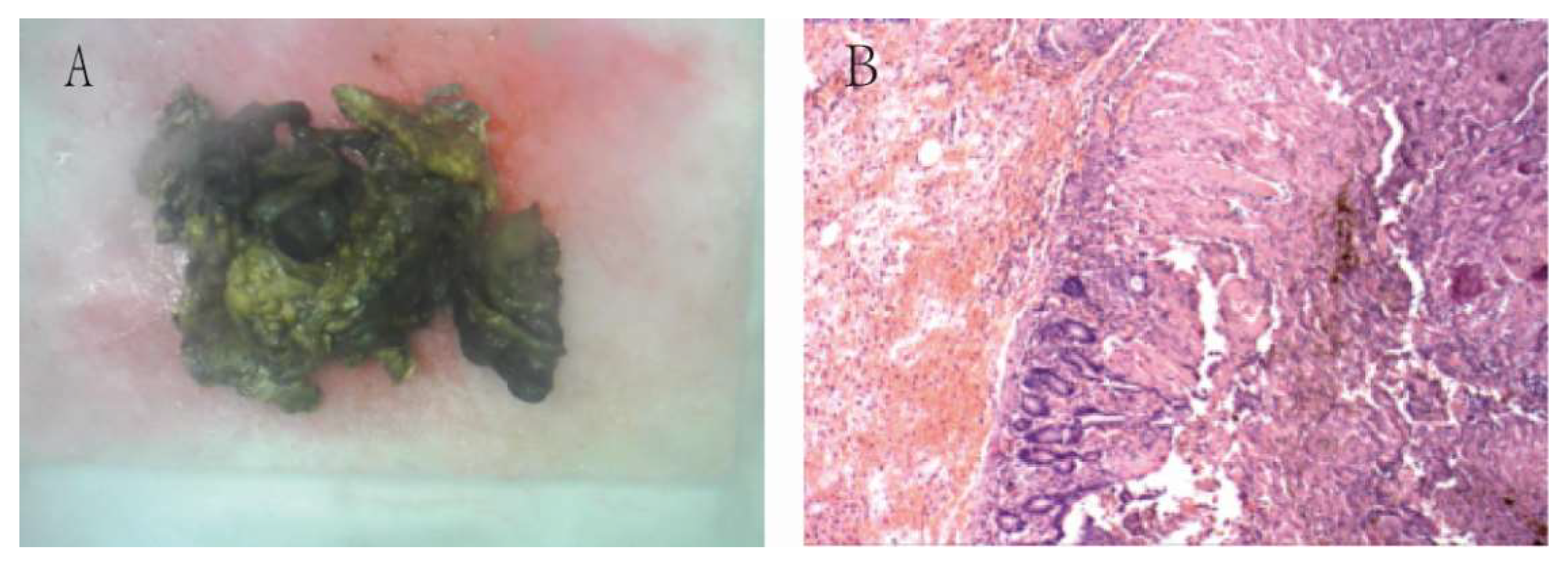

Table 1.
Changes in the patient’s laboratory findings following admission.
| Index | Normal range | 1st day | 2nd day | 3rd day | 4th day | 5th day | 6th day | 7th day | 2nd week | 3rd week |
|---|---|---|---|---|---|---|---|---|---|---|
| WBC | 5-12×109 | 24.69 | 10.22 | 7.77 | 6.17 | 6.20 | 10.1 | 13.61 | 12.5 | 27.86 |
| NEUT% | 40-75% | 90.6 | 87.3 | 85.8 | 89.3 | 81.1 | 88.9 | 90.2 | 84.6 | 77.2 |
| HGB | 105-145g/L | 143 | 118 | 101 | 75 | 65 | 64 | 65 | 52 | 20 |
| PLT | 140-440×109/L | 126 | 119 | 70 | 47 | 47 | 76 | 129 | 232 | 96 |
| CRE | 35-73μmol/L | 260 | 255 | 237 | 234 | 241 | 293 | 248 | 309 | 320 |
| CRP | 0-6mg/L | 61.45 | 220.80 | 330.36 | 383.12 | 361 | 193.03 | 139.82 | 218.3 | 255.09 |
| CK | 40-310u/L | 133 | 243 | 1894 | 3023 | 1004 | 1342 | 1975 | 1667 | 3472 |
| CK-MB | 0-25u/L | 47.1 | 27.9 | 46.7 | 32.7 | 13.0 | 15.9 | 26.7 | 24.6 | 36.7 |
| LDH | 120-250u/L | 1445 | 1062 | 563 | 476 | 393 | 290 | 313 | 355 | 374 |
| AST | 7-40u/L | 345.2 | 349.0 | 129.3 | 70.1 | 70.6 | 69.8 | 49.5 | 27.3 | 28.3 |
| ALT | 7-40u/L | 499.1 | 290.1 | 168 | 80.2 | 49.2 | 27.2 | 17.8 | 4.3 | 8.7 |
| LIPC | 1-63U/L | 4250.0 | 2608.2 | 961.6 | 280.1 | 94.7 | 78.9 | 135.3 | 194.6 | 245.5 |
| α-AMY | 20-90u/L | 1315.0 | 1604.1 | 898.2 | 409.1 | 206.1 | 195.4 | 208.9 | 328.2 | 273.1 |
WBC, white blood cell; NEU, neutrophil; HBG, hemoglobin; PLT, Platelets; CRE, creatinine; CRP, C-reactive protein; CK, creatine kinase; CK-MB, creatine kinase-MB; MB, myoglobin; LDH, lactate dehydrogenase; AST, aspartate aminotransferase; ALT, alanine aminotransferase; LIPC, hepatic lipase gene; α-AMY, α-amylase.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



