Submitted:
09 September 2024
Posted:
10 September 2024
You are already at the latest version
Abstract
Despite recent efforts by the government to combat Food Insecurity (FI), this issue remains a significant problem in Brazil, particularly among populations experiencing social vulnerability, such as Indigenous peoples. This study aimed to assess the prevalence and factors associated with FI in Indigenous families in the state of Alagoas. It was a population-based cross-sectional survey using a probabilistic sample (n=1270 families) representing the 11 ethnic groups present in the state. FI was defined according to the Brazilian Food Insecurity Scale. Factors associated with moderate and severe FI were determined through multivariable analysis using Poisson regression with robust variance adjustment (prevalence ratio – PR and 95% CI). The prevalence of FI was 69.1%, with 29.5% in moderate (23.2%) and severe (6.3%) forms. Factors associated (p<0.05) with moderate and severe FI included: female-headed households; houses made of mud or wood; with ≤4 rooms; head of the household with ≤8 years of schooling; retired or unemployed household head; and total family income <2 National Minimum Wages. The prevalence of FI among Alagoas Indigenous peoples is considerably high and associated with poorer demographic, socioeconomic, and environmental conditions, highlighting the social inequities they face and emphasizing the need for intersectoral public policies to address this scenario.
Keywords:
Food Insecurity
; malnutrition
; Indigenous Peoples
; Social Vulnerability
1. Introduction
Food insecurity (FI) represents a severe violation of the Human Right to Adequate Food, a condition guaranteed by the Federal Constitution of Brazil and various international treaties to which the country is a signatory. FI undermines the dignity and well-being of a significant portion of Brazilian families, particularly those in a state of social vulnerability. The lack of regular and permanent access to quality food in sufficient quantities perpetuates a cycle of poverty and exclusion, limiting social and economic development, exacerbating existing inequalities, and hindering the creation of a more just and equitable society [1,2].
FI is a multifactorial condition that affects traditional peoples and communities differently. For Indigenous peoples, the prevalence of FI is invariably higher compared to other population segments and is associated with greater social, economic, and demographic vulnerability [3,4]. Factors such as low educational attainment and changes in production methods, often imposed by territorial conflicts, further highlight the vulnerability of this population [3,4,5].
Indigenous peoples represent approximately 1.7 million individuals in Brazil. With an estimated population of 520,000 people, the Northeast region holds the second largest Indigenous population in the country, with approximately 25,000 of them residing specifically in the state of Alagoas [3].
The situation of FI among Brazilian Indigenous peoples has been little investigated, and there is even less research on the factors associated with this condition. The limited studies available reveal a concerning reality that reflects the social and economic inequalities faced by these peoples in Brazil [4]. The Brazilian Food Insecurity Scale (EBIA), the primary tool for assessing FI in families across the country, has also been used among Indigenous peoples, but it increasingly highlights the need for adaptations to suit the diverse realities of Brazil’s Indigenous populations [6].
The population of Alagoas has historically faced significant issues such as high illiteracy rates, low income, and inadequate public infrastructure. These conditions directly impact the fulfillment of essential rights such as food, basic sanitation, and access to healthcare. Moreover, the vast cultural diversity within the same territory, as seen in Alagoas, highlights the need for carefully designed and culturally appropriate policies to address the real needs of these communities [7].
Considering the historical social vulnerability of Indigenous peoples in Brazil, and specifically in Alagoas [7], and the lack of studies focused specifically on food insecurity and understanding the factors contributing to its prevalence, this study aimed to assess the prevalence and factors associated with food insecurity in Indigenous families in the state of Alagoas. The information produced may contribute to the planning, implementation, and evaluation of actions and public policies aimed at promoting Food and Nutrition Security and ensuring the Right to Adequate Food for these peoples.
2. Materials and Methods
2.1. Study Design, Population, and Sampling
This study is a cross-sectional, population-based survey derived from the Study on Nutrition, Health, and Food Security of Indigenous Peoples in the State of Alagoas (ENSSAIA). It assessed the 11 Indigenous ethnic groups present in Alagoas, distributed across 29 villages, most of which are located between the Agreste region and the Alto Sertão region of the state (Table 1).
To address the various objectives proposed in ENSSAIA, a sample prevalence of 50% was adopted in the sampling plan. This prevalence maximizes the sample size, providing sufficient power to assess any other outcome beyond food insecurity. The sample error calculation for this study was performed retrospectively: Considering a population of 8,575 families [3], an observed prevalence of 69.1%, a significance level of 5.0%, and a 95% confidence interval, the analyzed sample of 1,270 families is associated with a sample error of approximately 2.4%.
For the selection of the Indigenous communities included in the sample, all 11 ethnic groups in the state were represented. For the Aconã, Kariri-Xokó, Katokinn, and Wassú peoples, which have only one community, this community was selected with a probability of 1. For the other ethnic groups, simple random sampling was used to select one of their villages. However, if the selected village had a population exceeding 2,000 people, sectors within the coverage area of an Indigenous Health Agent were randomly selected to cover approximately one-third of the village's population. Conversely, if the selected village had fewer than 150 inhabitants, additional sectors from another village of the same ethnic group, and closer in proximity to the selected village, were included to reach at least one-third of the Indigenous population of the respective ethnic group.
All families residing in the selected communities were eligible for the study. Family identification was based on a registry provided by the local coordination of the Family Health Strategy, and data collection was conducted with the support and supervision of the responsible Indigenous Health Agent. The Family Health Strategy is the foundation of primary healthcare in Brazil. It utilizes multidisciplinary teams to provide continuous care to families in defined territories, with a focus on prevention and health promotion.
2.2. Data Collection
Data collection took place from September 2022 to December 2023 through home visits using structured forms, which were previously tested in a pilot study. The forms were developed electronically using the Epicollect5 app, version 4.0.0, installed on tablets with Android operating systems. At the end of each interview (or at the end of the morning/afternoon shift, depending on internet availability), the completed forms were uploaded, saved in the Google account linked to each tablet. Subsequently, the spreadsheets generated by the software were transferred to a computer for the creation of the research database.
Since the project aimed to include all Indigenous ethnic groups in the state, the pilot study was conducted in one of the communities (Cocal of the Wassú ethnicity), chosen for convenience (being closer to the municipality of Maceió, the capital of the state of Alagoas).
The field team consisted of 14 researchers. Considering the cultural particularities of the Indigenous peoples and to facilitate communication and participation, the team was supported by an Indigenous Health Agents, who was responsible for identifying households with registered Indigenous people in the Family Health Strategy. Additionally, an Indigenous collaborator from the village assisted the anthropometrist in transporting the equipment. Field activities were coordinated and supervised by a faculty member and a post-doctoral student with extensive experience in epidemiological surveys.
2.3. Variables and Data Collection Instruments
2.3.1. Dependent Variable
Food insecurity (FI) was defined according to the Brazilian Food Insecurity Scale (EBIA). The current version of the EBIA consists of a form with 14 closed-ended questions, with positive or negative responses regarding the family's food experience over the past three months. Based on the number of positive responses, the scale categorizes food insecurity from concerns about potential food shortages to experiencing a full day without eating [9].
Given the cultural specifics of the target population, a version of the EBIA adapted for the Terena Indigenous population was adopted [10].
Operationally, each affirmative response on the form represents 1 point. The classification of the scale is based on the total score, ranging from 0 to 14 points in households with individuals under 18 years old, and from 0 to 8 points in households without individuals in this age group (the last 6 questions pertain to individuals under 18).
2.3.2. Independent Variables
The independent variables related to demographic and socioeconomic conditions evaluated were: the head of household's gender (male; female); number of people in the household (≤ 4; > 4); head of household's education level in years of schooling (≤ 4; 5 to 8; ≥ 9); head of household's employment status (formal employment; informal employment; retired; unemployed); total family income in number of national minimum wages (0 to 1; > 1 to 2; > 2); and family participation in a direct income transfer social program, Bolsa Família Program - BFP (yes; no).
Regarding environmental conditions, the variables analyzed were: type of housing (masonry; mud/wood); total number of rooms (≤ 4; > 4); garbage destination (public collection; other); source of drinking water (adequate; inadequate); and waste disposal method (adequate; inadequate).
For the source of drinking water, "adequate" conditions were considered to be: public water supply network and mineral water; while sources such as cisterns, wells, small ponds, rivers, streams, springs, trucks, or other were classified as "inadequate." For waste disposal, "adequate" was classified as a septic tank or public sewage system, and "inadequate" was classified as a rudimentary pit, ditch, river, or other.
2.4. Data Processing and Analysis
The spreadsheets generated by the Epicollect5 software, version 4.0.0, were imported into Stata®, version 18.0, where the database was created (combine datasets) and all statistical analysis procedures were conducted. The database was initially checked for consistency, and when issues were identified, the information was reviewed to correct errors (e.g., typographical errors) or to exclude data when correction was not possible.
To enhance international comparability, the recommendations of the Food and Agriculture Organization of the United Nations (FAO) regarding food security (FS) assessment were adopted. The sum of moderate and severe food insecurity (MSFI) cases was considered as the outcome for analysis in identifying associated factors, thereby increasing the specificity of this indicator [11].
The unadjusted analysis was performed by comparing the prevalence of MSFI across different categories of independent variables (demographic, socioeconomic, and environmental). The chi-square test was used for this comparison. The measure of association was the prevalence ratio (PR) and its 95% confidence interval (CI), calculated using Poisson regression with robust variance adjustment, for both crude and adjusted analyses. Associations that showed significance at the unadjusted level of up to 20% (p<0.2) were subjected to multivariable analysis, following the hierarchical conceptual model adapted from Victora et al. [12] (Figure 1).
The hierarchical analysis began with the distal level, followed by the subsequent levels according to their proximity to the outcome of the investigation. For each analysis level, variables without statistical significance were successively eliminated using backward stepwise elimination, retaining only those with p<0.05. Therefore, all variables that showed p<0.05 at their respective level, even if they exceeded the significance level in the next level, were retained in the final model.
The ENSSAIA was approved by the National Research Ethics Commission (CONEP: 29121120.0.0000.5013), and all legal requirements related to ethical procedures for conducting research involving Indigenous peoples were observed [13,14,15]. All heads of households or eligible adults for the study, or those responsible for children or adolescents, were fully informed about the study's objectives, risks, benefits, and other details provided in the Informed Consent Form. Participation was only allowed for those who signed the consent form.
3. Results
A total of 1,296 families were assessed, with 26 (2.0%) excluded from the analysis due to incomplete data on the EBIA, resulting in a final sample of 1,270 families. Most of these families were headed by men (55.5%) and consisted of up to four members (75.6%). According to the EBIA, 69.1% of the families experienced some degree of FI, with 29.5% experiencing moderate (23.2%) and severe (6.3%) FI (Figure 2).
Regarding the hierarchical analysis (Table 2), the factors associated with MSFI at the distal level were: female-headed households (PR=1.38; 95% CI: 1.16-1.63), residing in houses made of mud or wood (PR=1.69; 95% CI: 1.25-2.28), and households with 4 or fewer rooms (PR=1.47; 95% CI: 1.18-1.84). At the intermediate level, factors included households headed by individuals with lower educational attainment: 5 to 8 years of schooling (PR=1.80; 95% CI: 1.38-2.34) and up to 4 years of schooling (PR=2.02; 95% CI: 1.61-2.53). Proximal variables independently associated with MSFI included households headed by retired (PR=1.73; 95% CI: 1.10-2.73) and unemployed individuals (PR=1.62; 95% CI: 1.03-2.54), as well as those with a total national family income equal to or less than two National Minimum Wage - NMW (≤ 1 NMW: PR=2.00; 95% CI: 1.44-2.76; >1 to 2 NMW: PR=1.69; 95% CI: 1.22-2.33). At the time of data collection, the NMW in Brazil was R$ 1,320.00, approximately $275.00 USD as of July 2023.
4. Discussion
Food insecurity is a concerning reality among Indigenous peoples in Alagoas and reflects the context of inequities in which their families are situated, underscoring the need for the development and implementation of effective cross-sectoral strategies to address the current situation. Most indigenous peoples in Alagoas are characterized by significant social vulnerability, a persistent struggle for land demarcation, and the preservation of their traditions, culture, and way of life [7]. These conflicts are part of the historical experience of these peoples and are associated with structural, demographic, socioeconomic, environmental, health, and educational challenges in their communities [16,17]. Given this context, the high prevalence of FI reported is not surprising, as living conditions in households can directly or indirectly affect FI status [18].
In the observed scenario, about 40% of families showed concern or uncertainty about regular access to food, indicating a mild form of FI. Regarding more severe forms of FI (moderate and severe), nearly 30% of families faced quantitative or qualitative restrictions in their food and nutritional needs. These restrictions suggest a real possibility of these families experiencing hunger [9].
The scarcity of data in the literature on FI among Brazilian indigenous peoples, especially concerning its associated factors, contributes to the invisibility of the issues faced, perpetuating disparities and inequities compared to the rest of society. Furthermore, this lack of knowledge hampers the implementation of actions aimed at improving the quality of life for this population [4].
The comparability of this study with results reported for other indigenous communities in the country is limited due to significant cultural differences related to the concept of food security for each group, particularly regarding food access methods such as agriculture, extraction, and financial access in local markets. Additionally, comparability is also affected by differences between studies, such as participant age and data collection timing, which are strongly influenced by political processes and established public health priorities.
Among the available studies similar to this one, a notable study was conducted in the state of Mato Grosso do Sul involving families from the Terena ethnic group, which identified moderate to severe food insecurity (MSFI) in 53.1% of households [10]. Another recently published study [4] involved indigenous families in Dourados, also in Mato Grosso do Sul, and found a total food insecurity prevalence of 64.1%%, similar to the prevalence observed in the present study. It is important to highlight that there is a significant time gap between the publication of the first study and the current one, and the second study employed a different tool for defining food insecurity, known as the Short Food Security Scale.
Worldwide, households headed by women and ethnic-racial minorities are at higher risk of food insecurity [19]. Although most indigenous households in Alagoas are headed by men, the situation of MSFI in female-headed households was comparatively higher (34.9% vs. 25.1%), maintaining a higher prevalence ratio at all levels in the hierarchical analysis. These results align with national and international data showing that, although most non-indigenous households are male-headed, MSFI is more prevalent in female-headed households [20,21,22].
In addition to gender and ethnic-racial differences, factors such as housing type, the disparity between the number of residents and rooms or living spaces, lower education of the head of the household, employment status, monthly family income, and rural versus urban housing locations have been associated with higher levels of household food insecurity in general populations. In this regard, the association between food insecurity and the factors presented in this study is consistent with what is observed in the general population, such as the association with housing quality observed in various studies [23,24,25].
Regarding the factors related to the environment where families live, this study points to concerning indicators of vulnerability, such as a large proportion of people without adequate access to drinking water, waste collection, and sanitation. In this context, Raupp et al. [26] confirmed the poor basic sanitation infrastructure of indigenous households in the country and reaffirmed inadequate sanitary conditions in indigenous homes in a comparative analysis between the 2000 and 2010 censuses, as well as the persistent significant racial and color inequalities in the country [25,26].
The education level of the household head proved to be an important factor for understanding associations with food insecurity, especially when this level is below 4 or up to 8 years of schooling. In this classification, the indigenous population of Alagoas shows that over 65% of household heads fall into this category, and this variable is independently associated with FI. Similar associations have also been confirmed in the non-indigenous population with comparable numbers [27,28]. Specifically, among indigenous populations, this association was also observed among the Terena, Ñandeva, and Kaiowá in Mato Grosso do Sul and the Kaingang in the Terra de Guarita in Rio Grande do Sul [4,29].
The association of MSFI with the absence of formal employment and lower total family income highlights the difficulties faced by this population. Bacarrin et al. [18] point out that, similar to the relationship between employment status and FI, inflation experienced by a country with high unemployment rates results in increased indicators related to FI.
In this context, and supporting the data on the income of the indigenous population in Alagoas, Brito et al. [30] found that an income below one minimum wage was associated with FI in a socially vulnerable community in São Luís, Maranhão [30]. As presented in our results, nearly 60% of the families were enrolled in the PBF, a group that was significantly more exposed to food insecurity compared to families not linked to the Program. This fact underscores the effective targeting of the PBF and its importance in addressing the vulnerability situation [31].
Studies show that lower family incomes directly impact the acquisition of food in terms of quantity and quality, raising concerns about families' access to food and compromising food security [23,28,30]. Similarly, lower educational levels can affect financial management, ensure adequate food intake, and, more importantly, the quality of food choices for the household [27,29]. Additionally, compromised access to quality water, coupled with inadequate sanitation and waste collection services, exacerbates the conditions of families already facing a history of social vulnerability and other determinants worsening their FI [25,26].
Due to factors such as the real increase in average worker income, the decline in the unemployment rate, and the reinstatement of effective social policies like the Bolsa Família Program, Brazil experienced a 40% reduction in the extreme poverty rate between 2022 and 2023 [32] This positively impacts purchasing power and food choices within families, establishing a favorable scenario for reducing the prevalence of food insecurity [18], However, it’s essential to recognize that socially vulnerable populations, such as Indigenous communities, Quilombolas, riverine groups, and other minority segments, still require significant attention to effectively address the persistent issue of food insecurity.
In this regard, the importance and need for studies like this one for epidemiological understanding of FI are emphasized. As the first study to assess this outcome in the indigenous population of Alagoas, it serves as a baseline for future evaluations and aids in the development and formulation of public policies that help understand and improve food security conditions in this population.
A critical issue in food insecurity scenarios is the increased exposure to conditions leading to malnutrition. Within such a context, there's a higher likelihood of individuals experiencing malnutrition early in life, which can have lifelong consequences. This phenomenon is explained by the Developmental Origins of Health and Disease (DOHaD) theory. According to this theory, adverse exposures during the first 1000 days of life, starting from conception, can alter a child's growth trajectory, prioritizing immediate survival but increasing the risk of diseases later in life. Therefore, populations facing food insecurity not only confront the immediate challenges of hunger but also an elevated risk of developing chronic diseases in adulthood, the roots of which originate in the early stages of their lives [33,34].
Regarding the limitations of this study, the cross-sectional design is notable, as it does not allow for the establishment of the incidence of the problem or direct cause-and-effect relationships between variables. Additionally, the data do not permit a qualitative assessment of the specific contexts of the indigenous communities studied.
Another significant limitation is the absence of a validated measurement tool for the target population. This issue is challenging to overcome, given the great diversity of indigenous ethnicities in Brazil, each with its distinct cultures, characteristics, and different ways of accessing food.
While the data presented facilitate the understanding of the epidemiological profile of FI among these populations, they highlight the need for the development of strategies to address the issue. It is essential to adopt approaches that consider their perspectives, traditions, cultures, and ways of life, including strengthening territorial rights and sustainable family agriculture to improve food access and the quality of life for Indigenous peoples.
5. Conclusions
The prevalence of FI among Alagoan Indigenous people is considerably high and associated with worse demographic, socioeconomic, and environmental conditions. This highlights the social inequities they face and underscores the need for intersectoral public policies to reverse this situation.
Author Contributions
E.R.S.A. and T.R.S. contributed to data collection during fieldwork, data analysis and interpretation, and writing the preliminary version of the article. H.S.F. was responsible for writing the project, obtaining funding, overall study coordination, data interpretation, and critical review of the manuscript. T.R.F. and E.A.S. contributed to writing the project and critical review of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the National Council for Scientific and Technological Development - CNPq (grant number 432249/2018-4), the Research Support Foundation of the State of Alagoas - FAPEAL (grant number 600300000000460/2020), the São Paulo Research Foundation - FAPESP (grant number 22739-4/2019), and the Coordination for the Improvement of Higher Education Personnel - CAPES (grant number 88887.836261/2023-00).
Institutional Review Board Statement
The ENSSAIA was approved by the National Research Ethics Commission - CONEP (CAAE 29121120.0.0000.5013, no 4.421.186), and all legal requirements related to ethical procedures for conducting research involving Indigenous peoples were observed.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author upon reasonable request.
Acknowledgments
We thank CNPq, FAPEAL, FAPESP, and CAPES for the financial support provided for the research. Our gratitude also goes to all members of the Basic and Applied Nutrition Laboratory (LNBA) for their assistance in data collection. We appreciate the team of Prof. Dr. Marly Cardoso dos Santos from the School of Public Health/USP for organizing the database. We are grateful to the Indigenous Health Agents and the entire Indigenous community for their hospitality and support, especially the chiefs and shamans
Conflicts of Interest:The authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| BFP | Bolsa Família Program |
| DOHaD | Developmental Origins of Health and Disease |
| EBIA | Brazilian Food Insecurity Scale |
| ENSSAIA | Study on Nutrition, Health, and Food Security of Indigenous Peoples in the State of Alagoas |
| FAO | Food and Agriculture Organization of the United Nations |
| FI | Food insecurity |
| FS | Food security |
| MSFI | The sum of moderate and severe food insecurity |
| NMW | National Minimum Wage |
| PR | Prevalence ratio |
| 95%CI | 95% confidence interval |
References
- Bezerra, M.S.; Jacob, M.C.M.; Ferreira, M.A.F.; Vale, D.; Mirabal, I.R.B.; Lyra, C.O. Insegurança alimentar e nutricional no Brasil e sua correlação com indicadores de vulnerabilidade. Ciência & Saúde Coletiva 2020, 25, 3833–3846. [Google Scholar]
- Brasil. Lei nº 11.346, de 15 de setembro de 2006. Cria o Sistema Nacional de Segurança Alimentar e Nutricional-SISAN com vistas em assegurar o direito humano à alimentação adequada e dá outras providências. Diário Oficial da União 2006, 143, 1–2. [Google Scholar]
- IBGE. Censo Demográfico 2022: Indígenas: primeiros resultados do universo. Rio de Janeiro, 2023.
- Jorge, C.A.S.; Souza, M.C.C. Insegurança Alimentar entre famílias indígenas de Dourados, Mato Grosso do Sul, Brasil. Saúde Coletiva (Barueri) 2023, 13, 13337–13356. [Google Scholar] [CrossRef]
- Pereira, T.M.G.; Magalhães, S.M.; Nazareno, E. Estado do conhecimento sobre história da alimentação indígena no Brasil. História: Questões & Debates 2020, 68. [Google Scholar]
- Segall-Corrêa, A.M.; Marín-Leon, L.; Amaral Azevedo, M.M.; Ferreira, M.B.R.; Gruppi, D.R.; Camargo, D.F.; Toledo Vianna, R.P.; Pérez-Escamilla, R. The Brazilian food security scale for indigenous Guarani households: development and validation. Food Security 2018, 10, 1547–1559. [Google Scholar] [CrossRef]
- Vieira, J.L.G. Povoamentos: ocupação e espoliação. In Alagoas: a herança indígena, Arapiraca: EdUneal, 2015.
- Alagoas. Estudo sobre as Comunidades Indígenas de Alagoas. Maceió, 2017; p 27.
- Segall-Corrêa, A.M.; Marin-León, L.; Melgar-Quiñonez, H.; Pérez-Escamilla, R. Refinement of the Brazilian household food insecurity measurement scale: recommendation for a 14-item EBIA. Revista de Nutrição 2014, 27, 241–251. [Google Scholar] [CrossRef]
- Fávaro, T.; Ribas, D.L.B.; Zorzatto, J.R.; Segall-Corrêa, A.M.; Panigassi, G. Segurança alimentar em famílias indígenas terena, Mato Grosso do Sul, Brasil. Cadernos de Saúde Pública 2007, 23, 785–793. [Google Scholar] [CrossRef]
- World Health Organization. The state of food security and nutrition in the world 2019: safeguarding against economic slowdowns and downturns; Food & Agriculture Org.: 2019; Vol. 2019.
- Victora, C.G.; Huttly, S.R.; Fuchs, S.C.; Olinto, M.T. The role of conceptual frameworks in epidemiological analysis: a hierarchical approach. International journal of epidemiology 1997, 26, 224–227. [Google Scholar] [CrossRef]
- Brasil. Resolução nº 304 de 09 de agosto de 2000. Aprova Normas para Pesquisas Envolvendo Seres Humanos – Área de Povos Indígenas. Diário Oficial da União 2000.
- Brasil. Resolução Nº 466, de 12 de dezembro de 2012. Aprova diretrizes e normas regulamentadoras de pesquisas envolvendo seres humanos. Diário Oficial da União. 2012.
- Brasil. Resolução Nº 510, de 07 de abril de 2016. Dispõe sobre as normas aplicáveis a pesquisas em Ciências Humanas e Sociais cujos procedimentos metodológicos envolvam a utilização de dados diretamente obtidos com os participantes ou de informações identificáveis ou que possam acarretar riscos maiores do que os existentes na vida cotidiana. Diário Oficial da União 2016.
- Borges, M.F.S.O.; Silva, I.F.d.; Koifman, R. Histórico social, demográfico e de saúde dos povos indígenas do estado do Acre, Brasil. Ciência & Saúde Coletiva 2020, 25, 2237–2246. [Google Scholar]
- Laschefski, K.A.; Zhouri, A. Povos indígenas, comunidades tradicionais e meio ambiente a" questão territorial" e o novo desenvolvimentismo no Brasil. Terra Livre 2019, 1, 278–322. [Google Scholar] [CrossRef]
- Baccarin, J.G.; Delgrossi, M.; Magro, J.P. Insegurança Alimentar e Nutricional no Brasil: Tendências e estimativas recentes. Instituto Fome Zero 2024, 26. [Google Scholar]
- World Health Organization. The State of Food Security and Nutrition in the World 2021: Transforming food systems for food security, improved nutrition and affordable healthy diets for all; Food & Agriculture Org.: 2021; Vol. 2021.
- IBGE. Pesquisa de Orçamentos Familiares 2017-2018: Análise da Segurança Alimentar no Brasil. Rio de Janeiro: IBGE, Coordenação de Trabalho e Rendimento, 2020. Availabe online: https://biblioteca.ibge.gov.br/visualizacao/livros/liv101749.pdf (Accessed on September 7th, 2024).
- IBGE. 10,3 milhões de pessoas moram em domicílios com insegurança alimentar grave. Availabe online: https://agenciadenoticias.ibge.gov.br/agencia-noticias/2012-agencia-de-noticias/noticias/28903-10-3-milhoes-de-pessoas-moram-em-domicilios-com-inseguranca-alimentar-grave (accessed on March 30th, 2024).
- Santos, L.A.; Ferreira, A.A.; Pérez-Escamilla, R.; Sabino, L.L.; Oliveira, L.G.; Salles-Costa, R. Interseções de gênero e raça/cor em insegurança alimentar nos domicílios das diferentes regiões do Brasil. Cadernos de Saúde Pública 2023, 38, e00130422. [Google Scholar] [CrossRef] [PubMed]
- Lignani, J.d.B.; Palmeira, P.d.A.; Antunes, M.M.L.; Salles-Costa, R. Relação entre indicadores sociais e insegurança alimentar: uma revisão sistemática. Revista Brasileira de Epidemiologia 2020, 23, e200068. [Google Scholar] [CrossRef] [PubMed]
- Pedraza, D.F. Insegurança alimentar e nutricional de famílias com crianças menores de cinco anos da Região Metropolitana de João Pessoa, Paraíba, Brasil. Ciência & Saúde Coletiva 2021, 26, 1511–1520. [Google Scholar]
- Raupp, L.; Cunha, G.M.; Fávaro, T.R.; Santos, R.V. Condições sanitárias entre domicílios indígenas e não indígenas no Brasil de acordo com os Censos nacionais de 2000 e 2010. Ciência & Saúde Coletiva 2020, 25, 3753–3763. [Google Scholar]
- Raupp, L.; Fávaro, T.R.; Cunha, G.M.; Santos, R.V. Condições de saneamento e desigualdades de cor/raça no Brasil urbano: uma análise com foco na população indígena com base no Censo Demográfico de 2010. Revista Brasileira de Epidemiologia 2017, 20, 1–15. [Google Scholar] [CrossRef]
- Coutinho, G.R.; Santos, S.M.C.; Gama, C.M.; Silva, S.O.; Santos, M.E.P.; Silva, N.J. Fatores demográficos e socioambientais associados à insegurança alimentar domiciliar nos diferentes territórios da cidade de Salvador, Bahia, Brasil. Cadernos de Saúde Pública 2022, 38, e00280821. [Google Scholar] [CrossRef]
- Schott, E.; Rezende, F.A.C.; Priore, S.E.; Ribeiro, A.Q.; Franceschini, S.C.C. Fatores associados à insegurança alimentar em domicílios da área urbana do estado do Tocantins, Região Norte do Brasil. Revista Brasileira de Epidemiologia 2020, 23, e200096. [Google Scholar] [CrossRef]
- Soares, G.H.; Mota, J.M.S.; Mialhe, F.L.; Biazevic, M.G.H.; Araújo, M.E.; Michel-Crosato, E. Insegurança alimentar domiciliar, cárie dentária e qualidade de vida relacionada à saúde bucal em Indígenas adultos brasileiros. Ciência & Saúde Coletiva 2021, 26, 1489–1500. [Google Scholar]
- Brito, A.P.; Lima, V.N.; Rêgo, A.S.; Dias, L.P.P.; Silva, J.D.; Carvalho, W.R.C.; Barbosa, J.M.A. Fatores associados à Insegurança Alimentar e Nutricional em comunidade carente. Revista Brasileira em Promoção da Saúde 2020, 33, 1–11. [Google Scholar] [CrossRef]
- Morais, D.C.; Lopes, S.O.; Priore, S.E. Indicadores de avaliação da Insegurança Alimentar e Nutricional e fatores associados: revisão sistemática. Ciência & Saúde Coletiva 2020, 25, 2687–2700. [Google Scholar]
- Observatório Brasileiro das Desigualdades. Taxa de extrema pobreza no Brasil cai 40% entre 2022 e 2023. Observatório Brasileiro das Desigualdades 2023.
- Ferreira, H.S.; Junior, A.F.S.X.; Assuncao, M.L.; Uchôa, T.C.C.; Lira-Neto, A.B.; Nakano, R.P. Developmental origins of health and disease: a new approach for the identification of adults who suffered undernutrition in early life. Diabetes, metabolic syndrome and obesity: targets and therapy 2018, 543-551.
- Silva, D.A.; Thoma, M.E.; Anderson, E.A.; Kim, J. Infant sex-specific associations between prenatal food insecurity and low birthweight: a multistate analysis. The Journal of Nutrition 2022, 152, 1538–1548. [Google Scholar] [CrossRef]
Figure 1.
Hierarchical analysis of factors associated with moderate and severe food insecurity.
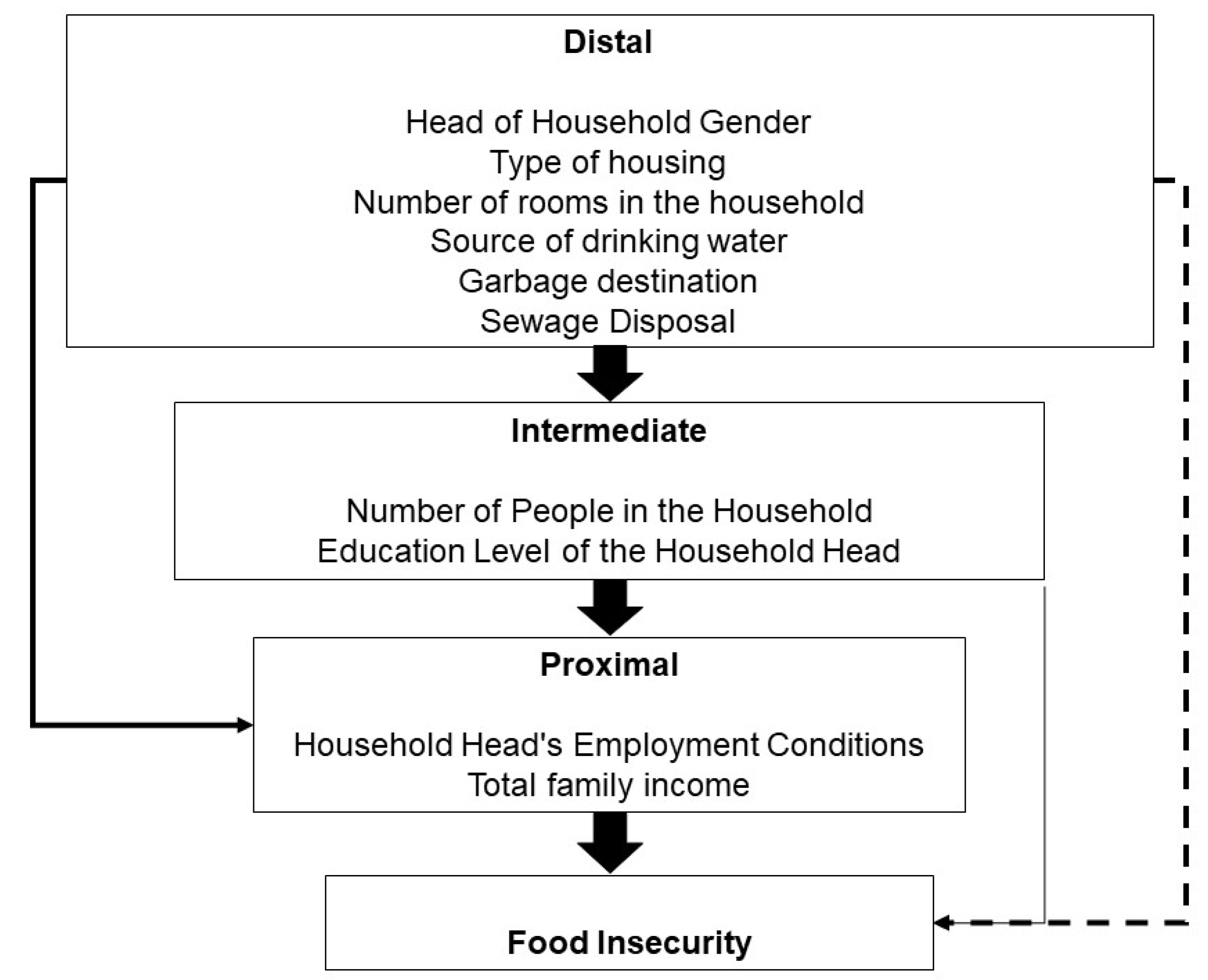
Figure 2.
Prevalence of Food Security and Food Insecurity (FI) according to the classification of the Brazilian Food Insecurity Scale in families from Indigenous communities in the state of Alagoas, Northeast Brazil, 2024.
Figure 2.
Prevalence of Food Security and Food Insecurity (FI) according to the classification of the Brazilian Food Insecurity Scale in families from Indigenous communities in the state of Alagoas, Northeast Brazil, 2024.
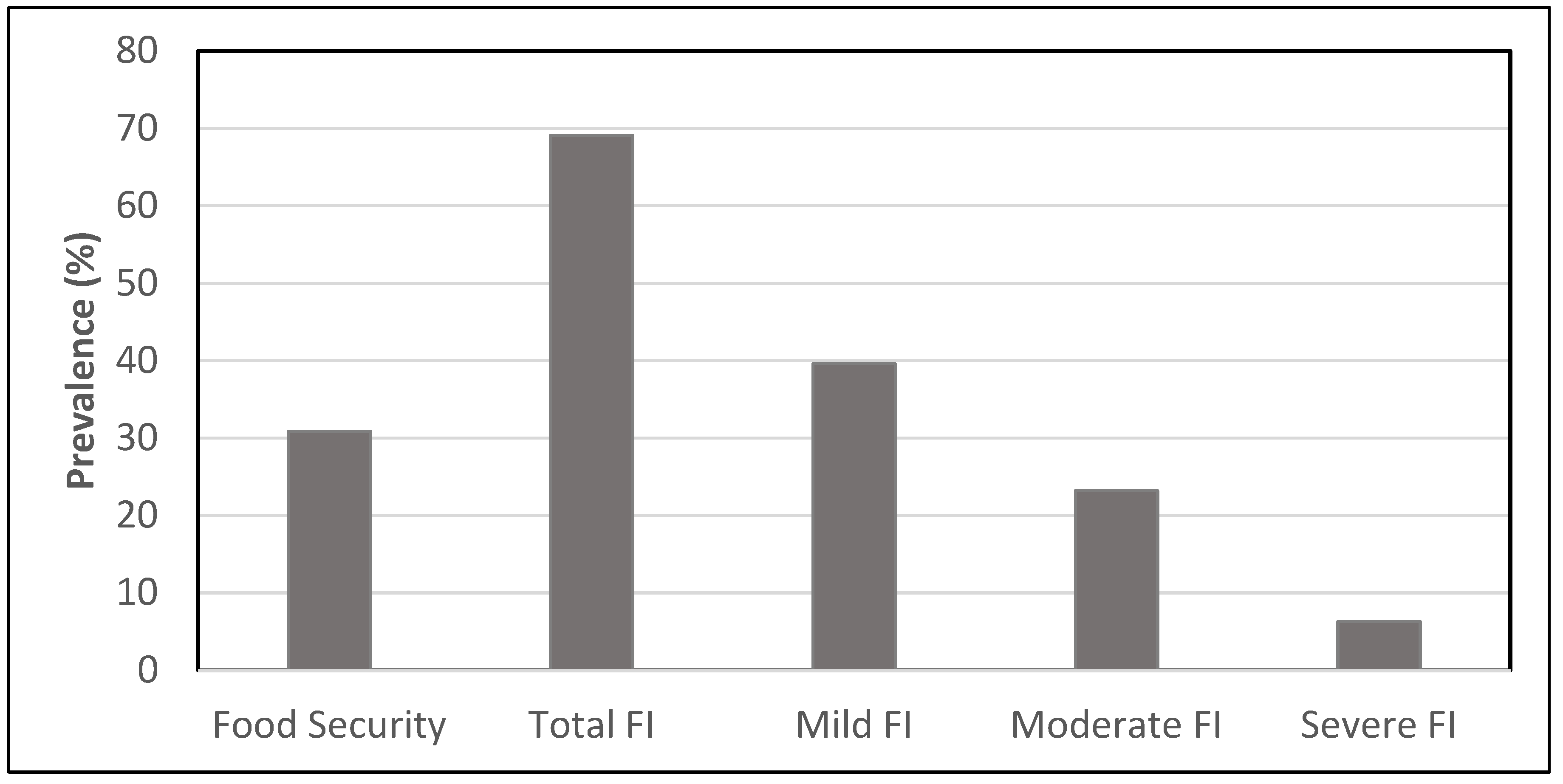

Table 1.
Indigenous communities in Alagoas by Region, Municipality, and Ethnicity.
| Region | Municipality | Ethnicity | Village |
|---|---|---|---|
| Agreste Region | Traipu | Aconã | Aconã |
| São Sebastião | Karapotó | Fazenda Terra Nova | |
| Plaki-ô | |||
| Campo Grande, Feira Grande |
Tingui-Botó | Tingui-Botó | |
| Olho D’Água do Meio | |||
| Alto Sertão Region | Água Branca | Kalankó | Januária |
| Lajedo do Couro | |||
| Sítio Gregório | |||
| Inhapi | Koiunpanká | Baixa do Galo | |
| Roçado | |||
| Baixa Fresca | |||
| Pariconha | Geripankó | Ouricuri | |
| Figueiredo | |||
| Moxotó | |||
| Serra do Engenho | |||
| Aratikun | |||
| Pariconha | Karuazu | Tanque | |
| Campinhos | |||
| Pariconha | Katokinn | Katokinn | |
| Baixo São Francisco Region | São Brás, Porto Real do Colégio | Kariri-Xokó | Kariri-Xokó |
| Planalto da Borborema Region | Palmeira dos Índios | Xucuru-Kariri | Fazenda do Canto |
| Boqueirão | |||
| Mata da Cafuna | |||
| Cafurna de Baixo | |||
| Serra da Capela | |||
| Serra do Amaro | |||
| Coité | |||
| Riacho Fundo | |||
| Serra dos Quilombos Region | Colônia Leopoldina, Joaquim Gomes, Matriz de Camaragibe, Novo Lino |
Wassú | Cocal |
| TOTAL | 11 | 29 | |
Source: Adapted from the State Secretariat for Planning, Management, and Heritage [8].
Table 1.
Prevalence of Food Insecurity (FI) according to the categories of demographic, socioeconomic, and environmental variables of indigenous communities in the state of Alagoas, Northeast Brazil, 2024.
Table 1.
Prevalence of Food Insecurity (FI) according to the categories of demographic, socioeconomic, and environmental variables of indigenous communities in the state of Alagoas, Northeast Brazil, 2024.
| Variable/Category | Total n (%) |
Presence of FI¹ n (%) |
Crude PR (CI 95%) | p-value |
|---|---|---|---|---|
| Demographics | ||||
| Head of Household Gender | ||||
| Male | 705 (55.51) | 177 (25.11) | 1 | - |
| Female | 565 (44.49) | 197 (34.87) | 1.39 (1.17-1.65) | < 0.001 |
| Number of People in the Household | ||||
| ≤ 4 | 960 (75.59) | 271 (28.23) | 1 | - |
| > 4 | 310 (24.41) | 103 (33.23) | 1.18 (0.97-1.41) | 0.088 |
| Socioeconomics | ||||
| Education Level of the Household Head (in completed years of schooling) | ||||
| ≥ 9 | 415 (32.68) | 76 (18.31) | 1 | - |
| 5 a 8 anos | 263 (20.71) | 84 (31.94) | 1.74 (1.33-2.28) | < 0.001 |
| ≤ 4 | 592 (46.61) | 214 (36.15) | 1.97 (1.57-2.48) | < 0.001 |
| Household Head's Employment Conditions | ||||
| Formal employment | 156 (12.31) | 19 (12.18) | 1 | - |
| Informal employment | 472 (37.25) | 126 (26.69) | 2.19 (1.40-3.42) | 0.001 |
| Retired | 296 (23.36) | 96 (32.43) | 2.66 (1.69-4.18) | < 0.001 |
| Unemployed | 343 (27.07) | 132 (38.48) | 3.16 (2.03-4.19) | < 0.001 |
| Total Family Income (in number of national minimum wages) | ||||
| > 2 | 272 (21.42) | 39 (14.34) | 1 | - |
| > 1 a 2 | 443 (34.88) | 128 (28.89) | 2.02 (1.46-2.79) | < 0.001 |
| 0 a 1 | 555 (43.70) | 207 (37.30) | 2.60 (1.91-3.55) | < 0.001 |
| Family receiving assistance from the Bolsa Família Program | ||||
| No | 541 (42.60) | 136 (25.14) | 1 | - |
| Yes | 729 (57.40) | 238 (32.65) | 1.30 (1.08-1.55) | 0.004 |
| Environmental | ||||
| Type of Housing | ||||
| Masonry | 1233 (97.09) | 352 (28.55) | 1 | - |
| Mud/Wood | 37 (2.91) | 22 (59.46) | 2.08 (1.57-2.76) | < 0.001 |
| Number of Rooms in the Household | ||||
| > 4 | 1133(89.21) | 312 (27.54) | 1 | - |
| ≤ 4 | 137 (10.79) | 62 (45.26) | 1.64 (1.34-2.01) | < 0.001 |
| Source of Drinking Water | ||||
| Adequate² | 662 (52.13) | 188 (28.40) | 1 | - |
| Inadequate | 608 (47.87) | 186 (30.59) | 1.08 (0.91-1.28) | 0.392 |
| Garbage Destination | ||||
| Public collection | 1014(79.84) | 287 (28.30) | 1 | - |
| Other³ | 256 (20.16) | 87 (33.98) | 1.20 (0.99-1.46) | 0.069 |
| Sewage Disposal⁴ | ||||
| Adequate | 485 (38.19) | 126 (25.98) | 1 | - |
| Inadequate | 785 (61.81) | 248 (31.59) | 1.22 (1.01-1.46) | 0.035 |
¹FI Moderate + Severe Forms. ² General Distribution Network and Mineral Water. 3 Burning, Vacant Land, Buried, or Other Methods. 4 Adequate (Septic Tank and/or Sewer System), Inadequate (Primitive Pit, Ditch, Lake, or Other).
Table 2.
Hierarchical analysis of factors associated with the prevalence of moderate and severe food insecurity in indigenous communities in the state of Alagoas, Northeast Brazil, 2024. .
Table 2.
Hierarchical analysis of factors associated with the prevalence of moderate and severe food insecurity in indigenous communities in the state of Alagoas, Northeast Brazil, 2024. .
| Variables | Distal Level | Intermediate Level | Proximal Level | |||
|---|---|---|---|---|---|---|
| PR (CI 95%) |
p-valor | PR (CI 95%) |
p-valor | PR (CI 95%) |
p-value | |
| Head of Household Gender | ||||||
| Male | 1 | 1 | 1 | |||
| Female | 1.38 (1.16-1.63) |
< 0.001 |
1.44 (1.23-1.71) |
< 0.001 |
1.26 (1.04-1.51) |
0.016 |
| Type of Housing | ||||||
| Masonry | 1 | 1 | 1 | |||
| Mud/Wood | 1.69 (1.25-2.28) |
0.001 |
1.56 (1.13-2.15) |
0.007 |
1.53 (1.12-2.10) |
0.008 |
| Number of Rooms in the Residence | ||||||
| > 4 | 1 | 1 | 1 | |||
| ≤ 4 | 1.47 (1.18-1.84) |
0.001 |
1.48 (1.17-1.86) |
0.001 |
1.29 (1.02-1.63) |
0.031 |
| Garbage Destination | ||||||
| Public collection | 1 | |||||
| Others¹ | 1.10 (0.88-1.36) |
0.397 |
||||
| Sewage Disposal ² | ||||||
| Adequate | 1 | |||||
| Inadequate | 1.14 (0.94-1.37) |
0.174 |
||||
| Number of People in the Household | ||||||
| ≤ 4 | 1 | |||||
| > 4 | 1.15 (0.96-1.38) |
0.133 |
||||
| Education Level of the Household Head (in completed years of schooling) | ||||||
| ≥ 9 | 1 | 1 | ||||
| 5 a 8 | 1.80 (1.38-2.34) |
< 0.001 |
1.55 (1.19-2.01) |
0.001 |
||
| ≤ 4 | 2.02 (1.61-2.53) |
< 0.001 |
1.78 (1.40-2.26) |
< 0.001 |
||
| Household Head's Employment Conditions | ||||||
| Formal employment | 1 | |||||
| Informal employment | 1.43 (0.91-2.22) |
0.112 |
||||
| Retired | 1.73 (1.10-2.73) |
0.018 |
||||
| Unemployed | 1.62 (1.03-2.54) |
0.036 |
||||
| Total Family Income (in number of national minimum wages)3 | ||||||
| > 2 | 1 | |||||
| > 1 a ≤ 2 | 1.69 (1.22-2.33) |
0.001 | ||||
| ≤ 1 | 2.00 (1.44-2.76) |
< 0.001 |
||||
¹ Burning, vacant land, buried, or other means. ² Adequate (septic tank and/or sewer system), Inadequate (rudimentary pit, ditch, lake, or other). 3 In Brazil, the federal minimum wage is the lowest amount a salaried worker must receive for their work performed over a month, provided they are a formal worker. Its value is set annually by a decree-law signed by the president. At the time of data collection, it was R$ 1,320.00 (approximately 275 USD at that time).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



