Submitted:
10 September 2024
Posted:
11 September 2024
You are already at the latest version
Abstract
Background: The absence of interdental papillae in dental prosthetics often results in unsatisfactory esthetic outcomes, such as black triangles and elongated clinical crowns. Although previous research has shown that gingival papillae can regenerate in a coronal direction, the mechanisms behind this phenomenon are not fully understood. Various theories have been proposed as potential explanations. Materials and Methods: This study evaluated several factors potentially influencing papilla growth, including adjacent elements, buc-cal-lingual papilla width, contact point position, convergent neck, crown overcontour, and intraoral negative pressure. A conceptual map was created to organize these factors, followed by their classification using a modified Overton Window. The principle of parsimony (Occam's Razor) was applied to identify the most plausible cause-related factors, categorizing them as causal relationship factors, filtered out factors, essential factors, or influencing factors. A mind map was used for visual grouping. Results: The analysis identified intraoral negative pressure as the most plausible cause-related factor for spontaneous papilla growth. Factors such as inflammation and drug-induced hyperplasia were excluded due to their association with unhealthy tissue. Other factors were classified as essential or influencing, but without direct causal links to papilla growth. Conclusions: Intraoral negative pressure is likely a key contributor to spontaneous papilla growth around implants. This finding, supported by abductive reasoning and the exclusion of less plausible factors, offers a new direction for enhancing esthetic outcomes in dental prosthetics, though further research is needed to confirm this causal relationship.
Keywords:
implant
; mucosa growth
; peri-implant mucosa
; keratinized tissue
; crown overcontour
; BOPT
; papilla growth
1. Introduction
In dental prosthetic treatments, an unsatisfactory esthetic result frequently arises from the absence of interdental papillae, leading to the appearance of black triangles and the pronounced elongation of clinical crowns due to the recession of marginal soft tissues. Our earlier research has demonstrated that gingival papillae and tissue margins are capable of naturally regenerating in a coronal direction [1,2]. Some theories have been proposed to explain this phenomenon, such as the inflammatory [3] and the intraoral negative pressure theories [1,2,4]. Moreover, several conditions have been identified as crucial for the occurrence of the phenomenon such as the existence of a sufficient band of crestal keratinized mucosa, both in terms of width and thickness [1,2]; the presence and positioning of the contact point [5,6,7]; an appropriate distance between adjacent teeth or implants [8,9]; an ideal bucco-lingual dimension of the alveolar ridge (crestal bucco-lingual thickness) [7]; and, lastly, the availability of spaces around the prostheses that can be occupied by the growth of crestal soft tissues [1,2,4].
In scientific research, the exploration of unresolved problems, such the spontaneous papilla growth, often leads to the formulation of multiple competing theories. Each theory offers a potential explanation, yet not all are equally valid or plausible. Max Weber argues that no explanation can be truly scientific unless it is also a causal explanation. He emphasizes that scientific inquiry must go beyond mere description, seeking to identify and understand the cause-and-effect relationships underlying a phenomenon [10,11]. Determining cause-effect relationships in research is crucial because it allows researchers to identify the underlying mechanisms that drive observed phenomena, ensuring that actions performed by clinicians are based on a clear understanding of how specific factors influence outcomes.
In the absence of a clear causal relationship, determining which theory most accurately reflects reality requires the application of certain principles that guide scientific methodology.
Hence, due to the lack of a clear cause-effect relationship among the various factors involved in spontaneous papilla growth around implants, this article aims to identify tools that can help pinpoint the factor most likely to be the key driver of this phenomenon.
2. Materials and Methods
2.1. Factors Evaluated
The following factors involved in the spontaneous papilla growth have been included in the analysis:
- Buccal-lingual papilla width: The likelihood of a fully filled papilla is greatly influenced by the bucco-lingual width of the papilla's base [7].
- Initial papilla height: A post-hoc analysis of the data of an already published article was planned to evaluate the influence of the initial height of the papilla on the outcome [1].
- Mucosa thickness/phenotype: In a recent Consensus report it was concluded that the presence of a thick mucosa provides a tendency of better esthetic outcomes [26].
- Timing: It has been shown that most of the height gain occur in the first year after prosthetic delivering [1].
2.2. Tools used for Evaluation
A preliminary conceptual map was first created to organize and structure all factors involved in the assessment.
A modified customized version of the Overton Windows, named after Joseph P. Overton, was used in the present study to classify all factors that might have any effect on the spontaneous growth of a healthy papilla around implants. The Overton Window provides a framework for understanding how public opinion shifts and how certain ideas become acceptable or even mainstream over time [27]. A modified version was used in the present study.
The analysis was conducted by five independent authors, all of them expert clinicians. Each author completed an Excel sheet that categorized all relevant factors into the four classifications outlined below. These categories were applied to each factor for consistency with the reported scientific evidence, together a rational analysis:
- Causal Relationship Factor - Identified when a potential cause-and-effect relationship with papilla growth is observed.
- Filtered Out Factor - Factors that exhibit a cause-and-effect relationship with papilla growth but whose effects are attributable to inflammation or drug influences, and therefore should not be associated with healthy tissue. This classification may also be applied to factors that are neither essential nor influential.
- Essential Factor - Determined as critical for papilla growth. Papilla growth cannot occur in the absence of this factor, despite no direct cause-and-effect relationship being observed.
- Influencing Factor - Recognized as having an impact on papilla growth, although not essential for it. No direct cause-and-effect relationship is observed with papilla growth.
Once the factors were classified, a mind map according to Tony Buzan was produces grouping the factors according to categorization [28]. A Mind Map is a diagram used to represent words, ideas, tasks, or other concepts that are connected and arranged around a central keyword or main idea [29].
Moreover, the Occam's Razor principle was applied during the categorization. Occam’s Razor (or Ockham’s Razor) is a principle attributed to the medieval philosopher and theologian William of Ockham (c. 1287–1347). The principle states that when faced with competing hypotheses, the one with the fewest and simplest assumptions should be selected [30].
3. Results
Factors were listed in a conceptual map in alphabetical order without being grouped, allowing for an unbiased evaluation according to the adopted classification (Figure 1). Some of the most important articles regarding each topic were reported in the map and considered for evaluation.
Each factor was evaluated for its role in papilla growth, beginning with an assessment of any potential cause-effect relationship. The analysis then determined whether the factor played an essential role in papilla growth or merely influenced the outcome. Additionally, if a causal relationship was identified, the evaluation distinguished whether the result reflected healthy papilla growth or was instead due to inflammation or drug-induced hyperplasia.
A modified Overton Window was adopted to assign to each factor the most suitable category (Figure 2) [27]. Each factor was initially examined to determine its causal relationship. If a positive causal link was identified, the factor's alignment with a healthy papilla was subsequently assessed. Factors that demonstrated both a positive causal relationship and congruency with a healthy papilla were retained within their respective category. If a factor did not meet these criteria, it was placed into a filtered-out group. In cases where no causal relationship was detected, the factor was categorized as either essential or influential, depending on whether its presence was deemed necessary or merely contributory.
The Occam's Razor principle was applied during the categorization [30].
The factors received the following evaluation:
- Buccal-lingual papilla width: No cause-related relationship was found. The buccal-lingual width was considered to influence papilla growth [7].
- Inflammatory theory: The inflammatory theory presented a causal relationship with papilla growth. However, an inflammatory condition that causes edema and inflammatory infiltrate, leading to tissue growth, cannot be considered healthy [3]. The biofilm theory was invoked primarily in the context of orthodontic treatment, given the noticeable papilla growth despite the absence of significant plaque accumulation [23].
- Initial papilla height: A post-hoc analysis of data from a previously published study1 revealed that a lower initial height of the papilla was associated with a greater increase in papilla score (Table 1). No cause-related relationship was found. This factor was considered to influence papilla growth [1].
- Mucosa thickness/phenotype: No cause-related relationship was found. The mucosa thickness was considered to influence papilla growth [24].
- Timing: No cause-related relationship was found. The timing was considered influencing papilla growth [1].
The five authors reached consensus on all factors except for the crown material and rotary curettage. One author believed that the crown material does not influence papilla growth, while two authors felt that rotary curettage is only applicable for tooth preparation. Consequently, the categorization of all factors was accepted.
4. Discussion
A well-defined cause-effect relationship for papilla growth has not yet been established. This study found that, among the various factors evaluated, intraoral negative pressure is the only one that remains as a potential cause-related factor. However, this does not imply that it is definitively the cause; it merely remains the most plausible explanation after other possibilities were excluded. Excluding other potential causes does not provide certainty about the remaining factor. A direct cause-effect relationship still needs to be conclusively demonstrated, and in the case of papilla growth, this direct relationship has not yet been proven.
To understand how the research approach function, an analysis of three types of inferential reasoning proposed by Charles Sanders Peirce (1839–1914) might be used, i.e.: deduction, induction, and abduction [31,32].
Deduction is an inferential process that begins with general premises and leads to specific conclusions. Deduction requires an initial rule, leading to a predictable result, heavily depending on the reliability of this rule. Deductive reasoning is deeply ingrained in our daily routines, from the morning alarm ringing at the precise time we set the night before, to the automatic steps we take while walking, or when we turn on the hot water faucet and expect hot water to flow out—each a predictable cause-and-effect sequence. In clinical practice, we rely on deductive processes similarly, such as when placing a dental implant in the alveolar bone, anticipating osseointegration based on established principles, or performing treatments with specific expected outcomes.
Induction, on the other hand, involves creating rules through experimentation. When existing rules are absent, we use inductive methods by conducting experiments or clinical research. For example, we might introduce a new variable to a test group while keeping a control group under standard conditions. By comparing the outcomes, we can identify significant differences, allowing us to develop new rules that can later be applied in deductive reasoning.
In the case of papilla growth, the exact cause remains unclear. Under such conditions, we begin by conjecturing or hypothesizing possible reasons for this growth, with negative pressure being just one of several potential causes identified. This type of reasoning is what Peirce referred to as abduction. Abduction is the inferential process of forming a plausible hypothesis based on a set of observations. It is often described as 'the best possible explanation' and plays a crucial role in generating new ideas and theories. Although abduction does not guarantee the truth of its conclusions or necessarily make them probable, it provides an initial explanation that can be further tested through induction. Abduction serves as the starting point of the scientific inquiry process, where the hypothesized explanation is tested and refined.
When several variables and factors are involved in the process, like in the spontaneous papilla growth, we need to use tools that can help us in the problem-solving process. The modified Overton Window applied in this study identified intraoral negative pressure as 'the best possible explanation' for the spontaneous papilla growth [27]. Three potential cause-related factors were considered, but two—inflammation and drug-induced hyperplasia—were excluded. The principle of parsimony, often referred to as Occam's Razor, played a key role in this exclusion [30].
When multiple theories can explain the same phenomenon, the simplest one, with the fewest assumptions, is preferred. Although parsimony does not guarantee that the simplest theory is correct, it serves as a heuristic that guides scientists in selecting between otherwise equally plausible explanations [30]. By applying this principle, we were able to exclude inflammation and drug-induced hyperplasia as less likely causes, thereby simplifying the selection of the most plausible cause-related relationship. This tool also aided in classifying the factors as either essential or influencing.
Other tools used for the present problem-solving study were the conceptual map and the mind map. The conceptual map helped to organize all information visually and to better understand a complex topic such as that of papilla growth, clarify relationships between ideas, enhances understanding of complex topics, and encourages critical thinking by visually organizing information.
Mind maps, popularized by Tony Buzan, are designed to mirror the brain's natural thinking process, encouraging free-flowing, non-linear thinking and fostering creativity [28]. The mind map helped to break down the complex topic of papilla growth into simpler, visual representations, making it easier to grasp the big picture and details simultaneously. The mind map included the Gestalt principles of similarity - stating the elements that are similar in appearance, e.g., color, shape, size, are perceived as part of the same group or pattern - and that of proximity, suggesting that elements that are close to each other in space are perceived as related or grouped together [33].
Additionally, it is important to note that one branch on the map was intentionally left open, indicating that other factors not yet considered may be added in the future. The mind map presented in the article was intentionally designed with only main branches, omitting sub-branches. While adhering to the original principles of mind mapping as suggested by Tony Buzan, a possible alternative result is illustrated in Figure 4. The structure of both mind maps allows for easy reassignment of factors to different categories, accommodating any alternative interpretations or preferences that readers might have regarding the authors' initial categorizations.
In this article, we discussed papilla growth, acknowledging that some might argue a papilla adjacent to an implant surface should not be considered a true papilla due to significant histological differences compared to periodontal tissue [34]. However, from a clinical perspective, these differences are not easily discernible, so we continue to use the term "papilla" to refer to the keratinized tissue filling the embrasure between elements.
It is important to emphasize that intraoral negative pressure is generated during swallowing and persists until the lips are opened. This pressure, while lower in intensity, lasts longer than the pressure during swallowing. Given that the person swallows in average about 500 to 700 times per day [35], this low-intensity negative pressure may act over extended periods. This "oral pump" effect [4,25] could gradually promote papilla growth into a recessed zone. This low negative pressure differs significantly from the “acute” suction effect in cupping therapy, an ancient alternative medicine technique where cups create suction on the skin aiming to possibly relieve of pain and inflammation, and to improve blood flow [36,37].
The present study identified intraoral negative pressure as the most plausible cause of spontaneous papilla growth around implants, after excluding other factors such as inflammation and drug-induced hyperplasia using the principle of parsimony. While this hypothesis provides a promising direction, it is important to note that the direct cause-effect relationship has not yet been conclusively demonstrated. Additionally, many of the factors influencing papilla growth around implants may also apply to tissue growth around teeth, particularly in relation to the Biologically Oriented Preparation Technique (BOPT) principle [17].
One limitation of this study is the reliance on theoretical analysis and existing literature, which may not fully capture the complexity of papilla growth. Additionally, the classification of factors using the modified Overton Window [27], and the principle of parsimony30 is inherently subjective and may have introduced bias. The study also did not include experimental or clinical trials to validate the identified relationships, limiting the ability to draw definitive conclusions.
Future research should focus on conducting controlled clinical trials to empirically test the hypothesis of intraoral negative pressure as a driver of papilla growth. Additionally, studies could explore the interaction between multiple factors, such as the combined effects of intraoral pressure, keratinized tissue presence, and contact point positioning. Further investigation into the biological mechanisms underlying this phenomenon would also be valuable, potentially involving histological studies to compare papilla formation in different conditions. Expanding the scope to include diverse patient populations and varying implant types could also provide more generalized insights.
This study did not aim to provide a systematic review of the available literature on the topics discussed. Instead, a selection of well-known articles was chosen, focusing on those that provided relevant data for each of the factors under consideration and were necessary to meet the objectives of the study. The authors apologize for any significant articles that may have been inadvertently omitted.
5. Conclusions
In conclusion, intraoral negative pressure was identified as the most plausible cause of spontaneous papilla growth around implants, following the exclusion of other factors like inflammation and drug-induced hyperplasia using the principle of parsimony. A modified Overton Window played a crucial role in categorizing several factors involved in the process. The conceptual and mind maps were instrumental in organizing complex data and guiding the analysis toward this conclusion. While promising, the hypothesis that the intraoral negative pressure is the cause of spontaneous papilla growth around implants still requires empirical validation through future research.
Author Contributions
Conceptualization, D.B. and I.A.; methodology, D.B.; software, D.B.; validation, R.Y., N.M., K.A.A.A., and Y.N.; formal analysis, D.B., I.A., R.Y., N.M., K.A.A.A., and Y.N.; investigation, D.B. and I.A.; resources, D.B. and Y.N.; data curation, D.B.; writing—original draft preparation, D.B. and I.A.; writing—review and editing, D.B., I.A., and K.A.A.A.; visualization, R.Y., N.M., and Y.N.; supervision, D.B.; project administration, D.B.; funding acquisition, D.B. and Y.N. All authors have read and agreed to the published version of the manuscript.
Funding
This research and the APC was funded by ARDEC Academy.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data is available following a reasonable request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Agabiti I, Apaza Alccayhuaman KA, Nakajima Y, Botticelli D. An enigmatic soft tissue creeping phenomenon: The spontaneous peri-implant mucosa margin and papilla growth. A retrospective clinical study. Clin Exp Dent Res. 2021, 7, 474–483. [CrossRef] [PubMed] [PubMed Central]
- Agabiti I, Apaza Alccayhuaman KA, Taniguchi Z, Kuwano K, Botticelli D. An Enigmatic Soft-Tissue Creeping Phenomenon: The Spontaneous Peri-Implant Mucosa Margin and Papilla Growth, Part Two-A Scientifically Supported Hypothesis Article. Dent J (Basel). 2024, 12, 216. [CrossRef] [PubMed] [PubMed Central]
- Jemt, T. Regeneration of gingival papillae after single-implant treatment. Int J Periodontics Restorative Dent. 1997, 17, 326–33. [Google Scholar] [PubMed]
- Harster, P. Tissue modeling: the oral pump. Quintessence Int. 2005, 36, 633–640. [Google Scholar]
- Tarnow DP, Magner AW, Fletcher P. The effect of the distance from the contact point to the crest of bone on the presence or absence of the interproximal dental papilla. J Periodontol. 1992, 63, 995–6. [CrossRef] [PubMed]
- Tarnow D, Elian N, Fletcher P, et al. Vertical distance from the crest of bone to the height of the interproximal papilla between adjacent implants. J Periodontol. 2003, 74, 1785–1788. [CrossRef]
- Chang M, Wennström JL. Soft tissue topography and dimensions lateral to single implant-supported restorations. a cross-sectional study. Clin Oral Implants Res. 2013, 24, 556–562. [CrossRef]
- Tarnow DP, Cho SC, Wallace SS. The effect of inter-implant distance on the height of inter-implant bone crest. J Periodontol. 2000, 71, 546–549. [CrossRef]
- Cardaropoli G, Wennström JL, Lekholm U. Peri-implant bone alterations in relation to inter-unit distances. A 3-year retrospective study. Clin Oral Implants Res. 2003, 14, 430–6. [CrossRef] [PubMed]
- Weber, M. (1949). The Methodology of the Social Sciences. Free Press.
- Strand, M. , & Lizardo, O. Chance, Orientation, and Interpretation: Max Weber’s Neglected Probabilism and the Future of Social Theory. Sociological Theory 2022, 40, 149–169. [Google Scholar] [CrossRef]
- Choquet V, Hermans M, Adriaenssens P, Daelemans P, Tarnow DP, Malevez C. Clinical and radiographic evaluation of the papilla level adjacent to single-tooth dental implants. A retrospective study in the maxillary anterior region. J Periodontol. 2001, 72, 1364–71. [CrossRef] [PubMed]
- Canullo L, Giuliani A, Furlani M, Menini M, Piattelli A, Iezzi G. Influence of abutment macro- and micro-geometry on morphologic and morphometric features of peri-implant connective tissue. Clin Oral Implants Res. 2023, 34, 920–933. [CrossRef] [PubMed]
- Agustín-Panadero R, Martínez-Martínez N, Fernandez-Estevan L, Faus-López J, Solá-Ruíz MF. Influence of Transmucosal Area Morphology on Peri-Implant Bone Loss in Tissue-Level Implants. Int J Oral Maxillofac Implants. 2019, 34, 947–952. [CrossRef]
- Rodríguez X, Navajas A, Vela X, Fortuño A, Jimenez J, Nevins M. Arrangement of Peri-implant Connective Tissue Fibers Around Platform-Switching Implants with Conical Abutments and Its Relationship to the Underlying Bone: A Human Histologic Study. Int J Periodontics Restorative Dent. 2016, 36, 533–540. [CrossRef]
- Morris, ML. Artificial crown contours and gingival health. J. Prosthet Dent 1962, 12, 1146–1156. [Google Scholar] [CrossRef]
- Loi I, Di Felice A. Biologically oriented preparation technique (BOPT): a new approach for prosthetic restoration of periodontically healthy teeth. Eur J Esthet Dent. 2013, 8, 10–23 PMID: 23390618. [PubMed]
- Thomason, J.M.; Seymour, R. A. Phenytoin-induced gingival overgrowth: a review of the molecular, immune, and inflammatory features. Journal of Clinical Periodontology 2006, 33, 739–744. [Google Scholar]
- Alabdulkarim, M.; Bukhari, H.M.; Sheikh, S.A. Drug-induced gingival overgrowth: A comprehensive review. International Journal of Health Sciences 2018, 12, 82–89. [Google Scholar]
- Tejnani, A.; Diwan, A.; Sajjan, P. Drug-Induced Gingival Overgrowth: A Review. Cureus 2020, 12, e9307. [Google Scholar]
- Ingraham R, Sochat P, Hansing FJ. Rotary gingival curettage: A technique for tooth preparation and management of the gingival sulcus for impression taking. Int J Periodont Rest Dent 1981, 1, 9–33.
- Thorburn, W.M. The Myth of Occam's Razor. Mind 1918, 27, 345–353. [Google Scholar] [CrossRef]
- Vincent-Bugnas, S.; Borsa, L.; Gruss, A.; Lupi, L. Prioritization of predisposing factors of gingival hyperplasia during orthodontic treatment: The role of amount of biofilm. BMC Oral Health 2021, 21, 84. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Fränkel, R. A functional approach to orofacial orthopaedics. Br J Orthod. 1980, 7, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Engelke W, Jung K, Knosel M. Intra-oral compartment pressures: a biofunctional model and experimental measurements under different conditions of posture. Clin Oral Investig. 2011, 15, 165–176.
- Jung RE, Becker K, Bienz SP, Dahlin C, Donos N, Hammächer C, Iglhaut G, Liñares A, Ortiz-Vigón A, Sanchez N, Sanz-Sánchez I, Thoma DS, Valles C, Weng D, Nart J. Effect of peri-implant mucosal thickness on esthetic outcomes and the efficacy of soft tissue augmentation procedures: Consensus report of group 2 of the SEPA/DGI/OF workshop. Clin Oral Implants Res. 2022, 33 (Suppl. 23), 100–108. [CrossRef] [PubMed]
- Mackinac Center for Public Policy. (2010). An introduction to the Overton window of political possibilities. Mackinac Center for Public Policy. Retrieved from https://www.mackinac.org/OvertonWindow.
- The Ultimate Book of Mind Maps – Tony Buzan - HarperThorsons, imprint of HarperCollins Publishers - New York City - New York, USA.
- Buzan, T. (1974). Use Your Head. London: BBC.
- Sober, E. (2015). Ockham's Razors: A User's Manual. Cambridge: Cambridge University Press.
- Peirce, C. S. Deduction, Induction, and Hypothesis. Popular Science Monthly 1878, 13, 470–482. [Google Scholar]
- Anderson, Douglas R. The evolution of Peirce’s concept of abduction. Transactions of the Charles S. Peirce Society 1986, 22, 145–164.
- Koffka, K. (1935). Principles of Gestalt Psychology. London: Routledge and Kegan Paul.
- Berglundh T, Lindhe J, Ericsson I, Marinello CP, Liljenberg B, Thomsen P. The soft tissue barrier at implants and teeth. Clin Oral Implants Res. 1991, 2, 81–90. [CrossRef] [PubMed]
- Lear, C.S.; Flanagan, J.B.; Moorrees, C.F. The frequency of deglutition in man. Archives of Oral Biology 1965, 10, 83–100. [Google Scholar] [CrossRef]
- Cao, H.; Li, X.; Liu, J. An updated review of the efficacy of cupping therapy. PLoS One 2012, 7, e31793. [Google Scholar] [CrossRef]
- Al-Bedah, A.M.; Elsubai, I.S.; Qureshi, N.A.; Aboushanab, T.S.; Ali, G.I.; El-Olemy, A.T.; Khalil, A.A. The medical perspective of cupping therapy: Effects and mechanisms of action. Journal of Traditional and Complementary Medicine 2019, 9, 90–97. [Google Scholar] [CrossRef]
Figure 1.
A conceptual map was created to illustrate all factors potentially involved in papilla growth, with relevant references included for each factor. Additional factors may still be added at the red branch.
Figure 1.
A conceptual map was created to illustrate all factors potentially involved in papilla growth, with relevant references included for each factor. Additional factors may still be added at the red branch.
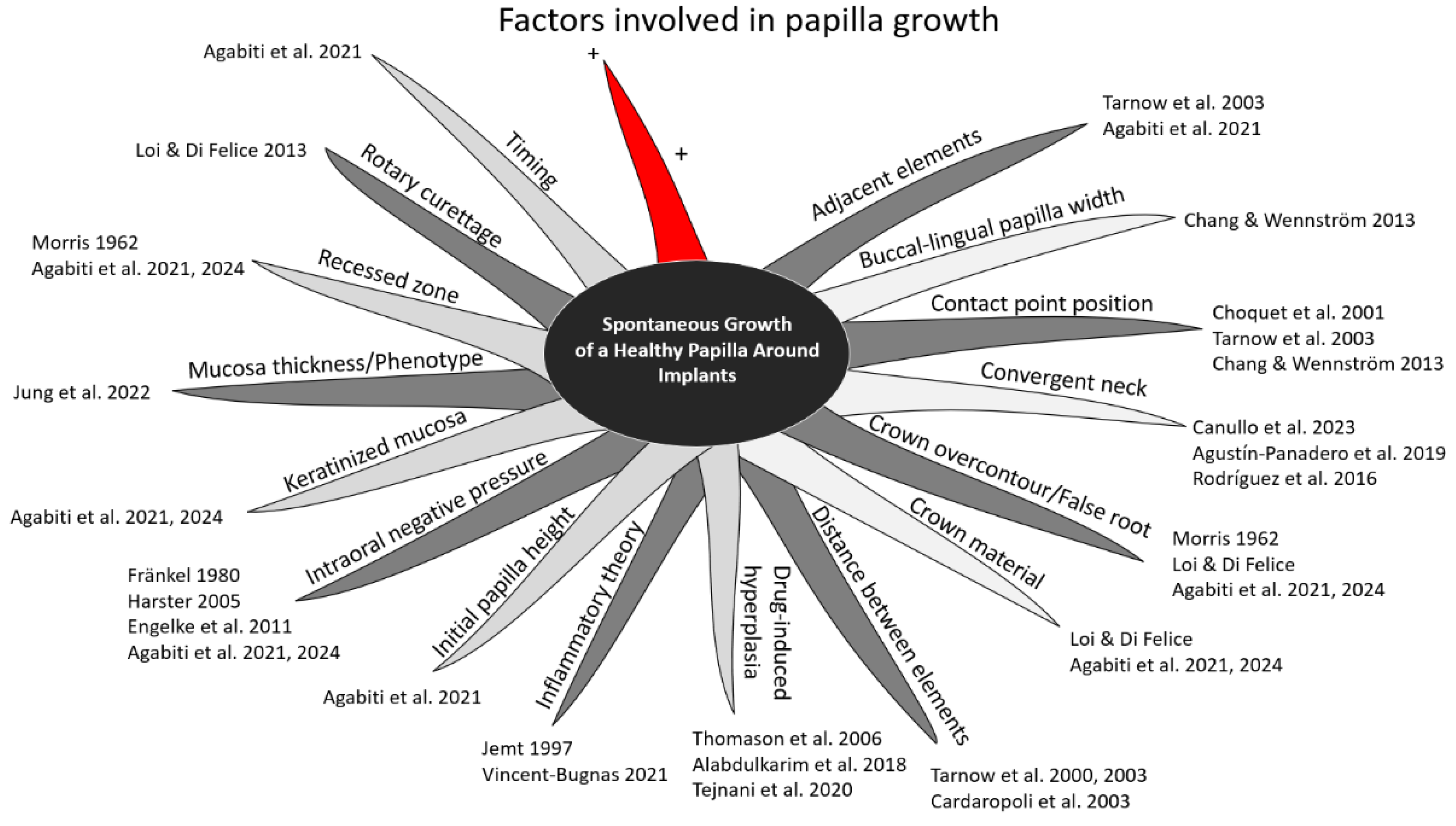
Figure 2.
A modified customized version of the Overton Windows. .
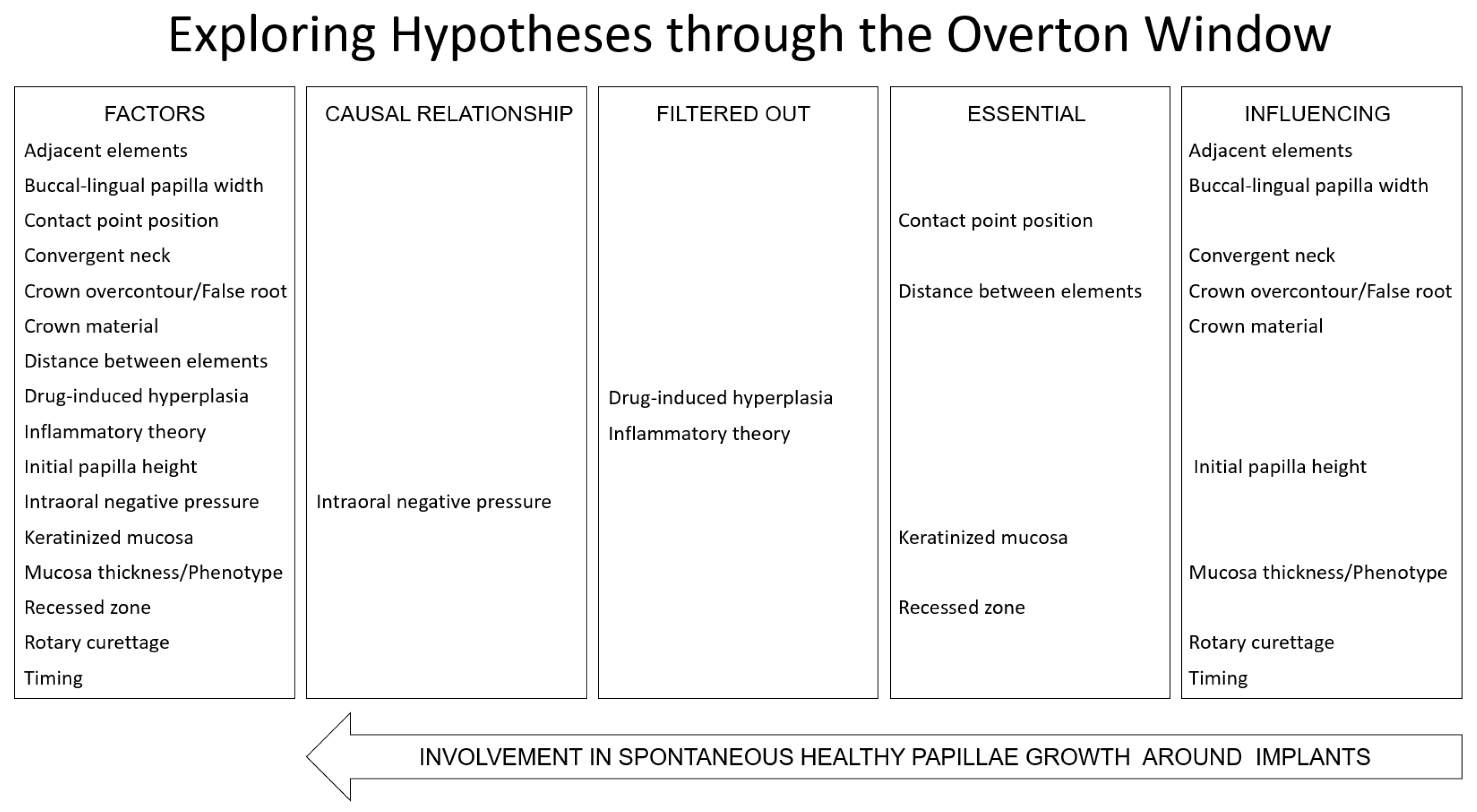
Figure 3.
The factors were organized into four distinct categories, each identified by different colors and boxed outlines to enhance visual clarity and differentiation between the categories. The white branch leaves room for additional factors may still be identified. Note that only main branches were used to enhance the map's visual clarity and to highlight the flexibility in categorization.
Figure 3.
The factors were organized into four distinct categories, each identified by different colors and boxed outlines to enhance visual clarity and differentiation between the categories. The white branch leaves room for additional factors may still be identified. Note that only main branches were used to enhance the map's visual clarity and to highlight the flexibility in categorization.
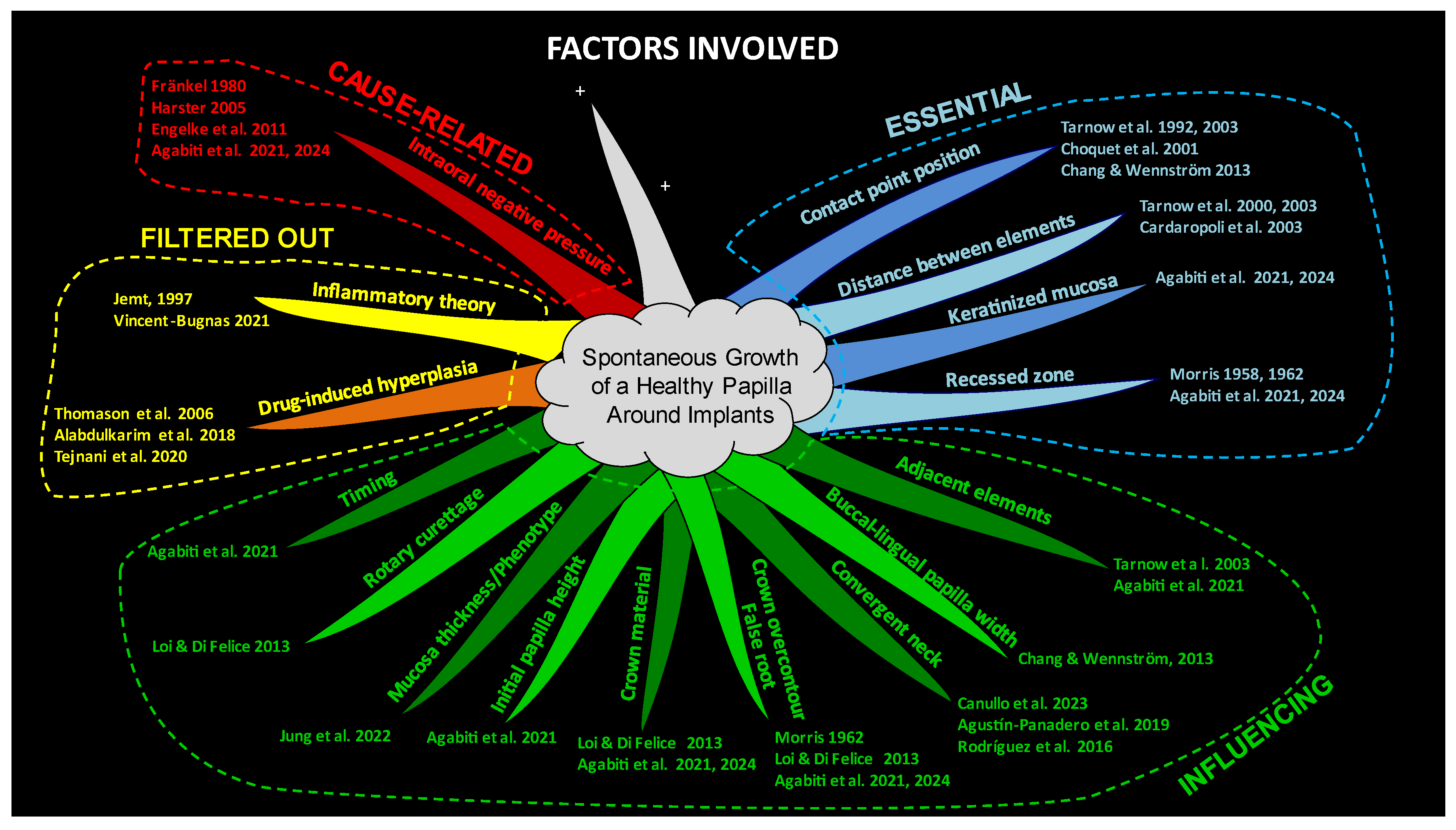
Figure 4.
Mind map with sub-branches, generated using specialized software.
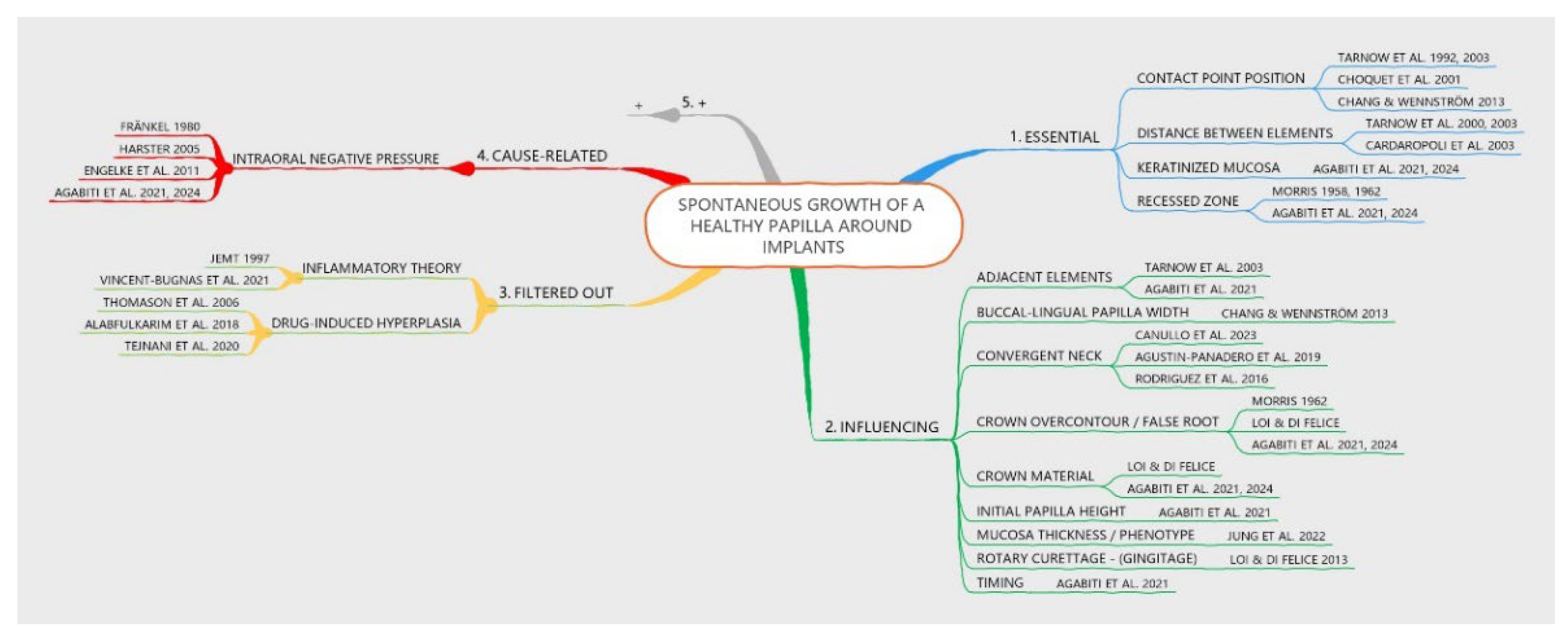

Table 1.
A post-hoc analysis of data from a previously published study. The gain in score between the baseline (initial score) and the last follow-up is reported at the mesial and distal aspects.
Table 1.
A post-hoc analysis of data from a previously published study. The gain in score between the baseline (initial score) and the last follow-up is reported at the mesial and distal aspects.
| Mesial aspect | Distal aspect | ||
|---|---|---|---|
| Initial score | Gain | Initial score | Gain |
| 0 | 2.1 | 0 | 1.8 |
| 1 | 1.0 | 1 | 1.0 |
| 2 | 0.5 | 2 | 0.7 |
| The following Jemt`s score3 was adopted: 0, absence of papilla; 1, less than half of interdental embrasure height; 2, more than half of interdental embrasure height; 3, fully papilla filled interdental embrasure. | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



