
Submitted:
11 September 2024
Posted:
11 September 2024
You are already at the latest version
Abstract
(1) Background: To further investigate the link between inadvertent tooth movements (ITMs) and mechanical properties of different retainers, the response upon vertical loading was compared in three different retainers (two stainless steel and one nickel-titanium). The influence of different reference teeth was also considered. (2) Methods: Three retainers (R1, R2, R3) were tested in a newly developed biomechanical analysis system (FRANS). They were bonded to 3D-printed models of the lower anterior jaw and vertically displaced up to 0.3mm. Developing forces and moments were recorded at the center of force. (3) Results: The vertical displacement caused vertical forces (Fz) and labiolingual moments (My) to arise. These were highest in the lateral incisors (up to 2.35±0.59N and 9.27±5.86Nmm for R1; 1.69±1.06N and 7.42±2.65Nmm for R2; 3.28±1.73N and 15.91±9.71Nmm for R3) for all analyzed retainers, and with the R3 retainer for all analyzed reference teeth, while the lowest Fz and My values were recorded with the R1 retainer. (4) Conclusions: Displacements of 0.2mm and larger provided forces and moments which could be sufficient to cause unwanted torque movements, such as ITMs in all analyzed retainers. Clinicians must be mindful of these risks and perform posttreatment checkups on patients with retainers of all materials.
Keywords:
biomechanics
; orthodontics
; retainer
; inadvertent tooth movements
; force
; torque
1. Introduction
After teeth have been moved orthodontically, it is necessary to stabilize them in their posttreatment position to prevent relapse [1,2,3]. This can be achieved by using fixed or removable retention devices [4]. Fixed bonded retainers have become increasingly popular since their introduction in the 1970s, as they are not dependent upon patient compliance [5,6]. Nowadays, most orthodontic retainers are made of thin multi-stranded stainless-steel (SS) wires [7]. Additionally, numerous non-metallic materials can be used for orthodontic retention, such as glass-fiber-reinforced composite [8] and PEEK [9]. Computer-aided-design (CAD) and computer-aided manufacturing (CAM) technology have also made it possible to use materials such as superelastic Nickel-Titanium (NiTi) [10], Titanium [11] and Yttria-stabilized zirconia [12] for the manufacturing of orthodontic retainers.
While twisted stainless-steel retainer wires represent the gold standard of orthodontic retention, they have become associated with unexpected complications, known as Inadvertent Tooth Movements (ITMs) [13]. ITMs involve a seemingly intact retainer and can occur as an X-Effect, in which a torque difference develops between two neighboring incisors, or as a Twist-Effect, in which one or both canines develop a labial or a lingual torque [13]. The prevalence of ITMs has been reported to lie between 1.1% and 5% [13,14,15], while some authors claim that moderate cases can be observed in up to 30% of patients [16]. Removal of the affected retainer wire can lead the ITM-malocclusion to partly reverse [17] and is the first step in treating ITMs. In severe cases of ITMs, orthodontic retreatment [18,19,20] or even extraction [21] can be required to restore a physiological tooth position and occlusal relationship.
The exact cause of ITMs has yet to be ascertained, although many hypotheses have been advanced. Some authors claim that patient-dependent features, such as pretreatment incisor inclination [14], age at debonding [14,16], or the persistence of oral dysfunctions [22] could be significant for the development of ITMs. Others suggest an iatrogenic influence, concluding that an important role is played by operator experience and wire passivity during bonding [13,20,23]. Still others propose that the cause of ITMs lies in the retainer wire itself, using “wire syndrome” [24] or “unintentionally active retainers” [7] as synonyms for Inadvertent Tooth Movements. A recent study highlights the role of the bonding site, theorizing that, in a bonding site without proper isolation, ITMs could be the clinical expression of teeth rotating around the retainer wire [25].
There have been several biomechanical studies regarding retainers in the past, most of which have focused predominantly on multistranded stainless steel retainers or on their comparison to other materials such as gold or glass-fiber reinforced composite [8,26,27,28,29,30]. Since the development of newer materials for orthodontic retainers, several studies have compared stainless-steel and CAD/CAM manufactured retainers in a clinical setting [31,32,33,34], while only few publications have analyzed these retainers from a biomechanical standpoint. In 2023, Roser et al. [35] analyzed a conventional SS retainer and six different CAD/CAM manufactured retainers in respect to aging and maximum load capacity. They found that the SS retainer performed better than all analyzed CAD/CAM manufactured retainers in both aspects, claiming that SS retainers could still be considered the gold standard.
To further understand the phenomenon of ITMs, and its relationship to different retainers, a new measurement system was developed and designed specifically for the biomechanical testing of retainers. The research question of this study was therefore to compare the resulting force and torque development of two stainless-steel (SS) retainers with a CAD/CAM fabricated nickel-titanium (NiTi) retainer, as well as the different force and moment development on different teeth at a standardized retainer bonding height.
2. Materials and Methods
2.1. Measurement Setup and Specimen
The Force-Torque Retainer Analysis System (FRANS) was developed in the Biomechanics Laboratory of the Department of Orthodontics and Dentofacial Orthopedics of the Ludwig-Maximilians University Hospital. Its purpose was to measure force and torque in relation to a vertical displacement, simultaneously in all three spatial planes. Forces and moments were measured at the center of force (CoF), which coincided with the retainer. The measurement setup is shown in Figure 1. It was designed using CAD software (Autodesk Inventor 2021, Autodesk, San Rafael, CA, USA) and had sockets for the placement of the lower canines and incisors (teeth 33, 32, 31, 41, 42, and 43). The sockets were perpendicular to the measurement table, simulating a lower incisor to mandibular plane angle (L1-ML) of 90°.
The table’s sagittal position was able to be altered to ensure a specific angulation of the vertical displacement force to the measured specimen, thus allowing the force to run through the specimen either perpendicularly, or at an angle.
The active element of the FRANS was a micrometer screw gauge, which, when activated, caused a continuous vertical displacement of a movable element perpendicular to the measurement table. This element was connected by means of coil springs and could only move along the vertical axis, ensuring that no unintentional movement occurred in other spatial planes. The screw gauge was also connected to a dial gauge, which allowed precise measurement of the obtained displacement with a resolution of 0.01 mm.
The experimental specimens were directly connected to a six-component Force/Torque Sensor (Force resolution 0.0125N, Moment resolution 0.626Nmm; Nano17 SI-50-0.5, ATI Industrial Automation, New York, NY, USA) using M3 screws, which were connected to an alterable pair of teeth. This allowed FRANS to analyze the effects of forces and moments acting upon these two reference teeth, as opposed to the whole arch. A computer program was specifically developed within LabVIEW 2020® (NI, Austin, TX, USA) to operate the test stand and to collect and analyze data while the measurements were being performed.
The scan of a patient who had completed orthodontic treatment was used as a template for the lower anterior region, from which the teeth were segmented and isolated using Autodesk Inventor 2021. A cylindric structure was then added basally to each tooth to simulate the root. The length of the simulated roots was based on average root length values for the respective tooth [36]. For each group, two teeth of the specimen were chosen as reference teeth and were designed with shorter roots and with M2 threads along their long axis, thus allowing the placement of the screws which connect the specimen to the sensor. The shorter roots allowed free movability of the respective teeth within the setup. All teeth in the setup were fabricated using a resin-based additive process with an SLA 3D printer (Formlabs 3Bt, Grey V4 resin, Formlabs GmbH, Berlin, Germany) set to a Z-resolution of 100 µm. The printed objects were postprocessed (washed and cured) following the device manufacturer’s protocol. After this, the inside of the burr holes was threaded manually with an M2 screw tap to accommodate the connecting screws. The teeth were printed en-bloc, ensuring a constant position of the teeth to each other, and separated with a fine cutting disc once the retainer had been bonded. This physical separation allowed each tooth to be biomechanically isolated from its neighboring teeth, the only connection between them being the retainer.
2.2. Measurement Procedure
Three retainer materials (R1, R2, and R3) were compared in this study with respect to their response to vertical loading up to 0.3 mm (Table 1). Each combination of reference teeth was analyzed (central incisors 31 and 41, lateral incisors 32 and 42, and canines 33 and 43) with a retainer of each type. Groups were formed to compare measurements with the same variables, with n=5 specimens per group and 45 total specimens. Each specimen was only measured once.
The two stainless steel retainers (R1 and R2) were adapted by using pliers and by hand, respectively. They were prepared with special attention to constant placement height, which was ensured by using a model with a visual marking to bend all retainers. All stainless-steel retainers were prepared by the same operator and checked for wire passivity by an experienced dental technician. The NiTi retainer (R3) was CAD/CAM manufactured and laser-cut from a superelastic NiTi sheet. Its placement height was determined through CAD software.
All retainers were bonded to the specimen in the middle third of the clinical crown using a silicone transfer jig and flowable composite (Transbond LV, 3M, St. Paul, MN, USA). Then, the connecting screws were placed inside the burr holes parallel to the long axis of the teeth. The specimens were placed into the sockets of the measuring table and the connecting screws were placed into contact with the sensor (magnified detail in Figure 1). The teeth were fixed in their sagittal position using Rendell-screws, ensuring force application through the long axis of these teeth. The FRANS was placed inside a temperature-controlled air-chamber, which was set at 36.0°C ±1.0°C to simulate body temperature. The temperature was controlled using a fan heater (PiccoVent, RO/SE Blechverarbeitung GmbH & Co. KG, Bad Birnbach, Germany). It was ensured that the measurement system was calibrated, and all forces and moments were equal to zero before the measurements were commenced.
The measurement was started by activating the micrometer screw gauge. A vertical force was applied continuously at a crosshead speed of 0.5 mm/min ±0.05 mm/min, extruding the specimen until a displacement of 0.3 mm was reached. During the measurement, force and torque values were recorded in all three spatial planes, at the center of force (CoF). Their values were recorded at a displacement range between 0 and 0.3 mm. In order to prevent collision between the base plate and the measured teeth the specimen had to be extruded rather than intruded, assuming that the force and torque tensors differ only by sign but not by value.
To analyze the effects of force and torque, a three-dimensional coordinate system was defined for each quadrant (Figure 2). The X-axis coincided with the labiolingual plane, the Y-axis coincided with the mesiodistal plane, while the Z-axis coincided with the vertical plane. A positive value on the Y-axis indicated a mesial movement, towards the midline; while a negative Y-value indicated a movement distally, away from the midline. According to the right-hand rule, in the lower left quadrant (33, 32, 31 according to the Fédération Dentaire Internationale (FDI) notation), a positive X-value indicated a labial movement, and a negative X-value indicated a lingual movement. Conversely, when considering the lower right quadrant (43, 42, 41 according to the FDI notation), a positive X-value denoted a lingual movement, and a negative X-value denoted a labial movement. In both quadrants, a positive Z-value illustrated an intrusion, a negative Z-value an extrusion. Thus, moments around the X-axis are indicative of mesiodistal tipping, moments around the Y-axis describe labiolingual torque, while moments around the Z-axis represent rotation around the tooth’s long axis.
Only measurements which reached 0.3 mm displacement with intact bonding sites were included in final data processing. Five measurements from the R1 group were excluded due to bonding failure: two had central incisors, two had lateral incisors, and one had canines as reference teeth. Eight measurements from the R2 group were also excluded due to bonding failure: all five measurements with central incisors as reference teeth were affected, as well as one with lateral incisors, and two with canines. One R3 measurement was excluded due to an incomplete failure and had central incisors as reference teeth.
The data from these measurements was analyzed using Excel 2016 (Microsoft Corporation, Redmond WA, USA), and OriginPro 2022b (OriginLab Corporation, Northhampton MA, USA). Descriptive statistics were performed in IBM SPSS 27 (IBM Corp., Armonk, NY, USA).
3. Results
The forces and moments measured during vertical loading at 0.1, 0.2 and 0.3 mm for the respective retainer groups are depicted in Table 2. The application of displacement caused forces and moments to arise in all three spatial planes.
Two aspects are examined in more detail. In the following, the focus is placed on Fz and My: the vertical force Fz is the direct acting component of the vertical displacement in case of mastication, while ITMs manifest as a labiolingual torquing moment (My). A curve of the measurements of all three analyzed retainers with the canines as reference teeth can be seen in Figure 3. The other samples showed comparable behavior.
3.1. Vertical Force
An increase in vertical displacement was accompanied by an increased vertical force Fz. At all levels of displacement, the lowest Fz values were observed in the R1 group with the canines as reference teeth ( 0.35±0.24N, 0.61±0.45N, and 0.88±0.63N), whereas the highest Fz values were found with the lateral incisors as reference teeth, in the R2 group for 0.1mm displacement, and in the R3 group for further displacements (1.04±0.71N, 2.06±1.09N, and 3.28±1.73N). The highest interquartile range (IQR) was observed when analyzing the lateral incisors, followed by the canines, whereas the central incisors showed a low IQR.
3.2. Labiolingual Moment
Labiolingual moments (My) increased in relation to vertical displacement as well. The lowest My values were observed in the R1 group with the central incisors as reference teeth at all levels of displacement (0.67±0.10 Nmm, 1.43±0.29 Nmm, and 2.01±0.43 Nmm). The highest My values were found in the R2 group with the lateral incisors as reference teeth at 0.1mm displacement (4.67±4.79 Nmm), while the highest My values arose in the R3 group with the lateral incisors as reference teeth (9.27±5.86 Nmm, and 15.91±9.71 Nmm) at 0.2 mm and at 0.3 mm displacement. Similarly to what was observed for the vertical force Fz, lateral incisors exhibited the highest IQR for My in almost all groups, followed by the canines, while the central incisors showed a low IQR.
Overall, R1 showed the lowest My values for the central incisors and canines, and comparatively low values for the lateral incisors at an initial displacement. Upon further displacement, R2 showed lower moment development than R1 at the lateral incisors. The results for My are depicted in Figure 5 and additionally shown in Table 2.
There were differences in force-moment expression when analyzing the data from measurements obtained from different reference teeth. The lateral incisors showed the highest forces and moments overall, in both intergroup and intragroup comparisons.
4. Discussion
The aim of the study was to investigate the resulting forces and moments upon loading of different retainers, considering differences in the individual teeth.
The R1 retainer showed the lowest forces and moments throughout displacement levels and comparably low forces and moments when considering reference teeth. While low force and moment development is favorable when considering physiological tooth mobility, it is also an expression of low resistance to torque, and, consequently, of the possible development of ITMs [26,37].
The results of the study highlight the direct proportionality of the vertical force component Fz and the labiolingual torquing moment My, as well as a general increase of force and moment amplitude with increasing displacement. The original data from the sensor showed a positive My moment in the third quadrant and a negative My moment in the fourth quadrant upon extrusion loading. According to the coordinate system (Figure 2), these moments are indicative of a lingual crown torque. Considering an in vivo setting, in which mastication forces lead to an intrusion of the mandibular anterior teeth, these moments would instead present as a labial crown torque of the affected reference teeth. Both situations reflect the clinical presentation of ITMs, which can manifest as a labial or as a lingual crown torque. The biomechanical situation during masticatory loading on one tooth is shown in Figure 6. The bonding site at which the retainer is fixed is assumed to be the center of rotation (CR). The masticatory force in Fz direction and distance d from the CR creates a labiolingual moment My, which might be involved in the development of ITMs.
We noted differences in force-moment development between the different materials being analyzed: lower forces and moments were present in the R1 group for all reference teeth. This is an expression of the low bending as well as torsional stiffness of multistranded retainer wires and of their acceptability with respect to physiological tooth movement [37]. The low stiffness of stranded SS wires has been previously described as a potential risk factor for the development of ITMs [26,38], as it cannot be excluded that a certain amount of torsion is already inherent in the wire due to manufacturing or is acquired while being subjected to masticatory forces [13,15,29]. Multistranded SS and NiTi wires seem to exhibit similar low stiffness, while NiTi exhibits higher flexibility and nonlinear elastic behavior [39]. The higher force and torque values recorded within the R3 group could be because this is the only retainer that did not consist of multiple stranded wires, but that was cut out of a single piece of sheet material. In addition, a marked difference could be seen when comparing the force-displacement and moment-displacement curves of the different retainer types. The R3 retainer (Figure 3e and 3f) produced more homogenous curves throughout all measurements, while the curves varied somewhat between individual measurements when considering R1 and R2 (Figure 3a and 3b, and 3c and 3d). While the R3 retainer is completely CAD/CAM manufactured and cut from a single NiTi sheet, the R1 and R2 retainers were bent using pliers and finger pressure, respectively. This could indicate that conventional retainers, being manufactured by humans rather than machines, are inherently less consistent in a testing situation compared to CAD/CAM manufactured products. We also noted differences in debonding behavior between different retainer materials and reference teeth. The highest number of debondings occurred in the R2 group, where they also occurred at lower displacements than in groups R1 and R3. This may be due to the flattened rectangular shape of the R2 retainer, which may not allow sufficient adhesion or even form fit between the composite and the wire surface. The more pronounced three-dimensional profile of the other two materials may allow for a better retention of the composite to the metal surface. In addition, the R2 retainer appears to have been rolled as part of its manufacturing process, while R1 has not. This signifies that the R1 retainer not only has a better form fit but allows for better adhesion of bonding and composite to its strands. The teeth most frequently affected by debondings were the central incisors, even though these teeth showed the lowest force-moment-developments in measurements without debondings.
When considering differences between reference teeth, the lateral incisors showed higher forces and moments than the other teeth. While other studies suggest that different behavior of the lateral incisors could be due to differences in root morphology [40], this influence could be excluded in our study since the roots were shaped uniformly and fixed mechanically into the base plate. It can be assumed that this may be due to the position of the lateral incisors within the retainer and its influence on the dissipation of bearing forces (Figure 7). While mastication forces are being applied to the lateral incisors (teeth 42 and 32), they are mechanically connected by short wire lengths at both sides of the point of force application. This leads to the development of moments, which potentially results in a rotation of the teeth around the retainer. In contrast, when a vertical force is applied to both central incisors (teeth 41 and 31), they are connected to each other by a flexible section of free wire mesially, with the mechanical fixation to the frame only on their respective distal side. This leads to lower stress in the retainer, and thus to lower amounts of generated moments. While the central and lateral incisors are supported on both sides by the retainer, the canines are only supported on one side. The canines are therefore less restricted in their movement compared to the incisors, leading to a lower force development Fz at the canines, which in return means that the retainer effect decreases. Additionally, the distance of free wire between the points of force application is longer between the canines than in all other setups, leading to higher moment development My due to the longer lever arms.
Several clinical studies have been performed to examine patient-dependent features of ITMs [14,22], while biomechanical in vitro studies analyzed the behavior of retainer materials under mechanical stress or loading. Sifakakis et al. [30] analyzed labiolingual and intrusive forces acting on three different stainless-steel retainer wires. Similarly to our results, they found that displacements of 0.2 mm in the vertical plane caused forces of 1 N or larger to arise. These forces would be sufficient to produce tooth movements despite the presence of a bonded retainer. In a follow up study [29], the same research group analyzed the effects of vertical force loading and unloading on different retainer materials to simulate the effects of mastication. All retainer types showed residual forces and moments after the loading phase, meaning that they had become active and that, consequently, ITMs could occur in a clinical setting. Additionally, it was hypothesized that the twist direction of the wire strands may have an influence on torque resistance, based on the assumption that it is significantly more difficult to strand a wire further than to untwist it against the direction of stranding. This effect could cause a different torsional moment on the teeth between the left and right lower quadrant, and, in turn, a more pronounced ITM manifestation on the twisted side of the retainer. This could be a decisive factor as to why some patients only develop ITM on one side, although further studies are needed to scientifically confirm this theory. Seide et al. [25] analyzed lingual retainers by applying horizontal force in vitro. They hypothesized that ITMs could occur due to unwinding of the wire at an intact wire-composite-interface, or due to rotation of the tooth around the wire at a compromised wire-composite-interface. This seems like a plausible explanation of this phenomenon. In contrast to the aforementioned study [25], we chose to apply a vertical force, since vertical forces (e.g. due to mastication) seem to act more directly on the retainer itself rather than horizontal ones. Our data seems to confirm a direct relationship between an increase in vertical force Fz and labiolingual torquing moment My, which is how ITMs present clinically. The application of a vertical displacement caused forces and moments to arise in all spatial planes, in accordance to the findings of Cooke and Sherriff [27]. This indicates that the FRANS offers a good simulation of the in-vivo situation, since a bonded retainer wire is subjected to multiple forces and moments, from multiple directions, such as vertical forces due to mastication and horizontal forces due to tongue function.
It is important to allow for a certain degree of horizontal and vertical tooth mobility during permanent retention, since failure to do so would result in detrimental effects, such as inactivity-related atrophy of the PDL [41]. This was already recognized by Schwarze et al. [28] in 1995, who performed in-vitro tests on various retainer materials to verify their compatibility with physiological tooth movement. They found the 0.0155” TwistFlex wire (Dentaflex, Dentaurum, Ispringen, Germany) to be acceptable in both an in vitro and an in vivo setting, even though tooth mobility was limited by the retainer. More recently, Roser et al. [37] compared the restriction of physiological tooth mobility in the presence of different retainer materials, including those used in our study in groups R1 and R3, in an in vitro investigation. They found that the NiTi retainer allowed more tooth mobility than the SS retainer but deemed both materials acceptable in regard to physiological tooth mobility.
The same research group also compared conventional SS retainers (analogous to group R1) to various CAD/CAM retainers (including those analyzed in group R3), in respect to simulated ageing and maximum load capacity [35]. In contrast to their findings, we found the NiTi retainer group to have the lowest bond failure rate of those analyzed. This may be due to the use of simulating ageing in the study by Roser et al. [35], and to differences in bonding protocol between studies: in our study, the surface of the specimen was not preconditioned, as synthetic resin (Grey V4) was used, and a sufficient bond strength with orthodontic resins was implied due to the characteristics of both materials. Vertical force values of 3.31 N and labiolingual torque values of up to 15.91 Nmm were reached, and debonding of the wire did not occur. This lies within the range of regular adhesive bond strength [42].
A significant difference between the FRANS and other biomechanical analysis systems, like the ones previously described [26,29,30] is the possibility to exert displacement only in one dimension. This may be seen as a limitation if dynamic measurements need to be performed, while the absence of unwanted movement in other dimensional planes may be an important advantage in other measurement setups, such as three-point-bending tests. In the FRANS setup, the measurement table can be moved in the sagittal dimension. This allows simulations of forces and moments acting upon protruded or retroclined lower incisors, or even for a comparison of buccal and lingual mechanics. The FRANS also allows a continuous application of displacement, and consequently of forces and moments, as opposed to an incremental application. This leads to a more accurate simulation of in-vivo conditions since biting forces are not exerted in constant increments in nature. Furthermore, the FRANS allows the analysis of two single, biomechanically isolated reference teeth directly. This provides important insight into the loading behavior of each tooth of the mandibular anterior arch, while also allowing a comparison between the behavior of different reference teeth.
Because of the design of the FRANS, it is possible to analyze only two symmetrical reference teeth at the same time: both central incisors, both lateral incisors, or both canines. In our study, the specimens were displaced for up to 0.3 mm vertically. Displacements of up to 0.2 mm have already been reported in in vivo studies on maxillary central incisors [43,44], as well as in in vitro biomechanical studies [29,30]. Since we did not consider an additional embedding of the specimen in a PDL-like structure, the specimens were displaced further, reaching 0.3 mm.
While there have been no clinical reports of ITMs with retainers other than multistranded SS retainers to the authors’ knowledge, the forces and moments recorded in this study could be sufficient to produce unwanted tooth movements with all analyzed retainer materials, especially when considering displacements of 0.2 mm or larger.
Further research is needed to exclude the possibility of ITMs arising from materials other than SS and to test the biomechanical properties of novel CAD/CAM developed retainer materials. While this present experimental setup simulated the effects of vertical displacement on two pairs of teeth at a time, future research could analyze the effects of a vertical displacement acting uniformly on the entire lower anterior segment.
5. Conclusions
The FRANS is a measurement system that can be reliably used to research the biomechanical properties of retainer wires and other orthodontic materials. In this present study, the development of forces and moments caused by a vertical displacement on different reference teeth was analyzed.
The forces and moments are expressed differently on each tooth in the lower anterior segment, with the lateral incisors in particular being exposed to higher force and torque levels than their neighboring teeth.
Our results show that a certain degree of labiolingual tooth movement can be expected when applying vertical forces, even though bonded retainers are present. All analyzed retainer materials showed a force and moment development sufficient to lead to the expression of unwanted torque movements such as ITMs. Clinicians should be mindful of this implication and check for ITM-like movements associated with retainers of materials other than stainless-steel. The clinician might also keep in mind that different retainer materials show different levels of force and moment development, and that these characteristics can impact physiologic tooth mobility and PDL health.
Author Contributions
Conceptualization, A.W. and M.M.; methodology, M.M. and H.S.; software, M.M. and H.S.; validation, L.H., M.M. and H.S.; formal analysis, F.T., L.H. and M.M.; investigation, F.T.; resources, A.W.; data curation, F.T.; writing—original draft preparation, F.T.; writing—review and editing, M.M., L.H. and H.S.; visualization, F.T. and L.H.; supervision, A.W. All authors have read and agreed to the published version of the manuscript.
Funding
The six component Force/Torque sensor (Nano17 SI-50-0.5, ATI Industrial Automation, New York, NY, USA) was provided by grants from the Friedrich-Baur-Stiftung (74/19). The CAD/CAM retainers were provided by SCHEU-DENTAL custom-made GmbH (Hilden, Germany) former CA Digital GmbH (Hilden, Germany).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Littlewood, S.J., Evidence-based retention: Where are we now? Seminars in Orthodontics, 2017. 23(2): p. 229-236.
- Melrose, C.; Millett, D.T. Toward a perspective on orthodontic retention?. Am. J. Orthod. Dentofac. Orthop. 1998, 113, 507–514, . [CrossRef]
- Reitan, K. Clinical and histologic observations on tooth movement during and after orthodontic treatment. Am. J. Orthod. 1967, 53, 721–745, . [CrossRef]
- Kramer, A., et al., Vacuum-formed retainer versus bonded retainer for dental stabilization in the mandible-a randomized controlled trial. Part I: retentive capacity 6 and 18 months after orthodontic treatment. Eur J Orthod, 2020. 42(5): p. 551-558.
- Littlewood, S.J.; Millett, D.T.; Doubleday, B.; Bearn, D.R.; Worthington, H.V. Retention procedures for stabilising tooth position after treatment with orthodontic braces. Cochrane Database Syst. Rev. 2016, 2016, CD002283, doi:10.1002/14651858.cd002283.pub4.
- Zachrisson, B.U. Clinical experience with direct-bonded orthodontic retainers. Am. J. Orthod. 1977, 71, 440–448, . [CrossRef]
- Padmos, J.A.; Fudalej, P.S.; Renkema, A.M. Epidemiologic study of orthodontic retention procedures. Am. J. Orthod. Dentofac. Orthop. 2018, 153, 496–504, . [CrossRef]
- Tacken, M.P.E.; Cosyn, J.; De Wilde, P.; Aerts, J.; Govaerts, E.; Vannet, B.V. Glass fibre reinforced versus multistranded bonded orthodontic retainers: a 2 year prospective multi-centre study. Eur. J. Orthod. 2010, 32, 117–123, . [CrossRef]
- Kadhum, A.S.; Alhuwaizi, A.F. The efficacy of polyether-ether-ketone wire as a retainer following orthodontic treatment. Clin. Exp. Dent. Res. 2021, 7, 302–312, . [CrossRef]
- Kravitz, N.D.; Grauer, D.; Schumacher, P.; Jo, Y.-M. Memotain: A CAD/CAM nickel-titanium lingual retainer. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 812–815, . [CrossRef]
- Koller, S.; Craveiro, R.B.; Niederau, C.; Pollak, T.L.; Knaup, I.; Wolf, M. Evaluation of digital construction, production and intraoral position accuracy of novel 3D CAD/CAM titanium retainers. J. Orofac. Orthop. Der Kieferorthopadie 2022, 84, 384–391, . [CrossRef]
- Stout, M.M.; Cook, B.K.; Arola, D.D.; Fong, H.; Raigrodski, A.J.; Bollen, A.-M. Assessing the feasibility of yttria-stabilized zirconia in novel designs as mandibular anterior fixed lingual retention after orthodontic treatment. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 63–73, . [CrossRef]
- Katsaros, C.; Livas, C.; Renkema, A.-M. Unexpected complications of bonded mandibular lingual retainers. Am. J. Orthod. Dentofac. Orthop. 2007, 132, 838–841, . [CrossRef]
- Kučera, J.; Marek, I. Unexpected complications associated with mandibular fixed retainers: A retrospective study. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 202–211, . [CrossRef]
- Renkema, A.M., et al., Long-term effectiveness of canine-to-canine bonded flexible spiral wire lingual retainers. Am J Orthod Dentofacial Orthop, 2011. 139(5): p. 614-21.
- Wolf, M.; Schulte, U.; Küpper, K.; Bourauel, C.; Keilig, L.; Papageorgiou, S.N.; Dirk, C.; Kirschneck, C.; Daratsianos, N.; Jäger, A. Post-treatment changes in permanent retention. J. Orofac. Orthop. Der Kieferorthopadie 2016, 77, 446–453, . [CrossRef]
- Knaup, I.; Bartz, J.R.; Schulze-Späte, U.; Craveiro, R.B.; Kirschneck, C.; Wolf, M. Side effects of twistflex retainers-3D evaluation of tooth movement after retainer debonding. J. Orofac. Orthop. Der Kieferorthopadie 2021, 82, 121–129, . [CrossRef]
- Kucera, J.; Streblov, J.; Marek, I.; Hanzelka, T. Treatment of Complications Associated with Lower Fixed Retainers. J Clin Orthod 2016, 50, 54–9.
- Pazera, P.; Fudalej, P.; Katsaros, C. Severe complication of a bonded mandibular lingual retainer. Am. J. Orthod. Dentofac. Orthop. 2012, 142, 406–409, . [CrossRef]
- Shaughnessy, T.G.; Proffit, W.R.; Samara, S.A. Inadvertent tooth movement with fixed lingual retainers. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 277–286, . [CrossRef]
- Singh, P. Canine avulsion: An extreme complication of a fixed mandibular lingual retainer. Am. J. Orthod. Dentofac. Orthop. 2021, 160, 473–477, . [CrossRef]
- Klaus, K.; Xirouchaki, F.; Ruf, S. 3D-analysis of unwanted tooth movements despite bonded orthodontic retainers: a pilot study. BMC Oral Heal. 2020, 20, 1–12, . [CrossRef]
- Egli, F.; Bovali, E.; Kiliaridis, S.; Cornelis, M.A. Indirect vs direct bonding of mandibular fixed retainers in orthodontic patients: Comparison of retainer failures and posttreatment stability. A 2-year follow-up of a single-center randomized controlled trial. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 15–27, . [CrossRef]
- Charavet, C.; Vives, F.; Aroca, S.; Dridi, S.-M. “Wire Syndrome” Following Bonded Orthodontic Retainers: A Systematic Review of the Literature. Healthcare 2022, 10, 379, . [CrossRef]
- Seide, M., et al., Inadvertent side effects of fixed lingual retainers : An in vitro study. J Orofac Orthop, 2022.
- Arnold, D.T.; Dalstra, M.; Verna, C. Torque resistance of different stainless steel wires commonly used for fixed retainers in orthodontics. J. Orthod. 2016, 43, 121–129, . [CrossRef]
- Cooke, M.E.; Sherriff, M. Debonding force and deformation of two multi-stranded lingual retainer wires bonded to incisor enamel: an in vitro study. Eur. J. Orthod. 2010, 32, 741–746, . [CrossRef]
- Schwarze, J.; Bourauel, C.; Drescher, D. Frontzahnbeweglichkeit nach direkter Klebung von Lingualretainern. J. Orofac. Orthop. Der Kieferorthopadie 1995, 56, 25–33, . [CrossRef]
- Sifakakis, I., T. Eliades, and C. Bourauel, Residual stress analysis of fixed retainer wires after in vitro loading: can mastication-induced stresses produce an unfavorable effect? Biomed Tech (Berl), 2015. 60(6): p. 617-22.
- Sifakakis, I.; Pandis, N.; Eliades, T.; Makou, M.; Katsaros, C.; Bourauel, C. In-vitro assessment of the forces generated by lingual fixed retainers. Am. J. Orthod. Dentofac. Orthop. 2011, 139, 44–48, . [CrossRef]
- Gelin, E.; Seidel, L.; Bruwier, A.; Albert, A.; Charavet, C. Innovative customized CAD/CAM nickel-titanium lingual retainer versus standard stainless-steel lingual retainer: A randomized controlled trial. Korean J. Orthod. 2020, 50, 373–382, . [CrossRef]
- Gera, A.; Pullisaar, H.; Cattaneo, P.M.; Gera, S.; Vandevska-Radunovic, V.; A Cornelis, M. Stability, survival, and patient satisfaction with CAD/CAM versus conventional multistranded fixed retainers in orthodontic patients: a 6-month follow-up of a two-centre randomized controlled clinical trial. Eur. J. Orthod. 2022, 45, 58–67, . [CrossRef]
- Jowett, A.C.; Littlewood, S.J.; Hodge, T.M.; Dhaliwal, H.K.; Wu, J. CAD/CAM nitinol bonded retainer versus a chairside rectangular-chain bonded retainer: A multicentre randomised controlled trial. J. Orthod. 2023, 50, 55–68, . [CrossRef]
- Shim, H.; Foley, P.; Bankhead, B.; Kim, K.B. Comparative assessment of relapse and failure between CAD/CAM stainless steel and standard stainless steel fixed retainers in orthodontic retention patients: A randomized controlled trial. Angle Orthod. 2022, 92, 87–94, . [CrossRef]
- Roser, C.J.; Bauer, C.; Hodecker, L.; Zenthöfer, A.; Lux, C.J.; Rues, S. Comparison of six different CAD/CAM retainers vs. the stainless steel twistflex retainer: an in vitro investigation of survival rate and stability. J. Orofac. Orthop. Der Kieferorthopadie 2023, 1–10, . [CrossRef]
- Hülsmann, M., Endodontie, ed. G. Thieme. 2008, New York, NY, USA.
- Roser, C.J.; Rues, S.; Erber, R.; Hodecker, L.; Lux, C.J.; Bauer, C.A.J. Tooth mobility restriction by multistranded and CAD/CAM retainers—an in vitro study. Eur. J. Orthod. 2024, 46, . [CrossRef]
- Annousaki, O.; Zinelis, S.; Eliades, G.; Eliades, T. Comparative analysis of the mechanical properties of fiber and stainless steel multistranded wires used for lingual fixed retention. Dent. Mater. 2017, 33, e205–e211, . [CrossRef]
- Rucker, B.K.; Kusy, R.P. Elastic flexural properties of multistranded stainless steel versus conventional nickel titanium archwires.. Angle Orthod. 2002, 72, 302–9, . [CrossRef]
- Chakroun, F.; Colombo, V.; Foek, D.L.S.; Gallo, L.M.; Feilzer, A.; Özcan, M. Displacement of teeth without and with bonded fixed orthodontic retainers: 3D analysis using triangular target frames and optoelectronic motion tracking device. J. Mech. Behav. Biomed. Mater. 2018, 85, 175–180, . [CrossRef]
- Niver, E.L.; Leong, N.; Greene, J.; Curtis, D.; Ryder, M.I.; Ho, S.P. Reduced functional loads alter the physical characteristics of the bone–periodontal ligament–cementum complex. J. Periodontal Res. 2011, 46, 730–741, . [CrossRef]
- Schulz RP, M.R., Oesterle LJ, Pierson WP., Bond strengths of three resin systems used with brackets and embedded wire attachments. . Am J Orthod, 1985. 87: p. 75-80.
- Boldt, J.; Knapp, W.; Proff, P.; Rottner, K.; Richter, E.-J. Measurement of tooth and implant mobility under physiological loading conditions. Ann. Anat. - Anat. Anz. 2012, 194, 185–189, . [CrossRef]
- Göllner, M.; Holst, A.; Berthold, C.; Schmitt, J.; Wichmann, M.; Holst, S. Noncontact intraoral measurement of force-related tooth mobility. Clin. Oral Investig. 2010, 14, 551–557, . [CrossRef]
Figure 1.
The FRANS setup with all its components. [A] Digital Displacement Measuring Device; [B] micrometer screw gauge and dial gauge for vertical displacement; [C] Springs to limit uncontrolled vertical movement; [D] Force / Torque sensor; [E] Connector piece for force/moment transmission between sensor and reference teeth; [F] Measurement table representing the lower jaw, with placement slots for the experimental setup, representing the alveolar sockets; [G] Screw gauge for sagittal displacement of the measuring table. In this instance, the R2 retainer with the lateral incisors as reference teeth is being analyzed.
Figure 1.
The FRANS setup with all its components. [A] Digital Displacement Measuring Device; [B] micrometer screw gauge and dial gauge for vertical displacement; [C] Springs to limit uncontrolled vertical movement; [D] Force / Torque sensor; [E] Connector piece for force/moment transmission between sensor and reference teeth; [F] Measurement table representing the lower jaw, with placement slots for the experimental setup, representing the alveolar sockets; [G] Screw gauge for sagittal displacement of the measuring table. In this instance, the R2 retainer with the lateral incisors as reference teeth is being analyzed.
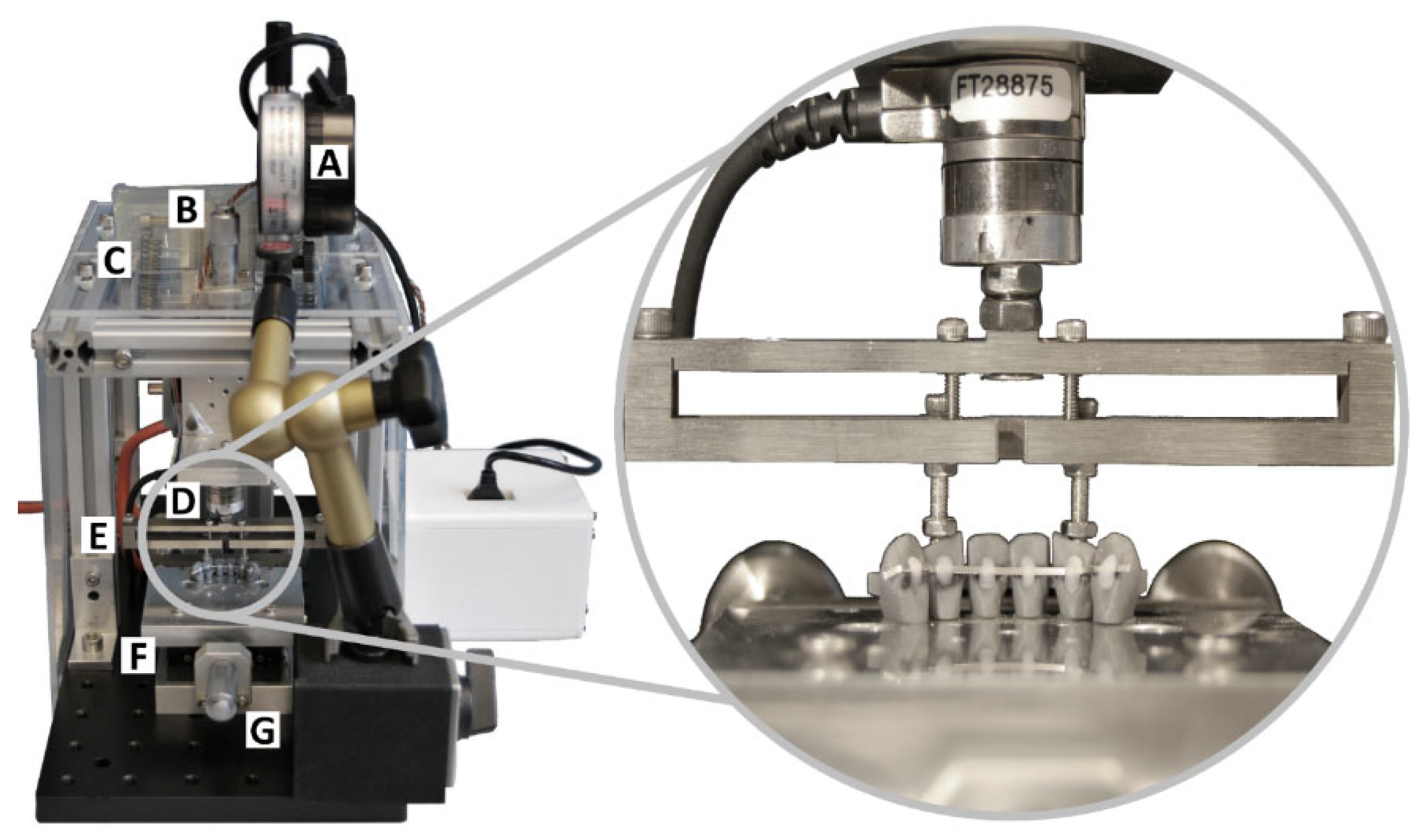
Figure 2.
The defined coordinate system for the third and fourth quadrant, viewed from the lingual aspect. In both quadrants, the positive Y-axis indicates a mesial movement, and the positive Z-axis indicates an intrusion. In the left quadrant, a positive X-axis indicates a labial movement; conversely, in the right quadrant, a positive X-axis indicates a lingual movement. Due to technical reasons, it was not possible to apply the Tweed convention to this coordinate system.
Figure 2.
The defined coordinate system for the third and fourth quadrant, viewed from the lingual aspect. In both quadrants, the positive Y-axis indicates a mesial movement, and the positive Z-axis indicates an intrusion. In the left quadrant, a positive X-axis indicates a labial movement; conversely, in the right quadrant, a positive X-axis indicates a lingual movement. Due to technical reasons, it was not possible to apply the Tweed convention to this coordinate system.
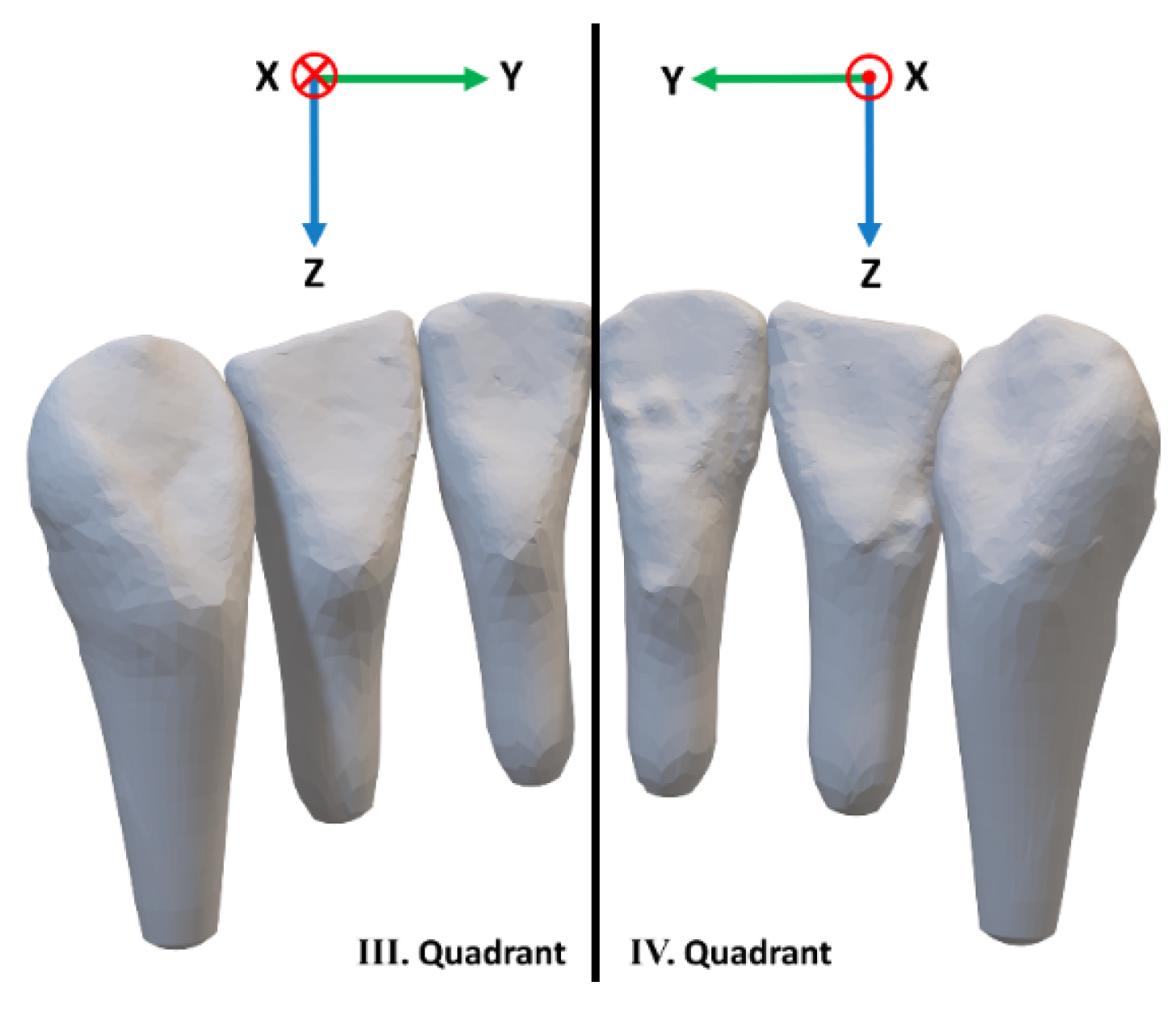
Figure 3.
Measured force Fz [Nmm] (left) and torque My [Nmm] (right) for all retainer types R1 (A, B), R2 (C, D), and R3 (E, F), exemplarily shown at the canines. The different measurements (a-e) are distinguished by color. A direct relationship between force and torque due to the direct proportionality via the lever arm is visible. While the curves for R3 (E and F) appear more homogenous, there are noticeable differences between measurements concerning R1 and R2.
Figure 3.
Measured force Fz [Nmm] (left) and torque My [Nmm] (right) for all retainer types R1 (A, B), R2 (C, D), and R3 (E, F), exemplarily shown at the canines. The different measurements (a-e) are distinguished by color. A direct relationship between force and torque due to the direct proportionality via the lever arm is visible. While the curves for R3 (E and F) appear more homogenous, there are noticeable differences between measurements concerning R1 and R2.
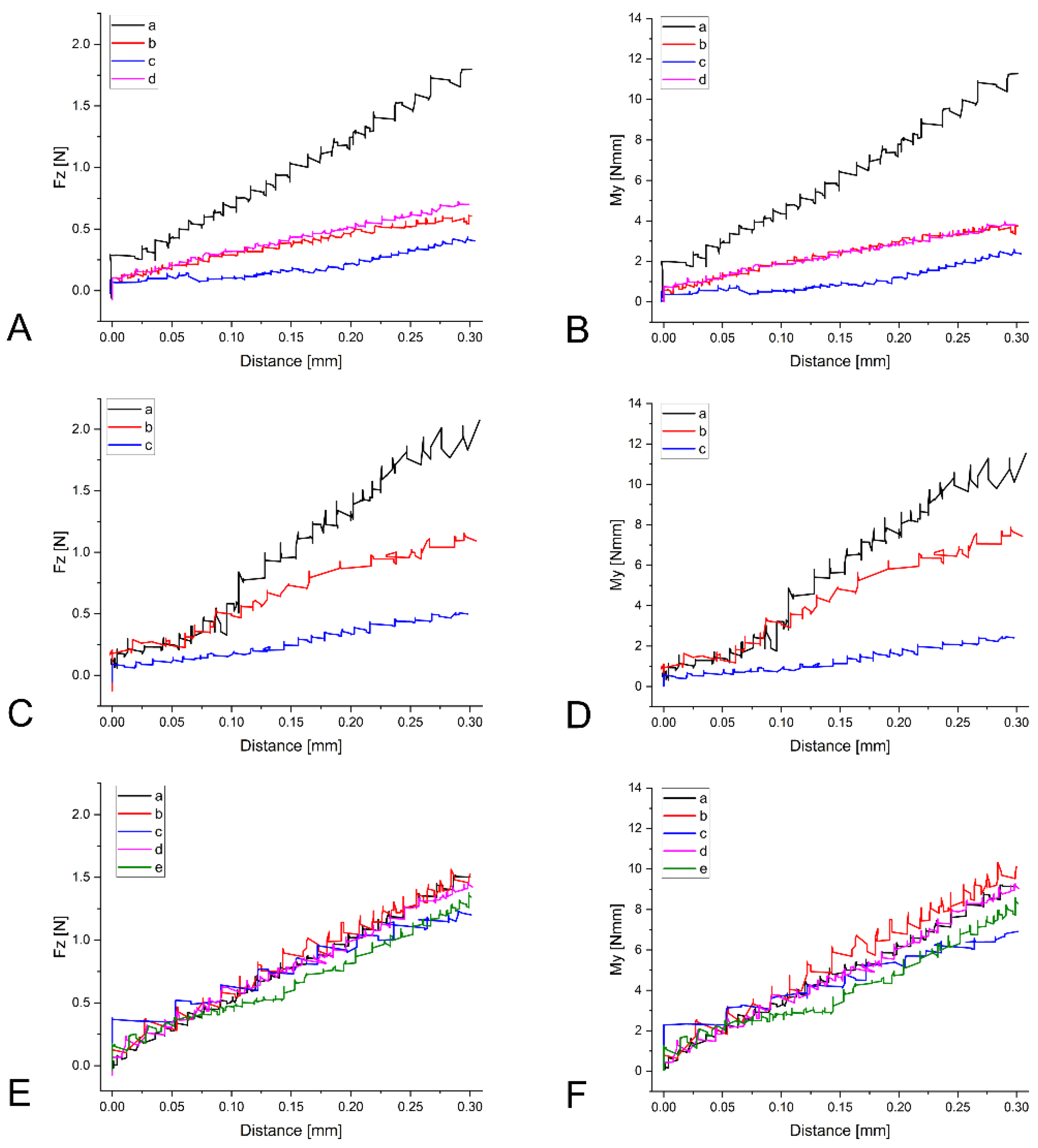
Figure 4.
Vertical force Fz for different retainer materials (R1, R2, R3) and different reference teeth (central incisor 1, lateral incisor 2, and canine 3) at a displacement of 0.1 mm, 0.2 mm, and 0.3 mm. The force Fz was measured at the center of force in N.
Figure 4.
Vertical force Fz for different retainer materials (R1, R2, R3) and different reference teeth (central incisor 1, lateral incisor 2, and canine 3) at a displacement of 0.1 mm, 0.2 mm, and 0.3 mm. The force Fz was measured at the center of force in N.

Figure 5.
Labiolingual torque My for different retainer materials (R1, R2, R3) and different reference teeth (central incisor 1, lateral incisor 2, and canine 3) at a displacement of 0.1 mm, 0.2 mm, and 0.3 mm. The moment My was measured at the center of force in Nmm.
Figure 5.
Labiolingual torque My for different retainer materials (R1, R2, R3) and different reference teeth (central incisor 1, lateral incisor 2, and canine 3) at a displacement of 0.1 mm, 0.2 mm, and 0.3 mm. The moment My was measured at the center of force in Nmm.
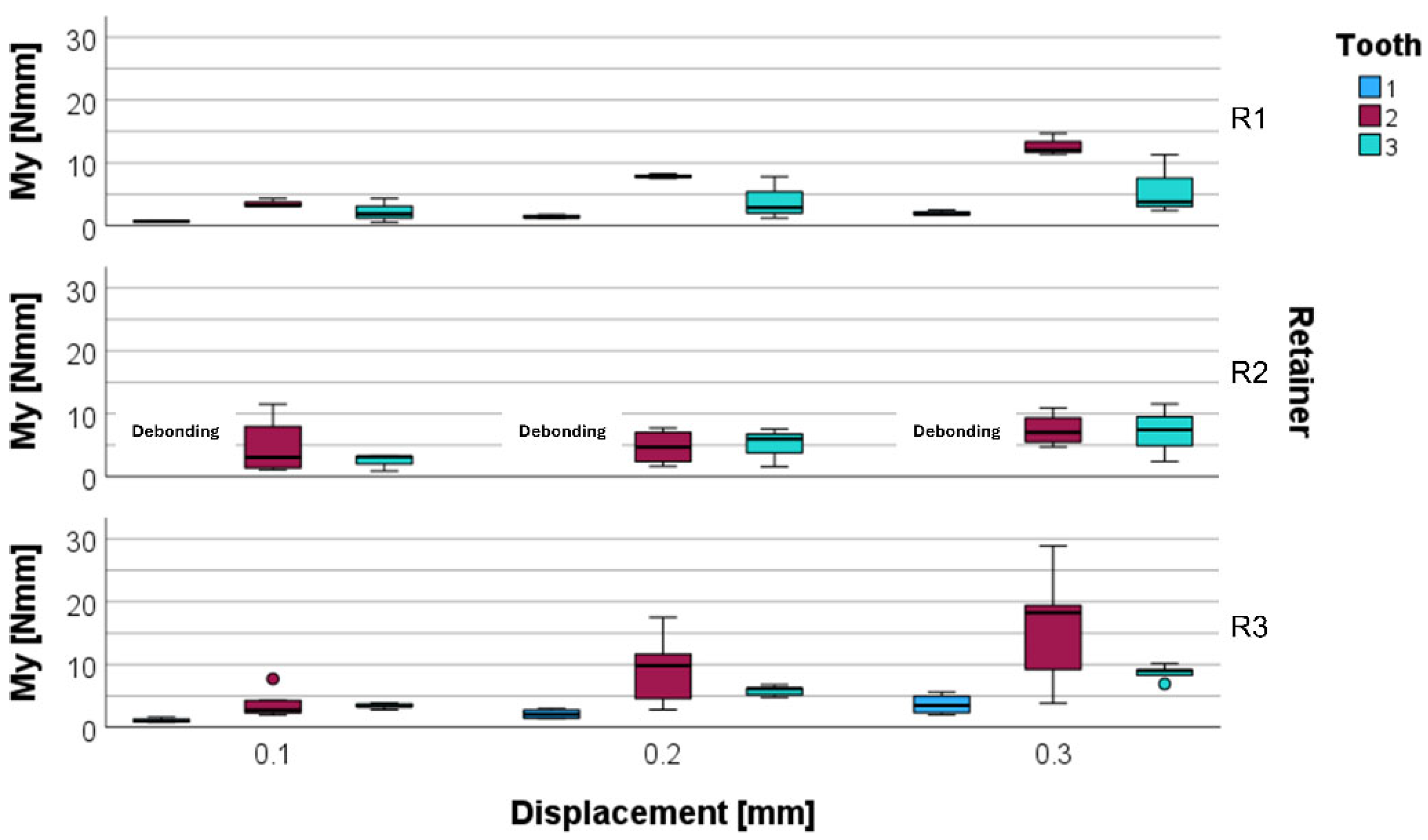
Figure 6.
Biomechanical situation of incisal loading during mastication in the presence of a retainer. The retainer serves as center of rotation (CR). The effect is expected to be more pronounced when a twisted retainer wire is used, as the twisted wires are assumed to be less resistant to torsional moments such as My.
Figure 6.
Biomechanical situation of incisal loading during mastication in the presence of a retainer. The retainer serves as center of rotation (CR). The effect is expected to be more pronounced when a twisted retainer wire is used, as the twisted wires are assumed to be less resistant to torsional moments such as My.

Figure 7.
The lower anterior segment during vertical mastication loading causes a force in the negative Fz direction. Arrows indicating the vertical force-components on individual teeth (43, 42, 41, 31, 32, 33 according to the FDI notation). It becomes evident that the loaded canines are (43 and 33) are only supported on one side whereas the lateral incisors (42 and 32) have support from the central incisors as well as from the canines. If the load is applied to the central incisors (41 and 31) the biomechanical support from the neighboring teeth is in-between the two previously mentioned cases. .
Figure 7.
The lower anterior segment during vertical mastication loading causes a force in the negative Fz direction. Arrows indicating the vertical force-components on individual teeth (43, 42, 41, 31, 32, 33 according to the FDI notation). It becomes evident that the loaded canines are (43 and 33) are only supported on one side whereas the lateral incisors (42 and 32) have support from the central incisors as well as from the canines. If the load is applied to the central incisors (41 and 31) the biomechanical support from the neighboring teeth is in-between the two previously mentioned cases. .
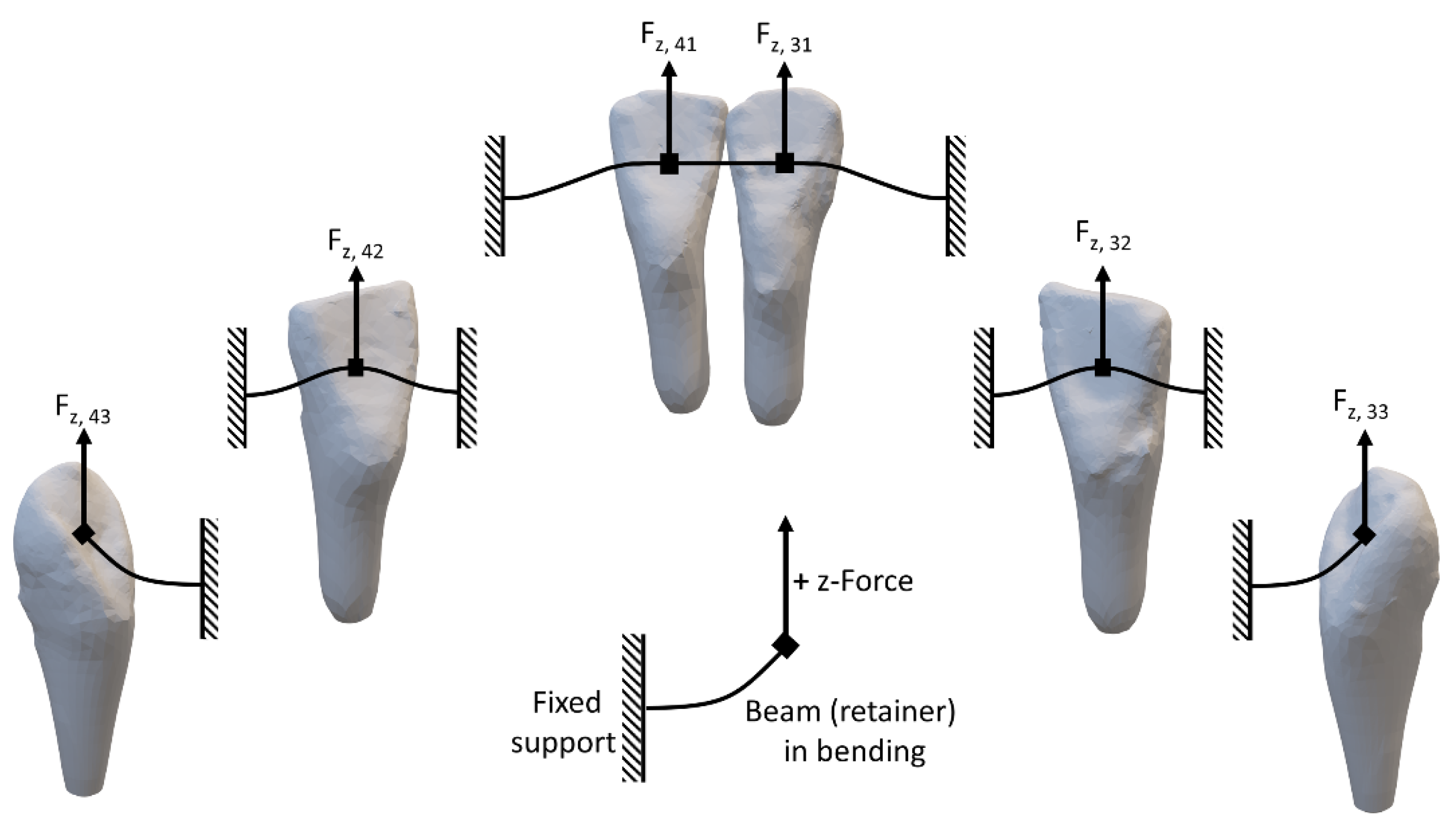

Table 1.
Retainer characteristics of the retainer wires analyzed in this study. The material, cross-sectional dimensions, shape, and manufacturing process are listed.
Table 1.
Retainer characteristics of the retainer wires analyzed in this study. The material, cross-sectional dimensions, shape, and manufacturing process are listed.
| Retainer | Material | Dimension | Shape | Manufacturing process |
|---|---|---|---|---|
| R1 | SS | 0.0215” | stranded, round | bent with pliers |
| R2 | SS | 0.010”x0.029” | stranded, rectangular, flat | adapted by hand |
| R3 | NiTi | 0.014”x0.014” | Rectangular | CAD/CAM laser cut from sheet |
SS: Stainless-steel; NiTi: nickel-titanium; CAD: Computer-aided design; CAM: computer-aided manufacturing.
Table 2.
Calculated mean and standard deviation for Fz [N] and My [Nmm] measured at the center of force (CoF) for different displacements (0.1mm, 0.2mm, 0.3mm), different retainers (R1, R2, R3) and different reference teeth (1, 2, 3). Data showing mean over left and right quadrant.
Table 2.
Calculated mean and standard deviation for Fz [N] and My [Nmm] measured at the center of force (CoF) for different displacements (0.1mm, 0.2mm, 0.3mm), different retainers (R1, R2, R3) and different reference teeth (1, 2, 3). Data showing mean over left and right quadrant.
| Displacement [mm] |
Retainer | Tooth | Fz [N] | My [Nmm] |
|---|---|---|---|---|
| Mean (SD) | Mean (SD) | |||
| 0.1 | R1 | 1 | 0.50 (0.18) | 0.67 (0.10) |
| 2 | 0.71 (0.04) | 3.52 (0.70) | ||
| 3 | 0.35 (0.24) | 2.16 (1.59) | ||
| R2 | 2 | 1.04 (0.71) | 4.67 (4.79) | |
| 3 | 0.42 (0.22) | 2.41 (1.34) | ||
| R3 | 1 | 1.01 (0.06) | 1.10 (0.34) | |
| 2 | 0.96 (0.42) | 3.80 (2.36) | ||
| 3 | 0.55 (0.05) | 3.41 (0.42) | ||
| 0.2 | R1 | 1 | 0.92 (0.25) | 1.43 (0.29) |
| 2 | 1.50 (0.25) | 7.86 (0.34) | ||
| 3 | 0.61 (0.45) | 3.70 (2.85) | ||
| R2 | 2 | 1.30 (0.85) | 4.67 (2.80) | |
| 3 | 0.84 (0.48) | 5.02 (3.09) | ||
| R3 | 1 | 1.72 (0.09) | 2.10 (0.76) | |
| 2 | 2.06 (1.09) | 9.27 (5.86) | ||
| 3 | 0.97 (0.09) | 5.82 (0.82) | ||
| 0.3 | R1 | 1 | 1.27 (0.48) | 2.01 (0.43) |
| 2 | 2.35 (0.59) | 12.68 (1.75) | ||
| 3 | 0.88 (0.63) | 5.30 (4.04) | ||
| R2 | 2 | 1.69 (1.06) | 7.42 (2.65) | |
| 3 | 1.22 (0.80) | 7.13 (4.57) | ||
| R3 | 1 | 2.45 (0.34) | 3.66 (1.63) | |
| 2 | 3.28 (1.73) | 15.91 (9.71) | ||
| 3 | 1.40 (0.13) | 8.70 (1.19) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



