
Submitted:
13 September 2024
Posted:
13 September 2024
You are already at the latest version
Abstract
Background: The acute hemodynamic response to isometric exercise in hypertensive patients ischemic heart disease (IHD) has been poorly investigated. The aim of this study was to assess acute changes on left ventricular myocardial work (MW) during isometric bilateral knee extension in patients with IHD. Methods. Twenty stable hypertensive patients with IHD and ten healthy, age-matched controls (HC) were enrolled. All subjects performed an isometric knee extension exercise, at 30% of their maximal voluntary contraction. The effort was maintained for three minutes or until exhaustion. At baseline, at peak exercise and after 10 minutes of recovery, echocardiography evaluation was perforned, blood pressure (BP) and heart rate (HR) were measurement. Results. The exercise was well tolerated by all subjects. At peak exercise: systolic BP in the IHD was significantly higher than HC (37.6± 7.2 vs 8.4±2.3 mmHg; p = 0.002). HC group had a greater increase in HR than IHD (19.7±6.2 vs 8.4±2.2 bpm; p = 0.009). E/E’ ratio increased in IHD and was unchanged in control. Global work index increased significantly in IHD compared to HC (+15% vs +3%; p 0.026). Global constructive work increased significantly in IHD compared to HC (+29.8% vs +7.4 respectively, p 0.031). Global waste work increased by 92.3% in IHD and was unchanged in HC. Global work efficiency decreased in IHD (-18%) while was unchanged in HC (between-groups p 0.019). Stroke volume decreased in IHD. and was unchanged in HC. Cardiac output was unchanged in IHD while it increased in HC. Conclusion: In patients with hypertension and underlying IHD, an acute isometric load caused a great increase in systolic BP and LV filling pressure. It follows a mostly ineffective increase of MW that fails to maintain stroke volume.
Keywords:
Isometric exercise
; ischemic heart disease
; myocardial work
1. Introduction
Exercise training is a well-established non pharmacologic intervention for the prevention and treatment of hypertension [1,2]. Though, traditionally, most studies have focused on the anti-hypertensive effects of continuous, moderate-intensity, aerobic exercise [3], beneficial effects elicited by resistance training or protocols combining aerobic and resistance training have also been underlined [4,5]. Resistance exercise that includes dynamic and isometric contractions, appears to be particularly indicated for hypertensive aged patients carrying chronic conditions, including those with cardiovascular diseases [2]. In these patients resistance exercise plays several beneficial effects, beyond the reduction of blood pressure (BP), including increased skeletal muscle trophism and strength, improvement of body composition and prevention of skeletal muscle loss. These effects help patients to preserve their ability to perform daily activities, and ultimately, contribute to improve their quality of life [6,7,8,9]. Isometric exercise (IE), characterized by sustained muscular contractions in which the length of the muscle does not change, has emerged as a convenient, time-efficient intervention whose anti-hypertensive effects have been supported in multiple meta-analyses and appear to be similar to or greater than those observed in traditional aerobic exercise training [10,11,12]. However, IE has been less extensively utilized than dynamic resistance exercise in the cardiac prevention and rehabilitation fields, the major concern being the fear of incurring in an excessive rise in BP, with a correspondent unwanted increase in cardiac work. This aspect seems to be particularly relevant for hypertensive patients with underlying ischemic heart disease (IHD), since maintaining a low double product during exercise is a primary therapeutic goal in this context. However the actual cardiac load occurring during IE is variable since the rise of BP depend on the mass of the muscle involved as well as on the intensity of the effort. It has been shown that, when using small-muscle mass, isometric and dynamic resistance exercises evoked equal increases in BP [13] and some authors have encouraged the handgrip IE prescription in hypertensive IHD patients because they observed adequate hemodynamic responses [14,15]. Conversely, the hemodynamic response to bilateral isometric knee extension in hypertensive patients with IHD has been less extensively studied. Pursuing the idea of implementing the use of IE for counteracting hypertension in patients undergoing secondary prevention/rehabilitation programs, it is mandatory to preliminary assess the tolerability of IE in IHD patients. This means to investigate how performing IE acutely affects cardiac function and contractile efficiency in patients evaluated before entering cardiac rehabilitation programs. A non-invasive detailed reconstruction of myocardial function is today possible trough speckle tracking echocardiography and in particular trough myocardial work (MW) that has been introduced in recent years as a non-invasive measurement of left ventricular (LV) function. MW uses a combination of LV global longitudinal strain (GLS) and systolic BP to obtain LV pressure-strain loops [16,17]. It provides valuable information regarding myocardial contraction efficiency that are particularly relevant in the interpretation of the myocardial performance during exercise [18]. In the present study we investigated changes in myocardial efficiency (MWE) as part of the acute hemodynamic response elicited by bilateral isometric knee extension exercise in untrained hypertensive patients with IHD and compared them with changes occurring in healthy subjects performing the same exercise.
2. Materials and Methods
Population. The study included a total of 30 subjects. Twenty of them were patients with diagnosed IHD and ten were healthy age-matched controls. Patients with IHD were referring to the outpatient’s service of cardiac rehabilitation of San Raffaele IRCCS of Rome. The following inclusion criteria were adopted: age over 45 years; previous diagnosis (made at least 6 months before recruitment) of arterial hypertension and of IHD, the latter including: history of stable angina, unstable angina/myocardial infarction; previous percutaneous coronary revascularization or previous coronary artery bypass grafting. Patients had to be in optimal medical therapy and in stable clinical conditions and in stable sinus rhythm for at least three months. The following exclusion criteria were adopted: myocardial ischemia or threatening arrhythmias during the resting assessment and/or during the ergometric test; previous diagnosis of heart failure; permanent atrial fibrillation; baseline blood pressure levels at rest over 160/100 mmHg; anemia with haemoglobin levels below 11 g/dl; concomitant diagnosis of chronic respiratory disease with documented FEV1 below <50%; previous diagnosis peripheral artery disease with exercise-limiting claudication; poor acoustic window. Subjects with concomitant severe heart valve diseases, previous diagnosis of hypertrophic cardiomyopathy, subjects being recently (less than six months) engaged in exercise training programs and those who declared to practice spontaneously regular exercise (more than 2 sessions/week) were also excluded. Healthy control were found among relatives of patients enrolled, and among relatives of the hospital staff. They did not have to take hemodynamic drugs and did not have to practice regular sports. The study complied with the Declaration of Helsinki and was approved by the local Ethics Committee of San Raffaele IRCCS (protocol number 18/2023). All patients gave written informed consent before entering the study.
Study design. The study flow chart is summarized in Figure 1. All participants were screened in a preliminarily visit. During this visit clinical history, anthropometric data, including body mass index (BMI), resting heart rate (HR) and BP were collected. Subjects meeting the inclusion and exclusion criteria were then invited to join the study and those who agreed and signed up the informed consent were then reconvened for a second visit that was scheduled within a week from the first one. During the second visit patients with IHD performed a symptom-limited ergometric test on a byke (Mortara Instrument, Casalecchio Di Reno, Italy), to rule out ischemic or arrhythmic conditions. In the same day all subjects were familiarized with the dynamometer and completed a double-leg isometric extension exercise test. For each subject, the experimental session was scheduled within another week from the second visit. Subjects of the HC group were tested on a non-working day.
Experimental sessions were held in the gym of the rehabilitation facility of S. Raffaele IRCCS. All tests were performed on a knee flex/extension dynamometer (Technogym Wellness System, Technogym, Cesena, Italy) and participants were asked to perform isometric double-leg (knee extension) exercise. All participants were asked to avoid performing strenuous exercise within 24 hours and agreed to abstain from alcohol and caffeine for a 12-hour period prior to the experimental session. Participants were seated on the dynamometer and the seat was adjusted appropriately for each individual so that the axis of rotation around the dynamometer shaft was adjacent to the lateral femoral condoyle of the subject’s right leg. Subjects were with their knee bent at a 90° angle. Both legs were positioned underneath the knee extension/flexion attachment arm of the dynamometer. Participants positioned their arms along their trunk so that the left arm did not obstruct the sonographer responsible for acquiring the echocardiographic data that was positioned on the left side of the examined subject. A manual sphygmomanometer cuff was placed on the right arm. The test for determining maximal voluntary contraction (MVC) consisted of 3 maximal contractions, each one lasting 3–5-s each, with 1-min rest between contractions [19]. During each contraction subjects were encouraged by the evaluator to exert their maximal efforts. The maximum force generated by the patient was recorded for each trial, and the maximum value over the three trials was used as the final measurement [18]. After the test subjects were asked to rest for 30 minutes, at the end of which they performed IE: the intensity of the exercise was set at 30% of their MVC and the duration of the exercise was 3 minutes. During the effort subjects were invited to breath regularly in order to avoid the Valsalva maneuver. Echocardiographic assessments and BP measurements were made at rest, during the exercise and after 10 minutes of recovery. The ultrasound acquisition during the exercise phase was started 90 second from the beginning of the exercise, since we estimated that it would take about one minute to carry out all the required assessments.
Transthoracic Echocardiography: the echocardiography was performed with patients in the sitting position with the sonographer placed on the left side of the subject examined. A cardiovascular ultrasound Vivid E95® (GE Healthcare, Chicago, IL) with a 4.0-MHz transducer was used for the echocardiography examinations during the entire study. Imaging windows and measurements were obtained according to the current guidelines of European Association of Cardiovascular Imaging [20]. During each examination, one-lead electrocardiography monitoring was placed in the chest of the subject. After the imaging acquisition, all the echocardiographic images were digitally stored and their analysis was performed offline. During the review process, an experienced technician, performed deformation measures by using a proprietary software (version 10.8, EchoPAC; GE Vingmed Ultrasound, Norway). Measures of left ventricular end-diastolic volume (LVEDV) and left ventricular end-systolic volume (LVESV) were obtained from the apical two and four chamber windows; LVEF was then calculated by using the modified Simpson’s method. Stroke volume (SV)was then calculated as EDV−ESV, cardiac output (CO) as HR × SV, and ejection fraction (EF) as EF = (EDV−ESV)/EDV). Measures of left atrium (LA) volume were obtained from standard apical four-chamber and three-chamber views at end of the systole, before the opening of mitral valve and the biplane Simpson’s method of disks was adopted. LA volume index (LAVI) was calculated by dividing LA volume by the body surface area of patients. The E/A ratio was the ratio between E wave, corresponding to peak left ventricle filling velocity in early diastole, during atrial relaxation, and A wave corresponding to peak velocity flow in late diastole during the atrial contraction. Colour tissue Doppler tracings were performed in the 4-chamber view with the range gate placed at the lateral mitral annular segments. The E/E’ ratio was the ratio between E wave velocity and the average between septal and lateral LV E’ wave velocities. Measurements for LV global longitudinal strain (LVGLS) were obtained from through two-, three-, and four-chamber views. Despite the software automatically detected LV endocardial boundaries, whenever deemed appropriate, the images were edited in order to be conformed to the visualized LV boundaries. The maximum negative value of strain during systole measured by the software was considered the maximum contractility for each segment. The average of the values from each segment was then calculated to determine LVGLS. LA strain was measured through two and four-chamber views. Measures of LA deformation tracking were carried out by using the R-R gating that uses the R wave as a starting point. The software traced automatically the endocardial and epicardial contours of the LA. Again, if necessary, manual adjustments were also made. The automatic algorithm placed a set of control points on the middle curve of the myocardial wall in the reference phase based on the drawn endocardial and epicardial contours. Longitudinal strain curves were generated for each segment by the software program and an average curve of each segment was calculated. LA reservoir strain, conduit strain and contractile strain were obtained from the subdivision of longitudinal strain measurements. PALS was measured as a positive peak during LV systole at the end of atrial diastolic phase; PACS was measured as a positive peak during early LV diastole, right before the start of the atrial systolic phase [26]. MW was evaluated from mitral valve closure to mitral valve opening. A 17-segments bull's eye with the segmental and global work index (GWI) corresponding to the area within the curve total work from mitral valve closure to mitral valve opening) values was obtained. We also achieved global constructive work (GCW) corresponding to work performed during shortening in systole adding negative work during lengthening in isovolumetric relaxation), global wasted work (GWW) corresponding to negative work performed during lengthening in systole adding work performed during shortening in isovolumetric relaxation; global work efficiency (GWE) corresponding to constructive work divided by the sum of constructive and wasted work. Pulse-wave Doppler recordings at mitral valve and aortic valve level was used to set valvular event times. and then confirmed by 2D evaluation of the apical long-axis view [21].
Statistical Analysis
Data were expressed as mean ± SD. The assumption of normality was checked using Shapiro–Wilks hypothesis test. Data obtained at rest, during exercise and at recovery were compared by using repeated measures two-way ANOVA, with Bonferroni corrections for post hoc testing. The Pearson correlation coefficient test was used to measure the strength of the linear association between two variables. The level of significance was set at p < 0.05. The statistical program, IBM SPSS Statistics v26.0, was used for the processing, presentation, and statistical analysis of the data.
3. Results
The exercise was well tolerated by all participants and no side effects occurred during the experimental sessions. Muscle exhaustion, during the isometric effort, occurred in eight IHD patients and in none of the HC group. Characteristics of patients and controls are summarized in Table 1. Sixteen out of 20 patients of the IHD groups had a previous myocardial infarction. Patients of the IHD groups were taking on average 2.3±1.1 drugs for treating hypertension. All of them were taking antiplatelet agents, statins and betablockers. Four subjects of the HC had hypercholesterolemia; three of them were taking statins and one ezetimibe. At rest, values of EF, LVGLS, GWI and GCW, were significantly higher while GWW and GWE were lower in HS compared to IHD. GWE was significantly higher in HS compared to IHD. The double product was similar between IHD and HC groups.
At peak exercise, systolic BP presented a greater increase in the IHD group comped to HC (37.6± 7.2 vs 8.4±2.3 mmHg; p 0.002); diastolic BP presented a greater increase in the IHD group compared to HC (19.4±4.6 vs 7.4 ±2.7 mmHg; p 0.036). HR presented a greater increase in the HC group compared to IHD (19.7±6.2 vs 8.4±2.2 bpm; p 0.009). Double product increased in a similar way in the two groups. LVDV and LVSV decreased significantly in the IHD while were unchanged in the HC (-18.1±4.6 and -9.3±2.7 vs 0.5±0.6 and -0.8±0.2 respectively; p 0.041 and p 0.038). No significant changes occurred in LVEF and in the two groups. LVGLS decreased significantly in the IHD and was unchanged in HC (Table 2). Deceleration time decreased significantly and E/E’ ratio increased significantly compared to rest values only in the IHD group. PALS decreased significantly in IHD compared to HC. PACS at peak exercise was unchanged compared to the rest condition, in both groups. GWI increased significantly in IHD compared to HC (+15% vs +3%; p 0.026). GCW increased of 30.4% in the IHD and was unchanged in the HC group HC (+29.8% vs +7.4 respectively, p 0.031). GWW increased of 91.4% in the IHD group and was unchanged in the HC group (between-groups p 0.0001). GWE decreased of 18% in the IHD group and was unchanged in HC (between-groups p 0.019) (Figure 2). SV decreased in IHD and was unchanged in HC. CO was unchanged in IHD while it increased in HC (Figure 3). In the IHD group, changers in GWW were significantly related to changes in E/E’ ratio (r= 0.45; p 0.003).
4. Discussion
A growing body of literature indicates that IE training is capable of producing BP reductions greater than that observed following the currently recommended exercise guidelines and similar to that of standard anti-hypertensive monotherapy [22]. However, in hypertensive patients with underlying IHD, there is a substantial risk that IE can lead to a maladaptive acute response with abnormal rise of BP and excessive increase in myocardial oxygen consumption [23,24]. A preliminary assessment of the acute hemodynamic response to IE can help in order to identify the best tolerated isometric protocol for these patients. In the present study we investigated the acute hemodynamic response evoked by isometric knee extension performed at 30% of MVC in hypertensive patients with IHD and compared it with the response evoked by the same exercise in HC. We focused particularly on changes in myocardial work assessed non-invasively by speckle tracking echocardiography. We observed that the response of IHD patients was characterized by a significant increase in systolic and diastolic BP, a modest increase in HR and by an increase in inotropism indicated by a significant rise in GWI. However, the MW increase model was dysfunctional with a clear prevalence of GWW over GCW and a consequent significant reduction in GWE. The exercise-induced rise of GWW meant that the increased contractility did not translate into hemodynamically productive work; at the contrary, the significant increase of LV uncoordinated contractions determined a significant loss of myocardial cells energy, with a reduction of contraction efficiency at peak exercise [25]. This LV inefficient contraction was associated with a decrease in SV at peak exercise. The decrease in SV, together with the inadequate increase in HR, was responsible for the lack of increase in CO at peak exercise registered in this group. Conversely in HC, at peak exercise there were not changes in GWI and GWE; the increase of CO was driven by a significant increase in HR and only modest changes in systolic and diastolic BP occurred in comparison to the rest condition. Interestingly, we found that in the IHD group resting values of GWI, GCW, and GWE were lower while GWW was higher compared to HC. These result are consistent with previous studies showing that MW indices are impaired in patients developing LV ischemic remodeling after myocardial infarction and in those undergoing coronary revascularization regardless of the presence of heart failure [26,27]. The resting reduction of GWE has been ascribed to a chronically impairment of energy metabolism that occurs in the remodeled myocardium [28] and has been associated to a lower performance during exercise in athletes [29]. We think that this research add new insight in the usefulness of measure MW indices for describing the acute hemodynamic response to IE in patients with IHD undergoing cardiac rehabilitation. The inotropic activation that we documented in IHD, together with the significant increase in systolic BP, can be ascribed to the exercise-mediated activation of sympathetic nervous system (SNS). An abnormal activation of SNS leading to an increase in systemic vascular resistance and to an inotropic response has been widely described during IE [30,31]. However the involvement of SNS remains speculative in the present study since we did not measure catecholamine levels or other indices of SNS activation. The hemodynamic response to IE that we observed in IHD was also characterized by a blunted increase in HR that we attributed to chronotropic incompetence determined by the systematic use of betablockers. In experimental models, when subjects with normal LV function, and with HR fixed at rest values, performed IE, SV increased and compensated for the lack of a chronotropic response, allowing for CO to rise and to produce the pressor response [32,33]. In such conditions, Nobrega et al. [33] demonstrated that a combination of increased contractility and the Frank-Starling mechanism were responsible for that increase in SV during IE. Conversely, in our study, in IHD patients SV at peak exercise decreased leaving us to hypothesize that, in pathologic conditions, these two mechanisms were not able to provide sufficient compensation. We found that in the IHD group LVEDV decreased at peak exercise compared to rest values: this would imply that Frank-Starling mechanism was not used by these patients. The decrease in LVDD denotes an impaired LV diastolic filling that may in part be related to the reduction in venous return arising from blood retention within the contracting muscles. Moreover an abnormal increase in LV filling pressures during IE may also have played a role in reducing LV filling. We observed that at peak exercise E/E’ ratio was higher and deceleration time was significantly shorter compared to rest values in the IHD group. Both of these finding suggest that IE was responsible for a significant increase in LV filling pressure in this group [34]. These results were also mirrored at atrial level by the reduction of PALS values compared to rest, indicating an increased LA pressure[35]. Taken together these data suggest the occurrence of LV diastolic dysfunction during the exercise phase in IHD. The significant corelation that we found between changes in GWW and changes in E/E’ ratio let us hypothesized that the rise in LV filling pressure further worsened the already impaired LV contractile efficiency. This result seems to comply with other recent studies. D’Andrea et al. [18] showed that GWE at rest was closely related to maximal watts reached as well as to LV E/E’. It should be noted that in the present study we documented a significant increase in BP in the IHD group while only modest changes in BP occurred in HC. Considering that in this research IE involved large muscle groups, a considerable rise in BP during IE was an expected result; in fact it has been shown that IE performed with larger muscle masses elicit greater BP responses than those involving smaller muscles [36]. However the probability to incur in an exaggerate BP rise is higher in hypertensive than in normotensive subjects [37] and this could explain the different BP response that we observed in IHD and HC. The majority of studies investigating the effects of IE research has utilised a handgrip protocol, generally performed at 30% of the participant’s MVC. Results of our study match perfectly previous research, carried out using invasive hemodynamic monitoring, and in which two different patterns of hemodynamic responses during IE have been described [22,38]: a first pattern, like that we encountered in HC, was characterized by a modest rise in systolic BP coupled with a rise in cardiac index, a significant increase in HR and no changes in systemic vascular resistance. A second pattern was instead characterized by a conspicuous rise in systolic BP, coupled with little or no change in cardiac index and by a small increase in HR. This latter pattern, that was close to that we described in IHD in the present study, has been typically observed in subjects with a certain degree of LV dysfunction, including hypertensive subjects with LV hypertrophy as well as in patients with IHD [24,39]. Limitations: the results of the present research have been obtained in a small group of subjects and further confirmations in larger studies are needed. The study tested the hemodynamic response to an isometric exercise that involved bilateral leg extension and a load corresponding to 30% of the MVC. Clearly we cannot rule out that IE involving different muscle groups or performed different intensities of IE could evoke a different myocardial response. For example, it has been demonstrated that BP increases are proportional to the amount of skeletal muscle that is contracting and that handgrip requires less BP increase than leg extension [37]. In this study, a very small proportion of subjects inf both groups were females; therefore, we think that our results cannot be generalized to the female gender.
5. Conclusions
In hypertensive patients with underlying IHD, the cardiac response occurring during bilateral isometric knee extension was characterized by a dysfunctional increase in contractility that, together with a blunted chronotropic response, prevented the increase in cardiac output. Further studies are needed for identifying the best tolerated “dose” of IE in the context of cardiac rehabilitation.
Author Contributions
M.A.P., F.I., and G.C., contributed to the conceptualization of the paper; V.M., C.C., D.D.B, M.C, V.D., and S.V., prepared the initial draft after acquisition, analysis, and interpretation of the results; V.M., M.V., and G..M. substantively revised it. All authors have read and agreed to the submitted version of the manuscript.
Funding
This work was supported by funding of the Italian Ministry of Health [Ricerca corrente]
Institutional Review Board Statement
In The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Ethics Committee of San Raffaele IRCCS of Rome (protocol code 18/2023).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been also obtained from the patients to publish this paper
Data Availability Statement
The data presented in this study are available on request from the corresponding authors.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Pelliccia A, Sharma S, Gati S, Bäck M, Börjesson M, Caselli S, Collet JP, Corrado D, Drezner JA, Halle M, Hansen D, Heidbuchel H, Myers J, Niebauer J, Papadakis M, Piepoli MF, Prescott E, Roos-Hesselink JW, Graham Stuart A, Taylor RS, Thompson PD, Tiberi M, Vanhees L, Wilhelm M; ESC Scientific Document Group. 2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease. Eur Heart J. 2021 Jan 1;42(1):17-96. Erratum in: Eur Heart J. 2021 Feb 1;42(5):548-549. 10.1093/eurheartj/ehaa835. [CrossRef]
- Mancia G, Kreutz R, Brunström M, Burnier M, Grassi G, Januszewicz A, Muiesan ML, Tsioufis K, Agabiti-Rosei E, Algharably EAE, Azizi M, Benetos A, Borghi C, Hitij JB, Cifkova R, Coca A, Cornelissen V, Cruickshank JK, Cunha PG, Danser AHJ, Pinho RM, Delles C, Dominiczak AF, Dorobantu M, Doumas M, Fernández-Alfonso MS, Halimi JM, Járai Z, Jelaković B, Jordan J, Kuznetsova T, Laurent S, Lovic D, Lurbe E, Mahfoud F, Manolis A, Miglinas M, Narkiewicz K, Niiranen T, Palatini P, Parati G, Pathak A, Persu A, Polonia J, Redon J, Sarafidis P, Schmieder R, Spronck B, Stabouli S, Stergiou G, Taddei S, Thomopoulos C, Tomaszewski M, Van de Borne P, Wanner C, Weber T, Williams B, Zhang ZY, Kjeldsen SE. 2023 ESH Guidelines for the management of arterial hypertension The Task Force for the management of arterial hypertension of the European Society of Hypertension: Endorsed by the International Society of Hypertension (ISH) and the European Renal Association (ERA). J Hypertens. 2023 Dec 1;41(12):1874-2071. [CrossRef]
- Whelton SP, Chin A, Xin X, He J. Effect of aerobic exercise on blood pressure: a meta-analysis of randomized, controlled trials. Ann Intern Med. 2002 Apr 2;136(7):493-503. [CrossRef]
- Cornelissen VA, Fagard RH, Coeckelberghs E, Vanhees L. Impact of resistance training on blood pressure and other cardiovascular risk factors: a meta-analysis of randomized, controlled trials. Hypertension. 2011 Nov;58(5):950-8. [CrossRef]
- López-Valenciano A, Ruiz-Pérez I, Ayala F, Sánchez-Meca J, Vera-Garcia FJ. Updated systematic review and meta-analysis on the role of isometric resistance training for resting blood pressure management in adults. J Hypertens. 2019 Jul;37(7):1320-1333. [CrossRef]
- Mcleod JC, Stokes T, Phillips SM. Resistance Exercise Training as a Primary Countermeasure to Age-Related Chronic Disease. Front Physiol. 2019 Jun 6;10:645. [CrossRef]
- Paluch AE, Boyer WR, Franklin BA, Laddu D, Lobelo F, Lee DC, McDermott MM, Swift DL, Webel AR, Lane A; on behalf the American Heart Association Council on Lifestyle and Cardiometabolic Health; Council on Arteriosclerosis, Thrombosis and Vascular Biology; Council on Clinical Cardiology; Council on Cardiovascular and Stroke Nursing; Council on Epidemiology and Prevention; and Council on Peripheral Vascular Disease. Resistance Exercise Training in Individuals With and Without Cardiovascular Disease: 2023 Update: A Scientific Statement From the American Heart Association. Circulation. 2024 Jan 16;149(3):e217-e231. [CrossRef]
- Fan Y, Yu M, Li J, Zhang H, Liu Q, Zhao L, Wang T, Xu H. Efficacy and Safety of Resistance Training for Coronary Heart Disease Rehabilitation: A Systematic Review of Randomized Controlled Trials. Front Cardiovasc Med. 2021 Nov 5;8:754794. [CrossRef]
- Marzolini S, Oh PI, Brooks D. Effect of combined aerobic and resistance training versus aerobic training alone in individuals with coronary artery disease: a meta-analysis. Eur J Prev Cardiol. 2012 Feb;19(1):81-94. [CrossRef]
- Carlson, D. J., Dieberg, G., Hess, N. C., Millar, P. J., & Smart, N. A. (2014). Isometric exercise training for blood pressure management: A systematic review and meta-analysis. Mayo Clinic Proceedings. 2014;89; 327–334. [CrossRef]
- López-Valenciano, A., Ruiz-Pérez, I., Ayala, F., Sánchez-Meca, J., & Vera-Garcia, F. J. Updated systematic review and meta-analysis on the role of isometric resistance training for resting blood pressure management in adults. Journal of Hypertension. 2019;37:1320–1333. [CrossRef]
- Cornelissen VA, Smart NA. Exercise training for blood pressure: a systematic review and meta-analysis. J Am Heart Assoc. 2013 Feb 1;2(1):e004473. [CrossRef]
- Kounoupis A, Papadopoulos S, Galanis N, Dipla K, Zafeiridis A. Are Blood Pressure and Cardiovascular Stress Greater in Isometric or in Dynamic Resistance Exercise? Sports (Basel). 2020 Mar 28;8(4):41. [CrossRef]
- Goessler K, Buys R, Cornelissen VA. Low-intensity isometric handgrip exercise has no transient effect on blood pressure in patients with coronary artery disease. J Am Soc Hypertens. 2016 Aug;10(8):633-9. [CrossRef]
- Gois MO, Simões RP, Porta A, Kunz VC, Pastre CM, Catai AM. Cardiovascular responses to low-intensity isometric handgrip exercise in coronary artery disease: effects of posture. Braz J Phys Ther. 2020 Sep-Oct;24(5):449-457. [CrossRef]
- Papadopoulos K, Özden Tok Ö, Mitrousi K, Ikonomidis I. Myocardial Work: Methodology and Clinical Applications. Diagnostics (Basel). 2021 Mar 22;11(3):573.
- Boe E, Skulstad H, Smiseth OA. Myocardial work by echocardiography: a novel method ready for clinical testing. Eur Heart J Cardiovasc Imaging. 2019 Jan 1;20(1):18-20. [CrossRef]
- D'Andrea A, Carbone A, Radmilovic J, Russo V, Fabiani D, Maio MD, Ilardi F, Giallauria F, Caputo A, Cirillo T, Bossone E, Picano E. Myocardial Work Efficiency in Physiologic Left Ventricular Hypertrophy of Power Athletes. J Cardiovasc Echogr. 2022 Jul-Sep;32(3):154-159. [CrossRef]
- Meldrum D, Cahalane E, Conroy R, Fitzgerald D, Hardiman O. Maximum voluntary isometric contraction: reference values and clinical application. Amyotroph Lateral Scler. 2007 Feb;8(1):47-55. [CrossRef]
- Nagueh SF, Smiseth OA, Appleton CP, Byrd BF 3rd, Dokainish H, Edvardsen T, Flachskampf FA, Gillebert TC, Klein AL, Lancellotti P, Marino P, Oh JK, Alexandru Popescu B, Waggoner AD; Houston, Texas; Oslo, Norway; Phoenix, Arizona; Nashville, Tennessee; Hamilton, Ontario, Canada; Uppsala, Sweden; Ghent and Liège, Belgium; Cleveland, Ohio; Novara, Italy; Rochester, Minnesota; Bucharest, Romania; and St. Louis, Missouri. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging. 2016 Dec;17(12):1321-1360. [CrossRef]
- Papadopoulos K, Özden Tok Ö, Mitrousi K, Ikonomidis I. Myocardial Work: Methodology and Clinical Applications. Diagnostics (Basel). 2021 Mar 22;11(3):573.
- Edwards JJ, Coleman DA, Ritti-Dias RM, Farah BQ, Stensel DJ, Lucas SJE, Millar PJ, Gordon BDH, Cornelissen V, Smart NA, Carlson DJ, McGowan C, Swaine I, Pescatello LS, Howden R, Bruce-Low S, Farmer CKT, Leeson P, Sharma R, O'Driscoll JM. Isometric Exercise Training and Arterial Hypertension: An Updated Review. Sports Med. 2024 Jun;54(6):1459-1497. [CrossRef]
- Taylor KA, Wiles JD, Coleman DD, Sharma R, Oʼdriscoll JM. Continuous Cardiac Autonomic and Hemodynamic Responses to Isometric Exercise. Med Sci Sports Exerc. 2017 Aug;49(8):1511-1519. [CrossRef]
- Hanson P, Nagle F. Isometric exercise: cardiovascular responses in normal and cardiac populations. Cardiol Clin. 1987 May;5(2):157-70.
- Russell K, Eriksen M, Aaberge L, Wilhelmsen N, Skulstad H, Gjesdal O, Edvardsen T, Smiseth OA. Assessment of wasted myocardial work: a novel method to quantify energy loss due to uncoordinated left ventricular contractions. Am J Physiol Heart Circ Physiol. 2013 Oct 1;305(7):H996-1003. [CrossRef]
- Lustosa R.P., van der Bijl P., El Mahdiui M., Montero-Cabezas J.M., Kostyukevich M.V., Marsan N.A., Bax J.J., Delgado V. Noninvasive Myocardial Work Indices 3 Months after ST-Segment Elevation Myocardial Infarction: Prevalence and Characteristics of Patients with Postinfarction Cardiac Remodeling. J. Am. Soc. Echocardiogr. 2020;33:1172–1179. [CrossRef]
- El Mahdiui M, van der Bijl P, Abou R, Ajmone Marsan N, Delgado V, Bax JJ. Global Left Ventricular Myocardial Work Efficiency in Healthy Individuals and Patients with Cardiovascular Disease. J Am Soc Echocardiogr. 2019 Sep;32(9):1120-1127. [CrossRef]
- Azevedo P.S., Minicucci M.F., Santos P.P., Paiva S., Zornoff L. Energy Metabolism in Cardiac Remodeling and Heart Failure. Cardiol. Rev. 2013;21:135–140. [CrossRef]
- Erevik CB, Kleiven Ø, Frøysa V, Bjørkavoll-Bergseth M, Chivulescu M, Klæboe LG, Dejgaard L, Auestad B, Skadberg Ø, Melberg T, Urheim S, Haugaa K, Edvardsen T, Ørn S. Myocardial inefficiency is an early indicator of exercise-induced myocardial fatigue. Front Cardiovasc Med. 2023 Jan 11;9:1081664. [CrossRef]
- Taylor KA, Wiles JD, Coleman DD, Sharma R, Oʼdriscoll JM. Continuous Cardiac Autonomic and Hemodynamic Responses to Isometric Exercise. Med Sci Sports Exerc. 2017 Aug;49(8):1511-1519. [CrossRef]
- MacDougall JD, McKelvie RS, Moroz DE, Sale DG,McCartney N, Buick F. Factors affecting blood pressure during heavy weight lifting and static contractions. J Appl Physiol (1985). 1992;73(4):1590---1597. [CrossRef]
- Haskell WL, Savin WM, Schroeder JS, Alderman EA, Ingles NB Jr, Daughters GT 2nd, Stinson EB. Cardiovascular responses to handgrip isometric exercise in patients following cardiac transplantation. Circ Res. 1981 Jun;48(6 Pt 2):I156-61.
- Nóbrega AC, Williamson JW, Garcia JA, Mitchell JH. Mechanisms for increasing stroke volume during static exercise with fixed heart rate in humans. J Appl Physiol (1985). 1997 Sep;83(3):712-7. [CrossRef]
- Nagueh SF. Non-invasive assessment of left ventricular filling pressure. Eur J Heart Fail. 2018 Jan;20(1):38-48. [CrossRef] [PubMed]
- Lee JH, Park JH, Hwang IC, Park JJ, Park JB. Decreased Peak Left Atrial Longitudinal Strain Is Associated with Persistent Pulmonary Hypertension Associated with Left Heart Disease. J Clin Med. 2022 Jun 18;11(12):3510. [CrossRef]
- Seals, DR. Influence of muscle mass on sympathetic neural activation during isometric exercise. J Appl Physiol (1985). 1989 Nov;67(5):1801-6. [CrossRef]
- Coneglian JC, Barcelos GT, Bandeira ACN, Carvalho ACA, Correia MA, Farah BQ, Ritti-Dias RM, Gerage AM. Acute Blood Pressure Response to Different Types of Isometric Exercise: A Systematic Review with Meta-Analysis. Rev Cardiovasc Med. 2023 Feb 10;24(2):60. [CrossRef]
- Ewing DJ, Irving JB, Kerr F, Kirby BJ. Static exercise in untreated systemic hypertension. Br Heart J. 1973 Apr;35(4):413-21. [CrossRef]
- Larsen, A.I. Strength and aerobic exercise training in coronary artery disease; it’s not “either-or.” Eur J Prev Cardiol. 2017;24(16):1686–1691. [CrossRef]
Figure 1.
Study flow-chart.
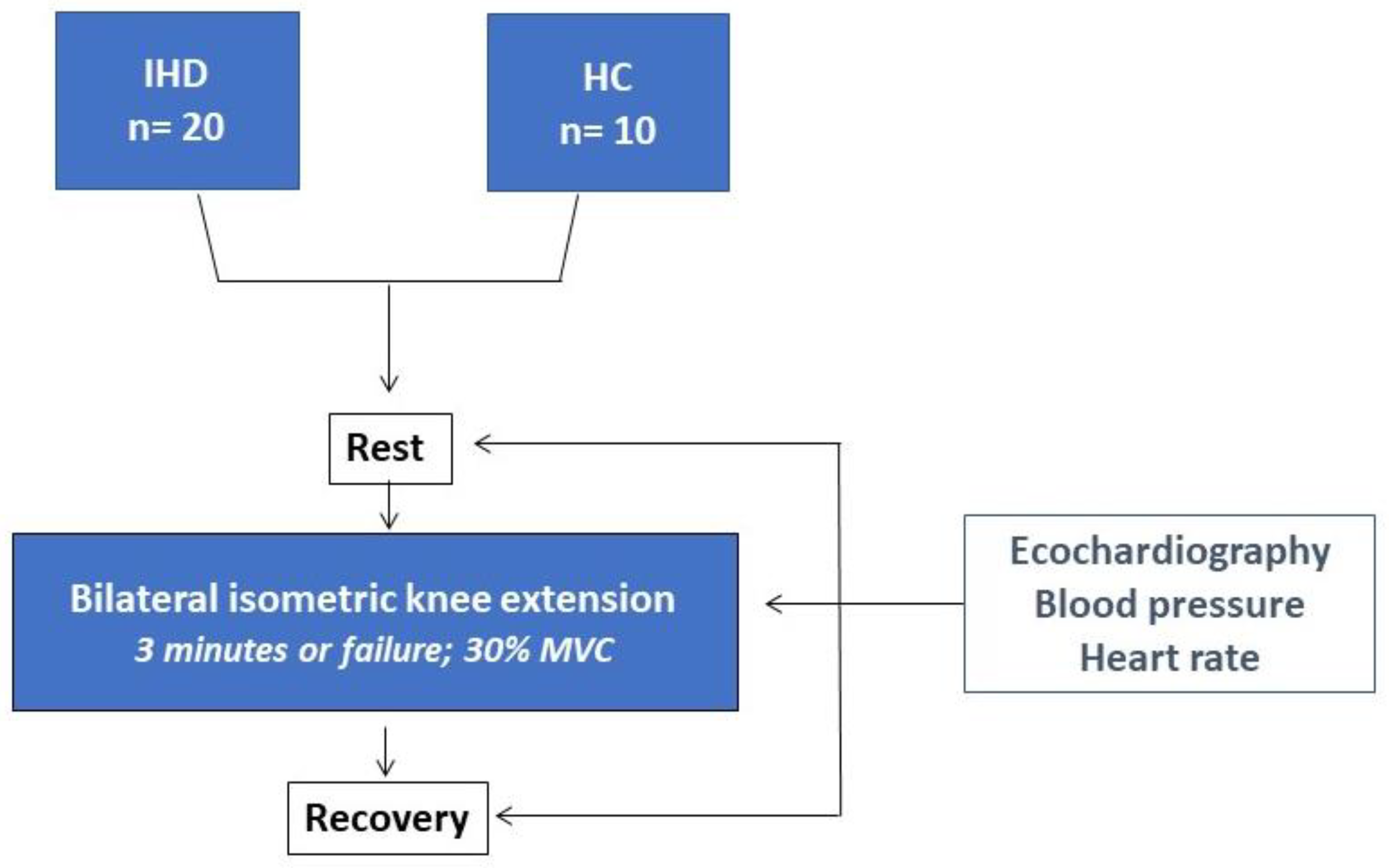
Figure 2.
Percentage changes in GWI, GWC, GWW (2A) and GWE (2B) during isometric knee extension (peak exercise vs rest) in the IHD (black bars) and HC (gray bars) groups.
Figure 2.
Percentage changes in GWI, GWC, GWW (2A) and GWE (2B) during isometric knee extension (peak exercise vs rest) in the IHD (black bars) and HC (gray bars) groups.
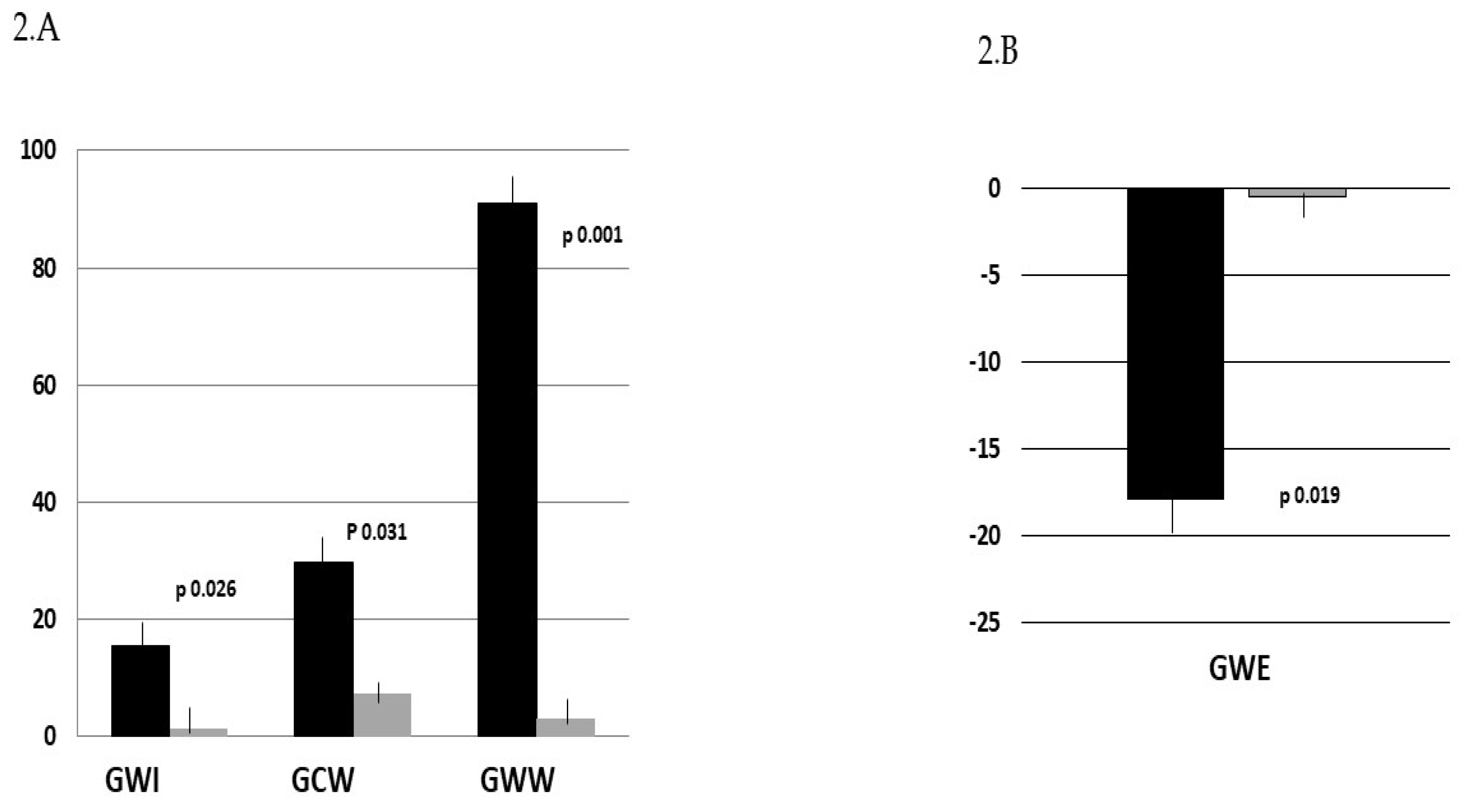
Figure 3.
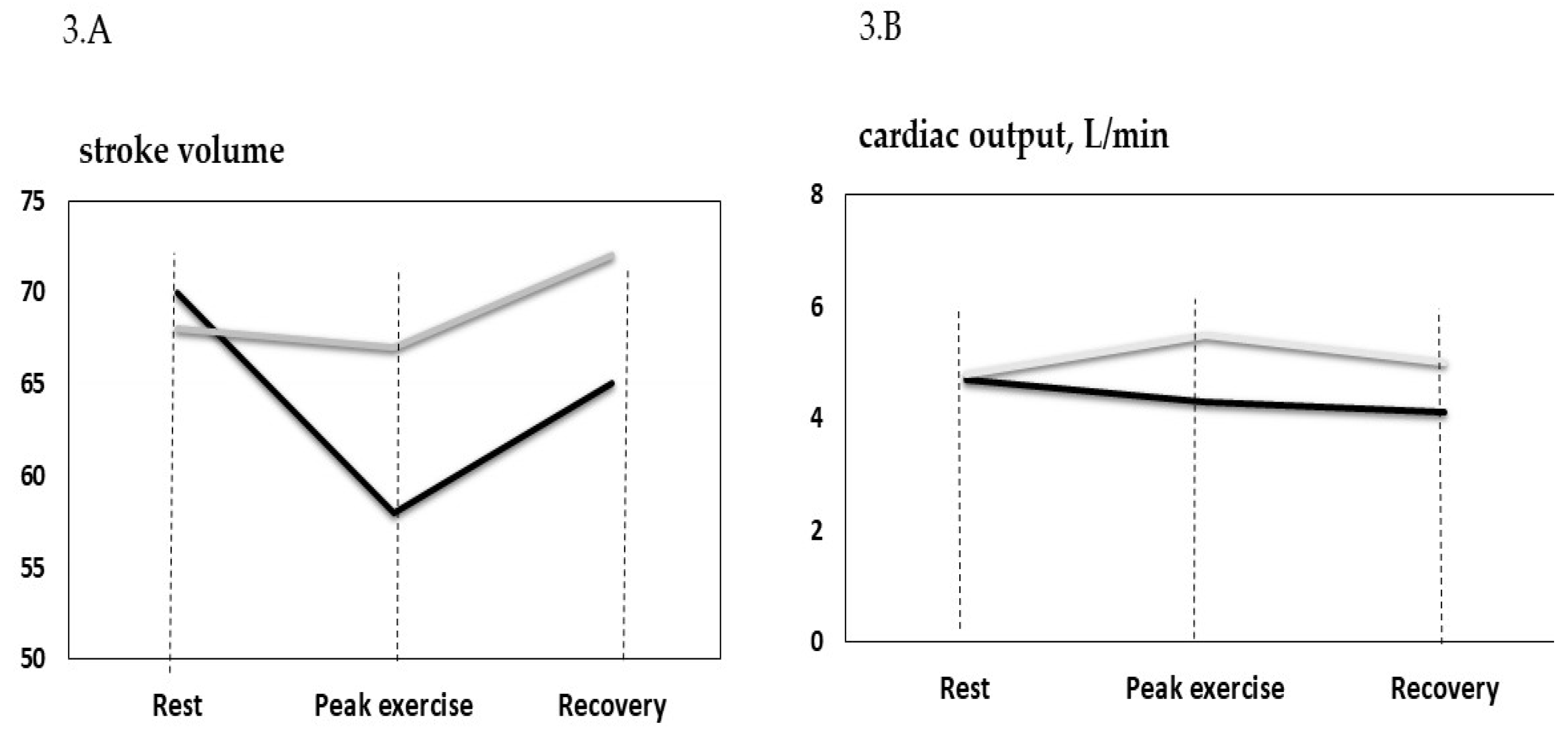

Table 1.
Anthropometric and clinical characteristics of patients.
| IHD (n= 20) | HC (n=10) | |
|---|---|---|
| Age, years | 63.4±7.5 | 61.8±4.8 |
| BMI, kg/m2 | 27.5±6.3 | 26.7±7.1 |
| Male/female | 16/4 | 7/3 |
| Previous PCI/CABG | 17/8 | - |
| EF, (%) | 50.2± 6.1† | 61.5± 7.3 |
| NT-pro BNP | 95.0±59.3 | 22 |
| Comorbidities | ||
| Carotid artery disease, n (%) | 8 (40) | - |
| Hypertension, n (%) | 20/(100) | - |
| Diabetes, n (%) | 5 (25) | - |
| Hypercholesterolemia, n (%) | 18 (90) | 4 (40) |
| Previous Smoke habit, n (%) | 13 (65) | 3 (30) |
| Treatment | ||
| Anti-platelets agents, n (%) | 20 (100) | |
| ACE-Is/ARBs, n (%) | 18 (90) | - |
| Betablockers, n (%) | 20 (100) | - |
| Diuretics, n (%) | 8 (40) | - |
| Ranolazine, n (%) | 4 (20) | |
| Ivabradine, n (%) | 1 (5) | |
| Statins, n (%) | 20 (100) | 3 (30) |
| Ezetimibe, n (%) | 12 (60) | 1 (10) |
BMI= body mass index; PCI = percutaneous coronary intervention; ACE-Is = angiotensin-converting enzyme inhibitors; ARBs = angiotensin receptor blockers;.
Table 2.
This is a table. Tables should be placed in the main text near to the first time they are cited.
Table 2.
This is a table. Tables should be placed in the main text near to the first time they are cited.
| IHD (n=20) | HC (n=10) | |||||
| Rest | Peak | Recovery | Rest | Peak | Recovery | |
| HR, b/mim | 68.7 ± 10.2 | 77.1 ± 14.6 | 63.1 ± 7.7 | 71.4 ± 12.0 | 91.1 ± 9.3*† | 75.1 ± 11.0 |
| SBP, mmHg | 124.6 ± 15.8 | 162.2 ± 34.6*† | 121.5 ± 14.6 | 124.1 ± 13 | 132.5 ± 11.2 | 120.7 ± 16.5 |
| DBP, mmHg | 77.8 ± 9.3 | 97.2 ± 20.2*† | 76.5 ± 6.0 | 75.0 ± 11.3 | 82.4 ± 7.6 | 76.3 ± 12.9 |
| DP | 8560.0±952.7 | 12505.6±883.1 | 7666.6±874.5 | 8860.7±652.8 | 12070,7±1023.2 | 9064.5±789.5 |
| Echocardiography | ||||||
| LVEDV, ml | 140.4 ± 33,4 | 122.3 ± 35.6*† | 137.1 ± 35.2 | 118.9 ± 18.2 | 119.4 ± 15.3 | 119.6 ± 16.1 |
| LVESV, ml | 70.5 ± 11.7 | 67.2 ± 16,1 | 72.2 ± 14.5 | 50.2 ± 7.9 | 49.3 ± 7.4 | 47.4 ± 6.5 |
| LVEF, % | 50.3 ± 7.4 | 49.7 ± 7.2 | 48.3 ± 5.6 | 58.4 ± 3.6 | 59.3 ± 3.2 | 59.5 ± 2.2 |
| LVGLS, % | -11.4 ± 3.8 | - 7.9 ± 2.7*† | -12.2 ± 3.8 | -18.4 ± 2.4 | -18.6 ± 2.5 | - 20.1 ± 2.6 |
| GWI, % | 1050.5 ± 412.6 | 1212.7 ± 356.4*† | 1145.6 ± 521.8 | 2033.0 ± 108.5 | 2025.7 ± 130.2 | 1573.1 ± 413.3 |
| GCW, % | 1501.3 ± 491.8 | 1958.1 ± 328.3*† | 1391.9 ± 469.0 | 2231.3 ± 85.8 | 2114.3 ± 126.7 | 2085.0 ± 348.6 |
| GWW, % | 289.7 ± 127.7 | 554.9 ± 304.7*† | 218.8 ± 128.7 | 52.7 ± 5.2 | 54.4 ± 3.1 | 58.5 ± 156.5 |
| GWE, % | 80.7 ± 11.7 | 66.4 ± 8.1*† | 82.3 ± 11.2 | 96.0 ± 2.9 | 95.3 ± 3.6 | 95.2 ± 9.6 |
| DT, ms | 248.7 ± 60.4 | 220.3 ± 57.6*† | 254.6 ± 56.3 | 194.8 ± 38.4 | 192.1 ± 53.6 | 192.4 ± 53.2 |
| E, cm/s | 48.1 ± 9.0 | 60.4 ± 15.2 | 48.5 ± 13.1 | 55.7 ± 13.4 | 55.4 ± 17.0 | 64.3 ± 12.9 |
| A, cm/s | 66.4 ± 16.1 | 77.5 ± 23.2 | 63.0 ± 15.2 | 48.6 ± 9.3 | 54.8 ± 9.8 | 51.2 ± 11.3 |
| E/A ratio | 0.75 ± 0.16 | 0.84 ± 15.2 | 0.78 ± 0.2 | 1.2 ± 0.3 | 1.5 ± 0.4 | 1.3 ± 0.4 |
| E’, cm/s | 7.4 ± 1.5 | 5.4 ± 4.4*† | 6.2± 3.1 | 11.7 ± 1.6 | 11.5 ± 2.8 | 11.9 ± 2.3 |
| E/E’ ratio | 6.7 ± 1.9 | 10.4 ± 7.4*† | 7.4 ± 2.4 | 5.2 ± 0.8 | 5.0 ± 1.1 | 6.4 ± 2.4 |
| TRV, m/s | 1.7 ± 0.4 | 1.7 ± 0.5 | 1.9 ± 0.5 | 1.7 ± 0.4 | 1.6 ± 0.4 | 1.7 ± 0.4 |
| PALS, % | 19.7 ± 8.5 | 16.8 ± 6.7 | 22.2 ± 8.4 | 22.6 ± 4.7 | 22.4 ± 8.1 | 23.7 ± 9.4 |
| PACS, % | -8.9 ± 3.5 | -11.7 ± 6.7 | -12.3 ± 8.0 | -12.6 ± 4.5 | -12.5 ± 7.5 | -13.4 ± 6.1 |
| LAVI, ml/m2 | 25.6 ± 7.2 | 21.3 ± 7.8 | 22.9 ± 7.2 | 19.4 ± 3.2 | 20.25 ± 6.2 | 18.8 ± 3.5 |
| SV, ml | 70.3 ± 14.3 | 58.5 ± 12.1*† | 64.7 ± 14.1 | 68.6 ± 11.8 | 67.1 ± 15.2 | 72.2 ± 6.1 |
| CO, l/min | 4.7 ± 1.1 | 4.3 ± 1.3† | 4.1 ± 1.1 | 4.9 ± 0.8 | 5.5 ± 0.7 | 5.2 ± 0.4 |
HR= heart rate; SBP= systolic blood pressure; DBP= diastolic blood pressure; DP= double product; CWI= global work index; GCW= global costructive work; GWW= global waste work, GWE= global work efficiency; DT= deceleration time; TRV= tricuspid regurgitation velocity; PALS= peak atrial longitudinal strain; PACS= Peak atrial contraction strain; SV= stroke volume; CO= cardiac output. *p <0.05 vs rest. † between groups p <0.005.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



