
Submitted:
12 September 2024
Posted:
12 September 2024
You are already at the latest version
Abstract
Background/Objectives: Obstructive Sleep Apnoea Syndrome (OSA) in children disrupts standard breathing patterns and sleep architecture, potentially leading to severe consequences. Early identification and intervention for OSA are crucial to prevent these issues. This study explored the relationships between waiting times for polysomnography (PSG), clinical history, age at the time of PSG, and PSG outcomes in children; Methods: Two hundred and fourteen children were prospectively enrolled. Data were extracted from medical records on the age at referral for PSG and at the time of its execution, the waiting time for PSG, diagnosis (primary snoring, mild, moderate, and severe OSA), history of snoring and apnoea, medications taken, surgical interventions, passive smoke exposure, and allergies. The records also included the Pediatric Sleep Questionnaire (PSQ); Results: The mean age at referral for PSG was 5.2 (2.8) years, the waiting time for PSG was 5.2 (5.0) months, and the age at the time of PSG was 5.6 (2.8) years. Children with a shorter history of OSA (≤12 months) underwent PSG at an earlier age (4.9 (2.7) years) compared to those with a more extended history (6.0 (2.7) years; p=0.006). A younger age at referral for PSG was associated with a lower PSQ score (r=0.167; p=0.015), a shorter history of apnoea (r=0.216; p=0.003) and snoring (r=0.187; p=0.023), but also with greater OSA severity, expressed as oxygen desaturation index (r=-0.152; p=0.026). In the correlation analysis, the waiting time for PSG, adjusted for age at referral, was longer in children with a prolonged history of apnoea (r=0.195; p=0.023) and snoring (r=0.259; p=0.002) but with a lower PSQ score (r=-0.172; p=0.045); Conclusions: Some children receive delayed treatment, increasing the risk of long-term complications. In evaluating children with suspected OSA, the duration of symptoms and the PSQ score at referral emerge as crucial factors that should be considered to optimise prioritisation for PSG access.
Keywords:
child
; obstructive sleep apnea
; Pediatric Sleep Questionnaire
; polysomnography
; sleep-disordered breathing
; waiting time
1. Introduction
Sleep-disordered breathing (SDB) encompasses a range of conditions such as primary snoring, upper airway resistance syndrome (UARS), obstructive hypoventilation, and obstructive sleep apnea (OSA) [1]. OSA is a significant condition characterised by intermittent upper airway obstructions, leading to disrupted sleep patterns, fluctuations in blood oxygen levels, and alternating episodes of hypoxia [2]. Polysomnography (PSG) is the preferred method for diagnosing OSA [3]. However, other methods, such as questionnaires, can help suspect the disorder (Villa et al., 2015) [4,5].
The prevalence of sleep-disordered breathing (SDB) is relatively high in children (2-4%) [6,7], with snoring occurring in 3-15% of cases and OSA (obstructive sleep apnoea) in 1-5%, particularly between the ages of 2 and 6, with no gender predominance [1,8].
The risk of SDB increases in specific conditions such as obesity, adenotonsillar hypertrophy, craniofacial malformations and neuromuscular disorders [1]. Other risk factors include prematurity, environmental smoke exposure, asthma, and allergic rhinitis [9]. Certain genetic conditions can increase the risk of developing OSA, particularly trisomy 21 (Down syndrome), achondroplasia, and Prader-Willi syndrome, which are characterised by anatomical malformations of the upper airways, such as maxillary hypoplasia, a high-arched palate, macroglossia, and muscle hypotonia [10,11,12].
OSA causes numerous complications affecting various organs and systems due to oxidative stress and the production of oxygen free radicals [13,14], including the cardiovascular system [15,16], leading to metabolic involvement [17], growth deficit [18], participation of the central nervous system [13] and neuropsychological aspects [19]. Early diagnosis of SDB is crucial to reduce the risk of short and long-term complications in pediatric age [7,20], as it can lead to significant improvements in a child's health, development, and quality of life [7,21].
In adults, OSA often remains undiagnosed in a significant proportion until the severe stages, with a wide range of health consequences [22]. The delay in diagnosis, termed in many studies as "total delay," comprises the "patient delay," the time between symptom recognition and seeking medical help, and the "provider/healthcare system delay," the time from the initial patient evaluation to diagnosis [23,24,25]. Factors influencing the delay in OSA diagnosis include low income, place of residence, occupation, and individual behavioural characteristics such as self-recognition and self-efficacy. The rate of delay in OSA diagnosis among adult patients (mean age 47 years, age range 18-76 years) was 91.9%, with a range of 0.5 to 28 months [25]. Significant delays in diagnosing and treating sleep-disordered breathing (SDB) have been reported in various countries, with wait times ranging from 2 to 36 months in Belgium and up to 60 months in Canada and the UK [26,27]. The waiting times vary widely across the country without clear geographical trends [28].
In general, waiting time represents a significant barrier to accessing healthcare for various health services in adults. Evidence shows that waiting time is unevenly distributed among those with a low socioeconomic status [29], exceeding recommended guidelines for timely assessment and treatment initiation [26]. Waiting times vary widely nationwide without clear geographical trends [26]. Waiting times vary widely nationwide without clear geographical trends [26].
In childhood, early diagnosis of paediatric OSA is crucial for preventing complications. Pediatric OSAS has often been neglected and underdiagnosed by both parents and healthcare professionals [30].
The study aims to improve the decision-making process in prescribing PSG, optimise the use of healthcare resources, and reduce diagnostic and therapeutic delays in children with suspected OSA.
2. Materials and Methods
2.1. Summary of Abbreviations
Adenoidectomy-T-1←: medical history of adenoidectomy performed before PSG prescription
Adenotonsillectomy-T-1←: medical history of adenotonsillectomy performed before PSG prescription
AHI (events/h): apnea-hypopnea index results obtained at PSG-T1 (years)
Apneas-T-1←: medical history of apneas before PSG prescription
Minimum SpO2 (%): minimum SpO2 (%) results obtained at PSG-T1 (years)
ODI (events/h): oxygen desaturation index results obtained at PSG-T1 (years)
Smoke exposure-T-1←: smoke exposure
PSG-T0 (years): age at PSG prescription
PSG-T0-1 (months): waiting time from prescription and PSG execution
PSG-T1 (years): age at PSG execution
PSQ-T0: results of PSQ administered at the same time of PSG-T0
Snoring-T-1←: medical history of snoring before PSG prescription
Snoring (% Total Sleep Time, TST): snoring (%) results obtained at PSG-T1 (years)
Therapy-T-1←: medical history of orally administered medications before PSG-T0
Tonsillectomy-T-1←: medical history of tonsillectomy performed before PSG prescription
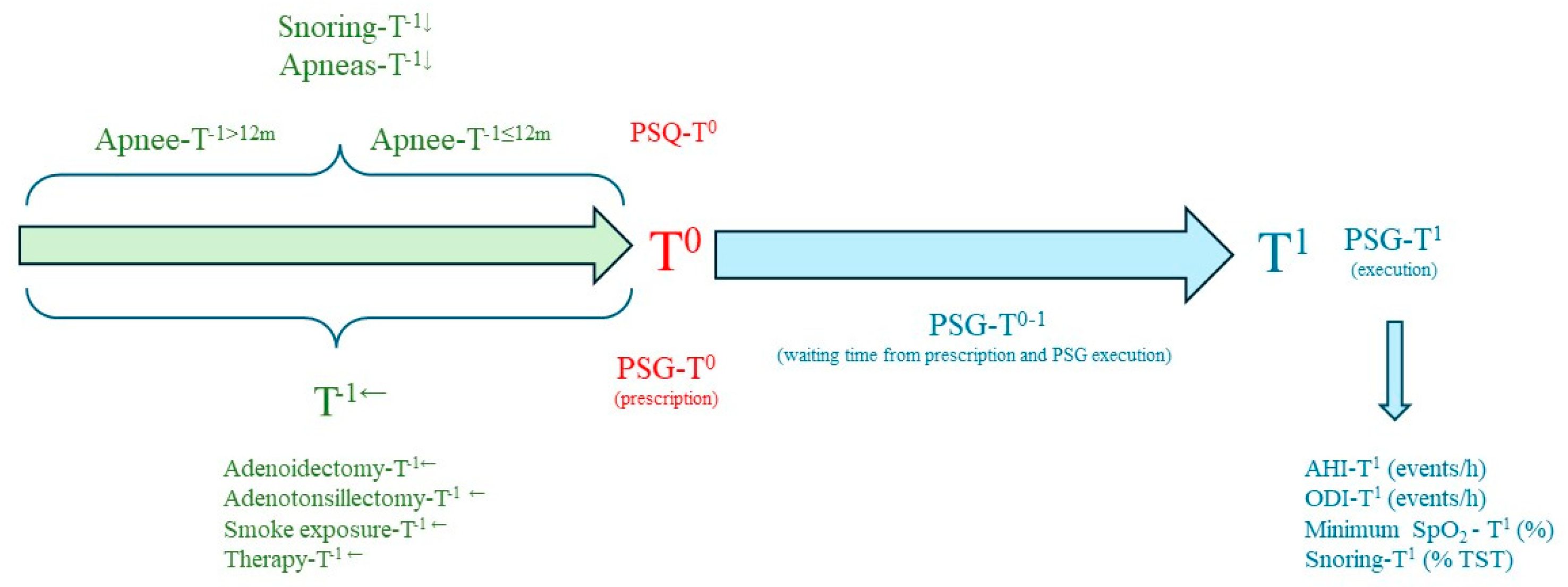
In the study, we defined 4 key investigation points: 1) apneas-T-1← and snoring-T-1←, 2) PSG-T0 and PSQ-T0, 3) PSG-T0-1, and 4) PSG-T1. Specifically, we retrospectively collected from medical records: PSG-T0 (years); PSG-T0-1 (months); PSG-T1 (years); PSQ-T0; PSG-T1 results as continuous variables: AHI (events/h), ODI (events/h), minimum SpO2 (%), and snoring (% Total Sleep Time, TST). PSG-T1 results as categorical variables of SDB severity: primary snoring, mild OSA, moderate, and severe; snoring-T-1←; apneas-T-1←; therapy-T-1← (orally administered medications: corticosteroids, antihistamines, anti-leukotrienes, spray or inhaler medications: corticosteroids, salbutamol); ENT surgery: adenoidectomy-T-1←, adenotonsillectomy-T-1←, and tonsillectomy-T-1←; passive smoke exposure-T-1←; allergies to inhalant allergens.
Figure 1.
Study design.
2.2. Polysomnography
A comprehensive overnight PSG-T1 study was conducted using a Healthdyne Technologies device (E-series Compumedics) [31]. The recorded parameters included nasal pressure, airflow (thermistor), thoracic/abdominal movements, pulse oximetry, electrocardiogram, and transcutaneous carbon dioxide. Sleep staging adhered to the Kales and Rechtshaffen criteria, utilising electroencephalogram, electrooculogram, and submental electromyogram data. Additionally, PSG incorporated audio/video recordings and a body position sensor. Sleep stage scoring criteria were established based on Kales and Rechtshaffen guidelines. Obstructive apnea is identified when a thermistor airflow of at least 90% reduction persists for at least two breaths. On the other hand, obstructive hypopnea is marked by a decrease in airflow between 50 and 90%, accompanied by a minimum of 3% oxygen desaturation or an EEG arousal. Oxygen desaturation was considered a ≥3% decrease from baseline oxygen saturation. The Apnea-Hypopnea Index (AHI) was computed as the total number of obstructive apneas and hypopneas divided by the total sleep time (TST, hours).
2.3. Pediatric Sleep Questionnaire
The PSQ-T0 is used for screening patient OSA [32]. It comprises 22 questions requiring a "yes", "no", or "do not know" response. The total score is determined by calculating the percentage of affirmative ('yes') responses, with a result deemed significant if positive responses account for more than 33% of the overall count.
2.4. Statistical Analysis
The Kolmogorov-Smirnov test is typically employed to determine if a continuous variable adheres to a normal distribution. The Mann-Whitney test, which is non-parametric, was utilised for a pair of values, yielding means and standard deviations (SD) for a range of outcome measures. The chi-square test was used in the exploration of categorical variables. Nevertheless, Fisher's exact test was preferred when the values fell below 5. The contingency coefficient was also calculated, providing information on the strength of association between variables. For variables reported as time intervals, the lower value was utilised. Bivariate correlation analysis was employed to calculate the Spearman correlation coefficient, expressed as r (p-value). The correlation between two variables, while adjusting for confounding variables, was ascertained using the zero-order correlation in partial correlations. Multiple linear regression was utilised to identify predictive factors for a specified dependent variable. Predictors are various factors that may influence the dependent variable under study. The table will present unstandardised coefficients, associated T-scores, standard errors, standardised coefficients (Beta), t-statistics, p-values, and 95% confidence intervals for coefficients. These data provide information on the strength and direction of the association between each predictor and the dependent variable and the statistical implication of these associations. A p-value < 0.05 was deemed statistically significant. Particularly in studies with smaller sample sizes, p-values between 0.05 and 0.1 should be interpreted with caution, as they can introduce greater uncertainty and elevate the risk of type I errors [33,34].
The data were entered into a Microsoft® Excel® database on a Windows 11 system and then subjected to statistical analysis using SPSS version 22.0 for Windows (SPSS Inc., Chicago, IL, USA).
The study complied with the Declaration of Helsinki and patients’ parents signed informed consent before the inclusion in the study. The clinical study was approved by Insubria Ethical Committee (on 25 May 2019, study number 14/2019).
3. Results
Table 1 (panels A and B) describes the statistical analyses performed on the continuous (panel A) and categorical (panel B) variables of the 214 enrolled pediatric patients in the study.
Table 2 (panel A) presents the comparison of continuous variables between patients with a short history of sleep apneas (apneas-T-1≤12m, ≤ 12 months) and a long history (apneas-T-1>12m, > 12 months) from the prescription of PSG-T0. Age at PSG-T0 was 4.6 years (SD 2.6) for patients with apneas-T-1≤12m and 5.5 years (SD 2.7) for those with apneas-T-1>12m, with a statistically significant difference (p = 0.027). PSG-T0-1 was 4.1 months (SD 3.8) for patients with apneas-T-1≤12m and 5.9 months (SD 3.8) for those with apneas-T-1>12m, with a statistically significant difference (p = 0.001). Additionally, age at PSG-T1 was 4.9 years (SD 2.7) for the apneas-T-1≤12m group and 6.0 years (SD 2.7) for the apneas-T-1>12m group, with a statistically significant difference (p = 0.006). None of the results of the PSG-T1 recording (AHI, ODI, SpO2 minimum, and snoring) were different between the apneas-T-1≤12m group and the apneas-T-1>12m group.
Table 2 (Panel B) presents the statistical analysis of categorical variables (gender, PSG outcome categories, pharmacological therapy, otorhinolaryngologic surgery on tonsils and adenoids, passive smoke exposure, allergies) among patients with apneas-T-1≤ 12m and apneas-T-1> 12m.
The comparison of the frequency distribution of otorhinolaryngologic surgeries between patients with apneas-T-1≤ 12m and apneas-T-1> 12m, including adenoidectomy-T-1←, tonsillectomy-T-1←, and adenotonsillectomy-T-1←, reach statistical significance (p = 0.012). However, a higher frequency of adenotonsillectomy-T-1← (13.3%) was observed in the apneas-T-1>12m group compared to the apneas-T-1≤ 12m group (6.9%). Additionally, a higher frequency of adenoidectomy-T-1← (9.7%) was noted in the apneas-T-1≤ 12m group compared to the apneas-T-1>12m group (1.3%).
The percentage distribution of PSG-T1-derived SDB categories, medication-T-1← categories (taken orally, nasally, or via inhalation), passive smoke exposure-T-1←, and allergies did not significantly differ between patients with apneas-T-1≤ 12m and apneas-T-1>12m.
The results expressed in Table 3 (Panel A) compare patients who underwent PSG within ≤ 3 months of waiting (PSG-T0-1 ≤ 3m) with those who had it done after > 3 months of waiting (PSG-T0-1 > 3m). The age at PSG-T0 (years) did not exhibit a statistically significant difference between PSG-T0-1 ≤ 3m and PSG-T0-1 > 3m (p = 0.688). However, the group with PSG-T0-1 > 3m had a higher mean age [5.8 (2.9) years] compared to the group with a shorter PSG-T0-1 ≤ 3m [5.1 (2.6) years; p = 0.053]. Additionally, the group with PSG-T0-1 > 3m had a longer mean duration of apnea-T-1← [17.7 (8.1) months] compared to the group with PSG-T0-1 ≤ 3m [11.6 (8.0) months; p < 0.001]. Similarly, the group with a longer PSG-T0-1 > 3m had a higher mean duration of snoring-T-1← [23.4 (13.8) months] compared to the group with PSG-T0-1 ≤ 3m [20.5 (14.2) months; p < 0.084]. No statistically significant differences were found in the PSG-T1 outcome for the considered scores (AHI, ODI, and snoring) between the PSG-T0-1 ≤ 3m and PSG-T0-1 > 3m groups. Finally, the PSQ-T0 score showed no statistically significant differences between the PSG-T0-1 ≤ 3m and PSG-T0-1 > 3m groups.
Table 3 (Panel B) presents the statistical analysis of categorical variables (gender, categories of PSG-T1 outcome, pharmacological therapy-T-1←, tonsil and adenoid surgery-T-1←, passive smoke exposure-T-1←, allergies) among patients with PSG-T0-1≤ 3m and PSG-T0-1>3m.
The categories of PSG-T1 outcome (% of patients) exhibited slight differences (C=0.173) between patients with PSG-T0-1≤ 3m and PSG-T0-1>3m (Pearson's chi-square p= 0.085). Specifically, the percentage of moderate and severe OSA-T1 was higher (50%) in patients who underwent PSG-T0-1≤ 3m compared to those with PSG-T0-1>3m (34.6%). Moreover, the percentage of patients with snoring-T1 in PSG-T1 was higher (16.2%) in the PSG-T0-1>3m category compared to those with PSG-T0-1≤ 3m (7.7%).
Finally, all other categorical variables (gender, medication, surgery, passive smoke exposure, allergy) were comparable between the PSG-T0-1≤3m and PSG-T0-1>3m groups.
Table 4 displays Spearman correlation coefficients and their corresponding two-tailed significance values for various correlated variables.
Age at PSG-T0 positively correlated with snoring-T-1← (r = 0.216, p = 0.003), apnea-T-1← (r = 0.187, p = 0.023), and PSQ-T0 (r = 0.167, p = 0.015). It negatively correlated with ODI-T1 (r = -0.152, p = 0.026). Adjusted for age at PSG-T1, age at PSG-T0 negatively correlated with apnea-T-1← (r = -0.290, p = 0.001).
/Age at PSG-T1 positively correlated with snoring-T-1← (r = 0.233, p = 0.001), apnea-T-1← (r = 0.237, p = 0.004), PSQ-T0 (r = 0.143, p = 0.037), and negatively with ODI-T1 (r = -0.162, p = 0.018). Additionally, age at PSG-T1, adjusted for age at PSG-T0, positively correlated with snoring-T-1← (r = 0.189, p = 0.027) and apnea-T-1← (r = 0.308, p < 0.001).
PSG-T0-1 (months) positively correlated with apnea-T-1← (r = 0.327, p < 0.001). Adjusted for age at PSG-T0, it positively correlated with snoring-T-1← (r = 0.195, p = 0.023) and apnea-T-1← (r = 0.259, p = 0.002), and negatively with PSQ-T0 (r = -0.172, p = 0.045). Adjusted for age at PSG-T1, PSG-T0-1 (months) positively correlated with apnea-T-1← (r = 0.241, p = 0.004), and negatively with PSQ-T0 (r = -0.179, p = 0.036).
The solutions of the linear regression analysis disclosed in Table 5 reveal two significant predictors of PSG-T0-1: apnea-T-1← and PSQ-T1 score. The positive and significant coefficient of the predictor apnea-T-1← indicates that an apnea-T-1← (months) increase is associated with a 0.12-unit increase in the dependent variable PSG-T0-1 (months). The PSQ-T0 has an unstandardised coefficient of -3.163, suggesting that a one-unit increase in PSQ-T0 score is associated with a decrease of 3.2 units in PSG-T0-1 (months).
4. Discussion
The study evaluated the relationship between a medical history of OSA (apnea and snoring), age at PSG prescription and PSQ scores, waiting time for PSG, and PSG results.
In summary, children with a shorter history of OSA undergo PSG evaluation at an earlier age than those with a more extended history of OSA. Additionally, there are no significant differences in PSQ score at referral and final PSG results between the two groups, indicating that the duration of OSA may not significantly influence the severity of the illness or the management response. Prolonged waiting times for PSG are associated with a more extended history of apnea, suggesting potential delays in diagnosis and treatment initiation. Interestingly, despite these differences in waiting times, there were no significant variations in PSG results or demographic factors such as age, sex, medication use, or exposure to smoke or allergens. However, when looking at the severity of SDB, children who had shorter waiting times showed a slightly higher rate of severe OSA. This highlights how crucial it is to conduct timely PSG evaluations for managing the condition. These findings emphasize the need for efficient healthcare systems to reduce waiting times and ensure quick diagnosis and treatment for children with sleep apnea.
The correlation analysis in this study offers intriguing insights into the factors influencing waiting times for PSG in children with sleep apnea. Surprisingly, younger children with shorter histories of apnea and snoring exhibited higher severity of SDB, measured by the oxygen desaturation index. This suggests that children with more recent symptoms of apnea are prioritised for PSG evaluations, potentially leading to quicker referrals. Conversely, it is worth noting that children with higher PSQ scores have shorter waiting times for PSG, which aligns with expectations. Adjusted data indicate that only a short history of apnea and high PSQ scores reliably predict shorter waiting times for PSG. These findings underscore the complex interplay of symptoms, severity, and healthcare access in managing pediatric sleep apnea.
Interestingly, there is a notable difference in the distribution of surgeries based on the duration of apnea history. Children with longer histories of apnea at referral were more likely to undergo adenotonsillectomy, while those with shorter histories tended to have adenoidectomies. Remarkably, none of the children underwent tonsillectomy alone. These findings emphasize the need to customize surgical interventions according to the duration and severity of apnea. Additionally, the study suggests that factors like passive smoke exposure, medication use, and PSG result categories didn’t significantly affect the choice of surgical procedure. With the high prevalence of OSA and increasing awareness of its health effects, laboratory sleep services are under considerable pressure. This has resulted in expanding waitlists and postponements in both diagnosis and treatment. There is an urgent need for accessible and cost-effective ambulatory methods to diagnose and manage OSA as an alternative to traditional laboratory-based approaches [35,36]. These measures are essential for addressing the growing disease burden and effectively meeting the increasing demand for sleep services [35].
Children with a shorter history of apnea are younger at the prescription and execution of PSG, and they have a shorter waiting time for PSG than children with a more prolonged history of apnea. Clinical symptoms may raise suspicion, but the diagnosis cannot be established without PSG [37]. At this age, a diagnostic delay is influenced by the availability of sleep centres and diagnostic equipment [4]. Conducting sleep studies in an outpatient setting can facilitate the early identification and management of OSA, potentially leading to significant cost savings. This method offers a viable alternative to traditional in-laboratory sleep studies, which may be more accessible and affordable for certain patient populations[38].
Moreover, recent findings indicate that there are no significant differences in PSQ scores or PSG parameters—such as the AHI, ODI, and snoring—between children with shorter versus longer histories of apnea. Children with shorter waiting times for PSG have shown a higher prevalence of moderate to severe OSA. According to a study, prolonged waiting times for PSG can range from several months to a year, potentially leading to underdiagnosis of OSAS [39]. Early diagnosis and treatment of pediatric OSA are crucial to prevent complications affecting children's growth, cognitive development, and behaviour [30,40].
It has been reported that the average waiting time for PSG can range from several months to a year, with potential undiagnosed cases of OSA and treatment delay [39]. Children with a longer waiting time for PSG had a longer history of apnea. Additionally, children with a longer waiting time for PSG exhibited a slightly longer history of snoring and were older at PSG execution. No differences were found regarding age at PSG prescription and PSQ score, and final results of PSG, expressed as AHI, ODI, and snoring. However, when PSG results were categorised as SDB severity, the severity distribution was mildly different, showing more severe OSA in children with a shorter waiting time for the final PSG.
Unexpectedly, children with more recent symptoms are identified and referred for PSG more rapidly (shorter waiting time). Conversely, a long onset period of apnea has not been associated with a shorter waiting time for PSG. Instead, both shorter and longer waiting times for PSG execution showed comparable mean scores on the PSQ. The PSQ is highly valued in screening patients with suspected OSA [41]. Finally, only history of apnea (short) and PSQ score (high) results are predictive of waiting time for PSG (short).
It has been reported that PSQ can be a helpful tool for evaluating the severity of OSA in children [41] and promptly directing them to appropriate treatment. Therefore, a simple medical history might not suffice; clinical assessment, medical history review, questionnaires, and objective measurements may be necessary [21].
Furthermore, the study found that children with a shorter history of OSA had comparable severity of SDB at PSG between shorter and longer history of OSA [42]. This suggests that the duration of symptoms is not correlated with the severity of the condition, as children with a recent history of OSA may have comparable forms of SDB severity.
Additionally, children with a more extended history of OSA had comparable passive smoke exposure to those with a shorter history. This data could indicate that less and more than one year of smoke exposure had a comparable effect on OSA severity. There is evidence suggesting a link between passive smoking and the development of OSA in children [43,44,45].
Lastly, the age of children at PSG prescription was positively correlated with their history of snoring and apnea and the PSQ score and negatively correlated with the ODI. Additionally, older children referred for PSG may have a more extended history of snoring and apnea, resulting in higher PSQ scores but potentially lower ODI values, indicating a less severe form of SDB at the final PSG assessment.
A cross-sectional study based on a large sample of children (1,014 from hospital and outpatient settings), suggested improving screening for SDB and ensuring effective management of SDB by planning standardised educational interventions [46]. Numerous challenges with screening and diagnosis leave a high number of cases of undiagnosed OSA [21]. Due to their unique relationship with parents, ambulatory paediatrics may play a significant role in developing a patient-centred model and reducing the time to diagnose SDB.
The awareness of the long-term impacts of pediatric SDB has led to an increase in consultations with pediatric respiratory sleep specialists, resulting in longer waiting lists. The introduction of pre-clinical electronic questionnaires and tests has doubled the consultation capacity for patients. A focused and efficient clinic that utilises electronic questionnaires for uncomplicated patients can improve waiting times for children referred to pediatric respiratory medicine for SDB evaluation [47].
The American Academy of Pediatrics (AAP) intends telemedicine to enhance high-quality pediatric care, particularly in rural areas [48]. A survey reported that over 20% of paediatricians in rural and urban areas are adopting telemedicine for follow-up care [49]. Although telemedicine provides convenience and easier access to healthcare, there are some drawbacks when it comes to managing OSAS. These include limitations in performing physical exams, accessing diagnostic tools, providing education and counseling, and dealing with technological and privacy issues. Adopting a hybrid approach, which integrates both in-person and virtual appointments, may effectively meet the needs of children with OSAS [50].
Heath developed a triage algorithm for pediatric OSA based on tonsil size. According to Brodsky, the study proposed referring healthy children with OSA to an otolaryngologist if the tonsil is grade 2, 3, or 4. Children with smaller tonsil sizes were referred to a respiratory paediatrician to streamline the referral process and reduce waiting times for appropriate care [51]. Lastly, the multidisciplinary expert group in Italy proposed a stepped approach for the diagnosis and management of pediatric SDB based on the child's age. This group suggests different age-specific stepped pathways. The pathway ensures that children with SDB receive timely and effective diagnosis and treatment, regardless of age [52].
In our study, children with a short medical history of apnea had a comparable severity of SDB at PSG to those with a more extended history. Additionally, at PSG prescription, younger children had higher PSQ scores. The waiting time for PSG was shorter in children with a high PSQ score and a shorter medical history of sleep apnea and snoring. Therefore, the medical history of OSA (short onset) and PSQ score (high) should be considered when planning waiting times for PSG. The present study revealed that these children can have more severe SDB. Healthcare providers should be familiar with OSA manifestations as children present with varied clinical symptoms and signs based on their developmental stages [30,51].
Our patients would undergo PSG as a post-surgical control following adenoidectomy or adenotonsillectomy due to persistent symptoms. The distribution of otorhinolaryngologic surgeries before evaluation with PSG (no surgery, adenoidectomy, tonsillectomy, and adenotonsillectomy) among children with short and longer histories of apnea differed. There was a higher frequency of adenotonsillectomy in children with a more extended history of apnea and adenoidectomies in children with a shorter history of apnea. We can hypothesise that children with a more extended history of apnea may potentially have a higher frequency of adenotonsillectomy due to the severity and chronicity of their condition. In addition, a history of more prolonged apnea and a milder severity of PSG outcome may be correlated with a higher frequency of adenotonsillectomy in these patients. The studies indicate that adenotonsillectomy is the first-line treatment for pediatric OSAS, associated with significant improvements in polygraphic parameters [53,54]. Adenotonsillectomy is a more significant intervention that can significantly impact the upper airway and respiratory system [55]. Moreover, children with a shorter history of apnea may undergo adenoidectomies more frequently as an initial treatment. The potential for residual symptoms or complications with adenoidectomies might be higher, and the potential for complications might be lower [56].
The study's strengths include the fact that it includes many children with OSA. The study also looked at how various factors affected waiting times and PSG outcomes, using suitable statistical methods. However, its retrospective design limits its ability to establish cause-and-effect relationships. Additionally, the study didn’t take into account other possible factors that might influence waiting times or PSG results. The results may not be applicable to different populations. Additionally, the study did not assess the impact of waiting time for PSG on long-term outcomes in children with OSA.
5. Conclusions
When evaluating and prescribing PSG for children suspected of having OSA, it's important to take into account both the onset of symptoms and the PSQ score at the time of referral. Children with a short history of OSA and high PSQ scores at the time of evaluation should be referred for PSG more promptly. Children with more recent symptoms are recognised more quickly and can begin treatment early, potentially improving clinical outcomes and reducing the risk of long-term complications. Older children at the time of PSG prescription may have a longer history of snoring and apnoea but lower severity of OSA at PSG execution, justified by more frequent successful adenotonsillectomy. However, children with a more extended history of apneas wait longer for PSG. These results suggest that there is a subset of children who could be treated late and with an increased risk of long-term complications. Optimize resource allocation to prioritize PSG for the patients who need it most. This highlights the need for a comprehensive evaluation and thoughtful review of medical history and questionnaire responses to speed up the child's referral for PSG. Further research is needed to determine the best approach to reduce PSG waiting times in children.
Author Contributions
Conceptualization, L.N. and M.A.; methodology, D.S.; software, M.Z.; validation, G.R.D., M.V. and H.A.; formal analysis, M.Z.; investigation, L.Z.; resources, M.A.; data curation, M.Z. and D.S.; writing—original draft preparation, M.Z.; writing—review and editing, G.R.D., M.V. and H.A.; visualisation, L.N.; supervision, M.A. and L.N. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Insubria Ethical Committee (protocol code 14/2019, 25 May 2019).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data are unavailable due to privacy and ethical restrictions.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Gipson, K.; Lu, M.; Kinane, T.B. Sleep-Disordered Breathing in Children. Pediatr Rev 2019, 40, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Sateia, M.J. International classification of sleep disorders-third edition: highlights and modifications. Chest 2014, 146, 1387–1394. [Google Scholar] [CrossRef] [PubMed]
- Kaditis, A.G.; Alonso Alvarez, M.L.; Boudewyns, A.; Alexopoulos, E.I.; Ersu, R.; Joosten, K.; Larramona, H.; Miano, S.; Narang, I.; Trang, H.; et al. Obstructive sleep disordered breathing in 2- to 18-year-old children: diagnosis and management. Eur Respir J 2016, 47, 69–94. [Google Scholar] [CrossRef] [PubMed]
- Villa, M.P.; Pietropaoli, N.; Supino, M.C.; Vitelli, O.; Rabasco, J.; Evangelisti, M.; Del Pozzo, M.; Kaditis, A.G. Diagnosis of Pediatric Obstructive Sleep Apnea Syndrome in Settings With Limited Resources. JAMA Otolaryngol Head Neck Surg 2015, 141, 990–996. [Google Scholar] [CrossRef]
- Chervin, R.D.; Weatherly, R.A.; Garetz, S.L.; Ruzicka, D.L.; Giordani, B.J.; Hodges, E.K.; Dillon, J.E.; Guire, K.E. Pediatric sleep questionnaire: prediction of sleep apnea and outcomes. Arch Otolaryngol Head Neck Surg 2007, 133, 216–222. [Google Scholar] [CrossRef] [PubMed]
- Bitners, A.C.; Arens, R. Evaluation and Management of Children with Obstructive Sleep Apnea Syndrome. Lung 2020, 198, 257–270. [Google Scholar] [CrossRef] [PubMed]
- Zaffanello, M.; Franchini, M.; Piacentini, G. Pediatric Sleep-Disordered Breathing and Long-Term Complications: Clinical and Health Implications. In J Clin Med; Switzerland, 2022; Volume 11.
- Piotto, M.; Gambadauro, A.; Rocchi, A.; Lelii, M.; Madini, B.; Cerrato, L.; Chironi, F.; Belhaj, Y.; Patria, M.F. Pediatric Sleep Respiratory Disorders: A Narrative Review of Epidemiology and Risk Factors. Children (Basel) 2023, 10. [Google Scholar] [CrossRef]
- Savini, S.; Ciorba, A.; Bianchini, C.; Stomeo, F.; Corazzi, V.; Vicini, C.; Pelucchi, S. Assessment of obstructive sleep apnoea (OSA) in children: an update. Acta Otorhinolaryngol Ital 2019, 39, 289–297. [Google Scholar] [CrossRef]
- Lee, C.F.; Lee, C.H.; Hsueh, W.Y.; Lin, M.T.; Kang, K.T. Prevalence of Obstructive Sleep Apnea in Children With Down Syndrome: A Meta-Analysis. J Clin Sleep Med 2018, 14, 867–875. [Google Scholar] [CrossRef]
- Zaffanello, M.; Antoniazzi, F.; Tenero, L.; Nosetti, L.; Piazza, M.; Piacentini, G. Sleep-disordered breathing in paediatric setting: existing and upcoming of the genetic disorders. Ann Transl Med 2018, 6, 343. [Google Scholar] [CrossRef]
- Zaffanello, M.; Pietrobelli, A.; Piacentini, G.; Guzzo, A.; Antoniazzi, F. The Impact of Growth Hormone Therapy on Sleep-Related Health Outcomes in Children with Prader-Willi Syndrome: A Review and Clinical Analysis. J Clin Med 2023, 12. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.-L.; Lu, C.-H.; Lin, H.-C.; Chen, P.-C.; Chou, K.-H.; Lin, W.-M.; Tsai, N.-W.; Su, Y.-J.; Friedman, M.; Lin, C.-P.; et al. White matter damage and systemic inflammation in obstructive sleep apnea. Sleep 2015, 38, 361–370. [Google Scholar] [CrossRef] [PubMed]
- Orrù, G.; Storari, M.; Scano, A.; Piras, V.; Taibi, R.; Viscuso, D. Obstructive Sleep Apnea, oxidative stress, inflammation and endothelial dysfunction-An overview of predictive laboratory biomarkers. Eur Rev Med Pharmacol Sci 2020, 24, 6939–6948. [Google Scholar] [CrossRef] [PubMed]
- Tagetti, A.; Bonafini, S.; Zaffanello, M.; Benetti, M.V.; Vedove, F.D.; Gasperi, E.; Cavarzere, P.; Gaudino, R.; Piacentini, G.; Minuz, P.; et al. Sleep-disordered breathing is associated with blood pressure and carotid arterial stiffness in obese children. J Hypertens 2016. [Google Scholar] [CrossRef]
- Burns, A.T.; Hansen, S.L.; Turner, Z.S.; Aden, J.K.; Black, A.B.; Hsu, D.P. Prevalence of Pulmonary Hypertension in Pediatric Patients With Obstructive Sleep Apnea and a Cardiology Evaluation: A Retrospective Analysis. J Clin Sleep Med 2019, 15, 1081–1087. [Google Scholar] [CrossRef]
- Agarwal, N.; Sharma, B.C. Insulin resistance and clinical aspects of non-alcoholic steatohepatitis (NASH). Hepatol Res 2005, 33, 92–96. [Google Scholar] [CrossRef]
- Zaffanello, M.; Piacentini, G.; La Grutta, S. Beyond the growth delay in children with sleep-related breathing disorders: a systematic review. Panminerva Med 2020, 62, 164–175. [Google Scholar] [CrossRef]
- Zaffanello, M.; Pietrobelli, A.; Zoccante, L.; Ferrante, G.; Tenero, L.; Piazza, M.; Ciceri, M.L.; Nosetti, L.; Piacentini, G. Mental Health and Cognitive Development in Symptomatic Children and Adolescents Scoring High on Habitual Snoring: Role of Obesity and Allergy. Children (Basel) 2023, 10. [Google Scholar] [CrossRef]
- Marcus, C.L.; Brooks, L.J.; Ward, S.D.; Draper, K.A.; Gozal, D.; Halbower, A.C.; Jones, J.; Lehmann, C.; Schechter, M.S.; Sheldon, S.; et al. Diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics 2012, 130. [Google Scholar] [CrossRef]
- Borrelli, M.; Corcione, A.; Cimbalo, C.; Annunziata, A.; Basilicata, S.; Fiorentino, G.; Santamaria, F. Diagnosis of Paediatric Obstructive Sleep-Disordered Breathing beyond Polysomnography. Children (Basel) 2023, 10. [Google Scholar] [CrossRef]
- Baker-Smith, C.M.; Isaiah, A.; Melendres, M.C.; Mahgerefteh, J.; Lasso-Pirot, A.; Mayo, S.; Gooding, H.; Zachariah, J. Sleep-Disordered Breathing and Cardiovascular Disease in Children and Adolescents: A Scientific Statement From the American Heart Association. J Am Heart Assoc 2021, 10, e022427. [Google Scholar] [CrossRef] [PubMed]
- Getnet, F.; Demissie, M.; Assefa, N.; Mengistie, B.; Worku, A. Delay in diagnosis of pulmonary tuberculosis in low-and middle-income settings: systematic review and meta-analysis. BMC Pulm Med 2017, 17, 202. [Google Scholar] [CrossRef] [PubMed]
- Muttamba, W.; Kyobe, S.; Komuhangi, A.; Lakony, J.; Buregyeya, E.; Mabumba, E.; Basaza, R.K. Delays in diagnosis and treatment of pulmonary tuberculosis in patients seeking care at a regional referral hospital, Uganda: a cross sectional study. BMC Res Notes 2019, 12, 589. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Liang, C.; Zhang, X.; Yu, H.; Yan, X.; Wang, L.; Tong, T.; Zhang, H.; Dai, H.; Tong, H. Factors influencing patient delay in individuals with obstructive sleep apnoea: a study based on an integrated model. Ann Med 2022, 54, 2828–2840. [Google Scholar] [CrossRef] [PubMed]
- Thornton, C.S.; Tsai, W.H.; Santana, M.J.; Penz, E.D.; Flemons, W.W.; Fraser, K.L.; Hanly, P.J.; Pendharkar, S.R. Effects of Wait Times on Treatment Adherence and Clinical Outcomes in Patients With Severe Sleep-Disordered Breathing: A Secondary Analysis of a Noninferiority Randomized Clinical Trial. JAMA Netw Open 2020, 3, e203088. [Google Scholar] [CrossRef]
- Thornton, C.S.; Povitz, M.; Tsai, W.H.; Loewen, A.H.; Ip-Buting, A.; Kendzerska, T.; Flemons, W.W.; Fraser, K.L.; Hanly, P.J.; Pendharkar, S.R. Impact of wait times for treatment on clinical outcomes in patients with obstructive sleep apnoea: protocol for a randomised controlled trial. ERJ Open Res 2022, 8. [Google Scholar] [CrossRef]
- Flemons, W.W.; Douglas, N.J.; Kuna, S.T.; Rodenstein, D.O.; Wheatley, J. Access to diagnosis and treatment of patients with suspected sleep apnea. Am J Respir Crit Care Med 2004, 169, 668–672. [Google Scholar] [CrossRef]
- McIntyre, D.; Chow, C.K. Waiting Time as an Indicator for Health Services Under Strain: A Narrative Review. Inquiry 2020, 57, 46958020910305. [Google Scholar] [CrossRef]
- Chang, S.J.; Chae, K.Y. Obstructive sleep apnea syndrome in children: Epidemiology, pathophysiology, diagnosis and sequelae. Korean J Pediatr 2010, 53, 863–871. [Google Scholar] [CrossRef]
- Nosetti, L.; Zaffanello, M.; Katz, E.S.; Vitali, M.; Agosti, M.; Ferrante, G.; Cilluffo, G.; Piacentini, G.; La Grutta, S. Twenty-year follow-up of children with obstructive sleep apnea. J Clin Sleep Med 2022, 18, 1573–1581. [Google Scholar] [CrossRef]
- Chervin, R.D.; Hedger, K.; Dillon, J.E.; Pituch, K.J. Pediatric sleep questionnaire (PSQ): validity and reliability of scales for sleep-disordered breathing, snoring, sleepiness, and behavioral problems. Sleep Med 2000, 1, 21–32. [Google Scholar] [CrossRef] [PubMed]
- Dekking, F.M. A Modern Introduction to Probability and Statistics: Understanding Why and How, Springer, 2005.
- Greenland, S.; Senn, S.J.; Rothman, K.J.; Carlin, J.B.; Poole, C.; Goodman, S.N.; Altman, D.G. Statistical tests, P values, confidence intervals, and power: a guide to misinterpretations. Eur J Epidemiol 2016, 31, 337–350. [Google Scholar] [CrossRef] [PubMed]
- Chai-Coetzer, C.L.; Antic, N.A.; McEvoy, R.D. Ambulatory models of care for obstructive sleep apnoea: Diagnosis and management. Respirology 2013, 18, 605–615. [Google Scholar] [CrossRef] [PubMed]
- Corral-Peñafiel, J.; Pepin, J.L.; Barbe, F. Ambulatory monitoring in the diagnosis and management of obstructive sleep apnoea syndrome. Eur Respir Rev 2013, 22, 312–324. [Google Scholar] [CrossRef] [PubMed]
- Nieminen, P.; Tolonen, U.; Löppönen, H. Snoring and obstructive sleep apnea in children: a 6-month follow-up study. Arch Otolaryngol Head Neck Surg 2000, 126, 481–486. [Google Scholar] [CrossRef] [PubMed]
- Phua, C.Q.; Jang, I.J.; Tan, K.B.; Hao, Y.; Senin, S.R.B.; Song, P.R.; Soh, R.Y.; Toh, S.T. Reducing cost and time to diagnosis and treatment of obstructive sleep apnea using ambulatory sleep study: a Singapore sleep centre experience. Sleep Breath 2021, 25, 281–288. [Google Scholar] [CrossRef]
- Hung, C.J.; Kang, B.H.; Lin, Y.S.; Su, H.H. Comparison of a home sleep test with in-laboratory polysomnography in the diagnosis of obstructive sleep apnea syndrome. J Chin Med Assoc 2022, 85, 788–792. [Google Scholar] [CrossRef]
- Halbower, A.C.; Degaonkar, M.; Barker, P.B.; Earley, C.J.; Marcus, C.L.; Smith, P.L.; Prahme, M.C.; Mahone, E.M. Childhood obstructive sleep apnea associates with neuropsychological deficits and neuronal brain injury. PLoS Med 2006, 3, e301. [Google Scholar] [CrossRef]
- Ferry, A.M.; Wright, A.E.; Ohlstein, J.F.; Khoo, K.; Pine, H.S. Efficacy of a Pediatric Sleep Questionnaire for the Diagnosis of Obstructive Sleep Apnea in Children. Cureus 2020, 12, e12244. [Google Scholar] [CrossRef]
- Zhai, F.; Li, Y.; Chen, J. Comparison of polysomnography, sleep apnea screening test and cardiopulmonary coupling in the diagnosis of pediatric obstructive sleep apnea syndrome. Int J Pediatr Otorhinolaryngol 2021, 149, 110867. [Google Scholar] [CrossRef]
- Corbo, G.M.; Fuciarelli, F.; Foresi, A.; De Benedetto, F. Snoring in children: association with respiratory symptoms and passive smoking. Bmj 1989, 299, 1491–1494. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Au, C.T.; Leung, T.F.; Wing, Y.K.; Lam, C.W.; Li, A.M. Effects of passive smoking on snoring in preschool children. J Pediatr 2013, 163, 1158–1162. [Google Scholar] [CrossRef] [PubMed]
- Jara, S.M.; Benke, J.R.; Lin, S.Y.; Ishman, S.L. The association between secondhand smoke and sleep-disordered breathing in children: a systematic review. Laryngoscope 2015, 125, 241–247. [Google Scholar] [CrossRef]
- Nosetti, L.; Paglietti, M.G.; Brunetti, L.; Masini, L.; La Grutta, S.; Cilluffo, G.; Ferrante, G.; Zaffanello, M.; Verrillo, E.; Pavone, M.; et al. Application of latent class analysis in assessing the awareness, attitude, practice and satisfaction of paediatricians on sleep disorder management in children in Italy. PLoS ONE 2020, 15, e0228377. [Google Scholar] [CrossRef] [PubMed]
- Lau, A.; Ewing, C.; Gnanapragasam, J.; Majaesic, C.; MacLean, J.; Mandhane, P.J. Changes to a pediatric sleep disordered breathing clinic improve wait-times and clinic efficiency. Pediatr Pulmonol 2016, 51, 1234–1241. [Google Scholar] [CrossRef]
- Burke, B.L., Jr.; Hall, R.W. Telemedicine: Pediatric Applications. Pediatrics 2015, 136, e293–e308. [Google Scholar] [CrossRef] [PubMed]
- Sisk, B.; Alexander, J.; Bodnar, C.; Curfman, A.; Garber, K.; McSwain, S.D.; Perrin, J.M. Pediatrician Attitudes Toward and Experiences With Telehealth Use: Results From a National Survey. Acad Pediatr 2020, 20, 628–635. [Google Scholar] [CrossRef]
- Rizzo, L.; Barbetta, E.; Ruberti, F.; Petz, M.; Tornesello, M.; Deolmi, M.; Fainardi, V.; Esposito, S. The Role of Telemedicine in Children with Obstructive Sleep Apnea Syndrome (OSAS): A Review of the Literature. J Clin Med 2024, 13. [Google Scholar] [CrossRef]
- Heath, D.S.; El-Hakim, H.; Al-Rahji, Y.; Eksteen, E.; Uwiera, T.C.; Isaac, A.; Castro-Codesal, M.; Gerdung, C.; Maclean, J.; Mandhane, P.J. Development of a pediatric obstructive sleep apnea triage algorithm. J Otolaryngol Head Neck Surg 2021, 50, 48. [Google Scholar] [CrossRef]
- Esposito, S.; Ricci, G.; Gobbi, R.; Vicini, C.; Caramelli, F.; Pizzi, S.; Fadda, A.; Ferro, S.; Plazzi, G. Diagnostic and Therapeutic Approach to Children and Adolescents with Obstructive Sleep Apnea Syndrome (OSA): Recommendations in Emilia-Romagna Region, Italy. Life (Basel) 2022, 12. [Google Scholar] [CrossRef]
- Locci, C.; Cenere, C.; Sotgiu, G.; Puci, M.V.; Saderi, L.; Rizzo, D.; Bussu, F.; Antonucci, R. Adenotonsillectomy in Children with Obstructive Sleep Apnea Syndrome: Clinical and Functional Outcomes. J Clin Med 2023, 12. [Google Scholar] [CrossRef] [PubMed]
- Connolly, H.V.; Tomaselli, L.T.; McKenna Benoit, M.K. Adenotonsillectomy for pediatric obstructive sleep apnea: how to predict those at risk for postoperative complications. J Clin Sleep Med 2020, 16, 3–4. [Google Scholar] [CrossRef] [PubMed]
- Tauman, R.; Gulliver, T.E.; Krishna, J.; Montgomery-Downs, H.E.; O'Brien, L.M.; Ivanenko, A.; Gozal, D. Persistence of obstructive sleep apnea syndrome in children after adenotonsillectomy. J Pediatr 2006, 149, 803–808. [Google Scholar] [CrossRef] [PubMed]
- Nath, A.; Emani, J.; Suskind, D.L.; Baroody, F.M. Predictors of persistent sleep apnea after surgery in children younger than 3 years. JAMA Otolaryngol Head Neck Surg 2013, 139, 1002–1008. [Google Scholar] [CrossRef]

Table 1.
A summarises the continuous variables of the enrolled pediatric patients in the study.
| Continuous Variable | Mean (SD) | 25° pc | 50° pc | 75° pc | Kolmogorov-Smirnov test* |
|---|---|---|---|---|---|
| Age PSG-T0 (years) | 5.2 (2.8) | 3.3 | 4.6 | 6.4 | <0.001 |
| PSQ-T0 (score) | 0.34 (0.19) | 0.22 | 0.36 | 0.45 | 0.012 |
| PSG-T0-1 (months) | 5.2 (5.0) | 2.1 | 4.2 | 8.2 | <0.001 |
| Age PSG-T1 (years) | 5.6 (2.8) | 3.8 | 5.0 | 6.8 | <0.001 |
| Weight-T1 (kg) | 22.5 (13.7) | 15 | 18 | 25 | <0.001 |
| Height-T1 (cm) | 113 (19) | 99 | 110 | 125 | 0.005 |
| PSG-T1 | |||||
| AHI-T1 (Events/h) | 7.0 (7.9) | 2.3 | 4.1 | 8.0 | <0.001 |
| ODI-T1 (Events/h) | 6.0 (7.4) | 2 | 3.5 | 6.3 | <0.001 |
| SpO2-T1 (%) | 96.8 (1.0) | 96.1 | 96.9 | 97.5 | 0.001 |
| SpO2 minimum-T1 (%) | 89.1 (4.4) | 88 | 90 | 92 | <0.001 |
| Snoring-T1 (%) | 4.5 (4.6) | 9 | 3.5 | 6.6 | <0.001 |
Legend: *, all variables of this table do not follow a normal distribution; AHI, apnea-hypopnea index; ODI, oxygen desaturation index; PSG, polysomnography; PSQ, pediatric sleep questionnaire; PSG-T0, age at medical prescription of the PSG; PSG-T0-1, waiting time for the execution of the PSG; PSG-T1, PSG execution (age, or results); SD, standard deviation.
Table 1.
B summarises the categorical variables of the enrolled pediatric patients in the study.
| Categorical variable | Subcategories | N (%) |
|---|---|---|
| Sex | Male | 133 (62.1) |
| Snoring-T-1← (minimum, months; missing=don't know) | I do not know | 21 (9.8) |
| 0-6 | 15 (7) | |
| 6-12 | 38 (17.8) | |
| 12-18 | 4 (1.9) | |
| 18-24 | 109 (50.9) | |
| > 24 | 27 (12.6) | |
| Apnee-T-1← (minimum, months; missing=don't know) | I do not know | 71 (33.1) |
| 0-6 | 18 (8.4) | |
| 6-12 | 30 (14) | |
| 12-18 | 29 (13.6) | |
| 18-24 | 5 (2.3) | |
| > 24 | 66 (30.8) | |
| Drugs-T-1← Taken orally | No | 186 (86.9) |
| Antihistamines | 10 (4.7) | |
| Corticosteroids | 5 (2.3) | |
| Antileukotrienes | 4 (1.9) | |
| Other | 4 (1.9) | |
| Drugs-T-1← spray, inhalant | No | 162 (75.7) |
| Steroids | 51 (23.8) | |
| Salbutamol | 0 | |
| Steroids, salbutamol | 1 (0.5) | |
| Otorhinolaryngology surgery-T-1← | Adenotonsillectomy | 15 (7.5) |
| Adenoidectomy | 9 (4.2) | |
| Tonsillectomy | 1 (0.5) | |
| Exposure to secondhand smoke-T-1← | Yes | 42 (19.6) |
| Allergy test (prick test) | Yes | 38 (17.8) |
| Not executed | 154 (72.0) | |
| Result of the PSG-T1 (Categories) | Primary snoring | 28 (13.1) |
| Mild | 100 (46.7) | |
| Moderate | 43 (20.1) | |
| Severe | 43 (20.1) |
Legend: T-1←, Clinical History of the symptom (snoring-T-1← e apnee-T-1←), drugs-T-1← or ENT surgery-T-1← (adenotonsillectomy, adenoidectomy e tonsillectomy) before PSG medical prescription; PSG-T1, PSG Execution.
Table 2.
A. Comparison of continuous variables between patients whose history of sleep apneas is ≤ 12 months (apneas-T-1≤ 12m) and >12 months (apneas-T-1>12m) from the medical prescription of polysomnography (PSG-T0). If continuous variables do not have a normal distribution, the Mann-Whitney U test was used as the statistical test.
Table 2.
A. Comparison of continuous variables between patients whose history of sleep apneas is ≤ 12 months (apneas-T-1≤ 12m) and >12 months (apneas-T-1>12m) from the medical prescription of polysomnography (PSG-T0). If continuous variables do not have a normal distribution, the Mann-Whitney U test was used as the statistical test.
| Apnee-T-1≤12m (n.72), Mean (SD) |
Apnee-T-1>12m (n. 75), Mean (SD) |
Test U (Mann-Whitney), P | |
|---|---|---|---|
| Apnee-T-1 (months) | 7.35 (3.74) | 23.2 (2.5) | 0.001 |
| Snoring-T-1 (months) | 15.2 (12.7) | 30.3 (10.8) | 0.001 |
| PSG-T0 (years) | 4.6 (2.6) | 5.5 (2.7) | 0.027 |
| PSQ-T0 (score) | 0.37 (0.2) | 0.34 (0.21) | 0.466 |
| PSG-T0-1 (months) | 4.1 (3.8) | 5.9 (3.8) | 0.001 |
| PSG-T1 (years) | 4.9 (2.7) | 6.0 (2.7) | 0.006 |
| AHI-T1 (events/h) | 7.9 (8.2) | 6.8 (7.5) | 0.224 |
| ODI-T1 (events/h) | 6.7 (7.6) | 6.0 (7.0) | 0.316 |
| SpO2-T1 minimum (%) | 87.9 (5.3) | 89.3 (4.3) | 0.127 |
| Snoring-T1 (% TST) | 4.3 (4.2) | 4.3 (4.4) | 0.946 |
Legend: AHI, apnea-hypopnea index; ODI, oxygen desaturation index; PSG, polysomnography; PSQ, pediatric sleep questionnaire; SD, standard deviation; TST, total sleep time. Apnee-T-1←, history of sleep apnea before PSG prescription; apnee-T-1≤6m, history of apnea ≤6 months; apnee-T-1>6m, storia di apnee >6 months; PSG-T0, PSG prescription; PSG-T0-1, waiting time to perform PSG; PSG-T1, PSG Execution.
Table 2.
B. Comparison of categorical variables between patients (n. 147, did not reply n. 67) who experienced the onset of sleep apnea for less than 12 months (apnea-T-1≤ 12m) or more than 12 months (apnea-T-1>12m) before the medical prescription of polysomnography (PSG-T0).
Table 2.
B. Comparison of categorical variables between patients (n. 147, did not reply n. 67) who experienced the onset of sleep apnea for less than 12 months (apnea-T-1≤ 12m) or more than 12 months (apnea-T-1>12m) before the medical prescription of polysomnography (PSG-T0).
| Categorical variables | Subcategories | Apnee-T-1≤ 12m (n. 72); % | Apnee-T-1>12m (n.75); % |
Pearson Chi-Square | Fisher's Exact Test | Contingency coefficient |
|---|---|---|---|---|---|---|
| Sex | Males | 63.9 | 60.0 | 0.647 | - | 0.040 |
| Adenoidectomy-T-1← | Yes | 9.7 | 1.3 | 0.027 | 0.182 | |
| Tonsillectomy-T-1← | Yes | 0 | 0 | - | - | - |
| Adenotonsillectomy-T-1← | Yes | 6.9 | 13.3 | - | 0.157 | 0.105 |
| 0.012 | - | 0.238 | ||||
| Secondhand smoke-T-1← | Yes | 16.7 | 18.7 | 0.751 | - | 0.026 |
| Allergy | Yes | 50.0 | 75.0 | - | 0.189 | 0.227 |
| Drugs-T-1← taken orally | Antihistamines | 2.8 | 2.7 | |||
| Steroids | 2.8 | 4.0 | ||||
| Antileukotrienes | 1.4 | 4.0 | ||||
| Other | 2.8 | 0.0 | 0.530 | - | 0.145 | |
| Drugs-T-1← spray or inhalants | Steroids | 29.2 | 25.3 | |||
| Salbutamol | 0 | 0 | ||||
| Steroids+salbutamol | 0 | 1.3 | 0.550 | 0.090 | ||
| PSG result-T1 (Categories, %) | Snoring | 9.7 | 10.7 | |||
| Mild OSA | 41.7 | 46.7 | ||||
| Moderate OSA | 22.2 | 21.3 | ||||
| Severe OSA | 26.4 | 21.3 | 0.885 | - | 0.066 |
Legend: OSA, obstructive sleep apnea; PSG, polysomnography; apnee-T-1←, history of apnea prior to PSG prescription; apnee-T-1≤6m, history of apnea ≤6 Months; apnee-T-1>6m, history of apnea > 6 months; drugs-T-1←, history of taking medication prior to prescribing PSG; PSG-T0, PSG prescription; PSG-T0-1, PSG waiting time; PSG-T1, PSG Execution.
Table 3.
A. Comparison between patients who underwent polysomnography within 3 months of receiving a medical prescription and those who underwent PSG after 3 months of receiving a medical prescription.
Table 3.
A. Comparison between patients who underwent polysomnography within 3 months of receiving a medical prescription and those who underwent PSG after 3 months of receiving a medical prescription.
| PSG-T0-1≤ 3m (n. 78); Mean (SD) | PSG-T0-1>3m (n.136); Mean (SD) | Test U (Mann-Whitney) P | |
|---|---|---|---|
| Snoring-T-1← (minimum, months; missing=don't know) | 20.5 (14.2) [Total Responses n. 74] |
23.4 (13.8) [Total Responses n. 120] |
0.084 |
| Apnee-T-1← (minimum, months; missing=don't know) | 11.6 (8.0) [Total Responses n. 55] |
17.7 (8.1) [Total Responses n. 92] |
< 0.001 |
| PSG-T0 (years) | 5.0 (2.6) | 5.3 (2.9) |
0.688 |
| PSG-T0-1 | 1.4 (1.0) | 7.4 (5.1) | < 0.001 |
| PSQ-T0 (score) | 0.35 (0.18) | 0.34 (0.20) | 0.313 |
| Age PSG-T1 (years) | 5.1 (2.6) | 5.8 (2.9) | 0.053 |
| AHI-T1 (Events/h) | 7.7 (8.5) | 6.6 (7.6) | 0.226 |
| ODI-T1 (Events/h) | 6.2 (7.4) | 5.8 (7.4) | 0.361 |
| Snoring-T1 (% TST) | 4.6 (4.7) | 4.5 (4.5) | 0.751 |
Legend: AHI, apnea-hypopnea index; ODI, oxygen desaturation index; PSG, Polysomnography; PSQ, pediatric sleep questionnaire; SD, standard deviation; SDB, sleep-disordered breathing. T-1←, History of SDB symptom (apnea, snoring) prior to prescription of PSG -T0; PSG-T0, prescription for PSG; PSG-T0-1, waiting time for PSG; PSG-T0-1≤ 3m, waiting time for PSG ≤ 3 Months; PSG-T0-1> 3m, PSG > 3 months waiting time.
Table 3.
B. Comparison of categorical variables (Pearson's chi-square or Fisher's exact test) between patients who had a waiting time for PSG ≤ 3 months (PSG-T0-1≤ 3m) from medical prescription PSG-T0 and those who underwent PSG > 3 months (PSG-T0-1>3m) from medical prescription PSG-T0.
Table 3.
B. Comparison of categorical variables (Pearson's chi-square or Fisher's exact test) between patients who had a waiting time for PSG ≤ 3 months (PSG-T0-1≤ 3m) from medical prescription PSG-T0 and those who underwent PSG > 3 months (PSG-T0-1>3m) from medical prescription PSG-T0.
| Categorical variables | Subcategories | PSG-T0-1≤ 3m, % | PSG-T0-1>3m; % | Pearson Square Chi | Fisher's Exact Test | Contingency coefficient |
|---|---|---|---|---|---|---|
| N. | - | 78 | 136 | - | - | - |
| Sex | Males | 64.1 | 61 | 0.656 | 0.383 | 0.030 |
| PSG result-T1 (Categories) | Snoring | 7.7 | 16.2 | |||
| Mild OSA | 42.3 | 49.3 | ||||
| Moderate OSA | 26.9 | 16.2 | ||||
| Severe OSA | 23.1 | 18.4 | 0.085 | - | 0.173 | |
| Medications taken orally-T-1← | Antihistamines | 7.7 | 2.9 | |||
| Steroids | 3.8 | 1.5 | ||||
| Antileukotrienes | 0 | 2.9 | ||||
| Other | 2.6 | 1.5 | 0.174 | - | 0.170 | |
| Pharmacy Spray Nasal-T-1← | Steroids | 26.6 | 22.8 | |||
| Salbutamol | 0 | 0 | ||||
| Steroids+salbutamol | 0 | 0.7 | 0.680 | - | 0.060 | |
| Adenotonsillectomy-T-1← | Yes | 10.3 | 5.9 | 0.242 | 0.183 | 0.080 |
| Adenoidectomy- T-1← | Yes | 3.8 | 4.4 | 0.843 | 0.573 | 0.014 |
| Tonsillectomy-T-1← | No | 100 | 99.3 | 0.448 | 0.636 | 0.052 |
| 0.588 | 0.094 | |||||
| Exposure to secondhand smoke-T-1← | Yes | 17.9 | 20.6 | 0.640 | 0.390 | 0.032 |
| Allergy | Yes | 68.4 | 61 | 0.578 | 0.398 | 0.072 |
Legend: OSA, obstructive sleep apnea; PSG, polysomnography. T-1←, Clinical History of the symptom (apnee- T-1←, snoring- T-1←) before PSG medical prescription; PSG-T0, prescription for PSG; PSG-T0-1, waiting time for PSG; PSG-T0-1≤ 3m, waiting time for PSG ≤ 3 mesi; PSG-T0-1> 3m, waiting time for PSG > 3 months.
Table 4.
The table presents the results of the Spearman correlation analysis between Age at PSG-T0, Age at PSG-T1, PSG-T0-1, and the history of SDB, along with the results of PSN and PSQ.
Table 4.
The table presents the results of the Spearman correlation analysis between Age at PSG-T0, Age at PSG-T1, PSG-T0-1, and the history of SDB, along with the results of PSN and PSQ.
| N | Age PSG-T0, years (SD) | Age PSG-T1, years (SD) | PSG-T0-1, Months (SD) | |
|---|---|---|---|---|
| Age, years (SD) | 5.2 (2.8) | 5.6 (2.8) | 5.2 (5.0) | |
| Spearman's rho correlation coefficient, r (Sign. a due code) | ||||
| Snoring-T-1← (minimum, months; missing=don't know) | 194 | 0.216 (0.003) | 0.233 (0.001) | 0.119 (0.098) |
| Apnee-T-1← (minimum, months; missing=don't know) | 147 | 0.187 (0.023) | 0.237 (0.004) | 0.327 (<0.001) |
| PSQ-T0 (score) | 214 | 0.167 (0.015) | 0.143 (0.037) | -0.091 (0.186) |
| AHI-T1 (events/hour) | 214 | -0.116 (0.091) | -0.127 (0.064) | -0.097 (0.157) |
| ODI-T1 (eventi/ora) | 214 | -0.152 (0.026) | -0.162 (0.018) | -0.089 (0.195) |
| Snoring-T1 (% TST) | 194 | 0.086 (0.210) | -0.075 (0.273) | -0.045 (0.512) |
| Spearman's rho correlation coefficient, r (Sign. Two-tailed); adjusted for age at the PSG-T0 | 214 | |||
| Snoring-T-1← (minimum, months; missing=don't know) | 214 | - | 0.189 (0.027) | 0.195 (0.023) |
| Apnee-T-1← (minimum, months; missing=don't know) | 214 | - | 0.308 (<0.001) | 0.259 (0.002) |
| PSQ-T0 (score) | 214 | - | -0.103 (0.230) | -0.172 (0.045) |
| AHI-T1 (events/hour) | 214 | - | -0.005 (0.957) | -0.052 (0.549) |
| ODI-T1 (events/hour) | 214 | - | -0.004 (0.959) | -0.041 (0.634) |
| Russamento-T1 (% TST) | 214 | - | -0.009 (0.916) | -0.004 (0.962) |
| Correlation coefficient rho of Spearman, r (Sign. a two-tailed); adjusted for age at the PSG-T1 | 214 | |||
| Snoring-T-1← (minimum, months; missing=don't know) | 214 | -0.158 (0.066) | - | 0.166 (0.052) |
| Apnee-T-1← (minimum, months; missing=don't know) | 214 | -0.290 (0.001) | - | 0.241 (0.004) |
| PSQ-T0 (score) | 214 | 0.111 (0.196) | - | -0.179 (0.036) |
| AHI-T1 (events/hour) | 214 | -0.019 (0.830) | - | -0.032 (0.714) |
| ODI-T1 (events/hour) | 214 | -0.019 (0.822) | - | -0.020 (0.813) |
| Snoring-T1 (% TST) | 214 | 0.024 (0.781) | - | -0.017 (0.841) |
Legend: AHI, apnea-hypopnea index; ODI, oxygen desaturation index; PSG, polysomnography; PSQ, pediatric sleep questionnaire; SD, standard deviation; TST, total sleep time. T-1←, History of the symptom (apnee-1←, snoring-1←) before PSG-T0; PSG-T0, prescription for PSG; PSG-T0-1, waiting time for PSG; PSG-T0-1≤ 3m, waiting time for PSG ≤ 3 Months; PSG-T0-1> 3m, waiting time for PSG > 3 Months; PSG-T1, PSG Execution. The colour orange has a positive correlation; the colour green has a negative correlation.
Table 4.
A linear regression analysis to identify predictive factors for the waiting time for PSG.
| Dependent variable: PSG-T0-1, Months (SD). Predictors: Age at PSQ-T0, years (SD); snoring-T-1←, apnee-T-1←; AHI-T1 (events/hour); ODI-T1 (events/hour); snoring-T1 (%); PSQ-T0 |
Non-standardised coefficients, T | S.E. | Standardised coefficients, Beta | t | p | C.I. per B 95 % (lower-upper) |
|---|---|---|---|---|---|---|
| Variables Entered in the Model | ||||||
| Apnee-T-1← (Months) | 0.118 | 0.037 | 0.264 | 3.225 | 0.002 | 0.046 – 0.191 |
| PSQ-T0 | -3.163 | 1.554 | -0.167 | -2.040 | 0.043 | -6.321 – (-0.096) |
| Constant | 4.174 | 0.852 | 4.9 | 0.001 | 2.489 – 5.858 |
Legend: AHI, apnea-hypopnea index; C.I., confidence interval; ODI, oxygen desaturation index; PSG, polysomnography; PSQ, pediatric sleep questionnaire; SD, standard deviation. T-1← History of the symptom (apnee-T-1←, snoring-T-1←; T-1≤6m, ≤ 6 months; T-1>6m, > di 6 mesi); PSG-T0, age of prescription of PSG; PSG-T0-1, waiting time to perform PSG; PSG-T0-1≤ 3m, waiting time for PSG ≤ 3 Months; PSG-T0-1> 3m, waiting time for PSG > 3 Months; PSG-T1, PSG Running Age.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



