
Submitted:
11 September 2024
Posted:
12 September 2024
You are already at the latest version
Abstract
This study aimed to identify whether the combined use of functional electrical stimulation (FES) reduces the motor torque of a gait exercise rehabilitation robot in spinal cord injury (SCI) and to verify the effectiveness of the developed automatic assist level adjustment in people with paraplegia. Acute and chronic SCI patients (1 case each) performed 10 min of gait exercises with and without FES using a rehabilitation robot. Reinforcement learning was used to adjust the assist level automatically. The maximum torque values and assist levels for each of the ten walking cycles when walking became steady were averaged and compared with and without FES. The motor's output torque and the assist level were measured as outcomes. The assist level adjustment allowed both the motor torque and assist level to decrease gradually to a steady state. The motor torque and the assist levels were significantly lower with the FES than without the FES under steady conditions in both cases. No adverse events were reported. The combined use of FES attenuated the motor torque of a gait exercise rehabilitation robot for SCI. Automatic assistive level adjustment is also useful for spinal cord injuries.
Keywords:
spinal cord injury
; functional electrical stimulation
; rehabilitation robot
; reinforcement learning
; assistive level
1. Introduction
Worldwide, approximately 15.4 million people were living with spinal cord injury (SCI). SCI is a major cause of long-term disability accounting for over 4.5 million years of life lived with disability in 2021 [1]. Many of these injuries are reported to result from high-energy trauma, such as motor vehicle accidents and falls. In contrast, the number of cases of incomplete SCI due to low-energy trauma from falls on level surfaces in older adults is increasing in Japan [2]. In particular, in the case of incomplete paralysis, appropriate assistance is needed in rehabilitation, in accordance with motor learning theory, depending on the recovery process of motor paralysis. A basic premise of motor learning is based on high-volume repetition and task-oriented training. Treatments based on this premise have become a major focus of research on the recovery of motor function in central nervous system disorders such as spinal cord injury and stroke [3,4]. For high-frequency training, robotic rehabilitation can provide more extensive training while compensating for the patient's lost functions and reducing the burden on supporting medical staff.
Neuromodulation techniques, such as functional electrical stimulation (FES), are important tools in restorative neurology [5]. FES can noninvasively activate paralyzed muscles or muscle groups through electrodes placed on the skin. Depending on whether the upper or lower motor neurons are damaged, stimulation directly activates the motor nerves or muscle fibers. Nerve stimulation relies on intact peripheral nerves and neural signal processing in the intact portion of the spinal cord below the lesion [6]. Previously, we developed a gait training rehabilitation robot with FES and confirmed that the robot torque was reduced by using FES in pseudo paraplegics [7]. In addition, a function for automatically adjusting the level of assistance using reinforcement learning has been developed, and its effectiveness in healthy subjects has been confirmed [8]. It is unknown whether using FES in combination with a gait training rehabilitation robot reduces motor torque in people with paraplegia with spinal cord injury. Moreover, there are currently no devices that automatically adjust the level of assistance. This study aimed to verify whether concurrent use of FES reduces the motor torque of a gait exercise rehabilitation robot in spinal cord injury and the effectiveness of the developed automatic assist level adjustment in people with paraplegia.
2. Materials and Methods
The subjects were a patient with acute thoracic spinal cord injury (33-year-old man), 2 weeks after injury, American Spinal Injury Association (ASIA) Impairment Scale (AIS) C, Neurological Level of Injury (NLI) T12 without spasticity, and a patient with chronic thoracic spinal cord injury (34-year-old man), 2 years after injury, AIS C, and NLI T11 with spasticity (Modified Ashworth Scale: grade 2). Patients performed 10 minutes of gait exercises with and without FES using a rehabilitation robot. The robot’s exoskeleton was designed based on the hip-knee-ankle-foot orthosis for paraplegia. The trunk, thigh, and lower leg were secured with belts. An ankle-foot orthosis (RAPS, Tomei Brace, Aichi, Japan) was used for the ankle joint, allowing for angle adjustment based on the patient's spasticity. The actuators driving the hip and knee joints were equipped with encoders, enabling the acquisition of joint angle data. Although the entire exoskeleton weighed 40 kg, it did not affect the patient during use owing to the weight being offset by a counterweight. The orthosis could be adjusted in length to fit each patient’s thigh and lower leg. The patients were lifted, and their weight was supported by a rehabilitation lift (SP-1000, Moritoh, Aichi, Japan); following this, they were walked under this condition on a treadmill (8.1T, JohnsonHealth Tech Japan, Tokyo, Japan). Bilateral quadriceps and hamstrings were stimulated using FES (Dynamid, DM2500, Minato Medical Science, Japan, Osaka) (Figure 1). The quadriceps, primarily the rectus femoris, were stimulated from mid-swing to mid-stance during the robotic gait cycle. The stimulation point was located at the motor point identified by palpation of the anterior superior iliac spine and lateral femoral condyle. The hamstrings, mainly on the lateral side, were stimulated from pre-swing to mid-stance, and the stimulation point was located at the motor point identified by palpation of the sciatic tuberosity and the head of the fibula. The exoskeleton system was pre-programmed using gait data from the joint angles of a healthy individual. The system performs walking motions by changing the positions of the hip and knee joints according to the gait data. The stimulus intensity was set to the lowest stimulus (15-20 mA, 25 Hz) that produced joint movement, and the stimulus timing was synchronized to the gait cycle [7].
The motor's output torque (Nm) was proportional to the stiffness parameter, and the range was divided into 50 parts, defined as the assist level. The higher the assistance level, the greater the amount of assistance. Force control was used to control the motor, and compliance control was used to vary the amount of assistance. The control equation used for compliance control is shown below.
𝜏 = 𝐾 ∙ 𝜃 + 𝐶 ∙ 𝜃̇1 + 𝐼 ∙ 𝜃̇2
In the equation, K (Nm/deg) represents the stiffness, C (Nm/deg∙s) represents the viscosity, I (Nm/deg ∙ s2) represents the inertia, θ (deg) is the deviation between the target joint angle and measured angle, θ̇1 (deg/s) and θ̇2 (deg/s2) are first and second derivative values of θ respectively, and τ (Nm) is the motor torque. The equation follows the equation of motion, and the first term indicates that the motor output increases as the difference between the target joint angle and measured joint angle increases. In the first term, the output torque is proportional to the stiffness parameter K. That is, when the stiffness parameter represented by K is large, the output torque increases; conversely, when K is small, the output torque decreases. In this study, the ranges of stiffness, viscosity, and inertia parameters were determined experimentally based on a previous study [9], and the range of stiffness (K) was divided into 50 parts and defined as the assist level. The assistance level provided feedback to the patient through data displayed on the computer monitor placed in front of the robot.
Reinforcement learning was used to adjust the assist level automatically. The method used was Q-learning, a type of off-policy temporal difference learning, and the ε-greedy method was used to determine the policy. The walking speed was set at 0.8 km/h. The maximum torque values and assist levels for each of the 10 walking cycles when walking became a steady condition were averaged and compared with and without FES. All statistical analyses were conducted using EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan) [10]. The motor torque and assistant level were compared using the paired t-test, with statistical significance set at P < 0.05.
This study was approved by our institution's Ethics Committee (approval number: CRB2180005). All the individuals voluntarily participated in the study and provided written informed consent.
3. Results
Assist level adjustment allowed both the motor torque and assist level to decrease gradually to a steady state. Each value reached a steady state between 60 and 120 seconds. The motor torque was significantly lower with the FES than without the FES under steady conditions in both cases (Table 1). Furthermore, the assist levels were significantly lower with FES than without FES in both cases (Table 2).
The electrical stimulation delivered via the FES did not cause any adverse effects, such as pain, and did not lead to any adverse events associated with robotic gait exercises.
4. Discussion
Combined use of FES attenuated the motor torque of the gait exercise rehabilitation robot for spinal cord injury. Further, automatic adjustment of the assistance level using reinforcement learning proved to be effective in gait exercises for patients with spinal cord injuries, and the combined use of FES attenuated the assistance level. This suggests that the intrinsic muscle activity generated by FES reconstructed some of the torque required for walking (Figure 2). In conventional robotic gait training, the gait is reconstructed by combining the robot torque with the patient's muscle torque; the use of FES in conjunction may help attenuate the robot torque. The addition of FES has previously been reported to reduce the electric motor torque of an exoskeletal assistive walking robot [11]. In addition, combining FES with a robot results in exercise associated with less muscle fatigue than FES alone [12], making hybrid FES-robot training useful for prolonged exercise. As a result, the use of a gait rehabilitation robot with FES improves the range of motion of the joints, the muscle strength and the ability to walk [13,14]. Robot-assisted training with FES appears to support the recovery of residual function after SCI and has been observed to lead to improvements in motor function and strength in the lower extremities [15]. In functional electrical stimulation therapy (FEST), three factors are crucial: the patient, FES, and the therapist. The therapist could be replaced by a robot. Furthermore, the potential of combining robotics and FES in rehabilitating patients with disorders affecting the central nervous system remains to be fully validated. Future validation is needed because robotic rehabilitation is expected to be integrated with brain-computer interface (BCI) [16] in the future.
Although machine learning and reinforcement learning in exoskeletal rehabilitation robots have previously been studied and reported on [17,18], this is the first report of their combination with FES for spinal cord injury. Automatic and appropriate adjustment of task difficulty according to the degree of paralysis is an effective rehabilitation tool from the perspective of motor learning [19]. Furthermore, the patients did not experience any discomfort during gait, and no adverse events were observed. Further research is required to ascertain the efficacy of this system's rehabilitative intervention.
The integration of FES with the robot may result in a reduction of motor torque, which could ultimately lead to a decrease in power consumption and size. The large size of conventional gait rehabilitation robots has been a substantial barrier their implementation in a broader range of settings. It is of paramount importance to reduce the size of the robot if the objective of achieving the generalization of robotic rehabilitation is to be met. The incorporation of artificial muscles may prove an efficacious solution to these challenges [20]. Given that the concurrent use of an exoskeleton-type robot and a treadmill represents a safe method for gait training rehabilitation, it is imperative to reduce the size of each to promote the overall effectiveness of robotic rehabilitation. Since FES reduces the torque generated by the robot's motor, it seems reasonable to employ FES to reduce the overall size of the robot. Consequently, the treadmill size can be reduced, thereby increasing compatibility with the treadmills that are commonly used. This may, in turn, facilitate the implementation of gait training rehabilitation robots in a wide range of applications, including the prevention of disabilities in the aging population.
This study included only two cases, but data were available for both acute and chronic cases. The automatic assist level adjustment system proved useful in both cases. However, further validation of the effects of rehabilitation using a sufficient number of patients is required. The walking speed and FES settings were fixed; further verification of the variations caused by changes in speed and FES settings is needed.
5. Conclusions
The combined use of a gait rehabilitation robot and FES reduced the robot’s motor torque in spinal cord injuries, and automatic assist level adjustment through reinforcement learning was effective in people with paraplegia. The clinical outcomes need to be evaluated.
Author Contributions
Conceptualization, R.K.; methodology, R.K., T.S.; software and hardware, T.I..; formal analysis, R.K.; investigation, T.S.; writing—original draft preparation, R.K.; writing—review and editing, Y.K., D.K., N.M.; supervision, N.M..; project administration, R.K.; funding acquisition, R.K. All authors have read and agreed to the published version of the manuscript.
Funding
This study was partly supported by the JSPS KAKENHI (Grant No. 23K16600) and the Japan Orthopaedics and Traumatology Research Foundation (Grant No.474).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by our institution's Ethics Committee (approval number: CRB2180005). All the individuals voluntarily participated in the study and provided written informed consent.
Data Availability Statement
Data are contained within the article. Contact the author for additional data.
Acknowledgments
We thank Sumito Musaka, Atsuko Harata, Yasufumi Yamaji, Tetsuya Yamauchi, Daiki Miura, Kai Maeda, Kaname Sasaki, Cao Yu, and Kota Odanagi for developing the rehabilitation robot. We thank Kazutoshi Hatakeyama, Motoyuki Watanabe, and Tomohiro Suda, for rehabilitation assistance and ideas for equipment development. We would like to thank Editage for English language editing.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- WHO spinal cord injury. Available online: https://www.who.int/news-room/fact-sheets/detail/spinal-cord-injury (accessed on 5 Sep 2024).
- Miyakoshi, N.; Suda, K.; Kudo, D.; Sakai, H.; Nakagawa, Y.; Mikami, Y.; Suzuki, S.; Tokioka, T.; Tokuhiro, A.; Takei, H.; et al. A nationwide survey on the incidence and characteristics of traumatic spinal cord injury in Japan in 2018. Spinal Cord 2021, 59, 626–634. [CrossRef]
- Hubli, M.; Dietz, V. The physiological basis of neurorehabilitation – Locomotor training after spinal cord injury. J Neuroeng Rehabil 2013, 10, 5. [CrossRef]
- Veerbeek, J.M.; van Wegen, E.; van Peppen, R.; van der Wees, P.J.; Hendriks, E.; Rietberg, M.; Kwakkel, G. What is the evidence for physical therapy poststroke? A systematic review and meta-analysis. PLOS ONE 2014, 9, e87987. [CrossRef]
- Holsheimer, J. Concepts and methods in neuromodulation and functional electrical stimulation: An introduction. Neuromodulation 1998, 1, 57–61. [CrossRef]
- Illis, L.S. Central nervous system regeneration does not occur. Spinal Cord 2012, 50, 259–263. [CrossRef]
- Inoue, J.; Kimura, R.; Shimada, Y.; Saito, K.; Kudo, D.; Hatakeyama, K.; Watanabe, M.; Maeda, K.; Iwami, T.; Matsunaga, T.; et al. Development of a gait rehabilitation robot using an exoskeleton and functional electrical stimulation: Validation in a pseudo-paraplegic model. Prog Rehabil Med 2022, 7, 20220001. [CrossRef]
- Maeda, K.; Iwami, T.; Kimura, R.; Shimada, Y. Development of an automatic adjustment system for the amount of assist using reinforcement leaning in gait rehabilitation robot for hemiplegic patients (in Japanese). Jpn J Inst Ind Appl Eng 2022, 10, 28–37.
- Antonio, J.d.; A.J.; Ángel, G.A.; Jose, L.P.; Juan, C.M. Hybrid FES-robot cooperative control of ambulatory gait rehabilitation exoskeleton. J NeuroEngineering Rehabil 2014, 11, 27. [CrossRef]
- Kanda Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013;48:452–8.
- Bao, X.; Molazadeh, V.; Dodson, A.; Dicianno, B.E.; Sharma, N. Using person-specific muscle fatigue characteristics to optimally allocate control in a hybrid exoskeleton – Preliminary results. IEEE Trans Med Robot Bionics 2020, 2, 226–235. [CrossRef]
- Kirsch, N.A.; Bao, X.; Alibeji, N.A.; Dicianno, B.E.; Sharma, N. Model-based dynamic control allocation in a hybrid neuroprosthesis. IEEE Trans Neural Syst Rehabil Eng 2018, 26, 224–232. [CrossRef]
- Zhang, D.; Ren, Y.; Gui. K.; Jia, J.; Xu, W. Cooperative control for a hybrid rehabilitation system combining functional electrical stimulation and robotic exoskeleton. Front Neurosci 2017, 11, 725. [CrossRef]
- del-Ama, A.J.; Gil-Agudo, Á.; Pons, J.L.; Moreno, J.C. Hybrid FES–robot cooperative control of ambulatory gait rehabilitation exoskeleton. J Neuroeng Rehabil 2014, 11, 27. [CrossRef]
- Bersch, I.; Alberty, M.; Fridén, J. Robot-assisted training with functional electrical stimulation enhances lower extremity function after spinal cord injury. Artif Organs 2022, 46, 2009–2014. [CrossRef]
- Marquez-Chin, C.; Popovic, M.R. Functional electrical stimulation therapy for restoration of motor function after spinal cord injury and stroke: A review. Biomed Eng OnLine 2020, 19, 34. [CrossRef]
- Pizzolato, C.; Saxby, D.J.; Palipana, D.; Diamond, L.E.; Barrett, R.S.; Teng, Y.D.; Lloyd, D.G. Neuromusculoskeletal modeling-based prostheses for recovery after spinal cord injury. Front Neurorobot 2019, 13, 97. [CrossRef]
- Luo, S.; Androwis, G.; Adamovich, S.; Nunez, E.; Su, H.; Zhou, X. Robust walking control of a lower limb rehabilitation exoskeleton coupled with a musculoskeletal model via deep reinforcement learning. J Neuroeng Rehabil 2023, 20, 34. [CrossRef]
- Spiess, M.R.; Steenbrink, F.; Esquenazi, A. Getting the best out of advanced rehabilitation technology for the lower limbs: minding motor learning principles. PM R 2018, 10, S165–S173. [CrossRef]
- Gonzalez-Vazquez, A.; Garcia, L.; Kilby, J.; McNair, P. Soft wearable rehabilitation robots with artificial muscles based on smart materials: A review. Adv Intell Syst 2023, 5, 2200159. [CrossRef]
Figure 1.
Gait exercise rehabilitation robot. The robot has an exoskeleton, rehabilitation lift, treadmill, and functional electrical stimulation (FES).
Figure 1.
Gait exercise rehabilitation robot. The robot has an exoskeleton, rehabilitation lift, treadmill, and functional electrical stimulation (FES).

Figure 2.
The motor torque. Conventional robots were constructed using robot torque and their own muscle torque for the torque required for walking. Motor torque is attenuated by the combined use of functional electrical stimulation (FES). Furthermore, the required motor torque decreases further as the patient’s muscle torque improves.
Figure 2.
The motor torque. Conventional robots were constructed using robot torque and their own muscle torque for the torque required for walking. Motor torque is attenuated by the combined use of functional electrical stimulation (FES). Furthermore, the required motor torque decreases further as the patient’s muscle torque improves.
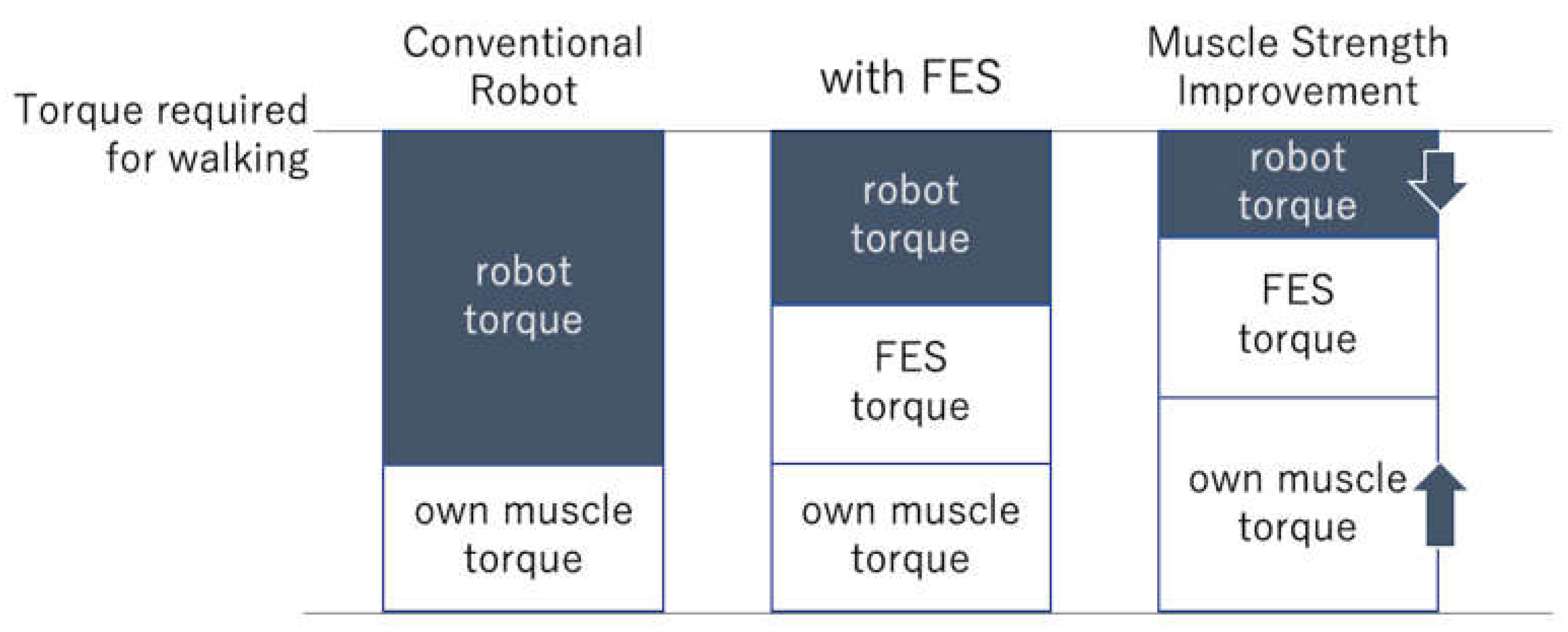

Table 1.
Motor torque.
| (Nm) | Case 1 | Case 2 | ||||
| FES (-) | FES (+) | P | FES (-) | FES (+) | P | |
| Hip Right |
18.6±1.5 | 16.6±1.7 | 0.0237 | 17.9±1.2 | 8.7±1.2 | <0.001 |
| Hip Left |
18.1±1.4 | 16±1.6 | 0.0181 | 14.7±1.3 | 11.9±1.7 | <0.001 |
| Knee Right |
20.3±1.8 | 13.1±1.5 | <0.001 | 15.4±1.2 | 13.4±1.6 | 0.0047 |
| Knee Left |
19.2±1.4 | 17.1±1.9 | 0.0226 | 18.4±1.5 | 12.2±1.3 | <0.001 |
Table 2.
Assist levels.
| Case 1 | Case 2 | |||||
|---|---|---|---|---|---|---|
| FES (-) | FES (+) | P | FES (-) | FES (+) | P | |
| Hip Right |
28.5±0.5 | 26.5±0.5 | <0.001 | 42.9±0.3 | 30.9±0.7 | <0.001 |
| Hip Left |
24.1±0.6 | 23.4±0.7 | 0.0445 | 38.9±0.3 | 30.9±0.3 | <0.001 |
| Knee Right |
30.8±0.4 | 23.9±0.3 | <0.001 | 25.4±0.5 | 20.6±0.5 | <0.001 |
| Knee Left |
29.5±0.5 | 17.5±0.5 | <0.001 | 33.9±0.3 | 21.4±0.5 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



