
Submitted:
09 September 2024
Posted:
11 September 2024
You are already at the latest version
Abstract
CTC numbers in the blood of cancer patients can indicate the progression and invasiveness of tumors and their prognostic and predictive value has been repeatedly demonstrated. However, the standard baseline CTC count at the beginning of treatment, while informative, is not completely reliable and may not adequately reflect the state of the disease. The growing number of studies indicate that long-term monitoring of CTC numbers in the same patient provides more comprehensive prognostic data and should be incorporated into clinical practice, as a factor that contributes to therapeutic decisions. This Review describes the current status of CTC enumeration as a prognostic and predictive factor, highlights the shortcomings of current solutions and advocates for longitudinal CTC analysis as a more effective method of the evaluation of developing disease, treatment efficacy, and long term-monitoring of the minimal residual disease.
Keywords:
circulating tumor cells
; longitudinal analysis
; CTC dynamics
1. Introduction
CTC enumeration is a well-documented prognostic and predictive biomarker in cancer management, but its implementation in clinical practice is still ongoing and encounters technical, logistic, and conceptual problems. Apart from the fact that CTC detection techniques need standardization and improvement, CTC enumeration is quite expensive and, while not very aggravating for patients, it requires skills and resources to meet the standards of clinical diagnostics. Improving its prognostic and predictive value would give clinicians more reliable tool, useful for therapeutic decisions. While technical improvements in CTC detection, classification and enumeration is one avenue of research that leads to this goal, the other one might be a longitudinal monitoring of the patient. As shown in this Review, data from serial blood collections are more reliable than only one, baseline evaluation, and enable to track the progress of the disease.
2. The Current Status of CTC Research
2.1. Old and New Blood-Based Cancer Biomarkers for Screening and Progression
Tumor biomarkers have critical value in cancer screening, early diagnosis, recurrence detection, and therapeutic monitoring. They are diverse and can be detected in blood, tissue samples, and biofluids (saliva, feces, urine). There are several known blood-derived tumor biomarkers, including tumor specific antigens: PSA (prostate-specific antigen), SCCA (squamous cell carcinoma antigen), AFP (alpha-fetoprotein specific to hepatocellular carcinoma), CA125 (glycosylated mucin specific mostly to ovarian cancer), CA19-9 (carbohydrate antigen 19-9, pancreatic and colorectal cancer), LDH (lactate dehydrogenase, melanoma, renal and colorectal cancer) and less specific ones such as CEA (carcinoembryonic antigen) or CA 15-3 (carbohydrate antigen 15-3, mucin) (see Reviews on tumor biomarkers [1,2]). Some biomarkers, such as, for example, CEA and CA15-3 in breast cancer, are associated with recurrence and metastasis [3] . However, the efficacy of these classic biomarkers is limited [4,5,6] and recently novel biomarkers have been introduced, including circulating tumor DNA (ctDNA) and circulating tumor cells. These new biomarkers, although still undergoing clinical trials or preclinical studies, have great potential for becoming a significant part of clinical practice and can improve the efficiency of treatment. There are several possible applications of CTC-based information in the clinic: screening and early detection of the tumor, early indication of the recurrence in postoperative patients, and the monitoring of the advanced disease. Molecular data acquired during CTC analysis (e.g., expression profiling or mutational analysis) can be used for the identification of new therapeutic targets, identifying the mechanisms of resistance, and, in general, tailoring the therapeutic response to the specific patient, paving the way to personalized medicine.
2.2. Biology and the Role of CTCs in the Metastatic Process
CTCs are extremely rare and difficult to observe, so despite the fact that they were first noticed in 1869 [7] most of our knowledge about them has been gathered in the last two decades. Due to the current development of the techniques of CTC detection we are able to not only detect and enumerate, but also isolate and characterize CTCs from the blood of the patients.
CTCs can be classified as single CTCs and CTC clusters, including homotypic clusters composed of tumor cells and heterotypic clusters with immune cells [8]. Several reports indicated that CTC clusters are more metastatic [9,10,11], but because of their rarity, there are only few reports on their clinical significance [12,13].
Many reports and clinical trials have demonstrated that CTC numbers are predictive and prognostic (described in Chapter 2.3), but we still need to gain a deep understanding of the importance of CTC dynamics and the correlation between CTC status and disease progression. Our current understanding of the metastatic cascade assigns the role of ‘metastatic seeds’ to CTCs, but this is true only for a very small fraction of these cells (0.01%, [14,15],). The fact that the high number of CTC in the advanced, metastatic disease is prognostic and predictive is probably due to a simple fact that progressing metastatic lesions produce and – proportionally – shed more cells, but it may also signify additional dissemination and seeding of new metastatic sites, which contributes to the metastatic burden. In postoperative disease, the increase in the numbers may reflect the fact that the disseminated cells started proliferation, creating a true macro-metastatic lesion, which is associated with shedding some of these cells to the bloodstream. In both cases, close monitoring of the CTC numbers should act as a warning sign preceding any clinical manifestation, and its detection should help in therapeutic decisions.
2.3. Molecular Characteristics of CTCs
Many reports focused on the molecular characteristics of isolated CTCs, as a way to determine specific changes in these cells toward a more metastatic phenotype, especially compared to primary tumor cells. If included in standard clinical practice, this may be a step towards personalized medicine. The characterized features included specific mutations [16,17,18], the EMT score [19,20,21], the expression of EpCAM and stem cell markers [22,23], DNA methylation dynamics [24,25,26] or the whole expression profile [27,28,29].
Several reports highlight the discrepancies between the genetic status of the primary tumor and CTCs; some characterize specific activating mutations that occur in CTC, which are not present in the primary tumor, for example, in luminal breast cancer, in the which mutations in ESR1 and PIK3CA genes are associated with resistance to hormonal therapy [30,31]. Mutational studies based on ctDNA, probably have a better clinical perspective than those based on CTCs, because of simpler procedure with similar significance [32,33,34].
From the accumulated studies on genotypic and phenotypic variability of CTC, we can conclude that CTCs are very heterogeneous, even within the same patient [18,23,35].This may reflect the initial heterogeneity of the primary tumor or changes that occur in secondary lesions, since in the metastatic setting the detected cells/DNA are derived from metastases.
Molecular analysis of CTCs is important from the perspective of basic scientific knowledge but also potentially holds clinical utility; further analyses of CTC biology, heterogeneity, and phenotypic plasticity should demonstrate the feasibility of including it into clinical evaluation.
2.4. Clinical Significance of CTC Enumeration and Profiling
Based on the accumulated evidence on the importance of CTCs as a prognostic marker in many cancers, researchers study the utility of CTC enumeration in the clinical settings. Several multicenter prospective clinical trials were performed, but only some ended with definitive positive results that may be helpful in the clinic. Currently, worldwide clinical guidelines do not consider the use of CTCs, (except the inclusion of CTCs for cM0 classification), however gained data predict their great potential in clinical applications.
Most data on the presence of CTCs were obtained in studies of the best investigated breast cancer (BC). In a pooled analysis of 3,173 patients with localized BC from 5 centers, with the cut-off set on ≥1 CTCs/7.5 ml of blood, the CTC count has been identified as an independent prognostic factor for disease-free survival ( DFS) and overall survival (OS) [36].
In another large trial in 1,697 early BC patients, a benefit of radiotherapy in the adjuvant setting for patients with detectable CTCs was shown [37]. The association between CTC presence during neoadjuvant settings (preneoadjuvant chemotherapy and presurgery) and OS or DSF has been reported in many recent studies [38]. Furthermore, CTCs detected in minimal residual disease (MRD) after removal of the primary tumor or ending of neoadjuvant treatment, when clinical parameters show a lack of active disease, may earlier predict recurrences [36].
In metastatic breast cancer (MBC) a number of ≥5 CTCs was set as correlated with poor survival [39]. The development of the disease and the response to therapy can be monitored by the CTC number. Cristofanilli et al. have shown that CTC levels and the dynamics of CTCs over time help to identify high-risk MBC patients. In a retrospective study of 2,436 MBC patients from 18 centers, they have demonstrated that CTC numbers are useful for the stratification of patients with advanced disease. Stage IVindolent patients ( <5CTC) had longer OS than those in stage IV aggressive (36.3 months vs. 16 months) independently of the disease subtype [40].
Numerous clinical trials were conducted to address the issue of CTCs that serve as a biomarker; in some of these trials, CTCs were only enumerated (SWOG S0500, [41] STIC CTC, https://doi.org/10.1158/1538-7445.SABCS18-GS3-07 [42] whereas in other a their phenotype was assessed (CirCe T-DM1 trial [43]. DETECT study, https://doi.org/10.1200/JCO.2016.34.15_suppl.TPS634 [44] These trials and other ongoing phase III and phase II clinical trials are overviewed and summarized in the reviews by Lin et al. [45] and Stoecklein et al. [46].
In many solid cancers an analogous correlation between CTC number and poor prognosis has been observed. The prognostic value of CTC for OS in localized colorectal cancer was observed in some studies and confirmed in a meta-analysis that included 3,687 patients from 20 centers. [47]. Another meta-analysis performed in 1,329 patients with metastatic CRC showed that OS and PFS decreased in patients with CTC [48]. The same conclusion was drawn from other studies and meta-analysis [49,50]. All data obtained in early and advanced CRC suggested a worse prognosis in the presence of CTCs.
The same observations have been made for lung cancer [51,52,53,54], prostate cancer [55], melanoma [56], and head and neck cancer [57].
The risk of recurrence correlates with the number of CTCs, more CTCs indicate a higher risk of recurrence, while decrease or clearance of CTCs correlates with good therapeutic response. However, in the phase III SUCCESS study, approximately 88% of patients with a high number of CTC did not show recurrence and metastatic progression after 36 months of follow-up [58]. The patients in this trial were treated with chemotherapy depending on the presence of CTCs. This result highlights the problem of overtreatment of many patients who may unnecessarily suffer side effects from redundant chemotherapy. Inversely, some patients with undetectable or low number of CTC will develop distant metastasis. Therefore, there is a great need for deeper CTC characteristics and additional biomarkers.
The other problem is that some studies have shown that changes in CTC number during therapy do not correspond to responses criteria defined in the RECIST (Response Evaluation Criteria in Solid Tumors guidelines) [59]. Therefore, the CTCs enumeration has not been included in the RECIST guidelines yet.
2.5. Shortcomings of a Single, Non-Recurrent CTC Analysis
Despite all the efforts and achievements presented in the previous chapter, the clinical utility of CTCs is still hindered by inconsistencies, from technical difficulties in standardization to more theoretical questions about the reliability of the zero CTC count in a single blood draw. These issues should be addressed, if CTC count is to become a reliable clinical tool.
2.5.1. The Methodology of CTC Detection Requires Standardization
Although CTC research has made a huge technological leap in the last two decades, there are still unsolved issues due to inconsistencies in protocols and differences in various detection systems. The two FDA-approved systems, CellSearch and Parsortix, differ in the principle of detection, which inevitably leads to the characterization of different subpopulations of CTCs, depending on the method.
Most of the results of CTC enumeration are obtained with CellSearch [60], the first FDA-approved system (in January 2004) for the detection and monitoring of CTCs in patients. The CellSearch method is based on immunoaffinity to EpCAM (Epithelial Cell Adhesion Molecule), and captures only cells with epithelial features, potentially omitting EpCAM-low and negative CTCs.
The second most popular system for the capture and harvest of CTCs - Parsortix PC1 - was approved by FDA in May2022. The Parsortix system uses a microfluidic technology enabling epitope-independent capture of all CTC phenotypes based on cell size and deformability, allowing for CTC enumeration and subsequent downstream analysis [61]. This system is currently being evaluated in many studies and clinical trials, as reviewed in Wishart et al., [62].
EpCAM-dependent enrichment was found more specific and suitable for clinical applications than size-dependent, label-free approaches, but the latter were found to be more suitable for molecular characterization [63]. The heterogeneity of CTC results in significant variations in surface biomarker expression [22,64], so the uniform recognition of all types of CTCs by labeling-dependent methods, using identical standard is impossible. Size-dependent or image-based approaches include subpopulations that may be lost in the EpCAM-dependent CellSearch system, namely cells after EMT, clusters and CTCs masked by the other types of cells. However, it has also been reported that since the CTCs are fragile, some methods of detection, particularly size-based, may damage them [65].
Additionally, there are many other systems, label-dependent, size-dependent or image-based, that do not have FDA approval and are used only for research (reviewed in [65,66,67]). In conclusion, it is necessary to establish maximally standardized protocols and address the problem of the group of cancers in which CTCs do not express EpCAM.
2.5.2. Fluctuations in CTC Numbers Depend on Circadian Rhythm, Clinico-Pathological Features and Therapeutic Interventions
The release of CTC from the tumor is not constant and may differ not only between different patients with comparable disease status, but also within the same patient at different time points. Moreover, it was demonstrated that CTCs can clear within minutes after release into the bloodstream [68], so the timing of the blood draw can be crucial. Several factors have been considered to promote the release of CTC. Donato et al. [69] have demonstrated that intravasation of highly metastatic CTC clusters is caused by hypoxia. There are also reports suggesting that CTC release may be regulated by the circadian rhythm and accelerates during the rest phase [70,71,72].
Several reports highlight the possibility that CTC shedding may be associated with specific treatment [73]. Surgical intervention was shown to increase the number of CTCs [74,75,76,77]. This effect may confuse statistical significance of the results, and should be considered for baseline time selection. Pang et al., [78] observed that CTCs measured up to the seventh day after surgery did not affect PFS and OS, while CTCs measured on day 14 after surgery were related to PFS. They concluded that the time point of the CTC measurement affects the prognostic value.
The increase in CTC number has been also reported after radiation therapy [79], and after needle biopsy [80,81], prompting the question if the mobilization of CTCs during cancer therapy may cause metastasis [82]. These data suggest that therapeutic intervention may inadvertently contribute to tumor cell dissemination, which could be counter-productive. This prompts the question whether we should address this problem on the clinical level, by, for example, introducing some perioperative course of cytotoxic or other CTC-targeting treatment?
The concerns of therapy-induced CTC mobilization were also expressed with respect to chemotherapy, although, due to the variability of the available treatments, these responses are more complex. Ito et al. [83] reported CTC mobilization after chemotherapy in xenograft mouse model of human pancreatic cancer. Ortiz-Otero et al. [84] reported chemotherapy-induced CTC release in metastatic cancer patients with a spectrum of cancer types.
On the other hand, many reports have shown that CTC numbers decrease after treatment. For example, Vetter et al. [85] demonstrated that denosumab treatment of metastatic BC significantly reduced the number of CTCs in patients’ blood. Denosumab is a monoclonal antibody against the receptor activator of the nuclear factor-κB ligand (RANKL). It suppresses osteoclasts and prevents bone resorption, mitigating the effects of breast cancer bone metastasis.
Bendahl et al. [86] also observed the decline of CTC numbers in small cell lung cancer, after standard chemotherapy, and Lozano et al., [87] observed the same effect upon docetaxel treatment in metastatic castration-resistant prostate cancer (mCRPC) patients. In this last case, early CTC decline after treatment was demonstrated to be a better predictor of survival than PSA.
The decline in CTC numbers after the therapy is usually interpreted as a sign of the efficacy of the specific treatment, which advocates using this parameter for therapy monitoring. Numerous reports indicate that persistent high CTC count during chemotherapy is prognostic, as well as low/none CTC numbers, which is a favorable treatment response (see Chapter 3).
3. Principles and Advantages of Longitudinal Analysis
To address some of the problems and challenges described in the previous chapter, Cristofanilli et al. [39] in an early study from 2004 on MBC attempted a more systematic approach and included a follow-up blood collection in addition to the baseline. They observed that CTC monitoring during treatment provided additional information. This was confirmed by the pooled study by Bidard et al. [88], in which the authors reported that CTC changes during treatment are significant for PFS and OS, and indicated that tracking CTC changes improves prognostic accuracy. This observation was followed by more articles with the baseline and the follow-up count, exploring the question of the clinical value of the follow-up count [41,89]. As a natural consequence, some other teams followed the obvious path of exploring wheather more blood collections are even more informative and clinically useful.
3.1. Serial Monitoring of CTC Dynamic in a Single Patient is Prognostically Superior to Single or Baseline/Follow-Up Blood Collection
CTC reports with more than two blood collections are still not very frequent, since they require much more work, coordination and cooperation with the clinic. Despite the greater workload and the level of complication, the number of longitudinal reports is increasing and they repeatedly demonstrate the usefulness of longitudinal studies. While most reports focus on CTC numbers, some reports include molecular analysis of isolated CTCs, which enables to trace genetic and phenotypic changes in some cancer-specific markers.
Gerratana et al., [90] investigated comparatively CTC count in longitudinal setting and ctDNA analysis for MBC monitoring. The CTCs were analyzed in 74 patients, with three blood collections: baseline, evaluation and progression. The authors observed an increase in CTC numbers only at progression. They also expressed an interesting opinion that while both, CTC enumeration and ctDNA characterization provided prognostic information, CTC numbers are more related to the underlying metastatic biology, whereas ctDNA provides a more quantitative assessment of tumor burden.
Szostakowska-Rodzos et al., [91] studied the dynamics of CTC numbers in a longitudinal study with three subsequent blood collections (every 3 months) from the 135 MBC patients. Statistical analysis demonstrated that constantly increasing CTC numbers are unfavorable, while the constant low (<5) CTC count is a strong favorable predictor for PFS and OS. These results indicate that the dynamics of CTC changes provides an additional, clinically important information.
Some reports focus not only on single CTCs but also take into account the numbers and prognostic value of CTC clusters. Larssen et al., [12] in a prospective observational trial analyzed CTCs/CTC clusters from 156 patients with MBC. They have analyzed CTC numbers from the baseline and the three subsequent blood collections (after 1,3 and 6 months). The results indicate that the prognostic value of CTC count ≥ 5 CTCs and CTC cluster evaluation increases over time, suggesting that the dynamic of CTCs and CTC clusters are more relevant to prognosis than a single baseline enumeration and that the presence of CTC clusters adds to prognostic value. Wang et al., [13] came to the same conclusions in their longitudinal study of MBC in which they also analyzed CTC clusters. They also observed that a larger-size CTC-cluster conferred a higher risk of death.
Longitudinal analysis not only provides the information concerning changes in CTC numbers in the same patient, but also allows for some additional analyzes, for example it enables to trace the evolution of the status of the selected markers. Forsare et al., [92] studied comparatively estrogen receptor (ER) status in primary tumor (PT) and CTCs in 147 breast cancer patients. ER expression has been evaluated in CTCs at baseline and after 1 and 3 months of endocrine therapy. The authors demonstrated a shift from ER positivity to negativity between PT and CTCs at different time points. They proposed that ER positivity of CTCs reflects the retention of a favorable phenotype that still responds to therapy, and as such, can be clinically useful.
Phenotypic plasticity was also observed by Cohen et al., [93]. The authors performed a microcavity array platform (size-based approach) to count and characterize CTCs from 184 MBC patients at up to 9 time points at 3-month intervals. Taking advantage of their approach, without bias towards epithelial characteristics, they observed that a shift from an epithelial to a mesenchymal expression pattern in the isolated CTCs is associated with inferior clinical outcomes.
Stergiopoulou et al., [94] reported molecular characterization of isolated CTCs as a tool for the early detection of minimal residual disease (MRD) in breast cancer. The study describes long-term CTC monitoring (up to 126 months) with a very comprehensive analysis of isolated CTCs (enumeration, phenotypic analysis, gene expression analysis, mutation analysis in CTCs and the corresponding plasma ctDNA, DNA methylation analysis) performed in 13 patients. The authors conclude that this type of analysis can reveal the presence of MRD 4 years before the appearance of clinically detectable metastasis. This proves that molecular characterization of CTCs holds a huge clinical potential.
Although breast cancer is the most studied, the other types are also explored. For example, Hendricks et al. [95] presented a prospective pilot study in which they monitored a cohort of 44 colorectal cancer (CRC) patients of miscellaneous tumor stages with as much as five blood collections in addition to the baseline. The study analyzes complicated kinetics of CTC in CRC patients after resection of the primary tumor and provides data concerning the CTC quantity over a long-term follow-up.
In a pursuit for a novel, more sensitive biomarker for MRD Ko et al., [96] performed a longitudinal analysis of CTCs (with four timepoints) in 21 metastatic patients with nasopharyngeal carcinoma (NPC). While limited with small sample-size and short follow-up time, this study also indicated the association of the CTC numbers with PFS and demonstrated that CTC detection could be a more sensitive tool for tracking MRD than standard methods (plasma EBV assay, PET-CT).
3.2. Clinical Relevance of Long Monitoring in Relation to Treatment
Usually, blood collection timepoints are designed to match significant clinical factors, such as the beginning of a new treatment or the scheduled clinical or radiological evaluation. This coordination of CTC enumeration with clinical procedures enables to evaluate the response to therapy. Establishing CTC count as an early predictor of progression and as a tool for systematic monitoring of the treatment efficacy is one of the main goals of these research. Consequently, several reports addressed the issue of longitudinal monitoring and its clinical value for ongoing treatment. The reports published so far indicate that CTC monitoring can be used as a complementary tool to the clinical evaluation as the basis for determining treatment efficacy and treatment choices.
Pang et al., [78] addressed the question of the optimal time points for CTC analysis in a study of 110 breast cancer patients in relation to treatment. Their study revealed that the most significant correlation between CTC numbers and PFS and OS is observed for the baseline and the end-point of follow-up collection, while CTCs detected before chemotherapy were only related to PFS. Furthermore, the numbers of CTCs at the last adjuvant chemotherapy were more correlated with prognosis than those before adjuvant chemotherapy. As mentioned before, they have also observed post-operative variability in CTC numbers, which indicates that this time point is unreliable.
Another recent study on MBC by Magbanua et al., [97] has been carried out with three or more serial blood draws from 469 patients for CTCs enumeration. In this study the data collected from patients were divided into 3 models used for PFS and OS endpoints estimation. The data from baseline blood collection (bCTC) which was drawn at the new cycle of chemotherapy was compared with the data at the end of the chemotherapy cycle to estimate the change in CTCs (cCTC). Survival analysis showed that patients negative for CTC at both time points had significantly higher median PFS than patients with CTCs in any or all time points. Moreover, the data from all collections were used for the CTC trajectory (tCTC) model development, which enables to estimate the trend of CTCs numbers during treatment: high, mid, low and negative. The results of this study showed that the patients with negative tCTC (without CTCs) had better prognosis for PFS and OS and that patients with tCTC high had the worst prognosis for PFS and OS.
In another study form the same group, Magbanua et al., [98] evaluated the prognostic and predictive value of CTC monitoring in hormone receptor–positive metastatic breast cancer. The patients were randomized to letrozole alone or letrozole plus bevacizumab in the first-line setting . The authors studied data from 294 patients at the baseline and in the three subsequent blood collections (before every third bevacizumab cycle and approximately 21-day intervals in the letrozole only arm). They have found that CTCs were highly prognostic for the addition of bevacizumab to first-line letrozole.
The study by Bendahl et al., [86] explored the prognostic value of CTC presence in small cell lung cancer (SCLC) and assessed the dynamics of CTCs in longitudinal samples from a patient cohort from the RASTEN phase III trial, a randomized controlled study designed to estimate the survival benefit of the addition of low-molecular-weight heparin (LMWH) to standard chemotherapy. Baseline blood collection and two other blood collections were performed in 42 patients with limited and extensive disease (even subgroups, 50%). The study demonstrated that the persistent presence of CTC during and after completion offers additional prognostic information in addition to baseline CTC.
The study by Ko et al., [99] (from the same group as in previously described study of MRD in NPC) provides the data of serial monitoring of treatment outcomes for locally advanced esophageal squamous cell carcinoma (ESCC). The 88 patients included in this analysis received neoadjuvant treatment and curative resection treatment and the goal was to establish whether CTC enumeration can be used as a tool for the prediction of treatment efficacies, prognostication and real-time tracking of MRD for earlier detection of the relapse. The authors concluded the clinical usefulness of specific time points of CTC detection, namely: pretreatment, post-treatment/presurgery, 1 month and 3-month post-surgery.
4. Conclusions
Longitudinal monitoring of CTCs holds the promise of a better, more sensitive and earlier prediction of the relapse or the development of drug resistance. The serial CTC count in patients during treatment should become a useful tool for monitoring and predicting tumor progression and guide treatment choices. As described in this Review, these type of studies (summarized in Table 1) repeatedly demonstrate the usefulness of CTC count in real-time treatment monitoring and risk stratification strategy, with the persistent high CTC count as strongly unfavorable and low/none CTC count strongly favorable factors. Incorporation of these assays in clinical practice (as proposed in Figure 1) should be highly beneficial. Molecular analysis of isolated CTCs also offers potential clinical benefits, providing more insight into the current state and the evolution of the disease. The CTC count was also investigated as a tool for long-term monitoring of MRD. These results form a reliable base for introducing CTC-based information in clinical practice.
CTC count at the baseline is prognostic, and may contribute to the choice of the more or less aggressive therapy, but cannot provide information about the efficiency of the treatment in the specific patient. During the subsequent evaluations of progression CTC count can serve as a complementary factor, with a persistent high/low CTC numbers as an indicator of the response to the treatment.
Funding
This research was funded by Narodowe Centrum Nauki, grant number 2016/21/B/NZ2/03473.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Zhou, Y.; Tao, L.; Qiu, J.; Xu, J.; Yang, X.; Zhang, Y.; Tian, X.; Guan, X.; Cen, X.; Zhao, Y. Tumor biomarkers for diagnosis, prognosis and targeted therapy. Signal Transduct Target Ther 2024, 9, 132. [Google Scholar] [CrossRef] [PubMed]
- Das, S.; Dey, M.K.; Devireddy, R.; Gartia, M.R. Biomarkers in Cancer Detection, Diagnosis, and Prognosis. Sensors (Basel) 2023, 24. [Google Scholar] [CrossRef]
- Uygur, M.M.; Gumus, M. The utility of serum tumor markers CEA and CA 15-3 for breast cancer prognosis and their association with clinicopathological parameters. Cancer Treat Res Commun 2021, 28, 100402. [Google Scholar] [CrossRef]
- Sekiguchi, M.; Matsuda, T. Limited usefulness of serum carcinoembryonic antigen and carbohydrate antigen 19-9 levels for gastrointestinal and whole-body cancer screening. Sci Rep 2020, 10, 18202. [Google Scholar] [CrossRef] [PubMed]
- Duffy, M.J.; Evoy, D.; McDermott, E.W. CA 15-3: uses and limitation as a biomarker for breast cancer. Clin Chim Acta 2010, 411, 1869–1874. [Google Scholar] [CrossRef]
- Varzaru, V.B.; Eftenoiu, A.E.; Vlad, D.C.; Vlad, C.S.; Moatar, A.E.; Popescu, R.; Cobec, I.M. The Influence of Tumor-Specific Markers in Breast Cancer on Other Blood Parameters. Life (Basel) 2024, 14. [Google Scholar] [CrossRef]
- T.R., A. A Case of Cancer in Which Cells Similar to Those in the Tumours Were Seen in the Blood after Death. The Medical Journal of Australia 1869, 14, 146–147. [Google Scholar]
- Szczerba, B.M.; Castro-Giner, F.; Vetter, M.; Krol, I.; Gkountela, S.; Landin, J.; Scheidmann, M.C.; Donato, C.; Scherrer, R.; Singer, J.; et al. Neutrophils escort circulating tumour cells to enable cell cycle progression. Nature 2019, 566, 553–557. [Google Scholar] [CrossRef] [PubMed]
- Cheung, K.J.; Padmanaban, V.; Silvestri, V.; Schipper, K.; Cohen, J.D.; Fairchild, A.N.; Gorin, M.A.; Verdone, J.E.; Pienta, K.J.; Bader, J.S.; et al. Polyclonal breast cancer metastases arise from collective dissemination of keratin 14-expressing tumor cell clusters. Proc Natl Acad Sci U S A 2016, 113, E854–863. [Google Scholar] [CrossRef]
- Aceto, N.; Bardia, A.; Miyamoto, D.T.; Donaldson, M.C.; Wittner, B.S.; Spencer, J.A.; Yu, M.; Pely, A.; Engstrom, A.; Zhu, H.; et al. Circulating tumor cell clusters are oligoclonal precursors of breast cancer metastasis. Cell 2014, 158, 1110–1122. [Google Scholar] [CrossRef]
- Wei, R.R.; Sun, D.N.; Yang, H.; Yan, J.; Zhang, X.; Zheng, X.L.; Fu, X.H.; Geng, M.Y.; Huang, X.; Ding, J. CTC clusters induced by heparanase enhance breast cancer metastasis. Acta Pharmacol Sin 2018, 39, 1326–1337. [Google Scholar] [CrossRef] [PubMed]
- Larsson, A.M.; Jansson, S.; Bendahl, P.O.; Levin Tykjaer Jorgensen, C.; Loman, N.; Graffman, C.; Lundgren, L.; Aaltonen, K.; Ryden, L. Longitudinal enumeration and cluster evaluation of circulating tumor cells improve prognostication for patients with newly diagnosed metastatic breast cancer in a prospective observational trial. Breast Cancer Res 2018, 20, 48. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Mu, Z.; Chervoneva, I.; Austin, L.; Ye, Z.; Rossi, G.; Palazzo, J.P.; Sun, C.; Abu-Khalaf, M.; Myers, R.E.; et al. Longitudinally collected CTCs and CTC-clusters and clinical outcomes of metastatic breast cancer. Breast Cancer Res Treat 2017, 161, 83–94. [Google Scholar] [CrossRef] [PubMed]
- Chambers, A.F.; Groom, A.C.; MacDonald, I.C. Dissemination and growth of cancer cells in metastatic sites. Nat Rev Cancer 2002, 2, 563–572. [Google Scholar] [CrossRef]
- Merino, D.; Weber, T.S.; Serrano, A.; Vaillant, F.; Liu, K.; Pal, B.; Di Stefano, L.; Schreuder, J.; Lin, D.; Chen, Y.; et al. Barcoding reveals complex clonal behavior in patient-derived xenografts of metastatic triple negative breast cancer. Nat Commun 2019, 10, 766. [Google Scholar] [CrossRef]
- Mego, M.; Karaba, M.; Sedlackova, T.; Benca, J.; Repiska, G.; Krasnicanova, L.; Macuch, J.; Sieberova, G.; Jurisova, S.; Pindak, D.; et al. Circulating tumor cells and breast cancer-specific mutations in primary breast cancer. Mol Clin Oncol 2020, 12, 565–573. [Google Scholar] [CrossRef]
- Wang, Q.; Zhao, L.; Han, L.; Tuo, X.; Ma, S.; Wang, Y.; Feng, X.; Liang, D.; Sun, C.; Wang, Q.; et al. The Discordance of Gene Mutations between Circulating Tumor Cells and Primary/Metastatic Tumor. Mol Ther Oncolytics 2019, 15, 21–29. [Google Scholar] [CrossRef]
- D'Oronzo, S.; Lovero, D.; Palmirotta, R.; Stucci, L.S.; Tucci, M.; Felici, C.; Cascardi, E.; Giardina, C.; Cafforio, P.; Silvestris, F. Dissection of major cancer gene variants in subsets of circulating tumor cells in advanced breast cancer. Sci Rep 2019, 9, 17276. [Google Scholar] [CrossRef]
- Genna, A.; Vanwynsberghe, A.M.; Villard, A.V.; Pottier, C.; Ancel, J.; Polette, M.; Gilles, C. EMT-Associated Heterogeneity in Circulating Tumor Cells: Sticky Friends on the Road to Metastasis. Cancers (Basel) 2020, 12. [Google Scholar] [CrossRef]
- Chen, Y.; Li, S.; Li, W.; Yang, R.; Zhang, X.; Ye, Y.; Yu, J.; Ye, L.; Tang, W. Circulating tumor cells undergoing EMT are poorly correlated with clinical stages or predictive of recurrence in hepatocellular carcinoma. Sci Rep 2019, 9, 7084. [Google Scholar] [CrossRef]
- Vardas, V.; Politaki, E.; Pantazaka, E.; Georgoulias, V.; Kallergi, G. Epithelial-to-mesenchymal transition of tumor cells: cancer progression and metastasis. Int J Dev Biol 2022, 66, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Gires, O.; Stoecklein, N.H. Dynamic EpCAM expression on circulating and disseminating tumor cells: causes and consequences. Cell Mol Life Sci 2014, 71, 4393–4402. [Google Scholar] [CrossRef] [PubMed]
- Agnoletto, C.; Corra, F.; Minotti, L.; Baldassari, F.; Crudele, F.; Cook, W.J.J.; Di Leva, G.; d'Adamo, A.P.; Gasparini, P.; Volinia, S. Heterogeneity in Circulating Tumor Cells: The Relevance of the Stem-Cell Subset. Cancers (Basel) 2019, 11. [Google Scholar] [CrossRef]
- Gkountela, S.; Castro-Giner, F.; Szczerba, B.M.; Vetter, M.; Landin, J.; Scherrer, R.; Krol, I.; Scheidmann, M.C.; Beisel, C.; Stirnimann, C.U.; et al. Circulating Tumor Cell Clustering Shapes DNA Methylation to Enable Metastasis Seeding. Cell 2019, 176, 98–112.e114. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Wu, X.; Zheng, J.; Dong, D. DNA methylome profiling of circulating tumor cells in lung cancer at single base-pair resolution. Oncogene 2021, 40, 1884–1895. [Google Scholar] [CrossRef]
- Markou, A.; Londra, D.; Tserpeli, V.; Kollias, I.; Tsaroucha, E.; Vamvakaris, I.; Potaris, K.; Pateras, I.; Kotsakis, A.; Georgoulias, V.; et al. DNA methylation analysis of tumor suppressor genes in liquid biopsy components of early stage NSCLC: a promising tool for early detection. Clin Epigenetics 2022, 14, 61. [Google Scholar] [CrossRef]
- Chang, Y.; Wang, Y.; Li, B.; Lu, X.; Wang, R.; Li, H.; Yan, B.; Gu, A.; Wang, W.; Huang, A.; et al. Whole-Exome Sequencing on Circulating Tumor Cells Explores Platinum-Drug Resistance Mutations in Advanced Non-small Cell Lung Cancer. Front Genet 2021, 12, 722078. [Google Scholar] [CrossRef]
- Manier, S.; Park, J.; Capelletti, M.; Bustoros, M.; Freeman, S.S.; Ha, G.; Rhoades, J.; Liu, C.J.; Huynh, D.; Reed, S.C.; et al. Whole-exome sequencing of cell-free DNA and circulating tumor cells in multiple myeloma. Nat Commun 2018, 9, 1691. [Google Scholar] [CrossRef] [PubMed]
- Si, J.; Huang, B.; Lan, G.; Zhang, B.; Wei, J.; Deng, Z.; Li, Y.; Qin, Y.; Li, B.; Lu, Y.; et al. Comparison of whole exome sequencing in circulating tumor cells of primitive and metastatic nasopharyngeal carcinoma. Transl Cancer Res 2020, 9, 4080–4092. [Google Scholar] [CrossRef]
- Szostakowska, M.; Trebinska-Stryjewska, A.; Grzybowska, E.A.; Fabisiewicz, A. Resistance to endocrine therapy in breast cancer: molecular mechanisms and future goals. Breast Cancer Res Treat 2019, 173, 489–497. [Google Scholar] [CrossRef]
- Jeselsohn, R.; Buchwalter, G.; De Angelis, C.; Brown, M.; Schiff, R. ESR1 mutations-a mechanism for acquired endocrine resistance in breast cancer. Nat Rev Clin Oncol 2015, 12, 573–583. [Google Scholar] [CrossRef] [PubMed]
- Mack, P.C.; Banks, K.C.; Espenschied, C.R.; Burich, R.A.; Zill, O.A.; Lee, C.E.; Riess, J.W.; Mortimer, S.A.; Talasaz, A.; Lanman, R.B.; et al. Spectrum of driver mutations and clinical impact of circulating tumor DNA analysis in non-small cell lung cancer: Analysis of over 8000 cases. Cancer 2020, 126, 3219–3228. [Google Scholar] [CrossRef] [PubMed]
- Ko, T.K.; Lee, E.; Ng, C.C.; Yang, V.S.; Farid, M.; Teh, B.T.; Chan, J.Y.; Somasundaram, N. Circulating Tumor DNA Mutations in Progressive Gastrointestinal Stromal Tumors Identify Biomarkers of Treatment Resistance and Uncover Potential Therapeutic Strategies. Front Oncol 2022, 12, 840843. [Google Scholar] [CrossRef] [PubMed]
- Ernst, S.M.; van Marion, R.; Atmodimedjo, P.N.; de Jonge, E.; Mathijssen, R.H.J.; Paats, M.S.; de Bruijn, P.; Koolen, S.L.; von der Thusen, J.H.; Aerts, J.; et al. Clinical Utility of Circulating Tumor DNA in Patients With Advanced KRAS(G12C)-Mutated NSCLC Treated With Sotorasib. J Thorac Oncol 2024, 19, 995–1006. [Google Scholar] [CrossRef]
- Rothe, F.; Venet, D.; Peeters, D.; Rouas, G.; Rediti, M.; Smeets, D.; Dupont, F.; Campbell, P.; Lambrechts, D.; Dirix, L.; et al. Interrogating breast cancer heterogeneity using single and pooled circulating tumor cell analysis. NPJ Breast Cancer 2022, 8, 79. [Google Scholar] [CrossRef]
- Janni, W.J.; Rack, B.; Terstappen, L.W.; Pierga, J.Y.; Taran, F.A.; Fehm, T.; Hall, C.; de Groot, M.R.; Bidard, F.C.; Friedl, T.W.; et al. Pooled Analysis of the Prognostic Relevance of Circulating Tumor Cells in Primary Breast Cancer. Clin Cancer Res 2016, 22, 2583–2593. [Google Scholar] [CrossRef]
- Goodman, C.R.; Seagle, B.L.; Friedl, T.W.P.; Rack, B.; Lato, K.; Fink, V.; Cristofanilli, M.; Donnelly, E.D.; Janni, W.; Shahabi, S.; et al. Association of Circulating Tumor Cell Status With Benefit of Radiotherapy and Survival in Early-Stage Breast Cancer. JAMA Oncol 2018, 4, e180163. [Google Scholar] [CrossRef]
- Bidard, F.C.; Michiels, S.; Riethdorf, S.; Mueller, V.; Esserman, L.J.; Lucci, A.; Naume, B.; Horiguchi, J.; Gisbert-Criado, R.; Sleijfer, S.; et al. Circulating Tumor Cells in Breast Cancer Patients Treated by Neoadjuvant Chemotherapy: A Meta-analysis. J Natl Cancer Inst 2018, 110, 560–567. [Google Scholar] [CrossRef]
- Cristofanilli, M.; Budd, G.T.; Ellis, M.J.; Stopeck, A.; Matera, J.; Miller, M.C.; Reuben, J.M.; Doyle, G.V.; Allard, W.J.; Terstappen, L.W.; et al. Circulating tumor cells, disease progression, and survival in metastatic breast cancer. N Engl J Med 2004, 351, 781–791. [Google Scholar] [CrossRef]
- Cristofanilli, M.; Pierga, J.Y.; Reuben, J.; Rademaker, A.; Davis, A.A.; Peeters, D.J.; Fehm, T.; Nole, F.; Gisbert-Criado, R.; Mavroudis, D.; et al. The clinical use of circulating tumor cells (CTCs) enumeration for staging of metastatic breast cancer (MBC): International expert consensus paper. Crit Rev Oncol Hematol 2019, 134, 39–45. [Google Scholar] [CrossRef]
- Smerage, J.B.; Barlow, W.E.; Hortobagyi, G.N.; Winer, E.P.; Leyland-Jones, B.; Srkalovic, G.; Tejwani, S.; Schott, A.F.; O'Rourke, M.A.; Lew, D.L.; et al. Circulating tumor cells and response to chemotherapy in metastatic breast cancer: SWOG S0500. J Clin Oncol 2014, 32, 3483–3489. [Google Scholar] [CrossRef] [PubMed]
- Bidard, F.-C.; Jacot, W.; Dureau, S.; Brain, E.; Bachelot, T.; Bourgeois, H.; Goncalves, A.; Ladoire, S.; Naman, H.; Dalenc, F.; et al. Abstract GS3-07: Clinical utility of circulating tumor cell count as a tool to chose between first line hormone therapy and chemotherapy for ER+ HER2- metastatic breast cancer: Results of the phase III STIC CTC trial. Cancer Research 2019, 79 (4_Supplement), GS3-07. [Google Scholar] [CrossRef]
- Jacot, W.; Cottu, P.; Berger, F.; Dubot, C.; Venat-Bouvet, L.; Lortholary, A.; Bourgeois, H.; Bollet, M.; Servent, V.; Luporsi, E.; et al. Actionability of HER2-amplified circulating tumor cells in HER2-negative metastatic breast cancer: the CirCe T-DM1 trial. Breast Cancer Res 2019, 21, 121. [Google Scholar] [CrossRef] [PubMed]
- Arkadius Polasik, A.S. , Thomas W. P. Friedl, Brigitte Kathrin Rack, Elisabeth Katharina Trapp, Peter A. Fasching, Florin-Andrei Taran, Andreas D. Hartkopf, Andreas Schneeweiss, Volkmar Mueller, Bahriye Aktas, Klaus Pantel, Franziska Meier-Stiegen, Pauline Wimberger, Wolfgang Janni, Tanja N. Fehm. The DETECT study concept: Individualized therapy of metastatic breast cancer. Journal of Clinical Oncology 2016, 34. [Google Scholar] [CrossRef]
- Lin, D.; Shen, L.; Luo, M.; Zhang, K.; Li, J.; Yang, Q.; Zhu, F.; Zhou, D.; Zheng, S.; Chen, Y.; et al. Circulating tumor cells: biology and clinical significance. Signal Transduct Target Ther 2021, 6, 404. [Google Scholar] [CrossRef]
- Stoecklein, N.H.; Oles, J.; Franken, A.; Neubauer, H.; Terstappen, L.; Neves, R.P.L. Clinical application of circulating tumor cells. Med Genet 2023, 35, 237–250. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.J.; Wang, P.; Peng, J.; Wang, X.; Zhu, Y.W.; Shen, N. Meta-analysis Reveals the Prognostic Value of Circulating Tumour Cells Detected in the Peripheral Blood in Patients with Non-Metastatic Colorectal Cancer. Sci Rep 2017, 7, 905. [Google Scholar] [CrossRef]
- Groot Koerkamp, B.; Rahbari, N.N.; Buchler, M.W.; Koch, M.; Weitz, J. Circulating tumor cells and prognosis of patients with resectable colorectal liver metastases or widespread metastatic colorectal cancer: a meta-analysis. Ann Surg Oncol 2013, 20, 2156–2165. [Google Scholar] [CrossRef]
- Huang, X.; Gao, P.; Song, Y.; Sun, J.; Chen, X.; Zhao, J.; Xu, H.; Wang, Z. Meta-analysis of the prognostic value of circulating tumor cells detected with the CellSearch System in colorectal cancer. BMC Cancer 2015, 15, 202. [Google Scholar] [CrossRef]
- Krebs, M.G.; Renehan, A.G.; Backen, A.; Gollins, S.; Chau, I.; Hasan, J.; Valle, J.W.; Morris, K.; Beech, J.; Ashcroft, L.; et al. Circulating Tumor Cell Enumeration in a Phase II Trial of a Four-Drug Regimen in Advanced Colorectal Cancer. Clin Colorectal Cancer 2015, 14, 115–122.e111-112. [Google Scholar] [CrossRef]
- Krebs, M.G.; Sloane, R.; Priest, L.; Lancashire, L.; Hou, J.M.; Greystoke, A.; Ward, T.H.; Ferraldeschi, R.; Hughes, A.; Clack, G.; et al. Evaluation and prognostic significance of circulating tumor cells in patients with non-small-cell lung cancer. J Clin Oncol 2011, 29, 1556–1563. [Google Scholar] [CrossRef] [PubMed]
- Kapeleris, J.; Kulasinghe, A.; Warkiani, M.E.; Vela, I.; Kenny, L.; O'Byrne, K.; Punyadeera, C. The Prognostic Role of Circulating Tumor Cells (CTCs) in Lung Cancer. Front Oncol 2018, 8, 311. [Google Scholar] [CrossRef] [PubMed]
- Punnoose, E.A.; Atwal, S.; Liu, W.; Raja, R.; Fine, B.M.; Hughes, B.G.; Hicks, R.J.; Hampton, G.M.; Amler, L.C.; Pirzkall, A.; et al. Evaluation of circulating tumor cells and circulating tumor DNA in non-small cell lung cancer: association with clinical endpoints in a phase II clinical trial of pertuzumab and erlotinib. Clin Cancer Res 2012, 18, 2391–2401. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Xiao, Y.; Zhao, J.; Chen, M.; Xu, Y.; Zhong, W.; Xing, J.; Wang, M. Relationship between circulating tumour cell count and prognosis following chemotherapy in patients with advanced non-small-cell lung cancer. Respirology 2016, 21, 519–525. [Google Scholar] [CrossRef] [PubMed]
- de Bono, J.S.; Scher, H.I.; Montgomery, R.B.; Parker, C.; Miller, M.C.; Tissing, H.; Doyle, G.V.; Terstappen, L.W.; Pienta, K.J.; Raghavan, D. Circulating tumor cells predict survival benefit from treatment in metastatic castration-resistant prostate cancer. Clin Cancer Res 2008, 14, 6302–6309. [Google Scholar] [CrossRef]
- De Souza, L.M.; Robertson, B.M.; Robertson, G.P. Future of circulating tumor cells in the melanoma clinical and research laboratory settings. Cancer Lett 2017, 392, 60–70. [Google Scholar] [CrossRef]
- Aktar, S.; Baghaie, H.; Islam, F.; Gopalan, V.; Lam, A.K. Current Status of Circulating Tumor Cells in Head and Neck Squamous Cell Carcinoma: A Review. Otolaryngol Head Neck Surg 2023, 168, 988–1005. [Google Scholar] [CrossRef] [PubMed]
- Rack, B.; Schindlbeck, C.; Juckstock, J.; Andergassen, U.; Hepp, P.; Zwingers, T.; Friedl, T.W.; Lorenz, R.; Tesch, H.; Fasching, P.A.; et al. Circulating tumor cells predict survival in early average-to-high risk breast cancer patients. J Natl Cancer Inst 2014, 106. [Google Scholar] [CrossRef]
- Massard, C.; Borget, I.; Farace, F.; Aspeslagh, S.; Le Deley, M.C.; Le Tourneau, C.; Bidard, F.C.; Pierga, J.Y.; Dieras, V.; Hofman, P.; et al. RECIST response and variation of circulating tumour cells in phase 1 trials: A prospective multicentric study. Eur J Cancer 2017, 83, 185–193. [Google Scholar] [CrossRef]
- Muller, V.; Riethdorf, S.; Rack, B.; Janni, W.; Fasching, P.A.; Solomayer, E.; Aktas, B.; Kasimir-Bauer, S.; Pantel, K.; Fehm, T.; et al. Prognostic impact of circulating tumor cells assessed with the CellSearch System and AdnaTest Breast in metastatic breast cancer patients: the DETECT study. Breast Cancer Res 2012, 14, R118. [Google Scholar] [CrossRef]
- Templeman, A.; Miller, M.C.; Cooke, M.J.; O'Shannessy, D.J.; Gurung, Y.; Pereira, T.; Peters, S.G.; Piano, M.; Teo, M.; Khazan, N.; et al. Analytical performance of the FDA-cleared Parsortix((R)) PC1 system. J Circ Biomark 2023, 12, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Wishart, G.; Templeman, A.; Hendry, F.; Miller, K.; Pailhes-Jimenez, A.S. Molecular Profiling of Circulating Tumour Cells and Circulating Tumour DNA: Complementary Insights from a Single Blood Sample Utilising the Parsortix((R)) System. Curr Issues Mol Biol 2024, 46, 773–787. [Google Scholar] [CrossRef] [PubMed]
- Zavridou, M.; Mastoraki, S.; Strati, A.; Koutsodontis, G.; Klinakis, A.; Psyrri, A.; Lianidou, E. Direct comparison of size-dependent versus EpCAM-dependent CTC enrichment at the gene expression and DNA methylation level in head and neck squamous cell carcinoma. Sci Rep 2020, 10, 6551. [Google Scholar] [CrossRef] [PubMed]
- Braso-Maristany, F.; Griguolo, G.; Pascual, T.; Pare, L.; Nuciforo, P.; Llombart-Cussac, A.; Bermejo, B.; Oliveira, M.; Morales, S.; Martinez, N.; et al. Phenotypic changes of HER2-positive breast cancer during and after dual HER2 blockade. Nat Commun 2020, 11, 385. [Google Scholar] [CrossRef]
- Ju, S.; Chen, C.; Zhang, J.; Xu, L.; Zhang, X.; Li, Z.; Chen, Y.; Zhou, J.; Ji, F.; Wang, L. Detection of circulating tumor cells: opportunities and challenges. Biomark Res 2022, 10, 58. [Google Scholar] [CrossRef]
- Deng, Z.; Wu, S.; Wang, Y.; Shi, D. Circulating tumor cell isolation for cancer diagnosis and prognosis. EBioMedicine 2022, 83, 104237. [Google Scholar] [CrossRef]
- Edd, J.F.; Mishra, A.; Smith, K.C.; Kapur, R.; Maheswaran, S.; Haber, D.A.; Toner, M. Isolation of circulating tumor cells. iScience 2022, 25, 104696. [Google Scholar] [CrossRef]
- Mathias, T.J.; Chang, K.T.; Martin, S.S.; Vitolo, M.I. Gauging the Impact of Cancer Treatment Modalities on Circulating Tumor Cells (CTCs). Cancers (Basel) 2020, 12. [Google Scholar] [CrossRef]
- Donato, C.; Kunz, L.; Castro-Giner, F.; Paasinen-Sohns, A.; Strittmatter, K.; Szczerba, B.M.; Scherrer, R.; Di Maggio, N.; Heusermann, W.; Biehlmaier, O.; et al. Hypoxia Triggers the Intravasation of Clustered Circulating Tumor Cells. Cell Rep 2020, 32, 108105. [Google Scholar] [CrossRef]
- Zhu, X.; Suo, Y.; Fu, Y.; Zhang, F.; Ding, N.; Pang, K.; Xie, C.; Weng, X.; Tian, M.; He, H.; et al. In vivo flow cytometry reveals a circadian rhythm of circulating tumor cells. Light Sci Appl 2021, 10, 110. [Google Scholar] [CrossRef]
- Diamantopoulou, Z.; Castro-Giner, F.; Schwab, F.D.; Foerster, C.; Saini, M.; Budinjas, S.; Strittmatter, K.; Krol, I.; Seifert, B.; Heinzelmann-Schwarz, V.; et al. The metastatic spread of breast cancer accelerates during sleep. Nature 2022, 607, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Aceto, N. Fluctuating numbers of circulating tumor cells in cancer patients and the meaning of zero counts. Oncotarget 2019, 10, 2658–2659. [Google Scholar] [CrossRef] [PubMed]
- Juratli, M.A.; Siegel, E.R.; Nedosekin, D.A.; Sarimollaoglu, M.; Jamshidi-Parsian, A.; Cai, C.; Menyaev, Y.A.; Suen, J.Y.; Galanzha, E.I.; Zharov, V.P. In Vivo Long-Term Monitoring of Circulating Tumor Cells Fluctuation during Medical Interventions. PLoS One 2015, 10, e0137613. [Google Scholar] [CrossRef] [PubMed]
- Gall, T.M.; Jacob, J.; Frampton, A.E.; Krell, J.; Kyriakides, C.; Castellano, L.; Stebbing, J.; Jiao, L.R. Reduced dissemination of circulating tumor cells with no-touch isolation surgical technique in patients with pancreatic cancer. JAMA Surg 2014, 149, 482–485. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.J.; Xiao, W.; Dong, S.L.; Liang, H.F.; Zhang, Z.W.; Zhang, B.X.; Huang, Z.Y.; Chen, Y.F.; Zhang, W.G.; Luo, H.P.; et al. Effect of surgical liver resection on circulating tumor cells in patients with hepatocellular carcinoma. BMC Cancer 2018, 18, 835. [Google Scholar] [CrossRef]
- Haga, N.; Onagi, A.; Koguchi, T.; Hoshi, S.; Ogawa, S.; Akaihata, H.; Hata, J.; Hiraki, H.; Honda, R.; Tanji, R.; et al. Perioperative Detection of Circulating Tumor Cells in Radical or Partial Nephrectomy for Renal Cell Carcinoma. Ann Surg Oncol 2020, 27, 1272–1281. [Google Scholar] [CrossRef]
- Camara, O.; Kavallaris, A.; Noschel, H.; Rengsberger, M.; Jorke, C.; Pachmann, K. Seeding of epithelial cells into circulation during surgery for breast cancer: the fate of malignant and benign mobilized cells. World J Surg Oncol 2006, 4, 67. [Google Scholar] [CrossRef]
- Pang, S.; Li, H.; Xu, S.; Feng, L.; Ma, X.; Chu, Y.; Zou, B.; Wang, S.; Zhou, G. Circulating tumour cells at baseline and late phase of treatment provide prognostic value in breast cancer. Sci Rep 2021, 11, 13441. [Google Scholar] [CrossRef]
- Martin, O.A.; Anderson, R.L.; Russell, P.A.; Cox, R.A.; Ivashkevich, A.; Swierczak, A.; Doherty, J.P.; Jacobs, D.H.; Smith, J.; Siva, S.; et al. Mobilization of viable tumor cells into the circulation during radiation therapy. Int J Radiat Oncol Biol Phys 2014, 88, 395–403. [Google Scholar] [CrossRef]
- Mathenge, E.G.; Dean, C.A.; Clements, D.; Vaghar-Kashani, A.; Photopoulos, S.; Coyle, K.M.; Giacomantonio, M.; Malueth, B.; Nunokawa, A.; Jordan, J.; et al. Core needle biopsy of breast cancer tumors increases distant metastases in a mouse model. Neoplasia 2014, 16, 950–960. [Google Scholar] [CrossRef]
- Kusukawa, J.; Suefuji, Y.; Ryu, F.; Noguchi, R.; Iwamoto, O.; Kameyama, T. Dissemination of cancer cells into circulation occurs by incisional biopsy of oral squamous cell carcinoma. J Oral Pathol Med 2000, 29, 303–307. [Google Scholar] [CrossRef] [PubMed]
- Martin, O.A.; Anderson, R.L.; Narayan, K.; MacManus, M.P. Does the mobilization of circulating tumour cells during cancer therapy cause metastasis? Nat Rev Clin Oncol 2017, 14, 32–44. [Google Scholar] [CrossRef] [PubMed]
- Ito, Y.; Kobuchi, S.; Kawakita, A.; Tosaka, K.; Matsunaga, Y.; Yoshioka, S.; Jonan, S.; Amagase, K.; Hashimoto, K.; Kanda, M.; et al. Mobilization of Circulating Tumor Cells after Short- and Long-Term FOLFIRINOX and GEM/nab-PTX Chemotherapy in Xenograft Mouse Models of Human Pancreatic Cancer. Cancers (Basel) 2023, 15. [Google Scholar] [CrossRef]
- Ortiz-Otero, N.; Marshall, J.R.; Lash, B.; King, M.R. Chemotherapy-induced release of circulating-tumor cells into the bloodstream in collective migration units with cancer-associated fibroblasts in metastatic cancer patients. BMC Cancer 2020, 20, 873. [Google Scholar] [CrossRef]
- Vetter, M.; Landin, J.; Szczerba, B.M.; Castro-Giner, F.; Gkountela, S.; Donato, C.; Krol, I.; Scherrer, R.; Balmelli, C.; Malinovska, A.; et al. Denosumab treatment is associated with the absence of circulating tumor cells in patients with breast cancer. Breast Cancer Res 2018, 20, 141. [Google Scholar] [CrossRef] [PubMed]
- Bendahl, P.O.; Belting, M.; Gezelius, E. Longitudinal Assessment of Circulating Tumor Cells and Outcome in Small Cell Lung Cancer: A Sub-Study of RASTEN-A Randomized Trial with Low Molecular Weight Heparin. Cancers (Basel) 2023, 15. [Google Scholar] [CrossRef]
- Lozano, R.; Lorente, D.; Aragon, I.M.; Romero-Laorden, N.; Nombela, P.; Mateo, J.; Reid, A.H.M.; Cendon, Y.; Bianchini, D.; Llacer, C.; et al. Value of Early Circulating Tumor Cells Dynamics to Estimate Docetaxel Benefit in Metastatic Castration-Resistant Prostate Cancer (mCRPC) Patients. Cancers (Basel) 2021, 13. [Google Scholar] [CrossRef]
- Bidard, F.C.; Peeters, D.J.; Fehm, T.; Nole, F.; Gisbert-Criado, R.; Mavroudis, D.; Grisanti, S.; Generali, D.; Garcia-Saenz, J.A.; Stebbing, J.; et al. Clinical validity of circulating tumour cells in patients with metastatic breast cancer: a pooled analysis of individual patient data. Lancet Oncol 2014, 15, 406–414. [Google Scholar] [CrossRef]
- Costa, C.; Muinelo-Romay, L.; Cebey-Lopez, V.; Pereira-Veiga, T.; Martinez-Pena, I.; Abreu, M.; Abalo, A.; Lago-Leston, R.M.; Abuin, C.; Palacios, P.; et al. Analysis of a Real-World Cohort of Metastatic Breast Cancer Patients Shows Circulating Tumor Cell Clusters (CTC-clusters) as Predictors of Patient Outcomes. Cancers (Basel) 2020, 12. [Google Scholar] [CrossRef]
- Gerratana, L.; Davis, A.A.; Zhang, Q.; Basile, D.; Rossi, G.; Strickland, K.; Franzoni, A.; Allegri, L.; Mu, Z.; Zhang, Y.; et al. Longitudinal Dynamics of Circulating Tumor Cells and Circulating Tumor DNA for Treatment Monitoring in Metastatic Breast Cancer. JCO Precis Oncol 2021, 5, 943–952. [Google Scholar] [CrossRef]
- Szostakowska-Rodzos, M.; Fabisiewicz, A.; Wakula, M.; Tabor, S.; Szafron, L.; Jagiello-Gruszfeld, A.; Grzybowska, E.A. Longitudinal analysis of circulating tumor cell numbers improves tracking metastatic breast cancer progression. Sci Rep 2024, 14, 12924. [Google Scholar] [CrossRef] [PubMed]
- Forsare, C.; Bendahl, P.O.; Moberg, E.; Levin Tykjaer Jorgensen, C.; Jansson, S.; Larsson, A.M.; Aaltonen, K.; Ryden, L. Evolution of Estrogen Receptor Status from Primary Tumors to Metastasis and Serially Collected Circulating Tumor Cells. Int J Mol Sci 2020, 21. [Google Scholar] [CrossRef] [PubMed]
- Cohen, E.N.; Jayachandran, G.; Gao, H.; Peabody, P.; McBride, H.B.; Alvarez, F.D.; Kai, M.; Song, J.; Shen, Y.; Willey, J.S.; et al. Phenotypic Plasticity in Circulating Tumor Cells Is Associated with Poor Response to Therapy in Metastatic Breast Cancer Patients. Cancers (Basel) 2023, 15. [Google Scholar] [CrossRef] [PubMed]
- Stergiopoulou, D.; Markou, A.; Strati, A.; Zavridou, M.; Tzanikou, E.; Mastoraki, S.; Kallergi, G.; Georgoulias, V.; Lianidou, E. Comprehensive liquid biopsy analysis as a tool for the early detection of minimal residual disease in breast cancer. Sci Rep 2023, 13, 1258. [Google Scholar] [CrossRef]
- Hendricks, A.; Dall, K.; Brandt, B.; Geisen, R.; Roder, C.; Schafmayer, C.; Becker, T.; Hinz, S.; Sebens, S. Longitudinal Analysis of Circulating Tumor Cells in Colorectal Cancer Patients by a Cytological and Molecular Approach: Feasibility and Clinical Application. Front Oncol 2021, 11, 646885. [Google Scholar] [CrossRef]
- Ko, J.M.; Vardhanabhuti, V.; Ng, W.T.; Lam, K.O.; Ngan, R.K.; Kwong, D.L.; Lee, V.H.; Lui, Y.H.; Yau, C.C.; Kwan, C.K.; et al. Clinical utility of serial analysis of circulating tumour cells for detection of minimal residual disease of metastatic nasopharyngeal carcinoma. Br J Cancer 2020, 123, 114–125. [Google Scholar] [CrossRef]
- Magbanua, M.J.M.; Hendrix, L.H.; Hyslop, T.; Barry, W.T.; Winer, E.P.; Hudis, C.; Toppmeyer, D.; Carey, L.A.; Partridge, A.H.; Pierga, J.Y.; et al. Serial Analysis of Circulating Tumor Cells in Metastatic Breast Cancer Receiving First-Line Chemotherapy. J Natl Cancer Inst 2021, 113, 443–452. [Google Scholar] [CrossRef]
- Magbanua, M.J.M.; Savenkov, O.; Asmus, E.J.; Ballman, K.V.; Scott, J.H.; Park, J.W.; Dickler, M.; Partridge, A.; Carey, L.A.; Winer, E.P.; et al. Clinical Significance of Circulating Tumor Cells in Hormone Receptor-positive Metastatic Breast Cancer Patients who Received Letrozole with or Without Bevacizumab. Clin Cancer Res 2020, 26, 4911–4920. [Google Scholar] [CrossRef]
- Ko, J.M.Y.; Lam, K.O.; Kwong, D.L.W.; Wong, I.Y.; Chan, F.S.; Wong, C.L.; Chan, K.K.; Law, T.T.; Chiu, K.W.H.; Lam, C.C.S.; et al. Circulating Tumor Cell Enumeration for Serial Monitoring of Treatment Outcomes for Locally Advanced Esophageal Squamous Cell Carcinoma. Cancers (Basel) 2023, 15. [Google Scholar] [CrossRef]
Figure 1.
Diagram depicting proposed monitoring of the disease and the efficiency of the therapy with CTC count (red arrows) complementing clinical evaluation.
Figure 1.
Diagram depicting proposed monitoring of the disease and the efficiency of the therapy with CTC count (red arrows) complementing clinical evaluation.
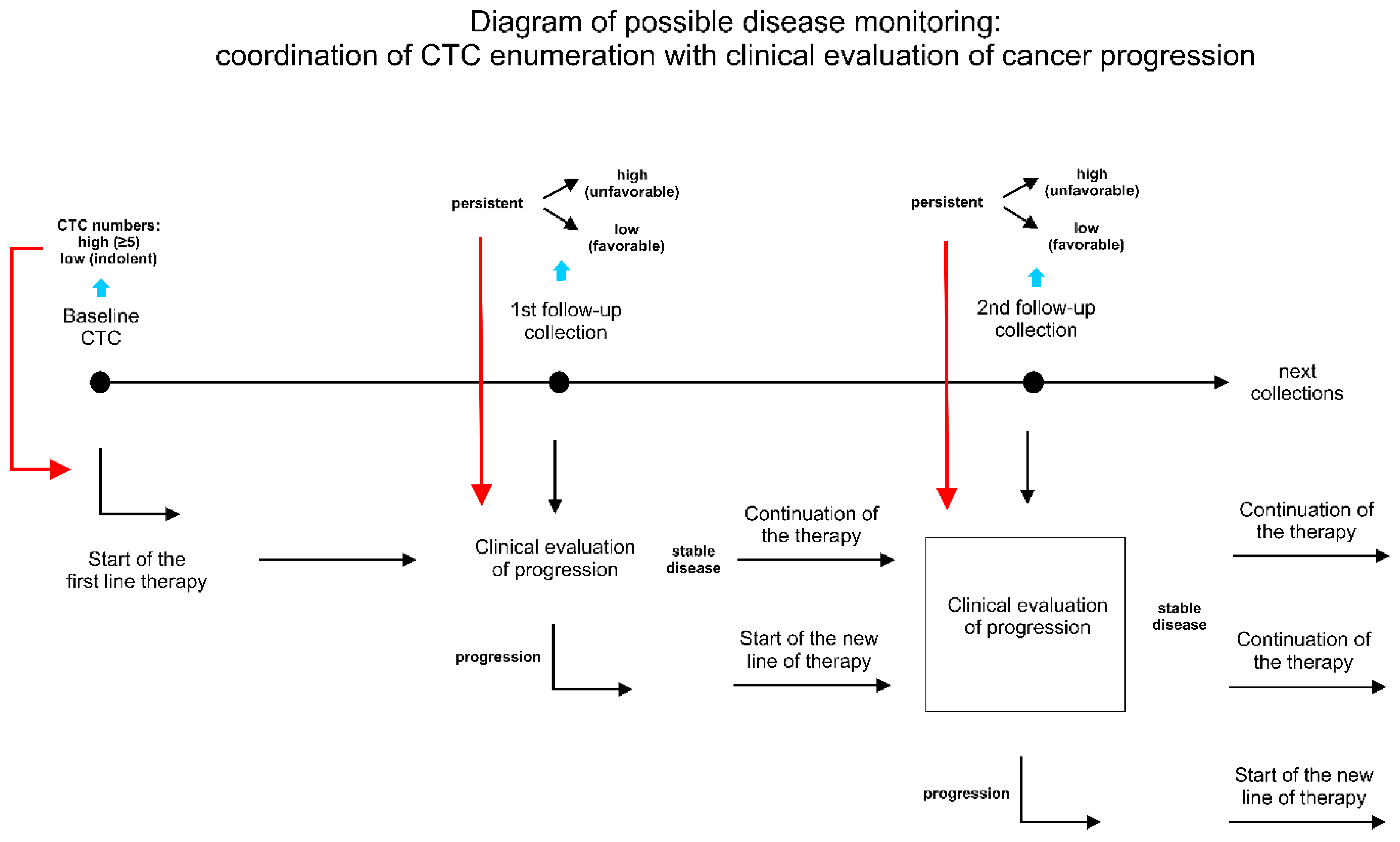

Table 1.
The current list of longitudinal CTC studies (with at least 3 blood collections).
| Cancer Type | Authors | Year | No. of patients included to analysis | No. of collections | CTC detection method | Main findings | REF# |
|---|---|---|---|---|---|---|---|
| Breast Cancer | Wang C, Mu Z, Chervoneva I,….,Cristofanilli M, Yang, H. | 2017 | 128 | 3 | CellSearch | CTC-clusters added additional prognostic values to CTC enumeration alone, and a larger-size CTC-cluster conferred a higher risk of death in MBC patients | [13] |
| Breast Cancer | Larsson AM, Jansson S, Bendahl PO, …., Rydén L. | 2018 | 152 | 4 | CellSearch | Longitudinal evaluation of CTC and CTC clusters improves prognostication and monitoring in patients with MBC starting first-line systemic therapy. Changes in CTC count throughout treatment significantly correlated with survival and the prognostic value was more prominent at later time points. High CTC counts and presence of clusters were identified as prognostic factors for OS and PFS. | [12] |
| Breast Cancer | Forsare C, Bendahl PO, Moberg E, …., Rydén L. | 2020 | 147 | 3 | CellSearch | A shift in ER-status from PT to DM/CTCs was demonstrated. Retained ER positivity of CTCs after initiation of systemic therapy was associated with better prognosis for PFS. This effect was observed only for followu-up samples, highlighting the importance of CTCs phenotyping during the treatment. | [92] |
| Nasopharyngeal carcinoma (NPC) | Ko JMY, Vardhanabhuti VV, Ng WT,…... Lung ML. | 2020 | 21 | 4 | CTChip®FR1 | CTCs were characterized as a more sensitive biomarker for MRD, when compared with imaging. Longitudinal changes in CTCs and EBV DNA along CT treatment for mNPC was found predictive for disease relapse. | [96] |
| Breast Cancer | Magbanua MJM, Hendrix LH, Hyslop T, ……. Rugo HS. | 2021 | 469 | ≥3 | CellSearch | The authors conducted the CTC trajectory model, which divided the patients into groups predicting the consistent trend for negative CTCs, low CTCs, mid CTCs and high CTCs status. The mid and high tCTC groups were identified with higher risk of early prgression, shorter PFS and OS. | [97] |
| Breast Cancer | Magbanua MJM, Savenkov O, Asmus EJ, ...., Rugo HS. | 2021 | 294 | 4 | CellSearch | CTCs positive patients at the baseline were identified with worse PFS and OS than CTC negative patients. The CTC positivity during the treatment or baseline was identified as risk factor for PFS and OS. Patients that became CTC positive in 1st follow-up had poorer prognosis for OS than patients that stayed CTC negative or patients that remain CTC positive since baseline. Patients who stayed CTC positive had poorer PFS and OS that patients who stayed CTC negative since baseline. | [98] |
| Breast Cancer | Gerratana L, Davis AA, Zhang Q, …….., Cristofanilli M. | 2021 | 107 | 3 | CellSearch | The ctDNA analysis revelaed that mutant allele frequency (MAF) changes follow the response to treatment, while CTC numbers increased only at the time of clinical progression. Conclusion: MAF could be more suitable for real-time disease monitoring, while CTCs could be more likely linked to metastatic biology. | [90] |
| Breast Cancer | Pang S, Li H, Xu S, …..., Zhou G. | 2021 | 164 | 4 | IMNs (immunomagnetic nanospheres) | Surgery led to an increase in the number and prevalence of CTCs on the first day after surgery and did not return to the preoperative level until 14 days after surgery. The CTC prevalence at the baseline and end-point follow-up visits was related to PFS and OS, while the CTCs detected before chemotherapy were only related to PFS. | [78] |
| Colorectal Cancer | Hendricks A, Dall K, Brandt B,…..., Sebens S. | 2021 | 47 | 5 | NYONE, RT-PCR | Surgery did not have any statistically significant effect on the quantity of CTC detected by the cytological approach utilizing the cell imager NYONE. In one of the patients constant increase in CTCs detected via both methods (9 months after the surgery) occured before the local clinical reccurence (13 months after surgery). | [95] |
| Breast Cancer | Stergiopoulou D, Markou A, Strati A,…….., Lianidou E. | 2023 | 13 | ≥10 | CellSearch | The molecular characteristics of CTCs were highly different even for the same patient at different time points, and always increased before the clinical relapse. Rapid increases in CTC numbers at months 74 and 122, were associated with metastatic disease documented by biopsy 6 months earlier. | [94] |
| Breast Cancer | Cohen EN, Jayachandran G, Gao H, ……….., Reuben JM. | 2023 | 184 | 9 | MCA (microactivity array) | The study reaffirmed the cut-off of ≥5 CTCs for inferior prognosis of patients with MBC. It also highlighted that epithelial CTC counts were prognostic before initiation of therapy and early in therapy, whereas a shift towards mesenchymal CTC phenotypes as detected by gene expression was associated with disease progression. | [93] |
| Esophageal Squamous Cell Carcinoma | Ko JMY, Lam KO, Kwong DLW, ………..., Lung ML | 2023 | 88 | 12 | CTChip®FR1 | The changes in CTCs status pre-surgery and 1 or 3 month after surger and pT staging after resection are independent prognostic factors of poor prognosis for locally advanced ESCC patients receiving surgical treatment, as well as the presence of CTC clusters, unfavorable CTC status at baseline, 1-month and 3-month post-surgery. | [99] |
| Small Cell Lung Cancer | Bendahl PO, Belting M, Gezelius E. | 2023 | 42 | 2 | CellSearch | CTCs presence at the baseline was identified as the poor prognostic factor for the survival in patients. The persistent CTCs presence at 2-month follow-up and baseline was associated with significantly higher HR for OS. | [86] |
| Breast Cancer | Szostakowska-Rodzos M, Fabisiewicz A, Wakula M, …………….., Grzybowska EA. | 2024 | 135 | 3 | CytoTrack | High CTCs count was independent poor prognosis marker for PFS and OS, regardless of time of the enumeration. The consistnet low CTCs numbers during the treatment was revealed t be favorable prognostic marker for PFS and OS. The rising values of CTC count was identified as predictor for rapid progression. | [91] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



