
Submitted:
11 September 2024
Posted:
12 September 2024
You are already at the latest version
Abstract
Objective: A 1964 study challenged the consensus that saturated fat consumption increased the risk for myocardial infarction (MI). Roseto Pennsylvania, an Italian-American enclave of 1600 people, had similar rates of cigarette smoking, obesity and higher saturated fat consumption as neighboring towns, but far lower MI death rates. More than 50 years later, it remains uncertain if Roseto’s residents had better heart health than the average American and if so, what factors were responsible. Methods: We compared MI deaths in Roseto and neighboring towns to the Framingham Heart Study cohort matched for age and sex. Results: We found no evidence that MI deaths were lower in Roseto, PA than in Framingham, MA when controlling for age and sex. While the role of social support in health is uncontested, methodological issues, confounding factors and biases challenge the validity of the Roseto study. Conclusions: The dramatically lower MI and MI mortality rates among males in Roseto reflects biases in sampling and comparison populations, which also impacted the contrasting Diet-Heart hypothesis that saturated fats cause heart disease. Although social support enhances health outcomes, the Roseto study neither supported nor refuted this connection.
Keywords:
diet
; obesity
; health
; social support
; saturated fat
Introduction
American men faced an apparent epidemic of myocardial infarction (MI) deaths in the 1950s. In 1964, Stewart Wolf and colleagues, reported that men in Roseto, Pennsylvania rarely died from MI [1]. This Italian-American enclave of 1600 people had similar rates of cigarette smoking and obesity and higher saturated fat consumption than did most of America. Wolf et al. interviewed and examined every Rosetan adult and many in the neighboring towns of Bangor, Nazareth, Stroudsburg and East Stroudsburg. Suspected risk factors were similar among residents in these towns. They argued that genetic factors were unlikely since other Italian-Americans and Rosetans who migrated out to other towns had higher MI rates than the Italian-Americans in Roseto.
The Roseto study challenged the prevailing consensus that saturated fat consumption was a risk factor for MI. By 1961, the Framingham Heart Study (FHS) identified older age, male sex, hypertension, hypercholesterolemia, and cigarette smoking as heart disease risk factors [2]. The “Diet-Heart hypothesis” [3], introduced by University of Minnesota physiology professor Ancel Keys, posited that rising 20th century fat consumption caused elevated cholesterol levels [3]. High cholesterol levels correlated with heart disease in the FHS and between nations (e.g, United States and England versus Italy and Greece) [3,4].
The Roseto study emerged during a ‘heart disease epidemic’ and ‘a changing American diet’. The role of genetics, dietary factors, and stress remained controversial. However, in 1961, the American Heart Association (AHA) recommended “The reduction or control of fat consumption under medical supervision, with reasonable substitution of poly-unsaturated for saturated fats, is recommended as a possible means of preventing atherosclerosis and decreasing the risk of heart attacks and strokes’ [5]. Discoveries in the early 1960s about the role of triglycerides, HDL and LDL subfractions, insulin resistance and metabolic syndrome had little influence on dietary recommendations. Reducing saturated fats remains the primary dietary intervention recommended by the AHA to prevent heart disease [6].
Wolf et al. found ‘the most striking feature of Roseto was the way in which the people seemed to enjoy life…one-class…simple, warm and very hospitable people…no crime in Roseto…mutually supporting” [1]. They later highlighted the ‘Old World values and customs’ [7] and their ‘cohesive social structure’ [8] as key factors contributing to their good health. Rosetans’ good health to social support and neighborhood cohesion, helping launch the social-support health discipline [1,7,8]. This observation was based on informal observation of social interactions, which were not systematically quantified in Roseto or neighboring towns. Social relationships can support cardiac, mental, and other positive health outcomes across populations and settings [9,10]. The ‘Roseto Effect’ had faded from lay and medical awareness as the Diet-Heart Hypothesis gained widespread acceptance, but re-entered the mainstream [11] with Malcolm Gladwell’s book Outliers (2002): “In Roseto, virtually no one under 55… showed any signs of heart disease. For men over 65, the death rate from heart disease in Roseto was roughly half that of the United States… The Rosetans were healthy because of where they were from, because of the world they had created.”
By contrast, Keys proposed that saturated fats caused heart disease, relying on: 1) feeding studies showed saturated fats increased total serum cholesterol, 2) population-based studied correlated total cholesterol consumption with heart disease risk, and 3) international comparisons showing that populations with high saturated fat consumption had higher cholesterol levels and heart disease rates [3,4]. Keys criticized the Roseto study because the heart disease rate was not lower than the United States average, and Keys recognized the potential diagnostic and selection biases [12]. Further, some older Rosetans were born in Italy, and their childhood and young adult diets likely differed from their diet in America. These valid criticisms also applicable to his Diet-Heart hypothesis.
Were Rosetan men healthier than contemporary American men? Only selected data summaries from Roseto and neighboring Bangor, Nazareth, Stroudsburg, and East Stroudsburg populations were published [1]. The original paper detailed age, sex, weight and height of Rosetans, and compared them to either neighboring towns or average Americans, not both. Deaths due to MI and other cardiac causes in Roseto and neighboring towns were reported but the only diet and cholesterol levels were reported for Rosetans; introducing potential confounding bias. No data was provided to support the contention that Rosetan men who moved out died at relatively young ages from MI. Finally, data on number of deaths due to cancer and other causes were not provided. With these limitations of the original paper, we revisit the Roseto study and explore five potential explanations for the ‘heart health’ of Rosetans.
Alternative Explanations
Diet
Dietary data for Roseto and the neighboring towns were limited. In Roseto, average daily calorie consumption was 3000 for men and 2300 for women [1], similar to other American adults. Calories were derived from fat (41%), protein (13%), carbohydrates (42%) and alcohol (5%). There were no data provided by Wolf and colleagues on the types of fats (saturated, mono- and poly-unsaturated, trans) or carbohydrates (refined versus unrefined) that were used by individuals in Roseto or neighboring towns typical of studies in that era. The Rosetans’ high saturated fat intake was supported only by anecdotal observations. Favorite dishes included peppers fried in lard and their bread was ‘dipped...in the lard gravy’. Prosciutto with ‘rim of fat, more than an inch thick’ was commonly consumed [1,7].
The Rosetan diet likely included few ultra-processed foods. Lard was used in Italy for millennia. Rosetans cooked with olive oil (57%), lard and butter (47%), while in Bangor, lard was used by 16% and butter by 11% [1]. Lard fat is 45% monounsaturated, 39% saturated (mainly palmitic and stearic acids) and polyunsaturated (11%). Palmitic acid, the main saturated fat in lard, comprises ~25% of fatty acids in our bodies. When dietary intake is high, our bodies synthesize less. Stearic acid is primarily metabolized to the monounsaturated oleic acid. Thus, ~70% lard fat is metabolized into mono- or polyunsaturated forms. Saturated fats increase the lighter and fluffier LDL fraction, which are not associated with heart disease risk; unlike the small dense LDL fraction which is associated with heart disease risk [6]. Saturated fats also raise HDL, associated with lower heart disease risk. We lack data on the saturated fat consumption of Rosetans or residents of neighboring towns.
During the 1950s and 1960s, Crisco cooking oil was commonly used in American homes, and contained trans and other synthetic fats. Internationally, the rise of cardiovascular disease (CVD) and other noncommunicable diseases (NCDs; e.g., obesity, diabetes, cancer, gout) is strongly linked to highly processed diets, as well as increased caloric intake. Consumption of sugar and other refined carbohydrates, potential causes of NCDs [13], were not studied in Roseto [1] nor in the Seven Countries Study [4]. Consumption of Crisco oil and other trans fats, as well as refined carbohydrates, may have differed between Roseto and the neighboring towns, and contributed to differences in NCDs.
Genetics
The Rosetans’ ancestors came from Roseto Valforte, a small town in southeastern Italy, suggesting possible genetic factors. Genetic and lifestyle factors are independently associated with coronary disease [6]. Genetic enclaves may have increased or decreased coronary disease risk [6,7]. However, no evidence supported or refuted genetic factors in Rosetans’ heart disease. Wolf and colleagues argued that immigrants from Roseto Valforte who settled in other American cities had higher rates of heart disease, but no evidence supported this claim. Wolf and colleagues later reported that as Rosetans assimilated into American culture, their rates of heart disease rose [8]. Thus, genetic factors, never systematically studied, were unlikely a major factor.
Comorbid Disorders and Risk Factors.
Data on CVD risk factors such as obesity, smoking, hypertension and hypercholesterolemia in Roseto and neighboring towns were limited. While obesity was more prevalent among Rosetans than neighboring towns, diabetes prevalence in Roseto was far lower than in Nazareth or Bangor [7]. Since diabetes increases CVD and CV mortality more than 50%, this could contribute to the relatively better cardiac health of Rosetans [14]. Rates of smoking were similar in Roseto and Bangor, although in neighboring towns, “the number of cigarettes smoked is somewhat higher than it is in Roseto” [1,8]. Among men, hypertension (>= 150/90) was more common in Roseto than Nazareth or Bangor, but rates in women were similar. Men’s mental health disorders were 50-300% lower in Roseto (162/100,000) compared to Bangor (289/100,000) and Nazareth (506 per 100,000) [8].
Did Neighboring Towns Have High Rates of CVD?
Rosetans’ heart health was compared to four neighboring towns. We assessed the incidence of deaths due to cardiovascular disease in Roseto relative to the age-adjusted rates for men over 45 years of age in Farmingham study (see Table 1). Men in Bangor over 45 years had > 4-fold than average CVD mortality (251/100,000) [1] compared to similar aged men in Framingham (Table 1). The Rosetan men’s heart health may partly reflect that Bangor was a ‘sick’ comparator group.
Wolf and colleagues combined MI deaths from autopsy-proven, clinically diagnosed and ‘presumed’, but did not provide data on each category. No diagnostic criteria were specified for the ‘presumed’ group. Given the a priori belief that Rosetans had low rates of MI deaths, which instigated Wolf et al.’s study, lack of blinding may have led to more liberal diagnosing presumed CVD deaths outside Roseto.
Outmigration and Birthplace
A paradox was the low percentage of older adult men in Roseto -- (8% ages 55-64 and 9% > 65 year old) [1] – lower than any four neighboring towns. Mortality rates in Roseto were reportedly low. Did Rosetan adult men leave after childhood or young adulthood, or did they die prematurely? The lack of data on the ‘missing men’ is a major limitation. Perhaps men who lived less healthy lifestyles and were less connected to the social community migrated out more frequently or died before Wolf et al.’s study? Older Rosetan men included a higher percentage of Italian-born individuals, whose early childhood lifestyle and diet was another confounding factor, and would be predicted to be associated with lower CVD mortality.
Chance
A striking finding was the lack of any CVD deaths among 55-64 year-old men in Roseto versus a ~1% annual CVD mortality in neighboring towns. CVD deaths were also uncommon among men over age 65 years. However, in Roseto, only 62 men were aged 55-64 and 70 were over 65 years. By contrast, in neighboring towns, the number (percentage) of men ages 55-64 and >65 in Bangor (400 (12%) and 400 (12%)), Stroudsburg (329 (12%) and 412 (15%)), East Stroudsburg (332 (9%) and 332 (9%)), and Nazareth (328 (11%) and 328 (11%)) were higher. These Roseto data for men >55 years old were limited by small numbers. Whenever sample sizes are small, people intuitively believe observations (e.g., low CVD rates) can be generalized, but this is a fallacy [15].
To assess the role of small n and chance’s potential role, we compared expected and observed mortality counts at Roseto, using Framingham Heart Study (FHS) rates. Framingham is the only place in the US with prospective mortality and CVD mortality data concurrent to the Roseto study. Therefore, we assessed whether Rosetans had lower MI mortality rate than those in Framingham? We investigated the divergence in observed and expected number of deaths in Roseto, when the underlying probability of MI death was similar to FHS.
First, age- and sex-specific MI mortality rates were computed from 1955 to 1964 among the original FHS cohort (2294 men and 2785 women, aged 28 to 74 years recruited in 1948-49). We then simulated the expected number of deaths using a binomial process with underlying FHS rate and population size from Roseto in 1950. Number of expected deaths was computed for age groups <35, 35-44, 45-54, 55-64 and 65+. Within each age group, deaths were repeatedly sampled for 1,000 times from the underlying binomial distribution. Age-specific mean number of deaths along with 95% confidence interval were compared with observed number of deaths from MI in Roseto from 1955-1964. If the observed deaths were within the 95% confidence interval of the expected deaths, then the observed number in Roseto was similar to FHS.
Table 1 summarizes age- and sex-specific deaths per 1000 population in FHS and Roseto. Figure 1 displays the simulated counts distribution in a histogram. The observed deaths in Roseto were within the 95% confidence interval of simulated deaths in all age groups except for the 65+ group, where it was higher than expected in Roseto. Observed deaths in Roseto were within the expected range compared to the FHS mortality rate.
Histograms representing distribution of simulated expected number of deaths for Roseto when the underlying probability of CVD death is similar to that of Framingham Heart Study. Red line represents observed count. Blue lines represent the lower 2.5 and upper 97.5 percentile of the simulated counts.
Discussion
The Roseto effect suggested that stress caused and social support prevented heart disease, while the Diet-Heart hypothesis considered saturated animal fats caused heart disease. Both conclusions were fraught with potential selection and confounding biases. Heart disease was considered epidemic in the early 1950s, but the apparent rise was largely attributable to an aging population, increased ECG use, revised diagnostic MI criteria, and 1949 revised cause-of-death criteria [16]. The latter increased cardiac deaths by 20-35% in one year [17]. The American Heart Association created a media campaign to promote the need for research funding. In 1953, Keys linked rising cholesterol levels to the 26.4% increase fat consumption by Americans between 1909-1952 [18]. This increase was primarily ‘cooking fats and oils’ excluding butter [18,19], and in 1953 Keys recommended reducing cooking fats and oils. Notably, lard, butter, and whole milk consumption declined >50% from 1900 to 1960 [19]. By the late 1950s, Keys advocated reducing saturated fats [20]. He modified the changing American diet narrative from rising vegetable oils, documented in USDA data [18], to rising animal fat consumption, which USDA data showed had declined [19].
Roseto became a model for the idea that inter-generational and community social support protecting against CVD and prolonging life. However, direct comparison of rates of CVD deaths without accounting for clinical, environmental and life-style confounders can create selection bias [21]. Although genetics and lifestyles likely differed between residents of Roseto PA and Framingham MA, we used Framingham as the best contemporaneously studied American population for CVD. The original FHS cohort was of European descent and free of CVD at enrollment. Our hypothesis that lower male CVD mortality in Roseto may reflect small population size and chance was supported by our analysis. Compared to FHS, observed MI death rates in Roseto were similar, except for subjects over age 65, where Roseto had a higher MI death incidence.
The flawed interpretation of Roseto data resulted from methodological issues. Wolf et al. did not assess a random selection of small towns. He was told Roseto had a low MI death rate, introducing the ‘sharpshooter bias’ [7,8]. He committed resources into a nonblinded, study limited by small numbers and had limitations in the methods of data collection and what data was collected. Roseto’s politicians and residents collected data and sought to promote their town favorably. Data sampling and interpretation were likely suffered from confounding biases. For example, many members of Roseto were in charge of collecting data and revealed that they aimed to present their community in a favorable light [22]. Confounding variables, such as far higher rates of diabetes (e.g., 26/1000 men and 37/1000 women in Roseto; 44 and 94/1000 for men and 30 and 102/1000 for women in Nazareth and Bangor, respectively) and mental health disorders (162/100,000 men and 234/100,000 women in Roseto; 505/100,000 men and 518/100,000 women in Nazareth; 289/100,000 men and 351/100,000 women in Bangor) in neighboring towns [23], were not considered. Demographic, anthropometric, dietary, medical, and cause-of-death data for Roseto and ‘control’ towns were scant. Social life was qualitatively assessed in Roseto only. Mortality data on men who left Roseto, used to refute potential genetic factors, were not presented. The paucity of Rosetan men over 55 conflicts with the narrative of healthy older men bonded to their community by potent intergenerational ties. Early life environment in Italy was another confounding factor. Data on comorbid disorders and risk factors, including diet, in comparison with towns are critical to evaluate potential causal factors, such as social support. While neighboring towns had relatively higher rates of cardiac deaths compared to Roseto, such deaths in Roseto were similar or higher than those in Framingham, MA over the same period.
A key lesson from the Roseto study is that biases are powerful, pervasive and persistent. The Roseto study never supported that social support improves heart health with solid evidence, yet it continues to be cited in medical, [24] best-selling nonfiction books [11], and in Wikipedia [25]. Promoted to refute saturated fats caused heart disease, its data on diet and disease were inadequate. Similarly, the Diet-Heart hypothesis has also been criticized due to correlative data that was plausible but unproven [26]. Both the Roseto and Diet-Heart Hypotheses, as well as Keys’ earlier total fat-heart disease hypothesis were confounded by selection bias [26,27] and uncontrolled variables (e.g., sugar and other highly processed foods) [19]. The Diet-Heart hypothesis was not supported by regional, national and international studies [26,28], as well as prospective observational and randomized controlled trials [26,29]. Further, although Keys used the rising consumption of all fats from 1909-1952 in America to implicate dietary fats in the rapid rise of heart disease, only polyunsaturated fat consumption rose dramatically during the first half of the 20th century, while saturated fat consumption declined during this period. Dietary trials in high-risk-for-CVD individuals that replaced saturated fats with vegetable oils showed heart disease deaths declined but overall mortality was unchanged [6,28,29]. The Framingham Heart Study Diet Study revealed that an individual’s dietary fat or saturated fat consumption did not correlate with their serum cholesterol or risk of heart disease [30]. However, publication of this study was suppressed [31]. Although the role of saturated fats in heart health remains controversial, a strident conviction without sufficient evidence is shared by the Roseto thesis and Diet-Heart Hypothesis.
Studies where variables over long durations cannot be accurately assessed, as in nutrition and medical outcomes, are liable to the narrative fallacy where a logical explanation makes them more cohesive and collectively compelling. When definitive data are elusive, when a theory is accepted by a small group, its success may relate more to the conviction of protagonists and contagion – how many times references are cited and the theory dominates high impact scientific and lay articles – than to its veracity. In most nutritional science, dozens of variables were imprecisely measured or ignored. Many of these limitations persist today. Notoriously difficult and unreliable measures include total daily calories, amount and type of macronutrients (e.g., sugar v. unrefined carbohydrates, saturated v. polyunsaturated fats). Further, these potential limitations are compounded because diets are sampled at one time while the pathogenic effects of diet develop over decades. The Roseto and Diet-Heart Hypotheses exemplify the vulnerability of science where precise data is lacking, confounded factors abound, and biases are fueled by authority and contagion.
Authors’ Contributions
All the authors, SA, OO, and OD wrote, prepared and reviewed the manuscript.
Institutional Review Board Statement
The New York University Langone Medical Center Institutional Review Board approved the study.
Informed Consent Statement
There is not a consent for publication as we used previously collected data.
Data Availability Statement
The manuscript contains third party material and obtained permissions are available on request by the Publisher.
Acknowledgments
This Manuscript was prepared using FRAMCOHORT Research Materials obtained from the NHLBI Biologic Specimen and Data Repository Information Coordinating Center and does not necessarily reflect the opinions or views of the FRAMCOHORT or the NHLBI.
Conflicts of Interest
None of the authors has competing interests.
References
- Stout C, Morrow J, Brandt EN, Wolf S. Unusually low incidence of death from myocardial infarction: study of an Italian American community in Pennsylvania. JAMA. 1964, 188, 845–849. [Google Scholar]
- Kannel WB, Dawber TR, Kagan A, Revotskie N, Stokes III J. Factors of risk in the development of coronary heart disease—six-year follow-up experience: the Framingham Study. Annals of internal medicine. 1961, 55, 33–50. [Google Scholar] [CrossRef] [PubMed]
- Keys, A. Arteriosclerotic heart disease in Roseto, Pennsylvania. JAMA. 1966, 195, 93–95. [Google Scholar] [CrossRef]
- Keys A. Seven countries. Seven Countries. Harvard University Press; Cambridge, MA, 2013.
- Page IH, Allen EV, Chamberlain FL, Keys A, et al. Central Committee for Medical and Community Program of the American Heart Assiciation. Dietary fat and its relation to heart attacks and strokes. Circulation. 1961, 23, 133–136. [Google Scholar] [CrossRef]
- Sacks FM, Lichtenstein AH, Wu JH, et al. Dietary fats and cardiovascular disease: a presidential advisory from the American Heart Association. Circulation. 2017, 136, e1–e23. [Google Scholar]
- Bruhn JG, Wolf S. The Roseto Story: An Anatomy of Health. Lippincott Williams Wilkins, Philadelophia; 1980.
- Wolf S, Grace KL, Bruhn J, Stout C. Roseto revisited: further data on the incidence of myocardial infarction in Roseto and neighboring Pennsylvania communities. Trans Amer Clinical Climatol Assoc. 1974, 85, 100. [Google Scholar]
- Tough H, Siegrist J, Fekete C. Social relationships, mental health and wellbeing in physical disability: a systematic review. BMC public health. 2017, 17, 1–18. [Google Scholar]
- Coughlin, SS. Social determinants of colorectal cancer risk, stage, and survival: A systematic review. Int J Colorectal Dis. 2020, 35, 985–995. [Google Scholar] [CrossRef]
- Gladwell M. Outliers: The story of success. Little, Brown; 2002.
- Keys, A. Arteriosclerotic heart disease in Roseto, Pennsylvania. JAMA 1966, 195, 137–139. [Google Scholar] [CrossRef]
- Pressler M, Devinsky J, Duster M, et al. Dietary transitions and health outcomes in four populations – Systematic Review. Front Nutr 2022, 9, 748305. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. National diabetes statistics report: Estimates of diabetes and its burden in the United States, 2014.Atlanta, GA: US Department of Health and Human Services; 2014.
- Tversky, A and Kahneman, D. Belief in the low of small numbers. Psychological Bulletin 1971, 76, 105–110. [Google Scholar] [CrossRef]
- Lew, EA. Some implications of mortality statistics relating to coronary artery disease. J Chron Dise. 1957, 6, 192–209. [Google Scholar] [CrossRef]
- Page IH, Stare FJ, Corcoran A, et al. Atherosclerosis and the fat content of the diet. Circulation. 1957, 16, 163–178. [Google Scholar] [CrossRef]
- Keys, A. Atherosclerosis: a problem in newer public health. J Mt Sinai Hosp NY 1953, 20, 118–39. [Google Scholar]
- Lee JH, Duster M, Roberts T, Devinsky O. United States dietary trends since 1800, Lack of association between saturated fatty acid consumption and non-communicable diseases. Front Nutr 2022, 8, 748847. [Google Scholar] [CrossRef] [PubMed]
- Keys A, Anderston JT, Grande F. Serum cholesterol response in man: diet fat and intrinsic responsiveness. Circulation 1959, 19, 201–214. [Google Scholar] [CrossRef]
- Haneuse, S. Distinguishing selection bias and confounding bias in comparative effectiveness research. Medical Care. 2016, 54, e23. [Google Scholar] [CrossRef]
- Patel SS. The eclipse of the community study: The Roseto study in historical context. PhD Dissertation, Univ of Pennsylvania, 2007.
- Wolf S, Bruhn JG. The Power of Clan. The influences of human relationships on heart disease. Transaction Pubs, New Brunswick, NJ, 1993.
- Roman GC, Jackson RE, Reis J, et al. Extra-virgin olive oil for potential prevention of Alzheimer disease. Rev Neurol 2019, 175, 705–723. [Google Scholar] [CrossRef] [PubMed]
- https://en.wikipedia.org/wiki/Roseto_effect.
- Mann, GV. Diet-Heart: end of an era. New Engl J Med 1977, 297, 644–50. [Google Scholar] [CrossRef]
- Yerushalmy J, Hilleboe HE. Fat in the diet and mortality from heart disease; a methodological note. NY State Med J 1957, 57, 2343–54.
- Taubes G. Good calories, bad calories. Knopf, NY 2007.
- Ramsden CE, Zamora D, Majchrzak-Hong S, et al. Re-evaluation of the traditional diet-heart hypothesis: analysis of recovered data from Minnesota Coronary Experiment (1968-73). Brit Med J 2016, 353, i1246. [Google Scholar]
- Kannel WB, Gordon T. The Framingham Study. Section 24. The Framingham Diet Study. US Government Printing, 1968.
- Mann GV. A short history of the Diet/Heart Hypothesis. In: Mann GV, ed. Coronary Heart Disease. The Dietary Sense and Nonsense. Janus Pub Co., London, England. 1993, pp 1-17.
Figure 1.
Exploring role of chance and effect of low sample size.
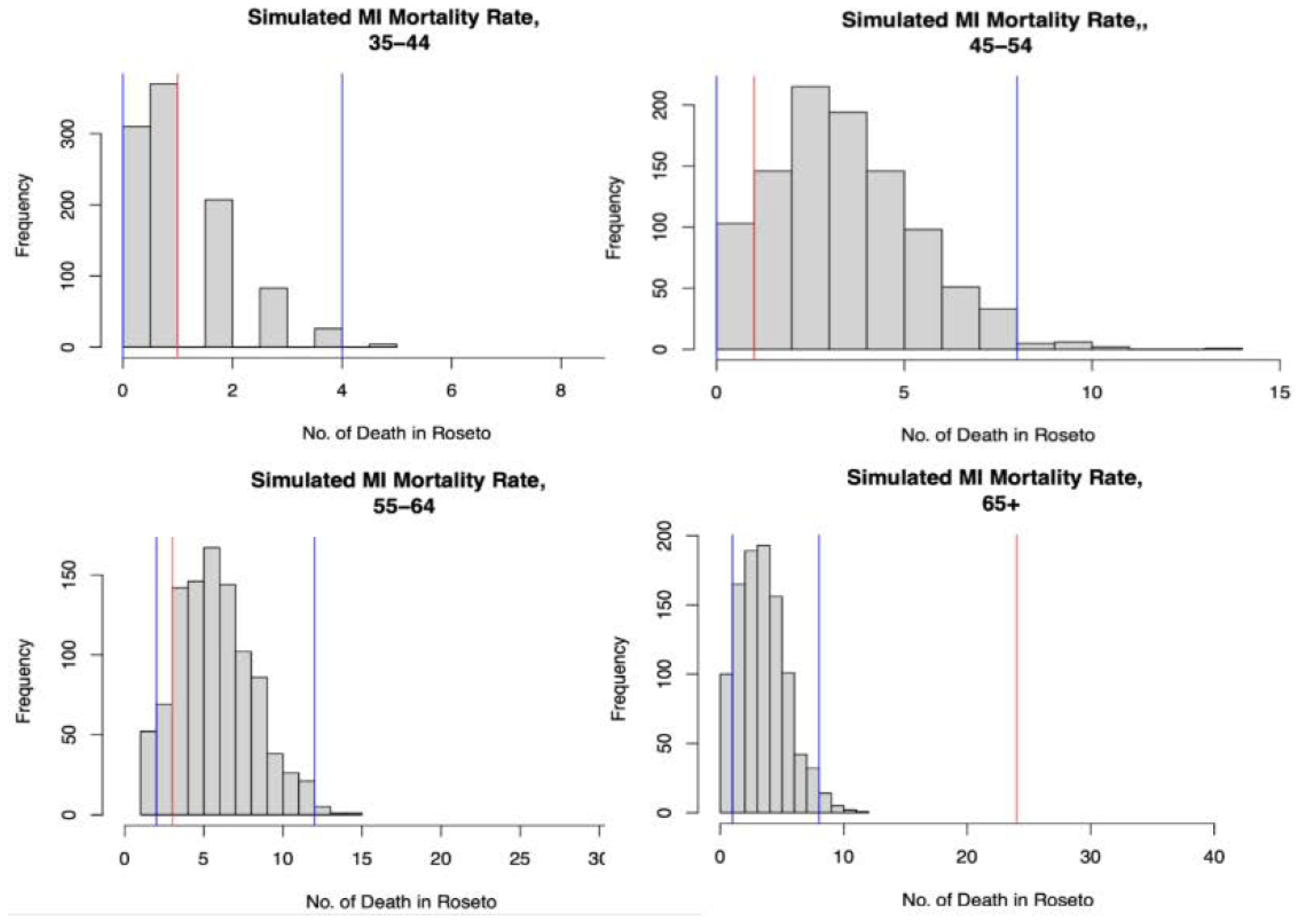

Table 1.
Age- and sex-specific deaths per 1000 from myocardial infraction between 1955 and 1974.
| Age group | ||||||
|---|---|---|---|---|---|---|
| Cohort | Year | Sex | 35-44 | 45-54 | 55-64 | 65+ |
| Framingham Heart study | 1955-1964 | M | 5.6 | 35.2 | 81.5 | 31.5 |
| F | 2.5 | 7.6 | 20.2 | 32.8 | ||
| Total | 4.3 | 23.5 | 55.6 | 32.1 | ||
| 1965-1974 | M | 0 | 11.7 | 42.9 | 87.1 | |
| F | 0 | 4.2 | 19.8 | 68 | ||
| Total | 0 | 8.1 | 31.9 | 78 | ||
| Roseto study | 1955-1964 | M | 8.3 | 9.8 | 29 | 211.3 |
| F | 0 | 0 | 15.9 | 120 | ||
| Total | 8.3 | 9.8 | 22.5 | 165.7 | ||
| 1965-1974 | M | 33.3 | 55 | 92.8 | 268.7 | |
| F | 0 | 0 | 15.9 | 181.8 | ||
| Total | 33.3 | 55 | 54.4 | 225.3 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



