
Submitted:
09 September 2024
Posted:
10 September 2024
You are already at the latest version
Abstract
Reliable access to electricity has become a necessity worldwide, and without it, no country can operate health systems and achieve sustainable development goals (SDGs). However, while developed countries have been successfully electrified for many decades, most developing countries have fallen short, contributing to significant impacts, particularly the health sector. The present study explores the relationship between electrification and health vulnerability in developing countries between 1990 and 2020 using the Feasible Generalized Least Square (FGLS) approach. The varied electrification across countries motivates the use of non-linear associations between electrification and health vulnerability. We demonstrate that electrification and health vulnerability have an inverted U-shaped association. Further analysis indicates that most developing countries have achieved a mature level of an inverted U-shaped curve, showing a reduction in health vulnerability with increasing electrification. There are few developing countries, mainly African countries, struggling to reach maturity. The results of this study indicate the need for increased access to electrification, in combination with a reduction in the use of biomass and fossil fuel feedstocks, to mitigate health vulnerability in developing countries.
Keywords:
Electrification
; Health vulnerability
; Feasible Generalized Least Square Method Inverted U-shaped curve
; Developing countries
1. Introduction
It is widely recognized that electricity plays a vital role in modern society. It is not just a matter of convenience, but necessary for everyday life. For instance, a strong connection exists between electricity and the health sector, including the operation of medical technologies and primary health facilities, with consequences for the provision of health services (Chen et al., 2019). Ensuring universal electrification is pivotal to achieving better health outcomes and sustainable development, as it helps to improve living standards, aids the sharing of health and other information, enhances the quality of health services, and contributes to a sustainable future (Langnel & Amegavi, 2020; Rehman et al., 2018). Hence, ensuring access to a safe and reliable electricity supply is a critical agenda item for all policymakers and practitioners working to address the challenges of electrification.
Despite this, many countries have so far failed to achieve this vital level of development for example Angola, Congo, Mozambique, Niger, South Sudan and Tanzania (Asghar et al. 2022). Most of these countries are African countries that are mainly relying on traditional energy sources (i.e., wood, coal, oil and gas) the excessive use of these sources is impacting the environment and their health. According to the estimates of the World Health Organization (WHO), almost one billion people in underdeveloped nations are treated in hospitals without electricity (WHO, 2013). For example, South Asia and African countries have no electricity from more than one out of 10 health facility centres, while in African states, almost 600 million people do not have access to electrification (Moore et al., 2020).
The availability of electricity plays a critical role in hospitals for the life and death of the patients. Electric power plays a basic role during medical operations because medical equipment extensively depends on electricity. Electricity plays a vital role in many aspects of healthcare services. For instance, healthcare centres with reliable electricity can provide better prenatal and antenatal care, and women in need of pregnancy-related care can be attended to even at night. Additionally, proper electricity supply enables the safe and efficient storage of various medicines for extended periods (Asghar et al., 2022).
Further, due to inadequate electrification, many people in the developing world are forced to depend on polluted energy sources for daily needs, particularly for heating and kitchen purposes. According to Rani et al. (2022), 2.4 billion people in developing countries are using traditional energy sources such as biomass for energy purposes. For example, in most rural areas, people use wood and cow dung for cooking, lighting, and heating their houses. Similarly, the World Bank reports that 79% of the global population uses fossil fuels and biomass for household energy purposes, especially in developing countries (World Bank, 2022). The inefficient burning of biomass contains fatal particles such as organic compounds, metals, sulphur dioxide and CO2 that affect human health (Hadj, 2021; Umar et al., 2021; Dai et al., 2022). In addition to this, Rana et al. (2021) point out that using solid fuel poses a threat to air quality, causing 3.1 million premature deaths annually. The massive use of fossil fuel and biomass-derived energy has been identified as a critical hurdle to achieving the world’s sustainable development goals (SDGs)(Amjad, 2023).
The 27th IPCC Conference of Parties (COP27) has emphasized the need to encourage the use of clean and green energy through electrification in various sectors, for example, transportation, construction, production, and agriculture (Inger, 2022). Most developed countries, including the UK, USA, Australia, Germany, and China, are working to mitigate climate change, and transitioning to green energy sources (Stern and Lankes., 2022). The Climate Action Agenda 2030 for Sustainable Development focuses on decarbonization by ensuring the use of renewables while providing greater access to affordable and reliable electricity in developing countries (Amesho and Edoun., 2019). Minimizing the use of traditional energy sources (i.e., wood, coal, oil, gas) will contribute to reduced carbon emissions, environmental degradation, and health vulnerability (Asghar et al., 2022).
As mentioned above, there is a strong correlation between electricity access and health vulnerability. Variance in electricity availability and primary healthcare facilities have been observed in industrialized and developing countries. Such disparities lead to significant differences not only in the health sector but also in other aspects of life (Casati et al., 2023). Despite efforts by countries worldwide to provide electricity to their citizens, lower-income countries still face major challenges in electrification (Falk et al., 2021).
To make smart investment decisions in electrification and healthcare, it is crucial to have a comprehensive understanding of how access to electricity affects health outcomes, reduces health vulnerability, and assists in accomplishing sustainable development goals in developing nations. Although some progress has been made in this domain, additional research is still essential to fully comprehend the extent to which electricity supply can contribute to improvements in health and well-being and the attainment of sustainable development goals. There is little research into the health implications of this disparity concerning third-world countries. This study aims to fill this research gap by inspecting the relationship between access to electricity and health vulnerability in the case of developing countries.
The concept of vulnerability has been used by various scholars for different purposes and perspectives in previous studies and still lacks a single recognized definition. Vulnerability has been at the core of multidiscipline such as socio-economic, ecological, human geography, engineering, and psychology. According to environmentalist views, the term vulnerability has been used in different contexts, such as climate change, risk management and natural disasters, food security and global health (Khan et al., 2021). However, the popular definition of vulnerability is the degree of sensitivity adversely affected by disturbance or change (Khan et al., 2021). Despite all these definitions of vulnerability, the Intergovernmental Panel on Climate Change (IPCC, 2001) specified climate change vulnerability based on three basic indicators such as sensitivity, adaptive capacity and exposure.
Exposure means the duration, degree, or range to which a system is exposed to disaster; likewise, sensitivity means the degree to which a disturbance affects a system. On the other hand, an adaptive capacity means the capability of a system to cope with or improve from the disturbance. Hahn et al. (2009) measured vulnerability in terms of exposure to climate variability and natural calamities, and susceptibility to water, food, and health security issues. Amjad (2023) used vulnerability in terms of material and emotional harm, which happened due to the limited adaptive capacity of a system. Asghar et al. (2022) followed the Notre Dame Global Adaptation Index (ND-GAIN) and replaced the climate vulnerability term with the index of health vulnerability.
Measuring vulnerability in the past was challenging due to the lack of data, appropriate methods, and suitable scales (Sarker et al., 2019). However, the ND-GAIN has identified six critical factors (food, health, water, human habitat, infrastructure, and ecosystem services) for ensuring the continuity of life. These factors are derived from 45 varied indicators and were used to measure the vulnerability index for 190 countries.
This study aims to investigate how increased access to electricity can reduce health vulnerability in developing countries, as measured by the Health Vulnerability Index (HVI). The study proposes that when access to electricity is limited, health vulnerability is higher, but when access to electricity increases, health vulnerability decreases. The present research deviates from previous studies that have concentrated on the effects of clean energy on health indicators such as infant mortality rate, life expectancy, and deaths (Wang et al., 2023; Sule et al., 2022; Sial et al., 2022; Dai et al., 2022). Instead, this study delves deeper into exploring the relationship between electrification and health vulnerabilities by using the unique HVI indicators developed by ND-GAIN. More importantly, the study uses a non-linear approach, the Feasible Generalized Least Square method (FGLS), which better explains the association between electrification and health vulnerability.
A comprehensive explanation of the relationship between accessibility to electricity, its effects on health, and sustainable development will aid policymakers. This knowledge is crucial for those striving to shift towards clean energy while also striving to enhance access to electricity in rural areas and regional health outcomes.
2. Literature Review
Numerous studies have assessed health problems using different variables and shown significant impacts on human health. Chen et al. (2019) examined the effect of electrification on India’s health system and found that electrification is an excellent instrument for strengthening critical healthcare components. Casey et al. (2020) examined the impact of power outages on communities, reporting that power outages had a negative impact on health, including cardiovascular, respiratory, and mortality. Moore et al. (2020) predicted that about 800 million people, predominantly in poorer countries, are deprived of access to electricity. This study also found that lack of accessibility, reliability, and affordability to electricity is a major problem for their health and safety.
Many studies refer to the lack of electrification as ‘energy poverty’ (EP). Banerjee et al. (2021) scrutinized the impact of lack of electrification on health across 50 least-developed countries and revealed that lack of electrification was correlated with the spread of different diseases and deaths. Awaworyi-Churchill and Smyth (2021) found an adverse relationship between energy poverty and health in Australia. Ani (2021) examined the role of power supply on health care delivery in Nigeria and found that power shortages resulted in the deaths of almost 40% of infants within the first day. Bakehe (2022) analyzed the relationship between EP and respiratory diseases in Cameroon in 2014 and concluded that EP enhances respiratory illness in women. Sule et al. (2022) investigated the link between electrification and mortality in 33 African countries and reported that increased household electrification decreased the mortality rate. Asghar et al. (2023) empirically analyzed the effect of urban and rural electrification on kids’ death rates from 1990 to 2020; this study indicated that electrification has an inverted U-shaped relationship with infant mortality in the case of developing and developed countries.
Wang (2018) assessed how urbanization is affecting global health, finding that, overall, urbanization has a positive role in enhancing global health. Abbasi et al. (2021) noted that urbanization increased worldwide by almost 2% in the last three decades. The primary reason behind this considerable transformation from rural to urban areas is the availability of better facilities in clean drinking water, accessibility and reliability of electricity, and advanced health facilities. Tripathi and Maiti (2023) measured the influence of urbanization on health in India from 1971 to 2011 and concluded that growing urbanization increased economic prosperity, which positively affects health outcomes. However, urbanization can also lead to a decline in health outcomes in urban areas due to massive numbers of pollutants. An empirical study by Wang et al. (2023) observed the irregular effect of citification on health risks in China and proposed a U-shaped curve for urbanization rate and mortality.
Like other sectors, the importance of the industrial sector for human health cannot be ignored. Feizpour et al. (2018) tested the impact of overspill on health in Iran. The study concluded that industrialization has a dual impact on human health and well-being. Rahman et al. (2018) examined the nexus between environmental pollution and health in the top 20 industrialized countries and found that environmental pollution from industry severely impacts human health. On the other hand, Crane-Kramer and Buckberry (2023) argue that modernization of science and technologies is closely associated with industrialization, which has positively impacted the medical and health sectors.
Education is another critical social determinant of health (Raghupathi and Raghupathi, 2018). Zajacova and Lawrence (2018) analyzed the relationship between health and education in the USA. The study revealed that more highly educated people live healthier lives than those with no education or a lower level of education. Fonseca et al. (2020) explored the connection between education and health in 14 OECD countries. This research found a causal relationship between health and education and concluded that higher education leads to better health outcomes. However, Pappas (2017) points out that nearly 200 million students in developing countries lose their schooling yearly due to illness and poor health conditions, contributing in turn to lower educational outcomes.
Gross fixed capital formation (GFCF) used in this study is an investment in the health sector, which is also known as a national budget, especially for the health sector which plays a significant role in better health outcomes. Akinci et al. (2014) empirically analyzed the impact of government and private expenses on health indicators for 19 Middle East and North Africa (MENA) countries. This study found that improvement in healthcare expenditure enhances health outcomes. Bein et al. (2017) revealed that spending on health positively affected the expectations for life in developing countries. Similarly, Rahman et al. (2018) tried to check the connection between health expenditure and health outcomes in the South Asian Association for Regional Cooperation (SAARC) and the Association of Southeast Asian Nations (ASEAN) countries. The overall findings of the study elucidated that there is a significant negative correlation between total health expenditure and poor health outcomes such as infant mortality rate and crude death rates.
We are aware of several studies that have investigated mortality rates and health outcomes with electricity security. These studies have used multiple variables and indicators, such as life expectancy and biomass energy consumption. However, there is little evidence in the literature of studies regarding the assessment of the extent of the association between health vulnerability and electricity. Therefore, this study will address this research gap by examining linear and non-linear relationships between health vulnerability and access to electricity at the global level, with a specific focus on developing countries.
3. Conceptual Framework
Kuznets (1955) used a curve to establish the relationship between per-capita income and income disparity and named it an inverted U-shaped curve, which is known as the Kuznets curve hypothesis. In addition to this, Grossman, and Krueger (1995) extended this idea and used the Environmental Kuznets Curve (EKC) hypothesis to examine the relationship between economic growth and environmental pollution. They discovered that there was an inverted U-shaped relationship, as the initial stages of economic growth tend to harm the environment, while higher levels of economic growth led to an improvement in environmental quality (Hanif et al., 2020). Haans et al. (2016) further developed the EKC hypothesis by investigating non-linear associations between economic growth and social factors such as performance, outcomes, and benefits in business settings. Since 1990, economists and environmentalists have been empirically testing the relationship between various variables inspired by the EKC hypothesis (Amjad, 2023; Sule et al., 2022; Sial et al., 2022; Asghar et al., 2022; Hanif et al., 2020).
On the foundation of the EKC hypothesis, the present study explores the non-linear relationship between access to electricity and population health vulnerability (Figure 1). The analysis focuses on the disparity in access to electricity across countries and examines the non-linear relationship to provide a better understanding of the association of access to electricity and health vulnerability. Specifically, the study aims to determine whether a U-shaped or inverted U-shaped curve can represent the relationship, as indicated by Haans et al. (2016).
4. Data and Methodology
We analyzed data from 79 developing countries, which were chosen because they typically have limited access to electricity. These countries are selected based on the availability of data and the World Development Indicators classification of 2022. Many people in these countries rely on energy sources that are harmful to their health; for example, Central Africa, Cameroon, Congo, Tanzania and Angola mentioned by Asghar et al. (2022). The data set for the annual Health Vulnerability Index (HVI) at the country level was taken from the (ND-GAIN) data source. Similarly, the percentage of the electrified population (with electricity access) for each country was taken from the World Development Indicators (WDI) covering the period between 1990 and 2020.
Apart from access to electricity, four more control variables were included: urban population, education, gross fixed capital formation, and industrial value added (Table 1). Many studies (Amjad, 2023; Sule et al., 2022; Sial et al., 2022; Rani et al., 2022; Hanif et al., 2020) have used these variables and found them significant to achieve better representations of health outcomes.
ND-GAIN is a free and open-source countries index system that tells the current state of a country’s climate change vulnerability and its preparedness in the form of investment for climate adaptation( https://gain.nd.edu/our-work/country-index/). The index is based on six life-supporting sectors including food, water, health, ecosystem services, human habitat, and infrastructure in assessing the vulnerability of the countries. The framework used by ND-GAIN to calculate climate change vulnerability follows the (IPCC) definition of climate vulnerability based on three components: magnitude, sensitivity, and adaptive capacity. (
The present study used the ND-GAIN vulnerability indicator in the health sector as the country-level HVI. The ND-GAIN HVI was calculated by following six steps.
- Firstly, we collected raw data on various health vulnerability aspects, including projected changes in deaths caused by climate change-related diseases, dependence on external resources for healthcare services, slum population, availability of medical staff (physicians, nurses, and midwives), and access to improved sanitation facilities. We then removed any tabulation errors and made appropriate transformations as required.
- In the second step, we filled in any missing data through interpolation. If any country had no data available for certain components, we marked those components as missing for that country.
- In the third and fourth steps, we established a baseline by identifying the largest and lowest values for the raw data.
- In the fifth step, we assigned a score to the raw data, ranging from 0 to 1. This means that the higher the score, the greater the vulnerability, and the lower the score, the lower the vulnerability.
- In the final stage, we calculated a health vulnerability score for each country.
The present study used an econometric technique, the Feasible Generalized Least Square (FGLS) technique, to obtain the empirical analysis (Parks, 1967). It considers the model’s cross-sectional heteroscedasticity, time-series autocorrelation, and cross-sectional autocorrelation (Afzal et al., 2017). Furthermore, FGLS is particularly appropriate for the fixed and long-panel data type, making it the ideal choice for this study.
To capture the non-linear relationship between HVI and access to electricity, this study also considers the quadratic term of electrification. The functional form of the model is given by,
By following equation (1), the multiple regression is formed by using the natural logarithm (LN) of all variables as:
In equation (2), LNHVI shows the natural logarithmic of health vulnerability and is used as the dependent variable. is a constant, while and are coefficients associated with the level and quadratic terms of LNACE. They determine the possibility of the curve’s shape either U or inverted U in the case of health vulnerability.
The cut-off value, which is estimated by using the ratio of both coefficients such as electricity and electricity square is calculated by,
The calculation of the linear marginal effect of (LNACE) is estimated by using the mean values of electricity access in the population of 79 lower-income countries. Similarly, the linear marginal effect for equation (3) is done by taking the first partial derivative with respect to LNACE which is given in equation (3).
5. Results
Based on the empirical estimations, we find that the relationship between electrification and health vulnerability has an inverted U-shaped curve. This curve indicates that lower electrification levels enhance health vulnerability until it reaches a certain point, beyond which higher electrification levels decrease health vulnerability. This study proposes the inverted U-shaped curve hypothesis, which states that lower levels of electricity increase health vulnerability and that access to electricity has a quadratic effect that reduces health vulnerability. The study was able to prove that higher levels of access to electricity decrease health vulnerability.
All countries, except Malawi, Burundi, Cameroon, and the African Central Republic, are energy-secure countries because they have achieved the maturity level of the curve and lie right side of the inverted U-curve. However, some African countries including Malawi, Burundi, Cameroon, and African Central Republic need to work on their access to electricity to achieve maturity level.
Figure 2 shows the bivariate analysis between electrification and health vulnerability, developed in R language. It explains the interdependency and relationship between two variables. The existence of the non-linear association between HVI and electrification has been seen and shows an inverted U-shaped relationship.
Table 2 describes a descriptive statistics analysis of the various determinants of health vulnerability in the case of developing countries. The overall mean value of health vulnerability is (4.0), which is higher than the value of its standard deviation (0.35), which presents a lower dispersion in the health vulnerability. The average values of variables are greater than their standard deviation, which means that they are under-dispersion, which further explains that data used in this model is not dispersed (Huang et al., 2023). All the skewness values show adversely skewed distribution and high values of Kurtosis present the outliers in the series, which means that heterogeneity exists across countries. Moreover, all probability values are significant, meaning variables may lack symmetry (Falak et al., 2022).
Figure 3 shows the correlation plot, designed using a correlation matrix. An econometric analysis uses a correlation matrix to establish the relationship or correlation between multiple variables. The dark blue balls show a strong positive correlation among the variables.
Table 3 describes the results of the Variance Inflation Factor (VIF) test. It is applied to verify the multicollinearity problem in the estimated model. The VIF measures and identifies the correlation among independent variables. When VIF scores are less than ten, it shows a lower issue of multicollinearity in the model. All values of VIF are less than ten, which explains that the multicollinearity problem does not exist in the estimated model. The minimum values of VIF reveal that the explanatory variables in the model are not correlated, and every variable has equal importance in the regression model (Bukhari et al., 2021; Fatima et al., 2021).
This study applies the Pedroni cointegration test to analyze the long-term cointegrating relationship among dependent and independent variables. This co-integration method is widely used to examine the relationship among different variables especially in the long-term (Sule et al., 2022). The cointegration is tested using STATA software through the command xtcointtest, which performs the Kao (1999), Westerlund (2005) and Pedroni (1999), tests. These three tests work differently but give the same results. In the case of no cointegration, these analyses believe in a general null hypothesis that no cointegration exists. However, the alternative hypothesis of the Pedroni tests and the Kao tests explains cointegration between variables exists in all panels. The Pedroni test is particularly useful in evaluating the co-integration among various time series variables, as it can examine their long-term connections. Additionally, it is appropriate for panel data analysis and addresses cross-sectional dependency in data analysis through multiple co-integration tests (Javaid et al., 2022). Table 4 presents the significant p-values (P<0.001) of all variables, indicating the sign of a cointegration relationship between variables for the long term.
Table 5 presents the detailed findings of the FGLS approach. For empirical estimation, 2015 observations were used in the model. The Wald test and Chi2’s significant values show that the overall model is fit. The coefficient of the logarithm of electrification (LNACE) is 0.22, which is positive and significant at P<0.01. This implies that HVI and access to electricity have a positive relationship. In other words, reduced access to electrification can make individuals more vulnerable to health issues. Moreover, a one percent increase in access to electrification can contribute to a 0.22 percent decrease in health vulnerability.
However, the negative quadratic coefficient of electrification (LNACE2) shows that a higher electrification level reduces the HVI. Following the webpage of Jermy Dawson (2014), (http://www.jeremydawson.co.uk/slopes.htm) which contains different Excel templates which help to check the two-way or three-way interaction effect among dependent and independent variables by incorporating the mean, standard deviation and estimated coefficient values of the estimated model into the given excel template. The study used this template and found the inverted U-shaped relationship is presented in Figure 4. The same results were estimated by Asghar et al. (2023) in the global perspective that lower electrification raises the newborn mortality rate whilst higher electrification reduces the infant mortality rate. People with lower electrification levels were compelled to use polluted power resources like dunk, agricultural residual, wood coal, and wood for cooking and lighting, which is the major cause of HVI and mortality due to toxic smoke emissions.
The urban population is used in this study as a first control variable. The natural logarithm of the urban population (LNURPOP) positively impacts health vulnerability in developing countries (Abbasi et al., 2021; Tripathi & Maiti, 2023; Wang, 2018; Wang et al., 2023). The rapid economic growth in developing countries has led to the risen use of polluted energy supplies in urban areas, resulting in significant environmental pollution and associated health problems.
Education (LNEDU) declines the HVI (Fonseca et al., 2020; Pappas, 2017; Raghupathi & Raghupathi, 2018; Zajacova & Lawrence, 2018). Generally, people with higher education tend to have more knowledge about health-related issues, which helps them achieve better health outcomes and longer lives. They practice health-promoting behaviours and receive timely health check-ups. Industrialization (LNIND) reduces the HVI because it impacts people’s income, and higher income means better health facilities (Crane-Kramer & Buckberry, 2023; Feizpour et al., 2018).
Gross Fixed Capital Formation (LNGFCF) has significant positive signs that show a 1% increase in GFCF will increase health vulnerability by 0.12% (Akinci et al., 2014; Bein et al., 2017; Rahman et al., 2018). The reason behind its positive impact on health vulnerability is when countries have more GDP, they increase their investment in industries, infrastructure, and development purposes so, on the one side, they grow and prosper, but on the other hand, this growth and development has negative impacts on the environment which increase health vulnerability, especially in the least developed countries. These countries do not have enough resources to use expensive renewable technologies to balance economic development and environmental destruction.
Table 6 presents the cut-off value of the inverted U-shaped curve. It is estimated through the ratio of the coefficients of electrification. The estimated cut-off value (1.93) is laid between the minimum and maximum value of the electrification value (Table 2). This finding supports the authenticity of the inverted U-shaped curve (Rani et al., 2022a).
Figure 4 depicts the quadratic association between electrification and health vulnerability. To validate this non-linear relationship, the study followed the procedure outlined by Jermey Dowson (2014). A low Logarithm of access to electricity (LANCE) indicates less access to electricity. When access to electricity is low, health vulnerability is high, as shown by point 4.7. However, as access to electricity increases, health vulnerability decreases from 4.7 to 4.1. Therefore, it can be concluded that higher access to electricity reduces health vulnerability in developing countries.
Table 7 presents the marginalized linear effect of level and quadratic electrification. We estimate marginalized because the findings of the FGLS model, illustrated in Table 5, reveal that access to electricity does not follow a constant return to scale. This means that some countries have increasing returns to scale while others have decreasing returns to scale. Valuable insights can be gained by examining each country on either side of the inverted U-shaped curve. To determine the countries that experience increasing or decreasing returns to scale in the case of access to electricity, we estimate the marginalized linear effect using equation 3. The results indicate, notably, that countries such as Burundi, Cameroon, Central African Republic, and Malawi demonstrate a positive association between electrification and HVI to the left of the curve. Conversely, all other third-world countries are positioned on the other side of the curve, indicating an inverse association between electrification and HVI. These findings suggest that access to electricity is a crucial factor for African countries to reach the maturity stage of the curve (Amjad & Rehman, 2023; H. Wang et al., 2022).
6. Discussion
Energy security has become an essential part of modern society, and it has become vital in improving the socioeconomic conditions and the quality of life of people, including better health. However, there is still a significant difference between industrialized and poor countries regarding the incidence of severe health issues. The outcomes of the study suggest an inverted U-shaped association between access to electricity and health vulnerability in the case of least-developed countries. Moreover, it shows a positive value for the level coefficient of access to electricity, while the quadratic coefficient value is negative. This indicates that a lower level of access to electricity can increase health vulnerability. However, the negative quadratic coefficient of electricity suggests that a higher level of electricity can decrease health vulnerability. Similarly, a positive relationship was observed between education, industrialization, gross fixed capital formation, urbanization, and health outcomes. These relationships are consistent and compatible with prior expectations and findings from existing literature. For example, Asghar et al. (2023), provided evidence to show that lower electrification rates resulted in higher infant mortality rates, whereas increased electrification led to a reduction in kids’ death rates.
The findings imply that some countries such as Burundi, Cameroon, Central African Republic, and Malawi have a positive association between electrification and health vulnerability and lie on the left side of the curve, based on the margin effects. However, all other developing countries are on the maturity side of the curve, indicating a negative correlation between electrification and health vulnerability. Particularly, these African countries could gain by providing reasonable and reliable access to electrification along with education and urbanization to improve health outcomes. While existing evidence suggests that many developing countries have reached the maturity level of the U-shaped curve and achieved specific gains in the health department. As examined before in the study, some conceptual proof has been provided for this relationship. Asghar et al., (2022) noted that most of these countries use traditional energy sources, which harms health. The use of polluted energy resources such as dunk, agricultural residual, charcoal, and wood for cooking and lighting purposes has been the primary cause of hazardous indoor air pollution and mortality due to toxic smoke emissions among low-income people with limited access to electricity.
However, Falak et al. (2021) asserted that electrification has enormous potential to improve people’s health and economic well-being. It directly impacts health care and eventually health status of the population. This confirms that economic conditions and health could significantly be improved because of a higher level of access to electricity. The condition is especially pertinent in African countries where several health facility centres lack access to electricity to provide better health care (World Bank, 2022). Our results emphasize the potential benefits of the health sector from higher access to electricity. Policy actions toward recognizing these benefits and leveraging them will be a significant move in the right direction.
In addition to analysing access to electricity, this study included four control variables: education, industrialization, gross fixed capital formation, and urban population. All these factors have been found to have a positive correlation with health outcomes. Furthermore, the results of this study are consistent with prior research conducted by (Amjad, 2023; Sule et al., 2022; Sial et al., 2022; Rani et al., 2022; Hanif et al.,2020).
The first control variable urban population positively impacted health vulnerability in least-developed countries, and similar findings were revealed by these studies (Abbasi et al., 2021; Tripathi & Maiti, 2023; Wang, 2018; Wang et al., 2023). These studies noted that the urban population uses polluted energy resources to fulfill the massive economic activities in developing countries. The studies suggest that people in urban areas in developing countries are not concerned about the influence of their actions on the environment, which exacerbates the situation. The government should control the use of polluted energy sources and provide subsidized clean and green energy sources. Higher education has a positive impact on health outcomes. This positive relationship between education and health is supported by several studies (Fonseca et al., 2020; Pappas, 2017; Raghupathi & Raghupathi, 2018; Zajacova & Lawrence, 2018).
Hence, the Government should promote higher education through the provision of domestic and international scholarships which will increase the desire for higher education. Highly qualified people are likely to have more knowledge about health-related problems, which helps them to attain better health outcomes. Moreover, industrialization also has a negative relationship with health vulnerability because it enhances the per capita income of the people, and when people have a high income, they can easily access better health facilities. These results are supported by these studies (Crane-Kramer & Buckberry, 2023; Feizpour et al., 2018). The findings suggest that access to electricity is a crucial factor for developing countries to improve people’s health and living conditions. Particularly, in South Asian countries such as Pakistan where lots have been done on the availability of electricity to the masses but electricity price per unit has proven to be an obstacle for the household. This is far too high even its more than the incomes of households.
This research thus focuses on the examination that comprehensive socio-economic growth through electrification can only be achieved if local people can afford it. Those countries that have achieved higher levels of access to electricity should focus on solving these problems. On the other hand, especially for African countries, if they want to reach the maturity stage of development (Amjad & Rehman, 2023; Wang et al., 2022). These African countries need to focus on improving accessibility, affordability, and reliability of energy, particularly in terms of providing electricity, which is essential for better health outcomes and reaching the right side of the development curve. Although not all countries are similarly vulnerable to energy poverty, access to electricity has become vital for the socio-economic aspects of human life.
The study was based on national-level data that included rural and urban populations. However, there is a significant disparity between metropolitan and countryside areas regarding health vulnerability, electrification, and disaster impacts. In fact, rural areas are more susceptible to these issues as compared to industrialized regions. For instance, individuals living in remote areas have limited resources, restricted access to services, and longer distances to public facilities. Moreover, they receive fewer government development funds than those living in urban areas with easy access to these facilities. Also, further in-depth research can be conducted on specific case study areas in developing countries to assess different vulnerabilities, including health, climate, agriculture, and livelihood.
7. Conclusion and Policy Recommendations
Based on the analysis, the study concludes that the level coefficient of electrification has a positive sign, and the quadratic coefficient has a negative sign, proposing an inverted U-shaped relationship between electrification and health vulnerability. More importantly, the study concludes that the majority of the countries are on the right side of the inverted U-shaped curve. This further indicates that most of the developing countries have reached the maturity stage have achieved higher levels of sustainable energy and have lower health vulnerability. However, a few poor countries particularly; Burundi, Cameroon, Central African Republic, Malawi, and South Sudan, have been unable to achieve the final stage of the inverted-U-shaped curve and have higher health vulnerability. Overall, the findings of the study reveal that urbanization and industrialization positively contribute to health vulnerability, while education negatively impacts health vulnerability in third-world countries.
To efficiently reduce carbon emissions, it is suggested that developing countries should mainly focus on easy access to electricity. The increased use of biomass and fossil fuels is the main cause of these emissions. The improved and easy access to electricity will lead to an enhanced health sector and decreased climate vulnerability. Governments of least-developed countries, especially sub-Saharan African regions, need to pay more attention to access to electricity to reach the maturity level of the inverted U-shaped curve. They need huge investments to install new-grade stations to provide access to electricity, improving the health of a large population. Moreover, aid agencies and development banks (e.g., World Bank and Asian Development Bank) should play their role in the form of investment in ensuring access to reliable access to electricity in these countries and they must work on better health and education facilities.
This study contributes to knowledge of the health sector by providing useful policy recommendations, especially for developing countries which can be applied worldwide to reduce health vulnerability through access to electricity. Moreover, this study is unique because there is not much literature on health vulnerability in the case of third-world countries. This existing research can be further extended by incorporating a resilience factor to improve health vulnerability. A comparison between developing and developing countries can be made to assess health vulnerability.
References
- Abbasi, K. R., Abbas, J., Mahmood, S., & Tufail, M. (2021). Revisiting electricity consumption, price, and real GDP: A modified sectoral level analysis from Pakistan. Energy Policy, 149(January), 112087. [CrossRef]
- Ahmad, M. I., & Ma, H. (2020). Climate change and livelihood vulnerability in mixed crop-livestock areas: The case of Province Punjab, Pakistan. Sustainability (Switzerland), 12(2), 12–16. [CrossRef]
- Akinci, F., Hamidi, S., Suvankulov, F., & Akhmedjonov, A. (2014). Examining the impact of health care expenditures on health outcomes in the Middle East and N. Africa. Journal of Health Care Finance, 41(1).
- Amjad, M. A. (2023). Moderating the role of social progress with greenhouse gases to determine the health vulnerability in developing countries. Environmental Science and Pollution Research. [CrossRef]
- Amjad, M. A., & Rehman, H. U. (2023a). The Long Run Dynamics of Sustainable Economic Development on Ecological Footprint in Developed and Developing Countries: Panel Quantile Regression. Review of Education, Administration & Law, 6(2), 191–210. [CrossRef]
- Ani, V. A. (2021). Powering primary healthcare centres with clean energy sources. Renewable Energy and Environmental Sustainability, 6, 7. [CrossRef]
- Asghar, N., Amjad, M. A., & Rehman, H. U. (2023). Analyzing the impact of access to electricity and biomass energy consumption on infant mortality rate: a global perspective. Environmental Science and Pollution Research International, 30(11), 29550–29565. [CrossRef]
- Asghar, N., Amjad, M. A., & Rehman, H. U. (2022). Analyzing the impact of access to electricity and biomass energy consumption on infant mortality rate: a global perspective. Environmental Science and Pollution Research, 30(11), 29550–29565. [CrossRef]
- Asghar, N., Amjad, M. A., Rehman, H., Munir, M., & Alhajj, R. (2022). Achieving sustainable development resilience: Poverty reduction through affordable access to electricity in developing economies. Journal of Cleaner Production, 376. [CrossRef]
- Awaworyi Churchill, S., & Smyth, R. (2021). Energy poverty and health: Panel data evidence from Australia. Energy Economics, 97. [CrossRef]
- Bakehe, N. P. (2022). Energy poverty: consequences for respiratory health and labour force participation in Cameroon. Journal of Environmental Economics and Policy, 11(3), 235–247. [CrossRef]
- Banerjee, R., Mishra, V., & Maruta, A. A. (2021). Energy poverty, health, and education outcomes: Evidence from the developing world. Energy Economics, 101. [CrossRef]
- Bauer, S. E., Im, U., Mezuman, K., & Gao, C. Y. (2019). Desert Dust, Industrialization, and Agricultural Fires: Health Impacts of Outdoor Air Pollution in Africa. Journal of Geophysical Research: Atmospheres, 124(7), 4104–4120. [CrossRef]
- Beck, N. (2001). Time-series–cross-section data: What have we learned in the past few years? Annual review of political science, 4(1), 271-293. https://www.annualreviews.org/doi/pdf/10.1146/annurev.polisci.4.1.271.
- Bein, M. A., Unlucan, D., Olowu, G., & Kalifa, W. (2017). Healthcare spending and health outcomes: evidence from selected East African countries. African Health Sciences, 17(1), 247–254. [CrossRef]
- Bukhari, S., Kalim, R., & Arshed, N. (2021). Prevailing Poverty in SAARC Countries: Can Education Help? Exchange Rate Modelling View project Accounting and Finance View project. https://www.researchgate.net/publication/353923334.
- Casati, P., Moner-Girona, M., Khaleel, S. I., Szabo, S., & Nhamo, G. (2023). Clean energy access as an enabler for social development: A multidimensional analysis for Sub-Saharan Africa. Energy for Sustainable Development, 72, 114–126. [CrossRef]
- Casey, J. A., Fukurai, M., Hernández, D., Balsari, S., & Kiang, M. V. (2020). Power Outages and Community Health: a Narrative Review. Current Environmental Health Reports, 7(4), 371–383. [CrossRef]
- Chen, Y. J., Chindarkar, N., & Xiao, Y. (2019). Effect of reliable electricity on health facilities, health information, and child and maternal health services utilization: evidence from rural Gujarat, India. Journal of Health, Population, and Nutrition, 38(1), 7. [CrossRef]
- Crane-Kramer, G., & Buckberry, J. (2023). Changes in health with the rise of industry. International Journal of Paleopathology, 40, 99–102. [CrossRef]
- Dai, H., Mamkhezri, J., Arshed, N., Javaid, A., Salem, S., & Khan, Y. A. (2022). Role of Energy Mix in Determining Climate Change Vulnerability in G7 Countries. Sustainability (Switzerland), 14(4). [CrossRef]
- Dangour, A. D., Green, R., Häsler, B., Rushton, J., Shankar, B., & Waage, J. (2012). Symposium 1: Food chain and health: Linking agriculture and health in low- and middle-income countries: An interdisciplinary research agenda. Proceedings of the Nutrition Society, 71(2), 222–228. [CrossRef]
- Dawson, J. F. (2014). Moderation in Management Research: What, Why, When, and How. Journal of Business and Psychology, 29(1), 1–19. [CrossRef]
- Dong, H., Xue, M., Xiao, Y., & Liu, Y. (2021). Do carbon emissions impact the health of residents? Considering China’s industrialization and urbanization. Science of the Total Environment, 758, 143688. [CrossRef]
- Amesho, K. T., & Edoun, E. I. (2019). Financing renewable energy in Namibia: A fundamental key challenge to the sustainable development goal 7: Ensuring access to affordable, reliable, sustainable, and modern energy for all. International Journal of Energy Economics and Policy, 9(5), 442-450.https://www.zbw.eu/econis-archiv/bitstream/11159/5125/1/1747801488.pdf.
- Falak, F., Ayub, F., Zahid, Z., Sarfraz, Z., Sarfraz, A., Robles-Velasco, K., & Cherrez-Ojeda, I. (2022). Indicators of Climate Change, Geospatial and Analytical Mapping of Trends in India, Pakistan, and Bangladesh: An Observational Study. International Journal of Environmental Research and Public Health 2022, Vol. 19, Page 17039, 19(24), 17039. [CrossRef]
- Fatima, R., Arshed, N., & Hanif, U. (2021). Do ecological factors dictate the longevity of human life? A case of Asian countries. Ukrainian Journal of Ecology, 0(0), 1–12. https://www.ujecology.com/articles/do-ecological-factors-dictate-the-longevity-of-human-life-a-case-of-asian-countries-86548.html.
- Feizpour, M. A., Samanpour, Z., & Mehrjardi, A. S. (2018). The Industrialization in Iran: Health Provider or Health Remover? Iranian Economic Review, 22(3), 719–740. [CrossRef]
- Fonseca, R., Michaud, P. C., & Zheng, Y. (2020). The effect of education on health: evidence from national compulsory schooling reforms. SERIEs, 11(1), 83–103. [CrossRef]
- Haans, R. F. J., Pieters, C., & He, Z. L. (2016). Thinking about U: Theorizing and testing U- and inverted U-shaped relationships in strategy research. Strategic Management Journal, 37(7), 1177–1195. [CrossRef]
- Hadj, T. B. (2021). Nonlinear impact of biomass energy consumption on ecological footprint in a fossil fuel–dependent economy. Environmental Science and Pollution Research, 28(48). [CrossRef]
- Hanif, N., Arshed, N., & Aziz, O. (2020). On the interaction of the energy: Human capital Kuznets curve? A case for technology innovation. Environment, Development and Sustainability, 22(8), 7559-7586. https://link.springer.com/content/pdf/10.1007/s10668-019-00536-9.pdf.
- Hahn, M. B., Riederer, A. M., & Foster, S. O. (2009). The Livelihood Vulnerability Index: A pragmatic approach to assessing risks from climate variability and change case study in Mozambique. Global Environmental Change, 19(1), 74–88. [CrossRef]
- Huang, X., Khan, Y. A., Arshed, N., Salem, S., Shabeer, M. G., & Hanif, U. (2023). Increasing social resilience against climate change risks: a case of extreme climate affected countries. International Journal of Climate Change Strategies and Management, 15(3), 412–431. [CrossRef]
- Inger, A. (2022). The Closing Window The Climate crisis calls for rapid transformation of societies.
- IPCC, T., 2001. Climate change 2001: synthesis report. Intergovernmental Panel on Climate Change (IPCC), Geneva, Switzerland.
- Javaid, A., Arshed, N., Munir, M., Zakaria, Z. A., Alamri, F. S., Abd El-Wahed Khalifa, H., & Hanif, U. (2022). Econometric Assessment of Institutional Quality in Mitigating Global Climate-Change Risk. Sustainability (Switzerland), 14(2). [CrossRef]
- Jessel, S., Sawyer, S., & Hernández, D. (2019). Energy, Poverty, and Health in Climate Change: A Comprehensive Review of an Emerging Literature. In Frontiers in Public Health (Vol. 7). Frontiers Media S.A. [CrossRef]
- Khan, N.A., Gao, Q., Abid, M. and Shah, A.A., 2021. Mapping farmers’ vulnerability to climate change and its induced hazards: evidence from the rice-growing zones of Punjab, Pakistan. Environmental Science and Pollution Research, 28(4), pp.4229-4244.
- Langnel, Z., & Amegavi, G. B. (2020). Globalization, electricity consumption and ecological footprint: An autoregressive distributive lag (ARDL) approach. Sustainable Cities and Society, 63. [CrossRef]
- Moore, N., Glandon, D., Tripney, J., Kozakiewicz, T., Shisler, S., Eyres, J., Zalfou, R., Daniela, M., Leon, A., Kurkjian, V., Snilstveit, B., & Perdana, A. (2020). Evaluation Independent Effects of Access to Electricity Interventions on Socioeconomic Outcomes in Low-and Middle-Income Countries Systematic Review Report.
- ND-GAIN. (2023). Country Index - Notre Dame Global Adaptation Initiative.
- Novignon, J., Atakorah, Y. B., & Djossou, G. N. (2018). How Does the Health Sector Benefit from Trade Openness? Evidence from Sub-Saharan Africa. African Development Review, 30(2), 135–148. [CrossRef]
- Pappas, A. (2017). The Relationship Between Healthcare and Education and Their Impact on Global Health. https://digitalcommons.lasalle.edu/honors_projects.
- Parks, R. W. (1967). Efficient Estimation of a System of Regression Equations when Disturbances are Both Serially and Contemporaneously Correlated Author (s): Richard W. Parks Source: Journal of the American Statistical Association, Vol. 62, No. 318 (Jun. 1967), p. Journal of the American Statistical Association, 62(318), 500–509.
- Qadir, N., & Majeed, M. T. (2018a). The Impact of Trade Liberalization on Health: Evidence from Pakistan. Empirical Economic Review, 1(1), 71–108. [CrossRef]
- Qadir, N., & Majeed, M. T. (2018b). The Impact of Trade Liberalization on Health: Evidence from Pakistan. Empirical Economic Review, 1(1), 71–108. [CrossRef]
- Raghupathi, W., & Raghupathi, V. (2018). An empirical study of chronic diseases in the United States: a visual analytics approach to public health. International journal of environmental research and public health, 15(3), 431.
- Rahman, M. M., Khanam, R., & Rahman, M. (2018). Health care expenditure and health outcome nexus: new evidence from the SAARC-ASEAN region. Globalization and Health, 14(1), 113. [CrossRef]
- Rana, J., Islam, R. M., Khan, M. N., Aliani, R., & Oulhote, Y. (2021). Association between household air pollution and child mortality in Myanmar using a multilevel mixed-effects Poisson regression with robust variance. Scientific Reports, 11(1). [CrossRef]
- Rani, T., Amjad, M. A., Asghar, N., & Rehman, H. U. (2022a). Exploring the moderating effect of globalization, financial development, and environmental degradation nexus: a roadmap to sustainable development. Environment, Development and Sustainability, 0123456789. [CrossRef]
- Rani, T., Amjad, M. A., Asghar, N., & Rehman, H. U. (2022b). Revisiting the environmental impact of financial development on economic growth and carbon emissions: evidence from South Asian economies. Clean Technologies and Environmental Policy, 24(9), 2957–2965. [CrossRef]
- Rehman, A., Deyuan, Z., Chandio, A. A., & Hussain, I. (2018). An empirical analysis of rural and urban populations’ access to electricity: Evidence from Pakistan. Energy, Sustainability and Society, 8(1), 1–9. [CrossRef]
- Sarker, M. N. I., Cao, Q., Wu, M., Hossin, M. A., Alam, G. M. M., & Shouse, R. C. (2019). Vulnerability and livelihood resilience in the face of natural disaster: A critical conceptual review. Applied Ecology and Environmental Research, 17(6), 12769–12785. [CrossRef]
- Sial, M. H., Arshed, N., Amjad, M. A., & Khan, Y. A. (2022). Nexus between fossil fuel consumption and infant mortality rate: a non-linear analysis. Environmental Science and Pollution Research, 29(38), 58378–58387. [CrossRef]
- Stern, N., & Lankes, H. P. (2022). Collaborating and Delivering on Climate Action through a Climate Club.
- Sule, I. K., Yusuf, A. M., & Salihu, M. K. (2022). Impact of energy poverty on education inequality and infant mortality in some selected African countries. Energy Nexus, 5. [CrossRef]
- Tripathi Assistant Professor, S. (2021). Munich Personal RePEc Archive Relationship between urbanization and health outcomes in Indian states Relationship between urbanization and health outcomes in Indian states.
- Tripathi, S., & Maiti, M. (2023). Does urbanization improve health outcomes: a cross country level analysis. Asia-Pacific Journal of Regional Science, 7(1), 277–316. [CrossRef]
- Umar, M., Ji, X., Kirikkaleli, D., & Alola, A. A. (2021). The imperativeness of environmental quality in the United States transportation sector amidst biomass-fossil energy consumption and growth. Journal of Cleaner Production, 285, 124863. [CrossRef]
- Wang, F., Liu, S., Chen, T., Zhang, H., Zhang, Y., & Bai, X. (2023). How urbanization affects residents’ health risks: evidence from China. Environmental Science and Pollution Research, 30(13), 35554–35571. [CrossRef]
- Wang, H., Amjad, M. A., Arshed, N., Mohamed, A., Ali, S., Haider Jafri, M. A., & Khan, Y. A. (2022). Fossil Energy Demand and Economic Development in BRICS Countries. Frontiers in Energy Research, 10(April), 1–15. [CrossRef]
- Wang, Q. (2018). Urbanization and Global Health: The Role of Air Pollution. In Iran J Public Health (Vol. 47, Issue 11).
- World Bank. (2022). Fossil fuel energy consumption (% of total). https://data.worldbank.org/indicator/EG.USE.COMM.FO.ZS.
- World Health Organization. (2023). Energizing health: accelerating electricity access in health-care facilities Executive summary.
- Zajacova, A., & Lawrence, E. M. (2018). The Relationship Between Education and Health: Reducing Disparities Through a Contextual Approach. Https://Doi.Org/10.1146/Annurev-Publhealth-031816-044628, 39, 273–289. [CrossRef]
Figure 1.
Hypothetical curves consist of three stages: an initial stage, a cut-off point, and a final stage. At the initial stage, where access to electricity is lower, health vulnerability in a country can either increase or decrease. The cut-off points separate countries based on their levels of access to electricity. The cut-off value is estimated by using the ratio of the estimated coefficients of electrification. At the final stage, the marginalized linear effect is estimated by using equation (3) to determine the position of each country on either side of the curve. Countries with lower electrification access are positioned on the left side of the curve. As for countries with higher access, they are on the other side of the curve. Health vulnerability in these countries can either decrease or increase, respectively. The given negative and positive signs of net effects values will determine the position of the country for example, countries with negative signs will lie on the right side of the inverted U-shaped curve which means that health vulnerability has a negative relationship with access to electricity. On the other hand, countries with positive signs will lie on the left-hand side of the curve which means that they have limited access to electricity therefore, they have a positive relationship with health vulnerability. This graph is modified from (Amjad & Rehman, 2023).
Figure 1.
Hypothetical curves consist of three stages: an initial stage, a cut-off point, and a final stage. At the initial stage, where access to electricity is lower, health vulnerability in a country can either increase or decrease. The cut-off points separate countries based on their levels of access to electricity. The cut-off value is estimated by using the ratio of the estimated coefficients of electrification. At the final stage, the marginalized linear effect is estimated by using equation (3) to determine the position of each country on either side of the curve. Countries with lower electrification access are positioned on the left side of the curve. As for countries with higher access, they are on the other side of the curve. Health vulnerability in these countries can either decrease or increase, respectively. The given negative and positive signs of net effects values will determine the position of the country for example, countries with negative signs will lie on the right side of the inverted U-shaped curve which means that health vulnerability has a negative relationship with access to electricity. On the other hand, countries with positive signs will lie on the left-hand side of the curve which means that they have limited access to electricity therefore, they have a positive relationship with health vulnerability. This graph is modified from (Amjad & Rehman, 2023).
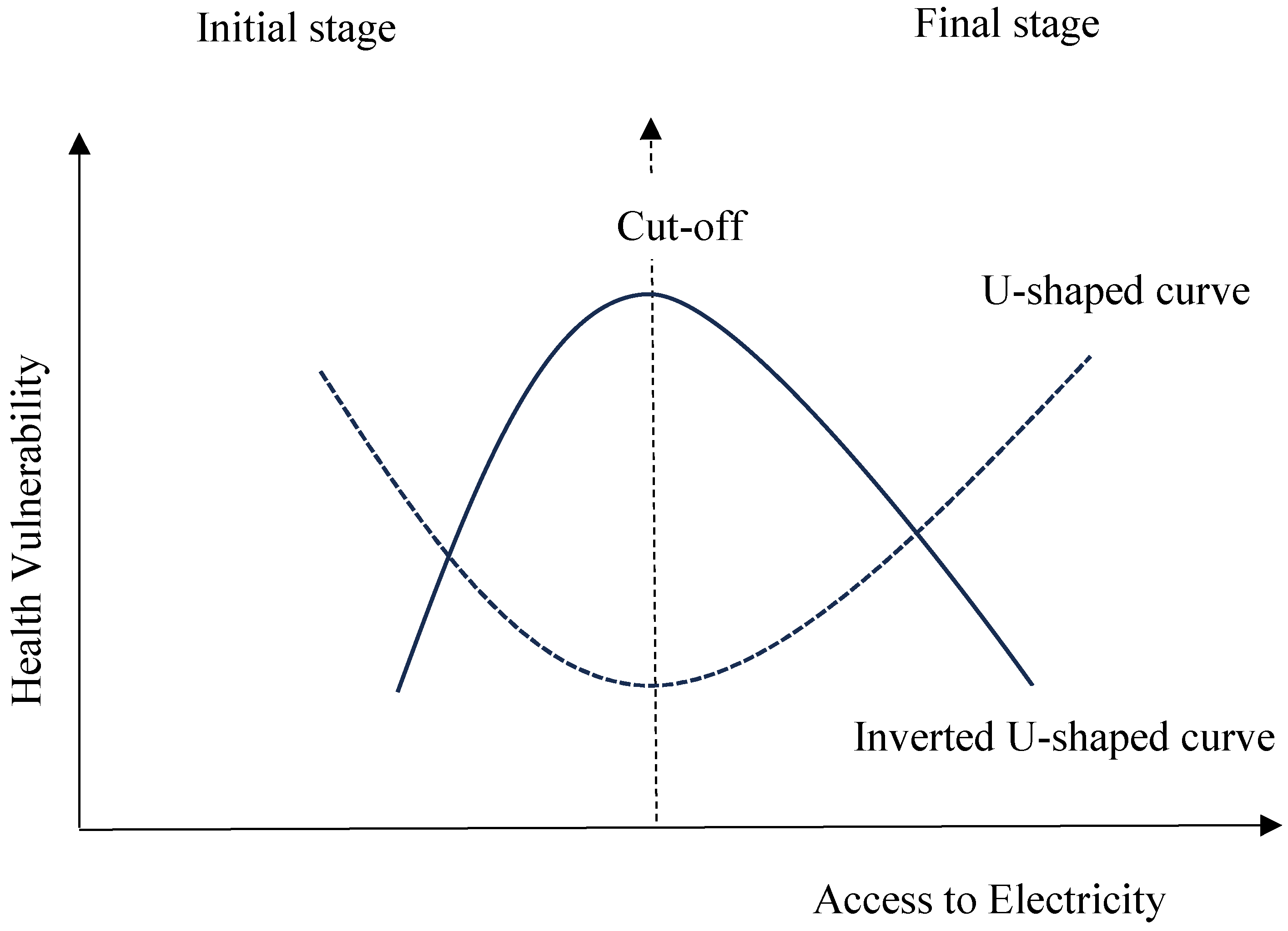
Figure 2.
Bi-variate analysis between electrification and health vulnerability. This graph represents the bi-variate analysis, and it shows the access to electricity on the x-axis and health vulnerability on the y-axis. Each data point on this scatter plot represents each year of a country. A clear pattern can be observed as most data points cluster at the top right corner of the graph and spread out to the lower right. It indicates that regions with higher access to electricity have lower health vulnerability. There are some outliers located in the lower right corner of the graph, which indicates that increased access to electricity is associated with lower health vulnerability. Moreover, this analysis is statistically significant as the mean values (represented by the blue line) fall within the 95% of confidence interval.
Figure 2.
Bi-variate analysis between electrification and health vulnerability. This graph represents the bi-variate analysis, and it shows the access to electricity on the x-axis and health vulnerability on the y-axis. Each data point on this scatter plot represents each year of a country. A clear pattern can be observed as most data points cluster at the top right corner of the graph and spread out to the lower right. It indicates that regions with higher access to electricity have lower health vulnerability. There are some outliers located in the lower right corner of the graph, which indicates that increased access to electricity is associated with lower health vulnerability. Moreover, this analysis is statistically significant as the mean values (represented by the blue line) fall within the 95% of confidence interval.
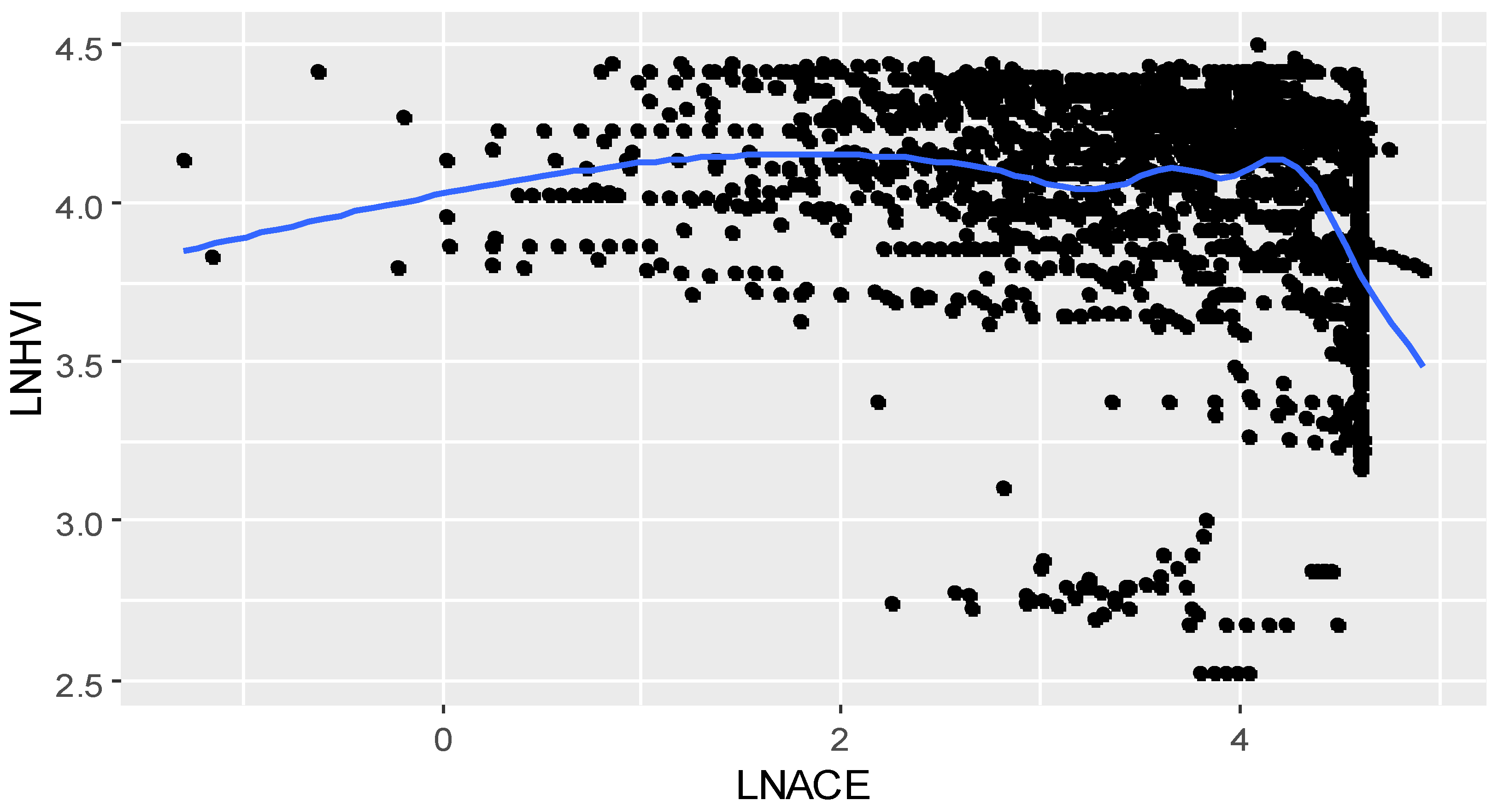
Figure 3.
Correlation coefficient plot. The above graph illustrates the correlation coefficient between various variables. Each ball in the correlation plot shows the correlation coefficient between two variables. Its range lies between -1 and 1, meaning that positive and negative values show a relationship direction between two variables. Moreover, nearly 1 indicates a perfect correlation; closer to 0 points, a weak correlation exists among variables. It is seen from the given visualization that dark blue balls show a strong positive correlation and red balls present a strong negative correlation. Moreover, white balls reveal there is no correlation, and it is seen that all balls in the light colours show a weak correlation among variables.
Figure 3.
Correlation coefficient plot. The above graph illustrates the correlation coefficient between various variables. Each ball in the correlation plot shows the correlation coefficient between two variables. Its range lies between -1 and 1, meaning that positive and negative values show a relationship direction between two variables. Moreover, nearly 1 indicates a perfect correlation; closer to 0 points, a weak correlation exists among variables. It is seen from the given visualization that dark blue balls show a strong positive correlation and red balls present a strong negative correlation. Moreover, white balls reveal there is no correlation, and it is seen that all balls in the light colours show a weak correlation among variables.
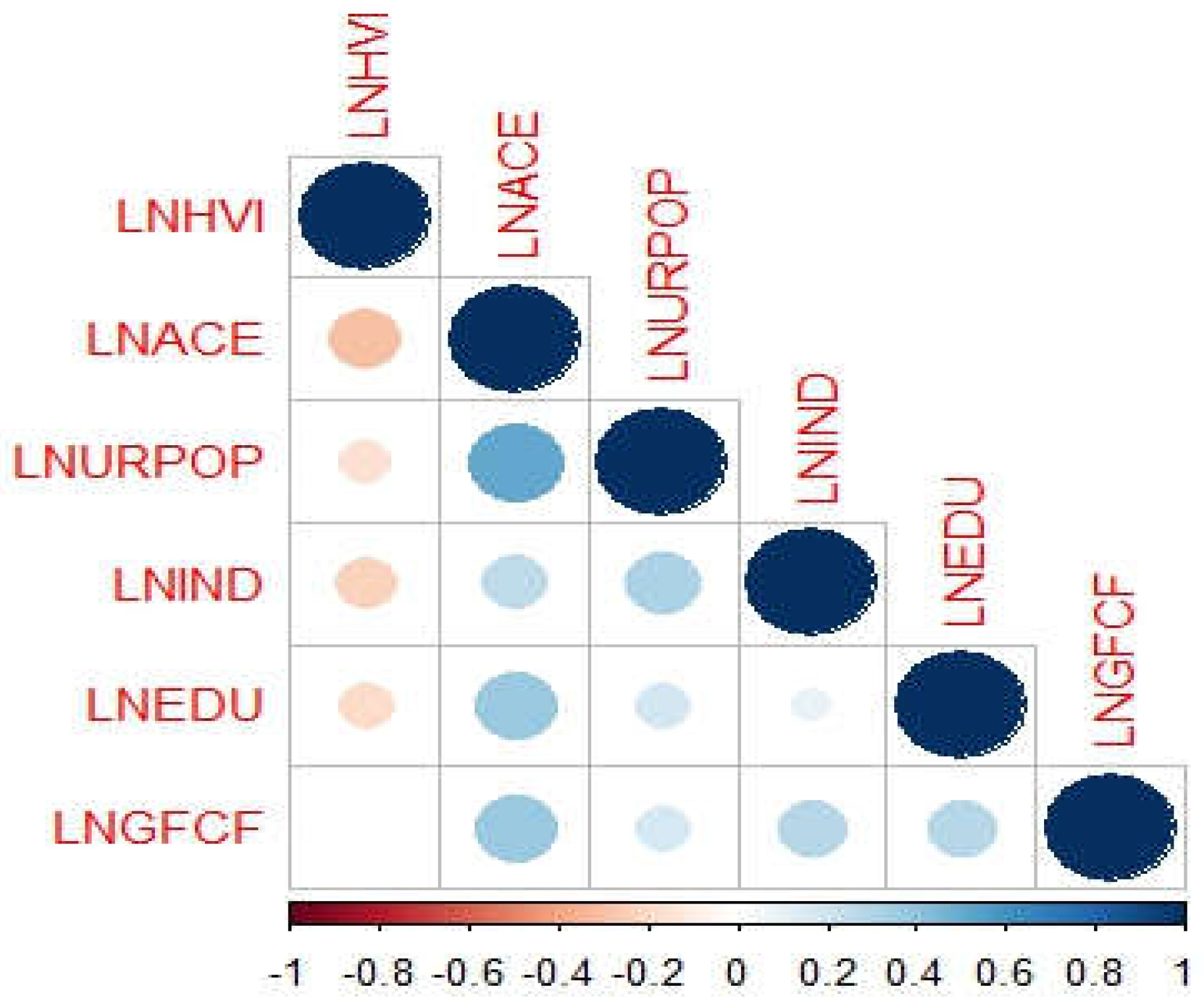
Figure 4.
Quadratic effect of electricity. This graph represents the quadratic effect of access to electricity, and it shows the access to electricity on the x-axis and health vulnerability on the y-axis.
Figure 4.
Quadratic effect of electricity. This graph represents the quadratic effect of access to electricity, and it shows the access to electricity on the x-axis and health vulnerability on the y-axis.
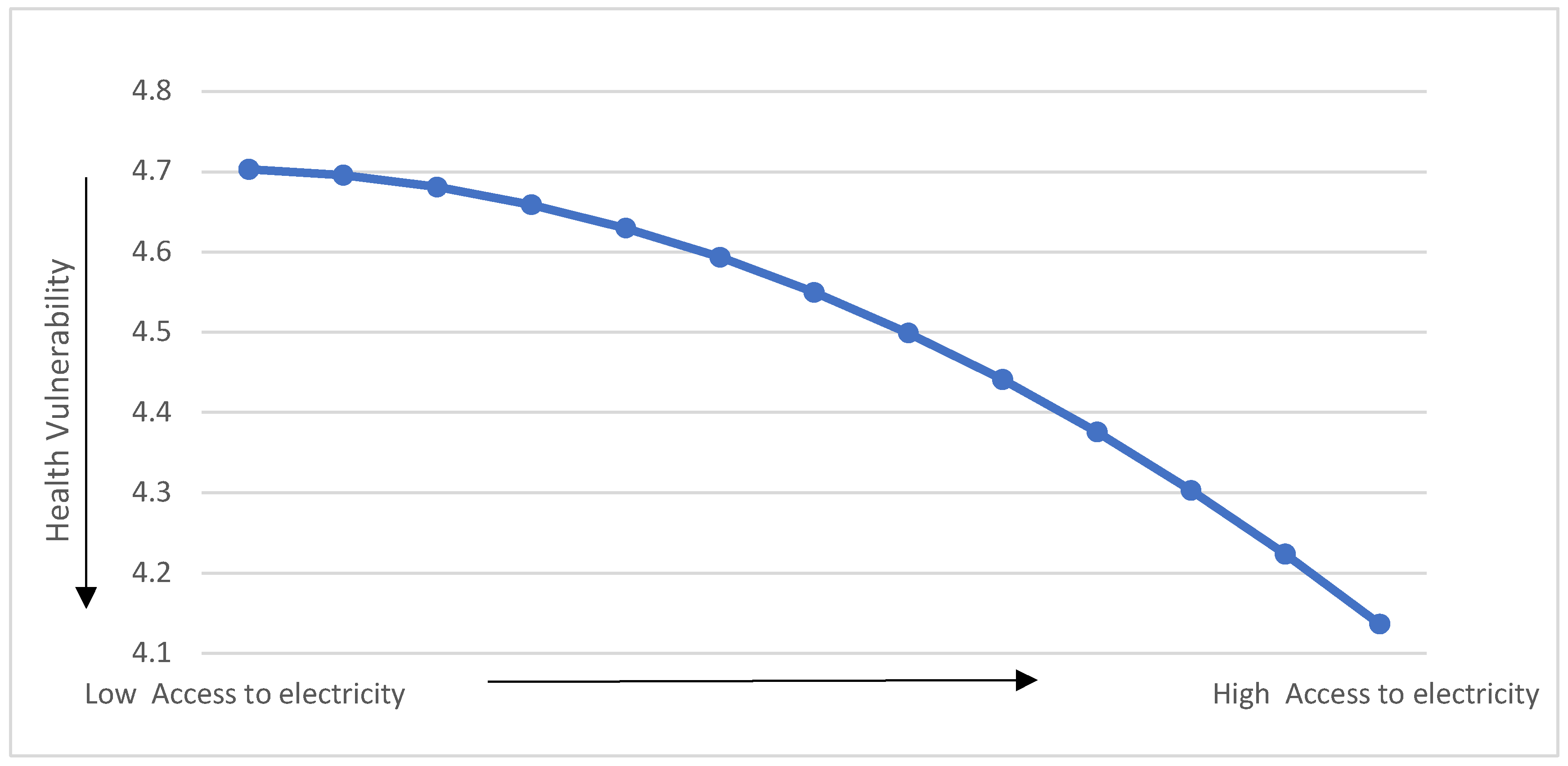

Table 1.
Variables description, units of measurement and data source.
| Symbol | Indicators | Description | Unit | Sources |
|---|---|---|---|---|
| HVI | Health vulnerability | The health vulnerability index is measured by:
|
Index | ND-GAIN |
| ACE | Access to electricity | It is the proportion of the population having an electricity facility | % of the whole population | WDI, 2022 |
| URP | Urban Population | Urban population describes the proportion of people living in metropolitan areas mentioned by the National Statistical Office. | % of the total population | WDI, 2022 |
| EDU | Primary school enrolment | The number of students, regardless of age and gender, enrol in schools in primary education. | % of total enrolment | WDI, 2022 |
| IND | Industrial value added | It is the net output of the industrial sector including mining, construction, manufacturing etc after adding all outputs and deducting all intermediate inputs. | % of GDP | WDI, 2022 |
| GFCF | Gross fixed capital formation | It is also known as gross domestic fixed investment, which is used for improving land, machinery and equipment purchases, and construction of roads, hospitals, railways, and buildings. | % of GDP | WDI, 2022 |
Table 2.
Descriptive Analysis of determinants of health vulnerability of developing countries.
| LNHVI | LNACE | LNEDU | LNGFCF | LNIND | LNURPOP | |
| Mean | 4.02 | 3.56 | 4.56 | 2.99 | 3.14 | 3.51 |
| Median | 4.11 | 3.79 | 4.61 | 3.02 | 3.20 | 3.55 |
| Maximum | 4.50 | 4.92 | 5.32 | 4.63 | 4.28 | 4.36 |
| Minimum | 2.52 | -2.49 | 3.05 | -1.23 | -1.79 | 1.69 |
| Std. Dev. | 0.36 | 0.99 | 0.27 | 0.52 | 0.45 | 0.48 |
| Skewness | -1.61 | -1.27 | -1.53 | -1.44 | -1.25 | -0.52 |
| Kurtosis | 5.93 | 4.92 | 6.85 | 10.50 | 11.27 | 2.91 |
| Jarque-Bera | 1599.65 | 853.02 | 2027.76 | 5423.34 | 6275.53 | 91.50 |
| Probability | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 |
| Sum | 8100.55 | 7169.86 | 9168.36 | 6022.18 | 6325.67 | 7075.12 |
| Sum Sq. Dev. | 255.32 | 2004.32 | 147.56 | 556.82 | 414.45 | 474.04 |
| Observations | 2015 | 2015 | 2015 | 2015 | 2015 | 2015 |
Notes: LNHVI denotes the Logarithm of the health vulnerability index; LNACE denotes the Logarithm of access to electricity; LNURPOP denotes the Logarithm of the urban population; LNEDU denotes the Logarithm of education; LNGFCF denotes the Logarithm of gross fixed capital formation; LNIND denotes Logarithm of industrialization.
Table 3.
Variance inflation factor (VIF).
| Variable | VIF | 1/VIF |
| LNACE | 1.67 | 0.60 |
| LNURPOP | 1.44 | 0.69 |
| LNGFCF | 1.26 | 0.79 |
| LNEDU | 1.2 | 0.83 |
| LNIND | 1.18 | 0.84 |
| Mean VIF | 1.35 |
Notes: LNACE denotes the Logarithm of access to electricity; LNURPOP symbolizes the Logarithm of the urban population; LNEDU denotes the Logarithm of education; LNGFCF denotes the Logarithm of gross fixed capital formation; LNIND denotes the Logarithm of industrialization.
Table 4.
Various co-integration assessments to analyze the long-term cointegrating relationship between dependent and independent variables.
Table 4.
Various co-integration assessments to analyze the long-term cointegrating relationship between dependent and independent variables.
| Kao test for cointegration | ||
| Statistic | p-value | |
| Modified Dickey-Fuller t | -6.79 | 0.000 |
| Dickey-Fuller t | -12.75 | 0.000 |
| Augmented Dickey-Fuller t | -4.39 | 0.000 |
| Unadjusted modified Dickey-Fuller t | -82.90 | 0.000 |
| Unadjusted Dickey-Fuller t | -36.42 | 0.000 |
| Pedroni test for cointegration | ||
| Modified Phillips-Perron t | -18.61 | 0.000 |
| Phillips-Perron t | -29.17 | 0.000 |
| Augmented Dickey-Fuller t | -25.16 | 0.000 |
| Westerlund test for cointegration | ||
| Variance ratio | -5.07 | 0.09 |
Table 5.
The description of Feasible Generalized Least Square Method (FGLS) results.
| Dependent variable: LNHVI | ||||
| Coef. | Std. Err. | z | P>z | |
| LNACE | 0.22 | 0.02 | 7.76 | 0.00 |
| LNACE2 | -0.05 | 0.004 | -12.08 | 0.00 |
| LNURPOP | 0.06 | 0.01 | 3.53 | 0.00 |
| LNEDU | -0.14 | 0.02 | -5.07 | 0.00 |
| LNGFCF | 0.12 | 0.01 | 8.56 | 0.00 |
| LNIND | -0.13 | 0.01 | -7.70 | 0.00 |
| _CONS | 4.48 | 0.14 | 31.44 | 0.0000 |
Notes: Number of observations:2015; Number of groups: 31; Wald chi2(6) = 523.94; Prob > chi2=0.000; LNHVI denotes Logarithm of health vulnerability index; LNACE denotes Logarithm of electrification; LNACE2 denotes Logarithm electrification square; LNURPOP denotes Log of the urban population; LNEDU: Logarithm of education; LNGFCF denotes Log of gross fixed capital formation; LNIND denotes Log of industrialization.
Table 6.
Algorithm classification criterion of access to electricity.
| Level coefficient | 0.22 |
| Quadratic coefficient | -0.058 |
| Cut-off value | 1.93 |
| Antilogarithm value | 7.37 |
Table 7.
Linearized Marginal Effect of Electrification on Health Vulnerability in.
| The Developing Countries | |||||||
| No. | Countries | Mean value of access to electricity | Net effect | No. | Countries | Mean value of access to electricity | Net effect |
| 1 | Afghanistan | 3.58 | -0.19 | 41 | Madagascar | 2.73 | -0.09 |
| 2 | Algeria | 4.59 | -0.30 | 42 | Malawi | 1.80 | 0.014* |
| 3 | Angola | 3.62 | -0.19 | 43 | Mali | 2.88 | -0.11 |
| 4 | Bangladesh | 3.67 | -0.20 | 44 | Mauritania | 3.14 | -0.14 |
| 5 | Benin | 3.16 | -0.14 | 45 | Mongolia | 4.21 | -0.26 |
| 6 | Bhutan | 4.01 | -0.24 | 46 | Morocco | 4.32 | -0.27 |
| 7 | Bolivia | 4.33 | -0.27 | 47 | Mozambique | 2.67 | -0.08 |
| 8 | Burki Faso | 2.37 | -0.05 | 48 | Myanmar | 3.84 | -0.22 |
| 9 | Burundi | 1.84 | 0.009* | 49 | Nepal | 3.70 | -0.20 |
| 10 | Cabo Verde | 4.18 | -0.26 | 50 | Nicaragua | 4.34 | -0.27 |
| 11 | Cote d’Ivoire | 3.70 | -0.20 | 51 | Niger | 2.26 | -0.03 |
| 12 | Cambodia | 3.82 | -0.22 | 52 | Nigeria | 3.83 | -0.22 |
| 13 | Cameroon | 1.85 | 0.008* | 53 | Pakistan | 4.26 | -0.27 |
| 14 | Central African R. | 1.47 | 0.05* | 54 | Papua New Guinea | 3.11 | -0.13 |
| 15 | Chad | 3.75 | -0.21 | 55 | Philippines | 4.36 | -0.28 |
| 16 | Comoros | 2.01 | -0.01 | 56 | Rwanda | 1.98 | -0.006 |
| 17 | Congo | 3.49 | -0.18 | 57 | Samoa | 4.51 | -0.29 |
| 18 | Congo (D. R.) | 3.85 | -0.22 | 58 | Sao Tome | 4.11 | -0.25 |
| 19 | Djibouti | 4.11 | -0.25 | 59 | Senegal | 3.75 | -0.21 |
| 20 | Egypt | 4.58 | -0.30 | 60 | Sierra Leone | 2.11 | -0.02 |
| 21 | El Salvador | 4.45 | -0.29 | 61 | Solomon I. | 3.54 | -0.18 |
| 22 | Eritrea | 3.47 | -0.17 | 62 | Somalia | 3.19 | -0.14 |
| 23 | Eswatini (K) | 3.42 | -0.17 | 63 | South Sudan | 0.95 | 0.11* |
| 24 | Ethiopia | 3.19 | -0.14 | 64 | Sri Lanka | 4.51 | -0.29 |
| 25 | Gambia | 3.52 | -0.18 | 65 | Sudan | 3.52 | -0.18 |
| 26 | Ghana | 3.92 | -0.23 | 66 | Syrian Arab | 4.52 | -0.30 |
| 27 | Guinea | 3.22 | -0.14 | 67 | Tajikistan | 4.56 | -0.30 |
| 28 | Guinea-Bissau | 2.37 | -0.05 | 68 | Tanzania | 2.52 | -0.06 |
| 29 | Haiti | 3.58 | -0.19 | 69 | Timor-Leste | 3.62 | -0.19 |
| 30 | Honduras | 4.28 | -0.27 | 70 | Togo | 3.19 | -0.14 |
| 31 | India | 4.21 | -0.26 | 71 | Tunisia | 4.55 | -0.30 |
| 32 | Indonesia | 4.40 | -0.28 | 72 | Uganda | 2.28 | -0.04 |
| 33 | Iran | 4.58 | -0.30 | 73 | Ukraine | 4.60 | -0.31 |
| 34 | Kenya | 3.13 | -0.13 | 74 | Uzbekistan | 4.60 | -0.30 |
| 35 | Korea (R) | 3.19 | -0.14 | 75 | Vanuatu | 3.46 | -0.17 |
| 36 | Kyrgyzstan | 4.60 | -0.30 | 76 | Viet Nam | 4.37 | -0.28 |
| 37 | Lao PDR | 4.00 | -0.24 | 77 | Yemen | 4.00 | -0.24 |
| 38 | Lebanon | 4.59 | -0.30 | 78 | Zambia | 3.11 | -0.13 |
| 39 | Lesotho | 2.78 | -0.09 | 79 | Zimbabwe | 3.57 | -0.19 |
| 40 | Liberia | 2.49 | -0.06 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



