
Submitted:
10 September 2024
Posted:
11 September 2024
You are already at the latest version
Abstract
Background/Objectives: Periodontitis (P), a chronic inflammatory condition that affects the supportive tissues around the teeth, is 3 to 4 times more prevalent in individuals with diabetes mellitus (DM), with a direct correlation between its severity and the levels of glycosylated haemoglobin (HbA1c). This study aimed to evaluate the periodontal clinical parameters following non-surgical periodontal treatment (NSPT) in patients with and without type 2 DM and P. Methods: Forty patients with P were divided into two groups: Group DM/P and Group P. All patients were assessed at baseline, and 90 and 180 days after receiving NSPT. The parameters evaluated included HbA1c levels, plaque index (PI), probing pocket depth (PPD), clinical attachment level (CAL), and bleeding on probing (BoP). Statistical analysis was performed with a significance level set at α = 5%. Results: There were significant differences in HbA1c levels between the DM/P and P groups at baseline, 90, and 180 days, as expected. Importantly, HbA1c levels did not change after NSPT. Group P showed a significant reduction in both PI and BoP values at 90 and 180 days (p < 0.05). In contrast, group DM/P demonstrated a significant increase in the percentage of sites with PPD ≥ 5mm at 180 days (p < 0.05). Additionally, group P exhibited an increase in sites with PPD ≤ 4mm and a decrease in sites with PPD ≥ 5mm at both 90 and 180 days (p < 0.05). Conclusions: Our findings suggest that DM may compromise the effectiveness of NSPT, potentially hindering favorable outcomes during the follow-up period.
Keywords:
Diabetes mellitus
; periodontitis
; periodontal disease
; scaling and root planing
; glycated hemoglobin
1. Introduction
Diabetes mellitus (DM), a chronic metabolic disease, is characterized by either a partial or total deficiency in insulin production (type 1 DM) or periphery resistance to insulin's action (type 2 DM). This condition disrupts glucose, protein, and lipid metabolism, leading to hyperglycemia and multiple systemic abnormalities [1], in which periodontitis being considered the sixth complication associated with DM. By 2045, it is estimated that nearly 693 million people will have DM, with approximately 90% of cases being type 2 DM [2,3].
DM can be classified into several types, including type 1, type 2, gestational, and other specific types [4]. DM1 results from the destruction of β-cells in the pancreatic islets of Langerhans, leading to complete insulin insufficiency, which may be associated with autoimmune processes or have an idiopathic origin. DM2, on the other hand, is a heterogeneous syndrome caused by defects in both insulin secretion and action, with its pathogenesis linked to genetic and environmental factors [5]. DM2 is the most common form and typically progresses from insulin resistance (reduced sensitivity of target tissues to insulin) to insulin deficiency due to secondary β-cell failure in the pancreas [1]. The incidence and prevalence of type 2 DM have been rising around the world, making it one of the most widespread diseases globally [6]. Symptoms of type 2 DM include polyuria (excessive urine production), polydipsia (increased thirst), weight loss, sometimes accompanied by polyphagia (excessive appetite), and blurred vision. Obesity is a significant risk factor for the disease [7].
Since 2009, glycosylated haemoglobin (HbA1c) has been used as a diagnostic marker for DM. HbA1c represents a fraction of hemoglobin formed in the presence of hyperglycemia; thus, higher blood glucose levels result in a higher proportion of HbA1c [8]. The HbA1c test is advantageous because it provides an estimate of average blood glucose levels over the previous 60 to 90 days, unlike fasting blood glucose or glucose tolerance tests, which measure glucose at specific points in time. Monitoring HbA1c is essential for evaluating glycemic control and reducing the incidence of complications [9].
Periodontitis, a multifactorial chronic inflammatory condition associated with dysbiotic bacterial plaque biofilm, is characterized by the progressive destruction of the tissues that support the teeth, including periodontal ligament, cement and alveolar bone [10,11]. The disease develops in response to bacterial presence and their toxins, triggering an immune-inflammatory response [12,13]. This process involves the release of pro-inflammatory cytokines, which influence immune cell activity, differentiation, proliferation, and survival, and also regulate the production and activity of other cytokines, either amplifying (pro-inflammatory) or attenuating (anti-inflammatory) the inflammatory response [14]. Of importance, periodontitis has been linked to aggravate other non-communicable chronic conditions such as cardiovascular disease [15,16], rheumatoid arthritis [17-19], DM [20,21], and nonalcoholic fatty liver disease [22].
The intensity of this response depends on both the pathogenicity of the microorganisms present and the host's susceptibility, which can lead to the destruction of periodontal tissues [23]. The bidirectional relationship between diabetes and periodontitis has been extensively studied [24-28]. DM is a major risk factor for periodontitis, with studies indicating that the risk of developing periodontitis is approximately 3 to 4 times higher in patients with poor glycemic control compared to normal glycemic patients [29-31]. Moreover, there is a direct relationship between the level of glycemic control and the severity of periodontitis [32]. Research suggests that DM reduces collagen levels in periodontal tissues, hinders collagen synthesis, and increases the degradation of the connective tissue [33]. Additionally, in individuals with DM, proteins undergo glycation, leading to the formation of advanced glycation end products (AGEs). These AGEs have various cellular interactions, including altering macrophage function and stimulating the release of inflammatory mediators such as growth factors and cytokines, which prolong the inflammatory response [34].
Non-surgical periodontal treatment (NSPT) interventions typically include oral hygiene instructions (OHI) and subgingival instrumentation (SI), sometimes combined with supportive therapies [35,36], such as chemical methods for plaque control. The "gold standard" for maintaining periodontal health is the mechanical removal of dental biofilm through conventional debridement, which is an effective approach to treating periodontitis [36]. SI is considered a fundamental and conventional therapy in periodontal treatment [37]. This approach reduces pathogenic microorganisms, decreases probing pocket depth (PPD), reduces bleeding on probing (BoP), and promotes clinical attachment level (CAL) gain [37]. SI effectively controls the inflammatory process and reduces PPD in patients with periodontitis [36]. However, the method used in SI is not the most critical determinant of periodontal treatment success [38]. The success of NSPT depends on a combination of detailed root debridement, adequate periodontal maintenance therapy, and patient compliance [37].
SI directly impacts HbA1c levels since the formation of AGEs is associated with prolonged exposure to hyperglycemia, which is a significant factor in the complications of DM and the impaired host response. This impaired response affects connective and vascular tissue, which in turn hinders tissue healing and promotes the progression of periodontitis [39]. Previous recent studies have shown that SI is effective in reducing the levels of HbA1c [40-42] in diabetic patients. Conversely, SI is less successful in decreasing the CAL or reduced inflammation in DM patients with P when compared to systemic health patients with P. Therefore, this study aimed to evaluate the effect of NSPT on both periodontal clinical parameters and glycemic metabolic control in patients with or without DM. The null hypothesis is that NSPT will not alter either periodontal parameters or glycemic metabolic control.
2. Materials and Methods
2.1. Study Design
This non-randomized clinical trial was conducted at a single facility between September 2020 and January 2021. The study protocol was submitted to and approved by the Research Ethics Committee of the Faculty of Dentistry of Araçatuba (CAAE: 15049819.1.0000.5420). It was also registered with the Brazilian Registry of Clinical Trials (RBR-777nzpz) on the International Clinical Trials Registry Platform (U1111-1299-1687), following the guidelines of the CONSORT Statement for clinical trials.
2.2. Sample Calculation
Based on previous studies [43,44], the sample size was calculated to achieve 80% power (α = 5%; type B error = 20%) for detecting a significant difference of 1 mm in PPD between the experimental groups, assuming a standard deviation of 0.90 mm. Consequently, a total of 15 patients were required. To account for a 20% attrition rate, 20 patients per group were included.
2.3. Sample Selection
A total of 40 individuals, aged 36 to 70 years, were included in this study. Twenty participants with poorly controlled type 2 DM (HbA1c ≥ 7.0%) and periodontitis were assigned to the DM/P group, while 20 participants with periodontitis but without DM (HbA1c ≤ 6.5%) were assigned to the P group.
Inclusion criteria were as follows: individuals of both sexes aged 30 to 70 years; diagnosis of stage II, III, or IV periodontitis [25]; no periodontal treatment within the last 3 months; a minimum of 15 teeth, excluding third molars; and, for the DM/P group, a diagnosis of type 2 DM (HbA1c ≥ 7.0%), while for the P group, no diagnosis of type 2 DM (HbA1c ≤ 6.5%).
Exclusion criteria included current or former smokers; individuals with anemia; those with active cancer or a history of chemotherapy; a history of antibiotic or anti-inflammatory therapy within the last 6 months; blood disorders; pregnancy; chronic kidney disease; those currently undergoing orthodontic treatment; and individuals requiring prophylactic antibiotic therapy [45].
Participants were recruited from the Periodontics Clinic of the School of Dentistry at Araçatuba – UNESP. Prior to enrollment, patients were thoroughly informed about the etiology of periodontitis and given OHI tailored to their needs, including the use of toothbrushes, dental floss, and interproximal brushes. Those who expressed interest in participating signed an informed consent form.
2.4. Examiner Calibration
Before the experimental phase, intra-examiner calibration was performed on 2 individuals, with 170 sites evaluated. Duplicate measurements of PPD and CAL were taken on two separate occasions, one week apart. The intra-examiner agreement for PPD and CAL was assessed using the Kappa test, yielding a value of 0.88, indicating substantial agreement.
2.5. Experimental Design and Treatment
Initial treatment for periodontitis consisted of NSPT combined with OHI. Participants underwent a 2-hour session of scaling and root planing (SRP) using an ultrasonic device (Dabi Atlante, Ribeirão Preto, SP, Brazil) and manual Gracey and McCall curettes (Hu-Frieday, Chicago, IL, USA), in accordance with clinical practice guidelines [36]. All SRP procedures were performed by a single, experienced periodontist (L.C.G.B.).
One week after SRP, participants were visually inspected for any adverse signs or symptoms. Follow-up visits were conducted at 90 and 180 days, during which clinical examinations were repeated, and laboratory tests were conducted using the same parameters as at baseline. During these follow-up visits, supragingival plaque control and OHI were reinforced according to each participant’s needs [15].
2.6. Primary and Secondary Clinical Outcomes
All clinical periodontal parameters were measured using a millimeter periodontal probe (PCPUNC-15, Hu-Friedy Co., Chicago, IL, USA). A single, previously calibrated, blinded examiner (J.V.S.R.) performed the clinical examinations at baseline, 90, and 180 days post-treatment. The primary clinical outcome was the reduction in PPD. Secondary outcomes included the number of teeth, CAL gain, BoP at all tooth sites (excluding third molars), plaque index (PI) across four sites per tooth, and HbA1c levels.
2.7. Clinical Analysis
Clinical data were tabulated, and the percentages of sites with PPD and CAL were categorized accordingly. The categorical data for PI and BoP were also converted into percentages, as previously described [46]
2.8. Glycemic Analysis
Glycemic control and the participants’ previous history of diabetes were assessed through a questionnaire (anamnesis) and the results of fasting blood glucose and glycated hemoglobin tests, which were conducted at baseline and 90 and 180 days after NSPT were recorded.
2.9. Statistical Analysis
Demographic data, clinical periodontal parameters, and HbA1c results were organized using Microsoft Excel and subjected to descriptive and analytical statistical analysis with GraphPad Prism 6.0. A significance level of 5% was established. The null hypothesis was rejected if p≤0.05. The data were tested for normality using the Shapiro-Wilk, D'Agostino & Pearson, and Kolmogorov-Smirnov tests. Since the data followed a normal distribution (p>0.05), parametric tests were applied.
The demographic characteristics of the studied sample, which remained stable during the evaluation period, are presented in Table 1, including age (mean and standard deviation) and sex (number and percentage of individuals in each sex). Clinical periodontal parameters and glycated hemoglobin levels were compared using repeated measures ANOVA with Tukey's post hoc test across baseline, 90 days, and 180 days. Comparisons between different groups (Group DM/P vs. Group P) at each time point were evaluated using the t-test. The results are presented in Table 2 as mean and standard deviation (SD).
3. Results
The results of this non-randomized clinical trial demonstrated that out of 64 participants considered for the study, 24 were excluded due to not meeting the eligibility criteria, leaving a total of 40 participants for the clinical study. In Group DM/P, three participants did not return for reevaluation, resulting in a final sample size of 17. In Group P, one participant was excluded due to antibiotic use during the study, resulting in a final sample size of 19. Figure 1 illustrates the flowchart for the initial sample composition.
The sample composition analysis revealed demographic and social homogeneity across groups, as detailed in Table 1. Participants' ages ranged from 36 to 70 years. The mean age in Group DM/P was 50.94 ± 11.55 years, whereas Group P had a mean age of 59.32 ± 8.29 years (p=0.01). Group P was older than Group DM/P, indicating a lower predisposition to diabetes and a longer duration of periodontal destruction in Group P compared to Group DM/P, which develops the disease earlier and more severely. The predominant gender in Group DM/P was male, while Group P was predominantly female. Ethnically, most participants identified as white, followed by mixed race and, to a lesser extent, black. Educational levels were similar across groups, with most participants having incomplete secondary education and a minority holding a university degree.
Table 2 compares periodontal clinical variables and HbA1c values at baseline, 90 days, and 180 days. There was no significant difference in the number of teeth between groups at baseline (p>0.05). However, Group DM/P exhibited greater tooth loss at 180 days (p<0.05). For PI) values, Group P showed a reduction at 90 and 180 days (p<0.05), whereas Group DM/P had no significant changes in PI over time.
Regarding BoP, Group DM/P showed an increase at 180 days, though not statistically significant (p>0.05). Group P demonstrated significant improvement in BoP at both 90 and 180 days compared to baseline (p<0.05).
There were fewer sites with PPD ≤ 4mm across both groups at baseline, with no significant difference. However, Group P experienced an increase in these sites at 90 and 180 days. Significant differences in the percentage of sites with PPD ≥ 5mm were observed between groups at baseline, 90, and 180 days (p<0.0001), with Group DM/P showing higher percentages. Additionally, Group DM/P demonstrated an increase in P PD ≥ 5mm at 180 days.
For CAL ≤ 3mm, no improvement was observed in Group DM/P at any time point. In contrast, Group P showed significant gains in CAL at 90 and 180 days compared to baseline. Both groups showed an increase in CAL for sites with CAL 4-5mm at 180 days, with Group P showing greater gains compared to Group DM/P at 90 days (p=0.001). The percentage of sites with CAL ≥ 6mm increased in Group P at 90 and 180 days compared to baseline. Group P had a higher percentage of CAL gain in sites with CAL ≥ 6mm compared to Group DM/P at baseline (p<0.0001), 90 days (p<0.01), and 180 days (p<0.001). Group P also had a higher CAL gain for CAL ≤ 3mm compared to Group DM/P at 90 and 180 days (p<0.0001).
Among diabetic patients, all participants had inadequate metabolic control, with HbA1c values greater than 7%. No significant differences were found within groups over time, but significant differences were observed between groups (p<0.0001).
Figure 2 presents the Pearson correlation matrix for the analyzed variables, including group, number of teeth, PI, BoP, and clinical outcome "clinical endpoint." The correlations, accompanied by p-values, indicate statistical significance. A strong negative correlation was observed between "group" and "clinical endpoint" (r = -0.94; p < 0.001), suggesting that group membership is a key determinant of clinical outcomes. A moderate negative correlation was found between BoP and clinical endpoint"\ (r = -0.47; p = 0.01), indicating that higher BoP levels are associated with a lower likelihood of achieving the clinical endpoint. Conversely, number of teeth (r = 0.17; p = 0.35) and PI (r = -0.21; p = 0.25) showed weak, non-significant correlations with the clinical endpoint, suggesting limited influence on the outcome. These results highlight that group and BoP are the main predictors of the clinical outcome, whereas number of teeth and PI have minimal association.
Additional comorbidities observed in Group DM/P included arterial hypertension, with around 65% of participants reporting the development of new conditions alongside their hyperglycemic status. Metformin (500 mg) was the most frequently used anti hyperglycemic medication among diabetic participants. Table 3 demonstrated the number of patients that have reached the clinical endpoint, established with ≤ 4 sites with PD ≥ 5mm after treatment. The results demonstrated that after 90 days 14 patients out of 19 achieved the endpoint. Similarly, after 180 days post-operative, 16 patients out of 19 reached the desired endpoint. Conversely, none of the participants in the DM/P group achieved the established endpoint of the study.
4. Discussion
Periodontitis and DM are chronic diseases with high global prevalence [47]. DM is characterized by chronic hyperglycemia [48], while periodontitis is a multifactorial chronic inflammatory disease associated with dysbiotic biofilm, leading to progressive destruction of the supporting periodontal structures [10]. Both conditions can trigger inflammatory immune responses locally and systemically. DM is considered a risk factor for periodontitis, influencing its progression. Conversely, hyperglycemic status (HbA1c ≥ 7) can accelerate periodontitis progression [49], making this association bidirectional. Therefore, the aim of this study was to investigate the clinical periodontal parameters in patients with DM following NSPT. Our findings indicate that DM impaired the clinical periodontal parameters, such as BoP, PI, PPD and diminished the CAL gain. Our data suggest that DM effectively deteriorates periodontal tissue and aggravates the severity of PPD and CAL after 6 months post-operatively.
Interventions for periodontitis typically include OHI, SRP, and in some cases, systemic or local antibiotics [24]. Mechanical debridement (subgingival instrumentation) remains the gold standard for maintaining periodontal health. However, deep periodontal pockets, furcation lesions and areas of limited assess may require adjunctive treatments to effectively manage the disease. Systemic antibiotic therapy, such as low-dose doxycycline combined with SRP, has been shown to statistically reduce HbA1c levels in diabetic patients [50]. In this study, SRP was performed without adjunctive therapies to strengthen the current evidence on the exclusive impact of DM on clinical periodontal parameters.
While some studies indicate that NSPT improves glycemic control in patients with type 2 DM and generalized chronic diseases [51-53], others studies report conflicting results, including an increase in HbA1c levels post-NSPT [54-56]. This study's findings align with these discrepancies, as no significant improvement in HbA1c levels was observed in-group DM/P at 90 or 180 days, though a modest average reduction of 0.23% was noted at 90 days, partially rejecting the null hypothesis. Meta-analyses on the effects of periodontal treatment on glycemic control in diabetic patients also show mixed results due to various metabolic changes [54,56]. The bidirectional relationship between DM2 and periodontitis suggests that type 2 DM increases the risk of periodontitis in poorly controlled patients and that periodontal inflammation can adversely affect glycemic control [57,58]. This study underscores the importance of this relationship. Potential explanations for the study's findings include patient non-compliance with biofilm control, psychosocial factors exacerbated by the COVID-19 pandemic, and uncontrolled variables such as changes in hypoglycemic medication use, dietary habits, and overall health management. Despite stable HbA1c levels during follow-up, NSPT aided in stabilizing glycaemia.
Periodontal parameters in-group DM/P was less favorable compared to group P, which showed significant improvement after NSPT. Group P presented participants that were older compared to the DM/P individuals associated with advanced gingival recession, which resulted in a higher percentage of sites with CAL > 6 mm, indicative of advanced periodontitis. Group P also exhibited a greater reduction in deep pockets and a higher percentage of sites with CAL ≤ 3 mm, indicating improved clinical attachment levels. Both groups experienced a loss of clinical attachment in sites with CAL 4-5 mm by 180 days.
Patients with uncontrolled hyperglycemic status experience systemic complications due to chronic hyperglycemia, which exacerbates the formation of AGEs and affects immune response and tissue integrity [59]. The bidirectional association between type 2 DM and periodontitis was evident, as DM exacerbates periodontitis and periodontal inflammation adversely affects glycemic control [27]. Some studies suggest that NSPT can improve oral health and have positive effects on metabolic control, including glycemic and lipid metabolism, and systemic inflammation in type 2 DM patients. However, others study, like the work conducted by Baeza et al. [32], have found NSPT to have minimal impact on metabolic control and systemic inflammation. Mohan et al. [60] reported that SRP led to greater changes in C-reactive protein (CRP) levels in patients with type 2 DM, emphasizing the marked systemic changes in this group.
Chen et al. [61] observed a significant association between improved periodontal status and decreased CRP levels, suggesting that NSPT contributes to better systemic inflammatory status and reduces the risk of microvascular complications in diabetics. The present study found significant reductions in the PI at 90 and 180 days in Group P. Conversely, group DM/P showed higher PI values, reflecting greater difficulty in maintaining plaque control, which is consistent with findings by Khader et al. [62], Shanmukappa et al. [63], and Bissong et al. [64], who reported worse oral hygiene in diabetic patients compared to non-diabetics. However, Sandberg et al. [65] found no significant differences in daily tooth brushing practices between diabetic and non-diabetic patients, though non-diabetics had slightly better interproximal hygiene. Jiang et al. [66] reviewed the impact of health plans and services during the pandemic, highlighting increased patient costs and healthcare spending, which may further challenge adherence to treatment.
5. Conclusions
This study concludes that patients with poorly controlled type 2 DM exhibit worse bacterial plaque control, greater progression of periodontitis, and increased severity compared to non-diabetic patients. Additionally, the response to initial NSPT was less favorable in diabetic patients, with no significant impact on glycemic control.
Author Contributions
Conceptualization, L.C.G.B., C.M.dS.F., J.V.S.R., T.C., R.S.dM., V.G.G., L.H.T.; Methodology, L.C.G.B., C.M.dS.F., J.V.S.R., T.C., R.S.dM., V.G.G., L.H.T.; Formal analysis and investigation, L.C.G.B., C.M.dS.F., J.V.S.R., T.C., R.S.dM., V.G.G., L.H.T.; Writing-original draft preparation, L.C.G.B., J.V.S.R., R.S.dM.; Writing-review and editing, L.C.G.B., C.M.dS.F., J.V.S.R., T.C., R.S.dM., V.G.G., L.H.T.; Funding acquisition, R.S.dM., V.G.G. and L.H.T.; Resources, V.G.G., C.M.dS.F. and L.H.T.; Supervision, V.G.G. and L.H.T. All authors have read and agreed to the published version of the manuscript.
Funding
This work has been carried out through funding by Coordenação de Aperfeiçoamento de Pessoal de Nível Superior-Brazil (CAPES), in the scope of CAPES/Print-Funding code: 001 (Process 88887.310463/2018-00). RSdM is currently supported by Sao Paulo Research Foundation - FAPESP (Fundação de Amparo a Pesquisa do Estado de Sao Paulo), grant #2023/15750-7.
Institutional Review Board Statement
The study was conducted after obtaining ethical approval from the Human Research Ethics Committee of the Dentistry School of Araçatuba (CAAE 15049819.1.0000.5420). It was also performed in accordance with the principles of the modified Helsinki code for human clinical studies, as revised in 2013. Written informed consent was obtained from each participant.
Informed Consent Statement
Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
Data generated in this research project is available by contacting the last author of this paper via email. It is stored electronically as Excel worksheets.
Acknowledgments
The authors would like to thank the Periodontics Department at the Araçatuba School of Dentistry, all the patients recruited at the São Paulo State University UNESP that consented to be part of this study and the Center for Dental Assistance to Persons with Disabilities (CAOE) at the São Paulo State University UNESP. We are extremely grateful to FAPESP and CAPES for supporting the researches and also for supporting this study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- American Diabetes, A. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2019. Diabetes Care 2019, 42, S13–S28. [Google Scholar] [CrossRef] [PubMed]
- Cho, N.H.; Shaw, J.E.; Karuranga, S.; Huang, Y.; da Rocha Fernandes, J.D.; Ohlrogge, A.W.; Malanda, B. IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res Clin Pract 2018, 138, 271–281. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Ley, S.H.; Hu, F.B. Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Nat Rev Endocrinol 2018, 14, 88–98. [Google Scholar] [CrossRef] [PubMed]
- Skyler, J.S.; Bakris, G.L.; Bonifacio, E.; Darsow, T.; Eckel, R.H.; Groop, L.; Groop, P.H.; Handelsman, Y.; Insel, R.A.; Mathieu, C. , et al. Differentiation of Diabetes by Pathophysiology, Natural History, and Prognosis. Diabetes 2017, 66, 241–255. [Google Scholar] [CrossRef]
- Cole, J.B.; Florez, J.C. Genetics of diabetes mellitus and diabetes complications. Nat Rev Nephrol 2020, 16, 377–390. [Google Scholar] [CrossRef]
- Mingrone, G.; Panunzi, S.; De Gaetano, A.; Ahlin, S.; Spuntarelli, V.; Bondia-Pons, I.; Barbieri, C.; Capristo, E.; Gastaldelli, A.; Nolan, J.J. Insulin sensitivity depends on the route of glucose administration. Diabetologia 2020, 63, 1382–1395. [Google Scholar] [CrossRef]
- Yaribeygi, H.; Farrokhi, F.R.; Butler, A.E.; Sahebkar, A. Insulin resistance: Review of the underlying molecular mechanisms. J Cell Physiol 2019, 234, 8152–8161. [Google Scholar] [CrossRef] [PubMed]
- International Expert, C. International Expert Committee report on the role of the A1C assay in the diagnosis of diabetes. Diabetes Care 2009, 32, 1327–1334. [Google Scholar] [CrossRef]
- Cao, R.; Li, Q.; Wu, Q.; Yao, M.; Chen, Y.; Zhou, H. Effect of non-surgical periodontal therapy on glycemic control of type 2 diabetes mellitus: a systematic review and Bayesian network meta-analysis. BMC Oral Health 2019, 19, 176. [Google Scholar] [CrossRef]
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F. , et al. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Periodontol, 2018; 89 Suppl 1, S173–S182. [Google Scholar]
- Van Dyke, T.E.; Bartold, P.M.; Reynolds, E.C. The Nexus Between Periodontal Inflammation and Dysbiosis. Front Immunol 2020, 11, 511. [Google Scholar] [CrossRef]
- Franco, E.J.; Pogue, R.E.; Sakamoto, L.H.; Cavalcante, L.L.; Carvalho, D.R.; de Andrade, R.V. Increased expression of genes after periodontal treatment with photodynamic therapy. Photodiagnosis Photodyn Ther 2014, 11, 41–47. [Google Scholar] [CrossRef] [PubMed]
- de Molon, R.S.; de Avila, E.D.; Cirelli, J.A.; Steffens, J.P. Periodontal research contributions to basic sciences: From cell communication and host-parasite interactions to inflammation and bone biology. Biocell 2022, 46, 633–638. [Google Scholar] [CrossRef]
- Figueredo, C.M.; Lira-Junior, R.; Love, R.M. T and B Cells in Periodontal Disease: New Functions in A Complex Scenario. Int J Mol Sci 2019, 20. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, J.V.S.; Claudio, M.M.; Franciscon, J.P.S.; Rosa, R.A.C.; Cirelli, T.; de Molon, R.S.; Figueredo, C.M.S.; Garcia, V.G.; Theodoro, L.H. The Effect of Non-Surgical Periodontal Treatment on Patients with Combined Refractory Arterial Hypertension and Stage III, Grade B Periodontitis: A Preliminary Prospective Clinical Study. J Clin Med 2023, 12. [Google Scholar] [CrossRef] [PubMed]
- Rosa, R.A.C.; Rodrigues, J.V.S.; Claudio, M.M.; Franciscon, J.P.S.; Mulinari-Santos, G.; Cirelli, T.; de Molon, R.S.; Gouveia Garcia, V.; Theodoro, L.H. The Relationship between Hypertension and Periodontitis: A Cross-Sectional Study. J Clin Med 2023, 12. [Google Scholar] [CrossRef] [PubMed]
- de Molon, R.S.; Rossa, C., Jr.; Thurlings, R.M.; Cirelli, J.A.; Koenders, M.I. Linkage of Periodontitis and Rheumatoid Arthritis: Current Evidence and Potential Biological Interactions. Int J Mol Sci 2019, 20. [Google Scholar] [CrossRef]
- de Aquino, S.G.; Abdollahi-Roodsaz, S.; Koenders, M.I.; van de Loo, F.A.; Pruijn, G.J.; Marijnissen, R.J.; Walgreen, B.; Helsen, M.M.; van den Bersselaar, L.A.; de Molon, R.S. , et al. Periodontal pathogens directly promote autoimmune experimental arthritis by inducing a TLR2- and IL-1-driven Th17 response. J Immunol 2014, 192, 4103–4111. [Google Scholar] [CrossRef]
- de Avila, E.D.; de Molon, R.S.; de Godoi Goncalves, D.A.; Camparis, C.M. Relationship between levels of neuropeptide Substance P in periodontal disease and chronic pain: a literature review. J Investig Clin Dent 2014, 5, 91–97. [Google Scholar] [CrossRef]
- Vlachou, S.; Loume, A.; Giannopoulou, C.; Papathanasiou, E.; Zekeridou, A. Investigating the Interplay: Periodontal Disease and Type 1 Diabetes Mellitus-A Comprehensive Review of Clinical Studies. Int J Mol Sci 2024, 25. [Google Scholar] [CrossRef]
- Lin, S.Y.; Sun, J.S.; Lin, I.P.; Hung, M.C.; Chang, J.Z. Efficacy of adjunctive local periodontal treatment for type 2 diabetes mellitus patients with periodontitis: A systematic review and network meta-analysis. J Dent 2024, 148, 105212. [Google Scholar] [CrossRef]
- Vegda, H.S.; Patel, B.; Girdhar, G.A.; Pathan, M.S.H.; Ahmad, R.; Haque, M.; Sinha, S.; Kumar, S. Role of Nonalcoholic Fatty Liver Disease in Periodontitis: A Bidirectional Relationship. Cureus 2024, 16, e63775. [Google Scholar] [CrossRef] [PubMed]
- Vieira Colombo, A.P.; Magalhaes, C.B.; Hartenbach, F.A.; Martins do Souto, R.; Maciel da Silva-Boghossian, C. Periodontal-disease-associated biofilm: A reservoir for pathogens of medical importance. Microb Pathog 2016, 94, 27–34. [Google Scholar] [CrossRef] [PubMed]
- de Molon, R.S.; Rodrigues, J.V.S.; Deroide, M.B.; da Silva Barbirato, D.; Garcia, V.G.; Theodoro, L.H. The Efficacy of Topical or Systemic Antibiotics as Adjuvants to Non-Surgical Periodontal Treatment in Diabetic Patients: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. J Clin Med 2024, 13. [Google Scholar] [CrossRef] [PubMed]
- Badiger, A.B.; Gowda, T.M.; Chandra, K.; Mehta, D.S. Bilateral Interrelationship of Diabetes and Periodontium. Curr Diabetes Rev 2019, 15, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Borgnakke, W.S. IDF Diabetes Atlas: Diabetes and oral health - A two-way relationship of clinical importance. Diabetes Res Clin Pract 2019, 157, 107839. [Google Scholar] [CrossRef] [PubMed]
- Oberti, L.; Gabrione, F.; Nardone, M.; Di Girolamo, M. Two-way relationship between diabetes and periodontal disease: a reality or a paradigm? J Biol Regul Homeost Agents 2019, 33, 153–159. [Google Scholar]
- Cavagni, J.; de Macedo, I.C.; Gaio, E.J.; Souza, A.; de Molon, R.S.; Cirelli, J.A.; Hoefel, A.L.; Kucharski, L.C.; Torres, I.L.; Rosing, C.K. Obesity and Hyperlipidemia Modulate Alveolar Bone Loss in Wistar Rats. J Periodontol 2016, 87, e9–17. [Google Scholar] [CrossRef]
- Saremi, A.; Nelson, R.G.; Tulloch-Reid, M.; Hanson, R.L.; Sievers, M.L.; Taylor, G.W.; Shlossman, M.; Bennett, P.H.; Genco, R.; Knowler, W.C. Periodontal disease and mortality in type 2 diabetes. Diabetes Care 2005, 28, 27–32. [Google Scholar] [CrossRef]
- Shlossman, M.; Knowler, W.C.; Pettitt, D.J.; Genco, R.J. Type 2 diabetes mellitus and periodontal disease. J Am Dent Assoc 1990, 121, 532–536. [Google Scholar] [CrossRef] [PubMed]
- Emrich, L.J.; Shlossman, M.; Genco, R.J. Periodontal disease in non-insulin-dependent diabetes mellitus. J Periodontol 1991, 62, 123–131. [Google Scholar] [CrossRef]
- Baeza, M.; Morales, A.; Cisterna, C.; Cavalla, F.; Jara, G.; Isamitt, Y.; Pino, P.; Gamonal, J. Effect of periodontal treatment in patients with periodontitis and diabetes: systematic review and meta-analysis. J Appl Oral Sci 2020, 28, e20190248. [Google Scholar] [CrossRef] [PubMed]
- Scardina, G.; Citarrella, R.; Messina, P. Diabetic Microagiopathy of Oral Mucosa Depends on Disease Duration and Therapy. Med Sci Monit 2017, 23, 5613–5619. [Google Scholar] [CrossRef] [PubMed]
- Pan, W.; Wang, Q.; Chen, Q. The cytokine network involved in the host immune response to periodontitis. Int J Oral Sci 2019, 11, 30. [Google Scholar] [CrossRef] [PubMed]
- Alberton Nuernberg, M.A.; Janjacomo Miessi, D.M.; Ivanaga, C.A.; Bocalon Olivo, M.; Ervolino, E.; Gouveia Garcia, V.; Wainwright, M.; Theodoro, L.H. Influence of antimicrobial photodynamic therapy as an adjunctive to scaling and root planing on alveolar bone loss: A systematic review and meta-analysis of animal studies. Photodiagnosis Photodyn Ther 2019, 25, 354–363. [Google Scholar] [CrossRef]
- Sanz, M.; Herrera, D.; Kebschull, M.; Chapple, I.; Jepsen, S.; Beglundh, T.; Sculean, A.; Tonetti, M.S.; Participants, E.F.P.W.; Methodological, C. Treatment of stage I-III periodontitis-The EFP S3 level clinical practice guideline. J Clin Periodontol 2020, 47 Suppl 22, 4–60. [Google Scholar] [CrossRef]
- Cobb, C.M.; Sottosanti, J.S. A re-evaluation of scaling and root planing. J Periodontol 2021, 92, 1370–1378. [Google Scholar] [CrossRef] [PubMed]
- Suvan, J.; Leira, Y.; Moreno Sancho, F.M.; Graziani, F.; Derks, J.; Tomasi, C. Subgingival instrumentation for treatment of periodontitis. A systematic review. J Clin Periodontol 2020, 47 Suppl 22, 155–175. [Google Scholar] [CrossRef]
- Soi, S.; Bains, V.K.; Srivastava, R.; Madan, R. Comparative evaluation of improvement in periodontal and glycemic health status of type 2 diabetes mellitus patients after scaling and root planing with or without adjunctive use of diode laser. Lasers Med Sci 2021, 36, 1307–1315. [Google Scholar] [CrossRef]
- Oliveira, V.B.; Costa, F.W.G.; Haas, A.N.; Junior, R.M.M.; Rego, R.O. Effect of subgingival periodontal therapy on glycaemic control in type 2 diabetes patients: Meta-analysis and meta-regression of 6-month follow-up randomized clinical trials. J Clin Periodontol 2023, 50, 1123–1137. [Google Scholar] [CrossRef]
- Dhingra, K.; Jeng, J.H. Does periodontal treatment improve glycaemic control in periodontitis patients with diabetes mellitus? Evid Based Dent 2023, 24, 12–14. [Google Scholar] [CrossRef]
- Simpson, T.C.; Clarkson, J.E.; Worthington, H.V.; MacDonald, L.; Weldon, J.C.; Needleman, I.; Iheozor-Ejiofor, Z.; Wild, S.H.; Qureshi, A.; Walker, A. , et al. Treatment of periodontitis for glycaemic control in people with diabetes mellitus. Cochrane Database Syst Rev 2022, 4, CD004714. [Google Scholar]
- Beiler, T.; de Mello Neto, J.M.; Alves, J.C.; Hamlet, S.; Ipe, D.; da Silva Figueredo, C.M. Impact of non-surgical periodontal treatment on salivary expression of cytokines related to bone metabolism. Odontology 2020, 108, 646–652. [Google Scholar] [CrossRef] [PubMed]
- Correa, F.O.; Goncalves, D.; Figueredo, C.M.; Gustafsson, A.; Orrico, S.R. The short-term effectiveness of non-surgical treatment in reducing levels of interleukin-1beta and proteases in gingival crevicular fluid from patients with type 2 diabetes mellitus and chronic periodontitis. J Periodontol 2008, 79, 2143–2150. [Google Scholar] [CrossRef] [PubMed]
- Davies, M.J.; D'Alessio, D.A.; Fradkin, J.; Kernan, W.N.; Mathieu, C.; Mingrone, G.; Rossing, P.; Tsapas, A.; Wexler, D.J.; Buse, J.B. Management of Hyperglycemia in Type 2 Diabetes, 2018. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2018, 41, 2669–2701. [Google Scholar] [CrossRef] [PubMed]
- Claudio, M.M.; Garcia, V.G.; Freitas, R.M.; Rodrigues, J.V.S.; Wainwright, M.; Casarin, R.C.V.; Duque, C.; Theodoro, L.H. Association of active oxygen-releasing gel and photodynamic therapy in the treatment of residual periodontal pockets in type 2 diabetic patients: A randomized controlled clinical study. J Periodontol 2024, 95, 360–371. [Google Scholar] [CrossRef]
- Preshaw, P.M.; Bissett, S.M. Periodontitis and diabetes. Br Dent J 2019, 227, 577–584. [Google Scholar] [CrossRef] [PubMed]
- Petersmann, A.; Muller-Wieland, D.; Muller, U.A.; Landgraf, R.; Nauck, M.; Freckmann, G.; Heinemann, L.; Schleicher, E. Definition, Classification and Diagnosis of Diabetes Mellitus. Exp Clin Endocrinol Diabetes 2019, 127, S1–S7. [Google Scholar] [CrossRef]
- Sanz, M.; Ceriello, A.; Buysschaert, M.; Chapple, I.; Demmer, R.T.; Graziani, F.; Herrera, D.; Jepsen, S.; Lione, L.; Madianos, P. , et al. Scientific evidence on the links between periodontal diseases and diabetes: Consensus report and guidelines of the joint workshop on periodontal diseases and diabetes by the International diabetes Federation and the European Federation of Periodontology. Diabetes Res Clin Pract 2018, 137, 231–241. [Google Scholar]
- Al-Zahrani, M.S.; Bamshmous, S.O.; Alhassani, A.A.; Al-Sherbini, M.M. Short-term effects of photodynamic therapy on periodontal status and glycemic control of patients with diabetes. J Periodontol 2009, 80, 1568–1573. [Google Scholar] [CrossRef]
- Chen, Y.F.; Zhan, Q.; Wu, C.Z.; Yuan, Y.H.; Chen, W.; Yu, F.Y.; Li, Y.; Li, L.J. Baseline HbA1c Level Influences the Effect of Periodontal Therapy on Glycemic Control in People with Type 2 Diabetes and Periodontitis: A Systematic Review on Randomized Controlled Trails. Diabetes Ther 2021, 12, 1249–1278. [Google Scholar] [CrossRef]
- Lee, J.Y.; Choi, Y.Y.; Choi, Y.; Jin, B.H. Efficacy of non-surgical treatment accompanied by professional toothbrushing in the treatment of chronic periodontitis in patients with type 2 diabetes mellitus: a randomized controlled clinical trial. J Periodontal Implan 2020, 50, 83–96. [Google Scholar] [CrossRef] [PubMed]
- Mauri-Obradors, E.; Merlos, A.; Estrugo-Devesa, A.; Jané-Salas, E.; López-López, J.; Viñas, M. Benefits of non-surgical periodontal treatment in patients with type 2 diabetes mellitus and chronic periodontitis: A randomized controlled trial. Journal of Clinical Periodontology 2018, 45, 345–353. [Google Scholar] [CrossRef] [PubMed]
- Corbella, S.; Francetti, L.; Taschieri, S.; De Siena, F.; Del Fabbro, M. Effect of periodontal treatment on glycemic control of patients with diabetes: A systematic review and meta-analysis. J Diabetes Invest 2013, 4, 502–509. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Lee, J.; Kim, W.K.; Lee, Y.K.; Kim, Y.S. HbA1c changes in patients with diabetes following periodontal therapy. J Periodontal Implan 2021, 51, 114–123. [Google Scholar] [CrossRef]
- Teshome, A.; Yitayeh, A. The effect of periodontal therapy on glycemic control and fasting plasma glucose level in type 2 diabetic patients: systematic review and meta-analysis. Bmc Oral Health 2016, 17. [Google Scholar] [CrossRef]
- Hong, M.; Kim, H.Y.; Seok, H.; Yeo, C.D.; Kim, Y.S.; Song, J.Y.; Lee, Y.B.; Lee, D.H.; Lee, J.I.; Lee, T.K. , et al. Prevalence and risk factors of periodontitis among adults with or without diabetes mellitus. Korean J Intern Med 2016, 31, 910–919. [Google Scholar] [CrossRef]
- Bui, F.Q.; Almeida-da-Silva, C.L.C.; Huynh, B.; Trinh, A.; Liu, J.; Woodward, J.; Asadi, H.; Ojcius, D.M. Association between periodontal pathogens and systemic disease. Biomed J 2019, 42, 27–35. [Google Scholar] [CrossRef]
- Genco, R.J.; Graziani, F.; Hasturk, H. Effects of periodontal disease on glycemic control, complications, and incidence of diabetes mellitus. Periodontol 2000 2020, 83, 59–65. [Google Scholar] [CrossRef]
- Mohan, M.; Jhingran, R.; Bains, V.K.; Gupta, V.; Madan, R.; Rizvi, I.; Mani, K. Impact of scaling and root planing on C-reactive protein levels in gingival crevicular fluid and serum in chronic periodontitis patients with or without diabetes mellitus. J Periodontal Implant Sci 2014, 44, 158–168. [Google Scholar] [CrossRef]
- Chen, L.; Luo, G.; Xuan, D.Y.; Wei, B.H.; Liu, F.; Li, J.; Zhang, J.C. Effects of Non-Surgical Periodontal Treatment on Clinical Response, Serum Inflammatory Parameters, and Metabolic Control in Patients With Type 2 Diabetes: A Randomized Study. Journal of Periodontology 2012, 83, 435–443. [Google Scholar] [CrossRef]
- Khader, Y.S.; Dauod, A.S.; El-Qaderi, S.S.; Alkafajei, A.; Batayha, W.Q. Periodontal status of diabetics compared with nondiabetics: a meta-analysis. J Diabetes Complications 2006, 20, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Shanmukappa, S.M.; Nadig, P.; Puttannavar, R.; Ambareen, Z.; Gowda, T.M.; Mehta, D.S. Knowledge, Attitude, and Awareness among Diabetic Patients in Davangere about the Association between Diabetes and Periodontal Disease. J Int Soc Prev Community Dent 2017, 7, 381–388. [Google Scholar] [CrossRef] [PubMed]
- Bissong, M.; Azodo, C.C.; Agbor, M.A.; Nkuo-Akenji, T.; Fon, P.N. Oral health status of diabetes mellitus patients in Southwest Cameroon. Odontostomatol Trop 2015, 38, 49–57. [Google Scholar] [PubMed]
- Sandberg, G.E.; Sundberg, H.E.; Wikblad, K.F. A controlled study of oral self-care and self-perceived oral health in type 2 diabetic patients. Acta Odontol Scand 2001, 59, 28–33. [Google Scholar] [CrossRef]
- Jiang, D.H.; Mundell, B.F.; Shah, N.D.; McCoy, R.G. Impact of High Deductible Health Plans on Diabetes Care Quality and Outcomes: Systematic Review. Endocr Pract 2021, 27, 1156–1164. [Google Scholar] [CrossRef]
Figure 1.
Flowchart of the study.
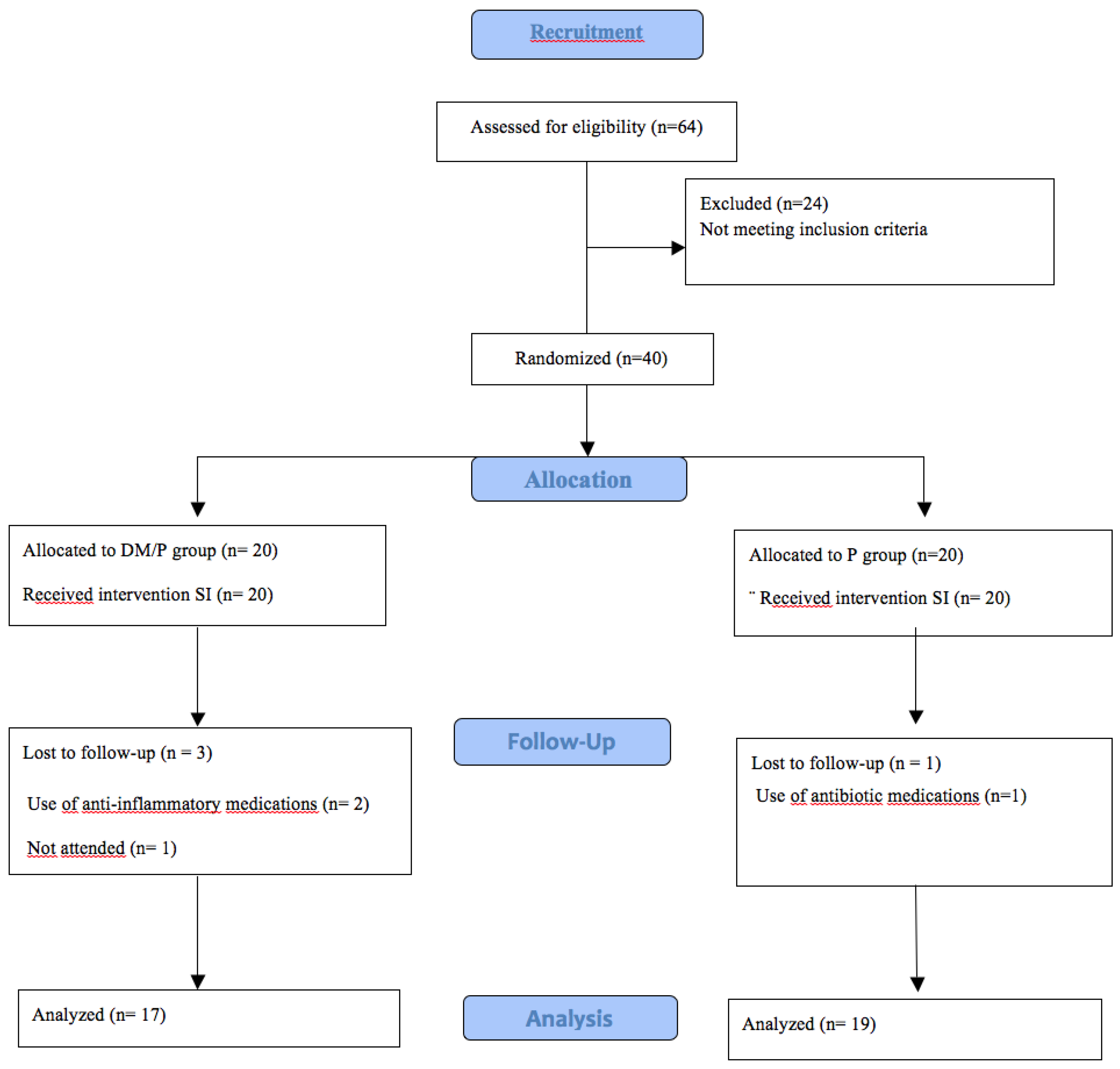
Figure 2.
Pearson Correlation Matrix between Predictor Variables and the Clinical Endpoint. Pearson correlation matrix between the variables "Group," "Number of Teeth," "Plaque Index (PI)," "Bleeding on Probing (BoP)," and the "Clinical Endpoint." The correlation values are accompanied by their respective p-values, indicated in parentheses. The intensity of the colors in the matrix reflects the strength and direction of the correlations, where colors closer to blue indicate negative correlations, and colors closer to red indicate positive correlations. Statistically significant correlations (p < 0.05) indicate important associations between the analyzed variables.
Figure 2.
Pearson Correlation Matrix between Predictor Variables and the Clinical Endpoint. Pearson correlation matrix between the variables "Group," "Number of Teeth," "Plaque Index (PI)," "Bleeding on Probing (BoP)," and the "Clinical Endpoint." The correlation values are accompanied by their respective p-values, indicated in parentheses. The intensity of the colors in the matrix reflects the strength and direction of the correlations, where colors closer to blue indicate negative correlations, and colors closer to red indicate positive correlations. Statistically significant correlations (p < 0.05) indicate important associations between the analyzed variables.
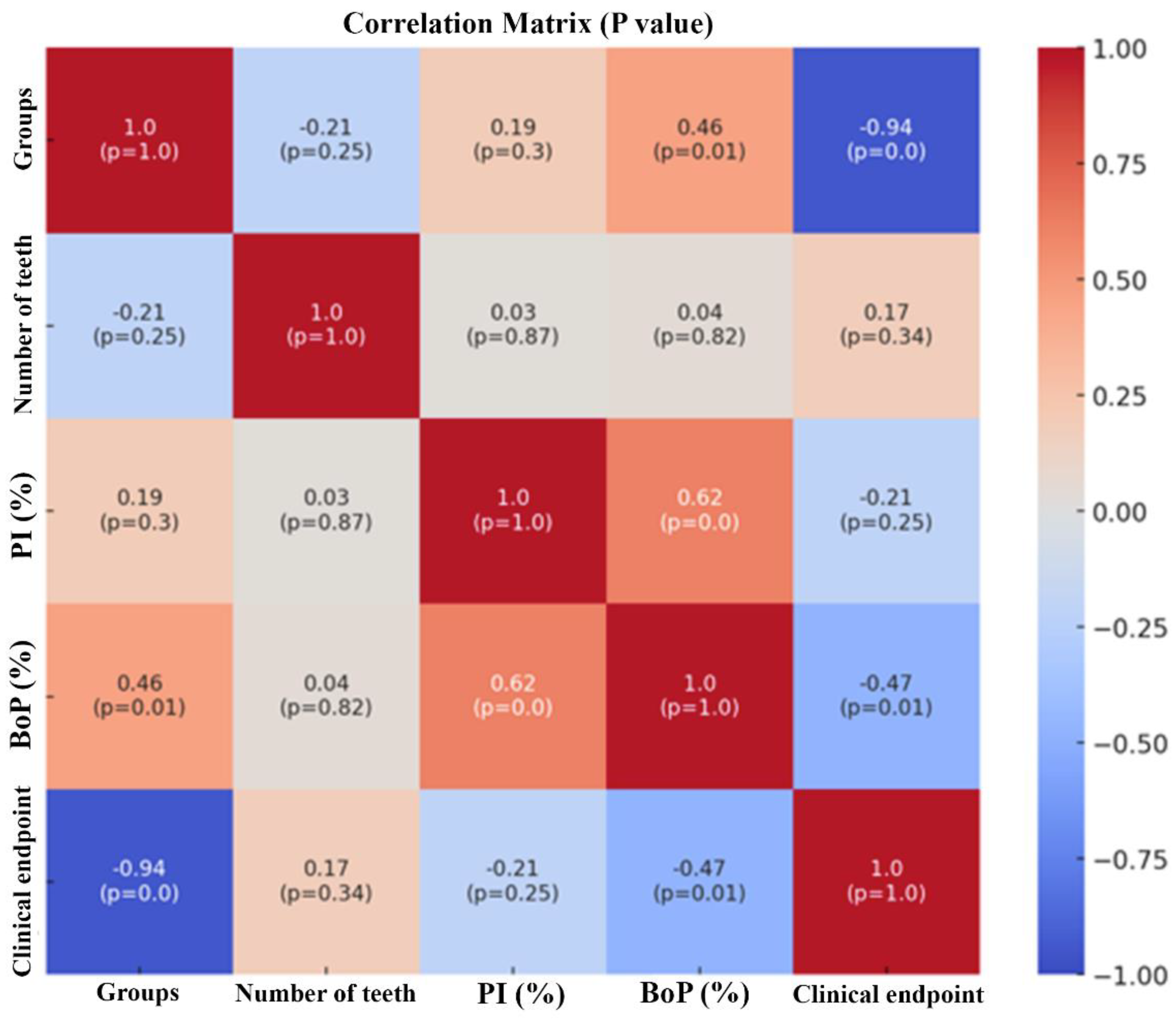

Table 1.
Demographic characteristics of the sample.
| Demographic characteristics | Group DM/P n=17 |
Group P n=19 |
p-value |
|---|---|---|---|
| Age - Mean (±SD) | 50.94 (± 11.55) | 59.32 (± 8.29) | 0.016 |
| Gender - n (%) | |||
| Male | 9 (52.94%) | 8 (47.06%) | NS |
| Female | 8 (42.11%) | 11 (57.89%) |
Abbreviations: SD, standard deviation, NS, not significant. Bold font, p-value <0.05. Comparison between the numerical variable (age) was made using the t test. To analyze the categorical variable (sex), the chi-square test was used.
Table 2.
Comparison of periodontal clinical parameters [mean (± SD)] and HbA1c levels evaluated at follow up periods.
Table 2.
Comparison of periodontal clinical parameters [mean (± SD)] and HbA1c levels evaluated at follow up periods.
| Parameter | Baseline | 90 days | 180 days |
|---|---|---|---|
| Tooth number | |||
| Group DM/P | 22.81 (±5.09)a | 22.19 (±5.17)a | 21.63 (±4.98)b |
| Group P | 23.41 (±4.11)a | 23.35 (±4.04)a | 23.29 (±4.01)a |
| PI (%) | |||
| Group DM/P | 41.84 (±30,15)a | 27.76 (±28.04)a | 27.16 (±21.08)a |
| Group P | 38.65 (±27,46)a | 15.06 (±6.77)b | 20.71 (±15.31)b |
| BoP (%) | |||
| Group DM/P | 29.15 (±11.93)a | 22.50 (±14.52) a | 35.46 (±26.90) a |
| Group P | 45.90 (±15.48)a | 20.97 (±9.65)b | 17.90 (±8.37)b |
| PPD ≤ 4mm (%) | |||
| Group DM/P | 70.05 (±25.27)a | 62.75 (±17.98) a | 55,96 (±19.86)a |
| Group P | 93.46 (±6.37)a | 98.92 (±1.55) b | 99.07 (±1.75) b |
| PPD ≥ 5mm (%) | |||
| Group DM/P | 32.09 (±19.83)a | 34.41 (±19.57) a | 43.23 (±19.51)b |
| Group P | 6.54 (±6.37)a**** | 1.08 (±1.55)b**** | 0.93 (±1.75)b**** |
| CAL ≤ 3mm (%) | |||
| Group DM/P | 31.34 (±18.73)a | 33.54 (±29.31)a | 23.07 (±19.38)a |
| Group P | 6.64 (±5.92)a**** | 1.10 (±1.59)b**** | 1.02 (±1.89)b**** |
| CAL 4-5mm (%) | |||
| Group DM/P | 58.05 (±17.50)a | 56.04 (±21.60)a,b | 67.81 (±18.25)b |
| Group P | 65.86 (±16.36)a | 75.06 (±14.24)a** | 76.12 (±15.25)b |
| CAL ≥ 6mm (%) | |||
| Group DM/P | 10.59 (±5.04)a | 11.58 (±12.40)a | 9.11 (±7.54)a |
| Group P | 27.50(±12.58)**** | 23.84 (±14.45)* | 22.85 (±14.49)** |
| HbA1c | |||
| Group DM/P | 9.01 (±2.09) a | 8.78 (±2.42) a | 8.89 (±2.12) a |
| Group P | 5.74 (±0.51)**** | 5.86 (±0.45)**** | 5.82 (±0.55)**** |
Abbreviations: SD, standard deviation; PI, plaque index; BoP, bleeding on probing; PPD, probing pocket depth, CAL, clinical attachment level; HbA1C, glycosylated haemoglobin A1c; a,b,c = different letter means statistically significant difference between the evaluated periods of the same group (p<0.05, repeated measures ANOVA test with Tukey's post-test). Comparisons between groups in the same period using the t test; *, p-value between 0.01-0.01 -0.05; **, p-value between 0.001-0.01; ***p-value between 0.0001-0.001; and ****<0.0001.
Table 3.
Analysis of the number of patients who reached the clinical endpoint of ≤ 4 sites with PD ≥ 5mm after treatment.
Table 3.
Analysis of the number of patients who reached the clinical endpoint of ≤ 4 sites with PD ≥ 5mm after treatment.
| Group DM/P | Group P | p-valor | |
|---|---|---|---|
| Variables | n=17 | n=19 | ** |
| Clinical endpoint, N (%) | |||
| Baseline | 0 (0) | 0 (100) | 1.000 |
| 90 days | 0 (0) | 14 (73.7%) | ≤0.0001 |
| 180 days | 0 (0) | 16 (84.2%) | ≤0.0001 |
** P-value of the comparison between groups in each evaluation period (Fisher test).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



